Günter Scheuerbrandt, PhD. Research Report, February 2013 Research approaches fo At an international meeting on research for Duchenne muscular dystrophy in 2000 at th Institutes of Health in Bethesda near Washi Scheuerbrandt, a biochemist in Germany, r would be important to let you, the families boys, and your doctors and other care-giver the scientists and clinicians at that meeting actual state of their research work. So, I wro report for you followed by many others. I d them with difficult “scientific” words, but i language so that you understand what is hap your boys in the laboratories even if you ha modern biochemistry and genetics. On my i www.duchenne-information.eu you can see these reports in English, German, and Span some interviews written since 2008. I am beginning this first part of my repo explication of how dystrophin is made in th cells, and how the absence of this importan causes Duchenne muscular dystrophy. As e is, at present, the most advanced genetic tec an effective therapy, this method with its m trials already completed, still underway or p described in all details in this part of the rep In the second part, to be ready later in th I will describe the most important non-skip ches, like the transfer of the gene, the possib stem cells, the upregulation of utrophin, the of myostatin, the use of steroids, and the dia procedures for finding the mutations in the gene of our Duchenne boys and young men Both parts of the report contain mainly in Genes are functional units of the genetic m ribonucleic acid, DNA. Its structure looks twined ladder of two strands, the double he described in 1953 by James Watson and F (see next page). Each rung of this ladder co four different small molecules, the bases: a nine, thymine, and cytosine, abbreviated A, which we can call the genetic letters. or a Therapy of Duchenne Musc Part 1: Exon Skipping a treatment of he National ington I, Günter realized that it with Duchenne rs, know what said about the ote my first did not write in a rather easy ppening for ave not studied internet pages e the last of nish and also ort with an he muscle nt protein exon skipping chnique for many clinical planned, is port. his year 2013, pping approa- ible use of e inhibition agnostic dystrophin n. nformation on therapeutic research. I know read my report, will send me search approaches, especially ped that might lead to a possi child or of yourself if you are of this report, on page 21, I e how I will handle these reque few personal data you are sen child will be able to benefit f In my summaries, I only m heads of laboratories, althoug students working as a team o but it is impossible to list the names of the scientists witho most of them are professors a degree. A list of some of the is given at the end of this rep numbers in parentheses, e.g. where they could give you m tion in my summaries. These to understand by you, but if y other sent by e-mail, please le I am thanking Pat Furlon American Parent Project Mus the Fight to End Duchenne”, and Kate Bushby, coordinato European Network of Excelle orders”, www.treat-nmd.eu , logos to show their support a explain what the researchers your children. How genes make proteins. material deoxy- like an inter- elix, which was Francis Crick ontains two of adenine, gua- , G, T, and C, The rungs can only contai the base pairs A-T and G-C, between the strands. 1 cular Dystrophy. that many of you, after you e-mails, asking which re- y which exon should be skip- ible treatment of your sick e an adult patient. At the end explain in a separate chapter ests and how I will keep the nding me so that you or the from it. mention the names of the gh they have colleagues and on the projects reported here, em all. I have written the out their academic titles, but and all have an MD or PhD most important publications port. They are indicated by (12), at the places in the text more details than I could men- e publications will not be easy you wish to have one or the et me know. ng, president of PPMD, the scular Dystrophy, “Leading , www.parentprojectmd.org , tor of TREAT-NMD, “The ence for Neuromuscular Dis- for the permission to use their and patronage for my efforts to are doing to find a therapy for in two base combinations, , because then they just fit
Transcript
Günter Scheuerbrandt, PhD.
Research Report, February 2013
Research approaches for a Therapy of Duchenne Muscular Dystrophy.
At an international meeting on research for a treatment of Duchenne muscular dystrophy in 2000 at the National Institutes of Health in Bethesda near Washington I, Scheuerbrandt, a biochemist in Germany, realized that it would be important to let you, the families with Duchenne boys, and your doctors and other care-givers, the scientists and clinicians at that meeting said about the actual state of their research work. So, I wrote my first report for you followed by many others. I did not write them with difficult “scientific” words, but inlanguage so that you understand what is happening for your boys in the laboratories even if you have not studied modern biochemistry and genetics. On my internet pages www.duchenne-information.eu you can see tthese reports in English, German, and Spanish some interviews written since 2008. I am beginning this first part of my report with an explication of how dystrophin is made in the muscle cells, and how the absence of this important protein causes Duchenne muscular dystrophy. As exon skipping is, at present, the most advanced genetic technique for an effective therapy, this method with its many clinical trials already completed, still underway or planned, described in all details in this part of the report. In the second part, to be ready later in this yeI will describe the most important non-skipping ches, like the transfer of the gene, the possible use of stem cells, the upregulation of utrophin, the inhibition of myostatin, the use of steroids, and the diagnostic procedures for finding the mutations in the dystrophin gene of our Duchenne boys and young men Both parts of the report contain mainly information on
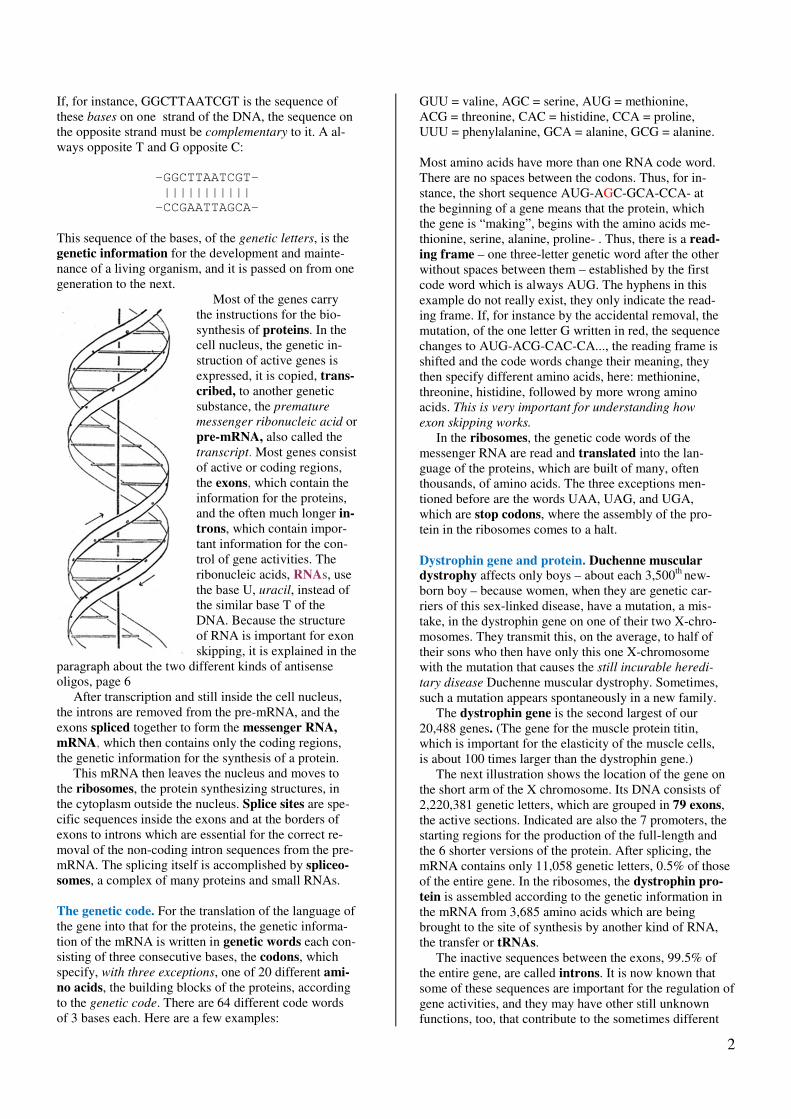
Genes are functional units of the genetic material ribonucleic acid, DNA. Its structure looks like an intertwined ladder of two strands, the double helix,
described in 1953 by James Watson and Franc
(see next page). Each rung of this ladder contains two of four different small molecules, the bases: ade
nine, thymine, and cytosine, abbreviated A, G, T, and Cwhich we can call the genetic letters.
approaches for a Therapy of Duchenne Muscular Dystrophy.
Part 1: Exon Skipping
t an international meeting on research for a treatment of Duchenne muscular dystrophy in 2000 at the National
ashington I, Günter
, a biochemist in Germany, realized that it would be important to let you, the families with Duchenne
givers, know what ing said about the I wrote my first
I did not write them with difficult “scientific” words, but in a rather easy language so that you understand what is happening for
even if you have not studied . On my internet pages
you can see the last of in English, German, and Spanish and also
report with an plication of how dystrophin is made in the muscle
cells, and how the absence of this important protein s exon skipping
most advanced genetic technique for py, this method with its many clinical
or planned, is part of the report.
this year 2013, skipping approa-
the transfer of the gene, the possible use of the upregulation of utrophin, the inhibition
the use of steroids, and the diagnostic procedures for finding the mutations in the dystrophin gene of our Duchenne boys and young men.
Both parts of the report contain mainly information on
therapeutic research. I know that many of you, after you read my report, will send me esearch approaches, especially which exon should be skipped that might lead to a possible treatment child or of yourself if you are an adult patient. At the end of this report, on page 21, I explain in a separate chapter how I will handle these requests and how I will keep the few personal data you are sending me so that you or the child will be able to benefit from it. In my summaries, I only mention the names of the heads of laboratories, although they have colleagues and students working as a team on the projects reported here, but it is impossible to list them all. I have written the names of the scientists without their academic titles, but most of them are professors and all have adegree. A list of some of the most important publications is given at the end of this report. They are indicated by numbers in parentheses, e.g. where they could give you more details than I could metion in my summaries. These publications will not be easy to understand by you, but if you wish to have one or the other sent by e-mail, please let me know. I am thanking Pat Furlong
American Parent Project Muscular Dystrophythe Fight to End Duchenne”,
and Kate Bushby, coordinator of TREATEuropean Network of Excellence for Neuromuscular Di
orders”, www.treat-nmd.eu, logos to show their support and patronage for my efforts to explain what the researchers are doing to find a therapy for your children.
How genes make proteins.
nal units of the genetic material deoxy-ture looks like an inter-double helix, which was
Francis Crick
contains two of adenine, gua-
abbreviated A, G, T, and C,
The rungs can only contain two base combithe base pairs A-T and G-C, because then they just fit between the strands.
1
approaches for a Therapy of Duchenne Muscular Dystrophy.
therapeutic research. I know that many of you, after you read my report, will send me e-mails, asking which re-search approaches, especially which exon should be skip-ped that might lead to a possible treatment of your sick child or of yourself if you are an adult patient. At the end
explain in a separate chapter how I will handle these requests and how I will keep the few personal data you are sending me so that you or the child will be able to benefit from it.
In my summaries, I only mention the names of the ies, although they have colleagues and
students working as a team on the projects reported here, but it is impossible to list them all. I have written the names of the scientists without their academic titles, but most of them are professors and all have an MD or PhD
some of the most important publications is given at the end of this report. They are indicated by numbers in parentheses, e.g. (12), at the places in the text where they could give you more details than I could men-
ummaries. These publications will not be easy to understand by you, but if you wish to have one or the
mail, please let me know. Pat Furlong, president of PPMD, the
American Parent Project Muscular Dystrophy, “Leading
Fight to End Duchenne”, www.parentprojectmd.org, coordinator of TREAT-NMD, “The
European Network of Excellence for Neuromuscular Dis-
, for the permission to use their their support and patronage for my efforts to
explain what the researchers are doing to find a therapy for
The rungs can only contain two base combinations,
C, because then they just fit
2
If, for instance, GGCTTAATCGT is the sequence of these bases on one strand of the DNA, the sequence on the opposite strand must be complementary to it. A al-ways opposite T and G opposite C:
-GGCTTAATCGT-
|||||||||||
-CCGAATTAGCA-
This sequence of the bases, of the genetic letters, is the genetic information for the development and mainte-nance of a living organism, and it is passed on from one generation to the next.
Most of the genes carry the instructions for the bio-synthesis of proteins. In the cell nucleus, the genetic in-struction of active genes is expressed, it is copied, trans-
cribed, to another genetic substance, the premature
messenger ribonucleic acid or pre-mRNA, also called the transcript. Most genes consist of active or coding regions, the exons, which contain the information for the proteins, and the often much longer in-
trons, which contain impor-tant information for the con-trol of gene activities. The ribonucleic acids, RNAs, use the base U, uracil, instead of the similar base T of the DNA. Because the structure of RNA is important for exon skipping, it is explained in the
paragraph about the two different kinds of antisense oligos, page 6 After transcription and still inside the cell nucleus, the introns are removed from the pre-mRNA, and the exons spliced together to form the messenger RNA,
mRNA, which then contains only the coding regions, the genetic information for the synthesis of a protein. This mRNA then leaves the nucleus and moves to the ribosomes, the protein synthesizing structures, in the cytoplasm outside the nucleus. Splice sites are spe-cific sequences inside the exons and at the borders of exons to introns which are essential for the correct re-moval of the non-coding intron sequences from the pre-mRNA. The splicing itself is accomplished by spliceo-
somes, a complex of many proteins and small RNAs. The genetic code. For the translation of the language of the gene into that for the proteins, the genetic informa-tion of the mRNA is written in genetic words each con-sisting of three consecutive bases, the codons, which specify, with three exceptions, one of 20 different ami-
no acids, the building blocks of the proteins, according to the genetic code. There are 64 different code words of 3 bases each. Here are a few examples:
GUU = valine, AGC = serine, AUG = methionine, ACG = threonine, CAC = histidine, CCA = proline, UUU = phenylalanine, GCA = alanine, GCG = alanine. Most amino acids have more than one RNA code word. There are no spaces between the codons. Thus, for in-stance, the short sequence AUG-AGC-GCA-CCA- at the beginning of a gene means that the protein, which the gene is “making”, begins with the amino acids me-thionine, serine, alanine, proline- . Thus, there is a read-
ing frame – one three-letter genetic word after the other without spaces between them – established by the first code word which is always AUG. The hyphens in this example do not really exist, they only indicate the read-ing frame. If, for instance by the accidental removal, the mutation, of the one letter G written in red, the sequence changes to AUG-ACG-CAC-CA..., the reading frame is shifted and the code words change their meaning, they then specify different amino acids, here: methionine, threonine, histidine, followed by more wrong amino acids. This is very important for understanding how
exon skipping works. In the ribosomes, the genetic code words of the messenger RNA are read and translated into the lan-guage of the proteins, which are built of many, often thousands, of amino acids. The three exceptions men-tioned before are the words UAA, UAG, and UGA, which are stop codons, where the assembly of the pro-tein in the ribosomes comes to a halt. Dystrophin gene and protein. Duchenne muscular dystrophy affects only boys – about each 3,500th new-born boy – because women, when they are genetic car-riers of this sex-linked disease, have a mutation, a mis-take, in the dystrophin gene on one of their two X-chro-mosomes. They transmit this, on the average, to half of their sons who then have only this one X-chromosome with the mutation that causes the still incurable heredi-
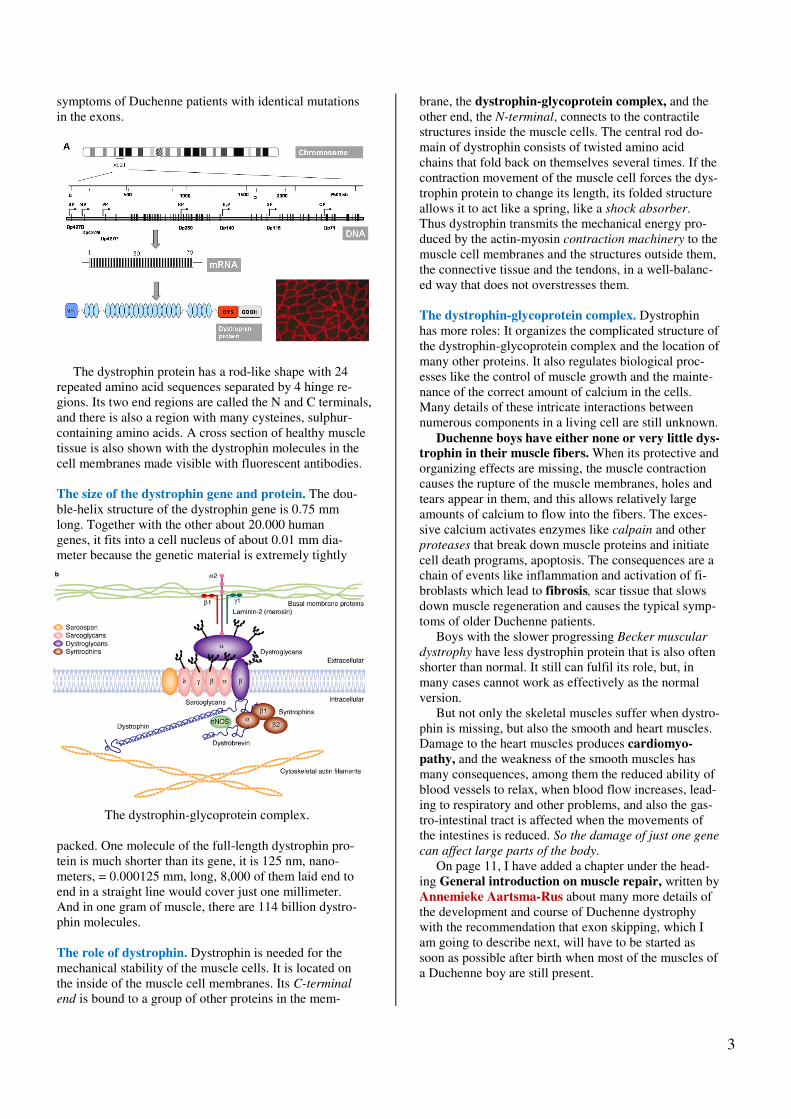
tary disease Duchenne muscular dystrophy. Sometimes, such a mutation appears spontaneously in a new family. The dystrophin gene is the second largest of our 20,488 genes. (The gene for the muscle protein titin, which is important for the elasticity of the muscle cells, is about 100 times larger than the dystrophin gene.) The next illustration shows the location of the gene on the short arm of the X chromosome. Its DNA consists of 2,220,381 genetic letters, which are grouped in 79 exons, the active sections. Indicated are also the 7 promoters, the starting regions for the production of the full-length and the 6 shorter versions of the protein. After splicing, the mRNA contains only 11,058 genetic letters, 0.5% of those of the entire gene. In the ribosomes, the dystrophin pro-
tein is assembled according to the genetic information in the mRNA from 3,685 amino acids which are being brought to the site of synthesis by another kind of RNA, the transfer or tRNAs. The inactive sequences between the exons, 99.5% of the entire gene, are called introns. It is now known that some of these sequences are important for the regulation of gene activities, and they may have other still unknown functions, too, that contribute to the sometimes different
3
symptoms of Duchenne patients with identical mutations in the exons.
The dystrophin protein has a rod-like shape with 24 repeated amino acid sequences separated by 4 hinge re-gions. Its two end regions are called the N and C terminals, and there is also a region with many cysteines, sulphur-containing amino acids. A cross section of healthy muscle tissue is also shown with the dystrophin molecules in the cell membranes made visible with fluorescent antibodies. The size of the dystrophin gene and protein. The dou-ble-helix structure of the dystrophin gene is 0.75 mm long. Together with the other about 20.000 human genes, it fits into a cell nucleus of about 0.01 mm dia-meter because the genetic material is extremely tightly
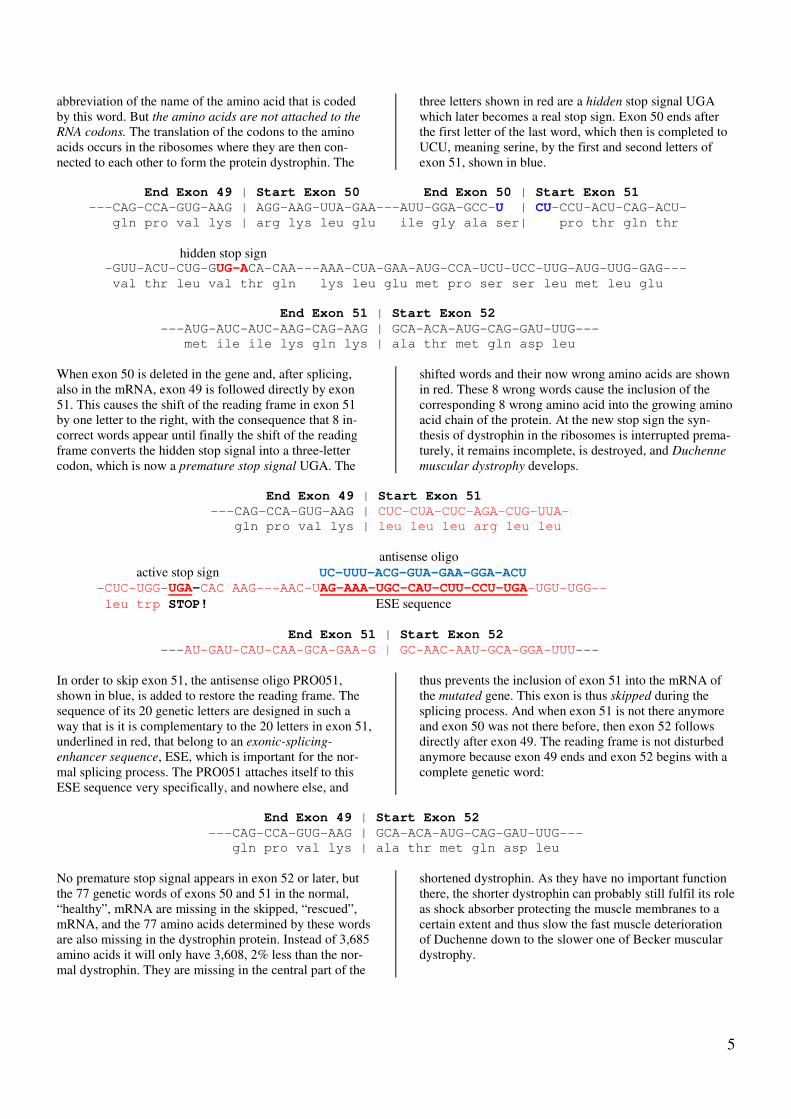
The dystrophin-glycoprotein complex. packed. One molecule of the full-length dystrophin pro-tein is much shorter than its gene, it is 125 nm, nano-meters, = 0.000125 mm, long, 8,000 of them laid end to end in a straight line would cover just one millimeter. And in one gram of muscle, there are 114 billion dystro-phin molecules. The role of dystrophin. Dystrophin is needed for the mechanical stability of the muscle cells. It is located on the inside of the muscle cell membranes. Its C-terminal
end is bound to a group of other proteins in the mem-
brane, the dystrophin-glycoprotein complex, and the other end, the N-terminal, connects to the contractile structures inside the muscle cells. The central rod do-main of dystrophin consists of twisted amino acid chains that fold back on themselves several times. If the contraction movement of the muscle cell forces the dys-trophin protein to change its length, its folded structure allows it to act like a spring, like a shock absorber. Thus dystrophin transmits the mechanical energy pro-duced by the actin-myosin contraction machinery to the muscle cell membranes and the structures outside them, the connective tissue and the tendons, in a well-balanc-ed way that does not overstresses them. The dystrophin-glycoprotein complex. Dystrophin has more roles: It organizes the complicated structure of the dystrophin-glycoprotein complex and the location of many other proteins. It also regulates biological proc-esses like the control of muscle growth and the mainte-nance of the correct amount of calcium in the cells. Many details of these intricate interactions between numerous components in a living cell are still unknown. Duchenne boys have either none or very little dys-trophin in their muscle fibers. When its protective and organizing effects are missing, the muscle contraction causes the rupture of the muscle membranes, holes and tears appear in them, and this allows relatively large amounts of calcium to flow into the fibers. The exces-sive calcium activates enzymes like calpain and other proteases that break down muscle proteins and initiate cell death programs, apoptosis. The consequences are a chain of events like inflammation and activation of fi-broblasts which lead to fibrosis, scar tissue that slows down muscle regeneration and causes the typical symp-toms of older Duchenne patients. Boys with the slower progressing Becker muscular
dystrophy have less dystrophin protein that is also often shorter than normal. It still can fulfil its role, but, in many cases cannot work as effectively as the normal version. But not only the skeletal muscles suffer when dystro-phin is missing, but also the smooth and heart muscles. Damage to the heart muscles produces cardiomyo-
pathy, and the weakness of the smooth muscles has many consequences, among them the reduced ability of blood vessels to relax, when blood flow increases, lead-ing to respiratory and other problems, and also the gas-tro-intestinal tract is affected when the movements of the intestines is reduced. So the damage of just one gene
can affect large parts of the body. On page 11, I have added a chapter under the head-ing General introduction on muscle repair, written by
Annemieke Aartsma-Rus about many more details of the development and course of Duchenne dystrophy with the recommendation that exon skipping, which I am going to describe next, will have to be started as soon as possible after birth when most of the muscles of a Duchenne boy are still present.
4
Exon Skipping
The task of research. A healthy 5-year old boy weighing 30 kg has about 12 kg muscles which contain 1.5 quadril-lion (1.5 x 1015) dystrophin molecules. A 5-year old Du-
chenne boy has already lost 30% of his muscles leaving him with only 8 kg of muscle mass. And theses remaining muscles contain only traces or no dystrophin at all, be-cause the information of the damaged gene cannot be cor-rectly read for biosynthesizing the protein. The small number of muscle cells, less than 3% of all, are called revertant fibers, contain traces of normal dystrophin which appeared by spontaneous exon skipping. It is not known how much dystrophin is needed to pre-vent the disease progression, but it seems that something is better than nothing (1). The new dystrophin doesn't have to be exactly as long as the normal one, it can be shorter, but it must be able to work properly. Exon skipping, a genetic Duchenne therapy. At a dis-cussion in the mid-90s, Gertjan van Ommen of the Uni-versity of Leiden in the Netherlands explained to me how a genetic therapy could accomplish this task for a long time without serious side effects. It is now called exon skipping and has been developed during the last 15 years by many research groups, above all in the Netherlands, France, Japan, Australia, the UK and the United States to such an extent that this procedure is not only being tested on labo-ratory animals but also in clinical trials on Duchenne pa-tients. Exon skipping means “jumping across exons”. Exons are the active sections of a gene. In the dystrophin gene of Duchenne boys mutations have occurred so that one or more exons are missing, deletions, or they are duplicated, duplications, or have mistakes in the sequence of their letters, point mutations. These mutations shift the reading frame in the sick boys by one or two letters from the nor-mal in-frame to the abnormal out-of-frame situation, and a premature stop codon appears soon after the mutation. The reading process of the genetic information for the protein biosynthesis is interrupted at such a “stop sign” so that no dystrophin can be made. These mistakes can be corrected, that is, the protein synthesis can be started
again, if one or more of the still present neighboring exons in the pre-mRNA are blocked in such a way that the me-chanism that joins, splices, the exons, skips over them and thus do not include them any more in the mRNA (2). For this blocking, antisense oligonucleotides are
needed, abbreviated antisense oligos or just oligos in this report. They are short pieces of the genetic material RNA, about 20 to 30 genetic letters long, with a special se-quence, so that they can attach themselves by the Watson-Crick binding to complementary, exactly fitting, sequences inside the exon or exons to be skipped and thus prevent their splicing to the other exons. Where does exon skipping happen? As explained before, the 2.2 million genetic letters of the dystrophin gene in the muscle cell nucleus is copied, transcribed, to the pre-mRNA. The very long intron sequences are then cut out, and only the 79 exon sequences – together only 11,000 letters long – are joined to each other, they are spliced, to the much shorter mRNA. Exon skipping happens during
this splicing process. The shortened mRNA without the deleted and the skipped exons leaves the nucleus and mi-grates to the ribosomes in the cytoplasm. There, the genet-ic information of the mRNA is read and translated into the language of the proteins, into the amino acid sequence of the dystrophin produced. Duchenne is converted into Becker dystrophy. Because of the missing exons – those deleted by the mutation and those skipped in addition –, the amino acids determined by these missing exons will also be missing in the newly made dystrophin. Thus, the new dystrophin will have a chain of amino acids that has fewer than the normal num-ber of 3,685 amino acids. But it will often still be able to protect to a certain extent the muscle cell membranes from the mechanical stress of muscle contraction. Therefore, the symptoms of the disease will be milder, the muscle degen-eration will proceed more slowly, and the life expectancy should increase significantly up to normal in some cases. The Duchenne dystrophy would then have been changed to the mild variant of this disease, to Becker muscular dys-trophy. A therapy but no cure yet. The aim of exon skipping is to convert the disease into a milder form and to slow down disease progression. Thus exon skipping is not a cure but
only a therapy. With this method of gene technology, the damaged gene itself will neither be replaced nor repaired, but only the mechanism of processing its information will be corrected.
Molecular details of skipping exon 51.
After the general explanation of exon skipping and how and where it works, I am showing you here the molecular details of one example of exon skipping: how the antisense oligo PRO051, used by Prosensa, skips exon 51 and thus restores the reading frame which was shifted by the dele-tion of exon 50 in the dystrophin gene of a Duchenne boy. In this and other explanations, I am using the word genetic
letter for the more scientific names base or nucleotide and genetic word for the scientific names triplet or codon. At the beginning I show you part of the sequence of the
letters in exons 50 and 51 of the mRNA as copied from the normal dystrophin gene as well as the sequences at the end of exon 49 and the beginning of exon 52. The hyphens show you only the reading frame and the vertical lines the borders of the exons, but, in reality, the genetic words consisting of 3 letters each follow each other without spaces and without visible borders. For reasons of space, I left out 29 genetic words in exon 50, and 52 words in exon 51. This is indicated by 3 hyphens. To show you what the genetic words mean, I have written below each word the
5
abbreviation of the name of the amino acid that is coded by this word. But the amino acids are not attached to the
RNA codons. The translation of the codons to the amino acids occurs in the ribosomes where they are then con-nected to each other to form the protein dystrophin. The
three letters shown in red are a hidden stop signal UGA which later becomes a real stop sign. Exon 50 ends after the first letter of the last word, which then is completed to UCU, meaning serine, by the first and second letters of exon 51, shown in blue.
End Exon 49 | Start Exon 50 End Exon 50 | Start Exon 51
When exon 50 is deleted in the gene and, after splicing, also in the mRNA, exon 49 is followed directly by exon 51. This causes the shift of the reading frame in exon 51 by one letter to the right, with the consequence that 8 in-correct words appear until finally the shift of the reading frame converts the hidden stop signal into a three-letter codon, which is now a premature stop signal UGA. The
shifted words and their now wrong amino acids are shown in red. These 8 wrong words cause the inclusion of the corresponding 8 wrong amino acid into the growing amino acid chain of the protein. At the new stop sign the syn-thesis of dystrophin in the ribosomes is interrupted prema-turely, it remains incomplete, is destroyed, and Duchenne
muscular dystrophy develops. End Exon 49 | Start Exon 51
---CAG-CCA-GUG-AAG | CUC-CUA-CUC-AGA-CUG-UUA-
gln pro val lys | leu leu leu arg leu leu
antisense oligo active stop sign UC-UUU-ACG-GUA-GAA-GGA-ACU -CUC-UGG-UGA-CAC AAG---AAC-UAG-AAA-UGC-CAU-CUU-CCU-UGA-UGU-UGG--
In order to skip exon 51, the antisense oligo PRO051, shown in blue, is added to restore the reading frame. The sequence of its 20 genetic letters are designed in such a way that is it is complementary to the 20 letters in exon 51, underlined in red, that belong to an exonic-splicing-
enhancer sequence, ESE, which is important for the nor-mal splicing process. The PRO051 attaches itself to this ESE sequence very specifically, and nowhere else, and
thus prevents the inclusion of exon 51 into the mRNA of the mutated gene. This exon is thus skipped during the splicing process. And when exon 51 is not there anymore and exon 50 was not there before, then exon 52 follows directly after exon 49. The reading frame is not disturbed anymore because exon 49 ends and exon 52 begins with a complete genetic word:
End Exon 49 | Start Exon 52
---CAG-CCA-GUG-AAG | GCA-ACA-AUG-CAG-GAU-UUG---
gln pro val lys | ala thr met gln asp leu
No premature stop signal appears in exon 52 or later, but the 77 genetic words of exons 50 and 51 in the normal, “healthy”, mRNA are missing in the skipped, “rescued”, mRNA, and the 77 amino acids determined by these words are also missing in the dystrophin protein. Instead of 3,685 amino acids it will only have 3,608, 2% less than the nor-mal dystrophin. They are missing in the central part of the
shortened dystrophin. As they have no important function there, the shorter dystrophin can probably still fulfil its role as shock absorber protecting the muscle membranes to a certain extent and thus slow the fast muscle deterioration of Duchenne down to the slower one of Becker muscular dystrophy.
6
Antisense-oligo-ribonucleotides, the potential exon skipping drugs. Different types of antisense oligos. For the animal expe-riments and the first exon skipping clinical trials, perform-ed by Prosensa and Sarepta, two kinds of antisense oligos were used. They have the basic structure of ribonucleic acids, RNAs, which is, besides DNA, the second important natural nucleic acid. RNA consists of long chains of alternating units of the sugar-like substance ribose and phosphoric acid. Each ribose unit carries one of the 4 genetic letters, adenine (A), guanine (G), cytosine (C), and, in this case, uracil (U), which is similar to the letter thymine (T) in DNA. The sequences of these letters are important for the function of the many kinds of long and short RNAs, because they can attach themselves to the complementary sequences of DNAs and other RNAs by the Watson-Crick binding rule: G to C and A to U (or T in DNA). This works like a very efficient zipper with 4 different kinds of teeth. The potential exon-skipping drugs, the antisense oli-
gos, are short pieces of RNA with only about 20 to 30 genetic letters. These short sequences are sufficient to guarantee that they attach themselves only to the RNA sequences they are intended to block, although our entire DNA of all our 46 chromosomes in each cell has a DNA sequence of more than 3 billion letters of which about 1%, or 30 million, belong to our about 20.000 genes and there-fore are copied into RNA when they are needed. This is very important, because an antisense oligo against Du-chenne is only allowed to interfere with the genetic infor-mation of the dystrophin gene on the sick boy’s X-chro-mosome and not with that of any other gene. Any such off-
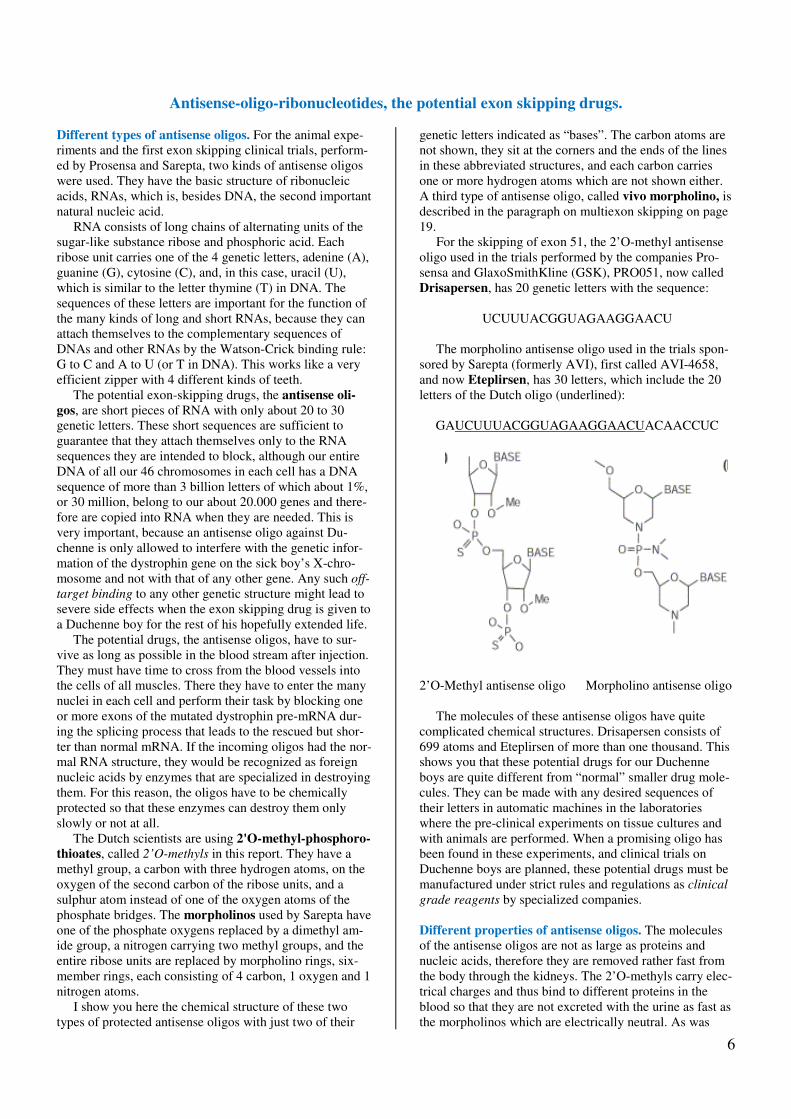
target binding to any other genetic structure might lead to severe side effects when the exon skipping drug is given to a Duchenne boy for the rest of his hopefully extended life. The potential drugs, the antisense oligos, have to sur-vive as long as possible in the blood stream after injection. They must have time to cross from the blood vessels into the cells of all muscles. There they have to enter the many nuclei in each cell and perform their task by blocking one or more exons of the mutated dystrophin pre-mRNA dur-ing the splicing process that leads to the rescued but shor-ter than normal mRNA. If the incoming oligos had the nor-mal RNA structure, they would be recognized as foreign nucleic acids by enzymes that are specialized in destroying them. For this reason, the oligos have to be chemically protected so that these enzymes can destroy them only slowly or not at all. The Dutch scientists are using 2'O-methyl-phosphoro-thioates, called 2’O-methyls in this report. They have a methyl group, a carbon with three hydrogen atoms, on the oxygen of the second carbon of the ribose units, and a sulphur atom instead of one of the oxygen atoms of the phosphate bridges. The morpholinos used by Sarepta have one of the phosphate oxygens replaced by a dimethyl am-ide group, a nitrogen carrying two methyl groups, and the entire ribose units are replaced by morpholino rings, six-member rings, each consisting of 4 carbon, 1 oxygen and 1 nitrogen atoms. I show you here the chemical structure of these two types of protected antisense oligos with just two of their
genetic letters indicated as “bases”. The carbon atoms are not shown, they sit at the corners and the ends of the lines in these abbreviated structures, and each carbon carries one or more hydrogen atoms which are not shown either. A third type of antisense oligo, called vivo morpholino, is described in the paragraph on multiexon skipping on page 19. For the skipping of exon 51, the 2’O-methyl antisense oligo used in the trials performed by the companies Pro-sensa and GlaxoSmithKline (GSK), PRO051, now called Drisapersen, has 20 genetic letters with the sequence:
UCUUUACGGUAGAAGGAACU
The morpholino antisense oligo used in the trials spon-sored by Sarepta (formerly AVI), first called AVI-4658, and now Eteplirsen, has 30 letters, which include the 20 letters of the Dutch oligo (underlined):
GAUCUUUACGGUAGAAGGAACUACAACCUC
2’O-Methyl antisense oligo Morpholino antisense oligo The molecules of these antisense oligos have quite complicated chemical structures. Drisapersen consists of 699 atoms and Eteplirsen of more than one thousand. This shows you that these potential drugs for our Duchenne boys are quite different from “normal” smaller drug mole-cules. They can be made with any desired sequences of their letters in automatic machines in the laboratories where the pre-clinical experiments on tissue cultures and with animals are performed. When a promising oligo has been found in these experiments, and clinical trials on Duchenne boys are planned, these potential drugs must be manufactured under strict rules and regulations as clinical
grade reagents by specialized companies. Different properties of antisense oligos. The molecules of the antisense oligos are not as large as proteins and nucleic acids, therefore they are removed rather fast from the body through the kidneys. The 2’O-methyls carry elec-trical charges and thus bind to different proteins in the blood so that they are not excreted with the urine as fast as the morpholinos which are electrically neutral. As was
7
shown in experiments with mice, the half life in serum, i.e. the time half of the oligos are removed from serum, is about 4-5 weeks for 2’O-methyls, while for the morpholi-nos, it is only about 2-3 hours. Therefore the 2’O-methyls have much more time than the morpholinos to be taken up by muscle cells where they can perform their therapeutic activity. The situation in humans is probably similar be-cause in the first clinical studies on patients with these two types of antisense oligos, as I am explaining later, much higher doses and longer treatment times of morpholinos were needed than by using the 2’O-methyls for obtaining similar results. As an exon-skipping treatment will quite possibly have to be given during the entire life of the boys, subcutaneous
injections – under the skin – will be more practical than intravenous injections into the blood stream, because sub-cutaneous injections can be done at home by lay people or the patient himself, while injections into a vein would re-quire frequent visits to a medical doctor’s office. For this reason the water-soluble 2’O-methyls are already being subcutaneously applied in their clinical trials, but the mor-pholinos cannot be dissolved in water at high doses and thus require injections or infusions into a blood vessel. As explained before, the muscle cells of Duchenne boys have no or very little dystrophin underneath their cell membranes, and the many different proteins that are asso-ciated with dystrophin are missing also. Thus the mem-branes do not have their “shock absorbers” anymore which protects the normal membranes from the mechanical stress during muscle contractions. This means that with time, the membranes break down and are getting tears and holes through which some of the cell contents are leaking into the blood stream, as for instance the enzyme creatine kinase, CK, whose concentration in the blood then increa-ses dramatically and gives the first indication that the boy has a muscular dystrophy. On the other hand, substances from outside can cross the damaged membranes much easier and faster than intact muscle cell membranes. Thus, for a technique like exon skipping that needs its active compounds to get into the muscle cells as fast and efficiently as possible, this mem-brane defect is an advantage. In fact, it has been said that Duchenne muscular dystrophy opens the cell membranes for letting drugs enter because “it likes to be cured”.
How to measure the therapeutic effect of a possible Du-chenne drug. In the exon skipping clinical trials it has to be proven that the antisense oligos really will be able to slow down the degeneration of the dystrophic muscles in Duchenne boys for many years. One way to do this is to use the six minute walk test, 6MWT, which is a so-called outcome measure that is accepted by FDA and EMA for measuring the effect of the treatment on muscular func-tion. Duchenne boys who can still walk, are asked to walk, not run without help as fast as they can for 6 minutes, for instance back and forth through a hospital hallway. The mean distance walked on different days before receiving the first injections is his average 6MWT baseline. A 10-year old boy can walk about 300 to 400 meters in 6 min-utes. At different times during the trial, for instance every 6 weeks, the test is repeated and usually shows that the distance walked decreases because of the progressing muscle wasting. This decrease in meters at different time points is plotted in a diagram which then illustrates the decline of muscle function and thus the progress of the disease. In order to show the combined results for a larger number of patients, the average 6MWT baseline for all patients in the group is set at zero from where the curves start that are obtained with different doses and the results of the placebo group. The points in the curves represent the average changes of all boys in a group in meters at different times, which, because of the decreasing distance are mostly negative. The purpose of such a graphic presentation is to deter-mine, and to make clear to see, whether the treatment in the clinical trial has the desired effect or not. But to do this reliably and objectively without any “human” influence, the trial has to be done double-blind, meaning that about one third or sometimes half of the patients in a trial do not receive the active drug material but a placebo, a material like, for instance, milk sugar, which looks like the drug but does not have any medical effect. The decision whether a patient gets the drug or the placebo is made by chance – the boy is said to be randomized to a group – and neither the parents or the patients nor the clinical or laboratory personnel know before the trial is completed and analyzed to which group a patient belongs.
8
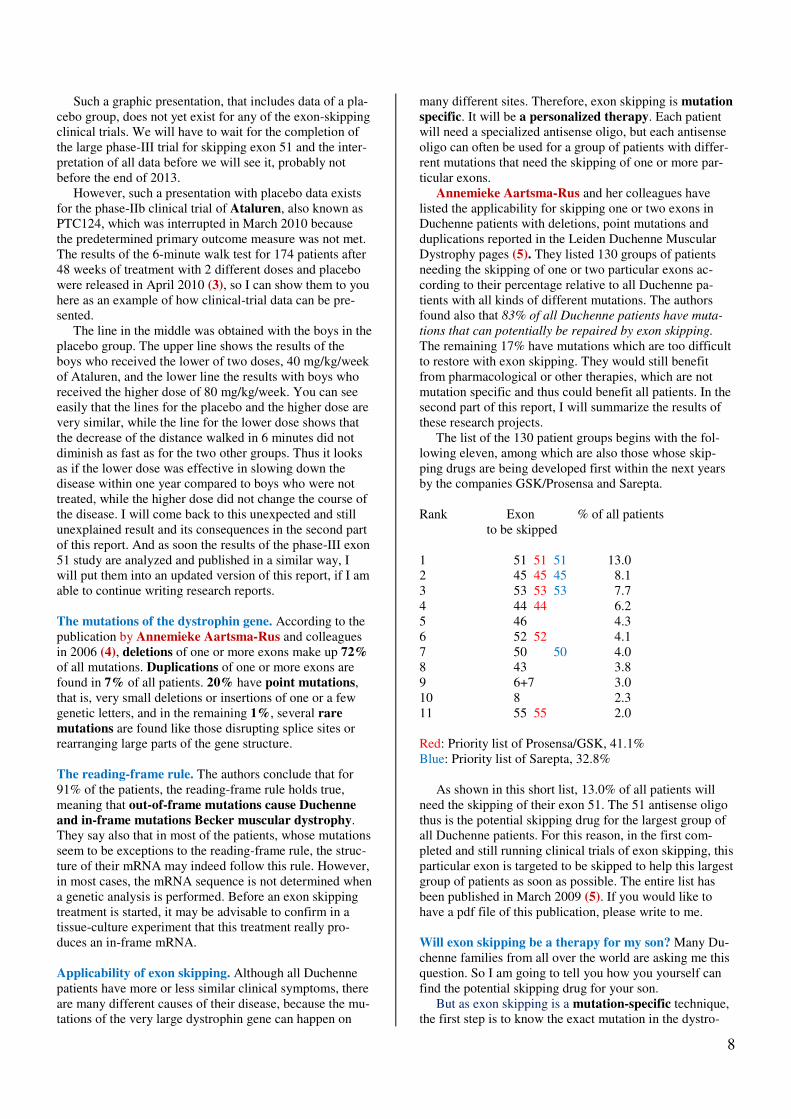
Such a graphic presentation, that includes data of a pla-cebo group, does not yet exist for any of the exon-skipping clinical trials. We will have to wait for the completion of the large phase-III trial for skipping exon 51 and the inter-pretation of all data before we will see it, probably not before the end of 2013. However, such a presentation with placebo data exists for the phase-IIb clinical trial of Ataluren, also known as PTC124, which was interrupted in March 2010 because the predetermined primary outcome measure was not met. The results of the 6-minute walk test for 174 patients after 48 weeks of treatment with 2 different doses and placebo were released in April 2010 (3), so I can show them to you here as an example of how clinical-trial data can be pre-sented. The line in the middle was obtained with the boys in the placebo group. The upper line shows the results of the boys who received the lower of two doses, 40 mg/kg/week of Ataluren, and the lower line the results with boys who received the higher dose of 80 mg/kg/week. You can see easily that the lines for the placebo and the higher dose are very similar, while the line for the lower dose shows that the decrease of the distance walked in 6 minutes did not diminish as fast as for the two other groups. Thus it looks as if the lower dose was effective in slowing down the disease within one year compared to boys who were not treated, while the higher dose did not change the course of the disease. I will come back to this unexpected and still unexplained result and its consequences in the second part of this report. And as soon the results of the phase-III exon 51 study are analyzed and published in a similar way, I will put them into an updated version of this report, if I am able to continue writing research reports. The mutations of the dystrophin gene. According to the publication by Annemieke Aartsma-Rus and colleagues in 2006 (4), deletions of one or more exons make up 72% of all mutations. Duplications of one or more exons are found in 7% of all patients. 20% have point mutations, that is, very small deletions or insertions of one or a few genetic letters, and in the remaining 1%, several rare
mutations are found like those disrupting splice sites or rearranging large parts of the gene structure. The reading-frame rule. The authors conclude that for 91% of the patients, the reading-frame rule holds true, meaning that out-of-frame mutations cause Duchenne
and in-frame mutations Becker muscular dystrophy. They say also that in most of the patients, whose mutations seem to be exceptions to the reading-frame rule, the struc-ture of their mRNA may indeed follow this rule. However, in most cases, the mRNA sequence is not determined when a genetic analysis is performed. Before an exon skipping treatment is started, it may be advisable to confirm in a tissue-culture experiment that this treatment really pro-duces an in-frame mRNA. Applicability of exon skipping. Although all Duchenne patients have more or less similar clinical symptoms, there are many different causes of their disease, because the mu-tations of the very large dystrophin gene can happen on
many different sites. Therefore, exon skipping is mutation
specific. It will be a personalized therapy. Each patient will need a specialized antisense oligo, but each antisense oligo can often be used for a group of patients with differ-rent mutations that need the skipping of one or more par-ticular exons. Annemieke Aartsma-Rus and her colleagues have listed the applicability for skipping one or two exons in Duchenne patients with deletions, point mutations and duplications reported in the Leiden Duchenne Muscular Dystrophy pages (5). They listed 130 groups of patients needing the skipping of one or two particular exons ac-cording to their percentage relative to all Duchenne pa-tients with all kinds of different mutations. The authors found also that 83% of all Duchenne patients have muta-
tions that can potentially be repaired by exon skipping. The remaining 17% have mutations which are too difficult to restore with exon skipping. They would still benefit from pharmacological or other therapies, which are not mutation specific and thus could benefit all patients. In the second part of this report, I will summarize the results of these research projects. The list of the 130 patient groups begins with the fol-lowing eleven, among which are also those whose skip-ping drugs are being developed first within the next years by the companies GSK/Prosensa and Sarepta. Rank Exon % of all patients
to be skipped 1 51 51 51 13.0 2 45 45 45 8.1 3 53 53 53 7.7 4 44 44 6.2 5 46 4.3 6 52 52 4.1 7 50 50 4.0 8 43 3.8 9 6+7 3.0 10 8 2.3 11 55 55 2.0 Red: Priority list of Prosensa/GSK, 41.1% Blue: Priority list of Sarepta, 32.8% As shown in this short list, 13.0% of all patients will need the skipping of their exon 51. The 51 antisense oligo thus is the potential skipping drug for the largest group of all Duchenne patients. For this reason, in the first com-pleted and still running clinical trials of exon skipping, this particular exon is targeted to be skipped to help this largest group of patients as soon as possible. The entire list has been published in March 2009 (5). If you would like to have a pdf file of this publication, please write to me. Will exon skipping be a therapy for my son? Many Du-chenne families from all over the world are asking me this question. So I am going to tell you how you yourself can find the potential skipping drug for your son. But as exon skipping is a mutation-specific technique, the first step is to know the exact mutation in the dystro-
9
phin gene of your sick boy. The mutation can best be de-termined in a modern genetic laboratory with the MLPA method (multiplex ligation-dependent probe amplifica-tion), which analyzes all 79 exons in Duchenne boys and their mothers and other female relatives. This and other diagnostic techniques will be summarized in the second part of this report. With the exact mutation known – mainly deletion, du-plication, or point mutation – you yourself may examine the sequence of the 11,040 genetic letters of the combined 79 exons of the dystrophin mRNA which contains the instructions for the assembly of the 3,685 amino acids of the normal dystrophin protein. You can download the 15 pages with this sequence from Leiden Muscular Dystrophy
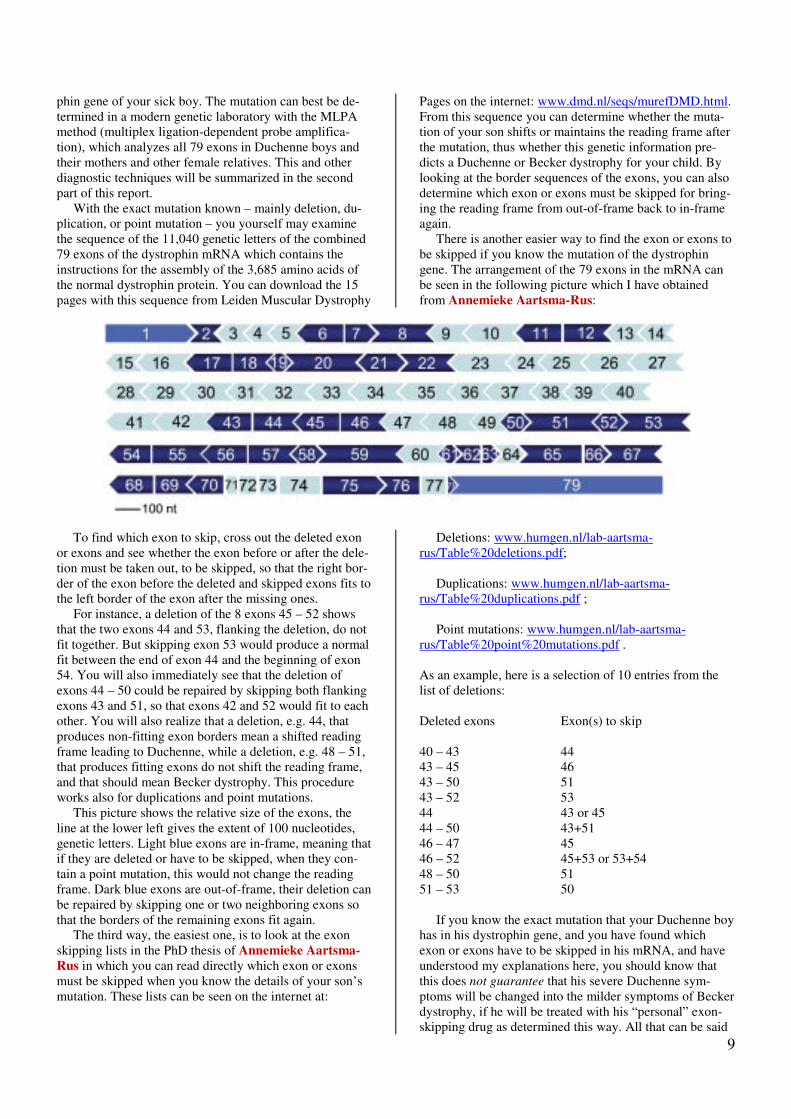
Pages on the internet: www.dmd.nl/seqs/murefDMD.html. From this sequence you can determine whether the muta-tion of your son shifts or maintains the reading frame after the mutation, thus whether this genetic information pre-dicts a Duchenne or Becker dystrophy for your child. By looking at the border sequences of the exons, you can also determine which exon or exons must be skipped for bring-ing the reading frame from out-of-frame back to in-frame again. There is another easier way to find the exon or exons to be skipped if you know the mutation of the dystrophin gene. The arrangement of the 79 exons in the mRNA can be seen in the following picture which I have obtained from Annemieke Aartsma-Rus:
To find which exon to skip, cross out the deleted exon or exons and see whether the exon before or after the dele-tion must be taken out, to be skipped, so that the right bor-der of the exon before the deleted and skipped exons fits to the left border of the exon after the missing ones. For instance, a deletion of the 8 exons 45 – 52 shows that the two exons 44 and 53, flanking the deletion, do not fit together. But skipping exon 53 would produce a normal fit between the end of exon 44 and the beginning of exon 54. You will also immediately see that the deletion of exons 44 – 50 could be repaired by skipping both flanking exons 43 and 51, so that exons 42 and 52 would fit to each other. You will also realize that a deletion, e.g. 44, that produces non-fitting exon borders mean a shifted reading frame leading to Duchenne, while a deletion, e.g. 48 – 51, that produces fitting exons do not shift the reading frame, and that should mean Becker dystrophy. This procedure works also for duplications and point mutations. This picture shows the relative size of the exons, the line at the lower left gives the extent of 100 nucleotides, genetic letters. Light blue exons are in-frame, meaning that if they are deleted or have to be skipped, when they con-tain a point mutation, this would not change the reading frame. Dark blue exons are out-of-frame, their deletion can be repaired by skipping one or two neighboring exons so that the borders of the remaining exons fit again. The third way, the easiest one, is to look at the exon skipping lists in the PhD thesis of Annemieke Aartsma-
Rus in which you can read directly which exon or exons must be skipped when you know the details of your son’s mutation. These lists can be seen on the internet at:
Deletions: www.humgen.nl/lab-aartsma-rus/Table%20deletions.pdf; Duplications: www.humgen.nl/lab-aartsma-rus/Table%20duplications.pdf ; Point mutations: www.humgen.nl/lab-aartsma-rus/Table%20point%20mutations.pdf . As an example, here is a selection of 10 entries from the list of deletions: Deleted exons Exon(s) to skip 40 – 43 44 43 – 45 46 43 – 50 51 43 – 52 53 44 43 or 45 44 – 50 43+51 46 – 47 45 46 – 52 45+53 or 53+54 48 – 50 51 51 – 53 50 If you know the exact mutation that your Duchenne boy has in his dystrophin gene, and you have found which exon or exons have to be skipped in his mRNA, and have understood my explanations here, you should know that this does not guarantee that his severe Duchenne sym-ptoms will be changed into the milder symptoms of Becker dystrophy, if he will be treated with his “personal” exon-skipping drug as determined this way. All that can be said
10
is that the particular skipping you have correctly identified will change the reading frame of the genetic message of the mRNA from the out-of-frame back to the in-frame si-tuation. It does not say that the in-frame genetic message will produce a “Becker”-dystrophin in every case, because the reading-frame rule has many exceptions. The reasons for these exceptions are not completely un-derstood in each case. For instance, the borders of the dele-tions in the dystrophin gene are in most cases not the same as the borders of the exons but lie somewhere inside the often very large introns between the exons. These deletion borders are normally not determined by the usual genetic test methods, and they may be different in patients with the same deletions. Because the introns contain sequences which are important for the regulation of genes, their pre-sence or absence may produce different disease symptoms. On the other hand, the dystrophin protein has a structure with regions of different importance. Some deletions to-gether with the skipped exons may, in some cases, produce an altered protein structure that does not allow the shor-tened dystrophin to function more or less normally. Thus, although an exon skipping therapy will in many cases produce a protein that reduces the dystrophic sym-ptoms, there might be surprises, which will become appa-rent during clinical trials and actual treatments. Mutations that cannot be repaired by exon skipping. As I said before, 17% of all Duchenne boys have muta-tions that cannot be treated by exon skipping. For instance, when either the first or the last exon is deleted, or when the mutations are in region of exons 64-70, which are needed for the essential cysteine-rich part of the protein, or when the deletions are large and involve the actine-binding or an important part of the central part of the protein, or when there are large rearrangements like inversions and trans-locations of sequences, which mix up the genetic message in an uncontrollable way. So, if the genetic test results of your son doesn’t allow you to find the exon or exons to be skipped by using my instructions here, or if you have other questions about what could be done for him, please write a personal e-mail to me, [email protected], in English, German, French, or Spanish, and I will answer as soon as possible, but only in English or German. Writing in French or Span-ish without too many mistakes is too difficult for me. How the exon-skipping drugs are made. Now, that you, after reading my explanations, know what kind of exon skipping could possibly be a therapy for your son, I will explain, how these potential drugs are being made. There are three parts of this chapter: First, what kinds of clinical trials have to be done, then, which drugs are being deve-loped first, and finally, which clinical trials have been already completed, which ones are being performed and which ones are planned for the near future. What kinds of clinical trials have to be done? The Fed-eral Drug Administration, FDA, in the United States, the European Medicines Agency, EMA, in London, and other regulation agencies require that the “normal” development of a classical drug has to go through the following stages:
The pre-clinical phase involving laboratory and animal studies to assess the potential drug’s safety, the biological activity, and the best method to give it to a patient. The clinical phase-I trial on 20 – 100 healthy volunteers to determine its safety in humans. The clinical phase-II trial on 100 – 500 patients to evalu-ate optimal dosages, safety, and efficacy. The clinical phase-III trial on 1,000 – 5,000 patients to confirm the drug’s safety and effectiveness when used for a long time. The cost of all three clinical investigational trials can be up to 500 million US$ for one drug and it may take up to 15 years from the first idea for a new drug until its market approval. The regulatory rules were made in an age when patient-specific types of research approaches as exon skipping were not yet being done. To get a personalized Duchenne drug through these stages, several challenges are encoun-tered and have to be overcome. For instance, phase-I safety studies with antisense oli-gos in healthy volunteers could shift the reading frame in a normal dystrophin mRNA and, if they are sufficiently effective, give the healthy volunteers Duchenne dystrophy, a very serious side effect which has nothing to do with normal adverse events. Another major concern would be off-target effects, meaning that exons could be skipped in the genetic information of other than the dystrophin gene and create severe and possibly unknown diseases. Another problem, not encountered in normal drug de-velopment, might be specific to Duchenne dystrophy: be-cause of the absence of dystrophin, the cell membranes of Duchenne muscles have tears and holes through which the exon skipping drugs can get into the cytoplasm of the cells and also into the nucleus where they are needed for their therapeutic action. Thus, certain adverse effects might appear only in Duchenne patients but not in people without this disease. Thus, a phase-I clinical trial with healthy volunteers
cannot be performed with potential exon skipping drugs.
Participation in clinical trials. Clinical trials on patients are indispensable steps to the full development of an exon skipping therapy. It is understandable that families are trying to get their sick children to be accepted in the trials because they hope that their child will then have a chance for an earlier therapy than having to wait many years more for the final approval of his personal medication. But clinical trials are just human experiments which also can go wrong. So the families should listen carefully to the information given by the clinicians performing the trial before they are ready to give their informed consent. Participation has also disadvantages which have been explained by Kate Bushby of TREAT-NMD in an inter-view I recorded with her in March 2009: “I don’t think that it is practical for children to come from far away to participate in clinical trials, because they have to be at the clinical centers every week for injections
11
and a lot of blood samples taken, so the best is when they live near the centers. Even when they live close by, the families have to put their whole life on hold. They should realize that the trials are only trials. In the later efficacy trials, their child could even be on placebo. It cannot help him for the duration of the trial and there may be unfore-seen side effects. Trials are really hard work. I would even say that the children in the trials are almost at a disadvan-tage. Because they have to go through a hassle to get to something everybody else will profit from later, provided it is proven to work. We are very grateful indeed to the families and boys who take all the time and effort to par-ticipate in these studies, which we really hope will move things forward for everyone.” However, there is one important potential advantage
for the participants: If a phase-II or phase-III trial shows that the treatment looks as if it is effective to some extent, then the trial may be followed by an open-label extension period over several years during which all boys – also those who had obtained a placebo during the trial – will receive the most effective dose used in the trial possibly until the drug is approved in their country. General introduction on muscle repair. The text of this paragraph has been written by Annemieke Aartsma-Rus after a workshop on muscle stem cells, which took place in New Orleans, USA, in July 2012. “Muscular dystrophies, such as Duchenne muscular dystrophy are characterized by continuous damage of muscle tissue, eventually leading to loss of muscle tissue and muscle function. Like most tissues, muscle is able to regenerate itself when it is damaged. However, unlike most tissues, muscles do not consist of single cells, but of fibers that originate from single cells that have fused to-gether. After this differentiation process, the muscle fibers are no longer able to divide or to regenerate. However, dedicated single cells, called satellite cells lying on top of muscle fibers, are able to divide and repair muscle. Once muscle fibers are damaged, damage factors are released that activate the satellite cells, which then start dividing, migrate to the damaged area and repair it by fusing with the muscle fibers, or – if there is a lot of dam-
age – by fusing to each other to form a new fiber. To make sure the muscle can be repaired during the next bout of damage, one of these cells becomes an inactive satellite cell, again located on top of the new or repaired muscle fiber. All people get muscle damage occasionally and the regeneration system makes sure the damage is repaired and the muscles grow bigger and stronger, to prevent damage in the future. The problem with Duchenne muscular dys-trophy is that muscle fibers are much more sensitive to being damaged, due to the loss of essential proteins that stabilize muscle fibers during contraction. These proteins are e.g. dystrophin and proteins associated to dystrophin. Thus, in Duchenne patients, muscle fibers will be da-maged easier and more frequently than in healthy people. This puts a chronic stress on the repair system and leads to inflammation. Normally, inflammatory cells play an im-portant role in muscle damage: they break down the da-maged tissues – they are a kind of a waste disposal system – to make room for new muscle fibers. However, due to the chronic nature of the disease, there is continuous in-flammation, which eventually leads to fibrosis, meaning that connective tissue is formed rather than new muscle tissue, because the inflammatory cells secrete signal pep-tides that make the satellite cells become fibroblasts rather than muscle forming cells. Fibroblasts produce signal peptides, short protein pieces, that sustain and enhance fibrosis formation. So this is a vicious circle where more and more fibrosis is formed and muscle repair happens less and less. As muscle tissue keeps getting damaged, eventu-ally most muscle fibers will be replaced by fibrotic tissue and muscle function will be lost.” The consequence of Annemieke’s explanation is that the most important effect of exon skipping therapy is the reappearance of the stabilizing protein dystrophin and its associated proteins of the dystrophin-complex in the sur-viving muscle fibers. This slows down or even stops the fibrotic process but the connective tissue once produced, does not disappear. Thus, exon skipping should be started
very early in the life of a Duchenne boy, before the fibrosis
has started and most of the muscle fibers are still present.
Clinical trials of exon skipping. The development of the personalized genetic exon skip-ping drugs will have to be done by companies with suffi-cient financial resources which will allow them to over-come the technical and ethical problems of completely new kinds of drugs that are designed to interfere with the genetic message of a human gene, although not with the gene itself. Three companies are to be mentioned here which have already brought the exon-skipping method to be the most advanced technique for a therapy of Duchenne muscular dystrophy. With about 400,000 patients worldwide, Du-chenne dystrophy belongs with cystic fibrosis to the most frequent hereditary diseases of childhood. I am not going to describe these companies here with
my own words, but give you their names and internet ad-dresses so that you can look at their home-pages of infor-mation on their Duchenne research work. Prosensa Therapeutics BV in Leiden, the Nether-lands, www.prosensa.com. GlaxoSmithKline PLC (GSK) with headquarters in London, www.gsk.com, enter “Duchenne” in the search space at the upper right and click on “go”. Sarepta Therapeutics (formerly AVI Biopharma) in Cambridge, MA, USA, www.sareptatherapeutics.com.
12
The first two clinical trials for skipping exon 51 in Duchenne boys.
After many years of preclinical work with antisense oligos on muscle cultures in the laboratory, with dystrophic mdx-mice which have a premature stop codon in their exon 23, and also with “humanized” mice, normal mice containing the human dystrophin gene, the first four clinical trials to skip the human exon 51 in Duchenne boys were started in 2006. Two of them were local ones, in which part of only one unimportant muscle was treated and thus could not provide a clinical benefit to the participating boys. The two other trials were systemic ones, in which the potential drugs, the exon-51 antisense oligos, were injected to gain access to the blood circulation, so that they could reach all muscles. The main question these four trials were designed to answer was not whether an improvement of the muscle function was possible by this treatment, but: are the poten-
tial new drugs safe and can evidence of new dystrophin be
seen? After all, if they work, they would later have to be given for many years during the hopefully extended life-time of the boys and therefore should not have any serious side effects and, above all, they should only repair the genetic message of the dystrophin gene and not interfere with any of the other more than 20,000 human genes and their information. Local open-label phase-II exon-51 skipping trial in the Netherlands. The first in-human trial with the exon skip-ping technique was performed by Judith van Deutekom, Jan Verschuuren, and others of Prosensa Therapeutics
and the Leiden University Medical Center between Janu-ary 2006 and March 2007. It was designed to provide a proof of principle only. It was a local study on a small area of the tibialis anterior muscle of the shin, which was treated with a 2’O-methyl antisense oligo against exon 51 called PRO051. The four non-ambulant boys in this open study without placebos were between 10 and 13 years old and had dele-tions of the exon(s) 50, 52, 48-50, or 49-50. Each boy re-ceived a single dose of 0.8 mg PRO051 injected directly into his shin muscle. After 4 weeks, muscle tissue was obtained in a biopsy from the injection site and tested for the skipped mRNA and new dystrophin protein. Up to 94% of the muscle fibers in the biopsy sample showed new dystrophin at their normal position under the muscle fiber membranes in levels of 33%, 35%, 17%, and 25% compared to healthy muscle tissue. The mRNAs were isolated and sequenced which showed that the bases, the genetic letters, of the deleted exons and the skipped exon 51 was missing from the normal sequence. This proved that exon skipping really skips the targeted exon in human muscle. This first application of the exon-skipping technique in Duchenne boys was published on 27 December 2007 in the New England Journal of Medicine (6). Systemic phase IIa trial in Sweden and Belgium to skip exon 51 in Duchenne boys. With the next step towards the full development of this technique, the scientists had to show that the antisense oligo PRO051 can also be applied
systemically by injection into the blood circulation so that the drug can reach and treat all muscle cells. Between July 2008 and January 2009, Prosensa per-formed this first systemic trial with 12 5-13-year old Du-chenne boys with the antisense oligo PRO051 injected subcutaneously, under the skin. The injections were done by the teams of Nathalie M. Goemans at the Department of Pediatric Neurology of the University of Leuven in Bel-gium and of Mar Tulinius at the Queen Silvia Children’s Hospital in Gothenburg in Sweden. In this open-label dose-escalation study, the four groups of three boys received the 51 antisense oligo once per week for five weeks in doses of 0.5, 2, 4, and 6 mg/kg. This trial is being followed by an open extension study, described in the next section. Muscle biopsies were taken before and after treatment in the first group and at two and seven weeks after treat-ment in the higher-dose group to see if any newly formed dystrophin was stable. The structure of the mRNA and the presence of new dystrophin protein were determined in all biopsy samples, analyzed as described for the local study, which showed that the exon skipping antisense oligo had skipped the targeted exons as intended and that the new dystrophin had, as expected, a molecular weight slightly lower than the normal one. Two weeks after the end of the study, 56-100% of the muscle fibers contained new dystrophin with the largest percentages found in the boys who received the two high-est doses. As expected from the short period of dosing, no improvement in muscle function was seen. But this trial showed for the first time that the subcuta-neous administration of PRO051 resulted in the specific skipping of exon 51 and induced the production of new dystrophin in a dose-related manner, meaning that the highest dose created the highest amount of dystrophin. This first systemic trial with an exon skipping agent in Duchenne was designed to answer the most important question: Is this genetic treatment safe? The whole-body therapy was well tolerated as no immune rejection of the new protein and no clinically significant problems were found in any of the 12 Duchenne patients in the study. All details of this trial were published in the New Eng-land Journal of Medicine in March 2011 (7). Prosensa – GSK partnership. The positive outcome of these two phase-II clinical trials – even before all the de-tails of the results were known – convinced the companies Prosensa and GlaxoSmithKline (GSK) to enter in an exclu-sive worldwide collaboration for the development and commercialization of their exon-skipping technology using the 2’O-methyl antisense oligoribonucleotides. Under this agreement, GSK obtains an exclusive license to develop and market Prosensa’s antisense oligo for the skipping of exon 51 of the dystrophin gene, and both companies will continue to work together for developing this oligo further. As the first step, they have begun in 2010 the pivotal, the decisive, international phase-III clinical trial with at least 180 Duchenne boys who need skipping of exon 51.
13
GSK will take over all costs for this large trial. In addition, GSK has the option to license three more antisense oligos for skipping exons 44, 45 or 53, and 52 or 55. Skipping of exon 44 is already in a phase-II study for
which results are expected in the course of 2013. And then clinical trials for skipping exons 45 and 53 will begin in 2013. GSK’s option rights can be exercised by a successful completion of the exon-44 trial.
The first clinical trials with morpholino antisense oligos for skipping exon 51. Before I continue to describe the trials being done by Pro-sensa and GSK, I am summarizing the two exon skipping trials (and an extension trial), which were similar to those performed by Prosensa but which used another type of antisense drugs, morpholinos, that were developed by the company AVI BioPharma in Bothell near Seattle in the US, now called Sarepta Therapeutics, and headquartered in Cambridge, Massachusetts. These two trials were performed in the UK and not in the USA, because it was easier and faster to obtain the per-mission to start them from the European Agency EMA than from the US Federal Drug Agency FDA.
First local clinical trial with a morpholino 51-antisense oligo in the UK. This phase-IIa exon-skipping trial was performed in the UK between the autumn 2007 and the end of 2008 under the direction of Kate Bushby of TREAT-NMD in Newcastle and Francesco Muntoni at the Imperial College in London. During the pre-clinical experiments, the morpholino antisense oligo, AVI-4658, developed by Steve Wilton in Perth (Australia) was shown by Dominic Wells in London to be sufficiently stable for a long-term clinical treatment. This trial was a local study to assess the safety and bio-chemical efficacy of this morpholino exon-51-skipping drug after one-time injections into a small and unimportant muscle, the extensor digitorum brevis (EDB) muscle at the outside of the foot. Seven 11-16-year old Duchenne boys needing exon-51 skipping – some of them non-ambulant – participated. Each of the 7 patients had less than 5% of revertant fibers in his muscles as determined by a biopsy before the treatment. Different low amounts of these dystrophin-posi-tive muscle fibers are present in many Duchenne boys. They are caused by spontaneous exon skipping. This trial was a single-blind study, meaning that inves-tigators who analyzed the muscle samples did not know whether the tissues came from the treated muscle of the boy or from the control muscle from his other foot. Two boys received 0.09 mg of the morpholino and then the other five a 10-times larger dose of 0.90 mg. Almost the entire treated EDB muscles were removed in biopsies between three and four weeks after the injections. The higher-dose led to an increased dystrophin produc-tion in all treated muscles that ranged from 22% to 32% of the intensity in muscles of healthy persons, and it was 11-21% greater than the background of the revertant dystro-phin in the control muscle from the other foot. Additional tests proved that the new dystrophin had indeed the re-duced molecular weight of the expected shortened Becker-type dystrophin. In the patients who received the very low dose of the drug, exon-skipped mRNA was detected, but no increase of the dystrophin protein could be proven, because the
protein test was not sensitive enough to detect very small protein differences. This in-vivo study showed that the antisense drug AVI-4658 induced the intended skipping of exon 51 and the production of new dystrophin that had moved to its normal place at the inside of the muscle cell membrane and then correctly connected there to the proteins of the dystrophin-glycoprotein complex. This treatment was not associated with any systemic or local adverse side effects or with any immune response against dystrophin. As with all local treatments, no therapeutic benefit for the participating boys was expected Both local studies, the Dutch and the English ones, were designed to furnish a proof-of-principle that exon skipping does work in human patients. And both studies proved that this is indeed the case. There were some tech-nical differences between the two studies, meaning that the results are not directly comparable in all details. The details of this local trial were published 2009 in The Lancet Neurology (8). First systemic clinical trial with a morpholino 51-anti-sense oligo in the UK. In this phase-II open-label trial, 19 still ambulant 6-13 year old boys needing skipping of exon 51 were treated sequentially during the year 2009 in Lon-don and Newcastle upon Tyne, also under the direction of Kate Bushby and Francesco Muntoni. The boys received doses of 0.5 to 20 mg/kg of the AVI-4658 antisense oligo for 12 weeks into the blood circulation by weekly intra-
venous injections so that it could reach all muscles. The aims of the trial were to test for safety and tolerability and not for changes of muscle function and strength. Two muscle biopsies from the biceps of each boy were taken before and after the treatment in order to determine the low amount of dystrophin in the revertant fibers and the increased amount after the treatment In the 7 patients who received the higher dosages of between 2 and 20 mg/kg new dystrophin between 9% and 16% of the normal amount could be detected above the re-vertant background by the analysis of the skipped mRNA and the shortened protein. Three of the four patients who received the highest dosage of 20 mg/kg had 21%, 15%, and 55% of fibers with dystrophin after the treatment. Also some of the dystrophin-associated proteins, which in Du-chenne patients are lost together with dystrophin, had re-appeared after the treatment at their normal location in the muscle cell membranes. No drug-related side effects had appeared during the entire duration of the trial. An improvement of the muscle function was not ex-pected, because the trial was too short for providing changes of muscle performance that could be reliably interpreted. The authors concluded that the safety of the treatment and the proof that the systemically applied AVI-4658 in-
14
deed caused the expected skipping of exon 51 “show the
potential of AVI-4658 to become a disease modifying me-
dication for Duchenne muscular dystrophy” (9).
Extension trial with Sareptas’s morpholino 51-anti-sense oligo, NCT01396239. This trial, called 4658-US-
201 is the double-blind part of the continuation of the previous systemic trial performed by Sarepta but with two higher doses of Eteplirsen, 30 and 50 mg/kg, and 24 weeks of treatment or placebo to see whether new dys-trophin could be shown in muscle tissue from several bi-opsies after the end of this double-blind part of the study. My summary of the organization and the results of this trial is based on a series of press releases by Sarepta, the most recent one dated 7 December 2012 (10). The trial started in February 2012 and is performed under the direc-tion of Jerry Mendell and his colleagues at the Nation-wide Children’s Hospital in Columbus, Ohio. For the first 24 weeks, 12 Duchenne boys in 3 groups received weekly intravenous injections: 4 boys received a dose of 30 mg/kg, 4 a dose of 50 mg/kg, and 4 a placebo. Biopsies to determine dystrophin were performed before the first injection, at 12 weeks (for 50 mg/kg dose) and 24 weeks (for the 30 mg/kg dose), and third biopsies in all boys after 48 weeks. To determine whether these treatments improved the clinical symptoms, various muscle function-tests were performed. But at the end of this double-blind part of the trial with the two doses of 30 and 50 mg/kg/week, the most important test, the 6-minute walk test, did not show a sig-nificant change for the treated patients after 12 or 24 weeks. Thus, after 24 weeks, the trial was continued without time limit as an open-label extension study called 4658-
US-202 to see whether under these conditions an improve-ment of the muscle function can be measured mainly by the 6-minute walk test. Two of the placebo-patients were added to the 4 who are receiving a 50 mg/kg dose, while the other two were added to the 30 mg/kg dose. Meanwhile, two boys in the 30 mg/kg group lost ambulation, so they were unable to participate in the 6 minute walk test. Thus there are now four groups: 4 boys receiving 50 mg/kg/week from the beginning, 4 boys receiving 30 mg/kg/week from the be-ginning, only two of which could participate in the 6 mi-nute walk test, and 4 “placebo-delayed” boys who were on placebo for 24 weeks followed by treatment with 50 or 30 mg/kg/week. As there were no significant differences of the results
with the 6-minute-walk test between the two groups treat-ed with 30 or 50 mg/kg/week Eteplirsen during 62 weeks, the results of only two patient groups are here discussed: Group I of 6 boys, treated from the beginning of the study for 62 weeks, and group II of 4 “placebo-delayed” boys, who were on placebo for the first 24 weeks of the study followed by 38 weeks with 30 or 50 mg/kg Eteplirsen. After 62 weeks of treatment, the 6 treated boys of group I walked 16 meters less in the 6-minute-walk test than at the beginning of the study, while the 4 placebo-delayed boys walked 78 meters less. Thus, the treated boys demon-
strated a significant benefit of 62 meters compared to the results for the 4 placebo-delayed boys. These results are averaged between the boys and rounded to full meters. The fact that the treated boys lost only 16 meters during the 62 weeks (1 year and 2½ months) means that they lost less than 5% of the about 400 meters they could walk in 6 minutes at the beginning of the treatment. The 4 placebo-delayed boys lost less than 10 meters during the 38 weeks of treatment. This suggests that there is a significant slow-
ing of the Duchenne towards the Becker symptoms as ex-
pected from an exon-skipping treatment. Annemieke’s comment: “However, these results have to be interpreted with caution, because the groups are very small and it is known that there is a lot of variation in di-sease progression between individual boys (e.g. underlined by the fact that also 2 of the treated patients lost ambula-tion during the trial).” The positive results of the dystrophin determinations in the muscle tissue obtained by biopsies are another indica-tion that this type of exon skipping works. The morpholino 51antisense oligo Eteplirsen at a dose of 30 mg/ kg/week produced a significant increase of between 16% and 29% of fibers with new dystrophin at 24 weeks of treatment. The shorter treatment, 12 weeks, did not show a significant increase in new dystrophin even when the higher dose of 50 mg/kg/week was used. This shows that a longer trea-
tment than about half a year is required before meaningful
levels of new dystrophin are produced for Eteplirsen. In the boys treated for 48 weeks with either dose, the percentage of muscle fibers containing new dystrophin raised from less than 5% to 47% of the normal level, whereas in the boys who were on placebo for the first 24 weeks, only 38% of fibers contained new dystrophin. Eteplirsen proved safe at both doses of 30 and 50 mg/kg/week over the entire trial period of 62 weeks. Sarepta have indicated they will be discussing these results with the FDA and preparing for a pivotal phase-III double-blind study to be started in 2014.
Clinical trials for skipping exons 51 performed by GlaxoSmithKline (GSK) and Prosensa At the writing of this report, the first four clinical trials to skip exon 51 were completed and their results published. A rather large number of additional trials for skipping exon 51 are now underway. They are being performed by GSK with Prosensa’s 51-antisense oligo PRO051, now called Drisapersen and GSK2402968. Each of these trials has a GSK identification number starting with DMD, and a “clinicaltrials.gov identifier” beginning with the letters NCT. Their details are documented and frequently updated
by the US National Institutes of Health (NIH) and publish-ed on the internet. In order to find the actual information about a specific trial, go to www.clinicaltrials.gov, enter the NCT number into the space for “search for study”, click on “search”, and then on the title of the trial. In the following paragraphs, I am giving short summaries of the most important Duchenne trials and mention their NCT numbers, and also their GSK names, if they are performed by GSK.
15
Prosensa open label extension study PRO051‐02. After the two open 51-trials performed by Prosensa alone, one local and the other systemic, described on page 12, all twelve boys who participated in the systemic trial, are receiving the highest dose, 6 mg/kg/week, of Drisapersen subcutaneously in an extension study which is ongoing for more than 3 years, and still no serious safety concerns have appeared. At the annual meeting of the Parent Project Muscular Dystrophy in the United States, PPMD, in Fort Lauder-dale, Florida, in June 2012, the first preliminary results of the 6-minute walk test after 96 weeks (22 months) were reported. At that time, 7 boys had retained their walking distance or had improved it. Of the 10 boys able to com-plete the 6-minute-walk test at the beginning of the exten-sion trial, two had lost their walking ability. They were those who were already at the end of their independent walking when they entered the trial. That means that the better performing boys at the beginning of the study pro-fited more from the treatment. This is an indication of the long-term positive efficacy of exon skipping, but the results must be cautiously inter-preted because all boys are treated and none are on pla-cebo, so a comparison with the normal course of the dis-ease is not possible. A graphic presentation similar to that shown on page 7 for the Ataluren study, is not yet avail-able.
Phase-III exon-51 GSK trial DMD 114044 . NCT 01254019. This pivotal, deciding, study is a double-blind, phase III trial with the aim to definitely prove that skipping of exon 51 reduces the speed of disease progression as measured by the 6-minute-walk test in Duchenne boys so that the 51-antisense oligo of the 2’O-methyl type, called Drisapersen, will be approved for marketing by the regu-latory agencies FDA in the US and EMA in Europe. This large trial is being performed at 45 clinical centers in 21 countries: Argentina, Belgium, Brazil, Canada, Chile, Czech Republic, Denmark, France, Germany, Hungary, Italy, Japan, South Korea, Netherlands, Norway, Poland, Russia, Serbia, Spain, Taiwan, and Turkey. The United States are missing in this list, because of different requirements by the FDA. Therefore, a similar trial using two different dosages is being performed as described on the right side of this page. The drug injections of the phase-III trial started in De-cember 2010, the last boys were recruited in the third quar-ter of 2012, so that the trial will be complete late in 2013 after the last boys have been treated for one year. The study results are expected to be available in 2014. They will then be presented at the first appropriate medical con-ference and published in an important scientific journal. For this pivotal study, 186 Duchenne boys have been recruited who were at least 5 years old and had received steroids for at least 6 months before entering the trial. The boys receive either 6 mg/kg of the potential drug or an inactive substance as placebo by subcutaneous injection each week for 48 weeks. The reason for having at least 180 boys participating was to make certain that the results are statistically signi-ficant. In this case, the study will be able to show a dif-
ference of at least 30 meters walking distance between treated and placebo boys The main outcome measure, the test to detect an im-provement of the muscle function, is, as in most other exon-skipping trials, the 6-minute walk test. Other tests of muscle strength and breathing performance are also being done. Muscle biopsies to look for new shortened dystro-phin are performed after the end of the treatment, and blood samples are taken throughout the trial for clinical analyses to assess safety. The changes in the quality of life are being followed by the completion of questionnaires. The presence of new shortened dystrophin in the musc-les of treated patients is not sufficient to prove efficacy that the drug really works. The dystrophin could be there but not being in its normal place and thus not be able to make the muscles more stable and to function better. The 6-minute walk test is the better method to prove improved function, because if the boys walk more meters in 6 mi- nutes than the placebo treated patients, the drug has a posi-tive effect. The 6-minute walk test has been accepted by FDA and EMA as the most reliable proof that a new drug for muscle diseases is effective.
Open label extension study, GSK trial DMD 114349, NCT 01480245. Similar to the extension study after the phase-II systemic trial performed by Prosensa, described on the precious page, this trial is a continuation of the treatment for those patients who completed their 48 weeks of injections in the phase-III trial GSK 114044 and of the trial GSK 114117 with intermittent dosages, see next page. All patients are receiving the dose of 6 mg/kg/ week also those who have been on placebos during the first trial. The treatment with steroids has also to continue without inter-ruption. This trial started in September 2011 and will be finished in December 2014. The boys are being treated in the same clinical centers they were treated during the trial itself. It is estimated that about 200 boys will participate. The results will be available early 2015 and then appear in an important medical journal.
Phase-II trial with 2 doses in the USA, GSK trial DMD 114876. NCT01462292. This study is similar to the inter-national phase-III study, but it uses two doses, 3 and 6 mg/kg/wk, and is being performed only in the USA in Sa-cramento CA, Stanford CA, Gulf Breeze FL, Iowa City IA, Kansas City KS, Baltimore MD, Minneapolis MN, St. Louis MO, New York NY, Durham NC, Cincinnati OH, Columbus OH, Portland OR, Dallas TX. Fifty-four patients at least 5 years old and still ambulant will participate. Each patient receives the drug or a placebo once weekly for 24 weeks followed by an observation period of 24 weeks, also called GSK trial DMD 114501
extension study. The injections started in October 2011 and the last boy will have completed his 1-year trial in towards the end of 2013. The outcome measures are the 6-minute walk test, dys-trophin determinations after biopsies and many others mainly to assess safety and the pharmacokinetics, by mea-suring how fast the drug entered the muscles, as well in what way and how fast it was degraded and then elimi-nated from the body. In addition, the new and expensive
16
magnetic resonance imaging (MRI) investigations are being done to check the state of limb, heart and diaphragm muscles to see in detail the effect of the 51-antisense oligo.
Skipping of exon 51 with intermittent treatment peri-ods, GSK trial DMD 114117, NCT01153932. The aim of this phase-II trial was to find out if an intermittent treat-ment with GSK’s anti-51 drug 2402968 would lead to better long-term safety with an equal therapeutic effect when compared with weekly dosing. The study was per-formed in 13 clinical centers in 9 countries: Australia, Belgium, France, Germany, Israel, Netherlands, Spain, Turkey, UK. The trial started in September 2010 and was completed in late 2012. Fifty-three Duchenne boys at least 5 years old and walking independently participated. They had to be on steroids for at least 6 months before and then also during the trial. About one third of the boys received 6 mg/kg of the drug each week injected under the skin for 48 weeks. Another one third were treated in five 10-week cycles: Twice weekly 6 mg/kg in weeks 1, 3, and 5, once weekly in weeks 2, 4, and 6, and no treatment in weeks 7 to 10. The last one third received a placebo, under the same con-ditions. Thus, this study was a double-blind trial. The pri-mary endpoint in this explorative study was the efficacy after 24 weeks of treatment. The results of the trial were determined by measuring repeatedly the change of the muscle function with the 6-minute walk test, the determination of the pharmacokine-tics, and the safety with a number of blood and urine ana-lyses. Muscle biopsies were performed before and after the trial to determine the amount of new and shortened dys-trophin as an effect of the skipping procedure. The results will be published as soon as they are fully analyzed and evaluated.
Skipping of exon 51 in wheelchair patients, GSK trial DMD 114118, NCT01128855. The purpose of this sys-temic trial was to study the safety and tolerability of skipp-ing exon 51 in 20 patients who could not walk anymore, who were older than 9 years and had to use a wheelchair for at least one year but not more than for 4 years. Because the trials with still walking boys have so far not shown any safety problems, the main aim of this study was to make sure that there are no additional safety pro-blems in wheelchair users. Since these boys are less active than those who are walking, and the body composition differs (less muscle) the behavior of the drug in the muscles and its elimination
from the body could be different, and that may mean that the dose required by them might be different. The results of this trial will give important information for further clinical trials with older Duchenne boys and young men. The 19 participants were assigned to 2 groups of 8 boys in which 6 boys received single subcutaneous injections of 3 or 6 mg/kg of GSK anti-51 drug 2402968. Two boys in each group received the same dose of an inactive sub-stance as placebo, thus, this study was a double-blind trial. In a third group of 3 boys, 2 received 9 mg/kg and one a placebo. One and 4 weeks after the injections, extensive clinical tests were performed. There were no serious side effects. The trial was performed in Columbus/Ohio, and in Paris. It started in July 2010 and ended in February 2012. The results will be published as soon as they are fully analyzed.
The exon-51 trials have to prove that exon skipping is effective. The trials for skipping exon 51 are the most important ones for getting antisense oligos against Du-chenne muscular dystrophy approved for marketing in Europe and the United States. If the results of all exon-51 studies can convince the two most important regulatory agencies FDA and EMA, that skipping of exon 51 is effec-tive and safe for a treatment of patients for many years, the permission for marketing of this first genetic drug for a serious genetic disease should be granted within a few years. But skipping of exon 51 would only help 13% of all Duchenne patients. For providing a skipping therapy for the remaining 70% of patients who have less frequent or rare mutations, more than 100 different antisense oligos would have to be developed. It will have taken about 10 years and many million of euros and dollars for the pre-clinical work and the three phases of clinical trials to get the exon-51 skipping drug approved. This time and these expenses must be considerably reduced for producing the many other skipping drugs for the majority of Duchenne patients. Discussions and negotiations by TREAT-NMD, PPMD and other patient organizations with FDA and EMA are underway, to convince the agencies of a quicker develop-ment path for individual oligos if the exon 51 oligo and a second oligo that have been tested extensively have been shown safe and effective. The oligo against exon 44 has been chosen to be this second potential exon-skipping drug, it would provide a therapy for 6.2% of all patients.
Clinical trials for skipping other exons than 51 Phase-II clinical trial for skipping exon 44. NCT 01037309. Prosensa is performing this open label trial with its drug PRO044-CLIN-01 in four clinical centers in Leu-ven, Belgium; in Leiden, the Netherlands; in Gothenburg, Sweden; and in Ferrara, Italy. The trial has started in De-cember 2009 and will be finished in the second half of 2013. The 18 participating Duchenne boys are between 5 and 16 years old, with three boys in each dosing group. These
groups receive different weekly dose-escalating subcuta-neous injections of 0.5, 1.5, 5, 8, 10, 12 mg/kg. Some of the boys are redosed with intravenous injections of 1.5, 5, and 12 mg/kg for 5 weeks. Thirteen weeks after the treatment, biopsies will be performed to determine how much new dystrophin has appeared in the muscle cells. With other tests, the safety, possible side effects, and the pharmacokinetics will be studied
17
If the results of this phase-II study have shown that the skipping of exon 44 is as effective and safe as skipping exon 51, FDA and EMA might not require a very time consuming and expensive phase-III trial for this exon also before agreeing to approve both skipping drugs. Skipping of other exons. In several press releases Prosen-sa has announced that the preclinical work for skipping the four exons 45, 52, 53, and 55, which are, besides exons 51 and 44, also on their priority list (see page 8) will be com-pleted soon. The first clinical trials for skipping exons 45 and 53 will start in 2013, followed by trials for exons 52 and 55 soon after. Similarly, Sarepta is planning trials for skipping exons 45, 50, and 53.
Newborn screening and clinical trial with pre-sympto-matic patients. GSK is planning to begin in 2013 a clini-cal trial for skipping exon 51 in boys younger than 5 years who have no or very few clinical signs of Duchenne dys-trophy, because exon skipping will only be able to treat muscle fibers that are still present and not too much da-maged by the dystrophic process. Lost fibers cannot be made to grow again. For that reason, this therapy could be more effective in pre-symptomatic boys, in those that still have enough muscles left before the disease becomes visible around the age of 3 years. The best solution would be to begin treatment within the first year after birth. To find these boys, newborn screening would be necessary for significantly increased activities of the enzyme creatine kinase, CK, in one spot of dry blood on filter paper. Very high CK activities of more than 1,000 U/L in the blood of a newborn boy mean that he probably has Duchenne dystrophy or another muscular disease like one of the limbgirdle dystrophies. As shown in a pilot newborn screening program per-formed by the group of Jerry Mendell in Columbus/Ohio, it is even possible to sequence the dystrophin gene in the DNA obtained from the leucocytes, the white blood cells, in the dry blood spots of boys with high CK activities (11). This would allow not only to find Duchenne boys right after birth, but also to know their gene mutation and thus a diagnosis within a month or so. An effective exon-skip-ping therapy could then start immediately which might possibly prevent the muscles from even starting to degene-rate. These Duchenne boys would then not have Duchenne
muscular dystrophy!
In the near future, such Duchenne screening programs will probably be added to the already established newborn screenings in many countries for other diseases that can be treated. The international workshop of the European Neu-romuscular Center, ENMC, on Duchenne screening, which took place from 14-16 December 2012 in Naarden near Amsterdam, will pave the way for the acceptance of this type of early screening, soon after Drisapersen, Prosensa/ GSK’s drug to skip exon 51 is definitely proven to be safe and effective. As many of the readers of my reports know, I started working in the field of muscular dystrophy after I founded in 1974 a private laboratory in my house in the village of
Breitnau in the Black Forest about 30 kms east of Frei-burg. Between 1977 and 2011, we performed a voluntary early detection program in Germany for 34 years until November 2011. Together with my colleagues, I described this program and the new bioluminescent test we used for the detection of creatine kinase in dry blood spots in 1986 (12). We tested 537,000 boys among whom we found 155 boys with Duchenne (1:3,600) and 35 with Becker muscu-lar dystrophy (1:15,300) within the first weeks after birth. Exon skipping with gene transfer. Researchers at the University of Versailles and the University of Oxford, Luis García, Aurélie Goyenvalle, Kay Davies and their colleagues are working on the combination of exon skip-ping and gene therapy with the aim to instruct the muscle cells to produce the antisense oligos themselves. They hope to need only one injection of viruses carrying a gene-tic structure for producing continuously the antisense oli-gos thus making repeated injections of free antisense oli-gos unnecessary during the entire possibly extended life-time of the patients. Already in 2004, the scientists created the gene thera-peutic part of this technique by attaching the RNA anti-sense sequences to U7-snRNAs (sn = small nuclear), which are members of the small nuclear RNA family, part of the biochemical machinery that joins the 79 exons in the nucleus to produce the active mRNA for synthesizing the protein dystrophin. These modified U7-snRNAs were then transported with vectors, with harmless adeno associated viruses, AAV, into the muscle cells where they moved into their nuclei to perform exon skipping there during the splicing process. These charged viruses were injected first locally into single muscles and then systemically into the blood circu-lation of mdx mice. In the muscle cells, the usual skipping of their exon 23 restored the reading frame. The new somewhat shortened dystrophin appeared in up to 80% of the fibers of the treated muscles where it migrated to its normal position underneath the cell membranes and was stable for more than one year without causing any immune reaction. The dystrophic processes in the mdx muscles, that is, their accelerated degeneration and regeneration, were com-pletely halted. The systemically treated mdx-mice did not develop the usual muscle damage found in non-treated mdx-mice (13). Five years ago, this U7-gene transfer technique was applied to treat the clinically golden retriever dog which is really sick like a Duchenne boy. These dogs have a muta-tion in the splice site of exon 7 which can be repaired by skipping exons 6 and 8. By using a dog-specific modified U7-snRNA containing antisense sequences against exons 6 and 8, shortened dystrophin at almost the normal level in many muscles was obtained after local injections into muscles and regionally by systemic injection into one leg with blocked circulation. Now, 5 years after these experiments, the long-term results of this treatment were published by Adeline Vulin,
Aurélie Goyenvalle, Luis García and their co-workers (14). After this time, skipped dystrophin was still present in the 6 treated dogs, but the number of fibers containing
18
this new dystrophin had slowly declined not by an immune response, but probably by a continuous dystrophic process such as occurs in human Becker muscular dystrophy. The main reason was probably due to the fact that the rescued
skipped dystrophin had not only the deleted exon 7 miss-ing and the 2 skipped exons 6 and 8 but also, for unknown reasons exon 9 which, however, does not affect the reading frame. Thus 158 amino acids determined by the missing exons 6-9 were lacking in the protein. They were part of the essential actin-binding structure at the one end of the protein that connects it with the stabilizing actin network inside the muscle cells. As this connection is not perfect, it may contribute to the still present but much slower muscle degradation process. The authors propose that this genetic exon-skipping could be used at the beginning of a long-term therapy, followed by normal exon-skipping injections a few years later. After this technique was shown in 2004 to skip exon 23 in mdx mice, which are not really sick, the researchers applied now the same method to so-called double-KO
mice, which neither contain dystrophin nor utrophin and, therefore, are as sick as Duchenne boys (15). After a single intravenous injection of the AAV viruses carrying the antisense sequences against exon 23 of the mice attached to U7-snRNA, near normal levels of dystrophin were re-stored in all muscles examined, including the heart. This resulted in a considerable improvement of their muscle functions, a normalization of the muscle structure as well as a remarkable prolongation of their life span from about 10 weeks to more than 1 year. The scientists have now developed specific U7snRNAs to skip the exons of the human dystrophin gene in order to apply this strategy to DMD patients (16). They also show that multiple U7snRNAs can be delivered by these modi-fied AAV viruses to allow the skipping of several exons at once. Altogether this work represents an important step to-wards clinical application on patients planned for 2015 by Génethon together with the Institut de Myologie and re-search teams in Nantes.
Multiexon skipping. Annemieke’s list of 130 skipping drugs (5) contains 77 which would skip one single exon, and 53 which would skip two exons. This means, that 64% of all patients could benefit from single exon skipping, and 19% would need the skipping of two exons. As I have mentioned on page 8, the development of the seven skippings on the priority lists of Prosensa/GSK and Sarepta of the exons 44, 45, 50, 51, 52, 53, and 55 would benefit 45.1% of all patients. Only some work on double-skipping drugs, those that would skip two neighboring or two separate exons, has been done so far – none are in clinical trials yet – because all the Duchenne work and the large financial investment of the three involved companies are directed first to the development of the priority drugs. When they are shown to be so safe and effective that they will be approved for marketing without delay, it is hoped that the skipping drugs for the less frequent and even rare and more complicated mutations will not have to go through the full series of trials and thus will need much less time and money. First try of skipping exons 45 – 55 with 2’O-methyls. There is, however, an exception to this outlook, namely skipping more exons than two with a mixture, a cocktail, of many antisense oligos: In 2007, Christophe Beroud and his co-workers at the university of Montpellier in southern France published their prediction (17), that skipping the 11 exons 45 to 55 would lead to a shortened dystrophin that would produce a Becker dystrophy with very mild or even no dystrophic symptoms in up to 63% of all Duchenne patients. In effect, several Becker patients have been described with a natural deletion of these exons 45 to 55 who are hardly handi-capped. In 2008, Annemieke Aartsma-Rus and her colleagues tried to remove in cell culture these 11 exons from the dys-trophin mRNA of a healthy person and from 2 Duchenne
patients. However, a cocktail of 2’O-methyl oligos against all 11 exons caused irregular splicing processes producing mixtures of partially skipped and a small amount of fully skipped mRNAs. The authors concluded that this tech-nique does not sufficiently support the clinical develop-ment of multi-exon 45-55 skipping at that time (18). Multiexon skipping in dystrophic dogs. The next step was to try the skipping of two or more exons with one cocktail of oligos. In 2008/09, Eric Hoffman and Terence
Partridge in Washington, Shin'ichi Takeda in Tokyo and their colleagues developed cocktails of 2’O-methyls and morpholino antisense oligos for multiexon skipping in dys-trophic CXMD beagle dogs (19). In contrast to the mdx mice with their mild dystrophic symptoms, these dogs have Duchenne-like symptoms. These dystrophic dogs have a mutation at the splice site of exon 7 in their dystrophin gene which causes the loss of exon 7 from the mRNA and a reading-frame shift with a premature stop codon soon afterwards. Skipping of the two flanking exons 6 and 8 would restore the reading frame. A number of different mixtures of 2’O-methyls and morpholinos were tested in tissue cultures until the most effective mixture was found, which contained two oligos against exon 6 and one against exon 8. Both types of oligo cocktails produced, after local in-jections into one muscle, up to 80% of skipped mRNA and almost normal levels of shortened dystrophin. However, not only the two targeted exons 6 and 8 were skipped, but, for unknown reasons, exon 9 also, which is an in-frame exon whose deletion does not shift the reading frame. For a systemic treatment, performed in Tokyo, three 2-month old dogs were treated by injecting the three-mor-
pholino antisense cocktail into their leg veins with weekly injections for 5, 7, and 50 weeks. In all tested skeletal muscles, but not in the heart muscle, new dystrophin was found in up to 50% of the normal level. As before, exon 9
19
was also skipped. The physical state of the dogs was stabi-lized as it was before the treatment started. This treatment seemed to have halted their muscle de-
generation. Thus, morpholino antisense oligos work well in a large mammal with a similar body structure as in hu-mans, and they are not toxic. Exon skipping with vivo-morpholinos. In 2009, the same groups of researchers in Washington and Tokyo started working with another type of antisense oligos, which were developed earlier by Qi Long Lu and his co-workers at the Carolinas Medical Center in Charlotte, North Carolina. To one end of a normal morpholino oligo, they had added a branched structure of 8 guanidine groups.
This octa-guanidine morpholino is called vivo-mor-
pholino. Its structure allows it to enter the skeletal muscles and also those of the heart with very high efficiency. Mdx-mice were treated with vivo-morpholinos against their exon 23, which contains a premature stop signal. A systemic bi-weekly treatment during 10 weeks produced up to 50% new dystrophin in all fibers of the skeletal mus-cles and in up to 10% of the cardiac muscles, and also in the smooth muscles of the blood vessels and intestines. The muscle functions were improved significantly and there were no serious side effects (20).
Multiexon skipping in dogs with vivo-morpholinos. After the positive results of treating mdx mice with vivo-morpholinos, the researchers repeated their skipping of the 3 dog exons with a cocktail of vivo-morpholinos (21). They used 3-5-month old beagle dogs that already showed mild dystrophic symptoms and injected into five different muscles one milliliter of a cocktail solution containing 120 mg of a mixture of 4 different vivo-morpholino oligos, two of which were directed against exon 6 and two against exon 8. Muscle biopsies were done 2 and 8 weeks after the injection. After two weeks, up to 70% of the muscle fibers con-tained new dystrophin, and after 2 months up to 60%. Al-though only exons 6 and 8 were targeted by the antisense oligos, exon 9 was skipped also as in the earlier experi-ment. Here is Annemieke’s explanation why this happens: “The reason is simple: intron 7 is 110, 000 letters long, intron 8 has only 1,100 . Thus most often exon 8 and 9 will be spliced together before exon 7 and 8 are spliced. So when preventing exon 8 from being joined to exon 7, you skip also exon 9, because it is linked already to exon 8.” Studies of toxicity, pharmacokinetics, and biodistribu-tion were not done after these dog experiments. They will
have to be performed before similar vivo-morpholinos are being used in clinical trials with Duchenne patients. Multiexon 45-55-skipping in mdx52 mice with vivo-morpholinos. Soon after their dog studies with vivo-morpholinos, the same research groups in Tokyo and Washington started preparatory work for skipping the entire block of the 11 exons 45-55 in Duchenne patients, which, as I explained before, would bring a therapy for 63% of all patients (22). Obviously, the researchers were aware of Annemieke’s rather disappointing results of trying the same multi-skip-ping with 2’O-methyl oligos. The Japanese-American re-searchers therefore selected vivo-oligos with sequences that avoided reactions between the different oligos and also self reactions between the two ends of the same oligo. First, experiments with mice had to be done, but not with the usual mdx mice, which need skipping of their exon 23, but specially bred mdx52 mice, which have a deletion of exon 52. Their interrupted dystrophin produc-tion would be restarted by skipping exon 52, one of the exons to be skipped in the multiexon approach. The experiments began in the laboratory with tests on myotubes from these mice. A mixture of 10 vivo-oligos against the ESE sequences, exonic splice enhancers, of the 10 exons 45-51 and 53 (not exon 52) were used for skip-ping with the results that the entire bloc of all 11 targeted exons were skipped as proved by sequencing the mRNAs after the skipping. And it is surprising that there were no
partially skipped mRNAs.
The next experiments were done on living 45-week old mdx52 mice which received 1.5 µg (microgram, 1.5 thou-sandth milligrams) of the 10-oligo vivo cocktail into one shin muscle. After 2 weeks, 70% of the muscle fibers con-tained the correctly shortened dystrophin without the ami-no acids whose genetic code words were in the 10 skipped exons and the one (52) deleted. Again there were no par-tially skipped products, neither mRNA nor protein. And all the proteins of the dystrophin complex were back again at up to100% of their normal level, except the nitric oxide synthase, NOS, which is not so important. Then these mice received systemic injections. Five biweekly intravenous injections were done with 12 mg/kg each with the result, that the skeletal muscles contained only the Becker dystrophin at 8-15% of the normal level and the heart at 2%. These treated mice showed much better muscle function and longer muscle endurance. The blood tests did not show any toxicity, and the CK activity was much reduced. The reason for the mild Becker dystrophy in patients without the exons 45-55 is not known. But it is known that the dystrophin of these patients has a part of the amino acid chain removed that does not upset its folding pattern too much. This might be the reason for its rather normal function in protecting the cell membranes from the mecha-nical stress of the muscle contractions. Advantages of this 45-55 skipping. Up to 63% of Du-chenne patients would benefit from this multi-skipping. The resulting Becker muscular dystrophy would be very mild or even without symptoms but with increased CK
20
activities. This skipping could also ameliorate more se-riously affected Becker patients with in-frame deletions in this region. By using just one or some of the vivo oligos from this mixture, a skipping therapy could be offered to patients who need one or more exons in this region being skipped. The next and most important step will now be the beginning of clinical trials with patients. Annemieke’s comment: “There are many challenges for multiexon skipping yet: Vivo morpholinos are toxic. It will be very costly to develop this mix of 11 AOs (even when
using another chemistry than vivo morpholinos). It is not known how safety tests would have to be done. If some-times you want to use only 2 or 3 oligos of the mix, or just one oligo of the mix for another mutation, you would have to test everything individually, so you do not benefit from having one mix for multiple people. If you want to develop it as a mixture, it is not known whether you can test the mix or have to do individual safety tests with the different components.”
Exon skipping for duplications, point and rare mutations. Exon skipping to repair duplications. Duplications of one or more exons causing a shift of the reading frame happened in about 7% of all Duchenne patients. In principle, they can be repaired by exon skipping also, if it were possible to remove the one additional set of the duplicated exons without touching the first, the original set of exons, the new dystrophin protein would have the nor-mal size. If enough new and normal dystrophin were pro-duced to stop the muscle degradation, this treatment would lead to a cure, and not only to a therapy. The problem is that the antisense oligos recognize both sets of exons that are exactly the same. So if one tries to skip one, both will be skipped. For single-exon duplica-tions, there might be a way out, because in some cases, one can skip a third exon before or after the duplicated ones, and thus restore the reading frame. But for larger dupli-cations, it becomes very complex and thus very challeng-ing, and may perhaps not be possible at all. A new project to correct duplications has been started by Kevin Flanigan and his team at the Nationwide Chil-dren’s Hospital in Columbus/Ohio. As a duplication of exon 2 is the most common single-exon duplication in Duchenne patients, a new laboratory mouse was developed which has such an exon-2 dupli-cation in its dystrophin gene and which develops sym-ptoms of a severe muscle disease. As soon as a sufficient number of these mice have been raised, in-vivo experi-ments will be possible for finding a way to repair this duplication. The researchers have already created cell cultures for laboratory experiments with cell lines from patients with different duplications. They are now trying to correct these duplications with the usual exon-skipping antisense oligos but also with the AAV U7-snRNA technique. This project is being financed by the American parent association Cure Duchenne. Exon skipping to repair point mutations. Point muta-tions are small changes of one or a few genetic letters in the gene itself. If the mutation has added or deleted one single letter, then the reading frame is shifted. Or one letter has been exchanged against another, then the reading frame is not shifted, but the code word now may mean another amino acid. If this exchange does not disrupt the structure of the dystrophin, then nothing happens. But if one of the three stop codons, TGA, TAG, or TAA, has appeared, then – although the reading frame is not shifted – the protein
synthesis is halted at such a premature stop sign, and the result is Duchenne dystrophy. This can often be repaired by skipping the particular exon containing the stop codon if it is an in-frame exon with borders between entire codons so that its deletion would not shift the reading frame. Or, if this does cause a frame shift, then, in some cases, a neighbouring exon would have to be skipped in addition. The drug Ataluren, formerly called PTC124, was de-veloped by the company PTC Therapeutics in New Jersey, USA, because it seemed to be able to read through these premature stop codons that have been caused by point mutations inside an exon. But difficulties during a large clinical trial have retarded its completion. In the second part of this report, I will describe the actual state of Ata-luren research. Exon skipping to repair rare mutations. On page 8, I in-troduced you to Annemieke’s list of 130 groups of pa-tients needing the skipping of one or two exons and that exon skippings are now only developed for 7 of the first 11 groups with the most frequent mutations. These priority skipping medications will be therapies for 45% of all Du-chenne patients. The remaining 38% of all patients who could also be helped by exon skipping belong to the other 123 groups of patients for whom no skipping drugs are being developed at this time. The large majority of them, namely 114 groups, contain only up to 1% of all patients, the 30 smallest not more than 0.02%! If about 400,000 Duchenne boys and young men are now living in the entire world, 1% means 4,000 and 0.02% 80 patients. There is very little chance that their exon skip-ping drug will be developed within their life time! To quote from my interview with Annemieke last year: “this is another problem, because there are only very few patients worldwide for each of the more than 100 groups of boys with rare mutations. Then it is very difficult to develop something, even if you want to do clinical trials, there are so few patients that it becomes statistically very problematic. But the problem is that most of the boys with rare muta-tions who have a proper diagnosis are in the western world, and the majority of the patients live in China and India. There are some parts of China and India where di-agnosis is very well done and care is also provided. How-ever, for the majority of patients care is probably less than in the western world, there is no diagnosis, no-one knows their mutation, and they probably don’t even recognize the
21
disease. I think that is the first problem. Theoretically there may be more than thousand patients in some groups of rare-mutation boys, but we don’t know them.” So, something should be done to change this situation, I have an idea, for instance getting the international Rotary
organization, to which I belong, to help finding the “un-known” patients by telling the pediatricians and family doctors in our organization how these patients can be found and what can be done for them especially in the less developed countries.
Exon skipping for older patients. As I have explained, an exon skipping treatment will be most effective if it is started very early in life of a Du-chenne boy, when most of his muscles are still present. This technique will quite probably be able to slow down or even stop the degradation of surviving muscle fibers, but it cannot make the lost muscle fibers grow again. However, as Gertjan van Ommen and Annemieke Aartsma-Rus have explained in their interviews, older patients, even when their disease has advanced, may also like to have their remaining muscles stabilized which would allow them to lead a meaningful life in spite of their handicap. Gertjan said: “I think exon skipping would be a major improvement for the boys, but their life is not going to be completely unhandicapped. And when you speak to Du-chenne patients, then very often, when they are like 10 to 16 years old, they understand what’s going on and they see that the doctors think that all they want is to live longer. But their main desire is to be able to get around better and to move their muscles better, and to get their hands on the desk so that they can use the computer and that they can use it longer. I have seen older Duchenne boys who, even if they are on steroids, get too weak even to put their hands on the table to use the keyboard of the computer. And losing that for them is really a major loss. And if you could retard that, then you would already help them quite a bit. I know that there are projects going on in technical schools and companies where devices, “bio-robots”, are being developed that would help Duchenne boys and young men making the movements that they are too weak
to do themselves.” And when I asked Annemieke: “Is it really worthwhile to prolong the life of older and very handicapped Du-chenne patients with all the modern management meth-ods?” she answered: “I think it is a good question. And there is only one person whom you can ask it: the patient himself. The patient has to decide whether or not he wants treatment and care. From our perspective, only to be able to move your finger or raising your finger and move your eyes may seem like a horrible situation. But I know pa-tients who are in that situation, and they say: “my life is very valuable to me, I like my life, and I have a computer, I can go to the theater, I can go to the movies, I can go to the soccer matches, and I am happy”. I think if a patient is happy and wants to live, then it is his decision. But if he says, “I don’t want to live, I don’t want this kind of life”, then it is also his decision. And once he is an adult, he can make this decision, not to con-tinue care. The positive attitude of Duchenne patients makes you quite ashamed about the complaining you do, while you are able to walk and to do everything, and this patient has only so little, and in spite of this, he is very content and happy. And if you look back 20, 30 years ago, Duchenne pa-tients didn’t have assisted ventilation then. Now they have it and the quality of their life improves a lot, because hav-ing enough air is very nice. Not only the duration of their life improved, but also its quality and that is what counts even more.”
A future Duchenne therapy for you will depend on your personal dystrophin mutation.
After you have read this report, many of you – the families with Duchenne boys and older Duchenne patients them-selves – will write to me asking to explain in a personal way which research approach might lead to a possible treatment, especially which exon or which exons should be skipped. Your e-mail letters come from all over the world, and in great numbers every time after I have sent a new report to all the about 1,500 addresses on my English, German, and Spanish e-mailing lists. And it is mostly the mothers who often write desperate letters that need special attention which sometimes are the beginning of an exten-sive correspondence. I will probably be able to give you a rather detailed answer to your questions, if you send me the results of a genetic test with the information on the mutation in the dystrophin gene of your son or of yourself, if possible determined with the MLPA method. Please let me have also your or his age and your country of residence. In addition to answering your e-mail, I will keep your data in my personal Duchenne-family list ordered by the
exon- or exons-to-be-skipped as determined by me, or by the name of another therapeutic method that would possi-bly help you. Please understand that this personal list is not like one of the official Duchenne data banks that exist in many countries and which are quite demanding and con-tain much more personal information than I have in my list which only contains the minimum data for allowing me to keep in contact with you. I strongly encourage you to sign up with your national DMD Registry! Here is an explana-tion of how you can find “your” data bank: Go to the home page of TREAT-NMD, www.treat-nmd.eu, then to Re-
sources, to global patient registries, then (on the left side) to registries: patient information, then to national DMD
registries, then to your country and finally click to regis-
ter. There you will find instructions of how to register and a huge amount of information about your national register. To make things easier, I will mention in my personal let-ters to you the direct link to your registry, for instance www.treat-nmd.eu/registry/353 for the United States or www.treat-nmd.eu/registry/354 for the United Kingdom.
Let me state at the end that as I have a scientific doctor title, PhD, and not a medical one MD, I cannot accept any legal liability for my information I am giving you in this report or in my letters. Therefore you should also consult a medical doctor or geneticist to check and confirm all my
Other research approaches. In this first part of my report I have explained all the details of the exon skipping technique and its application for finding a therapy for Duchenne muscular dystrophy. But not all patients will be able to benefit in the not too far future from it eitcause they have a mutation that cannot be repaired by skipping one or more exons, or because their mutation is so rare that their skipping drug will not be developed soon enough. But, as Gertjan van Ommen has said in the interview I recorded with him last year: “There are therapies being developed for Duchenne patients independent of themutation. Just to mention two of them: Improving myogenesis, muscle generation, by inhibiting myostatin
finding a replacement for dystrophin by upregul
utrophin. Fibrosis, the growth of connective tissue in plaes of lost muscle fibers, is also an important cause of mucle weakness. If you could reduce the fibrosis, then maybe you could give a Duchenne patient a disease that is like that of the mdx mouse, which has a much milder form of the disease. And so I really think that several of those pharmaceutical interventions will come along and improve the muscle condition. And they may be used by themselves or in combination with exon skipping“. In the second part of this report, which will be ready within a few months, I will describe the most important other techniques. This is my last report. I am sorry to say that this will be my last report because I am now 82 years old and really should find somebody who could continue my work of explaining to you and many other Duchenne families in the world what the scientists in many laboratories are ding for finding therapies or perhaps even a cure for the
(1) Li D, Yue Y, Duan D. Marginal level dystrophin epression improves clinical outcome in a strain of dystrphin/utrophin double knockout mice. PLoS One 2010; 5; e15286 (2) van Ommen GJ, van Deutekom JT, AartsmaThe therapeutic potential of antisense-mediated exon skiping. Curr. Opin. Mol. Ther. 2008; 10; 140- (3) Sarepta Therapeutics Announces Significant Clinical Benefit With Eteplirsen After 36 Weeks in Phase IIbfor the Treatment of Duchenne Muscular Dystrophy
I have a scientific doctor title, PhD, and not a medical one MD, I cannot accept any
my information I am giving you in this report or in my letters. Therefore you should also consult a medical doctor or geneticist to check and confirm all my
information. And let me say again that you should register your child or yourself in a DMD data banpossible and that you please confirm in writing by eto me that you have done it.
The future of my reports.
In this first part of my report I have explained all the details of the exon skipping tech-nique and its application for finding a therapy for Du-chenne muscular dystrophy. But not all patients will be able to benefit in the not too far future from it either be-cause they have a mutation that cannot be repaired by skipping one or more exons, or because their mutation is so rare that their skipping drug will not be developed soon
has said in the interview I There are therapies being
independent of their mproving myo-
myostatin, or upregulating
, the growth of connective tissue in plac-es of lost muscle fibers, is also an important cause of mus-cle weakness. If you could reduce the fibrosis, then maybe you could give a Duchenne patient a disease that is like
mouse, which has a much milder form of
And so I really think that several of those pharmaceu-tical interventions will come along and improve the muscle condition. And they may be used by themselves or in com-
In the second part of this report, which will be ready within a few months, I will describe the most important
I am sorry to say that this will be my last report because I am now 82 years old and really should find somebody who could continue my work of explaining to you and many other Duchenne families in
ratories are do-haps even a cure for the
Duchenne muscular dystrophy of your son. I have tried to find such a person, however with no success so far. Please, if you know someone continue my reports similarly as Iyears, who knows Duchenne and Duchenne research, who can write in English and some other languages, and knows or likes to know the scientists and likes to talk to them, who has a lot of time to do all this and, most important, does not need any financial help, please ask her or him to write to me. But until I have found one, I will probably write short reports once in a while if something important happens, just update this report, and I will continue to answer all emails which reach me from everywhere in the world with often desperate questions about this terrible disease and what can be done against it. So, I am thanking all who have helped me writing the reports, especially Annemieke Aartsmavan Ommen of Leiden University, PPMD, Kate Bushby of TREATscientists whose work I have described and who made sure that I made not many mistakes.
Li D, Yue Y, Duan D. Marginal level dystrophin ex-pression improves clinical outcome in a strain of dystro-phin/utrophin double knockout mice. PLoS One 2010; 5;
van Ommen GJ, van Deutekom JT, Aartsma-Rus A. mediated exon skip-
-149.
Sarepta Therapeutics Announces Significant Clinical Benefit With Eteplirsen After 36 Weeks in Phase IIb Study for the Treatment of Duchenne Muscular Dystrophy. News
Release, 24 July 2012. (4) Aartsma-Rus A, van Deutekom JCT, van Ommen GJB, den Dunnen JT. Entries in the Leiden Duchenne muscular dystrophy mutation database: An overview of mutation types and paradoxical cases that conform the readingframe rule. Muscle & Nerve 2006; 34; 135 (5) Aartsma-Rus A, et al. and van Deutekom J, van Ommen G-J, den Dunnen JT. antisense-mediated exon skipping for Duchenne muscular dystrophy mutations; Human Mutation 2009; 30; 293
22
information. And let me say again that you should register your child or yourself in a DMD data bank as soon as possible and that you please confirm in writing by e-mail
cular dystrophy of your son. I have tried to find such a person, however with no success so far.
Please, if you know someone who would be able to reports similarly as I have done it for 12
, who knows Duchenne and Duchenne research, who can write in English and some other languages, and knows or likes to know the scientists and likes to talk to them, who has a lot of time to do all this and, most important,
need any financial help, please ask her or him to
But until I have found one, I will probably write short reports once in a while if something important happens, or
and I will continue to answer all e-h reach me from everywhere in the world with
tions about this terrible disease and
So, I am thanking all who have helped me writing the Annemieke Aartsma-Rus and Gertjan
of Leiden University, Pat Furlong of of TREAT-NMD, and the many
tists whose work I have described and who made sure that I made not many mistakes. Good-bye to all of you!
Guenter Scheuerbrandt, PhD. Breitnau, Germany
online.de, information.eu
Rus A, van Deutekom JCT, van Ommen GJB, Entries in the Leiden Duchenne muscular
dystrophy mutation database: An overview of mutation paradoxical cases that conform the reading-
Muscle & Nerve 2006; 34; 135-144.
Rus A, et al. and van Deutekom J, van J, den Dunnen JT. Theoretic applicability of
mediated exon skipping for Duchenne muscular dystrophy mutations; Human Mutation 2009; 30; 293-299.
23
(6) Van Deutekom JC, et al. and van Ommen GJB. Local dystrophin restoration with antisense oligonucleotide PRO051. N Engl J Med 2007; 357; 2677-86. Hoffman, EP. Skipping toward personalized molecular medicine. N Engl J Med 2007; 357; 2719-22. (7) Goemans NM, Tulinius M, et al. and van Deutekom JC. Systemic administration of PRO051 in Duchenne’s muscular dystrophy. N Enbg J Med 2011; 364; 1513-22. (8) Kinali M, Arechavala-Gomeza V, et al. and Bushby K and Muntoni F. Local restoration of dystrophin expression with the morpholino oligomer AVI-4658 in Duchenne muscular dystrophy: a single-blind, placebo-controlled, dose-escalation, proof-of-concept study. The Lancet Neu-rology 2009; 8; 918-928. (9) Cirak S, Arechavala-Gomeza V, et al. and Bushby K, Muntoni F. Exon skipping and dystrophin restoration in patients with Duchenne muscular dystrophy after systemic phosphorodiamidate morpholino oligomer treatment: an open-label, phase 2, dose escalation study. Lancet 2011; 378; 595-605. (10) Sarepta Therapeutics announces a continued benefit on walking test through 62 weeks in phase IIb open-label extension study of Eteplirsen in Duchenne muscular dys-trophy. News Release, 7 December 2012. (11) Mendell JR, et al. and Weiss RB. Evidence-based path to newborn screening for Duchenne muscular dystro-phy. Ann Neurol 2012; 71; 304-313. (12) Scheuerbrandt G, Lundin A, Lövgren T, Mortier W. Screening for Duchenne muscular dystrophy: An improved screening test for creatine kinase and its application in an infant screening program. Muscle & Nerve, 1986; 9;11-23. (13) Goyenvalle, A, et al. and García L: Rescue of dys-trophic muscle through U7 snRNA-mediated exon skip-ping. Science, 2004, 306, 1796-1799. (14) Vulin A, et al, and Goyenvalle A, García L: Muscular function recovery in golden retriever muscular dystrophy after AAV1-U7 exon skipping, Molecular Therapy, 2012, 20, 2120-2133.
(15) Goyenvalle A, et al. and García L, Davies K.E.: Res-cue of severely affected dystrophin/utrophin-deficient mice through scAAV-U7snRNA-mediated exon skipping, Hum. Mol. Genetics, 2012, 21, 2559-2571. (16) Goyenvalle A, et al. and Garcia L, Davies KE. “Engi-neering multiple U7snRNA constructs to induce single and multiexon-skipping for Duchenne muscular dystrophy”. Mol Ther 2012; 20;1212-21. (17) Béroud C, Matsuo M, et al. Multiexon skipping lead-ing to an artificial DMD protein lacking amino acids from exons 45 through 55 could rescue up to 63% of patients with Duchenne muscular dystrophy. Human Mutation 2007; 28; 196-202. (18) Van Vliet L, et al. and van Deutekom JCT, van Om-men G-JB, Aartsma-Rus A. Assessment of the feasibility of exon 45-55 multiexon skipping for Duchenne muscular dystrophy. BMC Medical Genetics 2008; 9; 105 (19) Yokota T, Lu QL, Partridge T, Kobayashi M, Naka-mura A, Takeda S, and Hoffman E. Efficacy of systemic morpholino exon-skipping in Duchenne dystrophy dogs. Annals of Neurology 2009; 65; 667-676. (20) Wu B, et al., and Lu QL. Octa-guanidine morpholino restores dystrophin expression in cardiac and skeletal mus-cles and ameliorates pathology in dystrophic mdx mice. Molecular Therapy 2009; 17; 864-71. (21) Yokota T, et al., and Partridge T, Hoffman EP, Ta-keda S. Extensive and prolonged restoration of dystrophin expression with vivo-morpholino-mediated multiple exon skipping in dystrophic dogs. Nucleic Acid Ther. 2012; 22;306-15. (22) Yoshitsugu A, Yokata T, et al. and Hoffman EP, Par-tridge T, Takeda S. Bodywide skipping of exons 45-55 in dystrophic mdx52mice by systemic antisense delivery. Proc Natl Acad Sci 2012;109;13763-8.