22
Radio surgical treatment of cranial lesions; Refining the art Mohamed Abdulla M.D. Prof. of Clinical Oncology Kasr Al-Aini School of Medicine Cairo University.
| Date post: | 07-Aug-2015 |
| Category: |
Health & Medicine |
| Upload: | mohamed-abdulla |
| View: | 69 times |
| Download: | 0 times |

Radio surgical treatment of cranial lesions; Refining the art
Mohamed Abdulla M.D.Prof. of Clinical Oncology
Kasr Al-Aini School of MedicineCairo University.

Current View in 2015:
• Basic Definition by Leksell:“The delivery of a single high dose of irradiation to a small and critically located intracranial volume through the intact skull”
• Improvements of Pre-requisites of Application: 1. Neuroimaging.2. Neuroanatomy.3. Reliable radiation therapy delivery system.
• Achievements:1. Better understanding of radiobiological considerations.2. Introduction of more reliable radiation therapy devices.3. Extension to fractionated treatment (Extra-cranial targets).4. Dose/Volume constraints for normal tissues (OAR).

New Insights of SRS Radiobiology:
IR DNA Double Strand Breaks Variable Cellular Abilities of Repair Radiosensitivity.5Rs of Radiobiology:1. Repair.2. Redistribution.3. Repopulation.4. Reoxygenation.5. Radiosensitivity
Withers HR. The four R’s of radiotherapy. In: Lett JT AH, editor. Advances in Radiation Biology, Vol 5. New York: Academic Press; 1975. p. 241-271. Steel GG, McMillan TJ, Peacock JH. The 5Rs of radiobiology. Int J Radiat Biol 1989;56:1045-1048.
New Insights of SRS Radiobiology:
Radiobiological Effect of Single Fraction (> 10 Gy):1. Endothelial cell Damage Cytotoxicity & Apoptosis.2. Vascular Damage at High Doses ++ 2nd Cell Killing.3. Enhanced Anti-Tumor Immunity after Tumor Irradiation.4. Tumor Hypoxia is of Less Importance.
Fuks Z, Kolesnick R. Engaging the vascular component of the tumor response. Cancer Cell 2005;8:89-91.Clement JJ, Tanaka N, Song CW. Tumor reoxygenation and post- irradiation vascular changes. Radiology 1978;127:799-803. Hiniker SM, Chen DS, Knox SJ. Abscopal effect in a patient with melanoma. N Engl J Med 2012;366:2035. author reply 2035-2036.

• Brain is a late responding tissue; @/β = 2.• Radiobiological Classification of Cranial Targets:
1. Late responding target embedded in late responding tissues: AVM.
2. Late Responding target surrounded by late responding tissues: AN.
3. Early responding target embedded in late responding tissue: Low Grade Glioma.
4. Early responding target surrounded by late responding tissue: GBM and High Grade Glioma.
New Insights of SRSRadiobiological Complexity of Cranial Targets:
International Journal of Radiation Oncology Biology Physics, vol. 25, no. 3, pp. 557–561, 1993.
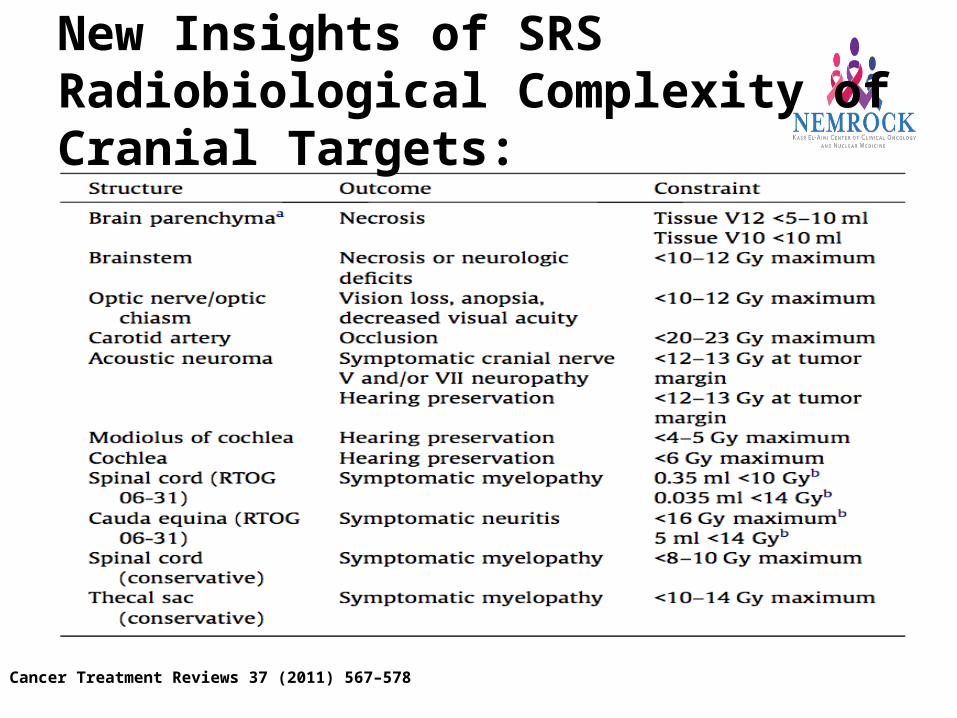
New Insights of SRSRadiobiological Complexity of Cranial Targets:
Cancer Treatment Reviews 37 (2011) 567–578

Gamma-Knife
LA based SRS Systems
BrainLAB Novalis Trilogy Tomotherapy
CyberKnife
Radiosurgery Tools:

Gamma knife
• Gamma-knife: 201 Cobalt source
• Only for intracranial lesions
• Rigid/ fixed frame required
• Single fraction treatment

Gamma-knifeIndications
- Small Meningiomas (<3 cm)
- Small acuastic schwannoma (<3 cm)
- Solitary / oligo brain metastasis with controlled primary (RPA Class I)
- Small residual LGG
- AVMs (<3 cm)
- Trigeminal neuralgia (Functional disorder)
More than 40 years experience / results with Gamma-Knife

CyberKnife: Unique propertiesHighly precise treatment delivery
Motion management
method Tumour tracking
‘Dose painting’
Excellent dose distribution
Fractionation schedule
No rigid fixation

‘CyberKnife is an extension of Gamma-Knife’ CK & GK: Similarity
- Principles of ‘field arrangement’
- Dose distribution pattern
- Multiple isocentre
-Treatment principles
- Treatment delivery accuracy similar
- Delivered dose in single fractions
- Intra-cranial indications
Hence, all the indications of GK are indications of CK also

CyberknifeIndications for single fraction treatment as
Gamma-Knife- Small Meningiomas (<3 cm)
- Small acuastic schwannoma (<3 cm)
- Solitary / oligo brain metastasis with controlled primary
- Small residual LGG
- AVMs (<3 cm)
- Trigeminal neuralgia
- Rec High grade glioma
- Craniopharyngioma
- Pituitary tumour
More than 40 years experience / results with Gamma-Knife

Cyberknife Vs Gamma-Knife: DissimilarityGK CK Comments
Immobilization device
RT source
Rigid frame
Co60
Orfit
6MV
LA
CK has favorable orfit
GK need to replace sources every 5/6 yrs
Favorable dosimetry in CK
Even neurosurgeons can plan in GK
GK: more dose heterogeniety
Radiobiology favorable in CK
Increased indications with CK
Plannin
g Planning
method
No complex
planning Simple
Inverse
planning
ComplexIsodose prescription
Fractions
Tumour size
Usually
50% Single
Only smaller lesions canbe treated
Usually 80-95%
May treat multiple fraction
Larger lesions also can be treated in fractionated schedule
Electricity
Possible
Energy source
Verificatio
n
Radiation
Not possible
GK can work with less electricity
Even Intra-fraction movement
canbe corrected
CK more economical
Indications Only brain lesions Both extra & intra cranial

Cyberknife Vs Gamma-Knife: DissimilarityAdvantage of Inverse planning
GK planning
CK planning
Dose to mesial temporal lobe & Choclea is higher with GK Mean dose to mesial temporal lobe >6 Gy with SRS: IQ decline
Romanalli, Lancet 2009

Cyberknife Vs Gamma-Knife Vs X-Knife:CK: Accuracy similar with Gamma-Knife
Treatment delivery accuracy: GK: ~1 mm
CK : ~1 mmLA based SRS: 1-2 mm (iso-
centric inacurracy; LUTZ test)
PTV margin:CK: <1 mmGK: <1 mmLA based SRS: 1-2 mm GK/CK LA based SRS
CK has the accuracy of GK and flexibility of LA based SRS

fSRSExtended Indications for multiple fraction treatment
- Larger meningiomas (>3 cm)
- Larger acuastic schwannoma (>3 cm)
- Large solitary / oligo brain metastasis with controlled primary
- Larger residual LGG
- AVMs (>3 cm)- Chordomas
- Rec HCC
- Craniopharyngioma
- Pituitary tumour
Short term data with robotic radiosurgery

Volumetric Modulated Arc Therapy
• Rotational IMRT Technique.• Highly conformal dose distribution with better
sparing of OAR.• Dose Modulation: Gantry movements, dose
rate, beam aperture.• Shorter treatment time and MU.• SRS & SBRT for cranial and body lesions.
Medical Dosimetry 40 (2015) 3–8

SRS and Brain Metastases:Current Status:• SRS is highly effective in local control of single and
multiple metastatic lesions.• Even for radioresistant tumors (melanoma &
Kidney).• No technical superiority.• Doses usually > 18 Gy in single sessions.• Lesions > 8 – 10 cc Resection first.• GK is equally effective as surgery for smaller lesions.• Re-irradiation is possible.
B. Lippitz et al. / Cancer Treatment Reviews 40 (2014) 48–59

SRS and Brain Metastases:Current Status:
Int J Radiation Oncol Biol Phys, Vol. 91, No. 4, pp. 710e717, 2015

Patients < 50 Years and 1 – 4 lesions Survival advantage for SRS alone, with no effect on distant brain relapse.
SRS and Brain Metastases:Current Status:
Int J Radiation Oncol Biol Phys, Vol. 91, No. 4, pp. 710e717, 2015
Take Home Message:
• The art of RS is continuously evolving.• Better understanding of radiobiology.• Better technologies of radiation therapy
delivery.• The conventional approach for management
of metastatic brain disease has been changed dramatically in the past 2 years WBRT can be omitted in selected patients.

Thank You

















