40
RECENT ADVANCES IN PANCREATIC CANCER Dr.E.Kaushik Kumar Department of General Surgery Stanley Medical College Hospital,Chennai
| Date post: | 27-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | kaushik-kumar-eswaran |
| View: | 67 times |
| Download: | 2 times |

RECENT ADVANCES IN PANCREATIC CANCER
Dr.E.Kaushik Kumar Department of General Surgery
Stanley Medical College Hospital,Chennai

• Molecular Genetics and Tumour Biology• Early Detection of Precursor Lesions• Investigation Modalities• Surgical Management• Adjuvant modalities

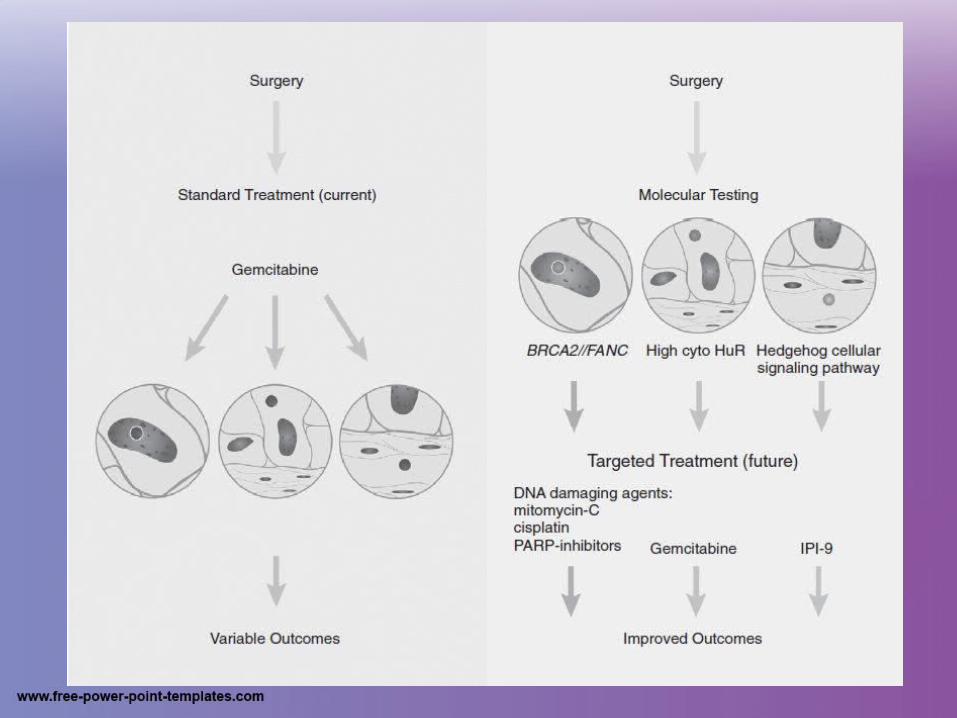
Molecular Genetics and Tumour Biology• Two eras
• Early Detection of Precursor Lesions– PanIN– IPMN– Mucinous Cystic Neoplasm

Investigation Modalities
• TAUS• EUS• IOUS• MD-CT• MRCP• Nuclear Imaging• Tumour Markers

ULTRASOUND
• Screening• 95.8% sensitive >3cm lesions• Newer machines- Tissue Harmonic Imaging• Colour Doppler • IV Contrast imaging-100% specific for vascular
involvement• PPV for unresectabilty-94%
EUS• <3cm tumours,ampullary lesions• Staging and resectability• Reassessment after NAC• EUS-FNA- 95% sensitivity,97% specificity,PPV
92%, 100% NPV• Therapeutic options
– Intra-tumoral therapy(activated lymphocytic cultures,viral vectors,oncolytic viruses)
– RFA/Cryotherapy– Celiac plexus neurolysis

Homogenous echoes
Hypoechoic,irregular borders
Cyst- anecohic
Endocrine tumours-iso-echoic
Improper vascular involvement, invasive,costly,operator dependent

Intra-operative US
• Depth of invasion
• Maximal longitudinal extent
• Vascular invasion
• Degree of resectability(20-35% will be unresectable)
• Liver mets
• Localise islet cell tumours


MDCT• Ill-defined, hypoattenuating focal mass with dilatation of
the upstream pancreatic and or biliary duct• Arterial,Pancreatic and portal phases• Very high spatial and temporal resolution• Pancreatic Protocol-1 to 3 mm slice collimation• challenging in the setting of
– pancreatitis forming mass effects– in the presence of loco-regional lymph node
involvement – small hepatic metastasis

• Vascular involvement include– Tumor involvement for one half of the vessel′s
circumference– Focal narrowing of the vessels – Dilatation of peripancreatic veins.
• Perfusion imaging– Angiogenesis in tumours– Predict response to CCRT

MRI-MRCP
• High soft tissue contrast resolution– Assessment of peripancreatic fat infiltration– Evaluation of vascular encasement– Peritoneal deposits and lymph nodal involvement
• MRS-differentiate CFP from pancreatic cancer– proton MRS, CP shows less lipid than pancreatic
carcinoma due to difference in fibrous tissue content in the two conditions

• Diffusion-weighted MRI differentiates the subtypes of pancreatic endocrine neoplasms – Tumor cellularity – Extracellular fibrosis – Various apparent diffusion coefficient (ADC)
values in these tumors
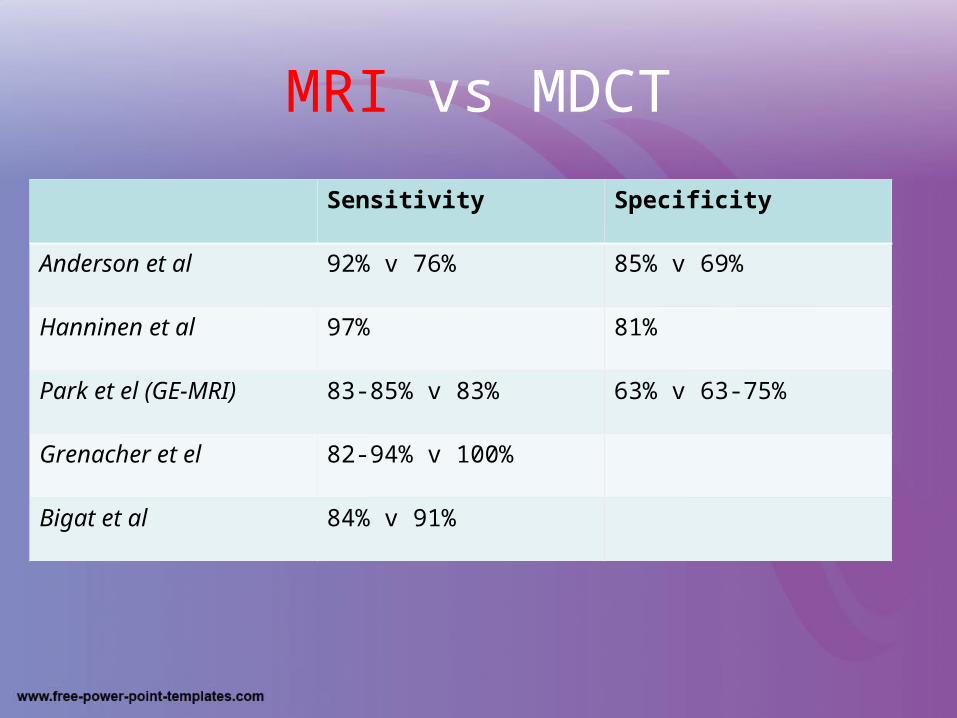
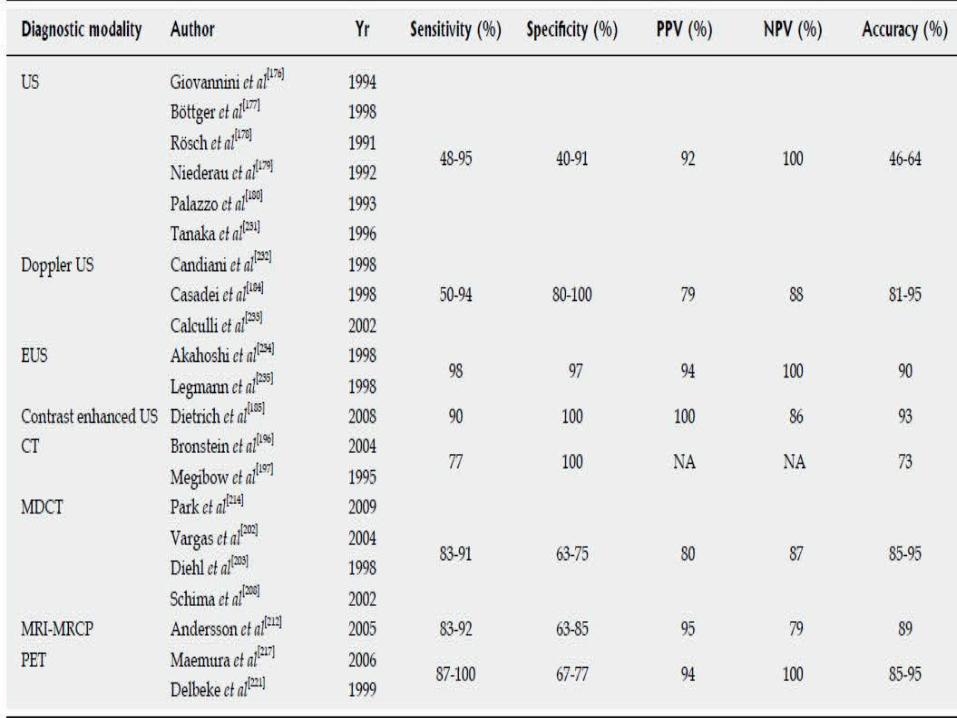
MRI vs MDCT
Sensitivity Specificity
Anderson et al 92% v 76% 85% v 69%
Hanninen et al 97% 81%
Park et el (GE-MRI) 83-85% v 83% 63% v 63-75%
Grenacher et el 82-94% v 100%
Bigat et al 84% v 91%

Nuclear Imaging
• Newly developed PET scanners can detect small PCs up to 7 mm in diameter
• Unsuspected Bone metastasis(40%)
• Inflammatory pathology
• Tumour viability
• Response to treatment
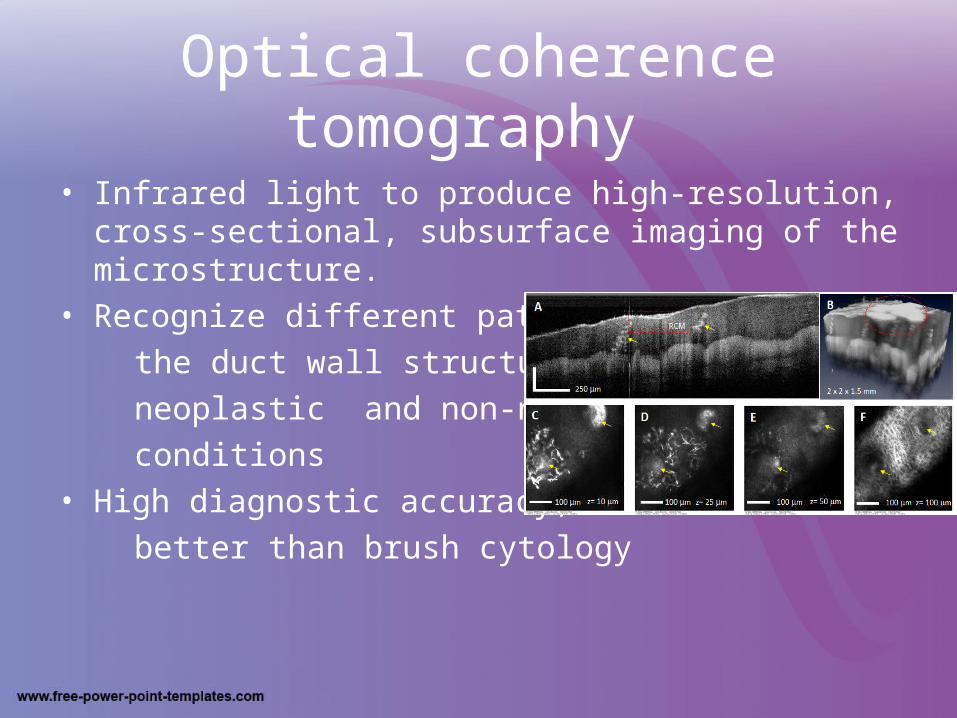
Optical coherence tomography
• Infrared light to produce high-resolution, cross-sectional, subsurface imaging of the microstructure.
• Recognize different patterns of
the duct wall structure in
neoplastic and non-neoplastic
conditions• High diagnostic accuracy,
better than brush cytology

Tumour MarkersMarker Sensitivity Specificity
CEA 45% 75%
CA 19-9 80% 43%
CA 242 60% 76%
CEA + CA 19-9 37% 84%
CEA + CA 242 34% 92%

• CA494• CEACAM1• PTHrP• TuM2-PK• CAM 17.1• Serum beta HCG

Surgical Management
• Resectability criteria– Resectable– Borderline Resectable– Unresectable

• Laparoscopy– Staging– Therapeutic– Safe and Better outcome

• Robotic Surgery– 3-Dimensional– Dexterity– Ergonomics

Adjuvant modalities
• FOLFIRINOX(5-fluorouracil, leucovorin, irinotecan, oxaliplatin)
– ACCORD trial -median overall (11.1 mo vs 6.8 mo)– Grade 3-4 toxicities
• Gemcitabine + nab-Paclitaxel (MPACT)– Improved median overall survival (8.5mo vs 6.7 mo) – Improved 1-year survival (35% vs 22%)– Improved 2-year survival (9% vs 4%)– Improved objective response rate
• Gemcitabine plus erlotinib– improved progression-free survival and
overall survival
– hNET1 expression Gemcitabine response


S-1
• An oral 5-fluorouracil (5-FU) prodrug– Tegafur (a prodrug of 5-FU)– Gimeracil [a potent dihydropyrimidine dehydrogenase
(DPD) inhibitor]– Oteracil(an inhibitor of phosphorylation of 5-FU in GIT)
• First-line Chemotherapy for Metastatic/Locally Advanced Pancreatic Cancer
• Second-line Therapy After Gemcitabine Failure• CRT For Locally Advanced Pancreatic Cancer• Adjuvant Chemotherapy For Resected Pancreatic Cancer• Improved ORR

• Neo-Adjuvant ChemoRadiotherapy– Chemotherapy provides control for a micro-
disseminated disease & also acts as a radiation sensitizer
– Radiotherapy(RT) may have a huge impact on the local control of the disease.


• Upfront chemotherapy followed by CRT– Early therapeutic approach may use not only
RT-sensitizing drugs and drugs that are more
effective against cancer such as 5-FU and Gemcitabine or Capecitabine
– Select patient who did not progress, thus avoiding the additional toxicity of unnecessary Radiotherapy (RT)
• End point – Resectability as per NCCN


• IORT– When followed after pre-operative
chemotherapy and surgery gives a 5-yr local control of 23.3%


Multidisciplinary

• Mortality and morbidity directly proportional to Institutional Volume of cases
• “A persistent nihilism of clinicians towards PC and pancreatectomy may be the most significant correctable factor that contributes to the current poor long-term outcomes of PC.”
• Birkmeyer et al,Bilimoria et al

• What have we understood?
• What has improved?
• Where do we stand?
• What needs to be done?


References• Blumgart textbook of HPB Diseases,5th edition• World Journal of Gastroenterology(2001-2014)
– Pancreatic cancer: Advances in treatment
– Recent advances in the surgical treatment of pancreatic cancer
– Selection criteria in resectable pancreatic cancer: A biological and morphological approach
– Imaging diagnosis of pancreatic cancer: A state-of-the-art review
– Diagnostic Imaging for Pancreatic Cancer Computed Tomography, Magnetic Resonance Imaging, and Positron Emission Tomography
– Advances in diagnosis, treatment and palliation of pancreatic carcinoma: 1990-2010
– S-1 in the treatment of pancreatic cancer Kentaro Sudo, Kazuyoshi Nakamura, Taketo Yamaguchi
– Recent standardization of treatment strategy for pancreatic neuroendocrine tumors Masayuki Imamura
– Neoadjuvant strategies for pancreatic cancer

Thank You

















