24
RENAL PHYSIOLOGY Physiology Unit 4
| Date post: | 12-Mar-2018 |
| Category: |
Documents |
| Upload: | phungnguyet |
| View: | 223 times |
| Download: | 0 times |
RENAL PHYSIOLOGY
Physiology
Unit 4
Func1ons
• Primary: regulate ECF through urine forma1on
• Kidneys – Regulate volume of blood plasma
– Regulate concentra1on of waste products – Regulate concentra1on of electrolytes – Regulate acid‐base balance – Produce and secrete hormones
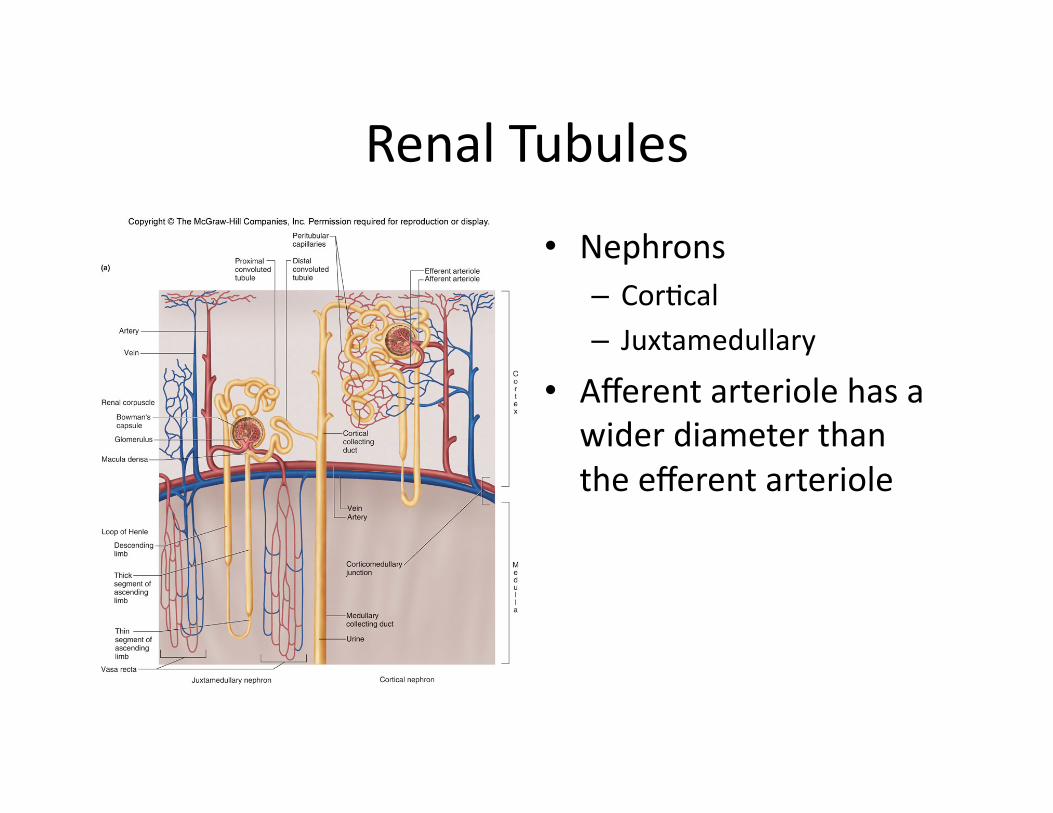
Renal Tubules
• Nephrons – Cor1cal – Juxtamedullary
• Afferent arteriole has a wider diameter than the efferent arteriole
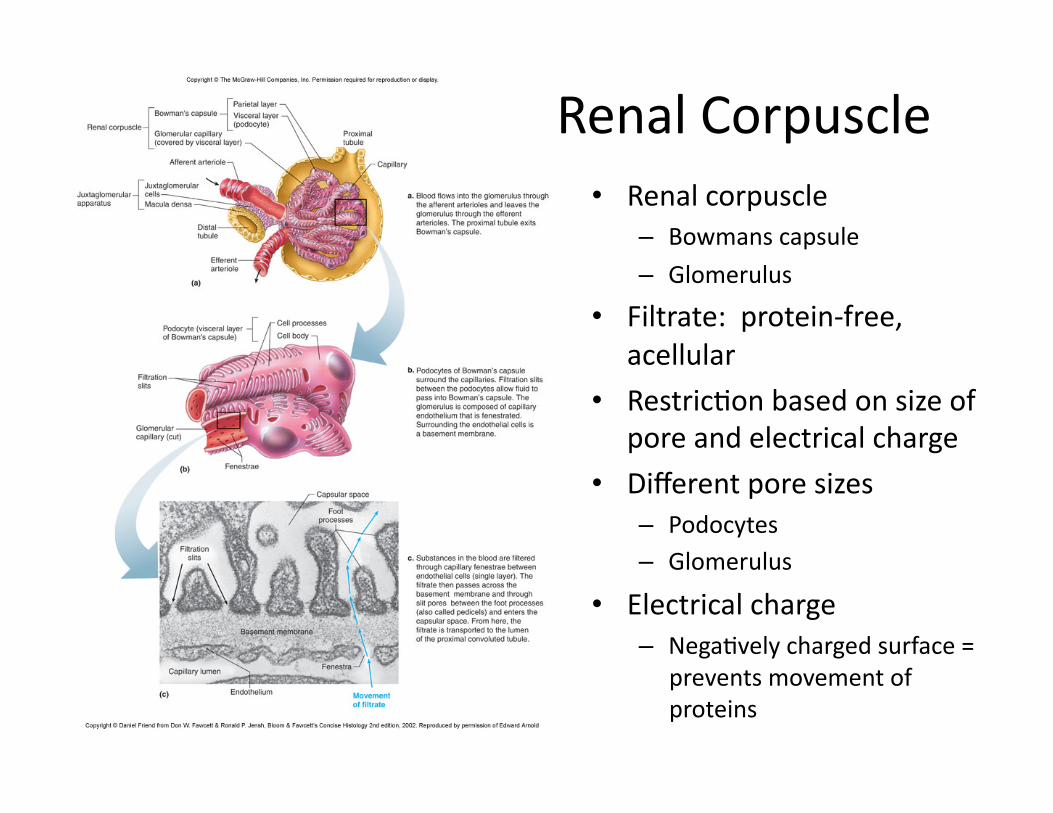
Renal Corpuscle • Renal corpuscle
– Bowmans capsule
– Glomerulus
• Filtrate: protein‐free, acellular
• Restric1on based on size of pore and electrical charge
• Different pore sizes – Podocytes – Glomerulus
• Electrical charge – Nega1vely charged surface =
prevents movement of proteins
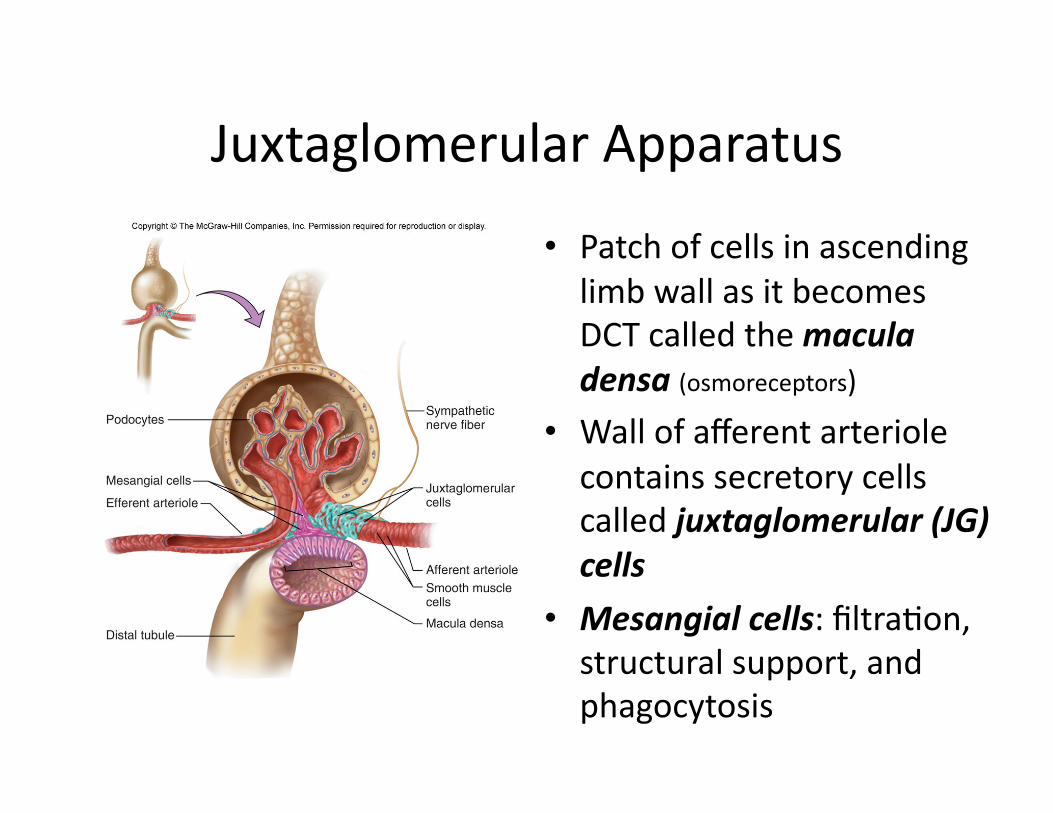
Juxtaglomerular Apparatus
• Patch of cells in ascending limb wall as it becomes DCT called the macula densa (osmoreceptors)
• Wall of afferent arteriole contains secretory cells called juxtaglomerular (JG) cells
• Mesangial cells: filtra1on, structural support, and phagocytosis

Renal Func1on

Glomerular Filtra1on • Starling forces
– hydrosta1c pressure vs. osmo1c pressure
• Net filtra1on pressure 16mmHg
• Subject to physiological control – Neural, hormonal input to afferent and efferent arterioles
– Cause changes in vessel diameter
Glomerular Filtra1on Rate
• Volume of filtrate produced by both kidneys per minute
• Factors – Net filtra1on pressure – Permeability of corpuscular membranes
– Surface area for filtra1on • At any given filtra1on pressure, GFR will be directly propor1onal to the membrane permeability and surface area – 115 ml/min in women (166 L/day) – 125 ml/min in men (180 L/day)
En1re plasma volume is filtered 60 1mes a day

Control of GFR
Glucose Reabsorp1on
• Glucose and amino acids are reabsorbed at proximal tubule
• Carrier mediated transport can become saturated – 325 mg/min is transport maximum
• Normally only 125 mg/min of glucose per 100ml of filtrate in tubules (1 mg/ml)
• When glucose is 180 mg per 100ml of filtrate, glucose gets into urine – Renal plasma threshold for glucose
• Diabetes mellitus is when there is not enough secre1on of insulin
• Lots of urine to help get glucose out

Regula1on of Ion and Water Balance
• 180 L of filtrate produced each day
• 99% reabsorbed • Obligatory water loss
– 444 mL
• Primary ac1ve transport of Na+ out of the cells and into inters11al fluid – PCT – Collec1ng duct – Na+/K+/ATPase pumps
As Na+ and Cl‐ are reabsorbed, H2O follows passively by osmosis
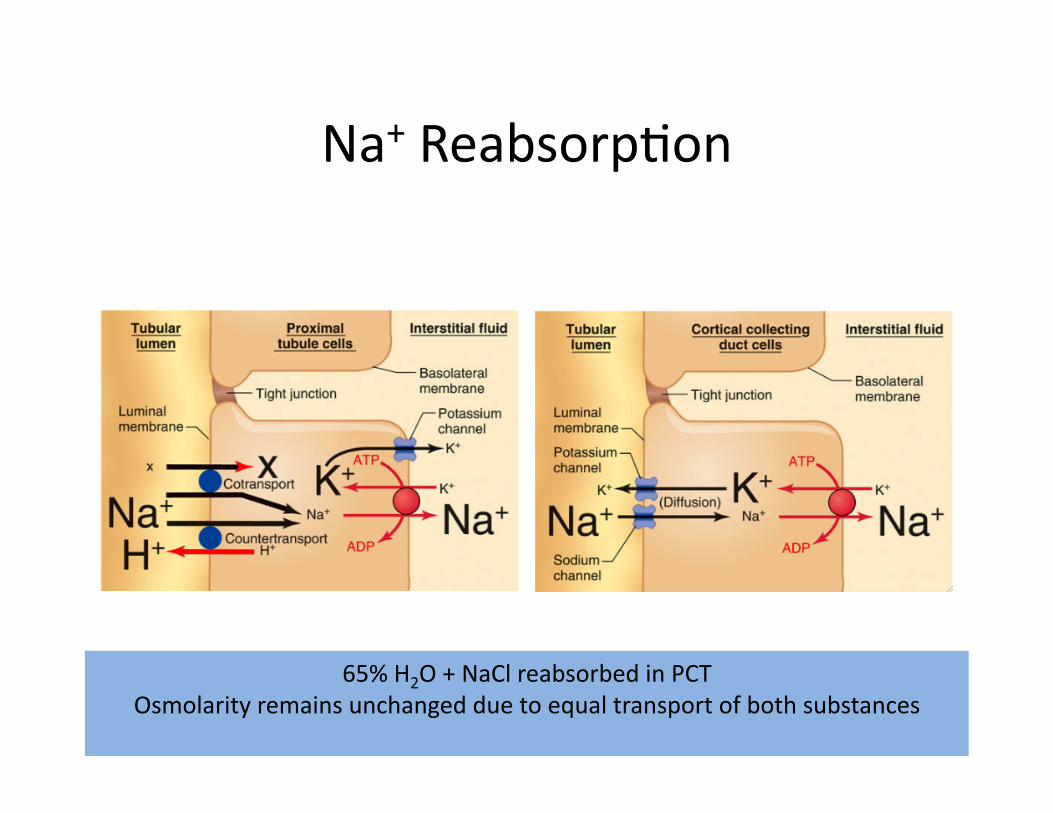
Na+ Reabsorp1on
65% H2O + NaCl reabsorbed in PCT Osmolarity remains unchanged due to equal transport of both substances

Coupling of H2O and Na+ Reabsorp1on
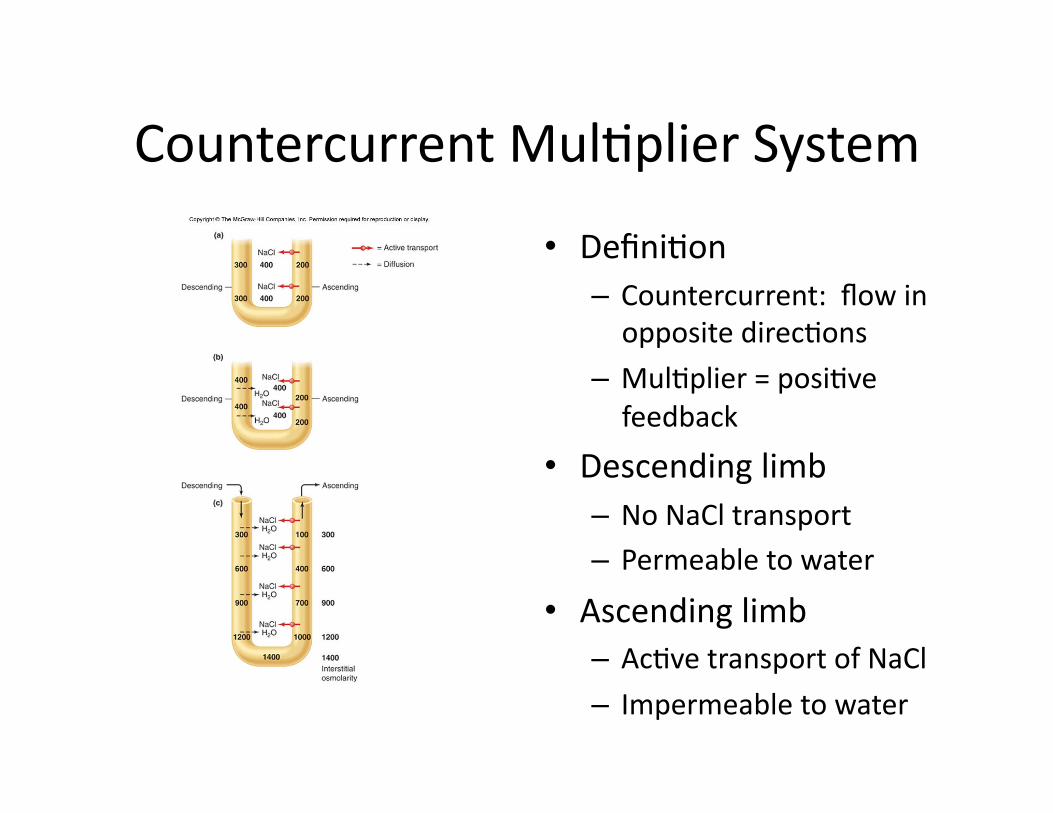
Countercurrent Mul1plier System
• Defini1on – Countercurrent: flow in opposite direc1ons
– Mul1plier = posi1ve feedback
• Descending limb – No NaCl transport – Permeable to water
• Ascending limb – Ac1ve transport of NaCl – Impermeable to water

Inters11al Fluid Osmolarity Gradient
• Collec1ng Ducts • Permeable to water, mostly impermeable to NaCl
• ADH increases number of water channels

Vasa Recta
• The hairpin loop structure of the vasa recta minimizes excessive loss of solute from the inters11um by diffusion
• Urea trapping • Effects of urea
– contributes to hypertonicity of 1ssues
Control of Na+ Reabsorp1on Aldosterone
• Role of aldosterone in Na+/K+ balance – Secreted by renal cortex – DCT – Na+ reabsorp1on
• aldosterone = Na+ reabsorbed =H20 = blood pressure
• When Na+ is reabsorbed, K+ is excreted
• 90% reabsorbed before DCT
• Without aldosterone – 8% reabsorbed – 2% filtered Na+ into urine
• With aldosterone – all Na+ reabsorbed
Control of Na+ Reabsorp1on Angiotensin II
• A component of the renin‐angiotensin system – Renin produced by JG cells
– Renin splits angiotensinogen (produced by the liver) into angiotensin I
– Angiotensin I converted to angiotensin II
• Angiotensin II – S1mulates secre1on of aldosterone
– Causes vasoconstric1on • Increases BP
– Levels are high during salt deple1on (Na+ levels are low) • Retension of Na+ and H20
• Increases BP

Control of Na+ Reabsorp1on Renin
• Renin acts as an enzyme that catalyzes spliing off of angiotensin I from angiotensinogen in plasma
• Juxtaglomerular apparatus – The macula densa
• Sensi1ve to a decrease in [Na+] in tubular fluid • Causes increased renin secre1on
– The juxtaglomerular (JG) cells • Sensi1ve to drop in BP • Secrete Renin
Control of Na+ Reabsorp1on Atrial Natriure1c Pep1de (ANP)
• Atrial Natriure=c Pep=de (ANP) produced by cardiac muscle cells in the atria
• Responds to high BP • Inhibits Na+ reabsorp1on in the kidney tubules • Can also act on renal blood vessels to increase GFR – Further increases Na+ excre1on
• Directly inhibits aldosterone secre1on – Further increases Na+ excre1on

Renal Regula1on of K+
• Cor1cal collec1ng ducts can secrete K+
• Normal ECF values range between 3.5‐5.0 mmol/L
• 90% reabsorbed in PCT • Without aldosterone
– 100% K+ reabsorbed in DCT
• With aldosterone – K+ secre1on into DCT & CD

Acid‐Base Balance
• Adults produce about 100 mmol/day of H+
• Goal: maintain rela1vely constant plasma pH in spite of daily varia1ons in produc1on of acids from metabolism and food intake
• Role of the kidney – Reabsorb all HCO3
‐ filtered and excre1ng H+ into urine • 90‐95% reabsorbed in PCT and DCT • Excre1ng 1‐2L of un‐buffered urine only eliminates 1mmol/day of H+
– Generate new HCO3‐
• Filterable phosphate is primary buffer anion in urine
• Nitrogen is excreted as ammonium rather than urea, sparing bicarbonate
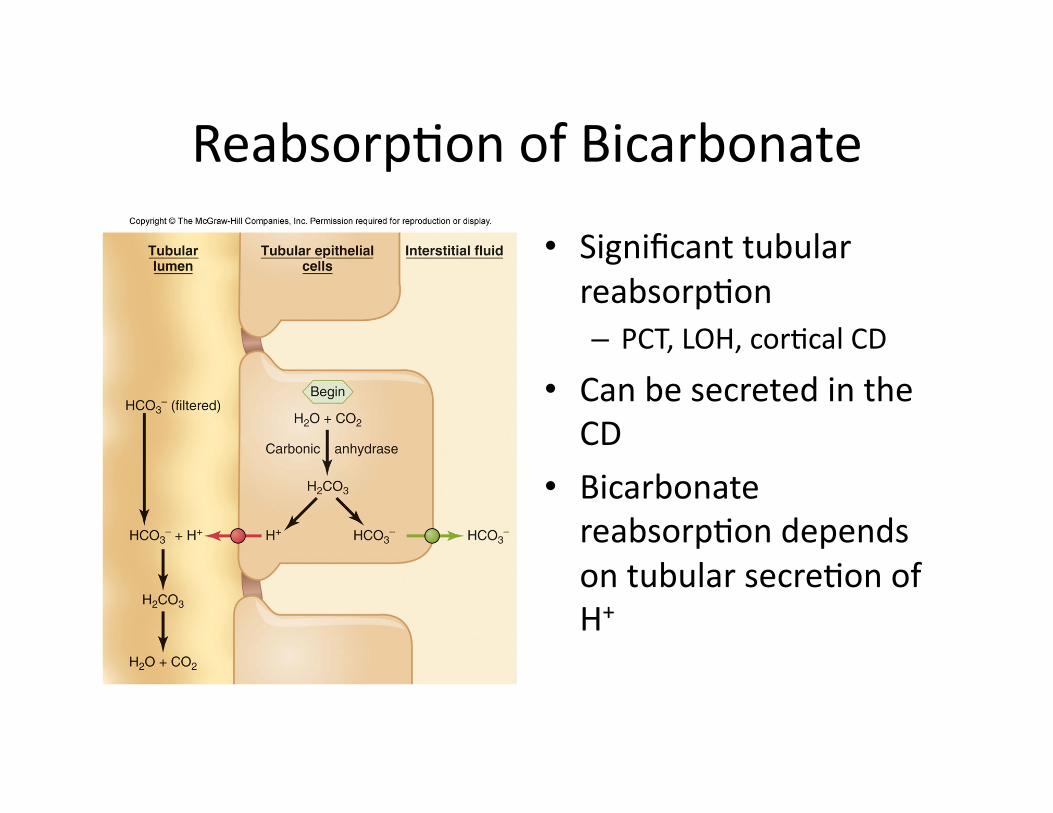
Reabsorp1on of Bicarbonate
• Significant tubular reabsorp1on – PCT, LOH, cor1cal CD
• Can be secreted in the CD
• Bicarbonate reabsorp1on depends on tubular secre1on of H+

Addi1on of New Bicarbonate
Tubular secre1on of H+ Renal metabolism of glutamine and excre1on of ammonium (NH4
+)

















