MICHAEL M. REINOLD; GLENN S. FLEISIG, PhD; and JAMES R. ANDREWS, MD American Sports Medicine Institute KEVIN E. WILK, PT HealthSouth Corporation GENE G. JAMESON, MS Tri-County Technical College Throwing is a complicated interaction of many muscles in the body. These muscles must generate forces to accelerate the ball, as well as control motion so as to not injure the body. Contributing muscles can be found throughout the entire nt durinq t m-r* .-+I.- the arm is f shoulder e the elbow ( . . ilizinq stru ully totked xternal roti - body and are coordi- nated in a kinetic chain from the foot of turps. the stride limb to the hand of the throwing arm. Neuromuscular timing of contractions between the muscula- maximal ture of specific links, l with ition. both concentrically The biomethan~cs oi should be tonsidere and eccentrically, is e is develo~ina a rehabilitation Droaram. necessary to provide ind and par ,,, L" :, Key Wc . . F throwing d when on1 . . the most efficient tial-effort .,,,,,c,l ;. throw possible. This LIIIUWIII~ tall UY IIItuIpuIawu 11lt0 Sequence of motions b rehabilitt transfers force from without r the lower extremities on the ell and trunk to the throwing arm through I rd the shoulder and el- b trdlninq, interval tnrowing program bow. The shoulder ""I.. Is: UIL, spo a , rk on form ressive tor( and elbow joints must not only contribute to the force to control and accelerate the ball but also withstand the forces after it is released. Forces and torques gener- ated in the upper extremity often reach levels that compromise the integrity of the stabiliz- ing structures. With repetitive exposure to these high-level torques, fatigue and eventual failure are imminent as a result of cumulative microtrauma to the tissue. The purpose of this article is to provide athletic trainers and therapists with knowledge of how injuries occur to the elbow during throwing and the clinical rationale for choos- ing sport-specific techniques during rehabili- tation. An understanding of proper throwing mechanics and the demands placed on the elbow during the throwing motion can help in the prevention and rehabilitation of elbow in- juries. Biomechanics of the Overhead Throw Fleisig, Escamilla, et al. (1 995) and Werner, Fleisig, Dillman, and Andrews (1993) charac- terize the biomechanics of throwing into six phases: wind-up, stride, arm cocking, arm acceleration, arm deceleration, and follow- through (Figure 1). The wind-up allows the ath- lete to assume a good starting position so that momentum can be generated to help acceler- ate the ball, and it creates little kinematic and kinetic activity in the elbow. During the stride, the athlete extends forward and might reach up to 85" of elbow flexion by the time of foot contact (Fleisig, Andrews, et al., 1995). The arm-cocking phase involves the athlete maxi- 12 I MAY 2 0 0 0 ZOO0 Human Kinetics. ATT S(3). pp. 12-18 ATHLETIC THERAPY TODAY
Transcript
MICHAEL M. REINOLD; GLENN S. FLEISIG, PhD; and JAMES R. ANDREWS, MD American Sports Medicine Institute KEVIN E. WILK, PT HealthSouth Corporation GENE G. JAMESON, MS Tri-County Technical College
Throwing is a complicated interaction of many muscles in the body. These muscles must generate forces to accelerate the ball, as well as control motion so as to not injure the
body. Contributing muscles can be found throughout the entire
n t durinq t m - r * .-+I.-
the arm is f shoulder e
the elbow ( . .
ilizinq stru
ully totked xternal roti
- body and are coordi- nated in a kinetic chain from the foot of
turps. the stride limb to the hand of the throwing arm. Neuromuscular timing of contractions between the muscula-
maximal ture of specific links, l with ition.
both concentrically The biomethan~cs oi should be tonsidere and eccentrically, is
e is develo~ina a rehabilitation Droaram. necessary to provide
ind and par ,,, L" :,,,
Key Wc . .
F throwing d when on1 . .
the most efficient
tial-effort .,,,,,c,l ;.
throw possible. This
LIIIUWIII~ ta l l UY IIItuIpuIawu 11lt0 Sequence of motions
b rehabilitt transfers force from without r the lower extremities on the ell and t runk to t he
throwing arm through I rd the shoulder and el- b trdlninq, interval tnrowing program bow. The shoulder
""I..
Is: UIL, spo a ,
rk on form ressive tor(
and elbow joints must not only contribute to the force to control and accelerate the ball but also withstand the forces after it is released. Forces and torques gener- ated in the upper extremity often reach levels
that compromise the integrity of the stabiliz- ing structures. With repetitive exposure to these high-level torques, fatigue and eventual failure are imminent as a result of cumulative microtrauma to the tissue.
The purpose of this article is to provide athletic trainers and therapists with knowledge of how injuries occur to the elbow during throwing and the clinical rationale for choos- ing sport-specific techniques during rehabili- tation. An understanding of proper throwing mechanics and the demands placed on the elbow during the throwing motion can help in the prevention and rehabilitation of elbow in- juries.
Biomechanics of the Overhead Throw
Fleisig, Escamilla, et al. (1 995) and Werner, Fleisig, Dillman, and Andrews (1 993) charac- terize the biomechanics of throwing into six phases: wind-up, stride, arm cocking, arm acceleration, arm deceleration, and follow- through (Figure 1). The wind-up allows the ath- lete to assume a good starting position so that momentum can be generated to help acceler- ate the ball, and it creates little kinematic and kinetic activity in the elbow. During the stride, the athlete extends forward and might reach up to 85" of elbow flexion by the time of foot contact (Fleisig, Andrews, et al., 1995). The arm-cocking phase involves the athlete maxi-
1 2 I MAY 2 0 0 0
ZOO0 Human Kinetics. ATT S(3). pp. 12-18
ATHLETIC THERAPY TODAY
Foot contact ER, Release IR,
mally externally rotating the arm, requiring a varus torque to counteract valgus extension at the elbow. This varus torque is provided mainly from the ulnar collateral ligament (UCL), with help from the wrist flexor-pronator group, as well as the anconeus and triceps muscles.
The critical instant during the throw at which the most stress is placed on the elbow occurs near the end of the arm-cocking phase (Figure 2). Kinematic data (describing the motion, i.e., joint displacement, velocity, and acceleration) of baseball pitchers reveal that at this instant, the arm is in approximately 165" of external rotation, 94" of horizontal adduction, and 95" of elbow flexion (Fleisig, Andrews, et al., 1995). Kinetics (what causes the motion, i.e., joint forces and torques) produced at this instant are 64 N . m of varus torque, 16 N . m of flexion torque, 300 N of medial force, 160 N of anterior force, and 270 N of proximal force (Table 1 ; Fleisig, Andrews, et al.). These forces place a great deal of stress on the elbow and increase the chance of injury to the stabilizing structures, in particular the UCL. Biomechanical analysis of foot- ball players has yielded similar data on this critical instant, most notably 1 1 3 O of elbow flexion, 280 N of medial force, and 54 N . m of varus torque (Fleisig, Escamilla, et al., 1995).
Figure 2 Maximum external rotation near the end of the arm-cocking phase. Modified with permission from G.S. Fleisig et al., Kinetics of baseball pitching with implications about injury mechanisms, American Journal of Sports Medicine, 1995, 23, 233-239.
ATHLETIC THERAPY TODAY MAY 2000 1 13
I . - . .. . , -: . . s . ! ' Baseball pirihing I
-- I
Fleisiq. ,\ndrcn,s. [.)illman, h fscatnilla. IQQ.', 6.1, 73 I I
1 Fleistg er ;tI., IO97n - 54 2 Q ! ! j f~lt:tsig, l :sc- i i~~~i l l ;~. e~ ;+I,. ! ~5 .- 5 I 28
nutz, & ti
al., 1994
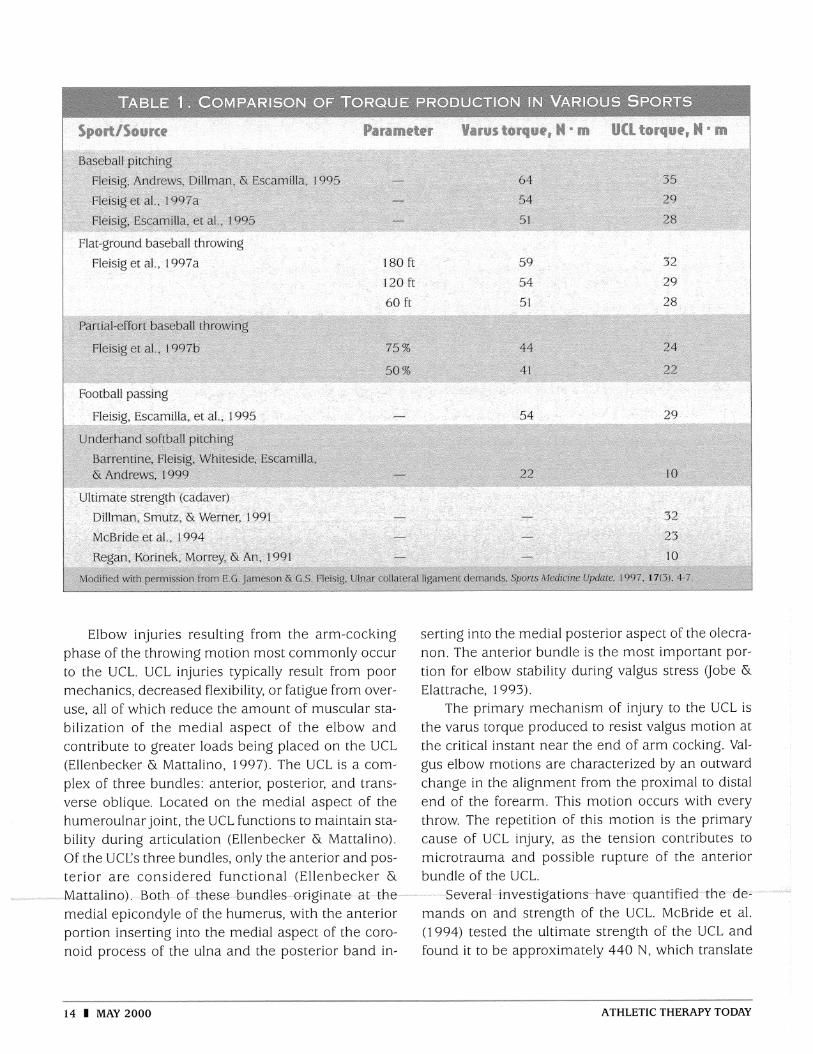
Elbow injuries resulting from the arm-cocking phase of the throwing motion most commonly occur to the UCL. UCL injuries typically result from poor mechanics, decreased flexibility, or fatigue from over- use, all of which reduce the amount of muscular sta- bilization of the medial aspect of the elbow and contribute to greater loads being placed on the UCL (Ellenbecker & Mattalino, 1997). The UCL is a com- plex of three bundles: anterior, posterior, and trans- verse oblique. Located on the medial aspect of the humeroulnar joint, the UCL functions to maintain sta- bility during articulation (Ellenbecker & Mattalino). Of the UCL's three bundles, only the anterior and pos- terior are considered functional (Ellenbecker & Mattalino), Both of these- bundles origi-nate- a& the- -
medial epicondyle of the humerus, with the anterior portion inserting into the medial aspect of the coro- noid process of the ulna and the posterior band in-
serting into the medial posterior aspect of the olecra- non. The anterior bundle is the most important por- tion for elbow stability during valgus stress Uobe & Elattrache, 1 993).
The primary mechanism of injury to the UCL is the varus torque produced to resist valgus motion at the critical instant near the end of arm cocking. Val- gus elbow motions are characterized by an outward change in the alignment from the proximal to distal end of the forearm. This motion occurs with every throw. The repetition of this motion is the primary cause of UCL injury, as the tension contributes to microtrauma and possible rupture of the anterior bundle of the UCL.
Several-investigations have quantified the des mands on and strength of the UCL. McBride et al. (1994) tested the ultimate strength of the UCL and found it to be approximately 440 N , which translate
14 1 MAY 2000 ATHLETIC THERAPY TODAY
to 23 N . m of varus torque during valgus motion (using 0.05 m as the moment arm length). Dillman, Smutz, and Werner (1991) performed a similar test and calculated the mean ultimate ligament strength as 642 N , corresponding to 32 N . m of varus torque. Yet another study reported the failure load of the UCL to be 260 N , translating to 10 N . m of varus torque (Regan, Korinek, Morrey, & An, 1991). The results of these studies varied because of methodological dif- ferences and cadaveric properties; however, they give a basis for comparison when estimating UCL loads during sport activities.
In order to understand the demands placed di- rectly on the UCL, sports medicine professionals must first understand how much varus torque is supplied by the UCL. Morrey and An (1 983), in an attempt to answer this question, performed an in vitro study on four cadaveric elbows. They estimated that the UCL contributed approximately 54 % of the total varus torque when the elbow was flexed at 90". With this information, and the results of subsequent research on athletic activities, the demands on the UCL during various sports can be estimated.
Several investigators have estimated the internal forces and torques during baseball pitching and re- port maximum varus torques ranging from 64 to 120 N . m (Feltner & Dapena, 1986; Fleisig, Andrews, et al., 1995; Werner, Fleisig, Dillman, & Andrews, 1993). For example, Fleisig, Andrews, et al. estimated the maximum varus torque to be 64 N . m among a sample of healthy professional baseball pitchers. This is at the moment when the shoulder is externally ro- tated at 165" and the elbow flexed at 85-90", the critical instant near the end of arm cocking. Using 54% as the UCCs contribution to total varus torque, the estimated torque produced by the UCL is 35 N .
m. This figure corresponds to a linear load of 692 N , surpassing all the failure-producing loads reported earlier. The failure loads reported in cadaveric stud- ies are subject to error, based on the age of the ca- davers used and the model employed to calculate the contribution percentage of the UCL, because these studies often neglect the contributions of muscles to total torque. However, Fleisig, Andrews, et al.'s results indicate that an athlete places excessive stress on the UCL with every pitch, possibly approaching the ulti- mate strength of the ligament.
Although they do not suffer overuse injuries as often as baseball pitchers do, football quarterbacks are another group of athletes who subject themselves to the stresses of overhand throwing. A common as- sumption is that because a football is more massive than a baseball, higher valgus stress must be resisted, resulting in higher varus torques. This, however, is not the case. A comparison of high school and col- lege quarterbacks and pitchers determined that maxi- mum elbow varus torques were not significantly different-54 N . m for passing and 51 N . m for pitching (Fleisig, Escamilla, et al., 1995). This implies that similar demands (29 N . m) are placed on the UCL during passing a football and pitching a base- ball, even though the football is three times the weight of a baseball. This is because there is less arm accel- eration when passing a football.
Also subject to injury during the arm-cocking phase is the flexor-pronator muscle group, as con- tractile forces develop muscle tension to help resist valgus stress (Pandya, Gillogly, & Andrews, 1998). The muscular activity of the flexor-pronator group provides dynamic stabilization of the medial elbow, along with the static restraint of the UCL. Because of this, the flexor muscle origin on the medial humeral epicondyle is a common site of muscle strain and inflammation.
Ulnar neuritis is another condition of the medial elbow that results from stresses during the arm- cocking phase. Although far less common than UCL injuries, ulnar neuritis can result from compression of the ulnar nerve in the cubital tunnel during elbow flexion (Pandya et al., 1998). Trauma from friction on a hypermobile ulnar nerve, as well as entrapment between the heads of the flexor carpi ulnaris, can fur- ther complicate the neuritis in throwing athletes (Pandya et al.).
Varus torque to resist valgus motion is produced by tension in the medial elbow compartment, as well as compression in the lateral elbow compartment. Lateral compression occurs between the radial head and the humeral capitellum and can result in avascu- lar necrosis, osteochondritis dissecans, or osteochon- dral chip fractures (Atwater, 1979). Although microtrauma to the UCL generally occurs before lat- eral compression injuries Uobe & Elattrache, 1993), as the UCL becomes damaged the amount of varus torque that it is capable of generating diminishes,
ATHLETIC THERAPY TODAY MAY 2000 1 15
causing increased compression on the lateral surface of the capsule (Ellenbecker & Mattalino, 1997). Lat- eral compression injuries occur most often during late arm cocking, when the arm approaches maximum external rotation.
The time from maximum external rotation to ball release is defined as the arm-acceleration phase. Dur- ing this phase the elbow extends at speeds near 2,000" Is, largely because of centrifugal force (Fleisig, Andrews, et al., 1995). Wilson (1 983) reported inju- ries to the posterior aspect of the elbow. The combi- nation of excessive valgus stress and rapid elbow extension during arm acceleration causes the olecra- non to impinge on the olecranon fossa. This valgus extension overload could lead to chondromalacia or osteophyte formation at the posteromedial olecranon tip (Wilson). Subsequently, these osteophytes might fracture and become loose bodies in the posterior aspect of the elbow (Pandya et al., 1998).
Arm deceleration begins just after ball release. A flexion torque generated by the elbow flexor muscles, particularly eccentric biceps activity, decelerates the elbow. Muscular activity of the triceps, anconeus, and wrist flexor muscles aid the UCL in stabilizing the el- bow joint through a proximal force near 90 % of body weight (Fleisig, Andrews, et al., 1995). The repetitive forceful elbow-extension motion and chronic overuse associated with overhead throwing also place strain on the triceps insertion at the olecranon, which can result in triceps tendinitis and possibly olecranon stress and avulsion fractures (Pandya et al., 1998).
The follow-through phase begins with maximum internal rotation of the arm and serves to dissipate energy away from the elbow through the body's ki- netic chain. The low kinematic and kinetic activity seen at the elbow during the follow-through phase has not been reported to commonly result in throw- ing injuries.
Most research has been dedicated to the analysis of the throwing motions in baseball and football; ten- nis serves, volleyball serves and spikes, and javelin overhead throws are activities in which internal forces and torques have not been estimated. The unique charaeteristjes-of-*each-sport-produce- slightly-ddffer- ent movement patterns and thus different kinematic and kinetic data. However, significant amounts of force and torque are assumed to be generated in or- der to produce and control these overhead motion
activities, potentially exposing all overhead athletes to similar injury mechanisms.
Barrentine, Fleisig, Whiteside, Escamilla, & Andrews (1 998) have analyzed the biomechanics of underhand throwing during softball pitching, estimating the amount of force experienced at the elbow. During the acceleration phase, before ball release, a proximal force equivalent to 438 N is exerted to resist distrac- tion of the forearm at the elbow. Distraction is caused by the centrifugal force on the forearm resulting from the upper arm rotating about the shoulder at 650°1s and the elbow flexing at 870'1s. A valgus torque equal to 45 N . m is generated at the elbow to resist varus stressed caused by the combination of flexion at the elbow and internal rotation at the shoulder.
Softball pitching is yet another activity in which varus torque is produced to counteract valgus motion (Barrentine et al., 1998). In softball pitching, maxi- mum varus torque is generated after release, during the deceleration phase. Varus torques are estimated to be 22 N . m at 60" flexion, considerably less than in baseball pitching. Thus, the softball pitch places less stress on the UCL than does a baseball pitch or football pass. However, Barrentine (1 999) and Barrentine et al. have noted that when normalized (percent body weight X height), the forces and torques exerted during underhand throwing are comparable to those experienced during overhead throwing. This appears to be influenced by gender, ball size and weight, and mound height (Barrentine).
Although UCL injuries in softball throwing are not common, ulnar neuritis has been reported when the medial elbow comes into contact with the hip just before ball release, and it is attributed to poor biome- chanics (Barrentine et al., 1998). After ball release, a proximal force equal to 338 N is exerted to resist distraction of the forearm at the elbow during the follow-through phase.
letes, whether conservative or surgical, begin with basic rehabilitation guidelines including eliminating inflammation, normalizing range of motion, and pre-
16 1 MAY 2000 ATHLETIC THERAPY TODAY
venting muscular atrophy. As the throwing athlete progresses to more advanced phases of rehabilitation, the biomechanics of throwing should be considered in choosing appropriate therapeutic exercises to re- gain the functional abilities that are specific to the demands of each sport.
Wilk, Arrigo, and Andrews (1993) have empha- sized working on extension early to prevent elbow flexion contractures and strengthening the muscles that help the UCL dynamically stabilize the elbow during valgus stress, particularly the elbow flexors, wrist flexors, and pronator muscles.
Athletic trainers and therapists should always re- member that the act of throwing is a full-body mo- tion that requires the precise interaction of muscles located proximally and distally in the kinetic chain. Emphasis on strength and flexibility conditioning of the lower extremities and trunk, as well as the rota- tor cuff and scapulothoracic musculature, should be maintained throughout rehabilitation of the elbow.
Rehabilitation programs should be specifically designed to meet the goals of the individual athlete and the demands of the particular sport and injury. The use of both open kinetic chain (OKC) and closed kinetic chain (CKC) exercises has been justified in lower extremity rehabilitation (Reinold, Fleisig, & Wilk, 1999) and might be applicable to the upper extremity using the same rationale. OKC exercises offer isolated muscular contraction and are used for particular muscular strengthening. CKC exercises are used in a weight-bearing position to provide joint pro- prioceptive input through the stimulation of mech- anoreceptors. CKC exercises also provide joint compression and muscular cocontractions through the summation of joint force couples (Wilk & Reinold, in press), which is critical to the dynamic stability of the joint during the throwing motion.
CKC exercises are often performed prior to the initiation of plyometric drills as a way to prepare the joints for the demands of the stretch-shortening cycle. Plyometric drills are often incorporated to mirror the imposed demands of athletic competition in the ad- vanced stages of rehabilitation. The throwing motion involves a plyometric-type muscular contraction and depends on the ability of the muscle to exert maxi- mal force output in a minimal amount of time (Wilk & Reinold, in press). Throwing athletes rely on the prestretch of the shoulder internal rotators and ad-
ductors during the cocking phase prior to producing a concentric muscular contraction of these muscles during the acceleration phase (Wilk, Arrigo, & Andrews, 1 995).
Finally, an interval sport program (Wilk, Andrews, et al., 1997) that gradually progresses the demands placed on the throwing athlete will ensure that the injured tissues are not stressed inappropriately. The number of throws, distance, intensity, and types of throws are monitored and advanced to facilitate the throwing athlete's return to competition (Wilk, Arrigo, & Andrews, 1995).
Fleisig, Zheng, et al. (1 997a) recently broadened their calculations for healthy pitchers to include quan- tification of flat-ground throwing biomechanics. Dur- ing this study, they found varus torque to be 54 N . m when pitching from the mound, with 29 N . m generated by the UCL. In addition, they calculated the maximum varus torques at 59, 54, and 51 N . m when throwing from flat-ground distances at 1 80, 120, and 60 ft, respectively. After applying Morrey and An's (1983) conclusions to these results, the torques on the UCL were estimated to be 32, 29, and 27 N . m, respectively. The same calculations were also per- formed for partial-effort baseball pitches thrown by the same group (Fleisig et al., 1997b). Full-effort (100 %-effort) throws produced the previously men- tioned varus torque of 54 N . m, whereas 75- and 50 %-effort pitches produced 44 and 41 N . m of varus torque, respectively. The corresponding torques on the UCL were 24 N . m at 75% and 22 N . m at 5 0 % .
These studies indicate that flat-ground throwing and partial-effort pitching might be useful tools dur- ing rehabilitation from an elbow injury and in off- season training and conditioning programs. These drills can be incorporated into programs to work on form without exerting large torques on the elbow. The similar kinematic data and decreased kinetic data of flat-ground and partial-effort throwing emphasize proper biomechanics while decreasing stress on the elbow.
Conclusions and implications
Research indicates that throwing motions exert large amounts of stress on the elbow. For athletes who participate in throwing sports, these motions
ATHLETIC THERAPY TODAY MAY 2000 1 17
inherently cause stress to the elbow. It i s i m p e r a t i v e
that precautions be taken to minimize stress during the throwing motion and reduce the chance of lost t i m e resulting from in ju ry . Total-body conditioning and flexibility e x e r c i s e s , as well as avoiding the tempta- tion to perform when not fully r e c o v e r e d , will help reduce athletes' r i s k of elbow i n j u r y , as well as en- hance and prolong their playing careers.
The rationale for choosing sport-specific rehabili- t a t i o n exercises has been p r o v i d e d based on biome- chanical research conducted on throwing athletes. Knowledge of throwing biomechanics and i n j u r y
mechanisms will help athletic trainers and therapists design appropriate rehabilitation p r o g r a m s . OKC and CKC e x e r c i s e s , p l y o m e t r i c d r i l l s , and a gradual return to throwing that includes flat-ground and partial- effort throwing are sport-specific techniques com- monly used to aid the r e h a b i l i t a t i o n specialist in re- turning throwing athletes to their previous functional levels as quickly as p o s s i b l e . II
Atwater, A.E. (1 979). Biomechanics of overarm throwing movements and of throwing injuries. Exercise Sports Science Reviav, 7, 43-85.
Barrentine, S.W. (1 999). Underhand pitching: A biomechanical examina- tion of the softball pitching motion. Sports Medicine Update, 14(2), 4- 7.
Barrentine, S.W., Fleisig, G.S., Whiteside, J.A., Escamilla, R.F., & Andrews, J.A. (1 998). Biomechanics of windmill softball pitching with implica- tions about injury mechanisms at the shoulder and elbow. Journal of Orthopaedic and Sports Physical Therapy, 28, 405-41 5.
Dillman, C.J., Smutz, P., &Werner, S.L. (1 991). Valgus extension overload in baseball pitching [Abstract]. Medicine and Science in Sports and Exercise, 23, 356.
Ellenbecker, T.S., & Mattalino, A.J. (1 997). The elbow in sport: Injury, treat- ment, and rehabilitation. Champaign, IL: Human Kinetics.
Feltner, M., & Dapena, J. (1986). Dynamics of the shoulder and elbow joints of the throwing arm during a baseball pitch. InternationalJour- nal ofsport Biomechanics, 2, 235-259.
Fleisig, G.S., Andrews, J.A., Dillman, C.J., & Escamilla, R.F. (1995). Kinet- ics of baseball pitching with implications about injury mechanisms. American Journal of Sports Medicine, 23, 233-239.
Fleisig, G.S., Escamilla, R.F., Andrews, J.R., Matsuo, T., Satterwhite, Y.. & Barrentine, S.W. (1 995). Kinematic and kinetic comparison between baseball pitching and football passing. Journal of Applied Biomechan- ics, 12, 207-224.
Fleisig, G.S., Zheng, N., Barrentine, S.W., Escamilla, R.F., Andrews, J.A., & Lemak, L.J. (1997a). Kinematic and kinetic comparison of baseball pitching from a mound and throwing from flat ground [Abstract].
American Society of Biomechanics Proceedings. Fleisig, G.S., Zheng, N., Barrentine, S.W., Escamilla, R.F., Andrews, J.A., &
Lemak, L.J. (1997b). Kinematic and kinetic comparison of full-effort and partial-effort baseball pitching [Abstract]. American Society of Biomechanics Proceedings.
Jobe, F.W., & Elattrache, N.S. (1993). Diagnosis and treatment of ulnar collateral ligaments in athletes. In B.F. Morrey (Ed.), The elbow and its disorders (pp. 566-572). Philadelphia: W.B. Saunders.
McBride, D.G., Azar, F., Moeini, S.R., Kelly, R., Andrews, J.A., & Fleisig, G.S. (1 994). Palmaris longus versus patellar tendon in elbow UCL re- construction. Unpublished manuscript.
Morrey, B.F., & An, K. (1983). Articular and ligamentous contributions to the stability of the elbow joint. American Journal of Sports Medicine, 11, 315-319.
Pandya, R.D., Gillogly, S.D., & Andrews, J.A. (1998). Throwing injuries to the elbow. In J.A. Andrews, B. Zarins, & K.E. Wilk (Eds.), Injuries in baseball (pp. 223-228). Philadelphia: Lippincott-Raven.
Regan, W.D., Korinek, S.L., Morrey, B.F., &An, K. (1991). Biomechanical study of the ligaments around the elbow joint. Clinical Orthopaedics and Related Research, 271, 170-1 79.
Reinold, M.M., Fleisig, G.S., & Wilk, K.E. (1999). Research supports both OKC and CKC activities. Biomechanics, 11S, 27-32.
Werner, S.L., Fleisig, G.S., Dillman, C.J., & Andrews, J.A. (1993). Biome- chanics of the elbow during baseball pitching. Journal of Orthopaedic and Sports Physical Therapy, 17, 274-278.
Wilk, K.E., Andrews, J.A., Arrigo, C., Chenielewski, T., Courson, R., DeHart, R., Dillman, C.J., Meadows, M., Williams, H., Wright, H., &Young, R. (1 997). Prevention & rehabilitation exercises for the shoulder and el- bow. Birmingham, AL: American Sports Medicine Institute.
Wilk, K.E., Arrigo, C., & Andrews, J.A. (1 993). Rehabilitation of the elbow in the throwing athlete. Journal of Orthopaedic and Sports Physical Therapy, 17, 305-31 7.
Wilk, K.E., Arrigo, C., & Andrews, J.A. (1995). Functional training for the overhead athlete. In W.D. Bandy (Ed.), Current concepts in the reha- bilitation ofthe shoulder. SPTS Home Study Course. APTA.
Wilk, K.E., & Reinold, M.M. (in press). Plyometric and closed kinetic chain exercise. In Therapeutic exercises: Intervention for individuals with musculoskeletal disfunctions.
Wilson, ED. (1983). Valgus extension overload in the pitching elbow. American Journal of Sports Medicine, 11, 83-88.
Michael M. Reinold is a student researcher at the American Sports Medicine Institute (ASMI) and is currently enrolled in Northeastern University's master's program in physical therapy.
Glenn S. Fleisig holds the Smith & Nephews Chair of Research at ASMI and adjunct faculty positions at the University of Alabama at Birming- ham and Troy State University.
Kevin E. Wilk is national director of research and clinical education for HealthSouth Corporation and associate clinical director at the HealthSouth Sports Medicine and Rehabilitation Center, Birmingham, AL.
Gene G. Jameson is on the faculty at Tri-County Technical College and is the former coordinator of clinical biomechanics at the ASMI.
James R. Andravs is medical director at the ASMI, clinical professor of orthopedic surgery at the University of Alabama at Birmingham, and an orthopedic surgeon at Alabama Sports Medicine and Orthopedic Center.