12
Recovery Audit Contractor (RAC) Denials 2010 Lean Symposium 4/20/2010 Presented by: Dennis McInerney representing The RAC Team $
| Date post: | 29-Dec-2015 |
| Category: |
Documents |
| Upload: | lionel-russell |
| View: | 218 times |
| Download: | 3 times |

Recovery Audit Contractor (RAC)Denials
2010 Lean Symposium
4/20/2010
Presented by: Dennis McInerney representing The RAC Team
$

2008-Present IHDM RAC Team CharterAim: To produce a complete and accurate medical record for each patient
encounter that reflects the quality and value of healthcare delivered. By August 31, 2009 the team will have implemented new processes which will achieve these goals.
Current State: CMS has hired the RAC (Recovery Audit Contractors) who are scheduled to identify and recoup improper Medicare payments. RAC implementation for Iowa is tentatively scheduled for Aug 1, 2009. On this date they will start to audit retrospectively back to Oct 1, 2007. It is estimated based on RAC take-back history that IHS-DM is vulnerable to an average annual $2.8MM loss (200 records every 45 days, take back rate of 35%,
and average $5k per claim). Currently the processes and documentation that produce our medical record are prone to errors and rework. We want to review , standardize and improve these processes. We also do not have a process in place to address response to RAC letters.
FOCUS: To develop a process for responding to RAC's by Aug 31,2009. This will consist of a baseline assessment of risks and development of processes: 1) to track and respond to RAC's denials and medical records requests, 2) to continuously improve documentation in the medical record in support of the RAC team aim and 3) to successfully implement these processes.
Measures: All will improve by August 31, 20091. Prebill IHDM edits and their turnaround time (time the edit made the edit list to the time the edit is billed will improve by 25%).
a. *CCI &*LCD/NCD: average days on list Dec 08 = 11.97 days turnaround, Feb 09 = 5.1 days turnaroundb. CCI &LCD/NCD: accounts sent to work list (accounts in) Dec 08= 5.1 million Feb 09=4.6 million
2. Discharged patient accounts not final billed due to documentation deficiencies will improve by 25%a. Post discharge coding query average unable to bill weekly 2008 – 2.5 million
2009 to date– 1.86 millionb. Dictation deficiency –unable to code and bill -average weekly 2008 – 2.1 million
2009 to date – 3.2 million3. Patients level of care changes will improve by 50% +
a. Dec 2008: 523 observation errors corrected. Average is 16.8 changes on a daily basis
*CCI: Correct Coding Initiative Edits*LCD/NCD: Local Coverage Determination/National Coverage Determinations
Team
Senior Leader: Mark Purtle, CMO
Team Leader: Patty Armstrong
Team Members: David Stubbs; Kara Dunham, Crystal Estabrook, Kim Hill, Nici Johnston, LeAnn Kai, Brenda Long, Barbara McLeod, Theresa Miller, George Morgan, Debra Myers, Susan Searcy, Glenda Seemiller, Janet Stipe, Joy Trude
Lean Advisors:
Dennis McInerney and Ray Seidelman
$

RAC Project Metrics
Measure Description Goal Baseline
1. PreBill IHDM edits and Turn around time
a. Turn Around Time – Average days on *CCI & LCD/NCD on list. Time the edit made the edit list to the time the edit is billed.
*CCI: Correct Coding Initiative Edits & LCD/NCD: Local Coverage Determination/National Coverage Determinations
b. Accounts In. $ accounts/volume sent to work list
a. 25% reduction
b. 25% reduction
a. Dec ’08 – 11.97 days
b. Dec ’08 – 5.1 MM
2.Documentation Deficiency
Average unbillable discharged patient accounts due to:
• Post discharge coding query• Dictation deficiencies
a. 25% reduction
b. 25% reduction
a. ’08 2.5 MM
b. ’08 2.1 MM
3. Level of Care (LOC) Changes
• Number Level of Care changes from original determination
• 50% reduction • Dec ’08 - 523 changes
Five measures in place to help drive improvements and lasting process improvement outcomes

RAC Project Improvement Metrics as of Jan ‘10
1a. HIM Claim Denials: Average Days on List
Average 72% Improvement!
Pre-Bill IHDM Edits - Average Days on List
0
2
4
6
8
10
12
14
Month
Ave
rag
e D
ays
on
Lis
t
0
10
20
30
40
50
60
70
80
90
% I
mp
rove
men
t to
Bas
elin
e
Average Days on List 11.97 5.24 4.95 3.75 2.31 4.1 5.03 4.79 3.04 2.23 1.83 2.62 2.81 2.87 2.24 2.04
% Improvement 56 59 69 81 66 58 60 75 81 85 78 77 76 81 83
Feb '09 Mar '09 Apr '09May '09
Jun '09 Jul '09 Aug '09 Sep '09 Oct '09 Nov '09 Dec '09 Jan '10 Feb '10 Mar '10
Average Discharge $'s
0
500,000
1,000,000
1,500,000
2,000,000
2,500,000
3,000,000
Month
Ave
rag
e D
isch
arg
e $'
s
0
10
20
30
40
50
60
70
80
% I
mp
rovm
ent
fro
m B
asel
ine
IMMC ILH % PNQ Change
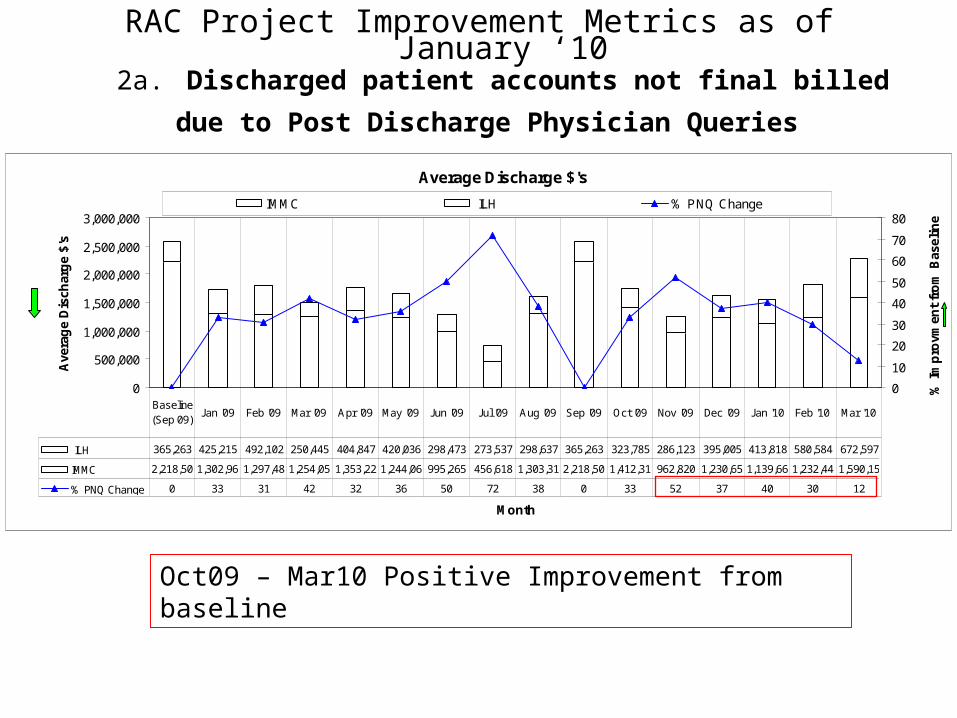
ILH 365,263 425,215 492,102 250,445 404,847 420,036 298,473 273,537 298,637 365,263 323,785 286,123 395,005 413,818 580,584 672,597
IMMC 2,218,50 1,302,96 1,297,48 1,254,05 1,353,22 1,244,06 995,265 456,618 1,303,31 2,218,50 1,412,31 962,820 1,230,65 1,139,66 1,232,44 1,590,15
% PNQ Change 0 33 31 42 32 36 50 72 38 0 33 52 37 40 30 12
Baseline(Sep 09)
Jan '09 Feb '09 Mar '09 Apr '09 May '09 Jun '09 Jul '09 Aug '09 Sep '09 Oct '09 Nov '09 Dec '09 Jan '10 Feb '10 Mar '10
RAC Project Improvement Metrics as of January ‘102a. Discharged patient accounts not final billed due to Post
Discharge Physician Queries
Oct09 – Mar10 Positive Improvement from baseline

RAC Project Improvement Metrics as of March ‘10
3. Level of Care Changes (adjusted for those in error)
Reduction in total LOC changes this March and a low of 6% Error Rate
Level of Care Changes
145 130 173110 107 124 109 133 146 142 108
155 232242
228 235 205 235 233 175 193169
2218
26
17 24 16 13 166
2146
0
100
200
300
400
500
May '09 Jun '09 Jul '09 Aug '09 Sep '09 Oct '09 Nov '09 Dec '09 Jan '10 Feb '10 Mar '10
Month
Ta
lly /
Co
un
t
Incorrect Input Clarifications Post Discharge
19% 15% 16% 6% 7% 7%
Incorrect InputsError Rate (Per Admissions)
7% 9% 9% 8% 6%

RAC Implementation Plan 3 “Work Streams”Denial Process Design, Error Reduction, Risk Management
April July
“Design in” RAC record submittal, appeal, and CBO/HIM/CM processes.
Improve the accuracy and completeness of current and future medical records
• Design and prototype record submittal, appeal, and recoup
• Simulate and redesign Sub processes
• Simulate “stress test” various high risk scenarios throughout all processes
Identify and fix any RAC impactful errors in past medical records and minimize financial loss
• Institutionalize new processes, roles, and responsibilities
• Identify areas in medical record with potential risk for inaccuracy and completeness
Design New and Improve Existing
Process Simulations & Overpayment
Identification & Disclosure
Communicate, Institutionalize
• Identify areas in medical record potential for RAC
• overpayment
• Fix any past records• Identify overpayments & Decide on
Disclosure
Dec
• Prioritize process improvements, ideate solutions, test, and refine
AnticipatedRAC
SubmittalsBegin
1
2
3
• Hardwire improvements and maintain the gains
Denial ProcessDesign
MR ErrorReduction
RiskManagement
Sep Ongoing

Denial Process Design“Lean from the Start”
• Team created Value stream maps always with the question “is this step necessary” and using Takt Time as a benchmark?• Integrated HIM processes with CBO system, CareMedic for efficient work flow• Designed in signals/triggers for any “handoffs”, utilize CareMedic software for work flow• Currently, testing work flow of process for additional streamlining
IHS-DM AUTOMATED RECOVERY AUDIT CONTRACTOR (RAC) PROCESS
RA
C
Coo
rdin
ato
rB
AC
KU
P: D
ata
Q
ualii
ty C
oord
. &
Den
ial C
oord
.
RACCoordinator
RACCoordinatorRAC
Coordinator
He
alth
Dat
a In
sig
ht
CM
SH
IMP
atie
nt
RA
C
Com
mitt
ee/O
ps
Gro
up/
UM
Com
mitt
ee
Ca
rrie
r/F
I /
MA
C
# Outcome
Cas
e M
gm
ntC
BO
RA
C A
ctio
n
Com
mitt
eeS
ervi
ce L
ines
/A
rea
sLe
gal
Legal
RAC Action
Committee
CBO
CaseMgmnt
CarrierFI
MAC
RAC Committee/Ops Group/
UM Committee
HIM
CMS
RAC
Hospital Depts
Patient
NO YES
YES
NO
NO
YES
NO
YES
NO
YES
NO
CareMedic
NO
RAC
Patient
AUTOMATED
CMSApproves
?
Review Daily CareMedic WorkList
AR Demand Letter
CarrierFI
MAC
Collect appropriate documents for Appeal
DOCUMENTATION
RAC
CarrierFI
MAC
Update Decision field in CareMedic
AR Appeal
CarrierFI
MAC
CMS
Medical Records Needed
?
CMS
Hospital Depts
Claim Determination . Send claim to Carrier /
FI/MAC
Automated Review
CMS
Charts, MR, UB
Within 15 days determine Root Cause and
Corrective Action and record on Template
AR Decision
Update CareMedic with Root Cause and Corrective
Action Template
AR Decision
ROOT CAUSE &
CORRECTIVE ACTION
Hospital Depts
CarrierFI
MAC
AppealRequest
?
Hospital Depts
Patient
Notify RAC Coord to Appeal or Not
AR Appeal
Issues Remittance Advice (RA)
Automated Review
CMS
Issues Demand LetterW $ and Appeal Rights
Automated Review
New Issue?
Hospital Depts
Begin Widespread review and update
Website
Automated ReviewSends New Issue
Review Request to CMS
Automated Review
Patient
RAC
Patient
RAC
HIM
Using CareMedic search and past records to Identify
any “Pattern /Criteria” for current patients admitted
Data Mining
Daily review in CareMedic possible delinquent
Request notifications
AR Request Mgmnt
RAC Action
Committee
Notify appropriate Dept and CC Exec Dir .
AR Request Mgmnt
Collect appropriate documents for Appeal
DOCUMENTATION
Escalation process
Update Dashboard with Root Cause & Corrective
Action Plan . Record response time
Dashboard Update
N432 posted on Remit
Automated Review
CaseMgmnt
Denial DashboardCase
Mgmnt
Need more information
?
RAC Action
Committee
CaseMgmnt
HIM
Applicable to Coding
Error?
CBO
CaseMgmnt
N432 posted on account “Adjustment based on
Recovery Audit”
Automated Review
RACCoordinator
HIM
RAC Action
Committee
RAC Committee/Ops Group/
UM Committee
CBOCBO
Assign and distribute Research Request in
Work Queue
AR Demand Letter
Present/Report to Exec Dir . New automated risk areas . Status of Root Cause and
Corrective Actions
Dashboard Update
Scan letter and attached to
corresponding accounts
AR Demand Letter
Send email ALERT to SELECT distribution on
Risk areas
Risk Alert
Make Copy of CD
DOCUMENTATION
RACCoordinator
RACCoordinator
CBO
HIM
Identify new posting and assign to appropriate
Work Queue
Dashboard Update
Present to committees status of appeals denied /justified by
Service area
Dashboard Update
PossibleDelinquent
Request?
Review CMS/HDI website for NEW risk areas
Auto/Complex Updates
Receive Demand Letter from Automated Review
AR Demand Letter
LegalLegal LegalLegal
YES REFER TO COMPLEX REVIEW
WPS
HDI website
------------------------------------------------------------------------
CareMedicDiscussion & Claim status
fieldsCareMedic
AUTOMATED
Are documents
In HPF?
YES
Deliver original documentation to RAC
Coordinator
DOCUMENTATION
CareMedic
NO
CareMedic CareMedicemail
------------------------------------------------------------
------------
RISK ALERT
TEMPLATECareMedic
------------------------------
------------------------------
------------
HPF
CareMedicCareMedicMore
Information Request
Update Level of Appeal in CareMedic
AR Appeal
CareMedic CareMedic
YES CareMedic
Package and ship CD to HDI
AR APPEAL
CareMedic
Denial Dashboard
CareMedic
ROOT CAUSE &
CORRECTIVE ACTION
CareMedic
CareMedic
Email, Call, face-to-face retrieval of
documentation
AR APPEAL
Denial Dashboard
CMS
RAC
Patient
HIM
Hospital Depts
Legal
CBO
RAC Action
Committee
CaseMgmnt
RAC Committee/Ops Group/
UM Committee
CarrierFI
MAC
Deliver to HIM for HPF archiving
DOCUMENTATION
Scan originals and index into HPF
DOCUMENTATION
HPF
Assemble ALL scanned documentation (Cover letters, records, notes,
etc.)
DOCUMENTATION
HPF
Scan originals and index into HPF
DOCUMENTATION
HPF
Burn all files onto CD
DOCUMENTATION
Deliver CD to RAC Coord
DOCUMENTATION
Are ALL filesVisible
?YES
NO
HPF
------------------------------------------------------------------------
Receive CD documentation & send
receipt
AR APPEAL
------------------------------------------------------------------------
Receive delivery receipt and update time in
CareMedic
AR APPEAL
------------------------------------------------------------
------------
Truck
LEGEND
Shapes
Paper
Flow
Computer Digital
Information
- - - - - - -
- - - - - - -
- - - - - - -
- - - - - - -
- - - - - - -
- - - - - - -
- - - - - - -
- - - - - - -
- - - - - - -
- - - - - - -
- -
LetterMail
Activity / Task / Step
# Outcome
AUTOMATED
#
Step
Database Information
Wait
Phone WalkActivity
TemplateStandard
Work
Outcome
)
/
Flow
/
Material
FlowPrint
Fax
Task
System
Information
(
Queue/
Data
COMPLEX
Report /Dashboard
?Decision
CD Rom
Receive email and review current select patients
matching criteria
Risk Alert
?
RISK ALERT
TEMPLATE
emailEscalation Process
Review daily work queue forAR letters
AR Demand Letter
Backup CD on Network and File CD
AR APPEAL
Share Drive
Record Delivery date ,And
Attach files to accounts in Caremedic
AR APPEAL
CareMedic
DATAMINING/RISK ALERTS AND AUTOMATED NOTIFICATION DECIDE ON APPEAL AND COLLECT AND ASSEMBLE DOCUMENTATION DELIVER DOCUMENTATION AND ESCALATION PROCESS FOR DELINQUENT
Automated Denial (“N432” posted”)
Complex Denial (“Requires Medical Record Review”)
1
Working Shifts per Day 1 ShiftsHours per Shift 8 Hours
Break Time per Shift 30 MinutesLunch Time per Shift 45 Minutes
Planned Downtime per Shift 60 MinutesCustomer Demand per Day 8 Units
Available Time per Shift 480 MinutesNet Working Time per Shift 345 MinutesNet Working Time per Shift 20,700 SecondsNet Available Time per Day 20,700 Seconds
Takt Time = 2,760 Seconds per PieceTakt Time = 46.0 Minutes per Piece
Takt Time Calculator
46 mins / recordAssuming 20 day
Intervals

Error ReductionFacts about Current Medical Record
In general current medical record contains:
1. 184 + documents types in HPF
2. Anywhere from 50 pages to over 2,000 + pages
3. Anywhere from 4 to 50 people can provide “input” through the course of the medical record “assembly” process
Observation Inpatient
Note: No Care Cast info added
From the floor …
40% (73) Handwritten 25% (46) Keyboard 24% (44) “Drop down / Pick list” 11% (21) Automated
4. The original source of input for the 184 documents are:
YIKES, Where do we start?
2

Error Reduction“Top 10” Medical Documents based on Risk Priority*
• *Risk Priority score is a function of four criteria1. The average # fields in the document2. The originating input method (see table to right)3. Annual Average number of people who can potentially enter
information4. Information in documents used by RAC (L,M,H)
Based on the prioritized
documents, sub teams were formed to verify potential risk, provide root cause analysis if
needed, implement solutions, and
ultimately improve accuracy and completeness.
Please bring on the EMR…
1Automated
3“Pick List”
6Keyboard
9Handwritten
Error Opportunity
WeightInput Method
1Automated
3“Pick List”
6Keyboard
9Handwritten
Error Opportunity
WeightInput Method
2
0 2000 4000 6000 8000 10000 12000 14000 16000 18000
Nursing AssessmentNursing Documentation
ReassessmentsRelease of Information DDS
Shift Assessment Transfusion Record
Clinical PathwaysObstetric Records
Phy Ord Adm Card Post CathPhy Ord Glycemic MgtDischarge InstructionsTransfusion Reaction
Interdisciplinary AssessmentPhy Ord Adm ACS Chest Pain
Phy Ord Adm Hrt FailurePhy Ord Adm Pneumonia
Phy Ord Adm General AdultPhy Ord Adm Postop Colon
Phy Ord Isc Stroke Tia Adm MedEmergency Department Records
Emergency Department ReportChemical Dependency
Outpatient DocumentationSleep Questionnaire
Phy Ord Susp Stroke Tia EdBirth Worksheet
Discharge PlanningDeath Report
Amendment of PHI by PatientTransfer Record
Release of InformationSelf Assessment
Clinical AssessmentCode Resuscitation
Intraoperative RecordRestrict Disclosure of PHI

Risk ManagementDisclosure or Not?
• Using an external audit team to identify overpayments & decide to make Disclosures versus appealing before RAC audit
Reduce potential denial pipeline by self disclosing known, unrecoverable, overpayments
3

Are we Ready?
Questions?













![Rowan - New England Friday.pptx [Read-Only]€¦ · 5/22/2012 3 Free‐Market Pruning: Amedisys LHC Group Gentiva Government Pruning: RHHI denials ZPIC extrapolations MAC audits RAC](https://static.documents.pub/doc/80x56/5fb7591be7c220771650648b/rowan-new-england-read-only-5222012-3-freeamarket-pruning-amedisys-lhc.jpg)



