98
Read more with the online version of the Silver Book at http://www.ests.org/collaboration/database_reports.aspx
| Date post: | 27-Dec-2018 |
| Category: |
Documents |
| Upload: | truongquynh |
| View: | 213 times |
| Download: | 0 times |

Read more with the online version of the Silver Book athttp://www.ests.org/collaboration/database_reports.aspx

1

2

3
EUROPEAN SOCIETY
OF THORACIC SURGEONS
DATABASE COMMITTEE Dr. Pierre-‐Emmanuel Falcoz (France) ESTS Director of Audit and Database pierre-‐[email protected] Dr. Alessandro Brunelli (U K) [email protected]
Dr. Dirk van Raemdonck (Belgium) [email protected]
Dr. Marcel Dahan (France) [email protected]
Dr. Gaetano Rocco (Italy) [email protected]
Dr. Herbert MA Decaluwe (Belgium) [email protected]
Dr. Gonzalo Varela (Spain) [email protected]
Dr. Michele Salati (Italy) [email protected]
Dr. Enrico Ruffini (Italy) [email protected]
Dr. Pierluigi Filosso (Italy) [email protected]
Dr. Marco Scarci (UK) [email protected]
Dr. Andrea Billè (Italy) [email protected]
Dr. Xavier Benoit D’journo (France) Xavier.D'JOURNO@ap-‐hm.fr
Dr Zalan Szanto (Hungary) [email protected]
Past members of the ESTS Database Committee Dr. Richard Berrisford (UK); Dr. Tom Treasure (UK)

4
INDEX Message from the President of ESTS
5
Message from the Director of ESTS Database Message from Clinical Leader of Thymoma section of ESTS Database
6
8
The European Society of Thoracic Surgeons Database
10
Key messages from this report
12
PART 1 -‐ European Database Cumulative Activity (2007-‐2013)
13
Overall age and gender distributions 14 Total surgical activity within the entire dataset 16 Lung resections 21 Primary lung cancer 32 Comparisons of outcomes between 2007-‐2010 vs 2011-‐2013 in the total dataset
37
PART 2 -‐ Nation-‐specific Activity & Comparative Analysis between Contributing Countries
39
Number of units enrolled in the ESTS database as of December 2013, by country 40 Epidemiologic data 41 Primary lung cancer per contributing nations 45 Observed versus predicted in-‐hospital mortality rates of major lung resections in
different European countries
49
PART 3 -‐ Thymoma Section
50
PART 4 -‐ Appendices
70
Appendix 1: Units contributing to ESTS Database July 2007-‐December 2013 71 Appendix 2: Database format and submission of data 74 Appendix 3: Definition of major cardiopulmonary complications listed in the
database 78
Appendix 4: ESTS institutional accreditation program 80 Appendix 5: ESTS dataset (global, follow-‐up and thymoma) 83 Parts 3 and 4 are only available in the online version for ESTS Database users

5
Message from the President of ESTS
Dear members of the ESTS, The ESTS Database was established by Richard Berrisford 13 years ago, in 2001; since then it has progressively grown exponentially and it now includes 66623 procedures with more than 51110 lung resections and 205 units voluntary reporting their activities, with approximately 105 contributing more than 100 cases. The Database was originally an initiative for quality improvement and patient safety, according to the mission statement of our Society and it now one of our strategic pillars. I would like to thank Pierre-‐Emmanuel Falcoz, Director of Database, Alessandro Brunelli, Secretary General and all the members of the Database Committee who worked so hard to produce this report, the sixth one, and the previous one. Future projects will include more national database, and data on specific fields, like thymic tumors, already included, esophageal cancer and mesothelioma. To comprehensively assess surgical performance on an international level is one of our main objectives. Under the leadership of Alessandro Brunelli, the ESTS has developed a composite performance score incorporating processes and outcomes measures available in the database and has applied it to stratify performance of participating units. Those that are above the 50th percentile of the composite score are invited to submit their application to the ESTS Institutional Accreditation Program. Final peer-‐review assessment is then based upon the required structural/procedural/professional characteristics that are listed at the end of this report. The ESTS Database also offers solid grounds for clinical research. To date, several publications have been elaborated from database outcomes and published in various scientific journals and textbooks. They have significantly contributed to advance understanding in our specialty. The ESTS database is now undoubtedly at the end of its beginning phase. I would like to strongly encourage you to participate in this important project for the benefit of your patients, your practice and our specialty.
Federico Venuta, MD, ESTS President [email protected]

6
Message from the Director of ESTS Database Dear ESTS members, This is the sixth annual report of the ESTS Thoracic database, called “Silver Book”. This year collection of data ranges from July 2007 to February 2014, in 235 contributing units throughout Europe, among which 105 are contributing for more than 100 cases. It provides the most current appraisal of the thoracic surgical activity in Europe, in the framework of a comprehensive, European-‐wide, population dataset. The aim of the report is to provide an “epidemiologic” overview of thoracic surgery activity in Europe. The structure of the current report changes with regard to the fifth previous one’s. There is a printed version (we want it “thinner but sharper” as compared to previous years) and an online “extended” version in which we add a dedicated section concerning thymoma’s procedures and several appendices (http://www.ests.org/collaboration/ database_reports.aspx). Nevertheless, the main focus still remains on lung resections, considered as the most representative procedures of our specialty (and those currently under consideration for the European Accreditation program). As will be seen from the following pages, the current report is divided in four parts. The first (Part 1) focuses on the overall European database cumulative thoracic surgical activity from 2007 (time of the internet version has been launched) to February 2014. This section is split in three main chapters providing epidemiologic information on: 1°) total surgical activity; 2°) lung resection as a whole; 3°) primary lung cancer surgery. At the end of the first part we report a comparison of outcomes between 2007-‐2010 versus 2011-‐2013 on the total dataset, in terms of 30-‐day mortality and prolonged air leak. The second section (Part 2) deals with nation-‐specific activities and comparative analysis between contributing countries. This section is split in two chapters: the first one shows the distribution of patients (proportion of elderly, measurement of preoperative DLOC, percentage of mediastinal staging, e.g.) in the contributing countries whereas the second chapter has a particular focus on primary lung cancer surgery per contributing nations. Last but not least, an unadjusted and risk-‐adjusted outcomes rate of in-‐hospital mortality is presented. The third section (Part 3) is available in the online version for database users only and focuses on thymoma’s surgical activity in Europe. Finally, the last section (Part 4) shows online several appendices among which the ESTS dataset (global, follow-‐up and thymoma specific). Where do we go next in the burgeoning field of data collection in Europe? The ESTS Database has been offered to all ESTS Members as a free database to collect data -‐ retrospectively and prospectively -‐ since 2007. It was designed initially to collect general Thoracic Surgery Procedures data, with adequate level of detail to cover all clinical areas. Each Contributor

7
has access to her/his own data directly, with no limitations, and each contributor can download data any time. It has served this purpose well particularly for Lung Procedures, which constitute about 80% of all data collected, as published in the past “Silver Books”. Over the years, it has nevertheless become clear that some sections of the Database require an increased level of detail: ESTS started the process of up-‐grading the clinical content by inviting Leading Clinicians to take charge of a particular area of Thoracic Surgery with the objective of improving a particular section of the ESTS Database. The first Clinical area to be revamped has been the Thymic Tumors registry, which was launched in 2013 and will have a sufficient number of procedures to be included with its own discrete section in the 2014 “Silver Book”. For 2014 ESTS will expand the scope of its dataset to include additional Registries, and collect more in depth clinical details for some selected areas: in addition to the Thymoma section, there will be a Mesothelioma section that will be presented for consultation and final approval in Copenhagen; it will be available for Contributors to use just after Copenhagen. Other Clinical Areas receiving an overall are: the Neuro-‐Endocrine Tumors and the Chest Wall Injuries and Malformations. Both are in the “work-‐in-‐progress” phase, and will be available for consultation later in the year. Last but not least, I want to hail as a leader in the ESTS institutional Certification process, the department of thoracic surgery of Antwerp (leading by Dr. Paul Van Schil) for having been this year the first European team re-‐certified. I hope to see you in Copenhagen! We together need to go forward…
Prof. Pierre-‐Emmanuel Falcoz Director of ESTS Audit and Database pierre-‐[email protected]

8
Message from Clinical Leader of the Thymoma section of ESTS Registry
Dear ESTS members, It is my pleasure to introduce in the present annual report of the ESTS Thoracic database the Thymic Section, which is intended to be a dedicated section collecting prospective data about patients with thymic tumors. The ESTS Database Committee decided to fund and support a dedicated section on Thymic Tumors, based on the recent international momentum in the clinical research of these rare tumors. Thymic tumors are classified as orphan diseases, due to their low prevalence, and most of our knowledge has been based so far from single-‐institution case series, usually spanned over a long time period to collect a sufficient number of cases to draw a statistically appropriate analysis. The creation of the International Thymic Malignancies Interest Group (ITMIG) in 2010 represented a major step forward towards the advancement of clinical and basic science related to thymic malignancies. In recent years, many Thoracic Societies encouraged the institutions of thymic working groups in their structure. The European Society of Thoracic Surgeons (ESTS), the most representative general thoracic surgical society in the world, started its thymic working group in 2010 with the intent to provide a common platform to its members interested in thymic tumors.
The ESTS thymic group first met at the ESTS annual meeting in Valladolid, Spain in 2010 where a list of interested centers were identified and a survey was designed about the current management of thymic tumors among ESTS members.
At the next ESTS annual meeting in Marseille, France in 2011 the ESTS thymic group launched the ESTS thymic retrospective database project to collect data of patients submitted to surgical resection of thymic tumors among interested ESTS centers.
At the 2012 ESTS annual meeting in Essen, Germany, the preliminary results of the thymic retrospective database were presented; on that occasion, it was decided to support a dedicated thymic section in the ESTS Registry using the official platform of the ESTS database (Dendrite Clinical System Italia srl.).

9
Finally, at the 2013 ESTS annual meeting in Birmingham, U.K., the ESTS prospective thymic database was officially launched into the thymic section of the ESTS Registry, where any ESTS member may upload his/her patients with thymic tumors prospectively. The major products of this extraordinary collaborative effort supported by ESTS have been 3 papers which have been published in the last 3 years, covering important aspects of the management of thymic tumors. The results of the survey were published in 2011 (J ThoracOncol 2011;6(3):614-‐23), followed by the analysis of the entire cohort of patients with thymic tumors in the ESTS database (Eur J CardiothoracSurg 2014; [Epub ahead of print]), and the subgroup analysis on patients with thymic carcinoma (J ThoracOncol 2014;9(4):541-‐8) Participation to the prospective thymic database is open to any ESTS Institution and it is strongly encouraged by ESTS. Access to the ESTS thymic database is through the ESTS general database via ESTS website. A personal login account can be requested by filling an application form which can be downloaded from the ESTS homepage. By joining the ESTS thymic prospective database, any participating institution may benefit, in addition to the current general benefits of the ESTS Registry (as mentioned in another part of the present report) from the following dedicated benefits:
• Being part of the ESTS thymic working group • Full access to the Registry data for studies, subjective to the approval of the project draft
by the ESTS Database Committee and the Thymic Group Steering Committee. Authorship rules are similar to those proposed for the Lung Cancer Section of the ESTS Registry.
• Full access to its own data in a standardized ESTS-‐endorsed dataset for internal analysis The ESTS thymic database therefore offers ESTS members a unique opportunity to work in a collaborative way with top-‐quality Institutions on the fascinating fields of thymic tumors, to be part of an active ESTS working group, to foster clinical research projects on thymic malignancies and, last but not least, to help consolidate the leading role of ESTS on different topics in the field of thoracic surgery, and to guide our current practice based on recent knowledge. I look forward to your participation to the ESTS thymic database.
Dr. Enrico Ruffini Chair of the ESTS Thymic Working Group [email protected]

10
The European Society of Thoracic Surgeons Database The European Society of Thoracic Surgeons Database was founded in 2001 by the ESTS Database Committee with the aim to develop risk-‐adjusted instruments for assessing the performance of thoracic surgery units across Europe. The first version of the Database lead to the publication of the first risk-‐ adjusted multinational risk-‐score for mortality (Berrisford R et al. Eur J Cardiothorac Surg 2005; 28:305-‐311) which has been already applied to compare the performance of different units (Brunelli A et al. Eur J Cardiothorac Surg 2008; 33:284-‐288). The second version of the Database was launched online in July 2007 and has so far accrued approximately 205 general thoracic surgical units. Data is anonymously reported, independently accessed and encrypted to other users. Participation to the Database project is totally free and voluntary, but strongly recommended by our Society. You can access the Database from ESTS website or by using the address: https://ests.dendrite.it/csp/ests/intellect/login.csp. To join the Database you need your own personal login account that you can request by downloading and completing an application form from the ESTS homepage (http://www.ests.org). To the benefit of your patients, your practice and your specialty, your data will contribute to the followings:
• Development of European benchmarks of performance through the analysis of outcomes and processes of care indicators.
• Performance assessment by risk-‐adjusted outcome and/or process indicators, which will allow you to compare your own institutional performance against European benchmarks.
• Analysis and development of new potential outcomes and processes of care indicators that may complement/substitute current quality of care measures.
• Implement a provider-‐led quality monitoring and improvement program with the aim to improve your practice.
• Feedback to document quality efforts and areas for improvement in quality of care. • Data for research projects, which can be used to assess new technologies/pathways of care
that can ultimately lead to improved patient care and outcomes. • Maintain your own data if data is requested or mandated by third parties. • Use for local hospital administration resource allocation. • Use for individual negotiations, public relations and expert witness. • Opportunity to participate in a European quality improvement effort for general thoracic
surgery that has a positive impact at the local, national and international levels. Participants benefits
• Participation to the ESTS Database is a pre-‐requisite to participate in the European Institutional Quality certification program.
• Participation will be acknowledged and, if requested, local institutional administrations made aware that your unit is enrolled in a European Thoracic Database aimed at implementing quality of care monitoring and improvement programs endorsed by ESTS and pre-‐requisite for future clinical Institutional European Accreditation.
• Your own data, collected in a standardized ESTS-‐endorsed Dataset, can be downloaded at local level and used for your internal quality analyses or institutional research purposes.
• As a future project, participants will receive a periodic confidential feedback on the quality of their data and their performance against International benchmarks.

11
• Participants can propose their own research projects based on the total data present in the database. Projects should be submitted to the ESTS database Committee for peer review and, if accepted, the requested and anonymized data will be provided to the proponent of the project. ESTS will retain the responsibility for the final analysis and interpretation of results. The proponent of the project will be the first Author of the final manuscript and he/she will be allowed to include, if requested, additional two colleagues, who helped in the elaboration of the manuscript. The members of the Database Committee who contributed to the review process and assisted in the development of the manuscript will be also included in the list of Authors.
As the ESTS Database approached a more mature stage, and more demanding aspects of data management will be required, it has been decided to make use of professional expertise in running and managing contents, data flow, data merge and so on of our Registry; in Nov 2009 the ESTS Council awarded this task to Dendrite Clinical System Italia srl. Since 1993 Dendrite has established a highly respected track record in setting up and running a variety of International Registries, with an underlying philosophy of long term partnership with numerous Clinical Associations within and outside Europe. The main reasons for their widespread activity in this field include:
• Bottom-‐up approach to data management: the range of products and services starts from database and electronic patient records and serves Clinicians daily needs; it escalates to hospital-‐wide systems, to regional, national and finally to international registries.
• User-‐friendly inclusion of all who wish to participate: Import Data Module allows any Contributor to use his chosen type of tool to collect data, and Dendrite will perform the correspondence and data merge required to add their data to the main ESTS Database, if there is conformity with the required dataset.
• Fool-‐proof suite of clinical statistical analysis integrated in the central data collection installation (server).
• Contributors can retain, download and use own data, from the ESTS site, in MS Excel format, which lends itself to be analyzed by any clinical software product.
• Unblemished track record of data handling integrity: not ever lost, leaked or misplaced third Party data to date.

12
KEY MESSAGES FROM THIS REPORT
1. The ESTS database is growing: from 56,656 procedures in 2012 to 66,623 in 2013. The database growth is a slow process, because it requires a change in prospective participants practice.
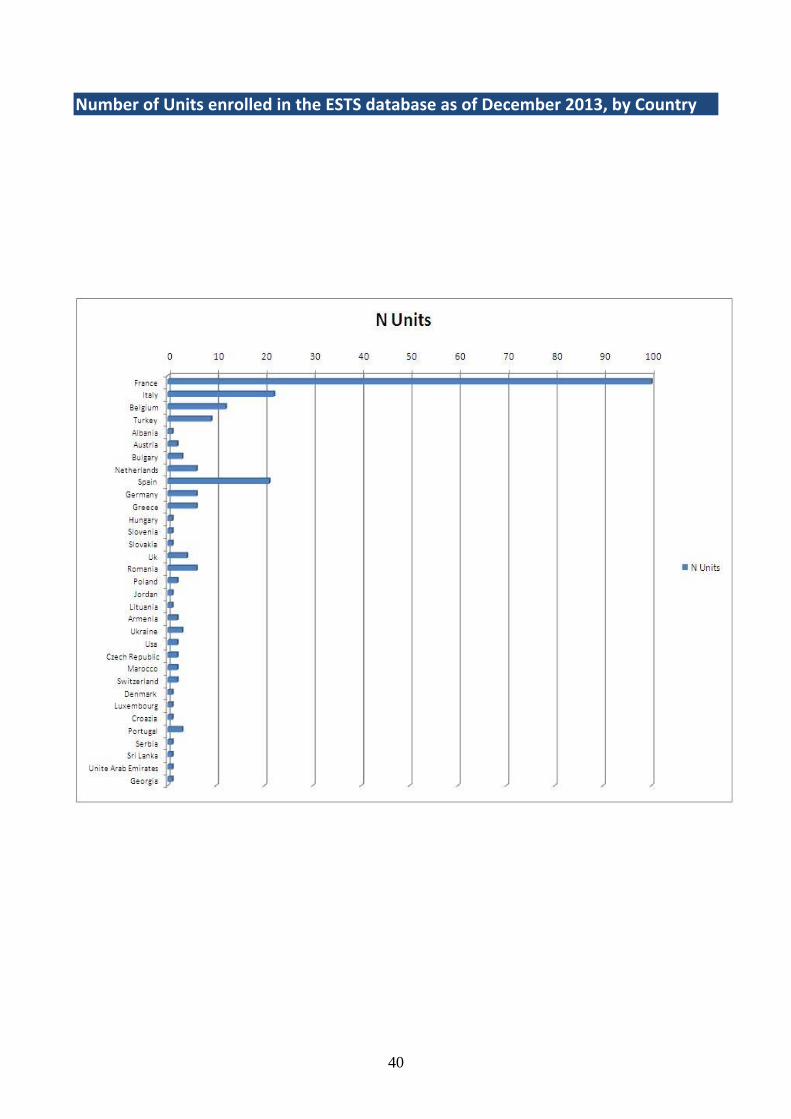
2. The majority of contributions to the ESTS database is direct from willing units and participants; only one nation (France) contributes to the database as a whole. More countries are expected in a near future, among which: Hungary, the Netherlands, Poland…
3. Completeness of the database is almost 100% in the major fields of the database, except for 30-‐day mortality.
4. The vast majority of ESTS database procedures is dedicated to lung surgery (n=53,486 patients), representing 80% of the procedures.
5. In lung resections, the proportion of VATS dramatically increases from 12.1% to 25.5% between 2007-‐2010 and 2011-‐2013. More specifically, VATS lobectomy increases from 4% to 17% between these two periods.
6. 30-‐day mortality of the entire ESTS database reaches 2% over the period 2011-‐2013, which corresponds to the international standards of other databases, such as the UK and USA.
7. 30-‐day mortality of the entire ESTS database decreased by 2 along the study period (2007-‐2013). This virtuous process implicitly means that “the longer the participation in the ESTS database, the better the outcome”.
8. Observed versus predicted mortality rates after major lung resections shows important discrepancies among European countries, indicating the need of starting to work on a new and refined predictive model.
9. Outcomes measured with feedback programs, benchmark and self-‐assessment capabilities – such as the ESTS database – are effective in improving surgical safety and patient care.
10. The ESTS database is a useful tool for surgeons as a benchmark of the thoracic surgical practice in Europe.

13
PART 1
EUROPEAN DATABASE
CUMULATIVE ACTIVITY (2007-‐2013)

14
Overall age and gender distributions Age (years)
Occurrences Percent ≤ 20 1530 2.3 21-‐30 2660 4.0 31-‐40 3157 4.7 41-‐50 7058 10.6 51-‐60 16831 25.3 61-‐70 20528 30.8 71-‐80 13121 19.7 >80 1645 2.5 Unknown 93 0.1 Total 66623 100.0

15
Gender according to age distribution (years)
Male (%) Female (%) ≤ 20 2.3 1.9 21-‐30 3.7 4.6 31-‐40 3.9 6.4 41-‐50 8.9 13.9 51-‐60 24.4 26.9 61-‐70 32.7 27.0 71-‐80 21.2 16.7 >80 2.5 2.4 Unknown 0.3 0.3

16
Total surgical activity within the entire dataset Group Definitions
Occurrences Percent Lung 53486 80.3 Pleura 4307 6.5 Chest Wall 1506 2.3 Trachea -‐ Bronchus 461 0.7 Mediastinum 4979 7.5 Upper GI 250 0.4 Diaphragm 133 0.2 Unknown 1501 2.3 Total 66623 100.0

17
Lung Subgroup
Occurrences Percent Lung Biopsy 1030 1.9 Lung Excision 51112 95.6 Lung Lesion 931 1.7 Lung Repair 267 0.5 Lung Transplant 88 0.2 Unknown 58 0.1 Total 53486 100

18
Mediastinum Subgroup
Occurrences Percent Mediastinoscopy 2631 52.8 Mediastinotomy 322 6.5 Mediastinum 1841 37 Thoracic Duct 9 0.2 Thyroid 145 2.9 Unknown 31 0.6 Total 4979 100
19
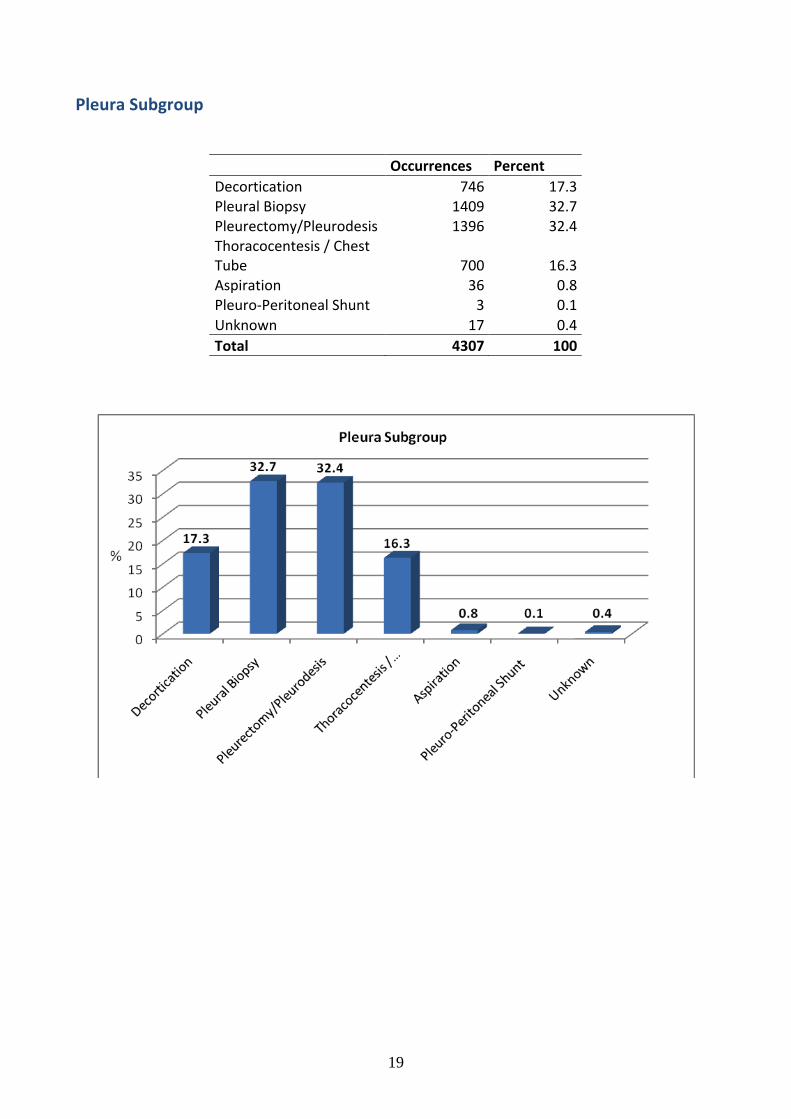
Pleura Subgroup
Occurrences Percent Decortication 746 17.3 Pleural Biopsy 1409 32.7 Pleurectomy/Pleurodesis 1396 32.4 Thoracocentesis / Chest Tube 700 16.3 Aspiration 36 0.8 Pleuro-‐Peritoneal Shunt 3 0.1 Unknown 17 0.4 Total 4307 100

20
Chest Wall Subgroup
Occurrences Percent Chest Wall 946 62.8 Costal Cartilage 58 3.9 Chest wall Incision 193 12.8 Reconstruction 118 7.8 Rib 141 9.4 Thoracoplasty 43 2.9 Unknown 7 0.5 Total 1506 100
21
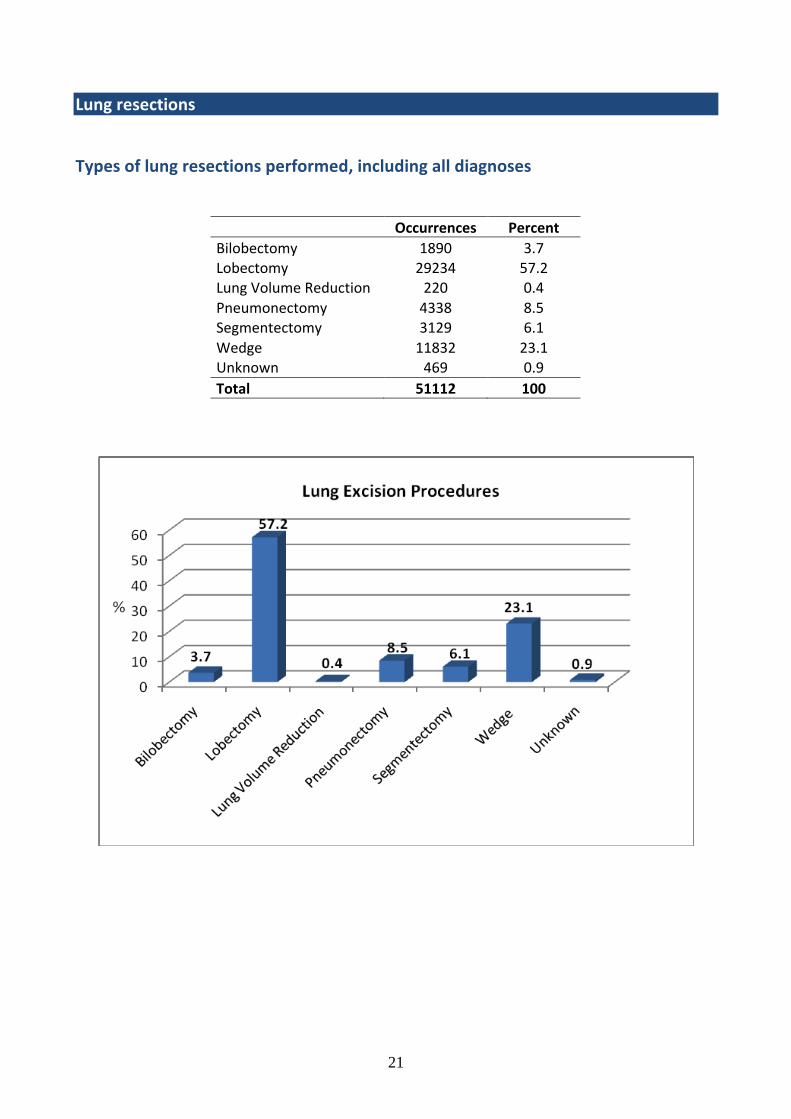
Lung resections Types of lung resections performed, including all diagnoses
Occurrences Percent Bilobectomy 1890 3.7 Lobectomy 29234 57.2 Lung Volume Reduction 220 0.4 Pneumonectomy 4338 8.5 Segmentectomy 3129 6.1 Wedge 11832 23.1 Unknown 469 0.9 Total 51112 100
22
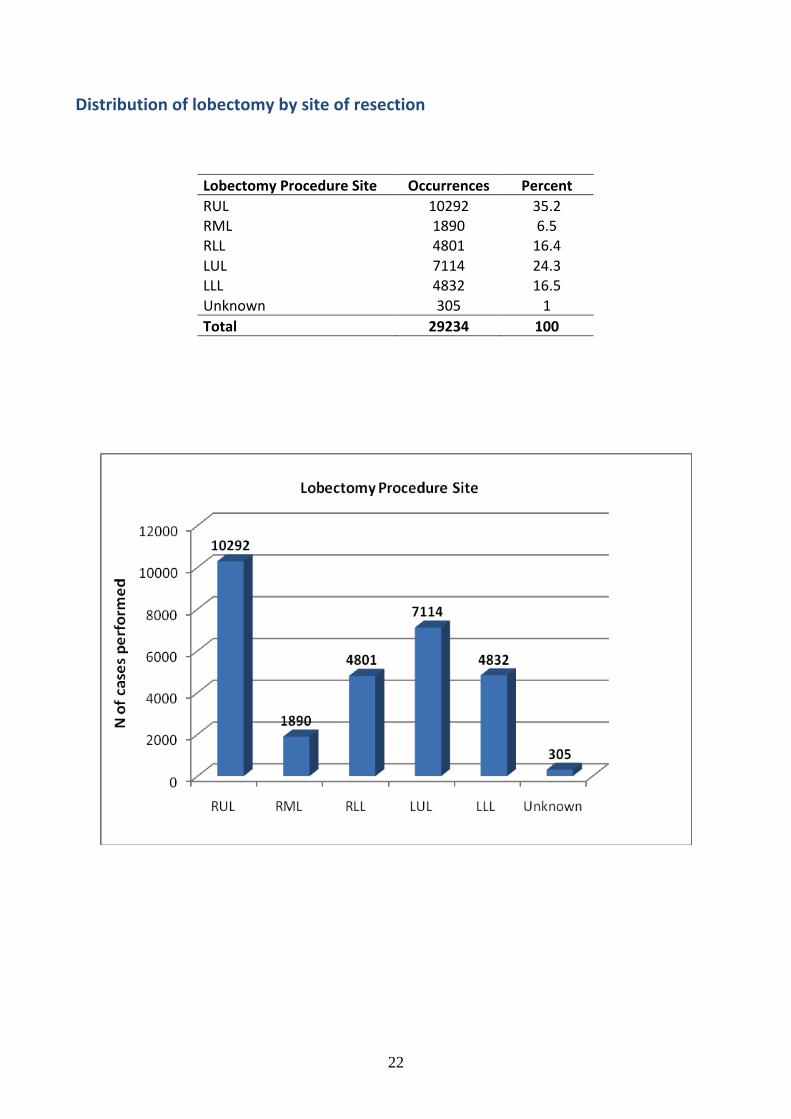
Distribution of lobectomy by site of resection
Lobectomy Procedure Site Occurrences Percent RUL 10292 35.2 RML 1890 6.5 RLL 4801 16.4 LUL 7114 24.3 LLL 4832 16.5 Unknown 305 1 Total 29234 100

23
Distribution of bilobectomy by site of resection
Bilobectomy Procedure Site Occurrences Percent RUM 791 41.9 RLM 1088 57.6 Unknown 11 0.6 Total 1890 100
24
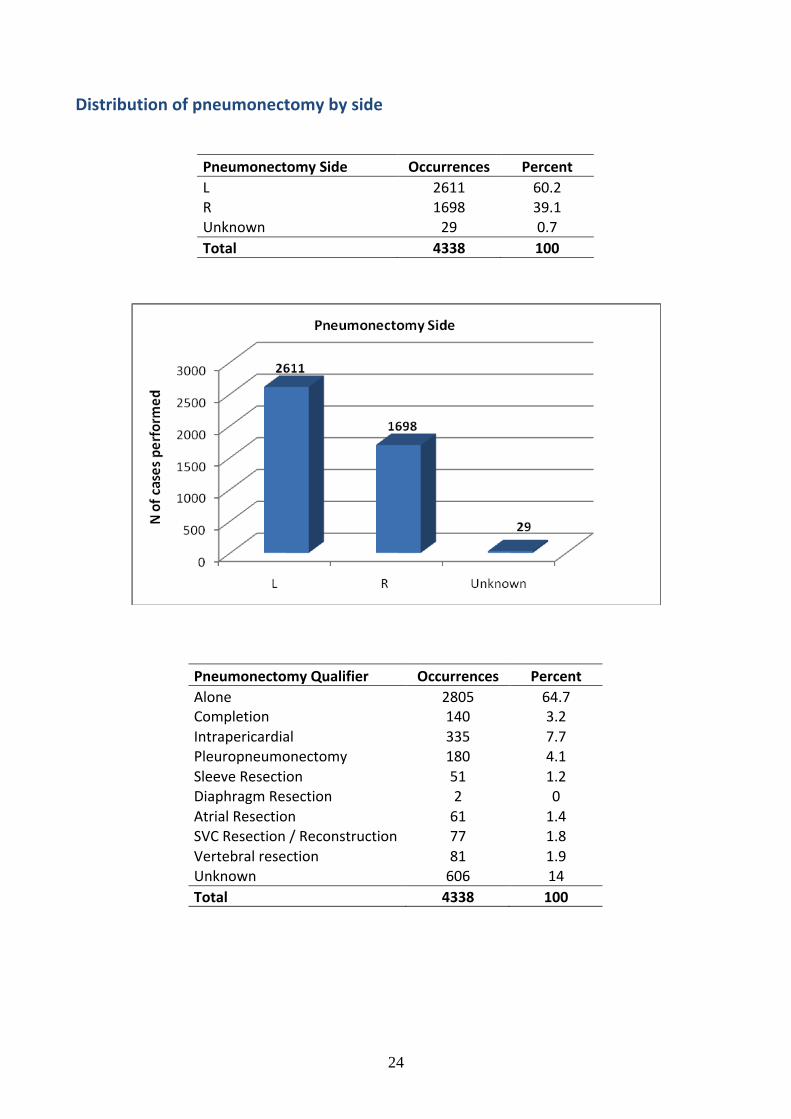
Distribution of pneumonectomy by side
Pneumonectomy Side Occurrences Percent L 2611 60.2 R 1698 39.1 Unknown 29 0.7 Total 4338 100
Pneumonectomy Qualifier Occurrences Percent Alone 2805 64.7 Completion 140 3.2 Intrapericardial 335 7.7 Pleuropneumonectomy 180 4.1 Sleeve Resection 51 1.2 Diaphragm Resection 2 0 Atrial Resection 61 1.4 SVC Resection / Reconstruction 77 1.8 Vertebral resection 81 1.9 Unknown 606 14 Total 4338 100

25
VATS as a proportion of all lung resections
VATS Occurrences Percent No 41843 81.9 Yes 9114 17.8 Unknown 155 0.3 Total 51112 100
No Yes Yes (%) 2007-‐2010 25400 3488 12.1 2011-‐2013 16443 5626 25.5 Total 41843 9114
VATS as a proportion of lobectomy
No Yes Yes (%) 2007-‐2010 16099 672 4.0 2011-‐2013 10322 2115 17.0 Total 26421 2787

26
Lung resections pathology
Morphology Occurrences Percent Non Neoplastic 5903 11.5 Neoplastic Benign 1799 3.5 Neoplastic Malignant Primary 34862 68.2 Neoplastic Malignant Secondary 7351 14.4 Unknown 1197 2.3 Total 51112 100
27
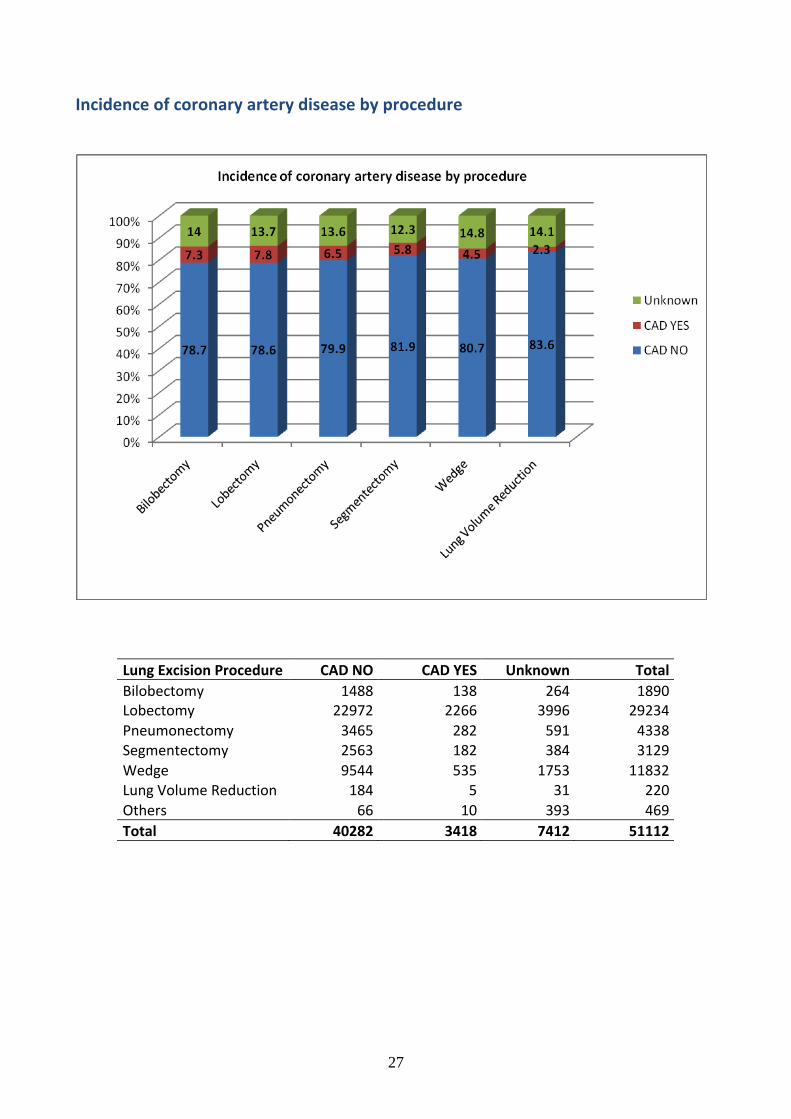
Incidence of coronary artery disease by procedure
Lung Excision Procedure CAD NO CAD YES Unknown Total Bilobectomy 1488 138 264 1890 Lobectomy 22972 2266 3996 29234 Pneumonectomy 3465 282 591 4338 Segmentectomy 2563 182 384 3129 Wedge 9544 535 1753 11832 Lung Volume Reduction 184 5 31 220 Others 66 10 393 469 Total 40282 3418 7412 51112
28
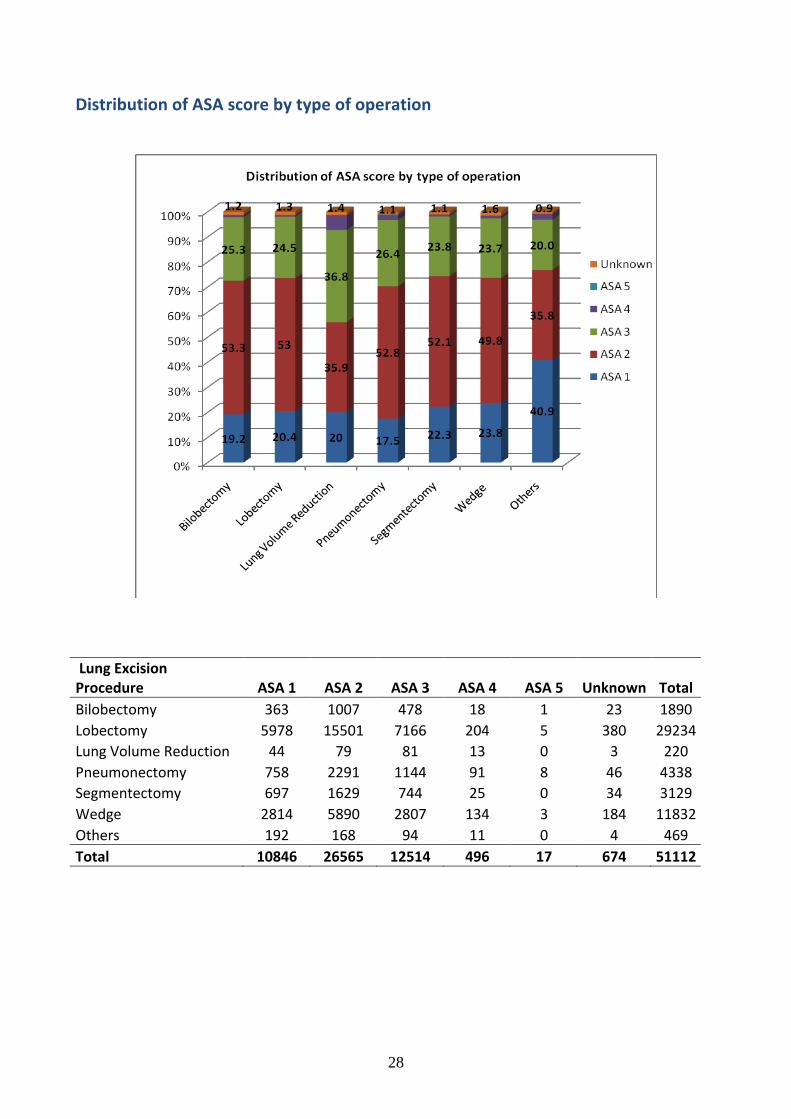
Distribution of ASA score by type of operation
Lung Excision Procedure ASA 1 ASA 2 ASA 3 ASA 4 ASA 5 Unknown Total Bilobectomy 363 1007 478 18 1 23 1890 Lobectomy 5978 15501 7166 204 5 380 29234 Lung Volume Reduction 44 79 81 13 0 3 220 Pneumonectomy 758 2291 1144 91 8 46 4338 Segmentectomy 697 1629 744 25 0 34 3129 Wedge 2814 5890 2807 134 3 184 11832 Others 192 168 94 11 0 4 469 Total 10846 26565 12514 496 17 674 51112

29
Distribution of ECOG score by type of operation
Lung Excision Procedure ECOG 0 ECOG 1 ECOG 2 ECOG 3 ECOG 4 Unknown Total Bilobectomy 838 767 136 22 2 125 1890 Lobectomy 13628 11229 2107 208 41 2021 29234 Lung Volume Reduction 45 98 44 11 0 22 220 Pneumonectomy 1736 1798 364 68 26 346 4338 Segmentectomy 1551 1109 222 32 7 208 3129 Wedge 5332 4399 968 197 38 898 11832 Others 261 143 37 9 3 16 469 Total 23391 19543 3878 547 117 3636 51112

30
Cardiopulmonary morbidity rate in different types of lung resections
CM No CM Yes Unknown Total Bilobectomy 1168 526 196 1890 Lobectomy 20212 5617 3405 29234 Lung Volume Reduction 162 31 27 220 Pneumonectomy 2755 1206 377 4338 Segmentectomy 2393 348 388 3129 Wedge 9617 672 1543 11832 Unknown 4 8 457 469
Total 36311 8408 6393 51112

31
Incidence of prolonged air leak (> 5days) in different types of lung resections
Air Leak > 5 days
Lung Excision -‐ PROCEDURE No (%) Yes (%) Unknown (%) Bilobectomy 82.3 11.2 6.5 Lobectomy 83.3 8.6 8.0 Lung Volume Reduction 71.4 23.6 5.0 Segmentectomy 83.5 6.7 9.8 Wedge 85.6 3.5 10.9
Total 85.3 6.3 8.4
Incidence of bronchopleural fistula (BPF) in pneumonectomy
BPF No BPF Yes Unknown Total Pneumonectomy (N) 3968 96 274 4338 Pneumonectomy (%) 91.5 2.2 6.3 100
32
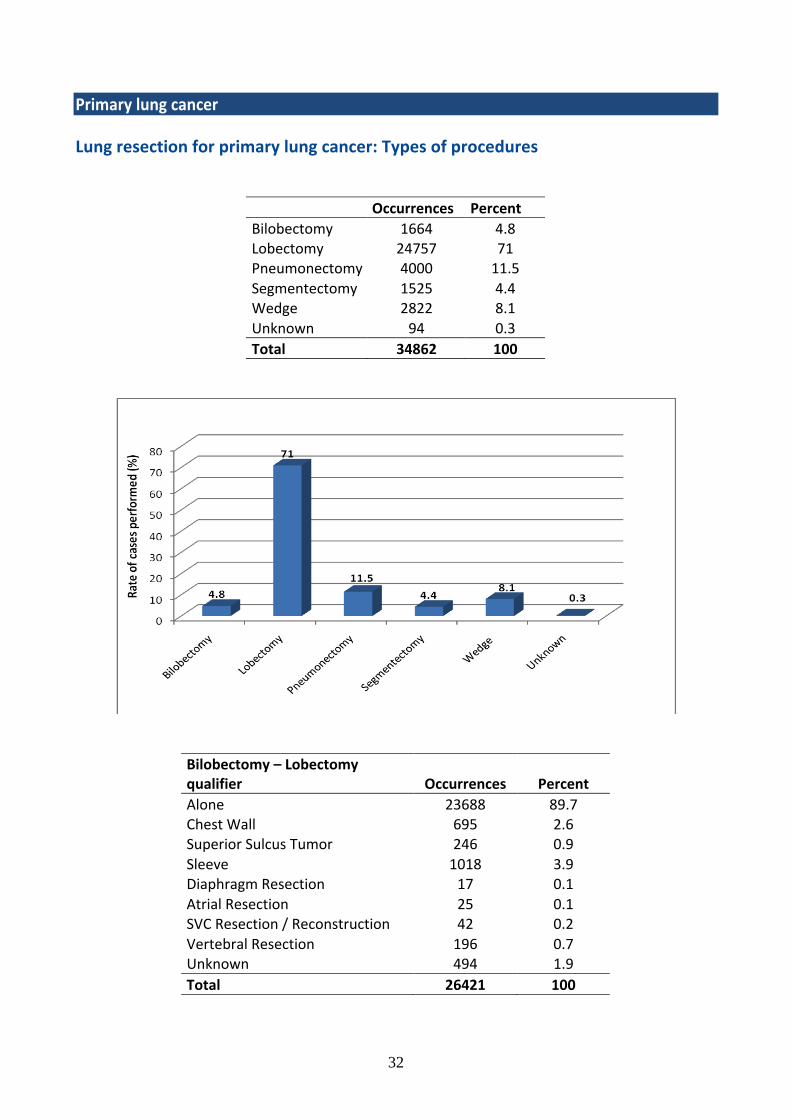
Primary lung cancer Lung resection for primary lung cancer: Types of procedures
Occurrences Percent Bilobectomy 1664 4.8 Lobectomy 24757 71 Pneumonectomy 4000 11.5 Segmentectomy 1525 4.4 Wedge 2822 8.1 Unknown 94 0.3 Total 34862 100
Bilobectomy – Lobectomy qualifier Occurrences Percent Alone 23688 89.7 Chest Wall 695 2.6 Superior Sulcus Tumor 246 0.9 Sleeve 1018 3.9 Diaphragm Resection 17 0.1 Atrial Resection 25 0.1 SVC Resection / Reconstruction 42 0.2 Vertebral Resection 196 0.7 Unknown 494 1.9 Total 26421 100

33
Distribution of lobectomy/bilobectomy by site of resection
Lobectomy procedure site Occurrences Percent RUL 9099 36.8 RML 1275 5.2 RLL 3974 16.1 LUL 6265 25.3 LLL 3894 15.7 Unknown 250 1 Total 24757 100
Bilobectomy procedure site Occurrences Percent RUM 675 40.6 RLM 979 58.8 Unknown 10 0.6 Total 1664 100

34
Distributions of pneumonectomy
Pneumonectomy Qualifier Occurrences Percent Alone 2616 75.9 Completion 109 3.2 Intrapericardial 304 8.8 Pleuropneumonectomy 148 4.3 Sleeve Resection 50 1.5 Diaphragm Resection 2 0.1 Atrial Resection 61 1.8 SVC Resection / Reconstruction 77 2.2 Vertebral resection 79 2.3 Total 3229 100.0
Pneumonectomy side Occurrences Percent L 2406 60.2 R 1566 39.2 Unknown 28 0.7 Total 4000 100

35
Distribution of VATS procedures in total lung resections
VATS Occurrences Percent No 30867 88.5 Yes 3857 11.1 Unknown 138 0.4 Total 34862 100
Distributions of VATS procedures in lobectomy/bilobectomy
VATS Occurrences Percent No 24003 90.8 Yes 2393 9.1 Unknown 25 0.1 Total 26421 100

36
Unadjusted in-‐hospital mortality rates in primary lung cancer resections
Outcome at Discharge -‐ Died in Hospital Occurrences Died in Hospital Percent
Bilobectomy 1631 67 4.1 Lobectomy 24043 541 2.3 Pneumonectomy 3917 246 6.3 Segmentectomy 1492 29 1.9 Wedge 2770 46 1.7 Total 33853 929 2.7
Overall unadjusted in-‐hospital mortality calculated in the total dataset (Only centers with yearly major resections N>50 were included)
37
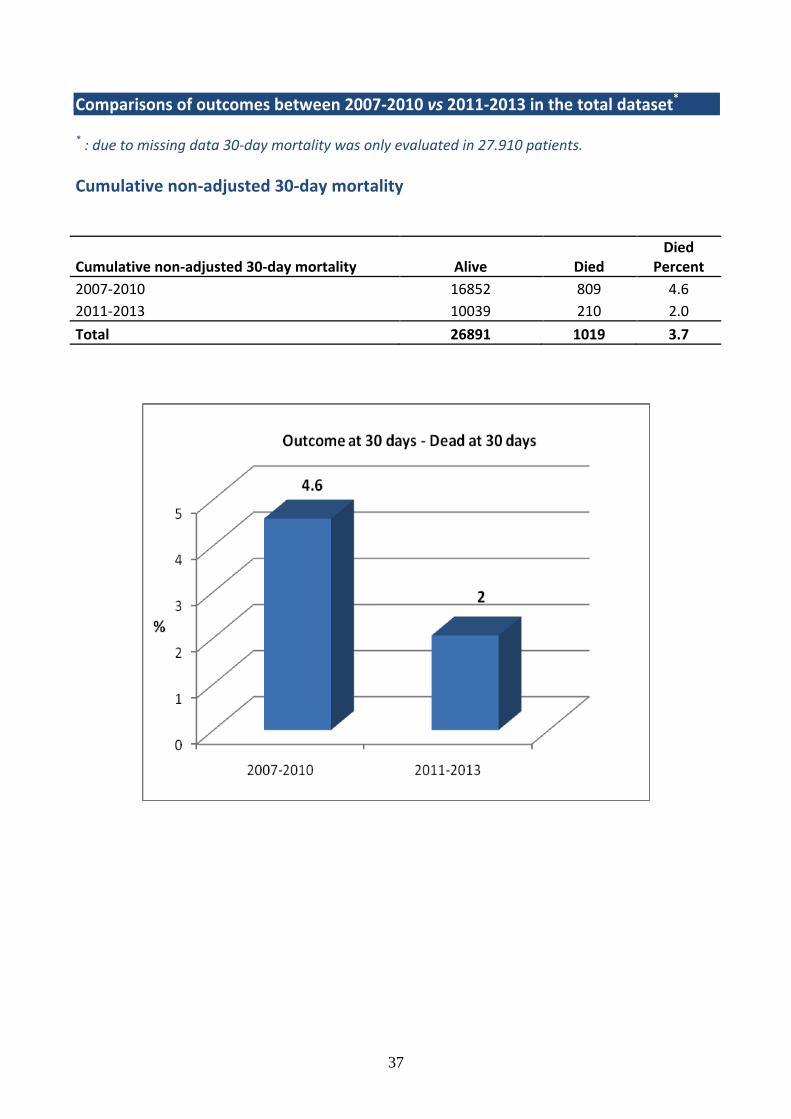
Comparisons of outcomes between 2007-‐2010 vs 2011-‐2013 in the total dataset*
* : due to missing data 30-‐day mortality was only evaluated in 27.910 patients. Cumulative non-‐adjusted 30-‐day mortality
Cumulative non-‐adjusted 30-‐day mortality Alive Died Died
Percent 2007-‐2010 16852 809 4.6 2011-‐2013 10039 210 2.0
Total 26891 1019 3.7

38
Prolonged air leak
Air leak > 5 Days No Yes Yes (%)
2007-‐2010 34576 2020 5.5 2011-‐2013 21912 1858 7.8
Total 56488 3878 6.4

39
PART 2
NATION-‐SPECIFIC ACTIVITY &
COMPARATIVE ANALYSIS
BETWEEN CONTRIBUTING COUNTRIES
Only countries contributing more than 100 lung resections were included
40
Number of Units enrolled in the ESTS database as of December 2013, by Country

41
Epidemiologic data Proportion of elderly patients (older than 70 years of age) operated on in different European countries
(°): Country with less than 500 patients included, results must be interpreted with caution

42
Percentage of patients submitted to major anatomic lung resections with preoperative measurement of DLCO in different European Countries.
(°): Country with less than 500 patients included, results must be interpreted with caution

43
Percentage of patients with primary neoplastic disease and suspicious clinical N2 stage (enlarged >1cm mediastinal nodes at CT scan or PET positive mediastinal nodes) who underwent at least one preoperative invasive mediastinal staging procedure (EBUS, EUS, mediastinoscopy, mediastinotomy, VATS, TEMLA etc.)
(°): Country with less than 500 patients included, results must be interpreted with caution

44
Percentage of patients submitted to lymph node dissection during major lung resection for malignant primary neoplastic disease grouped by Countries Lymph node dissection more extended than sampling alone or selected biopsy (as defined and recommended by the ESTS guidelines for intraoperative mediastinal staging) in lung cancer patients was a frequent procedure in all countries. This variable will be included in the composite performance score (CPS) used for the ESTS quality certification program.
(°): Country with less than 500 patients included, results must be interpreted with caution

45
Primary lung cancer per contributing Nations Percentage of lung excision procedures Bilobectomy Lobectomy Pneumonectomy Segmentectomy Wedge Unknown FRANCE 4.7% 70.9% 11.4% 4.4% 8.3% 0.3% ITALY 3.4% 73.7% 8.0% 4.9% 9.7% 0.2% BELGIUM 6.0% 67.6% 12.7% 4.5% 9.2% 0.1% HUNGARY 3.7% 77.3% 10.2% 5.1% 3.7% 0% NETHERLANDS 7.5% 79.4% 7.3% 0.9% 4.5% 0.3% SPAIN 4.5% 70.9% 11.1% 4.0% 9.5% 0.1% ROMANIA 5.0% 61.1% 25.5% 0.1% 8.2% 0.1% TURKEY 8.1% 70.2% 13.4% 3.3% 5.0% 0.0% ALBANIA° 7.6% 61.0% 26.3% 1.7% 3.4% 0% GERMANY° 5.3% 68.3% 14.0% 9.9% 2.5% 0% GREECE° 3.6% 53.8% 17.9% 18.8% 5.8% 0% SLOVAKIA° 3.7% 85.2% 9.6% 1.5% 0% 0% SLOVENIA° 6.4% 84.4% 9.2% 0% 0% 0% UK° 6.6% 81.8% 9.9% 0.8% 0.8% 0%
(°): Country with less than 500 patients included, results must be interpreted with caution

46
Percentage of Lobectomy – Bilobectomy
Alone Chest Wall
Superior Sulcus Tumor Sleeve
Diaphragm Resection
Atrial Resection
SVC Resection /
Reconstruction Vertebral Resection Unknown
FRANCE 90.3% 2.2% 0.8% 3.0% 0.0% 0.1% 0.2% 1.1% 2.4% ITALY 95.1% 2.4% 0.1% 2.0% 0.0% 0.1% 0.0% 0.0% 0.4% BELGIUM 84.2% 2.3% 2.2% 10.6% 0.2% 0.1% 0.1% 0.0% 0.3% HUNGARY 92.8% 2.7% 0.2% 2.8% 0.1% 0.0% 0.2% 0.0% 1.2% NETHERLANDS 80.5% 3.2% 6.6% 8.2% 0.5% 0.0% 0.0% 0.2% 0.7% SPAIN 89.4% 4.2% 1.1% 3.9% 0.1% 0.2% 0.1% 0.0% 1.0% ROMANIA 83.0% 6.9% 2.5% 7.5% 0.0% 0.0% 0.0% 0.0% 0.0% TURKEY 75.0% 6.3% 0.7% 15.5% 0.7% 0.4% 0.2% 0.4% 0.9% GERMANY° 81.6% 10.6% 0.6% 3.4% 2.2% 1.1% 0.6% 0.0% 0.0% GREECE° 94.5% 3.9% 0.0% 0.8% 0.0% 0.8% 0.0% 0.0% 0.0% SLOVAKIA° 97.5% 1.7% 0.0% 0.8% 0.0% 0.0% 0.0% 0.0% 0.0% SLOVENIA° 87.9% 3.0% 1.0% 6.1% 1.0% 0.0% 0.0% 0.0% 1.0% UK° 95.3% 4.7% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0%
(°): Country with less than 500 patients included, results must be interpreted with caution

47
Percentage of pneumonectomy (qualifier)
Alone
Completion
Intrap
ericardial
Pleu
ropn
eumon
ectomy
Slee
ve Resection
Diaph
ragm
Resection
Atrial R
esection
SVC Re
section /
Reconstruction
Vertebral resection
Unk
nown
FRANCE 77.2% 0.5% 0.1% 3.3% 1.2% 0% 2.0% 2.7% 2.8% 10.2% ITALY 31.8% 8.6% 24.7% 6.6% 1.0% 0.5% 0% 0% 0% 26.8% BELGIUM 46.4% 8.9% 33.3% 2.1% 0.4% 0% 0.4% 0% 0.8% 7.6% HUNGARY 70.4% 1.9% 19.4% 5.6% 0% 0% 0% 0% 0% 2.8% NETHERLANDS 36.2% 10.6% 21.3% 8.5% 0% 0% 0% 0% 0% 23.4% SPAIN 48.1% 6.6% 21.4% 7.0% 1.2% 0% 0.4% 0.8% 0% 14.4% ROMANIA 17.4% 4.3% 18.5% 3.3% 4.3% 0% 0.5% 0% 0% 51.6% TURKEY 49.5% 6.2% 19.6% 0% 1.0% 0% 0% 0% 0% 23.7% GERMANY° 8.8% 32.4% 14.7% 14.7% 2.9% 2.9% 8.8% 5.9% 0% 8.8% GREECE° 10.0% 10% 32.5% 0% 0% 0% 0% 0% 0% 47.5% SLOVAKIA° 100.0% 0% 0% 0% 0% 0% 0% 0% 0% 0% SLOVENIA° 30.0% 20% 10.0% 0% 10.0% 0% 0% 0% 0% 30% UK° 0% 8.3% 33.3% 0% 0% 0% 0% 0% 0% 58.3% ALBANIA° 35.5% 3.2% 38.7% 6.5% 0% 0% 3.2% 0% 0% 12.9%
(°): Country with less than 500 patients included, results must be interpreted with caution

48
Percentage of VATS
No Yes Unknown FRANCE 82.5 17.5 0 ITALY 82.4 17.0 0.6 SPAIN 84.0 16.0 0 BELGIUM 68.1 27.0 4.9 HUNGARY 72.3 27.1 0.6 ROMANIA 96.4 3.6 0 TURKEY 79.4 20.5 0.1 NETHERLANDS 74.5 24.9 0.6 GREECE° 83.5 15.7 0.8 GERMANY° 87.2 12.8 0 SLOVAKIA° 89.3 10.7 0 UK° 98.9 1.1 0 ALBANIA° 100.0 0.0 0 PORTUGAL° 58.1 41.9 0 SLOVENIA° 73.3 26.7 0
(°): Country with less than 500 patients included, results must be interpreted with caution

49
Observed versus predicted in-‐hospital mortality rates of major lung resections in different European Countries (risk adjustment according to Brunelli A et al. The European Thoracic Database project: Composite Performance Score to measure quality of care major lung resection. Eur J Cardiothorac Surg 2009; 35: 769-‐774).
Predicted and Observed Mortality rates (%) Predicted Mortality Observed Mortality FRANCE 2.2 3.0 ITALY 3.0 1.6 SPAIN 3.0 3.1 BELGIUM 3.1 2.5 HUNGARY 3.0 1.2 ROMANIA 3.9 1.7 TURKEY 2.9 3.4 NETHERLANDS° 2.9 3.2 GREECE° 2.7 6.0 GERMANY° 3.1 7.1 SLOVAKIA° 2.4 0.6 UK° 3.5 0.8 ALBANIA° 2.2 5.7 SLOVENIA° 2.9 0.9 (°): Country with less than 500 patients included, results must be interpreted with caution
50
PART 3
THYMOMA SECTION
(online version only)

51
Thymoma Section fields The thymoma section of the 2014 ESTS silver book is a novel section which reports the collaborative effort brought forward by the ESTS thymic working group with the help of the official platform of the ESTS database (Dendrite Clinical System, Italia srl), to prospectively collate patients with thymic tumors for clinical analysis. Several variables have been recorded, including demographics, preoperative information, details on the surgical access and extent of resection, pathological and staging information, notes on perioperative treatments and outcome. The period of collection starts on January 1st, 2007 and it closes on April 30th, 2014 for this edition of the silver book. Overall, data on more than 300 patients have been uploaded, which represents an amazing result for these rare tumors. The reader may scroll through the tables and graphs to have a look at the results, so there is no need to include additional details. However, few points should deserve consideration as an addendum to the data:
1. The number of patients with missing information is quite high: for most data fields a variable percentage from 25% to 44% is reported (page 69). This may result from the process of progressive upload from the centers according to the subsequent acquisition of new information following the discharge of the patient. An increased data completeness rate will supposedly be obtained once the individual centers complete the data acquisition.
2. The graphs and tables mainly mirror the results obtained from the ESTS retrospective database already published (see foreword, page 8-‐9). This is an important finding, which provides a sort of validation of the conclusions reached with the retrospective database.
3. Almost ¾ of the patients (72%) had early-‐stage tumors (Stage I/II). This is a slightly increased percentage as compared with other reports, possibly resulting from the accruing centers referral. An analysis of the distribution by stage corrected by centers and geographic distribution is under way to confirm this finding.
4. Almost 20% of the thymic tumor resections were performed using VATS/robotic techniques. This reflects a sort of changing attitude towards the surgical approach of thymic tumors. It will be interesting to analyze the long-‐term results according to the extent of resection (minimally vs. maximally invasive techniques), which will supposedly be available in the next few years.
In summary, these preliminary results of the ESTS prospective thymic database are extremely encouraging, providing a solid backbone for future implementations. Every ESTS center is welcomed and strongly encouraged to upload his/her patients with thymic tumors to the ESTS Registry. The progressive increase in the number of cases will be of help in the advancement of research for these patients, as well as an important collaborative effort for our society.

52
Thymic Tumors: prospective cases -‐ January 2007-‐ April 2014 -‐ N=305 Demographics: gender and age groups
Gender Occurrences Percent
Male 162 53.1
Female 143 46.9
Total 305 100

53
Associated paraneoplastic syndromes
920 Diagnosis of paraneoplastic -‐Autoimmune syndrome Occurrences Percent
None 95 55.6
Myasthenia Gravis 64 37.4
Red Cell Aplasia 2 1.2
Other autoimmune 10 5.8
Total 171 100 * Percentages calculated at the net of unknown cases (N=134; 43.9%)

54
Previous malignancy
923 Previous malignancy Occurrences Percent
None 153 89.0
Breast 2 1.2
Prostate 4 2.3
Skin 1 0.6
Lymphoma 1 0.6
Other 11 6.4
Total 172 100 * Percentages calculated at the net of unknown cases (N=133; 43.6%)

55
Preoperative diagnosis
924 Biopsy Occurrences Percent
No biopsy 122 71.8
FNA biopsy 5 2.9
Core biopsy 17 10.0
Mediastinotomy 8 4.7
VATS 3 1.8
Minithoracotomy 8 4.7
Other 7 4.1
Total 170 100 * Percentages calculated at the net of unknown cases (N=135; 44.3%)

56
Final pathologic diagnosis
Final pathologic diagnosis Occurrences Percent
Thymoma 162 72.0
Thymic carcinoma 24 10.7
Neuroendocrine thymic tumour (NETT) 6 2.7
Other malignancy 4 1.8
Benign 29 12.9
Total 225 100 * Percentages calculated at the net of unknown cases (N=80; 26.2%)

57
WHO histology (thymoma only)
WHO histology Occurrences Percent
A 17 10.6
AB 41 25.5
B1 35 21.7
B2 41 25.5
B3 27 16.8
Total 161 100.0 * Percentages calculated at the net of unknown cases (N=144;47.2%)

58
Tumor size Tumor size Occurrences Percent
<3cm 28 13.1
3-‐5 cm 66 30.8
>5cm 120 56.1
Total 214 100 * Percentages calculated at the net of unknown cases (N=91; 29.8%)
59
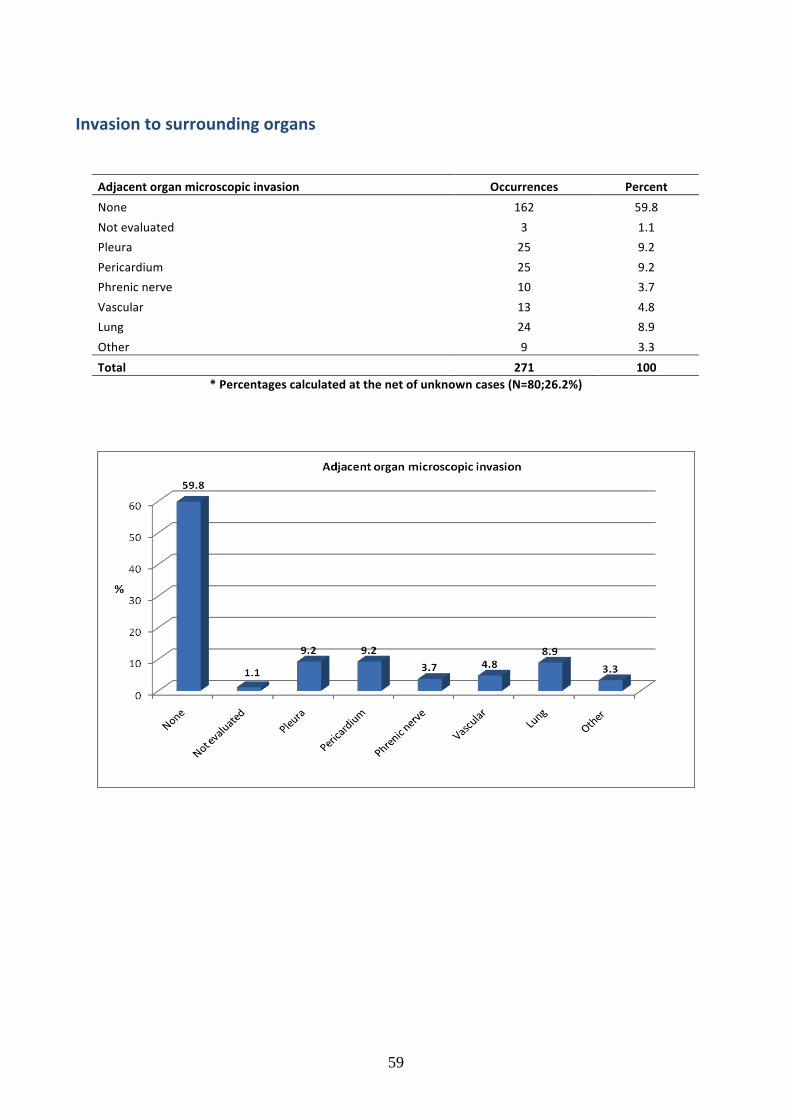
Invasion to surrounding organs
Adjacent organ microscopic invasion Occurrences Percent
None 162 59.8
Not evaluated 3 1.1
Pleura 25 9.2
Pericardium 25 9.2
Phrenic nerve 10 3.7
Vascular 13 4.8
Lung 24 8.9
Other 9 3.3
Total 271 100 * Percentages calculated at the net of unknown cases (N=80;26.2%)

60
Clinical (pre-‐treatment) stage according to Masaoka-‐Koga stage
Clinical (pre-‐treatment) Masaoka-‐Koga Stage Occurrences Percent
I 110 55.3
IIa 20 10.1
IIb 18 9.0
III 34 17.1
IVA 12 6.0
IVB 5 2.5
Total 199 100 * Percentages calculated at the net of unknown cases (N=106;34.8%)

61
Pathologic Masaoka-‐Koga stage Pathologic Masaoka-‐Koga Stage Occurrences Percent
No pathology 9 4.6
I 86 44.1
IIa 34 17.4
IIb 22 11.3
III 27 13.8
IVA 13 6.7
IVB 4 2.1
Total 195 100 * Percentages calculated at the net of unknown cases (N=110;36.1%)
62
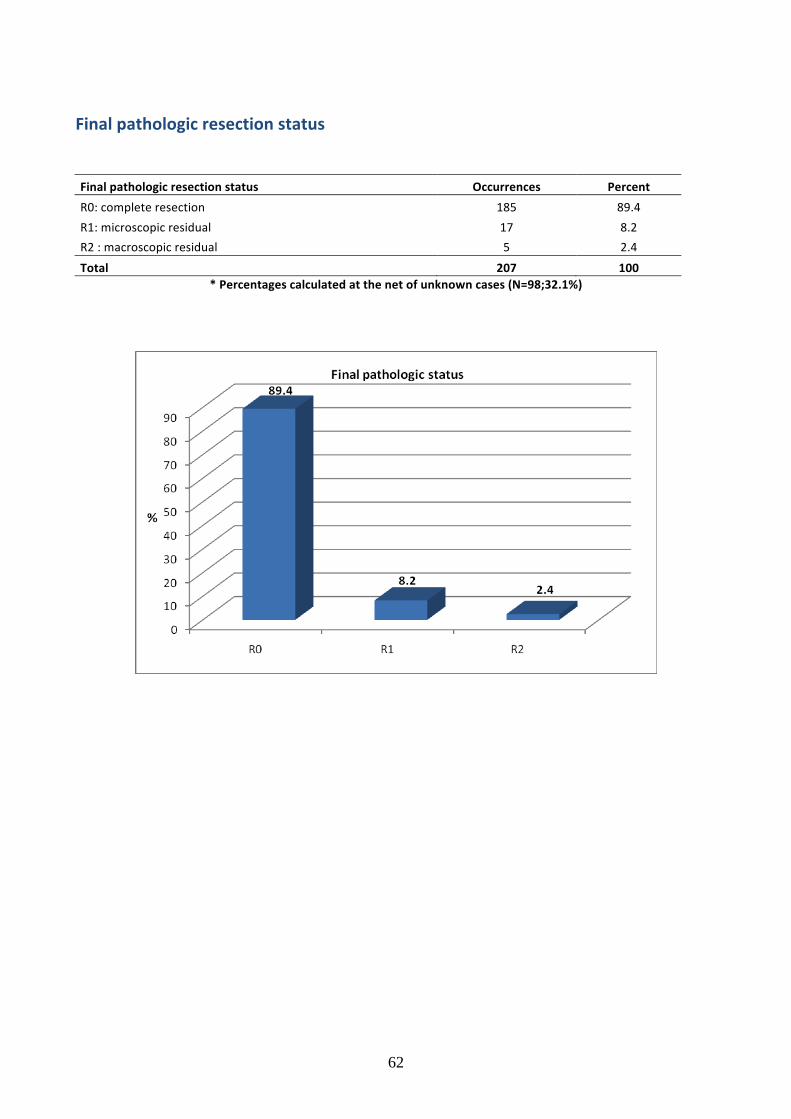
Final pathologic resection status Final pathologic resection status Occurrences Percent
R0: complete resection 185 89.4
R1: microscopic residual 17 8.2
R2 : macroscopic residual 5 2.4
Total 207 100 * Percentages calculated at the net of unknown cases (N=98;32.1%)
63
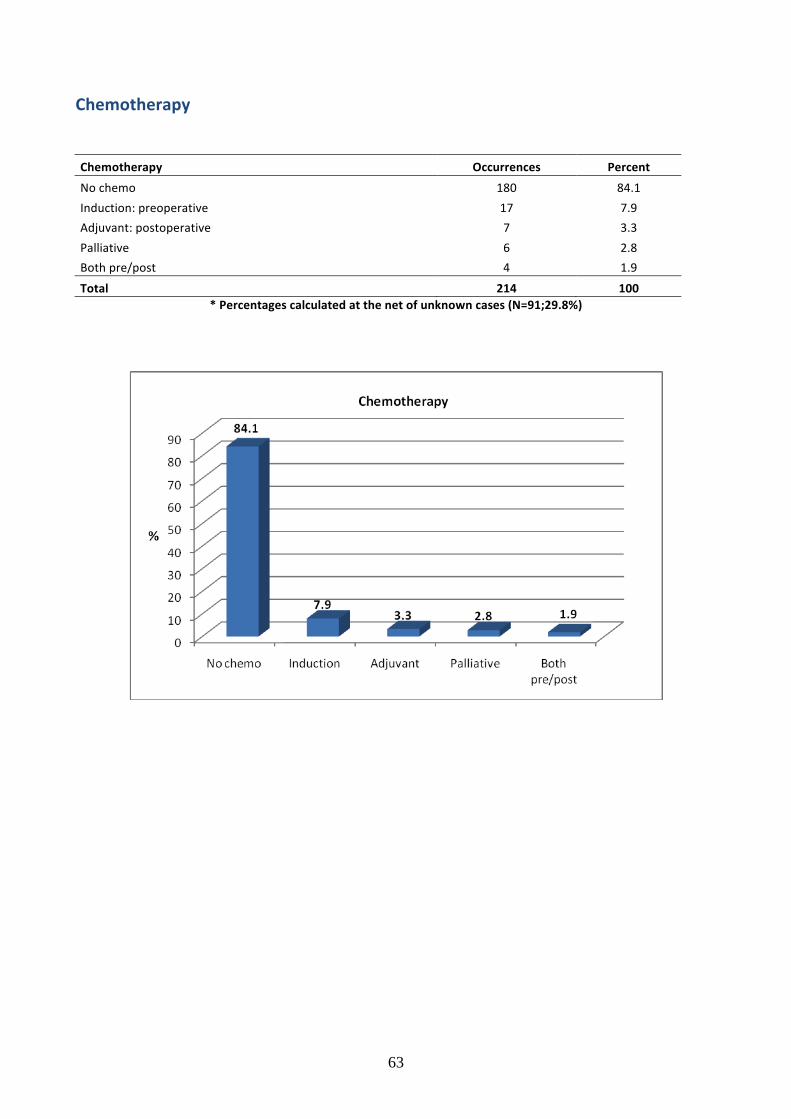
Chemotherapy
Chemotherapy Occurrences Percent
No chemo 180 84.1
Induction: preoperative 17 7.9
Adjuvant: postoperative 7 3.3
Palliative 6 2.8
Both pre/post 4 1.9
Total 214 100 * Percentages calculated at the net of unknown cases (N=91;29.8%)

64
Radiotherapy
Radiation therapy Occurrences Percent
No radiotherapy 155 73.1
Induction: preoperative 3 1.4
Adjuvant: postoperative 49 23.1
Palliative 2 0.9
Both pre/post 3 1.4
Total 212 100 * Percentages calculated at the net of unknown cases (N=93;30.5%)

65
Surgical approach
Surgical approach Occurrences Percent
Sternotomy 118 54.9
Thoracotomy 35 16.3
Hemi-‐clamshell 7 3.3
Clamshell 4 1.9
VATS 34 15.8
VATS-‐robotic 8 3.7
Transcervical 4 1.9
Transcervical+sternal split 3 1.4
Sternotomy+thoracotomy 2 0.9
Total 215 100 * Percentages calculated at the net of unknown cases (N=90; 29.5%)
66
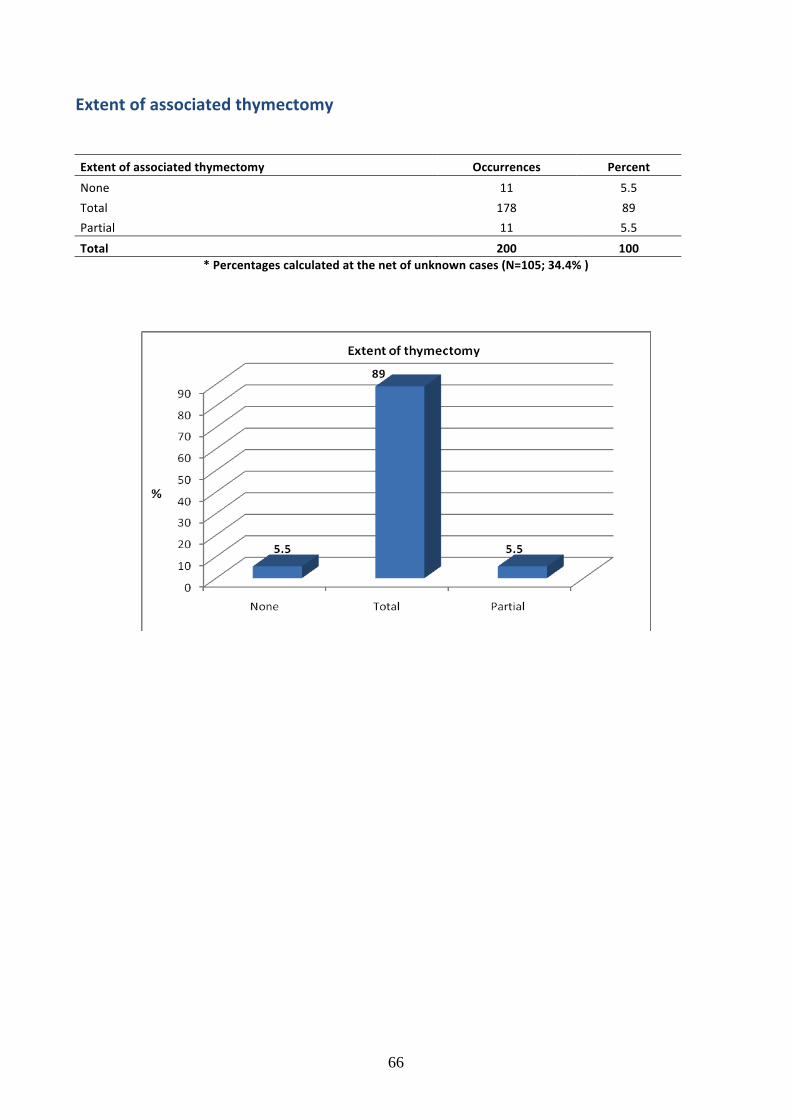
Extent of associated thymectomy
Extent of associated thymectomy Occurrences Percent
None 11 5.5
Total 178 89
Partial 11 5.5
Total 200 100 * Percentages calculated at the net of unknown cases (N=105; 34.4% )

67
Resected structures associated with thymic tumor resection
Resected structures Occurrences Percent
None 122 50.8
Pericardium 33 13.8
Pleura 30 12.5
Phrenic nerve 12 5.0
Lung wedge 27 11.3
Lung lobectomy 4 1.7
Innominate vein 7 2.9
SVC 2 0.8
Pleural implants 1 0.4
Diaphragm 1 0.4
Extrapleural pneumonectomy 1 0.4
Total 240 100 * Percentages calculated at the net of unknown cases (N=113; 37% )

68
Outcome at hospital discharge
Outcome at Discharge Occurrences Percent
Alive at Discharge 268 98.5
Died in Hospital 4 1.5
Total 272 100 * Percentages calculated at the net of unknown cases (N=33; 10.8%)
Outcome at 30 days 850 Outcome at 30 Days Occurrences Percent
Alive at 30 Days 212 98.6
Dead at 30 Days 3 1.4
Total 215 100 * Percentages calculated at the net of unknown cases (N=90;29.5%)

69
Data Completeness
Name of Field Unknown (%) Completeness(%)
Diagnosis of paraneoplastic -‐Autoimmune syndrome 44.3 55.7
Previous malignancy 43.6 56.4 Biopsy 44.3 55.7
Final pathologic diagnosis 26.2 73.8 WHO histology 47.2 52.8
Tumour size 29.8 70.2
Adjacent organ microscopic invasion 26.2 73.8 Clinical (pre-‐treatment) Masaoka-‐Koga Stage 34.8 65.2
Pathologic Masaoka-‐Koga Stage 36.1 63.9 Final pathologic resection status 32.1 67.9
Chemotherapy 29.8 70.2 Radiation therapy 30.5 69.5
Surgical approach 29.5 70.5
Extent of thymectomy 34.4 65.6 Resected structures 37 63
Outcome at Discharge 10.8 89.2 Outcome at 30 Days 29.5 70.5

70
PART 4
APPENDICES
(online version only)
71
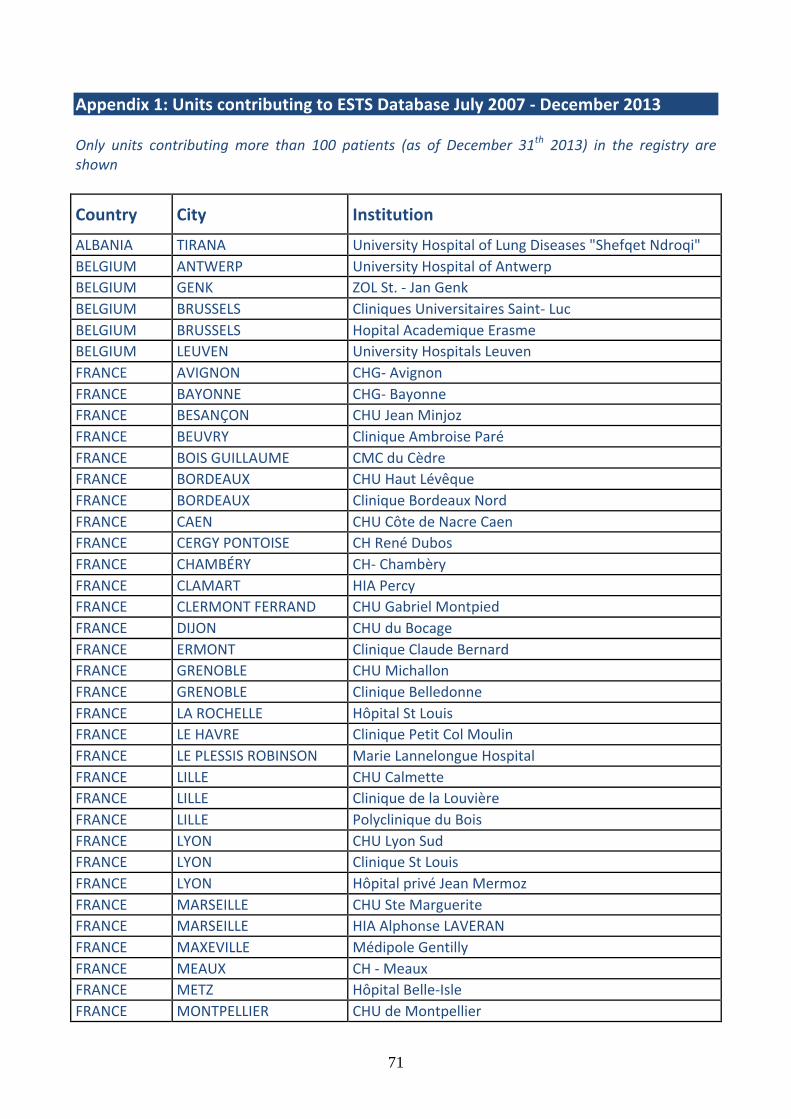
Appendix 1: Units contributing to ESTS Database July 2007 -‐ December 2013 Only units contributing more than 100 patients (as of December 31th 2013) in the registry are shown
Country City Institution
ALBANIA TIRANA University Hospital of Lung Diseases "Shefqet Ndroqi" BELGIUM ANTWERP University Hospital of Antwerp BELGIUM GENK ZOL St. -‐ Jan Genk BELGIUM BRUSSELS Cliniques Universitaires Saint-‐ Luc BELGIUM BRUSSELS Hopital Academique Erasme BELGIUM LEUVEN University Hospitals Leuven FRANCE AVIGNON CHG-‐ Avignon FRANCE BAYONNE CHG-‐ Bayonne FRANCE BESANÇON CHU Jean Minjoz FRANCE BEUVRY Clinique Ambroise Paré FRANCE BOIS GUILLAUME CMC du Cèdre FRANCE BORDEAUX CHU Haut Lévêque FRANCE BORDEAUX Clinique Bordeaux Nord FRANCE CAEN CHU Côte de Nacre Caen FRANCE CERGY PONTOISE CH René Dubos FRANCE CHAMBÉRY CH-‐ Chambèry FRANCE CLAMART HIA Percy FRANCE CLERMONT FERRAND CHU Gabriel Montpied FRANCE DIJON CHU du Bocage FRANCE ERMONT Clinique Claude Bernard FRANCE GRENOBLE CHU Michallon FRANCE GRENOBLE Clinique Belledonne FRANCE LA ROCHELLE Hôpital St Louis FRANCE LE HAVRE Clinique Petit Col Moulin FRANCE LE PLESSIS ROBINSON Marie Lannelongue Hospital FRANCE LILLE CHU Calmette FRANCE LILLE Clinique de la Louvière FRANCE LILLE Polyclinique du Bois FRANCE LYON CHU Lyon Sud FRANCE LYON Clinique St Louis FRANCE LYON Hôpital privé Jean Mermoz FRANCE MARSEILLE CHU Ste Marguerite FRANCE MARSEILLE HIA Alphonse LAVERAN FRANCE MAXEVILLE Médipole Gentilly FRANCE MEAUX CH -‐ Meaux FRANCE METZ Hôpital Belle-‐Isle FRANCE MONTPELLIER CHU de Montpellier

72
FRANCE MONTPELLIER Clinique du Millénaire FRANCE MORLAIX CMC de la Baie de Morlaix FRANCE NANCY CHU Central de FRANCE NANTES CHU -‐ Nantes FRANCE NANTES Clinique St Augustin FRANCE NANTES Nouvelle Clinique Nantaise FRANCE NICE CHU Pasteur FRANCE NICE Clinique Saint Georges FRANCE NIMES Clinique les Franciscaines FRANCE PARIS HEGP FRANCE PARIS Hôtel Dieu FRANCE PARIS IMM FRANCE PAU CHG -‐ Pau FRANCE POITIERS CHU -‐ Pointers FRANCE QUIMPER Clinique Quimper sud FRANCE REIMS Clinique Courlancy FRANCE ROUEN CHU Charles Nicolle FRANCE SAINT BRIEUC Hopital yves le Foll FRANCE SAINT CLOUD Clinique du Val D'or FRANCE SAINT ETIENNE CH Privé de la Loire FRANCE SAINT ETIENNE CHU – Saint Etienne FRANCE SAINT GRÉGOIRE CH Privé Saint Grégoire FRANCE STRASBOURG CHU -‐ Strasbourg FRANCE STRASBOURG Clinique St Odile FRANCE TALANT Clinique Bénigne Joly FRANCE TOULOUSE CHU Larrey FRANCE TOULOUSE Clinique Pasteur FRANCE TOURS CHU Trousseau FRANCE VALENCIENNES Clinique Teissier FRANCE VANNES Clinique Océane GERMANY BREMEN Klinikum Bremen-‐Ost -‐ Bremen GERMANY MONCHENGLADBACH Maria Hilf Kliniken GREECE ATHENS Evangelismos GREECE THESSALONIKI Ahepa University Hospital GREECE ATHENS Hygeia Hospital HUNGARY BUDAPEST National Institute of Oncology HUNGARY DEBRECEN University Of Debrecen HUNGARY SZEGED University of Szeged, Department of Surgery ITALY ANCONA Ospedali Riuniti Umberto I -‐ GM Lancisi – G Salesi di
Ancona ITALY BOLOGNA Discipline Chirurgiche, Rianimatorie e dei Trapianti Univ.
di Bologna ITALY FOGGIA Azienda Ospedaliero Universitaria Foggia – Dip.
Chirurgia Toracica

73
ITALY TORINO Azienda Ospedaliero Universitaria Molinette San Giovanni Battista
ITALY LECCE V. Fazzi Hospital ITALY MILANO Azienda Ospedaliero San Paolo ITALY MILANO Fondazione Ospedale Maggiore Policlinico ITALY GENOVA San Martino -‐ Genoa ITALY PARMA University Hospital Parma ITALY SIENA University Hospital Siena NETHERLANDS AMSTERDAM VUMC Dept of Surgery NETHERLANDS BREDA Amphia Hospital NETHERLANDS HAARLEM Kennemer Gasthuis PORTUGAL LISBON Santa Martha Hospital, Lisbon ROMANIA BUCHAREST Institute of Oncology Bucharerst ROMANIA BUCHAREST Marius Nasta Institute of Pneumonology ROMANIA DROBETA-‐TURNU
SEVERIN County Emergency Hospital
ROMANIA TIMISOARA Clinical Muncipal Emergency Hospital SLOVAKIA BRATISLAVA University Hospital Bratislava , Slovacchia SLOVENIA LJUBLJANA University Medical Centre Ljubljana SPAIN BARCELONA Hospital Clinic SPAIN BARCELONA Sagrat Cor University Hospital SPAIN HEBRON HG Vall d'Hebron SPAIN MADRID H. Clinico San Carlos SPAIN MADRID Hospital general Universitario Gregorio Maranon SPAIN NAVARRA Clinica Universitaria De Navarra SPAIN SALAMANCA University Hospital Salamanca SPAIN SEVILLA HHUU Virgen del Rocio SPAIN VALENCIA General University Hospital Valencia TURKEY BURSA Uludag University, School of Medicine TURKEY ISTANBUL Istanbul School of Medicine TURKEY ISTANBUL Istanbul University, Cerrahpasa Medical Faculty TURKEY ISTANBUL Sureyyapasa Chest Disease & Thoracic Surgery Hospital UK EXETER Royal Devon & Exeter NHS Foundation Trust

74
Appendix 2: Database format and submission of data The first step is to request and obtain a login account through the relevant link found in the ESTS homepage (http//www.ests.org) or by directly sending an email to one of the members of the Database Committee. Once you have a valid login account you can proceed through the following data entry interface (accessible through https://ests.dendrite.it/csp/ests/intellect/login.csp). The intellect Web logon screen shown below has been engineered to provide enhanced security facilities:
• Limiting users to 3 logon attempts before locking the user-‐account • Giving information on previously successful and unsuccessful logon attempts • Requiring users to have an eight-‐character password that contains at least one uppercase
character, one lowercase character and one digit.
Once you have logged in you are presented with the Database main menu, from which you can add new data, view or edit a procedure, modify your account details, and export your data in Excel for your own purposes.
Clicking on the Enter Clinical Data button opens the next screen “Patient Search”, where it is possible to search for patients already in the database or add new patients.

75
Clicking on the link Add New Patient, that can be found at the left of the screen in the section Options, you will be required to fill in the minimum data required to register a New Patient.
The newly created patient is ready to be entered into the database.
Now it is possible to select the available Database (1) (in our case there is only the one named ESTSR) and add the patient to the chosen Database by clicking on the button (2). Once you have clicked the Add Button, the first page of the selected Registry will appear. Now you can start inserting clinical data as showed in next page.

76
The Database is an all-‐purpose database designed for all general thoracic surgery procedures, but specifically focused on lung resections for which a number of additional items can be selected, including risk-‐scores, cardiopulmonary function data and calculation of predicted postoperative pulmonary function through a standardized calculator.
In addition to risk factors, diagnosis and staging details can be added in a following section.

77
The system auto-‐calculates for Lung Excision Procedure the Predicted Mortality(%) and Predicted Morbidity (%) Early outcomes, including in-‐hospital morbidity, in-‐hospital and 30-‐days mortality should be specified in the final section, before submitting the data.
78
Appendix 3: Definition of major cardiopulmonary complications listed in the database ARDS: Adult respiratory distress syndrome defined according to the American-‐European consensus conference. All of the following criteria should be met:
1. Acute onset 2. Arterial hypoxemia with PaO2/FIO2 ratio lower than 200 (regardless PEEP level) 3. Bilateral infiltrates at chest radiograph or CT scan 4. No clinical evidence of left atrial hypertension or pulmonary artery occlusive pressure < 18
mmHg 5. Compatible risk factors
Atrial Arrhythmia: new onset of atrial fibrillation/flutter (AF) requiring medical treatment or cardioversion. Does not include recurrence of AF which had been present preoperatively. Ventricular Arrhythmia: sustained ventricular tachycardia or ventricular fibrillation that has been clinically documented and treated by ablation therapy, implantable cardioverter defibrillator, permanent pacemaker, pharmacologic treatment or cardioversion. Bronchoscopy for atelectasis: postoperative atelectasis documented clinically or radiographically that needed bronchoscopy. Pneumonia: defined according to the last CDC criteria. Two or more serial chest radiographs with at least one of the following:
• New or progressive and persistent infiltrate • Consolidation • Cavitation
And at least one of the following: • Fever (>38°C or >100.4°F) with no other recognized cause • Leukopenia (<4000 WBC/mm3) or leukocytosis (>12,000 WBC/mm3) • For adults >70 years old, altered mental status with no other recognized cause
and at least two of the following: • New onset of purulent sputum, or change in character of sputum, or increased respiratory
secretions, or increased suctioning requirements • New onset or worsening cough, or dyspnea, or tachypnea • Rales or bronchial breath sounds
Worsening gas exchange (e.g. O2 desaturations (e.g., PaO2/FiO2 < 240), increased oxygen requirements, or increased ventilator demand). Pulmonary embolism: confirmed by V/Q scan, angiogram or CT scan.

79
DVT: deep venous thrombosis confirmed by Doppler study, contrast study or other study and that required treatment. Myocardial infarct: evidenced by one of the following criteria:
1. transmural infarction diagnosed by the appearance of a new Q wave in two or more contiguous leads on ECG.
2. Subendocardial infarction (non Q wave) evidenced by clinical, angiographic electrocardiographic signs.
3. Laboratory isoenzyme evidence of myocardial necrosis. Renal failure: defined as the onset of new renal failure in the postoperative period according to one of the following criteria:
1. increase of serum creatinine to greater than 2.0, and 2-‐fold the preoperative creatinine level.
2. a new requirement for dialysis postoperatively. Neurological complication: occurrence of one of the following central neurologic postoperative events not present preoperatively:
1. a central neurologic deficit persisting postoperatively for more than 72 hours 2. a transient neurologic deficit (transient ischemic attack or reversible ischemic neurological
deficit) with recovery within 72 hours 3. a new postoperative coma persisting at least 24 hours and caused by anoxic/ischemic
and/or metabolic encephalopathy, thromboembolic event or cerebral bleed.

80
Appendix 4: ESTS institutional accreditation program The ESTS Council has approved an Institutional Accreditation program open to all thoracic surgery units participating to the ESTS Database. The aim of the program is to set standards of good clinical practice across Europe with the intent to improve the quality of care possibly according to published guidelines. To be certified units must participate to the ESTS Database since at least 2 years and have contributed a sufficient number of patients. This pre-‐requisite is necessary to calculate a reliable Composite Performance Score, which is the metrics used to evaluate the Institutional performance. A recent document from the STS Quality Measurement task force elegantly explained the conceptual framework and the statistical consideration in the development of Composite Performance Scores in Cardiac Surgery. Based on a similar methodology, ESTS has recently developed and published a Composite Performance Score (CPS) for lung surgery (Brunelli A et al. The European Thoracic Database project: Composite Performance Score to measure quality of care major lung resection. Eur J Cardiothorac Surg 2009; 35: 769-‐774). The method consists in developing standardized outcome and process indicators covering all temporal domains of the lung resection care. The indicators were selected based on their evidence-‐based level. For the preoperative domain, we selected the proportion of patients with DLCO measured before major lung resection, and the proportion of patients with clinically suspicious N2 nodes at CT scan or PET scan submitted to some type of preoperative mediastinal invasive staging. For the intraoperative domain, we selected the proportion of patients with primary neoplastic disease submitted to major anatomic resections and at least lobe-‐specific nodal dissection. For the postoperative domain, we selected the risk-‐adjusted in-‐hospital cardiopulmonary and mortality rates. Each of these indicators has been rescaled according to their standard deviation in the entire population to obtain individual standardized indicators. These were then summed to obtain the composite score for each unit. To derive the regression models for morbidity and mortality, univariate screening of the following variables: age, gender, BMI, type of resection, ppoFEV1, induction therapy, extended resection, presence of cardiac co-‐morbidity. Variables with p-‐level<0.1 were used as independent predictors in backward logistic regression analysis validated by bootstrap resampling technique. Only significant (p<0.05) and reliable (bootstrap significancy frequency >50%) were retained in the final model. Updated logistic regression equation for mortality (c-‐index 0.74; Hosmer Lemeshow statistics, p=0.9)) Logit: -‐3.22 + 1.049Xpneumonectomy (coded as 1 vs. 0 lobectomy) + 0.928Xcardiac comorbidity (coded as 1 and including CAD, any previous cardiac surgery, history and treatment for arrhythmia, congestive heart failure, hypertension) -‐0.0175XppoFEV1%
81
Updated logistic regression equation for cardiopulmonary morbidity (c-‐index 0.66; Hosmer-‐Lemeshow statistics, p=0.4) Logit: -‐3.52 + 0.659Xpneumonectomy + 0.403Xextended resection (coded as 1 and including chest wall resection, pleuropneumonectomy, completion operation, intrapericardial operation) + 0.322Xcardiac comorbidity -‐0.0065XppoFEV1% + 0.0315Xage. Standardized scores are calculated by subtracting the observed risk-‐adjusted outcome or process incidence minus the average observed outcome or process incidence. The difference is then divided by the standard deviation of the observed outcome or process in the entire population. The 50th percentile of the CPS is the threshold selected by the Database Committee as a minimum criteria for accreditation and will be updated yearly. In the future, an automatic function will be implemented in the ESTS Database, which will allow the end-‐users to calculate their own CPS. In addition to their CPS, units must have certain structural, procedural and professional characteristics to be certified. These characteristics needs to be assessed and audited along a sample of data submitted to the database. To this purpose, ESTS has subcontracted an external auditing Company, which together with a thoracic surgeon will visit the applicant units and produce a report, which will be evaluated by the Database Committee. If the report will be judged satisfactory, the Accreditation will be granted by the ESTS Council. The following are the required structural/procedural/professional characteristics (based and modified from Brunelli A et al. European guidelines on structure and qualification of general thoracic surgery. Eur J Cardiothorac Surg (2014) doi: 10.1093/ejcts/ezu016). Hospital & Departmental structural criteria:
• Dedicated staff and institutional resources. • 1 fully equipped operating room per 300-‐400 major thoracic procedures per year. • Access to ICU with experience in thoracic surgical cases. • Dedicated GTS ward, with full supporting paramedical staff and specialized chest
physiotherapists. • The size of the unit should reflect the procedural volume and postoperative management
policy. • Access to outpatient facilities and radiology. • GTS must have easy access to support facilities that must include: hematological,
microbiological and biochemical labs, respiratory pathophysiology lab, endoscopic examinations (bronchoscopy, esophagoscopy), cardiologic examination, cardiopulmonary exercise test, radiology including C scan and PET, cytology, histopathology and frozen section analysis.
• In-‐house facilities for research and education (meeting room, medical libraries, email and internet)
Procedures Volume: A suggested minimum volume of 150 +/-‐ 50 major thoracic procedures per year is recommended. For esophageal resections a minimum volume of 20 +/-‐ 5 procedures per year is recommended. For lung transplant a minimum volume of 10 procedures per year is recommended.

82
Qualification of surgeons: All surgeons must be qualified to perform thoracic surgery according to individual national or European legislation. The Head of the unit must have a minimum experience of 5 years of clinical practice as qualified thoracic surgeon. Costs: The costs for the inspection and auditing (7,000 Euros) are the individual Unit’s responsibility. The accreditation will be valid for a 36 months period. After this period the unit must apply for revalidation. ESTS accreditation will provide a number of benefits to certified institutions:
1. Accredited units will be announced during the ESTS Annual meeting and their names listed in the ESTS home page and ESTS Annual Report.
2. Participation to ESTS quality improvement initiatives 3. Participation to high-‐profile scientific projects supported by the ESTS scientific committee 4. Accredited units may propose their own clinical research projects based on data present in
the ESTS database. The research projects will be then reviewed by the database committee and, if accepted, the unit will be granted full access to the data in the ESTS database needed for analysis.

83
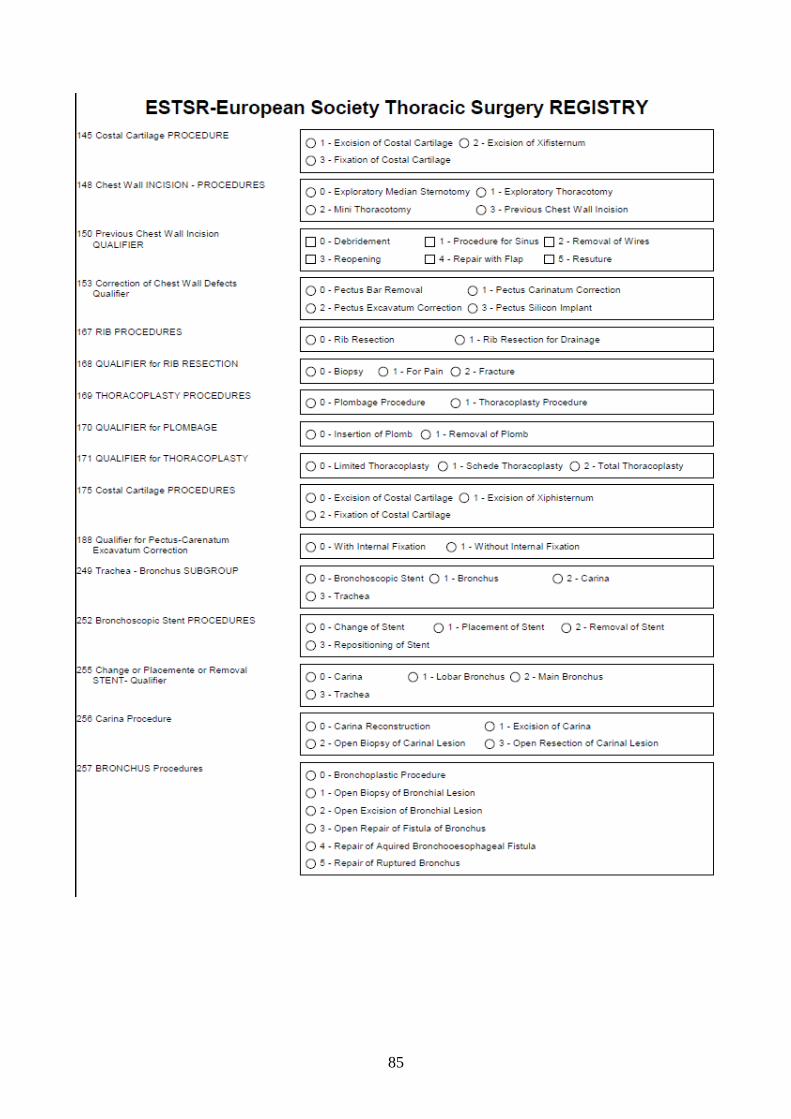
Appendix 5: ESTS dataset (global, follow-‐up and thymoma)

84
85

86

87

88

89

90

91

92

93

94

95

96

97

















