Recovery-oriented practices within an Australian psychosocial Clubhouse: A case study analysis. Toby Raeburn BN, MA (Nurse Practitioner) A thesis submitted to fulfil the requirements of a Doctor of Philosophy (PhD) Degree Western Sydney University May 2016
Transcript
Recovery-oriented practices within an Australian
psychosocial Clubhouse: A case study analysis.
Toby Raeburn
BN, MA (Nurse Practitioner)
A thesis submitted to fulfil the requirements of a
Doctor of Philosophy (PhD) Degree
Western Sydney University
May 2016
DEDICATION
To Prati, Mikaela, Matthew and Hope.
With much love and gratitude,
Dad x.
ACKNOWLEDGEMENTS
This PhD thesis would not have been possible without the generous
assistance of many people. Firstly, I cannot imagine having access to a
more fantastic team of research supervisors. I would like to sincerely thank
Professor Michelle Cleary, Professor Virginia Schmied and Professor
Catherine Hungerford for their constant encouragement and guidance. I
have benefitted greatly from each of these exceptional mentors, including
their graciousness, wisdom and skills.
Secondly I would like to thank the members and staff of the
psychosocial Clubhouse, for allowing me to study and write about them.
Their openness, honesty and willingness to engage in the research as they
worked towards recovery together, was inspiring. I would particularly like to
thank the individuals who allowed me to observe their work and those who
participated in interviews. I will continue to advocate widely for more
awareness and application of recovery-oriented practice in mental health
services through my teaching and research.
Finally, I am forever indebted to my family. Extra special thanks to
my wife and children for all your love, patience and understanding, I could
not have completed this thesis without you. Also to my parents and my
sister’s family for your interest and support, thank you.
I
TABLE OF CONTENTS
TABLES AND FIGURES iv
PUBLICATIONS, PRESENTATIONS AND AWARDS v
ABSTRACT viii
CHAPTER 1: INTRODUCTION 1
1.1 Introduction 1 1.2 Traditional approaches to understanding recovery 2 1.3 Personal recovery 3 1.4 The origin and philosophy of the Clubhouse model 5 1.5 Aim of the study 8 1.6 Research questions 8 1.7 Significance of the study 8 1.8 Structure of the thesis 10 1.9 Conclusion 13
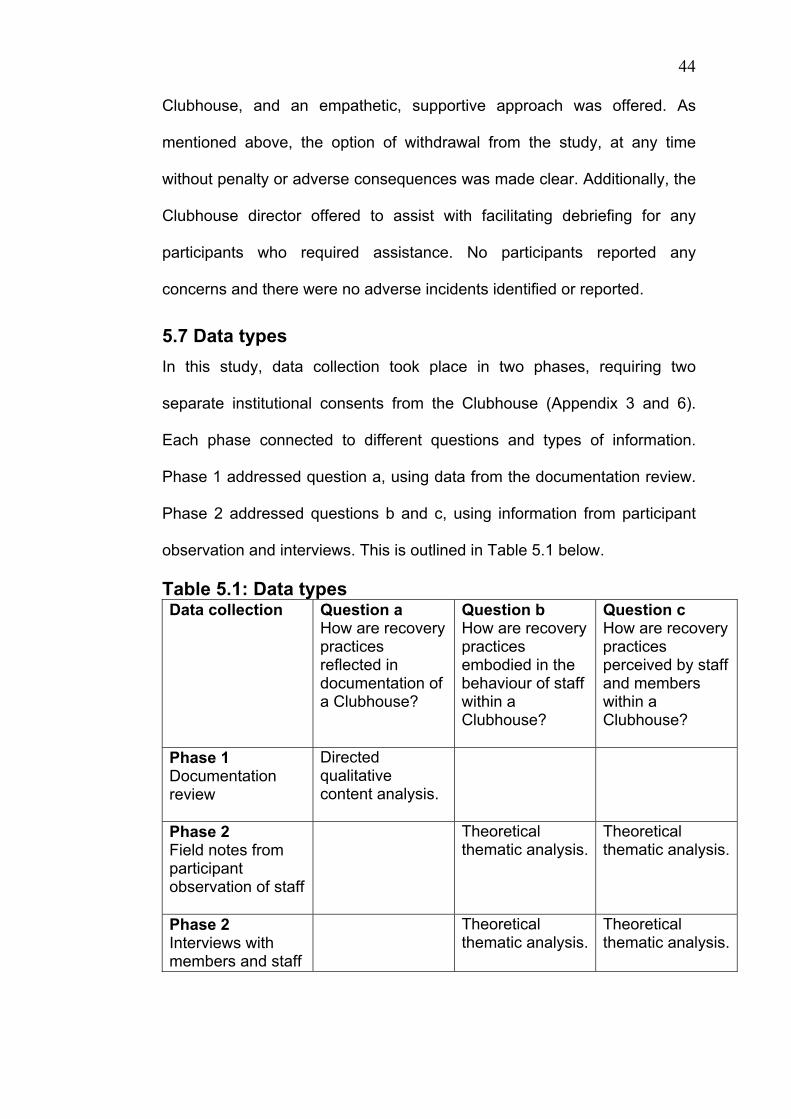
5.1 Introduction 38 5.2 Research questions 39 5.3 Self-determination theory 40 5.4 Research design 40 5.5 Setting 41 5.6 Ethics 42 5.6.1 University ethics approvals 42 5.6.2 Data storage, management and confidentiality 42 5.6.3 Vulnerable population considerations 43 5.7 Data types 44 5.8 Phase 1: Consent for documentation review 45 5.8.1 Data collection for documentation review 45 5.8.2 Establishing a corpus of documents 46 5.8.3 Qualitative content analysis of documents 47
II
5.9 Phase 2: Institutional consent for participant observation and interviews 47 5.9.1 Recruitment 48 5.9.2 Consent for participant observation of staff 48 5.9.3 Consent for interviews with staff and members 50 5.9.4 Data collection during participant observation 51 5.9.5 Data collection during interviews 53 5.9.6 Analysis of participant observation and interview data 54 5.10 Triangulation 55 5.11 Rigour 56 5.12 Reflexivity 58 5.13 Conclusion 60
CHAPTER 6: HOW ARE RECCOVERY-ORIENTED PRACTICES REFLECTED IN DOCUMENTATION WITHIN A CLUBHOUSE? 61
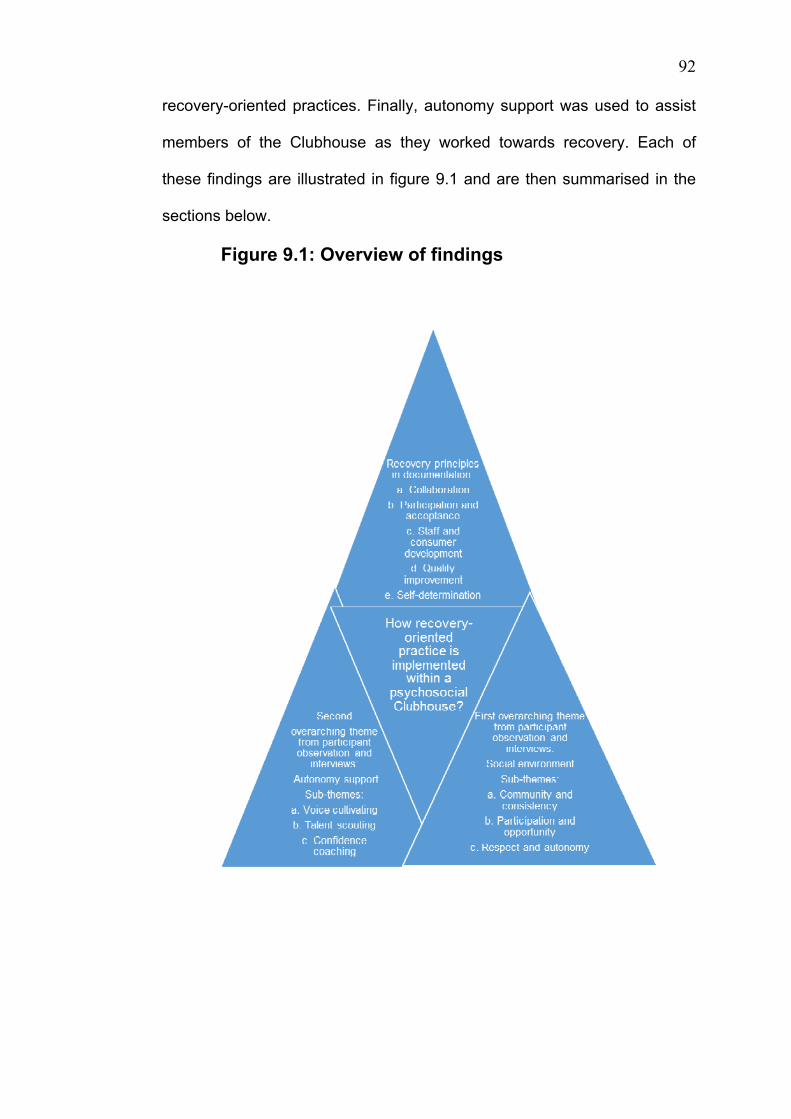
9.1 Introduction 90 9.2 The study 91 9.3 Overview of study findings 91 9.3.1. Documentation 93 9.3.2. Social environment 93 9.3.3. Autonomy support 93 9.4 Data triangulation 94 9.5 Discussion of study findings 96 9.5.1 The influence of the personal recovery concept 96 9.5.2 Utility of self-determination theory 98 9.5.3 Accreditation standards, flexibility and recovery 101 9.5.4 Representing the Clubhouse authentically 103 9.5.5 Viewing the Clubhouse as community 105 9.6 Implications of findings 107 9.6.1 Broaden the role of the Clubhouse 107 9.6.2 Promote recovery principles in documentation 109 9.6.3 Adopt a flexible approach to accreditation standards 110 9.6.4 Increase the evidence base of the Clubhouse 111 9.7 Strengths of the study 113 9.8 Limitations of the study 114 9.9 Final research reflections 116
III
9.10 Future research directions 120 9.11 Conclusion 121
REFERENCES 122
APPENDICES 140
Appendix 1 Ethics approval for documentation review 140 Appendix 2 Ethics approval for fieldwork 141 Appendix 3 Institutional consent for documentation review 142 Appendix 4 Study information sheet 143 Appendix 5 Permission to use the RPFS 145 Appendix 6 Institutional consent for fieldwork 146 Appendix 7 Staff participation information sheet 147 Appendix 8 Member participant information sheet 149 Appendix 9 Staff participant observation consent form 151 Appendix 10 Interview participant consent form 152 Appendix 11 Clubhouse director interview 153 Appendix 12 Clubhouse staff interview 155 Appendix 13 Clubhouse member interview 157
IV
TABLES AND FIGURES
Table 5.1 Data types 44 Figure 9.1 Overview of findings 92
V
PUBLICATIONS, PRESENTATIONS AND AWARDS
This thesis is presented as a series of six published papers. I am the first
author in each of these papers and assumed full responsibility for collecting
and analysing the data reported. All preliminary coding and analysis was
undertaken by me. This was then reviewed by my principal supervisor and
discussed and confirmed by my associate supervisors. I prepared the
drafts of each paper and my supervisors provided feedback on each draft
and revisions for journal submission. I drafted the response to journal
reviewers’ comments for each paper. My supervisors (co-authors) provided
feedback and guidance with final manuscript preparation.
Publications (International refereed journals)
Raeburn, T., Schmied, V., Hungerford, C., & Cleary, M. (2016). The use of
social environment in a psychosocial Clubhouse to facilitate recovery-
oriented practice. British Journal of Psychiatry Open, 2(2), 173-178.
at University of Western Sydney on July 19, 2014apy.sagepub.comDownloaded from at University of Western Sydney on July 19, 2014apy.sagepub.comDownloaded from
Reprints and permissions: sagepub.co.uk/journalsPermissions.nav
DOI: 10.1177/1039856213492235apy.sagepub.com
376
AP
Emerging from recognition that medical treatment alone did not meet the complex needs of people with severe mental illness, the original clubhouse
named “Fountain House” was established in 1948 by a group of ex patients from a New York psychiatric hos-pital.1 The methods at Fountain House have since been developed into the “clubhouse model” of psychiat-ric rehabilitation, which is currently used at over 300 sites, across more than 27 countries worldwide,2 includ-ing eight in Australia.3 The International Centre for Clubhouse Development website indicates there are four in Queensland, two in NSW, one in South Australia and one in Tasmania.3
While engaged in psychiatric rehabilitation, clubhouses have also been at the forefront of developing “recovery-oriented services”.4 According to Oades et al., recovery-focused mental health services often struggle to describe their model of care.5 The clubhouse model is an excep-tion, with 36 clearly articulated accreditation standards guided by the following four core principles3:
1) A right to a place to come;
2) A right to meaningful work;
3) A right to meaningful relationships;
4) A right to a place to return.
Using a social franchise approach reliant on both govern-ment and philanthropic funding, each clubhouse is organized as an independent center linked to Fountain House via a tri annual accreditation fee.2 Typically open Monday to Friday, modern clubhouses offer a broad range of programs designed to provide a safe environment, sup-portive relationships and employment opportunities.6
An overview of the clubhouse model of psychiatric rehabilitation
Toby Raeburn Nurse Practitioner, ROAM Communities Mental Health Nursing and PhD candidate School of Nursing & Midwifery, University of Western Sydney, Sydney, NSW, Australia
Elizabeth Halcomb Professor, Primary Health Care Nursing, School of Nursing & Midwifery & Indigenous Health, University of Wollongong, Wollongong, NSW, Australia
Garry Walter Professor of Child and Adolescent Psychiatry, University of Sydney, and Clinical Director, Child and Adolescent Mental Health Services, Northern Sydney Local Health District, Sydney, NSW, Australia
Michelle Cleary Associate Professor, Alice Lee Centre for Nursing Studies, Yong Loo Lin School of Medicine, National University of Singapore, Singapore
Abstract Objective: The aim of this article is to provide an overview of the clubhouse model and its capacity to assist people with severe mental illness.Method: The paper uses a sample vignette (with all identifying information removed) and survey of literature describing clubhouses over the last 15 years.Results: Strengths of the clubhouse model include its ability to provide a safe environment, supportive relationships and supported employment activities. Criticisms include its failure to provide onsite psychiatry clinics and a risk of promoting service dependence.Conclusions: Modern clubhouses continue to provide useful models of psychiatric rehabilitation which are popu-lar worldwide. Studying and describing the model is challenging due to its complexity. Mixed methodological approaches and recovery-orientated measurement tools may assist future research and development.
Correspondence:Associate Professor Michelle Cleary, Alice Lee Centre for Nursing Studies, Yong Loo Lin School of Medicine, National University of Singapore, Level 2, Clinical Research Centre, Block MD11, 10 Medical Drive 117597, Singapore. Email [email protected]
492235 APY21410.1177/1039856213492235Australasian PsychiatryRaeburn et al.2013
Psychiatric services
at University of Western Sydney on July 19, 2014apy.sagepub.comDownloaded from
The following vignette is used to illustrate some of the potential advantages of the model (all identifying infor-mation has been removed).
Vignette: ‘Susan’ had a complex history including devel-opmental disability, drug abuse and paranoid schizo-phrenia. She was referred to a local clubhouse by her government disability support pension caseworker. Through regular involvement, she started to feel more comfortable in the setting, forming friendships and engaging in prevocational skills-building activities that boosted her confidence. With the encouragement of members and staff, she soon began spending 3–4 days per week at the clubhouse, reducing social isolation which improved her self-esteem.
Managing Susan’s symptoms of paranoia and auditory hallucinations remained challenging due to her poor organizational skills, lack of disposable income and impulsivity. Two years after commencement at the club-house, her disability support pension caseworker was reviewing her file. She asked why Susan had been able to attend the clubhouse regularly but had been unable to find paid work in the competitive job market?
Overview
Like Susan, people seeking to overcome mental illness often cite improved social support as crucial to their recovery.7 In the clubhouse model, participants are referred to as “members” rather than patients or clients in an effort to engender shared ownership and involve-ment. Pursuing a satisfying life is preeminent, with a strong emphasis on identifying personal strengths rather than focusing on clinical symptoms.8 Members commonly cite increased confidence, acceptance, empowerment and hope through the opportunity to engage in supportive relationships with others who share their experience.9 Alongside supportive relation-ships, a wide range of rehabilitation programs are offered, typically including case management, social advocacy, housing assistance, psycho-educational and employment activities.2
Relevant to Susan’s involvement in confidence-building prevocational activities are the model’s employment pro-grams, which have been shown to be effective in rand-omized controlled trials.10,11 The model’s foundational prevocational program is an activity schedule referred to as “the work ordered day”.2 This follows the timetable of a typical working week, whereby instead of presenting for a time-limited appointment or therapeutic group, each day members are given the opportunity to work alongside paid staff. In this way, members build skills and relationships, while also assisting the function of the clubhouse, including reception and administration, meal preparation and building maintenance activities, etc.12
A second prevocational program offered by clubhouses is referred to as the “transitional employment program”. This provides short-term job placement positions
brokered between individual clubhouses and local busi-nesses, designed to provide a confidence-building step-ping stone towards paid employment.10 Finally, the model provides a “supported employment program”, which offers assistance and ongoing support to acquire and maintain work in the competitive job market.8
The multifaceted nature of modern clubhouses appears to have made them challenging for researchers to study and describe with consistency.13 For example, the club-house has been described as a “prevocational program”,14 a “multi service program”,10 a “self help group”,15 and an “intentional recovery community”.16 The apparent risk is that descriptions which focus on discrete clubhouse programs without acknowledging their place within the model’s wider context may lead to unfounded appraisal and false comparison.17
While the model’s complexity has proved challenging for researchers, it appears to have been viewed as a strength by people with severe mental illness who “vote with their feet”, averaging a daily attendance exceeding 160 participants per site at North American clubhouses.14 Indeed, the model has proved so popular amongst con-sumers and families in North America that it is now mandated in several states, and Hinden and colleagues suggest further programs should be developed through improved engagement and education of the children and families of members.15
Criticism
As suggested by Susan’s experience in the vignette, access-ing regular psychiatric review is often challenging for people with complex mental illness.16 A major gap in the clubhouse model is its failure to provide consistent access to on-site psychiatry clinics. With a few notable excep-tions in North America,8,18 this generally leaves members to organize their own access to psychiatric care.19 Relevant is research demonstrating that improved access to psychiatry leads to improved life satisfaction and higher rates of paid employment.20 There appears to have been an attempt to remedy this situation in recent times, with proponents such as Aquila and colleagues writing enthusiastically about the importance of providing improved access to psychiatry for clubhouse members.18
Another criticism may be found in the literature on models of supported employment, such as the Individual Placement Support (IPS) program which is recognized for its fast job placement of people with mental illness and provision of long-term clinical support.21 These studies often focus on comparing the IPS program with clubhouse’s two prevocational programs. Similar to Susan’s experience with her center link officer, concern is expressed in this research that members may become overly reliant on the relationships and activities within clubhouses, breeding a form of institutional depend-ence which compromising movement towards paid employment.21 If prevocational programs were all that clubhouses offered, then this criticism may be partly
at University of Western Sydney on July 19, 2014apy.sagepub.comDownloaded from
valid (notwithstanding the literature supporting the clubhouse’s value in the employment area18). However, while IPS is clearly an employment-focused program, the clubhouse model has multiple foci, emphasizing provision of a safe environment, social networks, edu-cational and employment opportunities.3
Implications and conclusion
The literature suggests that the modern clubhouse is a valuable model of psychiatric rehabilitation, providing a multifaceted mix of social, educational and employment programs that attract large numbers of people to over 300 sites worldwide.2 Opportunities to improve the model exist, and one example is the inclusion of onsite psychiatry clinics.18
The model’s complexity provides a challenging mixture of programs to describe and evaluate.13 Due to their applicability in complex healthcare settings, mixed methodological research approaches might be useful in future.22 Broad service evaluation paradigms such as recovery-orientated service measurement tools capable of adequately grasping the complexity of the clubhouse model might also be worth considering.23
DisclosureToby Raeburn is the founder and CEO of ROAM Communities, a mental health nursing charity that has been influenced by the clubhouse model.
References 1. Mowbray CT, Lewandowski L, Holter M and Bybee D. The clubhouse as an empowering
setting. Health & Social Work 2006; 31: 167–179.
2. McKay CE, Yates BT and Johnsen M. Costs of Clubhouses: An International Perspective. Adm Policy Ment Health 2007; 34: 62–72.
3. International Center for Clubhouse Development. International Center for Clubhouse Development. Available at: www.iccd.org (2012, accessed 21 June 2013).
4. Dudek KJ and Aquila R. Fountain house and recovery centers. Psychiatric Services 2012; 63: 396.
5. Oades L, Deane F, Crowe T, et al. Collaborative recovery: an integrative model for work-ing with individuals who experience chronic and recurring mental illness. Australas Psy-chiatry 2005; 13: 279–284.
6. Norman C. The Fountain House movement, an alternative rehabilitation model for people with mental health problems, members’ descriptions of what works. Scand J Caring Sci 2006; 20: 184–192.
7. Corrigan PW and Phelan SM. Social support and recovery in people with serious mental illnesses. Community Ment Health J 2004; 40: 513–523.
8. Stein LI, Barry KL, Dien GV, et al. Work and social support: a comparison of consumers who have achieved stability in ACT and clubhouse programs. Community Ment Health J 1999; 35: 193–204.
9. Wong KF. Implementation of Clubhouse Model programme: perception of mental health nurses. J Psychiatr Ment Health Nurs 2010; 17: 750–753.
10. Macias C, Rodican CF, Hargreaves WA, et al. Supported employment outcomes of a randomized controlled trial of ACT and clubhouse models. Psychiatr Serv 2006; 57: 1406–1415.
11. Cook JA, Razzano LA, Burke-Miller JK, et al. Effects of co-occurring disorders on employ-ment outcomes in a multisite randomized study of supported employment for people with severe mental illness. J Rehabil Res Dev 2007; 44: 837.
12. Staples L and Stein R. The clubhouse model: mental health consumer–provider partner-ships for recovery. Adv Med Sociol 2008; 10: 177–196.
13. Salkever DS. Policy priorities and shifting sands in the supported employment evidence base. Psychiatry Online 2006; 57: 1440.
14. Macias C, Jackson R, Schroeder C, et al. Brief report. What is a clubhouse? Report on the ICCD 1996 survey of USA clubhouses. Commun Ment Health J 1999; 35: 181–190.
15. Hinden B, Wolf T, Biebel K, et al. Supporting clubhouse members in their role as parents: necessary conditions for policy and practice initiatives. Psychiatr Rehabil J 2009; 33: 98–105.
16. Holmes A, Hodge M, Lenten S, et al. Chronic mental illness and community treatment resistance. Australas Psychiatry 2006; 14: 272–276.
17. Gregitis S, Glacken J, Julian C, et al. Comparing working role values of employed and unemployed Clubhouse members. Work 2010; 36: 39–46.
18. Aquila R, Malamud TJ, Sweet T, et al. The Store Front, Fountain House, and the Rehabili-tation Alliance. MedGenMed 2006; 8: 67.
19. Kightley M, Einfeld S and Hancock N. Routine outcome measurement in mental health: feasibility for examining effectiveness of an NGO. Australas Psychiatry 2010; 18: 167–169.
20. Cook JA, Leff HS, Blyler CR, et al. Results of a multisite randomized trial of supported employment interventions for individuals with severe mental illness. Arch Gen Psychia-try 2005; 62: 505.
21. Crowther RE, Marshall M, Bond GR, et al. Helping people with severe mental illness to obtain work: systematic review. BMJ 2001; 322: 204–208.
22. Creswell JW, Fetters MD and Ivankova NV. Designing a mixed methods study in primary care. Ann Fam Med 2004; 2: 7–12.
23. Burgess P, Pirkis J, Coombs T, et al. Assessing the value of existing recovery measures for routine use in Australian mental health services. Aust N Z J Psychiatry 2011; 45: 267–280.
at University of Western Sydney on July 19, 2014apy.sagepub.comDownloaded from
Self-determination Theory: A Framework for ClubhousePsychosocial Rehabilitation Research
Toby Raeburn, Nurse Practitioner; Psychiatry (MA, ACMHN, Churchill Fellow)ROAM Communities Mental Health Nursing and PhD candidate School of Nursing & Midwifery,University of Western Sydney, Sydney, Australia
Virginia Schmied, RN, PhDSchool of Nursing and Midwifery, University of Western Sydney, Sydney, Australia
Catherine Hungerford, RN, PhDDisciplines of Nursing and Midwifery, Faculty of Health, University of Canberra, Australia
Michelle Cleary, RN, PhDSchool of Nursing and Midwifery, University of Western Sydney, Australia
The Clubhouse model is a widely used approach to psychoso-cial rehabilitation that has been a pioneer in supporting recovery-oriented programmes. Little consideration has been given how-ever, to the theories that guide research of the recovery practicesused by Clubhouses. In this paper, we provide a description ofself-determination theory, including its philosophical backgroundfollowed by explanation of its relevance to health care and Club-house contexts. We argue that self-determination theory providesa robust social constructionist theoretical framework that is well-suited to informing research related to psychosocial rehabilitation,recovery-oriented practices and the Clubhouse model.
INTRODUCTIONRecovery-oriented approaches to providing health care to
people with a mental illness are now an important means of pro-viding consumer-centred services worldwide (Cleary, Horsfall,O’Hara-Aarons, & Hunt, 2012; Hungerford & Kench, 2013).The concept of ‘recovery’ in this context no longer refers totraditional medical approaches focussed on the treatment ofclinical symptoms, but rather to services that support people,as they negotiate the complex psychosocial challenges that sooften confound the efforts of people with mental illness to live asatisfying life (Warner, 2004, 2010). The evolution of recovery-oriented models of care has been strongly influenced by the
Address correspondence to Toby Raeburn, RN, MA, Nurse Prac-titioner, PhD candidate School of Nursing & Midwifery, Universityof Western Sydney, NSW, Australia. Post: ROAM Communities, POBox 154, Camden NSW, 2570, Australia. Tel: 0407608066. Email:[email protected]
pioneering work of the Clubhouse model of psychosocial reha-bilitation (Dudek & Aquila, 2012).
The original Clubhouse was started in New York towards theend of the great depression in the late 1940s, by a group of peoplewith a history of psychiatric hospitalisation, in an effort to pro-vide friendship and assistance to one another (Gregitis, Glacken,Julian, & Underwood, 2010). In the modern era, the Club-house model is now used by over 300 services, spread through-out the globe, providing a well-developed range of psychoso-cial programmes to people with mental illness (Warner, 2010).Programmes include peer support, educational, health promo-tion, vocational and supported employment activities (Raeburn,Schmied, Hungerford, & Cleary, 2014).
The extensive use of the model and wide variety of pro-grammes provided by Clubhouses internationally, highlightsthe need to identify a theoretical framework to inform researchexploring how recovery-orientated practices are used by theseservices (Anthony, Rogers, & Farkas, 2003). Mancini (2008)has identified a strong link between recovery-oriented prac-tices and the core propositions of self-determination theory. Heargues that self-determination theory provides a useful theo-retical framework for researching recovery-oriented practiceswithin services. This paper draws on the literature related toself-determination and argues that self-determination theory isalso a good fit for Clubhouse research.
As with all research, there is a need to explicate the theoret-ical lens, through which Clubhouse research data is examinedand interpreted. Acknowledging the importance of theory mayprovide an indication to other researchers, practitioners, policy-makers and educators of how recommendations derived fromresearch can be best interpreted (Kosciulek & Merz, 2001).
145
21
146 T. RAEBURN ET AL.
Indeed, the potential for a theoretical framework to affect thefindings of any research elevates the importance of theory inresearch, including the central tenets and philosophical under-pinnings of the theory.
SELF-DETERMINATION THEORYDeveloped by Edward Deci and Richard Ryan (2000), self-
determination theory is a general theory of human motivationfocussed on how the relationship between social environmentand psychological motivation can affect the wellbeing of peo-ple. The theory has been used to guide a wide range of stud-ies, including but not limited to the fields of physical health(Carroll, Fiscella, Epstein, Sanders, & Williams, 2012), edu-cation (Standage, Duda, & Ntoumanis, 2005) and employment(Gagne & Deci, 2005). Correlations between the principles ofself-determination theory with notions, such as psychologicalcapacity and social circumstance, suggest the theory may bewell suited to inform mental health research (Mancini, 2008).
The Principles that Frame Self-determination TheoryA central proposition of self-determination theory is the sug-
gestion that all people are born with three fundamental psycho-logical needs: competence, autonomy and relatedness (Ryan& Deci, 2000). Competence refers to people’s inherent desireto feel capable of influencing the outcomes of their lives andcontributing to their community. Relatedness refers to people’sneed for satisfying and supportive relationships. Finally, auton-omy is concerned with people’s freedom to make choices (Deci& Ryan, 2012).
According to proponents of self-determination theory, peo-ple have the potential to be either ‘a-motivated’, a state whereno motivation is present; ‘extrinsically motivated’, which in-cludes involvement in an activity to obtain external rewards; or‘intrinsically motivated’, which refers to activity undertaken tosatisfy a person’s core values or interests (Ryan & Deci, 2000).Stages of motivation are thought to be strongly influenced byhow people interact with their social environment and the qual-ity of their relationships (Kasser & Ryan, 1996). To exemplify,a person with a learning disorder who has been unemployed forover 5 years was referred to a pre-employment course by theiremployment services provider. However, while the course washeavily subsidised by the government making it affordable, itrequired good reading skills and was full of people who hadbeen recently employed. Unsurprisingly, the person quickly de-veloped feelings of a-motivation and this was reflected by poorparticipation. Alternatively, if the same person with mental ill-ness was offered a financial incentive to complete a readingskills course they may experience extrinsic motivation linkedto the perceived financial benefit they might receive by com-pleting the course. Finally, another person may be intrinsicallymotivated to engage in voluntary work teaching reading skillsbecause they value altruism.
A core tenet of self-determination theory is that people willinvolve themselves in activities and behaviours more if they
feel intrinsically motivated, thereby valuing their autonomy orability to choose (Deci, Koestner, & Ryan, 1999). As such, thetheory posits that the highest stage of motivation is intrinsic andthat the lowest stage is a-motivation. In-between these pointsare various stages of extrinsic motivation. According to thetheory, the more a person’s behaviour progresses from beingdriven by obvious extrinsic rewards towards the developmentof autonomous, intrinsic motivation, the more they are likelyto engage in self-motivated behaviours, thereby increasing theirsatisfaction with life (Stone, Deci, & Ryan, 2009). For example,a person living with chronic or severe schizophrenia, who isunemployed, socially isolated, and required by law to attend aClubhouse rehabilitation service 2 days per week, would havelower motivation to maintain a treatment plan than a person withthe same illness who has a job, social supports and the freedomto choose where and with whom he or she socialises.
The Philosophy Behind the Self-determination TheoryThe philosophy behind the self-determination theory largely
stems from an assertion made by the Greek philosopher Aris-totle (3–400 bc) that the final goal of all people’s thoughts andbehaviours, is the experience of happiness (Ryan & Deci, 2001).According to Aristotle, there are two broad ways people can ex-perience happiness. The first way involves the pursuit of goodcharacter, which he referred to as ‘eudaimonic’ happiness. Thesecond way includes the pursuit of feelings of pleasure, whichhe referred to as ‘hedonic’ happiness (Kashdan, Biswas-Diener,& King, 2008).
Aristotle claimed that hedonic happiness was of less worththan eudaimonic happiness because he observed that hedonic in-terests, such as power and wealth, while useful, were generallyassociated with temporary feelings that failed to provide lastinghappiness (Crisp, 2000). Furthermore, he maintained that whentoo much emphasis was placed on experiencing feelings of plea-sure, it could distract attention from the eudaimonic pursuit ofgood character – thereby impeding lasting happiness (Ryan &Deci, 2001).
In contrast, Aristotle posited that genuine, lasting happinesscan be achieved by engaging in persistent, virtuous behaviours,which lead to the development of good character and genuine,lasting happiness (Huta & Ryan, 2010). Shaped by the ancientculture in which he lived, Aristotle’s ideas of virtues includedtraits such as wisdom, courage, generosity and contemplation(Kashdan et al., 2008). Interestingly, he also believed one of themain impediments to the pursuit of virtue was poverty (Crisp,2000). For example, he contended that a level of wealth, helpfulparental guidance and a good education were all required forpeople to be able to pursue eudaimonic living. He further arguedthat providing the social platform for a society with access tosuch opportunities was the role of government (Crisp, 2000).This assertion differed from the viewpoints of other ancientphilosophers, such as Buddha (Honderich, 2005) and Christ(Adamut, 2011), who both taught that human happiness hadlittle to do with wealth or the role of government.
22
A FRAMEWORK FOR CLUBHOUSE PSYCHOSOCIAL REHABILITATION RESEARCH 147
Self-determination theorists have developed a modern inter-pretation of what it means to pursue eudaimonic living (Huta& Ryan, 2010). Consistent with Aristotle, they promote theidea that living a reflective life pursuing intrinsic values, suchas integrity and loving relationships, relies heavily on contex-tual factors, such as the opportunity to live in a free societythat allows autonomous choice (Ryan & Deci, 2001). Empha-sising the strong links between people’s levels of motivationand their contextual circumstance, positions self-determinationtheory within the social constructionist philosophical paradigm(Gergen, 2011).
Social constructionism contends that human knowledge isthe result of society’s ever-changing interpretation of the worldaround us (Christiansen, 2000). This philosophical approachchallenges the idea that purely rational, objective knowledgeexists, suggesting instead that knowledge actually arises fromprocesses related to ideology, interests and power (Conrad &Barker, 2010). Gergen (2011) suggests that another reason toview approaches such as self-determination theory as a socialconstructionist paradigm is the wide variety of ways in whichlanguage has been used to construct psychological concepts,such as motivation, throughout history, by a range of peopleand interest groups. For example, prominent theories, such asMaslow’s hierarchy of needs (Sheldon, 2011); Pavlov’s classicalconditioning (VanElzakker, Dahlgren, Davis, Dubois, & Shin,2013); and Skinner’s operant conditioning (Hahn, 2013), usedescriptive terms, such as ‘drives’, ‘behaviours’ and ‘needs’ todescribe motivation. In the same way, self-determination theorypromotes its own language to describe motivation, referring toideas, such as ‘psychological needs’, ‘autonomy’, ‘competency’and ‘relatedness’ (Deci & Ryan, 2012). These differences high-light the way in which the concepts are socially constructedaccording to context, setting, situation and, by association, the-oretical framework – and are discussed later in this paper.
The social constructionist approach that is inherent to socialdetermination theory has relevance to Clubhouse research be-cause of the implications this type of philosophy has for howmental illness and recovery are conceptualised (Gergen, 2011).When researchers adopt a traditional positivist medical theoret-ical framework, mental illness is viewed as a biological disease,independent of time, place and person. Using a social construc-tionist approach however, ideas regarding mental illness andrecovery are acknowledged as being connected to the meaningsand experiences attributed by social groups and cultural norms(Conrad & Barker, 2010).
As a leading proponent of recovery-oriented services,the Clubhouse model has strongly advocated for a re-conceptualisation of the experience of mental illness in a waythat acknowledges the link between social forces and recovery(Schiff, Coleman, & Miner, 2008). The Clubhouse model hasinvented its own language to reflect this stance, referring to par-ticipants as ‘members’ rather than patients or clients; and usingother terms, such as the ‘work ordered day’ or ‘transitional em-ployment’ to refer to concepts which remain quite unique to the
Clubhouse environment (Anderson, 1998). By adopting a socialconstructionist approach and focussing on the effect of contexton people’s motivation and behaviour, self-determination theoryis well-suited to Clubhouse research (Mancini, 2008). How thistheory has been applied in healthcare research and it relevanceto Clubhouse studies will now be described.
THE APPLICATION OF SELF-DETERMINATION THEORYSelf-determination theory, set within a social construction-
ist paradigm, provides an excellent framework to examine theprocesses related to enabling a person to make choices. This isbecause the key concepts of competence, autonomy and relat-edness, which are central to the theory, together with notionsof motivation and context, support consideration of what fac-tors are involved when people make choices. In the arena ofhealth care, links have been made between consumer-centredapproaches to health care and self-determination theory.
Relevance in Health-related ResearchSelf-determination theory has informed a wide variety of
health-related studies (Ng et al., 2012). For example, in mentalhealth, the theory has contributed to the development of thepsychological therapeutic approach, known as ‘motivationalinterviewing’ (Markland, Ryan, Tobin, & Rollnick, 2005). Ithas also begun to be referred to in positioning research related tomental health recovery (Cook et al., 2012). Researchers study-ing self-determination theory in health contexts have developedthe term ‘autonomy support’ to describe the role of healthpractitioners in assisting consumers to transition towards greaterlevels of motivated behaviour (Ryan, Patrick, Deci, & Williams,2008).
Autonomy support suggests that practitioners adopt a person-centred, motivational coaching approach, incorporating the per-spectives of the person they are supporting into the interventionsthat are planned (Ryan et al., 2008). Through the use of thistechnique, information is provided to enable informed decision-making by the person in need. This kind of practice is contrastedwith coercive, paternalistic or authoritarian approaches that havebeen used in the past and serve to pressure the person into takinga course of action that suits the health practitioner more than theperson in need (Barreira, Macias, Rodican, & Gold, 2008).
While the benefits of autonomy support include assisting theperson in need to self-determine, critics of the approach con-tend that the concept of autonomy lacks relevance in many ofthe world’s cultures (Chirkov, Ryan, Kim, & Kaplan, 2003). Forexample, it has been argued that in many cultures, collectivistvalues, such as conformity, family and social obligations, aremore important than individuality (Vansteenkiste, Zhou, Lens,& Soenens, 2005). Self-determination theory researchers haveobjected to this suggestion however, asserting that ideas re-lated to autonomy differ substantially from notions of indi-viduality because autonomy refers to the self-approval of aperson’s actions in the midst of community roles and values
23
148 T. RAEBURN ET AL.
(Lynch, La Guardia, & Ryan, 2009). In short, if a person from acollectivist culture is able to self-endorse their actions as part oftheir community, they are autonomous beings.
Studies framed by self-determination theory have also beenused to research practice within healthcare organisations, suchas management techniques, workplace culture, organisationalchange and productivity (Deci et al., 2001; Stone et al., 2009).For example, findings from one study suggested that staff whofeel that their sense of autonomy is supported by managementare more likely to take initiative and work as a team, therebyincreasing productivity without any increase in monetary reward(Stone et al., 2009). In the context of a mental health service,such as a psycho-social Clubhouse, this kind of empoweringculture may hold potential to translate into higher participationrates and improved recovery outcomes for people with mentalillness.
Relevance in the Clubhouse ContextAs already noted, Clubhouses provide a broad range of pro-
grammes to support people with a history of mental illness,inclusive of, social, educational, employment and health pro-motion activities (Raeburn et al., 2013). These programmes areconsumer-centred, and rely heavily on the participation of mem-bers (Dudek & Aquila, 2012; Pernice-Duca & Onaga, 2009).The Clubhouse environment, then, shares much in commonwith self-determination theory – in particular, an emphasis onthe social environment, and the attribution of meaning by thesocial group to which the person belongs, regarding notions ofmental illness and recovery. In the sections that follow, three ofthe core concepts of self-determination theory identified earlieron in this paper – competency, relatedness and autonomy – areconsidered in light of the Clubhouse model.
CompetencyIn self-determination theory, competency refers not only to
people’s vocational skills but more broadly to a sense of feel-ing involved and able to influence life outcomes in the con-text of community. In the same way, Clubhouse programmesseek to empower people with mental illness with a wide varietyof communication and relationship building skills. At its hearthowever, the Clubhouse model maintains its strongest emphasison employment preparation programmes that seek to build vo-cational competency among members, thereby addressing thehigh unemployment that faces people with mental illness world-wide (Harvey, Modini, Christensen, & Glozier, 2013). The ac-tivity schedule of each Clubhouse is organised around a dailytimetable called the ‘work ordered day’ (Norman, 2006). Thisapproach is designed to encourage and develop work skills inmembers through engagement in vocational activities (Gregitis,2010).
Using the structure of the work ordered day, Clubhousesengage in at least two forms of teaching. First, they engagemembers in a process of practical skills development by involv-
ing them in kitchen, clerical and maintenance tasks, which areall part of the Clubhouses daily routine. Second, there is anattempt to use language to teach subconscious messages – forexample, the concept of ‘work’ is promoted as a normal partof daily activity through repeated messaging in key documentsrelated to ‘work units’ or the ‘work ordered day’ (Raeburn et al.,2014). Similarly, Gregitis (2010) found that the vocational pro-grammes within a Clubhouse provided a valuable platform thatboth unemployed and employed members could derive a senseof improved competency and wellbeing from.
In another study that examined the education programmes in-side Clubhouses, Mowbray, Megivern, and Holter (2003) foundthat practicing assertive communication and information gath-ering provided an increased sense of competence in prepara-tion for paid employment opportunities. To encourage partici-pation in these programmes, course topics are designed from theideas of the Clubhouse members (Mowbray, Collins, Bellamy, &Megivern, 2005). This inclusive approach, involving membersin the design of their own programmes, aligns with the con-cept of relatedness that is a central tenet of self-determinationtheory.
RelatednessThe notion of relatedness is also promoted by Clubhouse
language, which specifically refers to participants as ‘members’rather than ‘patients’ or ‘clients’, thereby promoting a senseof shared ownership and partnership with paid staff (Coniglio,Hancock, & Ellis, 2010). Membership is voluntary, without timelimits and members are treated as equals with paid staff inthe day-to-day administration of Clubhouses (Aglen, Hedlund,& Landstad, 2011). This approach stands in stark contrast tothe power relations of traditional psychiatric and psychologicalservices, where a participant is typically viewed as a weakenedpatient in need of assistance from a clinician who is positionedas having the power to heal (Conrad & Barker, 2010).
Relatedness is similarly promoted by the Clubhouse employ-ment strategy of deliberately employing low numbers of paidstaff, thereby creating an environment where members need tobe relied upon to complete daily tasks (Norman, 2006). Theimportance of understanding how relationships are experiencedwithin a Clubhouse (Williams, Barclay, & Schmied, 2004) wasexplored by Coniglio et al. (2010), who observed that vocationalemployment activities generated a sense of shared achievementthrough doing which, along with social inclusion and inter-dependency, provided positive relational experiences within aClubhouse. In another study that focussed on the experience ofClubhouse members’ families, Scheyett, McCarthy, and Rausch(2006) observed that Clubhouses often alleviate the family andcaregiver burden by assisting in improving relationships be-tween Clubhouse members and their families. In summary, im-proved relatedness among people who engage with Clubhouseservices has been found to improve their autonomy (Aquila,Malamud, Aquila et al 2006).
24
A FRAMEWORK FOR CLUBHOUSE PSYCHOSOCIAL REHABILITATION RESEARCH 149
AutonomyTraditional mandatory hospital and criminal justice services
have a background of treating people with severe mental illnessin stigmatising and coercive ways (Horsfall, Cleary, & Hunt,2010). In contrast, the Clubhouse model provides a safe envi-ronment and invites people to participate voluntarily, assistingwith identification and pursuit of social, educational and em-ployment goals (Raeburn, Halcomb, Walter, & Cleary, 2013).This approach reflects the concept of autonomy support, whichis central to self-determination theory (Ryan et al., 2008). Club-house members have described their experience of recovery asautonomous choices made possible by a mixture of their ownmotivation and peer and paid staff member support (Herman,Onaga, Pernice-Duca, Oh, & Ferguson, 2005).
As already noted, Clubhouses operate in over 30 countriesworldwide. For this reason, there are cross-cultural consider-ations for the applicability of theoretical frameworks used toinform Clubhouse research. There are precedents, however. Forexample, the Swedish study of Norman (2006) highlights howthe supportive environment, employment programmes and so-cial activities provided by Clubhouses enhance the autonomyof members. Similarly, in a South Korean study undertaken byJung and Kim (2012), the findings indicated less stigma andhigher quality of life experienced by members of a Clubhousethan among participants of a comparison programme. Moreover,themes related to autonomy, such as being provided with the op-portunity to assume responsibility, to make a contribution and tobuild identity, were cited as crucial to facilitating recovery (Jung& Kim, 2012). While autonomy has been identified by some asan individualistic concept (Lynch et al., 2009), it has been shownto be cross-culturally applicable, suggesting the applicability ofself-determination theory to Clubhouses worldwide.
IMPLICATIONS AND RECOMMENDATIONS FOR THEFUTURE
Despite an international shift away from institutional-basedcare to community treatment modalities, substantial social in-equities continue to exist internationally that hamper the abil-ity of people with mental illness to live autonomous, self-determined lives (Mandiberg & Warner, 2013). For example,in countries such as Australia and the USA, three times morepeople with serious mental illness are unemployed than peoplewithout mental illness (Harvey et al., 2013; Ramsay et al., 2011).In addition, people with mental illness have double the chanceof experiencing comorbidities, such as substance use disorder(Hunt, Siegfried, Morley, Sitharthan, & Cleary, 2013); incar-ceration (Baillargeon, Binswanger, Penn, Williams, & Murray,2009; Butler, Indig, Allnutt, & Mamoon, 2010); and home-lessness (Australian Government, 2009; Baggett, O’Connell,Singer, & Rigotti, 2010).
The Clubhouse model has been a pioneer of recovery-orientated services, providing psycho-social programmes thatadopt a strong consumer-centred approach (Warner, 2010). If
services and policy-makers are to be adequately informed aboutthe practical implications of recovery-orientated practices, thenexploring how recovery practices are implemented by Club-houses needs to be prioritised. Theoretical frameworks suchas self-determination theory that can guide such exploration,are therefore highly relevant. Research on the way conditionswithin Clubhouses either foster or undermine members’ com-petence, relatedness and autonomy has great potential, becauseit may contribute to knowledge about how service practices andthe design of service environments can optimise the chances ofrecovery and wellbeing.
CONCLUSIONWith the increasing influence of recovery approaches in
mental health, a challenge has been the identification of the-oretical frameworks suitable to guide studies regarding howrecovery practices are implemented in services, such as Club-houses. Frameworks incorporating concepts, including motiva-tion, skills development and supportive relationships need tobe prioritised (Mancini, 2008). Self-determination theory ad-dresses each of these ingredients through the prism of its threecore principles: competency, relatedness and autonomy.
By seeking to highlight the connections between people’spsychological motivation and interaction with their social en-vironment, self-determination theory resonates harmoniouslywith the Clubhouse model. Clubhouse services adopt an in-clusive, collaborative approach that embrace the idea of mentalhealth recovery, as a subjective process, heavily reliant on socialenvironment and supportive relationships. Self-determinationtheory therefore has potential to inform research regarding therole of social environment on the choices and behaviours ofClubhouse members and how recovery practices are imple-mented within Clubhouse services.
Declaration of Interest: The authors report no conflicts ofinterest. The authors alone are responsible for the content andwriting of the paper.
REFERENCESAdamut, A. (2011). Social assistance and transmodernism in Christ’s activity.
European Journal of Science and Theology, 7(4), 9–23.Aglen, B. J., Hedlund, M., & Landstad, B. J. (2011). Self-help and self-help
groups for people with long-lasting health problems or mental health difficul-ties in a Nordic context: A review. Scandinavian Journal of Public Health,39(8), 813–822.
Anderson, S. B. (1998). We are not alone: Fountain House and the developmentof clubhouse culture. New York: Fountain House.
Anthony, W., Rogers, S., & Farkas, M. (2003). Research on evidence-basedpractices: Future directions in an era of recovery. Community Mental HealthJournal, 39(2), 101–114.
Aquila, R., Malamud, T., Sweet, T., & Kelleher, J. (2006). The Store Front, Foun-tain House, and the Rehabilitation Alliance. Medscape General Medicine,8(3), 67.
Australian Government. (2009). Fourth national mental health plan – An agendafor collaborative government action in mental health 2009–2014. Canberra:Author.
25
150 T. RAEBURN ET AL.
Baggett, T. P., O’Connell, J. J., Singer, D. E., & Rigotti, N. A. (2010). The unmethealth care needs of homeless adults: A national study. American Journal ofPublic Health, 100(7), 1326–1333.
Baillargeon, J., Binswanger, I., Penn, J., Williams, B., & Murray, O. (2009).Psychiatric disorders and repeat incarcerations: The revolving prison door.American Journal of Psychiatry, 166(1), 103–109.
Barreira, P., Macias, C., Rodican, C., & Gold, P. B. (2008). Choice of serviceprovider: How consumer self-determination shaped a psychiatric rehabilita-tion program. Psychiatric Rehabilitation Journal, 31(3), 202–210.
Butler, T., Indig, D., Allnutt, S., & Mamoon, H. (2010). Co-occurring mentalillness and substance use disorder among Australian prisoners. Drug andAlcohol Review, 30(2), 188–194.
Carroll, J., Fiscella, K., Epstein, R., Sanders, M., & Williams, G. (2012). A5As communication intervention to promote physical activity in underservedpopulations. BMC Health Services Research, 12(1), 374.
Chirkov, V., Ryan, R. M., Kim, Y., & Kaplan, U. (2003). Differentiating au-tonomy from individualism and independence: A self-determination theoryperspective on internalisation of cultural orientations and well-being. Journalof Personality and Social Psychology, 84(1), 97.
Christiansen, C. (2000). Identity, personal projects and happiness: Self con-struction in everyday action. Journal of Occupational Science, 7(3), 98–107.
Cleary, M., Horsfall, J., O’Hara-Aarons, M., & Hunt, G. (2012). Mental healthnurses’ views of recovery within an acute setting. International Journal ofMental Health Nursing, 22(3), 205–212.
Coniglio, F., D., Hancock, N., & Ellis, A. (2010). Peer support within clubhouse:A grounded theory study. Community Mental Health Journal, 48(2), 153–160.
Conrad, P. & Barker, K. K. (2010). The social construction of illness key insightsand policy implications. Journal of Health and Social Behavior, 51(1), 67–79.
Cook, J., Copeland, M., Floyd, C., Jonikas, J., Hamilton, M., Razzano, L., et al.(2012). A randomized controlled trial of effects of wellness recovery actionplanning on depression, anxiety, and recovery. Psychiatric Services, 63(6),541–547.
Crisp, R. (2000). Aristotle: Nicomachean Ethics. Cambridge: Cambridge Uni-versity Press.
Deci, E., Koestner, R., & Ryan, R. (1999). A meta-analytic review of exper-iments examining the effects of extrinsic rewards on intrinsic motivation.Psychological Bulletin, 125(6), 627–668.
Deci, E. & Ryan, R. (2012). Overview of self-determination theory. Oxford:Oxford University Press.
Deci, E., Ryan, R., Gagne, M., Leone, D., Usunov, J., & Kornazheva, B. (2001).Need satisfaction, motivation, and well-being in the work organisations ofa former eastern bloc country: A cross-cultural study of self-determination.Personality and Social Psychology Bulletin, 27(8), 930–942.
Dudek, K. J. & Aquila, R. (2012). Fountain house and recovery centers. Psy-chiatric Services, 63(4), 396.
Gagne, M. & Deci, E. L. (2005). Self-determination theory and work motivation.Journal of Organizational Behavior, 26(4), 331–362.
Gergen, K. J. (2011). The self as social construction. Psychological Studies,56(1), 108–116.
Gregitis, S., Glacken, J., Julian, C., & Underwood, K. (2010). Comparing work-ing role values of employed and unemployed Clubhouse members. Work,36(1), 39–46.
Hahn, C. (2013). The differences and similarities between classical and operantconditioning. Chicago: Grinn Verlag.
Harvey, S., Modini, M., Christensen, H., & Glozier, N. (2013). Severe mentalillness and work: What can we do to maximise the employment opportuni-ties for individuals with psychosis? Australian and New Zealand Journal ofPsychiatry, 47(5), 421–424.
Herman, S., Onaga, E., Pernice-Duca, F., Oh, S., & Ferguson, C. (2005). Senseof community in Clubhouse programs: Member and staff concepts. AmericanJournal of Community Psychology, 36(3–4), 343–356.
Honderich, T. (2005). The Oxford companion to philosophy. New York: OxfordUniversity Press.
Horsfall, J., Cleary, M., & Hunt, G. E. (2010). Stigma in mental health: Clientsand professionals. Issues in Mental Health Nursing, 31(7), 450–455.
Hungerford, C. & Kench, P. (2013). The perceptions of health professionalsof the implementation of Recovery-oriented health services: A case studyanalysis. Journal of Mental Health Training, Education and Practice, 8(4),5–5.
Hunt, G., Siegfried, N., Morley, K., Sitharthan, T., & Cleary, M. (2013).Psychosocial interventions for people with both severe mental illness andsubstance misuse (Review). Cochrane Database of Systematic Reviews, 10,CD001088.
Huta, V. & Ryan, R. M. (2010). Pursuing pleasure or virtue: The differential andoverlapping well-being benefits of hedonic and eudaimonic motives. Journalof Happiness Studies, 11(6), 735–762.
Jung, S. H. & Kim, H. J. (2012). Perceived stigma and quality of life of individ-uals diagnosed with schizophrenia and receiving psychiatric rehabilitationservices: A comparison between the clubhouse model and a rehabilitationskills training model in South Korea. Psychiatric Rehabilitation Journal,35(6), 460–465.
Kashdan, T. B., Biswas-Diener, R., & King, L. A. (2008). Reconsidering happi-ness: The costs of distinguishing between hedonics and eudaimonia. Journalof Positive Psychology, 3(4), 219–233.
Kasser, T., & Ryan, R. (1996). Further examining the American dream: Dif-ferential correlates of intrinsic and extrinsic goals. Personality and SocialPsychology Bulletin. 22(3), 280–287.
Kosciulek, J. F. & Merz, M. (2001). Structural analysis of the consumer-directedtheory of empowerment. Rehabilitation Counseling Bulletin, 44(4), 209–216.
Lynch, M. F., La Guardia, J. G., & Ryan, R. M. (2009). On being yourself indifferent cultures: Ideal and actual self-concept, autonomy support, and well-being in China, Russia, and the United States. Journal of Positive Psychology,4(4), 290–304.
Mancini, A. (2008). Self-determination theory: A framework for the recoveryparadigm. Advances in Psychiatric Treatment, 14(5), 358–365.
Mandiberg, J. M. & Warner, R. (2013). Is mainstreaming always the answer?The social and economic development of service user communities. ThePsychiatrist, 37(5), 153–155.
Markland, D., Ryan, R. M., Tobin, V. J., & Rollnick, S. (2005). Motivationalinterviewing and self–determination theory. Journal of Social and ClinicalPsychology, 24(6), 811–831.
Mowbray, C., Collins, M., Bellamy, C., & Megivern, D. (2005). Supportededucation for adults with psychiatric disabilities: An innovation for socialwork and psychosocial rehabilitation practice. Social Work, 50(1), 7–20.
Mowbray, C., Megivern, D., & Holter, M. (2003). Supported education pro-gramming for adults with psychiatric disabilities: Results from a nationalsurvey. Psychiatric Rehabilitation Journal, 27(2), 159–167.
Ng, J. Y., Ntoumanis, N., Thøgersen-Ntoumani, C., Deci, E. L., Ryan, R.M., Duda, J. L., et al. (2012). Self-determination theory applied to healthcontexts An meta-analysis. Perspectives on Psychological Science, 7(4),325–340.
Norman, C. (2006). The Fountain House movement, an alternative rehabilitationmodel for people with mental health problems, members’ descriptions of whatworks. Scandinavian Journal of Caring Sciences, 20(2), 184–192.
Pernice-Duca, F. & Onaga, E. (2009). Examining the contribution of social net-work support to the recovery process among clubhouse members. AmericanJournal of Psychiatric Rehabilitation, 12(1), 1–30.
Raeburn, T., Halcomb, E., Walter, G., & Cleary, M. (2013). An overview ofthe clubhouse model of psychiatric rehabilitation. Australasian Psychiatry,21(4), 376–378.
Raeburn, T., Schmied, V., Hungerford, C., & Cleary, M. (2014). Clubhousemodel of psychiatric rehabilitation: How is recovery reflected in documenta-tion? International Journal of Mental Health Nursing, Apr 4, [Epub ahead ofprint].
Ramsay, C. E., Broussard, B., Goulding, S. M., Cristofaro, S., Hall, D., Kaslow,N. J., et al. (2011). Life and treatment goals of individuals hospitalized forfirst-episode nonaffective psychosis. Psychiatry Research, 189(3), 344–348.
Ryan, R. & Deci, E. (2000). Self-determination theory and the facilitation ofintrinsic motivation, social development, and well-being. American Psychol-ogist, 55(1), 68–78.
26
A FRAMEWORK FOR CLUBHOUSE PSYCHOSOCIAL REHABILITATION RESEARCH 151
Ryan, R. & Deci, E. (2001). On happiness and human potentials: A review of re-search on hedonic and eudaimonic well-being. Annual Review of Psychology,52(1), 141–166.
Ryan, R., Patrick, H., Deci, E., & Williams, G. (2008). Facilitating healthbehaviour change and its maintenance: Interventions based on self-determination theory. European Health Psychologist, 10(1), 2–5.
Scheyett, A., McCarthy, E., & Rausch, C. (2006). Consumer and family viewson evidence-based practices and adult mental health services. CommunityMental Health Journal, 42(3), 243–257.
Schiff, J. W., Coleman, H., & Miner, D. (2008). Voluntary participation inrehabilitation: Lessons learned from a clubhouse environment. CanadianJournal of Community Mental Health, 27(1), 65–78.
Sheldon, K. M. (2011). Integrating behavioral-motive and experiential-requirement perspectives on psychological needs: A two process model.Psychological Review, 118(4), 552.
Standage, M., Duda, J. L., & Ntoumanis, N. (2005). A test of self-determinationtheory in school physical education. British Journal of Educational Psychol-ogy, 75(3), 411–433.
Stone, D. N., Deci, E. L., & Ryan, R. M. (2009). Beyond talk: Creating au-tonomous motivation through self-determination theory. Journal of GeneralManagement, 34(3), 75.
VanElzakker, M. B., Dahlgren, M. K., Davis, F. C., Dubois, S., & Shin, L. M.(2013). From Pavlov to PTSD: The extinction of conditioned fear in rodents,humans, and in anxiety disorders. Neurobiology of Learning and Memory,113, 3–18.
Vansteenkiste, M., Zhou, M., Lens, W., & Soenens, B. (2005). Ex-periences of autonomy and control among Chinese learners: Vital-izing or immobilizing? Journal of Educational Psychology, 97(3),468.
Warner, R. (2004). Recovery from schizophrenia: Psychiatry and political econ-omy. London: Psychology Press.
Warner, R. (2010). Does the scientific evidence support the recovery model?The Psychiatrist, 34(1), 3–5.
Williams, P., Barclay, L., & Schmied, V. (2004). Defining social support incontext: A necessary step in improving research, intervention, and practice.Qualitative Health Research, 14(7), 942–960.
27
28
3.3 Conclusion
This chapter has described SDT as a theory of human motivation that
seeks to address the relationship between psychological motivation and
people’s interaction with their social environment. The principle of self-
determination, or people’s entitlement to freedom, social and democratic
rights, has long been cited as fundamental to services efforts to facilitate
mental health recovery. In spite of this, people who live with mental illness
often struggle to experience self-determination.
Psychosocial Clubhouses adopt an inclusive approach to assisting
people towards self-determination that promotes SDT’s three core
principles, competence, relatedness and autonomy. SDT’s focus on the
influence of environmental factors on people’s motivation and behaviour,
makes it well suited to provide a theoretical framework for research within a
psychosocial Clubhouse. In the following chapter the research design that
was adopted to study recovery oriented practice within a psychosocial
Clubhouse will be discussed.
29
CHAPTER 4: CASE STUDY DESIGN
4.1 Introduction
As described in previous chapters, Clubhouses are accessed by adults with
a history of mental illness who have often experienced marginalisation and
stigma (Jung & Kim, 2012). Exploring phenomena in such contexts,
requires a study design that can enable in depth, but sensitive and
respectful research to be undertaken. One common approach capable of
meeting such challenges is case study design (Yin, 2009).
This chapter provides an overview of case study design and considers
its suitability for psychosocial Clubhouse research. A description of case
study design is provided. Concepts related to the advantages and
disadvantages of case studies are discussed, drawing on a series of
examples from previous research involving Clubhouses. Finally,
considerations for applying quality case study design in Clubhouse settings
are outlined, in an effort to promote future research in this field.
4.2 Publication
The following is from:
Raeburn, T., Schmied, V., Hungerford, C., Cleary, M. (2015). The
contribution of case study design to supporting research on Clubhouse
psychosocial rehabilitation. BMC Research Notes, 8 (1), 521.
Raeburn et al. BMC Res Notes (2015) 8:521 DOI 10.1186/s13104-015-1521-1
RESEARCH ARTICLE
The contribution of case study design to supporting research on Clubhouse psychosocial rehabilitationToby Raeburn1*, Virginia Schmied1, Catherine Hungerford2 and Michelle Cleary1
Abstract
Background: Psychosocial Clubhouses provide recovery-focused psychosocial rehabilitation to people with serious mental illness at over 300 sites in more than 30 countries worldwide. To deliver the services involved, Clubhouses employ a complex mix of theory, programs and relationships, with this complexity presenting a number of challenges to those undertaking Clubhouse research. This paper provides an overview of the usefulness of case study designs for Clubhouse researchers; and suggests ways in which the evaluation of Clubhouse models can be facilitated.
Results: The paper begins by providing a brief explanation of the Clubhouse model of psychosocial rehabilitation, and the need for ongoing evaluation of the services delivered. This explanation is followed by an introduction to case study design, with consideration given to the way in which case studies have been used in past Clubhouse research. It is posited that case study design provides a methodological framework that supports the analysis of either quan-titative, qualitative or a mixture of both types of data to investigate complex phenomena in their everyday contexts, and thereby support the development of theory. As such, case study approaches to research are well suited to the Clubhouse environment. The paper concludes with recommendations for future Clubhouse researchers who choose to employ a case study design.
Conclusions: While the quality of case study research that explores Clubhouses has been variable in the past, if applied in a diligent manner, case study design has a valuable contribution to make in future Clubhouse research.
Keywords: Case study, Clubhouse, Design, Mental health, Recovery, Research
BackgroundEstablished towards the end of the 1940′s, the Clubhouse model is one of the world’s oldest approaches to psycho-social rehabilitation [1]. Popular worldwide, there are currently over 300 Clubhouses operating in more than 30 countries [2]. People who attend Clubhouses typically have a history of serious mental illness and face a num-ber of challenges, including those related to their physical health, social welfare and employment [3]. In response, Clubhouses provide a wide range of social, health, educa-tional and employment support programs [2]. To encour-age a sense of empowerment and belonging, participants
in these programs are referred to as ‘members’ rather than ‘patients’ or ‘consumers’ [4].
Clubhouse members follow an activity schedule referred to as the ‘work ordered day’ [5], where they work alongside paid staff, often assuming lead roles and taking responsibility for all aspects involved in running the Clubhouse. By contributing in these proactive ways, members embrace opportunities to build confidence, friendships and skills, while also being encouraged to pursue educational and employment goals in the wider society [6]. Building on these activities, Clubhouse pro-grams referred to as Transitional Employment Programs (TEP) are then tailored to support members who decide to seek work in the competitive job market [6].
Clubhouses have been at the forefront of advocacy for consumer centred, recovery-oriented practice [7, 8].
Open Access
*Correspondence: [email protected] 1 School of Nursing and Midwifery, Western Sydney University, Locked Bag 1797, Penrith, NSW 2751, AustraliaFull list of author information is available at the end of the article
Page 2 of 7Raeburn et al. BMC Res Notes (2015) 8:521
Despite this, researching the complex nature of these ser-vices has proved challenging [9, 10]. Clubhouse research is further complicated by the highly personalised and context-dependent ways that people experience mental health recovery [11]. Reflection on such challenges has led to long consideration of the research design that best supports the exploration and explanation of the way in which Clubhouses work to support recovery—that is, the ‘recovery orientation’ of the Clubhouse model [12]. One research method with the potential to provide a rigorous framework for exploring phenomena within organisa-tions such as the Clubhouse is case study design [13, 14].
Case study design typically uses multiple perspectives to facilitate the examination of a particular phenomenon in its natural context [15, 16]. While this may sound simi-lar to the goal of many qualitative research approaches, case study design is different because it can be flexibly adapted as a framework that incorporates either quali-tative, quantitative or a mixture of qualitative and quan-titative research approaches [13]. Case study design is also unconstrained by a particular theoretical approach, meaning it can be pragmatically informed by or used to build or critique any theory related to the phenomena in question [17].
According to Tight [18], publications on the topic of case study from the past decade have been dominated by the work of two leading theorists, Yin [16] and Stake [19]. Yin [16] divides case studies into two broad groups. First, those that focus on an individual case, involving detailed exploration of either a person or an organisation. These are referred to as a ‘single case study’. Second, those that involve investigation of a group of cases for comparison and contrast are referred to as ‘multiple case studies’. Yin then makes a further division, categorising each case study as either exploratory, descriptive or explanatory.
Exploratory case studies are commonly pilot projects that seek to reveal what phenomena or theory exists within a field of interest. For example, a researcher inter-ested in how services assist people with mental illness to achieve recovery, may seek to discover if there are any guiding recovery principals used by mental health ser-vices. Such a study may uncover phenomena and/or the-ory that can then lead to further investigation.
In contrast, descriptive case studies begin with a theory about a phenomena, and then seek to chronicle how the phenomena is displayed through the lens of those theoretical assumptions. For example, a descrip-tive study may set out to elucidate how certain recovery principles are reflected in the practices of a Clubhouse. A risk with this type of case study is that the researcher may find that the theory brought to the project is not applicable which, in turn, may lead to the need for fur-ther exploratory work.
Finally, explanatory case studies seek to interpret why a particular phenomenon or theory has been revealed in the data. This approach is cited as being particularly useful in a multiple case study design, because pattern-matching can be used. For example, a study may seek to explain why work seems to be important to the reha-bilitation of people with mental illness at three different Clubhouses located across a variety of cultural contexts [16].
For Stake [19], case study design is focused on the exploration of a case and refining or revealing related concepts. Stake [19] divides case studies into intrin-sic, instrumental or collective designs. Intrinsic design is used when researchers have a particular interest in improving their understanding of a phenomenon. This method is described as being primarily aimed at explor-ing rather than understanding theoretical constructs. In contrast, instrumental design refers to those case studies that seek to elucidate phenomena and test or strengthen theory. With this approach, the case and its context are studied in depth to facilitate deep understanding of a concept. Finally, collective case studies include any study involving more than one case, similar to Yin’s [16] description of ‘multiple case design’.
Consideration of the explanations provided by Yin [16] and Stake [19] suggest that case study may be described as a flexible research design that may uti-lize either qualitative, quantitative or a mixture of both types of data, to illuminate, elucidate or interpret phenomena in their everyday context and support the development of theory. This definition is important in this paper because it provides a framework for consider-ing case study design in relation to Clubhouse research. For example, while several studies have described peo-ple’s subjective experience of recovery in psychoso-cial Clubhouses [11], there has been limited research exploring the way Clubhouses implement recovery-ori-ented practices. In this paper we review how case study research has contributed to the field of Clubhouse psy-chosocial rehabilitation.
MethodInitially, this paper was conceived as an integrative litera-ture review that examined the published case studies that have contributed to Clubhouse research. An electronic literature search was conducted seeking to identify full text peer reviewed journal articles written in English and published between 1960 and January 2015. The papers were required to refer to themselves as a ‘case study’ or derivative, and to have a focus on a Clubhouse or Fountain House. The search term ‘Fountain House’ was included because, as the name of the original Clubhouse, this term is popular in Clubhouse related literature.
31
Page 3 of 7Raeburn et al. BMC Res Notes (2015) 8:521
The search terms, “case stud*” AND “clubhouse” OR “fountain house” were combined across three databases, leading to initial identification of 41 papers from Psy-cINFO, 20 from CINAHL and 16 from Proquest Social Science Journals. Reference lists were checked for other relevant papers, then following article screening and removal of duplicates, five papers were identified as rel-evant to the review [20–24]. All based in North America, the five articles were all published more than a decade ago, with one published as early as 1960.
The quality of each paper was initially assessed by the Chief Investigator (TR), using the Critical Skills Appraisal Program (CASP) [25]. CASP posits there are three broad issues that should be considered when appraising qualita-tive research, these are;
• Are study results valid? • What are the results? • Will the results help locally? [25]
A ten question, three point scale was used to assess for validity, results and relevance. CASP ratings and notes were reviewed by all authors. The assessment was prob-lematic however, as the majority of papers identified had been published in an era when diligent approaches to case study research and reporting (such as ethics approval) were often not applied. The consensus view amongst the authors was that this small sample of case studies could not bear the scrutiny of modern analytical techniques as part of an integrative literature review. Despite this, the results did provide useful information regarding the use of case study design in Clubhouse research, including the advantages and disadvantages. In turn, this prompts a variety of considerations for researchers who may con-sider using case study design in Clubhouse settings in future, with these considerations outlined in the results and discussion section presented below.
Results and discussionAdvantages and disadvantages of case study design in Clubhouse researchIn common with qualitative research approaches such as ethnography, an emphasis on studying phenomena in its natural context means case study design incorporates the perspectives of participants who may come from vulner-able and voiceless groups in society [26]. For this reason, case studies have often been used to provide a framework to critique oppression and question social norms [27]. This suggestion was exemplified in the earliest evidence of a published Clubhouse case study, a paper by Goertzel et al. [22] published in 1960 that described the original Clubhouse in New York City during its early development. Using multiple data sources, the paper provided a rich
description of the theoretical orientation, history, facili-ties, staff, volunteers, membership and programs available [22]. The research is important because it was written in an era when society held stigmatizing attitudes towards people with serious mental illness, who often spent their lives in custodial psychiatric institutions [28, 29]. The paper by Goertzel et al. [22] conveyed ideas ahead of its time regarding the importance of involving people with a lived experience of mental illness in the development and delivery of mental health services. This case study, then, provides evidence of the early role that Clubhouses played in advocating for recovery-oriented models of mental health care.
Another advantage of case study design is the way in which it can be flexibly adapted to incorporate a mixture of qualitative and quantitative methods, as promoted by researchers such as Creswell [26, 30]. An example of a mixed methods case study was conducted by Boll [20], who undertook a case study of a Clubhouse in New Jersey to explore the phenomena of empowerment among Club-house members involved in a service evaluation. Using a combination of quantitative and qualitative data collec-tion methods, including survey questionnaires, participant observation, and individual interviews, the study found that researching Clubhouse members within the regular Clubhouse environment led to benefits such as enhanced engagement with new members and improved program quality [20].
A final advantage of undertaking case study research relates to the way in which it can support the testing of connections between theory and phenomena [31]. This characteristic was demonstrated in a Clubhouse case study conducted by Cowell et al. [24]. The study explored the concept of ‘function cost’, a theory designed to explain the financial cost to services that utilize co-pro-duction, where consumers are involved in both delivery and receipt of services. The boundaries in the study were difficult to ascertain because Clubhouse members were involved in the provision of tasks normally delivered by paid staff in hospital-based services. The research-ers addressed this dilemma pragmatically by using two standardised research scales to collect separate financial data about costs associated with paid staff and voluntary labour invested in activities. Results from the study sug-gested that the concept of ‘function cost’ may provide a way to explain the financial costs of Clubhouse programs utilising co-production practices [24].
As is evident from the above examples drawn from Clubhouse research, there is no standardised way to apply case study design. Instead, this flexible approach offers researchers the opportunity to select from a vari-ety of methods and data collection techniques to ensure a ‘best fit’ for the case in question. As with any style of
32
Page 4 of 7Raeburn et al. BMC Res Notes (2015) 8:521
research however, case study design also has some disadvantages.
One of the most commonly cited disadvantages of case studies is that findings can lack generalizability [15, 16]. This suggestion, along with arguments that case studies lack scientific credibility because replication is difficult, has led to research regulators such as Australia’s National Health and Medical Research Council (NHMRC) [32] ranking case study as the lowest form of credible research design. Following scientific convention, the NHMRC [32] has ranked the quality of the designs of research, with some designs posited as producing more rigorous evi-dence than other research designs. For example when evaluating the effectiveness of an intervention, a Ran-domised Controlled Trial (RCT) is regarded as providing the most reliable evidence [33].
The NHMRC [32] suggests that the processes inte-gral to RCTs minimize the risk of confounding factors and highlight that internal validity is generally stronger in randomized control trials. However external validity can be stronger in multiple case study designs, and can be weak in randomized control trials. Such weaknesses in RCT design have been exposed in a number of systematic reviews and secondary analyses. For example, Hunt, Sieg-fried, Morley, Sitharthan and Cleary [34] completed a Cochrane review of psychosocial interventions for people with serious mental illness examining 32 RCTs. Contrary to the view that RCTs provide a rigorous, dependable research design, the authors reported substantial difficul-ties with skewed data, risk of bias, poor trial methods, small sample sizes, low event rates and wide confidence intervals [34]. In another example related to Clubhouse employment programs, Johnsen et al. [35] conducted a secondary analysis of a multisite RCT and found that a limited definition of ‘competitive employment’ and vari-ability in ‘control’ conditions, across sites, led to skewed findings. Johnsen et al. [35, 36] together with other researchers, have gone on to observe that these kinds of variation in definition and control conditions in RCTs have led to substantial inconsistencies in research of employment services for people with serious mental illness.
Responding to criticism of case study design, theo-rists such as Yin [16] have suggested that generalisation of findings from case studies should focus on assess-ing the efficacy of theoretical constructs, rather than on the transferability of statistics. As mentioned previously, such a focus on theoretical concepts was exemplified in a case study by Cowell et al. [24], which explored the use-fulness of the ‘function cost’ concept. Stake [19] has also argued that case study findings can be transferable, but from a different point of view. He suggests that readers can normally relate to the findings of case studies, which
facilitate a kind of generalised understanding of phenom-ena [19]. For example, Jacobs used a case study design to provide an illuminating description of the challenges associated with improving access to psychiatry for mem-bers at a Clubhouse [23].
In contrast to his strong advocacy for the efficacy of case study design, one disadvantage observed by Yin [37] is that case study researchers can lack discipline, sometimes allowing detailed description and illustra-tive quotes to dominate findings. According to Yin, this is often at the expense of detailed accounts of research design procedures such as ethics, data collection and analytic procedures. An interesting technical point con-sistent across the five papers identified in this review was the lack of clarity regarding ethics and consent [20–24]. For example, Asmussen et al. [21] completed an inter-esting case study of a Clubhouse outreach program for homeless people, but failed to include any reference to ethical considerations.
In an effort to promote quality case study research, the-orists such as Feagin [38], Yin [16] and Stake [39] have sought to develop protocols and structures for applying case studies. The following section will outline some con-siderations for effective application of case study design in future Clubhouse research.
Considerations for conducting case studies in Clubhouse settingsAssuming that a research question has been identified and that the researchers’ choice of case study design is driven by a desire to explore a phenomenon in depth in its everyday context, the next logical step is to iden-tify whether the case best fits a single or multiple case design [16]. Single-case design may be a suitable choice if the case displays particular uniqueness—for example, a study into the unique cultural experience of needing to ‘save face’ experienced by members of a Hong Kong Clubhouse [40]; or the development of an innovative program integrating a psychiatry clinic into a Club-house [41]. A single case approach may also be useful for a study that has limited time and access to resources, such as a student undertaking higher degree studies that involve a research project. It is important at the outset that the researcher is clear about how findings will be analysed, and compared to or tested against a theoretical paradigm [19].
Alternatively, multiple-case design may work well in situations where there are several similar cases that can provide pathways for replication and comparison [39]. Replicating a case study in this way would then present the opportunity for pattern-matching, a technique that links several pieces of information from the same case to a theoretical proposition, thereby enhancing the rigour of
33
Page 5 of 7Raeburn et al. BMC Res Notes (2015) 8:521
findings and generalizability of theory [42]. For example, research providing theoretical observations about the Clubhouse’s supported employment programs might be strengthened by using a multiple case study design that includes Clubhouses of different sizes across a variety of cultures. This could then potentially enable generalisa-tion of findings to the Clubhouse model as a whole.
Following the identification of whether a single or multiple case study is best suited to a research question, Yin [16] contends that a structured approach to design should be taken to ensure quality and exploratory power in case study research. He suggests that case study design should include:
• An overview of the case study project citing objec-tives, issues and background.
• Written field procedures describing research location and access to data.
• Identification of research questions to be focused on during data collection.
• A reporting guide outlining a general format for the report.
By employing such points as a guide, then, research-ers will support consistency across case study research undertaken in a Clubhouse context.
Common data sources include but are not limited to, documentation, archival records, interviews, direct observation, participant observation and physical objects [16]. While no individual source should be consid-ered better than another, the rationale for using several sources of data is the triangulation of evidence. Triangu-lation provides checks and balances for the reliability of data collection [43]. For example, data drawn from par-ticipant observation and interviews could be used to cor-roborate the meaning and application of data revealed through review of a Clubhouse’s documentation.
Conducting research in any service for people living with mental illness requires special sensitivity [44]. To encourage empowerment and guard against any poten-tial harm to participants the Clubhouse model has a strong commitment to the co-production of research with members regularly encouraged to ask questions and share points of view [45]. With this in mind, a collabora-tive approach should be planned, actioned and reflected upon when conducting any Clubhouse case study.
A further consideration is promoting quality men-tal health research. People with serious mental illness often experience stigma and marginalization, and so it is important that research does not perpetuate this [44]. Developing a strong evidence base is crucial how-ever, and within fields of mental health research there is robust debate regarding the merits and weaknesses of
the different research paradigms [44]. Regardless of what approach is taken, consumers must be positioned at the centre of any mental health research—and genuine con-sultation with stakeholders is essential, including respect-ful processes, as well as ethical behaviours and practices, to ensure that research contributes to the nature, quality and the validity of the data gained [46].
Evaluation of case study designs may be conducted in a number of ways. As mentioned previously, the CASP [25] provides a ten point tool for systematic consid-eration of study design, results, validity and relevance. Alternatively, Popay’s [47] method of appraisal places a high value on studies that validate the expertise of consumers of healthcare and the theoretical general-izability of findings. Using this appraisal method, the research is rated as ‘thin’ if there is little consideration of consumer insights, limited explanation, and low rel-evance for generalization. On the other hand, studies are considered ‘thick’ if they lend weight to consumer descriptions, including detailed description of phenom-ena; and show potential for generalizability [48]. Much of the data found in older Clubhouse research, struggles to find relevance when tools like CASP [25] and Popay’s [47] approach are applied. While this does not diminish the value of early research, as the Clubhouse model con-tinues to evolve, appraisal tools may provide substantial benefit for evaluating and improving the quality of mod-ern Clubhouse case studies.
ConclusionPsychosocial Clubhouses serve some of the most vulner-able and marginalised people in society. The Clubhouse model has become an internationally regarded provider of consumer-centred recovery-focused psychosocial rehabilitation [7, 11, 49]. With these considerations in mind, there is high need for research designs capable of exploring and describing how Clubhouses implement recovery practices.
This paper has identified case study design as a flex-ible research design that may utilize either qualitative, quantitative or a mixture of both types of data, to illu-minate, elucidate or interpret phenomena in their every-day context and support the development of theory. As health science continues to evolve, case study design can provide a flexible framework for exploring the complex challenges presented by multidimensional mental health services like Clubhouses. Case study design enables con-sumers to play a central role in the development, imple-mentation, analysis and synthesis of research. It also supports the conduct of genuine consultation with stake-holders, including respectful processes, ethical behav-iours and practices to ensure the quality and validity of data gained.
34
Page 6 of 7Raeburn et al. BMC Res Notes (2015) 8:521
AbbreviationsCASP: Critical Skills Appraisal Program; NHMRC: Australia’s National Health and Medical Research Council; RCT: randomised controlled trial.
Authors’ contributionsThe authors have confirmed that all authors meet the ICMJE criteria for authorship credit (http://www.icmje.org/recommendations/browse/roles-and-responsibilities/defining-the-role-of-authors-and-contributors.html), as follows: (1) substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; (2) drafting the article or revising it critically for important intellectual content; and (3) final approval of the version to be published. All authors were involved in the development of the paper.TR drafted the initial manuscript. MC, VC and CH were also involved in manuscript revisions and supervision. All authors read and approved the final manuscript.
Author details1 School of Nursing and Midwifery, Western Sydney University, Locked Bag 1797, Penrith, NSW 2751, Australia. 2 School of Nursing, Midwifery, and Indig-enous Health, Faculty of Science, Charles Sturt University, Wagga Wagga, NSW, Australia.
AcknowledgementsThere was no funding source and there are nil applicable funding or acknowl-edgements for this discussion paper outside of the authors contributions.
Compliance with ethical guidelines
Competing interestsThe authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Received: 17 August 2014 Accepted: 21 September 2015
References 1. Drake R, Green A, Mueser K, Goldman H. The history of community men-
tal health treatment and rehabilitation for persons with severe mental illness. Community Ment Health J. 2003;39(5):427–40.
2. Coniglio FD, Hancock N, Ellis A. Peer support within clubhouse: a grounded theory study. Community Ment Health J. 2010;48(2):153–60.
3. McKay C. Health promotion in clubhouse programs: needs, barriers, and current and planned activities. Psychiatr Rehabil J. 2007;31(2):155–9.
4. Boyd AS, Bentley KJ. The relationship between the level of personal empowerment and quality of life among psychosocial clubhouse mem-bers and consumer-operated drop-in center participants. Soc Work Ment Health. 2005;4(2):67–93.
5. Magaw K. The vocational development functions of the clubhouse. New York: Springer; 2004.
6. Macias C, Rodican C, Hargreaves W, Jones D, Barreira P, Wang Q. Sup-ported employment outcomes of a randomized controlled trial of ACT and clubhouse models. Psychiatr Serv. 2006;57(10):1406–15.
7. Dudek KJ, Aquila R. Fountain house and recovery centers. Psychiatr Serv. 2012;63(4):396.
8. Pernice-Duca F, Onaga E. Examining the contribution of social network support to the recovery process among clubhouse members. Am J Psychiatr Rehabil. 2009;12(1):1–30.
9. Kightley M, Einfeld S, Hancock N. Routine outcome measurement in mental health: feasibility for examining effectiveness of an NGO. Australas Psychiatr. 2010;18(2):167–9.
10. Raeburn T, Halcomb E, Walter G, Cleary M. An overview of the clubhouse model of psychiatric rehabilitation. Australas Psychiatr. 2013;21(4):376–8.
11. Hancock N, Bundy A, Honey A, James G, Tamsett S. Improving measure-ment properties of the recovery assessment scale with rasch analysis. Am J Occup Ther. 2011;65(6):77–85.
12. Burgess P, Pirkis J, Coombs T, Rosen A. Assessing the value of existing recovery measures for routine use in Australian mental health services. Aust N Z J Psychiatry. 2011;45(4):267–80.
13. Luck L, Jackson D, Usher K. Case study: a bridge across the paradigms. Nurs Inq. 2006;13(2):103–9.
14. Hungerford C, Kench P. The perceptions of health professionals of the implementation of Recovery-oriented health services: a case study analy-sis. J Ment Health Train Educ Pract. 2013;8(4):5.
15. Zainal Z. Case study as a research method. J Kemanus. 2007;9:1–6. 16. Yin R. Case study research: design and methods, vol. 5. Fourth ed. Thou-
sand Oaks: Sage; 2009. 17. Eisenhardt KM, Graebner ME. Theory building from cases: opportunities
and challenges. Acad Manag J. 2007;50(1):25–32. 18. Tight M. The curious case of case study: a viewpoint. Int J Soc Res Meth-
odol. 2010;13(4):329–39. 19. Stake RE. The art of case study research. Thousand Oaks: Sage; 1995. 20. Boll J. Member roles in program evaluation: a case study from a psycho-
social clubhouse. Psychiatr Rehabil J. 1995;19(1):79–82. 21. Asmussen SM, Romano J, Beatty P, Gasarch L, Shaughnessey S. Old
answers for today’s problems: integrating individuals who are homeless with mental illness into existing community-based programs: a case study of Fountain House. Psychosoc Rehabil J. 1994;18(1):75.
22. Goertzel V, Beard JH, Pilnick S. Fountain House Foundation: case study of an expatient’s club. J Soc Issues. 1960;16(2):54–61.
23. Jacobs S, Davidson L, Steiner J, Hoge M. The integration of treatment and rehabilitation in psychiatric practice and services: a case study of a community mental health center. Community Ment Health J. 2002;38(1):73–81.
24. Cowell A, Pollio D, North C, Stewart A, McCabe M. Deriving service costs for a clubhouse psychosocial rehabilitation program. Adm Policy Ment Health Ment Health Serv Res. 2003;30(4):323–40.
26. Silverman D. Doing qualitative research: a practical handbook. London: SAGE Publications Limited; 2013.
27. Tellis W. Application of a case study methodology. Qual Rep. 1997;3(3):1–17.
28. Geller JL. The last half-century of psychiatric services as reflected in psychiatric services. Psychiatr Serv. 2000;51(1):41–67.
29. Porter R. The greatest benefit to mankind: a medical history of humanity. London: WW Norton & Company; 1999.
30. Creswell JW. Research design: qualitative, quantitative, and mixed meth-ods approaches. London: Sage Publications; 2008.
31. Gomm R, Hammersley M, Foster P. Case study method: key issues, key texts. London: Sage; 2000.
32. NHMRC. Australian code for the responsible conduct of research. Can-berra: National Health Medical Research Council; 2007.
33. Evans D. Hierarchy of evidence: a framework for ranking evidence evalu-ating healthcare interventions. J Clin Nurs. 2003;12(1):77–84.
34. Hunt G, Siegfried N, Morley K, Sitharthan T, Cleary M. Psychosocial interventions for people with both severe mental illness and substance misuse (Review). Cochrane Database Syst Rev. 2013;2013:10.
35. Johnsen M, McKay C, Henry AD, Manning TD. What does competitive employment mean? A secondary analysis of employment approaches in the Massachusetts Employment Intervention Demonstration Project. Res Community Ment Health. 2004;13:43–62.
36. Salkever DS. Policy priorities and shifting sands in the supported employ-ment evidence base. Psychiatry Online. 2006;57(10):1440.
37. Yin R. The case study crisis: some answers. Adm Sci Q. 1981;26(1):58–65. 38. Feagin JR, Orum AM. A case for the case study. Wilmington: UNC Press;
1991. 39. Stake RE. Multiple case study analysis. New York: Guilford Press; 2013. 40. Wong KF. Implementation of Clubhouse model programme: perception
of mental health nurses. J Psychiatr Ment Health Nurs. 2010;17(8):750–3. 41. Aquila R, Santos G, Malamud T, McCrory D. The rehabilitation alliance in
practice: the clubhouse connection. Psychiatr Rehabil J. 1999;23(1):19–23. 42. Denzin NK, Lincoln Y. Qualitative research. Thousand Oaks: Sage; 2000. 43. Bergen A, While A. A case for case studies: exploring the use of case study
design in community nursing research. J Adv Nurs. 2000;31(4):926–34. 44. Horsfall J, Cleary M, Walter G, Malins G. Challenging conventional practice:
placing consumers at the centre of the research enterprise. Issues Ment Health Nurs. 2007;28(11):1201–13.
45. Mowbray C, Lewandowski L, Holter M, Bybee D. The clubhouse as an empowering setting. Health Soc Work. 2006;31(3):167–79.
Page 7 of 7Raeburn et al. BMC Res Notes (2015) 8:521
46. Cleary M, Escott P, Horsfall J, Walter G, Jackson D. Qualitative research: the optimal scholarly means of understanding the patient experience. Issues Ment Health Nurs. 2014;35(11):902–4.
47. Popay J, Rogers A, Williams G. Rationale and standards for the systematic review of qualitative literature in health services research. Qual Health Res. 1998;8(3):341–51.
48. Noyes J, Popay J. Directly observed therapy and tuberculosis: how can a systematic review of qualitative research contribute to improving services? A qualitative meta-synthesis. J Adv Nurs. 2007;57(3):227–43.
49. Warner R. Does the scientific evidence support the recovery model? Psychiatrist. 2010;34(1):3–5.
Submit your next manuscript to BioMed Centraland take full advantage of:
• Convenient online submission
• Thorough peer review
• No space constraints or color figure charges
• Immediate publication on acceptance
• Inclusion in PubMed, CAS, Scopus and Google Scholar
• Research which is freely available for redistribution
Submit your manuscript at www.biomedcentral.com/submit
36
37
4.3 Conclusion
Case study design is a research approach that can be especially useful in
situations where boundaries between a phenomenon and its context are
unclear. This consideration is relevant when researching psychosocial
Clubhouses because they have a high reliance on the involvement of
people with lived experience of mental illness, who work in partnership with
staff, to deliver a wide range of interconnected programs. Past examples of
case studies reviewed in this chapter, have used designs of varying quality
to explore and explain a variety of phenomena within Clubhouses.
Overall, case study design is highly relevant to Clubhouse research,
as long as thorough technical and theoretical considerations such as
design, data collection and context are taken into account. When applied in
a disciplined way, case study design has the potential to facilitate
understanding of practices within Clubhouses and may also be useful for
testing and developing theory. The next chapter will describe the methods
used to conduct this case study.
38
CHAPTER 5: METHODS
5.1 Introduction
The opening chapter outlined the modern concept of mental health
recovery as a highly personal process, often influenced by social context. It
also provided a brief historical sketch of the origins of the Clubhouse
model. In chapter 2 an overview of the Clubhouse model and its core
programs, the work ordered day, transitional employment support and
supported employment was provided. The relevance of such programs to
recovery, were considered in relation to a case vignette. Chapter 3
provided a description of self-determination theory (SDT) (Deci and Ryan,
2012), outlining its philosophical background and potential as a theoretical
framework for Clubhouse research. In chapter 4 the value of qualitative
case study design was addressed (Stake, 1995; Yin, 2009). Strengths and
weaknesses of case study design in Clubhouse research were identified
and important issues for future case studies to consider were highlighted.
This chapter begins by identifying the questions researched in this
study. A brief review of the theoretical framework provided by SDT,
precedes a concise description of qualitative case study design. Important
ethical considerations for working with people who have a lived experience
of mental illness are addressed, followed by a description of the two
phases of data collection and analyses.
In phase 1, a documentation review using directed qualitative content
analysis was undertaken, investigating how recovery practices were
represented in documentation (reported in Chapter 6). Phase 2 involved
39
participant observation focused on staff behavior, and interviews which
gathered the perceptions of Clubhouse members and staff. Phase two data
were assessed using theoretical thematic analyses (reported in Chapters 7
and 8). Whether studying documentation, behaviours and perceptions
within the Clubhouse, qualitative methods facilitated collection and
analyses of rich, detailed information that elucidated how recovery
practices were implemented.
As the overview of the Clubhouse model in chapter 2 outlined,
psychosocial Clubhouse’s provide a wide variety of employment, education
and social programs. This meant the study had potential to be extremely
broad. It was therefore important to focus the research questions, so that
the study would not lose depth.
5.2 Research questions
The central research question this study sought to address was: How does
a psychosocial Clubhouse implement practices that promote recovery from
mental illness?
Specifically, the study explored the following three sub questions:
a. How are recovery practices reflected in the documentation of a
Clubhouse?
b. How are recovery practices embodied in the behaviours of staff
within a Clubhouse?
c. How are recovery practices perceived as being implemented by staff
and members within a Clubhouse?
40
5.3 Self-determination theory
As previously discussed in chapter 3, SDT (Deci & Ryan, 2012), has strong
potential to inform recovery-oriented research (Mancini, 2008). SDT
postulates that humanity not only has physical needs, such as water, food
and shelter, but also has three fundamental psychological needs.
According to SDT these psychological needs are: autonomy, which refers
to people’s need for a sense of freedom and choice; competency, which is
described as the desire to contribute to society; and relatedness, which
refers to the need for supportive relationships (Deci & Ryan, 2012). With its
focus on the connections between peoples psychological wellbeing and
their environment, SDT is well suited as a framework for psychosocial
Clubhouse research.
5.4 Research design
Case study design (Chapter 4), is a commonly used strategy for exploring
phenomena within organisations (Luck, Jackson, & Usher, 2006). Drawing
on a variety of data sources, case studies have been used to explore
services of varying size and complexity, ranging from small groups through
to multi-site organisations or even whole communities (Gerring, 2004).
Case studies tend to be pragmatic in their approach, commonly adapting
data collection methods to suit the research question and context of the
case (Verschuren, 2003).
As discussed in detail in Chapter 4, using multiple sources of
information is essential for conducting a reliable case study. Yin (2009)
describes six commonly used case study data sources including,
41
documentation, archival records, interviews, direct observation, participant
observation, and physical artefacts. Of these sources, this case study used
three: documentation, interviews and participant observation. Each source
was chosen due to its ability to provide a different angle or perspective,
regarding how recovery practices were implemented within the Clubhouse.
Another important consideration was the accessibility of sources, this was
negotiated through a two phase process between the researcher and the
Clubhouse involved institutional and individual consent (see sections 5.8
and 5.9). All data were collected from within the natural, everyday
environment of the Clubhouse. A description of the setting is outlined
below.
5.5 Setting
The case study took place at a Clubhouse located in a metropolitan suburb
of Australia. Housed in an open plan building, the Clubhouse employs a
team of six staff, who work with twenty-sixty Clubhouse members per day.
Open during business hours, programs run from 0900hrs-1700hrs, five
days per week, with occasional social and health promotion programs
scheduled on evenings and weekends. Access to membership of the
Clubhouse is open to anyone over the age of eighteen, with a history of
mental illness. Engagement in all activities is free of charge, funded by a
mixture of government grants, philanthropic foundations and private
donations.
Programs include educational, social and vocational work activities
that facilitate member’s involvement in all tasks required to run the
42
Clubhouse. Regular activities include but are not limited to, administration,
meal preparation, building and garden maintenance, website development,
writing health promotion material and grant applications.
5.6 Ethics
The Clubhouse model has a strong commitment to the involvement of
Clubhouse members in research (Mowbray, Lewandowski, Holter, &
Bybee, 2006). Members are regularly encouraged to ask questions and
share points of view. In response to this inclusive concept, the researcher
consulted closely with the Clubhouse director, staff and members, in order
to ensure that all research activity was conducted in ways that respectfully
aligned with Clubhouse expectations of member involvement (Horsfall,
Cleary, Walter, & Hunt, 2007; Mowbray et al., 2006).
5.6.1 University ethics approvals
Prior to commencement of data collection, two separate human research
ethics approvals were secured from Western Sydney University. The first,
for the documentation review, was secured in 2013 (University ethics
approval number H10375, see appendix 1). The second, for participant
observation and interviews, was approved in 2014 (University approval
number H10711, see appendix 2).
5.6.2 Data storage, management and confidentiality
The study followed guidelines outlined in the Australian Code for the
Responsible Conduct of Research (NHMRC, 2007). All data were coded,
de-identified, and only pseudonyms used in presentation of findings. All
study data has been stored in locked filing cabinets and identifying
43
information is kept separately from coded data. Information will be stored
for a period of five years following publication of findings, at that time
electronic files will be permanently destroyed and paper copies shredded.
5.6.3 Vulnerable population considerations
Conducting ethical research among people with lived experience of mental
illness, such as members of a Clubhouse, requires special sensitivity,
because people with mental illness have often been treated in
disempowering and stigmatising ways (Schomerus et al., 2012). With this
in mind, all study information sheets and consent forms were written in
clear and simple language (See appendix 4) and the option of withdrawal
from the study at any time, without penalty or adverse consequences, was
clearly stated.
Care was also taken to conduct interviews in a sensitive and
respectful manner. The use of interviews for research, has the potential to
prompt study participants to revisit memories and express perspectives that
may have a powerful experience, running the risk of threatening their
wellbeing (Patton, 2005). This is because, as memories are recalled, their
attributed meaning may be distressing, although likely no more distressing
than talking about these experiences with peers. On the other hand, the
interview process had the potential to have a beneficial effect for
participants, by providing opportunity for them to reflect critically on their
experiences (Liamputtong, 2006).
Given the potential for discomfort during interviews, participants were
provided with choice of a safe, private room either inside or outside the
44
Clubhouse, and an empathetic, supportive approach was offered. As
mentioned above, the option of withdrawal from the study, at any time
without penalty or adverse consequences was made clear. Additionally, the
Clubhouse director offered to assist with facilitating debriefing for any
participants who required assistance. No participants reported any
concerns and there were no adverse incidents identified or reported.
5.7 Data types
In this study, data collection took place in two phases, requiring two
separate institutional consents from the Clubhouse (Appendix 3 and 6).
Each phase connected to different questions and types of information.
Phase 1 addressed question a, using data from the documentation review.
Phase 2 addressed questions b and c, using information from participant
observation and interviews. This is outlined in Table 5.1 below.
Table 5.1: Data types Data collection Question a
How are recovery practices reflected in documentation of a Clubhouse?
Question b How are recovery practices embodied in the behaviour of staff within a Clubhouse?
Question c How are recovery practices perceived by staff and members within a Clubhouse?
Phase 1 Documentation review
Directed qualitative content analysis.
Phase 2 Field notes from participant observation of staff
Theoretical thematic analysis.
Theoretical thematic analysis.
Phase 2 Interviews with members and staff
Theoretical thematic analysis.
Theoretical thematic analysis.
45
5.8 Phase 1: Consent for documentation review
Farkas and colleagues (2005), emphasise the importance of analysing
documents such as mission statements, and the policies and procedures of
mental health services, because they can strongly influence recovery-
oriented practice. Institutional consent from the Clubhouse director, for
permission to conduct a documentation review, was secured in 2013 as per
section 5.6.1 (appendix 3). An information session for members and staff,
explaining which documents would be reviewed, and that no documents
containing personal information would be involved, was provided. Informal
conversations introducing the study, and further explanation, was also
given on a one to one basis as needed. As mentioned in the previous
ethics section, information sheets and explanations were provided in clear
and simple language (See appendix 4).
5.8.1 Data collection for documentation review
In order to establish a corpus of documents that would be useful for
exploring recovery-oriented practice, and to ensure rigour in analysis of the
documents, it was important to identify internationally regarded recovery
categories. This was achieved with the assistance of the Australian Mental
Health Outcomes and Classification Network (AMHOCN) (Burgess et al.,
2011). In their international review of recovery tools, AMHOCN identified
the Recovery Promotion Fidelity Scale (RPFS) (Armstrong & Steffen, 2009)
as an instrument of high quality (Burgess et al., 2011).
Armstrong and Steffen (2009) report that the development of the
RPFS began with a comprehensive literature review, which identified fifty
46
one possible recovery indicators. A series of five focus groups, comprising
participants from a range of backgrounds, including people with lived
experience of mental illness, health administrators, service providers, and
researchers then added a further thirty-five new indicators, for a total of 86
potential recovery scale items.
Review of the thirty five recovery indicators by consumer consultants
then reduced the list of indicators to twenty five, which underwent further
assessment (Armstrong & Steffen, 2009). Consultation with twenty-eight
multicultural consultants reduced the items still further, until the final five
recovery categories of the RPFS were confirmed. The categories are,
collaboration; participation and acceptance; self-determination and peer
support; quality improvement; staff and consumer development (Armstrong
& Steffen, 2009). Written permission was granted by Dr Nikki Armstrong
from Hawaii State University to use the RPFS in this case study (Appendix
5).
5.8.2 Establishing a corpus of documents
In consultation with the Clubhouse Director, one hundred and twenty pages
of information was collected during two site visits of three hours each. Data
collected included representative materials suggested by the RPFS
including:
1. Information from the Clubhouse website and promotional materials.
2. The service vision/mission statement.
3. Any available consumer satisfaction survey used by the service.
4. Any available lists or descriptions of the Clubhouse’s committees.
47
5. Any available committee or team meeting minutes.
6. Policies and procedures documents.
7. An example or template of consumer recovery plan or similar.
8. Any staff role descriptions or checklists/scales for monitoring
outcomes.
9. De identified outcome tracking data.
10. Any staff or consumer training curriculum and any other documents
identified.
5.8.3 Qualitative content analysis of documents
A directed qualitative content analysis approach was used to review
documentation. This approach to analysis differs from conventional
inductive content analysis, because it begins with categories derived from
previous research, and assumes a deductive strategy to coding (Hsieh &
Shannon, 2005). Directed qualitative content analysis began by building
familiarity with the recovery categories of the RPFS. A deductive approach
to coding was then applied, classifying phrase references within the
documents according to their exemplification of RPFS recovery categories
(Hsieh & Shannon, 2005). A detailed description of this process and the
findings of the documentation review are reported in chapter 6.
5.9 Phase 2: Institutional consent for participant
observation and interviews
Following application and receipt of the second university ethics approval
(University approval number H10711, see appendix 2), the director of the
Clubhouse was contacted and a second institutional consent secured
48
(Appendix 6). This enabled resumption of the second phase of the study
which occurred over a three-month period from November 2014 through to
and including January 2015. Phase two involved participant observation
and interviews which are described below.
5.9.1 Recruitment
Subsequent to completion of the second institutional consent and
consultation with the Clubhouse director, research within the Clubhouse
resumed. With permission of the members and staff, the researcher placed
posters describing the study on noticeboards within the Clubhouse and
began attending the Clubhouse for six to eight hours, up to three days per
week. Conveniently, the Clubhouse holds a daily morning meeting, which
the researcher made a point of attending each visit.
The morning meeting enabled introduction to members and staff each
day, and provided opportunity to explain and invite participation. Informal
conversations with interested individuals introducing the study, the
research process, contact information and anticipated participant
commitments were provided. Members and staff interested in participating
in the study then contacted the researcher by either, approaching him while
he was present in the Clubhouse, by phone or email and scheduled a
suitable time to participate. After this process was complete, individual
written consent from interested participants was sought.
5.9.2 Consent for participant observation of staff
As described in chapter 2, the Clubhouse provides programs in a
communal setting heavily reliant on group work. Conducting participant
49
observation of staff in an open setting where people are free to come and
go without notice can present challenges. In particular, the process of
obtaining consent and negotiating the boundaries between phenomena and
context were challenging. For this reason, two different types of consent
were sought. Firstly, institutional consent for fieldwork was secured from
the Clubhouse director including clarification that the focus of participant
observation would be on the behaviour of consenting staff only, not
Clubhouse members (Appendix 6). Secondly, individual written consent
was provided by each participating staff member regarding participant
observation (Appendix 9). Prior to providing consent all staff were given
interview participant information packs containing study information sheets
explaining that their involvement in participant observation was voluntary,
that they would not be disadvantaged by not participating and could
withdraw at any time (Patton, 2005). Once individual written consent had
been provided, the researcher worked with each staff participant to identify
convenient dates and times for participant observation.
With guidance from the Clubhouse director, it was not considered
necessary to seek individual consent from every Clubhouse member who
may be present in the Clubhouse, because the focus of participant
observation was on staff behaviour. It is important to note that during
participant observation, while staff were observed interacting with
Clubhouse members, field notes did not record interactions or verbal
exchanges between staff and members. This is because what staff were
doing and how they did it was the focus of participant observation rather
50
than what staff said. When the researcher was privy to close interactions
between staff and members, the researcher sought introduction to the
members, and any other people involved, offering explanations regarding
identity and role of the researcher.
If consent for this part of the study had been completely individualised,
it would have required consent from every member of the Clubhouse on a
daily basis, and this would have been logistically problematic due to the
unpredictable, fluid nature of the Clubhouse, whereby large numbers of
members are free to come and go on a daily basis without notice.
Furthermore, as previously outlined in section 5.5, the setting of the
Clubhouse building was very open, meaning that when engaged in
activities members interacted in an open plan environment, where multiple
groups could be observed at the same time. Individualised consent may
therefore have limited the quality and quantity of data able to be collected
due to variability in members attending. For example, if a new member
refused consent, it would have been extremely difficult to observe any
group activity that staff engaged in e.g. facilitating activities as part of the
work ordered day, or other Clubhouse activities. Studies which involve
similar approaches have been used previously in mental health settings
and are not uncommon, see for example Cleary and colleagues (2011)
review of studies in mental health services.
5.9.3 Consent for interviews with staff and members
Separate written consent for individual interviews was secured from each
staff and member participant. The researcher worked with each participant
51
to identify convenient dates and times for their interview. All participants
were provided with interview information packs that specified interviews
would be audio recorded, that participation in the study was voluntary, that
they would not be disadvantaged by not participating and could withdraw at
any time (Patton, 2005). Consent to participate in interviews was therefore
voluntary, specific and obtained from competent persons, using a process
that maintains confidentiality and autonomy and is consistent with best
practice of researching consumers and staff in mental health services
(Cleary, 2004) (Appendix 10).
5.9.4 Data collection during participant observation
Building on the documentation review, participant observation focused on
how staff implemented recovery practices. Participant observation is a
qualitative research technique often used to explore practices within
organisations (Spradley, 1980). It enables researchers to gain an insider’s
view, by getting involved in everyday activities alongside staff (Yin, 2009).
The approach can be applied using various levels of disclosure. Some
participant observation is carried out with the researcher operating
completely incognito, without disclosing their identity or role whilst in the
organisation. In other versions, the researcher fully discloses their identity
while participating alongside staff. In this case study the identity of the
researcher was fully disclosed throughout the study (Schneider, 2002).
As much as possible the researcher sought to blend in, by
participating as a member of Clubhouse work activities alongside staff
participants. Observing in this way, illuminated how recovery practices
52
were embodied in the behaviour of staff, from a frontline point of view
(Cleary et al., 2011). Spending one hundred and twenty hours, over three
months immersed in the everyday environment of the Clubhouse, enabled
the researcher to observe common activities, relationships and service
experiences (Rossman & Rallis, 2011). Observational field notes recorded
during this activity used Spradley’s (1980) observational framework
including the nine dimensions outlined below:
1. Space: referred to the place where staff were observed, during each
observation period, for example, in the cafeteria or the garden of the
Clubhouse.
2. Actor: recorded de identified notes of the people observed, for
example, two staff running newsletter writing group with ten
members.
3. Activity: included any series of events that the actors (staff
members) engaged in, for example a work group aimed writing grant
applications.
4. Object: described the physical artefacts observed during an activity,
for example, a large table with ten chairs and computers on it.
5. Act: denoted particular actions that individual actors engaged in, for
example, how a staff member used a whiteboard to facilitate a group
activity.
6. Event: involved broad descriptions of sets of activities that occurred,
for example, a fundraising day was organised and facilitated.
53
7. Time: recorded the times that different activities took place and how
long they ran, for example, there was a half hour long morning
meeting, at 0900hrs each day.
8. Goal: noted the intention of actors observed, for example,
Clubhouse staff attempted to maximise member involvement in
garden cultivation as much as possible.
9. Feeling: referred to the feelings that appeared to be conveyed by
actors during a period of observation, for example staff appeared
warm and welcoming when meeting new members for the first time.
The findings from participant observation and interviews are reported in
chapters 7 and 8. How analysis was conducted is described in section
5.9.6.
5.9.5 Data collection during interviews
Interviews were guided by three different interview schedules provided in
the RPFS, one for the director, one for staff, and another for members. The
questions were designed around the same five recovery categories used
during documentation review, including, collaboration; participation and
acceptance; self-determination and peer support; quality improvement; staff
and consumer development (See appendix 11, 12 and 13). When
interviewee answers were unclear or particularly brief, the researcher used
open ended prompts to explore questions further, by using phrases such
as, “Is there anything else you would like to say about that?” Digital
recordings and interview transcripts were coded so that participant’s
confidentiality was maintained.
54
5.9.6 Analysis of participant observation and interview data
In contrast to the directed qualitative content analysis used during the
documentation review, information collected during participant observation
and interviews was analysed using thematic analyses. One way to apply
this technique is through inductive thematic analysis, which involves
immersion in collected data through reading and re-reading, searching for
emerging themes and minimising reference to theory (Fereday & Muir-
Cochrane, 2008). Alternatively, a theory may be used to conduct a
Given this case study was informed by SDT (see chapter 3), a
theoretical thematic analyses approach was adopted. The first step in this
process involved gaining a thorough knowledge of SDT (Deci & Ryan,
2012) and how its core principles of relatedness, competency and
autonomy related to recovery-oriented practice, and the Clubhouse model
(see chapter 3). Analysis was then guided by the six steps suggested by
Braun & Clarke (2006) which included:
1. Familiarisation with collected information through repeated reading
of field notes, transcripts and listening to interviews.
2. Generating initial codes by establishing an initial list of data features.
3. Searching for themes by reflecting on codes to identify potential
themes.
4. Reviewing and refining identified themes.
5. Defining what is interesting about the themes and why.
6. Reporting the final analysis and writing a coherent logical report.
55
Following these six steps as a guide, the application of theoretical thematic
analysis involved searching for patterns in the data relevant to the research
question and SDT (Braun & Clarke, 2006). Coding involved repeatedly
reading field notes and transcripts and listening to interview recordings,
codes were then assigned to pieces of information, such as phrases or
paragraphs that explained how recovery practices were implemented.
Consideration was then given to similarities between coded pieces of data,
and their resonance with self-determination theory. This process led to two
overarching themes with three sub-themes each, related to how recovery
practices were implemented within the Clubhouse. These findings are
reported in chapters seven and eight.
5.10 Triangulation
The concept of triangulation originated in the field of navigation, where it
refers to using multiple reference points to calculate a location (Farmer,
Robinson, Elliott, & Eyles, 2006). In qualitative research, triangulation
strategies include but are not limited to the use of two or more, theories,
methods, approaches to analysis, data collection techniques or data
sources. It is used to balance any deficiency that might occur from relying
on a single strategy (Thurmond, 2001). Triangulation adds to study depth,
increasing the potential of findings that will improve practice. A wide variety
of triangulation techniques have been described by a range of authors
(Denzin, 1978; Patton, 2015). In this case study, two triangulation
techniques were employed in phase two. They were:
56
1. Data collection triangulation: Two data collection techniques were
triangulated, participant observation and interviews.
2. Data source triangulation: The perspectives of two different groups
(staff and members) within the Clubhouse were triangulated.
The way in which triangulation contributed to findings of the study will be
outlined in chapter 9.
5.11 Rigour
Being able to demonstrate rigor is an important part of high quality
qualitative research. In this study four common approaches were used to
maintain rigor. These were, credibility, transferability, dependability and
confirmability (Guba & Lincoln, 1982).
Credibility, refers to the ability of others to recognise the authenticity of
experiences described in a qualitative study (Thomas & Magilvy, 2011).
When reporting findings, the words of participants were used as much as
possible, to strengthen the credibility of findings. The use of SDT as a
theoretical framework and the RPFS as a research instrument for recovery
categories and interview questions, also enhanced credibility because SDT
has been widely researched (Deci & Ryan, 2012) and the RPFS has been
empirically validated (Armstrong & Steffen, 2009; Burgess et al., 2011).
Consistent research supervision, also enhanced the credibility of the
research. Throughout the study, the researcher engaged in regular three to
five weekly reviews and discussion with research supervisors, who are all
highly experienced qualitative researchers.
57
Transferability refers to the ability to transfer research methods and
findings to other qualitative research (Kuper, Lingard, & Levinson, 2008). A
strategy relevant to transferability applied during the documentation review,
was the use of the steps suggested by Elo & Kyngäs (2008). These are:
1. Establish a corpus of source materials.
2. Characterise each document; Noting when written? Where? By
whom? Why?
3. Develop categories.
4. Code and classify the documents according to how they exemplify
categories.
With reference to the transferability of methods during the participant
observation and interview phase, the first step involved becoming familiar
with SDT (see chapter 3). The researcher therefore had the core principles
of SDT clearly in mind prior to entering the field. SDT was then used as a
theoretical framework for interpreting and describing how recovery
practices were implemented. As described above in 5.9.6 this was applied
using the analytical process suggested by Braun and Clarke (2006).
Through a continuous process of reading, coding, reflection and
refinement, the overarching themes of ‘social environment’ (chapter 7) and
‘autonomy support’ (chapter 8) were developed.
The dependability and confirmability of qualitative studies refers to
the transparency of how decisions are made during the research process
and how information is interpreted (Krefting, 1991). As previously
mentioned in section 5.3, in this study an important consideration was the
58
breadth of interpretation possible in relation to what phenomena could
potentially be interpreted as ‘recovery-oriented practices’. To address this,
concern the researcher used SDT and the RPFS recovery categories, to
constrain how recovery practices could be interpreted. The ability of the
researcher to assess data from a purely subjective standpoint was
therefore restricted, increasing confirmability of findings.
An electronic file was kept recording phases of research planning,
data collection and analysis including notes from regular meetings with the
research supervisors. During the planning process consideration of issues
included but was not limited to the purpose of the study, data collection and
recruitment of participants, how information was to be analysed and how
findings were to be presented.
5.12 Reflexivity
Reflexivity refers to the importance of a researcher being self-aware of their
role as an instrument in a study at both a personal and epistemological
level (Dowling, 2006). The personal level refers to knowledge, experiences,
beliefs, motivations and biases the researcher brings form their past, which
hold potential to influence data. The epistemological level refers to the
importance of maintaining awareness of the researcher’s relationship to the
study and the influence of relationships formed with participants (Dowling,
2006).
With these concepts in mind, throughout data collection the researcher
engaged in a process of self-reflection, acknowledging their position in
relation to what they observed. This was maintained through a process of
59
regular journaling and writing field notes during and at the end of each day.
Reflection also took place during regular meetings with the research
supervisors. This process assisted the researcher to self-monitor, minimise
bias and ensure interpretations of information were reasonable (Denzin &
Lincoln, 2011).
At a personal level it was important to acknowledge and maintain
awareness of preconceived attitudes and beliefs about recovery that the
researcher had developed previously, during their career as a mental
health nurse, and how those ideas might affect the research process. As a
person without lived experience of mental illness, there was also a risk of
the researcher approaching analyses of data from the standpoint of an elite
outsider (Rossman & Rallis, 2011). At an epistemological level it was
important for the researcher observe the behavior of individual staff
towards both Clubhouse members, and other staff participants. It was also
important for the researcher to pay attention to the likely influence of the
researcher’s own presence on behaviour and interactions.
One way the researcher noticed the influence of their presence on
staff behaviour was during the morning meetings at the Clubhouse. When
the researcher was present, staff would give the researcher opportunity to
introduce himself and provide information about the study to any new
members present. Such introductions had an important function because
they enabled information about the study to be shared with members and
staff. Despite this, the researcher reflected on how staff may have acted if
they had not been aware of the researcher's presence in the Clubhouse. It
60
is likely that such announcements at the beginning of each day not only
provided information, but may also have heightened staff awareness that
they were being observed, thereby influencing behaviour.
5.13 Conclusion
The concept of recovery is increasingly relevant in the development and
delivery of mental healthcare, however there has been limited research into
how individual services implement recovery-oriented practices. Given
psychosocial Clubhouses have been a pioneer of recovery practices
internationally (Dudek & Aquila, 2012), exploring how recovery practices
are implemented within individual Clubhouses is important. This chapter
has described, how a case study design informed by SDT that included
direct data from documents, semi direct data gained through interviews and
indirect data from participant observation, has illuminated the
implementation of recovery practices within an Australian Clubhouse. The
findings of the case study will now be reported in chapters 6, 7 and 8,
before a final discussion in chapter 9.
61
CHAPTER 6: HOW ARE RECCOVERY-ORIENTED
PRACTICES REFLECTED IN DOCUMENTATION
WITHIN A CLUBHOUSE?
6.1 Introduction
The first of three findings chapters, this chapter presents findings from an
exploration of how recovery practices are reflected in the documentation of
the Clubhouse. Documents reviewed included representative samples of
key documents produced or utilised within the Clubhouse, including public
health promotion materials, and policy and membership documents. Data
were subjected to content analysis supported by the Recovery Promotion
Fidelity Scale (RPFS) (Armstrong & Steffen, 2007) leading to findings that
may be used to inform future research related to recovery-oriented practice
in Clubhouse settings.
6.2 Publication
The following is from:
Raeburn, T., Schmied, V., Hungerford, C., & Cleary, M. (2014).
Clubhouse model of psychiatric rehabilitation: How is recovery reflected in
documentation? International Journal of Mental Health Nursing, 23(5), 389-
397.
Feature Article
Clubhouse model of psychiatric rehabilitation:How is recovery reflected in documentation?
Toby Raeburn,1 Virginia Schmied,1 Catherine Hungerford2 and Michelle Cleary1
1School of Nursing & Midwifery, University of Western Sydney, Sydney, New South Wales, and 2Disciplines ofNursing and Midwifery, University of Canberra, Australian Capital Territory, Australia
ABSTRACT: Recovery-oriented models of psychiatric rehabilitation, such as the Clubhouse model,are an important addendum to the clinical treatment modalities that assist people with chronic andsevere mental illness. Several studies have described the subjective experiences of personal recovery ofindividuals in the clubhouse context, but limited research has been undertaken on how clubhouseshave operationalized recovery in practice. The research question addressed in this paper is: How arerecovery-oriented practices reflected in the documentation of a clubhouse? The documents examinedincluded representative samples of key documents produced or utilized by a clubhouse, includingpublic health-promotion materials and policy and membership documents. Data were subjected tocontent analysis, supported by the Recovery Promotion Fidelity Scale. The recovery categories iden-tified in the documents included collaboration (27.7%), acceptance and participation (25.3%), qualityimprovement (18.0%), consumer and staff development (14.5%), and self-determination (14.5%).These categories show how the clubhouse constructs and represents personal recovery through itsdocumentation. The findings are important in light of the role that documentation can play ininfluencing communication, relationships, and behaviour within organizations. The findings can alsobe used to inform future research related to recovery-oriented practices in clubhouse settings.
Personal recovery for people with chronic and severemental illness is a subjective process through whichpeople regain a satisfying, participatory life that may ormay not include enduring symptoms of mental illnessor challenges to social roles (Slade et al. 2012). Thus,personal recovery is a highly subjective process with nouniform definition. This stands in contrast to the moretraditional notion of clinical recovery, with its medicalfocus on the remission of symptoms and measureable
improvement of social functioning (Slade et al. 2012). Thelack of uniform definition of personal recovery also sug-gests reasons for the many challenges that have beenidentified in relation to researching the recovery orienta-tion of contemporary mental health services (Burgesset al. 2011; Williams et al. 2012).
The development of services that facilitate personalrecovery is now a national policy priority in many coun-tries, requiring quite a different organizational focus tothat traditionally taken by clinical services (Cleary et al.2012; Farkas 2007; Hungerford & Kench 2013). Theextent to which organizational practices reflect thevalues of personal recovery, including hope, acceptance,empowerment, engagement in productive activity, andmaintenance of supportive relationships, is referred to asthe ‘recovery orientation’ of a service (Williams et al.2012). The Clubhouse model, which is one approach tothe delivery of psychiatric rehabilitation services in the
Correspondence: Toby Raeburn, ROAM Communities MentalHealth Nursing and PhD Candidate School of Nursing & Midwifery,University of Western Sydney, Level 1, 125 Argyle Street, Camden,NSW 2570, Australia. Email: [email protected]
community, is at the forefront of developing recovery-oriented mental health services (Dudek & Aquila 2012;Ferguson 2004; Pernice-Duca & Onaga 2009).
Currently providing services at more than 300 sites inmore than 27 countries worldwide, the Clubhouse modelis making a substantial contribution to the field of psychi-atric rehabilitation (Raeburn et al. 2013). The delivery ofpsychosocial and employment services by clubhousescomplements the clinical work undertaken across themultidisciplinary spectrum. Even so, research exploringrecovery-oriented services and practices in the clubhousesetting is scant.
This gap in the literature is problematic. Forexample, Anthony et al. (2003) express concern thatmodels of psychiatric rehabilitation are often imple-mented, despite a lack of evidence regarding theirrecovery orientation. They highlight the importance ofunpacking the various components of care within theseservices and subjecting them to rigorous research(Anthony et al. 2003). By reviewing how the documen-tation within one clubhouse reflects recovery-orientedpractice, in the present study, we seek to contributeknowledge to this increasingly important area of mentalhealth service delivery.
BackgroundIn the late 1940s, a group of people with a lived experi-ence of mental illness commenced meeting on the stepsof the New York City library, to provide support to eachother. Poignantly, the early name of this support groupwas ‘WANA’, an acronym for ‘We are not alone’(Anderson 1998). As the group grew in number, it came tothe attention of a wealthy local philanthropist, who lentmembers the use of a house with a fountain in the back-yard to hold their meetings. On shifting the meetings tothe house, the group changed its name to ‘FountainHouse’ (Pratt et al. 2006). This pioneering service stillruns in New York today, and has grown to become atemplate for what is now referred to as the ‘Clubhousemodel’ of psychiatric rehabilitation internationally.
To promote solidarity and support within clubhouses,participants are referred to as ‘members’, whose attend-ance and contribution to activities are highly valued(Huelsmann 2009). In this way, people with mental illnessare treated as active participants, rather than recipients ofcare, by paid staff, working towards personal recoveryalongside these paid staff (Marshall et al. 2010). This prin-ciple is strongly supported by paid staff, who adopt gen-eralist roles that might include menial tasks, such asserving lunch or cleaning a bathroom, while also provid-ing more skilful assistance as caseworkers or providers of
incidental counselling. By sharing work and adopting ateam approach, barriers between the roles of paid staffand people with mental illness are broken down, increas-ing each member’s sense of connection with others,reducing social isolation, and building confidence (Wong2010).
Activities within each clubhouse are also linked tovocational initiatives, referred to as transitional employ-ment programs (TEP), which are designed to act as astepping stone to the competitive workforce. To establishTEP, clubhouses negotiate contracts with local busi-nesses, which agree to set aside a job for clubhousemembers. TEP arrangements are then owned as theresponsibility of the entire clubhouse, with paid staff andmembers agreeing to cover absences whenever TEPemployees are unable to attend. In addition, and as afollow up, clubhouses provide traditional supportedemployment programmes, providing members who enterthe competitive workforce with the assistance they needto maintain their job for the long term (Macias et al.2006).
The Clubhouse model has not been without opposi-tion. For example, clubhouses have been criticized fortheir tendency to promote a limited range of employmentpathways for members, leading to limited skill sets andexpectations incompatible with the competitive jobmarket (Waghorn & Lloyd 2005). In addition, Hindenet al. (2009) have criticized clubhouses for their generallack of engagement with the families of members. Theymake the point that, while clubhouses have been strongadvocates for mental health recovery, they have also beenlargely individualistic in their approach, failing to seizeopportunities to interact with families of members andinfluence parenting styles (Hinden et al. 2009).
In contrast to this criticism, however, members gener-ally report high levels of satisfaction with the opportu-nities provided in the clubhouse setting to experiencesupportive relationships and develop vocational skills(Jung & Kim 2012). These strengths of the Clubhousemodel can be linked to the suggestion that people livingwith chronic or severe mental illness can lack family andsocial supports, and have poor access to educational andemployment opportunities (Corrigan & Watson 2002;Morgan et al. 2011). Clubhouses offer a safety net forpeople with chronic and severe mental illness. In addi-tion, the Clubhouse model has been implemented acrossa range of cultures. For example, a Hong Kong-basedstudy conducted by Wong (2010) described improvedconfidence and coping skills that made it easier for club-house participants to cope with stigma, as they workedtowards personal recovery.
Study contextMany of the concepts that currently populate the mentalhealth recovery landscape have been derived from theClubhouse model (Dudek & Aquila 2012), with club-houses describing themselves as recovery-oriented com-munities (Ferguson 2004; Pernice-Duca & Onaga 2009).However, while there has been substantial researchdescribing experiences of personal recovery among club-house members (Coniglio et al. 2012; Hancock et al.2011), there has been little investigation into the specificsof recovery-oriented practices applied by clubhouses.
Prior (2008) emphasized the impact of documentationon behaviour within organizations, contending that docu-ments are not just static records, but materials that oftenprompt reflection and stimulate discussion that influencedecisions and behaviour. Hungerford (2014) argued thatthe documents produced or utilized by an organizationwill construct, represent, and also maintain the character-istics of that organization. Documents also provide animportant means of illuminating the major preoccupa-tions of the organization that produced them; preoccupa-tions that might otherwise remain covert (Hungerford2014). Silverman (2013) went on further, suggesting thatthe examination of documents provides a means of con-sidering not only the subject at hand, but also the contextin which that subject is located. Despite these many ben-efits, a search of the literature failed to identify any pre-vious study examining the way personal recovery isreflected in clubhouse documentation. In this paper, weseek to address this gap in the literature, and examine howrecovery-oriented practices are reflected in the documen-tation of a clubhouse.
METHODS
The ethical aspects of the study were reviewed andapproved by the human research ethics committeeattached to the university with which the researchers areassociated, with organizational consent also provided bythe clubhouse director. The research was conducted in2013 at one of the eight clubhouses that operate atgeographically-scattered locations throughout Australia.The analysis did not involve any documents containingpersonal information. To mitigate the potential concernsof clubhouse members regarding the researchers’ accessto personal information, the researchers worked closelywith the clubhouse director to provide information formembers interested in the study.
There are a variety of instruments available to measurethe recovery orientation of mental health services.However, these instruments are difficult to compare, as
they have been developed for a range of service types(Williams et al. 2012). This made it challenging to identifywhich instrument would be most suitable to guide thisstudy. Therefore, the instrument chosen was based on theinternational review of service recovery-orientation toolsconducted by the Australian Government’s Mental HealthOutcomes and Classification Network (AMHOCN)(Burgess et al. 2011). A small group of four instrumentswas recommended by the AMHOCN review as beingsuitable for application in Australian services. Of these, theRecovery Promotion Fidelity Scale (RPFS) (Armstrong &Steffen 2009) was selected to guide this analysis.
Although not specifically designed for the purpose ofdocumentation review, the RPFS was chosen because ofits psychometric soundness (Burgess et al. 2011).Armstrong and Steffen (2009) explained that constructionof the RPFS began with a comprehensive literaturereview, which identified 51 possible recovery categories.Development of the instrument included the use offocus groups comprising consumers, family and carers,administrators, service providers, representatives fromculturally- and linguistically-diverse cultures, andresearchers, to a total of 28 recovery experts. The fidelityscale comprises 12 recovery items and five recovery cat-egories: collaboration, participation and acceptance, self-determination, quality improvement, and staff/consumerdevelopment (Armstrong & Steffen 2009). Althoughdeveloped in the USA, Burgess et al. (2011) identified theRPFS as suitable for guiding the study of recovery prac-tices within Australian services.
According to Scott (1990), the data examined as part ofdocumentary analysis can include a variety of readablesources, including notes, newsletters, diaries, policy andprocedure documents, philosophical statements, adver-tisements, account statements, reports, and speechrecords. For the present study, the documents collectedwere the representative samples of public health-promotion materials: policy, service and organizationaldocuments, membership documents, and minutes ofmeetings, and included: (i) sample pages from the club-house website and other publically-available health-promotion materials, such as pamphlets, posters, andflyers; (ii) service vision and mission statement; (iii) clu-bhouse’s consumer satisfaction survey; (iv) a membershiphandbook describing the clubhouses to its subgroups; (v)de-identified minutes from the clubhouse’s most recentannual general meeting; (vi) sample policies and pro-cedure documents; (vii) template of the clubhouse’s indi-vidual goal-setting plan (recovery plan); (viii) staff jobdescription and appraisal monitoring template; (ix)de-identified outcome tracking data from the clubhouse’s
strategic plan; and (x) PowerPoint presentation used inthe public health promotion of the clubhouse.
With the assistance of the clubhouse director, thedocuments were collected during two 3-hour site visits,and comprised a total of 120 pages, electronically scannedfor data security.
In the linguistic and communication disciplines,content analysis is understood as a quantitative approachto analysing texts, and involves counting the number oftimes certain words, terms, or constructs occur in a text.While this approach might have value in some circum-stances, an arguable weakness lies with the assumptionthat the terms that appear most often in a document willreflect the greatest concerns of those who produce thedocument (Stemler 2001). For the current study, theapproach taken to content analysis was more attuned tothe nursing and health sciences, with a broader, qualita-tive focus to examine categories represented in the datacollected. A strength of this approach to content analysisis that it can effectively reduce large amounts of data intounderstandable categories, and thereby enable inferencesto be made, providing the opportunity for corroborationusing other methods of data collection (Graneheim &Lundman 2004). A weakness is the inherently subjectivenature of the approach.
There are a variety of ways to conduct a qualitativecontent analysis. For this study, a directed style wasemployed, deriving relevant categories from the RPFS,and applying a deductive approach to coding (Hsieh &Shannon 2005). To increase the rigour of the analysis, theresearchers also followed the steps suggested by Elo andKyngäs (2008): (i) we established a corpus, defining thesource materials from which the data was drawn; (ii) wecharacterized each document: when and where was itwritten? By whom? Why?; (iii) we developed a categori-zation table based on the RPFS and our research question(Armstrong & Steffen 2009); and (iv) we coded and clas-sified the documents for exemplification of categories.
Analysis of the material was guided by a criticalreflection of the findings, with regard to the categoriesof collaboration, participation and acceptance, self-
determination and peer support, quality improvement,and staff and consumer development (Armstrong &Steffen 2009).
To exemplify, one phrase reference was taken to con-stitute a category unit; for example, the phrase reference:‘I can be a bit high or a bit low, but still I’m alwaysaccepted at the clubhouse’, identified in a clubhouse pam-phlet, was considered a unit category of ‘participation andacceptance’. However, if a phrase reference appearedrepeatedly in the documents, it was only considered torepresent a single unit. For example, at the bottom ofeach clubhouse policy, a sentence referred to as a ‘state-ment of consultation’ had been inserted. Althoughrepeated on every policy document, this was only consid-ered to account for a single category unit.
Analysis of the documents identified 166 units.Numerical values and percentages were calculated for thecategories to illustrate and compare the ways recoverycategories were represented in the documentation.Analysis and categorization of the data were performed bythe researchers, who also calculated frequencies of occur-rence. The data were categorized twice, 2 weeks apart,and the correspondence rate was 96%. Following theanalytical design of Latvala et al. (2000), reliability can beassessed in terms of auditability of the results, along withassessing how the categories were formed, and how datawere collected and classified for analysis.
RESULTS
The findings are presented numerically in Table 1, re-flecting the recovery-oriented categories identified byArmstrong and Steffen (2009). The most represented cate-gory was collaboration; the least represented categorieswere self-determination and staff/consumer development.
CollaborationThe category of collaboration refers to the cooperativenature of the relationship between paid staff and consum-ers, including shared responsibility, decision-making, andproblem solving in working towards organizational goals
TABLE 1: Recovery categories, as represented in documentation provided by the clubhouse
CollaborationParticipation and
acceptanceSelf-determinationand peer support
Qualityimprovement
Staff and consumerdevelopment
n % n % n % n % n %
Extent recovery-oriented practicesreflected in documents?
46 27.7 42 25.3 24 14.5 30 18.0 24 14.5
n, number of times a phrase reference reflecting each category was identified in the 120 pages of data; %, represents each number as a percentageof the total 166 phrase references found.
(Armstrong & Steffen 2007). This category was the mostcommonly cited recovery category in the documentationexamined, and includes the repeated use of the word‘member’ throughout all documents to describe consum-ers. Another example, found in the explanatory materialon the clubhouse’s website and in promotional pam-phlets, is the description of members as:
Valued participants and colleagues rather than the tradi-tional view of people with mental illness as patients, con-sumers, clients or as people who need to be managed.
Collaboration is also represented in the documentsthrough descriptions of work-related activities. Forexample, there are detailed accounts of activities thatprovide members with opportunities to collaborate withpaid staff through programmes, such as the work-orderedday, and also transitional or supported employmentprogrammes.
The members’ handbook also points to the reliance ofthe clubhouse on collaboration between members andpaid staff, for the service to continue its operation. Thehandbook outlines policy, which states that the servicewill employ enough paid staff to engage members in activ-ities, but few enough to make fulfilling responsibilitiesimpossible without collaboration of members. This policyserves to encourage members to meaningfully collaboratein the delivery of services, with written procedures pro-vided to support members to engage in the activities ofthe work-ordered day, to orientate new members, to enrolin transitional or supported employment programmes,and so on.
The findings of the analysis of the public health-promotion documentation suggest that collaboration isnot just limited to activities inside the clubhouse, but alsoextends to relationships with local businesses and thewider community. Examples include advertising in thepromotional pamphlets of the clubhouse’s TEP, such astestimonies from business people describing their positiveexperiences of working with clubhouse members throughemployment placements. External collaboration with thewider community is also documented through the testi-monies of members who describe the value of transitionaland supported employment opportunities made possiblethrough clubhouse partnerships.
Participation and acceptanceParticipation and acceptance refers, first, to the involve-ment by members at all levels of operation, includinggovernance; and, second, to the attitude of paid staff andmembers to one another (Armstrong & Steffen 2007).This was the second strongest recovery category identi-
fied by the analysis, and included descriptions throughoutmembers’ handbook and policy documents that promotedthe participation of members at every level of activity,including participation in all decision-making groups.
Opportunities are outlined to participate in work pro-grammes, social activities, in public speaking, and also atpromotional events or on policy committees. For example,testimonies from members who have been involved inclubhouse activities appear in pamphlets and promotionalmaterials, and describe the sense of participation andacceptance they have experienced. Comments include:
A place to be somewhere with people who I can relate towhich gets me out of the house and into a more positiveenvironment,
I can be high or a bit low but still I’m always accepted atClubhouse.
These show potential members, and also the widersociety, how clubhouse values are upheld.
Self-determination and peer supportThe category of self-determination and peer support refersto whether consumers’ rights to freedom and choice areupheld by a service (Armstrong & Steffen 2007). While itwas one of the least referenced recovery categories exhi-bited in this documentation review, the concept was never-theless evident. For example, two of the standards in a listof guiding principles for this clubhouse stipulate that thereare no rules to enforce participation of members, and thatmembers have complete choice about which members andpaid staff they wish to work with. Another place where acommitment to promoting self-determination is illustratedis in the vision statement of the clubhouse, which includesspecific reference to assisting members to realize goals,maximize interaction with the wider community, andenhance quality of life. Also important are statements onthe website and health-promotion materials, which high-light the most essential values held at the clubhouse: thatevery member has a right to peer support and can recovera personally-satisfying life.
The provision of assistance towards higher levels ofself-determination through paid employment in widersociety was particularly evident in statements associatedwith the strategy and mission statements of the club-house. The effect of such programmes in increasing levelsof self-determination is then supported by testimonialsfrom participating members; for example:
Working is very important to me and helps me to keepwell, work makes me feel good and I like to make my ownmoney, the Clubhouse will always support me.
It appears, however, the support for self-determinationand peer support by the clubhouse does not occurthrough work-related activities alone. This is suggestedquite poetically by a member’s poetic description of theclubhouse:
A house of fun, A house of sun, A house of friendship, Ahouse of love, A home to everyone.
Quality improvementQuality improvement refers to whether a service hasmechanisms in place to facilitate ongoing, recovery-focused quality improvement in service delivery,internal decision-making processes, and administrativeprocedures (Armstrong & Steffen 2007). In the documen-tation of this clubhouse, commitment to quality improve-ment is demonstrated through annual member surveys,completed anonymously, which comprise two pages. Thesurvey collects data about members’ attendance andexperiences at the clubhouse. The documentation makesit clear that survey results are reported to a quality-improvement committee that comprises both paid staffand members.
Commitment to quality improvement is also exhibitedby a goal found in the vision statement of the clubhouse:to become Australia’s leading provider of psychosocialrehabilitation within 3 years. Other practical examplesdisplayed in the documentation include activities toengage with government-accreditation processes forfunding; goals to improve administrative, financial, anddata management systems; and the provision of ongoingtraining opportunities for paid staff and members. Themembers’ handbook goes on to describe the clubhouse’scommitment to including members in every decision-making panel or committee, and maintaining high-qualityservices by participating in the international clubhouseaccreditation process. This process is mentioned again inthe minutes of the annual general meeting, which cel-ebrate the clubhouse’s recent reaccreditation for a further3 years.
Consumer and staff developmentConsumer and staff development refers to a serviceculture that promotes the concept of continual improve-ment through the delivery of recovery training for staffand consumers on a consistent basis (Armstrong &Steffen 2007). Reference to the formal recovery trainingof paid staff and members appears in the minutes of theannual general meeting, with a brief mention of attend-ance at training events during the past year, includingnational and international conferences. The particulars of
what this training entailed, however, were not provided inthe documentation reviewed.
The documentation also outlines elements of a6-monthly recovery plan for members, and a regularappraisal process for paid staff. Policy documents suggestthat either paid staff or peer workers might be responsiblefor reviewing the recovery plans of members. The paidstaff appraisals, however, appear to be the responsibilityof the clubhouse director, who is accountable to the club-house board of directors.
DISCUSSION
The documents reviewed in this study strongly promotedthe recovery categories of collaboration, participation,and acceptance. This stands in contrast to traditional rep-resentations of the experience of chronic and severemental illness, which more often reflect themes, such assadness, struggle, and stigma (Corrigan et al. 2005;Horsfall et al. 2010). Importantly, representations of thepractices related to personal recovery in the documenta-tion were linked to undertakings or measures that wouldconvert policy or words into action. For example, archi-tectural plans to improve the quality of the space providedby this clubhouse, together with funding commitmentsfor the building, were reflected in the minutes of the mostrecent annual general meeting. Another example is thedescriptions of the collaborative undertakings betweenthe service and community partners. These descriptionsinclude the steps taken to facilitate TEP, and support jobplacements that enable members to move from activitiesinside the clubhouse to jobs in the competitive labourmarket. Such collaboration with community partners sup-ports evidence that the implementation of recovery-oriented practices is not confined to what organizations dofor participants internally. It also represents how organi-zations connect members with opportunities in widersociety (Drake et al. 2012; Drake & Latimer 2012).
The relatively low rating of the recovery category ofself-determination and peer support prompts reflectionabout the influence of groupthink on participants of theclubhouse. Macleod (2011) described ‘groupthink’ as thethinking that members of groups engage in when theirmotivation to maintain unanimity overrides desire tovoice alternative thoughts or actions. While groupthinkcan sometimes produce good decisions, thanks to itsability to pool knowledge and insights, it can also lead toindividual members failing to be heard, due to a tendencyby groups to be led by dominant dogma and personalitiesthat discourage individualized thought and expression(De Tezanos-Pinto et al. 2010).
In this clubhouse, dogma might be seen as beingevident in the documents use of term ‘standards’ thatmust be conformed to by the clubhouse for the purposesof accreditation, and references to the manager of theclubhouse as the ‘director’. These two examples might beunderstood to imply that organizational culture is unlikelyto encourage thinking that is innovative or ‘outside thebox’ in this clubhouse. Indeed, a kind of self-imposedconformity might become normalized, as a means ofmaintaining the perceived cohesiveness of the clubhouse(De Tezanos-Pinto et al. 2010). In turn, this mightprevent paid staff and members from hearing messagesrelated to weaker category units, such as self-determination. At its worst, this kind of dogma might riseto a kind of ‘groupspeak’, whereby repeated slogans andepithets are taken to represent the thinking of theclubhouse at the expense of self-expression. If negativeelements of groupthink and groupspeak becomeentrenched, paid staff and members might lose the abilityto be assertive, to respond to new information, or to adaptto societal change (Macleod 2011).
The influence of groupthink might also be linked toother challenges apparent in the clubhouse documenta-tion. One such challenge relates to the idea of work as auniversal panacea to every recovery hurdle. For example,the very notion of unpaid voluntary work inside the club-house might be seen as controversial, because of thebenefit paid staff receive as a derivative of members’ vol-untary contributions. This is contrary to the principlesof a social cooperative-type enterprise more commonin Europe, where members receive pay from activitiesengaged in by the organization in which they hold mem-bership (Mancino & Thomas 2005). Of course, this wouldbe different if the members of the clubhouse were choos-ing to pay the staff from funds that were transparentlyproduced by the clubhouse, similar to the way a sportingclub might procure the services of an administrator torun weekend competitions, manage financial accountsand maintain the grounds. However, in this clubhouse,minutes from the annual general meeting suggest paidstaff of the clubhouse are employed by a large non-government organization, which manages a budget in thevicinity of $A500 000 per year in government grants onbehalf of clubhouse members.
An alternative and more positive way of thinking aboutthe unpaid work of clubhouse members, however, mightbe found in the concept of ‘coproduction’ in service deliv-ery. This idea describes enlisting service consumers asproviders, in contrast to traditional approaches that tendto treat people with an illness as passive recipients of care.Coproduction attempts to harness the fact that people
generally have abilities that can contribute to theimprovement of services that they use (Needham 2009).As found in the documentation of this clubhouse, thecontributions that members ordinarily make are notusually financial, but include social capital, such as skillsand insights, and through the provision of intentional peersupport.
Overall, any reflection upon the concerns of group-think within this clubhouse should be balanced with criti-cism of the individualistic approaches often promotedby Western models of care towards people with severemental illness (Leighton 2004; Leong & Lau 2001). Suchcriticism has been linked to experiences of blame,estrangement, and stigma, all of which provide barriers tothe achievement of personal recovery (Corrigan et al.2005). Alternatively, collectivist approaches to mentalillness, where a person’s experience of chronic or severemental illness is owned as the responsibility of the wholecommunity, have been promoted as powerful communalsymbols of solidarity, which can greatly assist personalrecovery (Warner 2004). This kind of approach appears tobe exhibited in the collaborative approach of this club-house, which heavily promotes the value that peoplerecover best in community (Dudek & Aquila 2012;Pernice-Duca & Onaga 2009).
Finally, Anthony et al. (2003) highlighted the impor-tance of unpacking the various components of care withinmodels of psychiatric rehabilitation, and subjecting themto rigorous research to enable service improvement. Oneof the strengths of the present study was to focus on thedocumentation of a single clubhouse, which producedvaluable knowledge about the way this service applies arecovery-oriented framework. Another strength was thegenerous access to documentation granted by the siteclubhouse director and members. The study stands asan example of the use of qualitative content analysis inassessing the documentation of a psychiatric rehabilita-tion service, and might provide a basis for future com-parative studies.
As with all studies, however, there are also limitations.These include a limited generalizability of the findings,with the study involving only one clubhouse located inAustralia. Given the wide array of terms used to describerecovery concepts in mental health literature, anotherlimitation was the restriction of recovery categories tothose identified by the RPFS (Armstrong & Steffen 2009).In addition, and as stated earlier, the RPFS was originallydeveloped as a service measurement scale, and not as atool to guide content analysis, but the RPFS categoriesdid provide a useful guide for reducing the data to under-standable categories for comparison.
Overall, the present study demonstrated that personalmental health recovery and recovery-oriented practicesare strongly represented in the clubhouse documentationexamined. This finding is important in light of the powerof organizational documents to shape the way in whichthe people within that organization communicate, relate,and behave. Therefore, the results of this study promptthe question: how are recovery-oriented practices,reflected within the documentation of this clubhouse,translated into practice? Future studies to address thisquestion must consider the idiosyncratic nature of per-sonal recovery, and also the various ways in which recov-ery is embodied in the behaviour of paid staff andclubhouse members. This research has the potential tobenefit the ongoing development of clubhouse services,and also the personal recovery journey of people livingwith chronic and severe mental illness.
ACKNOWLEDGEMENTS
The authors would like to acknowledge and sincerelythank the clubhouse involved in this study for their will-ingness to participate.
REFERENCES
Anderson, S. B. (1998). We Are Not Alone: Fountain House andthe Development of Clubhouse Culture. New York: FountainHouse.
Anthony, W., Rogers, E. S. & Farkas, M. (2003). Research onevidence-based practices: Future directions in an era ofrecovery. Community Mental Health Journal, 39 (2), 101–114.
Armstrong, N. P. & Steffen, J. J. (2007). Hawaii RecoveryPromotion Fidelity Scale, Administration Manual. MentalHealth Services Research, Evaluation, and Training(MHSRET) Program. Adult Mental Health Division(AMHD). Hawaii: Hawai‘i Department of Health.
Armstrong, N. P. & Steffen, J. J. (2009). The recovery promotionfidelity scale: Assessing the organizational promotion ofrecovery. Community Mental Health Journal, 45 (3), 163–170.
Burgess, P., Pirkis, J., Coombs, T. & Rosen, A. (2011). Assessingthe value of existing recovery measures for routine use inAustralian mental health services. Australian and NewZealand Journal of Psychiatry, 45 (4), 267–280.
Cleary, M., Horsfall, J., O’Hara-Aarons, M. & Hunt, G. (2012).Mental health nurses’ views of recovery within an acutesetting. International Journal of Mental Health Nursing,22 (3), 205–212.
Coniglio, F. D., Hancock, N. & Ellis, A. (2012). Peer supportwithin a clubhouse: A grounded theory study. CommunityMental Health Journal, 48 (2), 153–160.
Corrigan, P. & Watson, A. (2002). Understanding the impactof stigma on people with mental illness. World Psychiatry,1 (1), 16–20.
Corrigan, P., Kerr, A. & Knudsen, L. (2005). The stigma ofmental illness: Explanatory models and methods for change.Applied and Preventive Psychology, 11 (3), 179–190.
De Tezanos-Pinto, P., Bratt, C. & Brown, R. (2010). What willthe others think? In-group norms as a mediator of the effectsof intergroup contact. British Journal of Social Psychology,49 (3), 507–523.
Drake, R. & Latimer, E. (2012). Lessons learned in developingcommunity mental health care in North America. WorldPsychiatry, 11 (1), 47–51.
Drake, R., Bond, G. & Becker, D. (2012). Individual Placementand Support: An Evidence-Based Approach to SupportedEmployment. New York: Oxford University Press.
Dudek, K. J. & Aquila, R. (2012). Fountain house and recoverycenters. Psychiatric Services, 63 (4), 396.
Elo, S. & Kyngäs, H. (2008). The qualitative content analysisprocess. Journal of Advanced Nursing, 62 (1), 107–115.
Farkas, M. (2007). The vision of recovery today: What it is andwhat it means for services. World Psychiatry, 6 (2), 68–74.
Ferguson, A. (2004). Clubhouse: The recovery model. MentalHealth Practice, 7 (9), 22–23.
Graneheim, U. H. & Lundman, B. (2004). Qualitative contentanalysis in nursing research: Concepts, procedures andmeasures to achieve trustworthiness. Nurse EducationToday, 24 (2), 105–112.
Hancock, N., Bundy, A., Honey, A., James, G. & Tamsett, S.(2011). Improving measurement properties of the RecoveryAssessment Scale with Rasch analysis. The American Journalof Occupational Therapy, 65 (6), 77–85.
Hinden, B., Wolf, T., Biebel, K. & Nicholson, J. (2009). Sup-porting clubhouse members in their role as parents: Neces-sary conditions for policy and practice initiatives. PsychiatricRehabilitation Journal, 33 (2), 98–105.
Horsfall, J., Cleary, M. & Hunt, G. E. (2010). Stigma in mentalhealth: Clients and professionals. Issues in Mental HealthNursing, 31 (7), 450–455.
Hsieh, H.-F. & Shannon, S. E. (2005). Three approaches toqualitative content analysis. Qualitative Health Research,15 (9), 1277–1288.
Huelsmann, L. (2009). If you build it, they will come: Creatinga new clubhouse was an inclusive process. BehavioralHealthcare, 29 (5), 27–29.
Hungerford, C. (2014). Recovery as a ‘model of care’? Insightsfrom an Australian case study. Issues in Mental HealthNursing, 35 (3), 156–164.
Hungerford, C. & Kench, P. (2013). The perceptions of healthprofessionals of the implementation of recovery-orientedhealth services: A case study analysis. The Journal of Mental
Health Training, Education and Practice, 8 (4), 208–218.
Jung, S. H. & Kim, H. J. (2012). Perceived stigma and quality oflife of individuals diagnosed with schizophrenia and receiv-ing psychiatric rehabilitation services: A comparison betweenthe clubhouse model and a rehabilitation skills trainingmodel in South Korea. Psychiatric Rehabilitation Journal,35 (6), 460–465.
Latvala, E., Janhonen, S. & Moring, J. (2000). Passive patients:A challenge to psychiatric nurses. Perspectives in PsychiatricCare, 36 (1), 24–32.
Leighton, K. (2004). Anglo-American nursing theory, individu-alism and mental health care: A social conflict perspective.International Journal of Nursing Studies, 41 (1), 21–28.
Leong, T. & Lau, S. (2001). Barriers to providing effectivemental health services to Asian Americans. Mental HealthServices Research, 3 (4), 201–214.
Macias, C., Rodican, C., Hargreaves, W., Jones, D., Barreira, P.& Wang, Q. (2006). Supported employment outcomes of arandomized controlled trial of ACT and clubhouse models.Psychiatric Services, 57 (10), 1406–1415.
Macleod, L. (2011). Avoiding ‘group think’: A manager’s chal-lenge. Nursing Management, 42 (10), 44–48.
Mancino, A. & Thomas, A. (2005). An Italian pattern of socialenterprise: The social cooperative. Nonprofit Managementand Leadership, 15 (3), 357–369.
Marshall, S., Deane, F. & Hancock, N. (2010). Increasingresearch familiarity amongst members of a clubhouse forpeople with mental illness. The Australian Journal of Reha-bilitation Counselling, 16 (02), 119–125.
Morgan, V., Waterreus, A., Jablensky, A., Mackinnon, A.,McGrath, J. & Carr, V. (2011). People Living with PsychoticIllness. Report on the Second Australian National Survey.Canberra: Commonwealth of Australia.
Needham, C. (2009). SCIE Research briefing 31:Co-production: An emerging evidence base for adult socialcare transformation. Policing, 8, 11.
Pernice-Duca, F. & Onaga, E. (2009). Examining the contribu-tion of social network support to the recovery process amongclubhouse members. American Journal of Psychiatric Reha-bilitation, 12 (1), 1–30.
Pratt, C. W., Gill, K. J., Barrett, N. M. & Roberts, M. M. (2006).Psychiatric Rehabilitation. San Diego, CA: Academic Press.
Prior, L. (2008). Repositioning documents in social research.Sociology, 42 (5), 821–836.
Raeburn, T., Halcomb, E., Walter, G. & Cleary, M. (2013). Anoverview of the clubhouse model of psychiatric rehabilita-tion. Australasian Psychiatry, 21 (4), 376–378.
Scott, J. (1990). A Matter of Record: Documentary Sources inSocial Research. Cambridge: Polity Press.
Silverman, D. (2013). Doing Qualitative Research: A PracticalHandbook. London: SAGE Publications.
Slade, M., Leamy, M., Bacon, F. et al. (2012). Internationaldifferences in understanding recovery: Systematic review.Epidemiology and Psychiatric Sciences, 21 (04), 353–364.
Stemler, S. (2001). An overview of content analysis. PracticalAssessment, Research & Evaluation, 7 (17), 137–146.
Waghorn, G. & Lloyd, C. (2005). The employment of peoplewith mental illness. Advances in Mental Health, 4 (2), 129–171.
Warner, R. (2004). Recovery from Schizophrenia: Psychiatryand Political Economy. New York: Psychology Press.
Williams, J., Leamy, M., Bird, V. et al. (2012). Measures of therecovery orientation of mental health services: Systematicreview. Social Psychiatry and Psychiatric Epidemiology,47 (11), 1827–1835.
Wong, K. F. (2010). Implementation of Clubhouse modelprogramme: Perception of mental health nurses. Journal ofPsychiatric & Mental Health Nursing, 17 (8), 750–753.
This chapter has presented the findings of a documentation review within a
psychosocial Clubhouse. It involved scrutinising a wide range of readable
sources, including but not limited to, health promotion pamphlets, policy
and procedure documents and minutes of meetings. Each of the recovery
categories used for analyses was reflected within the Clubhouse
documentation.
Documentation has the power to influence patterns of communication,
along with workplace and social behaviour. The results of this
documentation review prompt consideration of the question, how are
recovery-oriented practices reflected in documentation within the
Clubhouse embodied in the behaviour of its staff? The chapters that follow
will consider this question and will also explore, how recovery practices are
perceived by Clubhouse members and staff.
72
CHAPTER 7: RECOVERY-ORIENTED PRACTICES
AND SOCIAL ENVIRONMENT WITHIN A
CLUBHOUSE
7.1 Introduction
Thematic analysis of data from one hundred and twenty hrs of participant
observation of staff, and eighteen interviews with Clubhouse members and
staff identified ‘Social environment’ and ‘Autonomy support’ as overarching
themes that described how recovery practices were implemented within the
Clubhouse. This chapter describes ‘Social environment’ which included
three sub-themes, ‘community and consistency’, ‘participation and
opportunity’ and ‘respect and autonomy’.
7.2 Publication
The following is from:
Raeburn, T., Schmied, V., Hungerford, C., & Cleary, M. (2016).
Recovery-oriented practice and social environment in a psychosocial
Clubhouse. British Journal of Psychiatry, Open Access, 2(2), 173-178.
The use of social environment in a psychosocialclubhouse to facilitate recovery-oriented practiceToby Raeburn, Virginia Schmied, Catherine Hungerford and Michelle Cleary
BackgroundRecovery-oriented language has been widely adopted inmental health policy; however, little is known about howrecovery practices are implemented within individual services,such as psychosocial clubhouses.
AimsTo explore how recovery practices are implemented in apsychosocial clubhouse.
MethodQualitative case study design informed by self-determinationtheory was utilised. This included 120 h of participantobservation, interviews with 12 clubhouse members and6 staff members. Field notes and interview transcripts weresubject to theoretical thematic analysis.
ResultsTwo overarching themes were identified, each comprisingthree sub-themes. In this paper, the overarching theme of
,
social environment,is discussed. It was characterised by the
sub-themes,
,
community and consistency,,
,
participation andopportunity
,and
,
respect and autonomy,.
ConclusionsSocial environment was used to facilitate recovery-orientedpractice within the clubhouse. Whether recovery is experiencedby clubhouse members in wider society, may well depend onsupports and opportunities outside the clubhouse.
Despite substantial advancements in clinical treatment, people withmental illness continue to endure poor social predicaments,including high rates of stigma, unemployment and homelessness.1–3
Such challenges highlight the importance of delivering mentalhealthcare that addresses both clinical and social needs.4 Inresponse to consumer dissatisfaction with the traditional emphasison symptoms and disability, mental health policy in many countriesnow promotes the concept of personal recovery.5,6
Personal recovery refers to a process of restoring mental healthin accordance with a person’s goals and strengths, enabling pursuitof a satisfying and contributing life, with or without the presence ofcontinued symptoms.7 Interventions that promote personal recov-ery are commonly referred to as recovery-oriented practice. Abroad range of services from both hospital and community sectorshave adopted recovery-oriented practices, and the evaluation ofsuch practices is a growing field of research.5,8–10
The personalised nature of mental health recovery has reinforcedthe apparent pragmatism of many individualised approaches tomental healthcare, such as individual psychotherapy and individua-lised employment support.11 In tandemwith this, however, consumeraccounts commonly emphasise the importance of social environ-ments to their recovery.7 Social environments refer to the groups andneighbourhoods that people live in, the structure of workplaces andconventions that influence how people behave.12 One approach wellknown for its use of social environment and work to facilitaterecovery is the clubhouse model of psychosocial rehabilitation.
The clubhouse model is widely recognised as a pioneer ofrecovery-oriented practice.13 Open to adults with a history of mentalillness, there are over 300 clubhouses worldwide, including 8 in theUK.14 Referring to service participants as ‘members’, clubhousesplace strong emphases on employment, social environment andrecovery.15 For example, an unpaid vocational programme referredto as ‘the work ordered day’ involves members in daily activities,such as running a reception desk, working in a kitchen or clubhousebuilding maintenance. A transitional employment programme(TEP) offers paid semi-independent short-term job placements
with local businesses, encouraging pursuit of independent paidemployment. For members who have secured independent employ-ment but still wish to receive support, there is also an ongoingclubhouse-supported employment programme.16
While most clubhouse studies have been carried out in NorthAmerica, there is a growing body of research being conducted inclubhouses in other countries. For example, studies at clubhousesin South Korea17 and Hong Kong18 have found that participationin clubhouses improves quality of life and reduces psychiatricsymptoms. Because the prerequisite for membership is a historyof mental illness, clubhouses form a meeting place for peoplewith similar experiences, facilitating supportive connectionsand friendships.15 Two other studies at clubhouses in Sweden19
and Australia20 have found that peer support within clubhousescan contribute to improved self-esteem, promoting mental healthrecovery.
This paper reports findings from a qualitative case study thatexplored how recovery-oriented practices were implementedwithin an Australian clubhouse. The study sought to address thefollowing two questions: ‘how are recovery practices perceived bymembers and staff within a psychosocial clubhouse?’ and ‘howare recovery practices embodied in the behaviour of staff?’
Method
Design
Qualitative case study design was selected because of the usefulnessof the approach for elucidating phenomena within their naturalsetting.21 Similar to other qualitative designs, case studies draw onthe data from multiple perspectives – however, they are not boundby a particular theoretical paradigm, instead allowing research to beinformed by whatever theory is relevant to the case.21 This casestudy was informed by a modern theory well suited to recovery-oriented practice research, known as self-determination theory(SDT).22
BJPsych Open (2016)2, 173–178. doi: 10.1192/bjpo.bp.115.002642
A meta-theory of human motivation, SDT posits that humanity hasthree fundamental psychological needs: relatedness, competencyand autonomy, and that the fulfilment of these needs can beinfluenced by social environments.22 ‘Relatedness’ refers to people’sneed for supportive relationships. ‘Competence’ describes people’sdesire to feel a sense of contribution in their community.‘Autonomy’ denotes the importance of freedom and choice.22
Each of these needs is integral to the modern concept of recovery-oriented practice implemented within services such as psychosocialclubhouses.23
Setting
The setting was an Australian psychosocial clubhouse, which isfully accredited with the International Clubhouse Standards, asdisseminated by the original psychosocial clubhouse, known asFountain House, in New York City. Housed in an open-planbuilding, the clubhouse provides programmes to 20–60 people perday. Following the timetable of a typical 5-day working week,activities are delivered from 09:00 h to 17:00 h, Monday–Friday,with occasional social outings on evenings and weekends. Allactivities are free of charge and open to adults over the age of 18with a history of mental illness. Funding is drawn from a varietyof government grants and philanthropic donations.
Ethics
The first author (T.R.) liaised closely with the clubhouse director,staff and members, in order to ensure that all research activity wasaligned with clubhouse expectations of member involvement.24
Institutional consent for the study was secured from the club-house, and approval was granted by a university ethics committeein 2014 (H10711).
Participants and recruitment
All data were collected by T.R. between November 2014 throughto and including January 2015. The study aimed to recruit asample of 10 members for interviews and 5 staff members forparticipant observation and interviews. The study was promotedthrough notice-board advertisements and word of mouth amongmembers to recruit interview volunteers, and among staff, torecruit for both participant observation and interviews. Allparticipants were provided with ethics-approved informationsheets, with completed signed consent required prior toinvolvement.
Participant observation focused on how six clubhouse staffmembers implemented recovery practices and was guided by twofieldwork tools, Spradley’s field note domains,25 and the Recoveryand Promotion Fidelity Scale (RPFS).26 Spradley25 suggests fieldnotes should reflect nine domains, these are outlined in Table 1.Field notes were recorded in relation to each domain, with
reference to the way in which staff embodied the recoverycategories of the RPFS.26 The RPFS provides an empiricallyvalidated instrument for investigating the recovery orientation ofmental health services.27 It divides recovery practices into fivepotential categories: collaboration; participation and acceptance;self-determination and peer support; quality improvement; con-sumer and staff development.26
Interviews with member and staff participants took place in aprivate room in the clubhouse, using questions from the RPFS,26
which reflected the five recovery categories mentioned above. Thequestions addressed topics including but not limited to, memberinvolvement in the clubhouse, how feedback from members andstaff occurred, members’ goals within the clubhouse and howrecovery principles were promoted. Interviews were digitallyrecorded, transcribed and coded, so that participant confidenti-ality was maintained.28
Data analysis
Collected data were subjected to theoretical thematic analysis.29
This meant searching for patterns within the data relevant to theresearch questions and principles of SDT, including relatedness,competency and autonomy. Analyses followed the six-step processsuggested by Braun & Clarke.29
The first step involved immersion in the collected data tobuild familiarity with its meaning, this was achieved by readingand rereading field notes and interview transcripts. Second,initial codes were developed, which involved splitting the datainto pieces (phrases and paragraphs) that communicated parti-cular messages related to the research questions, in light of SDT.For example, as noted in the Results section below, one memberstated:In other services that I′ve been along to, there seems to be much more of a dividebetween staff – often there’d be uniforms or… desks and the person sits on oneside…. (while here) it′s very open and everyone′s sitting around together. (m11W)
This statement was coded as relevant to the research questionsand SDT, because it conveyed a member perspective about thesense of relatedness in the clubhouse.30 Third, similar coded piecesof data were grouped together into themes. Fourth, the themeswere refined and two overarching themes were developed, withthree sub-themes in each. Fifth, points of interest about thethemes were identified and linked together. Finally, a story aboutthe data was produced.
Rigour
In relation to the credibility or authenticity of this qualitativestudy,31 the words of participants were used in the description offindings as much as possible, to strengthen credibility. AdoptingSDT as a theoretical framework, and the RPFS for recoverycategories and interview questions, also improved credibility. Thisis because SDT has been widely researched22 and the RPFS hasbeen empirically validated.26,27 Throughout data collection and
Table 1 Field note application of Spradley’s nine domainsa
Space Locations where observations were recorded. For example, in the art room or cafeteria of the clubhouse.Actors Staff observed and number of members. For example, staff X and staff Y worked with a group of ten members.Activity Events that the actors (staff and members) engaged in. For example, a lunch-time cooking group.Object Physical artefacts present during an activity. For example, food ingredients, stove and other kitchen utensils.Act Individual behaviours that actors engaged in during an activity. For example, how a staff member used a whiteboard to facilitate task allocation
during a cooking group.Event Summary title for groups of activities. For example, a fundraising day.Time Times when periods of observation took place.Goal The apparent intention of actors during activities. For example, staff sought to involve members in food preparation as much as possible.Feeling Emotions conveyed by actors during activities. For example, staff appeared happy when several members volunteered to contribute to the
fundraising day activity.
a. From Spradley.25
Raeburn et al
174
74
analyses, T.R. engaged in regular reviews and discussions with theco-authors, who are all highly experienced qualitative researchers.This approach enhanced reflexivity throughout the study.32
Two overarching themes were developed: ‘social environment’and ‘autonomy support’. The overarching theme of ‘autonomysupport’ is explored in a separate publication.33 The current paperaddresses sub-themes related to the first overarching theme of‘social environment’.
Results
Participants
Research participants were 12 clubhouse members and 6 staffmembers; all study data came entirely from this cohort. Memberparticipants included eight males and four females, with an averageage of 47 years; all reported a diagnosis of either schizophrenia,bipolar disorder or schizoaffective disorder; each had been attend-ing the clubhouse for between 1 and 20 years. Staff participantsincluded two males and four females, with an average age of 39.Each had been working at the clubhouse for between 1 and 7 yearsand had professional qualifications (e.g. occupational therapy, arttherapy and social work).
Themes
The three sub-themes that related to social environment were,‘community and consistency’, ‘participation and opportunity’and ‘respect and autonomy’. Each of these themes will now bediscussed in turn, with direct quotes from field notes prefacedwith the prefix ‘fn’, interview quotes from members with theprefix ‘m’ and interview quotes from staff members with theprefix ‘s’.
Community and consistency
Staff members described the social environment at the clubhouseas being a community that sought to support each member’spersonal recovery journey. This was described by staff withcomments such as:We are a community before we are a service. The critical thing for us is to provide a safeand welcoming environment where members… can come in, belong to and take partin. (s3C)
Likewise, members compared the inclusive, community feel of thesocial environment to their experiences with other services. Forexample:In other services that I
,ve been along to, there seems to be much more of a divide
between staff - often there,d be uniforms or… desks and the person sits on one
side…. (while here) it,s very open and everyone
,s sitting around together. (m11W)
This sense of community-reflected principles is outlined in the 36guiding principles of the organisation, known as the InternationalClubhouse Standards.34 These standards were displayed at recep-tion and in various other places throughout the building, outliningthe purpose of the organisation, the rights of members andproviding guidance for daily activities. The sense of community atthe clubhouse, then, was sustained through the relational routinescrafted to reflect these standards. One such routine was describedin the following field note:Every day begins with a morning meeting of staff and members where a clubhousestandard is read aloud. A reflection and debate between members and staff thenfollows about the relevance of the standard to mental health recovery. (fn5N)
The standards, together with the routine connected to this readingof the standards, provided an important means of building andsupporting the community.
There was also debate however, among members and staff,about the cultural tone of the standards and whether they shouldallow more scope for local innovation. These concerns wereexemplified by comments such as:
The clubhouse model was developed so long ago. We feel there is need for itto evolve. Obviously when the accreditors came they were extremely workfocused, but their culture is American, which is obviously very different – inAustralia it
,s completely different. So I think it
,s important for that to be realised.
But everybody has said it takes a very long time for the clubhouse standards tochange. (s2X)
Concerns about how the standards were implemented had beenhighlighted during the clubhouse’s most recent accreditationprocess. Staff stated:The accreditor didn
,t see the benefit of members going for a walk around lunchtime.
He felt that it distracted from the work order day. But we made the point that inworkplaces people can exercise, and I think if you
,re given those options, you become
more motivated with your work. (s3Y)
Although there were concerns about how concretely the standardsinfluenced practice, the theme of community was further sup-ported by the fact that the only criterion to access the clubhousewas a history of mental illness. Guaranteed acceptance by theclubhouse was highly valued by members, who made commentsduring interviews such as:I was alienated from my family. I lost my support system. I lost my job. I couldn
,t pay
my mortgage. I had debts…The clubhouse was the only support system left wheneverything (was gone)…it′s been very… welcoming. (m6S)
Furthermore, notions of community and consistency continued tobe extended to members on a lifelong basis, no matter how manytimes they needed to access the service:I think the beauty of this model is that because it
,s open, you know you
,re a member
for life, you can transition on as many times as you want. People will transitionthrough and then we won
,t see them for a couple of years and then they
,ll have an
episode and be back in hospital and then they,ll transition out again through
us. (s6N)
The episodic nature of mental illness, and the fact that recovery isseldom a linear process, meant member’s reputation in theirfamily and friendship groups was often vulnerable. Communityand consistency at the clubhouse facilitated an accepting socialenvironment that members could rely on – thereby addressingtheir feelings of vulnerability.
Participation and opportunity
Another important component of the social environment was theopportunity for members to develop a sense of competencythrough participation in work. Members valued the chance tobuild confidence and skills through involvement in a range ofvocational activities. This was illustrated by quotes from inter-views such as:The clubhouse
,s goal is to work. In the sense of – what you decide work is. Is work
keeping well? Is work having a hobby or developing a business? Is work going in andworking in a kitchen? (m1R)
Although voluntary and unpaid, members perceived the voca-tional work activities as holding value other than money. This wasreflected in comments such as:Within the structure of the clubhouse you′ve got your daily work…(which) teachesskills for one… (I) had a lot of difficulty just shopping… but now I can do things. I′m alot more able to do things independently as a result of my time… spent atclubhouse. (m12G)
Many work activities provided opportunities to engage in admin-istrative duties. Some of these were recorded in the field note below:Members engage in a wide range of business related activity groups performingsecretarial/reception duties, writing grant applications and the weekly newsletter.They also publish and fold pamphlets for community groups and organize healthpromotion and fundraising events. (fnD5)
Other opportunities to participate included horticultural workmaintaining the clubhouse’s outdoor gardens. There was also arange of artistic activities for members with creative interests, asnoted below:I like the activities they have on like the art group and the art deco and thewriter
,s group and the drama group. I like to get involved. It helps me get
skills. (m5R)
While members generally enjoyed the participation and opportu-nities on offer, however, there are times that this seemed toengender such comfort within the clubhouse, that some members
The use of social environment in a psychosocial clubhouse
175
75
lost motivation to pursue opportunities in wider society. Thisobservation was reflected in the following statement by staff:Sometimes you
,ll have people that you
,re working with and it
,s actually quite short
term because you sort of can facilitate a lot of stuff and then they move on. It,s a little
more difficult with people I think who have been coming here for the last ten years.That can get a bit more blurry as to what it is you
,re trying to facilitate other than just
being sort of a social club. (s3Z)
Despite this, vocational programmes inside the clubhouse wereconnected to transitional employment support for membersseeking paid employment outside, in the competitive job market.The way this process worked was explained in the followingvignette provided by a staff member:…you
,re giving very practical tasks and showing them how to do them where there is
no sense of failure and then giving them that encouragement that they can do it…I had a man …with extremely high anxiety who… would just sit at the back of thedining room and not talk to anyone at all. I helped him work in the kitchen and then hedid one of those transitional employment positions… where they fulfil manual tasks…That gave him the courage to do a hospitality course… while he was doing it he said,,
I need to learn a bit more cooking,, so he was coming back to the kitchen to cook
once or twice a week. Then he got a job at the kiosk at the hospital and he,s been
there now two and a half years. Now he told me about six months ago he became ateam leader. (s1C)
Step-by-step, then, members were supported to gain confidenceand skills, building a sense of competency in relation to thecontribution they could make to the clubhouse and their widercommunity.
Respect and autonomy
The theme of ‘respect and autonomy’ was observed in the waystaff members encouraged respectful communication and beha-viour among members. A relaxed approach to how members usedthe service was adopted, meaning that while work activities wereconsistent, and participation was encouraged, staff members didnot force members to get involved. Such autonomy was appre-ciated by members who made comments such as:I,m allowed to work wherever I want, whenever I want, yep. That
,s what this
clubhouse is all about. Choice, yep. You have as much choice as you like. (m3G)
In a similar vein, members appreciated the way staff membersrespected their right to opt out of activities when they wanted to.This was reflected in statements such as:I like how you can say no if they ask you to help to work… – it
,s voluntary, you should
be able to say no at any time. (m10S)
Occasionally, however, promotion of autonomy needed to betempered by staff – particularly when individual members beganto speak or act in unsociable ways. Staff members were observedencouraging polite verbal interaction in a gentle but firm way tomaintain a safe social environment. This is highlighted in thefollowing comment made by staff:…they can
,t help it if they hear voices and respond to voices every so often. But if
they swear… because they do, that′s just not on… I just try to catch it and encouragepolite behavior (s3C)
At the same time, staff members were occasionally required tomonitor access to the service; this was exemplified in the followingvignette of an incident observed during participant observation:An inebriated man carrying several bags over his shoulder and a bottle of alcohol inhis hand entered the clubhouse and strode over to a computer station swearingunder his breath. Members working nearby appeared startled by the interruption,dropping their heads and falling silent. A staff member was quick to sense the effectof the man′s behavior and politely asked him to leave. The man replied he had ameeting scheduled for midday. The staff member then explained and reinforced thatthe clubhouse was supposed to be a safe place to work and socialize, negotiating forthe man to return later in the day for his meeting. (fnD7)
Perhaps the importance of respect and autonomy was bestsummed up by a member’s statement below:After hospitalization, if you
,ve had an episode, trusting yourself is something you need,
to rebuild again with confidence, and coming to the clubhouse there is automatic trustin the sense that people feel safe and staff treat you with respect
,(m1R)
The respect and autonomy facilitated by the social environment atthe clubhouse engendered feelings of safety, trust and confidence.By building such feelings, members could continue developing asense of self-determination and personal recovery.
Discussion
This study revealed three sub-themes that suggested socialenvironment was instrumental to the way in which recoverypractices were implemented within a clubhouse. The first sub-theme, ‘community and consistency’, was conveyed by memberand staff descriptions of the clubhouse social environment, asexceeding everyday notions of ‘service provision’. The sense ofcommunity and consistency within the clubhouse was built on aset of values and social routines crafted to reflect the InternationalClubhouse Standards.34 Because it provided a standardisedapproach and attendance was voluntary, the clubhouse tended toattract people amenable to its values. The longer members andstaff had spent within the clubhouse, the more familiar theyappeared to be with the language of the standards, and thisinfluenced how they interacted.
In some respects, the notion of drawing people into a mentalhealth community evoked imagery of traditional institutionalapproaches and ran contrary to more contemporary community-based services, which provide programmes focused on supportingpeople to integrate back into wider society. Despite this, Mandiberg& Warner14 contend that the intransigent social challenges faced bypeople with mental illness throughout history legitimise approachessuch as those used in clubhouses. They argue that because recoveryis a process and not an outcome, people with mental illness requiremore than services alone, and becoming a member of a communitycan restore a sense of identity and belonging, which can contributeto recovery.14
While promoting community and consistency, use of thestandards was open to critique, because they also appeared toconstrain local innovation. Staff members expressed concern thatthe language of the standards, and the way in which they wereinterpreted during accreditation, maintained old-fashioned andenculturated ideas about how work should be conducted. Theyalso reported that effecting any change to the language or tone ofthe standards would take a very long time because any changesrequired formal ratification by the central office of the interna-tional clubhouse movement. While service standards can bebeneficial for promoting purpose within organisations, SDTresearch suggests that overly centralised requirements to adhereto standards can dampen levels of motivation and innovation.22
Despite such concerns, the standards did enable the recoverypractice of quality assurance to be implemented, through theclubhouse accreditation process. This contrasted with concernsraised in other mental health research that recovery practices oftenlack standardisation, making evaluation difficult.8
The second theme, ‘participation and opportunity’, wasimportant because clubhouse members, like many people withmental illness, reported having experienced stigma, unemploy-ment and damage to their reputation, due to their mental illness.1
Importantly, daily work within the clubhouse was the responsi-bility not only of staff but also of members. This meant thatworking together, to keep the clubhouse functioning, automati-cally facilitated recovery practices, like collaboration and accep-tance between members and staff.
Staff members were observed facilitating a range of unpaidvocational work activities, including but not limited to telephonereception duties, managing the clubhouse website, producingmarketing and health promotion materials, horticultural work inthe clubhouse garden and food preparation in the clubhouse cafe.Every job was effectively broken down into achievable, explainabletasks and allocated to members, according to their level of interestand confidence. Viewed through the theoretical lens provided bySDT, such activities, although unpaid, provided a range of
Raeburn et al
176
76
opportunities, through which members could increase skills andconfidence, thereby increasing a sense of competency.
Perhaps the strongest criticism of the clubhouse approach hascome from research focused on models of supported employment,such as individual placement and support (IPS).11 Critics suggestthat facilitating vocational work in comfortable social environ-ments can slow people’s re-entry to paid work in wider society.35
During this study, such concerns appeared valid within theclubhouse, where some members reported having participated invocational activities for many years but were in no hurry to pursuepaid employment.
Quantitative outcome research in other psychosocial serviceshas viewed people who spend years in vocational programmeswithout moving on to paid employment, as struggling torecover.11,36 Such studies highlight the importance of how recoveryis conceptualised by research. Quantitative studies generally assumean outcomes-focused approach that differentiates between socialrecovery, including employment and interpersonal outcomes, andcomplete recovery, focused on symptom reduction.5 Such researchapproaches contrast with the notion of personal recovery, which asmentioned above has been used to describe a process of restoringidentity in the context of community.7,14
The final theme of ‘respect and autonomy’, referred to thetrust and freedom, members were accorded within the clubhouse.Members stated that while engaging and persevering with workactivities were encouraged, participation was not forced on them.They appreciated having the choice to join, or leave work groupsas they wished, or to stop working, and socialise with othermembers when they wanted. Members reciprocated the respectthey were shown by expressing respect for the staff and the rulesof the clubhouse. While firm rules governing safe behaviour, suchas zero tolerance for violence, were observed being enforced bystaff, occasions when this was required appeared rare. The themeof respect and autonomy connected with SDT, which suggests thatwhen people experience freedom to make their own choices, theyrespond by behaving in socially constructive ways and experiencea more satisfying life.22
Limitations
This study involved a single clubhouse and fieldwork wasconducted with a relatively small group of participants, suggestingthat the participation may have appealed more to people with ahigher rate of involvement in the clubhouse. While the studyexplored an accredited clubhouse, there is likely to be variation ininternational clubhouse settings depending on local socioeco-nomic and cultural circumstances. Information collected was alsolimited by using participant observation as a data collectiontechnique. This was because data could only be collected insituations the researcher was physically present to observe.37
Given the wide array of terms used to describe recoveryconcepts in mental health literature, another limitation was therestriction of recovery categories to those identified by the RPFS.26
Also, because of time constraints follow-up interviews withparticipants were not conducted. Such a process may have providedextra data, and guarded against missing points participants viewedas important.31 In relation to SDT, larger multisite research,exploring its use in other contexts and research designs, mayprovide confirmation of its viability for guiding recovery-orientedresearch.
Implications
It is now common for mental health recovery to be conceptualisedas a personal process requiring a broad range of supports.Delivering clinical treatment and addressing social determinantssuch as employment and housing are vital, however restoring
people’s sense of belonging and identity are also important. Thiscase study sought to address how recovery practices were perceivedby members and staff within a psychosocial clubhouse and howrecovery practices were embodied in the behaviour of staff.
Self-determination theory provided a helpful theoretical frame-work for the research, guiding in-depth exploration of recovery-oriented practice. Utilising participant observation and interviews,the study revealed that recovery practices were implemented byusing social environment to facilitate a sense of community,participation and respect. Whether recovery practices experiencedby members within the clubhouse facilitate recovery in widersociety may well depend on links with family, friends and employ-ment opportunities, outside the clubhouse.
Toby Raeburn, RN, MA, Virginia Schmied, RN, RM, PhD, School of Nursing &Midwifery, Western Sydney University, Sydney, NSW, Australia; CatherineHungerford, RN, NP, PhD, FACMHN, School of Nursing, Midwifery, and IndigenousHealth, Faculty of Science, Charles Sturt University, Bathurst, NSW, Australia; MichelleCleary, RN, PhD, School of Health Sciences, University of Tasmania, Sydney, NSW,Australia
Correspondence: Toby Raeburn, School of Nursing & Midwifery, Western SydneyUniversity, Post; 88 Mallet Street, Camperdown NSW 2006, Sydney, NSW, Australia.Email: [email protected]
First received 20 Dec 2015, accepted 11 Mar 2016
References
1 Smith M. Anti-stigma campaigns: time to change. Br J Psychiatry 2013; 202(suppl 55): s49–50.
2 Baggett TP, O’Connell JJ, Singer DE, Rigotti NA. The unmet health care needs ofhomeless adults: a national study. Am J Public Health 2010; 100: 1326–33.
3 Harvey SB, Modini M, Christensen H, Glozier N. Severe mental illness and work:what can we do to maximise the employment opportunities for individuals withpsychosis? Aust N Z J Psychiatry 2013; 47: 421–4.
4 Tew J, Ramon S, Slade M, Bird V, Melton J, Le Boutillier C. Social factors andrecovery from mental health difficulties: a review of the evidence. Br J Soc Work2012; 42: 443–60.
5 Slade M, Leamy M, Bacon F, Janosik M, Le Boutillier C, Williams J, et al.International differences in understanding recovery: systematic review. EpidemiolPsychiatr Sci 2012; 21: 353–64.
6 Tondora J, Miller R, Slade M, Davidson L. Partnering for Recovery in Mental Health:A Practical Guide to Person-Centered Planning. Wiley, 2014.
7 Leamy M, Bird V, Le Boutillier C, Williams J, Slade M. Conceptual framework forpersonal recovery in mental health: systematic review and narrative synthesis.Br J Psychiatry 2011; 199: 445–52.
8 Hungerford C. Recovery as a model of care? Insights from an Australian casestudy. Issues Ment Health Nurs 2014; 35: 156–64.
9 Slade M, Bird V, Clarke E, Le Boutillier C, McCrone P, Macpherson R, et al.Supporting recovery in patients with psychosis through care by community-basedadult mental health teams (REFOCUS): a multisite, cluster, randomised, controlledtrial. Lancet Psychiatry 2015; 2: 503–14.
10 Macpherson R, Pesola F, Leamy M, Bird V, Le Boutillier C, Williams J, et al. TheRelationship between Clinical and Recovery Dimensions of Outcome in MentalHealth. Schizophrenia Research, 2015.
11 Drake R, Bond G, Becker D. Individual Placement and Support: An Evidence-BasedApproach to Supported Employment. Oxford University Press, 2012.
12 Yen IH, Syme SL. The social environment and health: a discussion of theepidemiologic literature. Annu Rev Public Health 1999; 20: 287–308.
13 Dudek KJ, Aquila R. Fountain house and recovery centers. Psychiatr Serv 2012;63: 396.
14 Mandiberg JM, Warner R. Is mainstreaming always the answer? The social andeconomic development of service user communities. Psychiatrist 2013; 37:153–5.
15 Pernice-Duca F, Onaga E. Examining the contribution of social network support tothe recovery process among clubhouse members. Am J Psychiatr Rehabil 2009;12: 1–30.
16 Raeburn T, Halcomb E, Walter G, Cleary M. An overview of the clubhouse modelof psychiatric rehabilitation. Australas Psychiatry 2013; 21: 376–8.
The use of social environment in a psychosocial clubhouse
17 Jung SH, Kim HJ. Perceived stigma and quality of life of individuals diagnosed withschizophrenia and receiving psychiatric rehabilitation services: a comparisonbetween the clubhouse model and a rehabilitation skills training model in SouthKorea. Psychiatr Rehabil J 2012; 35: 460–5.
18 Tsang AWK, Ng RMK, Yip KC. A six-month prospective case-controlled study ofthe effects of the clubhouse rehabilitation model on Chinese patients withchronic schizophrenia. East Asian Arch Psychiatry 2010; 20: 23–30.
19 Schon U-K. The power of identification: peer support in recovery from mentalillness. Scand J Disabil Res 2010; 12: 83–90.
20 Coniglio FD, Hancock N, Ellis A. Peer support within clubhouse: a grounded theorystudy. Community Ment Health J 2010; 48: 153–60.
21 Stake RE. The Art of Case Study Research. Sage, 1995.
22 Deci E, Ryan R. Overview of Self-Determination Theory. Oxford UniversityPress, 2012.
23 Raeburn T, Schmied V, Hungerford C, Cleary M. Self-determination theory: aframework for clubhouse psychosocial rehabilitation research. Issues Ment HealthNurs 2015; 36: 145–51.
24 Horsfall J, Cleary M, Walter G, Hunt GE. Conducting mental health research: keysteps, practicalities, and issues for the early career researcher. Int J Ment HealthNurs 2007; 16 (suppl 1): S1–20.
25 Spradley J. Participant Observation. Holt Rinehart and Winston, 1980.
26 Armstrong N, Steffen J. The recovery promotion fidelity scale: assessing theorganizational promotion of recovery. Community Ment Health J 2009; 45:163–70.
27 Burgess P, Pirkis J, Coombs T, Rosen A. Assessing the value of existing recoverymeasures for routine use in Australian mental health services. Aust N Z JPsychiatry 2011; 45: 267–80.
28 Yin R. Case Study Research: Design and Methods. 4th edn. Sage, 2009.
29 Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol 2006;3: 77–101.
30 Mancini A. Self-determination theory: a framework for the recovery paradigm.Adv Psychiatr Treat 2008; 14: 358–65.
31 Thomas E, Magilvy JK. Qualitative rigor or research validity in qualitative research.J Spec Pediatr Nurs 2011; 16: 151–5.
32 Dowling M. Approaches to reflexivity in qualitative research. Nurse Res 2006; 13:7–21.
33 Raeburn T, Schmied V, Hungerford C, Cleary M. Autonomy support and recoverypractice at a psychosocial clubhouse. Perspect Psychiatr Care. 27 Jan 2016 (epubahead of print).
34 Macias C, Barreira P, Alden M, Boyd J. The ICCD benchmarks for clubhouses: apractical approach to quality improvement in psychiatric rehabilitation. PsychiatrServ 2001; 52: 207–15.
35 Ritsner MS. Handbook of Schizophrenia Spectrum Disorders, Volume III. Ther-apeutic Approaches, Comorbidity, and Outcomes. Springer, 2011.
36 Lim C, Barrio C, Hernandez M, Barragán A, Brekke JS. Recovery from schizo-phrenia in community-based psychosocial rehabilitation settings rates andpredictors. Res Soc Work Pract 2015; 1: 1–14.
37 Schneider Z. Nursing Research: Methods, Critical Appraisal and Utilisation. MosbyPublishers, 2002.
Raeburn et al
178
78
79
7.3 Conclusion
It is now widely accepted that facilitating mental health recovery requires
more than just medical treatment. Considerations such as, social support,
employment and access to services along with a wide range of other social
factors, all have an important role to play. This chapter presented findings
that Clubhouse staff operationalised recovery-oriented practices by
providing a social environment characterised by, ‘community and
consistency’, ‘participation and opportunity’ and ‘respect and autonomy’.
For people who have not experienced mental illness, the idea of
having access to an inclusive, respectful social environment where it is
possible to engage in unpaid work activities may not seem like much. For
members of the Clubhouse however, having access to such an opportunity
meant a great deal. Reflecting the practices found in Clubhouse
documentation, the social environment within the Clubhouse provided a
platform for providing autonomy support to members, as they worked
towards recovery together.
80
CHAPTER 8: AUTONOMY SUPPORT AND
RECOVERY-ORIENTED PRACTICES WITHIN A
CLUBHOUSE
8.1 Introduction
While a social environment has capacity to provide a platform for recovery,
how to conduct personal interactions in a way that implements recovery
oriented practice presents interpersonal challenges. In this, the last findings
chapter, the overarching theme of ‘Autonomy support’, which emerged from
participant observation and interviews, is described. Autonomy support
included three sub-themes. They were, ‘voice cultivating’, ‘talent scouting’
and ‘confidence coaching’.
8.2 Publication
The following is from:
Raeburn, T., Schmied, V., Hungerford, C., & Cleary, M. (2016).
Autonomy support and recovery practice at a psychosocial Clubhouse.
Perspectives in Psychiatric Care (early online, DOI: 10.1111/ppc.12149).
Perspectives in Psychiatric Care ISSN 0031-5990
Autonomy Support and Recovery Practice at a PsychosocialClubhouseToby Raeburn, RN, MA, Virginia Schmied, RN, RM, PhD, Catherine Hungerford, RN, NP, PhD, FACMHN,and Michelle Cleary, RN, PhD
Toby Raeburn, RN, MA, nurse practitioner is a PhD candidate, School of Nursing & Midwifery, Western Sydney University, Sydney, NSW, Australia;Virginia Schmied, RN, RM, PhD, is a Professor, School of Nursing and Midwifery, Western Sydney University, NSW, Australia; Catherine Hungerford,RN, NP, PhD, FACMHN, is a Professor and Head of School, School of Nursing, Midwifery, and Indigenous Health, Faculty of Science, Charles SturtUniversity, NSW, Australia; and Michelle Cleary, RN, PhD, is a Professor of Mental Health Nursing, Faculty of Health, University of Tasmania, Sydney,NSW, Australia
PURPOSE: To explore how recovery practices are embodied in the behavior of staffand implemented by staff and members at a psychosocial clubhouse.DESIGN AND METHODS: Case study design guided 120 hr of participationobservation and 18 interviews at a psychosocial clubhouse. Data were subjected tothematic analysis guided by self-determination theory.FINDINGS: “Autonomy support” emerged as an overarching theme, with threesubthemes: “voice cultivating,” “talent scouting,” and “confidence coaching.”PRACTICE IMPLICATIONS: Autonomy support is an important means ofsupporting the self-determination of clubhouse members. The findings of thisstudy inform the ongoing development of the clubhouse involved and also provideinsights for health services generally in relation to how to implement recovery-oriented practice.
Conflict of interest statementNone for any author.
First Received September 9, 2015; FinalRevision received November 9, 2015; Acceptedfor publication November 30, 2015
doi: 10.1111/ppc.12149
Recovery-oriented practice has been adopted by modernmental health systems worldwide (Hungerford & Kench,2013; Piat, Sabetti, & Bloom, 2010; Ramon, Healy, &Renouf, 2007). This approach holds substantial implicationsfor the way in which staff interact with people livingwith severe mental illness. Empirically validated principlesthat guide recovery-oriented practice include but are notlimited to providing hope, encouraging participation, andpromoting self-determination (Armstrong & Steffen, 2009).However, there has been a lack of research regarding howthese principles are implemented by individual mentalhealth services, which have historically relied on methodsthat empower staff rather than those who seek support(Cleary,Walter, &Hungerford, 2014; NationalMental HealthCommission, 2014). This paper explores how recoveryprinciples are implemented at an individual psychosocialclubhouse.Psychosocial clubhouses provide a collaborative approach
tomental health recovery (Dudek&Aquila, 2012). Followinga typical working week schedule, clubhouses provide peoplewho have a history of mental illness with the opportunityto engage in vocational and supported work programs,alongside paid staff. These programs include, but are notlimited to, business, hospitality, horticultural and social
activities (Raeburn, Halcomb, Walter, & Cleary, 2013).Rather than using traditional healthcare terms such as“patients” or “clients,” people who seek assistance are referredto as “members” of their clubhouse. In this way, an increasedlevel of equality and empowerment is achieved, as peoplewith mental illness are treated not as “recipients” of care,but rather as active and responsible participants (Gregitis,Glacken, Julian, & Underwood, 2010). Over 300 clubhousescurrently provide services in more than 30 nations—thereis limited research, however, focusing on how individualclubhouses put recovery principles into action (Raeburn,Schmied, Hungerford, & Cleary, 2014).Research at clubhouses has mostly been conducted in
North America where the clubhouse model originated, andits use is most prolific. There have also been a variety ofpapers describing clubhouses internationally, in countriessuch as Pakistan (Chaudhry & Mirza, 1983), Sweden(Norman, 2006), China (Tsang, Ng, & Yip, 2010), andAustralia (Coniglio, Hancock, & Ellis, 2010). Researchershave examined a number of issues related to clubhouseprograms. For example, Macias et al. (2006) focusedon clubhouse employment programs, emphasizing thatthey provide both vocational skills training and ongoingsupport once members move into paid employment. Aquila,
Autonomy Support and Recovery Practice at a Psychosocial Clubhouse
Malamud, Sweet, and Kelleher (2006) focused on theintegration of a psychiatry clinic at a clubhouse, suggestingthat integrating access to psychiatry services could providea helpful addition to psychosocial programs. While eachof these studies provided valuable knowledge regarding theefficacy of components of the clubhouse model, they alsohighlight the need for research exploring how emergingtrends in recovery are incorporated by individual clubhouses.This paper is therefore significant because it reports findingsfrom fieldwork conducted as part of a case study (Stake,1995; Yin, 2009) that explored how recovery practices areembodied in the behavior of staff and perceived by membersand staff across all programs within a clubhouse.
Methods
Setting and Design
The study took place at an Australian clubhouse that deliversa range of structured social, educational, and employmentprograms. The service is fully accredited in accordancewith the international clubhouse standards (Moxley, 1993).Approximately 20–60 people with mental illness, such asschizophrenia and bipolar disorder, frequent the clubhouseeach day.A research approach known as instrumental case study
design was adopted. This type of case study has a particularfocus on exploring phenomena and testing theory (Stake,1995). Two questions were considered, “how are recoverypractices embodied in the behaviors of paid staff withina clubhouse?” and “how are recovery practices perceivedas being implemented by the paid staff and members of aclubhouse?” The study was guided by ametatheory of humanmotivation known as “self-determination theory” (SDT;Deci& Ryan, 2012), which has particular relevance to recovery-oriented research (Mancini, 2008). SDT suggests that humanmotivation relies heavily on whether a person’s psychologicalneed for autonomy, competency, and relatedness is supportedby their social environment. Autonomy refers to a senseof freedom and choice, competency to a feeling of havingsomething to contribute to one’s community, and relatednessto the ubiquitous human need for relational support (Deci& Ryan, 2012; Raeburn, Schmied, Hungerford, & Cleary,2015).
Ethics and Recruitment
University Human Research Ethics Committee (HREC)approval was granted in September 2014 (H10711) andinstitutional consent was secured through meeting withthe director, staff, and members of the clubhouse.Participants included 6 paid staff and 12 clubhouse memberswho were recruited through noticeboard advertisementsand word of mouth among members and staff. Information
sheets approved by the HREC were distributed, discussedwith participants, and written consent was obtained.
Data Collection
Data collection was undertaken by the first author during3 months of fieldwork comprising 120 hr of participantobservation and 18 interviews. Participant observationinvolved the researcher observing how six paid staffimplemented recovery practices. Interviews were conductedwith the same 6 paid staff and 12 clubhouse members.During participant observation, the researcher joined staff
as they worked, seeking to blend in and be unobtrusive tonormal activities (Cleary, 2004). While staff were observedinteracting with clubhouse members during this activity,no narrative data were generated from such observationsas this was not the focus of this part of the study.Instead, participation observation involved the researcherfocusing on how recovery practices were embodied in staffbehavior, through common activities, relationships, andservice experiences (Rossman & Rallis, 2011).Observing individual and group behaviors in this way
illuminated the implementation of recovery practices atthe clubhouse from a front line point of view, facilitatinguncovering of meanings people use to make sense ofexperiences at the service (Cleary, Hunt, Horsfall, & Deacon,2011). Field notes, which are a common technique used byresearchers as a tool to collect observations made duringresearch, were recorded during this activity in order tofacilitate reflection and build understanding of how recoverypractices were implemented. The observational frameworkprovided by Spradley (1980) guided this process includingnine dimensions of space, actor, activity, object, act, event,time, goal, and feeling.Interviews were conducted with the same six staff who
were involved in participation observation and 12 members,in a private room at the clubhouse chosen by participants.Interviews were guided by questionnaires from the RecoveryPromotion Fidelity Scale (RPFS; Armstrong & Steffen,2009). The RPFS is a measurement tool identified bythe Australian Mental Health Outcomes ClassificationNetwork (AMHOCN; Burgess, Pirkis, Coombs, & Rosen,2011) as being highly relevant for investigating recoverypractices at Australian-based services (Burgess et al., 2011).AMHOCN found that the RPFS was developed usingappropriate scientific processes in item development andtesting including techniques such as concept mapping,principal components analysis, and factor analysis (Burgesset al., 2011). The scale includes a total of 12 recovery itemscovering 5 recovery principles: collaboration, participationand acceptance, self-determination and peer support,quality improvement, and staff and consumer development(Armstrong & Steffen, 2009).
Autonomy Support and Recovery Practice at a Psychosocial Clubhouse
Analysis
Data were analyzed using theoretical thematic analysis(Braun & Clarke, 2006). Rather than immediatefamiliarization with the data, the first stage involvedthe development of a theoretical frame of reference forthe analysis (Fereday & Muir-Cochrane, 2008) throughfamiliarization with the theory informing the study—in thiscase (Deci & Ryan, 2012). The second stage involved theresearcher analyzing the data—in this case, the recoverypractices at the clubhouse informed by the core principlesof SDT, including autonomy, competency, and relatedness.Analysis then involved coding and development of themesin light of SDT and the relevance of data to implementationof recovery practices at the clubhouse. For example, as notedin “Results” section, one staff commented:
I guess we just allow people to have a voice within theclubhouse sphere which then obviously down the linecan help them continue with that voice outside of theclubhouse as well. (s2R)
When this comment was considered with reference tothe principles of SDT, it was coded as relevant to theimplementation of recovery practices because it representedthe interpretation by staff of how they assist clubhousemembers to greater levels of self-expression. This quality isimportant because it is linked to people’s ability to experienceautonomy and self-determination, important components ofmental health recovery (Mancini, 2008).With close attention being given to points of intersection
between the data and principles of SDT, a cyclical analysisfrom coding through to developing themes was thenundertaken. This process was guided by Braun and Clarke’s(2006) six-step process including data familiarization,generating initial codes, reflection on codes for potentialthemes, refinement of identified themes, describing whatis interesting about the themes, and writing findings. Eachstep was attended to several times over, before the writingof a coherent and logical report was completed (Crawford,Brown, & Majomi, 2008).During analysis, two major, overarching themes emerged;
these were “autonomy support” and “social environment.”The overarching theme of social environment has beenaddressed in another paper (by authors), which is currentlyunder review. The sections that follow describe thesubthemes related to “autonomy support.”
Results
Participants
The group of staff participants was composed of four femalesand two males with an average age of 39 years. They had
been working at the clubhouse for between 1 and 7 years andall held professional qualifications in mental health relatedfields. The group of member participants was made up ofeight males and four females with an average age of 47years. Clubhouse attendance ranged between 1 and 20 yearsand all reported a history of either schizophrenia, bipolardisorder, or schizoaffective disorder, diagnoses typical of thepopulation who attended the clubhouse.Stemming from SDT (Deci & Ryan, 2012), autonomy
support is a contemporary approach to delivering healthcare that suggests people’s health has a greater chance ofimproving if health professionals validate the perspectivesof consumers, provide opportunity for choice, and promotehealthy behavior (Zuroff, Koestner, Moskowitz, McBride, &Bagby, 2012). Autonomy support emerged as an overarchingtheme that captured how staff embodied recovery practices,and how staff and members perceived recovery practices tobe implemented at the clubhouse. This overarching themeincluded the following three subthemes: voice cultivating,talent scouting, and confidence coaching. In the section thatfollows, direct quotes from field notes are preceded by theprefix “fn,” interview quotes frommembers preceded by “m,”and interview quotes from staff by “s.”
Voice Cultivating
“Voice cultivating” referred to the way staff constantlysought to encourage members to express themselves andrealize the value of their opinions. This process reflectedthe recovery principles of participation, acceptance, and self-determination, as explained by a staff member below:
I guess we just allow people to have a voice within theclubhouse sphere which then obviously down the linecan help them continue with that voice outside of theclubhouse as well. (s2R)
Such encouragement to express views and opinionscontrastedwithmembers’ experiences at someother services,where they reported having felt a need to be cautious aboutwhat they said, depending on who their audience was. Thiswas alluded to by one member in the following way:
Being in hospital can be a very isolating experiencebecause you just don’t know what to make of thesituation. Fundamentally, you’re frightened to saythings because of the consequences that might happen.(m12G)
Learning to overcome the effects of such past experiencesand the anxiety of engaging with a new social group meantthat voice cultivating was often a slow process. This wasreflected by member comments such as:
Autonomy Support and Recovery Practice at a Psychosocial Clubhouse
When I first came here I wasn’t very social but now I’mpretty social – it took me a few months to start beingsocial with people. (m5R)
Another way the theme of voice cultivating was evidentat the clubhouse was in the way the organization wasadministered. Members were observed participating inall activities. These included weekly service planningand monthly high-level management meetings. Suchinvolvement was recorded in field notes such as:
Members are involved in every aspect of managementexcept for staff wages – those are taken care of by theDirector. Member involvement in staff performanceevaluations and all management committees isguaranteed. (fn12D)
Members spoke with enthusiasm about their involvementin this flat and inclusive organizational management style asoutlined below:
I’m on the clubhouse advisory board … it meets once amonth, we provide advice on things like the goals,mission statements and things like that. (m9A)
Such involvement facilitated opportunities for membersto build skills through collaboration with staff. Voicecultivating was not limited to self-development activities, italso provided the chance for members to assist others, asreflected by member statements such as:
I’ve had input on hospital visitations in terms ofthrowing a lifeline to other people to help them out ofthe hospital back into the community, and also—in thatrespect I’ve been a consumer representative. (m12G)
Involvement in the organization’s quality assurance cyclewas also consistently encouraged through a mixture ofinformal discussion and formal surveys. This approach wasappreciated by members who stated:
There’s a suggestion box and you can be anonymous.Or you don’t have to be, you can always approach thestaff and say, well how does this work? Should wechange it? It’s totally encouraged, we’re on a very levelplaying field here. (m1R)
With such comments, members expressed a preference forproviding informal verbal feedback as needed.
Talent Scouting
The theme “talent scouting” described how staff sought toidentify member’s interests and strengths and then link themto opportunities to participate in work activities. As one staffmember explained:
My business card says I’m a “mental healthrehabilitation worker” [laughter], but I think I’m morelike a talent scout … suggesting members to have a go,to follow what they’re interested in or good at, and tostick with it. (s3C)
In this way, staff constantly sought to match member’sskills with work opportunities, encouraging them as activeparticipants in the day-to-day work of the service.The need for staff to work as talent scouts was heightened
because programs were deliberately structured to encouragemember involvement. This was observed in the followingfield note:
The clubhouse deliberately employs low numbers ofstaff, at times having as few as 3–4 staff providingprograms to 60 members. This has the effect of makingcompleting necessary work impossible without highmember involvement. (fn3N)
Staff viewed talent scouting as a skill essential tocompleting their day-to-day tasks, as captured by thefollowing remark:
You have to be good at engaging people to make surethat you build relationships so that eventually you havea reliable team that will help you do the work’. (s1C)
Members displayed a variety of employment backgroundssuch as computer technology, hospitality, military, buildingtrade, or financial sector. For some members, talent scoutinginvolved engaging in new activities and learning new skills.For others, it provided opportunity for them to rebuildconfidence in areas they already had previous experience in.For example:
I used to work at a hotel in Sydney … I’m involved inthe kitchen all the time now because they need a goodchef here. Plus just to show some of my experience tothem. (m2S)
Members also exhibited varying degrees ofmotivation andinterest in reentering the paid workforce. Some used theclubhouse as a resource to make a relatively quick transitionback into a paid job. This was reflected by statements such as:
My confidence is pretty good at the moment. … Ithink that next year I’ll be back in the job market. Iactually think that I have a lot to contribute. (m12G)
Other members were not seeking paid employment butstated they found the daily structured programs helpfulfor managing their symptoms of mental illness. This wasexpressed by comments such as:
Autonomy Support and Recovery Practice at a Psychosocial Clubhouse
I come to the Club to meet people and just being able todo something to concentrate. If I don’t concentrate andI don’t do anything the damn demons get me. (m8A)
Talent scouting therefore accepted and respectedmember’s self-determined choices regarding theirinvolvement in and use of programs at the clubhouse.Using this approach, staff sought to personalize work activityto each individual’s interests. Members appreciated thispersonalized approach making comments such as:
What happens is that you aren’t pigeonholed, youaren’t treated as a number, you aren’t treated asanything else but who you are, and the associateddifficulties you might be able to get help with. (m11W)
No matter what stage of their recovery journey, membersdescribed the strength identification and linking process,which took place in the process of talent scouting, as apersonally tailored experience.
Confidence Coaching
“Confidence coaching” captured the way staff inspired,guided, and worked alongside members to build confidence.This theme emerged from the way staff perceived the processof mental health recovery:
I mean the key principles of recovery to me are – it’sjust all about the self-direction and autonomy and theability to sort of choose your own version of recovery –you know and through that learning confidence. (s6N)
Interestingly, the process of facilitating such self-directionseldom involved directly speaking with members abouttheir mental health. Instead, staff interaction associated withconfidence coaching was normally work related:
I don’t probe them and say, how’s your mental illnesstoday? I never ask them questions about their illness.It’s more likely to be work oriented questions like whatdo we need in the kitchen? How’s the pantry looking?(s4R)
It was therefore less about reflecting on member’sexperience of illness and more focused on facilitatinginvolvement in activities that might assist them to build skillsand confidence:
You start building up confidence and with confidencecomes independence – if we’re ticking along really wellthe staff shouldn’t be doing anything without amember involved and also should always just be sort offacilitating as opposed to doing. (s5J)
Confidence coaching also included practical demons-tration and support as staff worked alongside members rolemodeling. This was appreciated by members:
They push but they do it in a really friendly way, not soclinical. They’ll come along with you… Like they’renot just going, ‘Do it, here’s a pamphlet’. They’ll comewith you and show you. (m8A)
Confidence coaching was facilitated through regularrecovery goal setting meetings as described in the followingfield note:
Each staff member has a group of members who theymeet with on a monthly basis for goal setting. Themeetings provide opportunity for staff to assistmembers to map their progress and make future goals.(fn10N)
Members described this as an incremental confidencebuilding exercise:
The staff help me … on the goal-planning sheet wewrite down when we expect to have the goals – webreak up the goals and work out where we’re going todo each step. (m4A)
In this way, confidence coaching included a mixture oftalking, evaluating, and goal setting.A stepped care approach was adopted, offering higher
levels of guidance to members who required it and taperingoff to lower levels of support as higher levels of confidencewas attained. The effect of the process was explained by amember:
I think you learn about becoming empowered, learningto stand on your own two feet … because people thinkyou’re a freak or something if you’ve got a mentalillness. They don’t realise that you’re just like anybodyelse. (m7J)
Confidence coaching therefore complimented voicecultivating and talent scouting, facilitating autonomysupport as members worked toward recovery together.
Discussion
Recovery-oriented principles are widely promoted bymodernmental health policy and are increasingly reflected inthe documentation of services (Raeburn et al., 2014). Thereis a substantial body of work focused on understandingand measuring peoples individual experiences of recoveryfrom mental illness (Lloyd, King, & Moore, 2010; Sklar,Groessl, O’Connell, Davidson, & Aarons, 2013) anda variety of authors have developed recovery-orientedservice measurement tools (Burgess et al., 2011). Despitethis research, it remains unclear how recovery principles
Autonomy Support and Recovery Practice at a Psychosocial Clubhouse
translate into the routine practices of individual psychosocialrehabilitation services such as psychosocial clubhouses(Raeburn et al., 2014).Research guided by SDT exploring healthcare practices at
hospitals andmedical and psychology clinics has highlightedthe importance of a concept called “autonomy support.”Effective autonomy support is characterized by actions thatvalidate the feelings, opinions, and choices of consumers(Williams et al., 2006). At this clubhouse, autonomy supportemerged as an overarching theme that described howrecovery practices were implemented. It included staffefforts in voice cultivating, talent scouting, and confidencecoaching.The process of voice cultivating, whereby staff encouraged
members to express and value their own perspectives, mayseem like common sense. But this does not always occurin healthcare settings, where several studies have indicatedthat encouraging the views of consumers is unusual becausehigher value is often placed on the priorities of staff and theobjectives of services (Cleary et al., 2014; Ng et al., 2012).One example of the positive effects that voice cultivatinghad at the clubhouse was observed in members’ willingnessto offer direct feedback to staff. Although a suggestion boxwas available for anonymous feedback, members stated theypreferred expressing their views verbally to staff because theyfelt confident that their opinions would be acknowledged andresponded to in a timely, appropriate manner.The comfort expressed by members regarding offering
direct feedback appeared to be a consequence of theencouragement and respect offered by staff at the clubhouse.In this context, the relevance of offering mechanisms foranonymous feedback may be questionable within a recoveryframework because in one sense such processes holdpotential to reinforce disproportionate power. For example,operationalizing anonymous feedback normally requires notonly the person offering feedback to be anonymous, butalso the people who have access to the feedback tend to bea small group (usually managers) within an organization.Encouraging the maintenance of small management groupswho have privileged access to certain types of informationmay be perceived as working against recovery principles suchas inclusiveness and collaboration.Organizations that fail to collaborate with staff and
adopt authoritarian management styles generally have anegative effect on employee well-being and struggle withlow productivity (Deci et al., 2001; Stone, Deci, & Ryan,2009). In contrast to such approaches, “talent scouting” at theclubhouse sought to identify members interests and providethem with choice regarding their level of involvement (Ryan,Lynch, Vansteenkiste, & Deci, 2010). Member commentsreflected their perception that their individuality and rightto choose their level of involvement was respected andinteractions between staff and members were not observed
to be controlling or coercive in any way. This approachdiffered considerably with members’ experiences at otherservices, where they reported feeling forced to engage inactivities. By engaging with and supporting the goals ofmembers, the clubhouse therefore stands in contrast withhistorically disempowering practices that have tended topressure people to repress their desires in order to avoidnegative consequences (Sheldon, Williams, & Joiner, 2008).When engaged in “confidence coaching,” staff adopted
a very accepting view of the variety of symptoms thatmembers may experience during any one day. This tendedto limit focus on members’ experiences of mental healthproblems and drive staff toward providing positive practicalassistance in the recovery process. For example, at timesmembers would exhibit episodic thought disorder anddisorganized behavior, but the clubhouse way of assistingthem was not to ask members if they had taken theirmedication or attempt to analyze their thoughts. Instead,while offering compassion and acknowledgment, staff wouldask members about an activity, encourage involvement, andcontinue working alongside them. As such, the clubhousedid not seek to adjust or control members’ thoughts,feelings, or attitudes. Instead, staff tended to be focusedon maintaining respectful communication that encouragedexpression, supported choice, and promoted freedom.
Limitations
Generalizability of these findings is limited because theresearch occurred at a single clubhouse. The study was alsorestricted to a small group of just 18 service participants’meaning that participation may have drawn people withhigher rates of motivation and participation, therebyaffecting results.
Conclusion
SDT is increasingly considered a viable theoreticalframework for informing recovery-oriented practiceresearch. Despite this, few studies have reported findingsoutlining its application to research of recovery practicein psychosocial care. This study found that a conceptderived from other health-related research involving SDTreferred to as “autonomy support” can be used for describinghow recovery practices are implemented at a psychosocialclubhouse.The findings of this study corroborate the applicability of
SDT and autonomy support to recovery-oriented research.The findings will benefit the clubhouse involved and may beuseful for other mental health services considering recovery-oriented practice. In future, a multisite case study thatincorporates several psychosocial clubhouses may be usefulto explore whether autonomy support and the subthemes of
Autonomy Support and Recovery Practice at a Psychosocial Clubhouse
voice cultivating, talent scouting, and confidence coachingare consistent qualities at other clubhouses.
Acknowledgments
No external or intramural fundingwas received for this study.The authors would like to acknowledge and thank the studyparticipants for their support.
References
Aquila, R., Malamud, T., Sweet, T., & Kelleher, J. (2006). The storefront, fountain house, and the rehabilitation alliance.MedscapeGeneral Medicine, 8(3), 67–79.
Armstrong, N., & Steffen, J. (2009). The Recovery PromotionFidelity Scale: Assessing the organizational promotion ofrecovery. Community Mental Health Journal, 45(3), 163–170.
Braun, V., & Clarke, V. (2006). Using thematic analysis inpsychology. Qualitative Research in Psychology, 3(2), 77–101.
Burgess, P., Pirkis, J., Coombs, T., & Rosen, A. (2011). Assessingthe value of existing recovery measures for routine use inAustralian mental health services. Australian and New ZealandJournal of Psychiatry, 45(4), 267–280.
Chaudhry, M. R., & Mirza, L. (1983). Fountain House, Lahore: Aunique experiment in cross cultural collaboration. IndianJournal of Psychiatry, 25(4), 322–327.
Cleary, M. (2004). The realities of mental health nursing in acuteinpatient environments. International Journal of Mental HealthNursing, 13(1), 53–60.
Cleary, M., Hunt, G., Horsfall, J., & Deacon, M. (2011).Ethnographic research into nursing in acute adult mentalhealth units: A review. Issues in Mental Health Nursing, 32(7),424–435.
Cleary, M., Walter, G., & Hungerford, C. (2014). Recovery andthe role of humility: Insights from a case study analysis. Issuesin Mental Health Nursing, 35(2), 108–113.
Coniglio, F., Hancock, D., & Ellis, N. A. (2010). Peer supportwithin clubhouse: A grounded theory study. CommunityMental Health Journal, 48(2), 153–160.
Crawford, P., Brown, B., & Majomi, P. (2008). Professionalidentity in community mental health nursing: A thematicanalysis. International Journal of Nursing Studies, 45(7),1055–1063.
Deci, E., & Ryan, R. (2012). In R. Ryan (Ed.),Motivation,personality, and development within embedded social contexts:An overview of self-determination theory. Oxford, UK: OxfordUniversity Press.
Deci, E., Ryan, R., Gagné, M., Leone, D., Usunov, J., &Kornazheva, B. (2001). Need satisfaction, motivation, andwell-being in the work organizations of a former eastern bloccountry: A cross-cultural study of self-determination.Personality and Social Psychology Bulletin, 27(8), 930–942.
Dudek, K. J., & Aquila, R. (2012). Fountain house and recoverycenters. Psychiatric Services, 63(4), 396.
Fereday, J., & Muir-Cochrane, E. (2008). Demonstrating rigorusing thematic analysis: A hybrid approach of inductive and
deductive coding and theme development. InternationalJournal of Qualitative Methods, 5(1), 80–92.
Gregitis, S., Glacken, J., Julian, C., & Underwood, K. (2010).Comparing working role values of employed and unemployedclubhouse members.Work, 36(1), 39–46.
Hungerford, C., & Kench, P. (2013). The perceptions of healthprofessionals of the implementation of recovery-orientedhealth services: A case study analysis. Journal of Mental HealthTraining, Education and Practice, 8(4), 208–218.
Lloyd, C., King, R., & Moore, L. (2010). Subjective and objectiveindicators of recovery in severe mental illness: Across-sectional study. International Journal of Social Psychiatry,56(3), 220–229.
Macias, C., Rodican, C., Hargreaves, W., Jones, D., Barreira, P., &Wang, Q. (2006). Supported employment outcomes of arandomized controlled trial of ACT and clubhouse models.Psychiatric Services, 57(10), 1406–1415.
Mancini, A. (2008). Self-determination theory: A framework forthe recovery paradigm. Advances in Psychiatric Treatment,14(5), 358–365.
Moxley, D. P. (1993). Clubhouse standards as a programdevelopment tool. Psychosocial Rehabilitation Journal, 17(2),177–183.
National Mental Health Commission. (2014). The national reviewof mental health programmes and services. Sydney: NationalMental Health Commission.
Ng, J., Ntoumanis, N., Thøgersen, C., Deci, E., Ryan, R., Duda, J.,& Williams, G. (2012). Self-determination theory applied tohealth contexts a meta-analysis. Perspectives on PsychologicalScience, 7(4), 325–340.
Norman, C. (2006). The Fountain House movement, analternative rehabilitation model for people with mental healthproblems, members’ descriptions of what works. ScandinavianJournal of Caring Sciences, 20(2), 184–192.
Piat, M., Sabetti, J., & Bloom, D. (2010). The transformation ofmental health services to a recovery-orientated system of care:Canadian decision maker perspectives. International Journal ofSocial Psychiatry, 56(2), 168–177.
Raeburn, T., Halcomb, E., Walter, G., & Cleary, M. (2013). Anoverview of the clubhouse model of psychiatric rehabilitation.Australasian Psychiatry, 21(4), 376–378.
Raeburn, T., Schmied, V., Hungerford, C., & Cleary, M. (2014).Clubhouse model of psychiatric rehabilitation: How isrecovery reflected in documentation? International Journal ofMental Health Nursing, 23, 389–397.
Raeburn, T., Schmied, V., Hungerford, C., & Cleary, M. (2015).Self-determination theory: A framework for clubhousepsychosocial rehabilitation research. Issues in Mental HealthNursing, 36, 145–151.
Ramon, S., Healy, B., & Renouf, N. (2007). Recovery from mentalillness as an emergent concept and practice in Australia andthe UK. International Journal of Social Psychiatry, 53(2), 108–122.
Rossman, G. B., & Rallis, S. F. (2011). Learning in the field: Anintroduction to qualitative research. Thousand Oaks, CA: Sage.
Autonomy Support and Recovery Practice at a Psychosocial Clubhouse
Ryan, R. M., Lynch, M. F., Vansteenkiste, M., & Deci, E. L. (2010).Motivation and autonomy in counseling, psychotherapy, andbehavior change: A look at theory and practice. CounselingPsychologist, 39(2), 193–260.
Sheldon, K. M., Williams, G., & Joiner, T. (2008).Self-determination theory in the clinic: Motivating physical andmental health. New Haven, CT: Yale University Press.
Sklar, M., Groessl, E., O’Connell, M., Davidson, L., & Aarons, G.(2013). Instruments for measuring mental health recovery: Asystematic review. Clinical Psychology Review, 33(8),1082–1095.
Spradley, J. (1980). Participant observation. New York: HoltRinehart and Winston.
Stake, R. E. (1995). The art of case study research. Thousand Oaks,CA: Sage.
Stone, D. N., Deci, E. L., & Ryan, R. M. (2009). Beyond talk:Creating autonomous motivation through self-determinationtheory. Journal of General Management, 34(3), 75–91.
Tsang, A. W. K., Ng, R. M. K., & Yip, K. C. (2010). A six-monthprospective case-controlled study of the effects of theclubhouse rehabilitation model on Chinese patients withchronic schizophrenia. East Asian Archives of Psychiatry, 20(1),23–30.
Williams, G., McGregor, H., Sharp, D., Levesque, C.,Kouides, R., Ryan, R., & Deci, E. (2006). Testing aself-determination theory intervention for motivatingtobacco cessation: Supporting autonomy andcompetence in a clinical trial. Health Psychology, 25(1),91–101.
Yin, R. (2009). Case study research: Design and methods (Vol. 5,4th ed.). Thousand Oaks, CA: Sage.
Zuroff, D. C., Koestner, R., Moskowitz, D., McBride, C., & Bagby,R. M. (2012). Therapist’s autonomy support and patient’sself-criticism predict motivation during brief treatments fordepression. Journal of Social and Clinical Psychology, 31(9),903–932.