14
Rebecca Sposato MS, RN
| Date post: | 16-Dec-2015 |
| Category: |
Documents |
| Upload: | ruby-crooker |
| View: | 219 times |
| Download: | 6 times |

Rebecca Sposato MS, RN

Normal SleepAdults need 6-8 hours of sleep to maintain
healthy physiology and optimal mental abilitiesChildren and infants need more
The brain uses sleep to:Reduce physiological demands on the bodyProcess emotions and memoriesLearning: long term potentiation of neuronsNeuro “housekeeping and repair”
Zeitgebers – cues and sensory input from the environment that influence circadian rhythmHuman circadian rhythm is actually 25hr long

Neurology of SleepNeuro-chemicals contributing to sleep: serotonin,
melatonin, anandamine
Suprachiasmatic Nerve: regulates circadian rhythm
Basal forebrain: active during deep slow wave sleepBrain temp decreases by 1-2 degrees
Atonia: the acetylcholine neurons in the medulla inhibit activity in the spinal cord during REM, so people do not act out their dreams
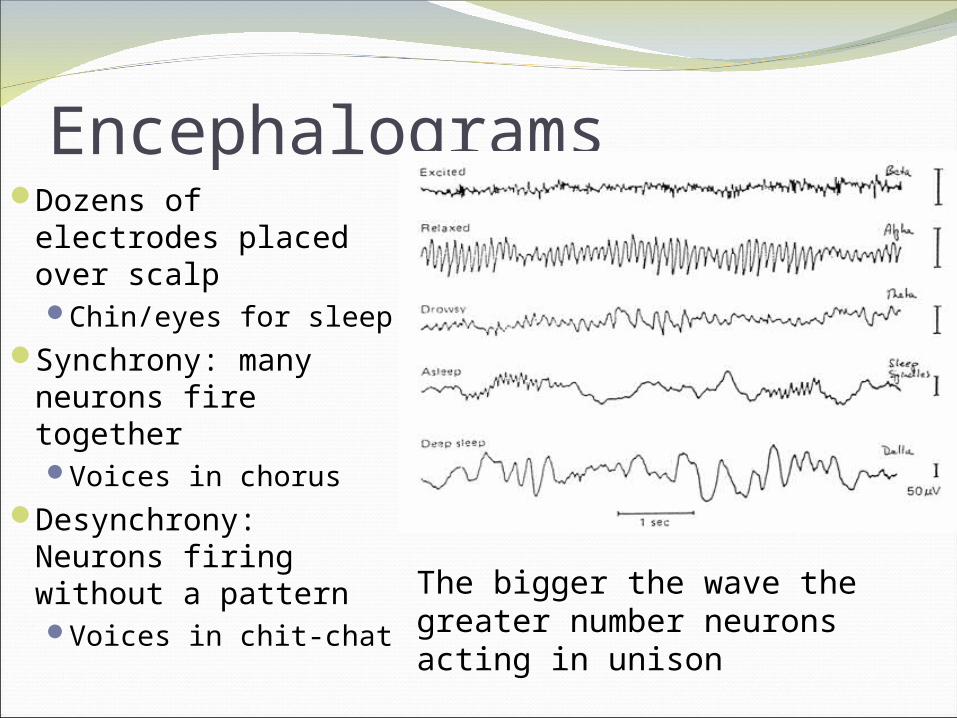
EncephalogramsDozens of electrodes
placed over scalpChin/eyes for sleep
Synchrony: many neurons fire togetherVoices in chorus
Desynchrony: Neurons firing without a patternVoices in chit-chat The bigger the wave the
greater number neurons acting in unison

EncephalogramsBeta: alert, active thinking
Alpha: alert, relaxed
Theta: Drowsy, K complex and sleep spindles felt as sleepiness
Stage 3: deeper sleep
Stage 4: deepest sleep, large broad waves, person feels refreshed afterwards
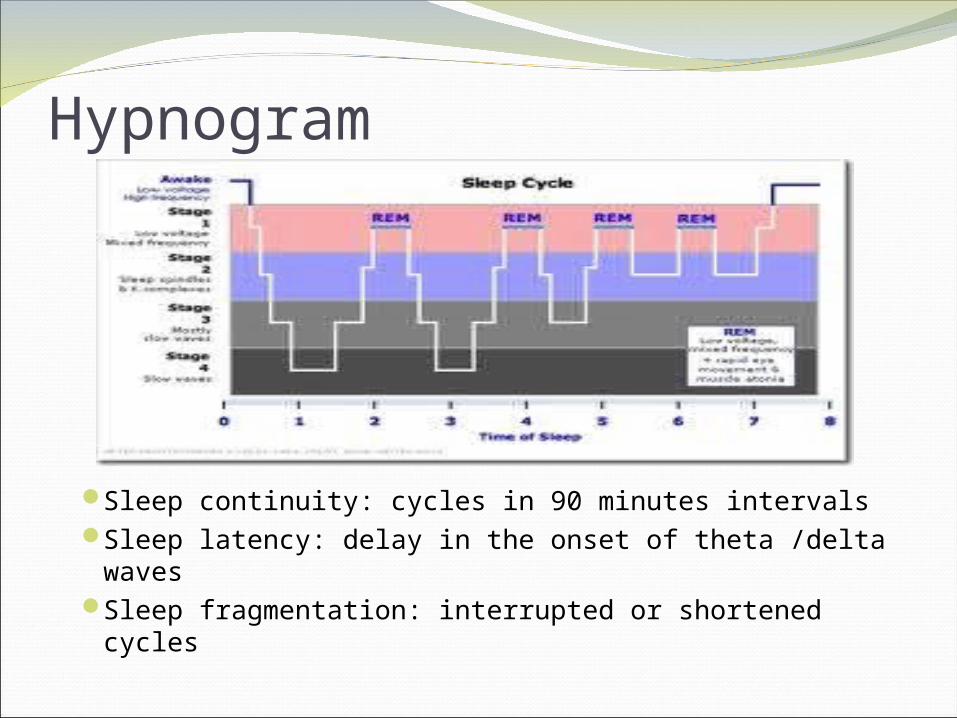
Hypnogram
Sleep continuity: cycles in 90 minutes intervals Sleep latency: delay in the onset of theta /delta wavesSleep fragmentation: interrupted or shortened cycles

Dyssomnias>35% of the population report impaired sleepingPrimary Hypersomnia: prolonged sleep,
accompanied by feelings of sleepiness during dayPrimary Insomnia: difficulty in initiating,
maintaining sleep or sleep experienced as non-restorative sustained over 1 monthEEG shows more alpha/beta and less theta/delta
Restless Leg Syndrome: Sensation of irritation precedes spastic movement of legs in early sleepWorst when stressed or pregnantMedicate with dopamine agonists

DyssomniasNarcolepsy: irresistible brief episodes of sleep
during waking routineOccur during periods of low stimulation, low
activity2-6 episodes per day, last about 20 minutes,
refreshingMust occur daily >3months
Cataplexy: loss of voluntary muscle tone, often triggered by emotional outburst (cry, laugh)Last seconds to minutes, retains consciousness70% of narcoleptics develop this feature
Hypnagogic hallucinations: dreamlike visions while awake

ParasomniaAbnormal sleep behaviors or physiological
events in association with specific stages of sleepNightmare (REM): vivid dreams with threatening
themes, often abruptly awaken personNight Terrors (deep stage): anxiety and
physiological arousal, results in abrupt awakening, person often lacks recall of dream or awakening
Sleepwalking (deep stage): complex motor behavior occurring out of bed, no recall of the event

Breathing related sleep disordersObstructive Sleep Apnea: brief episodes (20-30 sec)
of apnea or hypopnea related to obstructed airwaySnore-silence-gasp breathing pattern Occurs when flesh of the throat sags into the airwayContinuous positive airway pressure (CPAP) mask
Central Sleep Apnea: brief episodes of apnea or hypopnea not associated with chest or airway abnormalitiesMost often in elderly with cardio and neuro conditions
that affect ventilatory regulationAlveolar Hypoventilation Syndrome: low o2 levels
from impaired ventilatory control, no apnea

Circadian Rhythm Sleep DisorderPersistent or recurrent disruption in sleep
pattern from altered circadian rhythm or mismatch in sleep-wake cycle and external demands on timing and duration of sleepDelayed onsetJet-lagShift Work

Sleep and HealthInsomnia is physiologically taxing on the
mind/bodyMetabolic syndromeSuboptimal physical performanceImpaired memory and concentrationirritability

Sleep and Mental HealthLack of sleep can accentuate any mental
illnessPsychosis, delirium, anxiety
Many mental illnesses contribute to insomniaMania, depression, anxiety, schizophrenia etc. Depression can also contribute to
hypersomnolence
Substance use cause temporary insomnia, followed by rebound hypersomnolence

InterventionsSleep logPolysomnography – diagnostic sleep lab
study, includes:Video recordingHeart rate/oxygen monitor/resp. rate/depthEEG
Sleep hygiene –modify routine to promote sleep
Pharmacological – sedatives or hypnotic medications Benzodiazepines, Ambien, Lunesta etc.

















