Rapid Diagnostic Tests for Group A StreptococcalPharyngitis: A Meta-analysis
abstractBACKGROUND AND OBJECTIVE: Effective management of group A strep-tococcal (GAS) pharyngitis is hindered by impracticality of the gold stan-dard diagnostic test: throat culture. Rapid antigen diagnostic tests(RADTs) are a promising alternative, although concerns about their sen-sitivity and specificity, and variation between test methodologies, havelimited their clinical use. The objective of this study was to perform a sys-tematic review withmeta-analysis of the diagnostic accuracy of RADTs forGAS pharyngitis.
METHODS: Medline and Embase from 1996 to 2013 were used as datasources. Of 159 identified studies, 48 studies of diagnostic accuracy ofGAS RADTs using throat culture on blood agar as a reference standardwere selected. Bivariate random-effects regression was used to estimatesensitivity and specificity with 95% confidence intervals (CIs). Additionalmeta-analyses were performed for pediatric data.
RESULTS: A total of 60 pairs of sensitivity and specificity from 48 stud-ies were included. Overall summary estimates for sensitivity and spec-ificity of RADTs were 0.86 (95% CI 0.83 to 0.88) and 0.96 (95% CI 0.94 to0.97), respectively, and estimates for pediatric data were similar.Molecular-based RADTs had the best diagnostic accuracy. Considerablevariability exists in methodology between studies. There were insuffi-cient studies to allow meta-regression/subgroup analysis within eachtest type.
CONCLUSIONS: RADTs can be used for accurate diagnosis of GAS phar-yngitis to streamline management of sore throat in primary care. RADTsmay not require culture backup for negative tests in most low-incidencerheumatic fever settings. Newer molecular tests have the highest sen-sitivity, but are not true point-of-care tests. Pediatrics 2014;134:771–781
AUTHORS: Wei Ling Lean, MBBS, BMedSc,a Sarah Arnup,BSc(Hons), MPhil, MBiostat,b Margie Danchin, MBBS,FRACP, PhD,a,c,d and Andrew C. Steer, MBBS, BMedSc, MPH,FRACP, PhDa,c,e
aDepartment of General Medicine, Royal Children’s Hospital,Melbourne, Australia; bClinical Epidemiology and BiostatisticsUnit, cGroup A Streptococcal Research Group, and dVaccine andImmunisation Research Group, Murdoch Children’s ResearchInstitute, Melbourne, Australia; and eCentre for InternationalChild Health, Department of Paediatrics, University of Melbourne,Melbourne, Australia
KEY WORDSgroup A streptococcus, pharyngitis, rapid test, sensitivity,specificity
ABBREVIATIONSCI—confidence intervalELISA—enzyme-linked immunosorbent assayFISH—fluorescence in situ hybridizationGAS—group A b-hemolytic streptococcusOIA—optical immunoassayPCR—polymerase chain reactionQUADAS—Quality Assessment of Diagnostic Accuracy StudiesRADT—rapid antigen diagnostic testROC—receiver operating characteristicsS-ROC—summary receiver operating characteristics
Dr. Lean collected data for the study and drafted the initialmanuscript; Dr Arnup carried out the statistical analyses andreviewed and revised the manuscript; Drs Danchin and Steerconceptualized the study, supervised data collection, andcritically reviewed and revised the manuscript; and all authorsapproved the final manuscript as submitted.
www.pediatrics.org/cgi/doi/10.1542/peds.2014-1094
doi:10.1542/peds.2014-1094
Accepted for publication Jul 21, 2014
Address correspondence to A/Prof Andrew Steer, Centre forInternational Child Health, Department of Paediatrics, Universityof Melbourne, Royal Children’s Hospital, Flemington Road,Parkville, Vic 3052, Australia. E-mail: [email protected]
FINANCIAL DISCLOSURE: Drs Danchin and Steer receivedfunding for a clinical study conducted in 2012 of a QuidelCorporation rapid antigen diagnostic test product; the otherauthors have no financial relationships relevant to this article todisclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors have indicatedthey have no potential conflicts of interest to disclose.
PEDIATRICS Volume 134, Number 4, October 2014 771
REVIEW ARTICLE
by guest on June 4, 2018www.aappublications.org/newsDownloaded from
Sore throat is a common presentationto primary health care and emergencydepartments, especially in the pediatricpopulation. The most common bacterialcause of acute sore throat is the groupA b-hemolytic Streptococcus (GAS). Ina cohort study done in Australia, the in-cidence of pharyngitis caused by GAS inchildren aged 5 to 12 yearswas 13 casesper 100 person-years.1 GAS pharyngitiscauses a considerable cost to society; inthe United States it is estimated that GASpharyngitis in children alone costs be-tween $224 and $539million per year.2 Inaddition to the acute symptoms of sorethroat, GAS can lead to suppurative se-quelae, including peri-tonsillar abscess,and nonsuppurative sequelae, includingrheumatic fever, although this compli-cation is rare today in most industri-alized countries.
However, there are challenges in the di-agnosis of GAS pharyngitis. First, thesigns and symptoms of GAS pharyngitisareoften indistinguishable fromviralandother causes of sore throat. No symptomor sign in isolation has been shown tohave a sufficiently high likelihood ratio topermit an accurate diagnosis of GASpharyngitis.3 Combinations of symptomsand signs have been developed intoclinical prediction rules to help identifypatients who have a higher likelihood ofGAS infection. One of the most commonlyused prediction rules validated in bothadults and children are the Centor cri-teria, which use up to 4 clinical features(tonsillar exudates, swollen tender an-terior cervical nodes, fever, and the lackof cough). However, this rule identifiesonly 53% of patients with GAS culture–positive sore throat even when all 4criteria are present.4,5 Therefore, if theclinician intends to treat GASpharyngitis,it is generally recommended that labo-ratory confirmation of the presence ofGAS be sought to limit unnecessary an-tibiotic prescription.
The gold standard laboratory inves-tigation of GAS pharyngitis is bacterial
culture of a throat swab. However, ef-fective management is hindered by theimpracticality of throat culture becauseof the relatively long lag time betweenthe collection of the specimen and finalmicrobiological diagnosis.5 This delay isespecially problematic in low-resourcesettings, as it may not be feasible forpatients to return for further follow-upvisits and appropriate treatment.6
Rapid antigen diagnostic tests (RADTs)are a potentially more feasible alterna-tive because of their quick turnaroundtime, so that the clinician can makea decision regarding treatment at thepoint of care.7 Since their inception inthe early 1980s, there have been severalgenerations of RADTs that have useddifferent methodologies.8 The first-generation tests used latex agglutination,followed by enzyme-linked immuno-sorbent assays (ELISAs), lateral flowand immunochromatographic assays,and optical immunoassays (OIAs). Morerecently, molecular-based techniques,such as DNA probes, polymerase chainreaction (PCR), and fluorescence in situhybridization (FISH)methods, have beendeveloped.8 RADTs have been incorpo-rated into both the Infectious DiseasesSociety of America and the EuropeanSociety for Clinical Microbiology andInfectious Diseases clinical practiceguidelines,4,9 but are not used routinelyin all countries, including Australia.10
Widespread use of RADTs has beenhindered by low sensitivity for mostcommonly usedRADTs (immunoassays).Previous reviews of RADT performancehave identified considerable variabilityin the diagnostic accuracy, especiallysensitivity, between different test meth-odologies.4,11 The American guidelinesrecommend that negative RADTs inchildren and adolescents should bebacked up by a throat culture to reducethe number of missed GAS pharyngitiscases.9 These guidelines, along withEuropean guidelines,4 suggest that abackup culture in adults is not necessary
because the incidence of GAS pharyngitisis generally lower than in children andbecause the risk of rheumatic fever islow. However, most RADTs have highspecificity, meaning that a positive RADTresult does not require a backup cultureand that the rate of overdiagnosis is low.9
We conducted a systematic review withmeta-analysis to determine the diag-nostic accuracy of each class of RADTs inchildren and adults combined and chil-dren only with GAS pharyngitis, and toexplore the heterogeneity among stud-ies by analyzing subgroups classifiedaccording to type of test in both childrenand adults combined and restricted tochildren.
METHODS
Data Collection
We systematically searched Medline andEmbase via OvidSP for articles publishedbetween 1996 and 2013. We used thefollowing search terms: Streptococcuspyogenes, streptococcal infections, groupA streptococcal infection, pharyngitis,rapid test, diagnostic reagent kits, im-munoassay, immunoenzyme technique,enzyme immunoassay, latex fixation test,latex agglutination test, diagnostic test,molecular biology. The search was sup-plemented by a manual review of bib-liographies of articles meeting inclusioncriteria and the bibliographies of pre-vious reviews. The search was limited toEnglish-language articles only.
The abstract of all identified articleswas reviewed. We included articles inour review if they contained data on theaccuracy of GAS RADTs. Review articles,letters, comments, and study protocolswith incomplete data were excluded(Fig 1). After this, full articles were re-trieved and reviewed.
Eachstudywasassessed forquality andriskof biasby 2 investigators (WLL, ACS)using the Quality Assessment of Di-agnostic Accuracy Studies (QUADAS)tool for inclusionwithinameta-analysis
772 LEAN et al by guest on June 4, 2018www.aappublications.org/newsDownloaded from
of studies.12 The Cochrane version of 11QUADAS criteria was used in the qualityassessment of each study (SupplementalTable 2).12 All the analyzed studies usedculture on a blood agar plate as a mini-mum reference standard; data withinindividual studies that were not com-pared with blood agar culture were ex-cluded from analysis. Studies that usedonly throat culture as a backup for neg-ative RADTswere excluded from themeta-analysis because this methodologyassumes that all test-positives are true-positives, and there are no false-positives;as a result, specificity is assumed to be100% and sensitivity can be over-estimated. Only studies that used throatswabs, not mouth swabs, were included.
Data Extraction and Categorization
Multiple variables were extracted fromthe studies, including sample size, prev-alenceofGASculturepositivity, sensitivity,
specificity, and sample characteristics.Where sensitivity and specificity werenot presented in the article, we inde-pendently calculated sensitivity andspecificity from published raw data orfrom data submitted by authors at ourrequest. Studies were categorized on thebasis of the type of test, setting (emer-gency department, outpatient clinic,inpatient), and a subgroup of studiesperformed in children (aged,18 years)was defined. For type of test, we includedstudies that reported on lateral flow as-say and immunochromatographic assayin a single category, and DNA probe, PCRassay, and FISH in a single category(molecular technique), in addition to 4other categories: latex agglutination, li-posomal technology, ELISA, and OIA.
Statistical Analysis
A bivariate random-effects model wasused to estimate summary values of
sensitivity, specificity, and their 95%confidence intervals (CIs), for each RADTcategory with more than 3 pairs ofsensitivity and specificity and all cate-gories combined.13–15 Because a corre-lation may exist between sensitivity andspecificity across studies, each studymeasurement of sensitivity and speci-ficity was analyzed together as a pair.
To explore heterogeneity between stud-ies, we prepared forest plots of the in-dividualpairsof sensitivityandspecificitywith 95% confidence intervals; and plot-ted each pair in receiver operatingcharacteristic (ROC) space, along witha summary ROC (S-ROC) curve, summaryestimates of sensitivity and specificity,and a 95% confidence ellipse around thesummary estimates. The S-ROC curveillustrates the estimated relationshipbetweensensitivity andspecificityacrossstudies; where there is a correlationbetweensensitivity andspecificityacross
FIGURE 1Study flow diagram. This flow diagram follows the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA)76 with modifications.
REVIEW ARTICLE
PEDIATRICS Volume 134, Number 4, October 2014 773 by guest on June 4, 2018www.aappublications.org/newsDownloaded from
studies, the individual pairs of sen-sitivity and specificity are expected tolie along the S-ROC curve.16 Hetero-geneity was further investigated byperforming separate analyses in thefollowing clinical subgroups: RADTtypes with more than 3 studies (lateralflow/immunochromatographic assay,ELISA, OIA, molecular technique), andRADT types with more than 3 studiesincluding children only.
Many (19/48) studies reported morethan 1 pair of sensitivity and speci-ficity. Where the multiple sensitivityand specificity pairs were estimatedfrom different samples of patients,each pair is treated in our analysis asif it came from a separate study.6,17–20
Where a different RADT was tested inthe same sample of patients, we in-cluded each sensitivity and specificitypair in the subgroup analysis for therespective RADT.21–25
Where multiple sensitivity and speci-ficity pairs were estimated from thesame patients in a study, only 1 pair ofsensitivity and specificity was includedin our analysis.22,23,25–34 We selected thepairs that were the focus of primaryanalysis of the selected studies.
Statistical analysis was performed inStata12 (StataCorp, CollegeStation, TX)using the Metandi package.35
RESULTS
A total of 60 pairs of sensitivity andspecificity, comprising 23 934 patientsfrom 48 studies were included in thefinal analysis (Table 1). Of note, 7 studieswere excluded after application of themodified QUADAS tool; 6 of these studieswere excluded because of an inade-quate reference standard (Fig 1 andSupplemental Table 2).36–41 All studiesincluded used culture as the referencestandard to compare the RADT perfor-mance. Thirty-six of the 48 studies werecarried out in a developed country and12 in a developing country. Eight types ofRADTswere found among these articles.
The range of values for eachRADT type issummarized in Supplemental Table 3.
Sensitivity and Specificity Analysis:Summary Estimates
The summary estimate of sensitivity ofRADTs among all studies included was0.86 (95% CI 0.83 to 0.88), whereas thesummary estimate for specificity was0.96 (95% CI 0.94 to 0.97, SupplementalFig 4). We observed considerable vari-ability across studies in sensitivity, butlittle variability in specificity. Despitethis variability, we consider it appro-priate to estimate diagnostic accuracywith a summary measure for sensitivityand specificity, rather than with anS-ROC curve, because there was no evi-dence of a correlation between sensi-tivity and specificity when the RADTswere pooled (correlation coefficient0.06, 95% CI –0.26 to 0.37). Furthermore,the forest plot for all studies showed nosystematic decrease in specificity withincreasing sensitivity, illustrating thata threshold effect, such as variation incutoff value for a positive test resultbetween studies, does not account forthe observed variability in diagnosticaccuracy between studies.
Sensitivity and Specificity Analysis:Test Types
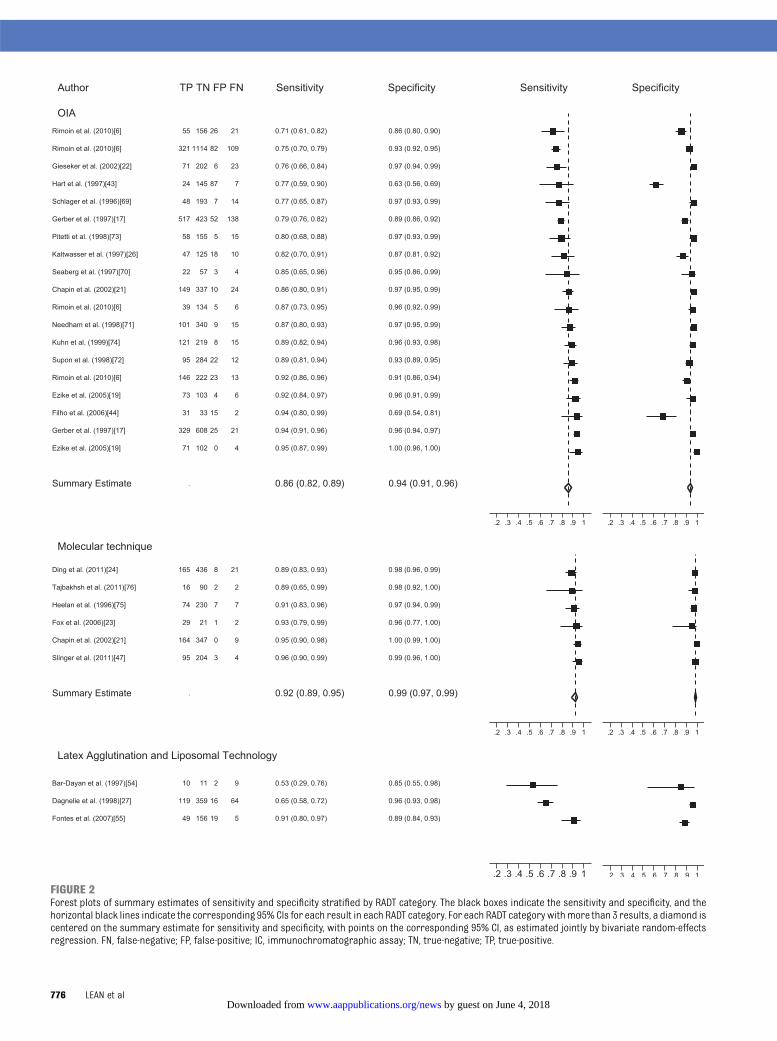
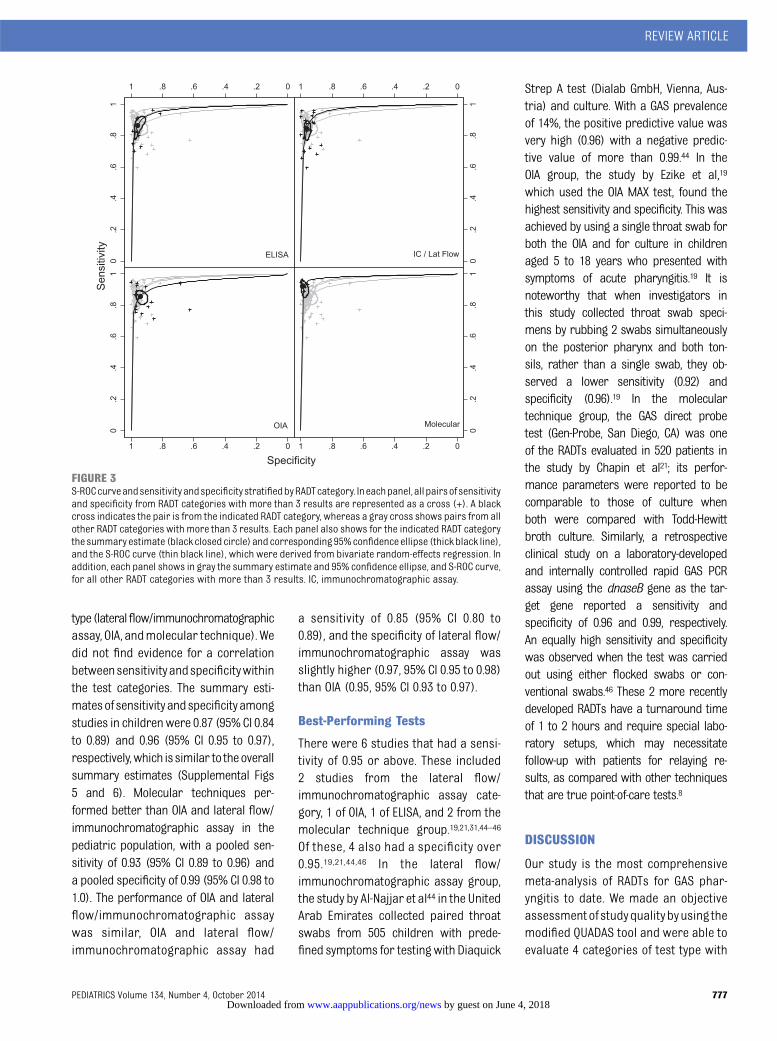
Results from4of the6categoriesofRADTwere pooled (Fig 2). Overall, specificitywas higher than sensitivity for all 4 testcategories. There was no evidence fora correlation between sensitivity andspecificity within the test categories.Test performance appeared best for themolecular technique category with apooled sensitivity and specificity of 0.92(95% CI 0.89 to 0.95) and 0.99 (95% CI0.97 to 0.99), respectively. The sensitivityand specificity of the other 3 test cate-gories were comparable with pooledsensitivity ranging from 0.84 to 0.86, andpooled specificity ranging from 0.94 to0.96. The S-ROC curves for each RADTtype compared with the other test cat-egories are shown in Fig 3.
We continued to observe a largeamount of variability in the sensitivityfound in studies within each cate-gory, particularly in the lateral-flow/immunochromatographic assay cate-gory where sensitivity ranged from 0.59to 0.96. Of the test types not included inthe meta-analyses described previously,both test types (latex agglutination andliposomal technology) had relativelypoor sensitivity (Supplemental Fig 4,Supplemental Table 3).
There was less variability in specificity,although there were 2 clear outliers intheOIA category inourmeta-analysis.42,43
The study by Hart et al42 comparedBioStar Strep A OIA RADT with a Selec-tive Strep Agar with 5% sheep bloodthat was incubated anaerobically. Theprevalence of GAS pharyngitis in thisstudy was 12%, which is much lowerthan the other studies of OIA included.This study found that weakly positivetest results were frequently associatedwith false-positive results; reclassifi-cation of these weakly positive testresults as negative results would in-crease the specificity of the OIA. Possi-ble cross-reactivity with groups B and Cstreptococci also were observed insome of the false-positive cases.42 Sim-ilarly, false-positive results were fre-quent in the study by Filho et al43 inBrazil, contributing to low specificity.This was a small study with a samplesize of 81, comparing the Strep A OIAMax RADT to the reference standard of5% goat blood agar culture medium inan aerobic environment. The high rateof false-positives (32.6%) was attributedto failure of the RADT method, detectingnonspecific bacterial antigens or cross-reaction with other nongroup A strep-tococci.43
Sensitivity and Specificity Analysis:Pediatric Population
Thirty-three paired sensitivity and speci-ficity results from 25 studies evaluatedRADTs in children only, and meta-analysiswas performed for 3 categories of test
774 LEAN et al by guest on June 4, 2018www.aappublications.org/newsDownloaded from
Lateral flow/immunochromatographic assaysFinger et al,28 1999 Quickvue Flex Strep A 3–16 777 ED, clinic VietnamNerbrand et al,25 2002 Quickvue In-Line Strep A test All ages 536 Clinic SwedenGieseker et al,22 2002 OSOM Ultra Strep A Children 302 ED, clinic USGieseker et al,30 2003 OSOM Ultra Strep A Children 887 Clinic USAtlas et al,55 2005 Acceava $18 148 Clinic USFox et al,23 2006 Signify Rapid Strep A Test 3–18 53 Hospital USForward et al,33 2006 Strep A Rapid Test Device, Nova Centuty Scientific Inc. All ages 818 Clinic CanadaAbu-Sabaah et al,32 2006 Immunostics Strep A Direct All ages 355 Hospital, clinic Saudi ArabiaVan Limbergen et al,56 2006 Quickvue+ Strep A Test Mean 3.85 201 ED ScotlandWright et al,57 2007 Quickvue In-Line Strep A test & OSOM Ultra 0–18 338 Clinic USMaltezou et al,58 2008 Link2 Strep A 2–14 451 Clinic GreeceCamurdan et al,59 2008 INTEX Strep A II #17 1248 Clinic TurkeyAl-Najjar et al,44 2008 Diaquick Strep A Test Children 496 Clinic UAETanz et al,60 2009 Quickvue 3–18 1848 Clinic USKim,45 2009 SD Bioline Strep A Children 193 Clinic KoreaLlor et al,34 2009 OSOM Strep A $14 222 Clinic SpainGurol et al,20 2010 Quickvue 0–90 1048 Clinic TurkeySarikaya et al,61 2010 Quickvue 18–64 100 ED USDing et al,24 2011 Clearview Exact Strep A #14 630 Clinic ChinaCohen et al,62 2012 StreptAtest, Dectrapharm 3–15 785 Clinic France
ELISAKurtz et al,29 2000 Abbott TestPack Plus 4–15 537 Clinic USRosenberg et al,63 2001 Abbott TestPack Plus .3 126 ED CanadaRoosevelt et al,64 2001 Abbott Signify Strep A 3–16 322 Hospital USSheeler et al,18 2002 Abbott TestPack Plus All ages 443 Clinic USNerbrand et al,25 2002 Abbott TestPack Plus All ages 536 Clinic SwedenSantos et al,65 2003 Abbott TestPack Strep A 1–12 49 Clinic BrazilJohansson et al,66 2003 Abbott TestPack Strep A Plus $4 169 Clinic SwedenLindbaek et al,31 2004 Abbott TestPack Strep A Plus Mean 23.9 306 Clinic NorwayMcIsaac et al,5 2004 Abbott TestPack Strep A Plus 3–69 787 Clinic CanadaHumair et al,67 2006 Abbott TestPack Plus Strep A .15 372 Clinic Switzerland
OIASchlager et al,68 1996 Biostar Strep A OIA All ages 262 Clinic USSeaberg et al,69 1997 Biostar Strep A OIA All ages 86 ED USKaltwasser et al,26 1997 Biostar Strep A OIA Children 200 ED USGerber et al,17 1997 Biostar Strep A OIA 1–51 2113 Clinic USHart et al,42 1997 Biostar Strep A OIA All ages 263 Clinic USNeedham et al,70 1998 Biostar Strep A OIA All ages 465 Clinic USSupon et al,71 1998 Biostar Strep A OIA MAX All ages 413 ED, clinic USPitetti et al,72 1998 Biostar Strep A OIA 1–18 233 ED, clinic USKuhn et al,73 1999 Biostar Strep A OIA 2–18 363 ED, clinic USChapin et al,21 2002 Thermo Biostar Strep A OIA Children 520 Clinic USGieseker et al,22 2002 Strep A OIA MAX Children 302 ED, clinic USEzike et al,19 2005 Strep A OIA MAX 5–18 363 ED USFilho et al,43 2006 Strep A OIA MAX $18 81 ED BrazilRimoin et al,6 2010 Strep A OIA MAX 2–12 2472 Clinic Brazil, Croatia,
Egypt, LatviaDNA probeHeelen et al,74 1996 Gen-Probe All ages 318 ED, clinic USChapin et al,21 2002 Gen-Probe Children 520 Clinic USFox et al,23 2006 Gen-Probe 3–18 53 Hospital US
PCR assaySlinger et al,46 2011 Laboratory developed Children 306 ED Canada
FISHTajbakhsh et al,75 2011 Not available All ages 110 Unknown IranDing et al,24 2011 Not available #14 630 Clinic China
ED, emergency department.
REVIEW ARTICLE
PEDIATRICS Volume 134, Number 4, October 2014 775 by guest on June 4, 2018www.aappublications.org/newsDownloaded from
FIGURE 2Forest plots of summary estimates of sensitivity and specificity stratified by RADT category. The black boxes indicate the sensitivity and specificity, and thehorizontal black lines indicate the corresponding 95% CIs for each result in each RADT category. For each RADT category withmore than 3 results, a diamond iscentered on the summary estimate for sensitivity and specificity, with points on the corresponding 95% CI, as estimated jointly by bivariate random-effectsregression. FN, false-negative; FP, false-positive; IC, immunochromatographic assay; TN, true-negative; TP, true-positive.
776 LEAN et al by guest on June 4, 2018www.aappublications.org/newsDownloaded from
type(lateralflow/immunochromatographicassay, OIA, andmolecular technique).Wedid not find evidence for a correlationbetweensensitivityandspecificitywithinthe test categories. The summary esti-matesofsensitivityandspecificityamongstudies in childrenwere 0.87 (95%CI 0.84to 0.89) and 0.96 (95% CI 0.95 to 0.97),respectively,which issimilar to theoverallsummary estimates (Supplemental Figs5 and 6). Molecular techniques per-formed better than OIA and lateral flow/immunochromatographic assay in thepediatric population, with a pooled sen-sitivity of 0.93 (95% CI 0.89 to 0.96) anda pooled specificity of 0.99 (95% CI 0.98 to1.0). The performance of OIA and lateralflow/immunochromatographic assaywas similar, OIA and lateral flow/immunochromatographic assay had
a sensitivity of 0.85 (95% CI 0.80 to0.89), and the specificity of lateral flow/immunochromatographic assay wasslightly higher (0.97, 95% CI 0.95 to 0.98)than OIA (0.95, 95% CI 0.93 to 0.97).
Best-Performing Tests
There were 6 studies that had a sensi-tivity of 0.95 or above. These included2 studies from the lateral flow/immunochromatographic assay cate-gory, 1 of OIA, 1 of ELISA, and 2 from themolecular technique group.19,21,31,44–46
Of these, 4 also had a specificity over0.95.19,21,44,46 In the lateral flow/immunochromatographic assay group,the study by Al-Najjar et al44 in the UnitedArab Emirates collected paired throatswabs from 505 children with prede-fined symptoms for testingwith Diaquick
Strep A test (Dialab GmbH, Vienna, Aus-tria) and culture. With a GAS prevalenceof 14%, the positive predictive value wasvery high (0.96) with a negative predic-tive value of more than 0.99.44 In theOIA group, the study by Ezike et al,19
which used the OIA MAX test, found thehighest sensitivity and specificity. This wasachieved by using a single throat swab forboth the OIA and for culture in childrenaged 5 to 18 years who presented withsymptoms of acute pharyngitis.19 It isnoteworthy that when investigators inthis study collected throat swab speci-mens by rubbing 2 swabs simultaneouslyon the posterior pharynx and both ton-sils, rather than a single swab, they ob-served a lower sensitivity (0.92) andspecificity (0.96).19 In the moleculartechnique group, the GAS direct probetest (Gen-Probe, San Diego, CA) was oneof the RADTs evaluated in 520 patients inthe study by Chapin et al21; its perfor-mance parameters were reported to becomparable to those of culture whenboth were compared with Todd-Hewittbroth culture. Similarly, a retrospectiveclinical study on a laboratory-developedand internally controlled rapid GAS PCRassay using the dnaseB gene as the tar-get gene reported a sensitivity andspecificity of 0.96 and 0.99, respectively.An equally high sensitivity and specificitywas observed when the test was carriedout using either flocked swabs or con-ventional swabs.46 These 2 more recentlydeveloped RADTs have a turnaround timeof 1 to 2 hours and require special labo-ratory setups, which may necessitatefollow-up with patients for relaying re-sults, as compared with other techniquesthat are true point-of-care tests.8
DISCUSSION
Our study is the most comprehensivemeta-analysis of RADTs for GAS phar-yngitis to date. We made an objectiveassessmentofstudyqualitybyusing themodified QUADAS tool and were able toevaluate 4 categories of test type with
FIGURE 3S-ROCcurveandsensitivityandspecificitystratifiedbyRADTcategory. Ineachpanel,all pairsofsensitivityand specificity from RADT categories with more than 3 results are represented as a cross (+). A blackcross indicates the pair is from the indicated RADT category, whereas a gray cross shows pairs from allother RADT categories with more than 3 results. Each panel also shows for the indicated RADT categorythe summary estimate (black closed circle) and corresponding 95%confidenceellipse (thick black line),and the S-ROC curve (thin black line), which were derived from bivariate random-effects regression. Inaddition, each panel shows in gray the summary estimate and 95% confidence ellipse, and S-ROC curve,for all other RADT categories with more than 3 results. IC, immunochromatographic assay.
REVIEW ARTICLE
PEDIATRICS Volume 134, Number 4, October 2014 777 by guest on June 4, 2018www.aappublications.org/newsDownloaded from
pooled results. Overall, the sensitivity ofincluded RADTs in our study was 0.86(95% CI 0.83 to 0.88) and specificity 0.96(95% CI 0.94 to 0.97), although withnoticeable variability among individualtests. These results indicate that RADTsin general have high diagnostic accu-racy. The sensitivity and specificity ofthese tests when analyzed in pediatricstudiesaloneweresimilar to theoverallestimates. Overall, thenewermoleculartechniques were the best-performingtests, particularly in terms of theirsensitivity, although a minority of non-molecular tests also performed ex-tremely well. There was less variabilityin sensitivity observed for the morerecently developed RADTs comparedwith the older tests.
The 2 recently published major US andEuropean guidelines both recommendthe use of RADTs in routine clinicalpractice,4,9 although with differences inthe indications for their use and in-terpretation of their results. There isalso considerable variability in recom-mendations for use of RADTs when otherguidelines are considered, and somecountries, including Australia, do notcurrently recommend the use of RADTs.47
The recent US guidelines recommendRADTs for the diagnosis of GAS pharyn-gitis in adults and children at least 3years of age with acute sore throat whodo not have clinical features suggestiveof a viral etiology (cough, rhinorrhea,hoarseness, and oral ulcers).9 Theseguidelines recommend the use ofbackup culture for negative RADTs inchildren (but not in adults) because ofconcern regarding low sensitivity. Therecent European guidelines recommendusing the Centor criteria to guide the useof RADTs in the diagnosis of GAS phar-yngitis; physicians can consider the useof RADTs in patients with 3 to 4 Centorcriteria, whereas there is no need toroutinely use RADTs in patients with 0 to2 criteria.4 These guidelines do not rec-ommend a backup culture for negative
RADTs in either adults or children.9 Thereasons for these differences in recom-mendations are not immediately clear,but may relate to differing opinions be-tween the expert groups as to theperceived necessity of treating GASpharyngitis to prevent suppurative andnonsuppurative complications, particu-larly acute rheumatic fever.47 We con-sider that our data show that the overallsensitivity of RADTs is sufficiently highthat a backup culture is generally notnecessary, with the possibility of missing14% of potential GAS pharyngitis casesbeing an acceptable level of risk giventhe low risk of acute rheumatic fever inmost industrialized settings, but thisdecision is likely to be at the treatingphysician’s discretion. The high overallspecificity of RADTs means that thesetests can prevent unnecessary antibioticprescription due to minimal overdiag-nosis of GAS pharyngitis in the vast ma-jority of cases.
Although rheumatic fever is uncommonin Europe and the United States, with anincidence of ,1 per 100 000, the dis-ease remains an important cause ofcardiac morbidity and mortality inmany tropical developing countrieswhere the incidence is frequently.50per 100 000.48 In these countries, thereis a clear indication for treatment ofGAS pharyngitis to prevent rheumaticfever and its chronic and disablingsequelae, rheumatic heart disease.49 Ahighly sensitive ($95%) and inexpensiveRADT with a very rapid turnaround timecould make a major contribution to con-trol efforts for rheumatic fever. Based onour data, however, no single test cur-rently fulfills all 3 of these criteria.
When cost is considered in the man-agement of pharyngitis, RADTs havebeenshown tobe themorecost-effectiveoption when compared directly withculture (as treating all and none haveunacceptable costs).50,51 In terms of di-rect costs, in Australia, RADTs cost ap-proximately AUD$5 to AUD$10 per test
compared with AUD$30 per test forculture, whereas costs in the UnitedStates and Europe are more difficult tocompare because of the wide range ofpricing by individual commercial com-panies . The practice of using confir-matory cultures to back up RADTs hasbeen shown to cost .$8 million peradditional case of rheumatic heart dis-ease prevented,52 and should be ques-tioned as a cost-effective approach tomanagement.
There are several limitations to ourstudy. Despite our best efforts to ex-clude low-quality studies, particularlythose with an inadequate referencestandard, there was considerable var-iability in methodology among studies.This includednumberand typeof throatswabs used, aswell as techniques usedto obtain these throat swabs.19,23,29,46
Methods of sample collection were notclearly reported in all studies andthere is no way to control the quality ofthe swab samples. Studies includedalso differed in their settings and theclinical severity of included patients.For example, we included studies thatassessed diagnostic accuracy of RADTsamong patients both before receiving,and after receiving, antibiotic treat-ment.18,28 These factors are potentialconfounders in the estimation of di-agnostic accuracy and may explainsome of the observed heterogeneityacross each type of RADT. However, be-cause of insufficient numbers of studieswithin each test type, we were unable toperform either a meta-regression ora subgroup analysis to determine theimportance of these factors. In terms ofquality of included studies, blinding ofreference standard results was not wellreported inmost of the included studies.Information on uninterpretable resultswas also poorly reported. It was notpossible to determine if uninterpretableresults occurred in 24 of the includedstudies. In addition, withdrawals wereunclear or not explained in 16 of the
778 LEAN et al by guest on June 4, 2018www.aappublications.org/newsDownloaded from
included studies (Supplemental Table 2).Finally, we included studies published inthe English language only, which mayhave reduced the numbers of studiesincluded in our meta-analysis.
The diagnostic accuracy of the morerecently developed RADTs (moleculartechniques) is encouraging. However,further research could focus on im-proving the practicality of these tests,especially when they are used in theprimary care settings. A considerabledrawback of these tests is that none are
truly “point-of-care” tests with a turn-around time between 1 and 3 hours,whereas the immune-based tests havea turnaround time as fast as 30 sec-onds. Other factors that may have animpact on sensitivity and specificity ofthe RADTs, such as the type of throatswab and sampling techniques, alsoneed to be further investigated in well-designed studies, to further improve thediagnostic accuracy of RADTs. Finally,studies to examine cost-effective analy-sis of each class of RADTs compared
with culture and antibiotic treatment,especially in the pediatric population,would be beneficial for policy makersand clinicians with regard to choice ofRADT and treatment decisions.
Our meta-analysis shows that RADTs canbe used as accurate, rapid tests for thediagnosis of GAS pharyngitis and thatgenerally backup culture for negativetests are not necessary in most low-incidence rheumatic fever settings, par-ticularly if tests with a high sensitivity areused, includingthenewermolecular tests.
REFERENCES
1. Danchin MH, Rogers S, Kelpie L, et al.Burden of acute sore throat and group Astreptococcal pharyngitis in school-agedchildren and their families in Australia.Pediatrics. 2007;120(5):950–957
2. Pfoh E, Wessels MR, Goldmann D, Lee GM.Burden and economic cost of group Astreptococcal pharyngitis. Pediatrics. 2008;121(2):229–234
3. Shaikh N, Swaminathan N, Hooper EG. Ac-curacy and precision of the signs andsymptoms of streptococcal pharyngitis inchildren: a systematic review. J Pediatr.2012;160(3):487–493, e3
4. Pelucchi C, Grigoryan L, Galeone C, et al;ESCMID Sore Throat Guideline Group. Guide-line for the management of acute sore throat.Clin Microbiol Infect. 2012;18(suppl 1):1–28
5. McIsaac WJ, Kellner JD, Aufricht P, VanjakaA, Low DE. Empirical validation of guide-lines for the management of pharyngitis inchildren and adults. JAMA. 2004;291(13):1587–1595
6. Rimoin AW, Walker CL, Hamza HS, et al. Theutility of rapid antigen detection testing forthe diagnosis of streptococcal pharyngitisin low-resource settings. Int J Infect Dis.2010;14(12):e1048–e1053
7. Clegg HW, Dallas SD, Roddey OF, et al;Presbyterian Pediatric Research Group.Extrapharyngeal group A Streptococcusinfection: diagnostic accuracy and utility ofrapid antigen testing. Pediatr Infect Dis J.2003;22(8):726–731
8. Leung AK, Newman R, Kumar A, Davies HD.Rapid antigen detection testing in di-agnosing group A beta-hemolytic strepto-coccal pharyngitis. Expert Rev Mol Diagn.2006;6(5):761–766
9. Shulman ST, Bisno AL, Clegg HW, et al.Clinical practice guideline for the diagnosisand management of group A streptococcalpharyngitis: 2012 update by the InfectiousDiseases Society of America. Clin Infect Dis.2012;55(10):1279–1282
10. Danchin MH, Curtis N, Nolan TM, CarapetisJR. Treatment of sore throat in light of theCochrane verdict: is the jury still out? MedJ Aust. 2002;177(9):512–515
11. Ruiz-Aragón J, Rodríguez López R, MolinaLinde JM. Evaluation of rapid methods fordetecting Streptococcus pyogenes. System-atic review and meta-analysis [in Spanish].An Pediatr (Barc). 2010;72(6):391–402
13. Hamza TH, van Houwelingen HC, Stijnen T.The binomial distribution of meta-analysiswas preferred to model within-study vari-ability. J Clin Epidemiol. 2008;61(1):41–51
14. Chu H, Cole SR. Bivariate meta-analysis ofsensitivity and specificity with sparse data:a generalized linear mixed model ap-proach. J Clin Epidemiol. 2006;59(12):1331–1332, author reply 1332–1333
15. Reitsma JB, Glas AS, Rutjes AW, Scholten RJ,Bossuyt PM, Zwinderman AH. Bivariateanalysis of sensitivity and specificity pro-duces informative summary measures indiagnostic reviews. J Clin Epidemiol. 2005;58(10):982–990
16. Chappell FM, Raab GM, Wardlaw JM. Whenare summary ROC curves appropriate for
diagnostic meta-analyses? Stat Med. 2009;28(21):2653–2668
17. Gerber MA, Tanz RR, Kabat W, et al. Opticalimmunoassay test for group A beta-hemolyticstreptococcal pharyngitis. An office-based,multicenter investigation. JAMA. 1997;277(11):899–903
18. Sheeler RD, Houston MS, Radke S, Dale JC,Adamson SC. Accuracy of rapid strep test-ing in patients who have had recentstreptococcal pharyngitis. J Am Board FamPract. 2002;15(4):261–265
19. Ezike EN, Rongkavilit C, Fairfax MR, ThomasRL, Asmar BI. Effect of using 2 throat swabsvs 1 throat swab on detection of group Astreptococcus by a rapid antigen detectiontest. Arch Pediatr Adolesc Med. 2005;159(5):486–490
20. Gurol Y, Akan H, Izbirak G, et al. The sensi-tivity and the specificity of rapid antigentest in streptococcal upper respiratory tractinfections. Int J Pediatr Otorhinolaryngol.2010;74(6):591–593
21. Chapin KC, Blake P, Wilson CD. Performancecharacteristics and utilization of rapid an-tigen test, DNA probe, and culture for de-tection of group a streptococci in an acutecare clinic. J Clin Microbiol. 2002;40(11):4207–4210
22. Gieseker KE, Mackenzie T, Roe MH, Todd JK.Comparison of two rapid Streptococcuspyogenes diagnostic tests with a rigorousculture standard. Pediatr Infect Dis J. 2002;21(10):922–927
23. Fox JW, Marcon MJ, Bonsu BK. Diagnosis ofstreptococcal pharyngitis by detection ofStreptococcus pyogenes in posterior pha-ryngeal versus oral cavity specimens. J ClinMicrobiol. 2006;44(7):2593–2594
REVIEW ARTICLE
PEDIATRICS Volume 134, Number 4, October 2014 779 by guest on June 4, 2018www.aappublications.org/newsDownloaded from
24. Ding JY, Wang P. Methods for the rapidscreening of group A streptococci: fluo-rescent in situ hybridization versus immu-nochromatography. Med Princ Pract. 2011;20(6):504–508
25. Nerbrand C, Jasir A, Schalén C. Are currentrapid detection tests for Group A Strepto-cocci sensitive enough? Evaluation of 2commercial kits. Scand J Infect Dis. 2002;34(11):797–799
26. Kaltwasser G, Diego J, Welby-Sellenriek PL,Ferrett R, Caparon M, Storch GA. Poly-merase chain reaction for Streptococcuspyogenes used to evaluate an optical im-munoassay for the detection of group Astreptococci in children with pharyngitis.Pediatr Infect Dis J. 1997;16(8):748–753
27. Dagnelie CF, Bartelink ML, van der Graaf Y,Goessens W, de Melker RA. Towards a bet-ter diagnosis of throat infections (withgroup A beta-haemolytic streptococcus) ingeneral practice. Br J Gen Pract. 1998;48(427):959–962
28. Finger R, Ho SH, Ngo TT, Ritchie CD, NguyenTN. Rapid streptococcal testing in Viet-namese children with pharyngitis. Asia PacJ Public Health. 1999;11(1):26–29
29. Kurtz B, Kurtz M, Roe M, Todd J. Importanceof inoculum size and sampling effect inrapid antigen detection for diagnosis ofStreptococcus pyogenes pharyngitis. J ClinMicrobiol. 2000;38(1):279–281
30. Gieseker KE, Roe MH, MacKenzie T, Todd JK.Evaluating the American Academy of Pedi-atrics diagnostic standard for Streptococ-cus pyogenes pharyngitis: backup cultureversus repeat rapid antigen testing. Pedi-atrics. 2003;111(6 pt 1). Available at: www.pediatrics.org/cgi/content/full/111/6pt1/e666
31. Lindbaek M, Høiby EA, Lermark G, SteinsholtIM, Hjortdahl P. Which is the best method totrace group A streptococci in sore throatpatients: culture or GAS antigen test?Scand J Prim Health Care. 2004;22(4):233–238
32. Abu-Sabaah AH, Ghazi HO. Better diagnosisand treatment of throat infections causedby group A beta-haemolytic streptococci. BrJ Biomed Sci. 2006;63(4):155–158
33. Forward KR, Haldane D, Webster D, Mills C,Brine C, Aylward D. A comparison betweenthe Strep A Rapid Test Device and conven-tional culture for the diagnosis of strepto-coccal pharyngitis. Can J Infect Dis MedMicrobiol. 2006;17(4):221–223
34. Llor C, Calviño O, Hernández S, et al. Rep-etition of the rapid antigen test in initiallynegative supposed streptococcal pharyn-gitis is not necessary in adults. Int J ClinPract. 2009;63(9):1340–1344
35. Harbord RM, Whiting P. Metandi: meta-analysis of diagnostic accuracy using hi-erarchical logistic regression. Stata J.2009;9(2):211–229
36. Mirza A, Wludyka P, Chiu TT, Rathore MH.Throat culture is necessary after negativerapid antigen detection tests. Clin Pediatr(Phila). 2007;46(3):241–246
37. Edmonson MB, Farwell KR. Relationshipbetween the clinical likelihood of groupa streptococcal pharyngitis and the sensi-tivity of a rapid antigen-detection test ina pediatric practice. Pediatrics. 2005;115(2):280–285
38. Armengol CE, Schlager TA, Hendley JO.Sensitivity of a rapid antigen detection testfor group A streptococci in a private pe-diatric office setting: answering the RedBook’s request for validation. Pediatrics.2004;113(4):924–926
39. Hall MC, Kieke B, Gonzales R, Belongia EA.Spectrum bias of a rapid antigen detectiontest for group A beta-hemolytic strepto-coccal pharyngitis in a pediatric pop-ulation. Pediatrics. 2004;114(1):182–186
40. Dimatteo LA, Lowenstein SR, Brimhall B,Reiquam W, Gonzales R. The relationshipbetween the clinical features of pharyngitisand the sensitivity of a rapid antigen test:evidence of spectrum bias. Ann Emerg Med.2001;38(6):648–652
41. Kayaba H, Tamura H, Fujiwara Y. Evaluationof the therapy for streptococcal pharyngitisusing Abbott Test Pack strep A. Acta Pae-diatr Jpn. 1996;38(1):8–11
42. Hart AP, Buck LL, Morgan S, Saverio S,McLaughlin JC. A comparison of the BioStarStrep A OIA rapid antigen assay, group ASelective Strep Agar (ssA), and Todd-Hewittbroth cultures for the detection of group AStreptococcus in an outpatient familypractice setting. Diagn Microbiol Infect Dis.1997;29(3):139–145
43. Araujo Filho BC, Imamura R, Sennes LU,Sakae FA. Role of rapid antigen detectiontest for the diagnosis of group-A beta-hemolytic streptococcus in patients withpharyngotonsillitis. Braz J Otorhinolar-yngol. 2006;72(1):12–15
44. Al-Najjar FY, Uduman SA. Clinical utility ofa new rapid test for the detection of groupA Streptococcus and discriminate use ofantibiotics for bacterial pharyngitis in anoutpatient setting. Int J Infect Dis. 2008;12(3):308–311
45. Kim S. The evaluation of SD Bioline Strep Arapid antigen test in acute pharyngitis inpediatric clinics. Korean J Lab Med. 2009;29(4):320–323
46. Slinger R, Goldfarb D, Rajakumar D, et al.Rapid PCR detection of group A Strepto-
coccus from flocked throat swabs: a retro-spective clinical study. Ann Clin MicrobiolAntimicrob. 2011;10(33):33
47. Matthys J, De Meyere M, van Driel ML, DeSutter A. Differences among internationalpharyngitis guidelines: not just academic.Ann Fam Med. 2007;5(5):436–443
48. Steer AC, Carapetis JR. Prevention andtreatment of rheumatic heart disease inthe developing world. Nat Rev Cardiol.2009;6(11):689–698
49. Robertson KA, Volmink JA, Mayosi BM.Antibiotics for the primary prevention ofacute rheumatic fever: a meta-analysis.BMC Cardiovasc Disord. 2005;5(1):11
50. Webb KH, Needham CA, Kurtz SR. Use ofa high-sensitivity rapid strep test withoutculture confirmation of negative results: 2years’ experience [published correctionappears in J Fam Pract. 2000;49(4):378]. JFam Pract. 2000;49(1):34–38
51. Mayes T, Pichichero ME. Are follow-upthroat cultures necessary when rapid an-tigen detection tests are negative for groupA streptococci? Clin Pediatr (Phila). 2001;40(4):191–195
52. Ehrlich JE, Demopoulos BP, Daniel KRJ Jr,Ricarte MC, Glied S. Cost-effectiveness oftreatment options for prevention ofrheumatic heart disease from Group Astreptococcal pharyngitis in a pediatricpopulation. Prev Med. 2002;35(3):250–257
53. Bar-Dayan Y, Bar-Dayan Y, Shemer J. Theeffect of a rapid kit for detection of strep-tococcal pharyngitis on the accuracy of thephysicians’ diagnoses. Mil Med. 1997;162(12):798–801
54. Fontes MJ, Bottrel FB, Fonseca MT, LasmarLB, Diamante R, Camargos PA. Early diag-nosis of streptococcal pharyngotonsillitis:assessment by latex particle agglutinationtest. J Pediatr (Rio J). 2007;83(5):465–470
55. Atlas SJ, McDermott SM, Mannone C, BarryMJ. The role of point of care testing forpatients with acute pharyngitis. J Gen In-tern Med. 2005;20(8):759–761
56. Van Limbergen J, Kalima P, Taheri S, BeattieTF. Streptococcus A in paediatric accidentand emergency: are rapid streptococcaltests and clinical examination of any help?Emerg Med J. 2006;23(1):32–34
57. Wright M, Williams G, Ludeman L. Compar-ison of two rapid tests for detecting groupA streptococcal pharyngitis in the pediatricpopulation at Wright-Patterson Air ForceBase. Mil Med. 2007;172(6):644–646
58. Maltezou HC, Tsagris V, Antoniadou A, GalaniL, Douros C, Katsarolis I, et al. Evaluation ofa rapid antigen detection test in the diag-nosis of streptococcal pharyngitis in children
780 LEAN et al by guest on June 4, 2018www.aappublications.org/newsDownloaded from
and its impact on antibiotic prescription. JAntimicrob Chemother. 2008;62(6):1407–1412
59. Camurdan AD, Camurdan OM, Ok I, Sahin F,Ilhan MN, Beyazova U. Diagnostic value ofrapid antigen detection test for strepto-coccal pharyngitis in a pediatric pop-ulation. Int J Pediatr Otorhinolaryngol.2008;72(8):1203–1206
60. Tanz RR, Gerber MA, Kabat W, Rippe J,Seshadri R, Shulman ST. Performance ofa rapid antigen-detection test and throatculture in community pediatric offices: im-plications for management of pharyngitis[published correction appears in Pediatrics.2009;124(2):846]. Pediatrics. 2009;123(2):437–444
61. Sarikaya S, Aktas C, Ay D, Cetin A, CelikmenF. Sensitivity and specificity of rapid antigendetection testing for diagnosing pharyngi-tis in the emergency department. Ear NoseThroat J. 2010;89(4):180–182
62. Cohen JF, Chalumeau M, Levy C, et al.Spectrum and inoculum size effect ofa rapid antigen detection test for group Astreptococcus in children with pharyngitis.PLoS ONE. 2012;7(6):e39085
63. Rosenberg P, McIsaac W, Macintosh D, Kroll M.Diagnosing streptococcal pharyngitis in theemergency department: is a sore throat scoreapproach better than rapid streptococcal an-tigen testing? CJEM. 2002;4(3):178–184
64. Roosevelt GE, Kulkarni MS, Shulman ST.Critical evaluation of a CLIA-waived strep-tococcal antigen detection test in theemergency department. Ann Emerg Med.2001;37(4):377–381
65. Santos O, Weckx LL, Pignatari AC, PignatariSS. Detection of Group A beta-hemolyticStreptococcus employing three differentdetection methods: culture, rapid antigendetecting test, and molecular assay. Braz JInfect Dis. 2003;7(5):297–300
66. Johansson L, Månsson NO. Rapid test,throat culture and clinical assessment inthe diagnosis of tonsillitis. Fam Pract. 2003;20(2):108–111
67. Humair JP, Revaz SA, Bovier P, Stalder H.Management of acute pharyngitis in adults:reliability of rapid streptococcal tests andclinical findings. Arch Intern Med. 2006;166(6):640–644
68. Schlager TA, Hayden GA, Woods WA, Dudley SM,Hendley JO. Optical immunoassay for rapiddetection of group A beta-hemolytic strepto-cocci. Should culture be replaced? ArchPediatr Adolesc Med. 1996;150(3):245–248
70. Needham CA, McPherson KA, Webb KH.Streptococcal pharyngitis: impact of a high-
sensitivity antigen test on physician out-come. J Clin Microbiol. 1998;36(12):3468–3473
71. Supon PA, Tunnell S, Greene M, Ostroff RM.Rapid detection of group A streptococcalantigen with a new optical immunoassay.Pediatr Infect Dis J. 1998;17(4):349–351
72. Pitetti RD, Drenning SD, Wald ER. Evaluationof a new rapid antigen detection kit forgroup A beta-hemolytic streptococci. PediatrEmerg Care. 1998;14(6):396–398
73. Kuhn S, Davies HD, Katzko G, Jadavji T,Church DL. Evaluation of the Strep A OIAassay versus culture methods: ability todetect different quantities of group AStreptococcus. Diagn Microbiol Infect Dis.1999;34(4):275–280
74. Heelan JS, Wilbur S, Depetris G, LetourneauC. Rapid antigen testing for group AStreptococcus by DNA probe. Diagn Micro-biol Infect Dis. 1996;24(2):65–69
75. Tajbakhsh S, Gharibi S, Zandi K, Yaghobi R,Asayesh G. Rapid detection of Streptococ-cus pyogenes in throat swab specimens byfluorescent in situ hybridization. Eur RevMed Pharmacol Sci. 2011;15(3):313–317
PEDIATRICS Volume 134, Number 4, October 2014 781 by guest on June 4, 2018www.aappublications.org/newsDownloaded from
DOI: 10.1542/peds.2014-1094 originally published online September 8, 2014; 2014;134;771Pediatrics
Wei Ling Lean, Sarah Arnup, Margie Danchin and Andrew C. SteerRapid Diagnostic Tests for Group A Streptococcal Pharyngitis: A Meta-analysis
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/134/4/771including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/134/4/771#BIBLThis article cites 72 articles, 15 of which you can access for free at:
Subspecialty Collections
bhttp://www.aappublications.org/cgi/collection/infectious_diseases_suInfectious Diseasefollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on June 4, 2018www.aappublications.org/newsDownloaded from