8
QUICK REFERENCE FOR HEALTHCARE PROVIDERS Ministry of Health Malaysia Academy of Medicine Malaysia Malaysian Thoracic Society

QUICK REFERENCE FOR HEALTHCARE PROVIDERS
Ministry of Health Malaysia Academy of Medicine Malaysia Malaysian Thoracic Society

Management of Tuberculosis (Third Edition)
2
KEY MESSAGES
1. Tuberculosis (TB) is a notifiable infectious disease. Timely diagnosis, prompttreatment&adherencetomedicationarekeyfactorsincombatingTB.
2. ScreeningofTBshouldbedoneinhighriskgroupsincludingallclosecontacts(especiallyhouseholdcontacts).
3. Patients with symptoms of TB should have sputum smear for acid fast bacilli(AFB),mycobacterium culture & sensitivity (C&S), & chest x-ray (CXR) done.Nucleic Acid Amplification Tests (NAAT) plays a role in rapid detection ofMycobacterium tuberculosis & multidrug-resistantTB(MDR-TB).
4. TB serology should not be used to diagnose pulmonary TB (PTB) orextrapulmonarytuberculosis(EPTB).
5. ForlatentTBinfection(LTBI),tuberculinskintest(TST)isthepreferredmethodfordiagnosis.InterferonGammaReleaseAssaymaybeusedasanalternative.Treatmentshouldbeconsideredforhighriskpatients.
6. AdailyantiTBregimenisrecommendedforbothintensive&maintenancephases.Aproperdefaultertracingsystemshouldbeinplacetodetectearlyinterruptionintreatmentandfollow-up.PoorlymanagedTBwillleadtodrug-resistantTB.
7. Fixed-DoseCombinations are preferred to separate-drugs combination for thetreatmentofTB.
8. Infants & children under 5 years of agewith close contact are at high risk ofdevelopingactiveTB.
9. ActiveTBshouldberuledoutinallHIV-positivepatients.
10. PreventivemeasuresshouldbeemployedtoreduceTBriskamonghealthcareworkers.
ThisQuickReferenceprovideskeymessagesandasummaryofthemainrecommendationsintheClinicalPracticeGuidelines(CPG)ManagementofTuberculosis(3rdEdition).
Detailsof theevidencesupporting these recommendations canbe found in theaboveCPG,availableonthefollowingwebsites:MinistryofHealthMalaysia:www.moh.gov.myAcademyofMedicineMalaysia:www.acadmed.org.myMalaysianThoracicSociety:www.mts.org.my
CLINICAL PRACTICE GUIDELINES SECRETARIATHealthTechnologyAssessmentSection
MedicalDevelopmentDivisionMinistryofHealthMalaysia
4thFloor,BlockE1,ParcelE,62590PutrajayaTel:603-88831246E-mail:[email protected]

Management of Tuberculosis (Third Edition)
3
HIGH RISK GROUPS
• CloseTBcontactsespeciallyinfants&childrenunder5yearsofage• Immunocompromised patients such as those with diabetes mellitus, HIV
infection, end-stage renal disease,malnutrition, use of immunosuppressantdrugs,etc.
• Intravenousdrugusers• Peoplelivinginovercrowdedconditions
INVESTIGATIONS • PTB
o CXR (PA) should be taken in symptomatic & high risk patients. Anyabnormalitywarrantsfurtherdiagnosticinvestigation.
o A minimum of 2 sputum samples (including 1 early morning sample)shouldbesentforTBmicroscopy.OnesampleshouldbesubjectedtoM. tuberculosisC&Stesting.
o Spontaneously produced sputum is generally used for laboratory testing;however sputum induction could be carried out if patient is unable toexpectorate.
o NAAT can be carried out for the rapid identification of M. tuberculosis anddetectionofMDR-TB.ThistestcanbecarriedoutinaTBrisklevel2laboratory.
• EPTBo Patient with EPTB should have aCXR to exclude or confirm co-existing
PTB.Imaging(ultrasound,computerisedtomography&magneticresonanceimaging)may be carried on the area of interest to demonstrate featuressuggestiveofTB.
o Bodyfluidsor tissuesamplessuspectedofTBshouldbesubjectedtoTBC&S.
o NAATtestingcanbecarriedoutonpositiveTBcultures.
TREATMENT FOR NEW TB CASES
• Fornewly-diagnosedPTB,thestandardantiTBtreatmentisa6-monthregimenconsistingofdaily2-monthofEHRZfollowedbydaily4-monthofHR.
Dosages of First-Line AntiTB Drugs
Drug
Recommended doseDaily 3 times per week
Dose (range) in mg/kg
body weight
Maximum in mg
Dose (range)in mg/kg
body weight
Daily maximum
in mg
Isoniazid(H)* 5(4-6) 300 10(8-12) 900Rifampicin(R) 10(8-12) 600 10(8-12) 600Pyrazinamide(Z) 25(20-30) 2000 35(30-40)** 3000**Ethambutol(E) 15(15-20) 1600 30(25-35)** 2400**Streptomycin(S) 15(12-18) 1000 15(12-18)** 1500**
*Pyridoxine10-50mgdailyneedstobeadded.**Dailytreatmentisthepreferredregimen.Fixed-Dose Combination Dosing
Drug Body weight Dose
Akurit-430-37kg 2tabletsdaily38-54kg 3tabletsdaily55-70kg 4tabletsdaily
Morethan70kg 5tabletsdaily
Management of Tuberculosis (Third Edition)
4
• Any deviation from the standard regimen or previously treated TB should bereferredtospecialistwithexperienceinTBmanagement.
• Durationoftreatmentmaybeprolongedincertaincircumstances:-o PersistentlyAFBsmearpositiveafter2months o EPTBo ExtensivecavitationonCXR
LATENT TB INFECTION• Only individuals who are at high risk of acquiring LTBI or developing TB
reactivationshouldbeinvestigated.TreatmentmightbeconsideredforthosewhoarepositiveforLTBI.
Positive TST for LTBI
Positive TST Reaction Types of Individual≥5mm •HIV-infectedpersons
•Organtransplantrecipients•Personswhoareimmunosuppressedforotherreasons
≥15mm •IndividualsfromcountrieswithlowincidenceofTB≥10mm •Closecontacts
•Recentimmigrants•Injectingdrugusers•Residents&employeesofhighriskcongregatesettings(suchascorrectionalfacilities,nursinghomes,homelessshelters,hospitals&otherhealthcarefacilities)
•PersonswithfibroticchangesonCXR
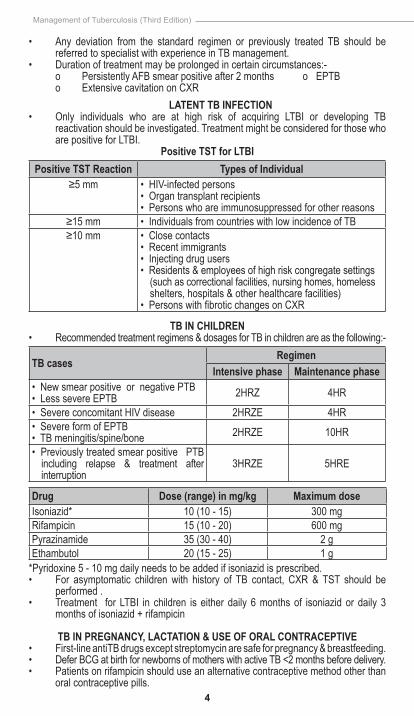
TB IN CHILDREN• Recommendedtreatmentregimens&dosagesforTBinchildrenareasthefollowing:-
TB casesRegimen
Intensive phase Maintenance phase•NewsmearpositiveornegativePTB•LesssevereEPTB 2HRZ 4HR
•SevereconcomitantHIVdisease 2HRZE 4HR•SevereformofEPTB•TBmeningitis/spine/bone 2HRZE 10HR
•PreviouslytreatedsmearpositivePTBincluding relapse & treatment afterinterruption
3HRZE 5HRE
Drug Dose (range) in mg/kg Maximum doseIsoniazid* 10(10-15) 300mgRifampicin 15(10-20) 600mgPyrazinamide 35(30-40) 2gEthambutol 20(15-25) 1g*Pyridoxine5-10mgdailyneedstobeaddedifisoniazidisprescribed.• For asymptomatic children with history of TB contact, CXR & TST should be
performed.• Treatment for LTBI in children is either daily 6months of isoniazid or daily 3
monthsofisoniazid+rifampicin
TB IN PREGNANCY, LACTATION & USE OF ORAL CONTRACEPTIVE• First-lineantiTBdrugsexceptstreptomycinaresafeforpregnancy&breastfeeding.• DeferBCGatbirthfornewbornsofmotherswithactiveTB<2monthsbeforedelivery.• Patientsonrifampicinshoulduseanalternativecontraceptivemethodotherthan
oralcontraceptivepills.

Management of Tuberculosis (Third Edition)
5
TB-HIV CO-INFECTION• Isoniazidprophylaxistherapyfor6monthsshouldbeofferedtoallHIVpatients
afteractive TB is ruled out.• Highly Active Antiretroviral Therapy (HAART) during TB treatment reduces
mortality&resultsinearliersputumsmear/cultureconversion.
CD4 count (cells/µl) Timing of HAART initiation
<50 2weeksafterstartingintensivephaseofantiTBtreatment
>50 AftercompletionofintensivephaseofantiTBtreatment
>350 ContinueantiTBtreatment&monitorCD4.CommenceHAARTifCD4drops<350cells/µl.
• Efavirenz is the preferred Non-Nucleoside Reverse Transcriptase Inhibitor(NNRTI) incombinationwith2NucleosideReverseTranscriptase Inhibitors forHIV-TBco-infection.
• ImmuneReconstitution Inflammatory Syndrome (IRIS) usually occurs within 3monthsofantiTBtreatment,typicallywithin2-12weeksafterstartingHAART:o EspeciallyinpatientswithCD4<50cells/µl,anaemiaorEPTBo Majormanifestationsarefeverorlymphadenitis
• Co-trimoxazoleprophylaxisshouldbegivenforTB-HIVco-infection&throughoutantiTBtreatment.
FLOW CHART FOR THE RECOMMENDED 6-MONTHS TREATMENT OF PTB
Visit Duration Regimen Investigations1.
2.
3.
4.
5.
Startoftreatment
2-4weeks
2months
4months
6months
HR
HR
Completionof6monthstreatment
H3R3
H3R3
EHRZ/SHRZ
EHRZ/SHRZ
FBC,RBS,RP,LFT,HIVSputumAFBdirectsmearSputumMTBC&S,CXR
LFTifnecessarySputumAFBdirectsmear*SputumMTBC&Sifsmearremainspositive,CXR
LFT
SputumAFBdirectsmear&CXRonlyifthereisnoclinicalimprovement
SputumAFBdirectsmearCXR
Patients with initial sputum smear negative should have repeat sputum smear at 2monthsofantiTBtreatment.Ifstillnegative,nofurthersputumsampleisrequired.*IfsmearAFBremainspositiveat2months,refertospecialistswithexperienceinTBmanagement,&repeatsputumAFB&sputumMTBC&Sat3months.H3R3=thriceweeklyofisoniazid&rifampicin
E-Ethambutol FBC-Fullbloodcount,RBS-RandombloodsugarH-Isoniazid RP-Renalprofile,CXR-Chestx-rayR-Rifampicin LFT-LiverfunctionTest,HIV-HIVscreeningtestZ-Pyrazinamide MTBC&S-Mycobacterium tuberculosisculture&sensitivity
• Follow-upmaynotbeconductedroutinelyaftercompletionofantiTBtreatment.Patientsshouldbewell-informedonsymptomsofTBrecurrence.

Management of Tuberculosis (Third Edition)
6
FIR
ST-L
INE
AN
TITB
MED
ICAT
ION
S: C
OM
MO
N S
IDE
EFFE
CTS
, DR
UG
-DR
UG
INTE
RA
CTI
ON
S &
HA
AR
T C
ON
CER
N
Dru
gC
omm
on S
ide
Effe
cts
Dru
g-D
rug
Inte
ract
ions
Ant
iTB
& H
AA
RT
Con
cern
Isoniazid
Skin
rash,
jaundice,
hepatitis,
drow
siness,
anorexia,
nausea,
abdominalpain,burning,n
umbnessor
tinglingsensationinthehandsorfeet
•R
eductioninphenytoin&diazepamlevel
•Increaseinthe
toxicityofanticonvulsa
nts,
benzodiazepines,
paracetamol,
serotonergic
antidepressants,w
arfarin&theophylline
Careis
neededw
hentakin
gitwithH
AART
medica
tionsthatcan
cause
peripheral
neuropathy,particularlystavudine
(d4T)&
didanosin
e(ddI)
Rifampicin
Skinrash,jaundice
,hepatitis,anorexia
,nausea,abdominalpain,orangeor
redurine&flusyndrom
e(fever,chills,
malaise,headache,bonepain)
Reductioninplasm
alevelofanti-infectives,hormone
therapy
(inclu
dingethinylestradiol,norethindrone,
tamoxifen,levothyroxine),
methadone,
warfarin,
cyclo
sporine,
corticosteroid,
anticonvulsa
nts,
cardiovascularagents,theophylline,sulfonylurea,
HMG-CoAreductase
inhibitors,
antipsychotics,
benzodiazepines&possiblere
ductioninefficacyof
azoleantifungaldrug
Reduceslevelsofproteaseinhibitors&NNRT
Is
Pyrazin
amide
Skinrash,jaundice
,hepatitis,anorexia
,nausea,abdom
inalpain&jointpain
Excretionmaybeblockedbyprobenecid
Shouldbetaken2hoursbeforedidanosine
(ddI)
Ethambutol
Visualim
pairm
ent
Absorption
delayed
orreduced
byalum
inium
hydroxide
-
Streptom
ycin
Skinrash,
deafness(no
waxon
otoscopy),
dizziness
(vertigo
&nystagmus),decreasedurineoutput
Mayincreaseototoxicity&nephrotoxicitywhenuse
witham
inoglycoside,am
photericinB
,cephalosporins,
cyclo
sporin,cisp
latin,frusemide&vancom
ycin
-

Management of Tuberculosis (Third Edition)
7
ALG
OR
ITH
M O
N M
AN
AG
EMEN
T O
F C
HIL
DR
EN W
ITH
PO
SITI
VE H
ISTO
RY O
F C
ON
TAC
T W
ITH
TB
Note:
•Mantouxtestmaybenegativeinchildrenwhoaremalnourishedandimmunocom
prom
ised.
•Contacttracingandinvestigationsinchildrenaretobedonew
ithin
6 w
eeksofdiagnosisoftheindexpatient.

Management of Tuberculosis (Third Edition)
8
PTB Close Contact*
Symptomatic
Asymptomatic
Mantoux test
10 mm <10 mm
CXR Discharge with advice**
Normal – manage as LTBI
Abnormal – evaluate for active TB
Evaluate for active TB • CXR • Sputum AFB • Mantoux test
(optional)
"
Diagnosis confirmed – treat
Diagnosis inconclusive – refer specialist
ALGORITHM ON INVESTIGATIONS FOR TB CONTACT TRACING IN ADULTS
*Immunocompetentclosecontacts**ToseekmedicaladviceifpatienthassymptomssuggestiveofTBsuchasfever,coughetc.formorethan2weeks.
• ThefollowingconditionsshouldbereferredtospecialistswithexperienceinTBmanagement:-o UnsureofTBdiagnosiso RetreatmentofTBo AdverseeventsfollowingantiTBdrugso MDR-TB&extensivelydrug-resistantTBo EPTBexceptfortuberculouslymphadenitiso Renal&/orliverimpairmentwithTBo HIV-TBco-infectiono SmearnegativeTBo Smearpositiveafter2monthsoftreatmento AllchildrendiagnosedwithTBo MaternalTBo ComplexTBcasesrequiringsurgicalintervention
REFERRAL CRITERIA

















