28

Outline● Relevant female anatomy● Relevant male anatomy● Female reproductive physiology● Male reproductive physiology● Physiology of fertilisation● Physiology of labour● Physiology of newborn

Female anatomy

Female anatomyUterus: fibromuscular organ divided into 3 layers, the endometrium, myometrium and serosa. Supplied by uterine artery (internal iliac artery branch). Inferiorly it is continuous with the cervix. Communicates with fallopian tubes at each cornu
Endometrium: mucous membrane which undergoes cyclical changes in structure and function in response to ovarian hormonal stimulation. In the first 14 days the endometrium proliferates; glands thicken and elongate under oestrogen influence (proliferative phase). In days 14-28, under the influence of progesterone, the glands swell and blood supply increases (secretory phase)
Myometrium: smooth muscle layer, relevant to menstruation and labour
Cervix: dense fibrous connective tissue, continuous with the uterus at internal os. The cervical canal opens into the vagina at external os
Fallopian Tubes: 2 tubes which can be divided into: isthmus, ampulla and infundibulum (withfimbriae)
Ovaries: supplied by ovarian artery (abdominal aorta branch). Outer cortex covered by germinal epithelium, contains follicles and theca cells. Inner medulla contains blood vessels and CT

Oogenesis

Oogenesis (Simply: diploid cell ‐> haploid cell)
The development of mature ova (haploid) from their primitive precursors: oogonia(diploid)Oogonia divide by mitosis during foetal life to produce primary oocytes. This is the only source of the mature ova (22 autosomes and 1 sex chromosome) which begin to develop from puberty, in contrast with the continuous replication of spermatogonia in post pubertal males. Primary oocytes begin the first meiotic division before birth. All further development arrests until puberty, when the first meiotic division is completed. This produces a cytoplasm and nutrient rich secondary oocyte (haploid, with 2 copies of each unpaired chromosome) and a small polar body of chromosomal material.Formation of the secondary oocyte is delayed until just prior to ovulation, (stimulated by LH surge) and the secondary oocyte only completes its second meiotic division if it isfertilised.

● 5-15 Primary follicles begin to develop at the start of each menstrual cycle● Granulosa cells multiply and secrete fluid which pools to form the Antrum
producing the Graafian/Antral follicle● After 7-10 days one follicle become dominant and enlarges further● Remaining follicles become atretic● At ovulation the developing follicle distorts the ovarian surface. Rapid fluid
accumulation increases the intrafollicular pressure and proteolytic enzymes digest the overlying tissue and the egg is released
Follicular development


Hypothalamus‐pituitary‐ovarian axisHypothalamus acts as central processing unit of the reproductive system; neuronal stimuli from the cerebral cortex are converted by the hypothalmus into pulses of GnRH.At the end of the menstrual cycle, oestrogen levels are low, stimulating GnRH release.
The pituitary gland’s anterior lobe secretes luteinising hormone (LH) and follicle stimulating hormone (FSH) which are also known as GONADOTROPHINS. They are released under the influence of GnRH.
FSH stimulates follicular development by activating granulosa cell division and secretion of oestrogen. The increasing amount of oestrogen produced by the developing follicles acts to reduce GnRH and gonadotrophin levels by negative feedback; such that only one follicle, the dominant or graafian follicle can ovulate.
LH has 3 known functions: 1. Stimulates theca cells, and thus the secretion of androgens, which act as precursors for the synthesis of oestrogens.2. Triggers ovulation of the dominant follicle – ‘LH surge’, when suddenly, increasing oestrogen levels trigger a positive feedback mechanism, causing a surge in LH and FSH, and thus ovulation.3.Additionally, LH stimulates luteinisation of the follicular remnants to form the corpus luteum, which secretes oestrogen and progesterone to support the endometrium, and the potential developing embryo.

Oestrogen and ProgesteroneOestrogen Progesterone
Secondary sexual characteristics‐thelarche (breast development)‐adrenarche (axillary and pubic hair development)
Menstrual cycle: induces formation of secretory endometrium during which the glands become saw toothed and tortuous, producing glycogen suitable for implantation
Menstrual cycle: development of mature dominant follicle and ovulation, and preparation of proliferative endometrium
Induces lobuloalveolar maturation of the breasts in conjunction with prolactinduring pregnancy to allow for milk production and lactation
Bone protection Promotes conditions in utero suitablefor pregnancy
Duct growth of breasts in pregnancy Thickens cervicalmucus
Promotes conditions in utero suitablefor pregnancy
Menstrual Cycle

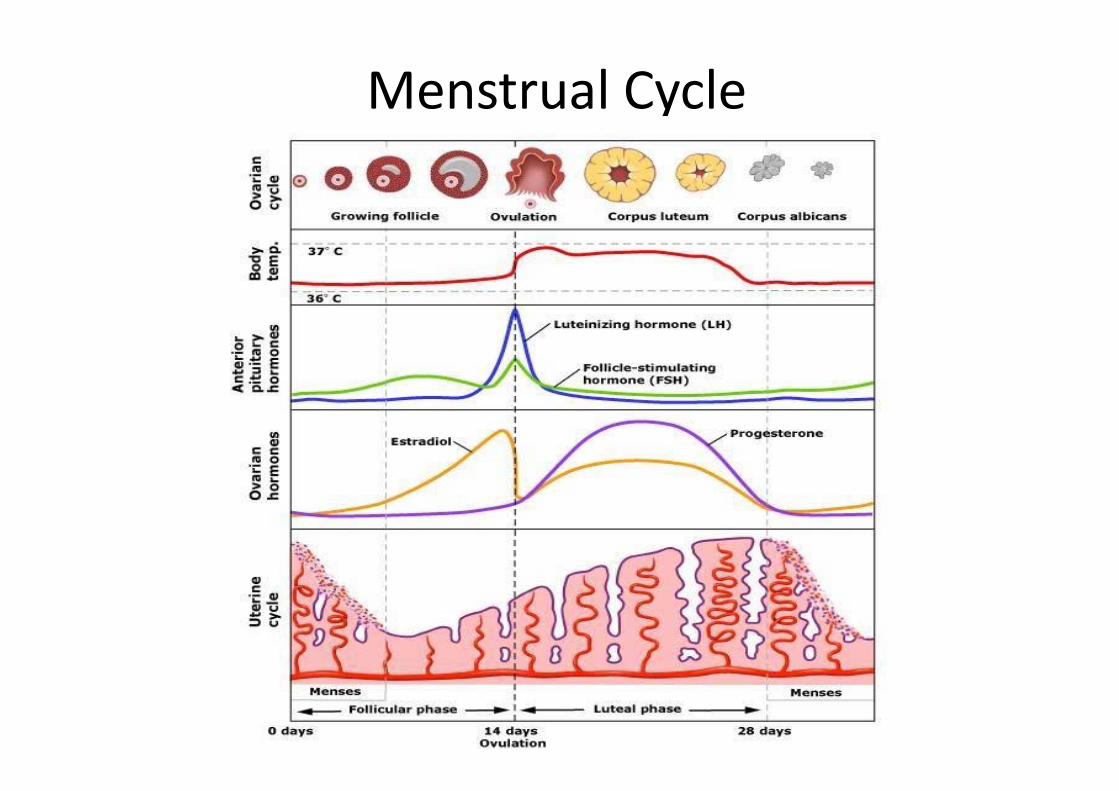
Menstrual CycleDays 1-4: Menstruation.Endometrium is shed as hormonal support is withdrawn. Myometrial contraction expels the endometrial lining. Oestrogen and progesterone concentration falls
Days 5-13: Proliferative Phase.Pulses of GnRH from hypothalamus increase, stimulating release of FSH and LH inducing follicular growth. Oestrogen and progesterone levels rise, thus suppressing thegonadotrophins by negative feedback such that only one dominant follicle matures.However, as oestrogen continues to rise, a switch to a positive feedback loop on the hypothalamus and pituitary causes an LH surge, stimulating ovulation. The high oestrogen causes the endometrium to become proliferative, and the glands to proliferate.
Days 14-28: secretory/luteal phaseFormation of the corpus luteum: the granulosa and theca cells of the ovary become swollen by fat droplets, and the structure becomes more vascular.The corpus luteum secretes oestrogen, but significantly more progesterone. This induces secretory changes in the endometrium, to support an implanted embryo. If the oocyte is not fertilised, the lack of placental b-hcg to support the corpus luteum causes it to fail, and hormonal withdrawal. The endometrium thus breaks down in menstruation, and the cycle starts again.

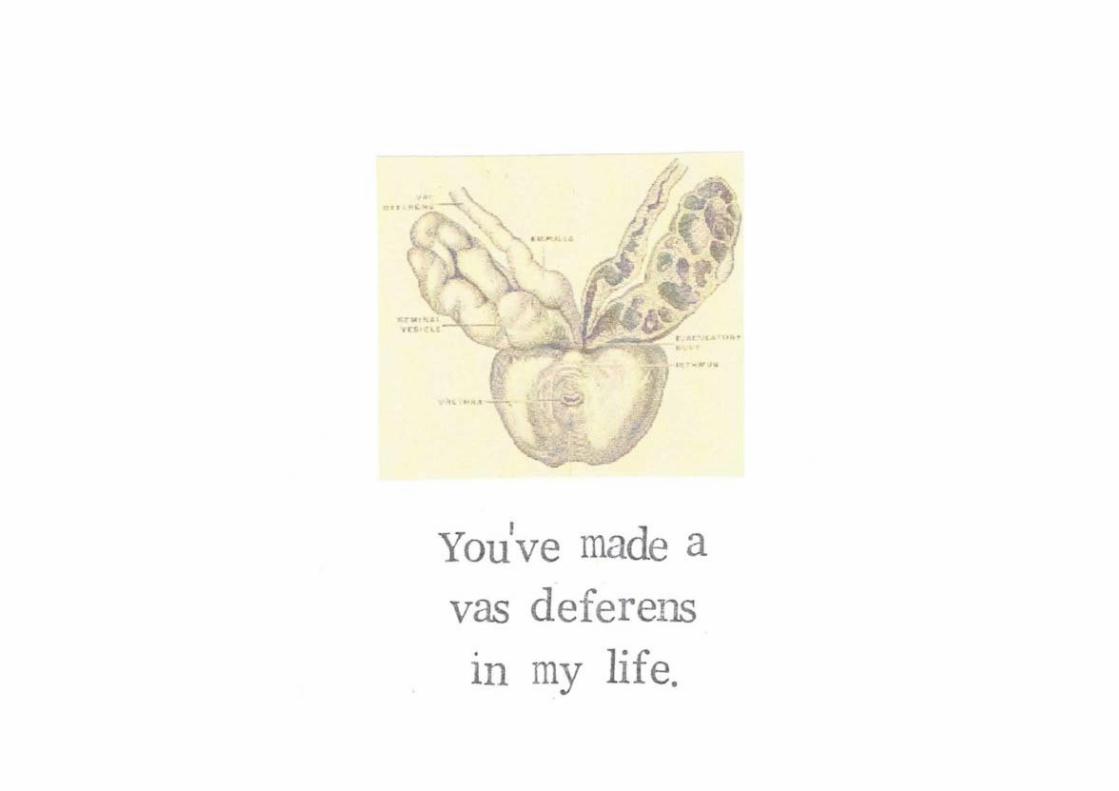
Male anatomyTestes:Exo and endocrine function, production of testosterone and spermatogenesis
Seminal vesicle:Contributes to 70% of semen production and importantly provides fructose
Prostate gland:Contributes to 30% of semen production and creates alkalinity of semen
Epididymis:Storage and maturation ofspermatozoa
Vas deferens:Causes propulsive force of spermatozoa into the Ejaculatory duct where itmixes with semen before ejaculation

Spermatogenesis
● Spermatogenesis occursin seminiferous tubules found in the testes
● Spermatids are deposited in the lumen of the seminiferous tubules to undergo maturation intospermatozoa
● The most mature cells arethen stored in theepididymis
● Supportive cells – Leydigand Sertoli cells
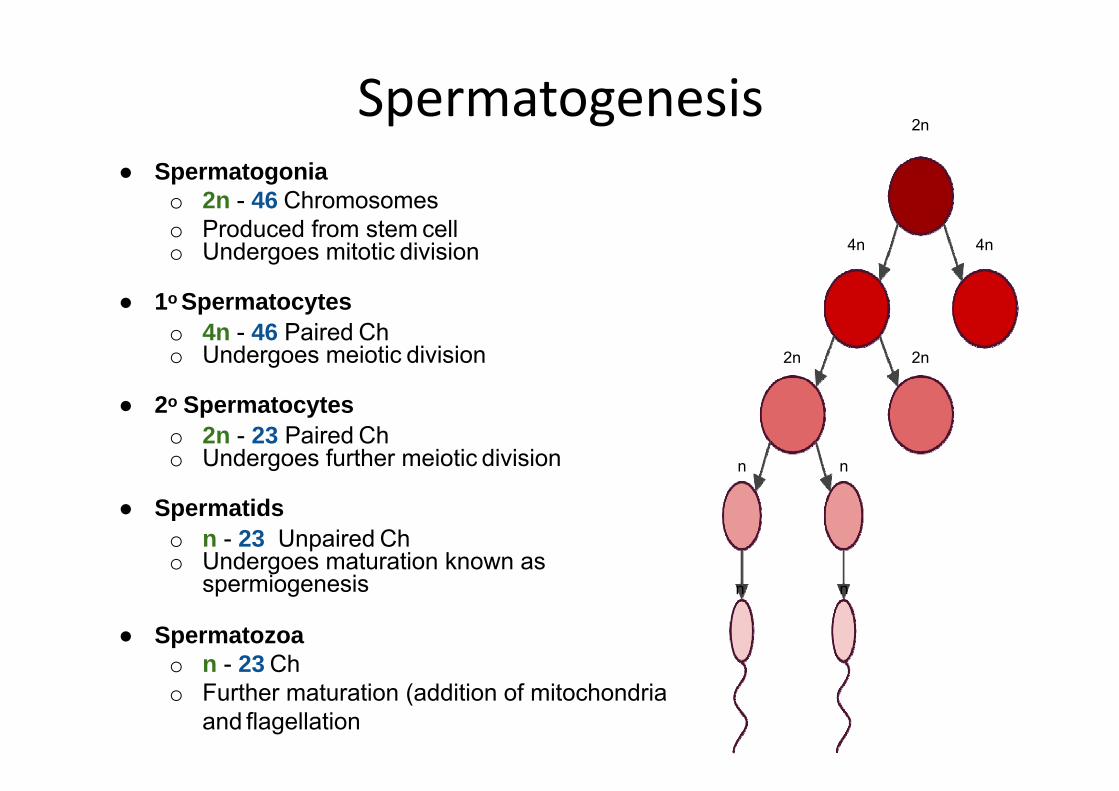
Spermatogenesis● Spermatogonia
o 2n - 46 Chromosomeso Produced from stem cello Undergoes mitotic division
● 1o Spermatocyteso 4n - 46 Paired Cho Undergoes meiotic division
● 2o Spermatocyteso 2n - 23 Paired Cho Undergoes further meiotic division
● Spermatidso n - 23 Unpaired Cho Undergoes maturation known as
spermiogenesis
● Spermatozoao n - 23 Cho Further maturation (addition of mitochondria
and flagellation
4n
2n
4n
2n 2n
n n
n n

Fertilisation• Following ovulation the ovum is propelled by cilia lining the fallopian tube• Spermatozoa must penetrate the mucus of the vagina - this occurs at ovulation when the ratio
of oestrogen to progesterone is highest, and the mucus is thinner and less dense• Uterus contracts to aid spermatozoa motility to the fallopian tubes• Fallopian tubes contract by retrograde peristalsis to increase chances of fertilisation• 300 X 10^6 spermatozoa per ejaculate and ‘capacitation’ happens in reproductive tract• Fertilisation requires the sperm to penetrate the corona radiata and zona pellucida which
surround the ovum. This is aided by:1. Sperm motility to force their way between granulosa cells of corona radiata2. Digestive acrosomal enzymes break down zona pellucida
When the first spermatozoa contacts theplasma membrane of the secondary oocyte, the zona pellucida changes chemically, becomig impermeable to othersperm. This completes the 2nd meiotic division, and a diploid zygote is formed.
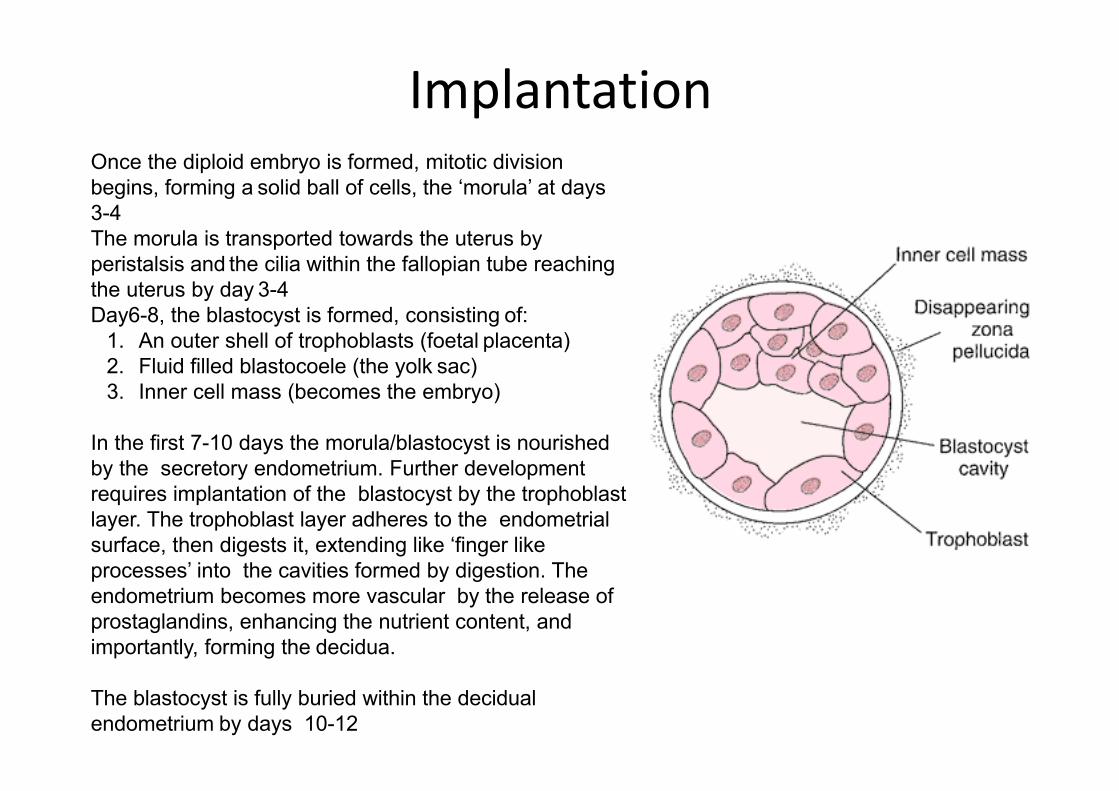
ImplantationOnce the diploid embryo is formed, mitotic division begins, forming a solid ball of cells, the ‘morula’ at days3-4The morula is transported towards the uterus by peristalsis and the cilia within the fallopian tube reachingthe uterus by day 3-4Day6-8, the blastocyst is formed, consisting of:
1. An outer shell of trophoblasts (foetal placenta)2. Fluid filled blastocoele (the yolk sac)3. Inner cell mass (becomes the embryo)
In the first 7-10 days the morula/blastocyst is nourished by the secretory endometrium. Further development requires implantation of the blastocyst by the trophoblast layer. The trophoblast layer adheres to the endometrial surface, then digests it, extending like ‘finger like processes’ into the cavities formed by digestion. The endometrium becomes more vascular by the release of prostaglandins, enhancing the nutrient content, and importantly, forming the decidua.
The blastocyst is fully buried within the decidual endometrium by days 10-12

PlacentaFunctions:• nutrient and gas exchange• removal of fetal waste products by diffusion into maternal blood• partial protection from teratogens and infectious agents in maternal circulation• endocrine function, including secreting oestrogen and progesterone
NB soon after implantation, the chorion of the developing placenta secretes BHCG, which acts on the corpus luteum to prevent regression. Thus oestrogenand progesterone productionfrom the CL continues until theplacenta becomes the chiefsource (approx 3 months into the pregnancy)

Placental Development• After the first few weeks the placenta must develop to sustain the growing foetus• The chorion erodes the maternal capillaries of the decidua so more blood filled spaces develop, into which the chorion’s finger like processes will project, forming placental villi• Fetal blood from umbilical arteries (deoxy) is circulated through the chorionic capillaries within these villi (site of foetal‐maternal exchange) and is then recirculated by the umbilical vein (oxy)• By week 5, the placenta is well established with both fetal (chorionic)and maternal (decidual) components• The maternal and fetal blood are separated by chorionic tissueand capillary endothelium providing a protective barrier and allows necessary exchange.

Labour● If full term, between 37 and 42 weeks gestation
● It is split into 3 stages:
1. Onset of contractions until full cervical dilatation2. Full cervical dilatation to birth of child3. Delivery of placenta

1st stage (3-24 hrs)• Dilatation of the cervix up to 10cm• As the baby’s head descends => release of oxytocin from
the posterior pituitary• Oxytocin driven with positive feedback loop causes
contraction that increase in frequency & strength with time• Prostaglandins also cause uterine contraction• Relaxin softens connective tissue to ease passage of baby
2nd stage (30-120 mins)
• Delivery of baby through vaginal tract with the aid of abdominal and uterine muscle contraction
• No longer than 2 hours in nulliparous and 1 hour in multiparous
3rd stage (15-30mins)
• Delivery of placenta• Essential that entirety of placenta is evacuated• Followed by uterine contraction
Oxytocin
Myometrial contraction
Cervical stretch
Spinal afferents
Hypothalamus
Post. pituitary
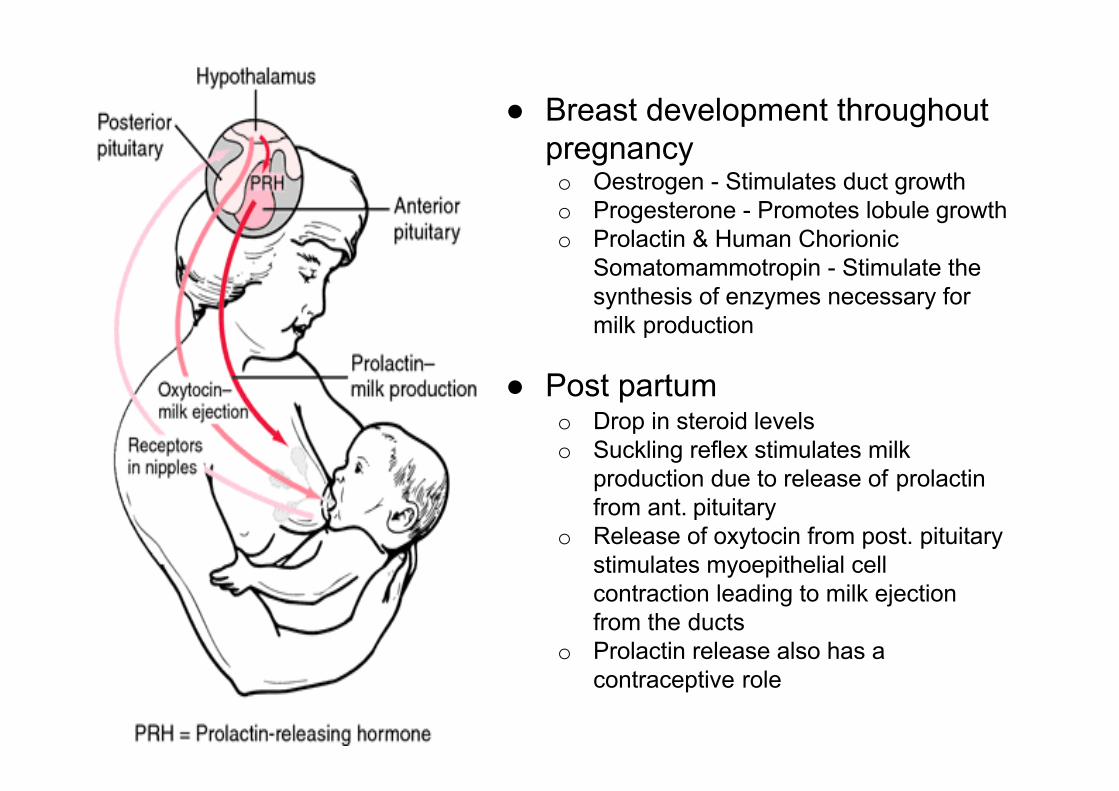
● Breast development throughoutpregnancyo Oestrogen - Stimulates duct growtho Progesterone - Promotes lobule growtho Prolactin & Human Chorionic
Somatomammotropin - Stimulate the synthesis of enzymes necessary for milk production
● Post partumo Drop in steroid levelso Suckling reflex stimulates milk
production due to release of prolactinfrom ant. pituitary
o Release of oxytocin from post. pituitary stimulates myoepithelial cell contraction leading to milk ejection from the ducts
o Prolactin release also has a contraceptive role

Newborn cardiac changes
● Foetal shunts:o Ductus Venosuso Foramen Ovaleo Ductus Arteriosus
● Changes at birtho Pulmonary vascular resistance decreases => pulmonary blood flow
increases => pressure in RA + RV fallo Systemic vascular resistance increases => increased systemic BPo R→L shunt moves to L→R and closes foramen ovaleo Closure of Ductus Arteriosus happens within 1-8 dayso Closure of Ductus Venosus happens within 1-3 hours



Melissa is a 25 year old female who was involved in a fight on a night out. You decide to x-ray Melissa’s facial bones to exclude possible fracture. As a precaution you ask about her menstrual history.
Her last menstrual period was 8 weeks ago. You decide to order a pregnancy test.1. What chemical substance is found in the urine to confirm early pregnancy, and by what tissue is it synthesised ? (2 marks)
2. What 3 important items of advice about nutrition and life-style should be given to a woman in early pregnancy ? (3 marks)
EXAMPLE QUESTIONS

1. BHCG is detected in the urine from 2-3 weeks of fertilisation soon after implantation the chorion of the developing placenta secretes this hormone. BHCG acts on the corpus luteum so that instead of regressing after ovulation as normal it is stimulated to develop further when a pregnancy is established to prevent the fall in progesterone and oestrogen.
2. Folic acid, stop smoking, stop alcohol intakeAvoid soft cheeses, unpasteurised milk, raw eggs or meat and others… Avoid those with chickenpox and shinglesRationalise medication eg Diabetes/Epilepsy Rubella status and vaccinations
ANSWERS














![Male Reproductive Physiology[1]](https://static.documents.pub/doc/80x56/55cf8e9d550346703b93f717/male-reproductive-physiology1.jpg)


