169
Understanding rehabilitation and return to work under the Safety, Rehabilitation and Compensation Act 1988 REHABILITATION HANDBOOK

Understanding rehabilitation and return to work under the Safety, Rehabilitation and Compensation Act 1988
REHABILITATION HANDBOOK
2
Comcare, the Commonwealth of Australia, their officers, servants and agents, and the Safety, Rehabilitation and Compensation Commission and its members, will not be liable for any loss or damage however caused, whether due to negligence or otherwise, resulting directly or indirectly from any use of, or reliance on, any statement, information or advice provided in the contents of this publication whether or not the contents of this publication involve any error, omission or otherwise.
The contents of the publication are provided as a guide for general information only. This publication should not be used by any individual who has not undertaken the Rehabilitation Case Manager’s training provided by Comcare. No warranty is given as to the accuracy of the information contained in this publication. The contents of the publication should not be relied upon for the purpose of any particular action or decision. Independent legal advice from an appropriately qualified professional person should be obtained before relying on the contents of this publication.
© Commonwealth of Australia 2017
All material presented in this publication is provided under a Creative Commons Attribution 3.0 Australia (http://creativecommons.org/licenses/by/3.0/au/deed.en) licence.
For the avoidance of doubt, this means this licence only applies to material as set out in this document.
The details of the relevant licence conditions are available on the Creative Commons website (accessible using the links provided) as is the full legal code for the CC BY 3.0 AU licence (http://creativecommons.org/licenses/by/3.0/legalcode).
Use of the Coat of ArmsThe terms under which the Coat of Arms can be used are detailed on the It’s an Honour website.
Contact usEnquiries regarding the licence and any use of this document are welcome at:
Corporate Strategy and Communications Comcare GPO Box 9905 Canberra ACT 2601 Ph: 1300 366 979 Email: [email protected]

3
CONTENTS
Introduction............................................................................................... 7How to use this handbook ........................................................................................7
The Comcare scheme ..............................................................................................8
Employer obligations under the SRC Act .................................................................8
Copies of this handbook ..........................................................................................9
Part 1: Section 1, The Safety, Rehabilitation and Compensation Act 1988 ......................................................................... 10Key points.................................................................................................................11
What is the SRC Act and who does it cover? ........................................................11
What are the principles of the SRC Act? ................................................................12
Part 2: Section 2, Workplace rehabilitation ............................................ 18Key points.................................................................................................................19
Work for unwell, injured and disabled people .......................................................19
Good work is good for our health and wellbeing .................................................20
What does ‘good work’ look like? ...........................................................................20
What is workplace rehabilitation? ..........................................................................20
Why rehabilitation? ..................................................................................................21
The benefits of workplace rehabilitation ...............................................................21
Early intervention—A key element of Comcare’s workplace rehabilitation model ................................................................................................................................22
A biopsychosocial approach.................................................................................25
Evidence-based decisions .....................................................................................27
Suitable duties .........................................................................................................27
An individual rehabilitation program .....................................................................28
A coordinated approach .......................................................................................28
Case conferences ...................................................................................................29
Injury prevention ......................................................................................................29
Key stakeholders in workplace rehabilitation: responsibilities and support for rehabilitation ............................................................................................................29
Comcare..................................................................................................................35
4
Part 2: Section 3, The role of the rehabilitation authority ....................... 36Key points.................................................................................................................37
RCMs under the SRC Act and delegation .............................................................37
Legislation ................................................................................................................38
Role of the rehabilitation authority .........................................................................38
Liable authority and the rehabilitation authority ...................................................39
Part 2: Section 4, The role of the Rehabilitation Case Manager ........... 46Key points ................................................................................................................47
RCM role outline ......................................................................................................47
Part 2: Section 5, Role of the Workplace Rehabilitation Provider ...... 50Key points.................................................................................................................51
Workplace rehabilitation providers under the SRC Act .........................................51
Part 3: Section 6, Step-by-step guide to workplace rehabilitation ........ 59Key points.................................................................................................................60
Risk management framework for rehabilitation ....................................................60
Part 3: Section 7, Employee and Rehabilitation Authority (Employer) rights and responsibilities ..................................................................... 108Key points...............................................................................................................109
Employee rights .....................................................................................................109
Part 3: Section 8, Case studies ............................................................. 114Case study 1 ..........................................................................................................115
Case study 2 ..........................................................................................................123
Part 3: Section 9, Return to work forms ................................................. 132Key points...............................................................................................................133
Authority and consent for the release of medical information ..........................133
Rehabilitation Assessment examination (section 36 assessment) .........................134
Suitable duties ......................................................................................................135
Rehabilitation program (section 37 rehab program) .........................................136
Rehabilitation program alteration ........................................................................137
Rehabilitation program closure form ...................................................................138
Work trial agreement .............................................................................................139

5
Part 4: Section 10, Privacy ..................................................................... 141
Part 4: Resources .................................................................................. 143Legislation ..............................................................................................................144
Comcare resources ..............................................................................................144
Safety Rehabilitation Compensation courses include: .......................................145
Customer forums ...................................................................................................145
Publications ...........................................................................................................146
References .............................................................................................................146
Part 4: Glossary ..................................................................................... 148
Part 4: Appendices ............................................................................... 152Appendix 1 ............................................................................................................153
Appendix 2 ............................................................................................................154
Appendix 3 ............................................................................................................156
Appendix 4 ............................................................................................................160
Appendix 5: Samples responses for section 37(3) a–h.......................................161

6

7
INTRODUCTIONThis handbook has been developed to help scheme employers and workplace rehabilitation providers offer effective rehabilitation programs for employees. It gives guidance on maintaining employees at work or achieving an early, safe and durable return to work. It also provides a resource that enables employees to understand their responsibilities in the rehabilitation and return to work process.
How to use this handbookEmployers covered by the Safety, Rehabilitation and Compensation Act 1988 (SRC Act), are required to support employees that have sustained an injury or disease in the course of their employment to return to work through individualised rehabilitation programs. This handbook is designed to help with this process.
It will help the reader understand:
» the Comcare scheme and the SRC Act
» the importance of workplace rehabilitation
» how rehabilitation authorities can fulfil their responsibilities to provide workplace rehabilitation
» how to develop effective individualised rehabilitation programs
» how to support workplace rehabilitation
» what is expected of a Rehabilitation Case Manager, the employee and other significant people in the rehabilitation process
» how various stakeholders can work effectively together
» legislative requirements for workplace rehabilitation under the SRC Act
» how to monitor and evaluate rehabilitation programs and processes
» how to minimise the human and financial costs of workplace injuries and diseases.
Part 1 contains information about the legal responsibilities under the SRC Act, the principles of the SRC Act and the requirements of the Guidelines for Rehabilitation Authorities 2012 issued under section 41 of the SRC Act.
Part 2 describes the general principles of workplace rehabilitation.

8
Part 3 describes the rehabilitation process in detail, with a step-by-step process for developing and coordinating rehabilitation programs. This section provides the information Rehabilitation Case Managers need to perform their role under the SRC Act.
Part 4 contains additional information to support the rehabilitation process, including information about privacy and confidentiality and rehabilitation, and return to work resources.
The Comcare schemeThe Comcare scheme provides employers with an integrated safety, rehabilitation and compensation system regardless of which state or territory they operate in or where their employees are based.
The scheme:
» works in partnership with employers to prevent workplace injuries and diseases
» uses appropriate regulatory sanctions on employers who fail to deliver a duty of care to their employees
» encourages employers to work with their employees to support employees in the workplace and to achieve an early, safe and durable return to work
» places on employers a duty to provide employees with suitable employment
» provides employees with a statutory package of economic and non-economic benefits, such as:> a high standard of income support
(until retirement age if necessary)> medical assistance, household
services, permanent impairment benefits, aids and certain alterations.
Employer obligations under the SRC ActThe SRC Act requires the employer to manage and coordinate workplace rehabilitation for their employees. The SRC Act specifies that the employer (under the scheme) is the ‘rehabilitation authority’ for its employees. The Principal Officer of the employer generally delegates this responsibility (in writing) to an employee of the employer who is known as the Rehabilitation Case Manager. This means that in practice the Rehabilitation Case Manager has delegation for rehabilitation and therefore has the responsibility to arrange and manage all aspects of the rehabilitation process, including the assessments and delivery of rehabilitation programs for employees.
Under Part III of the SRC Act employers have the following functions, powers and duties:
» the function and power to arrange the assessment of an employee’s capability to undertake a rehabilitation program (section 36)
» the power to determine that an employee should undertake a rehabilitation program (section 37)
» the power to arrange for a workplace rehabilitation provider to develop a rehabilitation program for an employee (section 37) or to provide a rehabilitation program independently
» the duty to take all reasonable steps to provide an employee who is undertaking, or has completed, a rehabilitation program with suitable employment—or to assist the employee to find such employment (section 40).
These functions, powers, responsibilities and duties are outlined in this handbook.
9
Copies of this handbookThis handbook is only available in PDF format on the Comcare website. If you wish to have a printed version of the handbook it is recommended that you print and bind a copy. As Comcare regularly updates publications to ensure that they are current, be sure to check that you are using the most recent version. For more information regarding this handbook contact Comcare on 1300 366 979.
10
PART 1
SECTION 1
THE SAFETY, REHABILITATION AND COMPENSATION ACT 1988
This section of the handbook provides information about the Safety, Rehabilitation and Compensation Act 1988 (SRC Act). This includes the principles outlined in the SRC Act, who is covered by the SRC Act and Comcare’s role in administering the Act.

11
Key points
» The SRC Act provides a comprehensive workers’ compensation and injury management scheme.
» Comcare regulates the SRC Act.
» Legislation and guidance is provided by the SRC Act and the Guidelines for Rehabilitation Authorities 2012 (Rehabilitation Guidelines) issued by Comcare.
» The SRC Act has a strong focus on workplace rehabilitation. Employers are responsible for coordinating and managing an employee’s return to work.
» Comcare manages workers’ compensation claims for employees of the Australian Government and ACT Government.
» Workers’ compensation claims for employees of licensees are managed according to the terms of the self-insurance licences.
What is the SRC Act and who does it cover?The SRC Act provides a workers’ compensation and injury management scheme. The scheme is administered by Comcare and covers employees of Australian Government departments and statutory authorities, the ACT Government and corporations which have been granted a licence to self-insure. Employees working full-time, part-time, ongoing or on a non-ongoing or probationary basis may be covered by the SRC Act.
Under the SRC Act, if an employee sustains an injury or disease in the course of their employment, rehabilitation programs aim to ensure a safe and durable return to work. According to the SRC Act, employers are responsible for workplace rehabilitation. Individually tailored rehabilitation programs assist employees to return to work.
In order to meet their obligations, an employer needs to have an understanding of the SRC Act, in particular the rehabilitation process detailed in Part III.
Workplace rehabilitation is coordinated by the employer and is usually managed by a Rehabilitation Case Manager within that organisation. Rehabilitation Case Managers exercise the rehabilitation authority’s powers to arrange rehabilitation assessments and rehabilitation programs for employees.
Guidance for how rehabilitation is conducted is outlined in the Guidelines for Rehabilitation. These are sometime referred to as the section 41 guidelines as they are issued under section 41 of the SRC Act. See the resource section of this manual for more information.
Comcare also administers the Work Health and Safety Act 2011 (WHS Act). The WHS Act places the responsibility for the safety

12
of employees in the workplace on the employer. This means that the employer must promote prevention as the primary means of reducing the incidence and cost of workplace injuries. The SRC Act and the WHS Act provide employers with a comprehensive, holistic and cost-effective approach to injury prevention, workplace health and safety and rehabilitation and compensation.
What are the principles of the SRC Act?The principles which underpin the SRC Act include:
» a focus on returning employees to the workforce
» the rehabilitation authority (generally the employer) has a statutory responsibility for workplace rehabilitation of employees
» a premium system and licensing arrangements where the employer is financially accountable for the cost of work-related injury and disease
» employers have access to skilled and efficient workplace rehabilitation providers
» a ‘no fault’ scheme with limited access to common law
» a comprehensive benefit structure with entitlements to payments for medical, rehabilitation, incapacity payments, and other related costs associated with treating or managing work-related injuries and diseases
» fair decision making by the Claims Manager and the Rehabilitation Case Manager
» the capacity to suspend benefits when an employee does not comply with rehabilitation.
A focus on returning employees to the workforceThe SRC Act recognises that arranging an employee’s return to work as quickly as possible after a work-related injury or disease is important to both the employer and the employee. Implementing a rehabilitation program promptly provides the optimal conditions for a durable return to work. This will also help to minimise costs to the employer and the employee.
Employers have a statutory responsibility for workplace rehabilitation of employeesThe SRC Act requires that the Rehabilitation Authority (generally but not always the employer) take responsibility for arranging workplace rehabilitation. The employer is best placed to provide the duties and support required to achieve a safe, successful and durable return to work.
The Rehabilitation Authority has the responsibility to:
» provide suitable employment
» comply with guidelines issued by Comcare
» have a documented commitment to provide rehabilitation to employees
» ensure that a Rehabilitation Case Manager with appropriate skills is available to coordinate individual rehabilitation programs.
Note: References in this handbook to the Rehabilitation Case Manager refer to the employee(s) of the organisation given the delegation under section 41A of the SRC Act to make decisions about rehabilitation programs in regard to sections 36 and 37 of the SRC Act.

13
A premium system and licensing arrangements where the employer is financially accountable for the cost of work-related injury and disease
Employers are financially accountable for the cost of work-related injury and disease. This includes costs associated with benefits paid to or on behalf of the employee, such as costs for workplace rehabilitation.
Comcare calculates a premium for each financial year based on the claims liability an Australian Government department/agency or the ACT Government is expected to incur during that year. The premium rate is determined by the agency’s claim frequency and average claim cost in relation to overall claims trends, and the total amount Comcare needs to collect from all departments to cover the costs of workplace injury and disease. The premium amount includes an estimated administrative cost for that year. Comcare manages these claims for Australian Government departments and the ACT Government, determines liability and arranges compensation payments.
If the organisation is a Commonwealth Authority or private sector organisation that has been granted a licence to self-insure under the SRC Act, it will pay a licence fee to Comcare and a WHS regulatory contribution. These fees are determined by the Safety, Rehabilitation and Compensation Commission (SRCC). Compensation claims management arrangements are outlined in the terms of the licence to self-insure. Compensation claims submitted by employees of the organisation can be determined and financially managed by that organisation, or by a claims agent nominated by that organisation and approved by the SRCC. There are financial and prudential conditions on all self-insurer
licences to ensure that each organisation is able to meet its workers’ compensation liabilities.
For all employers in the Comcare scheme, the message about cost benefits and savings is clear. There are two effective ways to reduce the human and financial cost of workplace injury. The first is to reduce incidence through injury-prevention strategies. The second is to reduce the cost of claims by limiting the impact of workplace injuries on the employee and the employer. Minimising incapacity or time off work by effectively managing workplace rehabilitation will help to reduce premium rates.
For further information about premiums, licence conditions, performance standards and the Premium Calculator see the SRCC website at www.srcc.gov.au.
Employers have access to skilled and efficient workplace rehabilitation providersComcare has adopted the Principles of Workplace Rehabilitation and other requirements of the nationally consistent approval framework endorsed by the Heads of Workers’ Compensation Authorities. This includes service delivery standards, practice standards and Comcare specific return to work rates. Employers therefore have access to skilled rehabilitation providers who can provide expert and objective advice to assist in the safe, timely and durable return to work of an employee. The circumstances in which workplace rehabilitation providers are used are set out in the Rehabilitation Guidelines. The approval requirements and standards for workplace rehabilitation providers are issued under section 34 of the SRC Act. Workplace rehabilitation providers are monitored against

14
the mandatory approval requirements and are subject to Comcare review every three years.
To ensure the delivery of quality and cost effective workplace rehabilitation programs, the employer is responsible for actively monitoring individual rehabilitation programs. This includes monitoring the workplace rehabilitation provider’s effectiveness in achieving timely, safe and durable return to work outcomes for individual employees. Monitoring each rehabilitation program’s performance is part of the rehabilitation management systems reporting required by the Rehabilitation Guidelines.
You can obtain further information about the requirements for rehabilitation providers in the Comcare publication Criteria and operational standards for rehabilitation providers, on the Comcare website. A list of workplace rehabilitation providers is also available on www.comcare.gov.au.
A ‘no fault’ scheme with limited access to common lawEmployees can claim compensation for injuries arising out of or in the course of employment. Injuries that occur at work, during work-related business, or while travelling for work or work-related business may be compensable. Neither the employer nor the employee are required by the legislation to demonstrate that one or other was at fault, or caused the injury.
The decision about liability for a work-related illness or disease depends on whether the employee’s employment contributed to the disease, or the aggravation of the disease, to a significant degree.
The circumstances where liability may not be accepted for an employee‘s claim under the SRC Act include:
» there is no medical evidence linking the injury or disease to the workplace
» employment was not a significant contributing factor to the development of the disease
» the injury occurred as a result of reasonable administrative action taken in a reasonable manner—reasonable appraisal of the employee’s performance, reasonable counselling, suspension or disciplinary action, failure to obtain a promotion, reclassification, transfer or benefit, or to retain a benefit
» there has been serious and wilful misconduct—unless the injury results in death or serious and permanent injury
» the injury was intentionally self-inflicted
» the injury occurred while travelling between home and work.
Note: This information is not exhaustive and is provided as a guide only. The final decision about a claim will be made by Comcare or the relevant claims agent.

15
A comprehensive benefit structure with entitlements to incapacity payments, payments for medical, rehabilitation and related costs associated with the treatment of work-related injury and disease
The SRC Act provides a comprehensive benefit structure. It ensures that those employees with serious injuries are not disadvantaged. It also ensures that there are financial incentives for employees to return to work.
The benefits that employees have access to include:
» payment of full pre-injury earnings for up to 45 weeks, where the employee is unable to work
» reduced payments after 45 weeks, with financial incentives to return to work
» medical expenses, funeral and death benefits, permanent impairment and non-economic loss payments
» household services, attendant care, aids, appliances, alterations and modifications.
Fair decision-making by the Rehabilitation Case Manager and the Claims Manager The SRC Act requires fair decision making by the Rehabilitation Case Manager and the Claims Manager. The general principles of fair decision making are:
» Lawfulness—the decision is made under legal authority by an authorised person, following correct procedures.
» Natural justice—also known as procedural fairness. There are two primary rules of natural justice. The first rule is the ‘hearing rule’, where those affected by a decision must be given the opportunity to express their views to the decision maker. The second rule is the ‘bias rule’, where the decision maker must be impartial and have no personal stake in the matter to be decided.
» Evidence, facts and findings—decisions are based on facts. The decision maker must determine all the facts that are necessary for a decision. Facts must be evaluated to ensure that decisions are based on all the available evidence.
» Reasons—the SRC Act specifies that the decision maker must provide the employee with written reasons for the decision. A statement of reasons for the decision provides the employee with an opportunity to have the decision explained in plain English and to dispute the reasons for the decision.
» Accountability—decision makers are accountable for their decisions. This enables external bodies such as the Commonwealth Ombudsman to investigate complaints. It gives employees the right to apply to a court or tribunal for a review of the decision and enables employees to access their records.
16
The capacity to suspend benefits (excluding medical treatment) when an employee does not comply with rehabilitationThe employee must participate actively in workplace rehabilitation. This means that an employee must attend assessment examinations of capability arranged by the employer. It also means that the employee must comply with a rehabilitation program developed for them.
Unreasonable failure to meet these responsibilities may affect an employee’s rights to some compensation benefits. For example, the employee’s rights to incapacity payments may be suspended until they comply.
You can find further information about the SRC Act, liability determinations and compensation benefits on the Comcare website www.comcare.gov.au.
What is Comcare’s role?Comcare is established under the SRC Act.
Comcare has functions and responsibilities under the SRC Act, the WHS Act and the Asbestos-related Claims (Management of Commonwealth Liabilities) Act 2005 (ARC Act). Under this legislation Comcare has roles as insurer, regulator and scheme manager.
Comcare provides expert advice and services to the SRCC and the Seacare Authority, and manages the Commonwealth’s asbestos-related claims liabilities.
Comcare’s outcome statement describes its success and provides strategic focus for all its efforts:
» Supporting participation and productivity through healthy and safe workplaces that minimise the impact of harm in workplaces covered by Comcare.
Comcare’s role is to have a positive impact on reducing injury and harm in the workplace.
Comcare’s work underpins quality workplaces and plays a vital role supporting workforce participation and productivity, as well as making an important contribution to the Australian Government’s deregulation agenda.

17
Comcare’s business prioritiesComcare’s key business priorities remain unchanged, our Comcare 2016–17 Corporate Plan builds on the new direction we began in 2015–16 that has already seen business improvements and improvement in financial health. It sets a clear path to transform our business and deliver our four business priorities:
» Leading insurer—working with employers and employees to minimise the impact of harm in workplaces, facilitate return to work and recovery at work, and deliver sustainable management of the fund.
» National regulator—working with employers, employees and other stakeholders to deliver consistent, risk-based regulation to improve work health, safety and rehabilitation outcomes.
» Excellence in scheme management and design—working with scheme participants to achieve sustainable and better practice national schemes.
» Efficient and effective operations—working together to achieve our outcome.

18
PART 2
SECTION 2
WORKPLACE REHABILITATION
Employers are responsible for the workplace rehabilitation of their employees. This section provides information about the principles of workplace rehabilitation.

19
Key points» Good work is good for our health
and wellbeing and that of our family, community and our workplace.
» Healthy workers are productive workers.
» Being off work for long periods has serious health effects and is one of the greatest known risks to public health.
» Good work is the most effective means to improving the wellbeing of individuals, their families and communities.
» Returning to an unsafe workplace can be as detrimental to health as worklessness.
» Returning to former lifestyle, including work activities, after injury or illness will assist recovery and reduce risks of long-term disability.
» Both the employer and employee benefit from effective workplace rehabilitation.
» Comcare has developed a comprehensive workplace rehabilitation model.
» There are key responsibilities for stakeholders including senior managers, supervisors, the Rehabilitation Case Manager, the employee, the workplace rehabilitation provider, treating medical practitioners, Comcare and the Claims Manager.
There is a strong evidence base showing that work is generally good for physical and mental health and wellbeing. Worklessness is associated with poorer physical and mental health and wellbeing. Work can be therapeutic and can reverse the adverse health effects of unemployment. That is true for healthy people of working age, for many people with disabilities, for most people with common health problems and for compensation and social security
beneficiaries. The nature and quality of the work and its social context must be considered—jobs should be safe and accommodating. Returning to an unsafe workplace can be as detrimental as worklessness. Overall, the beneficial effects of good work outweigh the risks of work, and are greater than the harmful effects of absence due to injury or illness. Good work is generally good for health and wellbeing.
Work for unwell, injured and disabled peopleThere is broad consensus around multiple disciplines, healthcare providers, disability groups, employers, insurers, unions and government—based on extensive clinical experience and principals of fairness and social justice—that when their health condition permits, unwell, injured or disabled people (particularly those with common health problems) should be supported and encouraged to remain in or to return to work as soon as possible because it:
» is therapeutic
» helps promote recovery and rehabilitation
» leads to better health outcomes
» minimises the harmful physical, mental and psychosocial effects of long-term absence (sick leave)
» reduces the risk of long-term incapacity
» promotes full participation in society, independence and human rights
» reduces poverty
» improves quality of life and wellbeing.

20
Good work is good for our health and wellbeingWorkplaces have an opportunity to influence, educate and support health and wellbeing. If we consider that employees spend more time at work than anywhere else throughout their working lives, this provides employers with a space to provide education on health matters as a means to supporting their employees to prevent injury, ill health and lost productivity. Research tells us where an individual recovering from injury or illness is supported to remain at work, or simply keep in touch with the workplace during their recovery, they are likely to recover more quickly and with less incidences of relapse.
Staying at work (where appropriate) with reasonable adjustments to the work and or workplace decreases absenteeism and presenteeism.
What does ‘good work’ look like?Good work is described as meaningful to the worker and the work team. Research has identified the following factors of work context and content:
» The worker is able to manage the demands—workload, work patterns and working environment.
» The individual has control—they have a say in the way that they do their work.
» There is support—encouragement, sponsorship and resources are provided by the organisation, managers/supervisors and colleagues.
» There are cohesive working relationships with sound and effective communication practices—positive working practices build positive working relationships to avoid conflict and deal with unacceptable behaviour.
» People understand their role within the organisation.
» Organisational change is communicated and managed.
Note: Work absence tends to perpetuate itself: that is, the longer someone is off work, the less likely they are ever to return. If the person is off work for:
» 20 days the chance of ever getting back to work is 70 per cent
» 45 days the chance of ever getting back to work is 50 per cent
» 70 days the chance of getting back to work is 35 per cent.
What is workplace rehabilitation?Workplace rehabilitation assists an employee to remain at work or return to pre-injury employment as quickly and safely as possible. It is a managed process involving early intervention with appropriate, adequate and timely services based on assessed needs. It is the Rehabilitation Case Manager’s responsibility to initiate, coordinate and manage rehabilitation programs within their organisation.

21
Why rehabilitation?The SRC Act defines employers as ‘rehabilitation authorities’. This means they have statutory powers and functions for the rehabilitation and return to work of employees. Comcare has promoted a return to work model to help employers exercise these powers and functions. The model is supported by the proposition that work in general is good for health and wellbeing. It has a strong focus on an early return to work.
The benefits of workplace rehabilitation The benefits for the employer are:
» increased retention of experienced and skilled employees
» a reduction of costs associated with work-related injury and disease
» improved organisational health
» commitment to looking after their employees
» increased productivity
» improved employee morale.
The benefits for employees are:
» maintaining connection with the workplace, social cohesion and support
» resumption of normal activity and lifestyle
» staying active helps rather than hinders healing
» well-designed modified duties focus on ability rather than disability
» increased confidence in managing their condition in their circumstances
» minimised risk of long-term disability and development of other health issues such as depression
» skill development continuity
» reduced risk of long-term incapacity and absence from the workplace
» minimised impact on family
» demonstration of employer commitment
» continuity with the workplace and co-workers.
Social inclusionWork offers many benefits on health and happiness by providing material conditions for good health, control of life circumstances and social networks. Participation in employment is an important aspect of the Australian Government’s social inclusion agenda. Inability to participate in employment is a risk factor for social exclusion. Policies and service delivery should focus on examining the barriers that prevent access to employment, providing additional assistance and ensuring that the service delivery culture treats the employee with respect and dignity. The development of individually tailored solutions to workplace rehabilitation will enable employers to meet their obligations under the SRC Act as well as the broader responsibilities towards the Australian Government’s social inclusion agenda.
For further information about social inclusion visit www.socialinclusion.gov.au.

22
EARLY INTERVENTION— A key element of Comcare’s workplace rehabilitation model
Early interventionThe term ‘early intervention’ can refer to an employer’s WHS processes that aim to prevent injury in the workplace. It may also be a process designed to respond to early warning signs or intervene early when an employee is identified as having a condition or injury (whether compensable or non-compensable). Lastly it can mean the support provided to an employee who has sustained a work injury or disease and has submitted a claim for workers compensation. The term ‘early intervention’ in this handbook, in general, refers to the second and third definitions—support when an employee has submitted a workers’ compensation claim or has sustained an injury or developed a condition that may lead to a workers’ compensation claim.
Early intervention involves providing an employee with support and injury management as soon as possible after the injury occurs. Early intervention has been shown to lead to optimal rehabilitation outcomes. Optimal conditions for a safe and durable return to work for the employee will be in place if potential risks are identified, individual needs are assessed and an individualised rehabilitation program is tailored as soon as possible after injury.
The employer will lose valuable opportunities to assist recovery and to prevent long-term disability if injury management is dependent on acceptance of a workers’ compensation claim.
This principle has been endorsed by the Guidelines for Rehabilitation Authorities 2012.
Early intervention involves:
» identifying and responding to early warning signs
» allocation of a Rehabilitation Case Manager to coordinate rehabilitation and make and maintain contact with the employee
» contact with the manager or supervisor and work area to assist them to support a successful return to work
» provision of prompt attention and intervention as soon as possible after the employee’s injury
» early identification of psychosocial barriers to recovery and workplace rehabilitation
» active coordination of injury management
» integration of treatment and rehabilitation activities
» action to ensure that further workplace injuries are prevented.
Early intervention has the following benefits:
» a productive and supportive workplace which demonstrates that the employee is valued
» prevention of long-term absence from the workplace and development of chronic illness
» reduction in adverse effects on co-workers from the employee’s absence
» improvement in staff confidence and morale
» optimisation of management involvement in the injury management process
» increased probability of return to work and containment of the cost of incapacity
» reduction in the indirect costs to employers through lost productivity, recruitment and training costs for replacement staff.

23
Note: ‘And where the cause of loss of work is itself impaired health then unwarranted delay in return to work is often associated with delayed recovery. In most instances we do not have to recover completely before returning to work, provided there is a will and there are means to accommodate the fullest possible restoration of function; physically, mentally and socially.’1
A focus on increasing activity and return to workThe employer can increase the opportunity for an employee to remain at work or return to work sooner if suitable duties are provided which take into account the person’s capabilities and restrictions.
Focus on return to work involves:
» developing goals focused on return to work and function in collaboration with the employee at the beginning of the program
» developing treatment goals that relate to return to work and function
» identifying and delivering appropriate services to maximise return to work
» activities which focus on the employee’s pre-injury employment wherever possible, or with another employer if necessary
» designing treatment and rehabilitation which promotes the employee’s transition to independence and self-management
» promoting positive health at work strategies
» recognising and responding to early symptoms
» flexibility in return to work options by providing suitable duties
» flexibility in accommodating employees with persistent or recurring symptoms.
A key to achieving an employee’s early and successful rehabilitation and maintenance at work lies in the employer’s willingness, ability and commitment to providing work within the employee’s capabilities.
The success of workplace rehabilitation relies heavily on a number of rehabilitation management strategies. These include:
» commitment of management to return to work that promotes a culture and organisational climate where employee health and wellbeing is valued
» policies and procedures that support return to work
» effective systems and resource allocation
» opportunities for early intervention that enable workplace rehabilitation to begin as soon as possible after injury regardless of claim status
» manager accountability for return to work outcomes
» a continuous improvement approach to rehabilitation policies, procedures and practices.
Supervisors are the key to how workplace policy and practices are perceived. The way they respond to an employee is critical for return to work success.
1 Aylward, M et al. 2010, Realising the health benefits of work, a position statement, The Australasian Faculty of Occupational and Environmental Medicine, Sydney.

24
Payment of sections 36 and 37 rehabilitation costs prior to Comcare issuing a section 14 determination of liability (Commonwealth employers and ACT Government)An early, safe and durable return to work is promoted by arranging a rehabilitation assessment and, if required, developing a rehabilitation program as soon as possible following an injury or the onset of a disease. This also helps minimise costs associated with a claim for compensation under the SRC Act.
Early intervention rehabilitation provides the employer with the opportunity to commence rehabilitation under its Part III powers of the SRC Act prior to a decision by Comcare to accept liability. Early intervention action will reduce potential compensation costs associated with time off work.
Arranging an assessment or examination under section 36 or providing a program under section 37, prior to a section 14 determination of liability being issued by Comcare, means the employer is exercising their rehabilitation authority powers under the SRC Act.
Comcare will pay for any assessment and program cost incurred from the date of injury. If liability is subsequently denied, rehabilitation costs will be reimbursed up to the date Comcare has denied liability.
For further information see the Comcare fact sheet Payment of section 36 and 37 rehabilitation costs prior to a section 14 determination of liability at www.comcare.gov.au.
The benefits of coordinating the workplace rehabilitation of an employee at the workplace include:
» the employee is actively involved in the rehabilitation process, and maintains a connection with the employer and the workplace
» the Rehabilitation Case Manager and supervisor understand the workplace and are best placed to negotiate duties
» the Rehabilitation Case Manager can negotiate other workplace arrangements such as identifying alternative duties in other sections of the workplace
» early intervention is more likely as Rehabilitation Case Managers are best placed to quickly establish the most effective workplace rehabilitation program
» the opportunity for an employee to remain at work or safely return to work sooner than would otherwise be possible is greatly increased
» the supervisor and manager remain actively involved in planning and monitoring their employee’s rehabilitation program
» remedial workplace health and safety action is taken.
If an employee is not able to return to work with their original employer, alternative vocational options can be considered. However, redeployment and vocational retraining should only be considered after all other return to work options have been considered and these options are unlikely to achieve required outcomes. Consideration of options does not necessarily mean pursuing each option but instead deciding that an alternative option will lead to the most successful outcome. If the Rehabilitation

25
Case Manager decides that redeployment and/or retraining are preferred options, then a workplace rehabilitation provider should be engaged to aid the process and coordinate consultation between all parties including the Claims Manager.
Some medical conditions necessitate time off work. For example, a person recovering from surgery or someone experiencing debilitating pain requires recovery time and may be unable to attend the workplace. However, with many medical conditions there is a substantial discretionary element to work absence. ‘Discretionary element’ means while the person has a health condition, they are able to attend work if the accommodation is appropriate. In these instances, work absence is at the discretion of the employee, their doctor or employer—there is no medical requirement that the employee stay away from work. See the certificate of capacity at www.comcare.gov.au.
A biopsychosocial approachWorkplace rehabilitation is directed at addressing the physical, psychological and social factors involved in human illness and disability. This is known as the biopsychosocial approach to rehabilitation.
The traditional medical model assumes a linear relationship between disease, symptoms and disability, and incapacity for work. We know that this thinking is too simplistic as it fails to take sufficient account of the personal and social dimensions of disability. Therefore, from the time of injury, treatment of the employee should include management of the multiple factors that affect return to work outcomes:
» Biological refers to the physical or mental health condition.
» Psychological recognises that personal and psychological factors also influence functioning.
» Social recognises the importance of the social context, pressures and constraints on functioning.
An individual-centred model to personal injury management should be used that considers the individuals, their health problems and their social context. This encompasses all the activities associated with ensuring an employee’s safe and early return to the workplace. It includes treatment, claims management, and employment practices as well as occupational rehabilitation.
Rehabilitation should be directed to overcoming biopsychosocial obstacles to recovery and return to work. These principles are fundamental to better clinical and workplace rehabilitation management. Figure 1 highlights the interactive nature of variables that can impact on recovery and return to work. Adopting this model recognises that employees’ fears and beliefs about their injuries and the impact of their return to work on their health, are critical domains that should be included in injury management approaches. Likewise, an injured employee’s level of motivation to return to work is influenced by workplace variables such as the presence or absence of support from managers and co-workers, flexible accommodation and the availability of suitable duties, and the organisation’s willingness to invest in health and safety (Workcover SA, 2008).

26
Dimensions of disability
Obstacles to return to work Corresponding rehabilitation interventionInteractions communication
Bio
Health condition (+ health care)
Capacity + activity level -v- job demands
Effective and timely health care
Increasing activity levels and restoring function
Modified work
All players onside
Psycho Personal/psychological factors
Psychological aspects of work
Shift perceptions, attitudes and beliefs
Change behaviour
Social Organisational + system obstacles
Attitudes to health and disability
Involvement of employer critical
Social support
Organisational policy, process and attitudes
Figure 1: Biopsychosocial obstacles to return to work are classified, and the corresponding rehabilitation interventions are shown by Waddell and Burton.2
In 75 per cent of cases, psychosocial factors such as an individual’s lifestyle and social circumstances are the dominant barriers to successful return to work. This reinforces that for those who have difficulties returning to work, focusing on the medical condition alone is not enough. Talking with employees, addressing barriers and building trust and confidence to return to work are critical to prevent disability and long-term worklessness.
Incapacity costs in workers’ compensation can be significantly reduced through a biopsychosocial approach, which involves working together with all stakeholders and influencing a fundamental shift in thinking about these conditions in health care, in the workplace and in society.
Note: ‘Studies have shown that best practice injury management—i.e. that which not only meets statutory obligations but also takes into account the complex social, psychological and medical aspects of injury and illness—saves money in the long term.’3
Indicators of poor rehabilitation outcomes identified by the biopsychosocial framework are outlined in the Flags model.
Refer to Appendix 2 for further information.
2 Waddell, G & Burton AK, 2004, Concepts of rehabilitation for the management of common health problems, The Stationary Office, London.
3 Aylward, M et al. 2010, Realising the health benefits of work, a position statement, The Australasian Faculty of Occupational and Environmental Medicine, Sydney.

27
Evidence-based decisionsExtensive research has been conducted on the value of different treatments for most injuries and diseases. This evidence should direct clinical and rehabilitation decision-making to promote effective rehabilitation outcomes, ensuring:
» assessments demonstrate the need for particular treatment and rehabilitation interventions
» the most appropriate and effective interventions are used
» the types of treatment and service selected for an employee are linked to functional outcomes, especially an improvement in ability to perform usual daily activities, including work activities
» injury management interventions demonstrate measurable effectiveness.
Suitable dutiesWorkplace rehabilitation aims to return employees to their pre-injury duties in their own workplace. This principle is supported by a hierarchy of preferences for return to work outcomes, referred to as the ‘return to work hierarchy’:
» same job, same employer
» similar job, same employer
» new job, same employer
» same job, new employer
» similar job, new employer
» different job, new employer.
The return to work hierarchy should be considered when developing programs and goals for an employee. It is important to consider each level, but not necessary to attempt every level of the hierarchy before considering the next level. At times it is clear
from medical evidence that the person is unable to return to their previous duties and role, so something further down the hierarchy should be attempted in the first instance.
For example, consideration should be given to how the person can be supported to maintain some or all of their pre-injury tasks and roles in the organisation. Where this is not possible, a thorough vocational assessment can help determine suitable training and vocational options and appropriate ongoing alternative employment. The hierarchy does not imply that rehabilitation should attempt a return to work at each level, rather that decisions are based on adequate assessment. The final decision about the return to work hierarchy should be made in consultation with the employee and their medical practitioner, and using the findings of a rehabilitation assessment.
The aim is to return the worker to their pre-injury duties at their pre-injury work hours wherever possible. Where this is not possible, reduced or graduated hours are considered. This is a common approach to building an employee’s work capacity.
Section 6 of this handbook provides a step-by-step guide to implementing a rehabilitation program based on the return to work hierarchy.
Refer to the Comcare publication First Steps Back: a guide to suitable employment for Rehabilitation Case Managers for further information about finding suitable employment for an injured employee.

28
An individual rehabilitation programA rehabilitation program is a structured series of planned activities, consistent with medical advice, offered to employees to enable a coordinated return to work. This ensures the individual needs of employees are considered in regard to their workplace rehabilitation. It also demonstrates employer commitment to supporting the return to work.
A rehabilitation program will include:
» a structured rehabilitation plan
» an outline of rehabilitation goals and time frames
» if a workplace rehabilitation provider is engaged, the rehabilitation provider’s services and estimated costs
» responsibilities of all parties in relation to the employee’s rehabilitation.
A rehabilitation program may also include:
» a suitable duties plan or return to work schedule
» a work trial agreement.
A rehabilitation program should:
» be developed in consultation with the employee and there should be evidence of this consultation (it is good practice to include the medical practitioner and other relevant stakeholders in this consultation)
» be individualised, outcome-based and clearly set out the steps to be followed in achieving the return to work
» be available to every employee who has a capacity to work
» be developed using appropriate expertise, such as a workplace rehabilitation provider
» recognise the existing skills, experience and capabilities of the employee for suitable duties to be identified
» contain mechanisms for regular review against the program goals and targets
» consider retraining and redeployment only when it is not possible for the employee to return to pre-injury duties.
A coordinated approachWhile many employees may return to work without assistance, workplace rehabilitation is a process to strategically manage rehabilitation and return to work effectively. Evidence shows that a coordinated and supportive approach promotes shared understanding of recovery timeframes and return to work goals.
A Rehabilitation Case Manager must adopt a coordinated approach involving cooperation and consultation between the employee, the medical practitioner, the supervisor and the workplace rehabilitation provider. As noted above, return to work outcomes are affected by many factors, not only the nature of the injury, but also a range of work and non-work related factors. A holistic approach that considers personal and environmental factors that impact on return to work is more effective than an approach that considers only the nature of the injury. Cooperation and consultation between the stakeholders is vital, so all parties have a shared understanding about the potential barriers, what happens during rehabilitation and return to work, what support is available to assist a successful return to work and the planned activities.
Effective case management involves proactive communication and coordination among the stakeholders to ensure adequate information collection and sharing, as well as providing opportunities for consultation and feedback.

29
Case conferencesThis information describes case conferences for claims managed by Comcare. The claims managed by licensees may run with a similar format.
A case conference is a key activity that allows stakeholders to develop a shared plan to assist an employee to return to health and return to work. They provide an opportunity to discuss complex cases and cases where return to work has stalled or to be proactive in sharing information early in a claim to ensure all stakeholders are working towards the same goal. Case conferences bring multiple stakeholders together and may include:
» the employee
» Rehabilitation Case Manager
» supervisor
» treating practitioners (GP, psychologist, physiotherapist)
» workplace rehabilitation provider (WRP)
» Claims Manager
» Comcare injury management adviser.
Case conferences vary depending on the required outcome but may be one of the following:
» Comcare case conference—meeting between Comcare and an employer to discuss liability and/or rehabilitation matters in relation to a particular claim or collection of claims.
» Return to work case conference—connecting the GP, the employer, the employee, other treatment providers and the insurer to support return to work.
See Case Conferences on the Comcare website: www.comcare.gov.au.
Appendix 3 contains further information about case conferences.
Injury preventionEvery employer has an obligation to ensure the safety of employees in the workplace. This means that if an injury occurs in a workplace, the employer must take action to ensure that further workplace injuries are prevented.
When a manager is notified about injuries in the workplace they must report them to the appropriate person for follow up.
Refer to Comcare’s website for further information about preventing and managing risks in the workplace.
Key stakeholders in workplace rehabilitation: responsibilities and support for rehabilitation
Stakeholders in the rehabilitation process
Employer responsibilities
Employers (where they are the Rehabilitation Authority) are responsible for ensuring that effective processes are in place to review, monitor and continuously improve workplace rehabilitation systems. Employers have a number of specific responsibilities under the SRC Act.
Under Comcare’s workplace rehabilitation model, the Rehabilitation Authority (generally the employer) is responsible for managing and monitoring individual rehabilitation programs in consultation with medical practitioners and specialist rehabilitation providers. It means that each injured employee should be assigned a Rehabilitation Case Manager who has the responsibility and resources to manage, monitor and support the employee’s return to work. The Principal Officer of the employer

30
generally delegates this responsibility (in writing) to an employee of the employer who is known as the Rehabilitation Case Manager (RCM).
Rehabilitation Case Manager responsibilities
RCMs have both operational and strategic responsibilities. Key aspects of the role are to:
» inform staff about the case management role and RCM contact details
» initiate, manage and monitor rehabilitation in consultation with all parties to achieve successful return to work outcomes
» ensure that the organisation complies with the Guidelines for Rehabilitation Authorities 2012 issued by Comcare
» develop rehabilitation management systems to support strategic direction
» promote continuous improvement for rehabilitation management
» encourage senior management commitment to rehabilitation
» monitor and evaluate rehabilitation outcomes in line with measures and targets.
For a more detailed description of the RCM’s role including the Rehabilitation Case Manager Core Capabilities, see Part 2: Section 4, The role of the RCM in this handbook.
See also Rehabilitation Case Manager Core Capabilities at www.comcare.gov.au.
The RCM plays a leading role in rehabilitation. Rehabilitation Case Managers are responsible for initiating, coordinating and monitoring the workplace rehabilitation program in consultation with
other stakeholders. It is the RCM’s job to manage individual rehabilitation programs and to foster understanding about the organisation’s return to work approach.
Employee responsibilities
The employee has the responsibility to:
» find out about the organisation’s rehabilitation and return to work policy
» let the supervisor or RCM know if they are intending to be away from work for an extended period because of a work-related injury
» undergo an assessment for rehabilitation if requested
» talk to the RCM about obligations and rights regarding workplace rehabilitation
» actively participate in the rehabilitation program
» talk to the RCM or supervisor about any concerns about the rehabilitation program
» submit a claim for compensation without delay for injuries or diseases arising out of the course of their employment.
Employees are required to actively participate in the development and implementation of their rehabilitation programs. Evidence shows that this is a critical factor in successful return to work outcomes. There are many benefits for the employee in actively participating in the rehabilitation program:
» higher levels of self-efficacy prevent long-term absence
» improved self-management of chronic health conditions reduces disability and improves long-term health outcomes
» improved self-confidence.

31
The RCM can facilitate the employee’s participation in rehabilitation through consultation, information and support.
Active participation is outlined as a key responsibility for an employee in Comcare’s Return to work easy reference guide. The SRC Act allows for penalties in extreme cases where the employee is not compliant with the rehabilitation program, for example, suspension of some benefits.
Section 4 of this handbook provides more detail about the suspension process in the event of non-compliance with rehabilitation.
For more information about the rights and responsibilities of employees see Part 3: Section 7—Employee and Rehabilitation Authority (Employer) rights and responsibilities in this handbook.
Senior managers
Effective performance of the case management function requires a supportive and enabling framework within the organisational systems and processes. Senior management backing is essential for developing and supporting this enabling framework.
Senior managers support rehabilitation by:
» developing a workplace culture that prevents injury and supports employees
» showing commitment to effectively implementing the organisation’s rehabilitation policy
» providing resources to enable effective rehabilitation
» ensuring that Rehabilitation Case Managers receive organisational support to fulfil their role
» keeping informed of the organisation’s rehabilitation performance, accessing
performance reports that track the organisation’s claim costs and rehabilitation outcomes
» addressing identified problems with rehabilitation systems
» reviewing and improving the effectiveness of the organisation’s rehabilitation strategies.
Engaging senior managers
To gain the support of senior management for effective and efficient rehabilitation systems you can provide them with information about:
» financial benefits and cost savings of returning employees to work
» the direct and indirect costs of failure to adequately support early intervention and rehabilitation processes—direct costs include the annual premium (for premium payers) and workers’ compensation costs (for licensees); indirect costs include those associated with lowered productivity, absenteeism, low morale, recruitment and separation, and retraining
» the responsibilities of the employer under the SRC Act and the Rehabilitation Guidelines, developed by Comcare under section 41 of the SRC Act
» reports, data and analysis on the organisation’s rehabilitation, work health and safety performance costs—Comcare’s publication Improving outcomes through rehabilitation management systems: a continuous improvement guide provides a systematic approach to reviewing rehabilitation practices
» performance indicators against return to work performance reported by the Safety Rehabilitation and Compensation Commission (SRCC).

32
Further information about systems to support workplace rehabilitation is described in Part 2: Section 3, The role of the rehabilitation authority in this handbook.
Supervisors
The employee’s supervisor has a critical role to play in the rehabilitation process. Without the support and cooperation of the supervisor it is very difficult to achieve successful and durable return to work outcomes. The supervisor has a key role in providing suitable duties, in monitoring the return to work activities and supporting rehabilitation. The supervisor must:
» foster a supportive workplace which encourages safe work practices and early reporting of injuries
» advise the RCM as soon as becoming aware of an injury
» ensure steps are taken to prevent further injury by understanding the cause of injury and putting safeguards in place
» keep in close contact with the employee—be supportive and identify the assistance available to enable a return to work
» work with the RCM to identify suitable duties and provide ongoing support
» consider changing the way work is done or modifying the work environment
» be involved and contribute to the development of the rehabilitation program for the employee
» manage performance issues
» support return to work
» manage workloads and the operational needs of the work area
» promptly advise the RCM of any concerns raised by the employee or co-workers
» after an employee has returned to work, work with them to ensure that this outcome is sustained
» maintain the employee’s privacy.
See also Supervisor core capabilities at www.comcare.gov.au.
Engaging supervisors
Supervisor support usually relies on a suitable organisational framework which promotes workplace rehabilitation and injury management.
To engage the supervisor in actively supporting workplace rehabilitation you can provide information about the role, the importance of supervisor support and their responsibilities under relevant policies and legislation:
» what workplace rehabilitation is, and what it is not
» support available from the Rehabilitation Case Manager
» the important role of the supervisor in optimum rehabilitation outcomes
» organisation policies—for example, the Rehabilitation policy, which outline the supervisor’s role
» responsibilities under the SRC Act and the Rehabilitation Guidelines issued by Comcare
» financial benefits and cost savings of returning employees to work
» devolution of workers’ compensation costs within the organisation
» direct costs of failure to adequately support workplace rehabilitation, for example, the annual premium (for premium payers) and workers’ compensation costs (for licensees)

33
» indirect costs of failure to adequately support workplace rehabilitation, for example, lowered productivity, absenteeism, low morale, recruitment and separation, and retraining.
The treating medical practitioner
Medical practitioner responsibilities
The medical practitioner is responsible for the medical treatment of the work-related injury or illness. The medical practitioner also provides advice on the capacity for workplace rehabilitation, restrictions imposed by the injury, possible alternative duties and appropriate workplace modifications. The medical practitioner is expected to:
» provide medical treatment for the employee
» provide treatment and services selected for an employee that link to functional outcomes
» provide accurate medical assessments of capacity to return to work which is documented on Comcare’s certificate of capacity
» provide advice on alternative duties or modifications to the workplace
» ensure that the RCM and workplace rehabilitation provider are informed of the employee’s abilities so that tailored duties can be organised within the employee’s capacity
» monitor and support workplace rehabilitation
» be available and accessible for case conferences.
Encouraging the treating medical practitioner’s support
Consult the treating medical practitioner about the rehabilitation program. This is best done through a return to work case conference. See Comcare’s website for more information on organising a return to work case conference.
Tips for RCMs working with GPsUnderstand their business and how they work.
» Practice managers and reception staff facilitate access to the GP so develop a relationship with the reception staff.
» As they are running a business, they need to be paid for their time.
» Ensure you are clear on how the account will be paid—many practices need payment at the time of the appointment.
» When engaging a WRP set clear expectations about engagement with GPs.
Ensure the time with the GP is well spent by:
» booking a long appointment to ensure enough time is allocated
» asking yourself what the GP needs to know
» preparing what you are going to say, saying it clearly and saying it once only
» keeping anything you send to the GP to one page (GPs are time poor)
» advising the GP who will be attending an RTW case conference
» sending through an agenda for the meeting so the GP is clear about the purpose and expected outcomes of the consultation
» Earning their trust and treating them with respect.

34
Comcare’s GP LiaisonComcare’s employs a GP Liaison Officer to provide direct contact for GPs and GP practice staff with Comcare. The GP Liaison offers the following to GP practices:
» guidance on use of the certificate of capacity
» tailored support and advice about navigating the Comcare Workers’ Compensation Scheme
» practice visits
» information on fee schedules and billing requirements
» link to the relevant person in Comcare where follow up is required
» help with complex cases by linking with the Injury Management Advisory Service
» information on upcoming education events.
The GP Liaison can be contacted on:
Phone: +61 419 512 964
Feel free to tell GPs about this service and encourage them to make contact.
Claims Manager responsibilitiesFor premium payers, Australian Government, and ACT Government employers, Comcare determines the liability for workers’ compensation claims, pays benefits and manages the claim. These tasks are performed by the Comcare Claims Manager.
Comcare does not manage the workers’ compensation claims of licensees. This is arranged by the employer (Licensee) and is outlined in the conditions of the employer’s licence to self-insure under the SRC Act. Claims management may be performed
in-house or by an external organisation. These external organisations generally refer to those who manage claims as Claims Managers. This handbook refers to the Claims Manager. This role may be similar between Comcare and licensees but not identical in other organisations and should be read as such. The responsibilities of the Claims Manager are to:
» provide support and guidance to the to the employee in relation to their claim and their return to work and health
» make accurate and timely decisions on compensation claims
» communicate with all stakeholders and effectively manage the employee’s claim.
For Australian and ACT Government agencies, the Claims Manager may also:
» review rehabilitation programs
» identify cases requiring return to work intervention
» provide advice about the development of rehabilitation programs
» conduct high cost claims reviews
» conduct reconsiderations of rehabilitation authority determinations upon request
» participate in case conferences and high cost claim reviews
» advise employees about what to do if they disagree with a decision.
Licensees should contact their Claims Manager to discuss the services they offer.
See also Claims Manager Core Capabilities at www.comcare.gov.au.

35
ComcareThe Comcare scheme (the scheme) provides all scheme employers with a rehabilitation and compensation system, no matter what Australian state or territory an employer operates in or where its employees are located.
The scheme:
» works in partnership with employers and their employees to prevent workplace injuries
» appropriately uses regulatory sanctions if there has been any demonstrable failure of the employer’s duty of care
» empowers employers to work with their employees to maintain an employee at work or to achieve an early, safe and durable return to work
» gives employers a duty to provide employees with suitable employment
» provides employees with a statutory package of economic and non-economic benefits, such as:
> a high standard of income support (until retirement age if necessary)
> medical and home help assistance, permanent impairment benefits, aids and certain alterations and other benefits.
Resources» Rehabilitation and workers’
compensation regulatory functions
» Scheme statistics (available on the SRCC website)
LegislationWorkers Compensation in the Commonwealth jurisdiction is governed by the Safety, Rehabilitation and Compensation Act 1988 (SRC Act). Rehabilitation is addressed in Part III of the SRC Act.
Section 41 of the SRC Act gives Comcare the power to issue rehabilitation guidelines to rehabilitation authorities in relation to the performance or exercise by those authorities of their functions or powers under Part III of the Act. The current guidelines are the Guidelines for Rehabilitation Authorities 2012. More information about the guidelines can be found at Rehabilitation guidelines FAQs.
The SRC Act is available on Comcare’s website www.comcare.gov.au.

36
PART 2
SECTION 3
THE ROLE OF THE REHABILITATION AUTHORITY
The SRC Act provides for the rehabilitation of employees following a work-related injury. The legislation is designed to ensure that the employer is responsible and accountable for the safe and early return to work of their employees. The employer is best placed to monitor incidents or absences, intervene early, create opportunities for suitable duties and ensure that the employee is appropriately and actively managed to the best possible outcome following a work-related injury.
37
Key points» Case management operates within
the range of organisational policies, processes and procedures.
» Effective rehabilitation case management relies on a structured framework which documents implementation, management, monitoring and evaluation of workplace rehabilitation.
» A rehabilitation management system provides a comprehensive structured approach, outlines senior management commitment to workplace rehabilitation, and identifies actions for continuous improvement.
» To exercise their rehabilitation powers under Part III of the SRC Act, RCMs require appropriate delegation.
» These powers can only be delegated by the rehabilitation authority to an officer of or a person employed by the organisation.
» RCMs play a pivotal role in the rehabilitation process.
» The role of the Rehabilitation Case Manager is varied and involves management of individual cases as well as broader organisational issues.
» Consultant and contract RCMs may provide specialist expertise but do not have the delegated powers to complete all functions—this means they cannot determine rehabilitation matters under sections 36 and 37 of the SRC Act.
» Workplace rehabilitation providers may provide specialist expertise but do not have the delegated powers to complete all functions—this means they cannot determine rehabilitation matters under sections 36 and 37 of the SRC Act.
» Comcare provides training and other resources to assist with the role.
RCMs under the SRC Act and delegationIn this handbook, the term Rehabilitation Case Manager (RCM) refers to the delegated RCM who has a written instrument of delegation from the rehabilitation authority under section 41A of the SRC Act. The employer is the rehabilitation authority for the employee.
Employers are able to manage their return to work activities by delegating the responsibilities to one or more RCMs. This role has a specific set of responsibilities in the Comcare return to work model.

38
LegislationThe employer of the employee is the rehabilitation authority for the purposes of the SRC Act. The rehabilitation authority is responsible for:
1. Complying with guidelines issued by Comcare, meeting the performance standards and reporting requirements, or exercising the rehabilitation authority’s functions or powers under section 41 of the SRC Act.
2. Making a determination that the employee shall undergo an assessment of capability to undertake a rehabilitation program where the ‘employee suffers an injury resulting in an incapacity for work or an impairment’ (section 36 of the SRC Act).
3. Making a determination as to whether ‘an employee who has suffered an injury resulting in an incapacity for work or an impairment should undertake a workplace rehabilitation program’ and, making ‘arrangements with a workplace program provider for that provider to provide a rehabilitation program for the employee’ (section 37 of the SRC Act).
4. Making a determination about suspension of incapacity payments as a result of failure to ‘undergo an examination assessment’ or ‘to undertake a rehabilitation program’, without reasonable excuse (sections 36(4) and 37(7) of the SRC Act).
5. Advising the employee in writing of any decisions made under sections 36 and 37 of the SRC Act.
6. Providing suitable duties and/or undertaking job search activities associated with the provision of suitable employment (section 40 of the SRC Act).
Role of the rehabilitation authorityThe rehabilitation authority is able to ascertain the need for a rehabilitation assessment. It is able to develop and determine an appropriate rehabilitation program and actively monitor compliance and the success of the rehabilitation program.
The rehabilitation authority has a specific meaning under the SRC Act:
(a) where the employee is employed by an exempt authority—Comcare
(b) where the employee is employed by a licensed authority—the principal officer of that authority
(ba) if the employee is employed by a licensed corporation—the principal officer of that corporation
(c) if the employee is employed by an Entity or a Commonwealth authority, other than an exempt authority—the principal officer of the Entity or the Commonwealth authority in which the employee is employed
(d) if the employee is a serving member of the Australian Defence Force, and sustained an injury before 1 July 2004:
> the Chief of the relevant Service is the applicable rehabilitation authority; or
> ceases to be a member of the Permanent Force, then the Military Rehabilitation and Compensation Commission (MRCC) is the applicable rehabilitation authority; or
> continues or ceases to be a member of the part-time Reserves, then the MRCC is the applicable rehabilitation authority.

39
Liable authority and the rehabilitation authorityIf the employee works for a Commonwealth agency, the liable agency is the employer who employed the person when the injury occurred. This agency is also the rehabilitation authority. If the employee leaves the liable agency and commences employment with another Commonwealth agency then the receiving agency becomes the rehabilitation authority.
Where an employee exits a licensee employer, and is subsequently employed by another licensee or an Australian Government agency (those employed by the ‘Commonwealth’ or a ‘Commonwealth authority’), the rehabilitation authority is the new licensee or Australian Government agency. This also applies where an employee leaves a licensee and joins an ACT Government agency. The current rehabilitation authority in that case will be the relevant ACT Government agency. The arrangements are the same because the ACT Government is taken to be a Commonwealth authority for the purposes of the SRC Act. For more details on the Prescribed Rehabilitation Authority see the Guidelines for Rehabilitation Authorities 2012, Attachment C, page 29. This advice is the current interpretation at the time of publication. Please contact Comcare to ascertain if this advice has altered.
DelegationThe Rehabilitation Case Manager must:
» be an employee of the organisation
» have a current and written delegation provided by the relevant rehabilitation authority.
Only employees with written delegation are able to sign off on the forms associated with rehabilitation programs. These forms include the Referral for rehabilitation assessment examination, the Rehabilitation program, Rehabilitation program alteration and the Rehabilitation program cessation forms. The Rehabilitation Case Manager should have sighted their delegation and know where it is stored so they can produce it if necessary. The Rehabilitation Management System is a good place to file the written delegations.
Some organisations use contract RCMs who do not have the written delegation to perform some of the tasks associated with workplace rehabilitation. This separation of tasks is permissible under the SRC Act. Contract RCMs may complete the forms, liaise with the employee and other stakeholders and actively manage the rehabilitation program. However, they do not have the delegation under section 41A of the SRC Act, so they do not have authority to determine an appropriate rehabilitation program. They cannot sign off on a Rehabilitation assessment examination or Rehabilitation program form, or any other form associated with workplace rehabilitation. These determinations can only be made by a delegated employee of the organisation.

40
Supporting effective workplace rehabilitationThe employer provides information, systems and resources so that the Rehabilitation Case Manager (RCM) can identify and support employees to safely stay at work and/or return to work.
For example:
» information about employees to enable them to make decisions about RCM involvement
» information about workplace injuries, illnesses and prolonged absences, so the RCM can offer appropriate and timely assistance and support
» human resource information systems which allow the RCM to collect, monitor and evaluate WHS incident reports, absence and illness data
» access to an early intervention budget and guidelines about how and when to use this budget
» supervisor support for rehabilitation through provision of suitable duties for employees
» performance measures to monitor and improve injury management and rehabilitation practices.
A comprehensive workplace rehabilitation management system which incorporates these and provides access to information, resources and systems, is the key to developing and maintaining effective workplace rehabilitation.
The rehabilitation management systems approachA management system is a documented framework of processes and procedures formulated from an organisation’s strategic direction. A rehabilitation management system documents all stages of rehabilitation and return to work using a methodical, structured framework including identification, management, resourcing, monitoring and evaluation.
Why use a management systems approach to rehabilitation?
Rehabilitation management systems allow scheme employers to:
» provide a safe and healthy workplace for employees
» meet duty of care responsibilities
» assist employees
» communicate rehabilitation responsibilities to employees
» determine accountability of rehabilitation processes and outcomes
» demonstrate compliance with legislation
» promote management accountability for workplace injuries and rehabilitation
» implement continuous evaluation and improvement processes
» ensure that WHS issues are investigated after workplace injuries
» recognise and address failures in workplace rehabilitation
» recognise and strengthen successful steps in workplace rehabilitation.

41
Developing a rehabilitation management systemComcare has developed a complete guide to rehabilitation management systems—Improving outcomes through rehabilitation management systems: a continuous improvement guide. It provides guidance materials and examples to help develop a rehabilitation system or to review current systems for continuing development and improvement.
The guide contains a five-step model for rehabilitation management which provides for continuous improvement. The following are selected examples from each of the five steps. For full details, refer to the complete guide on the Comcare website.
1. Commitment and corporate governance
Sound corporate governance is the process by which organisations are directed, controlled and held to account. The employer’s executive will provide stewardship for its rehabilitation management systems and commit adequate resources to ensure continuous improvement.
The employer will document its commitment to rehabilitation. This documentation will benchmark the employer’s objectives, be used to formulate strategic direction and be reviewed to ensure it remains relevant to the employer and strives for continuous improvement. It will be endorsed and supported at the executive level and be relevant to the employer’s overall values, vision and business objectives.
Senior management promotes a workplace culture which supports active participation in workplace rehabilitation by:
» taking workplace rehabilitation issues seriously
» ensuring that the role of RCMs is valued and acknowledged as important
» encouraging supervisor support for rehabilitation
» discussing workplace rehabilitation at high-level meetings
» promoting efficient workplace rehabilitation practices as important for productivity.
Compliance with legislation—to achieve effective return to work outcomes consistent with employer obligations under the SRC Act, the organisation needs to have a rehabilitation policy which describes how injuries will be managed and outlines an employer’s commitment to injury management and workplace rehabilitation.
A rehabilitation policy should be:
» developed in conjunction with employees
» endorsed by senior management, communicated throughout the organisation, and accessible to all employees
» tailored to the specific requirements of the organisation.
42
A rehabilitation policy should include information about:
» senior management commitment and accountability
» rehabilitation objectives
» early intervention
» communication strategies
» ongoing monitoring and evaluation mechanisms
» case management delegation, role and responsibilities
» workplace rehabilitation provider management.
The Rehabilitation Guidelines will assist organisations to formulate a rehabilitation policy. The guidelines form a starting point for the development, monitoring and evaluation of workplace rehabilitation.
2. Planning
In consultation with relevant stakeholders, the employer develops plans to support its management systems. During the planning stage procedures for rehabilitation management and objectives, and targets and measures for success of injury management performance should be identified. Rehabilitation management planning should include procedures for early intervention and arrangements with workplace rehabilitation providers.
Rehabilitation management—document the approach to developing, managing, monitoring and reviewing all aspects of rehabilitation programs, from initiation through employee consultation and engagement to program finalisation and closure.
Early intervention—a management systems framework to enable early intervention. It includes:
» providing employees with clear information about reporting, contact procedures and the assistance available
» monitoring and managing absence and risk factors
» ensuring that appropriately skilled professionals are available to inform the workplace response to injury
» allocating rehabilitation resources to treat employees fairly and consistently
» providing training to develop people-management skills, and resources to support supervisors and RCMs to carry out their responsibilities in early intervention
» focusing on strategies to improve leadership and positive atmosphere to build a healthier workplace.
Injury management performance—objectives should be aimed at improving prevention and management of injuries in the workplace. They enable evaluation and improvement of performance and reporting against external injury prevention and management indicators.
Workplace rehabilitation provider arrangements—the employer is responsible for monitoring the quality, timeliness and cost of workplace rehabilitation providers. Service level agreements provide a formalised arrangement about the method for monitoring quality, timeliness and cost of services.

43
3. Implementation
The employer ensures that sufficient resources and supporting mechanisms are provided to achieve its strategic plans. This stage documents the resources, capabilities and mechanisms required to achieve the rehabilitation outcomes. Some aspects to consider include how suitable duties will be identified for employees and how privacy will be ensured.
Identification of suitable duties—the rehabilitation policy and management system should provide documentation to encourage supervisors to find and develop suitable duties which match the capabilities and restrictions of an employee. This in turn enables a smooth, early and safe return for the employee.
Privacy legislation aims to protect the rights of individuals by regulating the way information about them is collected, stored, used and disclosed. Ensure that procedures for protecting the information about employees are documented and that there is access to adequate secure storage facilities and a private room for phone calls and meetings.
4. Measurement and evaluation
The employer measures, monitors and evaluates its performance and takes prompt corrective action when necessary. The employer provides data for analysing the quality and outcome of its rehabilitation programs, reporting to senior management, to employees and to Comcare, and to develop plans for improvement.
This stage requires that the employer measure and evaluate a range of rehabilitation markers including rehabilitation programs, determinations, workplace rehabilitation provider performance, costs, and timeframes, and compare them with the measures, objectives and targets developed during the development of the rehabilitation systems.
5. Management systems review and improvement
The employer regularly reviews and continually improves its systems. Review of the rehabilitation performance during the previous stage allows the organisation to learn from past experiences, implement remedial actions where appropriate, and develop plans for continuous improvement.
These five stages form a framework for the development, management and constant evaluation of the rehabilitation management systems. For a comprehensive review of your current systems, refer to the complete guide.
44
Options for the provision of case management services
There are several options for providing workplace rehabilitation case management services that satisfy the requirements of the SRC Act:
1. Resource the function fully in-house:
» The organisation’s RCMs are employees with delegation under the SRC Act to provide all rehabilitation authority functions and powers. One variation under this option is to have a small number of specified staff who have delegation. They work closely with return to work coordinators who do not have delegation but perform many of the case management tasks.
2. Contracting external RCMs:
» An external consultant contract RCM can be engaged. However, rehabilitation powers or delegations cannot be outsourced, and remain with an employee delegate in the employer organisation. These services will not be paid by Comcare as the organisation is contracting out an HR function.
3. Mixture of both:
» This allows the organisation to effectively allocate expertise, resources and staff as necessary. This model can be useful in managing resources.
» Check the organisation’s rehabilitation management system about case management delegation and resourcing.
Consultant and contract RCMsIf the organisation outsources case management functions, the SRC Act requires that some of the powers of case management are performed by employees of the organisation (see Delegation).
Rehabilitation arrangements that have been outsourced require:
» nominating a specifically delegated manager in the organisation with whom contract RCMs must liaise
» the delegated manager, as an employee of the organisation, approving and signing off key paperwork including all rehabilitation determinations
» compliance with privacy obligations under the Privacy Act 1988
» a rehabilitation management system that clearly outlines how using a contract case manager will still meet the employers obligations under the SRC Act.

45
Organisational resources for rehabilitation case managementFor the case management function to be performed efficiently and effectively, the organisation must provide adequate staffing, support, practical and financial resources.
As outlined above, the role of the RCM involves many functions at operational and strategic levels. To determine caseload allocation for individual RCMs consider the following:
» the expertise and experience of individual RCMs
» the number and complexity of the cases being managed
» support systems available to assist the return to work process
» the organisation’s commitment to workplace rehabilitation
» the geographic spread of cases and need for travel
» providing services to remote localities
» other tasks performed by the RCM.
For more information see Rehabilitation resourcing: How do you know that you are allocating adequate resources to manage rehabilitation?
There are some practical considerations relating to privacy and confidentiality issues. Rehabilitation case managers require access to private meeting areas to hold confidential discussions with employees, supervisors and rehabilitation providers. Secure storage facilities for confidential case management files are also necessary.
To avoid interruptions to an employee’s rehabilitation program, there must be alternative arrangements to cover a RCM’s absence, increases in workloads, or other unforeseen circumstances.
New RCMs should be supported to ensure that they are able to support rehabilitation outcomes effectively. They should be made aware of the organisation’s policies and procedures (including the rehabilitation management system), given access to injury data and contact details for support and advice.
See the resources section of this handbook for further information about resources available to support RCMs working in the Comcare scheme.

46
PART 2
SECTION 4
THE ROLE OF THE REHABILITATION CASE MANAGER
Section 2 described workplace rehabilitation and its underpinning principles. This section discusses the role of the Rehabilitation Case Manager (RCM) in managing rehabilitation and return to work.

47
Key points » Rehabilitation Case Managers (RCMs)
have operational roles and strategic roles
» Comcare provides supports for RCMs in the form of training and education, forums, a helpdesk and publications.
RCM role outlineThe role as a RCM covers both strategic and operational responsibilities. The RCM is normally the focal point within the employing organisation for achieving a critically important human resource objective—the reduction of the impact of injury in the workplace.
The functions of a RCM fall broadly into two areas:
» operational—providing assistance to individual employees
» strategic—managing broader issues of return to work in the organisation.
The operational responsibilities include: planning for rehabilitation programs, consultation and day-to-day coordination of individual rehabilitation programs, and management of rehabilitation providers.
The strategic responsibilities include: planning, monitoring and evaluating the organisation’s policies, programs, systems and resources which impact on workplace rehabilitation. These provide a framework to ensure that all the tasks required to achieve the rehabilitation objectives and implement continuous improvement plans can be fulfilled.
Functions of a RCM—OperationalThe operational focus of the RCM’s role is to assist employees and their supervisors following an injury or illness which is compensable under the SRC Act.
This handbook is targeted at the rehabilitation management of injuries and illness compensable under the SRC Act. However in some organisations, RCMs may also provide support and assistance to employees with non-compensable injuries and diseases. The principles of workplace rehabilitation are similar for both. Minimising the human and financial cost of injury and illness is the responsibility of the RCM, and occurs through early and effective workplace rehabilitation. Much of the advice in this handbook is applicable to non-compensable injuries and illnesses.
The role of the RCM includes:
» facilitating early assessment of the employee’s workplace rehabilitation needs
» ensuring that the employee receives appropriate early intervention services as soon as possible following injury or illness—this is not dependent on claim submission or claim determination
» supporting line managers with injury management and resolving workplace issues that may impact on the success of the employee’s return to work
» working in partnership with Claims Managers to ensure a shared understanding of rehabilitation goals and alignment with medical treatment
» ensuring that all key stakeholders consult and participate in developing and implementing the rehabilitation program
48
» working with the employee, their supervisor, medical practitioner and the workplace rehabilitation provider to determine the rehabilitation goals and content of the rehabilitation program
» communicating clearly with the employee’s medical practitioner
» outlining potential suitable duties for a safe and early return to work
» maintaining a focus on return to work
» engaging and monitoring the services of the workplace rehabilitation provider in line with requirements detailed in Comcare’s Operational standards for rehabilitation program providers
» ensuring that the rehabilitation program follows the return to work hierarchy
» maintaining contact with the employee, coordinating workplace meetings and case conferences
» if recovery does not progress and there is a delay in the return to work, arranging a review of possible barriers and implementing a revised program to address the identified barriers
» ensuring the confidentiality of information about the employee
» ensuring the employee receives ongoing support in the workplace.
Selection of a RCMThe RCM‘s role is critical in reducing the impact of injury in the workplace.
Section 41 of the Rehabilitation Guidelines state that the rehabilitation authority should:
… ensure that people with case management responsibilities are delegated, have the skill, experience and influence to achieve effective return to work outcomes.
It is crucial that staff appointed as RCMs are skilled and empowered to influence effective return to work outcomes. Case management requires strong management, project management, and administration and people skills. A RCM needs adequate training and comprehensive support from senior managers to ensure that they are able to undertake the role effectively.
Functions of a RCM—StrategicIn addition to individual case management procedures, the RCM often has a strategic role in developing, reviewing and evaluating rehabilitation practices and policies within their organisation. These will be described fully in the next section.
Training, education and support
Training programs
Comcare has developed training, education and resource material to support RCMs in their role, and they can attend Comcare training such as:
» SRC Act in a day
» A rehabilitation delegates guide to case management
» A rehabilitation delegates guide to complex cases.
See www.comcare.gov.au/training for more information.

49
RCM core capabilities
Comcare has developed a comprehensive framework that outlines RCM core capabilities and is available on our website.
Help desk
The Injury Management Advisory Service (IMAS) provides a help desk service to assist RCMs, employers and workplace rehabilitation providers to support people back to work. IMAS also provide information on the Comcare website to answer frequently asked questions (FAQs). For the help desk service, call Comcare and ask for the IMAS helpdesk, or email [email protected].
More information and FAQs are available at www.comcare.gov.au.
Forums and conferences
Comcare conducts RCM forums and a biennial conference to keep RCMs informed of developments in workplace rehabilitation practices. See the Comcare Events page at www.comcare.gov.au.
Publications
Comcare has a range of publications on the Comcare website to support RCMs to perform their role effectively.

50
PART 2
SECTION 5
ROLE OF THE WORKPLACE REHABILITATION PROVIDER
The SRC Act provides for the rehabilitation of employees of scheme employers following a work-related injury. The legislation is designed to ensure that the employer, as the rehabilitation authority, is responsible and accountable for the safe and early return to work of their employees. Rehabilitation providers play an important role in this process.

51
Key points» Workplace rehabilitation providers
(WRPs) play a pivotal role in the return to work process.
» The employer, as the rehabilitation authority, has access to Comcare approved workplace rehabilitation providers.
» A workplace rehabilitation provider can be contracted by the rehabilitation authority to undertake services under sections 36 and 37 of the SRC Act.
» The Rehabilitation Guidelines stipulate the circumstances in which a WRP shall be engaged and when a WRP should be engaged.
Workplace rehabilitation providers under the SRC ActComcare WRPs are organisations with approved consultants who are able to provide rehabilitation assessments and rehabilitation programs to employees of scheme employers. Comcare’s approval and renewal process ensures that employers have access to skilled and cost-effective rehabilitation providers. The full list of approved providers is published on the directory of approved workplace rehabilitation providers.
A rehabilitation authority can provide a rehabilitation program itself for the employee. However, if the rehabilitation authority requests an external person or organisation to provide the rehabilitation program, it must be a rehabilitation provider who has been approved by Comcare.
Comcare approves providers under the Nationally consistent approval framework for workplace rehabilitation providers which was introduced by all workers compensation jurisdictions in 2010.
This framework has introduced the following:
» mandatory conditions of approval (which are the overarching requirements to operate as a provider)
» principles of workplace rehabilitation (which are the foundation elements of the organisation’s service delivery model and define service provision, organisational and administrative infrastructure, staffing and quality principles)
» a model of workplace rehabilitation which is aimed at an early and safe recovery at, or return to work
» minimum qualifications and experience for individual consultants
» use of evidence-based methods for identification of barriers to return to work
» an agreed code of conduct for WRPs
» practice standards for workplace assessment, functional assessment, and vocational assessment and counselling
» a consistent and transparent self-evaluation (and independent audit) process and audit tools.
In limited cases (for example in a remote location) the rehabilitation authority may be unable to engage a suitable WRP. In these cases it may be possible for Comcare to provide a one off limited approval for a local practitioner that meets Comcare’s requirements. For more information contact Rehabilitation provider approvals at [email protected].
There are three return to work (RTW) rates for WRPs which are published on the Comcare website.

52
WRPs are required to achieve the following RTW rates measured at the cessation of provider services (final rehabilitation program closure):
1. Same employer RTWTarget: 90% RTW rate
2. New employer RTWTarget: 60% RTW rate
3. Rehabilitation program success—RTW durability.
The WRP is required to achieve the following proportion of workers who remain in employment 13 weeks following their final rehabilitation program closure:
Target: 85% RTW rate
For Comcare claims, information on the RTW rates achieved by the provider is collected via the submission of closure forms. The submission of these is mandatory at the end of every rehabilitation program managed by the provider.
In addition, every individual rehabilitation consultant wishing to deliver rehabilitation program services must have an ID number demonstrating that they:
» meet qualification, professional registration and membership criteria
» have relevant workplace rehabilitation experience or are being supervised by an approved provider
» have attended Comcare training about the SRC Act and their role in workplace rehabilitation.
Each WRP company has a unique Comcare number, and each individual rehabilitation consultant has a consultant ID number.
WRPs are approved for a three-year period. Full details of the approval requirements for WRPs are available on Comcare’s website at www.comcare.gov.au.
Circumstances in which a workplace rehabilitation provider is engagedThe circumstances in which a WRP/approved rehabilitation provider is engaged are outlined in the Rehabilitation Guidelines. For further information see:
» Chapter 4—Part II, Rehabilitation program
» paragraph 27, Circumstances where an approved rehabilitation provider shall be used
» paragraph 28, Circumstances where an approved rehabilitation provider should be considered.
Functions of the workplace rehabilitation provider A WRP can undertake one or several of the following services.
Rehabilitation assessment (section 36, SRC Act)
A rehabilitation provider can undertake a rehabilitation assessment to determine an employee’s capability to undertake a rehabilitation program.
Part 3: Section 6, Step-by-step guide to workplace rehabilitation in this handbook contains detailed information about rehabilitation assessments. The following information provides a brief summary.
The assessment should include, but is not restricted to:
» an initial interview
» a worksite assessment
» a workplace meeting involving the supervisor/manager
» meeting and consulting with the treating medical practitioner
» liaison with other treating practitioners.

53
Some rehabilitation assessments may involve more comprehensive services, depending on the nature and severity of the injury and the nature of the employment. These may include:
» specific work tolerance assessment for the employee’s pre-injury job
» job analysis
» identification of transferable work skills
» ergonomic assessment
» psychological assessment for return to work
» development of a rehabilitation program
» development of return to work strategies such as graduated return to work schedule, modified duties or pacing activities.
The WRP documents the findings of the rehabilitation assessment and makes recommendations in the assessment report about a suggested rehabilitation program. These recommendations should be discussed with the employee, the treating medical practitioner and the delegated RCM.
Rehabilitation and return to work (section 37 of the SRC Act)
Development and approval of the rehabilitation program
The rehabilitation assessment forms the basis of the rehabilitation program the WRP develops for the employee. The rehabilitation program documents the rehabilitation goals, expected timelines and dates, and may include a return to work schedule. This document also details the services the rehabilitation provider will provide during the rehabilitation program and the costs associated with those services.
Examples of rehabilitation programs are included in section 8 of this handbook.
After consulting with the employee and the WRP, the delegated RCM—as the representative of the rehabilitation authority—should consider the recommendations and determine whether the employee should undertake the specified rehabilitation program. By approving the rehabilitation program, the RCM is also approving the services and costs.
Refer to rehabilitation planning in section 6 for further information on developing a rehabilitation program.
Management of return to workThe WRP is responsible for managing the workplace rehabilitation program and for the delivery of all services detailed in the rehabilitation program. These services might include:
» monitoring the rehabilitation program
» liaising with the employee, supervisor, treating medical practitioners and RCM
» attending workplace meetings
» attending medical review appointments
» developing return to work schedules which detail upgrade of suitable duties and work hours
» providing rehabilitation progress reports
» maintaining or improving the employee’s performance of activities of daily living.
Liaison with key stakeholders
WRPs liaise with a variety of stakeholders in the return to work process and provide the link between the workplace and medical practitioners. With their experience in consultation and negotiation, their service and support is significant in ensuring that

54
all stakeholders understand what happens during workplace rehabilitation and their role in the process. They also maintain the focus on optimal return to work outcomes.
Specialised services (section 37, SRC Act)
WRPs can provide specialised services. These can be included as part of a rehabilitation assessment or rehabilitation program, or provided as a separate assessment service.
Functional assessments
A functional assessment determines the employee’s current functional capacity and work potential by evaluating the employee’s abilities and limitations against the work tasks and identified work-related criteria.
Functional assessments can assist with informing the medical practitioner about the employee’s capabilities, and how to ensure safety at work.
Cognitive assessments
A cognitive assessment tests cognitive functions such as memory, attention, concentration, new learning, planning and problem-solving capacity, spatial abilities and the ability to make decisions and carry them through.
Vocational assessments
During a vocational assessment the WRP assesses the nature of the employee’s work, and assesses the suitability of work duties, by assessing the physical, psychosocial, cognitive and communication demands of the job. The assessment identifies any risk factors that may place the employee at risk of any physical or psychosocial injury or illness, and determines whether workplace modifications or job redesign are required to support a safe return to work.
If necessary, the vocational assessment might analyse possible alternative duties or employment.
Vocational counselling
Vocational counselling might be required if an employee cannot return to pre-injury duties. Counselling assists the employee to explore realistic job options, and to identify and strengthen job maintenance skills and motivation. If necessary, vocational counselling assists the employee to adjust to changed employment circumstances and/or to seek new vocational goals. It might include identifying and assessing a suitable and realistic range of vocational options based on the return to work hierarchy and in line with the definition of ‘suitable employment’ as defined in part I, section 4 of the SRC Act.
Refer to section 6 for more information on the return to work hierarchy and suitable employment.
Job search activities
WRPs work with the rehabilitation authority to find positions suitable for the employee within the workplace, wherever possible. However, if it is not possible to find an appropriate position within the organisation, and the employee is unable to return to the pre-injury employer, WRPs can provide job search support. They can assist with searching and negotiating an outside placement for work trials and permanent placement if redeployment is necessary.
55
Activities of daily living assessments
An ‘activities of daily living assessment’ (ADL) is conducted at the employee’s home to identify and solve problems caused by the impact of the injury on mobility, personal care and household activities. The assessment focuses on maintaining independence by providing modification of tasks, equipment prescription, as well as education and advice. The ADL provides coping strategies for self-care, home duties and recreational activities, thereby improving overall mental state and wellbeing. It provides education on correct techniques and task simplification and promotes an increase in functional abilities through a graduated home activity program. The ADL eliminates non-work related factors that may be inhibiting successful return to work. In addition, many of these coping strategies can be transferred to the work situation.
Driving assessments
A driving assessment will determine whether training or vehicle modifications are needed after a workplace injury.
A driving assessment is strongly advised for an employee about to begin driving who:
» has never driven before or not driven for a prolonged period since sustaining an injury
» is ambivalent about their ability to manoeuvre a vehicle, to see or react quickly to other vehicles or dangerous situations
» has experienced a change in physical ability since sustaining the injury.
Injury management education and training WRPs can provide or arrange for injury management education and training for employees. The training provides general education about how to manage a type of injury or condition to prevent further injury—for example, correct posture at work and office ergonomics. This training enables the employee to safely achieve an early return to work.
Selecting a workplace rehabilitation providerBefore engaging a WRP to deliver services under the SRC Act, ensure that Comcare has approved the rehabilitation provider. This means that the company has a Comcare WRP number and the individual rehabilitation consultant also has an ID number.
Comcare maintains details about current WRPs on its website, including:
» contact details on a state-by-state basis
» the services offered by each WRP
» geographic coverage
» areas of interest and expertise.
The choice of WRP is the rehabilitation authority’s responsibility and is, therefore, at the RCM’s discretion. Issues that should be considered in choosing the WRP include the nature of the injury and the qualifications and expertise of the rehabilitation provider. For example, in general, occupational therapists and physiotherapists are trained and experienced to undertake workplace assessments and manage employees with physical conditions. Psychologists and rehabilitation counsellors may have better skills in managing employees with psychological conditions. However

56
there are some occupational therapists and physiotherapists that have extensive experience in dealing with employees with psychological injuries and psychologists and rehabilitation counsellors that manage physical injuries very competently. The key element here is to understand the skills and experience of the rehabilitation provider and match the needs to the employee. Do not just base it on the professional qualification of the rehabilitation provider.
Other factors to consider when choosing a rehabilitation provider include:
» the geographical location of the employee
» work related factors, such as workplace conflict, which may impact on rehabilitation outcomes
» non-work related factors
» the services and skills of the WRP, including any relevant areas of expertise
» contractual arrangements with a preferred WRP in the organisation’s procurement guidelines
» consultation with the employee on the choice of WRP
» WRP’s costs, timeframes and outcomes
» the arrangements for monitoring the quality of the WRP’s services.
As already noted, the delegate of the rehabilitation authority can choose the rehabilitation provider for individual rehabilitation programs. However, the employee may have strong preferences about the selection. As a successful return to work outcome is more likely when an employee has confidence in the rehabilitation provider, the employee’s choice and preference can be considered in the decision. If there is disagreement about the choice of WRP, the RCM makes the final
decision. The RCM must be clear about the reasons for the decision and the employee should be given the opportunity to explain their reasons for a different preference.
The delegate for the rehabilitation authority is responsible for:
» selecting the WRP organisation
» selecting an individual consultant within the WRP organisation with experience and skills in the specific medical condition experienced by the employee
» monitoring each rehabilitation program
» providing Comcare with information about WRP performance.
Preferred workplace rehabilitation providers A rehabilitation authority can establish contracts with one or a number of preferred WRPs. The advantages of using a preferred WRP include:
» specialist expertise in managing injury types common to the organisation
» familiarity with the workplace
» consistent achievement of durable return to work outcomes
» an in-principle agreement which allows employees to be referred quickly for specialised rehabilitation services
» specialised prevention services such as workplace assessments
» early intervention before submission of a claim
» a negotiated fee structure
» service level agreements with expectations for rehabilitation outcomes.

57
The Criteria and operational standards for workplace rehabilitation providers 2015 have been developed to ensure that Comcare consider all relevant aspects of the national framework when approving and renewing providers. This and the Heads of Workers Compensation Authorities Guide: Nationally consistent approval framework for workplace rehabilitation providers are a starting point for service arrangements and form a minimum expectation for service delivery. These documents are available from the Comcare and the Heads of Workers’ Compensation Authorities websites.
If the organisation has preferred rehabilitation providers, this should be identified in the rehabilitation policy.
Approved in-house workplace rehabilitation providers
In-house rehabilitation providers are employees of the employer organisation who solely provide rehabilitation programs to the employees. The role of an in-house provider is the same as an external rehabilitation provider and should not be confused with the RCM role.
The process for approval of an in-house rehabilitation provider is the same as the approval process for all other WRPs. The employer organisation must apply to Comcare to have the in-house rehabilitation provider approved in the usual manner and meet the same standards as external WRPs.
Visit Comcare’s website for further information about approval for rehabilitation providers to operate under the Comcare scheme.
If the organisation has applied to Comcare to operate as an in-house WRP, referral to the in-house service must not be compulsory. The delegate of the rehabilitation authority always has the option to refer individual employees to an external WRP.
Procurement of servicesOnce a suitable WRP is identified a referral is made for a rehabilitation assessment under section 36 of the SRC Act. For Australian and ACT Government, an assessment can be requested using the Comcare form Rehabilitation assessment examination. Licensees have a similar form specific to their organisation.
Before accepting the referral, the WRP is expected to negotiate the nature of the required services, the expected outcome, timeframe and proposed costs for the rehabilitation assessment. The RCM’s signature on the referral form approves the assessment and the associated assessment costs specified in the referral.
Once the assessment has been completed and the assessment report accepted, the RCM chooses who will develop the rehabilitation program. This is usually the WRP who completed the rehabilitation assessment and report, but it does not need to be.
During development of the rehabilitation program, the WRP is expected to negotiate the services and costs required for the program.
Once the RCM has signed the rehabilitation program, they have approved the rehabilitation services, timeframes and costs specified in the program and forms a contract with the WRP.

58
Monitoring workplace rehabilitation provider performanceThe performance of a WRP is monitored in two ways.
Comcare monitors WRPs against the nationally consistent approval framework conditions and requirements throughout the approval period and at renewal (each three years). Comcare must be satisfied that they have met and will be able to continue to meet the required standards. In addition, Comcare may conduct an audit of the provider’s performance at any time.
In addition to formal approval and monitoring by Comcare, there is a role for the RCM as the delegate of the rehabilitation authority to actively monitor and manage rehabilitation provider performance across individual assessments and programs. This is because the WRP delivers services directly to the employer organisation rather than to Comcare. If the organisation has a contract with the WRP and formalised service level arrangements, these arrangements can be applied. If there is no formalised contract, their performance should be monitored against the Comcare prescribed criteria and standards.
Changing the workplace rehabilitation providerThe rehabilitation authority can change the rehabilitation provider during a rehabilitation program. This means that the RCM can change the rehabilitation provider if they are not satisfied with their performance. The RCM can also consider changing the rehabilitation provider if the employee requests a change, however they must agree with this decision and see a benefit in doing so.
If the RCM considers that a change in rehabilitation provider is necessary, Comcare recommends the following actions:
» evaluate the WRP’s performance against the service level agreements
» provide feedback to the WRP and the opportunity to respond and improve performance
» consider the cost implications and the disruption to the rehabilitation program
» consider if using another consultant from the same WRP organisation might overcome the issues
» discuss the reasons for wishing to change WRP with the employee
» provide feedback to the provider approval team at Comcare.
Contact Comcare’s provider approval team in the Authorisation and Audit Team if you wish to lodge a formal complaint about the WRP’s performance.

59
PART 3
SECTION 6
STEP-BY-STEP GUIDE TO WORKPLACE REHABILITATION
This section provides a step-by-step guide to workplace rehabilitation and return to work under the SRC Act. It details the activities and tasks involved at each step of a return to work.

60
Key points» Adopt a risk-management framework to
rehabilitation planning.
» Evidence shows that early intervention is a vital element in achieving optimal rehabilitation outcomes.
» Ensure adequate stakeholder engagement in the workplace rehabilitation process.
» Careful planning of assessment and rehabilitation programs sets realistic and achievable goals.
» Incorporate legislative and guidance requirements, including Guidelines for Rehabilitation Authorities 2012 issued by Comcare.
» Monitor and review cases as determined by the risk-management approach.
» Adopt regular evaluation mechanisms to continually improve organisational practice in workplace rehabilitation.
Risk management framework for rehabilitationSome employees return to work with little or no help or support. However, many require assistance to return to work and some may need considerable help and support. In some cases recovery from injury can be significantly delayed, and these employees may experience incapacity from work for extended periods. These employees need active management to improve not only their return to work outcomes but also their recovery from injury. Being able to identify and manage risk factors is crucial to the success of this framework.
The approach outlined below will help the RCM to follow a clear protocol and accepted framework for injury management. The injury management checklist can be used to ensure that the important aspects of the rehabilitation and return to work process have been considered.

61
Injury management checklist
Yes No Comments and datesList the reference in the Rehabilitiation Guidelines that you have applied
Injury occurs
Is intervention required?
Rehabilitation assessment requested?
Decision made as to who will conduct the assessment?
WRP engaged?
Medical practitioner engaged?
Supervisor engaged?
Section 36 assessment received?
Actions from section 36
Rehabilitation program developed?
Sign off—delegate
Sign off—WRP
Sign off—employee
Sign off—supervisor
Copy provided to GP/treating doctor
Progress reports received (provide dates)
Contact with employee (provide dates)
Contact with supervisor (provide dates)
Alteration required?
Alteration signed?
Table 1: Injury management checklist
Early intervention is the foundation of the risk management framework for rehabilitation. It focuses on immediate integrated active management to maintain employees at work or plan and assist their safe and early return to work.
62
Identifying and managing risk factorsResearch undertaken by Professor Sir Mansel Aylward CB (Director of the Centre for Psychosocial and Disability Research at Cardiff University), provides evidence that biopsychosocial factors, such as belief, have a proactive role in the presentation of illness, recovery and probability of return to, and retention in, work. His research The Power of belief: harnessing its potential to bring about behavioural and cultural change around health, illness and work reports that ill health and disability do not exclusively result from demonstrable pathology but may be meaningfully explained in terms of psychological and socio-cultural factors. These risk factors, sometimes called ‘flags’, include an individual’s beliefs and perceptions—for example about pain and injury—and perceived features of the work or the social environment—such as unsupportive management, perceived time pressure or low job control. These risk factors, together with practices in medicine, employment and compensation systems, can lead employees to experience periods of incapacity and absence from work that can be quite disproportionate to the nature of the injury.
The RCM can identify cases at risk of poor return to work outcomes using risk identification tools such as the ‘flags model’ (refer to appendix 2). This model addresses many risk factors which affect return to work outcomes. In 75 per cent of cases the psychosocial factors, such as the individual’s lifestyle, social circumstance and personal factors, are the dominant barriers to return to work. This tells us that for those who have difficulties returning to work, focusing on the medical condition alone is not enough. Talking with employees, addressing barriers, and building trust and confidence to return
to work are critical to prevent disability and long-term worklessness. The support of the workplace and the way supervisors respond to an injury are important dimensions. A biopsychosocial approach is needed for these cases.
Professor Aylward says:
… long-term worklessness is one of the greatest risks to health in our society. It is more dangerous than the most dangerous jobs in the construction industry, or [working on an oil rig in] the North Sea, and too often we not only fail to protect our patients from long-term worklessness, we sometimes actually push them into it, inadvertently.
Workplace rehabilitation and return to work efforts should include strategies to address these factors and enable early and safe return to work.
Note: It is important that the RCM apply a sense of urgency to the management of these factors within the first 12 weeks—preferably, rehabilitation planning should address these factors by the two to four week mark. To be successful, this approach requires pro-active injury management, as well as effective communication and coordination between the RCM, the employee, supervisor, Claims Manager, medical practitioner and rehabilitation provider. Early intervention at the workplace level has been shown to reduce lost time to one third, halve total claims costs, and have a major impact on reducing long-term off-work claims.
The following steps of the risk management framework follow the rehabilitation flowchart in figure 2.
63
Step 1—Risk identificationThe first step in the rehabilitation process is to identify employees who are at risk of poor rehabilitation outcomes and, therefore, may need the RCM’s assistance to stay at or return to work. An early conversation with the employee will help the RCM to make the decision about whether there are indicators for poor rehabilitation outcomes.
Contacting the employee
Initiating early contact with employees gives the RCM an opportunity to collect information, and to check their need for assistance with rehabilitation. It will also establish a sound basis for a positive working relationship, and provides the employee with information and support.
The choice of time and location for the first meeting will depend on the nature of the workplace, the severity and type of injury, and the personal preference of the employee. If the meeting is at home or in hospital, make sure that this is acceptable to the employee, can be arranged at a convenient time, and does not disrupt treatment activities. If the meeting is at the workplace, consider privacy issues. Privacy is discussed in Part 4: Section 10—Privacy in this handbook.
Improved outcomes with early intervention
A Canadian review of return to work literature4 found that early contact with the employee significantly reduced the duration of work disability, and recommended early contact as a core disability management strategy.
Some questions that may be posed to an employee at an early meeting include:
» Have you had time off work in the past for your injuries?
» What do you understand is the cause of your pain?
» What help or assistance do you think will benefit you?
» How are your employer, your co-workers and your family responding to your condition?
» What are you doing to cope with your pain?
» When do you think you will return to work?
» Do you enjoy your job?
» Have any of your injuries in the past taken a long time to improve?
» Are you worried about not getting better?
Alternatively, the employee may be asked to complete a questionnaire to initiate the RCM’s awareness of issues that need to be explored and potentially addressed or resolved.
The key question to be addressed is ‘What can be done to help this person experience less distress and less disability?’
Other issues that should be covered in the first contact include:
» explain the case management role and that of the other rehabilitation and health professionals engaged in the process
» obtain more information from the employee to establish the need for a rehabilitation assessment and support for return to work
» explain the return to work process, the employer’s role and legislative responsibility
4 Page 5, Institute for Work and Health 2004, Workplace-based Return-to-Work Interventions: a systematic review of the quantitative and qualitative literature, Summary, report prepared by Franche, RL, Cullen, K, Clarke, J, MacEachen, E, Frank, J, Sinclair, S, Reardon, R, Institute for Work & Health, Toronto.
64
» explain the benefits of return to work for the employee
» explain the employee’s rights and obligations in the return to work process
» ensure that the employee is kept in contact with the workplace
» ensure that the RCM obtains a signed Authority and consent for the collection and release of medical information from the employee specifically for the employer to access and share their medical information with relevant parties.
Early interventionEarly workplace rehabilitation activities should begin as soon as possible after an injury, and should not be impeded by a delay in determining liability for the claim—this approach has been endorsed by the Rehabilitation Guidelines. To enable effective early intervention, the organisation should have structures and mechanisms in place to ensure that the RCMs are notified about all work-related injuries, even if the employee is not yet absent from work. Early intervention is described in more detail in section 2 of this handbook.
Remember the importance of early intervention:
And where the cause of loss of work is itself impaired health then unwarranted delay in return to work is often associated with delayed recovery. In most instances we do not have to recover completely before returning to work, provided there is a will and there are means to accommodate the fullest possible restoration of function; physically, mentally and socially.
…
Even health problems that are frequently attributed to work—for example, musculoskeletal and mental health conditions—have been shown to benefit from activity-based rehabilitation and an early return to suitable work.5
Comcare has an Authority and consent for the collection and release of medical information form that authorises the collection and sharing of information between Comcare and various parties. It is available on the forms and publications page on Comcare’s website.
In theory the Comcare claim form provides this authority, however, just as Comcare at times chooses to obtain this additional authority the employer may also wish to develop their own separate authority.
It is also important that the employee’s supervisor maintains contact with the employee during this time, particularly if there has been, or is expected to be, extended absence from the workplace. The supervisor may need the RCM’s support in doing this. The RCM should alert the supervisor to the importance of maintaining regular contact and offer suggestions about how to go about doing this.
5 Australasian Faculty of Occupational and Environmental Medicine Position Statement, 2010, Realising the health benefits of work.

65
Step 2—Rehabilitation assessment under section 36 of the SRC ActNow that the RCM understand the employee’s circumstances, the next step is to determine whether there is a need to arrange a rehabilitation assessment.
The purpose of a rehabilitation assessment is to provide the RCM with an expert, impartial and informed written opinion about whether an employee is capable of undertaking a rehabilitation program. Where the employee is assessed as being capable, recommendations should be made on the kind of program the employee is capable of undertaking, including measures that should be included in such a program.
An RCM exercises the rehabilitation authority’s powers to arrange rehabilitation assessments and rehabilitation programs for employees with a workplace injury or disease. The RCM has this power delegated to them in writing by the Principal Officer of the Rehabilitation Authority. If you are the RCM ensure that you have this written delegation before you sign a determination under section 36 or 37 of the SRC Act.
Assessment may not be required if the RCM is in possession of a written opinion from a legally qualified medical practitioner or suitably qualified person that addresses the capability to participate in a rehabilitation program.
The assessment can be performed by a legally qualified medical practitioner nominated by the rehabilitation authority; a suitably qualified person (other than a medical practitioner) or a panel comprising legally qualified medical practitioners or suitably qualified persons.
It should be noted that the RCM may arrange an assessment but may not perform that assessment unless they are suitably qualified. Experience in case management is not a qualification.
Usually the RCM decides on the need for a rehabilitation assessment. However, if an employee requests a rehabilitation assessment in writing, the RCM must arrange for a formal assessment.
As quoted above, section 36(1) of the SRC Act requires that the employer must provide a rehabilitation assessment at the written request of an employee.
A rehabilitation assessment is usually required if the employee with a workplace injury or disease needs help to safely and effectively return to work. A rehabilitation assessment provides valuable information for the rehabilitation process and the nature of this information will vary depending on the employee’s individual circumstances, the complexity of the injury, the workplace and type of work, and personal and environmental factors that may be relevant to the success of rehabilitation efforts.
The choice of assessor depends on the information required. If information is required about the medical capacity to participate then a legally qualified medical practitioner or a suitably qualified person (such as a psychologist or physiotherapist) will be engaged. If assessments are required to ascertain the capacity to develop and participate in a rehabilitation program, then a suitably qualified person (usually a workplace rehabilitation provider) will be engaged. See Who is most appropriate to perform the assessment?

66
LegislationThe SRC Act tells us that:
Where an employee suffers an injury resulting in an incapacity for work or an impairment,’ an employer ‘may arrange for the assessment of the employee’s capability of undertaking a rehabilitation program.
Impairment has a specific meaning in the SRC Act:
Impairment means the loss, loss of the use, or the damage or malfunction, of any part of the body or of any bodily system or function or part of such system or function.
Section 36(1) of the SRC Act also requires that the employer must provide a rehabilitation assessment at the written request of an employee.
If a rehabilitation assessment is requiredA rehabilitation assessment is usually required if the employee needs help to safely and effectively return to work.
An assessment is recommended in the following circumstances:
» the condition has a slow onset and the symptoms have developed over a period of time—for example, occupational overuse syndrome, and some back and soft tissue injuries
» psychological injury
» medical evidence and the prognosis suggest that there is a possibility of re-injury at work
» if the injury is severe and the employee has significant limitations to work capacity
» there has already been, or is likely to be, more than 3 days off work
» the employee has had a previous injury, or has several concurrent injuries
» relationships with supervisor and/or co-workers have broken down
» if the RCM identifies medical, personal, workplace or social risk factors for poor rehabilitation outcomes and delayed recovery.
The flags model and other useful screening tools for indicators of poor rehabilitation outcomes or delayed recovery are at Appendix 2.
The use of these screening tools is demonstrated in Part 3: Section 8—Case Studies.
Assessments and risk-screening toolsA risk screening tool can help identify employees at risk of long-term disability, development of persistent pain, and failure to return to work.
» They can be a useful addition to a comprehensive assessment.
» They can be used as a brief screen to identify issues that require review, risk factors for the development of a chronic injury or other health sequels, and barriers to recovery.
» Related outcome measures can be used to assist in evaluating treatment effectiveness, and assist in informing clinical decisions about continuing, changing or ceasing treatment.
» They can facilitate communication with RCM and/or rehabilitation providers to assist with required services.
» Standardised measures can be useful for assessment and report writing.

67
While an assessment is being organised the RCM should continue to support the employee.
Studies have shown that best practice injury management—i.e. that which not only meets statutory obligations but also takes into account the complex social, psychological and medical aspects of injury and illness—saves money in the long term.6
Continue to help the employee in the following ways:
» Provide a positive expectation that the employee will return to work and normal activity. This is true of the majority of injuries other than catastrophic injuries.
» Encourage the supervisor to regularly contact and show interest in the employee.
» Help to maintain positive cooperation and collaboration between the employee, the supervisor, the claims and rehabilitation staff and other health professionals.
» Communicate that having more time off work reduces the likelihood of a successful return to work. In fact, longer periods off work result in reduced probability of ever returning to work and to normal life activities.
» Keep the employee active and at work if at all possible, even for a small part of the day. This will help to maintain work habits and work relationships.
» Consider reasonable requests for selected duties and modifications to the workplace.
» Promote self-management and self-responsibility. Encourage the development of self-efficacy to return to work. If recovery is hindered by fear of movement, fear of pain or fear of re-injury, these issues need to be specifically addressed through advice, incentives and feedback from the medical practitioner.
Acknowledgement: information about the risk screening tools and self-management practices courtesy of Safework SA.
If a rehabilitation assessment is not requiredThere will be times when a formal assessment by an external assessor is not required. An external rehabilitation assessment may not be required if most of these circumstances are present:
» the treating doctor supports an early and safe return to work and provides clear medical guidance
» the employee does not have an incapacity for work or has only minor restrictions in capability for work duties
» the type or circumstances of injury are not complex and no delays in recovery are expected
» the RCM’s experience, skills and capacity are sufficient to manage the return to work so long as they accord with the requirements of the Rehabilitation Guidelines
» the RCM has the full support of both the employee and supervisor to achieve an early and safe return to work
» there are effective relationships and open communication between the RCM, the treating doctor, the supervisor and the employee.
6 Australasian Faculty of Occupational and Environmental Medicine, 2010, Realising the health benefits of work—Position statement.

68
If formal assessment for rehabilitation is not arranged then a review process should be established to monitor the situation. The key to this process should be engagement with the employee’s supervisor and the treating medical practitioner. The RCM will be aware of the employee’s current injury status, return to work status and problems as they arise if they maintain communication with the medical practitioner, the employee and the supervisor.
Remember that a rehabilitation assessment can be initiated at any time. Similarly, a referral to undertake a rehabilitation assessment or to develop a rehabilitation program can be made at any time.
If there is uncertainty about the necessity of a rehabilitation assessmentIt is better to be cautious and refer for a rehabilitation assessment if there are any doubts about the need for an assessment or the need for support for the employee to return to work. This is preferable to delaying the decision and discovering later that rehabilitation assistance was required.
If unsure about what to do, the RCM should:
» discuss the situation with the employee’s medical practitioner
» contact the Claims Manager or Comcare injury management advisor for further advice.
Arranging a rehabilitation assessmentThe first step in arranging for a rehabilitation assessment involves choosing an assessor who is legally able to provide an assessment. A rehabilitation assessment under the SRC Act can only be made by:
» a person who is a legally qualified medical practitioner—this could be the treating doctor or another medical practitioner such as an occupational physician
» a suitably qualified person other than a medical practitioner—best practice is to engage a rehabilitation provider approved by Comcare
» a panel of people—one of whom should be the treating doctor.
A suitably qualified person includes:
(a) an approved workplace rehabilitation provider
(b) in relation to an assessment of an injured defence force member, a person nominated by the Military Rehabilitation and Compensation Commission or the relevant Service Chief under paragraph 148(1)(b) of the Act
(c) any person [whether or not an approved workplace provider] who meets the qualifications for a workplace rehabilitation provider consultant.
The RCM arranging the assessment may not perform the assessment unless they satisfy any of the above three criteria—see the Rehabilitation Guidelines for details.

69
Who is most appropriate to perform the assessment?The second step is to choose the most appropriate type of professional to perform the assessment.
Use a WRP both if specified in paragraph 27 of the Rehabilitation Guidelines and if:
» identification of suitable duties and development of a rehabilitation program is required
» the treating medical practitioner is supportive and available to contribute to the development and implementation of the rehabilitation program.
Use a legally qualified medical practitioner (LQMP) if:
» there is a question about work capacity and capacity to participate in a rehabilitation program
» there are complex or significant injuries—for example, psychological injury
» there is an unclear diagnosis or prognosis
» there are significant barriers to returning the employee to the workplace
» there has been prolonged absence or proposed long-term absence from the workplace
» there is more than one injury or disease.
Use a Panel Assessment (which can be a combination of treating general practitioner, medical specialists, such as a psychiatrist or occupational physician, other treatment providers and/or a workplace rehabilitation provider) if:
» the treating medical practitioner and treating medical specialist are uncertain about the work capacity and medical expertise is required regarding work capacity
» there are multiple medical conditions influencing capacity to work
» There is conflicting evidence between medical and treating practitioners in regard to capacity or prognosis
» there are complex psychosocial issues, including psychological injury
» a rehabilitation program is not progressing
» a comprehensive overview of the work capacity and restrictions will benefit decision-making about workplace rehabilitation.
After deciding which type of assessment, consider the type of injury and characteristics of the employee and match them to the skills and expertise of the assessor. For example, an occupational physician or physiotherapist may be suitable for a physical injury and a psychiatrist or psychologist for psychological injuries.
Once a decision is made as to who will undertake the rehabilitation assessment, the next step is to complete a referral for a rehabilitation assessment. Rehabilitation providers that perform assessments under section 36 of the SRC Act must be approved by Comcare as outlined in section 5 of this handbook.
70
Completing the referral for a rehabilitation assessment examinationFor ACT and Australian Government agencies, you may use the Comcare Rehabilitation assessment examination form. A link is included in Part 3: Section 9—Return to work forms in this handbook. Licensees will have a standard referral form designed specifically for their organisation.
Include with the referral form a signed copy of the Authority and consent for the collection and release of medical information pertaining to my claim form, so that the assessor can contact the treating medical practitioners. Information about privacy considerations and the use of this form is provided in section 10 of this handbook.
The Referral for Rehabilitation Assessment form (SRC 116) has been revised following an extensive consultation process during 2012, in line with the Rehabilitation Guidelines. It has been designed to include all the information that is mandatory when sending an employee for an assessment. For example: the assessment includes (amongst other things) information on time and place for the assessment and the employees’ rights in regards to attending the assessment or requesting a review of the decision to send them for an assessment. Sending an employee for a section 36 assessment is a determination under the SRC Act. If you choose to design your own assessment it is recommended that you include all the mandatory elements to ensure that it is a compliant determination. The current forms are regularly reviewed so if your organisation chooses to design their own form based on the current form ensure there is a process for monitoring whether the Comcare form has been updated to meet changes in the workers compensation environment.
The request and referral for a rehabilitation assessment examination must be documented in writing. If the decision to request a rehabilitation assessment is made under section 36 of the SRC Act, this request must follow the requirements of the Rehabilitation Guidelines for a determination. This means that it must be supplied in writing to the employee. It must give the reasons for the decision, and must inform the employee about what to do if they does not agree with the decision.
Content of a rehabilitation assessment reportThe rehabilitation assessment report forms the basis for decisions about the rehabilitation program. Therefore, a comprehensive assessment will include:
» a meeting with the employee to undertake the assessment and examination to determine the employee’s work capacity
» a workplace visit and meeting with the supervisor to plan for the employee’s return to work
» analysis of the employee’s pre-injury duties
» liaison with the treating medical practitioner and other treating practitioners to determine appropriate rehabilitation goals, expected timeframes for recovery, and to ensure that treatment options are evidence based and support return to work
» consideration of suitable alternative duties, or other rehabilitation options if the employee will not be able to return to pre-injury duties in the short or longer term

71
» other specific and appropriate assessments such as functional capacity assessment, ergonomic assessment, work tolerance assessment, transferable skills analysis, vocational assessment or home assessment
» identification of any potential barriers to return to work, and actions and strategies to manage these—the flags model (appendix 2) can be used to identify barriers
» documentation of the rehabilitation assessment and examination findings with a written report containing recommendations about a rehabilitation program.
Note: If the employer has obtained an assessment of fitness for continued duty, this information may be considered when developing a rehabilitation program. However, this cannot be the only information when making a determination—it may, however, be used to support information obtained from a separate assessment for rehabilitation under the SRC Act.
Questions for a rehabilitation assessment under section 36 of the SRC Act with a medical specialistThe RCM should develop questions that will provide them with the most appropriate information to support the employee back to health and to work. What is the key information that is required?
Limit the number to approximately four with an absolute maximum of six questions. Medical practitioners are more likely to provide a thorough, considered response to a few well written questions than a page of questions that appear to repeat themselves.
The questions below are examples only. Comcare does not recommend the use of these specific questions. It is important that the questions used are tailored to the person and their condition and will elicit the required information. Choose the best wording for each individual case.
In general, is it better to provide the doctor with a specific list of available duties and job descriptions that have been assessed as potentially being suitable, rather that ask the medical practitioner to describe the duties the person can undertake.
Example questions/requests
» Please provide guidance in relation to the attached draft rehabilitation program including specific hours and duties.
» Please comment on the suitability of the attached duties and any other advice or recommendations which may assist in a durable and successful rehabilitation program.
» Do you recommend any further rehabilitation assessments or services?
» If a graduated return to work is to be progressed in the future, what timeframes would you suggest, and do you have any other recommendations about this?
» Is X’s compensable condition preventing them from working full-time hours and duties as outlined in the attached workplace assessment report and duty statement?
» Is X fit to perform the inherent duties of a [position] officer?
» Is it appropriate that due to X’s condition, they be assigned alternative duties? If so, what type of duties may be suitable?

72
» Is it appropriate that due to X’s condition, they be assigned alternative duties? If so, are the attached duties suitable?
» Would a graduated return to work program be suitable and, if so, what would be an appropriate program?
» If X is not fit to return to their pre-injury duties, when would you consider it appropriate to conduct a review?
» In your opinion are there any motivational or attitudinal factors impacting on X‘s ability to undertake their pre-injury duties?
» Is the employee fit for duty? If not, when will X be fit for duty?
» Is a graduated return to work program appropriate? If so, please provide guidelines on hours/days per week and the rate of increase in hours.
» How is X‘s condition currently impacting on their capacity to return to work?
» Are any modifications required to the employee’s duties?
» Are there any other issues which should be considered in assisting this employee to return to work?
» Identify X’s capacity to undertake a rehabilitation program given that X has been out of the workforce for an extended period.
» Identify the nature of work X is safe to undertake, given the current status of the compensable condition.
» Identify any requirements that need to be in place to allow a rehabilitation program to be implemented to ensure a safe and durable return to work.
» Identify any barriers that may prevent a return to pre-injury or suitable duties, and suggest some strategies to overcome these.
» Identify current specific work capacity in terms of hours, days and rest breaks required in order to participate in a rehabilitation program.
» Identify a specific upgrading regime for X to ensure a sustainable work outcome is achieved while preventing injury or re-aggravation.
» Suggest a reasonable timeframe for review of capacity to undertake a rehabilitation program if X remains totally incapacitated after this assessment.
» Suggest activities that can be undertaken if X is currently unfit for work that may facilitate a safe return to work in the future.
» How does the current treatment impact on X’s ability to perform pre-injury duties or suitable alternative duties?
A rehabilitation assessment with a workplace rehabilitation providerIf a Workplace Rehabilitation Provider (WRP) is requested to undertake a rehabilitation assessment under section 36 of the SRC Act, the RCM should specify the assessment services required. These might include an initial needs assessment, a proposed suitable duties assessment, a workplace assessment and task analysis. Please refer to section 5 of this manual for information on the services that a rehabilitation provider is able to provide.
During this information gathering stage, the RCM will work closely with the assessor. This facilitates efficient coordination and can produce a faster and less expensive assessment. For example, the RCM should liaise with the supervisor and employee, to document the employee’s pre-injury duties, and identify potential suitable duties available in the workplace. This will assist

73
the treating medical practitioner and the assessor to understand the nature of the duties available in the workplace, and to individualise these to suit the employee’s capacity.
The rehabilitation assessment report forms the basis for decisions about the rehabilitation program. Therefore, a comprehensive assessment report should include:
» an opinion supported by evidence as to whether the employee is fit to undertake a rehabilitation program
» the proposed rehabilitation goals—final and interim goals of the rehabilitation program
» guidance about the duties that the employee is fit to perform, such as potential suitable duties
» recommendations about activities to be avoided—for example, restrictions
» indication of the hours that the employee has the capacity to work
» identification of any psychosocial risk factors for poor rehabilitation outcomes or delayed recovery
» suggestions about how to overcome these risk factors and barriers to return to work
» strategies required to achieve early and safe return to work
» timeframes in which the plan is to be achieved
» the treating medical practitioner’s agreement to the proposed program and associated recommendations
» where the proposed services require a WRP to achieve the program, what those services are and their associated costs.
Where the above information has been obtained and the circumstances align with those prescribed in paragraph 29 of the Rehabilitation Guidelines, the RCM may provide the rehabilitation program without the services of a WRP.
Step 3—Rehabilitation planning
Deciding on a rehabilitation program
The Rehabilitation Guidelines state that in deciding whether an employee should undertake a rehabilitation program the RCM shall have regard for the following:
(a) the recommendations of the rehabilitation assessment
(b) the matters under section 37(3) of the SRC Act, including consultation with the employee, their treating practitioner, supervisor and the approved workplace rehabilitation provider as to the program’s content
(c) where the current rehabilitation authority is not the liable employer, the potential views and contributions of the liable employer to the rehabilitation program content shall be sought including their ability to provide suitable employment.
74
Deciding not to provide a rehabilitation program
Where an assessment has occurred and the RCM decides—having regard to the assessment—that a rehabilitation program is not currently required, the RCM shall make a determination under section 37(1) of the SRC Act and provide written notice of the determination to the employee advising them of the reasons for that decision and the right to request a review of the determination. This can be achieved by completing the Rehabilitation program form and ticking the ‘No’ box in the ‘Is rehabilitation required’ field and then in the space provide document the reasons for the determination.
The RCM shall also provide the employee (in writing) information regarding their rights to request a review of this decision.
Who can provide a rehabilitation program?
Where the RCM determines under section 37(1) of the SRC Act that an employee should undertake a rehabilitation program they shall also decide who is to provide the program. The SRC Act states that:
(a) the employer may provide a rehabilitation program for the employee itself
(b) the case manager may make arrangements for the provision of a rehabilitation program by a rehabilitation provider approved by Comcare
(c) in the case of a current or former defence force member, an approved rehabilitation provider nominated or a person nominated by the rehabilitation authority under section 148(1)(b) of the SRC Act.
Circumstances where an approved workplace rehabilitation provider shall be used
When a decision has been made to provide a rehabilitation program an approved WRP shall be used to deliver rehabilitation services under that program where:
(a) any one or more of the following apply:
(i) the nature of the disease, injury or intended employment requires identified rehabilitation services to support the employee
(ii) bio-psychosocial obstacles for recovery and return to work have been identified that require rehabilitation services
(iii) where the employee is no longer employed by the Commonwealth agency or licensee [or they are unable to provide suitable employment] and the employee requires assistance to obtain suitable employment [for example job seeking and redeployment activities]
(iv) the employee’s condition significantly deteriorates potentially impacting on the program success and they require rehabilitation assistance to remain or return to work
(v) the employee has been or will be medically discharged from military service
(b) the employee requires assistance to return to work or maintain durability at work with the services of an approved WRP as a result of the consideration made under the following paragraph.

75
Circumstances where an approved workplace rehabilitation provider should be considered
The use of an approved WRP should be considered when:
» the employee and case manager are in different geographical locations
» the employee’s disease or injury results, in whole or part, from any perceived or actual conflict in the workplace
» the employee has previously unreasonably failed to undertake or complete a rehabilitation program.
Requirements on the rehabilitation authority when providing a program for the employee itself
A rehabilitation program can only be provided by the case manager [not involving the use of an approved WRP] where:
(a) the circumstances described above (where an approved WRP shall be used), and an approved WRP has been considered unnecessary having regard to the circumstances described under the previous paragraph; and
(b) the case manager has sufficiently clear medical guidance on the proposed rehabilitation program from:
(i) an assessment that been performed under section 36 of the SRC Act, or
(ii) available reports by medical practitioners or other health professionals relating to the employee’s injury, fitness for duty, incapacity for work or impairment, to support and manage the employee’s return to work, maintenance at work, or upgrade of hours or duties without the need for WRP services.
Under any of the circumstances just described, a copy of the rehabilitation program is to be forwarded to Comcare or the relevant authority (for example, a licensee).
Developing a rehabilitation programFor the most effective workplace rehabilitation outcomes, a rehabilitation program should be individualised, outcome based, and have clearly set out steps to be followed to achieve the rehabilitation goals.
Matters that must be considered in determining a rehabilitation programIn determining that the employee should undertake a rehabilitation program a Rehabilitation Authority (in practice the RCM) shall have regard to the requirements of section 37(3) of the SRC Act and:
(a) if it has previously been determined that the employee should undertake a rehabilitation program [whether in respect of the same or a different injury] a case manager shall have regard to whether:
(i) the employee completed the program; and
(ii) if the program resulted in any improvement in the employee’s capacity to work or activities of daily living; or
(iii) if the employee did not complete that program, whether the employee had a reasonable excuse for failing or refusing to complete that program; and
(b) section 15 of the Disability Discrimination Act 1992.

76
When return to work is complicated by both a compensable and a non-compensable condition
There are times when management of rehabilitation and return to work for an employee medically declared as having some or full capacity to work is later incapacitated because they become partially or totally incapacitated due to a separate, non-compensable injury. In these cases please contact the Claims Manager.
If the employee becomes totally incapacitated due to a non-compensable injury, then rehabilitation efforts may have to be modified or stopped until the employee’s capacity improves. If the non-compensable injury is only causing a partial incapacity, then rehabilitation may continue, keeping in mind any restrictions relating to both the compensable and non-compensable conditions. Seek assistance from the Injury Management Advisory Service if in doubt about how to manage these situations.
If the claim is managed by Comcare, issues relating to incapacity payments, personal leave and deeming ability to earn in such circumstances will be managed by the Comcare Incapacity Management Team and the relevant Comcare Claims Manager. If the claim is managed by a licensee then contact the Claims Manager.
Considerations under section 37(3)a–hSection 37 of the SRC Act includes criteria that must be considered in developing and approving the rehabilitation program. These criteria are outlined in section 37(3) and the employer must have regard to these matters in developing and approving the rehabilitation program.
There are eight matters listed in section 37(3) for consideration:
(a) any written assessment given under subsection 36(8)
(b) any reduction in the future liability to pay compensation of the program is undertaken
(c) the cost of the program
(d) any improvement in the employee’s opportunity to be employed after completing the program
(e) the likely psychological effect on the employee of not providing the program
(f) the employee’s attitude to the program
(g) the relative merits of any alternative and appropriate rehabilitation program
(h) any other relevant matter.
In particular, note that point (f) requires that the RCM should have regard to the employee’s attitude to the program. To satisfy this requirement the RCM must be able to demonstrate that the employee’s attitude has been considered. To do this, note the contributions of the employee to the assessment for rehabilitation services, ensure that the employee is provided with the proposed rehabilitation program to consider, and has the opportunity to discuss the program with a medical practitioner, family and other people they might wish to consult. The RCM should document discussions with the employee about responsibilities under the SRC Act, attitude to the program and options if they disagree with the program.

77
This criterion does not mean that a rehabilitation program cannot be provided if the employee does not agree with the program and has requested a reconsideration. The employee is expected to participate in the program. This criterion demonstrates that the employee’s attitude has been acknowledged and addressed as appropriate.
Case law
It has been successfully argued in the Federal Court that unless there is evidence that the employee’s attitude to the rehabilitation program has been considered, the employee may have a reasonable excuse for non-compliance.7
This does not mean that the employee’s attitude should be the determining factor, but it does need to be one of the considerations along with other matters in section 37(3).
Practical implicationsA written draft rehabilitation program should be provided to an employee before making a determination under section 37(1) of the SRC Act.
The goals, responsibilities and timeframes described in the draft program should be explained to the employee, with particular reference to each of the criteria under section 37(3) of the SRC Act. This could be done in writing.
The employee should be given a reasonable opportunity to comment against the draft program and raise any concerns.
Under section 37(3)(f) the employee’s attitude to the draft program should be sought.
The employee should be given the opportunity under section 37(3)(h) to raise any other matter that may be relevant.
Any required changes to the draft program should be made, and the rehabilitation authority should proceed with the determination under section 37(1), if appropriate.
The rehabilitation authority should demonstrate its consideration of section 37(3) in the written reasons for the decision to provide a rehabilitation program (issued under section 37(1)).
Note: The RCM should ensure that they do not simply give ‘token’ or ‘nominal’ regard, but give appropriate weight to each of the matters. Failure to take into account one of the factors in section 37(3) may invalidate the rehabilitation program and result in the provision of a program that would have no legal effect.
The space on the rehabilitation program is generally insufficient to address these criteria adequately. Write the words ‘see attached’ in the space and outline the section 37(3)a–h considerations on a separate document. Attach this document to the program.
Part 2: Section 5, Role of the WRP in this guide provides sample responses for each of these criterion and issues that you need to consider when deciding to provide a rehabilitation program for an employee.
7 McGuinness v Comcare [2007] FMCA 1486 (31 August 2007).

78
The Rehabilitation Guidelines (section 41) issued by Comcare As well as complying with the requirements of the SRC Act, you must also comply with guidelines issued by Comcare. These are the Guidelines for Rehabilitation Authorities 2012 issued under section 41 of the SRC Act. They provide information to assist you, as the RCM, to develop an effective approach to the rehabilitation of employees, consistent with your obligations under the SRC Act.
These guidelines provide information to consider in relation to:
» arranging early assessment of the employee’s capability to undertake rehabilitation, and consider arranging such an assessment when an employee is likely to be away from work for more than 3 days
» assessing the need for, developing, monitoring and closing a rehabilitation program and return to work schedule
» accessing and monitoring the provision of rehabilitation services by an approved WRP
» ensuring the rehabilitation program and return to work schedule are in line with the return to work hierarchy
» maintaining regular contact with the employee and other relevant parties
» ensuring ongoing consultation with the treating medical practitioner
» negotiating workplace trials, placements, graduated return to work and redeployment
» ensuring the confidentiality of information about the employee
» measuring and evaluating and improving rehabilitation services through an effective management and transparent management system.
Case law
A rehabilitation program must be developed in consultation with the employee and the treating doctor to render it valid.8
The Administrative Appeals Tribunal (AAT) has stressed this in its decision to render a rehabilitation program invalid.
Making and notifying the rehabilitation program decisionThe case manager shall:
(a) give written notice to the employee of any rehabilitation program determination made
(b) give a copy of all rehabilitation program determinations to:
(i) the relevant authority
(ii) the approved WRP
(iii) the treating doctor
(iv) the employee’s manager or supervisor
(v) if the employer is not the liable employer, the liable employer irrespective of whether the rehabilitation program was provided by an approved WRP or by the rehabilitation authority itself.
Where costs are incurred in relation to an employee’s rehabilitation program:
(a) the case manager shall promptly provide any certified tax invoices or receipts to the relevant authority; and/or
(b) if the employer is not the liable employer, the liable employer.
8 Ranasinghe and Australian Postal Corporation [2008] AATA 66 (24 January 2008).

79
The return to work hierarchyAfter injury, better health and return to work outcomes are achieved by assisting the employee to resume their former lifestyle, including work activities, as quickly and safely as possible. Workplace rehabilitation addresses an important aspect of this principle through returning the employee to pre-injury duties in their own workplace wherever possible. This principle is supported by a hierarchy of preferences for return to work outcomes.
This does not mean that workplace rehabilitation should attempt a return to work at each successive level. The RCM should consider each level and make an informed decision about return to work goals based
on the rehabilitation assessment findings, and in consultation with the employee and treating medical practitioner. The return to work hierarchy should be considered for developing the short-term return to work goal, and the ultimate goal for the rehabilitation program.
The case studies in section 8 provide examples of rehabilitation planning based on the return to work hierarchy. Case study 1provides an example of a rehabilitation program with the employee working on modified duties, with the same employer. Case Study 2provides an example of a more complex injury requiring different duties with the same employer.
Figure 3: The return to work hierarchy

80
9 Telstra Corporation Ltd v. Slater (2001).
If the employee is separated from ongoing employment, by resigning, being terminated, or accepting a redundancy, then suitable employment becomes any employment for the purposes of rehabilitation.
Case law
For an injured employee on a fixed-term contract, the employer’s liability under the SRC Act does not cease simply because the original contract period has ended. The duty to provide suitable employment continues after the end of the contract period.9
Suitable employment must be work for which the employee is suited, considering:
» the employee’s age, experience, training, language and other skills
» the employee’s suitability for workplace rehabilitation or vocational retraining—this is an important consideration because workplace rehabilitation has an impact on the employee’s capacity to work not only in terms of hours of work, but also the type of work
» where employment is available—employment may well be available for an employee, but it may not be reasonable to expect an employee to move to a different residential location
» any other relevant matter.
A key step in providing suitable employment is identifying suitable duties to assist the employee to return to work as soon as possible. Suitable duties may involve modifications to duties, providing alternative duties, or modifying working hours while on a rehabilitation program. Finding suitable duties and suitable employment requires a constructive and creative approach with cooperation from supervisors and commitment from senior managers.
SUITABLE EMPLOYMENTThe provision of suitable employment is the responsibility of the Rehabilitation Authority (usually the employer).
Legislation
Suitable employment is defined in part I section 4 of the SRC Act:
If the employee who has suffered an injury is an ongoing employee of the Commonwealth then suitable employment is any employment within the Commonwealth.
If the employee who has suffered an injury is an ongoing employee of the ACT Government then suitable employment is any employment within the ACT Government.
If the employee who has suffered an injury is an ongoing employee of a licensee then suitable employment is any employment within the licensed corporation.
If the employee wishes to pursue other employment other than in the above examples then they will need to elect to separate from the organisation (i.e. for employees that continue to be employed, an offer of employment elsewhere in the private sector or outside the Commonwealth is not suitable employment).
If the employee was on a fixed term contract with Commonwealth or ACT Government or licensee at the time of the injury and the contract expires before they are back at work then suitable employment is any employment.

81
To help identify suitable employment:
» ensure that the supervisor and senior managers understand the employer’s legislative responsibility to provide suitable employment under section 40 of the SRC Act
» ensure that the supervisor understands the employer’s responsibility under the organisation’s return to work policy or rehabilitation management system
» discuss with the supervisor any difficulties in finding suitable employment, work collaboratively to identify suitable employment and address any problems which may hinder the provision of suitable employment.
» clarify for the supervisor the consequences of failure to find suitable duties including long-term costs and the implications for the workers’ compensation premium and costs for the organisation
» ask human resources staff to identify vacancies within the organisation
» consider duties in other sections of the organisation
» ask other areas in the organisation to consider suitable projects which the employee could undertake
» ask the employee if they knows of other duties in the organisation which may be suitable
» use the hierarchy of return to work options to identify alternatives, such as a work trial
» ask the WRP for assistance to identify external work trial or employment options
» talk with the Claims Manager.
For further information please refer to Suitable employment: A guide for Rehabilitation Case Managers (PUB 78) on Comcare’s website.
A rehabilitation programA rehabilitation program contains:
» rehabilitation goals (vocational or prevocational)
» communication strategies» timelines » a detailed return to work schedule to
guide the activities the employee will undertake
» clear and detailed list of roles and responsibilities of all parties involved
» activities and costs for the WRP if one will be involved in the program
» information about the rights and responsibilities of the employee
» signature section.
The Rehabilitation Guidelines issued under section 41 of the SRC Act state:
A rehabilitation program should:
(a) be developed in consultation with the employee and the treating medical practitioner
(b) be individualised, outcome-based and set out the steps to be followed in achieving the return to work
(c) be available to an employee with a work capacity (unless contraindicated, for example, where the employee has retired)
(d) be developed using appropriate expertise, such as workplace rehabilitation providers, where required
(e) recognise the existing skills, experience and capabilities of the employee to enable suitable duties to be found
(f) if necessary, utilise retraining and redeployment when it is not possible for the employee to return to pre-injury duties.

82
There are examples of completed rehabilitation program forms used for Australian and ACT Government employees on Comcare’s website.
Studies have shown that in most cases an early return to work (or remaining at work) is beneficial for health and wellbeing and people with musculoskeletal conditions who are helped to return to work enjoy better health than those who remain off work.10
Return to work strategies There are some commonly used methods to support employees during the early stages of their rehabilitation. These include graduated return to work programs, pacing, work trials, redeployment, study and retraining.
Graduated return to work
Graduated return to work can be offered as part of a rehabilitation program and allows employees to return to work on reduced hours or duties when, due to a medical reason, they are unable to return to their full pre-injury hours and/or duties. The graduated return to work recognises that an employee may be able to manage a selected range of tasks for reduced periods.
Graduated return to work is effective because it builds up the employee’s physical and/or psychological ability to manage tasks by using actual work tasks. This form of workplace rehabilitation is called work hardening or work conditioning. It also helps employees maintain their generic work habits such as getting up to go to work, interacting with co-workers, and keeping pace with changes and developments in the workplace, rather than ‘being sick and isolated at home’.
Pacing
Pacing allows an employee to attend the workplace for full normal weekly hours, by alternating between periods of work and periods of rest. The benefit of this approach is that employees do not have extended periods out of the workplace—the work phase of each day is simply increased in line with medical recommendations. As a result the employee maintains periods of attending the workplace for the usual work hours, maintains contact with fellow employees, and does not lose their identity as an employee. This is different from a graduated return to work program, in which the employee is at work for short periods of time, but is working for the majority of that time.
Pacing overcomes the major difficultly identified with the graduated approach to return to work, whereby employees become stuck on four or five hours a day. With pacing, the employee does not have to alter travel, childcare or other arrangements each time the hours of productivity are upgraded. It simply increases the work phase of each hour or day.
If the employee has physical restrictions limiting the number of hours they can work, the employee’s other skills and knowledge do not have to be lost to the organisation for part of the work day, as occurs with part-time graduated return to work schedules.
Pacing can also help prevent the development of longer term disability and pain as it tends to maintain normal daily patterns and regular work routine.
10 Aylward, M et al, Realising the health benefits of work, a position statement. The Australasian Faculty of Occupational and Environmental Medicine, Sydney.

83
How is an employee paid during a pacing program?
Employees are paid their full salary while undertaking a pacing program. There are two options for payment which should be discussed with the Claims Manager.
These are:
» payment of full salary based on the concept that the employee is being paid for attendance, not productivity
» payment as a combination of salary for productive hours and compensation for rest or other periods—this approach can become complicated to administer.
If the employee has been receiving incapacity payments for longer than 45 weeks, the Claims Manager will determine compensation on the basis of the number of hours the employee attends the workplace.
Work trials
A work trial places the employee with a host employer for a defined period of time. The employee continues to be employed by the pre-injury employer.
A work trial may be chosen to:
» provide short-term suitable duties where because of the medical restrictions, the employer is unable to provide suitable duties
» rebuild work skills and self-confidence, and establish work routines after an injury and absence from the workforce
» allow work hardening through a program aimed at improving physical or psychological work tolerances
» promote a return to pre-injury work with the pre-injury employer or, alternatively, placement with a new employer
» learn work skills to improve opportunities for employment
» establish a working relationship with a potential new employer.
The work trial should:
» be an active process involving the pre-injury employer (who remains the rehabilitation authority) the work trial employer, the WRP and the employee
» have clearly defined goals
» have clearly defined, short-term timeframes
» be fully documented in a rehabilitation program.
Issues to consider:
» engage a rehabilitation provider to implement and coordinate the work trial
» the host employer has the same work health and safety responsibilities for the employee as for all other employees of the organisation
» the host employer must monitor the rehabilitation program and make the workplace available to a rehabilitation provider
» the host employer is expected to monitor performance issues and absences and notify the RCM about problems
» changes to the rehabilitation program must be made in consultation with the RCM, the treating medical practitioner and rehabilitation provider
» the employee must adhere to the host employer’s work policies
» the employee must maintain contact with the rehabilitation authority RCM and the rehabilitation provider.
While on a work trial the pre-injury employer is the rehabilitation authority. This means that as the rehabilitation case manager for the pre-injury employer, the RCM is the delegate and has responsibility for the employee. The RCM
84
must oversee the program and sign the forms for the rehabilitation program. The employee’s salary continues to be paid by their pre-injury employer. A Work trial agreement should be attached to the rehabilitation program. Workers’ compensation coverage is by Comcare for Australian and ACT Government employees, and a specified insurer for licensees. For employees of self-insured licensees, the relevant authority is the licensee.
A link to the Work trial agreement for Australian and ACT Government employers is included in section 9 of this handbook.
Further details about work trials are available on the Comcare website: www.comcare.gov.au.
Redeployment
In cases where it is absolutely certain that an employee is permanently medically unable to return to work with the pre-injury employer, the RCM should consider redeployment to a new employer.
However, it is important to be clear about the definition of suitable employment before identifying a job goal outside the pre-injury organisation.
Legislation
Part I section 4 of the SRC Act includes definitions which specify the following in regard to suitable employment:
Where the injured employee is a permanent employee of the Commonwealth the workplace rehabilitation goal must be employment within the Commonwealth.
Similarly, for an employee of the ACT Government, suitable employment must be employment within the ACT Government.
However, if the employee separates from his or her permanent employment, then employment outside the pre-injury employment can be considered.
The same applies if the injured employee is a permanent employee of a licensee. Suitable employment must be found within the licensed corporation unless the employee separates from this employment.
For employees on fixed-term contracts within the Australian or ACT Governments or licensee at the time of injury, if the contract expires before they are back at work, then suitable employment is any employment.
See Suitable employment: A guide for Rehabilitation Case Managers on the Comcare website for more information.
Once redeployment has been identified as the only return to work option, the rehabilitation program should be developed incorporating the same principles as for any rehabilitation program. This includes a thorough rehabilitation assessment, medical support for the program and consideration of the return to work hierarchy.
85
Study and retraining
In unique circumstances study and retraining may form part of a rehabilitation program where opportunities for suitable employment are limited and need to be increased. However, study and retraining are not automatic entitlements after a workplace injury. It is recommended that they be considered against the return to work hierarchy, be linked to future employment outcomes, be based on objective assessments and be assessed in regard to the likelihood that the training will lead to achievement of the rehabilitation goal. Other issues for consideration include the criteria of section 37(3) such as the impact on the cost of the rehabilitation program.
When is retraining appropriate?Retraining may be appropriate when it will significantly improve employment and/or redeployment options. Use the following hierarchy when considering retraining:
1. Transferable skills to a new vocational goal with no training required.
2. Transferable skills to a new vocational goal with on the job training.
3. Transferable skills to a new vocational goal with a combination of on the job training and a short training course.
4. Transferable skills but need to be supplemented by short training course.
5. Transferable skills but need to be supplemented by a long and/or expensive training course.
6. No transferable skills—a complete change in vocation is required, with an intensive and/or expensive training course. This should only be considered as a last resort.
The RCM should also consider the following:
» the employee’s preferences
» the cost of the program
» which training option will most likely lead to gainful employment
» the job market.
The RCM should write the study or training course into the rehabilitation program for the same reasons that a formalised program is developed—to provide a clear and accountable program for the employee to follow. In addition, the rehabilitation program approves training costs. Under the SRC Act, the Claims Manager cannot pay a training institute directly. This is because a training institute is not considered a WRP and is therefore unable to provide rehabilitation services. By including retraining in a rehabilitation program, the Claims Manager is able to reimburse the WRP for the retraining costs. Alternatively, if no WRP is involved, the Claims Manager can reimburse the employer directly for the retraining costs.
The RCM should develop a new rehabilitation program at the beginning of each semester. After the initial approval to begin a course, approval for each subsequent semester becomes dependent on the employee gaining adequate results in the previous semester. If the employee fails to obtain adequate grades and must repeat a particular unit, the employee is required to pay the relevant tuition fees. If this happens the RCM should reconsider the appropriateness of the retraining program.
If the employee becomes able to return to duties before the course is completed, the RCM must decide whether to continue funding ongoing training costs or to negotiate other arrangements for the employee to pay his/her own tuition and other study related expenses.

86
The following table highlights the uses and benefits of these methods.
Table 2 Return to work strategiesReturn to work strategy
Use Benefits
Graduated suitable duties program
If the employee is unable to return to full pre-injury hours and/or duties.
» The employee may be able to manage a selected range of tasks for reduced periods of time
» builds up ability to manage tasks
» maintain generic work habits
» avoids isolation.Pacing To allow attendance at the workplace
for full normal weekly hours.» Avoids extended periods out of the
workplace
» avoids employee becoming stuck on a few hours a day
» uses the full range of employee’s skills and expertise
» maintains normal daily patterns and regular work routine
» prevents the development of longer-term disability.
Work trial To provide short-term suitable duties where, because of medical restrictions, the employer is unable to provide suitable duties.
» Rebuilds work skills, self- confidence and establishes work routines after injury
» improves opportunities for employment.
Redeployment If an employee is permanently medically unable to return to work with the pre-injury employer.
» Improves opportunities for employment.
Retraining If opportunities for suitable employment are limited and need to be increased.
» Improves opportunities for employment.

87
Approving a rehabilitation programBefore the RCM approves the rehabilitation program, all parties must be clear about:
» Responsibilities and expected outcomes, including the medical recovery and expected return to work timeframes for the injury or illness. The RCM should consult the employee, and other important stakeholders—the treating medical practitioner, the supervisor and WRP. These consultations must be carefully and thoroughly documented as evidence of consultation. This evidence will demonstrate that the RCM has satisfied the requirements of section 37(3) and the guidelines issued by Comcare.
» Communication and reporting requirements, particularly between the RCM and the WRP. For example, the RCM can specify regular updates by reporting at meetings, through phone or face-to-face discussions and written reports.
As a rehabilitation program is a determination for the purposes of the SRC Act, employees must be made aware of their rights and responsibilities. If they do not agree with the rehabilitation program they are able to request a review of the determination. The employee should understand this process. They should also understand that if they fail to comply with the rehabilitation program, without reasonable excuse, their rights to incapacity payments may be suspended until they comply.
Refer to Part 3: Section 7—Employee and Rehabilitation Authority (Employer) rights and responsibilities in this handbook for information on employee and employer rights and responsibilities.
Once the RCM has considered and documented all these issues, they can make a formal decision to sign the rehabilitation program.
Who should sign the rehabilitation program?
The RCM should sign the program.
The SRC Act requires that only specified people are able to approve a rehabilitation program for employees. As described in section 3 of this handbook, under section 41A of the SRC Act, it is the delegated RCM who has the authority to approve the proposed rehabilitation program. This means that the signature of the delegated RCM formalises the document as a determination under section 37 of the SRC Act and that the rehabilitation program is now a formal document:
» detailing the course of the rehabilitation program
» specifying duties and hours to be worked by the employee
» outlining the roles and responsibilities of the stakeholders: you, the employee, the supervisor, and the WRP
» outlining communication strategies
» providing timelines, rehabilitation goals, outcomes and milestones for review and evaluation
» requiring compliance by the employee with penalties for non-compliance
» formalising the contract for the services to be provided by the WRP
» approving the costs for the program.
Before you sign the proposed rehabilitation program, check that:
» you are a delegate under section 41A of the SRC Act
» you have completed the determination section of the rehabilitation program
» the program was developed in consultation with the employee and the medical practitioner

88
» you have considered, communicated and documented each of the criteria under section 37(3)
» the proposed rehabilitation interventions, codes, costs, timeframes and services are appropriate to the employee’s needs.
As the rehabilitation program forms the basis for payment of the WRP accounts, a copy must be sent promptly to the Claims Manager. The Rehabilitation Guidelines also state that a copy of the rehabilitation program shall be sent to:
(i) the relevant authority
(ii) the approved WRP
(iii) the treating doctor
(iv) the employee’s manager or supervisor
(v) if the employer is not the liable employer, the liable employer irrespective of whether the rehabilitation program was provided by an approved WRP or by the rehabilitation authority itself.
The workplace rehabilitation providerIf a WRP has developed the rehabilitation program and has responsibilities under the program, their signature represents commitment to following the program, performing the activities outlined in the program, and submitting accounts as outlined in the program.
A referral must be received from a RCM (or employer delegate) before the WRP can commence service delivery.
The Relevant Authority (Comcare or the licensee) is able to pay rehabilitation invoices for initial rehabilitation services prior to claim determination in certain circumstances.
All rehabilitation invoices should clearly identify the code for the service provided and invoiced.
Codes for rehabilitation payments and invoices
This section is relevant for claims managed by Comcare.
Rehabilitation services are invoiced to Comcare under specific cost codes depending on the service provided. This assists the relevant authority to keep track of the services that are being provided under rehabilitation. This is not a list of services to which a claimant is entitled; these are services that may be provided under rehabilitation (after a determination by the RCM) and a process for invoicing those services.
Rehabilitation capability assessment—initial needs assessment (INA)
Code 90
Activities that are identified as Code 90 are those costs that are part of a rehabilitation assessment. This is an assessment of an employee’s capacity to return to work and undertake, or continue to undertake a rehabilitation program.
Activities include:
» meeting with the employee and conducting an assessment
» workplace visit and meeting
» workplace (ergonomic) assessment
» job analysis and identification of suitable duties
» consultation/meeting with the medical practitioner

89
» liaison with other treating practitioners
» report including:
> recommendations for a proposed rehabilitation program and return to work (as applicable)
> rehabilitation goals and timeframes> barriers to return to work and
strategies for addressing these> return to work (or maintenance at
work) arrangements> a proposed return to work schedule> rehabilitation services and costs.
Approved workplace rehabilitation providers must undertake assessment services in accordance with Comcare’s Operational standards (service standards 1.1–1.6).
The following services may form part of an initial needs assessment (section 36) or rehabilitation program (section 37):
» workplace (ergonomic) assessment
» functional capacity assessment
» activities of daily living assessment*
» aids and appliances assessment*
» home modification assessment*
» household help and attendant care assessment*
» vocational assessment
» cognitive assessment
» driving assessment.
Note*: The Claims Manager is the decision maker for such a referral.
For billing purposes, code 90 is used if the service formed part of an initial needs assessment. Code 92 is used if the service is delivered as part of a rehabilitation program. Single services may be undertaken as part of a rehabilitation assessment under section 36 but must be part of a broader assessment of the employee’s capacity to undertake a rehabilitation program. For example if the person only requires a workplace (ergonomic) assessment then it will be either a code 92 cost if there is a rehabilitation program or it may be paid by the employer as a WHS cost. If it is part of the overall assessment it is a code 90 cost.
Where the Claims Manager has engaged a WRP to undertake one of the assessment services marked with an asterisk, code 90 is used for billing purposes.
Rehabilitation program services
Code 92
Rehabilitation services can only be delivered by approved consultants employed or engaged to work with an approved workplace rehabilitation provider. Each approved consultant is issued with a consultant identification number.
Services involved in the management and monitoring of an employee’s rehabilitation program (including return to work activities) are to be itemised on the rehabilitation program. This should include:
» development, coordination and monitoring of the rehabilitation program
» employee liaison and support
» advice on workplace or work process modifications
» organising assistive equipment and ensuring the employee can safely use the equipment

90
» workplace meetings and liaison with RCM, supervisor and/or manager
» workplace assessment, task analysis, job redesign or upgrading
» development of suitable duties schedule
» case conferences
» GP visits, liaison with treatment providers
» progress or closure report
» provider travel
» job search and redeployment activities such as:
> vocational assessment
> negotiating/monitoring work trials
> interview preparation
> job search and adjustment to disability counselling.
Note: All services should be delivered in accordance with Comcare’s Operational Standards (service standards 1–3 and outcome standards 1–3).
A Comcare approved workplace rehabilitation provider is able to deliver both ‘return to work—same employer’ and ‘return to work—new employer’ services. However, the services an individual consultant can deliver will be dependent on their professional qualifications and experience.
Return to work support services
Code 93
There may be some services (and associated costs) required to support the employee’s return to work that are provided by a third party. These are identified on the rehabilitation program as code 93 return to work support services, and can include:
» taxi vouchers—to allow the employee to attend the workplace or other return to work activities—this does not include transport to attend treatment
» vocational counselling or adjustment to disability counselling where it is not provided by the WRP
» external training—for example, course fees, tutoring costs and materials
» equipment specifically required to facilitate return to work that is outside the workplace’s WHS obligations and is not treatment related—such as voice recognition software
» costs of GP case conference/visit or GP report.
Comcare is unable to pay a third party directly (as they are not approved by Comcare to deliver rehabilitation program services) so all code 93 costs must be paid by the rehabilitation provider and reimbursement sought from Comcare.
This is in accordance with Comcare’s Operational standards (service standard 6.4).

91
Workplace rehabilitation does not include:
» work conditioning
» pain management programs
» treatment (including therapeutic counselling)
» overseeing/monitoring of employee’s treatment
» determining employee’s ongoing entitlements
» claims management
» employer case management activities.
The employee
It is recommended that the employee to sign the rehabilitation program. Their signature is evidence that they have been involved in the development of the rehabilitation program and the return to work schedule and that they understand their rights and obligations under the SRC Act. The employee must be given a copy of the rehabilitation program including the information pages which explain their rights and responsibilities.
If, after adequate consultation, discussion and negotiation, the employee does not agree with the contents of the rehabilitation program, they may refuse to sign it. The employee can submit a request for a reconsideration of the decision that they should undertake the program. See section 7 for further information about reconsiderations.
Options for the RCM to consider include further consultation, discussion and negotiation with the employee, the treating medical practitioner and the WRP. However, if the RCM is satisfied that the rehabilitation program is appropriate, after revisiting the section 37(3) criteria, they can decide to proceed with the program. In this case, the RCM will document all relevant information,
inform the employee and the treating medical practitioner and continue with implementation.
Failure of the employee to sign a rehabilitation program and the decision of the employee to request a reconsideration of the program is not in itself considered a reasonable reason for the employee not to participate in the program.
The treating medical practitioner
The treating medical practitioner is an important stakeholder in the return to work process. During all stages of the rehabilitation assessment and the development of the rehabilitation program, ensure there is adequate consultation and cooperation with the medical practitioner and that the medical practitioner is kept informed about all aspects of the program.
Ideally, the treating medical practitioner should sign the rehabilitation program to demonstrate commitment and approval. However, rehabilitation program forms in the Comcare scheme do not have a formalised section for this signature. Therefore to demonstrate consultation and approval by the medical practitioner, the RCM should carefully document all consultation and negotiations.
Even if the treating medical practitioner does not approve the program and the return to work outcomes, and the RCM relies on other medical evidence to support the program, there must be evidence to demonstrate that the medical practitioner has been consulted.
See Part 2, Section 2 of this guide for more information about medical practitioner responsibilities and working effectively with medical practitioners.

92
The supervisor
The supervisor should sign the rehabilitation program to demonstrate support for the program, and commitment to following and monitoring the program.
Employee leave during a rehabilitation program
There are special provisions for leave while an employee is on a rehabilitation program under section 37 of the SRC Act. This ensures that the employee maintains the program without jeopardising progress towards a sustainable return to work. This provision also provides the RCM with an awareness of the type of leave and reasons for leave requested during the course of a rehabilitation program.
LegislationThe SRC Act in section 116 states that:
In spite of the provisions of any other Act or an award, an employee is not entitled to be granted any kind of leave with pay (other than maternity leave) during, or in respect of, any period when the employee is or was on post-determination compensation leave.
This section of the SRC Act means that an employee on a rehabilitation program must request leave through the RCM rather than through the usual organisational processes. This section serves to protect the rights of both the employee and employer.
For the employee it protects the exploitation of leave entitlements, ensuring that leave is not used for a compensable condition. For example, the rehabilitation authority (employer) cannot schedule an employee’s
annual leave into the rehabilitation program to satisfy operational requirements. The employer cannot request an employee to use personal leave rather than compensation leave when they are absent because of the compensable condition.
For the employer it provides some authority over the rehabilitation process, as the employer decides when and how an employee can access leave while on a rehabilitation program. The RCM does have discretion about approval of leave during rehabilitation programs. This means that the RCM is able to approve leave if they think it is appropriate and approval would not jeopardise the rehabilitation program. As a general rule, an employee should not be granted approval to take leave immediately before or during a rehabilitation program, unless there are special circumstances where not approving it would jeopardise the program. Therefore, it is important that employees are informed of this section of the SRC Act, their obligations regarding leave, and the reasons for restrictions on taking leave while on a rehabilitation program. In cases where the graduated return to work has plateaued at a particular level for some time, there may not be a risk in approving annual leave and as such, the leave could probably be assessed for approval in the normal manner. The RCM should also ensure that the employee’s supervisor is aware that all leave requests must be submitted to the RCM for discussion and approval.
93
Non-compliance with the rehabilitation process
Legislation
Under section 36(4) of the SRC Act, an employee can be found to be non-compliant if they fail, refuse or obstruct, without reasonable excuse, to attend or participate in a rehabilitation examination or assessment with the purpose of determining their capability of undertaking a rehabilitation program.
Under section 37(7) of the SRC Act, an employee can be found to be non-compliant if they fail, refuse or obstruct, without reasonable excuse, to undertake and participate in their rehabilitation program.
Non-compliance under the SRC Act can lead to suspension of compensation entitlements excluding compensation for medical treatment. The authority to make a determination to suspend compensation under the SRC Act is with an individual with the appropriate delegated powers from the rehabilitation authority.
Paragraph 33 of the Rehabilitation Guidelines provides the criteria that forms the framework of the decision process for determining that an employee is to attend an examination or undertake a rehabilitation program.
Non-compliance may include, but is not limited to:
» failure to attend an appointment for the purpose of undertaking a rehabilitation assessment or examination
» failure to attend an appointment with their rehabilitation provider, for the purpose of reviewing their rehabilitation program progress
» failure to attend a training course or any other activity included in their rehabilitation program
» failure to undertake an examination or other activity connected with a training course or other rehabilitation program activity
» failure to seek suitable work.
Who can make a determination to suspend benefits?The Rehabilitation Guidelines state at paragraph 33.5:
… a person delegated by the rehabilitation authority with the power to effect suspension of compensation under the Act [referred to the delegated person].
This may be the RCM or this specific role may be delegated to another officer within the rehabilitation authority; also:
The delegated person is the officer most appropriate because they:
(i) are best experienced or qualified to deal with the nature of the refusal, failure or obstruction [such as medical disability, personnel or industrial issues etc];
(ii) are of suitable seniority within the employer
(iii) have no conflict of interest [such as the employee’s supervisor]; or
(iv) are unlikely to jeopardise any future rehabilitation of the employee by being the delegated person; and

94
(d) the RCM shall ensure the opportunity to undertake an examination or resume the rehabilitation program remains available to the employee even where a suspension of compensation or rights under the Act has occurred.
Points (d) and (iv) simply mean that by having a separate delegate for suspension, it may be possible to maintain a positive working relationship between the RCM and the employee, and therefore, not jeopardising the pathway back to ‘compliance’ for the employee. The formal decision to suspend benefits is at ‘arm’s length’ from the RCM who is assisting the employee to achieve agreed rehabilitation goals.
Making a decision to suspend benefitsSuspension of entitlements should only take place where all reasonable steps have been taken to resolve the issues causing the non-compliance. The RCM should have:
» held discussions with the employee, their WRP, the Claims Manager and any other key stake holders involved with the employee’s rehabilitation, such as a member of Comcare’s injury management advisory service
» documented all discussions and actions to support any determination of non-compliance on the part of the employee—the importance of thorough and complete documentation is imperative, that is, if an activity is not documented it will be seen as not having occurred, the chain of evidence is broken and the activity cannot be substantiated. True copies of all letters that are sent to the employee must be saved to their file.
Where an employee presents a reason for their non-compliance, you or the person with the delegated power, must consider whether the employee had a reasonable excuse for their failure, refusal or obstruction. Any reasons provided should be acknowledged, in writing, and if not considered valid, a clear statement should be communicated to the employee as to why the reason is not considered a reasonable excuse.
The employee should also, where reasonable, be given an opportunity to demonstrate compliance.
At all times it is the RCM’s responsibility to keep the employee informed of their rights and obligations regarding non-compliance under the SRC Act.
An employee who refuses to sign a rehabilitation program is not considered to be non-compliant. The rehabilitation program does not formally exist until it has been signed by the delegated officer under the SRC Act, usually the RCM.
In such cases the RCMs should do the following:
» sign the rehabilitation program
» prepare a covering letter, that is to be sent to the employee, with a copy of the signed rehabilitation program explaining that should they fail, refuse or obstruct any activity included in their rehabilitation program then action may be taken to suspend their compensation entitlements
» attach to the employee’s copy of the program, a full copy of the rehabilitation rights and responsibilities, and forward to the employee.

95
This action provides the employee with the opportunity to participate in their rehabilitation program, with full knowledge of the consequences to their rights to compensation.
Once a decision is made to suspend compensation entitlements, an employee removes their right to claim retrospective entitlements for the period of suspension. Entitlements can only be reinstated on and from the date upon which the person actually becomes compliant.
Decisions to suspend compensation entitlements must be communicated to the employee in writing. Decisions to reinstate benefits must also be communicated to the employee in writing.
What constitutes a reasonable excuse?An employee’s notification of their reason/s for failing, refusing or obstructing their examination/assessment or any activity included in their rehabilitation program must be assessed. Each case must be assessed on its own merits.
The following, but not limited to, can be used as a guide to what constitutes a reasonable excuse:
» unexpected medical condition requiring medical attention or hospitalisation
» transport issues—last minute flight cancelations, traffic delays, road closures, suitable transport not available, for example, ambulance if that is medically required
» written notification of the required activity not received or not received in time to allow the employee to attend or to request a reschedule—it is advisable that any requests to attend rehabilitation
appointments such as section 36 assessments are notified in writing and sent by registered mail with at least 14 days’ notice of the appointment.
How does an employee become compliant following suspension of benefits?Following suspension of benefits it is not sufficient for an employee to merely agree to comply for benefits to be reinstated. The employee is required to demonstrate their compliance by their actions.
If an employee’s benefits have been suspended because they failed to attend or obstructed a rehabilitation assessment examination or other appointments arranged as part of their rehabilitation program, then they must attend that appointment before benefits can be reinstated. On the day the employee attends the appointment benefits should be reinstated. If the employee and/or the service provider are unable to reschedule the appointment for several days, then the suspension remains in place until the appointment takes place.
In some instances an employee’s non-compliance may have longer term implications. For example, where an employee fails to undertake a training course and the rehabilitation program is delayed for up to a semester of study. Each case must be considered on its own merits. However, the general principle is that once an employee recommences their rehabilitation program then their benefits should be reinstated. Where an employee repeatedly frustrates the rehabilitation process consideration may be given to whether the deeming provision under the SRC Act is appropriate.

96
Reconsideration and review mechanismsWhere an employee disagrees with a decision regarding their rehabilitation, they may request a reconsideration or review of that decision.
The Federal Court has held that under the SRC Act, a client does have the right to seek a reconsideration or review of a decision to suspend their compensation entitlements in accordance with subsections 36(4) or 37(7).
For all determinations made regarding rehabilitation activities under the SRC Act the employee should be informed in writing of the terms and reasons for the determination and their right to have the decision reviewed or reconsidered.
The following table shows the possible steps after non-compliance with workplace rehabilitation.
Note: Suspension after non-compliance is not an automatic decision. It is preferable to resolve the issues and to prevent progression to suspension.

97
Emp
loye
e n
on
-co
mp
lian
ce
with
wo
rkp
lac
e re
ha
bili
tatio
n
The
reh
ab
ilita
tion
au
tho
rity
The
em
plo
yee
Ou
tco
me
Rea
son
s fo
r n
on
-co
mp
lian
ce
Dis
cu
ssio
n w
ith a
ll p
art
ies
is e
sse
ntia
l
Dis
cu
ssio
n w
ith th
e e
mp
loye
e, t
o d
isc
ove
r th
e
rea
son
s fo
r no
n-c
om
plia
nc
e.
Dis
cu
ssio
n w
ith th
e w
ork
pla
ce
reh
ab
ilita
tion
p
rovi
de
r, th
e tr
ea
ting
do
cto
r, to
ob
tain
the
ir in
pu
t to
ad
d to
yo
ur o
wn
un
de
rsta
nd
ing
.
Dis
cu
ssio
n w
ith th
e C
laim
s M
an
ag
er i
f a
pp
rop
riate
.
Pro
vid
e re
aso
ns
for n
on
-co
mp
lian
ce
.
Co
op
era
te w
ith th
e e
mp
loye
r to
fac
ilita
te
wo
rkp
lac
e re
ha
bili
tatio
n.
Ac
tive
ly p
art
icip
ate
in th
e p
rob
lem
so
lvin
g
pro
ce
ss.
Reso
lve
issu
es
an
d p
rog
ress
re
ha
bili
tatio
n a
nd
retu
rn to
wo
rk.
Gre
ate
r effo
rt h
ere
to a
void
su
spe
nsi
on
.
Sup
po
rt fo
r p
art
icip
atio
n in
reh
ab
ilita
tion
Co
op
era
tion
in t
he
reh
ab
ilita
tion
pro
ce
ss
Ma
ke n
ec
ess
ary
mo
difi
ca
tion
s to
the
re
ha
bili
tatio
n p
rog
ram
in c
on
sulta
tion
with
tre
atin
g d
oc
tor a
nd
reh
ab
ilita
tion
pro
vid
er.
Co
op
era
te w
ith th
e e
mp
loye
r to
fac
ilita
te
wo
rkp
lac
e re
ha
bili
tatio
n.
Ac
tive
ly p
art
icip
ate
in th
e p
rob
lem
so
lvin
g
pro
ce
ss.
Reso
lve
issu
es
an
d p
rog
ress
re
ha
bili
tatio
n a
nd
retu
rn to
wo
rk.
Emp
loy
gre
ate
r effo
rt h
ere
to a
void
su
spe
nsi
on
.
Co
nse
qu
en
ce
s o
f no
n-c
om
plia
nc
e
Info
rma
tion
Reite
rate
em
plo
yee
resp
on
sib
ility
to p
art
icip
ate
in
reh
ab
ilita
tion
.
Exp
lain
the
co
nse
qu
en
ce
s o
f fa
ilure
to p
art
icip
ate
in
reh
ab
ilita
tion
with
ou
t re
aso
na
ble
exc
use
.
Ac
tive
ly p
art
icip
ate
in w
ork
pla
ce
reh
ab
ilita
tion
.Re
solv
e is
sue
s a
nd
pro
gre
ss
reh
ab
ilita
tion
an
d re
turn
to w
ork
.
Emp
loy
gre
ate
r effo
rt h
ere
to a
void
su
spe
nsi
on
.

98Em
plo
yee
no
n-c
om
plia
nc
e w
ith w
ork
pla
ce
reh
ab
ilita
tion
The
reh
ab
ilita
tion
au
tho
rity
The
em
plo
yee
Ou
tco
me
Co
ntin
ue
d n
on
-co
mp
lian
ce
Tow
ard
s su
spe
nsi
on
Writ
e to
em
plo
yee
req
ue
stin
g re
aso
ns
for n
on
-c
om
plia
nc
e—
sen
ior m
an
ag
em
en
t to
sig
n le
tter.
Inc
lud
e in
form
atio
n a
bo
ut t
he
em
plo
yee
’s ri
gh
ts
for r
ec
on
sid
era
tion
.
Allo
w s
uffi
cie
nt t
ime
for r
ep
ly.
Resp
on
d w
ith re
aso
ns
an
d e
vid
en
ce
.Le
ss p
refe
rred
ou
tco
me
.
Co
ntin
ue
to a
ttem
pt r
eso
lutio
n o
f is
sue
s.
Co
nsi
de
r re
aso
ns
for n
on
-co
mp
lian
ce
Tow
ard
s su
spe
nsi
on
The
exc
use
for n
on
-co
mp
lian
ce
mu
st b
e
‘rea
son
ab
le’.
Do
cu
me
nt c
on
sid
era
tion
of t
he
ex
cu
ses.
Less
pre
ferre
d o
utc
om
e.
Co
ntin
ue
to a
ttem
pt r
eso
lutio
n o
f iss
ue
.
Susp
en
sio
n
Writ
e to
em
plo
yee
ad
visi
ng
of s
usp
en
sio
n—
sen
ior
ma
na
ge
me
nt t
o s
ign
lette
r.
Inc
lud
e in
form
atio
n a
bo
ut t
he
em
plo
yee
’s ri
gh
ts
for r
ec
on
sid
era
tion
.
No
tify
sta
keh
old
ers
.
Lea
st p
refe
rred
ou
tco
me
.

99
Non-compliance checklist: factors to consider
Section 36—Assessment of capacity for a rehabilitation program
Was the employee issued with a valid determination as defined by section 61(1) of the SRC Act? This includes a copy of the signed Rehabilitation assessment examination form and notice of rights.
Yes No
Was the employee provided with reasonable notice toattend the assessment?
Yes No
Was the employee assisted with travel to the assessment, if appropriate? Yes No
Was the employee referred to a medically qualified practitioner with an appropriate speciality for the condition?
Yes No
Section 37—Rehabilitation program
Is there a rehabilitation program in place that is current? That is, it covers the current time frames?
Yes No
Have there been any changes in circumstance or incidence that render the current rehabilitation program void or inappropriate and therefore anew program or altered program needs to be issued prior to pursuing non-compliance?
Yes No
Is the current rehabilitation program signed by an appropriate rehabilitation delegate?
Yes No
Does the rehabilitation program have an attached return to work schedule and if so did this form part of the determination?
Yes No
Was the employee consulted in the development of the rehabilitation program?
Yes No
Was the employee issued with a valid determination as defined by section 61(1) of the SRC Act? This includes a copy of the signed Rehabilitation program, notice of rights and details of the start date and suitable duties?
Yes No
Is there medical evidence or other supporting evidence that supports the rehabilitation program and return to work schedule?
Yes No
For support when considering suspension for non-compliance contact the Injury Management Advisory Service (IMAS) at Comcare. Each case is different and it is important to ensure that all documentation is correct and all correct processes have been followed before proceeding to suspension.
100
Monitoring should provide information about:
» attendance and task completion
» progress against agreed milestones
» medical or other problems
» supervisor and colleague support
» performance of the workplace rehabilitation provider against agreed activities
» any other criteria in the rehabilitation program
» any other relevant information.
When monitoring the rehabilitation program the RCM needs to coordinate the parties involved by keeping in regular contact with them and ensuring that the WRP, supervisor and employee have undertaken what they have agreed to do.
To ensure effective communication consider:
» regular contact with the employee and supervisor
» regular workplace meetings involving some or all parties
» regular progress reports—for Australian and ACT Government employers, copies of these progress reports must be forwarded to Comcare.
Step 4: Monitor and reviewOnce the rehabilitation program has been finalised, it forms the employee’s individualised plan for daily activities. The program also formalises the coordination, cooperation and communication between stakeholders; and the monitoring and management of the rehabilitation program.
Ensure that there is a regular review to assess effectiveness of injury management interventions and the progress of return to work. This process is important to ensure that rehabilitation programs are responsive to the barriers to return to work that have been identified, match the employee’s needs, and are effective for this stage of recovery.
Monitoring and review should include:
» relevant outcome measures relating to functional goals of injury management
» close management and monitoring of rehabilitation programs in consultation with all parties
» a standardised screening tool is used to identify and review risks of longer term incapacity when recovery has not progressed as expected, or when risk factors have been identified.
Where recovery is delayed, all parties should work together to consider and act on new information and ensure that the program for treatment and return to work addresses psychosocial factors and aims to reactivate functional activity to minimise the likelihood of persistent pain and functional loss.
Pain of longer than three months’ duration can be referred to as persistent pain, and is usually the result of a complex relationship between physical and psychosocial factors—multi-disciplinary activity focused programs are indicated to address persistent pain related disability.
Note: It is the Rehabilitation Case Manager’s responsibility to monitor the rehabilitation program and ensure that all parties are completing agreed activities.

101
What to do if the rehabilitation program does not progress as expected
Resolve any issues associated with communication, negotiation and conflict resolution as soon as a problem is identified. A WRP can assist the RCM with this in individual cases if objectivity and rehabilitation expertise are required.
Here are some examples of problems with rehabilitation programs and some suggestions for addressing them:
Stalled progress or the employee seems resistant
If progress has stalled or the employee is resistant to the rehabilitation program, a case conference involving some or all of the stakeholders is a useful tool to help sort through the issues. Case conferences improve communication and provide a means for clarifying the issues blocking progress and identifying strategies to overcome the barriers. Case conferences are described in Appendix 3.
Other suggestions for overcoming stalled progress or employee resistance include:
» talk to the employee and revisit employee rights and responsibilities
» irregular workload distribution or conflict issues can be addressed through appropriate communication, negotiation and mediation if necessary
» discuss the issues with the treating medical practitioner
» use the skills and expertise of the WRP
» arrange another rehabilitation assessment—an assessment by a legally qualified medical practitioner might provide further useful information
» make modifications to the rehabilitation program to accommodate problems
» consider a pacing program
» consider that non-work issues may be impacting on the program
» ask the WRP to use the flags model or other screening tool to identify and address barriers.
Medical diagnosis or prognosis changes
If the medical diagnosis or prognosis changes, the RCM should consider the following strategies:
» Find out how the changes affect the employee’s ability to return to work and participate in the rehabilitation program. Seek specific information which allows decisions to be made. Contact the treating medical practitioner and request that the Medical diagnosis and prognosis form be completed again.
» Reassess the rehabilitation program goals and services, by considering the following:
> Are the timeframes, costs and services still appropriate? If not, the program may need to be altered or a new rehabilitation program developed.
> Is the final goal still achievable? If not, the current program will need to be closed and a new program developed.

102
Work performance issues
This is a particularly difficult situation with the potential to impact significantly on successful return to work outcomes. Often performance issues have been an underlying problem before the workplace injury, and become highlighted during the return to work process.
It is important to keep separate the rehabilitation program and the process for dealing with work performance. The RCM should:
» Clearly identify the restrictions imposed by the injury and separate these from work performance issues. Often there is difficulty in separating the cause of certain behaviours within the workplace, therefore it is important that the WRP and/or treating medical practitioner identify medical restrictions and the effect of these on work performance. For example, an employee with an adjustment disorder may be frequently absent from work and when at work can be aggressive and non-productive at times. It is possible that this behaviour is symptomatic of the condition or it could be indicative of job dissatisfaction. At this stage it is reasonable to request a new or supplementary rehabilitation assessment under section 36 of the SRC Act to seek further clarification and separation of these issues.
» Encourage communication and cooperation between all parties, particularly between the RCM, the supervisor and the human resources area.
» Request that the supervisor and human resource area agree to keep the rehabilitation program and work performance issues separate.
There are two options for managing this situation:
1. The usual expectation would be that work performance processes would begin or continue while the employee is on a rehabilitation program. Therefore,
> the supervisor and human resource area need ongoing information about restrictions on work performance due to injury and progress
> the supervisor and human resource area must notify the RCM about procedures to deal with work performance which may affect the rehabilitation program.
2. In exceptional cases it may be appropriate to suspend the performance management processes while the employee recovers from the injury or illness. This may be the preferred option when the medical condition directly impacts on the work performance and as a result the medical restrictions do not allow for a meaningful assessment of the employee’s performance. If a performance process is to be suspended, all parties need to have a clear understanding about when performance management will recommence.
Performance management, code of conduct issues and grievances should not be managed by the person who is managing the employee’s rehabilitation.

103
Altering or closing an existing rehabilitation programA rehabilitation program is altered when the RCM decides that the rehabilitation program services, associated costs, program timeframes, end date or goals need to be changed.
A determination altering an existing rehabilitation program can only apply to rehabilitation provided on or after the date of that determination.
Before determining under section 37(1) of the SRC Act whether or not an employee should undertake an altered rehabilitation program or cease to undertake a rehabilitation program altogether, the RCM is required to:
(a) consult with the approved WRP [if engaged]
(b) consider any advice from that provider or medical practitioner regarding more appropriate rehabilitation program goals, services, timeframes and the employee’s capacity to undertake a rehabilitation program
(c) consider the need for a repeat rehabilitation assessment in accordance with paragraph 18, of the Rehabilitation Guidelines
(d) discuss the proposed program alterations or closure with the employee and supervisor.
Where the RCM determines that the rehabilitation program should be altered or closed, the RCM shall provide the employee with written notice advising the terms of, reasons for and the right to request a review of, that determination.
Where a RCM decides to close a rehabilitation program the RCM may at a later date arrange an assessment of the employee’s capability to undertake a new rehabilitation program in accordance with paragraphs 18 to 25 of the Rehabilitation Guidelines.
Circumstances frequently change during the course of a rehabilitation program. For example, the employee may not meet expected improvement timeframes, or their medical condition may change for the worse. Alternatively there may be changes in the workplace. For example, suitable duties may no longer be available because of structural changes or outsourcing of functions. In these circumstances the RCM must decide whether to continue the rehabilitation program, make modifications to it, or close the program and begin a new one.
In all of these situations, the RCM must discuss the proposed changes and the need for change with the WRP, the employee, the supervisor and the treating medical practitioner before a final decision.
What if the goals stay the same but the employee needs a little more time on the rehabilitation program?
The program should be amended using a Rehabilitation program alteration form.
Usually this involves an increase in WRP services or the timeframe in which they will be delivered. As services which have not been included in the rehabilitation program will not be paid for by the Claims Manager, the WRP must amend the program to ensure payment will proceed. These alterations must be approved by the RCM before these extra services are provided.

104
Once the RCM has signed the alteration form, it becomes a formal variation to the contract. In this way it is also a determination under the SRC Act and certain requirements apply. These are that:
» the person signing is a delegate under section 41A of the SRC Act
» the determination section of the rehabilitation program has been completed
» the RCM considers, communicates and documents each of the criteria under section 37(3)
» the proposed rehabilitation interventions, codes, costs, timeframes and services are appropriate to the employee’s needs.
Hence the employee should sign the form indicating acknowledgement of alteration to the services and/or timeframe, and must comply with the alterations.
It is the employer’s responsibility to submit a Rehabilitation program alteration form to the Claims Manager promptly. Failure to do this may result in accounts presented by the rehabilitation provider being rejected or incorrectly processed.
What if the goals of the rehabilitation program change?
When the current rehabilitation program goals are no longer achievable and a new rehabilitation program with a different goal is required, the program is closed using a Rehabilitation program cessation form. A new rehabilitation program is developed if still required.
The employee may need a new rehabilitation assessment before a new rehabilitation program is developed. The RCM makes the decision about the need for another rehabilitation assessment in consultation with the WRP, the employee and the treating medical practitioner.
What happens to the rehabilitation program if the workplace rehabilitation provider organisation changes during the program?
If a new rehabilitation provider organisation is going to take over involvement with the rehabilitation program, the current program must be closed using the Rehabilitation program cessation form. A new rehabilitation program must be developed for the new rehabilitation provider.
Progress reports
The employer/rehabilitation authority (in practice—the RCM) may request progress reports from the Workplace Rehabilitation Provider. The nature of these reports is negotiated between the rehabilitation authority and the WRP. For example: a detailed report may be required once per month or a brief email update may suitable. This will depend on the nature of the injury and length of the return to work program.

105
Closing the rehabilitation program
Where the rehabilitation program’s goals have been achieved the RCM shall:
(a) advise the employee that the rehabilitation program is now closed
(b) document the rehabilitation program outcome.
When all the objectives of the rehabilitation program have been achieved, or as much as possible has been achieved, the RCM should close the program using the Rehabilitation program cessation form. Closure of a rehabilitation program does not prevent further rehabilitation services being provided to the employee in the future if circumstances change. Similarly, closure of the rehabilitation program does not imply that compensation benefits will be affected.
The rehabilitation program is usually closed:
» when the goals and objectives of the rehabilitation program have been achieved
» when a return to pre-injury duties or optimum level of functioning in the workplace has been achieved
» when the current rehabilitation program goals are no longer achievable and a new rehabilitation program with a different goal is required
» when specialist rehabilitation provider services are no longer required
» when further workplace rehabilitation is no longer appropriate.
The RCM makes the final decision to close the rehabilitation program and must ensure that the Rehabilitation program cessation form is completed and signed detailing the rehabilitation outcomes achieved.
Note: All rehabilitation programs should be closed as it demonstrates that an end has been reached, and also specifies that the rehabilitation goals have or have not been achieved.
The closure of the rehabilitation program signals the end of the contract between the employer and the WRP. The Claims Manager will not pay for services associated with rehabilitation programs after the closure date.
At the time of closure the RCM should:
» submit the completed closure form to the Claims Manager
» review the case with the employee and his/her supervisor, to ascertain whether the return to work has been durable—for example, the employee is back at work, is able to perform the duties safely and to the required standards
» reassess the employee’s circumstances and potential for employment if a successful and durable return to work has not been achieved—in this case another rehabilitation assessment or a new rehabilitation program may be required for the employee.

106
Step 5: Evaluation after closureThorough evaluation provides the RCM with information about what helped or hindered the return to work process and whether similar approaches should be used in future rehabilitation programs.
What information should be collected and evaluated?
Information about the rehabilitation provider
The agency or employer engages the workplace rehabilitation provider (WRP) and should therefore evaluate the performance of WRP.
The best way to ensure that WRPs are meeting the performance standard is to set very clear expectations on engaging their service. On initial contact with the WRP organisation ensure that the WRP allocated to the case has the relevant experience to manage the needs of the employee. Clearly stipulate the expectations and services required of the WRP, for example, does the WRP need to attend doctor’s appointments; how often should they submit a progress report; what specific assessments and services will the WRP provide in what time frames? This may be some of the specific information outlined in the agency’s service level agreement with the workplace rehabilitation provider.
To evaluate the rehabilitation provider’s performance, use the following standards:
» the Comcare Operational standards and criteria for workplace rehabilitation providers—the standards are in appendices 6 and 7, and are available on the Comcare website
» the employer’s service level agreements with rehabilitation providers.
Comcare monitors the success of rehabilitation programs for premium paying agencies in relation to:
» an agency’s rehabilitation performance
» the WRP’s performance based on the workplace rehabilitation provider outcome standards—these are median plan cost, return to work durability, such as 12 weeks or greater, and return to work rate calculated for all closed rehabilitation programs managed by the rehabilitation provider.
This information is collected and monitored by Comcare through Rehabilitation program forms, Rehabilitation cessation forms, reports and payment details.
All RCMS may be surveyed by Comcare about WRP performance as part of the rehabilitation provider renewal process.
Information about operational and strategic responsibilities
Evaluation provides an opportunity to review what worked for the current case, and may alert the RCM to the need for future interventions, assessments and rehabilitation programs for the same employee. It also enables the RCM to evaluate and refine the rehabilitation and injury management practices of the organisation. For example, could a case conference have been arranged, should an assessment been organised earlier, or could the RCM have been more assertive in pursuing suitable duties with the supervisor?

107
Thorough evaluation also provides an opportunity to identify possible changes in policies or practices and workplace factors which would increase the likelihood of more cost effective, successful rehabilitation programs in the future. For example, if the employer is routinely informed of workplace injuries 3 to 7 days post-injury, valuable time is lost to implement early intervention strategies that could improve rehabilitation outcomes and significantly reduce time off work. Typically, slow notification of injuries and absences demonstrates that the RCMs might need to forge closer links with the personnel area.
It is also possible that during the workplace rehabilitation process the RCM will identify injury prevention issues and WHS performance. For example, over a 12-month period the RCM may notice a significant increase in psychological injury notifications. Issues such as these should be referred to management and the health and safety representative (HSR) or WHS committee for action.
In summary, after closure of rehabilitation programs, each case should be evaluated and recommendations made about:
» the effectiveness of the performance of the Rehabilitation Case Manager
» the effectiveness of the workplace rehabilitation provider
» the effectiveness of the organisation’s procedures and policies
» changes which will improve the management of future cases
» prevention activities to reduce the incidence of injury.

108
PART 3
SECTION 7
EMPLOYEE AND REHABILITATION AUTHORITY (EMPLOYER) RIGHTS AND RESPONSIBILITIES
Employees and rehabilitation authorities (Employers) have rights as well as responsibilities under the SRC Act. The rights and responsibilities described in this section are based on those outlined in the SRC Act sections 36(4), 37(7) and 38.

109
Key points» Employees and their employers have
rights and responsibilities under the SRC Act.
» The Rehabilitation Case Manager (RCM) must clearly communicate to employees their rights and responsibilities under the SRC Act.
» Rights of the employee include the right to fair and transparent decision making, to be provided with information, to access information about themselves, to have a clear line of responsibility for reconsideration and review of significant decisions, and to privacy and confidentiality.
» Responsibilities of employees include the expectation that they will actively participate in their rehabilitation.
» Where an employee fails to actively participate in rehabilitation the RCM should have a conversation to explore and address barriers to participation. If there are no reasonable grounds for non-participation, suspension of incapacity benefits is an option.
» Employer rights include the expectation that the employee will actively participate in rehabilitation, and the ability to impose suspension if this does not occur.
» Employer responsibilities include providing employees with managed rehabilitation programs.
Employee rightsThe employee has the right to information, advice and support to minimise the impact of the workplace injury. The specific rights of the employee include the following:
The right to receive appropriate entitlements under the SRC Act (section 14)These entitlements will be determined by the Claims Manager and include incapacity payments, medical expenses and household services.
The right to be provided with information about entitlements, rights and responsibilities (sections 38, 61, 63, SRC Act)
Employees have the right to be informed about all aspects of their workers’ compensation and workplace rehabilitation under the SRC Act. This information is usually supplied in at least two distinct ways: by the RCM and through the organisation’s return to work policy documents. All forms used during the claim and rehabilitation processes include information about the rights and responsibilities of the employee. For example, when the employee receives the decision about whether or not the Claims Manager accepts liability on behalf of the employer, included is a statement about the right to have the decision reconsidered and how to go about this. The forms for a rehabilitation assessment and rehabilitation program also contain information about how the employee can request reconsideration about these. The forms contain information about the requirement for the employee to comply, and what will happen in the event of non-compliance.
110
The right to access documents relating to the workers’ compensation claim (section 59, SRC Act)
The Claims Manager must respond to written requests for information about the claim within one month of receipt. If this timeline is not possible, the Claims Manager will provide a revised timeline.
The right to request a rehabilitation assessment for capability to undertake a rehabilitation program (section 36(1), SRC Act)
If an employee requests an assessment for a rehabilitation program, in writing, the rehabilitation authority must arrange one. This provision of the SRC Act provides the employee with an opportunity to be proactive about assessment of their capacity to return to work.
The right to request a reconsideration of decisions made by the employer (section 38, SRC Act)
In accordance with the principle of fair decision-making, the employee must be supplied with the reasons for decisions, which must be written in plain English. This provides the employee with the opportunity to dispute the reasons and request that the decision be reviewed. Decisions must be reviewed by an independent person who had no involvement with the disputed decision.
This principle applies to decisions made by the Claims Manager about liability for the injury. It also applies to decisions made by the employer about assessment for capacity for a rehabilitation program, and also about the rehabilitation program. This means that the employee can request a reconsideration
of decisions the employer makes about rehabilitation. In the first instance the employee can request a reconsideration under section 38. If the employee is unsatisfied with the reconsideration, there is recourse to the Administrative Appeals Tribunal. This process must be fully described in the information sent to the employee.
The right to request reasonably practicable adjustments to the workplace to minimise the chance of further injury and to assist the employee to safely remain at, or return to, work (section 39 and 40, SRC Act)
Support for the employee to stay at work or to return to work will minimise the impact of the injury on the employee and on the workplace. This support may involve adjustments to the type or amount of work, to the flow of work, or to the workplace itself to ensure the safety of the employee.

111
The right to be supported by a RCM, and if necessary, a rehabilitation provider, who will organise the development of an individually tailored rehabilitation program (Rehabilitation Guidelines issued under section 41, SRC Act)
Each employer must choose one or more RCMs who have responsibility for developing, managing and monitoring rehabilitation programs to support employees. This means that the RCMs have the primary responsibility and authority to support safe and early return to work after workplace injury.
Research into the impact of parental unemployment on children has found:
A higher likelihood of chronic illnesses, psychosomatic symptoms and lower wellbeing for children in families where neither parent has worked in the previous six months.11
The right to access the employer’s return to work policy, and to participate in its design or change (Rehabilitation Guidelines issued under section 41, SRC Act)
Employee engagement in the design of a return to work policy contributes to the development of a custom-fit document which is responsive to the needs of this important stakeholder group. This will contribute significantly to the employee’s rehabilitation.
The right to privacyThe right to privacy (see Part 4: Section 10—Privacy of this guide for more detail) must be balanced with the need for a safe return to work, therefore the RCM, rehabilitation provider, supervisor and treating practitioners must share information about the employee. However, this information-sharing process must occur in the context of the employee’s right to privacy.
For compensable injuries, the Claim for workers’ compensation form contains a privacy and personal information section which the employee must sign to claim compensation benefits. This form is available on the Comcare website. Licensees generally have their own claim form for compensation. Including the rights and authority to release information on the claim form allows information to be collected, used and disclosed for the purposes of managing the claim. The people who may be able to access this information include the employer, medical practitioners and other health professionals, rehabilitation providers, legal advisors and law enforcement authorities and other government entities where there are obligations under law to do so. This means that information relevant to the employee’s rehabilitation only can be collected, used and disclosed if it can be demonstrated that this collection, use and disclosure is relevant for the purposes of rehabilitation and observes privacy requirements.
Rehabilitation authorities may choose to obtain a signed Authority and consent for the collection and release of medical information specifically designed for the employer in addition to the authority provided on the claim form. In theory the Comcare claim form provides this authority however this provides treatment providers with additional evidence of consent to discuss the employee with the employer.
11 Aylward, M et al. 2010, Realising the health benefits of work, a position statement, The Australasian Faculty of Occupational and Environmental Medicine, Sydney.

112
The right to fair decision making in accordance with the principles of natural justice (sections 38, 61, 62, 63, 72, SRC Act)
The general principles of fair decision making include the principles of natural justice, lawfulness and decision making based on facts. These principles are detailed in Part 1 of this handbook as this is a fundamental principle of the SRC Act.
Comcare’s publication, Better practice guide to decision making, contains further information about the principles of fair decision making.
Employee responsibilitiesThe employee’s responsibilities are:
Attend any medical examinations and rehabilitation assessments arranged by the Claims Manager (section 57, SRC Act) or the employer (section 36, SRC Act)
Medical examinations arranged by the Claims Manager provide information about the employee’s medical condition, the work-relatedness of the condition and whether there is liability for payments relating to the medical condition. Medical examinations and rehabilitation assessments arranged by the employer are focused on the workplace and provide information to support safe and early return to work. Employees are required to attend these examinations. If there is a good reason for not attending, the employee must request an alternative.
Failure to attend the assessment or obstruction of the assessment for rehabilitation may result in suspension of incapacity payments. Once the employee attends the examination, benefits may be reinstated, but there is no retrospective payment of benefits for the suspension period.
Undertake the rehabilitation program provided by the employer (section 37, SRC Act)
Undertaking the rehabilitation program provided by the employer and active participation in the rehabilitation process smooths the safe and early return to work for the employee. This also ensures that entitlements to incapacity payments and benefits under the SRC Act continue.
Failure to comply with the rehabilitation program may result in suspension of incapacity payments. On resuming the rehabilitation program, benefits may be reinstated, but there is no retrospective payment of benefits for the suspension period.
Cooperate with the RCM and workplace rehabilitation provider (sections 36 and 37, SRC Act)
The RCM and rehabilitation provider support the rehabilitation program and ensure that the return to work process progresses smoothly. Cooperation with them facilitates the process and ensures that entitlements to incapacity payments and benefits under the SRC Act continue.
Report any changes in circumstances (sections 114, 116 and 120, SRC Act)
A change in circumstances may affect decisions made by the Claims Manager or by the RCM, and may affect the support required by the employee. This could include changes to the medical condition, changes to home circumstances which might impact on the injury, or changes to financial circumstances.
113
Employer rightsEmployers have rights as well as responsibilities under the SRC Act. The rights and responsibilities described in this section are based on those outlined in sections 36, 37, 38, 40, and 41 of the SRC Act.
This means that the employer can expect the employee will:
» cooperate with the RCM, supervisor and rehabilitation provider
» actively participate in the arrangements provided for workplace rehabilitation
» provide accurate, timely and complete information to the treating medical practitioner, employer and Claims Manager
» be polite and courteous.
Employer responsibilitiesEmployers, as the rehabilitation authority, have the capacity and the responsibility to reduce the cost of workplace injury by providing timely and effective rehabilitation for employees. As outlined in section 2, there are significant responsibilities for employers under the SRC Act.
Briefly, the rehabilitation authority responsibilities include:
» committing to workplace rehabilitation through senior management participation and support
» developing and maintaining a rehabilitation management system
» a comprehensive rehabilitation policy
» appropriate monitoring, and evaluation processes for continuous improvement
» early intervention strategies and a budget to support early intervention
» appointing and supporting RCMs with suitable skills and training.
For individual employees, this means that the employer provides:
» accurate and timely information and advice about workers’ compensation
» early intervention where appropriate
» managed rehabilitation programs tailored to the employee’s needs
» a rehabilitation case manager with appropriate skills, support and resources
» comprehensive and easily accessible information about rights and responsibilities of all key stakeholders.
In line with the principle ‘good work is good for people’, employers acknowledge the influence they have on employees’ health and wellbeing by:
» ensuring that workplaces are safe, and having a workplace culture conducive to health and wellbeing
» accommodating ill or employees to remain in the workplace where possible
» moving beyond legislative requirements to embracing the spirit of inclusive employment practices and best practice injury management.12
Non-complianceFor information on non-compliance and suspension of benefits see Step 3—Rehabilitation planning in this handbook.
12 Aylward, M et al. 2010, Realising the health benefits of work, a position statement, The Australasian Faculty of Occupational and Environmental Medicine, Sydney.

114
PART 3
SECTION 8
CASE STUDIES

115
Case study 1
Sue, an administrative assistant for an Australian Government department, fractured her hand in a fall at work. She attended hospital, received appropriate treatment and has now been certified unfit for her current administrative duties.
Sue has contacted her supervisor and advised that she is unable to fulfil her current role. Having been notified of Sue’s condition, John, the Rehabilitation Case Manager (RCM), should initiate action in line with the organisation’s early intervention framework. Which action should John initiate?
Option 1:
» Contact Sue as soon as possible to discuss her leave of absence.
» Advise her of the medical services available that may assist in improving her capacity, such as physical therapies.
» Express support and concern about her condition.
» Advise her that once she is fit enough for her current duties she can return to work on reduced hours to assist her to return to her pre-injury hours.
Option 2:
» Contact Sue as soon as possible to ascertain her need for assistance.
» Express support and concern about her condition.
» Advise her of the rehabilitation services available, including the possibility of a graduated return to work on modified duties and/or reduced hours as approved by her treating medical practitioners.
» Contact her supervisor and ensure that her supervisor is in regular contact with Sue.
Option 3:
» Contact Sue as soon as possible to discuss her leave of absence.
» Ensure that she submits the correct leave forms.
» Advise her of the medical services available that may assist in improving her capacity, such as physical therapies.
» Advise her to contact him once she has fully recovered, is fully fit and has medical clearance to return to her normal pre-injury hours and duties.
» Contact her supervisor to ensure that her work is allocated to other members of the team except for non-urgent work, which should be kept for her return.
Answer: Option 2

116
Option Consequences Risks
1 Contacting Sue has provided John with the opportunity to ascertain her need for assistance, understand her condition and the expected time off work. However, he has not used this opportunity constructively.
He has also set the expectation that Sue must be fit for her pre-injury duties before she returns to work. He misses the opportunity to discuss modifications to the workplace to allow Sue to return to other duties if her medical condition permits. He has established the basis for a sound rapport between them.
He has not established any communication protocols or the expectation that Sue will be fully supported by both her supervisor and by her RCM.
Long-term absence and disconnection from the workplace.
Delayed recovery from injury.
High cost injury.
2 Contacting Sue and expressing support and concern for her has provided John with the opportunity to ascertain her need for assistance, understand her condition and the expected time off work. It has established the basis for a sound rapport between them. He has already let her know that she will be supported to return to work on modified duties and for reduced hours, and that she does not need to be fully fit before returning. This sets the expectation of return to work and provides a sound basis for ongoing contact and communication.
Ensuring that her supervisor keeps in touch with her reduces the likelihood that she will lose touch with the workplace.
Most effective approach, which increases the likelihood of safe and early return to work.
Establishes communication and expectation of return to work.
Minimises risks of long-term incapacity, delayed recovery and poor rehabilitation outcomes.
3 Contacting Sue provides an opportunity to express support, evaluate whether she may need support to return to work, and establishes workplace rehabilitation as a focus for the future. Focusing on the practical issues of leave misses a valuable opportunity to establish the importance of workplace rehabilitation. While it is important to ensure that the correct forms are completed, and that a workers’ compensation form is submitted if necessary, this should only form one aspect of your first conversation.
As a RCM you should not focus on medical treatment but on services that are available to improve work capacity and independence.
Discussing contact only after Sue is fully fit sets the expectation that she can only return when she has fully recovered and excludes the option of modified duties and reduced hours.
John has not included the supervisor’s responsibilities for ongoing contact and support for Sue. He should ensure that her supervisor reallocates her work.
Long-term absence and disconnection from the workplace.
Delayed recovery from injury.
High cost injury.

117
Sue’s specialist has indicated that although she is unfit for her current pre-injury duties, it is possible that a rehabilitation program could be developed. This would be a program with her same employer, but with different duties as described by the return to work hierarchy. This approach would be effective in maintaining Sue in the workplace, utilising her skills and ensuring a safe and early rehabilitation.
Sue completes the Employer’s Medical authority for consent form (see Authority and consent for the release of medical information page 133) so John can contact her medical specialist to seek guidance about suitable duties for her rehabilitation program. The specialist provides the following restrictions:
» no typing
» restricted phone usage
» no written work
» no lifting.
Sue’s restrictions are significant given that her role is as an administrative assistant and her primary duties involve phone and computer work. Having more insight into Sue’s condition, John now has to determine what action he should take to facilitate a return to work for Sue. Which of the following options should John take?
Option 1:
Organise rehabilitation without a formal rehabilitation assessment under section 36 of the SRC Act. The treating medical practitioner supports an early and safe return to work, has provided clear medical guidance and John has sufficient experience, skills and capacity to manage it.
Option 2:
A formal rehabilitation assessment under section 36 of the SRC Act needs to be organised so that a rehabilitation program can be developed.
Option 3:
Organise a workplace rehabilitation provider to coordinate rehabilitation without a formal rehabilitation assessment. The rehabilitation provider can liaise with Sue’s medical practitioner and refer and approve services for her rehabilitation program under section 37 of the SRC Act.
Answer: Option 3

118
Option Consequences Risks
1 John has the skills and experience to manage or oversee rehabilitation for Sue but does not necessarily have the skills around identifying suitable duties or modified duties that meet her restrictions.
There are no indicators of long-term absence, delayed recovery or conflict in the workplace that might suggest difficulties in Sue’s return to work. John and her supervisor have kept in regular contact with Sue and developed the expectation that she will return to work in a supportive environment with adaptations for her medical restrictions.
As the medical specialist supports rehabilitation and has provided clear guidance about restrictions, there are no indicators that rehabilitation will be complex. However Sue is unable to perform her previous tasks. It will be necessary to identify suitable duties, adaptive techniques and potentially have discussions with the doctor about modifying the restrictions based on adaptive equipment or techniques. A workplace rehabilitation provider will be required to do this.
Sue develops complications and return to work is delayed
John must maintain regular contact with Sue’s medical practitioner and ensure approval of her rehabilitation program.
2 As there is already medical advice that Sue can participate in a rehabilitation program and there are no apparent expectations of delayed rehabilitation or recovery a formal assessment may not be necessary.
However, if any indicators for delayed rehabilitation or recovery emerge, John should immediately arrange for a formal assessment.
Effective approach with possibly unnecessary increased costs.
Delay in providing a rehabilitation program.
3 Engaging a rehabilitation provider is indicated in this scenario.
John should expect the rehabilitation provider to liaise with the manager and identify suitable duties and liaise with the medical practitioner regarding adaptive techniques.
John has delegation for the rehabilitation authority and must sign the rehabilitation program. The rehabilitation provider does not have this delegation. So John must have involvement in the development of the rehabilitation program and cannot completely revoke his responsibilities.
Costs incurred.
The rehabilitation provider must liaise regularly with Sue’s medical practitioner and ensure that her rehabilitation program is approved.

119
A formal assessment by an external assessor is not always required. The Rehabilitation Case Manager (RCM) can decide if the return to work will be straightforward and an assessment not necessary. In this circumstance:
» the treating doctor supports an early and safe return to work and provides clear medical guidance
» the type or circumstances of injury are not complex and no delays in recovery are expected
» the RCM has the full support of both the employee and supervisor to achieve an early and safe return to work
» there are effective relationships and open communication between the treating medical practitioner, the supervisor, the RCM and the employee.
However, someone needs to identify suitable duties that meet her restrictions. If this is not within the capability of the RCM, then a workplace rehabilitation provider will need to be engaged.
If you have any doubts about the need for support for the employee to return to work, it is better to err on the side of caution and refer for a rehabilitation assessment. This is preferable to delaying the decision and discovering later that rehabilitation assistance was required.
John now considers how the rehabilitation program should be developed. Which course of action do you think John should take?
Option 1:
Develop the rehabilitation program in conjunction with a WRP, giving consideration to the return to work hierarchy, recommendations by the treating medical practitioner and suitable employment.
Option 2:
Develop the rehabilitation program independently, giving consideration to the return to work hierarchy, medical practitioner recommendations and suitable employment.
Option 3:
Decide not to provide a rehabilitation program, as there are no suitable duties to sustain Sue’s rehabilitation program without adversely impacting on operational requirements.
Answer: Options 1 and 2 are both correct. John’s discretion and workload will determine his approach

120
Option Consequences Risks
1 John has the skills and experience to manage or oversee rehabilitation for Sue. However, he can engage the help of a rehabilitation provider if necessary. This may be if he has limited time to provide ongoing support for Sue and regular contact with important stakeholders.
John and/or the rehabilitation provider must maintain regular contact with Sue’s medical practitioner and ensure approval of her rehabilitation program.
Effective approach, which increases the likelihood of safe and early return to work.
2 As there are no apparent expectations of delayed rehabilitation or recovery, John can arrange the rehabilitation program independently.
However, if any indicators for delayed rehabilitation or recovery emerge, John should immediately arrange for the involvement of a WRP and possibly a formal assessment.
If John developed the rehabilitation program, another delegate within the organisation must sign the plan.
Effective approach, which increases the likelihood of safe and early return to work.
There may be a risk of conflict of interest, so John must ensure that another delegate reviews and approves the rehabilitation program. There is also a risk that John is unable to identify suitable duties that meet Sue’s restrictions.
3 As Sue has some capacity for work, her rehabilitation should not be delayed. Short-term considerations such as this may result in higher costs in the long term.
High costs if rehabilitation is delayed.
There is a high risk that Sue will experience delayed recovery and long-term absence from work.
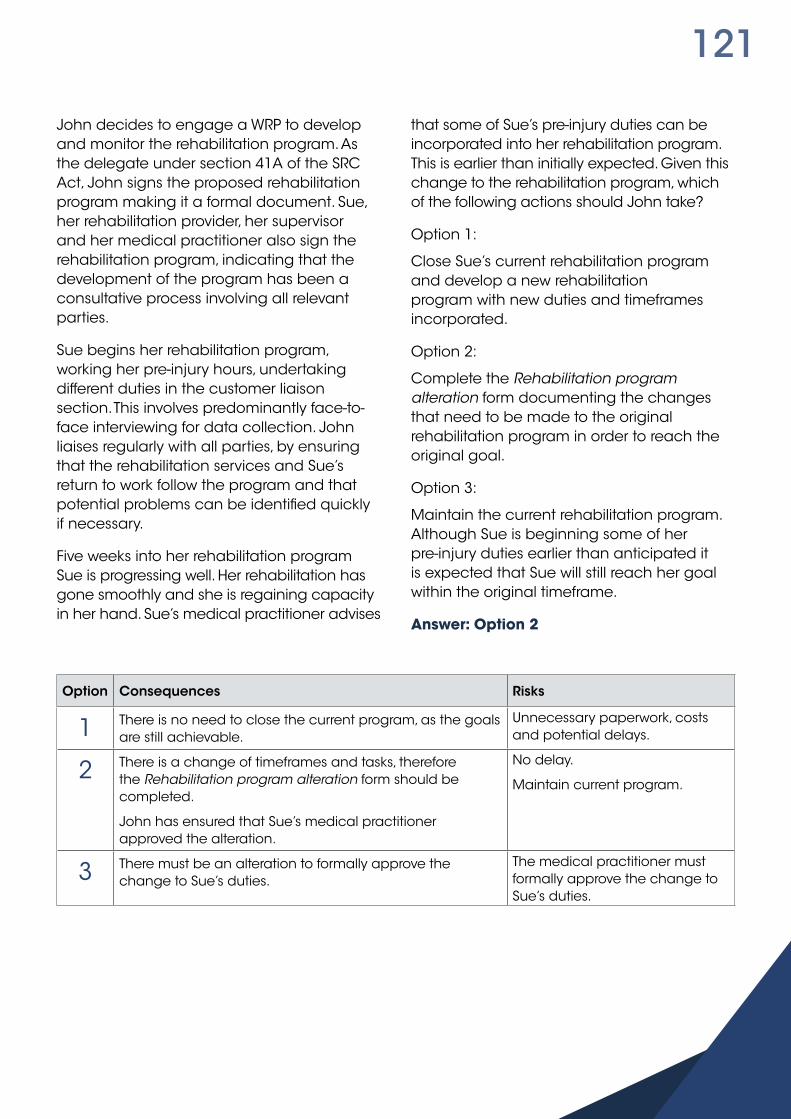
121
John decides to engage a WRP to develop and monitor the rehabilitation program. As the delegate under section 41A of the SRC Act, John signs the proposed rehabilitation program making it a formal document. Sue, her rehabilitation provider, her supervisor and her medical practitioner also sign the rehabilitation program, indicating that the development of the program has been a consultative process involving all relevant parties.
Sue begins her rehabilitation program, working her pre-injury hours, undertaking different duties in the customer liaison section. This involves predominantly face-to-face interviewing for data collection. John liaises regularly with all parties, by ensuring that the rehabilitation services and Sue’s return to work follow the program and that potential problems can be identified quickly if necessary.
Five weeks into her rehabilitation program Sue is progressing well. Her rehabilitation has gone smoothly and she is regaining capacity in her hand. Sue’s medical practitioner advises
that some of Sue’s pre-injury duties can be incorporated into her rehabilitation program. This is earlier than initially expected. Given this change to the rehabilitation program, which of the following actions should John take?
Option 1:
Close Sue’s current rehabilitation program and develop a new rehabilitation program with new duties and timeframes incorporated.
Option 2:
Complete the Rehabilitation program alteration form documenting the changes that need to be made to the original rehabilitation program in order to reach the original goal.
Option 3:
Maintain the current rehabilitation program. Although Sue is beginning some of her pre-injury duties earlier than anticipated it is expected that Sue will still reach her goal within the original timeframe.
Answer: Option 2
Option Consequences Risks
1 There is no need to close the current program, as the goals are still achievable.
Unnecessary paperwork, costs and potential delays.
2 There is a change of timeframes and tasks, therefore the Rehabilitation program alteration form should be completed.
John has ensured that Sue’s medical practitioner approved the alteration.
No delay.
Maintain current program.
3 There must be an alteration to formally approve the change to Sue’s duties.
The medical practitioner must formally approve the change to Sue’s duties.

122
Within 12 weeks Sue has reached her goal of pre-injury hours and duties. John reviews the case with all parties and ascertains that the return to work is durable. After this review, John closes the rehabilitation program and submits the closure form to the Claims Manager.
Through evaluation of his recent cases, John becomes aware of an increasing number of workplace injuries resulting from falls within a certain section of the building, the section where Sue sustained her fracture. Having identified this potential WHS issue what should John do?
Option 1:
Report the issue to management and the health and safety representative (HSR) or WHS committee for action.
Option 2:
Not wanting to cause too much disruption, John inspects the potentially dangerous site himself to look for any obvious risks to employees. Though not qualified in WHS, he feels he is competent to carry out this task.
Option 3:
Given the relatively small number of incidents it may be just a coincidence, so John decides to monitor future notifications that may indicate ongoing problems in that area.
Answer: Option 1
Option Consequences Risks
1 The increased number of falling incidents in this area could be an indicator of increased risk, which should be addressed.
Issues such as this should be reported to help reduce the number of workplace incidents. In this way the rehabilitation process is useful in identifying injury prevention practices. It also assists in developing early intervention strategies that provide the foundation for the risk management framework for rehabilitation.
Further falls in this area if the risk is not addressed.
Evaluation of all workplace incidents and rehabilitation programs should inform future practice.
2 As John is not qualified he should not undertake this activity.
As an employee he has a responsibility to report WHS issues.
Further WHS preventable incidents.
3 As John does not have sufficient information he should report the incident to the appropriate areas in his organisation.
Further preventable WHS incidents.

123
Case study 2
Jake, a customer service officer, works for an employer who has a licence to self-insure under the SRC Act. Jake has contacted his employer to advise he is taking a week off work because of a work-related illness. Jake has been experiencing frequent anxiety attacks and sleep disturbances which he attributes to stress from recent work changes.
Having been notified of Jake’s absence, Jill, the RCM needs to initiate action in line with the organisation’s early intervention framework. Which action should Jill initiate?
Option 1:
Contact Jake toward the end of his leave period to check on his wellbeing and his need for assistance. Advise Jake of the rehabilitation services that will be available to assist him once paperwork for his claim has been lodged.
Option 2:
Contact Jake as soon as possible. Advise him of the rehabilitation services that will be available to assist him once determination of his claim is made.
Option 3:
Contact Jake as soon as possible to ascertain his need for assistance to return to work, making him aware of the rehabilitation services that are available now to assist him in his recovery.
Answer: Option 3

124
Option Consequences Risks
1 Contacting Jake has provided Jill the opportunity to ascertain his need for assistance, understand his condition and the expected time off work. However she has left this contact until too late during Jake’s absence and not used this opportunity constructively.
She has not set any expectation that Jake will be supported to return to work.
She offers help only after submission of a workers’ compensation claim.
This is a psychological injury claim—a potentially expensive claim. This injury requires extra thought and care about employer support for rehabilitation, as well as early and proactive intervention.
High risk of long-term absence and disconnection from the workplace.
Delayed recovery from injury.
Very high cost injury.
2 You should not wait for claim determination to begin rehabilitation activities.
In this scenario, Jill has contacted Jake during an early stage of his injury. This provides a valuable opportunity to establish contact, evaluate his rehabilitation needs and to establish expectations for early and safe return to work. However, Jill has not done this and has increased the likelihood of long-term incapacity.
She should also ensure that Jake’s supervisor establishes and maintains contact with him during his absence.
Long-term absence and disconnection from the workplace.
Delayed recovery from injury.
High cost injury.
3 Contacting Jake provides an opportunity to express support, evaluate the support needed for an early and safe return to work, and establish workplace rehabilitation as a focus for the future.
Jill has contacted him during the very early stage of his absence, increasing the likelihood of an early return to work.
However, she also needs to continue regular contact, engage Jake’s supervisor and arrange a workplace rehabilitation assessment. As this is a psychological injury, Jill should engage a workplace rehabilitation provider as soon as possible to arrange a rehabilitation assessment.
Jill should follow up on suggested WHS issues of workplace change raised by Jake’s diagnosis.
Most effective approach, which increases the likelihood of safe and early return to work.
Establishes communication and expectation of return to work.
Minimises risks of long-term incapacity, delayed recovery and poor rehabilitation outcomes.
Extra tasks as suggested will ensure adequate intervention to minimise risk of long-term incapacity.
125
Given the symptoms of Jake’s injury, anxiety, fatigue and depression, it was agreed he may benefit from accessing the Employee Assistance Program (EAP). Jake discloses to Jill that conflict with his manager has contributed to his condition and he is adamant that he cannot return to work under his manager’s supervision.
After this conversation Jake has been certified unfit for work for an additional three weeks and is planning on lodging a workers’ compensation claim for his condition.
Having more insight into Jake’s situation, Jill is now able to undertake a risk assessment and determine what action she should take to facilitate a safe and early return to work for Jake. Which of the following actions should Jill take?
Option 1:
Organise mediation between Jake and his supervisor as soon as possible to resolve any issues and facilitate a timely return to work.
Option 2:
Give Jake time to attend EAP and manage his symptoms. Advise Jake that she will maintain regular contact over the next three weeks and will meet toward the end of this time to determine how he feels about returning to work.
Option 3:
Given that the period of Jake’s incapacity is going to be greater than ten days, organise a rehabilitation assessment to determine his injury status.
Answer: Options 1 and 3

126
Option Consequences Risks
1 Early intervention is crucial.
Commence mediation as soon as possible to help facilitate Jake’s return to work and assist with his injury management.
Mediation can be run concurrently with the referral for a rehabilitation assessment.
This case has many indicators of long-term absence and delayed recovery, including conflict with the supervisor and expected absence of more than ten days.
Early intervention requires a multi-faceted approach.
Effective approach, if supported by medical evidence which increases the likelihood of safe and early return to work.
Other interventions must also be instigated to support early intervention.
Reduces risks of long-term incapacity, delayed recovery and poor rehabilitation outcomes.
2 Jill should not wait for symptoms to resolve.
However, Jill has said she will contact him regularly. This enables her to monitor his condition and evaluate the need for assessment. It also establishes a connection between them.
Risk of prolonged absence and poor rehabilitation outcomes.
Delay in providing a rehabilitation program may lead to increased costs.
3 As the expected duration of absence is greater than 10 days, Jill should immediately arrange for an assessment of Jake’s capacity for workplace rehabilitation.
Undertaking a rehabilitation assessment now will give Jill the opportunity to determine Jake’s work capacity at an early stage and take advantage of the benefits of early intervention. The assessment will provide the basis for a decision about Jake’s rehabilitation program.
However, as above, Jill must also maintain contact with Jake and deal with the workplace conflict.
Effective approach, which increases the likelihood of safe and early return to work.
Other interventions must also be instigated to support early intervention.
Reduces risks of long-term incapacity, delayed recovery and poor rehabilitation outcomes.

127
The Mental Health Council of Australia advises that early intervention is an effective way to support people with mental issues back to work. In fact, the longer that someone with a mental health problem is out of the workforce, the harder it becomes for them to find work and sustain that employment.
Jill is uncertain about how Jake’s assessment should be managed. Should she arrange for the assessment to be provided internally or externally? Jake’s medical practitioner has provided clear information about Jake’s current symptoms. However, there are no stated specific restrictions or any information about prognosis. Jill is experienced in managing employees with psychological injuries. However, given the conflicted relationship the employee has with his supervisor, she feels it may be better to manage the assessment externally. Which option should Jill choose?
Option 1:
Manage rehabilitation without a formal assessment. Generally this is recommended where the injury is not complex, the medical practitioner has provided clear medical advice, no delays in recovery are expected and the RCM has the full support of both Jake and his supervisors to achieve a return to work.
Option 2:
Arrange a rehabilitation assessment under section 36 of the SRC Act. Generally this is recommended when the injury is complex, no clear medical advice has been provided, the employee has limited or no work capacity and there is no effective relationship between the treating medical practitioner, the employee and supervisor. The Rehabilitation Guidelines state that a workplace rehabilitation provider SHALL be used when ‘bio-psychosocial obstacles for recovery and return to work have been identified that require rehabilitation services’. Jake’s case would fall into this criterion.
Option 3:
Wait until the mediation is complete. As mediation has begun and has been productive, Jill decides to defer the referral for assessment, as it may not be necessary if all the issues are resolved.
Answer: Option 2
Option Consequences Risks
1 In this case, there are several indicators of potential long-term absence and delayed recovery. There is conflict with Jake’s supervisor that suggests potential difficulties in Jake’s return to work. There are more than 10 days of absence. There is no indication that Jill has spoken to Jake’s medical practitioner to demonstrate that Jake will receive extensive support to return to work.
High risk of long-term incapacity and slow recovery.
High cost workers’ compensation claim.
Decreased workplace productivity.
2 As there are significant indicators of delayed incapacity and recovery, a WRP should be engaged immediately and an assessment arranged. This aligns with the recommendations in the Rehabilitation Guidelines.
Increased opportunity for positive rehabilitation outcomes.
3 There are significant indicators of poor rehabilitation outcomes. Do not delay assessment or early intervention.
High costs and long-term incapacity.

128
One in five Australians experiences a mental illness every year. Jill is therefore dealing with a very common issue and one that many Rehabilitation Case Managers will need to manage. Despite the difficulties ‘all Australians have a right to work and are entitled to a safe and healthy workplace’.13 Workers with Mental Illness: a Practical Guide for Managers, by the Australian Human Rights Commission, can help you to understand and manage these illnesses.
Jill receives the section 36 assessment report from the workplace rehabilitation provider. It states that Jake has a current capacity of 12 hours a week and three days a week; he should have minimal customer contact; and should not work under the direction of his current supervisor. The report suggests that Jake will require a six month graduated return to full-time work. Incorporating these recommendations into Jake’s rehabilitation program will be difficult for Jill, who is concerned about the effect they will have on operational requirements.
The rehabilitation program can be provided either by Jill herself or in conjunction with a WRP. In managing the rehabilitation program, which course of action do you think Jill should take?
Option 1:
Develop the rehabilitation program in conjunction with a WRP, implementing as many of the recommendations as possible without interfering with operational requirements.
Option 2:
Develop the rehabilitation program in conjunction with a WRP, giving consideration to the return to work hierarchy, section 36 assessment recommendations and suitable employment.
Option 3:
Decide not to provide a rehabilitation program, as there is no availability of suitable duties to sustain Jake’s rehabilitation program without adversely impacting on operational requirements.
Answer: Option 2
Option Consequences Risks
1 There are significant indicators of poor rehabilitation outcomes, long-term absence and delayed recovery. Conflict with his supervisor suggests that there may be difficulties in Jake’s capacity to return to work.
These suggest that operational requirements should not be a deciding factor in finding suitable duties for Jake.
Poor rehabilitation outcomes.
Poor recovery and long-term incapacity.
High cost claim.
2 These are important requirements for a successful return to work.
Jill should also ensure ongoing mediation if necessary and regular communication with Jake.
Increased opportunity for positive rehabilitation outcomes.
3 There are significant indicators of poor rehabilitation outcomes, long-term absence and delayed recovery. Conflict with his supervisor suggests that there may be difficulties in Jake’s capacity to return to work.
These suggest that operational requirements should not be a deciding factor in finding suitable duties for Jake.
Poor rehabilitation outcomes.
Poor recovery and long-term incapacity.
13 www.humanrights.gov.au/sites/default/files/document/publication/workers_mental_illness_guide_0.pdf.
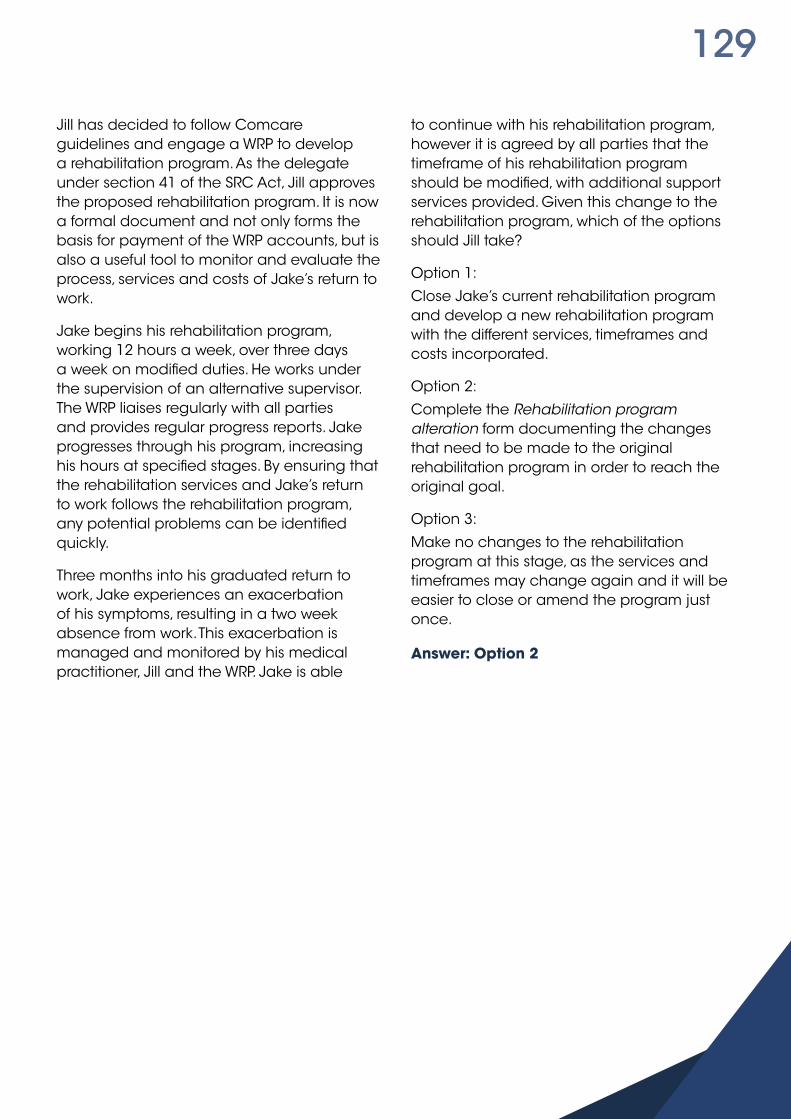
129
Jill has decided to follow Comcare guidelines and engage a WRP to develop a rehabilitation program. As the delegate under section 41 of the SRC Act, Jill approves the proposed rehabilitation program. It is now a formal document and not only forms the basis for payment of the WRP accounts, but is also a useful tool to monitor and evaluate the process, services and costs of Jake’s return to work.
Jake begins his rehabilitation program, working 12 hours a week, over three days a week on modified duties. He works under the supervision of an alternative supervisor. The WRP liaises regularly with all parties and provides regular progress reports. Jake progresses through his program, increasing his hours at specified stages. By ensuring that the rehabilitation services and Jake’s return to work follows the rehabilitation program, any potential problems can be identified quickly.
Three months into his graduated return to work, Jake experiences an exacerbation of his symptoms, resulting in a two week absence from work. This exacerbation is managed and monitored by his medical practitioner, Jill and the WRP. Jake is able
to continue with his rehabilitation program, however it is agreed by all parties that the timeframe of his rehabilitation program should be modified, with additional support services provided. Given this change to the rehabilitation program, which of the options should Jill take?
Option 1:
Close Jake’s current rehabilitation program and develop a new rehabilitation program with the different services, timeframes and costs incorporated.
Option 2:
Complete the Rehabilitation program alteration form documenting the changes that need to be made to the original rehabilitation program in order to reach the original goal.
Option 3:
Make no changes to the rehabilitation program at this stage, as the services and timeframes may change again and it will be easier to close or amend the program just once.
Answer: Option 2

130
Option Consequences Risks
1 The rehabilitation program should be closed in the following circumstances:
» when a return to pre-injury duties or optimum function has been achieved
» when the current program’s goals are no longer achievable and a new program with new goals is required
» when the rehabilitation authority changes due to change in employment circumstances or due to machinery of government (MOG) changes
» when you change the rehabilitation provider
» when workplace rehabilitation is no longer required.
These circumstances do not apply here.
Unnecessary costs and paperwork
2 The Rehabilitation program alteration form is to be completed when there is a change of services, change of the interim goals or timeframes but no change to the final goal.
Jill should also consider whether possible modifications to the rehabilitation program might be helpful. She might consider holding a case conference to plan further actions. It is good practice to consult with the employee and the medical practitioner about the changes to the rehabilitation program.
Correct procedure.
Avoid unnecessary paperwork.
3 The Rehabilitation program alteration form must be completed regardless of projected future activity.
Incorrect procedure.

131
Despite this setback, Jake continues to improve and within eight months he is on his pre-injury duties and pre-injury hours under the supervision of an alternative supervisor. This current arrangement is satisfactory and sustainable for both Jake and his organisation. Jill is considering closing the program. Which of the following should she undertake?
Option 1
Review the case with all parties to ascertain whether the return to work has been durable and reach agreement on closure of the rehabilitation program. Request the WRP to submit the closure form to the licensee’s Claims Manager.
Option 2:
Review the case with all parties to ascertain whether the return to work has been durable and ask all parties to sign the closure form. Jill submits the closure form to the licensee’s Claims Manager.
Option 3:
Review the case with all parties to ascertain whether the return to work has been durable. After this review Jill decides whether to close the rehabilitation program. Jill submits the closure form to the licensee’s Claims Manager.
Answer: Option 3
Option Consequences Risks
1 The RCM makes the final decision to close the rehabilitation program and signs the Rehabilitation program cessation form, detailing the outcome achieved.
Incorrect procedure—the WRP signature does not close the rehabilitation program.
2 The RCM makes the final decision to close the rehabilitation program. This decision should be made in conjunction with the other parties, but their signatures are not required.
Unnecessary procedure.
3 The RCM makes the final decision to close the rehabilitation program and signs the Rehabilitation program cessation form, detailing the outcome achieved.
It is important that the program is closed as it demonstrates that the end has been reached and also specifies which goals have or have not been achieved.
The completed and signed Rehabilitation program cessation form signals the end of the contract between Jill and the WRP. The Claims Manager will not pay for services associated with rehabilitation programs after the closure date.
Correct procedure.

132
PART 3
SECTION 9
RETURN TO WORK FORMS
This section of the handbook describes the forms used by premium payers in the workplace rehabilitation process. As there are differences for licensees in the arrangements for reconsideration of decisions, these forms need to be amended if licensees wish to use them.

133
Most licensees have produced forms unique to their organisations, which have been approved for use in workplace rehabilitation.
Key points» Forms are available for each of the steps
in the return to work process.
» These forms contain information about the rights and responsibilities of the employee.
» Each decision about rehabilitation assessment and rehabilitation program for an employee must be in writing, must contain the reasons for the decision, and must alert the employee to all their rights and responsibilities under the SRC Act. They must be signed with the correct delegation, that is, by the delegated Rehabilitation Case Manager (RCM). The forms have appropriate sections to satisfy these requirements.
» Sample completed forms are available on the Comcare website to help you understand the required content.
» it is not mandatory for employers to use the Comcare forms however the forms contain all the mandatory information required. If an organisation chooses to develop their own forms they must include all the information on the Comcare forms.
Authority and consent for the release of medical information
Comcare form SRC131www.comcare.gov.au/Forms_and_Publications/forms2/claims_forms2/claims_forms/authority_and_consent_for_release_of_med_info
This form is used by Comcare to obtain the employee’s agreement to release medical and other relevant information to parties involved in the return to work process. The form is designed to allow appropriate sharing of information. In theory the Comcare claim form provides this authority however Comcare at times chooses to obtain this additional authority.
The employer may also choose to obtain a signed Authority and consent for the collection and release of medical information specifically designed for the employer in addition to the authority provided on the claim form.
The form must be explained to employees, and signed by them at your first meeting. A copy of the form should accompany the Rehabilitation assessment examination form.

134
Rehabilitation Assessment examination (section 36 assessment)
Comcare form SRC116www.comcare.gov.au/Forms_and_Publications/forms2/injury_management_forms/injury_management_forms/Rehabilitation_assessment_examination
What is it used for?This form authorises a suitably qualified person—WRP, legally qualified medical practitioner or panel—to undertake a rehabilitation assessment of the employee under section 36 of the SRC Act. This assessment assesses the employee’s capacity to participate in a rehabilitation program.
When is it used?This form is normally completed as soon as it is established an assessment under section 36 is required. The form satisfies the legal requirements for a referral and provides the relevant contact details to the assessor.
How is it used?A copy of the Employer’s Authority for the release of medical information form should accompany the Rehabilitation assessment examination form to the assessor.
Does the referral form need to be used?No. If the delegate is able to document the referral details and document the determination that the employee shall undergo a section 36 assessment in a letter to the employee, if they prefer. However, they must ensure the employee is provided with information on all rights and responsibilities under the SRC Act.
Whose job is it to complete the form?The RCM who has delegation under the SRC Act completes and signs the form.
Who makes sure it is done?The RCM has sole responsibility.
Why is the form important?This form documents a determination made under section 36 of the SRC Act that the employee shall undergo an assessment of capability to undertake a rehabilitation program.

135
Suitable duties
Comcare form SRC109www.comcare.gov.au/Forms_and_Publications/forms2/injury_management_forms/injury_management_forms/suitable_duties_src109
What is it used for?This form is designed to assist the RCM and WRP to work with the employee, their supervisor and treating doctor to clarify, identify and match suitable duties to the employee’s assessed capacity.
While this form is not mandatory, it is an aid that will enhance the assessment and consideration process when identifying suitable duties for an employee.
When is it used?This form:
» is in three parts to enable the RCM or WRP (where engaged) to bring together information about the pre-injury work, potential suitable duties and medical recommendations on work—the whole form or just relevant part should be forwarded to the treating doctor for their input
» may be used when completing an assessment of an employee’s capacity to undertake a rehabilitation program
» can be provided to the treating doctor to assist them with understanding the requirements of the job and making an informed decision about return to work capacity and any medically required restrictions.
Whose job is it to complete the form?The RCM or WRP can arrange for this form to be completed in consultation with the employee, their treating doctor (if required), the employee’s supervisor and the employee’s treating doctor. The suitable duties form should be attached to the rehabilitation program and the rehabilitation program should indicate that it is attached. This ensures that the activities referred to in the suitable duties program are included in the rehabilitation program and clearly indicates to all parties that these activities must be completed as part of participating in the program.
Who makes sure it is done?This form provides the RCM, WRP (where engaged), treating doctor, treatment providers and the employee and their supervisor with a shared understanding of the employee’s pre-injury duties and possible options when alternative duties are required to maintain the employee in the workplace or enable an early return to work. This allows everyone to work together to facilitate a safe and durable return to work.

136
Rehabilitation program (section 37 rehab program)
Comcare form SRC40www.comcare.gov.au/Forms_and_Publications/forms2/injury_management_forms/injury_management_forms/Rehabilitation_program
What is it used for?The rehabilitation program (initiated under section 37 of the SRC Act), sometimes referred to as the return to work plan, details the rehabilitation program developed in consultation with the employee, WRP, RCM and after consultation with the treating doctor. The rehabilitation program represents a contract between the employer, the employee and the WRP.
How is it used?The rehabilitation program is developed usually by the RCM and WRP (if involved) in consultation with the employee, supervisor and after medical consultation. It documents the rehabilitation goals, WRP services and costs, the responsibilities of all parties, and the expected outcome and timeframes for the rehabilitation program. The rehabilitation program must be discussed with the employee, whose attention must be drawn to the statement of obligations and rights detailed on the initial pages of the form. A date is agreed for the program to begin, and when it will end. After this process has been completed, the employee, RCM and WRP all sign it to acknowledge their involvement in the program. Copies of the entire rehabilitation program are then given to the employee, the treating medical practitioner, the RCM, the WRP and the Claims Manager.
Whose job is it to complete the form?The RCM has overall responsibility for completing this document. The WRP (if involved) may be asked to document the responsibilities section, which details the WRP activities and outcomes, service codes and costs. The WRP may also complete the documentation of the rehabilitation goals and other details on the form as a draft document. The RCM who has delegation under the SRC Act is responsible for reviewing the draft, ensuring consultation with all parties and completing the determination section and signing it.
The employee, RCM and supervisor sign the rehabilitation program to indicate that they have been involved in the development of the program. The WRP signs the rehabilitation program to document that they agree to provide the rehabilitation program as described. However the ONLY signature required making this a legal determination is the signature of the RCM that has a written delegation under the SRC Act. It must be signed and dated by the RCM before the start date of the program.
Who makes sure it is done?The RCM with delegation under the SRC Act is responsible for deciding (or not) to develop a rehabilitation program for the employee, and for ensuring that the determination under section 37(1) of the SRC Act is documented correctly. In doing so, the RCM needs to ensure that all the matters have been considered as detailed in subsection 37(3)(a)–(h), and in particular that section 37(3)(f), the employee’s attitude to the program, has been considered. Failure to consider all the matters and to adequately document this may lead to the rehabilitation program being invalid.

137
The Rehabilitation program form includes a section for the RCM to document the reasons for the determination, and this section must be completed. The space on the form may be too small to do this effectively. In this case address part 3 a–h on a separate document and write ‘see attached’ in the box provided on the form. See appendix 5 for guidelines and suggestions for completing the form in relation to section 37(3).
The RCM must ensure that a proposed rehabilitation program is discussed with the employee. The employee must be given adequate time to consider the proposed rehabilitation program, before all parties sign it. Every concern raised by the employee must be considered, and these discussions must be carefully and thoroughly documented. This is generally addressed in the Part 3 a–h considerations.
Why is the form important?The rehabilitation program documents a formal determination made under section 37(1) of the SRC Act that the employee shall undertake a described rehabilitation program. It also describes the services provided by the WRP and documents approval of rehabilitation costs. This is the basis on which accounts for rehabilitation program services submitted by the WRP will be paid by the Claims Manager.
Pages 1 and 2 of the Rehabilitation program form contain important explanatory information for the RCM, the WRP, the employee and supervisor. This information concerns the purpose of the form, the delegation, employee responsibilities and the employee’s rights in requesting a review of the rehabilitation program if they do not agree with the determination made by the employer.
Rehabilitation program alteration
Comcare form SRC86www.comcare.gov.au/Forms_and_Publications/forms2/injury_management_forms/injury_management_forms/Rehabilitation_program_alteration
What is it used for?This form is used to document any changes to a workplace rehabilitation program once it has been agreed.
When is it used?This form is used when the WRP or RCM decides that the rehabilitation program should be changed to achieve the final goal. These changes might include altered timeframes or rehabilitation costs, or when additional services are required. This form does not change the final goal.
How is it used?The WRP discusses the progress of the rehabilitation program with all parties.
The RCM, WRP supervisor and employee meet, agree to any proposed changes and sign the Rehabilitation program alteration form.
Copies of the Rehabilitation program alteration form must be distributed to all parties, including the Claims Manager.

138
Whose job is it to complete the form?It is the RCM’s role to complete this form however they may ask the WRP to draft the Rehabilitation program alteration form. It is signed by the employee and WRP (and the treating practitioner if appropriate) as evidence of consultation but it is signed by the RCM making it a formal determination under the SRC Act.
Who makes sure it is done?The RCM with delegation under the SRC Act is responsible for ensuring that this form has been completed.
Why is it important?The Claims Manager will not accept liability for payment of any additional services by the WRP unless this form has been completed before the services are provided. It also ensures that all parties have been consulted, and have given their consent to the proposed changes.
Failure to complete the form could also mean the RCM has not changed the original determination, and has not advised the employee in accordance with the requirements of the SRC Act.
Rehabilitation program closure form
Comcare form SRC41www.comcare.gov.au/Forms_and_Publications/forms2/injury_management_forms/injury_management_forms/Rehabilitation_program_closure_recordion
What is it used for?This form when signed by the delegate (usually the RCM) constitutes a determination by the rehabilitation authority, under subsection 37(1) of the SRC Act that the rehabilitation program which commenced on a specified date is to close or cease.
Signing the Rehabilitation program closure form also completes your contract with the WRP.
When is it used?A closure determination must be made when the delegate decides to close the rehabilitation program prior to its planned completion date and/or achievement of the goal. Where the rehabilitation program has been completed, that is, the goals have been achieved and/or the end date reached, a formal determination is not required. However, page 2 of this form must be completed and a copy sent to Comcare.
A rehabilitation program may be closed if the original return to work goals cannot be achieved and new goals need to be developed. This requires negotiation of a new rehabilitation program.

139
How is it used?The RCM makes the decision to close the program in consultation with all parties.
The RCM, WRP, employee and supervisor meet to sign the Rehabilitation program closure form.
Copies of the Rehabilitation program closure form are distributed to all parties, including the Claims Manager.
The WRP is responsible for writing a closure report summarising the rehabilitation services provided and the outcomes achieved.
Whose job is it to complete the form?The WRP (if involved) drafts the Rehabilitation program closureform ensuring all details of the employee’s return to work and the achievement of the rehabilitation goals are recorded. The employee, RCM, WRP and supervisor all sign it.
Who makes sure it is done?The RCM is responsible for ensuring that this form has been completed at the conclusion of the rehabilitation program.
Why is it important?In cases where a rehabilitation program is closed prior to its completion the form is a legal document indicating that the delegate has made a determination.
In other cases the closure record formally closes the rehabilitation program. It is important to document the success or otherwise in achieving rehabilitation outcomes and this is done formally by completing the Rehabilitation program closure form. It also ensures that all parties
have been consulted, and have given their consent to close the rehabilitation program.
The closure of the rehabilitation program also means that the WRP cannot provide services against that program after the closure date. If circumstances change, the RCM is able to reengage a WRP to undertake another rehabilitation assessment or develop a new rehabilitation program.
Work trial agreement
Comcare form SRC64www.comcare.gov.au/Forms_and_Publications/forms2/injury_management_forms/injury_management_forms/work_trial_agreement
What is it used for?A work trial allows the employee the opportunity to work with a different employer as an interim measure before returning to pre-injury employment or before taking on longer term duties with a new employer. A work trial needs to be fully documented to ensure that all parties are informed about the process, have committed to the process, and understand their responsibilities. This agreement aims to secure a common understanding and commitment to the work trial, and may be modified after consultation with all parties. This agreement should be developed in consultation with the employee, medical practitioner, host employer, WRP and RCM.

140
Whose job is it to complete the form?The completion of this form is the responsibility of the RCM or WRP in conjunction with the treating medical or health practitioner, employee, supervisor and host employer. The rehabilitation program should refer to the work trial agreement and the rehabilitation program should indicate that the work trial form is attached.
Who makes sure it is done?The RCM with delegation under the SRC Act retains the delegation and responsibility for rehabilitation for the employee at all times. Therefore, the RCM must be involved in each step of the process, overseeing the development and implementation of a rehabilitation program involving a work trial.
Why is it important?A negotiated work trial agreement is an essential requirement for ensuring the success of a work trial placement. It should outline the expectations of each party, the duties, medical considerations and restrictions, work hours, and timeframe of the agreement. This ensures that all parties share a common understanding of each other’s role in the process, in addition to the direction and aim of the work trial placement. This agreement is specific to each placement.
141
PART 4
SECTION 10
PRIVACY
142
Throughout the workplace rehabilitation process, it is necessary to collect, store, use and disclose an employee’s personal information.
This section provides general information about obligations under the Privacy Act 1988 (Privacy Act) when handling an employee’s personal information during the rehabilitation process.
The Privacy Act sets the minimum standards that must be met when collecting, using, storing and disclosing an individual’s personal information.
Personal information is broadly defined in the Privacy Act as information or opinion about an individual whose identity is apparent or can be reasonably ascertained from the information or opinion.
Some examples of personal information include:
» names, addresses, phone numbers or email addresses
» medical certificates, clinical notes or medical reports
» payslips and bank statements
» witness statements.
Personal information dealt with in the rehabilitation process may include information regarding the employee’s employment, living arrangements, health and other medical information. Health and medical information is considered sensitive personal information and as such, the Privacy Act provides extra protections for its handling.
The Privacy Act contains 13 Australian Privacy Principles (APPs) which:
» set out legally binding standards for handling personal information
» regulate how entities collect, store, use and disclose personal information
» allow people to access the information that the agencies keeps about them
» allow people to correct or update their information.
A copy of the APPs are available on the OAIC’s website: www.oaic.gov.au.
Further information can be obtained from:
» your organisation’s privacy officer or legal adviser
» the Office of the Australian Information Commissioner at www.oaic.gov.au
» Comcare at www.comcare.gov.au/about_us/privacy.

143
PART 4
RESOURCES
This section contains resources and other information to support you in your role as a Rehabilitation Case Manager.

144
LegislationThe SRC Act is the Act that relates to workplace rehabilitation and workers’ compensation for eligible employees. This includes employees of the Australian and ACT Governments and statutory authorities, and some national employers who have been granted a licence to self-insure for workers’ compensation under the SRC Act.
The SRC Act is available on Comcare’s website at www.comcare.gov.au.
Comcare resources
Comcare reporting, advice and assistanceComcare produces a number of reports, publications, policy advice and other documents to educate and inform employers, employees and other stakeholders. Comcare also provides education, advice and assistance to help you to fulfil your role as Rehabilitation Case Manager (RCM).
Comcare reportingIf you are a RCM in a premium paying organisation, Comcare makes determinations about liability and benefits for your employees. Comcare can provide you with relevant reports for those claims.
Incapacity payment authority reportThe incapacity payment authority report is a notice available to employers through the Customer Information System (CIS) that advises when Comcare makes a decision to pay or void a period of incapacity on a particular claim.
EFT/cheque reimbursement and remittance adviceSent weekly, fortnightly, four-weekly (two pay periods) or calendar-monthly to the postal address or the nominated email address attached to your cheque receiving cost centre. The remittance advice contains details of each incapacity period being reimbursed in the cheque or EFT payment. The remittance advice is also available on CIS.
Customer Information System (CIS)CIS is a service that gives your agency access to your injury management and claims information. You can use this information to measure and monitor your agency’s injury management and claims performance. Access to CIS is to authorised personal only. For more information about CIS please contact the Comcare Employer Account Management team.
Comcare assistance
Comcare Injury Management Advisory Service (IMAS)
Comcare offers advice to rehabilitation authorities to help you manage the rehabilitation of employees at risk of poor rehabilitation outcomes, by providing information about:
» early intervention for potentially high cost claims
» complying with guidelines issued by Comcare
» developing strategies for improving prevention and injury management performance
» identifying and promoting better practice for rehabilitation
» analysing rehabilitation performance » case conferences» case reviews.
145
Comcare Injury Management Advisors are available to answer questions and provide advice and assistance on rehabilitation and return to work issues.
For assistance you can contact Comcare at 1300 366 979 and ask to speak to an injury management adviser or email [email protected].
Training, information and education
Comcare provides training and education courses to help you understand and manage your responsibilities.
Other training
Comcare conducts several programs about the SRC Act and the WHS Act to support organisations operating under the Comcare scheme.
Safety Rehabilitation Compensation courses include:
» Workplace Rehabilitation Provider
» Type of Occurrence Classification System (TOOCS)
» Workers’ Compensation: a payroll perspective
» A Rehabilitation Delegates guide to: Case management
» A Rehabilitation Delegates guide to: Complex cases
» SRC Act in a day
» A supervisor’s role in early intervention and rehabilitation
A full listing of Comcare’s training programs is available from the Comcare website at: www.comcare.gov.au/training/full_course_list or by phoning the Education Team on 1300 366 979.
Customer forumsComcare hosts and delivers a number of events during the year designed to educate, enhance and challenge organisations to achieve their workplace safety, compensation and rehabilitation objectives. Forums are generally hosted by the Employer Account Management team or the Injury Management Advisory Service.
Through these forums Comcare can communicate with industry representatives and providers on a range of issues, topics and policies. These events provide participants with the opportunity to meet industry peers and take part in discussions and activities.
See the Comcare Events section of the website for details.

146
PublicationsComcare produces a number of publications to provide advice and assistance on injury management as well as other issues related to working within the Comcare scheme. These include fact sheets, jurisdictional policy advices, newsletters and research reports.
Injury management publications include information about body stressing injuries, early rehabilitation intervention, Guidelines for Rehabilitation Authorities 2012 and leadership commitment.
Many of the relevant publications and guidance materials have been referred to in this handbook. They are available on the Comcare website www.comcare.gov.au.
Research reportsResearch and emerging trends help to inform Comcare’s future priorities and policy development. Research reports relevant to injury management include the Health Benefits of Work; management of body stressing injuries; and prevention and management of customer aggression. The Australia and New Zealand Return to Work Monitor is a national survey of employees who have had 10 days or more compensation. This is a valuable source of information about return to work trends, successful return to work strategies, and the extent to which stakeholders help or hinder the return to work process.
For information about workers’ compensation claim statistics and claims data, see the Compendium of OHS and Workers’ Compensation Statistics endorsed by the Safety Rehabilitation and Compensation Commission (SRCC) on the SRCC website at www.srcc.gov.au.
Comcare’s annual reportComcare’s annual report documents the activities and performance of Comcare during the financial year. It highlights Comcare’s approach to workplace health and safety, to claims determination and to injury management.
These publications and reports are available on Comcare’s website.
ReferencesThese are the references used in this handbook.
Australian Institute of Social Research 2008, The Role of the Workplace in Return to Work: Discussion Paper, Workcover SA, Adelaide.
Australian Medical Association 2002, Privacy Resource Handbook for all Medical Practitioners in the Private Sector, Australian Medical Association, Canberra.
AMA—see Australian Medical Association.
Australian Human Rights Commission, 2010, Workers with Mental Illness: a Practical Guide for Managers, Australian Human Rights Commission, Sydney.
Bio-psycho-social Injury Management, Heads of Workers’ Compensation Authorities, www.hwca.org.au.
Comcare, Improving outcomes through rehabilitation management systems: a continuous improvement guide, Comcare, Canberra.
Hu-Tech Associates Ltd. 2006, The costs and benefits of active case management and rehabilitation for musculoskeletal disorders, Research Report 493, Health and Safety Executive, UK.

147
Institute for Work & Health 2004, Workplace-based Return-to-Work Interventions: a systematic review of the quantitative and qualitative literature, Summary, report prepared by Franche, RL, Cullen, K, Clarke, J, MacEachen, E, Frank, J, Sinclair, S, Reardon, R, Institute for Work & Health, Toronto.
Office of the Privacy Commissioner 2001, Privacy Obligations for Commonwealth Contracts, Information Sheet No 14, Office of the Privacy Commissioner, Canberra.
Planning Occupational Health and Safety: a guide to OHS Risk management, 8th edn, CCH Australia.
Privacy NSW 1999, A guide to the Information Protection Principles, Privacy NSW, Sydney.
The Royal Australasian College of Physicians, Australasian Faculty of Occupational and Environmental Medicine, 2010, Position Statement on Realising the Health Benefits of Work, Sydney.
SA Workcover 2010, Suggested steps to help those workers who may be ‘at risk’, viewed 24 May 2010, http://main.workcover.com/site/home.aspx.
The Australian Public Service Social Inclusion policy design and delivery toolkit, www.socialinclusion.gov.au.
Waddell G, 2006, Preventing incapacity in people with musculoskeletal disorders, UnumProvident Centre for Psychosocial and Disability Research Cardiff University, UK.
Waddell G, Burton AK, 2004, Concepts of rehabilitation for the management of common health problems, The Stationary Office, London.

148
PART 4
GLOSSARY

149
AATAdministrative Appeals Tribunal. The AAT conducts independent merits review of administrative decisions made under Commonwealth laws by Australian Government agencies.
Claims Manager (CM)Comcare employee who manages claims for compensation made by employees of Australian and ACT Government according to the SRC Act.
An employee of a licensee (self-insurer) or outsourced organisation who manages claims for compensation made by employees of self-insurers.
Commission indicatorsA reporting framework to provide the Safety Rehabilitation and Compensation Commission (SRCC) with an overview of the performance of a jurisdiction. The SRCC indicators address prevention, claims management, return to work and scheme administration performance.
Compensable condition An injury or disease for which liability has been accepted under the SRC Act.
CIS—Customer information system Comcare’s CIS provides access to injury management and claims information for Australian and ACT Government employee claims, through a secure website.
DelegationThe written assignment of authority and responsibility to another person to carry out specific duties.
DeterminationA decision made by Comcare or the employer under specific sections of the SRC Act.
Determining authorityThe person who made the determination. This is Comcare or the licensee if the determination is about the workers’ compensation claim. The determining authority is the employer if the determination is about workplace rehabilitation.
Early interventionAssisting an employee as soon as possible after injury, even before a determination about liability for the injury.
EmployeeAn employee who has an accepted claim for compensation.
FOI ActFreedom of Information Act 1982
Graduated return to work (GRTW)When an employee returns to specified duties on reduced hours/duties, and increases those hours/duties gradually.
INAInitial needs assessment. An initial assessment, or rehabilitation assessment, examines the needs of an injured or ill worker and the workplace requirements to develop a rehabilitation plan. The assessment includes the services and treatments recommended to assist the worker to return to pre-injury duties.
IncapacityA diminished ability to earn. The SRC Act defines incapacity as ‘an incapacity to engage in any work or an incapacity to engage in employment at the same level’.
Injury managementA coordinated approach to managing the symptoms and impacts of an employee’s injury.

150
LQMPLegally qualified medical practitioner.
OHSOccupational health and safety.
Operational standardsThe Operational standards for rehabilitation program providers set out under section 34e of the SRC Act ensure that WRPs deliver high quality services that contribute to successful rehabilitation outcomes.
PremiumThe amount paid by an Australian or ACT Government employer for workers’ compensation costs for a given financial year.
Premium payerAustralian or ACT Government department that pays Comcare a premium to manage liability under the SRC Act.
ReconsiderationA review of a determination by Comcare or an employer.
Rehabilitation assessmentAn assessment under section 36 of the SRC Act of an employee’s capability of undertaking, or continuing to undertake, a rehabilitation program.
Rehabilitation authorityThe principal officer of the organisation employing the employee at the time of workplace rehabilitation. If an organisation is an exempt authority, Comcare is the rehabilitation authority.
RCM—Rehabilitation Case ManagerAn employee who coordinates and manages the rehabilitation of employees and in most situations has delegations under the SRC Act. An employee of the rehabilitation authority. In the Guidelines for Rehabilitation Authorities 2012 this role is referred to as a Case Manager.
Rehabilitation Guidelines/section 41 guidelinesGuidelines for Rehabilitation Authorities 2012 issued by Comcare to assist employers to meet their responsibilities under the SRC Act.
Rehabilitation management systemA documented statement of senior management’s commitment to providing employees with effective rehabilitation. It sets standards for the employer’s objectives and is used to establish strategic direction. The rehabilitation management system establishes systems which:
» recognise compliance obligations
» provide for effective rehabilitation arrangements
» promote continuous improvement
» promote communication of relevant information to employees
» provide for internal and external accountability
» put in place adequate control structures to manage risk.
Rehabilitation programProgram developed under section 37 of the SRC Act to support an employee to return to work. It is a structured series of activities and assistance to maintain or return an employee in suitable employment, and maintain or improve an employee’s activities of daily living. A rehabilitation program may include a return to work schedule.

151
Return to work hierarchyThe following descending order of goals for suitable employment of an employee:
(a) same duties and role in the same workplace
(b) modified duties and role in the same workplace
(c) different duties and role in the same workplace
(d) same duties and role in a different workplace
(e) modified duties and role in a different workplace
(f) different duties and role in a different workplace.
RTW—Return to Work policyReturn to work policy developed by the employer under section 41 of the SRC Act. The return to work policy may form part of the rehabilitation management system.
SRCC—Safety Rehabilitation and Compensation CommissionThe Safety, Rehabilitation and Compensation Commission is established under the Safety, Rehabilitation and Compensation Act 1988 (SRC Act). It is a statutory body that carries out regulatory functions in relation to Comcare and other authorities that determine workers’ compensation claims under the SRC Act.
Section 41 guidelines/Rehabilitation GuidelinesGuidelines for Rehabilitation Authorities 2012 issued by Comcare to assist employers to meet their responsibilities under the SRC Act.
SRC ActSafety, Rehabilitation and Compensation Act 1988
Suitable employmentThe definition of suitable employment varies depending on the employee’s circumstances and the nature of employment. Usually, suitable employment is employment within the organisation the employee works for. If the employee has left the organisation, then suitable employment is any employment.
Suitable dutiesSuitable duties are those appropriate to the employee’s capabilities, skills and experience, and take into consideration medical limitations and restrictions.
WHS ActWork Health and Safety Act 2011
Workplace rehabilitationA managed process involving early intervention with appropriate, adequate and timely services based on assessed needs which are aimed at maintaining or ill employees in, or returning them to, suitable employment.
WRP—Workplace rehabilitation providerA person or organisation providing rehabilitation services to help employees with work-related injuries or diseases to return to work. WRPs must be approved by Comcare in accordance with section 34 of the SRC Act. This includes in-house rehabilitation providers which the employer directly employs to provide rehabilitation services to employees. Rehabilitation Case Managers may use only rehabilitation providers approved by Comcare. The workplace rehabilitation provider was formerly known as an approved rehabilitation provider (ARP). These terms may be interchangeable.

152
PART 4
APPENDICES

153
Appendix 1Early intervention checklist for senior managersLeadership commitment1. Executive has endorsed an early intervention policy (consistent with the definition of
early intervention) which clearly defines early intervention objectives and the roles and expectations of each of the groups of stakeholders.
Yes
No
2. Other relevant policies that may help employees to remain at work or return to work after an absence have been reviewed for consistency with the early intervention policy.
Yes
No3. Early intervention and injury management are included as standing items on executive
meeting agendas.Yes
NoSystems review and improvement4. Systems for reporting and investigating incidents have been developed and
implemented to underpin early intervention.Yes
No5. Contracts with external providers (such as EAP, mediation, training and development,
workplace rehabilitation providers) are developed and reviewed to ensure consistency with the early intervention policy, and to meet the identified needs of the organisation.
Yes
No
6. Regular review of the resources, training and support for Rehabilitation Case Managers is undertaken with a view to continuous improvement of workplace rehabilitation outcomes.
Yes
No
7. Management systems for early intervention and return to work are assessed at defined intervals against the organisation’s stated objectives and available performance data, and opportunities for improvement are identified.
Yes
No
Accountability8. Systems are in place to ensure that managers are accountable for the preventing and
managing illness and injury in their workplaces (for example clear expectations are established though performance management frameworks, workplace agreements, or premium/cost devolution).
Yes
No
9. Rehabilitation Case Managers have regular performance review against injury management performance indicators and return to work outcomes.
Yes
No10. The organisation has clearly defined targets and positive performance indicators (both
lead and lag) for return to work that are regularly reported to executive meetings.Yes
No11. The organisation’s annual report includes performance against injury management
targets and/or key indicators of injury management performance.Yes
NoInformation and training
12. Information has been provided to employees about reporting and contact procedures and what assistance is available if they are off work, or experiencing health problems that prevent them from working at their normal functional level.
Yes
No
13. Line managers have been trained to recognise warning signs, support employees at risk of injury or illness, and manage an employee with illness or injury in the workplace.
Yes
No14. Information has been provided to employees to increase their awareness of mental
health issues and their understanding of behaviours that assist recovery in the workplace.Yes
No15. Rehabilitation providers have been given information about the agency’s early
intervention approach and the requirement for assessment to include identifying and addressing risks of long-term absence from work.
Yes
No
Incentives
16. Good performance in injury management is recognised and rewarded within the organisation.
Yes
No

154
Appendix 2Flags modelThere are several risk screening tools which can be used to identify indicators of poor rehabilitation outcomes. The flags model for injury management identifies indicators of poor outcomes or delayed recovery.
Flag OutcomesRed flags
Medical
Serious pathology/diagnosisCo-morbidity (co-existence of other diseases)Failure of treatment
Orange flags
Mental health
Mental health disorders, including anxiety and depressionPersonality disorders
Medication and alcohol misuse
Poor coping strategies
Yellow flags
Psychosocial
Beliefs about pain and injury (for example that there is a major underlying illness/disease, that avoidance of activity will help recovery, that there is a need for passive physical treatments rather than active self-management)Psychological distress (for example depression, anger, bereavement, frustration)Unhelpful coping strategies (for example fear of pain and aggravation, catastrophising, illness behaviour, overreaction to medical problems)Perceived inconsistencies and ambiguities in information about the injury and its implications
Failure to answer patients’ and families’ worries about the nature of the injury and its implications
Blue flags
Perceived features of work or the social environment
High demand/low controlUnsupportive management style
Perceived time pressure
Lack of job satisfaction
Work is physically uncomfortable
Black flags
Not matters of perception, affect all workers equally
Employer’s rehabilitation policy deters gradual reintegration or mobilityThreats to financial security
Qualification criteria for compensation (such as where inactivity is a qualification criterion)
Financial incentives
Lack of contact with the workplace
Duration of sickness absence

155
ReferencesPsychology, Personal Injury and Rehabilitation, A Report of a Working Party of the International Underwriting Association of London and the Association of British Insurers, 2004.
Guide to Assessing Psychosocial Yellow Flags in Acute Low Back Pain, Risk Factors for Long-Term Disability and Work Loss, Accident Compensation Commission, New Zealand, January 1997.
Additions based on Main, CJ, Sullivan, MJL and Watson, PJ 2008, Pain Management: practical applications of the biopsychosocial perspective in clinical and occupational settings, Churchill Livingstone, Edinburgh, New York.

156
Appendix 3
Case conferencesA case conference is a key activity that allows stakeholders to develop a shared plan to assist an employee to return to health and return to work. They provide an opportunity to discuss complex cases and cases where return to work has stalled or to be proactive in sharing information early in a claim to ensure all stakeholders are working towards the same goal. Case conferences bring multiple stakeholders together and may include:
» the employee
» Rehabilitation Case Manager (RCM)
» supervisor
» treating practitioners (GP, psychologist, physiotherapist)
» workplace rehabilitation provider (WRP)
» Claims Manager
» Comcare injury management advisor.
Case conferences vary depending on the required outcome but may be one of the following—follow the links below to find out more.
» Comcare case conference—meeting between Comcare and an employer to discuss liability and/or rehabilitation matters in relation to a particular claim or collection of claims.
» Return to work case conference—connecting the GP, the employer, the employee, other treatment providers and the insurer to support return to work.
Comcare case conferenceA Comcare case conference is a meeting between Comcare and an employer to discuss liability and/or rehabilitation matters in relation to a particular claim, or several claims. The purpose of this type of case conference is either to:
» develop an agreed plan for the management of the claim
» develop an agreed plan to progress and ensure safe and successful recovery at and return to work
» provide mentoring/support from rehabilitation subject matter experts
» ensure both Comcare and the employer are meeting their responsibilities under the Safety, Rehabilitation and Compensation Act 1988 (SRC Act).
Case conferences can be used to:
» identify or clarify issues about the claim
» review activities including progress towards and barriers against rehabilitation goals
» clarify roles and responsibilities
» resolve conflicts and/or discuss possible actions to achieve outcomes
» adjust current rehabilitation programs
» allow all relevant stakeholders to exchange views in a constructive manner.
A case conference may be requested with Comcare when the Rehabilitation Authority would like to discuss liability issues with the Claims Manager or if the RCM would like support and assistance from an injury management adviser in identifying appropriate return to work strategies.

157
To request an individual case conference, please visit the case conference request form page on our website.
To request a multiple claim case conference, please visit the multiple claim case conference request form page on the Comcare website.
There may be a number of indicators to identify cases that would benefit from being included in a case conference. Some examples could include:
» an employee’s return to work is not progressing as expected
» an employee has been working the same reduced hours for an extended period of time—for example, two months or longer
» an employee has been off work for a prolonged period
» an employee has not returned to work since the date of injury
» you are having difficulties contacting the employee and the treating medical practitioner won’t communicate with you
» multiple rehabilitation programs have been tried with little success
» you cannot continue to offer suitable duties unless the employee is able to increase work capacity.
Case conferences can be held at routine intervals or when particular issues arise. Case conferences may be held face-to-face, by phone, videoconference or a combination of these.
What information is required when requesting a case conference with Comcare?
When requesting a case conference Comcare needs specific information to enable the Claims Manager to prepare and invite other attendees, such as the injury management adviser (IMA) or team leader. Providing Comcare with thorough information improves the case conference outcome.
Required information includes:
» employee details such as Comcare claim number (if known), full name, date of birth, date of injury, history of other injuries/claims and relevant vocational information (length of service, position or level held, specialist vocational skills)
» case conference requester’s name and details
» agency details and whether the agency is the rehabilitation authority for the claim—if not, provide rehabilitation authority details
» reason/s for the request, such as barriers to rehabilitation identified, stalled or delayed recovery and rehabilitation, multiple conditions, previous attempts at rehabilitation have had little success
» WRP details, if a WRP has been engaged, and for what purpose
» when the goals of the rehabilitation program were last reviewed
» whether a Comcare IMA has been contacted previously about the case and, if so, did the IMA provide recommendations and have these been addressed—if not please explain why these recommendations were not achieved.

158
Who can request a case conference?Case conferences can be initiated either by you, by the employee or by the Claims Manager. An employee can nominate an advocate or treating practitioner to attend, for example, a union representative, legal representative or treating practitioner.
Attendees at a case conferenceThe table below outlines the roles of potential attendees at a case conference.
Attendee When to attend Role
Rehabilitation Case Manager
Required at all case conferences
To provide information about the case management aspect of the claim from the employer’s perspective and raise issues that need to be resolved.
Employee Required at all case conferences except when indicated otherwise
To engage and empower the employee.
Employee’s representative
When the employee requests a representative
As support for, and to provide the perspective of, the employee.
Workplace rehabilitation provider (WRP)
Complex or sensitive cases To provide information about an employee’s return to work and any potential or actual barriers to return to work.
Employee’s supervisor
Complex or sensitive cases To assist in identifying suitable duties or raise particular concerns. Increase the supervisor’s knowledge of the return to work model and how to support the employee.
HR Manager Complex or sensitive cases May attend if the claim is complex or sensitive, for example, if there are disciplinary or performance issues.
Treating medical practitioner (LQMP)
Complex or sensitive cases To provide treatment options to facilitate a positive outcome, outline medical restrictions and provide the treating medical practitioner with greater understanding of the workplace.
Comcare injury management adviser
Complex or sensitive cases To provide detailed information about the claim and relevant policy or legislative advice.
Other stakeholders the Rehabilitation Case Manager invites
When the Rehabilitation Case Manager requests their inclusion
To provide additional information that may be relevant.
Claims Manager (CM)
As required To provide detailed information about the claim and relevant policy or legislative advice.

159
Return to work case conferencingReturning to work following an injury or disease or staying in work whilst managing injury or disease is an important part of rehabilitation and recovery. Participation in the workplace can have a significant impact on an employee’s emotional, social and physical wellbeing.
Return to work (RTW) case conferencing connects the medical practitioner, employer, employee, other treatment providers and insurer at the right time to best support return to work outcomes.
RTW case conferencing provides the opportunity to:
» discuss the requirements for RTW
» consider the employee’s capacity for work
» discuss what supports may be required to support the employee to RTW—for example, flexible work arrangements, workplace adjustments, alternative duties, equipment supports
» agree on actions that focus on and support the employee’s RTW.
The RTW case conference model was developed in consultation with medical practitioners, employers, consumers, insurers and workplace rehabilitation providers (WRPs). The model provides a consistent approach on how to organise and undertake a case conference.
An effective RTW case conference:
» requires preparation to ensure there is a clear purpose, plan and expectations
» involves those that can contribute to the employee’s recovery at and return to work
» ensures the employee feels respected, trusted and listened to.
RTW case conferencing resources are available for all stakeholders to support positive employee return to work outcomes. The resources available include:
» Return to work case conferencing (model)
» When is return to work case conferencing most useful? (a guide)
» Return to work case conferencing checklist for RCM and WRP
» Return to work case conferencing for RCM and WRP (flowchart)
» Return to work case conference roles and responsibilities (for all involved parties)
» Return to work case conference plan (a template)
» Return to work case conference—FAQs for employees
» Billing for GP involvement in RTW case conferencing.
See the Comcare website for further details.

160
Appendix 4
Building rehabilitation case manager capabilityComcare has developed capability products for the roles of RCMs, Supervisors and Claims Managers. The products define a set of core capabilities for each of the three roles and will assist in maintaining a skilled injury management workforce.
The purpose of the capability products is to:
» create a scheme standard to inform capability requirements
» support recruitment of appropriately skilled and experienced people to these roles
» maximise the opportunity for the best possible outcomes for employees
» provide a framework to assess related training needs
» provide guidance to individuals on the capabilities they need to attain and maintain in their respective roles.
The capability products consist of:
» Rehabilitation Case Manager Core Capabilities [PDF]
» Supervisor—Supporting Return to Work—Core Capabilities [PDF]
» Claims Manager Core Capabilities [PDF]
For more information go to www.comcare.gov.au/recovery/rehabilitation/capability_products.

161
Appendix 5: Samples responses for section 37(3) a–hSample responses for section 37(3) criteria and important considerations for the RCM.
Section 37(3) a–h, SRC Act, Provision of rehabilitation programs guideline and example responses
(a) any written assessment given under subsection 36(8)
Consider:
» current medical certificates
» dated current medical reports
» dated and any other rehabilitation or specialist assessments for example Initial Needs Assessment reports, section 36 assessments
» any additional comments (if there are conflicting medical opinions).
Example statement section 37(3) (a)
1. Mr/Ms Employee has been assessed under subsection 36(8) by Dr X from Y. The agency sought assistance in determining Mr/Ms Employee’s capacity to return to work after a lengthy period of incapacity and reported frustration from the treating doctor.
2. As a result of the medical assessment, Dr X has cleared Mr/Ms Employee to return to work for XX hours a week and provided guidance for work duties. This information concurred, and it was determined, after consultation between Dr X and the treating GP, who are reported by Dr X to have reached agreement of the return to work hours and medical restrictions.
3. No written assessments have been undertaken. Mr/Ms Employee’s treating GP is encouraging him/her to participate in a return to work program and the only restriction imposed is that they not return to a [HR role] in [name of organisation] as his/her supervisor is the cause of his/her distress.
4. Mr/Ms Employee has been cleared to return to work at XX hours a day for a period of (timeframe) days/weeks. These hours will increase to full time over a period of (timeframe) days/weeks.
5. Mr/Ms Employee is willing to participate in the process and has indicated his/her willingness to return to work. They have requested assistance with the identification of a work trial and assistance with job seeking.
6. With assistance from the rehabilitation provider, Mr/Ms Employee is expected to make a successful return to work.
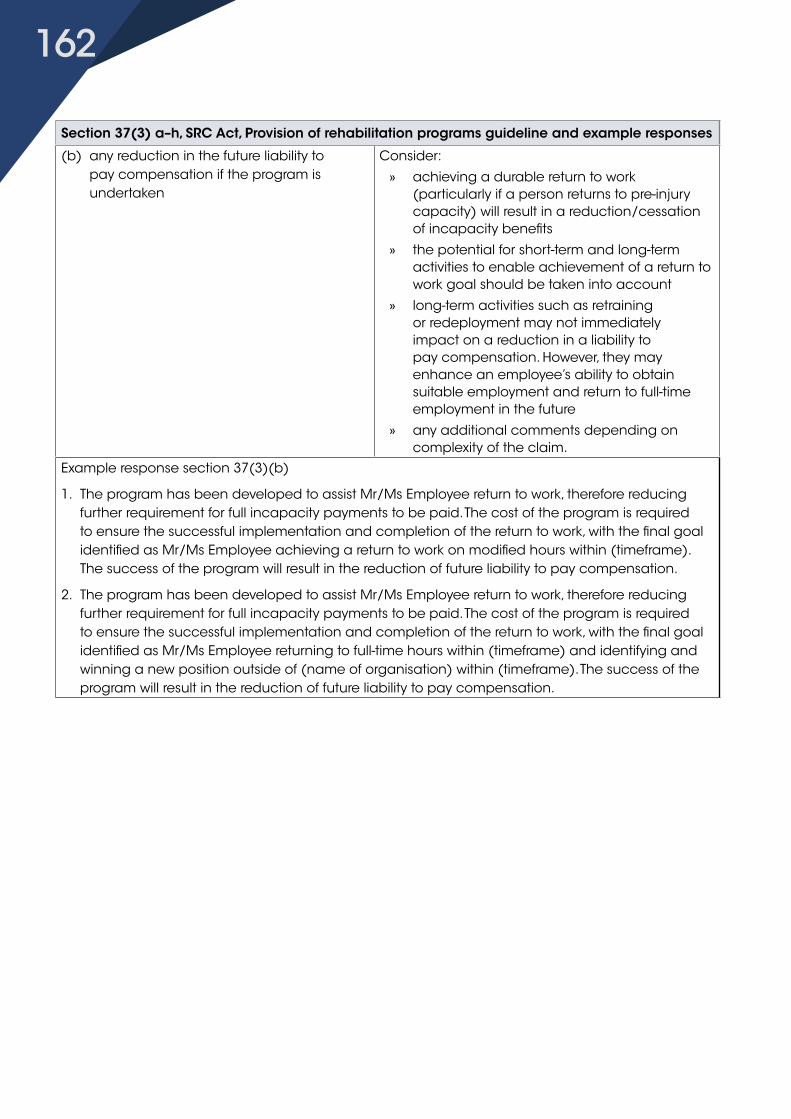
162
Section 37(3) a–h, SRC Act, Provision of rehabilitation programs guideline and example responses
(b) any reduction in the future liability to pay compensation if the program is undertaken
Consider:
» achieving a durable return to work (particularly if a person returns to pre-injury capacity) will result in a reduction/cessation of incapacity benefits
» the potential for short-term and long-term activities to enable achievement of a return to work goal should be taken into account
» long-term activities such as retraining or redeployment may not immediately impact on a reduction in a liability to pay compensation. However, they may enhance an employee’s ability to obtain suitable employment and return to full-time employment in the future
» any additional comments depending on complexity of the claim.
Example response section 37(3)(b)
1. The program has been developed to assist Mr/Ms Employee return to work, therefore reducing further requirement for full incapacity payments to be paid. The cost of the program is required to ensure the successful implementation and completion of the return to work, with the final goal identified as Mr/Ms Employee achieving a return to work on modified hours within (timeframe). The success of the program will result in the reduction of future liability to pay compensation.
2. The program has been developed to assist Mr/Ms Employee return to work, therefore reducing further requirement for full incapacity payments to be paid. The cost of the program is required to ensure the successful implementation and completion of the return to work, with the final goal identified as Mr/Ms Employee returning to full-time hours within (timeframe) and identifying and winning a new position outside of (name of organisation) within (timeframe). The success of the program will result in the reduction of future liability to pay compensation.

163
Section 37(3) a–h, SRC Act, Provision of rehabilitation programs guideline and example responses
(c) the cost of the program Consider:
» The rehabilitation authority, usually the RCM, needs to take into account the goal of the rehabilitation program and the nature of the proposed rehabilitation services, and the cost of the services to ensure that the overall cost of the program is reasonable and within industry standards.
» The Operational standards for rehabilitation program providers (workplace rehabilitation providers) should also be considered. These are designed to ensure that high quality and cost-effective services are delivered which contribute to successful return to work outcomes.
The operational standards prescribe target outcome measures for the provider entity as a whole, and include measures for return to work rate, cost of rehabilitation programs and return to work durability. However, costs and services of individual rehabilitation programs will depend on the case complexity and the nature of the vocational rehabilitation services provided in each instance.
Example response section 37(3)(c)
Provide justification of all rehabilitation costs including additional costs such as travel, vocational training, return to work aids and workplace assessments.

164
Section 37(3) a–h, SRC Act, Provision of rehabilitation programs guideline and example responses
(d) any improvement in the employee’s opportunity to be employed after completing the program
Consider:
» The successful completion of a rehabilitation program should result in a person having an enhanced capacity to obtain or to retain paid employment (within the definition of suitable employment). The RCM may need to consider both short and long term goals, such as helping with alternative duties or work trials to allow the employee to upgrade physical or psychological work capacity.
» If an employee cannot return to, or remain with, the pre-injury employer, a rehabilitation program with a goal of redeployment may be required. However, all options within the hierarchy of return to work must be first considered:
a) same job, same employer
b) similar job, same employer
c) new job, same employer
d) same job, new employer
e) similar job, new employer
f) new job, new employer.
» Any recommendations made in a vocational assessment to increase a person’s employment opportunities should be considered for inclusion in the rehabilitation program, such as:
» consolidation of transferable skills
» benefit of providing training
» work trial options
» information on the labour market (if relevant).

165
Section 37(3) a–h, SRC Act, Provision of rehabilitation programs guideline and example responses
Example response section 37(3)(d)
1. It is anticipated that two return to work plans will be required to help Mr/Ms Employee return to his/her full time capacity. During this time, Mr/Ms Employee has been provided with the opportunity to develop and consolidate a range of skills they have not had high-level exposure to. These include [duties] and stakeholder liaison, all of which had been identified to the supervisor as areas in which new skills would be appreciated. The return to work program, in conjunction with the suitable duties schedule, provide Mr/Ms Employee with an opportunity to enhance skills with the likely outcome being more able to access employment opportunities in the public and private sectors.
2. The employee has a wide range of skills appropriate to his/her profession as a [name of role]. They have, however, lost confidence in their skills and themselves. The work trial will enable him/her to up-skill and regain confidence. It will also provide him/her with an opportunity to network. A work trial has been identified with [name of organisation] and the duties involve mainly [type of work] which is most appropriate and should not cause Mr/Ms Employee any additional stress. Mr/Ms Employee’s chances of gaining employment will be enhanced by his/her participation in the program.
(e) the likely psychological effect on the employee of not providing the program
Consider:
» the person’s current psychological state and medical recommendations
» motivation and attitude
» potential for worsening of symptoms if a program is not provided
» support mechanisms that may need to be put in place to assist the person with return to work
» preventive measures to reduce the potential risk of a new incident or worsening of symptoms occurring as a result of the return to work.
Example response section 37(3)(e)
1. The program has been developed after unsuccessful attempts at structured return to work programs in the past. In light of the limited successes to date, Mr/Ms Employee’s psychological state has had a negative impact. This has resulted in not only a lengthy period of incapacity, but also reported conflict within the workplace and increased physical symptoms. If the proposed return to work program is not provided, it is expected that Mr/Ms Employee will remain totally incapacitated and require increasing amounts of treatment to manage his/her condition.
2. During the initial needs assessment meeting, Mr/Mrs Employee expressed eagerness to return to work and participate in a rehabilitation program. They require assistance because they have lost confidence. Therefore the psychological impact of his/her not participating in a program is very high.

166
Section 37(3) a–h, SRC Act, Provision of rehabilitation programs guideline and example responses
(f) the employee’s attitude to the program The RCM should seek to ascertain the employee’s attitude to the proposed rehabilitation program and consider the reasons given by the employee, with appropriate weight being given to the issues raised.
The following issues should be considered:
» The employee’s level of support for the program. The rehabilitation authority should consider supporting a program where the employee is asking for assistance from the RCM or rehabilitation provider in order to remain at or return to work.
» The appropriateness of the rehabilitation goal.
» The appropriateness of the actions included in the rehabilitation program.
» Any alternative proposals offered.
» Whether the employee is ‘unwilling’ to comply with the proposed rehabilitation program and the reasons for this, or if they is considered to be ‘medically unable’ to undertake the rehabilitation program.
» The employee does not need to display a positive attitude towards a rehabilitation program, as the Court stated in McGuinness v Comcare Australia: ‘if the employee’s attitude to the program was negative, it does not mean that the program therefore fails, but simply that the attitude is taken into account and appropriate weight given to the attitude’.
» The employee’s understanding of the rehabilitation goal and services. The employee may have an unrealistic expectation of rehabilitation services finding him/her another job in another agency, or support to undertake retraining in order to further a career. For example, this is not deemed to be the appropriate rehabilitation goal, or in line with the return to work hierarchy.

167
Section 37(3) a–h, SRC Act, Provision of rehabilitation programs guideline and example responses
Example response section 37(3)(f)
Mr/Ms Employee reports a desire to return to work within a supportive work environment and as such, has demonstrated a positive attitude to the attempts made to date. Before signing the rehabilitation program, Mr/Ms Employee was requested to take the plan home, review it and provide feedback on both the positive and negative aspects of the plan in writing to the RCM.
You should consider the following in your response:
Make note of the employee’s attitude and give appropriate consideration to issues raised, for example, training requests, new employer.
Document the employee’s attitude, particularly if negative. Ensure that you give consideration to the issues. Formulate your response to the situation.(g) the relative merits of any alternative and
appropriate rehabilitation programConsider if the rehabilitation program and the actions included in the rehabilitation program are consistent with the most appropriate rehabilitation goal. The hierarchy of return to work should be followed when considering any alternative rehabilitation program:
a) same employer, same duties
b) same employer, modified duties
c) same employer, new duties
d) different employer, same duties
e) different employer, modified duties
f) different employer, new duties.Example response section 37(3)(g)
1. Previous attempts at returning to work have been unsuccessful, and as such, a highly supported rehabilitation program, with clear expectations for all stakeholders, has been developed to ensure success and durability of the return to work. The level of support provided and level of clearly outlined expectations were guided by the independent medical assessment organised by the [name of organisation] to ensure adherence to medical restrictions and all psychosocial factors have been taken into account when developing the program.
2. I have considered the merits of alternative programs. However, this program best meets the employee’s current capacity to undertake a rehabilitation program.

168
Section 37(3) a–h, SRC Act, Provision of rehabilitation programs guideline and example responses
(h) any other relevant matter This requires the rehabilitation authority to consider the individual circumstances of each case.
Consider:» medical support for the program (particularly
if this is conflicting)
» the requirement for the relevant authority to provide suitable employment or to take all reasonable steps to help the employee find suitable employment (section 40(1), SRC Act)
» the definition of suitable employment (section 4, SRC Act) dictates whether suitable employment is considered to be employment by the Commonwealth, or licensee, external employment or self-employment—for a permanent employee who continues to be employed, consideration must be given to the employee’s age, experience, training, language and other skills, the employee’s suitability for rehabilitation or retraining, the location of the employment (and whether the employee may reasonably be required to change his/her place of residence), and other relevant matters
» non-compensable conditions
» family or other psychosocial issues
» workplace issues such as workplace investigations, grievance procedures, conflict.
Example response section 37(3)(h)
1. Mr/Ms Employee’s rehabilitation program has been developed with careful consideration of all medical information available, history of his/her return to work efforts to date, and liaison with stakeholders. The program has tried to address previous concerns in relation to unclear expectations and, together with the return to work schedule attached, provides a clear, succinct guideline for all stakeholders to follow.
2. I am not aware of any other relevant matters in consultation with all stakeholders, including Dr X, etc.
PUB 043 July 2017

169

















