Rejuvenation of the Anterior Neck The When and Why Jayson Terres, MD, DDS, FACS, FAACS Introduction One of the most common complaints of the cosmetic patient is the neck region. Excessive skin, muscle laxity, and increased fatty deposition are all factors that lead to an unwanted aging effect. Nevertheless, the esthetic improvement of the anterior neck complex remains one of the most challenging aspects of facial rejuvenation. 1e13 This area is often one of the first places people complain of during the “aging” process: whether it is an early accumulation of unwanted fatty deposition, an increased prominence of platysma banding, decreased defini- tion in the cervicomental angle, or loss of skin-muscle tone. There are several combinations of these complaints among a wide variety of ages (Fig. 1). It is important to understand what the patients’ primary concerns are and which proposed treat- ment would give a maximum outcome. It is also important to have an artistic eye and predict the patient’s outcome for their desired procedures to ensure that the other local facial structures will not hamper treatment results. Preoperative understanding of the patient’s desired outcome is paramount in selecting the appropriate surgery. Younger patients that still possess good skin elasticity may be able to have a simple liposculpture procedure, whereas an older patient having the same procedure may not be as pleased with the outcome due to unmasked jowling that is now more apparent or possibly the insufficient intrinsic contractility of skin. Complete fat removal in neck tissue does not lend itself to the optimal result (Fig. 2). An understanding of the patient’s current anatomic state will then most commonly dictate what type of procedure will be performed. These procedures can range from simple liposculpture, to direct lipectomy, pla- tysmaplasty, or complete cervicoplasty encompassing a com- bined facelift (Box 1). Effects on aging/variability of neck types The anterior neck region is more of a sweeping topographic landscape with smooth undulations versus its more flat upper facial counterparts. 1e5 A youthful-appearing facial and neck region has a smooth textured appearance, well-defined cervi- comental angle, and appropriate suspended fullness. Ellenb- ogen 1 has long established the visual aspects of a youthful neck appearance. A youthful neck appearance has been classified as having a cervicomental angle between 105 and 120 with a distinct mandibular border and smooth nonbanded overlying skin draping (Fig. 3). 2 However, as our aging process begins, the initial tone and texture of the more superficial structures is the first visible structure change. Further substructural changes within muscle then give way. It is this laxity of suspensory neck muscles in combination of increased fatty deposits and inferior gravitational movement of the patient’s jowls that account for aging of the neck region. Furthermore, the accumulation of excessive fat deposits is increased with aging, weight gain, and certain medical conditions. Several classification systems have been introduced to characterize this process. I have adapted the Baker classification system, 3 as its 4 subtypes seem to encompass most of my patients’ aging attributes (Box 2, Fig. 4). In addition, there other components that this author thinks can potentiate this aging appearance over time, such as sub- mandibular gland ptosis and mandibular bony atrophydboth of which contribute to a poor cervicomental angle and loss of volume. They can further pose some difficulties to the surgeon, as the decision needs to be made in regards to which procedure or procedures should be performed to maximize outcome and achieve the highest success with the patient’s expectations. Patient expectations In evaluating the patient’s anterior neck region, several factors come into play. First and foremost is the patient’s biggest concern, their chief complaint. In my presurgical consultations, The author has nothing to disclose. Maxillofacial Trauma, Mother Frances Health System, Tyler, TX, USA E-mail address: [email protected]KEYWORDS Rejuvenation Anterior neck Liposculpture Cervicoplasty KEY POINTS Rejuvenation of the anterior neck region requires a complex artistic interpretation of the patient’s desires and potential anticipated outcomes. Whether it is a minimal invasive liposculpture procedure to a full cervicoplasty with chin augmentation and full facelift, the outcome will be optimal if the anticipated areas of complaints are fully addressed. Understanding the patient’s relative aging process will ultimately lead to the correct proposed treatment. Atlas Oral Maxillofacial Surg Clin N Am 22 (2014) 25–36 1061-3315/14/$ - see front matter ª 2014 Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.cxom.2013.10.001 oralmaxsurgeryatlas.theclinics.com
Transcript
Rejuvenation of the Anterior Neck
The When and WhyJayson Terres, MD, DDS, FACS, FAACS
� Rejuvenation of the anterior neck region requires a complex artistic interpretation of the patient’s desires and potentialanticipated outcomes.
� Whether it is a minimal invasive liposculpture procedure to a full cervicoplasty with chin augmentation and full facelift, theoutcome will be optimal if the anticipated areas of complaints are fully addressed.
� Understanding the patient’s relative aging process will ultimately lead to the correct proposed treatment.
Introduction
One of the most common complaints of the cosmetic patient isthe neck region. Excessive skin, muscle laxity, and increasedfatty deposition are all factors that lead to an unwanted agingeffect. Nevertheless, the esthetic improvement of the anteriorneck complex remains one of the most challenging aspectsof facial rejuvenation.1e13 This area is often one of the firstplaces people complain of during the “aging” process: whetherit is an early accumulation of unwanted fatty deposition, anincreased prominence of platysma banding, decreased defini-tion in the cervicomental angle, or loss of skin-muscle tone.There are several combinations of these complaints among awide variety of ages (Fig. 1). It is important to understand whatthe patients’ primary concerns are and which proposed treat-ment would give a maximum outcome. It is also important tohave an artistic eye and predict the patient’s outcome for theirdesired procedures to ensure that the other local facialstructures will not hamper treatment results.
Preoperative understanding of the patient’s desiredoutcome is paramount in selecting the appropriate surgery.Younger patients that still possess good skin elasticity may beable to have a simple liposculpture procedure, whereas anolder patient having the same procedure may not be as pleasedwith the outcome due to unmasked jowling that is now moreapparent or possibly the insufficient intrinsic contractility ofskin. Complete fat removal in neck tissue does not lend itselfto the optimal result (Fig. 2). An understanding of the patient’scurrent anatomic state will then most commonly dictate whattype of procedure will be performed. These procedures canrange from simple liposculpture, to direct lipectomy, pla-tysmaplasty, or complete cervicoplasty encompassing a com-bined facelift (Box 1).
The author has nothing to disclose.Maxillofacial Trauma, Mother Frances Health System, Tyler, TX, USAE-mail address: [email protected]
Atlas Oral Maxillofacial Surg Clin N Am 22 (2014) 25–361061-3315/14/$ - see front matter ª 2014 Elsevier Inc. All rights reserved.http://dx.doi.org/10.1016/j.cxom.2013.10.001
Effects on aging/variability of neck types
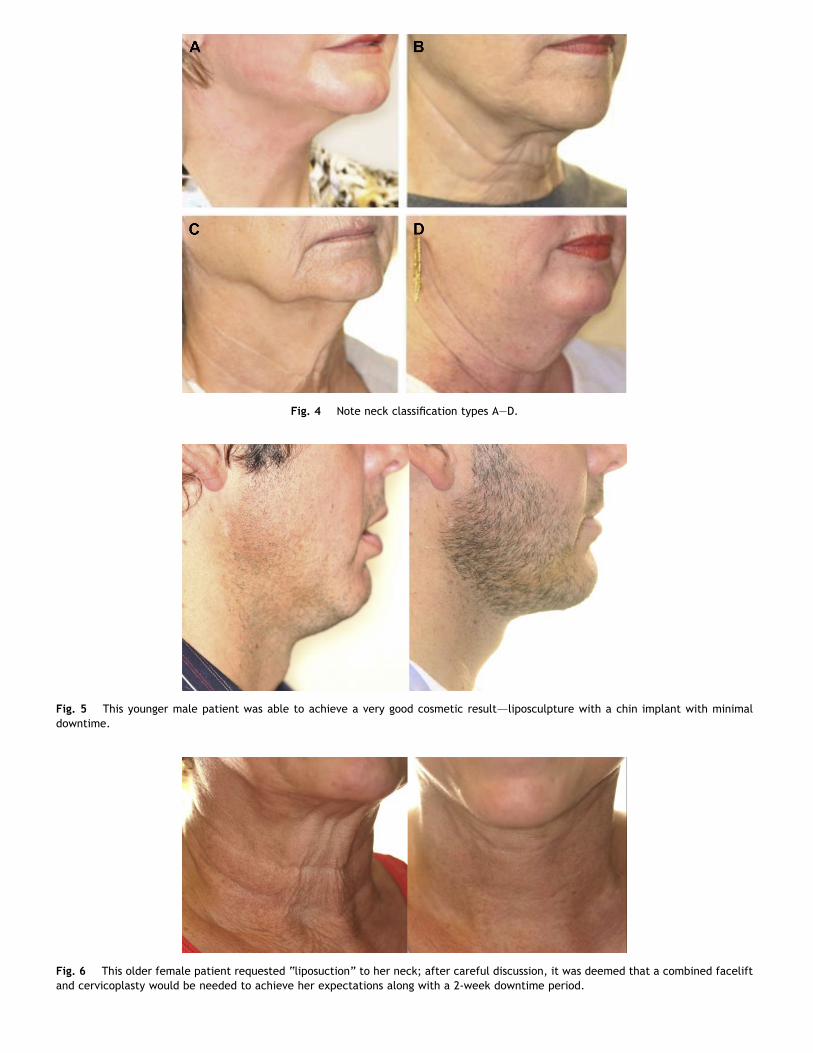
The anterior neck region is more of a sweeping topographiclandscape with smooth undulations versus its more flat upperfacial counterparts.1e5 A youthful-appearing facial and neckregion has a smooth textured appearance, well-defined cervi-comental angle, and appropriate suspended fullness. Ellenb-ogen1 has long established the visual aspects of a youthful neckappearance. A youthful neck appearance has been classified ashaving a cervicomental angle between 105 and 120� with adistinct mandibular border and smooth nonbanded overlyingskin draping (Fig. 3).2 However, as our aging process begins, theinitial tone and texture of the more superficial structures is thefirst visible structure change. Further substructural changeswithin muscle then give way. It is this laxity of suspensory neckmuscles in combination of increased fatty deposits and inferiorgravitational movement of the patient’s jowls that account foraging of the neck region. Furthermore, the accumulation ofexcessive fat deposits is increased with aging, weight gain, andcertain medical conditions. Several classification systems havebeen introduced to characterize this process. I have adaptedthe Baker classification system,3 as its 4 subtypes seem toencompass most of my patients’ aging attributes (Box 2,Fig. 4).
In addition, there other components that this author thinkscan potentiate this aging appearance over time, such as sub-mandibular gland ptosis and mandibular bony atrophydboth ofwhich contribute to a poor cervicomental angle and loss ofvolume. They can further pose some difficulties to the surgeon,as the decision needs to be made in regards to which procedureor procedures should be performed to maximize outcome andachieve the highest success with the patient’s expectations.
Patient expectations
In evaluating the patient’s anterior neck region, several factorscome into play. First and foremost is the patient’s biggestconcern, their chief complaint. In my presurgical consultations,
Fig. 1 Note the difference in neck structural types. Patient on the left exhibits mild submental lipomatosis, whereas the patient on theright has redundant tissue, lipomatosis, and banding. Also, note the second patient has much more prominent jowls and mandiblenotching.
26 Terres
I always explain to the patient that we both must see theirissuedif I cannot, this becomes a flag to me, or if I see some-thing that the patient does not complain of, I will point it out,because I can see a potential issue that may become exacer-bated in the future if the wrong surgery is performed.
In listening to my patients, I often hear that they do notwant anything too invasive or they only want a few days ofdown time or they do not want a facelift, just fix their saggingneck. Well, as I like to explain to my patients, there is the“right answer” for their problem and then there is the “rightprocedure” for their problem. What I mean by this is, forexample, if a 60-year-old patient comes into my office andwants his/her neck “tightened” and his/her eyes “lifted”dwhat he/she likely needs is a brow lift, upper/lower eyelid lift,full face/neck lift, laser resurfacing, and possibly chin andcheek implants. They need 2 to 3 weeks of downtime to ach-ieve this simple complaint. Explaining this to a patient thatliposuction and a blepharoplasty will not provide an optimaloutcome on her/him (like it did on a 40-year-old friend) can bedifficult. Therefore, even though the optimal procedure forthis type of patient would be a more classic complete facialrejuvenation, I may tailor the surgery to meet my patient’smore specific requests. I am not advocating a “quick-fixprocedure,” but think it is very important to keep all of thepatient’s expectations in mind to the best of my abilities. At
Fig. 2 This patient had prior neck liposuction. The result wasoversculpture and now a more visualized platysma band (arrow).
this point, I may recommend staged surgeries or give the pa-tient a complete understanding of why the “quicker” proce-dure would not be most beneficial for her/him (Figs. 5 and 6).
Indications for neck rejuvenation
Given the complexity and variability of the anterior neck re-gion, most treatment options will be individualized for eachpatient. Age, gender, race, social history, habits, and geneticsall play major roles in the aging process. Table 1 provides abrief description of the problem areas and their respectivetreatments and is a basic guide for what would be necessary tocorrect the problem. Often it is the combination of 2 or moreof these procedures that is necessary to maximize outcomes.An in-depth description of neck subregions is described later inthis article.
Surgical anatomy concepts
The anatomy of the neck is complex and in itself is the subjectof full textbooks. The anatomy of the platysma has beenextensively studied4,5 and a brief summary will not do it anyjustice, although a brief overview and some important land-marks to aid with the rejuvenation surgical aspect have beenincluded.
Box 1. Terms
� Liposculpture: classic liposuction, but in the neck theartistic ability to “sculpt” fatty areas, removing more incertain areas and less in others to maximize cosmeticappearance
� Direct lipectomy: removal of fat under direct vision(can be with lipocannula, surgical scissors, bovie, etc)
� Platysmaplasty: retightening the platysma muscle inthe anterior neck regions. Various methods are used,whether it is a single or double layered “corset”approachdwith or without back cuts
� Complete cervicoplasty: encompasses direct removalof fat, platysmaplasty, and possibly facelift (short inci-sion, superficial musculo-aponeurotic system (SMAS), ordeep plane)
Fig. 3 Note the youthful, smooth neck contour and acceptable chin neck angle.
Rejuvenation of the Anterior Neck 27
The anatomic structure of the anterior neck is a complexlaminate, made up of layers of skin and soft tissue (fat, fascia,muscle) that encompass nerves, vessels, and lymphatics.6
When performing full neck rejuvenation, it is paramount tostay in the right plane, which will not only give the surgeon anoptimal outcome but also keep you away from any troubledareas (ie, nerves or great vessels). There are several classicdescriptions of the series of “muscle triangles” described bytheir relative locations and particular borders.7 The complexityof the neck anatomy can be overwhelming and not the basis ofthis surgical anatomic discussion. Rather, anatomic estheticsubunits, what they encompass, and how to correct them arethe focused on.
Feldman7 describes the anatomic face as a set of 5 regionalesthetic subunits, with the neck being one. It can be describedas an undulating trapezoid; the neck extends from below themandibular border, down toward the collarbones and post-eriorly to the occiput region, just anterior to the trapeziusmuscles. He then further divides into 8 smaller subunits: (1)jawline bands, (2) chin subunit, (3) submental zone, (4) ver-tical midline strip, (5) middle neck lowland, (6) lateral neckhighland, (7) small musclulomandibular triangle, and (8)
Box 2. Patient types
� Type I patients have slight cervical skin laxity withsubmental fat and early jowls
� Type II patients have moderate cervical skin laxity,moderate jowls and submental fat
� Type III patients have moderate cervical laxity, but withsignificant jowling and active platysmal banding
� Type IV patients have loose, redundant cervical skin andfolds below the cricoid, significant jowls, and activebands
postauricular hinterland. The analysis of these subunits asa whole must take into account the varying degrees of thepatient’s skin tone texture and tightness, along with the un-derlying support structure (muscle) and any laxity it may havedeveloped, and finally, the varying degrees of fat deposition(Fig. 7).
The first area, the jawline bands, is a very commoncomplaint of “ jowling.” The degree of facial jowling and theprejowl notch will dictate the amount of fatty tissue in thearea that needs to be removed and the degree of subcu-taneous release of the mandibular ligament, which will alsolead into the chin subunit. Identifying the patient for chinaugmentation can accomplish several esthetic goals. First, animprovement in the cervicomental angle, and second,camouflaging a prejowl notch. (Even in patients who do notneed anterior-posterior chin advancement, I use a prejowlimplant with no anterior-posterior projection to aid in a deepprejowl notch.)
The next 2 areas of concern are the submental zone andvertical midline strip. These areas are going to give the mostinformation about the rejuvenation process of the neck,whether it is a young patient with good skin overtone andmoderate lipomatosis or an elderly patient with skin laxity,muscle banding, and severe lipomatosis. This region dictatesminimal invasive liposculpture to submentalplasty to completecervicomentalplasty with combined facelift. The region con-tains both supra- and subplatysma fat structure, platysmamuscles, hyoid bone, anterior jugular vein, and its communi-cating branches. The 2 leading edges of the platysma will havesome decussation in most patients, and a small percentage willhave none, although it is this area where redundant tissue(both muscle and fat) will be excised and tightened (Fig. 8).The deeper muscle structures, such as the anterior digastricmuscles, may also need to be trimmed or tighteneddbut Iusually find this is on a prior operated neck where otheroverlying structures have been repositioned or removed inexcess.
Fig. 4 Note neck classification types AeD.
Fig. 5 This younger male patient was able to achieve a very good cosmetic resultdliposculpture with a chin implant with minimaldowntime.
Fig. 6 This older female patient requested “liposuction” to her neck; after careful discussion, it was deemed that a combined faceliftand cervicoplasty would be needed to achieve her expectations along with a 2-week downtime period.
Table 1 Problem areas and treatments
Problem Area Treatment
1. Subcutaneousfat
Liposculpture or direct lipectomydagedependent
2. Excessive skin Direct excision with redraping (isolatedneck/or facelift)
3. Subplatysma fat Direct excision with platysma tightening
4. Platysma bands Platysma plication with inferior back cut
5. Retrogenia Alloplastic implant or orthognathicsurgery
6. Poor neck angle Combinations of all the above
Rejuvenation of the Anterior Neck 29
The midneck lowland region is an important clinical areathat needs to be thoroughly examined before a final treatmentis proposed. The midneck lowland region is the region whereexcessive jowling and submandibular salivary gland distinctionmust be made. Not only is this an area of excessive lipomatosis,but also the submandibular gland can be prominent and easilycamouflaged by excess fat. Palpation of this area from both anintraoral and an extraoral approach can provide great insightas to whether the gland will require a partial resection, sus-pension, or oversew in the supporting muscle.
The lateral neck highland area is the topographic areaoverlying the sternocleidomastoid muscle and is the mostdifficult area for cutaneous flap elevation. The fascia fibersoverlying the muscle structure are in greatest number here andmake dissection challenging. However, it is of great impor-tance to dissect enough tissue away to ensure a proper skin“redraping”; otherwise a gathered tissue appearance will givea noticeable “operated” neck.
The final 2 described areas are small triangle regions. Thefirst area is the musculomandibular triangle, just inferior to theearlobe. This area can be somewhat problematic becauseinferior earlobe distortions from improper suspension can bequite visible. The classic “pixie-ear” deformity from an iso-lated neck lift or complete face and neck lift is formed fromimproper suspension of tissue and excessive skin pull (Fig. 9).This area can also be affected if there is too much fatty tissueleft behind, causing a blunting of the posterior border of themandible. Careful attention is also warranted to ensure that
Fig. 7 The subdivisions of the n
there is no excessive parotid tissuedif present, I prefer toleave the gland structure but will remove excessive fatty tissueto improve the clinical cervicomental angle. The final area isthe postauricular hinterland; the region is just posterior to theauricle, where the final resting place of newly suspended tissueresides. Passive tissue will give the most optimal results.Excessive removal will lead to wound breakdown and widenedscar bands. Too little removal can leave “tissue rolls” that maytake several months to soften and often patients will complainof lumpy tissue.
Nonsurgical techniques
There are several nonsurgical modalities for improving theaging neck. These techniques can include anything from neckmuscle exercises, botulism injections, and skin tightening withlasers, radiofrequency, or even chemical peeling. In my opinionthese are very patient-specific and yield only temporaryresults. Some are discussed, because they remain popularrequests among patients.
Botulinum toxin
Chemodenervation with Botulinum toxin (Botox, Dysport, andothers) will help with static platysma bands. Muscle atrophycan ensure and a loss of prominence can improve the anteriorneck appearance.8 Dynamic bands can also be treated withBotox injections. Softening of these “active” muscle bands candelay the formation of static platysma lines with repeatedinjections. Just as Botox reduces dynamic and static line for-mation in the forehead and glabella regions, it can be helpfulin the anterior neck as well. However, due to differences in theaffected muscle structures, overlying skin tone, textures, andsubunit attachments, the benefits are usually not as great asthose seen in the forehead area.
Laser resurfacing
Laser resurfacing to the anterior neck can improve the toneand texture of the skin and to some degree collagen tighteningwill also occur. However, these treatments must take intoaccount the skin difference from the upper facial units: theamount of sebaceous type tissue and the skin epidermal and
eck as described by Feldman.
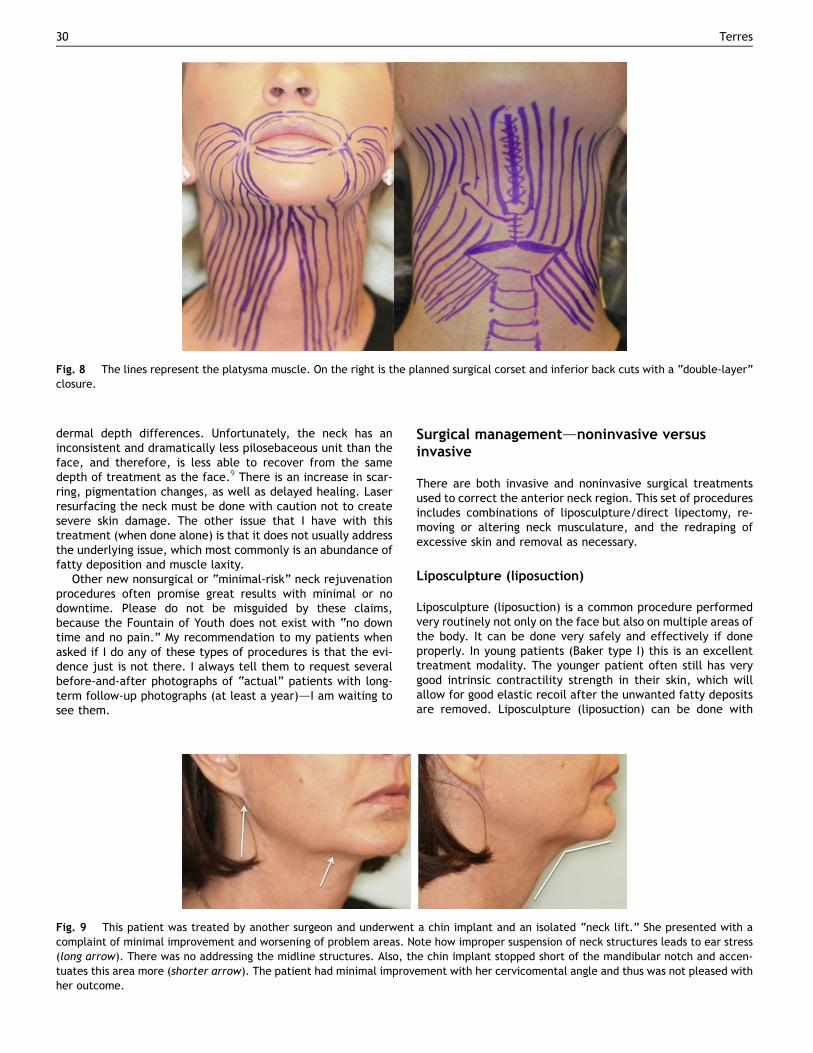
Fig. 8 The lines represent the platysma muscle. On the right is the planned surgical corset and inferior back cuts with a “double-layer”closure.
30 Terres
dermal depth differences. Unfortunately, the neck has aninconsistent and dramatically less pilosebaceous unit than theface, and therefore, is less able to recover from the samedepth of treatment as the face.9 There is an increase in scar-ring, pigmentation changes, as well as delayed healing. Laserresurfacing the neck must be done with caution not to createsevere skin damage. The other issue that I have with thistreatment (when done alone) is that it does not usually addressthe underlying issue, which most commonly is an abundance offatty deposition and muscle laxity.
Other new nonsurgical or “minimal-risk” neck rejuvenationprocedures often promise great results with minimal or nodowntime. Please do not be misguided by these claims,because the Fountain of Youth does not exist with “no downtime and no pain.” My recommendation to my patients whenasked if I do any of these types of procedures is that the evi-dence just is not there. I always tell them to request severalbefore-and-after photographs of “actual” patients with long-term follow-up photographs (at least a year)dI am waiting tosee them.
Fig. 9 This patient was treated by another surgeon and underwentcomplaint of minimal improvement and worsening of problem areas. N(long arrow). There was no addressing the midline structures. Also, thtuates this area more (shorter arrow). The patient had minimal improvher outcome.
Surgical managementdnoninvasive versusinvasive
There are both invasive and noninvasive surgical treatmentsused to correct the anterior neck region. This set of proceduresincludes combinations of liposculpture/direct lipectomy, re-moving or altering neck musculature, and the redraping ofexcessive skin and removal as necessary.
Liposculpture (liposuction)
Liposculpture (liposuction) is a common procedure performedvery routinely not only on the face but also on multiple areas ofthe body. It can be done very safely and effectively if doneproperly. In young patients (Baker type I) this is an excellenttreatment modality. The younger patient often still has verygood intrinsic contractility strength in their skin, which willallow for good elastic recoil after the unwanted fatty depositsare removed. Liposculpture (liposuction) can be done with
a chin implant and an isolated “neck lift.” She presented with aote how improper suspension of neck structures leads to ear stresse chin implant stopped short of the mandibular notch and accen-ement with her cervicomental angle and thus was not pleased with
Rejuvenation of the Anterior Neck 31
minimal anesthesia and a relatively uneventful postoperativecourse. However, whereas liposuction does have a role incosmetic surgery of the submental area, it is not a compre-hensive procedure and does not address all of the anatomiccomponents leading to submental fullness.10
Direct lipectomy
Direct lipectomy is performed in younger patients with moreneck fullness caused by excessive fatty deposition, but stillgood skin tone (Baker type I and some IIsdthis is difficult tojudge and clinical experience is the only way to determine ifyou can achieve adequate results in these types of patients).Again, anesthesia is the surgeon’s preference. However, theseare commonly done through a slightly larger incision thangeneral liposculpture, and both lipocannulas and facelift scis-sors are used for direct fat removal.
Platysmal plication
Once muscle laxity has occurred, whether the patient dem-onstrates a single- or double-banded structure in the anteriorneck, the platysma needs to be tightened (Baker type IIeIII).There are too many ways to list on how this is performed, butthe procedure involves a submental crease exposure, fattycutaneous plane, and direct visualization of the platysmamuscle. Excessive muscle tissue is removed in the midline, and2 leading edges are clearly identified. The subplatysma fat canbe removed here as deemed necessary; then the muscle isclosed overlying this area and is done in 1 or 2 layers. Variousback cuts have been described.2,5,7 The complete surgicaldetails are presented later in this article. At this point theoptions for isolated posterior neck tightening or the addition ofa formal facelift are done. The addition of a chin implant canbe considered as well.
The goal of this procedure is to provide an improvement in thecervicomental angle, smooth and uniform skin contour, and adecrease in the amount of unwanted fatty tissue deposits. It ismost important not to overdo any particular portion or un-wanted asymmetries or uneven skin texture may hamper youroverall results.
My surgical techniques are very similar for all my “com-plete-neck” or cervicoplasty rejuvenation patients. These pa-tients usually fit the Baker type IIIeIV classification and I stillperform almost the same surgical procedure with the excep-tion of an additional suture corsets layer in the last group.
A rhytidectomy in conjunction with a neck rejuvenationprocedure is my preferred operation for almost all my pa-tients. The addition of the SMAS elevation with neck rejuve-nation allows for a smoother and controlled elevation andrepositioning of the soft tissues, especially aiding in thelateral neck area. Performing anterior neck surgery alone cansometimes accentuate jowling and lateral neck fullness aswell as place more of an unwanted visual focus on the pa-tient’s other aging facial features.7 There are surgeons whoclaim that the posterior neck pull after an anterior plicationdoes not make sense, and the increased in posterior tensionwill have an increased likelihood of midline failure but this isnot what I usually see. I think the posterior resuspension
needs to be done carefully and not “overly” tightened to givea good harmonious neck contour. I do not always do a sub-mentalplasty corset. There are some patients who presentwith such severe jowling that requires a large “pull-up” ofSMAS tissue and in these cases if I can just perform anteriormidline resection of excessive laxed muscle tissue andremove excessive fat, I can maximize their lift and fix thejowling without being held back by an excessive midlineplatysma tightening.
Operative techniques
All of my surgical patients are seen in my accredited ambula-tory surgery center. I use varying depths of anesthesia, but myusual routine is done with an laryngeal mask airway andgeneral anesthetic gas (sevoflurane). Of course, all of thefollowing procedures can be done with IV sedation, or a gen-eral anesthetic, and some people will do with PO sedation andlocal anestheticdbut this is not my preferred method.
Operative steps: noninvasive and invasive
Noninvasive liposcultureIn the preoperative setting, I mark the desired area for lip-osculpture with the patient in an upright position; using amirror, I have the patient directly visualize the anticipatedareas while I mark them. I then outline key anatomic areasdmandible border, hyoid, muscle structures, and nerve course. Iuse 3 small incisions, one submental, and the other 2 justbehind the earlobes. After I complete these markings, I reclinethe patient into the anticipated surgical position and reinspectmy markings.
Once in the operating room, a standard sterile drape andpreparation (hibiclens prep is my preferred choice) iscompleted. The surgical sites are infiltrated with a smallamount of 1% lidocaine and then the anterior neck is infiltratedwith tumescent solution (my mixture is 0.01% lidocaine with1 part per million epinephrine) (Fig. 10).
I use 3 small stab incisions when doing liposculpture alone,but if I plan for a direct lipectomy, the submental incision isextended to 3 cm in the shadow just posterior to the submentalskin crease.
Starting from the submental incision, bluntly dissect in asubcutaneous plane, overlying the platsyma with one hand andhold the neck skin with the other using the cannula in a star-burst pattern. It is very important to maintain the same plane;this dissection is relatively easy, so do not overforce it! Afterfanning the anterior region of the neck, do the same procedurefrom each of the lateral areasdkeeping in mind relativeanatomic structures, nerve courses, and vascular position.After the dissection is completed, a lipocannula is used to“sculpt the neck,” with continual sweeping motion with directvisualization of the cannula underlying the skin. (There areseveral types of cannulas for this procedure. I tend to use bothflat spatulas and round cannulas or varying sizes. I also usecannulas attached to wall suction or with a syringe and Johnny-lock device [Fig. 11].) You can turn the suction opening “to-ward” the skin surface, but it is only recommended doing thisin certain areas where the fatty deposits are thicker or moreirregular. The goal is NOT to remove all the fat, just unnec-essary fat, and provide a smooth plane of dissection above theplatysma muscle to allow an even redraping of skin tissue. I dooccasionally have to do subplatysma fat liposculpture in the
Fig. 10 Tumescence solution being infiltrated into subcutaneous tissue. After 12 minutes, tissue blanching in the picture on the right canbe noted.
32 Terres
anterior region as well in more full-neck patients, remem-bering not to overreduce or you could make the underlyingstructures (thyroid cartilage, digastric muscles, hyoid bone)more apparent.
My surgical approach is exactly the same for direct lipec-tomy, except following the initial liposculpture, I open thesubmental incision to 2.5 to 3 cm and use a lighted retractor toremove any excessive fatty deposits with direct vision. Onesmall 6-0 nylon suture is used to close each of the access in-cisions (more for direct lipectomy) and soft gauze pads areopened and placed in the anterior neck and an elastic headwrap is placed. My typical protocol is for the patient to wearthe head wrap for 1 week for 24 hours except when showeringand then an additional week only at night (Box 3).
Invasive cervicoplastyAs discussed earlier, there is great variability between indi-vidual neck types. The proposed surgical technique is a com-mon standard procedure that will encompass the rejuvenationprocess for most of these types. Certain steps may be omittedor overly emphasized pending the individual patient.
As previously described, the anterior neck is a harmonioustopographic architecture that needs to be smooth. I like tothink of it as a lump of clay on a potter’s wheel; the clay is spunand the potter smooths it centrally and brings its up. Thistechnique is our goal for neck surgical rejuvenation; smoothout the tissues and “bring them up.” Platysma laxity, sub-mental lipomatosis, and cervical lipomatosis cannot be ade-quately addressed solely through a preauricular incision. Thegoal of achieving an improved and cosmetically enhanced
Fig. 11 Standard liposuction cannulas, one with a lock-syringedevice and the other for wall suction.
cervicomental angle is done by the anterior midline platysmaplication, inferior muscle release, and its facial componentthat allows for a superior lateral anchor that minimizes tensionof the anterior corset (Fig. 12).11
The initial portion of this is the same as mentioned abovefor liposculpture, using the extended 3-cm incision just pos-terior to the submental crease. The anterior neck is completelyexposed using facelift scissors with both a vertical and a hor-izontal motion.
The surgical plane established will vary on neck and patienttype but usually extends to below the cricoid (again, inferiorextension varies in each patient), carried out laterally to theposterior angle of the mandible (Fig. 13). Using lighted re-tractors, any bulbous fatty deposits are directly removed, andhemostasis is achieved. This exposure will allow for anadequate platysmaplasty. Under direct vision the medialleading edges of the platysma are freed from the underlyingsubplatsyma fat and digastric muscles and grasped and broughtto the midline. Excessive muscle and fat are excised and theleading edges are imbricated together with 1 to 2 layers ofrunning suture. A release is performed low in the neck to allowfor adequate muscle redrape. This technique will tighten theplatysma and improve the cervicomental angle. I directlyvisualize the areas where the submandibular glands are andpending any herniation or enlarged gland tissue I will eitherplace a row of support sutures, or if the gland is easily visu-alized, I will just remove a portion of it. Some authors dodescribe an intraoral resuspension,2,5,12 but rarely have I hadto do this.
Although this procedure can be very beneficial in youngerpatients, I find that most patients will require lateral neck
Box 3. Quick summary
1. Mark patient2. Tumescence through 3 small incisionsdwait 15 min3. Dissect with flat cannula4. Liposculpt with 4e5 mm flat/round cannula5. Closure6. Wrap with head dressing for 1 wk
Fig. 12 Preoperative markings for combined neck rejuvenation with SMAS lift.
Rejuvenation of the Anterior Neck 33
approaches to maximize their expected outcome. I almost al-ways combine complex neck rejuvenation with a facelift pro-cedure and by doing so it will allow the surgeon to address theneck as well as any unwanted jowling or other aging issues. Mypreferred adjunctive facelift procedure is an SMAS elevationwhereby a portion of the SMAS flap is elevated superior andanother is transposed posterior to the ear to affect lateral neckcontour (Fig. 14). This portion of the SMAS is secured to themastoid fascia with permanent suture. One technical point is
Fig. 13 (A) Surgical access for anterior neck. (B) Exposure openingaccess for SMAS lift component. (D) Connection of face and neck flaps
clear: cervical rhytidectomy suspension with a predominantlysuperior vector will serve to sharpen the jawline and crisplydefine the face-to-neck transition (Fig. 15).11
Chin implant
Patients who are retrognathic and/or retrogenic are goodcandidates for chin augmentation. Whether the surgeryrelies on an artistic appreciation of facial harmony or a formal
for direct lipectomy and anterior platysma plication. (C) Surgical.
Fig. 14 Sequential operative technique for anterior neck rejuvenation (direct lipectomy, platysma plication with back cut, and SMASelevation). (A) Note extensive cutaneous elevation. (B) SMAS with direct platysma pull. (C) Marking SMAS for partial resection and posteriorplication. (D) SMAS resection.
34 Terres
soft/hard tissue cephalometric analysis is completed, chinaugmentation can have a profound effect on cervicomentalenhancement. Whether a formal horizontal mandibularosteotomy is carried out or an alloplastic implant is placeddboth can dramatically improve a poor cervicomental angle andprovide an optimal esthetic and functional outcome.14,15
Submandibular gland
The submandibular gland is the one area that that I admit-tedly overlooked when I first began doing full face and neckrejuvenation procedures over 10 years ago. Basically, it justwas not an issue in most of my early procedures. Now,though, this is one of the key areas that I make certain toaddress before any procedure is done, from basic lip-osculpture to full facial rejuvenation. The reason for doing sois that after a very well-orchestrated surgery, if the glandbecomes a visualized problem, it becomes the only thing thepatient focuses on. That being said, there are a few ways toensure that the gland does not become as issue. I routine willplace overlying mattress suspension sutures in the platysmato create a substructural support if the gland is not overlylarge. I also perform a partial gland resection if the superiorhead of the gland is excessively prominent or noticeablyherniating through the underlying muscle. Finally, glandsuspension with suspension sutures with a combined intraoralapproach can be done if the gland itself is thought to beexcessively large or not amenable to the other listedprocedures.12
Fat grafting
Patients who have already had a prior facelift with neckcombination and have a noted middling “trough” appearanceare candidates for fat grafting. Esthetic surgeons have beenperforming facial rejuvenation that usually involves excisionand resuspension, but there are many times that restoringfacial volume (lost with aging) with provide similar or betterresults.13 In the anterior neck region, the usual patient issomeone that had an overaggressive resection of the supra-/subplatysma fat, now with lax platysma or a howled out areawith a tethered skin appearance. I perform my routine openneck from a submental incision and identify and free up theanterior leading edges of the platysma; if they are connectedin the midline, I separate them and do a direct fat graft intothe subplatsyma area and then perform a double-layeredclosure of the muscle. Grafting between the platysma andcutaneous layer is then a clinical decision. It has been myexperience that the more uniform the grafted fat, the betterthe outcome. I routinely overfill by about 15% to 20%.
Pitfallsdareas that are often overlooked� Low hyoid� Subplatysma fat content� The chindchin augmentation can improve cervicomentalangle, soften or decrease to mandible prejowl notch
� Submandibular gland� Elderly patients almost always require full cervicoplastyto achieve optimal results
Fig. 15 All patients (AeC) shown underwent a full anterior neck rejuvenation with SMAS facelift. All result photographs are 1-yearpostoperative.
Rejuvenation of the Anterior Neck 35
36 Terres
Summary
Rejuvenation of the anterior neck region requires a complexartistic interpretation of the patient’s desires and potentialanticipated outcomes. Whether it is a minimally invasiveliposculpture procedure or a full cervicoplasty with chinaugmentation and full facelift, the outcome will be optimal ifthe anticipated areas of complaints are fully addressed. Un-derstanding the patient’s relative aging process will ultimatelylead to the correct proposed treatment.
References
1. Ellenbogen RK. Visual criteria for success in restoring the youthfulneck. Plast Reconstr Surg 1980;66(6):826e37.
2. Ramirez OM. Advanced considerations determining procedureselection in cervicoplasty. Clin Plast Surg 2008;35(4):670e90.
3. Baker DC. Lateral SMASectomy, plication and short scar facelifts:indications and techniques. Clin Plast Surg 2008;35(4):533e50.
4. Vistnes LM, Souther SG. The platysma muscle. Anatomic consid-erations for aesthetic surgery of the anterior neck. Clin Plast Surg1983;10:441.
5. De Castro CC. Anatomy of the neck and procedure selection. ClinPlast Surg 2008;35:625.
6. Burnham MA. Facial nerve anatomy relevant to cosmetic surgery.Oral Maxillofac Surg Clin North Am 2000;12(4):613e21.
7. Feldman JJ. Neck lift. St Louis (MO): Quality Medical Publishing;2006.
8. Brandt FS, Boker A. Botulinum toxin for the treatment of necklines. Dermatol Clin 2004;22:159e66.
9. Toft KM, Blackwell KE, Keller GS. Submentoplasty. Facial Plast SurgClin North Am 2000;8(2):183e92.
10. Fattahi T. Submental liposuction versus formal cervicoplasty:which one to choose? J Oral Maxillofac Surg 2012;70(12):2854e8.
11. Wachholz JH. Surgical treatment of the heavy face and neck.Facial Plast Surg Clin North Am 2009;17(4):603e11.