Region IV and Region VI Infant Mortality Summit January 12-13, 2012 New Orleans Belinda Pettiford, MPH NC Division of Public Health, Women’s Health Branch Sarah Verbiest, DrPH, MSW, MPH University of NC at Chapel Hill, Center for Maternal and Infant Health Working Together to Improve Birth Outcomes in North Carolina
Transcript
Region IV and Region VI Infant Mortal i ty SummitJanuary 12-13, 2012
New Orleans
Bel inda Pett i ford, MPHNC Divis ion of Publ ic Health, Women’s Health
Branch
Sarah Verbiest , DrPH, MSW, MPHUniversi ty of NC at Chapel Hi l l , Center for
Maternal and Infant Health
Working Together to Improve Birth Outcomes in North Carolina
Thanks to our amazing partners! Women, men, and families! NC Child Fatality Task Force Division of Medical Assistance (Medicaid) UNC Center for Maternal and Infant Health NC Community Health Center Association NC Healthy Start Foundation Community Care of North Carolina Perinatal Quality Collaborative of NC NC Chapter of March of Dimes Division of Mental Health, Dev. Disabilities, and Substance
Abuse Svs. NC Medical, Pediatric, and NC OB/GYN Societies NC Academy of Family Practice Local health departments, local CCNC networks, and other
providers Numerous universities, colleges, faith entities, and CBOs And the Division of Public Health (home of Title V and
OMHHD) and many more!
A society's infant mortality rate is considered an important indicator of its health, because infant mortality is associated with socioeconomic status, access to health care, and the health status of women of childbearing age. (Congressional Budget Office, 1992)
Every day, two babies die in North Carolina
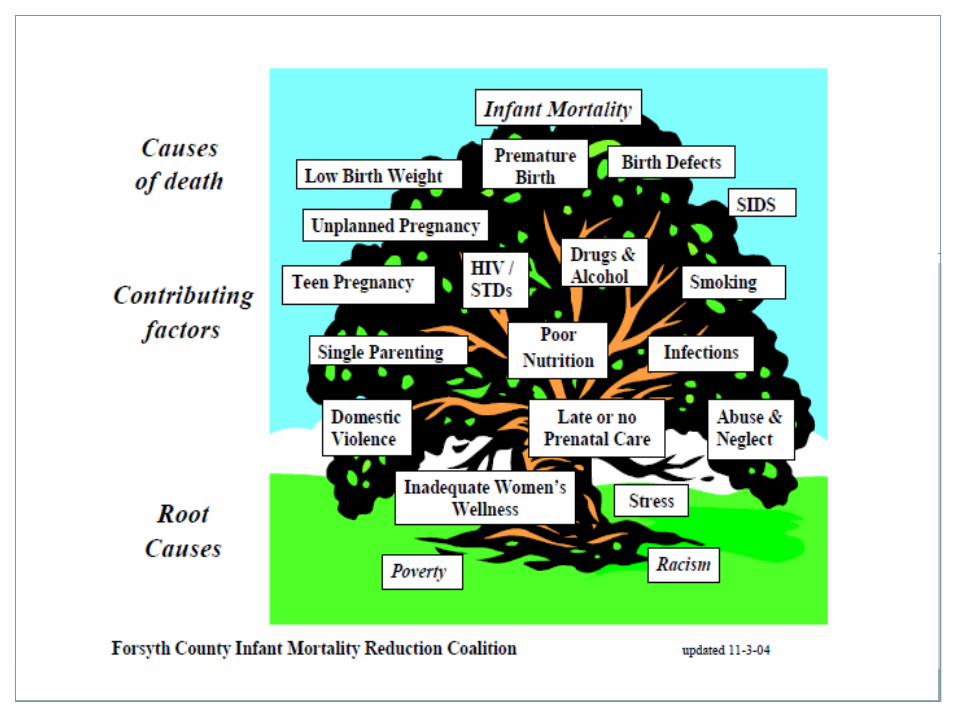
Leading Causes of Infant Mortality
LOW BIRTH WEIGHTPREMATURITY
PERINATAL CONDITIONS RELATED TO MATERNAL HEALTH
BIRTH DEFECTSSUDDEN INFANT DEATH SYNDROME (SIDS)
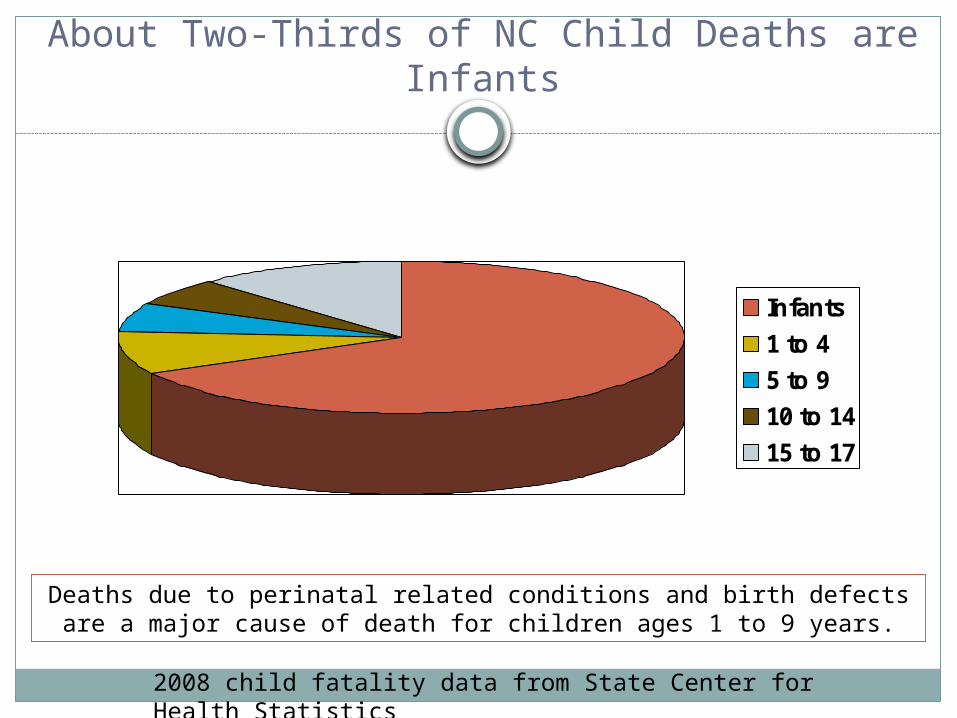
About Two-Thirds of NC Child Deaths are Infants
Infants
1 to 4
5 to 9
10 to 14
15 to 17
2008 child fatality data from State Center for Health Statistics
Deaths due to perinatal related conditions and birth defects are a major cause of death for children ages 1 to 9 years.
Racial Distribution of North Carolina Live Births, 2010
There were 122,302 births in NC; 3.5% decrease from 2009.
Approximately 24% of live births in North Carolina were to African Americans, 71% to Whites, and 5% to other races.
While nearly 16% of NC live births are to women who report an Hispanic ethnicity, most of these Hispanic births are counted in the White racial category, according to NCHS vital statistics coding rules.
Infant Mortality Rate North Carolina, 1988-2010
0
5
10
15
20
25
1988 1991 1994 1997 2000 2003 2006 2009
Af. Am. White
Data Review
o In 1988, NC’s overall IM rate was 12.5 per 1000 live births; the 2nd highest in the country.
o The downward trend in the NC infant mortality rates has slowed since the mid-1990s, then fluctuated between 8.1 and 8.8 between 2000 and 2008. NC’s IM rate was at an all time low in 2010 (7.0 per 1000 live births); 44% reduction since 1988.
o The largest decrease in 2010 was among non-Hispanic African American (19.6% reduction); NH White IMR declined 3.6%.
o Racial disparities in IMR remain, with African American NH continuing to have an IMR more than two times (2.3) higher than White NH.
Data Review
The neonatal mortality rate (deaths occurring during the first 28 days of life) decreased 7.5% overall in 2010; there were substantial differences between whites and minorities. The White NH rate increased slightly (2.9%) while the African American NH rate decreased 14.0% (after showing a 13.8% increase the previous year). The Hispanic rate decreased 13.6% after showing a 4.8 percent increase the previous year.
The post-neonatal mortality rate (28 days to one year) declined 19.2% overall in 2010, with White NH showing a decline of 10.5%, African American NH a decline of 30.8%, and Hispanics a decline of 15.4%.
Birth Weight Data
The percentage of infants delivered very low birthweight (less than 1500 grams) remained about the same in 2010 (1.7% in 2010 compared to 1.8% in 2009).
However, NH African American women experience markedly higher rates of low and very low birthweight births (14.1%) than did NH White (7.8%) and Hispanics (6.3%).
The percentage of babies that were delivered by Cesarean section decreased slightly to 31.4% -- down from 31.7% in 2009.
Birth Weight Trends
In 2010, more than one in ten (12.6 percent) of all resident births were premature (less than 37 weeks gestation). This is down slightly from 13.2% of all births in 2009.
While the percentage of live births that are low birth weight has remained somewhat steady, the mortality rates in each birth weight category have decreased dramatically until recently.
The greatest increase in low birthweight has been for babies born under 500 grams; steady for 2010 for a rate of 0.2%.
Clinical / Quality Improvement
Reducing Recurring PTB – 17P Initiative
Increase appropriate utilization of 17P through a) education of public health leaders, clinicians, and women, b) addressing systems and access issues.
Funded by DPH (via General Assembly) since 2006. Strong partnership with Medicaid and CCNC.
NC has 27 federally qualified health centers13 of 27 provide OB servicesReport to HRSA %LBW babies delivered and
the trimester entered into prenatal careMajority pregnant women served are
Hispanic womenRecently received a special grant from HRSA
to focus on tobacco cessation counseling
NC Federally Qualified Health Centers
Babies born (2005 – 2009)7% born low birthweight
63% enter care in the first trimester
High percent uninsured
In 2010, the % of LBW babies born to Hispanic/Latina women was lower than the percent of LBW babies born to non-Hispanic/Latina women (7% vs. 11%, respectively).
Tobacco Cessation
You Quit Two Quit Project – funded by former Health & Wellness Trust Fund (2008-2012) QI projects in 4 counties based in health departments Statewide educational and outreach efforts including
NICUsNew Project for Low SES Women of CBA
funded by Fed Office of Women’s Health (2011-2013) Focused QI on 8 practices in one CCNC network Training and TA will be provided to all Chronic
Disease and Pregnancy Care Managers within the CCLCF network
Training opportunities will be made available to all practices within the network
Hope to expand to a larger statewide QI program in the future
www.YouQuitTwoQuit.com
Patient Education Materials18
www.MinuteToAsk.com
Perinatal Quality Collaborative of NC (PQCNC)
Mission: • Promote high value perinatal care
• Spread best evidenced practice and reduce variation
• Partner with families and patients• Optimize resources
• Make North Carolina the best place to be born
PQCNC Initiatives
Hospital Based Initiatives:Eliminating elective deliveries under 39
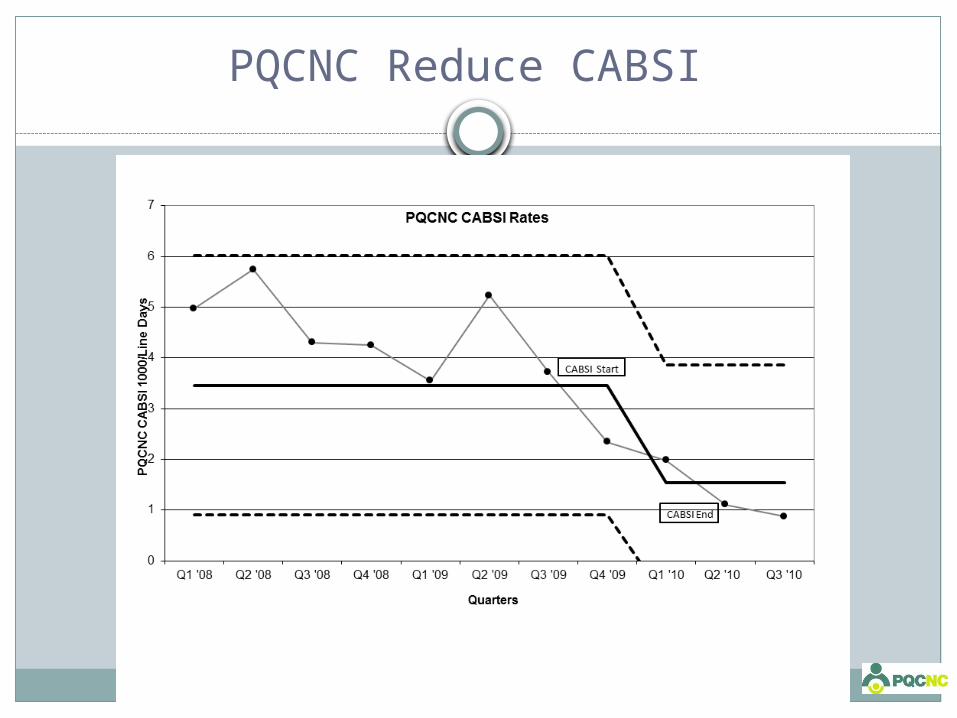
Infections (CABSI) by 75% in participating centers
Increase Exclusive Human Milk Mother - Baby
Increase Exclusive Human Milk NICUSupport for Intended Vaginal Birth (SIVB)
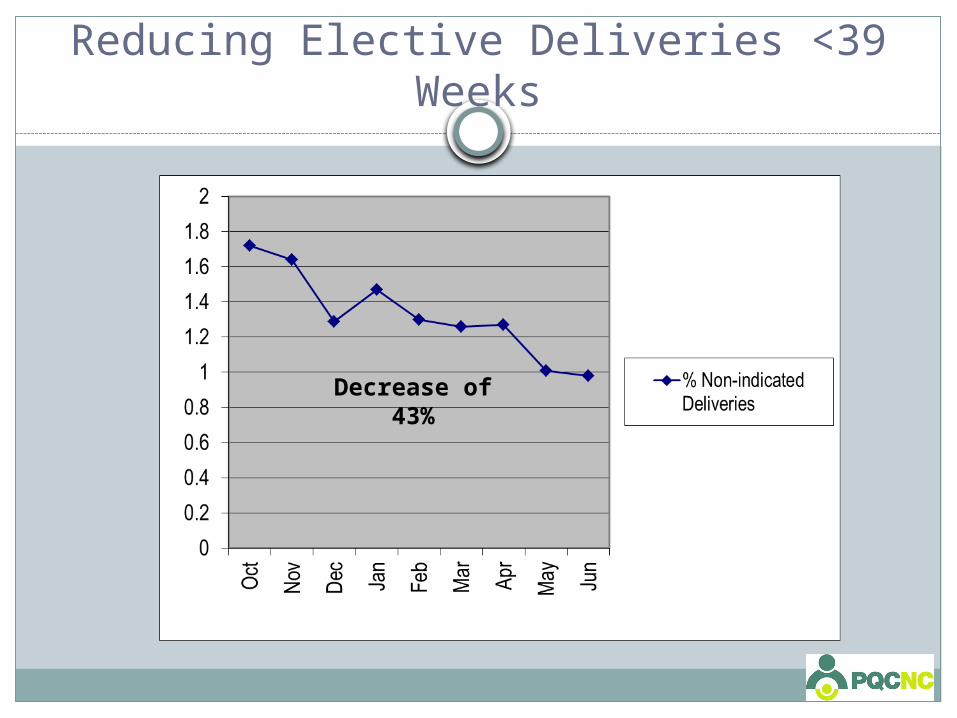
Reducing Elective Deliveries <39 Weeks
Decrease of 43%
PQCNC Reduce CABSI
Pregnancy Medical Home
Improve birth outcomes in the North Carolina Medicaid population Provide evidence-based, high-quality maternity care to
Medicaid patients Focus care management resources on those women at
highest risk for poor birth outcomeImprove stewardship of limited perinatal
health resources In this program, quality improvement goals are
aligned with cost savings goals – keeping more babies out of the NICU and avoiding associated expenses
Methods
Quality Improvement focus for Pregnancy Medical Home practices Identify outliers, work with them to improve
performance
Specific, required performance measures Support, training and resources
Pregnancy Case Management is the key intervention Identify the population most at risk of poor birth
outcome and focus resources on these women
Pregnancy Medical Home Responsibilities
Provide comprehensive, coordinated maternity care to pregnant Medicaid patients and allow chart audits for evaluation purposes for QI measures
Postpartum visit must include: depression screening using a validated screening tool; addressing the patient’s reproductive life plan; and connecting the patient to ongoing care if it will not be provided in the PMH practice
Provide information on how to obtain MPW, WIC, Family Planning Waiver
Collaborate with public health OBCM to ensure high-risk patients receive care management
Pregnancy Medical Home Responsibilities
Eliminate elective deliveries (induction of labor and scheduled cesareans) before 39 weeks
Maintain primary c-section rate at or below threshold level Primary C/S rate of 20% or lower Risk-adjusted (term, singleton,vertex) primary C/S
rate of 16% or lowerOffer and provide 17p to eligible patientsConduct standardized risk screening on all
Medicaid patientsClinical integration with care management
teams
Priority Risk Factors focus on preterm birth prevention
History of preterm birth (<37 weeks)
History of low birth weight (<2500g)
Chronic disease that might complicate the pregnancy
Late entry to prenatal care/missing 2 or more prenatal appointments without rescheduling
Provider request for care management assessment
Benefits of being a Pregnancy Medical Home
Support from CCNC network
Data-driven approach to improving care and outcomes
Incentives: Increased rate of reimbursement for global fee for vaginal
deliveries to equal that of c-section global fee (similar increase for providers who do not bill global fee)
$50 incentive payment for risk screening $150 incentive payment for postpartum visit No prior authorization required for OB ultrasounds
What is CCNC?
• Improves Health Outcomes & Reduces Care Costs:• Manages care via population management
strategies• Supports the primary care medical home• Care Management Services• Community-based, provider-led• Focuses on quality improvement• Data driven
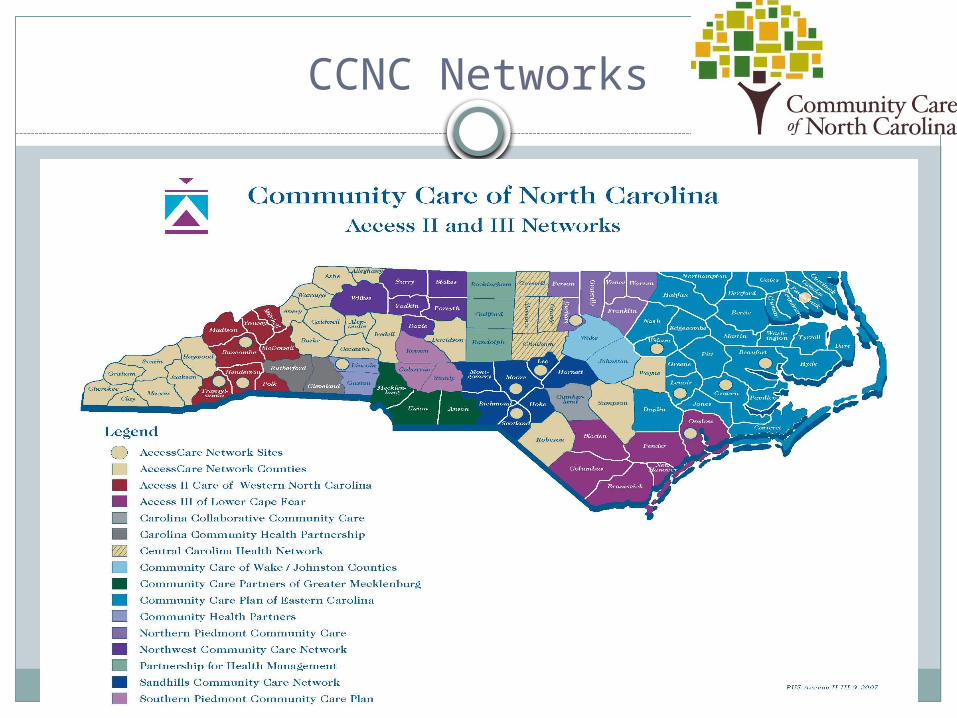
CCNC Networks
Programs & Campaigns
Healthy Beginnings 12 NC communities
Primarily paraprofessionals provide outreach, care coordination and education with specific focus on breastfeeding promotion, folic acid, safe sleep, environmental tobacco reduction/elimination, healthy weight and reproductive life planning.
Services provided to 900 women in 2010; with no infant deaths.
Working with Communities to Reduce Disparities
Working with Communities to Reduce Disparities
NC Healthy Start Programs Healthy Start Corps & Baby Love Plus 15 communities in our state Focus primarily within African American and
American Indian communities. Include outreach, health education, case management,
depression screening, interconception care, and community engagement.
Most (80%) of the communities showed an improvement in birth outcomes among minority families in 2010.
Community Health Ambassador (OMHHD)
NC Maternal, Infant, and Early Childhood Home Visiting Program
Goal: Coordinate an effective statewide planning and implementation system through a strong alliance with key partners in support of a continuum of home visiting services for families.
North Carolina receives $3.2 million annually through the formula grant created by the Patient Protection and Affordable Care Act of 2010 (P.L. 111-148) to support evidence-based home visiting.
North Carolina implementation: Supports four home visiting models:
Nurse-Family Partnership Healthy Families America Parents as Teachers Early Head Start/Home Based Option
Home Visiting cont.
Seven sites at Local Health Departments & Community Based Organizations
Partnership with the National Implementation Research Network and The Finance Project to support implementation and sustainability planning
Current status: Implementation began on December 1, 2011 Oversight from the Governor’s Early Childhood
Advisory Division of Public Health staff support sites in
achieving fidelity to the model, learning continuous quality improvement and implementation science through training and technical assistance.
Breastfeeding Promotion
Breastfeeding Promotion
NC Maternity Center Breastfeeding-Friendly Designation
Expansion of Regional Training Center Infrastructure (6 centers that provide training and TA)
Expansion of the Breastfeeding Peer Counselor Program (70 funded programs covering 86 Counties as of July 2011)
Office of State Personnel Lactation Policy that covers all SPA employees with paid break time and space (the ACA only covers hourly workers)
Child Care Regulation providing onsite space to mothers to pump or feed their infant (s)
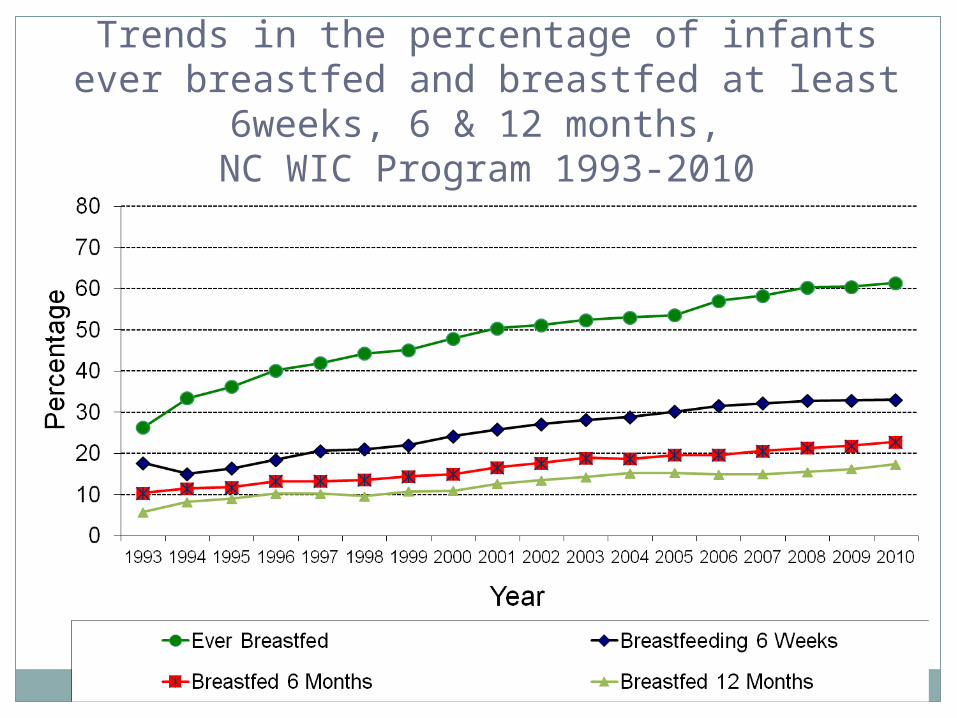
Trends in the percentage of infants ever breastfed and breastfed at least 6weeks, 6 &
12 months, NC WIC Program 1993-2010
Breastfeeding Challenges
Poverty-in rural areas due to our unfortunate and uncomfortable history of slavery, breastfeeding is seen as a “poor” act and a reminder of the past since many slaves were wet nurses.
PRAMS data shows that going back to work and school is a major barrier to continuation of breastfeeding.
Race-there are assumptions by some providers that African American and American Indian women will not breastfeed so they may not “push” the issue.
NC Infant Safe Sleep Campaign (formerly Back to Sleep)
Established in 1994Partnership with Division of Public Health
(Title V)Adheres to American Academy of Pediatrics
(AAP) Standards
Administered by NC Healthy Start Foundation Uses evidence-based research, epidemiology,
principles of public health Incorporates social marketing strategiesNationally recognized for outreach and social
marketingChild care, communities, media, etc. (providers
and public)
Safe Sleep History in NC
1994
NC’s Back to Sleep
Campaign started
2003
NC SIDS Law for
Childcare: ITS-SIDS
2005
BESST begins to
strengthen community outreach
www.nchealthystart.org • www.mamasana.org
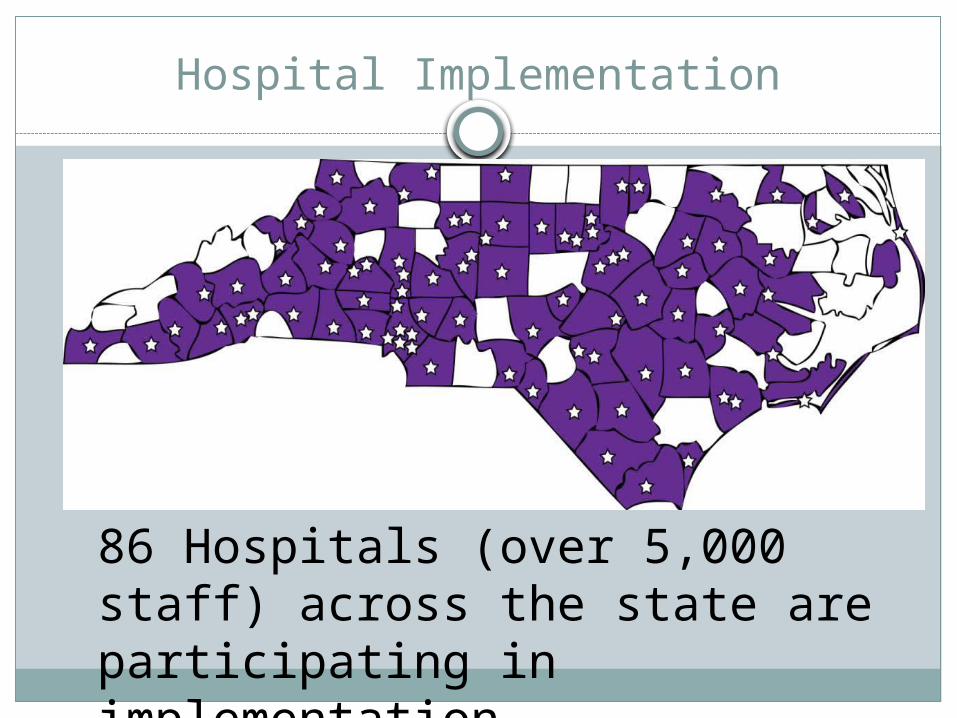
North Carolina leads the way…
Largest and most comprehensive Shaken Baby Syndrome Prevention program in the United States.
3 basic components: Hospital education of parents of newborns Community reinforcements Media campaign
86 Hospitals (over 5,000 staff) across the state are participating in implementation
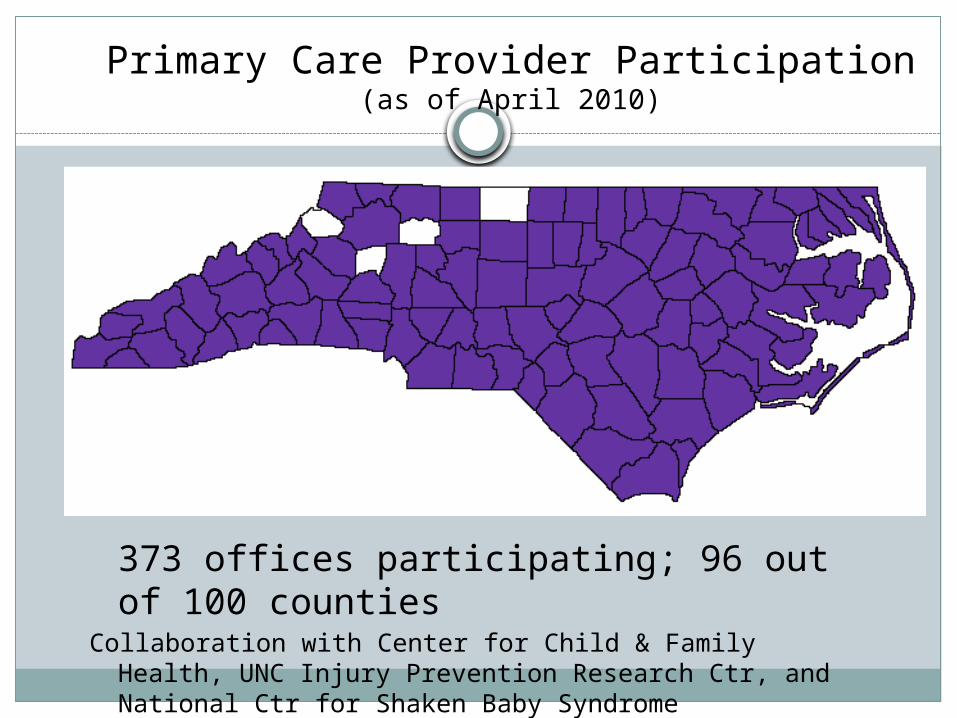
Primary Care Provider Participation (as of April 2010)
373 offices participating; 96 out of 100 countiesCollaboration with Center for Child & Family Health, UNC Injury
Prevention Research Ctr, and National Ctr for Shaken Baby Syndrome
Initiated in Jan 2007 ‐ leadership team formed
Initial focus areas: pregnancy intendedness and healthy weight.
NC Preconception Health Strategic Plan released in November 2008.
From June 2008 –July 2011: 4 workgroups meeting regularly to move from strategies to action.
Preconception Health Coalition
Preconception Health Coalition
Over 150 people.Representatives from DPI, DHHS, local
health departments, public and private universities, community based organizations, non-profit agencies and consumers.
Restructuring coalition so that instead of workgroups, the larger coalition will meets more frequently; will use webinar and videoconference to engage new participants.
Minutes from meetings and other pertinent info available at www.everywomannc.org
Reproductive Life Planning
Postpartum Visit Project
Women’s Wellness Materials
NC Preconception Health Campaign
March of Dimes is home of CampaignFunded by state and federal contractsWorks closely with State’s NC Preconception
Health Coalition and state leadershipFocuses on educating public and health care
providers about the importance of being healthy prior to pregnancy
Grew out of state’s successful folic acid campaign
NC Preconception Health Campaign
Current Campaign Topics
Folic acidReproductive life planningHealthy weightTobacco cessation
Healthy weight trainings
Empowering providers in public and private clinics across the state to use BMI as tool to start discussions about weight with their patients Link between overweight/obesity and maternal and
infant health outcomes Common barriers for providers & patients Evidence-based Eat Smart Move More strategies
Offering new Healthy Habits for Life booklet in English & Spanish for providers to use with their patients, BMI/gestation wheels, posters, etc.
Successes
10-year NTD reduction of 39%; 72% reduction in western NC
More than 550 health care practices and thousands of providers trained over 5-year period
Consumer education using peer education – 100-150 lay health educators trained each year who in turn reach 5,000-10,000 women each year
Preconception Peer Education
Reach college-age population with targeted health messages emphasizing preconception health and healthcare.
Train college students as peer educators.Arm peer educators with materials, activities and
exercises to train their peers in college and in the community at large.
NC Participating Universities
A & T State University Duke University East Carolina University Fayetteville State University Johnson C Smith University NC Central University
NC State University Shaw University UNC-Chapel Hill UNC-Greensboro Winston Salem State
University
NC’s 2010 teen pregnancy rate was lowest in state history – 49.7 per 1000 live births (15-19 years)
Currently supports 29 sites in the state
10 additional PREP (Prepare for Success) sites
Healthy Youth Act – NC law requires all NC public schools to offer abstinence-based, comprehensive sex education to 7th through 9th graders.
Adolescent Pregnancy Prevention
Life Course Perspective
Motivational Interviewing
Community Transformation Grant (NEW) Tobacco free living Active living and healthy eating High impact evidence-based clinical and other
preventive services
Innovations
Policy & Collaborations
Family Planning Waiver
North Carolina’s Be Smart Family Planning Waiver program is designed to reduce unintended
pregnancies and improve the wellbeing of children and families in N.C. by extending eligibility for
family planning services to eligible women ages 19 through 55 and men ages 19 through 60 who meet
the eligibility requirements for participation.
N.C. Medicaid Family Planning Waiver (FPW) Program Update
Based on the 2010 federal health care reform legislation, States now have the option to provide family planning services through a Medicaid State Plan amendment without the formal process of routinely needing to seek Federal approval for a waiver
The Division of Medical Assistance submitted a State Plan amendment (SPA) to Centers for Medicare and Medicaid services (CMS) on 8/18/11.
CMS approved North Carolina’s request to extend the current FPW through 1/31/12 while processing North Carolina’s SPA application for Family Planning Services
FPW recipients who are at or below the 185% of the federal poverty level will continue to receive services under the new option.
N.C. Medicaid FPW Program Update (cont.)
In addition to providing services currently covered under the waiver, the State is proposing screening and treatment for STIs, which will be covered for any or all of the six periodic visits allowed under the new SPA program.
The State is proposing screening only for HIV, which will be covered for any or all of the six periodic visits allowed under the new SPA program.
Under the SPA, there will no longer be restrictions for eligibility based age to receive family planning services.
The SPA will provide an opportunity for North Carolina to further reduce the rate of unintended pregnancies and improve the well-being of children and families by continuing the services previously covered under the FPW.
Advocate for Environmental and Policy Changes that Support Preconception Health
Maternity Leave Checklist and Benefits List created for state employees - covers benefit and health tips for women prior to pregnancy, during each trimester and postpartum.
Advocate for Environmental and Policy Changes that Support Preconception Health
Healthy Babies Healthy Business, a free intranet- based tool from March of Dimes now posted on the state health plan website
Promote BMI assessment and healthy weight guidance in the family planning and maternity clinics
Promoting appropriate gestational weight gain through trainings and/or web materials for public and private providers
Tobacco Cessation Policies
Smoke-Free Hospitals and Campuses
House Bill 2 – Smoke-Free Restaurants and Bars
Quitline – Free NRT
5As Counseling requirement for MH clinics; strongly encouraged in Title X clinics
Alliance for Health and Other Groups trying to protect tobacco use prevention dollars
Child Fatality Task Force
Charged with making and implementing recommendations for changes to laws, rules and policies to support the safe and healthy development of our children and to prevent child abuse, neglect and death.
Purpose is to develop a communitywide approach to understand the causes of childhood deaths, and identify any gaps or deficiencies that may exist in the delivery of services to children and their families.
Comprised of Appointed Members (including legislators) to the Task Force and wider Membership on its Three Committees: Unintended Death Intended Death Perinatal Health
Comprised of over 125 members from across the state.
Studied many different issues over the years – some brought forward by the public, partners and legislators
Introduces fiscal items as well as policy items.Currently focusing on two new areas:
Health Inequities in Birth Outcomes Synchronizing / Systematizing core public health
messages for pregnant and new parents and families
PHC: Focus on Disparities in Birth Outcomes
Increase collective knowledge and understanding of health inequities in birth outcomes and any evidence and best practices available to address those inequities across North Carolina.
Increase connections among members of the PHC and others who have an interest in working together on this issue.
Develop a response to this issue which could include study, policy, research, program or legislative items. ONGOING
Birth Equity Council
Follow up to PHC Series – Initial Funding via NIH U13
25+ member leadership team representing a variety of sectors including Commerce
60+ member CouncilPurpose: develop an actionable strategic plan to
address disparities in birth outcomes…then fund and implement
Council in process of deciding on focus and framework for this work. Strong interest in addressing underlying social determinants of health
Will launch over 15 stakeholder forums across NC as part of this process
Timeline for completion and funding – Fall 2013
Contribution to Regional Efforts
A systems-based, integrated approach to the design and delivery of women’s health services, policies and programs to include mental health and wellness
Distance Education Resources (Free) Orientation webinar series – archived Foundation - 6 online, self-paced modules Academy – intensive online, instructor led New MCH library knowledge pathway
• Go to www.EveryWomanSoutheast.org – Training
Funded by U.S. Health Resources &Services Administration’s Maternal &Child Health Bureau
Women’s Integrated Systems for Health (WISH)
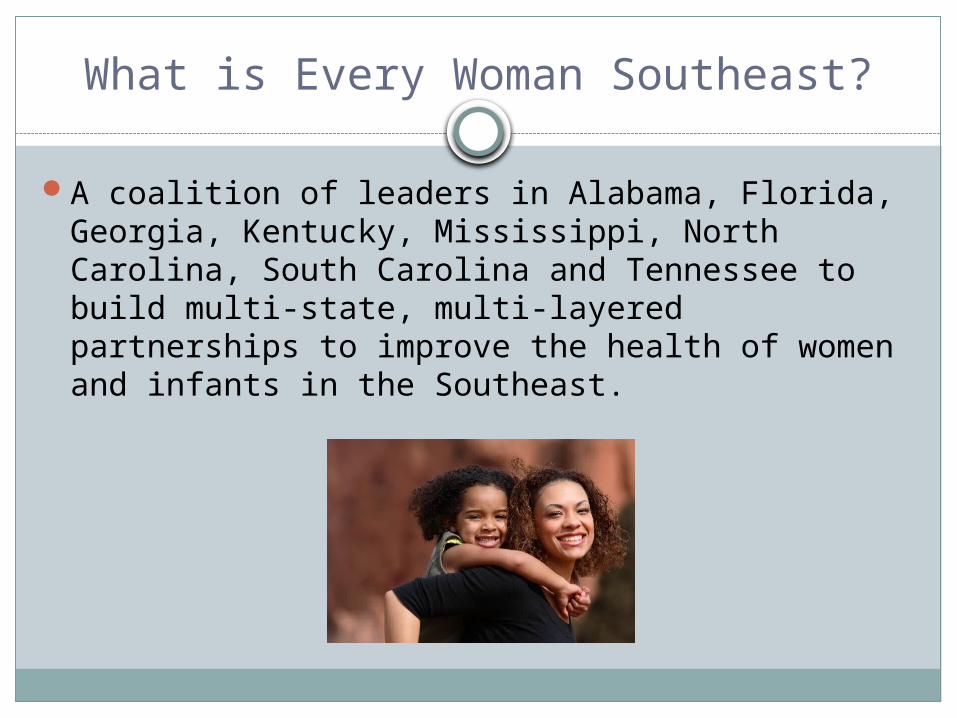
What is Every Woman Southeast?
A coalition of leaders in Alabama, Florida, Georgia, Kentucky, Mississippi, North Carolina, South Carolina and Tennessee to build multi-state, multi-layered partnerships to improve the health of women and infants in the Southeast.
Objectives
Operationalize the life course model.
Promote health equity.
Train leaders to facilitate connectivity between sectors, to think about populations, and to address social determinants of health.
Leverage policy and advocacy opportunities.
Build on social media and social capital.
Re-engage business and faith communities.
Focus on the “grass tips” approach.
Accomplishments to date
Conducted an online survey Recruited Regional and State TeamsHeld planning meeting on March 2, 2010.Produced a compendium of activitiesLaunched blog, website and Facebook pageLaunched webinar seriesNational Preconception Summit PartnerTeam conversations, idea generating, studyLogic model and grant submissions – In