Page 1
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018
Integrated Report
ResCu
Non-interventional study to monitor effectiveness, tolerability, and quality of life in real world patients in Crohn’s disease or ulcerative
colitis treated with Remsima®
Type of study: Non-interventional study according to § 4 (23) 3 German Medicinal
Products Act (AMG)
Study code: IFX9502
Indication: Crohn’s disease and ulcerative colitis
Study drug: Remsima® 100 mg powder for concentrate for solution for infusion
Active substance: Infliximab
Survey data: First Examination: 11th of June 2015
Last Examination: 31st of March 2017
Responsible
person for
medical affairs:
Mundipharma GmbH
Mundipharmastraße 2
65549 Limburg (Lahn)
Responsible
person for
statistics:
ANFOMED Gesellschaft für angewandte Forschung in der Medizin mbH
Röttenbacher Straße 17
91096 Möhrendorf
Page 2
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 I
Synopsis
Title Non-interventional study to monitor effectiveness, tolerability, and quality of life in real world patients in Crohn’s disease or ulcerative colitis treated with Remsima®.
Country Germany
Type of study Non-interventional study according to § 4 (23) 3 German Medicinal Products Act (AMG);
Multicenter, prospective and observational study
Clinical phase Post Marketing Authorisation, non-interventional
Indication Crohn’s disease and ulcerative colitis
Study drug Remsima® 100 mg powder for solution for infusion
Active substance Infliximab
Area of application Treatment of moderate to severe, active Crohn‘s disease, treatment of fistulising, active Crohn‘s disease and moderate to severe active ulcerative colitis in adult patients who have not responded despite a full and adequate course of therapy with conventional treatment or who are intolerant to or have medical contraindications for such therapies.
Study objectives The aim of the non-interventional study was to document the efficacy and safety of Remsima® in patients with inflammatory bowel disease under real life conditions. The influence on quality of life, fatigue, depression, and abdominal pain should be documented.
End point of study Primary end points of study
The activity of Crohn‘s disease and ulcerative colitis were determined with Harvey-Bradshaw-Index (HBI) and Mayo-Score.
Secondary end points of study
The influence on quality of life was documented by the Inflammatory Bowel Disease Questionnaire (IBDQ-D), fatigue by the Brief Fatigue Inventory (BFI), depression by the General Depression Scale (long version, ADS-L), and abdominal pain by the Short-form McGill (SF-McGill) questionnaire.
Study sites 70 specialists for gastroenterology planned
70 specialists for gastroenterology involved
Sample size 400 patients planned
381 patients enrolled and statistically analysed
Study duration 28th of September 2015 until 15th of May 2017 (after extension)
First Patient First Visit 11th of June 2015 (included retrospectively)
Last Patient Last Visit 31st of March 2017
Observation period An observational period per patient of about 14 weeks was intended.
Administration According to the usual therapeutic procedure of the attending physician and in accordance with the authorized indications and summary of product characteristics (SmPC).
Page 3
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 II
Dosage According to SmPC
Procedure of the study
Patients were included in the study when physicians decided in advance to start treatment with Remsima® according to the local SmPC. The physician had to obtain patient‘s written consent. Data were documented in following survey periods:
• Baseline of data collection (Visit 0): before start of treatment
• Follow-up data collection (Visit 1): about 2 weeks after start of treatment
• Follow-up data collection (Visit 2): about 6 weeks after start of treatment
• Final survey of data collection (Visit 3): about 14 weeks after start of treatment
Patient questionnaire forms were handed out at baseline, at follow-up examinations and at final examination to be filled out by the patient. These forms had to be returned to the attending physician at the same examination.
Survey data • Date of visits
• Demographic data
• Medical history of CIBD (chronic inflammatory bowel disease)
• Assessment of severity of acute episode (HBI, Mayo-Score)
• Localisaton and description of acute episode
• Imaging diagnostics (if available)
• Laboratory parameters (if available in the routine clinical practice)
• (Pre-) treatment of CIBD
• Treatment with Remsima®
• Concomitant diseases and medication
• Questionnaires for evaluation of quality of life (IBDQ-D)
• Questionnaires for evaluation of influence on fatigue (BFI)
• Questionnaires for documentation of depression (ADS-L)
• Questionnaires for evaluation of abdominal pain (SF-McGill)
• Adverse events and adverse drug reactions
• Assessment of Remsima® therapy by the attending physician and the patient
Statistical Methods Data processing and statistical analysis were performed with the SAS™ program system. Taking into account the non-interventional character of the study, the statistical analysis was performed in a descriptive and explorative way. Collected variables were illustrated using graphical diagrams and frequency or parameter tables. If reasonable, lists of individual patient data were prepared. Adverse events/adverse drug reactions were coded according to MedDRA. All cases were listed in frequency tables based on preferred terms and system organ classes. A line listing of all events was prepared.
Adverse Drug Reactions
Any adverse drug reaction (serious or non-serious) during the non-interventional study, in which relation to Remsima® therapy could not be excluded, had to be, independet of severity, carefully documented in the „ADR report section“ of the eCRF within 24 hours. This ADR report was then automatically forwarded to the drug safety department of ANFOMED GmbH and after processing to Mundipharma GmbH. Additionally, all adverse events (AE), in which relation to Remsima® therapy could be excluded, had to be documented in the eCRF.
Page 4
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 III
Principal investigator
Scientific Advisor
Summary of results
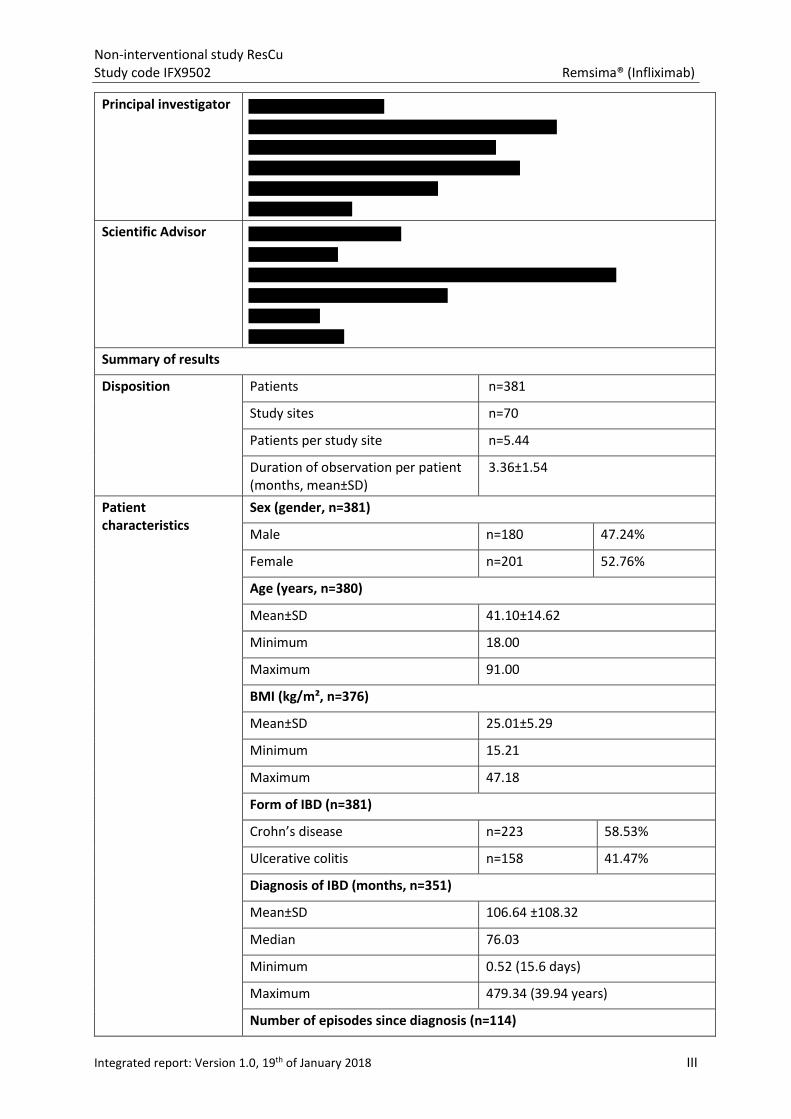
Disposition Patients n=381
Study sites n=70
Patients per study site n=5.44
Duration of observation per patient (months, mean±SD)
3.36±1.54
Patient characteristics
Sex (gender, n=381)
Male n=180 47.24%
Female n=201 52.76%
Age (years, n=380)
Mean±SD 41.10±14.62
Minimum 18.00
Maximum 91.00
BMI (kg/m², n=376)
Mean±SD 25.01±5.29
Minimum 15.21
Maximum 47.18
Form of IBD (n=381)
Crohn’s disease n=223 58.53%
Ulcerative colitis n=158 41.47%
Diagnosis of IBD (months, n=351)
Mean±SD 106.64 ±108.32
Median 76.03
Minimum 0.52 (15.6 days)
Maximum 479.34 (39.94 years)
Number of episodes since diagnosis (n=114)
Page 5
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 IV
Mean±SD 4.73±6.18
Minimum 1.00
Maximum 30.00
Intestinal resection due to CIBD (n=378)
Yes n=61 16.14%
No n=317 83.86%
Number of intestinal resections (n=378)
Mean±SD 0.20±0.51
Minimum 0.00
Maximum 3.00
Duration of acute episode (months, n=374)
Mean±SD 14.34±43.72
Median 2.93
Minimum 0.00
Maximum 380.20 (31.68 years)
Hospitalization due to acute episode (n=375)
Yes n=82 21.87%
No n=293 78.13%
Duration of hospitalization (weeks, n=82)
Mean±SD 2.51±3.50
Median 1.43
Minimum 0.14
Maximum 20.00
Pre-treatment of acute episode (n=381)
Without pre-treatment n=127 33.33%
With pre-treatment n=254 66.67%
Continued pre-treatment of acute episode (n=381)
Without treatment n=240 62.99%
With treatment n=141 37.01%
Imaging procedures (n=381)
Without imaging procedures n=123 32.28%
With imaging procedures n=258 67.72%
- Endoscopy n=223 58.53%
- Sonography n=110 28.87%
- Magnetic resonance imaging n=25 6.56%
Page 6
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 V
…
Laboratory parameters
Erythrocytes (Mio/µl) n=327 4.52 (±0.56)
Leukocytes (Tsd/µl) n=335 9.24 (±3.80)
Thrombocytes (Tsd/µl) n=334 344.77 (±129.40)
Hemoglobin (mmol/l) n=350 8.30 (±1.51)
Hematocrit (%) n=301 39.33 (±5.42)
Serum iron (µmol/l) n=130 12.96 (±6.88)
Ferritin (µg/l) n=140 98.27 (±108.72)
Transferrin (mg/dl) n=71 268.62 (±56.15)
Transferrin saturation (%) n=74 21.29 (±15.87)
Urea (mg/dl) n=94 18.10 (±14.22)
Creatinine (mg/dl) n=242 0.85 (±0.22)
C-reactive protein (mg/l) n=345 37.69 (±80.59)
Erythrocyte sedimentation rate (mm)
n=72 25.21 (±19.70)
Calprotectin (µg/g) n=147 747.20 (±831.44)
Pre-treatment of underlying IBD (n=381)
Without pre-treatment n=55 14.44%
With pre-treatment n=326 85.56%
- Immunosuppressive agents n=193 50.66%
- Antidiarrheals, intestinal anti-inflammatory/antiinfective agents
n=184 48.29%
- Corticosteroids for systemic use n=89 23.36%
...
Concomitant disease (n=381, MedDRA preferred term)
Without concomitant disease n=281 73.75%
With concomitant disease n=100 26.25%
- Hypertension n=18 4.72%
- Depression n=8 2.10%
- Hypothyroidism n=8 2.10%
...
Treatment of concomitant disease (n=381, ATC anatomical main group)
Page 7
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 VI
Without treatment n=302 79.27%
With treatment n=79 20.73%
- Agents acting on the renin-angiotensin system
n=14 3.67%
- Corticosteroids for systemic use n=11 2.89%
- Drugs for acid related disorders n=8 2.10%
...
Reason for the prescription of Remsima® (n=381)
No reason specified n=4 1.05%
Reason specified n=377 98.95%
- Low effectiveness of the previous medication
n=240 62.99%
- Due to contraindication or intolerance to conventional therapy
n=92 24.15%
- Due to low tolerability of the previous medication
n=37 9.71%
...
Treatment with Remsima®
Remsima® Dose (mg/kg, patients with infusion only)
Mean±SD Minimum Maximum
Visit 0 (n=376) 5.09(±0.62) 3.00 10.00
Visit 1 (n=244) 5.07(±0.47) 3.00 7.81
Visit 2 (n=252) 5.13(±0.53) 3.00 9.57
Visit 3 (n=238) 5.22(±0.93) 2.90 10.00
<5mg/kg <5mg/kg <5mg/kg
Visit 0 (n=376) 4.52% 84.04% 11.44%
Visit 1 (n=244) 5.33% 78.69% 15.98%
Visit 2 (n=252) 3.57% 79.76% 16.67%
Visit 3 (n=238) 5.04% 77.31% 17.65%
Premature end of Remsima® treatment (n=381)
Without premature end of therapy n=336 88.19%
Premature end of therapy n=45 11.81%
- Adverse drug reaction n=31 8.14%
- Lack of efficiency n=7 1.84%
- At patient’s request n=7 1.84%
...
Treatment of underlying IBD during the study (n=381)
Page 8
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 VII
Without treatment n=173 45.41%
With treatment n=208 54.59%
- Antidiarrheals, intestinal anti- inflammatory/antiinfective agents
n=128 33.60%
- Corticosteroids for systemic use n=75 19.69%
- Immunosuppressive agents n=66 17.32%
...
Hospitalization during the study because of an acute episode (n=364)
With hospitalization n=13 3.57%
Without hospitalization n=351 96.43%
Duration of hospitalization during the study (weeks, n=12)
Mean±SD 1.48±0.93
Minimum 0.29 (2 days)
Maximum 4.00
Imaging procedures during the study (n=366)
No n=321 87.70%
Yes n=45 12.30%
- Sonography n=26 7.10%
- Endoscopy n=23 6.28%
...
Surgical measures of acute episode during the study (n=366)
Without surgical measure n=362 98.91%
With surgical measure n=4 1.09%
- Fistula drainage n=2 0.55%
- Abscess drainage n=1 0.27%
- Hemicolectomy n=1 0.27%
Results in effectiveness
Inflammatory bowel disease questionnaire (IBDQ)
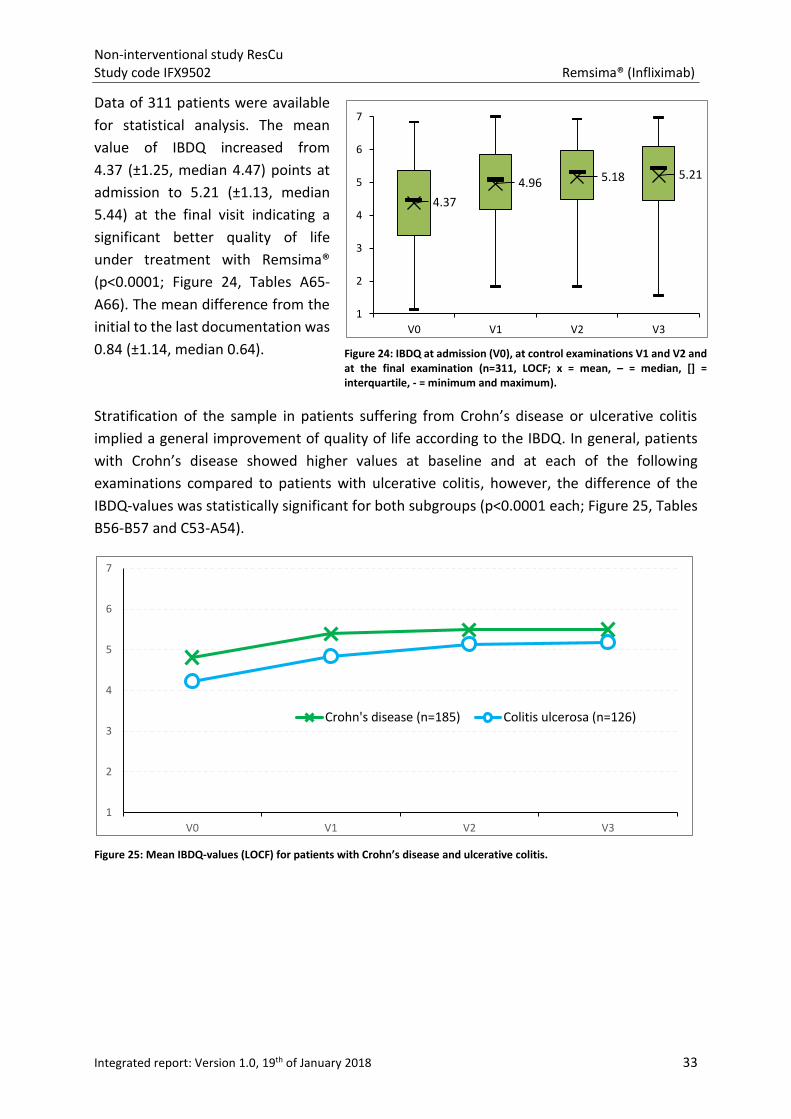
Data of 311 patients were available for analysis of life quality. The mean value of IBDQ total score (1 = poorest quality of life, 7 = best quality of life) increased from 4.37 (±1.25, median 4.47) points at admission to 5.21 (±1.13, median 5.44) at the end of the NIS indicating a significant better quality of life under treatment with Remsima® (p<0.0001). The mean difference from the first to the last documentation was 0.84 (±1.14, median 0.64).
Brief fatigue inventory (BFI)
A total of 318 patients were included in the analysis of fatigue. The mean value of BFI (0 = no impairment, 10 = complete impairment) decreased from 4.55 (±2.31, median 4.67) points at baseline to 3.62 (±2.30, median 3.28) points at the final examination. The mean reduction of BFI points from the
Page 9
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 VIII
initial to the last documentation was statistically significant (p<0.0001). BFI was reduced by 0.94 (±2.16, median 0.77) points.
General depression scale – long version (ADS-L)
ADS-L values of 277 patients were analyzed. A significant decrease of the ADS-L mean value was determined from admission (20.69±11.84, median 20.00) to final examination (15.91±11.70, median 14.00) with a difference of 4.79 (±11.09, median -4.00; p<0.0001). Nevertheless, mean values of ADS-L suggested an absence of clinically relevant depressive symptoms prior to Remsima® therapy and during the observation period.
Short-form McGill Pain questionnaire (SF-McGill)
VAS-values (0 = no pain, 100 = worst imaginable pain) of 282 patients were available for evaluation. A significant decrease of mean value was determined from the baseline (27.23±25.39, median 23.00) to the last documentation (18.22±22.16, median 7.00) showing a difference of 9.00 (±25.90, median 4.00; p<0.0001).
Disease activity of Crohn’s disease
Disease activity of Crohn’s disease was reduced during the treatment with Remsima®. The mean Harvey-Bradshaw-Index (HBI) of 6.91 (±4.14, median 7.00) points at baseline significantly decreased to 3.06 (±3.25, median 2.00) at the last documentation (p<0.0001), indicating a positive impact on disease activity from mild disease to remission state.
Disease activity of ulcerative colitis
Disease activity of ulcerative colitis was determined by Mayo score at baseline, at the follow-up examinations and at the final documentation. The mean score significantly decreased from 7.27 (±2.66, median 8.00) points to 2.81 (±2.59, median 2.00) points (p<0.0001) indicating a substantial improvement of disease activity from moderate-severe to mild disease.
Global assessment of efficacy
Efficacy of Remsima® was assessed once by the physicians and once by the patients themselves at the end of the NIS.
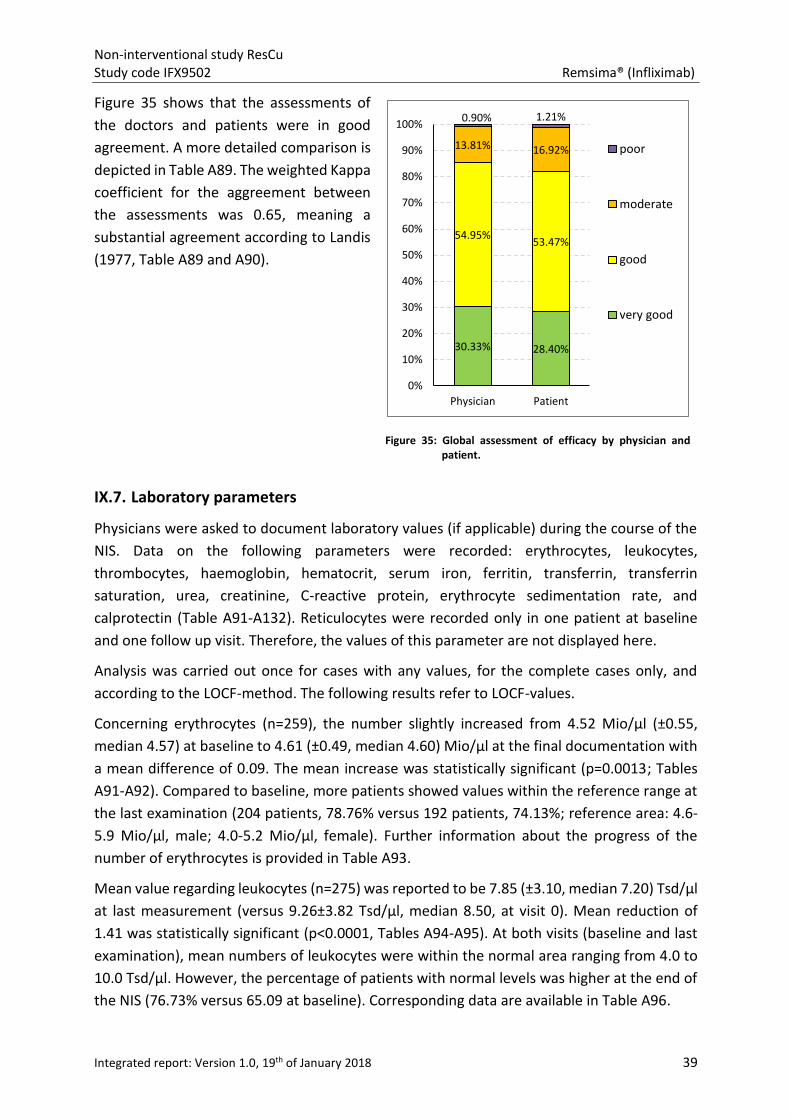
The attending physicians evaluated the effectiveness of Remsima® treatment as very good for 30.33% (101 patients) of the patients at the final documentation. The efficacy was documented to be good in 54.95% (183 patients) of the cases, moderate in 13.81% (46 patients) and poor in 0.90% (3 patients) of enrolled patients.
Concerning the result of patient’s assessment, the percentage distribution was comparable to the documentation of the physicians. Efficacy of Remsima® treatment was rated as very good by 28.40% (94 patients) of the patients at last assessment. The percentage of patients who assessed effectiveness as good was 53.47% (177 patients) whereas 16.92% (56 patients) of the patients assessed the efficacy as moderate and 1.21% (4 patients) as poor.
Laboratory parameters
Concerning erythrocytes, the number slightly increased from 4.52 Mio/µl (±0.55, median 4.57) at baseline to 4.61 Mio/µl (±0.49, median 4.60) at the final documentation with a mean difference of 0.09. The mean increase was statistically significant (p=0.0013). Compared to visit 1, more patients showed
Page 10
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 IX
values within the reference range at the last examination (204 patients, 78.76% versus 192 patients, 74.13%).
Mean value regarding leukocytes was reported to be 7.85 (±3.10, median 7.20) Tsd/µl at admission (versus 9.26 Tsd/µl at visit 1). Mean reduction of 1.41 was statistically significant (p<0.0001). At both visits (baseline and last examination), mean numbers of leukocytes were within the normal area. However, the percentage of patients with normal levels was higher at the end of the NIS (76.73% versus 65.09% at baseline).
Number of thrombocytes significantly decreased by 46.24 (±92.64) from 345.63 (±124.06, median 317.50) Tsd/µl at baseline to 299.39 (±97.03, median 281.50) Tsd/µl at the final documentation (p<0.0001). 55.11% of the patients had normal thrombocyte levels at the end of the NIS (versus 41.61% at start of Remsima® therapy).
Haemoglobin concentration was documented to be 8.28 (±1.52, median 8.20) mmol/l at admission and 8.57 (±1.91, median 8.32) mmol/l at the final documentation, respectively. The mean value significantly increased by 0.30 (±2.05, p<0.0001). Compared to the start of the NIS, more patients showed values within the reference area: 149 patients (51.38%) at visit 1 and 170 patients (58.62%) at last visit, respectively.
Hematocrit proportion was comparable between admission and final examination. Mean value was reported to be 39.04 (±4.59, median 39.90) % at visit 1. At the end of the study, the mean value was 39.68 (±5.16, median 40.00) % displaying an increase of 0.64 percentage points under treatment with Remsima®. At baseline, 48.05% of the patients had a hematocrit proportion within the normal range. At the last visit, a higher percentage of patients showed normal values (59.74%).
Regarding serum ion, a mean concentration of 12.74 (±7.05, median 11.47) µmol/l was recorded at baseline. The mean value slightly increased by 1.42 (±8.83) during the course of the NIS and was found to be 14.17 (±7.61, median 13.15) µmol/l at the end of the study. Number of patients with values within the reference area increased from admission to the last visit with percentages of 61.63% compared to 66.28%.
Ferritin levels decreased under therapy with Remsima®. Mean concentration was reported to be 108.32 (±128.74, median 69.50) µg/l at baseline and 89.18 (±106.42, median 65.00) µg/l at the end of the study (mean difference of 19.14 µg/l, ±113.56). Compared to baseline, the number of patients with reference values had increased during the NIS (73.17% versus 78.05% at the last visit).
Concerning transferrin concentration at baseline and final visit, a mean difference of 2.60 mg/dl (±52.89) was documented. Mean values slightly increased from 273.06 (±52.74, median 270.00) mg/dl up to 275.66 (57.26, median 280.00). 92.00% of the patients had normal transferrin levels at the end of the study (versus 88.00% at admission). Furthermore, transferrin saturation increased from 21.91 (±17.38, median 18.00) % at baseline to 20.65 (±12.18, median 18.00) % at last visit and the percentage of patients with normal levels between 18.0 and 45.0% simultaneously rose from 45.61% to 49.12%.
Mean urea level somewhat increased during the NIS and was reported as follows: 16.00 (±15.02, median 6.45) mg/dl at baseline and 16.20 (±13.54, median 8.05) mg/dl at the end of the study. The number of patients with a normal urea concentration was equal at visit 1 and final examination (26.47%
Page 11
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 X
each). Mean creatinine concentration did not change under the treatment with Remsima®. Mean value was reported to be 0.83 mg/dl at both visits (V1 and V3). However, number of patients with normal values increased during the observational time from 92.74% (baseline) to 96.09% (final documentation).
The amount of C-reactive protein was 34.97 (±75.42, median 10.70) mg/l at admission and decreased down to 21.11 (±38.65, median 5.62) mg/l at last visit. Mean reduction of 13.86 (±70.12) was statistically significant (p<0.0001). In contrast to a percentage of 48.56% at baseline, 63.67% of the patients had normal values at the end of the NIS.
Concerning the sedimentation rate of erythrocytes, mean values were higher at admission (24.85±21.78 mm, median 22.00 versus 16.96±15.93, median 11.50). Mean difference was 7.89 (±17.39). Number of patients with normal values rose from 37.50% to 62.50% during the observation.
Mean calprotectin concentration was reported to be 865.63 (±818.77, median 578.00) µg/g at baseline. Mean value decreased by 298.23 (±1158.06) down to 567.40 (±831.14, median 310.00) µg/g at last visit. A reference value ≤50.0 µg/g was achieved by 19.67% of the patients (versus 6.56% at baseline).
Results in safety
Global assessment of tolerability
Evaluation of tolerability of Remsima® was performed once by the physicians and once by the patients at the end of the NIS.
The attending physicians evaluated tolerability of Remsima® treatment at the last visit as very good for 40.72% (136 patients) and as good for 54.79% (183 patients) of the patients. The number of patients for whom tolerability was recorded to be moderate (3.59%, 12 patients) or poor (0.90%, 3 patients) was low.
Concerning the result of patient’s assessment, 116 patients (34.73%) rated tolerability as very good at last assessment. The number of patients who evaluated tolerability as good was 194 (58.08%). Only 19 (5.69%) and 5 patients (1.50%) assessed tolerability as moderate and poor, respectively, at last visit.
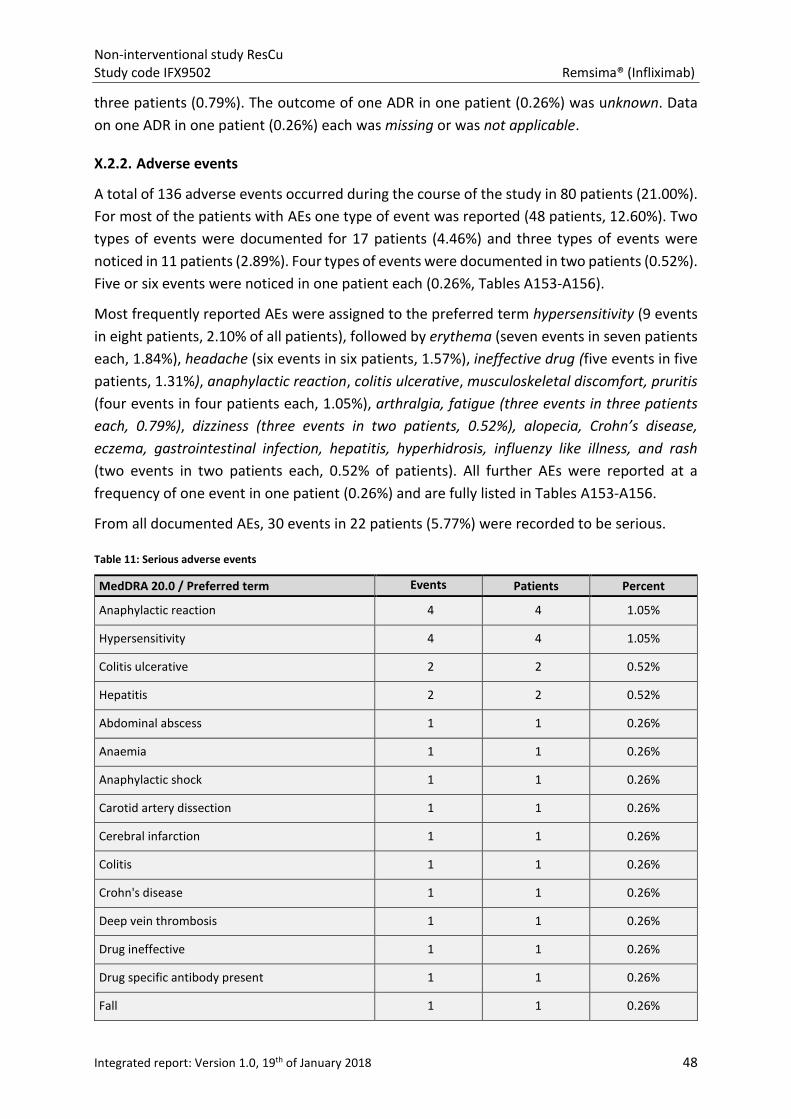
Adverse drug reactions
In this study, 136 adverse events (AE) were reported in 80 patients (21.00% of all patients) and 65 adverse drug reactions (ADR) occurred in 48 patients (12.60%) during the observation period of approximately 14 weeks. For the majority of the patients with ADRs one type of reaction was reported (37 patients, 9.71%). Most frequently reported ADRs were assigned to the MedDRA preferred term (PT) hypersensitivity (8 patients, 2.10% of all patients), followed by erythema (6 patients, 1.57%), ineffective drug (5 patients, 1.31%), anaphylactic reaction (4 patients, 1.05%), dizziness, alopecia, fatigue, pruritus, and rash (2 patients each, 0.52%). All further ADRs were reported at a frequency of one patient (0.26%).
The ADRs documented in this NIS were most often associated with the following MedDRA system organ classes (SOC): skin and subcutaneous tissue dirsorders (14 patients, 3.67% of all patients), immune system disorders (13 patients, 3.41%), general disorders and administration site conditions (8 patients, 2.10%), nervous system disorders (4 patients, 1.05%), gastrointenstinal disorders (3 patients, 0.79%), infections and infestations (3 patients, 0.79%), vascular disorders, musculoskeletal and connective tissue
Page 12
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 XI
disorders, and respiratory, thoracic and mediastinal disorders (2 patients each, 0.52%).
From all documented ADRs, 23 events in 18 patients (4.72% of all patients) were recorded to be serious. Hypersensitivity and anaphylactic reaction were the most frequently reported serious ADRs (4 events in 4 patients each, 1.05%). All other serious events occurred at a frequency of one and were reported for one patient in each case.
Seven events that occurred in four patients (1.05% of all patients) were classified as suspected unexpected serious adverse reactions (SUSARs, 10.77% of reported ADRs): anaemia, anaphylactic shock, carotid artery dissection, cerebral infarction, deep vein thrombosis, hypertensive crisis, and thrombophlebitis.
From 65 reported ADRs, the outcome was stated to be ongoing for two events (3.08% of all reported ADRs, 1 patient, 0.26%), recovering for eight events (12.31%, 7 patients, 1.84%) and recovered for the majority of ADRs (47 events, 72.31%, 35 patients, 9.19%). Status was reported to be not recovered for five events (7.69%, 3 patients, 0.79%). The outcome of one ADR was still unknown (1.54%, 1 patient, 0.26%). Data on one event each were missing and were not applicable, respectively (1.54%, 1 patient, 0.26% each).
Conclusion In conclusion, results of the non-interventional study presented here strongly support the effectiveness of Remsima® in the treatment of patients with Crohn’s disease and ulcerative colitis, respectively. Patient cohort analysed was considered to be representative. Safety analysis indicated general tolerability of Remsima® under routine medical practice conditions. Furthermore, effectiveness and tolerability of Remsima® were predominantly evaluated within the global assessment by physicians and patients as very good or good.
Date of report 19th of January 2018
Page 13
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 XII
Signatures
CRO
ANFOMED GmbH
_____________________ Date
______________________ Signature
Biometrics
ANFOMED GmbH
_____________________ Date
______________________ Signature
Head of Medical Affairs
Mundipharma GmbH
_____________________ Date
______________________ Signature
Page 14
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 XIII
Table of contents
I. STUDY ADMINISTRATIVE STRUCTURE .................................................................................................. 1
I.1. Sponsor ......................................................................................................................................... 1
I.2. Contract Research Organization (CRO) ......................................................................................... 1
I.3. Data management......................................................................................................................... 1
I.4. Statistics ........................................................................................................................................ 1
I.5. Medical writing ............................................................................................................................. 1
II. INTRODUCTION ................................................................................................................................... 2
III. GENERAL REGULATIONS ..................................................................................................................... 3
IV. STUDY OBJECTIVES ............................................................................................................................. 4
IV.1. Primary endpoints of the study .................................................................................................. 4
IV.2. Secondary endpoints of the study .............................................................................................. 4
V. STUDY DESIGN AND SAMPLE SIZE CALCULATION ............................................................................... 4
V.1. Study design ................................................................................................................................. 4
V.2. Sample size calculation ................................................................................................................ 5
VI. STUDY PLAN AND PROCEDURES ........................................................................................................ 5
VI.1. Study plan ................................................................................................................................... 5
VI.2. Participating sites and patient selection ..................................................................................... 6
VI.3. Treatment ................................................................................................................................... 6
VI.4. Observational period and total duration of the non-interventional study ................................ 7
VI.5. Conducting the study .................................................................................................................. 7
VI.6. Documentation ........................................................................................................................... 7
VI.6.1. Documentary components .................................................................................................. 8
VI.6.2. Data ..................................................................................................................................... 8
VI.6.2.1. Demographics and anamnesis ......................................................................................8
VI.6.2.2. Efficacy measurements .................................................................................................9
VI.6.2.3. Safety measurements ...................................................................................................9
VI.6.2.4. Data from patient questionnaires .................................................................................9
VI.6.3. Definition and reporting of adverse events (AE)/Adverse drug reactions (ADR) .............. 10
VI.7. Data management, quality control and statistical analysis ...................................................... 10
VI.7.1. Data management ............................................................................................................. 10
VI.7.2. Quality control ................................................................................................................... 11
VI.7.3. Statistical analysis .............................................................................................................. 11
VI.7.3.1. Missing values and last observation carried forward method .................................. 11
Page 15
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 XIV
VI.7.3.2. Significance tests and weighted kappa coefficient .................................................... 12
VI.7.3.3. Limitations .................................................................................................................. 12
VI.7.3.4. Software ..................................................................................................................... 12
VI.7.3.5. Dictionaries and coding systems used ....................................................................... 12
VI.7.3.6. Conventions used in this report ................................................................................. 13
VII. DISPOSITION .................................................................................................................................... 13
VIII. STUDY SUBJECTS ............................................................................................................................ 14
VIII.1. Patient characteristics ............................................................................................................ 14
VIII.1.1. Age ................................................................................................................................... 14
VIII.1.2. Sex ................................................................................................................................... 15
VIII.1.3. Height and Weight ........................................................................................................... 15
VIII.1.4. Body Mass Index .............................................................................................................. 15
VIII.2. Anamnesis ............................................................................................................................... 16
VIII.2.1. Type of inflammatory bowel disease .............................................................................. 16
VIII.2.2. Duration of CIBD .............................................................................................................. 16
VIII.2.3. Intestinal resection due to CIBD ...................................................................................... 17
VIII.2.4. Description of acute episode (Visit 0) ............................................................................. 17
VIII.2.4.1. Duration of acute episode........................................................................................ 17
VIII.2.4.2. Hospitalization ......................................................................................................... 17
VIII.2.4.3. Pre-treatment .......................................................................................................... 18
VIII.2.4.4. Ongoing pre-treatment ............................................................................................ 19
VIII.2.4.5. Surgical measures for pre-treatment of acute episode ........................................... 19
VIII.2.5. Disease activity ................................................................................................................ 19
VIII.2.5.1. Activity of Crohn’s disease ....................................................................................... 19
VIII.2.5.2. Activity of ulcerative colitis ...................................................................................... 21
VIII.2.6. Imaging diagnostics ......................................................................................................... 22
VIII.2.7. Laboratory parameters .................................................................................................... 22
VIII.2.8. Pre-treatment of underlying inflammatory bowel disease (IBD) .................................... 24
VIII.2.9. Concomitant disease ....................................................................................................... 24
VIII.2.10. Treatment of concomitant disease ............................................................................... 25
VIII.3. Treatment with Remsima® ..................................................................................................... 26
VIII.3.1. Switch to Remsima® ........................................................................................................ 26
VIII.3.2. Administered dose of Remsima® .................................................................................... 26
VIII.3.3. Premature end of therapy with Remsima® ..................................................................... 28
VIII.3.4. Treatment of underlying inflammatory bowel disease (IBD) during the study .............. 28
Page 16
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 XV
VIII.3.5. Acute episode .................................................................................................................. 30
VIII.3.5.1. Hospitalization ......................................................................................................... 30
VIII.3.5.2. Imaging procedures ................................................................................................. 31
VIII.3.5.3. Surgical measures .................................................................................................... 32
VIII.3.6. Antibodies before and during the study ......................................................................... 32
IX. EFFICACY RESULTS ............................................................................................................................ 32
IX.1. Inflammatory bowel disease questionnaire (IBDQ) .................................................................. 32
IX.2. Brief fatigue inventory (BFI) ...................................................................................................... 34
IX.3. General depression scale – long version (ADS-L) ...................................................................... 35
IX.4. Short-form McGill Pain questionnaire (SF-McGill) .................................................................... 36
IX.5. Assessment of disease activity .................................................................................................. 37
IX.5.1. Crohn’s disease assessed by Harvey Bradshaw index ....................................................... 37
IX.5.2. Ulcerative colitis assessed by Mayo-score ........................................................................ 38
IX.6. Global assessment of efficacy ................................................................................................... 38
IX.7. Laboratory parameters ............................................................................................................. 39
X. SAFETY RESULTS ................................................................................................................................ 42
X.1. Global assessment of tolerability ............................................................................................... 42
X.2. Adverse events and adverse drug reactions .............................................................................. 43
X.2.1. Categories ........................................................................................................................... 43
X.2.1. Adverse drug reactions ....................................................................................................... 43
X.2.2. Adverse events ................................................................................................................... 48
X.3. Pregnancies ................................................................................................................................ 49
XI. DISCUSSION AND CONCLUSION ....................................................................................................... 50
XI.1. Discussion .................................................................................................................................. 50
XI.1.1. Discussion of demographic and baseline characteristics .................................................. 50
XI.1.2. Discussion of therapy with Remsima®............................................................................... 52
XI.1.3. Discussion of results in effectiveness ................................................................................ 53
XI.1.4. Discussion of results in safety ............................................................................................ 55
XI.2. Limitations on collected data .................................................................................................... 57
XI.3. Clinical relevance and overall conclusions ................................................................................ 58
XII. REFERENCES .................................................................................................................................... 59
Page 17
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 XVI
List of abbreviation and definitions of terms
Abbreviation Explanation
ADR Adverse drug reaction
ADS-L General depression scale – long version (Allgemeine Depressionsskala – Langform)
AE Adverse event
AMG German medicinal product act (Arzneimittelgesetz)
AS Ankylosing spondylitis
ATC Anatomic therapeutic classification
BfArM Federal Institute for Drugs and Medical Devices (Bundesinstitut für Arzneimittel und Medizinprodukte)
BFI Brief Fatigue Inventory
BMI Body Mass Index
CIBD Chronic inflammatory bowel disease
CHMP Committee for Medicinal Products for Human Use
CL Confidence limit
CRF Case report form
CRO Contract research organization
GEP Good Epidemiological Practice
HBI Harvey-Bradshaw-Index
IBD Inflammatory bowel disease
IBDQ Inflammatory bowel disease questionnaire
kg Kilogram
kg/m2 Kilogram per square metre
LOCF Last observed carried forward
mAb Monoclonal antibody
MedDRA Medical Dictionary for Regulatory Activities
mg Milligram
n Number of patients
NIS Non-interventional Study
p Probability
PEI Paul-Ehrlich-Institute
PF Preferred Term
PK Pharmacokinetic(s)
RA Rheumatoid arthritis
SAP Statistical Analysis Plan
SAS Statistical Analysis System
SD Standard deviation
SF-McGill Short-form McGill questionnaire
SmPC Summary of product characteristics
SOC System Organ Class
SUSAR Suspected unexpected serious adverse reactions
TNF Tumor necrosis factor alpha
WHO World Health Organization
Page 18
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 XVII
Tables
Table 1: Study plan .................................................................................................................................. 5
Table 2: Coding systems used in this report ......................................................................................... 13
Table 3: Number of patients and performed visits (n=381) .................................................................. 14
Table 4: Laboratory parameters ............................................................................................................ 23
Table 5: Laboratory parameters at final examination (LOCF) ............................................................... 42
Table 6: Category and frequency of ADRs occurred and number of patients affected (n=381) ........... 43
Table 7: Adverse drug reactions listed according to the preferred term (n=381) ................................ 44
Table 8: ADRs listed according to the system organ class by MedDRA 20.0 (n=381) ........................... 45
Table 9: Serious adverse drug reactions ............................................................................................... 47
Table 10: Suspected unexpected serious adverse reactions................................................................. 47
Table 11: Serious adverse events .......................................................................................................... 48
Figures
Figure 1: Distribution of patients’ age (n=380). .................................................................................... 15
Figure 2: Distribution of patients’ sex (n=381). ..................................................................................... 15
Figure 3: Distribution of patients’ BMI (n=376). ................................................................................... 16
Figure 4: Frequency of Crohn’s disease and ulcerative colitis (n=381). ................................................ 16
Figure 5: Duration of IBD since diagnosis (n=351). ............................................................................... 17
Figure 6: Pre-treatment of acute episode according to ATC anatomical main group (n=381). ............ 18
Figure 7: Assessment of Crohn’s disease according to the HBI (n=221). .............................................. 19
Figure 8: Intestinal localization of Crohn’s disease according to the Montreal-classification
(n=220). ............................................................................................................................................ 20
Figure 9: Extraintestinal localization of Crohn’s disease (n=54 patients with extraintestinal
manifestation). ................................................................................................................................. 20
Figure 10: Assessment of ulcerative colitis according to the Mayo-score (n=154). ............................. 21
Figure 11: Intestinal localization of ulcerative colitis according to the Montreal-classification
(n=158). ............................................................................................................................................ 21
Figure 12: Extraintestinal localization of ulcerative colitis (n=158). ..................................................... 22
Figure 13: Pre-treatment of underlying IBD according to ATC anatomical main group (n=381). ......... 24
Figure 14: Reasons to start a therapy with Remsima® (n=377). ........................................................... 26
Figure 15: Remsima dose (mg/kg body weight, patients with infusion only) at admission (V0,
n=376), V1 (n=244), V2 (n=252), and V3 (n=238; x = mean, – = median, [] = interquartile, - =
minimum and maximum). ................................................................................................................ 27
Figure 16: Distribution of Remsima® dose (mg/kg BW) during the course of the NIS. ......................... 27
Page 19
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 XVIII
Figure 17: Frequency of patients with discontinuation of treatment with Remsima® (n=381). .......... 28
Figure 18: Reasons for premature discontinuation of therapy with Remsima® (n=381). .................... 28
Figure 19: Treatment of underlying IBD during the study, classified according to ATC anatomical
main group (n=381). ......................................................................................................................... 29
Figure 20: Treatment of underlying IBD during the study, classified according to ATC chemical
substances (n=381). ......................................................................................................................... 30
Figure 21: Hospitalization due to an acute episode during the NIS (n=364). ....................................... 30
Figure 22: Imaging procedures during the study (n=366). .................................................................... 31
Figure 23: Finding of imaging diagnostics during the NIS. .................................................................... 31
Figure 24: IBDQ at admission (V0), at control examinations V1 and V2 and at the final examination
(n=311, LOCF; x = mean, – = median, [] = interquartile, - = minimum and maximum). .................. 33
Figure 25: Mean IBDQ-values (LOCF) for patients with Crohn’s disease and ulcerative colitis. ........... 33
Figure 26: Mean IBDQ-values (LOCF) for patients with Crohn’s disease and ulcerative colitis. ........... 34
Figure 27: BFI at admission (V0), at control visits (V1, V2) and at the end of the NIS (V3; n=318,
LOCF; x = mean, – = median, [] = interquartile, - = minimum and maximum). ................................ 34
Figure 28: Mean BFI-values (LOCF) of patients with Crohn’s disease and ulcerative colitis. ................ 35
Figure 29: ADS-L values at admission (V0), at control examinations (V1 and V2) and at the end of
the study (V3; n=277, LOCF; x = mean, - = median, [] = interquartile, - = minimum and
maximum). ....................................................................................................................................... 35
Figure 30: Mean ADS-L values (LOCF) for patients with Crohn’s disease and ulcerative colitis. .......... 36
Figure 31: VAS values of SF-McGill at admission (V0), at control examinations (V1, V2) and at the
final documentation (n=282, LOCF; x = mean, – = median, [] = interquartile, - = minimum and
maximum). ....................................................................................................................................... 36
Figure 32: Mean VAS values (LOCF) of SF-McGill for patients with Crohn’s disease and ulcerative
colitis. ............................................................................................................................................... 37
Figure 33: Activity of Crohn’s disease assessed with HBI at admission (V0), at control examinations
V1 and V2, and at the last visit (V3; n=213, LOCF; x = mean, – = median, [] = interquartile, - =
minimum and maximum). ................................................................................................................ 37
Figure 34: Activity of ulcerative colitis assessed with Mayo-score at admission (V0), at follow-up
visits (V1 and V2) and at the last documentation (V3; n=143, LOCF; x = mean, – = median, [] =
interquartile, - = minimum and maximum). ..................................................................................... 38
Figure 35: Global assessment of efficacy by physician and patient. ..................................................... 39
Figure 36: Assessment of tolerability of Remsima®. ............................................................................. 43
Page 20
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 XIX
List of appendices
Appendix A: Statistical analysis
A – Total sample
Subgroup analysis:
B – Crohn’s disease
C – Ulcerative colitis
D – Patients with and without antibody pre-treatment
E - Patients with antibody pre-treatment: switch ≤ 56 days, > 56 days
Appendix B: Study documents (observational study plan, CRF, SmPC)
Page 21
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 XX
INDEX OF TABLES IN APPENDIX
Page A – Total sample
1-2 Number of centers and patients
3 Visits present
4 Duration of observation
5 Demographic data - Age
6 Demographic data - sex
7-8 Demographic data - height, weight, BMI
9-13 Anamnesis
14-23 Description of acute episode (Visit 1)
24-25 Imaging procedures
26-27 Laboratory parameters / Visit 1
28-29 Pre-treatment of underlying inflammatory bowel disease / ATC - anatomical main group
30-31 Pre-treatment of underlying inflammatory bowel disease / ATC - chemical substances
32 Pre-treatment of underlying inflammatory bowel disease / antibody pre-treatment
33-36 Concomitant disease / MedDRA 20.0 - preferred code
37-38 Concomitant disease / MedDRA 20.0 - Primary system organ classes
39-40 Treatment of concomitant diseases / ATC - anatomical main group
41-43 Treatment of concomitant diseases / ATC - chemical substances
44-49 Treatment with Remsima
50 Treatment of underlying inflammatory bowel disease during study / ATC - anatomical main group
51-52 Treatment of underlying inflammatory bowel disease during study / ATC - chemical substances
53-57 Description of acute episode
58-64 Antibodies before and during study
65-74 IBDQ-D score / Inflammatory bowel disease questionnaire
75-76 BFI / Brief Fatigue Inventory (0-10 points)
77-78 ADS-L / Allgemeine Depressionsskala (0-60 points)
79-86 SF-McGill / Short-form McGill Pain Questionnaire
87-90 Global assessment of effectiveness
Page 22
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 XXI
91-132 Laboratory parameter
133-134 Global assessment of tolerability
135-136 Adverse drug reactions / MedDRA 20.0 - preferred terms
137 Adverse drug reactions / MedDRA 20.0 - Primary system organ class
138-144 Adverse drug reactions / MedDRA 20.0 - Hierarchy
145-146 Adverse drug reactions / MedDRA 20.0 - preferred terms / Seriousness
147-148 Adverse drug reactions / MedDRA 20.0 - preferred terms / SUSAR
149-152 Adverse drug reactions / MedDRA 20.0 - preferred terms / Outcome
153-156 Adverse events / MedDRA 20.0 - preferred terms
157-158 Adverse events / MedDRA 20.0 - Primary system organ class
159-162 Adverse events / MedDRA 20.0 - preferred terms / Seriousness
163-166 Adverse events / MedDRA 20.0 - preferred terms / Relation
167-174 Adverse events / MedDRA 20.0 - preferred terms / Outcome
175-194 Adverse events / individual patient data listing
Page B – Crohn’s disease
1-2 Number of centers and patients
3 Duration of observation
4 Demographic data - Age
5 Demographic data - sex
6-7 Demographic data - height, weight, BMI
8-11 Anamnesis
12-14 Description of acute episode (Visit 1)
15 Assessment of disease activity of Crohn's disease (Harvey-Bradshaw Index)
16-24 Localization of the acute episode (Montreal-classification)
25-26 Imaging procedures
27-28 Laboratory parameters / Visit 1
30-31 Pre-treatment of underlying inflammatory bowel disease / ATC - chemical substances
32 Pre-treatment of underlying inflammatory bowel disease / antibody pre-treatment
33-35 Concomitant disease / MedDRA 20.0 - preferred code
36-37 Concomitant disease / MedDRA 20.0 - Primary system organ classes
38-39 Treatment of concomitant diseases / ATC - anatomical main group
40-41 Treatment of concomitant diseases / ATC - chemical substances
Page 23
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 XXII
42-46 Treatment with Remsima
47 Treatment of underlying inflammatory bowel disease during study / ATC - anatomical main group
48 Treatment of underlying inflammatory bowel disease during study / ATC - chemical substances
49-53 Description of acute episode
54-57 Assessment of disease activity of Crohn's disease (Harvey-Bradshaw Index, patients with Crohn's disease only)
58-67 IBDQ-D score / Inflammatory bowel disease questionnaire
68-69 BFI / Brief Fatigue Inventory (0-10 points)
70-71 ADS-L / Allgemeine Depressionsskala (0-60 points)
72-79 SF-McGill / Short-form McGill Pain Questionnaire
80-82 Global assessment of effectiveness
83-124 Laboratory parameter
125-126 Global assessment of tolerability
127 Adverse drug reactions / MedDRA 20.0 - preferred terms
128 Adverse drug reactions / MedDRA 20.0 - Primary system organ class
129-133 Adverse drug reactions / MedDRA 20.0 - Hierarchy
134 Adverse drug reactions / MedDRA 20.0 - preferred terms / Seriousness
135 Adverse drug reactions / MedDRA 20.0 - preferred terms / SUSAR
136-137 Adverse drug reactions / MedDRA 20.0 - preferred terms / Outcome
138-139 Adverse events / MedDRA 20.0 - preferred terms
140 Adverse events / MedDRA 20.0 - Primary system organ class
141-142 Adverse events / MedDRA 20.0 - preferred terms / Seriousness
143-144 Adverse events / MedDRA 20.0 - preferred terms / Relation
145-148 Adverse events / MedDRA 20.0 - preferred terms / Outcome
Page C – Ulcerative colitis
1-2 Number of centers and patients
3 Duration of observation
4 Demographic data - Age
5 Demographic data - sex
6-7 Demographic data - height, weight, BMI
8-11 Anamnesis
12-14 Description of acute episode (Visit 1)
Page 24
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 XXIII
15 Assessment of disease activity of ulcerative colitis (Mayo score, patients with ulcerative colitis only)
16-23 Localization of the acute episode (Montreal-classification, patients with ulcerative colitis only)
24-25 Imaging procedures
26-27 Laboratory parameters / Visit 1
28 Pre-treatment of underlying inflammatory bowel disease / ATC - anatomical main group
29-30 Pre-treatment of underlying inflammatory bowel disease / ATC - chemical substances
31 Pre-treatment of underlying inflammatory bowel disease / antibody pre-treatment
32-33 Concomitant disease / MedDRA 20.0 - preferred code
34 Concomitant disease / MedDRA 20.0 - Primary system organ classes
35-36 Treatment of concomitant diseases / ATC - anatomical main group
37-38 Treatment of concomitant diseases / ATC - chemical substances
39-43 Treatment with Remsima
44 Treatment of underlying inflammatory bowel disease during study / ATC - anatomical main group
45-46 Treatment of underlying inflammatory bowel disease during study / ATC - chemical substances
47-51 Description of acute episode
52-55 Assessment of disease activity of ulcerative colitis (Mayo score)
56-65 IBDQ-D score / Inflammatory bowel disease questionnaire
66-67 BFI / Brief Fatigue Inventory (0-10 points)
68-69 ADS-L / Allgemeine Depressionsskala (0-60 points)
70-77 SF-McGill / Short-form McGill Pain Questionnaire
78-80 Global assessment of effectiveness
81-122 Laboratory parameter
123-124 Global assessment of tolerability
125 Adverse drug reactions / MedDRA 20.0 - preferred terms
126 Adverse drug reactions / MedDRA 20.0 - Primary system organ class
127-131 Adverse drug reactions / MedDRA 20.0 - Hierarchy
132 Adverse drug reactions / MedDRA 20.0 - preferred terms / Seriousness
133 Adverse drug reactions / MedDRA 20.0 - preferred terms / SUSAR
Page 25
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 XXIV
134-135 Adverse drug reactions / MedDRA 20.0 - preferred terms / Outcome
136-137 Adverse events / MedDRA 20.0 - preferred terms
138 Adverse events / MedDRA 20.0 - Primary system organ class
139-140 Adverse events / MedDRA 20.0 - preferred terms / Seriousness
141-142 Adverse events / MedDRA 20.0 - preferred terms / Relation
143-146 Adverse events / MedDRA 20.0 - preferred terms / Outcome
Page D – Patients with and without antibody pre-treatment
1 Pre-treatment of underlying inflammatory bowel disease / antibody pre-treatment
2-3 Anamnesis - Which form of inflammatory bowel disease (IBD) is the patient suffering from?
4-9 Assessment of disease activity of Crohn's disease (Harvey-Bradshaw Index, patients with Crohn's disease only)
10-15 Assessment of disease activity of ulcerative colitis (Mayo score, patients with ulcerative colitis only)
16-45 IBDQ-D score / Inflammatory bowel disease questionnaire
46-51 BFI / Brief Fatigue Inventory (0-10 points)
52-57 ADS-L / Allgemeine Depressionsskala (0-60 points)
58-81 SF-McGill / Short-form McGill Pain Questionnaire
82-83 Global assessment of effectiveness
84-85 Global assessment of tolerability
Page E - Patients with antibody pre-treatment: switch ≤ 56 days, > 56 days
1 Pre-treatment of underlying inflammatory bowel disease / antibody pre-treatment
2-3 Anamnesis - Which form of inflammatory bowel disease (IBD) is the patient suffering from?
4-9 Assessment of disease activity of Crohn's disease (Harvey-Bradshaw Index, patients with Crohn's disease only)
10-15 Assessment of disease activity of ulcerative colitis (Mayo score, patients with ulcerative colitis only)
16-45 IBDQ-D score / Inflammatory bowel disease questionnaire
46-51 BFI / Brief Fatigue Inventory (0-10 points)
52-57 ADS-L / Allgemeine Depressionsskala (0-60 points)
58-81 SF-McGill / Short-form McGill Pain Questionnaire
82-83 Global assessment of effectiveness
84-85 Global assessment of tolerability
Page 26
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 1
I. STUDY ADMINISTRATIVE STRUCTURE
I.1. Sponsor
Mundipharma GmbH
Mundipharmastraße 2
65549 Limburg (Lahn)
I.2. Contract Research Organization (CRO)
ANFOMED GmbH
Röttenbacher Straße 17
91096 Möhrendorf
I.3. Data management
ANFOMED GmbH
Röttenbacher Straße 17
91096 Möhrendorf
I.4. Statistics
ANFOMED GmbH
Röttenbacher Straße 17
91096 Möhrendorf
I.5. Medical writing
ANFOMED GmbH
Röttenbacher Straße 17
91096 Möhrendorf
Page 27
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 2
II. INTRODUCTION
Monoclonal antibodies have been established as a major product class of biotechnology-
derived medicinal products. Different mAb products share some properties, e.g. being
cytotoxic to their target, or neutralizing a cytokine, but differ in aspects like the mechanism of
action. They are structurally complex and may have several functional domains within a single
molecule, depending on the isotype (antigen-binding region, complement-binding region,
constant part interacting with Fc receptors). Each individual mAb presents a unique profile
with respect to the antigen-binding region, the Fc cytotoxic effector function, and binding to
Fc receptors. Tumor necrosis factor alpha (TNFα) inhibition is an important treatment option
for several chronic inflammatory disorders in rheumatology and gastroenterology. TNFα is a
multipotent cytokine that occurs in monomeric and trimeric soluble and transmembrane
forms. Infliximab is a chimeric human-murine monoclonal antibody that binds with high
affinity to both, soluble and transmembrane forms of TNFα. TNFα receptor activation is
prevented by infliximab through binding to TNFα, thereby neutralising the biological activity
of TNFα. This monoclonal antibody was first authorised in the European Union in August
1999 under the invented name of Remicade®. It is currently approved for the following
indications: rheumatoid arthritis, ankylosing spondylitis, psoriatic arthritis, psoriasis, adult and
paediatric Crohn’s disease, and adult and paediatric ulcerative colitis. In June 2013, the
European Medicines Agency’s Committee for Medicinal Products for Human Use
recommended the authorisation of Remsima® (Inflectra®, CT-P13) as a biosimilar medicinal
product containing infliximab (Committee for Medicinal Products for Human Use (CHMP)
2013). As part of the comparability exercise, it was shown that all major physicochemical
characteristics and biological activities of Remsima® were comparable to those of the
reference product Remicade®.
The clinical data demonstrating similarity between Remsima® and Remicade® consisted of two
main clinical trials: a pivotal pharmacokinetic study in patients with ankylosing spondylitis
(PLANETAS study CT-P13 1.1) (Park et al. 2016) and a pivotal efficacy and safety study in
patients with active rheumatoid arthritis (PLANETRA study CT-P13 3.1) (Yoo et al. 2013). The
pharmacokinetic trial in ankylosing spondylitis patients showed, at the dose of 5 mg/kg,
comparable profiles between Remsima® and Remicade® at steady state (after 5 doses) with
the 90% confidence intervals of the geometric means ratios (%) of both primary parameters
AUCτ and Cmax,ss within the pre-specified bioequivalence interval: AUCτ:104.10 (93.93-
115.36) and Cmax,ss: 101.47 (94.57-108.86). In addition, the results of the main secondary
pharmacokinetic parameters such as Tmax, Cmin, ss, T½, CLss, Vss between weeks 22 and 30,
as well as Cmax and Cmin after the 9 treatment doses were also comparable in the Remsima®
and Remicade® treatment arms, providing further evidence of a similar pharmacokinetic
behaviour. Additional supportive data regarding the similarity at the dose of 3 mg/kg were
provided from the second main study. The efficacy and safety trial in rheumatoid arthritis
patients achieved its primary endpoint since the 95% confidence interval for the difference in
the ACR20 response rate at week 30 was contained within the predefined equivalence margin
(±15%) in both the all-randomised (95% CI: -0.06, 0.10) and per protocol populations (95% CI:
Page 28
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 3
-0.04, 0.12). At week 30, the results of the secondary endpoints (in particular ACR50 and
ACR70, decreases in DAS28, SDAI and CDAI, increases in SF-36) were all consistent with the
results of the primary endpoint. These data were further supported by comparable response
rates at week 54. Additional supportive efficacy data were provided in another indication by
the pharmacokinetic study CT-P13 1.1 conducted in ankylosing spondylitis patients. The
efficacy results were comparable between treatment arms up to week 54. The evaluation of
the safety profile of the biosimilar medicinal product was supported mainly by the results from
the two clinical studies mentioned above. The type and incidence of adverse drug reactions
observed with Remsima® and Remicade® in the respective studies were generally similar and
no new safety concern was identified. Based on the robust comparisons of the
physicochemical and in vitro and ex vivo biological analyses, Remsima® was considered
biosimilar to the reference product Remicade®. These data, in combination with clinical data
demonstrating pharmacokinetic and therapeutic equivalence in rheumatology conditions,
allow for extrapolation to all other indications of Remicade® (Committee for Medicinal
Products for Human Use 2012; Assessment report Remsima 2013).
Remsima® is now recommended and available for the clinical use in patients with Crohn’s
disease and ulcerative colitis in the European Union. To date, only few data were collected
regarding clinical outcomes achieved with Remsima® for these indications. Prior studies
showed the safety and efficacy in rheumatoid arthritis and ankylosing spondylitis, however,
potential similarity in the treatment of IBD was not documented so far and is therefore
addressed in the following presentation of the prospective, multicenter, non-interventional
ResCu study.
III. GENERAL REGULATIONS
The general notification requirement according to § 67 (6) German Medicines Law (AMG)
stipulated that the National Association of Statutory Health Insurance Physicians (KBV), the
National Association of Statutory Health Insurance Funds (Spitzenverband Bund der
Krankenkassen) and the Fund for Private Health Insurances (Verband der privaten
Krankenversicherung e.V.) had to be notified (Gesetz über den Verkehr mit Arzneimitteln
2013). The names and lifetime number of all attending physicians involved had to be reported
to the KBV and the National Association of Statutory Health Insurance Funds as well as the
kind and level of quarterly achieved remuneration.
Recognized principles for conducting non-interventional studies had been observed
(Arbeitsgruppe Epidemiologische Methoden der Deutschen Arbeitsgemeinschaft für
Epidemiologie 2004; Victor et al. 1997; La Haye 2000; Sickmüller 2009; Elm et al. 2008).
Documentation was conducted according to non-interventional principles under the sole
therapeutic and medical responsibility of the attending physician. Each physician involved
assured by signing the contract that the collected data were documented according to the
observational plan.
Page 29
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 4
Participating physicians were remunerated for completion of eCRF forms. Remuneration was
calculated on basis of the German physician fee scale (GOÄ). Terms of payment were settled
in the contract of participation.
An ethics committee was consulted before start of survey.
IV. STUDY OBJECTIVES
IV.1. Primary endpoints of the study
The aim of the non-interventional observational (NIS) study was to document efficacy and
safety of Remsima® in the treatment of Crohn‘s disease and ulcerative colitis under real life
conditions. The activity of Crohn‘s disease and ulcerative colitis were determined by Harvey-
Bradshaw-Index (HBI) (Harvey und Bradshaw 1980) and Mayo-Score (Lewis et al. 2008).
IV.2. Secondary endpoints of the study
The influence on quality of life, fatigue, depression and abdominal pain was documented by
validated patient questionnaire forms. The German version of the Inflammatory Bowel
Disease Questionnaire (IBDQ-D) recorded the quality of life of patients (Janke et al. 2005).
Furthermore, by using the Brief fatigue inventory (BFI), the influence of treatment with
Remsima® on fatigue was recorded (Radbruch et al. 2003). The ADS-L was used to document
depression (Hautzinger und Bailer 1993) and the SF-McGill Questionnaire to evaluate
abdominal pain (Melzack 1987).
V. STUDY DESIGN AND SAMPLE SIZE CALCULATION
V.1. Study design
The current study was a non-interventional observational trial according to the definition of
§ 4, (23), sentence 3 of the German Medicinal Products Act (AMG): ”(…) this is a study within
the scope of findings resulting from persons’ treated with medicinal products that are
analyzed using epidemiological methods pursuant to the specification for use, contained in
the marketing authorization; the treatment, including the diagnosis and monitoring, shall not
follow a predetermined trial protocol but shall result exclusively from current medical
practice.”
A prospective, multicenter, non-interventional, observational study was suited best to seek
information in order to clarify all listed issues and to investigate an adequate number of
patients. Additionally, it was the only means available to gain information on therapeutic
behaviour of physicians in routine medical practice without accompanying conditions or other
influences. Enrolment of patients into the non-interventional observational study is based
solely on the physicians’ assessment on medical usefulness and necessity.
Planning, conduction and evaluation of the study was based on the relevant combined
recommendation of BfArM (The Federal Institute for Drugs and Medical Devices) and Paul-
Ehrlich Institute (PEI).
Page 30
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 5
V.2. Sample size calculation
Enrolment of about 400 patients was planned. A total number of 400 patients was intended
considering the feasibility of this non-interventional study in the routine medical practice for
obtaining a representative number of patients in the named indication.
Based on 400 documented cases:
in case of dichotomous variables for the underlying binominal probability, a 95%-
confidence interval of in maximum 10.02 percentage points in length are reached,
95%-confidence intervals on the underlying means of quantitative variables have a
length of 0.197 standard deviations,
rare events with an incidence down to 0.007 (1:134) are included at least once in
the sample with a probability of 95%.
VI. STUDY PLAN AND PROCEDURES
VI.1. Study plan
Data were documented in an electronic case report from (eCRF) or by patient questionnaire
forms. Four survey dates were planned:
Baseline of data collection (Visit 0): before start of treatment
Follow-up data collection (Visit 1): about 2 weeks after start of treatment
Follow-up data collection (Visit 2): about 6 weeks after start of treatment
Final survey of data collection (Visit 3): about 14 weeks after start of treatment
The exact examination dates were to be determined by the attending physician.
Details on each visit are listed in Table 1.
Table 1: Study plan
Baseline
(Visit 0)
Follow-up after about 2 weeks
(Visit 1)
Follow-up after about 6 weeks
(Visit 2)
Final survey after about
14 weeks (Visit 3)
Date of visit X X X X
Demographic data X
Medical history of CIBD X
Assessment of severity of acute episode
X X X X
Localization and description of acute episode
X
Imaging diagnostic X X X X
Laboratory parameter X X X X
Pre-treatment of CIBD X
Treatment with Remsima® X X X X
Page 31
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 6
Concomitant diseases and medication
X X X X
IBDQ-D X X X X
BFI X X X X
ADS-L X X X X
SF-McGill X X X X
Harvey-Bradshaw Index (patients with Crohn's disease only)
X X X X
Mayo score (patients with ulcerative colitis only
X X X X
Global assessment of Remsima® therapy by physician and patient
X X
Adverse drug reactions and adverse events
X X X
VI.2. Participating sites and patient selection
A total number of 70 participating physicians specialized in gastroenterology was intended.
The distribution of the physicians extended throughout Germany.
It was estimated that one physician should enrol a maximum of 6 patients. But in the
discretion of time schedule and medical practice during the non-interventional trial,
enrolment of more than 6 patients per site was accepted.
A patient was included in the study when the physician decided in advance to start treatment
with Remsima® according to the local SmPC (Mundipharma 2015). The prescription of
Remsima® was independent of enrolment in the non-interventional study and not determined
by the observational plan in advance.
A signed patient consent form was required for participation in the study. Only patients of full
age who were capable of understanding the nature, significance and implications of the study
and to form a rational intention in the light of the facts, were enrolled in the study.
VI.3. Treatment
Remsima® is indicated for symptomatic treatment of moderate to severe, active Crohn‘s
disease, treatment of fistulising, active Crohn‘s disease and moderate to severe active
ulcerative colitis in adult patients who have not responded despite a full and adequate course
of therapy with conventional treatment or who are intolerant to or have medical
contraindications for such therapies.
According to the summary of product characteristics (SmPC) the recommended dose is
5 mg/kg as an intravenous infusion (Mundipharma 2015). Application of Remsima® was
according to usual therapeutic procedure of the attending physician and in accordance with
the authorized indications and SmPC (Mundipharma 2015).
Page 32
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 7
VI.4. Observational period and total duration of the non-interventional study
Observational period per patient was about 14 weeks. The non-interventional study started
on 28th of September 2015. Last patient was enrolled on 31st of December 2016. End of the
non-interventional study was 31st of April 2017. Data entry into eCRF was possible until 15th
of May 2017 (after extension).
VI.5. Conducting the study
Sales representatives of Mundipharma GmbH were responsible for distributing study
documents and were at hand to answer administrative questions related to survey
conduction. Distribution of documents was executed according to the FSA codex (Kodex zur
freiwilligen Selbstkontrolle 2013) and were not linked to any pharmaceutical advertising
actions. Central coordination of the study was conducted by the assigned clinical research
organization ANFOMED GmbH.
To obtain individual user name and password for log in on the study website, physician had to
forward the filled out and signed contract to ANFOMED GmbH. Physicians received the access
data in written form.
The physician selected suitable patients who met all the required criteria for data collection
within the scope of the non-interventional study and obtained their written consent. It should
be particularly noted that selection of patients, who were included in the study, was based
solely on the assessment of medical sense and necessity by the attending physician. Patients
were considered for enrollment, after treatment with Remsima® had been decided on.
The physician investigated selected patients at scheduled dates and documented the data in
the eCRF. Study website was subdivided into different visits leading the physician through the
documentation of the examination.
The patient questionnaire forms were handed out at baseline, at follow-up examinations and
at final examination to be filled out by the patient. These forms had to be returned to the
attending physician at the same examination. The physician forwarded the completed patient
questionnaires directly after each visit to ANFOMED GmbH for data entry, validation and
evaluation.
VI.6. Documentation
The documentation occurred online on a password-protected website. The online
documented data were proofed for completeness and plausibility according to defined and
validated rules. Following conditions were required for online documentation in the eCRF:
internet access
working browser (e.g. Microsoft Internet Explorer etc.)
The attending physician had to log in on the internet website (https://www.NIS-
Remsima.com) with individual user name and password for the documentation.
Page 33
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 8
Patient data were pseudonymized. Each attending physician had only access to the data of his
supervised patients.
The eCRF was structured in several pages. When changing to a next page, entered data were
proofed for completeness, consistency and formatting. Sections of the eCRF with erroneous
input were highlighted and an error message appeared.
For security reasons, the whole data transfer between client and web server followed Secure
Socket Layer protocol (SSL) with 128-bit encoding. The study database was copied to a second
hard disc each hour and to tape once a day.
Patient questionnaire forms were available on paper. After completion by the patient they
were forwarded to ANFOMED GmbH for electronic registration.
Patient data and physician data were subject to data protection requirements according to
legal regulation of protecting against abuse of personal data in data processing (federal data
protection act).
VI.6.1. Documentary components
At the beginning of the non-interventional study the attending physician received a
documentary folder containing all required documents for 6 patients, including:
• two contracts of participation (one original and one copy for physician)
• a short summary of the survey
• patient overview
• the observational plan
• the SmPC of Remsima®
• ethics committee vote
• patient information and consent forms (one copy for patient and one for physician)
• patient questionnaire forms
• manual for eCRF
• return envelopes to send the contract of participation and patient questionnaire
forms
VI.6.2. Data
The following data were documented within the NIS:
VI.6.2.1. Demographics and anamnesis
Patient data (year of birth, sex, height, weight)
Anamnesis (date of diagnosis and type of IBD, information on relapses and intestinal
resections)
Data on acute episode (hospitalization, assessment of activity, localization, imaging
diagnostics, laboratory parameters)
Page 34
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 9
(Pre-)Treatment of IBD and acute episode
Treatment with Remsima® (reason for adjustment, therapy start, batch-number,
dosage)
VI.6.2.2. Efficacy measurements
Dosage, therapy change, continuation of treatment with Remsima®
Data on acute episode during therapy with Remsima® (hospitalization, assessment
of activity, imaging diagnostics, laboratory parameters)
Treatment of IBD and acute episode
Concomitant medication
Physicians‘ assessment of efficacy
VI.6.2.3. Safety measurements
Adverse events/adverse drug reactions
Physicians‘ assessment of tolerability
VI.6.2.4. Data from patient questionnaires
All patients received patient questionnaire forms which were to be filled out completely.
Questionnaires had to be returned to the physician at baseline, at follow-up examinations and
at final visit.
The physician forwarded the completed patient questionnaires directly after each visit to
ANFOMED GmbH for electronic registration and further processing.
Inflammatory Bowel Disease Questionnaire
The German version of the Inflammatory Bowel Disease Questionnaire (IBDQ-D) was designed
to find out how the patient had been feeling in the last two weeks and was therefore used to
document the quality of life of patients (Janke et al. 2005).
Brief Fatigue Inventory
The Brief Fatigue Inventory (BFI) served to quickly assess the severity of fatigue as well as its
impact on patients’ capability over the previous 24 h (Radbruch et al. 2003).
General depression scale
The general depression scale (Allgemeine Depressionsskala – Langform, ADS-L) was used as a
self assessment tool to evaluate the impairment due to depressive symptoms within the last
week. Emotional, motivational, cognitive, somatic and motoric complaints were asked
(Hautzinger und Bailer 1993).
Short-Form McGill Pain Questionnaire
The German version of the Short-Form McGill Pain Questionnaire (SF-McGill) was used in this
non-interventional study to evaluate abdominal pain (Melzack 1987).
Page 35
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 10
VI.6.3. Definition and reporting of adverse events (AE)/Adverse drug reactions (ADR)
Attending physicians were responsible to document carefully all serious and non-serious
adverse drug reactions (ADR) in the eCRF, independent of severity, in which relation to
Remsima® therapy was not excluded and occurred during the course of the study.
The ADR report section recorded all information such as type and duration, measures or
therapies and assessment of causality. Additionally, all adverse events (AE), in which relation
to Remsima® therapy was excluded, were to be documented in the eCRF.
Adverse drug reactions (ADR) are defined in § 4, (13) of the German Medicinal Products Act
(AMG) as ”noxious and adverse reactions to a drug, in medicines intended for use in humans”.
Serious adverse drug reactions are reactions that
result in death,
are life threatening,
require hospitalization or prolong an existing hospitalization,
result in persistent or significant disability or incapacity,
result in congenital anomaly or birth defect and
are a medically important condition.
Medically important conditions were events that threatened the patient significantly and
possibly required a medical or surgical intervention to prevent a serious adverse event.
Any adverse drug reaction (serious or non-serious) during the non-interventional study, in
which relation to Remsima® therapy could not be excluded, independent of severity, had to
be carefully documented in the “ADR report section” of the eCRF within 24 hours. This ADR
report was automatically forwarded to the drug safety department of ANFOMED GmbH and
after processing to Mundipharma GmbH.
Mundipharma was responsible for further processing of all case reports concerning adverse
drug reactions including acquisition, documentation, scientific assessment and any report
required according to AMG §63c.
VI.7. Data management, quality control and statistical analysis
VI.7.1. Data management
Data management was based on the “Guidelines and recommendations for ensuring Good
Epidemiological Practice (GEP)” (Deutsche Arbeitsgemeinschaft für Epidemiologie 2004).
This non-interventional study was based on online documentation. Entered data were
automatically transmitted to central data collection of ANFOMED GmbH for statistic analysis.
Consistency of the ADR data was ensured by comparing the project database with the drug
safety database of Mundipharma GmbH. Discrepancies were resolved by joint consultation.
Page 36
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 11
VI.7.2. Quality control
In case of incomplete or incorrect entered data in the eCRF physicians directly received an
automatically generated warning message to correct entered data. Once an adverse drug
reaction was entered in the eCRF, physicians received a warning message to fill out the „ADR
report section”. Furthermore, the data in the eCRF were checked for suspicious ADRs and also
checked at regular intervals for updates in the data files of the patients with ADRs.
VI.7.3. Statistical analysis
Taking into account the non-interventional character of the study, the statistical analysis was
performed in a descriptive and explorative way. In detail, the following descriptive procedures
were used:
• Absolute, relative and adjusted relative frequencies were computed; for the latter, patients
with missing data were omitted.
• Multiple entries, e.g. drug names, were counted; the relative frequencies referred to the
number of cases so that the total of 100% could be exceeded through multiple entries per
case. In each case, the number of patients that had given multiple replies was recorded. This
included relative (related to the population) and adjusted relative frequencies (related to the
population minus the missing data).
• Cross tables:
The results tables include two types of cross tables: The first input value for the first type is a
grouping variable and the second are the various expressions or qualities of the analysed
variable. The percentage relates to the sum of the line (last column) that contains the number
of patients per group. In the second type of cross tables, the two input values are formed by
the expression of the same variable. The percentage relates to the total of the patients
represented in the table that can be read from the crossing point of the last line and the last
column. This type of illustration is used to investigate shifts between two specific time points.
• Calculations of mean, standard deviation, quartiles, 95%-confidence limits (95%-CL) and
also listing of maximum and minimum values.
AEs/ADRs were entered separately and coded according to MedDRA. All cases were listed in
frequency tables on the basis of preferred terms (PT) and system organ class (SOC). A line
listing of all events was prepared.
When reasonable, lists of individual data were prepared.
VI.7.3.1. Missing values and last observation carried forward method
For variables that had been documented once in the course of the study, missing values were
not replaced. The frequency of missing values of each parameter was listed in the tables.
For variables that had been documented several times in the course of the investigation, an
analysis according to the last observation carried forward method (LOCF) was given in addition
to the representation of all existing values and complete cases. With LOCF, missing values in
Page 37
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 12
the course of the study were replaced by the last actual observation. Condition for the
application of this method was the existence of a baseline value and a value after baseline.
VI.7.3.2. Significance tests and weighted kappa coefficient
No statistical hypotheses were formulated in advance. If considered as relevant, tests of
significance were presented for important parameters, but should be interpreted in a
descriptive-exploratory way only. The p-values reported were two-tailed and an alpha level of
0.05 was used to assess statistical significance. No correction of alpha level for multiple tests
was performed.
Tests used were:
Bhapkar's test of marginal homogeneity: marginal homogeneity refers to the situation
where the marginal distributions of row and column variables of an n*k table (shift-table)
are the same.
Wilcoxon's signed-rank test: the Wilcoxon signed-rank test is a non-parametric statistical
hypothesis test used when comparing two related samples, matched samples, or repeated
measurements on a single sample to assess whether their population mean ranks differ.
The weighted kappa coefficient is a statistic that measures inter-rater agreement for
ordinal items. Values < 0 are considered as indicative for no agreement, 0–0.20 for slight,
0.21–0.40 for fair, 0.41–0.60 for moderate, 0.61–0.80 for substantial, and 0.81–1 for almost
perfect agreement (Landis 1977).
VI.7.3.3. Limitations
Due to missing reference group of patients without or with alternative therapy, the efficacy
of Remsima® treatment could not be mathematically isolated. One advantage of this study
design was the better transfer to non-selected patients in non-study situations.
VI.7.3.4. Software
The statistical analysis was done using the SASTM Version 9.4 on a personal computer with
Windows 10TM.
VI.7.3.5. Dictionaries and coding systems used
Pre-treatments, concomitant therapies and ADRs were coded according to the coding system
in Table 2.
Page 38
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 13
Table 2: Coding systems used in this report
Variable Coding system used
Previous and concomitant therapies ATC (Anatomic Therapeutic Classification, 2017)
Adverse events/reactions MedDRA 20.0
Concomitant diseases MedDRA 20.0
VI.7.3.6. Conventions used in this report
Unless otherwise stated, percentages presented in this report are adjusted percentages,
meaning subjects with missing values for a particular parameter were not taken into account.
References to tables with an A- to E-prefix (i.e. Table A11) refer to tables in appendixes,
whereas references without a prefix refer to tables within this report.
VII. DISPOSITION
Data of 381 patients were available for statistical analysis. These patients were under
physicians care of 70 centres (Table A1). The number of patients per centre was on average
(±SD) 5.44 (±3.66, median 4.50) and varied from one patient up to 13 patients. Data were most
frequently documented on three, one or six patients per centre (11 centres, 15.71% of the
centers; 10 centres, 14.29%; 10 centres, 14.29%; Table A2).
The first patient was enrolled on 11th of June 2015 retrospectively. The last documentation of
the last patient was performed on 31th of March 2017.
Data of all visits (admission to final examination, V0-V3) were available for 291 patients
(76.38% of all patients) for statistical analysis. Overview about the number of patients and the
visits performed is given in Table 3 (Table A3).
Page 39
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 14
Table 3: Number of patients and performed visits (n=381)
Mean duration of observation was 3.36 (±1.54, median 3.25) months with a minimum of
0.36 months and a maximum of 12.20 months. The most frequent duration was 3-4 months
(179 patients, 49.18% of all patients with data concerning duration of treatment). The sum of
the observed patient years was 101.87 years. Data of 17 patients were missing (Table A4).
VIII. STUDY SUBJECTS
VIII.1. Patient characteristics
VIII.1.1. Age
Patients’ mean age was 41.10 (±14.62, median 39.00) years with a range of 18 to 91 years.
Attending patients were predominantly between 20 to <40 years (180 patients, 47.37% of the
patients with data on age) old (Table A5).
The distribution of patients’ age is depicted in detail in Figure 1.
Admission
(V0)
Control
examination
(V1)
Control
examination
(V2)
Final
examination
(V3)
Number of patients
(n)
Percent (%)
X . . . 15 3.94
X . . X 3 0.79
X . X . 2 0.52
X . X X 14 3.67
X X . . 22 5.77
X X . X 4 1.05
X X X . 30 7.87
X X X X 291 76.38
Number of patients (n)
381 347 337 312 381 100.00
Percent (%)
100.00 91.08 88.45 81.89 . .
Page 40
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 15
Figure 1: Distribution of patients’ age (n=380).
VIII.1.2. Sex
Gender was reported for 381 patients. Of
these, 180 patients (47.24%) were male
and 201 patients (52.76%) were female
(Figure 2, Table A6).
Figure 2: Distribution of patients’ sex (n=381).
VIII.1.3. Height and Weight
Mean height of 376 patients was 173.34 cm (±8.95, median 172.50) and varied between the
minimum of 152.00 cm and the maximum of 203.00 cm. Data were missing for five patients
(Table A7). Concerning weight, a mean value of 75.33 (±17.66, median 73.50) kg was
calculated from data of 376 patients. Weight information of five patients was not available
(Table A7).
VIII.1.4. Body Mass Index
The mean body mass index (BMI) of 376 patients was 25.01 (±5.29, median 24.12) kg/m2 and
varied between 15.21 and 47.18 (Table A7).
0%
1%
2%
3%
4%
5%
17 22 27 32 37 42 47 52 57 62 67 72 77 82 87
47.24%52.76%
Male
Female
Page 41
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 16
Most of the patients were of standard
weight (187 patients, 49.73%) and
111 patients (29.52%) were overweight.
Minority of patients were obese
(53 patients, 14.10%) or underweight
(25 patients, 6.65%). Figure 3 shows the
distribution of the patients to the weight
classes. Values of five patients were
missing (Tables A8).
Figure 3: Distribution of patients’ BMI (n=376).
VIII.2. Anamnesis
VIII.2.1. Type of inflammatory bowel disease
The type of inflammatory bowel disease
(IBD) was documented for 381 patients.
Crohn’s disease was more frequently
diagnosed than ulcerative colitis
(223 patients, 58.53% vs. 158 patients,
41.47%; Figure 4, Table A9).
Figure 4: Frequency of Crohn’s disease and ulcerative colitis (n=381).
VIII.2.2. Duration of CIBD
Mean duration since diagnosis was 106.64 (±108.32, median 76.03) months with a range of
about a half month to more than 39 years, but frequently less than 5 years (157 patients,
44.73% of the patients with data on duration; Figure 5). Data of 30 patients were missing
(Table A10).
6.65%
49.73%29.52%
14.10%
Underweight
Standard weight
Overweight
Adiposity
58.53%
41.47%
Crohn's disease
Ulcerative colitis
Page 42
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 17
Figure 5: Duration of IBD since diagnosis (n=351).
The mean number of episodes since diagnosis was reported for 114 patients with a mean of
4.73 (±6.18, median 2.00) episodes. Most patients stated occurrence of one episode since
diagnosis (35 patients, 30.70%). Data on the frequency of episodes were not available for
267 patients (Table A11).
VIII.2.3. Intestinal resection due to CIBD
An intestinal resection due to CIBD was performed in 61 patients (16.14% of patients with
data on intestinal resection) whereas 317 patients (83.86%) were without an intestinal
resection in the past. Information was missing for three patients (Table A12). Up to
three intestinal resections were reported (one resection, 47 patients, 12.43%; two resections,
12 patients, 3.17%; three resections, 2 patients, 0.53%; Table A13).
VIII.2.4. Description of acute episode (Visit 0)
VIII.2.4.1. Duration of acute episode
Data on duration of acute episodes at study start were available in 374 patients. The mean
duration of acute episodes at enrolment was 14.34 (±43.72, median 2.93) months. Most of
the patients suffered from an acute episode for less than 6 months (262 patients, 70.05%) and
in 78 patients the acute episode started >6-24 months before baseline (78 patients, 20.86%).
Further information is given in Table A14.
VIII.2.4.2. Hospitalization
Concerning hospitalization prior to study start, patients were asked if they had been
hospitalized due to the current episode. Most patients answered in the negative (293 patients,
78.13% of the patients with data on hospitalization). Information of six patients was missing
(Table A15).
Patients with hospitalization stayed on average 2.51 (±3.50, 1.43 median) weeks at the
hospital. The time varied from one day up to 20 weeks. The number of weeks in hospital was
quite diverse, but most patients stayed up to one week (32 patients, 39.02%), followed by up
9.40%
16.52%
18.80%
22.22%20.80%
12.25%
0%
5%
10%
15%
20%
25%
> 0 - 6 months > 6 - 24 months > 24 - 60 months > 5 - 10 years > 10 - 20 years > 20 years
Duration
Page 43
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 18
to two weeks (25 patients, 30.49%) and up to three weeks (11 patients, 13.41%). Additional
information is given in Table A16.
VIII.2.4.3. Pre-treatment
Most patients stated a pre-treatment of acute episode (254 patients, 66.67%) while
127 patients (33.33%) were not previously treated. Almost three-quarters of pre-treated
patients stated one pre-treatment (73.23% of patients with pre-treatment), followed by two
(16.14%), three (7.48%), and four pre-treatments (2.36%). Only for one single patient five and
six pre-treatments, respectively, were documented (0.39%).
Medication was classified according to the ATC anatomical main group (Table A17). Treatment
with corticosteroids for systemic use (172 patients, 45.14% of all patients) and
antidiarrheals/intestinal antiinflammatory or antiinfective agents (80 patients, 21.00%) were
most frequently reported (Figure 6).
Figure 6: Pre-treatment of acute episode according to ATC anatomical main group (n=381).
In addition, medication was classified according to ATC chemical substances (Table A18). Most
commonly reported chemical compounds were prednisolone (137 patients, 35.96% of all
patients) and mesalazine (55 patients, 14.44%). Azathioprine (9.71%) was indicated for
37 patients and budesonide was reported for 31 patients (8.14%). All other chemical
substances were documented with a percentage below 5%. All chemical substances are listed
in Table A18-A19.
45.14%
21.00%
16.27%
2.36%
1.84%
1.84%
1.05%
0.79%
0.79%
0.79%
0.79%
0.26%
0.26%
0.26%
0.26%
0.26%
0.26%
0.26%
33.33%
0% 10% 20% 30% 40% 50%
Corticosteroids for systemic use
Antidiarrheals, intestinal antiinflammatory/…
Immunosuppressive agents
Antibacterials for systemic use
Analgesics
Stomatological preparations
Vitamins
Antianemic preparations
Corticosteroids, dermatological preparations
Cytostatics
Drugs for acid related disorders
Antiprotozoals
Antivirals for systemic views
Drugs for functional gastrointestinal…
Laxatives
Lipid modifying agents
Mineral supplements
Other dermatological preparations
Without pre-treatment
Page 44
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 19
VIII.2.4.4. Ongoing pre-treatment
At enrolment, continuation of pre-treatment of acute episode was documented for 141 from
381 patients (37.01%). One continued pre-treatment was recorded for most of them
(113 patients, 80.14% of patients with ongoing pre-treatment when medication was classified
according to the anatomical main group; Table A20).
Medication was classified according to ATC anatomical main group (Table A20) and chemical
substances (Table A21-A22), respectively. With regard to the anatomical main group,
corticosteroids for systemic use were most frequently reported (93 patients, 66.67% of the
patients with continued pre-treatment), followed by antidiarrheals/intestinal
antiinflammatory or antiinfective agents (46 patients, 32.62%) and immunosuppressive agents
(18 patients, 12.77%). Concerning chemical classification, the following compounds were
specified most often: prednisolone, mesalazine, azathioprine, budesonide, and cortisone
(70 patients, 49.65%; 32 patients, 22.70%; 18 patients, 12.77%; 17 patients, 12.06%;
15 patients, 10.64%).
VIII.2.4.5. Surgical measures for pre-treatment of acute episode
From 381 patients, the majority was without any surgical measures for pre-treatment of acute
episode before start of the NIS (358 patients, 93.96%). Operative interventions were reported
for 23 patients (6.04%). 19 patients had one measure (4.99%) and two patients each had two
or three operations (0.52%). Ileocecal resection was the most frequently noted measure
(8 patients, 34.78% of the patients with operation), followed by abscess drainage (4 patients,
17.39%), fistula drainage, hemicolectomy, and small bowel resection (3 patients each,
13.04%). Additional information is given in Table A23.
VIII.2.5. Disease activity
Disease activity was assessed for patients suffering from Crohn’s disease by the Harvey-
Bradshaw-Index (HBI) and for patients with ulcerative colitis by the Mayo-score.
VIII.2.5.1. Activity of Crohn’s disease
Data on disease activity according to the
HBI was available for 221 patients and was
classified as follows: remission
(0-4 points), mild disease (5-7 points) and
moderate disease (8-16 points). The mean
value was 6.84 (±4.15, median 7.00)
points. A remission of disease was
determined for 74 patients (33.48%), a
mild disease activity for 54 patients
(24.43%) and a moderate disease activity
for 93 patients (42.08%, Figure 7). Data of
two patients were missing (Table B15). Figure 7: Assessment of Crohn’s disease according to the HBI
(n=221).
33.48%
24.43%
42.08%
Remission
Mild disease
Moderate disease
Page 45
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 20
The intestinal localisation of acute episodes of Crohn’s disease according to the Montreal-
classification was available for 220 patients (98.65% of all patients with Crohn’s disease). Most
intestinal manifestations were located at the terminal ileum (91 patients, 41.36% of the
patients with data on intestinal localisation), the colon (88 patients, 40.00%), and the ileocolon
(80 patients, 36.36%). Other parts of the gastrointestinal tract were less frequently affected.
An overview of all localizations stated is given in Figure 8 and listed in Table B16.
Figure 8: Intestinal localization of Crohn’s disease according to the Montreal-classification (n=220).
Information on fistula and extraintestinal manifestations were documented for 220 patients
and 223 patients, respectively. Formation of fistulae was affirmed by 39 patients (17.73%) and
extraintestinal manifestation was confirmed by 54 patients (24.22%). Most of the patients
with extraintestinal complaints suffered from arthralgia (27 patients, 50.00% of the patients
with extraintestinal manifestation; Figure 9, Table B17).
Figure 9: Extraintestinal localization of Crohn’s disease (n=54 patients with extraintestinal manifestation).
41.36%
40.00%
36.36%
6.82%
0.91%
0.45%
0.45%
0.45%
0.45%
0.45%
0.45%
0% 5% 10% 15% 20% 25% 30% 35% 40% 45%
Terminal ileum
Colon
Ileocolon
Upper gastrointestinal tract
Duodenum
Anastomosis
Ileocecal valve
Lower gastrointestinal tract
Neoterminal ileum
Perianal area
Preterminal ileum
50.00%
24.07%
14.81%
5.56%
3.70%
3.70%
3.70%
1.85%
1.85%
1.85%
1.85%
1.85%
0% 10% 20% 30% 40% 50% 60%
Arthralgia
New fistulae
Anal fissures
Aphthous ulcerations
Abscess
Erythema nodosum
Uveitis
Fistula
Hydronephrosis
Ileocoecal resection
Myalgias
Pyoderma gangrenosum
Page 46
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 21
VIII.2.5.2. Activity of ulcerative colitis
Disease activity was classified according to
the Mayo-score either as normal
(0-1 point), mild (2-5 points) or
moderate/severe (>5 points). For
154 patients, the mean value was
7.32 (±2.65, median 8.00) points. Normal
activity of disease was calculated for
6 patients (3.90%), a mild disease activity
for 23 patients (14.94%) and a moderate to
severe disease activity for 125 patients
(81.17%; Figure 10). Information of
four patients was missing (Table C15). Figure 10: Assessment of ulcerative colitis according to the
Mayo-score (n=154).
Information on the intestinal localisation of the acute episode of ulcerative colitis according
to the Montreal-classification was available for 156 patients (98.73% of all patients with
ulcerative colitis). Intestinal manifestations were mostly described as a left-hand colitis of the
descending and sigmoid colon (84 patients, 53.16% of patients with information on intestinal
manifestation) as well as a pancolitis of the colon (62 patients, 39.24%). An overview of all
types is depicted in Figure 11 and listed in Table C16.
Figure 11: Intestinal localization of ulcerative colitis according to the Montreal-classification (n=158).
Extraintestinal manifestations were noticed for 27 patients (17.09% of all patients with
ulcerative colitis). Mostly stated complaint was arthritis (14 patients, 8.86%; Figure 12, Table
C17).
53.16%
39.24%
10.13%
0.63%
0.63%
0.63%
0.63%
0% 10% 20% 30% 40% 50% 60%
Left-hand colitis
Pancolitis
Proctitis
Colon
Colon descendens
Cytomegalovirus infection
Subtotal colitis
3.90%
14.94%
81.17%
Normal
Mild
Moderate/severe
Page 47
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 22
Figure 12: Extraintestinal localization of ulcerative colitis (n=158).
VIII.2.6. Imaging diagnostics
At baseline (visit 0), physicians documented whether and which imaging procedure(s) were
already carried out in order to assess the condition of the mucous membrane. In addition,
physicians were asked for global assessment of the acute episode (normal findings, mild,
moderate or severe episode). No imaging procedure was applied to 123 patients (32.28%)
whereas 258 patients (67.72%) were investigated by imaging diagnostics.
For most patients who underwent an imaging procedure, endoscopy was documented
(223 patients), followed by sonography (110 patients) and magnetic resonance imaging
(25 patients).
For 10 patients with an endoscopic examination, the acute episode was assessed by
endoscopy as unobtrusive (normal finding, 4.48%). 29 patients (13.00%) had a mild episode,
99 patients (44.39%) a moderate episode and for 85 patients (38.12%) the episode was
reported severe. Result of sonography was stated to be normal in 23 cases (20.91%).
Furthermore, the acute episode was assessed as mild in 16 patients (14.55%), moderate in
54 patients (49.09%) or severe in 17 patients (15.45%). Three patients (12.00%) with magnetic
resonance imaging had a normal finding. For four patients (16.00%) the acute episode was
mild, for 10 patients (40.00%) it was moderate and eight patients (32.00%) suffered from a
severe episode.
Other imaging procedures were reported for fewer patients. Detailed information is listed in
Table A25.
VIII.2.7. Laboratory parameters
Physicians documented at the start of the NIS whether and which laboratory parameters were
determined prior to treatment with Remsima®. A full list of reported laboratory data is given
in Tables A26-27. Mean values including standard deviations of individual parameters are
depicted in the following table (Table 4).
8.86%
3.16%
1.27%
1.27%
1.27%
0.63%
0.63%
0.63%
0.63%
0.63%
0.63%
0% 2% 4% 6% 8% 10%
Arthritis
Bechterew's disease
Erythema nodosum
Primary sclerosing…
Psoriasis
Anaemia
Glaucoma
Gonarthritis
Joint trouble
Pankreatitis
Uveitis
Page 48
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 23
Table 4: Laboratory parameters
Parameter Patients Mean value (±SD)
Erythrocytes (Mio/µl) 327 4.52 (±0.56)
Leukocytes (Tsd/µl) 335 9.24 (±3.80)
Thrombocytes (Tsd/µl) 334 344.77 (±129.40)
Hemoglobin (mmol/l) 350 8.30 (±1.51)
Hematocrit (%) 301 39.33 (±5.42)
Serum iron (µmol/l) 130 12.96 (±6.88)
Ferritin (µg/l) 140 98.27 (±108.72)
Transferrin (mg/dl) 71 268.62 (±56.15)
Transferrin saturation (%) 74 21.29 (±15.87)
Urea (mg/dl) 94 18.10 (±14.22)
Creatinine (mg/dl) 242 0.85 (±0.22)
C-reactive protein (mg/l) 345 37.69 (±80.59)
Erythrocyte sedimentation rate (mm) 72 25.21 (±19.70)
Calprotectin (µg/g) 147 747.20 (±831.44)
Concerning data on erythrocytes, most of 327 patients showed values within the reference
range1 (241 patients, 73.70%; reference 4.6-5.9 Mio/µl, male; 4.0-5.2 Mio/µl, female). Values
regarding leukocytes were also for most of the 335 patients within the normal area ranging
from 4.0 to 10.0 Tsd/µl (216 patients, 64.48%). For 191 patients (57.19%), the number of
thrombocytes was higher than the reference (150.0-300.0 Tsd/µl) and 140 patients (41.92%)
had normal values.
About half of 350 patients had normal haemoglobin levels (184 patients, 52.57%) and 42.29%
of the patients had a concentration below the reference area (reference 8.7-11.2 mmol/l,
male; 7.5-9.9 mmol/l, female; 148 patients).
From 301 patients, 146 patients each (48.50%) had a hematocrit proportion within or below
the normal range of 43.0-49.0% (males) and 37.0- 45.0% (females), respectively.
For 63.85% of the patients, serum iron concentration was documented to be within the
reference area (9.0- 29.0 µmol/l, males; 9.0- 27.0 µmol/l, females; 83 patients from
130 patients with measurement) and for 33.08% values were below the normal range
(43 patients).
Applied reference area of ferritin for males was between 30.0-300.0 µg/l and for females
between 10.0-200.0 µg/l, respectively. About three quarters of a total of 140 documented
patients had levels within the normal range (75.71%).
1 Center-specific reference values were not available, therefore global values were applied. All reference values
used are depicted in Table A27.
Page 49
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 24
Additional information and details about laboratory parameters at baseline are available in
the corresponding Tables A26-A27.
VIII.2.8. Pre-treatment of underlying inflammatory bowel disease (IBD)
Pre-treatment of IBD was documented for 326 patients (85.56% of all patients). For the
majority of patients one or two pre-treatments were recorded by the physicians (183 patients,
48.03%; 107 patients, 28.08%). Most commonly reported treatments were
immunosuppressive agents (193 patients, 50.66%), antidiarrheals/intestinal antiinflammatory
or antiinfective agents (184 patients, 48.29%) and corticosteroids for systemic use (89 patients,
23.36%) when classified according to ATC anatomical main group (Tables A28). An overview is
given in Figure 13.
Figure 13: Pre-treatment of underlying IBD according to ATC anatomical main group (n=381).
Concerning chemical classification, the following compounds were specified most frequently:
mesalazine, azathioprine, prednisolone, budesonide, adalimumab and infliximab
(158 patients, 41.47%; 133 patients, 34.91%; 71 patients, 18.64%; 57 patients,
14.96%; 57 patients, 14.96%; 36 patients, 9.45%). All other chemical substances were reported
with a proportional distribution below 5.00% and are fully listed in Tables A30-A31. Pre-
treatment with one or two compounds was most commonly reported (146 patients, 38.32%;
115 patients, 30.18%; Table A30).
VIII.2.9. Concomitant disease
From 381 patients, 100 patients (26.25%) suffered from concomitant disease. One or two
diseases were most frequently reported (60 patients, 15.75%; 20 patients, 5.25%; Table A33).
As classified according to the MedRA preferred code, hypertension (18 patients, 4.72%),
50.66%
48.29%
23.36%
6.30%
1.57%
0.79%
0.52%
0.52%
14.44%
0% 10% 20% 30% 40% 50% 60%
Immunosuppressive agents
Antidiarrheals, intestinal antiinflammatory/antiinfective agents
Corticosteroids for systemic use
Cytostatics
Stomatological preparations
Antiinflammatory and antirheumatic products
Antianemic preparations
Drugs for acid related disorders
…
Without pretreatment
Page 50
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 25
depression (8 patients, 2.10%), hypothyroidism (8 patients, 2.10%), gastrooesophageal reflux
disease (6 patients, 1.57%), and coronary artery disease (5 patients, 1.31%) were most
commonly mentioned (Table A33). Further details on all documented concomitant diseases
are listed in Tables A33-36.
The most frequent system organ classes according to MedDRA were gastrointestinal disorders
(23 patients, 6.04%), vascular disorders (22 patients, 5.77%), musculoskeletal and connective
tissue disorders (17 patients, 4.46%), metabolism and nutrition disorders (14 patients, 3.67%),
cardiac disorders (10 patients, 2.62%), and endocrine disorders (10 patients, 2.62%; Table
A37).
Further concomitant diseases specified by MedDRA system organ class were documented for
less than 10 patients and are listed in Tables A37-A38.
VIII.2.10. Treatment of concomitant disease
A medical treatment of concomitant illness was documented in 79 patients (20.73%). One or
two treatments were most frequently reported (50 patients, 13.12%; 20 patients, 5.25%;
Table A39).
Medication was classified according to ATC anatomical main group (Tables A39-A40) and
chemical substances (Table A41-A43), respectively. With regard to the anatomical main group,
agents acting on the renin-angiotensin system (14 patients, 3.67% of patients with co-
medication), corticosteroids for systemic use (11 patients, 2.89%) and drugs for acid related
disorders (8 patients, 2.10%) were most frequently reported.
Concerning chemical classification, the following compounds were specified most commonly:
prednisolone, ramipril, iron (iii) hydroxide polymaltose complex, levothyroxine sodium, and
pantoprazole (10 patients, 2.62%; 7 patients, 1.84%; 6 patients, 1.57%; 6 patients, 1.57%;
6 patients, 1.57%; Table A41-A43).
Page 51
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 26
VIII.3. Treatment with Remsima®
VIII.3.1. Switch to Remsima®
At baseline (visit 0), physicians were asked why the patients were to be treated with
Remsima®. From a total of 381 patients, reasons were specified for 377 patients (98.95%). For
the majority of patients, one reason was documented (346 patients, 90.81%). Up to
three reasons were recorded by the attending physician (Table A44).
The most frequently stated reasons to start a therapy with Remsima® were switch of
treatment due to low effectiveness of the previous medication (240 patients, 63.66% of
patients with data on reasons for switch) and treatment initiated due to contraindication or
intolerance to conventional therapy (92 patients, 24.40%).
Further details and reasons for prescription of Remsima® are illustrated in the following figure
(Figure 14). An entire list of all mentioned reasons is available in Tables A44-A45.
Figure 14: Reasons to start a therapy with Remsima® (n=377).
VIII.3.2. Administered dose of Remsima®
Details on dose of Remsima® were analyzed at baseline (visit 0) for 376 patients, at visit
1 (about two weeks after start of treatment) for 244 patients, at visit 2 (about six weeks after
therapy start) for 252 patients, and at visit 3 (about 14 weeks after start of treatment) for
238 patients.
63.66%
24.40%
9.81%
2.65%
1.86%
0.80%
0.80%
0% 10% 20% 30% 40% 50% 60% 70%
Switch of treatment due to loweffectiveness of the previous medication
Treatment initiated due to contraindicationor intolerance to conventional therapy
Switch of treatment due to low tolerabilityof the previous medication
No reason specified
Recommencement of treatment after break
Cortisone/steroid dependency
Start of treatment
…
Page 52
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 27
Mean dose of Remsima® was
documented by the attending
physicians at baseline, control visits
(1-2) and at the end of the study
(visit 3). Dosage was relatively stable
during the course of the NIS and
increased only slightly from
5.09 mg/kg body weight (BW) at
baseline to 5.22 mg/kg BW at the
last documentation (Figure 15, Table
A46).
Figure 15: Remsima dose (mg/kg body weight, patients with infusion only) at admission (V0, n=376), V1 (n=244), V2 (n=252), and V3 (n=238; x = mean, – = median, [] = interquartile, - = minimum and maximum).
According to SmPC, Remsima® dose should be 5 mg/kg body weight (BW). The majority of
patients received the recommended dosage during the course of the NIS (316 from a total of
376 patients at V0; 192 from a total of 244 patients at V1; 201 from a total of 252 patients at
V2; 184 from a total of 238 patients at V3; Table 47). A moderate increase of patients who
received >5 mg/kg BW was recorded from baseline to visit 3 (11.44% versus 17.65%) whereas
the number of patients treated with 5 mg/kg BW was slightly reduced (84.04% versus 77.31%).
An overview of the distribution of dose is given in Figure 16.
Figure 16: Distribution of Remsima® dose (mg/kg BW) during the course of the NIS.
5.09 5.07 5.13 5.22
0
2
4
6
8
10
12
V0 V1 V2 V3
4.52% 5.33% 3 57% 5.04%
84.04% 78.69% 79.76% 77.31%
11.44% 15.98% 16.67% 17.65%
0%
20%
40%
60%
80%
100%
Visit 0 (n=376) Visit 1 (n=244) Visit 2 (n=252) Visit 3 (n=238)
>5 mg/kg BW
5 mg/kg BW
<5 mg/kg BW
Page 53
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 28
VIII.3.3. Premature end of therapy with Remsima®
Most of the patients did not abort
Remsima®-treatment during the course
of the NIS (336 patients, 88.19%; Figure
17). Patients who discontinued the study
prematurely (45 patients, 1.81%) stated
in most cases one reason for termination
(36 patients, 80.00% of patients with
premature end). Two causes were
mentioned by nine patients (20.00%,
Table A49).
Figure 17: Frequency of patients with discontinuation of Reasons for a premature termination of treatment with Remsima® are depicted in the
following figure (Figure 18). Adverse drug reaction, lack off efficacy and due to patients’
request were the most frequent causes for dropout (31 mentions, 8.14%; 7 mentions, 1.84%;
7 mentions, 1.84%). Further details are given in Table A49.
Figure 18: Reasons for premature discontinuation of therapy with Remsima® (n=381).
VIII.3.4. Treatment of underlying inflammatory bowel disease (IBD) during the study
Treatment of underlying IBD during the study was documented for 208 patients (54.59%). For
the majority of patients one or two treatments were recorded by the physicians (140 patients,
67.31% of patients with concomitant treatment; 54 patients, 25.96%). Most commonly
reported treatments were antidiarrheals/intestinal antiinflammatory or antiinfective agents
(128 patients, 61.54% of patients with treatment of IBD), corticosteroids for systemic use
(75 patients, 36.06%), and immunosuppressive agents (66 patients, 31.73%) when classified
according to ATC anatomical main group (Tables A50). An overview of most frequently
documented treatments is given in Figure 19 (percentage distribution of all patients).
8.14%
1.84%
1.84%
1.05%
0.52%
0.52%
0.26%
0% 2% 4% 6% 8% 10%
Adverse drug reaction
Lack of efficiency
At patient's request
Adverse event
On request of health insurance
Other biosimilar
Patient stayed away
88.19%
11.81% Withoutpremature end oftherapy
Premature end oftherapy
Page 54
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 29
Figure 19: Treatment of underlying IBD during the study, classified according to ATC anatomical main group (n=381).
Concerning chemical classification of concomitant IBD treatment, the following compounds
were specified most frequently: mesalazine, azathioprine, prednisolone, budesonide,
cortisone and prednisone (109 patients, 52.40% of patients with concomitant treatment
during the NIS; 64 patients, 30.77%; 60 patients, 28.85%; 24 patients, 11.54%; 10 patients,
4.81%; 7 patients, 3.37%). Treatment with one or two compounds was most commonly
reported (127 patients, 61.06%; 59 patients, 28.37%; Table A51). Figure 20 shows the most
often recorded chemical substances (percentage distribution of all patients). All other
chemical substances are listed in Tables A51-A52.
33.60%
19.69%
17.32%
1.05%
1.05%
45.41%
0% 10% 20% 30% 40% 50%
Antidiarrheals, intestinal antiinflammatory/antiinfective agents
Corticosteroids for systemic use
Immunosuppressive agents
Antianemic preparations
Cytostatics
…
Without treatment
Page 55
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 30
Figure 20: Treatment of underlying IBD during the study, classified according to ATC chemical substances (n=381).
VIII.3.5. Acute episode
VIII.3.5.1. Hospitalization
Regarding hospitalization during the
study, physicians were asked if patients
had to be treated in the clinic due to an
acute episode. Almost all patients were
not hospitalized during the whole study
period (351 patients, 96.43% of the
patients with data on hospitalization
versus 13 patients, 3.57%). Information
of one patient was missing (Table A53).
Figure 21: Hospitalization due to an acute episode during the NIS (n=364).
Patients with hospitalization stayed on average 1.48 (±0.93, 1.29 median) weeks at the
hospital. The time varied from 0.29 (minimum) up to 4.00 weeks (maximum). 66.67% of the
patients who had been hospitalized stayed more than one to two weeks in the clinic
(8 patients), followed by up to one week (3 patients, 25.00%) and more than tree to four weeks
(1 patient, 8.33%). Information was missing for one patient. Corresponding data are given in
Table A54.
28.61%
16.80%
15.75%
6.30%
2.62%
1.84%
45.41%
0% 10% 20% 30% 40% 50%
Mesalazine
Azathioprine
Prednisolone
Budesonide
Cortisone
Prednisone
…
Without treatment
3.57%
96.43%
Withhospitalization
Withouthospitalization
Page 56
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 31
VIII.3.5.2. Imaging procedures
Physicians documented at each visit throughout the NIS whether and which imaging
procedures were performed in order to assess the condition of the mucous membrane (Figure
22).
As a result, 321 patients (87.70%) had not
been examined by imaging procedures
whereas a total of 45 patients (12.30%)
had been investigated by imaging
diagnostics during the NIS (Figure 22,
Table A55).
Figure 22: Imaging procedures during the study (n=366).
In addition, physicians were asked for global assessment of the acute episode (categorized
into normal findings, mild, moderate or severe episode). Details are depicted below in Figure
23 and refer to data in Table A56.
Figure 23: Finding of imaging diagnostics during the NIS.
For most patients who underwent an imaging procedure, sonography was documented
(26 patients), followed by endoscopic examination (23 patients), magnetic resonance imaging
(3 patients), and examination by CAT scanner (2 patients).
50.00
33.33
26.09
61.54
34.78
23.08
50.00
66.67
17.39
7.69
21.74
7.69
0% 20% 40% 60% 80% 100%
CAT scanner (n=2)
Magnetic resonanceimaging (n=3)
Endoscopy (n=23)
Sonography (n=26)
Normal findings Mild episode Moderate episode Severe episode
12.30%
87.70%
Yes No
Page 57
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 32
For 26 patients with sonographic examination, the acute episode was assessed as unobtrusive
(normal finding, 61.54%). Six patients had a mild episode (23.08%), two patients a moderate
episode (7.69%) and for two patients the episode was reported severe (7.69%). Result of
patients with an endoscopy was stated to be normal in six cases (26.09%). Furthermore, the
acute episode was assessed as a mild (8 patients, 34.78%), moderate (4 patients, 17.39%) or
severe episode (5 patients, 21.74%). One patient (33.33%) showed a normal finding and for
two patients (66.33%) a severe episode was documented when examined by magnetic
resonance imaging. Two patients were examined by CAT scanner, which resulted in a normal
condition and moderate episode, respectively (50% each; Table A56).
VIII.3.5.3. Surgical measures
From a total of 365 patients, almost all patients were without any surgical measures for
treatment of acute episode during the NIS (377 patients, 98.95%). Operative interventions
were reported for four patients (1.05%). Two of them had a fistula drainage (50.00% of
patients with an operation) and for one patient each an abscess drainage and hemicolectomy,
respectively, was documented during the study (25.00% each, Table A57).
VIII.3.6. Antibodies before and during the study
Physicians should report data on antibody detection (if applicable) for patients under
infliximab treatment at each visit. Data were provided for 35 patients and are listed in Tables
A58-64.
IX. EFFICACY RESULTS
Investigation of the patient’s questionnaires was performed for the total sample as well as for
the subgroups (patients with Crohn’s disease and patients with ulcerative colitis). Analysis was
carried out once for cases with any values, for the complete cases only, and according to the
LOCF-method. The following results refer to LOCF-values.
IX.1. Inflammatory bowel disease questionnaire (IBDQ)
The IBDQ is an international validated disease specific instrument to assess the health-related
quality of life and consists of 34 questions, which are divided in 4 topics: subjective
experienced bowel symptoms, emotions, systemic symptoms, and social functions (Janke et
al. 2005). A value of one point indicates the worst quality of life whereas the best quality of
life corresponds to seven points.
Page 58
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 33
Data of 311 patients were available
for statistical analysis. The mean
value of IBDQ increased from
4.37 (±1.25, median 4.47) points at
admission to 5.21 (±1.13, median
5.44) at the final visit indicating a
significant better quality of life
under treatment with Remsima®
(p<0.0001; Figure 24, Tables A65-
A66). The mean difference from the
initial to the last documentation was
0.84 (±1.14, median 0.64).
Figure 24: IBDQ at admission (V0), at control examinations V1 and V2 and at the final examination (n=311, LOCF; x = mean, – = median, [] = interquartile, - = minimum and maximum).
Stratification of the sample in patients suffering from Crohn’s disease or ulcerative colitis
implied a general improvement of quality of life according to the IBDQ. In general, patients
with Crohn’s disease showed higher values at baseline and at each of the following
examinations compared to patients with ulcerative colitis, however, the difference of the
IBDQ-values was statistically significant for both subgroups (p<0.0001 each; Figure 25, Tables
B56-B57 and C53-A54).
Figure 25: Mean IBDQ-values (LOCF) for patients with Crohn’s disease and ulcerative colitis.
4.37
4.96 5.18 5.21
1
2
3
4
5
6
7
V0 V1 V2 V3
1
2
3
4
5
6
7
V0 V1 V2 V3
Crohn's disease (n=185) Colitis ulcerosa (n=126)
Page 59
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 34
Figure 26 depicts the subscores of the IBDQ. The figure shows that an improvement was
achieved in all areas.
Figure 26: Mean IBDQ-values (LOCF) for patients with Crohn’s disease and ulcerative colitis.
IX.2. Brief fatigue inventory (BFI)
The BFI score was originally developed to measure severity of fatigue in cancer patients. It
includes the following 6 items: activity, mood, walking ability, work, relations to other people,
and enjoyment of life (Radbruch et al. 2003). Rating of 0 means no fatigue and rating of
10 corresponds to fatigue as bad as one can imagine. Scores are categorized into mild
(1-3 points), moderate (4-6 points) or severe (7-10 points).
A total of 318 patients were included
in the analysis of fatigue. Mean BFI
value decreased from 4.55 (±2.31,
median 4.67) points at baseline to
3.62 (±2.30, median 3.28) points at
the final examination. The mean
reduction of BFI points from the
initial to the last documentation was
statistically significant. BFI was
reduced by 0.94 (±2.16,
median 0.77) points (p<0.0001;
Figure 27, Tables A75-A76).
Figure 27: BFI at admission (V0), at control visits (V1, V2) and at the end of the NIS (V3; n=318, LOCF; x = mean, – = median, [] = interquartile, - = minimum and maximum).
1
2
3
4
5
6
7Bowel symptoms
Emotional function
Systemic symptoms
Social function
1=worst quality of life , ..., 7=best quality of life
V0
Last measurement
4.553.82 3.73 3.62
0
2
4
6
8
10
12
V0 V1 V2 V3
Page 60
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 35
BFI-values significantly decreased in patients with Crohn’s disease and in patients with
ulcerative colitis (p<0.0001). Patients with ulcerative colitis had lower values at baseline and
at each examination compared to patients with ulcerative colitis (Figure 28, Tables B68-
B69 and C66-C67).
Figure 28: Mean BFI-values (LOCF) of patients with Crohn’s disease and ulcerative colitis.
IX.3. General depression scale – long version (ADS-L)
The ADS-L served as a self assessment tool to evaluate the impairment due to depressive
symptoms. It contains 20 items on emotional, motivational, cognitive, somatic, and motoric
complaints. The sum score may range between 0 and 60 points whereas values >23 points
indicate serious depressive disorders (Hautzinger und Bailer 1993).
ADS-L values of 277 patients were
analyzed. A significant decrease of
the ADS-L mean value was
determined from the admission to
the last value of the final
examination with a difference of
4.78 (±11.09, median 4.00;
p<0.0001). Nevertheless, mean
values of ADS-L suggested an
absence of clinically relevant
depressive symptoms prior to
Remsima® therapy and during the
observation period (Figure 29).
Corresponding data are shown in
Tables A77-A78.
Figure 29: ADS-L values at admission (V0), at control examinations (V1 and V2) and at the end of the study (V3; n=277, LOCF; x = mean, - = median, [] = interquartile, - = minimum and maximum).
1
2
3
4
5
6
7
V0 V1 V2 V3
Crohn's disease (n=191) Colitis ulcerosa (n=127)
20.6917.18 15.74 15.91
0
10
20
30
40
50
60
V0 V1 V2 V3
Page 61
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 36
ADS-L values were significantly reduced for both, patients with Crohn’s disease and ulcerative
colitis (p<0.0001). Patients with ulcerative colitis showed slightly lower values during the
whole study compared to patients with Crohn’s disease. However, neither the change of
values during the study nor the difference between the two groups of patients might be
medically significant (Figure 30, Tables B70-71 and C68-A69).
Figure 30: Mean ADS-L values (LOCF) for patients with Crohn’s disease and ulcerative colitis.
IX.4. Short-form McGill Pain questionnaire (SF-McGill)
The SF-McGill was used to evaluate abdominal pain. It consists of 15 items (11 sensory and
4 affective) rated on an intensity scale from 0 (=no pain) to 3 (=severe pain). Additionally, the
present pain intensity (PPI) and a visual analogue scale (VAS) ranging from 0 (=no pain) to
100 (=worst imaginable pain) were included to provide overall pain intensity scores (Melzack
1987). The following results refer to analyses of the VAS-values of the SF-McGill questionnaire.
VAS-values of 282 patients were
analyzed. A significant decrease of
mean value was determined from
the baseline (27.32±25.39; median
23.00) to the last documentation
(18.22±22.16, median 7.00) showing
a difference of 9.00 (±25.90, median
4.00; p<0.0001; Figure 31). Further
details are presented in Tables A85-
A86.
Figure 31: VAS values of SF-McGill at admission (V0), at control examinations (V1, V2) and at the final documentation (n=282, LOCF; x = mean, – = median, [] = interquartile, - = minimum and maximum).
Subgroup analysis revealed that patients suffering from ulcerative colitis showed slightly
higher VAS-values at baseline compared to patients with Crohn’s disease (27.71 versus 26.91).
0
10
20
30
40
50
60
V0 V1 V2 V3
Crohn's disease (n=163) Colitis ulcerosa (n=114)
27.2320.90 17.70 18.22
0
10
20
30
40
50
60
70
80
90
100
V0 V1 V2 V3
Page 62
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 37
The decrease from admission to the last documentation was statistically significant for both
subgroups (p<0.0001; Figure 32), but reduction of mean values was more pronounced in
patients with ulcerative colitis than in patients suffering from Crohn’s disease (10.51 versus
8.01; Tables B78-B79 and C76-C77).
Figure 32: Mean VAS values (LOCF) of SF-McGill for patients with Crohn’s disease and ulcerative colitis.
IX.5. Assessment of disease activity
IX.5.1. Crohn’s disease assessed by Harvey Bradshaw index
The Harvey Bradshaw index (HBI) was used to assess disease activity of Crohn’s disease and
consists of the following clinical parameters: general well-being, abdominal pain, number of
liquid stools per day, abdominal mass, and complications (Harvey und Bradshaw 1980). A
score less than 5 points indicated a remission state and patients with higher scores were
considered to have a mild (5-7 points), moderate (8-16 points) or severe (>16 points) disease.
Activity of Crohn’s disease was
reduced during the treatment with
Remsima® (Figure 33). The mean
HBI-value of 6.91 (±4.14, median
7.00) points at baseline significantly
decreased to 3.06 (±3.25, median
2.00) at the last documentation
(p<0.0001; Tables B54-B55).
Figure 33: Activity of Crohn’s disease assessed with HBI at admission (V0), at control examinations V1 and V2, and at the last visit (V3; n=213, LOCF; x = mean, – = median, [] = interquartile, - = minimum and maximum).
0
10
20
30
40
V0 V1 V2 V3
Crohn's disease (n=170) Colitis ulcerosa (n=112)
6.91
3.943.22 3.06
0
2
4
6
8
10
12
14
16
V0 V1 V2 V3
Page 63
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 38
IX.5.2. Ulcerative colitis assessed by Mayo-score
The Mayo-score includes clinical and endoscopic characteristics to evaluate the disease
activity of ulcerative colitis: stool frequency, rectal bleeding, mucosal appearance, and
physician rating of disease activity (Lewis et al. 2008). Values between 2-5 correlate to a mild
disease and values of 6-12 indicate a moderate to severe finding.
Disease activity of ulcerative colitis
was determined at baseline, at the
follow-up visits and at the last
examination. The mean score
significantly decreased from
7.27 (±2.66, median 8.00) points to
2.81 (±2.59, median 2.00) points
(p<0.0001, Tables C52-C53).
Development of disease activity
during Remsima®-treatment is
illustrated in Figure 34.
Figure 34: Activity of ulcerative colitis assessed with Mayo-score at admission (V0), at follow-up visits (V1 and V2) and at the last documentation (V3; n=143, LOCF; x = mean, – = median, [] = interquartile, - = minimum and maximum).
IX.6. Global assessment of efficacy
Efficacy of Remsima® was assessed once by the physicians and once by the patients.
At the final assessment, the attending physicians evaluated the effectiveness of Remsima®
treatment as very good for 30.33% (101 patients). The efficacy was documented to be good
in 54.95% of the cases (183 patients), moderate in 13.81% (46 patients) and poor in 0.90%
(3 patients, Table A87).
Concerning the result of patient’s assessment, the percentage distribution was comparable to
the documentation of the physicians. Efficacy of Remsima® treatment was rated as very good
by 28.40% of the patients (94 patients) at the last assessment. The percentage of patients who
rated effectiveness as good was 53.47% (177 patients) whereas 16.92% of the patients
(56 patients) assessed the efficacy as moderate and 1.21% (4 patients) as poor, respectively
(Table A88).
7.27
3.97
2.98 2.81
0
2
4
6
8
10
12
V0 V1 V2 V3
Page 64
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 39
Figure 35 shows that the assessments of
the doctors and patients were in good
agreement. A more detailed comparison is
depicted in Table A89. The weighted Kappa
coefficient for the aggreement between
the assessments was 0.65, meaning a
substantial agreement according to Landis
(1977, Table A89 and A90).
Figure 35: Global assessment of efficacy by physician and patient.
IX.7. Laboratory parameters
Physicians were asked to document laboratory values (if applicable) during the course of the
NIS. Data on the following parameters were recorded: erythrocytes, leukocytes,
thrombocytes, haemoglobin, hematocrit, serum iron, ferritin, transferrin, transferrin
saturation, urea, creatinine, C-reactive protein, erythrocyte sedimentation rate, and
calprotectin (Table A91-A132). Reticulocytes were recorded only in one patient at baseline
and one follow up visit. Therefore, the values of this parameter are not displayed here.
Analysis was carried out once for cases with any values, for the complete cases only, and
according to the LOCF-method. The following results refer to LOCF-values.
Concerning erythrocytes (n=259), the number slightly increased from 4.52 Mio/µl (±0.55,
median 4.57) at baseline to 4.61 (±0.49, median 4.60) Mio/µl at the final documentation with
a mean difference of 0.09. The mean increase was statistically significant (p=0.0013; Tables
A91-A92). Compared to baseline, more patients showed values within the reference range at
the last examination (204 patients, 78.76% versus 192 patients, 74.13%; reference area: 4.6-
5.9 Mio/µl, male; 4.0-5.2 Mio/µl, female). Further information about the progress of the
number of erythrocytes is provided in Table A93.
Mean value regarding leukocytes (n=275) was reported to be 7.85 (±3.10, median 7.20) Tsd/µl
at last measurement (versus 9.26±3.82 Tsd/µl, median 8.50, at visit 0). Mean reduction of
1.41 was statistically significant (p<0.0001, Tables A94-A95). At both visits (baseline and last
examination), mean numbers of leukocytes were within the normal area ranging from 4.0 to
10.0 Tsd/µl. However, the percentage of patients with normal levels was higher at the end of
the NIS (76.73% versus 65.09 at baseline). Corresponding data are available in Table A96.
30.33% 28.40%
54.95%53.47%
13.81% 16.92%
0.90% 1.21%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Physician Patient
poor
moderate
good
very good
Page 65
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 40
Number of thrombocytes (n=274) significantly decreased by 46.24 (±92.64, median 34.00)
from 345.63 (±124.06, median 317.50) Tsd/µl at baseline to 299.39 (±97.03, median 281.50)
Tsd/µl at the final documentation (p<0.0001, Tables A97-A98). 55.11% of the patients had
normal thrombocyte levels within the reference of 150.0-300.0 Tsd/µl at the end of the NIS
(versus 41.61% at start of Remsima® therapy; Table A99).
Haemoglobin concentration (n=290) was documented to be 8.28 (±1.52, median 8.20) mmol/l
at admission and 8.57 (±1.91, median 8.32) mmol/l at the final documentation, respectively.
The mean value significantly increased by 0.30 (±2.05, median 0.19, p<0.0001, Tables A100-
A101). Compared to the start of the NIS, more patients showed values within the reference
area (8.7-11.2 mmol/l, male; 7.5-9.9 mmol/l, female): 149 patients (51.38%) at visit 0 and
170 patients (58.62%) at last measurement, respectively (Table A102).
Haematocrit proportion (n=231) was comparable between admission and final examination.
Mean value was reported to be 39.04 (±4.59, median 39.90) % at visit 0. At the end of the
study, the mean value was 39.68 (±5.16, median 40.00) % displaying an increase of 0.64 (±5.17,
0.20) percent points under treatment with Remsima® (Table A103-A104). At baseline, 48.05%
of the patients had a haematocrit proportion within the normal range of 43.0-49.0% (males)
and 37.0- 45.0% (females), respectively. At the last visit, a higher percentage of patients
showed normal values (59.74%, Table A105).
Regarding serum ion (n=86), a mean concentration of 12.74 (±7.05, median 11.47) µmol/l was
recorded at baseline. The mean value slightly increased by 1.42 (±8.83, median 1.09) during
the course of the NIS and was found to be 14.17 (±7.61, median 13.15) µmol/l at the end of
the study (Tables A106-A107). As shown in Table A108, number of patients with values within
the reference area (9.0- 29.0 µmol/l, males; 9.0- 27.0 µmol/l, females) increased from
admission to the last visit with percentages of 61.63% compared to 66.28%.
Ferritin levels (n=82) decreased under therapy with Remsima®. Mean concentration was
reported to be 108.32 (±128.74, median 69.50) µg/l at baseline and 89.18 (±106.42, median
65.00) µg/l at the end of the study (Tables A109-A110; mean difference was 19.14 µg/l±13.56,
median 5.95). Reference area of ferritin for males is between 30.0-300.0 µg/l and for females
between 10.0-200.0 µg/l, respectively. Compared to baseline, the number of patients with
reference values had increased during the NIS (73.17% versus 78.05% at the last visit). Further
information is given in Table A111.
Concerning transferrin concentration (n=50) at baseline and final visit, a mean difference of
2.60 (±52.89, median 8.99) mg/dl was documented. Mean values slightly increased from
273.06 (±52.74, median 270.00)mg/dl up to 275.66 (±57.26, median 280.00; Table A112 and
A113). 92.00% of the patients had normal transferrin levels at the end of the study (versus
88.00% at admission). Reference range of transferrin is between 170.0-330 mg/dl (male) and
160.0-350.0 mg/dl (female), respectively (Table A114).
Furthermore, transferrin saturation (n=57) increased from 21.91 (±17.38, median 18.00) % at
baseline to 20.65 (±12.18, median 18.00) % at last measurement and the percentage of
Page 66
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 41
patients with normal levels between 18.0% and 45.0% simultaneously rose from 45.61% to
49.12% (Tables A115-A117).
Mean urea level (n=68) somewhat increased during the NIS and was reported as follows:
16.00 (±15.02, median 6.45) mg/dl at baseline and 16.20 (±13.54, median 8.05) mg/dl at the
end of the study (Tables A117-A118). The number of patients with a normal urea
concentration was similar at visit 0 and final examination (26.47% each; reference ranges from
6.0-26.0 mg/dl). Additional information is available in the corresponding Table A120.
Creatinine concentration (n=179) did not change under the treatment with Remsima®. Mean
value was reported to be 0.83 mg/dl at baseline (±0.22, median 0.80) and last measurement
(±0.17, median 0.82; Tables A121-A122). However, number of patients with normal values
(male: 0.6-1.2 mg/dl; female: 0.5-1.0 mg/dl) increased during the observational time from
92.74% (baseline) to 96.09% (final documentation, Table A123).
The amount of C-reactive protein (n=278) was 34.97 (±75.42, median 10.70) mg/l at admission
and decreased down to 21.11 (±38.65, median 5.62) mg/l at last measurement (Tables A124-
A125). Mean reduction of 13.86 (±70.12, median 1.80) was statistically significant (p<0.0001).
In contrast to a percentage of 48.56% at baseline, 63.67% of the patients had normal values
at the end of the NIS (reference range ≤ 10.0 mg/l). Further information is shown in Table
A126.
Concerning the sedimentation rate of erythrocytes (n=46), mean values were higher at
admission (24.85±21.78 mm, median 22.00 versus 16.96±15.93, median 11.50). Mean
difference was 7.89 (Tables A127-A128). Number of patients with normal values rose from
56.52% to 78.26% during the NIS (reference range of male: ≤20.0 mm; reference range of
female: ≤30.0 mm). Corresponding data are listed in Table A129.
Mean calprotectin concentration (n=61) was reported to be 865.63 (±818.77, median 578.00)
µg/g at baseline. Mean value decreased by 298.23 (±1158.06, median 232.00) down to
567.40 (±831.14, median 310.00) µg/g at last measurement (Tables A130-A121). A reference
value ≤50.0 µg/g was achieved by 19.67% of the patients at last measurement (versus 6.56%
at baseline, Table A132).
Page 67
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 42
Table 5: Laboratory parameters at final examination (LOCF)
Parameter Patients Mean value (±SD)
Erythrocytes (Mio/µl) 259 4.61 (±0.49)
Leukocytes (Tsd/µl) 275 7.85 (±3.10)
Thrombocytes (Tsd/µl) 274 299.39 (±97.03)
Haemoglobin (mmol/l) 290 8.57 (±1.91)
Haematocrit (%) 231 39.68 (±5.16)
Serum iron (µmol/l) 86 14.17 (±7.61)
Ferritin (µg/l) 82 89.18 (±106.42)
Transferrin (mg/dl) 50 275.66 (±57.26)
Transferrin saturation (%) 57 20.65 (±12.18)
Urea (mg/dl) 68 16.20 (±13.54)
Creatinine (mg/dl) 179 0.83 (±0.17)
C-reactive protein (mg/l) 278 21.11 (±38.65)
Erythrocyte sedimentation rate (mm)
46 16.96 (±15.93)
Calprotectin (µg/g) 61 567.40 (±831.14)
X. SAFETY RESULTS
X.1. Global assessment of tolerability
Evaluation of tolerability of Remsima® was performed once by the physicians and once by the
patients (Figure 36).
Page 68
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 43
At the final assessment, the attending physicians evaluated tolerability of Remsima® as very good for 40.72% (136 patients) of the patients. The tolerability was documented to be good in 54.79% of the cases (183 patients), moderate in 3.59% (12 patients) and poor in 0.90% of patients (3 patients, Table A133).
Tolerability of Remsima® treatment was rated as very good by 34.73% (116 patients) of the patients at last assessment. The percentage of patients who rated the tolerability as good was 58.08% (194 patients) whereas 5.69% of the patients (19 patients) assessed the tolerablity as moderate and 1.50% (5 patients) as poor, respectively (Figure 36, Table A134).
Figure 36: Assessment of tolerability of Remsima®.
X.2. Adverse events and adverse drug reactions
All adverse events (AE) and adverse drug reactions (ADR, serious and non-serious) that
occurred during this non-interventional study had to be reported by the attending physician.
The documented events were analysed according to their preferred term and their system
organ class by MedDRA. Low-level terms were not considered in statistical analysis.
X.2.1. Categories
An overview of the categories of events that occurred during the study is given in Table 6.
Table 6: Category and frequency of ADRs occurred and number of patients affected (n=381)
Category Frequency events Frequency patients
n %
Adverse drug reaction (ADR) 65 48 12.60%
− Non-serious ADRs 42 30 7.87%
− Serious ADRs 23 18 4.72%
− Suspected unexpected serious adverse reactions
(SUSAR) 7 4 1.05%
Adverse events (AE) 136 80 21.00%
X.2.1. Adverse drug reactions
The majority of patients were without any adverse drug reaction during the course of the
study (333 from 381 patients, 87.40%). 65 ADRs occurred in 48 patients (12.60%).
40.72%34.73%
54.79%58.08%
3.59% 5.69%
0.90% 1.50%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Physician Patient
poor
moderate
good
very good
Page 69
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 44
For most of the patients with ADRs one type of reaction was reported (37 patients, 77.08% of
the patients with ADRs). Two types were documented for seven patients (14.58%) and four
types of reactions were recorded for four patients (8.33%). In one patient each, the reaction
hypersensitivity and the reaction dizziness, respectively, were recorded twice (Tables A135-
A136).
Most frequently reported ADRs were assigned to the preferred term hypersensitivity (9 events
in 8 patients, 2.10% of all patients), followed by erythema (6 events in 6 patients, 1.57%),
ineffective drug (5 events in 5 patients, 1.31%), and anaphylactic reaction (4 events in
4 patients, 1.05%). The event dizziness was documented for two patients (0.52%, in one
patient twice and in the other one once). Alopecia, fatigue, pruritus, and rash were recorded
as 2 events each in two patients (0.52%). All further ADRs were reported at a frequency of one
event in one patient (0.26%) and are fully listed in the following table according to their
preferred term by MedDRA 20.0.
Table 7: Adverse drug reactions listed according to the preferred term (n=381)
MedDRA 20.0 / Preferred term Events Patients Percent
Hypersensitivity 9 8 2.10%
Erythema 6 6 1.57%
Drug ineffective 5 5 1.31%
Anaphylactic reaction 4 4 1.05%
Dizziness 3 2 0.52%
Alopecia 2 2 0.52%
Fatigue 2 2 0.52%
Pruritus 2 2 0.52%
Rash 2 2 0.52%
Abdominal abscess 1 1 0.26%
Abdominal pain upper 1 1 0.26%
Anaemia 1 1 0.26%
Anaphylactic shock 1 1 0.26%
Arthralgia 1 1 0.26%
Asthenia 1 1 0.26%
Carotid artery dissection 1 1 0.26%
Cerebral infarction 1 1 0.26%
Colitis 1 1 0.26%
Crohn’s disease 1 1 0.26%
Deep vein thrombosis 1 1 0.26%
Drug specific antibody present 1 1 0.26%
Eczema 1 1 0.26%
Page 70
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 45
MedDRA 20.0 / Preferred term Events Patients Percent
Headache 1 1 0.26%
Hepatitis 1 1 0.26%
Hyperhidrosis 1 1 0.26%
Hypertensive crisis 1 1 0.26%
Libido disorder 1 1 0.26%
Musculoskeletal discomfort 1 1 0.26%
Pleural effusion 1 1 0.26%
Pruritus allergic 1 1 0.26%
Psoriasis 1 1 0.26%
Pulmonary tuberculosis 1 1 0.26%
Pustular psoriasis 1 1 0.26%
Rash macular 1 1 0.26%
Stridor 1 1 0.26%
Swelling face 1 1 0.26%
Thrombophlebitis 1 1 0.26%
Upper respiratory tract infection 1 1 0.26%
Urticaria 1 1 0.26%
Uveitis 1 1 0.26%
The ADRs were most frequently associated with the following MedDRA system organ classes
(SOC): skin and subcutaneous tissue dirsorders (14 patients, 3.67%), immune system disorders
(13 patients, 3.41%), general disorders and administration site conditions (8 events, 2.10%),
nervous system disorders (4 patients, 1.05%), gastrointenstinal disorders (3 patients, 0.79%),
infections and infestations (3 patients, 0.79%), vascular disorders, musculoskeletal and
connective tissue disorders, and Respiratory, thoracic and mediastinal disorders (2 patients
each, 0.52%). All further SOCs were affected at a frequency of one (0.26%). Table 8 presents
all affected system organ classes (Table A137).
Table 8: ADRs listed according to the system organ class by MedDRA 20.0 (n=381)
MedDRA 20.0 / System organ class Patients Percent
Skin and subcutaneous tissue disorders 14 3.67%
Immune system disorders 13 3.41%
General disorders and administration site conditions 8 2.10%
Nervous system disorders 4 1.05%
Gastrointestinal disorders 3 0.79%
Infections and infestations 3 0.79%
Vascular disorders 2 0.52%
Musculoskeletal and connective tissue disorders 2 0.52%
Page 71
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 46
MedDRA 20.0 / System organ class Patients Percent
Respiratory, thoracic and mediastinal disorders 2 0.52%
Blood and lymphatic system disorders 1 0.26%
Eye disorders 1 0.26%
Hepatobiliary disorders 1 0.26%
Investigations 1 0.26%
Psychiatric disorders 1 0.26%
Information on structural hierarchy according to MedDRA of the 64 ADRs (48 patients) is given
in Tables A138-A144.
From all documented ADRs, 23 events were recorded to be serious (18 patients, 4.72% of all
patients). The following table shows a list of all serious events (Table 9). Corresponding data
are available in Tables A145-A146. Hypersensitivity and anaphylactic reaction were the most
frequently reported serious ADRs (4 events in 4 patients each, 1.05%). All other serious events
occurred once.
Page 72
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 47
Table 9: Serious adverse drug reactions
MedDRA 20.0 / Preferred term Events Patients Percent
Anaphylactic reaction 4 4 1.05%
Hypersensitivity 4 4 1.05%
Abdominal abscess 1 1 0.26%
Anaemia 1 1 0.26%
Anaphylactic shock 1 1 0.26%
Carotid artery dissection 1 1 0.26%
Cerebral infarction 1 1 0.26%
Colitis 1 1 0.26%
Deep vein thrombosis 1 1 0.26%
Drug ineffective 1 1 0.26%
Drug specific antibody present 1 1 0.26%
Hepatitis 1 1 0.26%
Hypertensive crisis 1 1 0.26%
Pleural effusion 1 1 0.26%
Pulmonary tuberculosis 1 1 0.26%
Pustular psoriasis 1 1 0.26%
Thrombophlebitis 1 1 0.26%
From all reported adverse drug reactions, seven events that occurred in four patients (1.05%
of all patients) were classified as suspected unexpected serious adverse reactions (SUSARs).
SUSARs were analysed according to PT and are listed in Tables A147-A148. An overview is
given in the following table (Table 10).
Table 10: Suspected unexpected serious adverse reactions
MedDRA 20.0 / Preferred term Events Patients Percent
Anaemia 1 1 0.26%
Anaphylactic shock 1 1 0.26%
Carotid artery dissection 1 1 0.26%
Cerebral infarction 1 1 0.26%
Deep vein thrombosis 1 1 0.26%
Hypertensive crisis 1 1 0.26%
Thrombophlebitis 1 1 0.26%
Current clinical status of documented ADRs and affected patients, respectively, is shown in
Tables A149-A152. The outcome was stated to be ongoing for two events in one patient
(0.26%), recovering for eight events in seven patients (1.84%), and recovered for the majority
of 47 events in 35 patients (9.19%). Status was reported to be not recovered for five events in
Page 73
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 48
three patients (0.79%). The outcome of one ADR in one patient (0.26%) was unknown. Data
on one ADR in one patient (0.26%) each was missing or was not applicable.
X.2.2. Adverse events
A total of 136 adverse events occurred during the course of the study in 80 patients (21.00%).
For most of the patients with AEs one type of event was reported (48 patients, 12.60%). Two
types of events were documented for 17 patients (4.46%) and three types of events were
noticed in 11 patients (2.89%). Four types of events were documented in two patients (0.52%).
Five or six events were noticed in one patient each (0.26%, Tables A153-A156).
Most frequently reported AEs were assigned to the preferred term hypersensitivity (9 events
in eight patients, 2.10% of all patients), followed by erythema (seven events in seven patients
each, 1.84%), headache (six events in six patients, 1.57%), ineffective drug (five events in five
patients, 1.31%), anaphylactic reaction, colitis ulcerative, musculoskeletal discomfort, pruritis
(four events in four patients each, 1.05%), arthralgia, fatigue (three events in three patients
each, 0.79%), dizziness (three events in two patients, 0.52%), alopecia, Crohn’s disease,
eczema, gastrointestinal infection, hepatitis, hyperhidrosis, influenzy like illness, and rash
(two events in two patients each, 0.52% of patients). All further AEs were reported at a
frequency of one event in one patient (0.26%) and are fully listed in Tables A153-A156.
From all documented AEs, 30 events in 22 patients (5.77%) were recorded to be serious.
Table 11: Serious adverse events
MedDRA 20.0 / Preferred term Events Patients Percent
Anaphylactic reaction 4 4 1.05%
Hypersensitivity 4 4 1.05%
Colitis ulcerative 2 2 0.52%
Hepatitis 2 2 0.52%
Abdominal abscess 1 1 0.26%
Anaemia 1 1 0.26%
Anaphylactic shock 1 1 0.26%
Carotid artery dissection 1 1 0.26%
Cerebral infarction 1 1 0.26%
Colitis 1 1 0.26%
Crohn's disease 1 1 0.26%
Deep vein thrombosis 1 1 0.26%
Drug ineffective 1 1 0.26%
Drug specific antibody present 1 1 0.26%
Fall 1 1 0.26%
Page 74
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 49
MedDRA 20.0 / Preferred term Events Patients Percent
Fistula 1 1 0.26%
Hypertensive crisis 1 1 0.26%
Pleural effusion 1 1 0.26%
Pulmonary tuberculosis 1 1 0.26%
Pustular psoriasis 1 1 0.26%
Thrombophlebitis 1 1 0.26%
Urinary tract infection bacterial 1 1 0.26%
Outcome of documented AEs and affected patients is indicated in Tables A167-A174. The
outcome was stated to be ongoing for 28 events in 20 patients (5.25%), recovering for
17 events in 14 patients (3.67%) and recovered for 76 AEs in 50 patients (13.12%). Status was
reported to be not recovered for five events in three patients (0.79%) and information about
one event in one patient (0.26%) was missing. Furthermore, the outcome was unknown for six
events in three patients (0.79%) and fatal for one event in one patient (0.26%). Data on two
events in two patients (0.52%) were not applicable.
X.3. Pregnancies
One patient got pregnant during the study.
Page 75
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 50
XI. DISCUSSION AND CONCLUSION
Biosimilars generally represent worthwhile alternatives to their originator biological drugs and
may lead to considerable cost savings for the health community and possibly more patients
globally will gain access to therapy when indicated. Biosimilar infliximab, known by its brand
name Remsima®, is the world’s first biosimilar monoclonal antibody to be approved by the US
Food and Drug Administration and the European Medicines Agency. Remsima® is a medicinal
product biologically similar to the original reference product Remicade®. Although both
products share an identical amino acid sequence and are produced in the similar cell line,
murine hybridoma cells, it is not excluded that differences in the production process may
influence functional properties. Up until now, clinical trials demonstrated no significant
differences with Remicade® in treatment of rheumatoid arthritis and the related condition
ankylosing spondylitis. Remsima® is likely as effective and safe for other indications, including
psoriasis and inflammatory bowel conditions like Crohn's disease and ulcerative colitis,
however, it was not tested against those conditions in detail and reliable data are needed to
finally evaluate effectiveness and safety.
The aim of this non-interventional study was to document the efficacy, safety, and tolerability
of Remsima® in the treatment of Crohn’s disease and ulcerative colitis under real life
conditions. The disease activity was assessed by HBI and Mayo-score. Furthermore, the
influence on quality of life, fatigue, depression, and abdominal pain were documented with
the patient’s questionnaire forms IBDQ, BFI, ADS-L, and SF-McGill.
XI.1. Discussion
XI.1.1. Discussion of demographic and baseline characteristics
Data of 381 patients investigated at 70 study sites were statistically analysed. Slightly more
female than male patients were included (52.76% versus 47.24%). Female predominance in
inflammatory bowel disease is not a general feature and when present, it is subject to the
geographical location (Zelinkova 2014). In Europe and North-America female:male ratio can
vary from 2.5:1 to equal distribution in different study populations (Bernstein et al. 2001;
Freeman 2004; Kyle 1992; Shivananda et al. 1996; Sincic et al. 2006). In contrast, the
population of Asia is rather characterized by male predominance (Yang et al. 2001; Ishige et
al. 2010; Yang et al. 2008). Reasons for these geographical differences are still unclear.
Differential cultural habits and gender-specific exposure of women and men to certain IBD risk
factors might contribute to these results.
In the western industrial nations, the incidence rates of Crohn’s disease and ulcerative colitis
increased in both genders in recent decades, with a high prevalence of both diseases
(Jacobsen et al. 2006). For ulcerative colitis, incidence rates in women increased from 8.3 in
1978-1982 to 17.0 per 100,000 person-years in 1998-2002. The corresponding values for men
were 7.7 and 16.7 per 100,000 person-years. For Crohn's disease, the incidence rates in
women increased from 4.1 in 1978-1982 to 10.7 per 100,000 person-years in 1998-2002 and
for men from 3.2 to 8.5 per 100,000 person-years. The prevalence of ulcerative colitis and
Crohn's disease was 294 and 151 per 100,000 inhabitants, respectively (Jacobsen et al. 2006).
Page 76
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 51
Crohn's disease and ulcerative colitis are usually diagnosed in the second or third decade of
life; however, studies from Europe and New York showed a second incidence peak occurring
later in life (Quezada et al. 2013; Loftus et al. 2007; Sonnenberg 2010; Quezada und Cross
2012). Lapidus et al. reported that the mean age of Chron’s disease diagnosis increased from
25 years in 1955 to 32 years of age in 1989. A bimodal peak in incidence rates by age group
was noted, with the first peak occurring between the ages of 15–29 years and a second peak
occurring between the ages of 55–59 years (Lapidus et al. 1997). Also for ulcerative colitis,
recent studies have shown that 11% of newly diagnosed cases are greater than 60 years old
(Piront et al. 2002). Diagnosis of ulcerative colitis beyond age 40 years was found to be
associated with decreased disease extent compared to younger age groups (Quezada und
Cross 2012).
In this study, mean age of patients was 41.10 years with a range of 18 to 91 years whereby
about half of the patients was between 20 to <40 years (47.37%) old. Concerning the type of
IBD, patients with Crohn’s disease were more frequently included than ulcerative colitis
(58.53% versus 41.47%).
The mean BMI of patients included in this NIS was 25.01 kg/m2. This value is comparable to
the mean value of 25.7 that is reported for the adult population in Germany (Statistisches
Bundesamt 2009).
The mean duration of IBD since diagnosis was about nine years. The median number of
episodes was 2.00 but most patients stated occurrence of one episode since diagnosis. An
intestinal resection due to IBD was performed in 16.14% of patients. In more than 70% of the
patients the acute episode lasted up to 6 months at enrolment and most of the patients were
not hospitalized in the past due to the current episode.
Crohn’s disease activity according to the HBI was available for 221 patients. The mean value
was 6.84±4.15 (median 7.00) points. A remission of disease was determined for 74 patients
(33.48%), a mild disease activity for 54 patients (24.43%) and a moderate disease activity for
93 patients (42.08%).
Disease activity of ulcerative colitis was classified according to the Mayo score. For
154 patients, the mean value was 7.32±2.65 (median 8.00) points. Normal activity of disease
was calculated for six patients (3.90%), a mild disease activity for 23 patients (14.94%) and a
moderate to severe disease activity for 125 patients (81.17%).
For most patients pre-treatment of IBD was documented (85.56%) commonly with
immunosuppressive agents (50.66% of all patients), antidiarrheals/intestinal
antiinflammatory or antiinfective agents (48.29%) and corticosteroids for systemic use
(23.36%).
Page 77
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 52
Patients with or without concomitant disease(s) were enrolled into this study. 26.25% of the
patients suffered from concomitant disease. For patients with an accompanying illness,
hypertension (4.72%), depression (2.10%), and hypothyroidism (2.10%) were most commonly
mentioned.
In general, this study design represents an important tool to collect real life data concerning
treatment with Remsima® of patients with multiple comorbidities, comedications, and risk
factors. These patients are usually excluded from controlled clinical trials. Based on the
demographic and baseline characteristics, the study cohort analysed here seems to be a
representative population of the routine medical practice and can be considered
characteristic for patients with IBD.
XI.1.2. Discussion of therapy with Remsima®
The most frequently stated reasons to start a therapy with Remsima® were due to low
effectiveness of the previous medication (62.99% of all patients) and due to contraindication
or intolerance to conventional therapy (24.15%).
Mean dose of Remsima® was relatively stable during the course of the NIS and increased only
slightly from 5.09 mg/kg body weight (BW) at baseline up to 5.22 mg/kg BW at visit 3.
According to SmPC, administered Remsima® dose should be 5mg/kg BW (Mundipharma
2015). The majority of patients received the recommended dosage during the course of the
NIS. A moderate increase of patients receiving > 5mg/kg BW was recorded from baseline to
visit 3 (11.44% versus 17.65%) whereas the number of patients treated with 5mg/kg BW was
slightly reduced (84.04% versus 77.31%).
Most of the patients did not prematurely end Remsima®-treatment during the course of the
NIS (88.19%). In patients who discontinued the study prematurely, most frequently a dropout
due to adverse drug reactions, lack of efficiency, and at patients request was documented.
Adherence in IBD patients, especially to maintenance medication regimens, has traditionally
been poor, although regularly scheduled infusions of infliximab are necessary to maintain drug
levels and thus, to prevent the development of anti-infliximab antibodies. While infliximab has
demonstrated effectiveness in randomized controlled trials, its efficacy may be hampered by
poor compliance in real life settings. A systematic review of data from 4322 IBD patients
revealed widely varying rates of nonadherence to maintenance medication regimens,
including some studies showed nonadherence rates as high as 72%, but most studies reported
that 30-45% of patients were non-adherent (Jackson et al. 2010).
In this regard, a Canadian retrospective cohort study was conducted evaluating patients with
Crohn’s disease or ulcerative colitis on an induction or maintenance regimen of regularly
scheduled infliximab from 2008 to 2010. In this study, including a total of 215 patients,
nonadherence was defined by a discrepancy of >72 h between the scheduled date of infusion
and the actual date of administration. Patients were defined as nonadherent if they received
<80% of their infliximab infusions per schedule. As a result, three-quarters of patients were
Page 78
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 53
adherent to infliximab induction therapy while fewer than one-third of the patients remained
adherent to their scheduled maintenance infliximab regimen (Ma et al. 2015).
Concomitant treatment of IBD during the study was documented for 54.59%. Most common
reported treatments were antidiarrheals/intestinal antiinflammatory or antiinfective agents
(33.60% of all patients), corticosteroids for systemic use (19.69%) and immunosuppressive
agents (17.32%).
Only 13 patients (3.57%) were hospitalized during the whole study period. Patients with
hospitalization stayed on average 1.48 weeks at hospital.
For four patients, operative interventions for treatment of acute episode during the NIS were
reported (1.05%). Two of them had a fistula drainage and for one patient each an abscess
drainage and hemicolectomy, respectively, was documented.
XI.1.3. Discussion of results in effectiveness
Our study data show positive clinical outcomes following administration of Remsima® in
patients suffering from IBD. Activity of Crohn’s disease and ulcerative colitis was reduced
during this non-interventional study. The mean HBI value of 6.91 points at baseline
significantly decreased to 3.06 at the last documentation. Disease activity of ulcerative colitis
also developed positively as illustrated by the Mayo score that fell from 7.27 to 2.81. The
effectiveness of infliximab Remicade® in patients suffering from IBD has been demonstrated
in many studies. In general, a clinical response in patients with Crohn’s disease is reported in
two-thirds of the treated patients and even remission in one-third of the patients under
infliximab treatment (D'haens et al. 1999; Targan et al. 1997; Present et al. 1999). In this study,
remission of Chron’s disease was reached in 155 patients (72.77%), however, disease activity
had already been in remission in 70 patients (32.86%) at baseline. A study evaluating the
clinical response in patients with ulcerative colitis reported remission rates of 64.5% for
patients treated with 5 mg/kg infliximab (versus 29.3% for patients in the placebo group)
(Rutgeerts et al. 2005). These results are in line with a Korean study of a total of 110 patients
with IBD that reported clinical remission rates of 77.3% in patients with Crohn’s disease and
of 47.8% patients with ulcerative colitis by Remsima® treatment in infliximab naive patients
at week 30 (Jung et al. 2015). Moreover, reports from several other observational studies in
patients with IBD support the use of Remsima® for this indication (Keil et al. 2016; Kang et al.
2015, 2015; Sieczkowska et al. 2016a; Sieczkowska et al. 2016b; Farkas et al. 2016; Gecse et
al. 2016). Results are in line with data from our study showing that the activity of Crohn’s
disease and ulcerative colitis were significantly reduced during the treatment with Remsima®.
Mean activity of Crohn’s disease was improved from mild disease classification to remission
state and of ulcerative colitis from moderate-severe to mild disease classification at week 14.
Fatigue is a well-known and often reported symptom in patients with IBD, even when the
disease is in remission, with severe consequences for quality of life. Fatigue was reported in
40% of IBD patients with quiescent disease and an even higher prevalence and level of fatigue
is associated with disease activity (Minderhoud et al. 2003; Minderhoud et al. 2007). Patients
frequently experience a rapid reduction of fatigue after treatment with infliximab, as shown
Page 79
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 54
by a previous, placebo-controlled study, which was based on a health related quality of life
questionnaire (Lichtenstein et al. 2002). In our study, nearly all patients had received a pre-
treatment of IBD prior to treatment with Remsima® and the initial BFI values at baseline
examination already showed a moderate level of fatigue in patients with Crohn’s disease and
ulcerative colitis. Fatigue symptoms slightly decreased during treatment with Remsima®, but
were still classified as moderate for patients with Crohn’s disease whereas patients suffering
from ulcerative colitis displayed a mild to moderate level of fatigue at the end of the study.
Moreover, the quality of life significantly improved during Remsima® treatment. This is in line
with previous studies, including a randomised, placebo-controlled study where patients with
active Crohn’s disease received a single intravenous infusion of either placebo or infliximab (5,
10 or 20 mg/kg). Changes from baseline in overall IBDQ-D score and individual dimensions at
4 weeks post-infusion were compared and showed significantly larger improvement in overall
IBDQ-D score and in all IBDQ dimensions than those treated with placebo at 4 weeks
(Lichtenstein et al. 2002). We also demonstrated a beneficial effect of Remsima® on
depression, the most common psychiatric diagnosis in Crohn’s disease and a putative risk
factor for failure to achieve remission with infliximab (Persoons et al. 2005). TNF-alpha has
been reliably shown to be elevated in depressed patients (Dowlati et al. 2010), however, only
limited data are available from studies investigating the potential of the antidepressant effect
of infliximab. Findings have included improvements of depression in patients with ankylosing
spondylitis (Ertenli et al. 2012), which is supported by animal models (Karson et al. 2013), and
a correlation between a reduced remission rate and the presence of depression in patients
with Crohn’s disease under infliximab treatment (Persoons et al. 2005). In contrast, a recently
conducted, randomised, placebo-controlled trial by Raison et al. (2013) did not note an overall
association of infliximab with antidepressant effects, however, in the subgroup with increased
levels of baseline inflammatory biomarkers, infliximab improved the antidepressant response
(Raison et al. 2013). A limitation of the study was that, since no guidelines presently exist for
anti-inflammatory agents and depression, adjunctive medication could have been under or
overdosed. Other limitations were the follow-up period that was rather short and the number
of patients that was also small (Boufidou und Nikolaou 2016).
Furthermore, the majority of the analysed laboratory parameters improved during the study,
for instance erythrocyte, leukocyte, thrombocyte, haemoglobin level and C-reactive protein
(CRP) level. In particular, C-reactive protein serves as a reliable marker for inflammatory bowel
disease. An increased CRP (>45 mg/L) in patients with IBD predicts with a high certainty the
need for colectomy and this by reflecting severe ongoing and uncontrollable inflammation in
the gut (Vermeire et al. 2004). C-reactive protein levels correspond closely with clinical and
pathological indices of relapse, remission and response to therapy in patients with Crohn's
disease (Fagan et al. 1982). Effectiveness of therapy was evaluated by the measurement of
CRP level in this NIS. The mean amount of C-reactive protein was 34.97 mg/l at admission and
decreased down to 21.11 mg/l at last visit. Mean reduction of 13.86 was statistically significant
(p<0.0001). In contrast to a percentage of 48.56% at baseline, 63.67% of the patients had
normal values (≤ 10 mg/l) at the end of the NIS. Compared to data from the observational
Page 80
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 55
study with 52 IBD patients under CT-P13 therapy, conducted by Keil et al., median CRP level
of both men and women decreased after 14 weeks of therapy to 1.0 mg/l (men, p=0.001) and
5.0 mg/l (women, p=0.011). However, compared to data presented here, baseline level were
substantially lower, namely 28.0 mg/l for men and 11.0 mg/l for women, respectively (Keil et
al. 2016).
Efficacy was globally assessed by the physicians and by the patients themselves. Overall,
efficacy was evaluated as very good or good for about 85% of the patients when physicians
were asked and about 82% when patients were asked.
XI.1.4. Discussion of results in safety
According to the summary of product characteristics (Mundipharma 2015), upper respiratory
tract infection was the most common adverse drug reaction (ADR) reported in clinical trials,
occurring in 25.3% of infliximab-treated patients compared with 16.5% of control patients.
The most serious ADRs associated with the use of TNF blockers that have been previously
reported for infliximab include HBV reactivation, CHF, serious infections (including sepsis,
opportunistic infections and TB), serum sickness (delayed hypersensitivity reactions),
haematologic reactions, systemic lupus erythematosus/lupus-like syndrome, demyelinating
disorders, hepatobiliary events, lymphoma, HSTCL, leukaemia, Merkel cell carcinoma,
melanoma, paediatric malignancy, sarcoidosis/sarcoid-like reaction, intestinal or perianal
abscess (in Crohn’s disease), and serious infusion reactions.
In this study, 136 adverse events were reported in 80 patients (21.00%) and 65 adverse drug
reactions occurred in 48 patients (12.60%) during the observation period of approximately
14 weeks. For the majority of the patients with ADRs one type of reaction was reported
(37 patients, 9.71%). Most frequently reported ADRs were assigned to the preferred term
hypersensitivity (9 events in 8 patients, 2.10%), followed by erythema (6 events in 6 patients,
1.05%), ineffective drug (5 events in 5 patients, 1.31%), anaphylactic reaction (4 events in
4 patients, 1.05%), dizziness (3 events in 2 patients, 0.52%), alopecia, fatigue, pruritius, and
rash (2 events in 2 patients each, 0.52%). All further ADRs were reported at a frequency of one
event in one patient each (0.26%).
According to the special warnings and precaution section of the SmPC, infliximab has been
associated with acute infusion related reactions, including anaphylactic shock, and delayed
hypersensitivity reactions. In a recent prospective, nationwide, multicentre, observational
cohort that was designed to examine the efficacy, safety, and immunogenicity of CT-
P13 infliximab, adverse events were experienced in 17.1% of all IBD patients (n=210) until
week 30. Compared to our NIS with a total of 136 reported adverse events in 80 patients
(21.00%), the number of adverse events was lower. Infusion reactions occurred in 6.6% of all
patients (Gecse et al. 2016). Further studies also demonstrated an association of acute
infusion reaction with infliximab treatment (Dignass et al. 2012; van Assche et al. 2010).
Intensity as well as frequency of these reactions can differ. One centre showed at least one
infusion reaction in 9.7% of patients and 6.1% of infusions were accompanied by infusion
reactions (Cheifetz et al. 2003). Another study reported about the occurrence of infusion
Page 81
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 56
reactions in 5.2% of patients (Park et al. 2015), which is comparable to data of the present NIS
where patients suffered from the following infusion reactions: hypersensitivity, 2.10% of all
patients; anaphylactic reaction, 1.05%; anaphylactic shock 0.26%).
Based on experience from clinical studies as well as adverse reactions reported from post-
marketing experience, anaphylactic reaction and serum sickness (delayed hypersensitivity
reaction) are known common adverse reactions (≥1/100 to <1/10). Furthermore, erythema,
which had been observed in six patients (1.57%) in this NIS, is known as a rare event
(≥1/10,000 to <1/1,000) while dizziness, alopecia and rash are categorized as common ADRs
(≥1/100 to <1/10).
The ADRs documented in this NIS were most frequently associated with the following MedDRA
primary system organ classes (SOC): skin and subcutaneous tissue disorders (14 patients,
3.67%), immune system disorders (13 patients, 3.41%), general disorders and administration
and site conditions (8 patients, 2.10%), nervous system disorders (4 patients, 1.05%),
gastrointenstinal disorders (3 patients, 0.79%), infections and infestations (3 patients, 0.79%),
vascular disorders, musculoskeletal and connective tissue disorders, and Respiratory, thoracic
and mediastinal disorders (2 patients each, 0.52%). All further reactions struck one SOC only
(0.26%).
From all documented ADRs, 23 reactions in 18 patients (4.72%) were recorded to be serious.
Hypersensitivity and anaphylactic reaction were the most frequently reported serious ADRs
(4 events in 4 patients each, 1.05%). All other serious ADRs occurred at a frequency of one and
were reported for one patient (0.26%) in each case: abdominal abscess, anaemia,
anaphylactic shock, carotid artery dissection, cerebral infarction, colitis, deep vein thrombosis,
drug ineffective, drug specific antibody present, hepatitis, hypertensive crisis, pleural effusion,
pulmonary tuberculosis, pustular psoriasis, and thrombophlebitis. Three of these
complications were classified as infectious events according to MedDRA: abdominal abscess
(primary SOC), pulmonary tuberculosis (primary SOC), and upper respiratory tract infection
(non-primary SOC). In the above mentioned infliximab study from Gecse et al., serious
infectious adverse events occurred in 5.7% of all patients (Gecse et al. 2016).
TNFα mediates inflammation and modulates cellular immune responses. Experimental data
show that TNFα is required for the clearing of intracellular infections. As described in the
special warning and precaution section of the SmPC, patients taking TNF-blockers are more
susceptible to serious infections. Tuberculosis, bacterial infections, including sepsis and
pneumonia, invasive fungal, viral, and other opportunistic infections have been observed in
patients treated with infliximab. There have been reports of active tuberculosis in patients
receiving infliximab. It should be noted that in the majority of these reports tuberculosis was
extrapulmonary, presenting as either local or disseminated disease. If active tuberculosis is
diagnosed, Remsima therapy must not be initiated. If a latent tuberculosis is diagnosed,
treatment must be started with antituberculosis therapy before the initiation of Remsima
(Mundipharma 2015). As mentioned above, one patient suffered from tuberculosis. In this
case, a pulmonary tuberculosis was diagnosed. According to SmPC, tuberculosis is categorized
as an uncommon adverse reaction (≥1/1,000 to <1/100).
Page 82
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 57
Some ADRs mentioned in the SmPC were hardly reported or not at all. This is probably based
on a limited observation period of the underlying NIS and the phenomenon of under-reporting
in non-interventional trials as physicians may tend to under-report events already mentioned
in the SmPC (Lopez-Gonzalez et al. 2009).
Not all reported ADRs were known effects of treatment with Remsima®. From all reported
adverse drug reactions during the NIS presented here, a total of seven events that occurred in
four patients (1.05% of all patients) were classified as suspected unexpected serious adverse
reactions (SUSARs, 11.86% of reported ADRs): anaemia, anaphylactic shock, carotid artery
dissection, cerebral infarction, thrombophlebitis, hypertensive crisis, and deep vein
thrombosis. In a recent CT-P13 study in 52 patients with ulcerative colitis or Crohn’s disease,
four adverse events were identified after 14 weeks of therapy (n=1 each). Similar to the
current study, one patient was affected by deep vein thrombosis, however, it could not be
confirmed whether it was treatment-related (Keil et al. 2016).
The outcome was stated to be ongoing for two adverse reactions in one patient (0.26%),
recovering for eight events in seven patients (1.84%), and recovered for the majority of
47 events in 35 patients (9.19%). Status was reported to be not recovered for five events in
three patients (0.79%). The outcome of one ADR in one patient (0.26%) was unknown. Data
on one ADR in one patient (0.26%) each was missing or assessment was not applicable.
Tolerability of Remsima® was assessed by the physicians and by the patients themselves.
Tolerability was evaluated as very good or good in most cases. At last assessment, physicians
evaluated tolerability for about 96% of the patients as very good or good and 93% of the
patients rated tolerability as very good or good.
XI.2. Limitations on collected data
In general, this study design represents an important tool to collect real life data concerning
treatment with Remsima® of patients with multiple comorbidities, comedications and risk
factors, patients usually excluded from controlled clinical trials.
The initially planned sample size of 400 patients was almost achieved in the course of the
observation period. 381 patients were included. The number was sufficient to obtain a
representative cohort of patients treated in the routine medical practice of 70 centres
throughout Germany. The study was designed as a non-interventional study including non-
randomization of the study population and the absence of a comparative placebo- or parallel-
group. Therefore, the treatment effect of Remsima® was not directly compared to placebo
and/or other drugs. Patients were not selected by specific inclusion or exclusion criteria but
indication and contraindications mentioned in the SmPC were to be considered. The
advantage of this study design was the better transfer to non-selected patients in non-study
situations. However, due to a missing reference group of patients (without or with alternative
therapy), the efficacy of Remsima® treatment could not be conclusively assessed.
Page 83
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 58
XI.3. Clinical relevance and overall conclusions
The population analysed in the course of the NIS was considered characteristic for patients
with Crohn‘s disease and ulcerative colitis conditions. Therapy with Remsima® resulted in an
overall positive therapeutic effect on disease activity of patients with Crohn‘s disease and
ulcerative colitis. Furthermore, quality of life, fatigue and pain symptoms were improved
during the study. Concerning depression, a significant decrease of the ADS-L mean value was
achieved (but note that mean values of ADS-L suggested an absence of clinically relevant
depressive symptoms prior to Remsima® therapy). In addition, the majority of the analysed
laboratory parameters improved during the study, for instance erythrocyte, leukocyte,
thrombocyte, haemoglobin level and C-reactive protein level.
Effectiveness and tolerability of Remsima® were predominantly evaluated within the global
assessment by physicians and patients as very good or good. Safety analyses of the study
indicated general tolerability of the drug, but under-reporting of events by health-care
professionals in contrast to previously performed clinical trials cannot be excluded in this
practical-use study setting.
In conclusion, results of the ResCu study provide evidence for the effectiveness and tolerability
of Remsima® in the treatment of Crohn‘s disease and ulcerative colitis conditions under
routine medical practice settings.
Page 84
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 59
XII. REFERENCES
Arbeitsgruppe Epidemiologische Methoden der Deutschen Arbeitsgemeinschaft für Epidemiologie
(2004): Leitlinien und Empfehlungen zur Sicherung von Guter Epidemiologischer Praxis, 2004.
Assessment report Remsima (2013): EMA/CHMP/589317/2013, 27.06.2013.
Bernstein, C. N.; Blanchard, J. F.; Rawsthorne, P.; Yu, N. (2001): The prevalence of extraintestinal
diseases in inflammatory bowel disease: a population-based study. In: The American journal of
gastroenterology 96 (4), S. 1116–1122. DOI: 10.1111/j.1572-0241.2001.03756.x.
Boufidou, F.; Nikolaou, C. (2016): Alphanti-Inflammatory medication as adjunctive antidepressive
treatment. In: Psychiatrike = Psychiatriki 27 (2), S. 106–117.
Cheifetz, Adam; Smedley, Michelle; Martin, Sara; Reiter, Monica; Leone, Grace; Mayer, Lloyd; Plevy,
Scott (2003): The incidence and management of infusion reactions to infliximab: a large center
experience. In: The American journal of gastroenterology 98 (6), S. 1315–1324. DOI: 10.1111/j.1572-
0241.2003.07457.x.
Committee for Medicinal Products for Human Use (2012): Guideline on similar biological medicinal
products containing monoclonal antibodies – nonclinical and clinical issues:
EMA/CHMP/BMWP/403543/2010, 30.05.2012, S. 1–15.
Committee for Medicinal Products for Human Use (CHMP) (2013): Remsima. Procedure No.
EMEA/H/C/002576/0000. International non-proprietary name: Infliximab, zuletzt geprüft am
18.02.2016.
Deutsche Arbeitsgemeinschaft für Epidemiologie (2004): Leitlinien und Empfehlungen zur Sicherung
von guter Epidemiologischer Praxis (GEP).
D'haens, G.; van Deventer, S.; van Hogezand, R.; Chalmers, D.; Kothe, C.; Baert, F. et al. (1999):
Endoscopic and histological healing with infliximab anti-tumor necrosis factor antibodies in Crohn's
disease: A European multicenter trial. In: Gastroenterology 116 (5), S. 1029–1034.
Dignass, Axel; Eliakim, Rami; Magro, Fernando; Maaser, Christian; Chowers, Yehuda; Geboes, Karel et
al. (2012): Second European evidence-based consensus on the diagnosis and management of
ulcerative colitis part 1: definitions and diagnosis. In: Journal of Crohn's & colitis 6 (10), S. 965–990.
DOI: 10.1016/j.crohns.2012.09.003.
Dowlati, Yekta; Herrmann, Nathan; Swardfager, Walter; Liu, Helena; Sham, Lauren; Reim, Elyse K.;
Lanctot, Krista L. (2010): A meta-analysis of cytokines in major depression. In: Biological psychiatry
67 (5), S. 446–457. DOI: 10.1016/j.biopsych.2009.09.033.
Elm, Erik von; Altman, Douglas G.; Egger, Matthias; Pocock, Stuart J.; Gøtzsche, Peter C.;
Vandenbroucke, Jan P. (2008): The Strengthening the Reporting of Observational Studies in
Epidemiology (STROBE) statement: guidelines for reporting observational studies. In: Journal of
clinical epidemiology 61 (4), S. 344–349. DOI: 10.1016/j.jclinepi.2007.11.008.
Ertenli, I.; Ozer, S.; Kiraz, S.; Apras, S. B.; Akdogan, A.; Karadag, O. et al. (2012): Infliximab, a TNF-
alpha antagonist treatment in patients with ankylosing spondylitis: the impact on depression, anxiety
and quality of life level. In: Rheumatology international 32 (2), S. 323–330. DOI: 10.1007/s00296-010-
1616-x.
Page 85
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 60
Fagan, E. A.; Dyck, R. F.; Maton, P. N.; Hodgson, H. J.; Chadwick, V. S.; Petrie, A.; Pepys, M. B. (1982):
Serum levels of C-reactive protein in Crohn's disease and ulcerative colitis. In: European journal of
clinical investigation 12 (4), S. 351–359.
Farkas, Klaudia; Rutka, Mariann; Golovics, Petra A.; Vegh, Zsuzsanna; Lovasz, Barbara D.; Nyari, Tibor
et al. (2016): Efficacy of Infliximab Biosimilar CT-P13 Induction Therapy on Mucosal Healing in
Ulcerative Colitis. In: Journal of Crohn's & colitis 10 (11), S. 1273–1278. DOI: 10.1093/ecco-jcc/jjw085.
Freeman, Hugh J. (2004): Comparison of longstanding pediatric-onset and adult-onset Crohn's
disease. In: Journal of pediatric gastroenterology and nutrition 39 (2), S. 183–186.
Gecse, Krisztina B.; Lovasz, Barbara D.; Farkas, Klaudia; Banai, Janos; Bene, Laszlo; Gasztonyi, Beata et
al. (2016): Efficacy and Safety of the Biosimilar Infliximab CT-P13 Treatment in Inflammatory Bowel
Diseases: A Prospective, Multicentre, Nationwide Cohort. In: Journal of Crohn's & colitis 10 (2), S.
133–140. DOI: 10.1093/ecco-jcc/jjv220.
Gesetz über den Verkehr mit Arzneimitteln. Arzneimittelgesetz-AMG, 16. Novelle, aktualisiert am 10.
Oktober 2013 (2013).
Harvey, R. F.; Bradshaw, J. M. (1980): A simple index of Crohn's-disease activity. In: Lancet (London,
England) 1 (8167), S. 514.
Hautzinger, M.; Bailer, M. (1993): Allgemeine Depressions Skala. Manual. Göttingen.
Ishige, Takashi; Tomomasa, Takeshi; Takebayashi, Tohru; Asakura, Keiko; Watanabe, Mamoru;
Suzuki, Tomoko et al. (2010): Inflammatory bowel disease in children: epidemiological analysis of the
nationwide IBD registry in Japan. In: Journal of gastroenterology 45 (9), S. 911–917. DOI:
10.1007/s00535-010-0223-7.
Jackson, C. A.; Clatworthy, J.; Robinson, A.; Horne, Rob (2010): Factors associated with non-
adherence to oral medication for inflammatory bowel disease: a systematic review. In: The American
journal of gastroenterology 105 (3), S. 525–539. DOI: 10.1038/ajg.2009.685.
Jacobsen, Bent A.; Fallingborg, Jan; Rasmussen, Henrik H.; Nielsen, Kari R.; Drewes, Asbjorn M.; Puho,
Erzsebet et al. (2006): Increase in incidence and prevalence of inflammatory bowel disease in
northern Denmark: a population-based study, 1978-2002. In: European journal of gastroenterology &
hepatology 18 (6), S. 601–606.
Janke, K-H; Steder-Neukamm, U.; Bauer, M.; Raible, A.; Meisner, C.; Hoffmann, J. C. et al. (2005):
Lebensqualität bei chronisch entzündlichen Darmerkrankungen (CED): die deutsche Version des
Inflammatory Bowel Disease Questionnaire (IBDQ-D) zur krankheitsspezifischen
Lebensqualitätsmessung -- erste Anwendung und Vergleich mit anderen internationalen Fassungen.
In: Gesundheitswesen (Bundesverband der Ärzte des Öffentlichen Gesundheitsdienstes (Germany))
67 (8-9), S. 656–664. DOI: 10.1055/s-2005-858579.
Jung, Yoon Suk; Park, Dong Il; Kim, Young Ho; Lee, Ji Hyun; Seo, Pyoung Ju; Cheon, Jae Hee et al.
(2015): Efficacy and safety of CT-P13, a biosimilar of infliximab, in patients with inflammatory bowel
disease: A retrospective multicenter study. In: Journal of gastroenterology and hepatology 30 (12), S.
1705–1712. DOI: 10.1111/jgh.12997.
Kang, Yun-Seong; Moon, Hyoung Ho; Lee, Seung Eun; Lim, Yun Jeong; Kang, Hyoun Woo (2015):
Clinical Experience of the Use of CT-P13, a Biosimilar to Infliximab in Patients with Inflammatory
Page 86
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 61
Bowel Disease: A Case Series. In: Digestive diseases and sciences 60 (4), S. 951–956. DOI:
10.1007/s10620-014-3392-z.
Karson, Ayse; Demirtas, Tugce; Bayramgurler, Dilek; Balci, Fuat; Utkan, Tijen (2013): Chronic
administration of infliximab (TNF-alpha inhibitor) decreases depression and anxiety-like behaviour in
rat model of chronic mild stress. In: Basic & clinical pharmacology & toxicology 112 (5), S. 335–340.
DOI: 10.1111/bcpt.12037.
Keil, Radan; Wasserbauer, Martin; Zádorová, Zdena; Hajer, Jan; Drastich, Pavel; Wohl, Pavel et al.
(2016): Clinical monitoring: infliximab biosimilar CT-P13 in the treatment of Crohn's disease and
ulcerative colitis. In: Scandinavian journal of gastroenterology 51 (9), S. 1062–1068. DOI:
10.3109/00365521.2016.1149883.
Kodex zur freiwilligen Selbstkontrolle (2013): Freiwillige Selbstkontrolle für die Arzneitmittelindustrie
e.V., Kodex für die Zusammenarbeit der pharmazeutischen Industrie mit Ärzten, Apothekern und
anderen Angehörigen medizinischer Fachkreise. Neuauflage 2013 inkl. Leitlinien.
Kyle, J. (1992): Crohn's disease in the northeastern and northern Isles of Scotland: an epidemiological
review. In: Gastroenterology 103 (2), S. 392–399.
La Haye, Rainer de (2000): Anwendungsbeobachtungen. Leitfaden für die praktische Durchführung.
Aulendorf: ECV - Editio-Cantor-Verl. (Pharmind-Serie Dokumentation).
Lapidus, A.; Bernell, O.; Hellers, G.; Persson, P.; Lofberg, R. (1997): Incidence of Crohn's disease in
Stockholm County 1955-1989. In: Gut 41 (4), S. 480–486.
Lewis, James D.; Chuai, Shaokun; Nessel, Lisa; Lichtenstein, Gary R.; Aberra, Faten N.; Ellenberg, Jonas
H. (2008): Use of the noninvasive components of the Mayo score to assess clinical response in
ulcerative colitis. In: Inflammatory bowel diseases 14 (12), S. 1660–1666. DOI: 10.1002/ibd.20520.
Lichtenstein, Gary R.; Bala, Mohan; Han, Chenglong; DeWoody, Kimberly; Schaible, Thomas (2002):
Infliximab improves quality of life in patients with Crohn's disease. In: Inflammatory bowel diseases
8 (4), S. 237–243.
Loftus, Conor G.; Loftus, Edward V., JR; Harmsen, W. Scott; Zinsmeister, Alan R.; Tremaine, William J.;
Melton, L. Joseph 3rd; Sandborn, William J. (2007): Update on the incidence and prevalence of
Crohn's disease and ulcerative colitis in Olmsted County, Minnesota, 1940-2000. In: Inflammatory
bowel diseases 13 (3), S. 254–261. DOI: 10.1002/ibd.20029.
Lopez-Gonzalez, Elena; Herdeiro, Maria T.; Figueiras, Adolfo (2009): Determinants of under-reporting
of adverse drug reactions: a systematic review. In: Drug safety 32 (1), S. 19–31. DOI:
10.2165/00002018-200932010-00002.
Ma, Christopher; Evaschesen, Chad J.; Gracias, Grenvil; Huang, Vivian W.; Fedorak, Darryl K.; Kroeker,
Karen I. et al. (2015): Inflammatory bowel disease patients are frequently nonadherent to scheduled
induction and maintenance infliximab therapy: A Canadian cohort study. In: Canadian journal of
gastroenterology & hepatology 29 (6), S. 309–314.
Melzack, R. (1987): The short-form McGill Pain Questionnaire. In: Pain 30 (2), S. 191–197.
Minderhoud, Itta M.; Oldenburg, Bas; van Dam, P. Sytze; van Berge Henegouwen, Gerard P. (2003):
High prevalence of fatigue in quiescent inflammatory bowel disease is not related to adrenocortical
insufficiency. In: The American journal of gastroenterology 98 (5), S. 1088–1093. DOI:
10.1111/j.1572-0241.2003.07414.x.
Page 87
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 62
Minderhoud, Itta M.; Samsom, Melvin; Oldenburg, Bas (2007): Crohn's disease, fatigue, and
infliximab: is there a role for cytokines in the pathogenesis of fatigue? In: World journal of
gastroenterology 13 (14), S. 2089–2093.
Mundipharma (2015): SmPC Remsima® 100 mg. Pulver für ein Konzentrat zur Herstellung einer
Infusionslösung, März 2015.
Park, Sang Hyoung; Kim, Young-Ho; Lee, Ji Hyun; Kwon, Hyeok Jin; Lee, Suck-Ho; Park, Dong Il et al.
(2015): Post-marketing study of biosimilar infliximab (CT-P13) to evaluate its safety and efficacy in
Korea. In: Expert review of gastroenterology & hepatology 9 Suppl 1, S. 35–44. DOI:
10.1586/17474124.2015.1091309.
Park, Won; Yoo, Dae Hyun; Jaworski, Janusz; Brzezicki, Jan; Gnylorybov, Andriy; Kadinov, Vladimir et
al. (2016): Comparable long-term efficacy, as assessed by patient-reported outcomes, safety and
pharmacokinetics, of CT-P13 and reference infliximab in patients with ankylosing spondylitis: 54-
week results from the randomized, parallel-group PLANETAS study. In: Arthritis research & therapy
18, S. 25. DOI: 10.1186/s13075-016-0930-4.
Persoons, P.; Vermeire, S.; Demyttenaere, K.; Fischler, B.; Vandenberghe, J.; van Oudenhove, L. et al.
(2005): The impact of major depressive disorder on the short- and long-term outcome of Crohn's
disease treatment with infliximab. In: Alimentary pharmacology & therapeutics 22 (2), S. 101–110.
DOI: 10.1111/j.1365-2036.2005.02535.x.
Piront, Patricia; Louis, Edouard; Latour, Pascale; Plomteux, Olivier; Belaiche, Jacques (2002):
Epidemiology of inflammatory bowel diseases in the elderly in the province of Liege. In:
Gastroenterologie clinique et biologique 26 (2), S. 157–161.
Present, D. H.; Rutgeerts, P.; Targan, S.; Hanauer, S. B.; Mayer, L.; van Hogezand, R. A. et al. (1999):
Infliximab for the treatment of fistulas in patients with Crohn's disease. In: The New England journal
of medicine 340 (18), S. 1398–1405. DOI: 10.1056/NEJM199905063401804.
Quezada, Sandra M.; Cross, Raymond K. (2012): Association of age at diagnosis and ulcerative colitis
phenotype. In: Digestive diseases and sciences 57 (9), S. 2402–2407. DOI: 10.1007/s10620-012-2081-
z.
Quezada, Sandra M.; Steinberger, Eileen K.; Cross, Raymond K. (2013): Association of age at diagnosis
and Crohn's disease phenotype. In: Age and ageing 42 (1), S. 102–106. DOI: 10.1093/ageing/afs107.
Radbruch, Lukas; Sabatowski, Rainer; Elsner, Frank; Everts, Jan; Mendoza, Tito; Cleeland, Charles
(2003): Validation of the German version of the brief fatigue inventory. In: Journal of pain and
symptom management 25 (5), S. 449–458.
Raison, Charles L.; Rutherford, Robin E.; Woolwine, Bobbi J.; Shuo, Chen; Schettler, Pamela; Drake,
Daniel F. et al. (2013): A randomized controlled trial of the tumor necrosis factor antagonist
infliximab for treatment-resistant depression: the role of baseline inflammatory biomarkers. In:
JAMA psychiatry 70 (1), S. 31–41. DOI: 10.1001/2013.jamapsychiatry.4.
Rutgeerts, Paul; Sandborn, William J.; Feagan, Brian G.; Reinisch, Walter; Olson, Allan; Johanns, Jewel
et al. (2005): Infliximab for induction and maintenance therapy for ulcerative colitis. In: The New
England journal of medicine 353 (23), S. 2462–2476. DOI: 10.1056/NEJMoa050516.
Shivananda, S.; Lennard-Jones, J.; Logan, R.; Fear, N.; Price, A.; Carpenter, L.; van Blankenstein, M.
(1996): Incidence of inflammatory bowel disease across Europe: is there a difference between north
Page 88
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 63
and south? Results of the European Collaborative Study on Inflammatory Bowel Disease (EC-IBD). In:
Gut 39 (5), S. 690–697.
Sickmüller, B. (2009): "Points to Consider" zu Anwendungsbeobachtungen / Empfehlungen des
Bundesverbands der Pharmazeutischen Industrie zur Durchführung von Anwendungsbeobachtungen.
In: Die pharmazeutische Industrie 71 (5), S. 764. Online verfügbar unter
http://www.zbmed.de/ccmedimages/2009/83758.pdf,
Sieczkowska, J.; Jarzebicka, D.; Banaszkiewicz, A.; Plocek, A.; Gawronska, A.; Toporowska-Kowalska, E.
et al. (2016a): Switching Between Infliximab Originator and Biosimilar in Paediatric Patients with
Inflammatory Bowel Disease. Preliminary Observations. In: Journal of Crohn's & colitis 10 (2), S. 127–
132. DOI: 10.1093/ecco-jcc/jjv233.
Sieczkowska, Joanna; Jarzebicka, Dorota; Meglicka, Monika; Oracz, Grzegorz; Kierkus, Jaroslaw
(2016b): Experience with biosimilar infliximab (CT-P13) in paediatric patients with inflammatory
bowel diseases. In: Therapeutic advances in gastroenterology 9 (5), S. 729–735. DOI:
10.1177/1756283X16650155.
Sincic, Brankica Mijandrusic; Vucelic, Boris; Persic, Mladen; Brncic, Nada; Erzen, Dubravka Jurisic;
Radakovic, Bogdan et al. (2006): Incidence of inflammatory bowel disease in Primorsko-goranska
County, Croatia, 2000-2004: A prospective population-based study. In: Scandinavian journal of
gastroenterology 41 (4), S. 437–444. DOI: 10.1080/00365520500320094.
Sonnenberg, Amnon (2010): Age distribution of IBD hospitalization. In: Inflammatory bowel diseases
16 (3), S. 452–457. DOI: 10.1002/ibd.21058.
Statistisches Bundesamt (2009): Verteilung der Bevölkerung auf Body-Mass-Index-Gruppen in
Prozent. Mikrozensus - Fragen zur Gesundheit, Statistisches Bundesamt, Zweigstelle Bonn.
Targan, S. R.; Hanauer, S. B.; van Deventer, S. J.; Mayer, L.; Present, D. H.; Braakman, T. et al. (1997):
A short-term study of chimeric monoclonal antibody cA2 to tumor necrosis factor alpha for Crohn's
disease. Crohn's Disease cA2 Study Group. In: The New England journal of medicine 337 (15), S.
1029–1035. DOI: 10.1056/NEJM199710093371502.
van Assche, Gert; Dignass, Axel; Panes, Julian; Beaugerie, Laurent; Karagiannis, John; Allez, Mathieu
et al. (2010): The second European evidence-based Consensus on the diagnosis and management of
Crohn's disease: Definitions and diagnosis. In: Journal of Crohn's & colitis 4 (1), S. 7–27. DOI:
10.1016/j.crohns.2009.12.003.
Vermeire, Severine; van Assche, Gert; Rutgeerts, Paul (2004): C-reactive protein as a marker for
inflammatory bowel disease. In: Inflammatory bowel diseases 10 (5), S. 661–665.
Victor, N.; Windeler, J.; Hasford, J. (1997): Empfehlungen zur Durchführung von
Anwendungsbeobachtungen. In: Informatik, Biometrie und Epidemiologie in Medizin und Biologie 28,
S. 247–252.
Yang, S. K.; Loftus, E. V., JR; Sandborn, W. J. (2001): Epidemiology of inflammatory bowel disease in
Asia. In: Inflammatory bowel diseases 7 (3), S. 260–270.
Yang, Suk-Kyun; Yun, Sungcheol; Kim, Jin-Ho; Park, Joon Yong; Kim, Hak Yang; Kim, Young-Ho et al.
(2008): Epidemiology of inflammatory bowel disease in the Songpa-Kangdong district, Seoul, Korea,
1986-2005: a KASID study. In: Inflammatory bowel diseases 14 (4), S. 542–549. DOI:
10.1002/ibd.20310.
Page 89
Non-interventional study ResCu Study code IFX9502 Remsima® (Infliximab)
Integrated report: Version 1.0, 19th of January 2018 64
Yoo, Dae Hyun; Hrycaj, Pawel; Miranda, Pedro; Ramiterre, Edgar; Piotrowski, Mariusz; Shevchuk,
Sergii et al. (2013): A randomised, double-blind, parallel-group study to demonstrate equivalence in
efficacy and safety of CT-P13 compared with innovator infliximab when coadministered with
methotrexate in patients with active rheumatoid arthritis: the PLANETRA study. In: Annals of the
rheumatic diseases 72 (10), S. 1613–1620. DOI: 10.1136/annrheumdis-2012-203090.
Zelinkova, Zuzana (2014): Gender and Inflammatory Bowel Disease. In: J Clin Cell Immunol 05 (04).
DOI: 10.4172/2155-9899.1000245.