50
By. Dr. Sumit Kamble Dept. of Neurology GMC, Kota
| Date post: | 15-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | neurologykota |
| View: | 424 times |
| Download: | 0 times |
By.
Dr. Sumit Kamble
Dept. of Neurology
GMC, Kota

INTRODUCTION
Parkinson’s disease (PD) is the second most
common neurodegenerative disease, affecting 1%
of the population over 55 years of age.
Disease is characterized by the loss of ~50–70% of
the dopaminergic neurons in the substantia nigra, a
profound loss of dopamine (DA) in the striatum, and
the presence of intracytoplasmic inclusions called
Lewy bodies (LB).
2

PREVALENCE OF PARKINSONISM IN
INDIA
Very few studies are available on the prevalence of
PD in India.
Different studies have shown that the crude
prevalence rate (CPR) of PD is 14 per 100,000 in
the north India, 27 per 100,000 in south India and
16 per 100,000 in east India. However, in one study
of Parsis in Mumbai revealed a CPR of 328 per
100,000.
3

CLINICAL FEATURES
Four cardinal symptoms:
resting tremor
bradykinesia
muscle rigidity
postural insatability
4

UK PDS BRAIN BANK CRITERIA FOR THE
DIAGNOSIS OF PARKINSON'S DISEASE
Step 1. Diagnosis of a parkinsonian syndrome
Bradykinesia and at least one of the following:
• muscular rigidity
• rest tremor (4–6 Hz)
• postural instability unrelated to primary visual,
cerebellar, vestibular or proprioceptive dysfunction.
5
Step 2. Exclusion criteria for Parkinson's disease
(PD)
History of :
• repeated strokes with stepwise progression
• repeated head injury
• antipsychotic or dopamine-depleting drugs
• definite encephalitis and/or oculogyric crises on no
drug treatment
• more than one affected relative
• sustained remission
6
Step 3. Supportive criteria for PD
Three or more required for diagnosis of definite PD :
unilateral onset
excellent response to levodopa
rest tremor present
severe levodopa-induced chorea
progressive disorder
levodopa response for over 5 years
persistent asymmetry affecting the side of onset most
clinical course of over 10 years.7

HOEHN AND YAHR STAGING
Stage I: Unilateral involvement only usually with
minimal or no functional disability
Stage II:Bilateral or midline involvement without
impairment of balance
Stage III: Bilateral disease; mild to moderate
disability with impaired postural reflexes; physically
independent
Stage IV: Severely disabling disease; still able to
walk or stand unassisted
Stage V: Confinement to bed or wheelchair unless
aided 8
9
Section 1. Communication
Section 2. Diagnosis and Progression
Section 3. Treatment
A. Pharmacological therapy for motor symptoms in
early PD
B. Pharmacological therapy for motor symptoms in later
PD
C. Surgery
D. Other Treatment Options
Section 4. Non-motor Features and Their Treatment
A. Mental Health
B. Sleep disorders
C. Autonomic dysfunction
Guidelines on Parkinson’s Disease –
overview

10
AAN - American Academy of Neurology
NICE - National Institute for Health and Clinical
Excellence
EFNS - European Federation of Neurological Societies
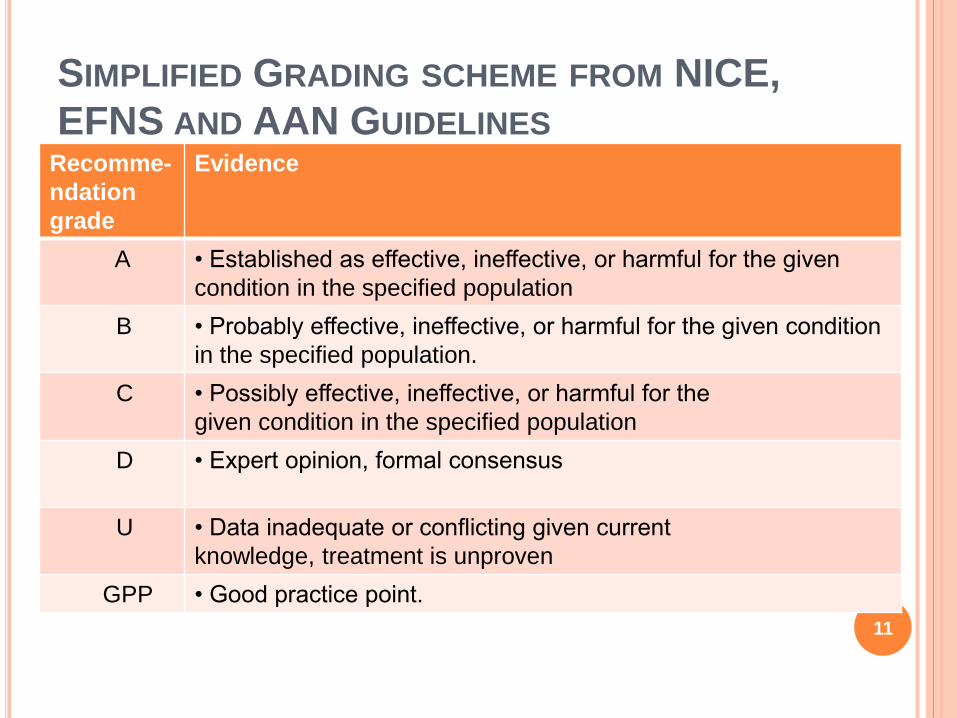
SIMPLIFIED GRADING SCHEME FROM NICE,
EFNS AND AAN GUIDELINESRecomme-
ndation
grade
Evidence
A • Established as effective, ineffective, or harmful for the given
condition in the specified population
B • Probably effective, ineffective, or harmful for the given condition
in the specified population.
C • Possibly effective, ineffective, or harmful for the
given condition in the specified population
D • Expert opinion, formal consensus
U • Data inadequate or conflicting given current
knowledge, treatment is unproven
GPP • Good practice point.
11

COMMUNICATION
Because people with PD may develop impaired
cognitive ability, a communication deficit and/or
depression, they should be provided with: both oral
and written communication throughout the course
of the disease, which should be individually tailored
and reinforced as necessary; and consistent
communication from the professionals involved.
NICE Level D (GPP)
12

DIAGNOSIS AND PROGRESSION
Parkinson’s disease should be suspected in people
presenting with tremor, stiffness, slowness, balance
problems and/or gait disorders. NICE Level D
(GPP)
Determining the presence of the following clinical
features in early stages of disease should be
considered to distinguish PD from other
parkinsonian syndromes:
1) falls at presentation and early in the disease
course;
2) poor response to levodopa;
3) symmetry at onset; 13
4) rapid progression (to Hoehn and Yahr stage 3 in
three years);
5) lack of tremor; and
6) dysautonomia (urinary urgency/ incontinence
and fecal incontinence, urinary retention requiring
catheterization, persistent erectile failure or
symptomatic orthostatic hypotension). AAN Level B
D (GPP)
14

In patients with newly diagnosed PD, older age at
onset and rigidity/hypokinesia as an initial symptom
should be used to predict more rapid rate of motor
progression. AAN Level B
The presence of associated comorbidities (stroke,
auditory deficits, and visual impairments), Postural
Instability/Gait difficulty (PIGD), and male sex may
be used to predict faster rate of motor progression.
AAN Level C
15

16

PHARMACOLOGICAL THERAPY FOR MOTOR
SYMPTOMS IN EARLY PD
The decision about initiation of pharmacologic
therapy in PD patients should be tailored to the
individual with the goal of reducing motor
symptoms, and improving quality of life without
causing side effects.
Factors that influence this decision include:
symptom severity, whether the symptoms affect the
dominant hand, embarrassment, ability to continue
working and/or participate in activities such as
hobbies, cost, and patient preference.
If symptoms are very mild, the patient may choose
not to begin therapy. 17
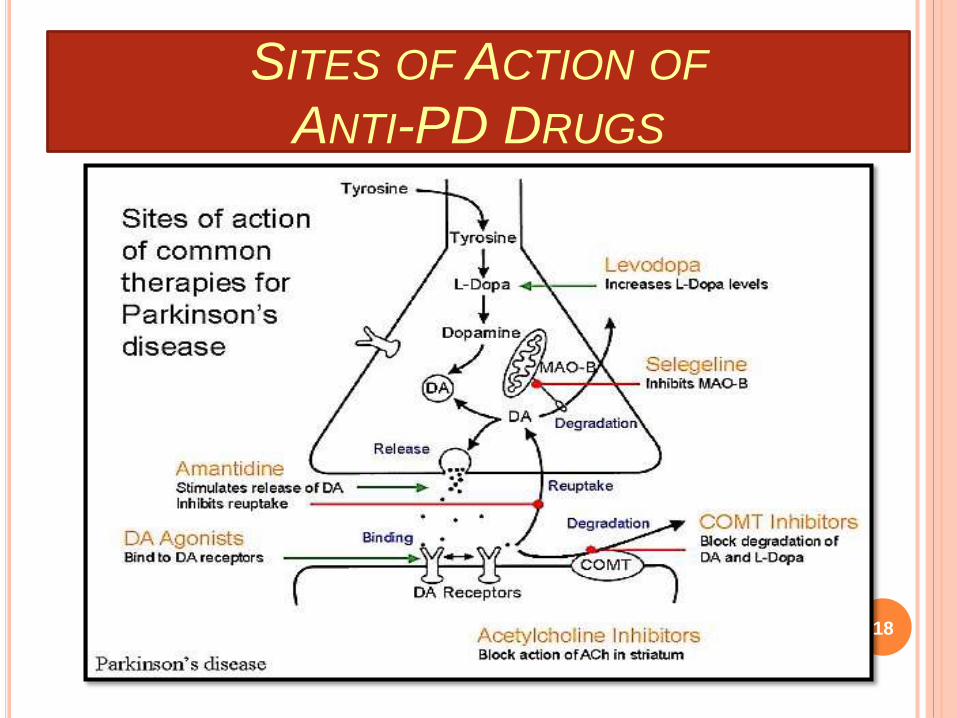
SITES OF ACTION OF
ANTI-PD DRUGS
18

NEUROPROTECTIVE THERAPY
Vitamin E should not be used as a neuroprotective
therapy for people with PD. NICE Level A
Co-enzyme Q10, dopamine agonists, monoamine
oxidase B (MAO-B) inhibitors should not be used as
a neuroprotective therapy for people with PD,
except in the context of clinical trials. NICE Level B
19

LEVODOPA
Levodopa remains the most effective medication for the
treatment of motor symptoms. It is always given in
combination with carbidopa to prevent decarboxylation in
the periphery.
Levodopa used as a symptomatic treatment for people
with early PD. NICE Level A
The dose of levodopa should be kept as low as possible
to maintain good function in order to reduce the
development of motor complications. NICE Level A
Modified-release levodopa preparations should not be
used to delay the onset of motor complications in people
with early PD. NICE Level A
20

DOPAMINE AGONISTS
Dopamine agonists stimulate dopamine receptors directly,
and unlike levodopa, do not need to be converted in the
brain to be active.
Dopamine agonists are the second most potent class of
medication (after levodopa) for control of motor symptoms
in PD with good evidence that they can be used in early
PD with success.
Dopamine agonists have less likelihood of producing
fluctuations in early disease, but are less effective, and
are associated with a higher prevalence of side effects
and they are also more expensive than levodopa.
21

Dopamine agonists may be used as a symptomatic
treatment for people with early PD. NICE Level A
A dopamine agonist should be titrated to a clinically
efficacious dose. If side effects prevent this, another
agonist or a drug from another class should be used
in its place.NICE Level D (GPP)
22

MAO-B inhibitors may be used as a symptomatic
treatment for people with early PD. NICE Level A
Amantadine may be used as a treatment for people
with early PD but should not be a drug of first
choice. NICE Level D (GPP)
23
Anticholinergics may be used as a symptomatic
treatment typically in young people with early PD
and severe tremor,but should not be drugs of first
choice due to limited efficacy and the propensity to
cause neuropsychiatric side effects. NICE Level B
Beta-adrenergic antagonists may be used in the
symptomatic treatment of selected people with
postural tremor in PD, but should not be drugs of
first choice. NICE Level D (GPP)
24

PHARMACOLOGICAL THERAPY FOR MOTOR
SYMPTOMS IN LATER PD
Up to 50% of patients on LD for 5 years’
experience motor fluctuations and dyskinesia.
These symptoms are, especially, common in
patients with onset of PD before 50 years of age.
they are unique to LD, and are not produced by the
other anti-Parkinson drugs.
Wearing off is the most common type of MF. It
refers to the predictable return of parkinsonian
symptoms in the hours before the next dose as the
plasma level of the drug falls below the critical level.
25

On/off is the unpredictable reappearance of parkinsonian symptoms at a time when central levels of anti-parkinsonian drugs are expected to be within the target of therapeutic range.
Delayed on is delay in the onset of symptom relief after a dose.
Dose failure is a complete failure to develop a favorable response to an incremental dopaminergicdose.
Protein-related offs occur when the transport of LD across the intestinal wall is impeded by competition for facilitated transport by large amounts of neutral amino acids.
26

Manipulation of the dose or frequency of levodopa can
be a first strategy but eventually the emergence of
dyskinesias will preclude this.
For patients with PD with motor fluctuations the
available evidence suggests: Entacapone and
rasagiline should be offered to reduce off time. AAN
Level A
Selegiline is associated with 2.2 hrs reduction in total
number of off hours compared to placebo (
waters et al 2004).
27
Entacapone, a COMT inhibitor and rasagiline, a
MAO-B inhibitor, have both been shown in clinical
trials to reduce off time by approximately 1.5
waking hours per day
Pramipexole and ropinirole should be considered to
reduce off time.AAN Level B
Dopamine agonists such as pramipexole, ropinirole
and bromocriptine have been shown in clinical trials
to reduce off time by approximately 15%.
28
Modified-release levodopa preparations may be
used to reduce motor fluctuations in people with
later PD but should not be drugs of first choice.
NICE Level B
Modified release levodopa remains most useful in
addressing overnight wearing off.
Amantadine may be considered for patients with
PD with motor fluctuations in reducing dyskinesias.
AAN Level C
29

TREATMENT - SURGERY
The surgical treatment for PD is currently
considered in advanced patients when the
optimized medical treatment has failed in treating
motor symptoms (such as motor fluctuations and/or
dyskinesia).
Although pallidotomy and thalamotomy might still
be performed in selected patients, deep brain
stimulation (DBS) is currently the surgical treatment
of choice in advanced PD patients.
The most used current targets for PD are: the
thalamus (Vim nucleus), the subthalamic nucleus
(STN), and the globus pallidus internus (GPi). 30

DBS of the STN may be considered as a treatment option in PD patients to improve motor function and to reduce motor fluctuations, dyskinesia, and medication usage. Patients need to be counselledregarding the risks and benefits of this procedure. AAN Level C
The overall improvement of ADLs and motor UPDRS scores in the off medication/on stimulation condition has been reported to be on average 50% when compared to the off medications condition before surgery.
Levodopa-induced dyskinesia has also been reduced by 69% on average after surgery. 31
Adverse events (AEs) due to the surgical procedure
include:
infections (6.1%), migration or misplacement of the
leads (5.1%), lead fractures (5%), intracranial
hemorrhage (3%), and skin erosion (1.3%)
The most reported complications possibly related to the
stimulation (especially STN DBS) and persistent in the
long-term follow-up include: eyelid opening apraxia
(1.8-30%), dysarthria/hypophonia (4-17%), gait
disturbances (14%), postural instability (12.5%) weight
gain (8.4%) and verbal fluency decline.
32

Preoperative response to levodopa should be
considered as a factor predictive of outcome after
DBS of the STN. AAN Level B
Age and duration of PD may be considered as
factors predictive of outcome after DBS of the STN.
Younger patients with shorter disease durations
may possibly have improvement greater than that
of older patients with longer disease durations. AAN
Level C
33

Bilateral GPi stimulation may be used in people
with PD who:
• have motor complications that are refractory to
best medical treatment
• are biologically fit with no clinically significant
active comorbidity •
are levodopa responsive •
have no clinically significant active mental health
problems, for example depression or dementia.
NICE Level D
34

GPi DBS may be perticularly useful for patients who
may have troublesome dyskinesia as well as mild
cognitive or behavioral impairment, whereas
bilateral STN DBS may be a choice for patients
who are cognitively intact but in whome reduction in
levodopa dosage is primary goal.
35

Thalamic DBS may be considered as an option in
people with PD who predominantly have severe
disabling tremor and where STN stimulation cannot
be performed. NICE Level D
Eliminate contralateral rest tremors in 75% to 85%
of patients , but there is less effect on rigidity and
no effect on bradykinesia.
36
OTHER TREATMENT OPTIONS
Physical and exercise therapies should be available
for people with PD. Particular consideration should
be given to:
• gait re-education, improvement of balance and
flexibility •
enhancement of aerobic capacity
• improvement of movement initiation
• improvement of functional independence,
including mobility and activities of daily living
• provision of advice regarding safety in the home
environment. NICE Level B37

PARKINSON’S MEDICINES IN THE PIPELINE
A gene therapy in development comprises an
adeno-associated virus (AAV) vector that delivers
the gene for aromatic L-amino acid decarboxylase
(AADC) to cells in a part of the brain that controls
movement.
An intraduodenal gel formation in development is a
com-bination of levodopa and carbidopa, which
helps prevent levodopa from being degraded before
it reaches the brain. This mechanism of delivery
helps prevent levodopa degradation and promotes
faster absorp-tion, and maintenance of more
constant levels of levodopa. 38

deacetylase inhibitors -target the transport system
and reverse the defects caused by the faulty
LRRK2 within nerve cells. The study is published
(15 October 2014) month in Nature
Communications.
Nicotine- Intake of nicotine has shown to slow the
degeneration of neurons.Acts similar to levodopa.
Melatonin-Serotonin derivative that helps insomnia.
Also shown to cause a reduction in production of
neurodegenerative radicals
39

Apomorphine (subcutaneous infusion or
injections)-Apomorphine is the most potent
dopamine receptor agonist and it can provide
symptom relief similar to that of L-dopa.
Apomorphine is rapidly absorbed, with onset of
effect within 5-15 minutes of subcutaneous
injection.
40
NON-MOTOR FEATURES OF PD -
MENTAL HEALTH
Depression -
1. Consider emotional fluctuations associated with
“OFF” periods → Reduce “OFF” time
2. Involvement of geriatric or neuro-psychiatrist;
3. SSRIs
)5. Pramipexole may have antidepressant effects
over and above its antiparkinsonian effects
Amitriptyline may be considered in the treatment of
depression associated with PD. AAN Level C
6. ECT in severe refractory cases 41

Psychotic Symptoms
1. R/o secondary (e.g., metabolic) causes; PD
medications should be eliminated in the following
order: anticholinergics → amantadine → DAs →
MAO-B inhibitors. L-dopa has the greatest motor
effect with the least mental SEs; the lowest dose that
satisfactorily controls PD symptoms should be used
2. Atypical antipsychotics for problematic psychosis:
3. Cholinesterase inhibitors may have anti-psychotic
effects in PD
4. ECT in severe refractory cases
42

Dementia-
Discontinue potential aggravators;
• Anticholinergics. EFNS Level B
• Amantadine, tricyclic antidepressants,
benzodiazepines, tolterodine and oxybutynin. EFNS
Level C
Donepezil should be considered for the treatment
of dementia in PD. AAN Level B
Rivastigmine should be considered for the
treatment of dementia in PD or Dementia with Lewy
Bodies. AAN Level B 43

Sleep Disorders-
Good sleep hygiene should be advised in people
with PD with any sleep disturbance and includes
NICE Level D (GPP)
Care should be taken to identify and manage
restless legs syndrome (RLS) and rapid eye
movement (REM) sleep behaviour disorder in
people with PD and sleep disturbance. NICE Level
D (GPP)
Modafinil may be considered for daytime
hypersomnolence in people with PD. NICE Level
D(GPP) 44

Autonomic dysfunction
General measures for treating urinary urgency and incontinence include avoiding coffee before bedtime, limit water ingestion before bedtime, etc.• Add peripherally acting anticholinergic drugs. EFNS (GPP)
Constipation
For gastrointestinal motility problems in PD:
• apply general measures for treating constipation. These include diet, laxatives, etc
• Reduce or discontinue drugs with anticholinergics
activity. EFNS (GPP)
• Add domperidone. EFNS Level B45

Orthostatic hypotension (OH)- 1. Non-pharmacological: ↑ fluid intake, ↑ dietary salt, avoid alcohol / large meals (frequent small meals instead) / excessive warmth, elevate head of bed. Patients should be advised to rise slowly, especially in morning or after sitting/lying for a period of time
2. Discontinue unnecessary medications, e.g., antihypertensives
3. Fludrocortisone
4. Domperidone
5. Midodrin
6. Consider pyridostigmine46

Management of Parkinson’s Disease REM behaviour disorder -Family history
Anosmia -Gene carrier
Constipation Pre diagnostic -Abnormal imaging
Reduced cardiac features -(dopamine marker)
R-R variability - ? Biomarker
Classic Feature Increased liklhood of diagnosis
Bradykinesia if following are present :
Rest Tremors Diagnosis based on -Rest tremor
Rigidity U K Brain bank crieteria -Asymmetry
Gait disturbances and supported by -Good response to levodopa
prediagnostic features -? Imaging of dopamine
system
Disease Modification - Seligiline ? ?
Non pharmacological - Rasagiline?
approach -Dopamine agonist???
-Exercise,education ,nutrition pramipexol,ropinirol
-Social and mentle activity
47
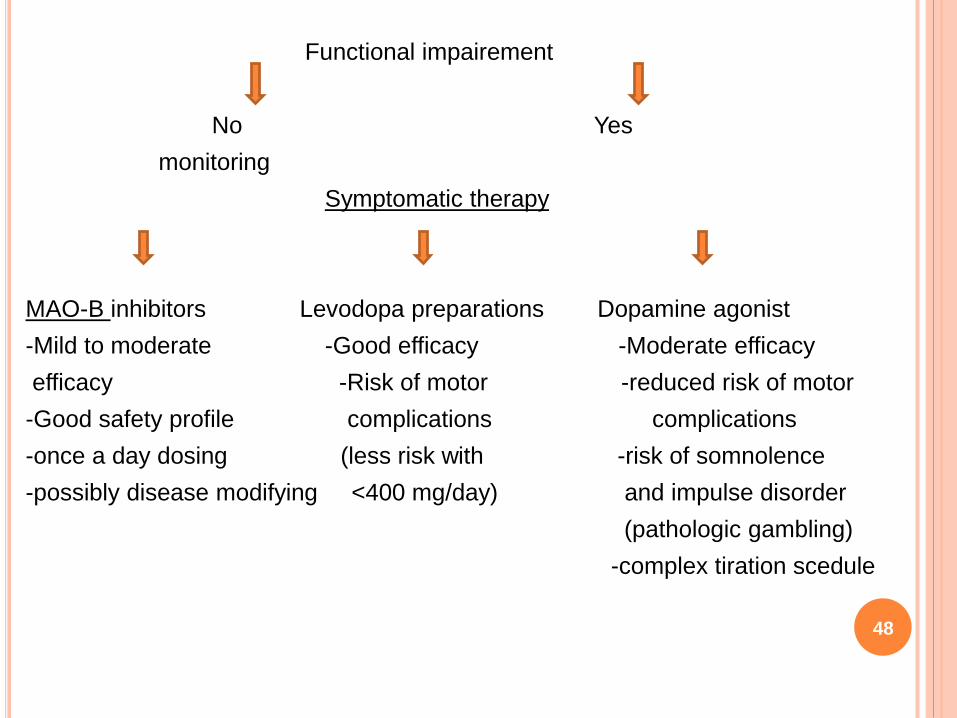
Functional impairement
No Yes
monitoring
Symptomatic therapy
MAO-B inhibitors Levodopa preparations Dopamine agonist
-Mild to moderate -Good efficacy -Moderate efficacy
efficacy -Risk of motor -reduced risk of motor
-Good safety profile complications complications
-once a day dosing (less risk with -risk of somnolence
-possibly disease modifying <400 mg/day) and impulse disorder
(pathologic gambling)
-complex tiration scedule
48
49
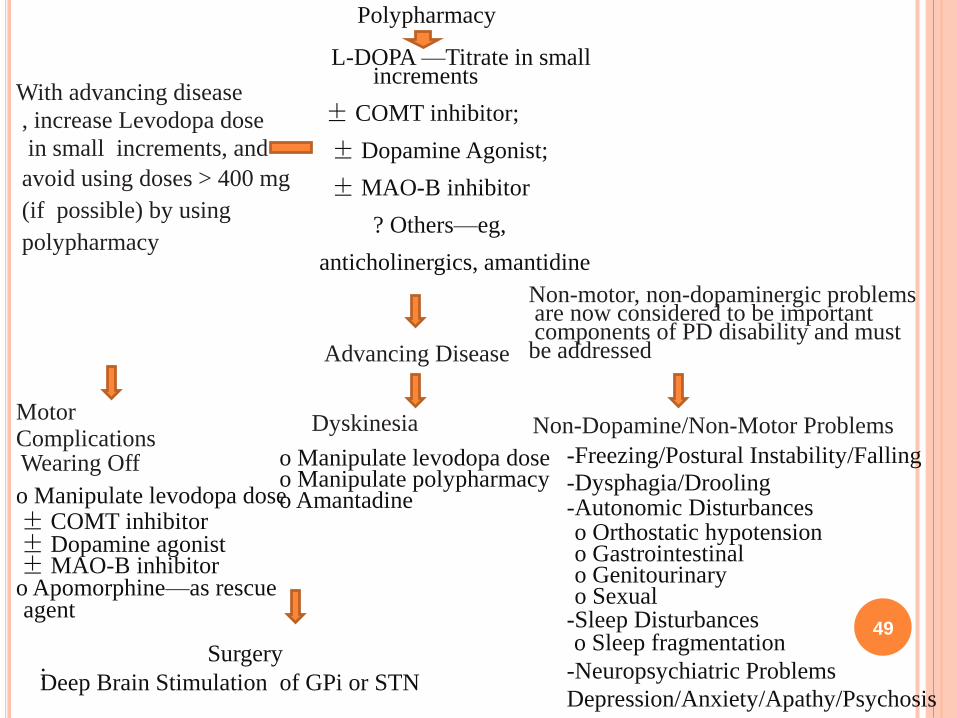
Polypharmacy
L-DOPA —Titrate in smallincrements
± COMT inhibitor;
± Dopamine Agonist;
±MAO-B inhibitor
? Others—eg,
anticholinergics, amantidine
Advancing Disease
With advancing disease
, increase Levodopa dose
in small increments, and
avoid using doses > 400 mg
(if possible) by using
polypharmacy
MotorComplicationsWearing Off
o Manipulate levodopa dose± COMT inhibitor± Dopamine agonist±MAO-B inhibitoro Apomorphine—as rescueagent
Dyskinesia
o Manipulate levodopa doseo Manipulate polypharmacyo Amantadine
Non-motor, non-dopaminergic problemsare now considered to be importantcomponents of PD disability and mustbe addressed
Non-Dopamine/Non-Motor Problems
-Freezing/Postural Instability/Falling
-Dysphagia/Drooling-Autonomic Disturbanceso Orthostatic hypotensiono Gastrointestinalo Genitourinaryo Sexual
-Sleep Disturbanceso Sleep fragmentation
Surgery:Deep Brain Stimulation of GPi or STN
-Neuropsychiatric Problems
Depression/Anxiety/Apathy/Psychosis

50

















