Die 5-Well Schale von Minitüb ist wieder erhältlich!
Nach einer kurzen Pause bietet Minitüb ab sofort die bewährte 5-Well- Schale wieder an. Die Kulturschale wird in Deutschland aus hochwertigem Rohstoff hergestellt. Jede Charge durchläuft nach der Produktion eine strenge Validierung in mehreren Schritten (Mausembryo-
Test, Endotoxin-Test, Bioburden-Test), bevor sie freigegeben wird.
Die Minitüb 5-Well-Schale bietet Ihnen mehrere Vorteile: – Vertiefungen mit großem Durchmes-
ser (19 anstatt der üblichen 16 mm)
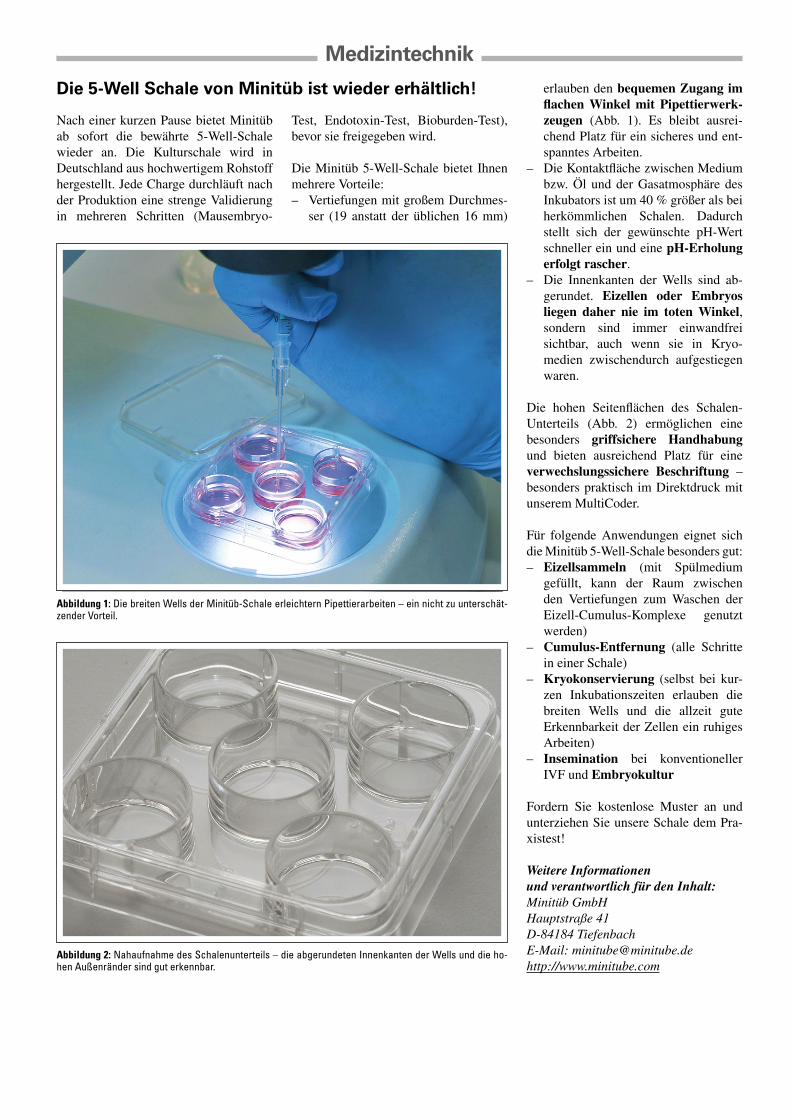
erlauben den bequemen Zugang im flachen Winkel mit Pipettierwerk-zeugen (Abb. 1). Es bleibt ausrei-chend Platz für ein sicheres und ent-spanntes Arbeiten.
– Die Kontaktfläche zwischen Medium bzw. Öl und der Gasatmosphäre des Inkubators ist um 40 % größer als bei herkömmlichen Schalen. Dadurch stellt sich der gewünschte pH-Wert schneller ein und eine pH-Erholung erfolgt rascher.
– Die Innenkanten der Wells sind ab-gerundet. Eizellen oder Embryos liegen daher nie im toten Winkel, sondern sind immer einwandfrei sichtbar, auch wenn sie in Kryo-medien zwischendurch aufgestiegen waren.
Die hohen Seitenflächen des Schalen-Unterteils (Abb. 2) ermöglichen eine besonders griffsichere Handhabung und bieten ausreichend Platz für eine verwechslungssichere Beschriftung – besonders praktisch im Direktdruck mit unserem MultiCoder.
Für folgende Anwendungen eignet sich die Minitüb 5-Well-Schale besonders gut: – Eizellsammeln (mit Spülmedium
gefüllt, kann der Raum zwischen den Vertiefungen zum Waschen der Eizell-Cumulus-Komplexe genutzt werden)
– Cumulus-Entfernung (alle Schritte in einer Schale)
– Kryokonservierung (selbst bei kur-zen Inkubationszeiten erlauben die breiten Wells und die allzeit gute Erkennbarkeit der Zellen ein ruhiges Arbeiten)
– Insemination bei konventioneller IVF und Embryokultur
Fordern Sie kostenlose Muster an und unterziehen Sie unsere Schale dem Pra-xistest!
Weitere Informationen und verantwortlich für den Inhalt:Minitüb GmbHHauptstraße 41D-84184 TiefenbachE-Mail: [email protected]://www.minitube.com
Abbildung 2: Nahaufnahme des Schalenunterteils – die abgerundeten Innenkanten der Wells und die ho-hen Außenränder sind gut erkennbar.
Abbildung 1: Die breiten Wells der Minitüb-Schale erleichtern Pipettierarbeiten – ein nicht zu unterschät-zender Vorteil.
Recurrent Spontaneous Abortions – An Update onDiagnosis and Management
S. Pildner von Steinburg, K. T. M. Schneider
Recurrent spontaneous abortions (RSA), defined as three or more consecutive miscarriages, affect 1 % of couples trying to conceive. Risk of abortion is15 % in every pregnancy, increasing with the number of previous miscarriages. While 50–70 % of sporadic abortions are attributed to chromosomaldefects, mostly trisomies, in RSA there are different underlying disorders of uterine, genetic, infectious, endocrine, immune or thrombophilic etiology,but about 25–40 % are of still unknown etiology. While specific therapy for uterine, infectious, and endocrine disorders may be applied, treatmentoptions for some immunologic and thrombophilic disturbances are still under examination. Careful counseling must be offered to patients with RSAof unknown etiology, as not all treatment options widely offered are based on sufficient evidence yet. J Reproduktionsmed Endokrinol 2009; 6 (1):11–6.
Received: January 2, 2009; accepted after revision: January 21, 2009.From the Abteilung Perinatalmedizin, Frauenklinik und Poliklinik der Technischen Universität München, Klinikum rechts der Isar, GermanyCorrespondence: Dr. med. Stephanie Pildner von Steinburg, Abteilung Perinatalmedizin, Frauenklinik und Poliklinik der Technischen Universität München, Klinikum rechts derIsar, D-81675 München, Ismaninger Straße 22; e-mail: [email protected]
Introduction
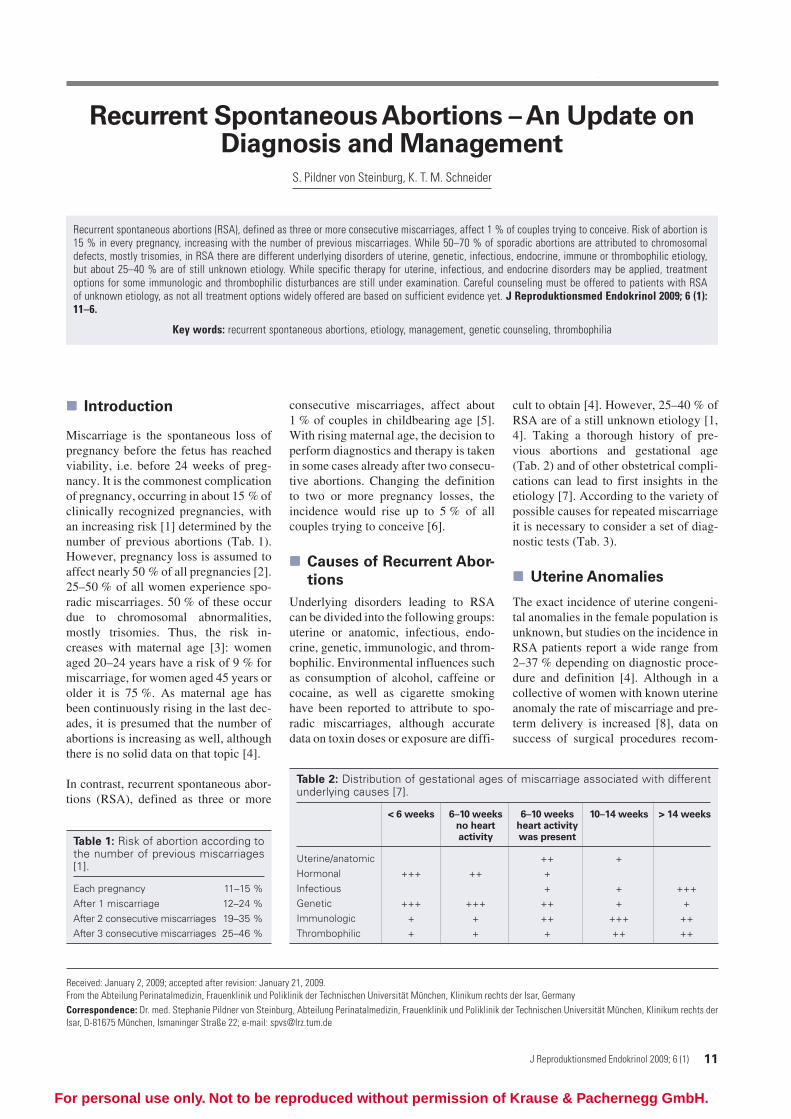
Miscarriage is the spontaneous loss ofpregnancy before the fetus has reachedviability, i.e. before 24 weeks of preg-nancy. It is the commonest complicationof pregnancy, occurring in about 15 % ofclinically recognized pregnancies, withan increasing risk [1] determined by thenumber of previous abortions (Tab. 1).However, pregnancy loss is assumed toaffect nearly 50 % of all pregnancies [2].25–50 % of all women experience spo-radic miscarriages. 50 % of these occurdue to chromosomal abnormalities,mostly trisomies. Thus, the risk in-creases with maternal age [3]: womenaged 20–24 years have a risk of 9 % formiscarriage, for women aged 45 years orolder it is 75 %. As maternal age hasbeen continuously rising in the last dec-ades, it is presumed that the number ofabortions is increasing as well, althoughthere is no solid data on that topic [4].
In contrast, recurrent spontaneous abor-tions (RSA), defined as three or more
consecutive miscarriages, affect about1 % of couples in childbearing age [5].With rising maternal age, the decision toperform diagnostics and therapy is takenin some cases already after two consecu-tive abortions. Changing the definitionto two or more pregnancy losses, theincidence would rise up to 5 % of allcouples trying to conceive [6].
Causes of Recurrent Abor-
tions
Underlying disorders leading to RSAcan be divided into the following groups:uterine or anatomic, infectious, endo-crine, genetic, immunologic, and throm-bophilic. Environmental influences suchas consumption of alcohol, caffeine orcocaine, as well as cigarette smokinghave been reported to attribute to spo-radic miscarriages, although accuratedata on toxin doses or exposure are diffi-
cult to obtain [4]. However, 25–40 % ofRSA are of a still unknown etiology [1,4]. Taking a thorough history of pre-vious abortions and gestational age(Tab. 2) and of other obstetrical compli-cations can lead to first insights in theetiology [7]. According to the variety ofpossible causes for repeated miscarriageit is necessary to consider a set of diag-nostic tests (Tab. 3).
Uterine Anomalies
The exact incidence of uterine congeni-tal anomalies in the female population isunknown, but studies on the incidence inRSA patients report a wide range from2–37 % depending on diagnostic proce-dure and definition [4]. Although in acollective of women with known uterineanomaly the rate of miscarriage and pre-term delivery is increased [8], data onsuccess of surgical procedures recom-
Table 2: Distribution of gestational ages of miscarriage associated with differentunderlying causes [7].
For personal use only. Not to be reproduced without permission of Krause & Pachernegg GmbH.
12 J Reproduktionsmed Endokrinol 2009; 6 (1)
Recurrent Spontaneous Abortions
mended have not been the focus of arandomized study.
At least 30 % of women aged 35 years orolder show uterine fibroids. Intramurallyor submucosally located fibroids areoften assumed responsible for IVF fail-ure or early pregnancy loss and hystero-scopic resection of submucosal fibroidsis recommended, although evidence forthis recommendation is incomplete [9].
The Asherman syndrome, i.e. partial orcomplete obliteration of the uterine cav-ity due to traumatic lesion of the endo-metrium, occurs in two thirds of the re-ported cases after surgical evacuation ofthe uterus for miscarriage or terminationof pregnancy [10]. The prevalence of theAsherman syndrome is unknown as aconsequence of different awareness anddiagnostic equipment of physicians.Hysteroscopic adhesiolysis is the treat-ment of choice, with better pregnancyrates than with expectant management,although high recurrence rates are de-scribed [10].
Infections
Uterine infections as a cause for recur-rent spontaneous abortions in the firsttrimester are discussed controversially.As infections with chlamydia, urea-plasma, and mycoplasma are diagnosedmore often in women with RSA, manyexperts screen for these infections al-though there is no data that treatmentimproves pregnancy outcomes [1]. Re-peated second-trimester fetal losses fol-
lowing cervical dilatation or rupture ofmembranes can be attributed in manycases to bacterial infections, as well asearly preterm delivery. These patientsshould be screened for bacterial vaginalinfections and treated – if treatment iscarried out before 20 weeks of gestation,it succeeds in preventing pretermdelivery, as shown by a recent Cochranemeta-analysis [11]. In some Germancenters, a surgical procedure, a total cer-vix occlusion established by E. Saling(described in [12]), is applied success-fully in these cases [13], although thereare no randomized studies on this topic.
Endocrine Disorders
Many endocrine disturbances have beenassumed to be responsible for RSA. Glu-cose metabolism, thyroid hormones, andsex hormones have been the target formany studies. If insulin-dependent dia-betes is well-controlled, there is no riskfor RSA or for congenital malformations[14]. But in diabetic women with highlevels of blood glucose and glycosylatedhemoglobin during the first trimester therisk for abortion is significantly in-creased [14]. Thyroid antibodies, espe-cially thyroperoxidase (TPO) antibod-ies, have been associated with abortionsbut not with RSA, and therapeutic inter-ventions besides corrections in hormonemetabolism have to be further investi-gated [15].
The luteal phase defect has long beenthought to be a cause of abortion, but theevidence linking the luteal phase defectto recurrent abortion is subject to criti-cism and their association remains specu-lative. Hyperprolactinemia is found to beassociated with RSA and treatment withbromocriptine significantly improveslive birth rates [16]. Despite many stud-ies on the prevalence of PCOS in recur-rent miscarriage, the extent to whichPCOS contributes to recurrent miscar-riage remains highly uncertain due todifferent definitions used. Some evi-dence suggests that weight loss, ovariandrilling and metformin could help to re-duce the rate of miscarriage [17].
Genetic Disorders
As mentioned above, 50–70 % of spo-radic abortions are due to genetic disor-ders. In women with RSA, the rate ofkaryotypic abnormalities is much lower.
The most common aberrant karyotypesare autosomal trisomies (up to 60 %), ofwhich trisomy 16 is the most frequent,monosomy X (up to 20 %), polyploidy(up to 20 %) and structural anomalies(4 %). However, the earlier pregnancyloss occurs, the higher is the percentageof genetic anomalies: 90 % in anembry-onic specimen, 50 % between 8 and 11gestational weeks and approximately30 % at 16–19 gestational weeks [7].
Detection of aneuploidy in abortusspecimens increases the probability ofaneuploidy in a following miscarriage:after abortion with detection of a trisomyin the specimen the risk for the same(homotrisomy) or a different trisomy(heterotrisomy) is increased. For indi-vidual risk assessment the knowledge ofthe type of trisomy and the maternal ageare crucial, concerning all women witheither spontaneous or recurrent abor-tions [18].
In 3–5 % of couples with RSA, one part-ner shows a balanced chromosome rear-rangement, more likely the mother [7].In these phenotypically normal parents,separation of chromosomes duringmeiosis may lead to an abnormal numberof copies of chromosomal segments,causing partial trisomy or monosomy inthe offspring. In couples with one ormore early miscarriages plus one childstillborn or born with congenital malfor-mation, the rate of chromosomal struc-tural anomaly found in one partner risesup to 5.4 %. This probability is approxi-mately 10 %, if a couple has had one ormore early abortions and if there arerelatives with further abortions or mal-formed children [18].
Also, microdeletions or single gene dis-orders may influence pregnancy out-come. Consanguinity increases the riskfor these conditions. Alpha thalassemiamajor is an example of a single-gene dis-order, leading to repeated pregnancy loss[7]. Inherited thrombophilic mutationsare discussed in the respective chapter.
As a consequence, thorough geneticcounseling with a family history of atleast three generations and karyotypingof the partners should be part of the diag-nostic procedures for RSA. Informationavailable from cytogenetic testing ofabortus specimens enables more detailedgenetic counseling, independent from
Table 3: Diagnostic test proposed forpatients/couples presenting with RSA
• Pelvic ultrasound scan; where neces-sary hysteroscopy*
• Early follicular-phase FSH, luteal-phaseLH and progesterone
• TSH, TPO antibodies, oral glucose toler-ance test
• Cervical swabs for (atypical) bacteria*• Peripheral blood karyotype for both
partners• Antiphospholipid antibodies and lupus
anticoagulant• Factor V Leiden and prothrombin muta-
tion, protein C, protein S• Factor VIII, factor XII, polymorphisms of
MTHFR, PAI-1, ACE*• Where applicable karyotyping of abor-
tus specimen*
* optional
Recurrent Spontaneous Abortions
J Reproduktionsmed Endokrinol 2009; 6 (1) 13
the number of prior miscarriages. Forexample, a woman under 30 years of agewith a history of one miscarriage due totrisomy bears an increased risk for tri-somy in the next pregnancy and requiresprenatal counseling or diagnostic proce-dures.
Immunologic Disorders
Pregnancy is an extraordinary challengeto the maternal immune system allowingthe only partially identical fetus to grow.In recent publications, a cooperative in-teraction between the maternal immunesystem and fetal antigens to establishthis allogenic unresponsiveness has beendiscussed [19]. Natural killer cells in themucosal layer of the uterus have beenimplicated in this immune tolerance andit is widely hypothesized that distur-bance of this immune tolerance may beinvolved in RSA, but mechanisms arenot fully understood [20]. However, al-though many studies with differenttherapeutic concepts (e. g. paternal lym-phocytes, intravenous immunoglobines)have addressed this topic, no consistentevidence has been established. A recentmeta-analysis found intravenous immu-noglobines not to significantly increaselive birth rates when compared with pla-cebo for treatment of recurrent miscar-riage (OR 1.28; 95 %-CI: 0.78–2.10).Effects reported in secondary RSA baseon a very small number of patients [21].
In general, maternal autoimmune disor-ders except for systemic lupus erythema-tosus improve during pregnancy. Apartfrom that, antiphospholipid syndrome(APS) often is only diagnosed on thebasis of miscarriages. It is defined bydetection of antiphospholipid antibodies(including lupus anticoagulant and anti-cardiolipin antibodies) and one of thefollowing clinical symptoms: arterial orvenous thrombosis, three or more unex-plained miscarriages before 10 weeks,one or more unexplained fetal deathsafter 10 weeks or one preterm deliverybefore 34 weeks associated with severepreeclampsia or growth retardation. Itaccounts for nearly 15–20 % of RSA.Although many different therapeuticregimens have been used, only a combi-nation of heparin and aspirin was provento be effective in a meta-analysis [22].Low molecular heparin is widely usednow, although not many data exist on itsuse. The biggest study using LMW
heparin up to now showed a successfulpregnancy outcome in 89 %, including98 APS patients [23].
Thrombophilic Disorders
Pregnancy adaptations early lead tohypercoagulability, to prevent bleedingduring establishment of the hemochorialplacenta. Thrombosis of placental vas-culature in cases of mothers with pre-ex-isting thrombophilia was thought to beresponsible for miscarriage. But in thelast years, experiments with thrombo-modulin-deficient mice reported tissuefactor-dependent activation of bloodcoagulation directly causing cell deathand inhibiting growth of trophoblastcells (summarised in [24]).
Known inherited risk factors of venousor arterial thromboembolism are defi-ciencies of antithrombin, protein C andprotein S, factor V Leiden and pro-thrombin 20210A mutations, mildhyperhomocysteinemia, elevated levelsof factor VIII, and factor XII deficiency.
Association of the above mentionedthrombophilic disorders with adverse
pregnancy outcome have been subject tostudies since the 1990ies. Table 4 sum-marizes the frequencies of genetic disor-ders in a healthy population [25–27] andresults of recent meta-analyses concern-ing association with RSA [24, 28, 29].
As mentioned above, hyperhomocys-teinemia is a predisposition to thrombo-philia. Hyperhomocysteinemia may beinduced by malnutrition with folic aciddeficiency, potentially caused by a fastfood diet. Another quite common co-factor is a variant in the MTHFR gene(Tab. 4), a C-to-T substitution at cDNAposition 677, which may lead to an in-creased level of plasma homocysteine.Although initial studies suggested an as-sociation between homozygosity forMTHFR C677T itself and RSA, a meta-analysis could not confirm such an asso-ciation [28]. But 23 % of the white popu-lation show a combined heterozygosityfor C677T and another known polymor-phism of the MTHFR gene, A1298C[30]. It has been shown that this com-pound heterozygosity for C677T andA1298C, but not homozygosity forA1298C alone, is associated with in-creased fasting and post-methionine
Table 4: Frequency of thrombophilic disorders [25–27] and association with RSAfrom meta-analyses of case-control studies [24, 28, 29]. Definition of first trimesterRSA varies between studies.
Frequency inGenetic healthy population/
Thrombophilia mechanism frequency of genes Association with RSA
OR = odds ratio; 95 %-CI: 95 % confidence interval
14 J Reproduktionsmed Endokrinol 2009; 6 (1)
Recurrent Spontaneous Abortions
load homocysteine plasma levels [30]and with recurrent pregnancy loss [31,32]. In all these variants, homocysteinelevels usually stay within normal rangeif sufficient folic acid substitution is ap-plied. Thus, such a predisposition couldbe missed when no genetic testing hasbeen performed. Therefore, the regularfolic acid intake is essential especiallyfor carriers of a predisposing MTHFRgenotype.
Buchholz et al report that homozygosityfor the D allele of the angiotensin-con-verting enzyme (ACE) gene, which re-sults in elevated plasminogen activatorinhibitor- (PAI-) 1 concentrations andhypofibrinolysis, is associated with anelevated risk of RSA; and the combina-tion of the D/D ACE genotype with two4G alleles of the PAI-1 promoter, whichfurther increases PAI-1 plasma levels,is significantly more frequent in RSApatients compared with controls [33].
There is also an association of some ofthe thrombophilic disorders mentionedabove (factor V and prothrombin muta-tion, protein C, protein S and antithrom-bin deficiency, PAI-1 and MTHFR poly-morphism) with obstetric complicationslater in pregnancy, as late fetal loss, pre-eclampsia and fetal growth retardation[24]. This implicates that careful coun-seling of patients concerned and man-agement of high-risk pregnancies in co-operation with specialized centers isnecessary.
Management
A proposed set of diagnostic tests forRSA patients is summarized in Table 3.If diagnostic testing suggests infectiousor endocrine causes for RSA, specifictreatment should be applied. The ex-pected success rates of surgical proce-dures because of uterine anomalies haveto be discussed with the couple, and ifapplicable pre-implantation testing maybe offered.
It is important to understand that – inde-pendent of the therapeutic managementoffered – the overall miscarriage ratecannot decrease below about 15 %, com-prising genetic or nidation failures. Fur-thermore, about one third of coupleswith a history of three consecutive mis-carriages have lost pregnancies purelyby chance alone, due to sporadic fetal
aneuploidy. Such couples have a 75-%-chance of a successful pregnancy nexttime with no therapeutic intervention[4].
Progesterone
In a recent Cochrane meta-analysis [34],a subgroup analysis of three trials in-volving women who had recurrent mis-carriages (three or more consecutivemiscarriages), progesterone treatmentshowed a statistically significant de-crease in miscarriage rates compared toplacebo or no treatment (OR 0.38; 95 %-CI: 0.20–0.70). But no evidence wasestablished to support the routine use ofprogesterone to prevent sporadic miscar-riage in early to mid-pregnancy.
Aspirin
In APS, a combination of heparin andaspirin was proven to be effective in ameta-analysis [22]. In patients withknown thrombophilic predisposition ofvarious etiologies (Factor V or pro-thrombin mutation, protein S defi-ciency), Gris et al reported significantlyhigher live birth rates in the group ofwomen treated with heparin alone com-pared those treated with aspirin alone– which showed a live birth rate of 29 %comparable to untreated women [35].Concerning this result, other authorsraised methodological concerns becauseof inclusion in the trial not before the8th week of pregnancy and the ran-domization procedure [24]. However, alater trial with a similar study designconfirmed the results [36].
On the contrary, the only interventionstudy concerning factor XII deficiencyand RSA was performed with aspirin,showing reduced miscarriage rates, butincluded only a small number of patients[37].
Heparin
It seems obvious that heparin is thetherapy of choice for prevention ofrecurrent miscarriage in patients withthrombophilia. However, no placebo-controlled, randomized studies confirmthis hypothesis. In the study by Gris et al,the live birth rate was 23 out of 80women (29 %) in the aspirin group ver-sus 69 out of 80 (86 %) in the enoxaparingroup in patients with known thrombo-
philic predisposition [35]. In another co-hort study with patients with hereditarythrombophilia and RSA, 26 of the 37pregnancies (70 %) in heparin-treatedpatients resulted in live births, comparedwith 21 of 48 (44 %) in untreated pa-tients (OR 3.03; 95 %-CI: 1.12–8.36).The beneficial effect was seen mainlyin women with no previous live births(OR 9.75; 95 %-CI: 1.59–52.48) [38]. AGerman observational study, the ETHiGtrial, designed for assessment of lowmolecular weight heparin efficacy forprophylaxis of thromboembolism, in-cluded 810 pregnant women with priorthrombosis or hereditary thrombophilia.Of the 272 pregnants starting dalteparinbefore 12 weeks of gestation, 270 (99 %)had a history of prior miscarriage, butshowed under therapy with dalteparinonly 31 (11 %) pregnancy losses [39].The LIVE-ENOX trial randomized fortwo different doses of enoxaparin (40and 80 mg) for treatment of women withinherited thrombophilia and showed nodifference in live birth rates (84 % and78 %, respectively) [40]. Critics arguethat in many reports the prognosis ofwomen with RSA is good and do notsupport general recommendations forthe use of heparin for RSA in womenwith thrombophilia, without well-de-signed randomized trials available [24].Thus, it is necessary to understand thatheparin for RSA in women with throm-bophilia is widely used but evidence isnot sufficient yet. However, Germanguidelines for RSA recommend treat-ment of women with thrombophilia withheparin [41].
First evidence for the use of heparin forRSA of unknown etiology came from atrial by Tzafettas et al who comparedpregnancy outcome of two groups ofwomen with a history of two or moremiscarriages, 24 with known and 27 withexcluded thrombophilia. Both groupswere treated with heparin and aspirin,and similar live birth rates of 83.3 %and 85.1 % were reported [42]. How-ever, a recently published study investi-gated pregnancy outcome of 340 womenwith unexplained recurrent pregnancyloss randomized either to treatment withenoxaparin and folic acid or folic acidalone [43]. The rates of early miscarriageof 4.1 % vs. 8.8 %, respectively, wereregarded as a significant effect of lowmolecular weight heparin, but are verylow in comparison to other studies. An-
Recurrent Spontaneous Abortions
J Reproduktionsmed Endokrinol 2009; 6 (1) 15
other recently published, prospective,randomized trial compared treatmentof 160 women with RSA of unknownetiology with enoxaparin alone or pred-nisone, aspirin and progesterone or pla-cebo [44]. They reported live birth ratesof 81 %, 85 % and 42 %, respectively,showing efficacy of treatment. A Ger-man study, the ETHiG II trial, is stillrecruiting [45]. It was designed to in-clude a sufficient number of patients fora randomized placebo-controlled treat-ment, to strengthen evidence and answersome of the still open questions.
Psychological Support
Since the 1980ies it is known that dedi-cated care may beneficially influencepregnancy outcome in patients with un-explained recurrent miscarriage. Regu-lar specific antenatal counseling andpsychological support during the firsttrimester in women with three or moreconsecutive abortions led to a live birthrate of 86 % as compared to a successrate of 33 % observed in women whowere given no specific antenatal care[46]. Thus, success of the above-men-
Practical Aspects
• Recurrent spontaneous abortions have to be considered as a multi-causal con-dition, with genetic fetal or parental chromosomal abnormalities, anatomic,infectious, endocrine, immunologic, and thrombophilic factors playing a rolein its etiology.
• If diagnostic testing suggests infectious or endocrine etiology, specific treat-ment should be applied; surgical procedures may be offered for uterine anoma-lies.
• Patients with antiphospholipid syndrome should receive a combination of hep-arin and aspirin, patients with inherited thrombophilia in the majority of casesheparin, although evidence is incomplete.
• For RSA of unknown etiology, heparin is suggested to be effective, ran-domised studies are still in progress; dedicated care may beneficially influencepregnancy outcomes as well.
• However, independent of the therapeutic management offered, the overall mis-carriage rate cannot decrease.
tioned interventions has to be testedagainst tender loving care before evi-dence-based decisions can be taken.
Summary
Recurrent spontaneous abortions have tobe considered as a multi-causal condi-tion, with genetic fetal or parental chro-mosomal abnormalities, anatomic, in-fectious, endocrine, immunologic, andthrombophilic factors playing a role intheir etiology, which are not mutuallyexclusive. A set of diagnostic tests forRSA patients is proposed. If diagnostictesting suggests infectious or endocrinecauses for RSA, specific treatmentshould be applied. Surgical proceduresmay be offered for uterine anomalies.There is evidence for the use of proges-terone in RSA. Patients with antiphos-pholipid syndrome should receive acombination of heparin and aspirin,patients with inherited thrombophilia inthe majority of cases heparin, althoughevidence is incomplete. For RSA ofunknown etiology, heparin is suggestedto be effective, randomized studies arestill in progress.
References:
1. Marzusch M, Pildner von Steinburg S. Frühschwanger-schaft: Klinische Aspekte. In: Schneider H, Husslein P,Schneider KTM (Hrsg). Die Geburtshilfe. 3. Aufl. SpringerMedizin Verlag, Heidelberg, 2006; 18–9.
2. Wilcox AJ, Weinberg CR, O’Connor JF, Baird DD, SchlattererJP, Canfield RE, Armstrong EG, Nisula BC. Incidence of earlyloss of pregnancy. N Engl J Med 1988; 319: 189–94.
3. Nybo Andersen AM, Wohlfahrt J, Christens P, Olsen J,Melbye M. Maternal age and fetal loss: population basedregister linkage study. Br Med J 2000; 320: 1708–12.
4. Rai R, Regan L. Recurrent miscarriage. Lancet 2006; 368:601–11.
6. Hogge WA, Byrnes AL, Lanasa MC, Surti U. The clinical useof karyotyping spontaneous abortions. Am J Obstet Gynecol2003; 189: 397–400.
7. Warren JE, Silver RM. Genetics of pregnancy loss. ClinObstet Gynecol 2008; 51: 84–95.
8. Grimbizis GF, Camus M, Tarlatzis BC, Bontis JN, Devroey P.Clinical implications of uterine malformations and hystero-scopic treatment results. Hum Reprod Update 2001; 7: 161–74.
9. Li TC, Makris M, Tomsu M, Tuckerman E, Laird S. Recurrentmiscarriage: aetiology, management and prognosis. HumReprod Update 2002; 8: 463–81.
10. Yu D, Wong YM, Cheong Y, Xia E, Li TC. Asherman syn-drome – one century later. Fertil Steril 2008; 89: 759–79.
11. McDonald HM, Brocklehurst P, Gordon A. Antibiotics fortreating bacterial vaginosis in pregnancy. Cochrane DatabaseSyst Rev 2007 (1): CD000262.
12. Artmann A, Schuchardt R, Gnirs J, Schelling M, SchneiderKTM. Der totale Muttermundverschluss – eine effizienteMaßnahme bei prolabierender Fruchtblase im Bereich derextremen Frühgeburtlichkeit? Zeitschr Gebh Neonat 2001; 4:143–6.
13. Odoj A, Schneider KTM, Pildner von Steinburg S. Verschluss-operationen am Muttermund – eine retrospektive Auswertungüber 11 Jahre. Geburtsh Frauenheilk 2008; 68 (Suppl 1): S92;DOI: 10.1055/s-0028-1088944. Abstract.
14. Rosenn B, Miodovnik M, Combs CA, Khoury J, Siddiqi TA.Glycemic thresholds for spontaneous abortion and congenitalmalformations in insulin-dependent diabetes mellitus. ObstetGynecol 1994; 84: 515–20.
16. Hirahara F, Andoh N, Sawai K, Hirabuki T, Uemura T,Minaguchi H. Hyperprolactinemic recurrent miscarriage andresults of randomised bromocriptine treatment trials. FertilSteril 1998; 70: 246–52.
17. Cocksedge KA, Li TC, Saravelos SH, Metwally M. A reap-praisal of the role of polycystic ovary syndrome in recurrentmiscarriage. Reprod Biomed Online 2008; 17: 151–60.
18. Wieacker P, Hehr U, Gromoll J, Ludwig M. Empfehlungenzur genetischen Diagnostik bei Aborten. [Recommendationsfor Genetic Diagnostics in Abortions.] J ReproduktionsmedEndokrinol 2005; 2: 148–50.
19. Moffett-King A. Natural killer cells and pregnancy. Nat RevImmunol 2002; 2: 656–63.
20. Shimada S, Kato EH, Morikawa M, Iwabuchi K, Nishida R,Kishi R, Onoé K, Minakami H, Yamada H. No difference innatural killer or natural killer T-cell population, but aberrantT-helper cell population in the endometrium of women withrepeated miscarriage. Hum Reprod 2004; 19: 1018–24.
21. Hutton B, Sharma R, Fergusson D, Tinmouth A, Hebert P,Jamieson J, Walker M. Use of intravenous immunoglobulinfor treatment of recurrent miscarriage: a systematic review.Br J Obstet Gynaecol 2007; 114: 134–42.
22. Empson M, Lassere M, Craig JC, Scott JR. Recurrent preg-nancy loss with antiphospholipid antibody: a systematic re-view of therapeutic trials. Obstet Gynecol 2002; 99: 135–44.
23. Schleussner E, Thaler CJ, Fischer T, Bauersachs R.Dalteparin und ASS 100 zur Therapie des Antiphospholipid-Syndroms (APS): Ergebnisse der ETHiG I Studie. GeburtshFrauenheilk 2008; 68 (Suppl 1); DOI: 10.1055/s-0028-1088653.Abstract.
24. Middeldorp S. Thrombophilia and pregnancy complications:cause or association? J Thromb Haemost 2007; 5 (Suppl 1):276–82.
25. Bogdanova N, Markoff A. Genetic Predispositions to Throm-bophilia Associated with Recurrent Pregnancy Loss. J Repro-duktionsmed Endokrinol 2008; 5: 101–5.
26. Kluijtmans LA, den Heijer M, Reitsma PH, Heil SG, BlomHJ, Rosendaal FR. Thermolabile methylenetetrahydrofolatereductase and factor V Leiden in the risk of deep-vein throm-bosis. Thromb Haemost 1998; 79: 254–8.
27. Jood K, Ladenvall P, Tjärnlund-Wolf A, Ladenvall C,Andersson M, Nilsson S, Blomstrand C, Jern C. Fibrinolyticgene polymorphism and ischemic stroke. Stroke 2005; 36:2077–81.
28. Rey E, Kahn SR, David M, Shrier I. Thrombophilic disordersand fetal loss: a meta-analysis. Lancet 2003; 361: 901–8.
29. Sotiriadis A, Makrigiannakis A, Stefos T, Paraskevaidis E,Kalantaridou SN. Fibrinolytic defects and recurrent miscar-riage: a systematic review and meta-analysis. Obstet Gynecol2007; 109: 1146–55.
30. Hanson NQ, Aras O, Yang F, Tsai MY. C677T and A1298Cpolymorphisms of the methylentetrahydrofolate reductasegene: incidence and effect of combined genotypes on plasmafasting and post-methionine load homocysteine in vasculardisease. Clin Chem 2001; 47: 661–6.
31. Goodman CS, Coulam CB, Jeyendran RS, Acosta VA,Roussev R. Which thrombophilic gene mutations are risk fac-tors for recurrent pregnancy loss? Am J Reprod Immun 2006;56: 230–6.
32. Subrt I, Ulvova-Gallova Z, Bibkova K, Micanova Z, HejnalovaM, Cerna M, Hradecky L, Novotny Z. Recurrent pregnancy lossand frequency of eight antiphospholipid antibodies and genetic
16 J Reproduktionsmed Endokrinol 2009; 6 (1)
Recurrent Spontaneous Abortions
thrombophilic factors in Czech women. Am J Reprod Immun2008; 59: 193–200.
33. Buchholz T, Lohse P, Rogenhofer N, Kosian E, Pihusch R,Thaler CJ. Polymorphisms in the ACE and PAI-1 genes areassociated with recurrent spontaneous miscarriages. HumReprod 2003; 18: 2473–7.
34. Haas DM, Ramsey PS. Progestogen for preventing miscar-riage. Cochrane Database Syst Rev 2008 (2): CD003511.
35. Gris JC, Mercier E, Quéré I, Lavigne-Lissalde G, Cochery-Nouvellon E, Hoffet M, Ripart-Neveu S, Tailland ML, DauzatM, Marès P. Low-molecular-weight heparin vs. low-dose aspi-rin in women with one fetal loss and a constitutional thrombo-philic disorder. Blood 2004; 103: 3695–9.
36. Dendrinos S, Kalogirou I, Makrakis E, Theodoridis T,Mahmound EA, Christopoulou-Cokkinou V, Creatsas G. Safetyand effectiveness of tinzaparin sodium in the management ofrecurrent pregnancy loss. Clin Exp Obstet Gynecol 2007; 34:143–5.
37. Ogasawara MS, Iinuma Y, Aoki K, Katano K, Ozaki Y,Suzumori K. Low-dose aspirin is effective for treatment of
recurrent miscarriage in patients with decreased coagulationfactor XII. Fertil Steril 2001; 76: 203–4.
38. Carp H, Dolitzky M, Inbal A. Thromboprophylaxis improvesthe live birth rate in women with consecutive recurrent mis-carriages and hereditary thrombophilia. J Thromb Haemost2003; 1: 433–8.
39. Bauersachs RM, Dudenhausen J, Faridi A, Fischer T, FungS, Geisen U, Harenberg J, Herchenhan E, Keller F, Kemkes-Matthes B, Schinzel H, Spannagl M, Thaler CJ. Risk stratifica-tion and heparin prophylaxis to prevent venous thromboembo-lism in pregnant women. Thromb Haemost 2007; 98: 1237–45.
40. Brenner B, Hoffman R, Carp H, Dulitsky M, Younis J. Effi-cacy and safety of two doses of enoxaparin in women withthrombophilia and recurrent pregnancy loss: the LIVE-ENOXstudy. J Thromb Haemost 2005; 3: 227–9.
41. Deutsche Gesellschaft für Gynäkologie und Geburtshilfe.Leitlinien, Empfehlungen, Stellungnahmen. Diagnostik undTherapie beim wiederholten Spontanabort. AWMF 015/050(S1), 2008.
42. Tzafettas J, Petropoulos P, Psarra A, Delkos D, PapaloukasC, Giannoulis H, Kalogiros G, Gkoutzioulis F. Early antiplateletand antithrombotic therapy in patients with a history of recur-rent miscarriages of known and unknown aetiology. Eur JObstet Gynecol Reprod Biol 2005; 120: 22–6.
43. Badawy AM, Khiary M, Sherif LS, Hassan M, Ragab A,Abdelall I. Low-molecular weight heparin in patients withrecurrent early miscarriages of unknown aetiology. J ObstetGynaecol 2008; 28: 280–4.
44. Fawzy M, Shokeir T, El-Tatongy M, Warda O, El-RefaieyAA, Mosbah A. Treatment options and pregnancy outcome inwomen with idiopathic recurrent miscarriage: a randomizedplacebo-controlled study. Arch Gynecol Obstet 2008; 278: 33–8.
45. The ETHiG II trial group; http://www.ethig2.de (letzterZugriff: 02.02.2009)
46. Stray-Pedersen B, Stray-Pedersen S. Etiologic factors andsubsequent reproductive performance in 195 couples with aprior history of habitual abortion. Am J Obstet Gynecol 1984;148: 140–6.
Haftungsausschluss
Die in unseren Webseiten publizierten Informationen richten sich ausschließlich an geprüfte und autorisierte medizinische Berufsgruppen und entbinden nicht von der ärztlichen Sorg-faltspflicht sowie von einer ausführlichen Patientenaufklärung über therapeutische Optionen und deren Wirkungen bzw. Nebenwirkungen. Die entsprechenden Angaben werden von den Autoren mit der größten Sorgfalt recherchiert und zusammengestellt. Die angegebenen Do-sierungen sind im Einzelfall anhand der Fachinformationen zu überprüfen. Weder die Autoren, noch die tragenden Gesellschaften noch der Verlag übernehmen irgendwelche Haftungsan-sprüche.
e-Journal-AboBeziehen Sie die elektronischen Ausgaben dieser Zeitschrift hier.
Die Lieferung umfasst 4–5 Ausgaben pro Jahr zzgl. allfälliger Sonderhefte.
Unsere e-Journale stehen als PDF-Datei zur Verfügung und sind auf den meisten der markt-üblichen e-Book-Readern, Tablets sowie auf iPad funktionsfähig.
Bestellung e-Journal-Abo
Haftungsausschluss
Die in unseren Webseiten publizierten Informationen richten sich ausschließlich an geprüfte und autorisierte medizinische Berufsgruppen und entbinden nicht von der ärztlichen Sorg-faltspflicht sowie von einer ausführlichen Patientenaufklärung über therapeutische Optionen und deren Wirkungen bzw. Nebenwirkungen. Die entsprechenden Angaben werden von den Autoren mit der größten Sorgfalt recherchiert und zusammengestellt. Die angegebenen Do-sierungen sind im Einzelfall anhand der Fachinformationen zu überprüfen. Weder die Autoren, noch die tragenden Gesellschaften noch der Verlag übernehmen irgendwelche Haftungs-ansprüche.
e-Journal-AboBeziehen Sie die elektronischen Ausgaben dieser Zeitschrift hier.
Die Lieferung umfasst 4–5 Ausgaben pro Jahr zzgl. allfälliger Sonderhefte.
Unsere e-Journale stehen als PDF-Datei zur Verfügung und sind auf den meisten der markt-üblichen e-Book-Readern, Tablets sowie auf iPad funktionsfähig.
Bestellung e-Journal-Abo
Besuchen Sie unsere Rubrik
Medizintechnik-Produkte
InControl 1050 Labotect GmbH
Aspirator 3 Labotect GmbH
Philips Azurion: Innovative Bildgebungslösung
Neues CRT-D Implantat Intica 7 HF-T QP von Biotronik