Research Program Overview Ruth Brannon, MSPH, MA Associate Director, Division of Research Sciences National Institute on Disability and Rehabilitation Research Office of Special Education and Rehabilitative Research U.S. Department of Education www.ed.go v/about / offices/ list/ osers/nid rr NIDRR
Transcript
Research Program Overview
Research Program OverviewRuth Brannon, MSPH, MAAssociate Director, Division of Research SciencesNational Institute on Disability and Rehabilitation ResearchOffice of Special Education and Rehabilitative ResearchU.S. Department of Education
Ruth Brannon, MSPH, MAAssociate Director, Division of Research SciencesNational Institute on Disability and Rehabilitation ResearchOffice of Special Education and Rehabilitative ResearchU.S. Department of Education
www.e
d.go
v/ab
out/o
ffice
s/lis
t/ose
rs/
nidr
r
www.e
d.go
v/ab
out/o
ffice
s/lis
t/ose
rs/
nidr
r
NIDRRNIDRR
Organization DetailsOrganization Details
• Office of Special Education and Rehabilitative Services (OSERS) includes:– Rehabilitation Services Administration (RSA)
– Office of Special Education Programs (OSEP)
– National Institute on Disability and Rehabilitation Research (NIDRR)
• Legislative Authority:– Title II, Rehabilitation Act, as amended
– Assistive Technology Act of 1998
• Office of Special Education and Rehabilitative Services (OSERS) includes:– Rehabilitation Services Administration (RSA)
– Office of Special Education Programs (OSEP)
– National Institute on Disability and Rehabilitation Research (NIDRR)
• Legislative Authority:– Title II, Rehabilitation Act, as amended
– Assistive Technology Act of 1998
NIDRR’s Statutory ChargeNIDRR’s Statutory Charge
To support research to maximize the self-sufficiency individuals with disabilities of all ages
To support research to maximize the self-sufficiency individuals with disabilities of all ages
Domains of NIDRR ResearchDomains of NIDRR ResearchFocus on the WHOLE PERSON
Interacting with SOCIETY
And the ENVIRONMENT
Focus on the WHOLE PERSON
Interacting with SOCIETY
And the ENVIRONMENT
Values That Drive Disability and Rehabilitation Research at NIDRR
Interventions Technology Data Training Int'national
Mil
lio
ns
Funding Amt.
0
1
2
3
4
5
6
7
ModelSystems
Interventions Technology Data Training Int'national
Mil
lio
ns
Funding Amt.
The Traumatic Brain Injury Model Systems of Care
The Traumatic Brain Injury Model Systems of Care
A project funded by the
National Institute on Disability and Rehabilitation ResearchOffice of Special Education and Rehabilitative Services
United States Department of Education
Current Traumatic Brain Injury Model Systems
Current Traumatic Brain Injury Model Systems
Centers and Key Personnel (cont.)Centers and Key Personnel (cont.)• University of Alabama - Birmingham, AL - Thomas Novack , Ph.D.
• Santa Clara Valley Medical Center - San Jose, CA - Tamara Bushnik, Ph.D.
• Craig Hospital - Englewood, CO - Gale Whiteneck, Ph.D.
• The Spaulding Rehabilitation Hospital - Boston, MA - Mel Glenn, M.D.
• Rehabilitation Institute of Michigan/Wayne State University - Detroit, MI - Robin Hanks, Ph.D.
• Mayo Foundation - Rochester, MN - James Malec, Ph.D.
• Mississippi Methodist Rehabilitation Center - Jackson, MS - Mark Sherer, Ph.D.
• University of Alabama - Birmingham, AL - Thomas Novack , Ph.D.
• Santa Clara Valley Medical Center - San Jose, CA - Tamara Bushnik, Ph.D.
• Craig Hospital - Englewood, CO - Gale Whiteneck, Ph.D.
• The Spaulding Rehabilitation Hospital - Boston, MA - Mel Glenn, M.D.
• Rehabilitation Institute of Michigan/Wayne State University - Detroit, MI - Robin Hanks, Ph.D.
• Mayo Foundation - Rochester, MN - James Malec, Ph.D.
• Mississippi Methodist Rehabilitation Center - Jackson, MS - Mark Sherer, Ph.D.
Centers and Key Personnel (cont.)Centers and Key Personnel (cont.)• JFK - Johnson Rehabilitation Institute - Edison, NJ - Keith Cicerone, Ph.D.
• Mount Sinai School of Medicine - New York, NY - Wayne Gordon, Ph.D.
• Charlotte Institute of Rehabilitation/Carolinas HealthCare System - Charlotte, NC - Flora Hammond, M.D.
• The Ohio State University - Columbus, OH - John Corrigan, Ph.D.
• Moss Rehabilitation Research Institute - Philadelphia, PA - Tessa Hart, Ph.D.
• U. of Pittsburgh Medical Center - Pittsburgh, PA - Ross Zafonte, D.O.
• U. of Texas Southwestern Medical Center - Dallas, TX - Ramon Diaz-Arrastia, M.D., Ph.D.
• Medical College of Virginia - Richmond, VA - Jeffrey Kreutzer, Ph.D.
• University of Washington - Seattle, WA - Kathleen Bell, M.D.
• JFK - Johnson Rehabilitation Institute - Edison, NJ - Keith Cicerone, Ph.D.
• Mount Sinai School of Medicine - New York, NY - Wayne Gordon, Ph.D.
• Charlotte Institute of Rehabilitation/Carolinas HealthCare System - Charlotte, NC - Flora Hammond, M.D.
• The Ohio State University - Columbus, OH - John Corrigan, Ph.D.
• Moss Rehabilitation Research Institute - Philadelphia, PA - Tessa Hart, Ph.D.
• U. of Pittsburgh Medical Center - Pittsburgh, PA - Ross Zafonte, D.O.
• U. of Texas Southwestern Medical Center - Dallas, TX - Ramon Diaz-Arrastia, M.D., Ph.D.
• Medical College of Virginia - Richmond, VA - Jeffrey Kreutzer, Ph.D.
• University of Washington - Seattle, WA - Kathleen Bell, M.D.
Design and DefinitionDesign and Definition
• The first prospective, longitudinal multi-center study conducted to examine the course of recovery and outcomes following the delivery of a coordinated system of acute neurotrauma and inpatient rehabilitation.
• Includes large scale follow-up to 13 years post-injury.
• The first prospective, longitudinal multi-center study conducted to examine the course of recovery and outcomes following the delivery of a coordinated system of acute neurotrauma and inpatient rehabilitation.
• Includes large scale follow-up to 13 years post-injury.
Project ObjectivesProject Objectives
• Demonstrate and evaluate cost-benefit and service delivery outcomes of comprehensive delivery system.
• Demonstrate and evaluate development and application of improved and innovative methods essential to care and rehabilitation of individuals with TBI.
• Participate in multi-center studies of the Brain Injury Model System concept by contributing to a national database.
• Demonstrate and evaluate cost-benefit and service delivery outcomes of comprehensive delivery system.
• Demonstrate and evaluate development and application of improved and innovative methods essential to care and rehabilitation of individuals with TBI.
• Participate in multi-center studies of the Brain Injury Model System concept by contributing to a national database.
Key ComponentsKey Components
1. Comprehensive continuum of services from acute care through community integration
2. Accessibility of care
3. Coordination of services
4. Patient volume
5. Clinical research and evaluation
6. Strong linkages with acute and post-acute personnel
1. Comprehensive continuum of services from acute care through community integration
2. Accessibility of care
3. Coordination of services
4. Patient volume
5. Clinical research and evaluation
6. Strong linkages with acute and post-acute personnel
Key Clinical ComponentsKey Clinical Components
1. Emergency medical services - Level I Trauma Center(s)
4. Long-term interdisciplinary follow-up and rehabilitation services.
Definition of TBIDefinition of TBI
• The individual has sustained a TBI external mechanical force causing damage to brain tissue, as evidenced by any of the following:– loss of consciousness
– post-traumatic amnesia (PTA)
– objective neurological findings
– skull fracture
* based on Centers for Disease Control definition
• The individual has sustained a TBI external mechanical force causing damage to brain tissue, as evidenced by any of the following:– loss of consciousness
– post-traumatic amnesia (PTA)
– objective neurological findings
– skull fracture
* based on Centers for Disease Control definition
TBI Model Systems National Database - NIDRR 2/2000 / Thurman DJ, Sniezek JE, Johnson D, Greenspan A. Guidelines for Surveillance of Central Nervous System Injury. National Center for Injury Prevention and Control, Centers for Disease Control and Prevention: Atlanta, GA; 1995.
VII. Measure and Predict Outcome at Follow-upVII. Measure and Predict Outcome at Follow-up
Handicap (cont.):
• Drug use
• Alcohol use (NHSDA/BRFSS)
• Transportation
• Income and source
Handicap (cont.):
• Drug use
• Alcohol use (NHSDA/BRFSS)
• Transportation
• Income and source
VII. Measure and Predict Outcome at Follow-upVII. Measure and Predict Outcome at Follow-up
Handicap (cont.):
• Arrests
• Psychiatric problems
• Satisfaction with Life Scale (SWLS)
Handicap (cont.):
• Arrests
• Psychiatric problems
• Satisfaction with Life Scale (SWLS)
Sources of DataSources of Data
• Abstract from medical records
• Pre-existing database
• Specialized data collection forms
• Patient examination/interview/testing
• Family interview
• Abstract from medical records
• Pre-existing database
• Specialized data collection forms
• Patient examination/interview/testing
• Family interview
External DisseminationExternal Dissemination
TBI Model Systems Website
TBIMS.ORG
Age At InjuryAge At Injury
n =3279
Mean = 37 years
GenderGender
n = 3278
RaceRace
Other12%
African American
27%
Caucasian61%
Other12%
African American
27%
Caucasian61%
n = 3278
Marital Status At InjuryMarital Status At Injury
n = 3274
Level of Education At InjuryLevel of Education At Injury
< H.S. 40%
HS Diploma
31 %
Some College
17%
College Degree
12%
< H.S. 40%
HS Diploma
31 %
Some College
17%
College Degree
12%
n = 3080
Employment Status At InjuryEmployment Status At Injury
Employed60%
Student11%
Unemployed18%
Retired/homemaker/other11%
Mgr/prof
Tech/sales
Service
Prod/craft
Oper/fabr/labor
12%
26%
17%
27%
Occupational Category
Other6%
12%
N=3279N=3279
Comparison of Demographic CharacteristicsComparison of Demographic Characteristics
Data Source
Mean Age at Injury % Male % White
% Never Married at
injury
% Employed at Injury
% Not Completed
High School at
Injury
TBI Model Systems
37 75 61 50 60 40
Traumatic Coma Data
Bank30 77 81 44 52 49
SCI Model Systems
32 82 67 54 64 38
SummarySummary
Demographic Characteristics of the Population• Average age = 37
• Male (75%)
• Large minority population (39%)
• Not married at injury (70%)
• High school education or less (71%)
• 60% employed at injury
• Most substantial difference in demographic characteristics between studies is race
Demographic Characteristics of the Population• Average age = 37
• Male (75%)
• Large minority population (39%)
• Not married at injury (70%)
• High school education or less (71%)
• 60% employed at injury
• Most substantial difference in demographic characteristics between studies is race
Etiology of InjuryEtiology of Injury
n = 3258
Falls15%
Other11%
Assault19%
Vehicular55%
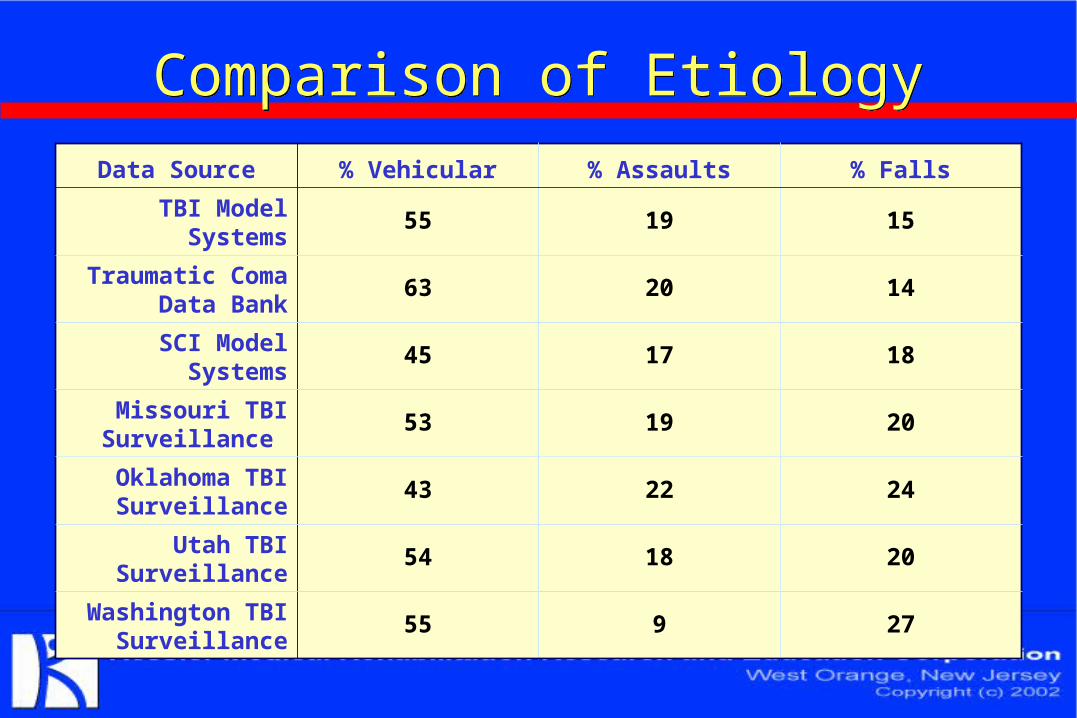
Comparison of EtiologyComparison of Etiology
Data Source % Vehicular % Assaults % Falls
TBI Model Systems 55 19 15
Traumatic Coma Data Bank
63 20 14
SCI Model Systems 45 17 18
Missouri TBI Surveillance
53 19 20
Oklahoma TBI Surveillance
43 22 24
Utah TBI Surveillance
54 18 20
Washington TBI Surveillance
55 9 27
Blood Alcohol LevelBlood Alcohol Level
n = 3053n = 3053
At Emergency Department Admission* At Emergency Department Admission*
* excluded cases not
tested = 7%
* excluded cases not
tested = 7%
Negative43%
<100 mg/dl2%
=>100mg/dl55%
SummarySummary
Causes of Injury:
• Primary cause is vehicular (55%), followed by assaults (19%) and falls (15%)
• The % of vehicle-related injuries is similar to other studies; the % of assaults is higher, and the % of falls is lower
• High incidence of alcohol-related injuries (57%)
Causes of Injury:
• Primary cause is vehicular (55%), followed by assaults (19%) and falls (15%)
• The % of vehicle-related injuries is similar to other studies; the % of assaults is higher, and the % of falls is lower
• High incidence of alcohol-related injuries (57%)
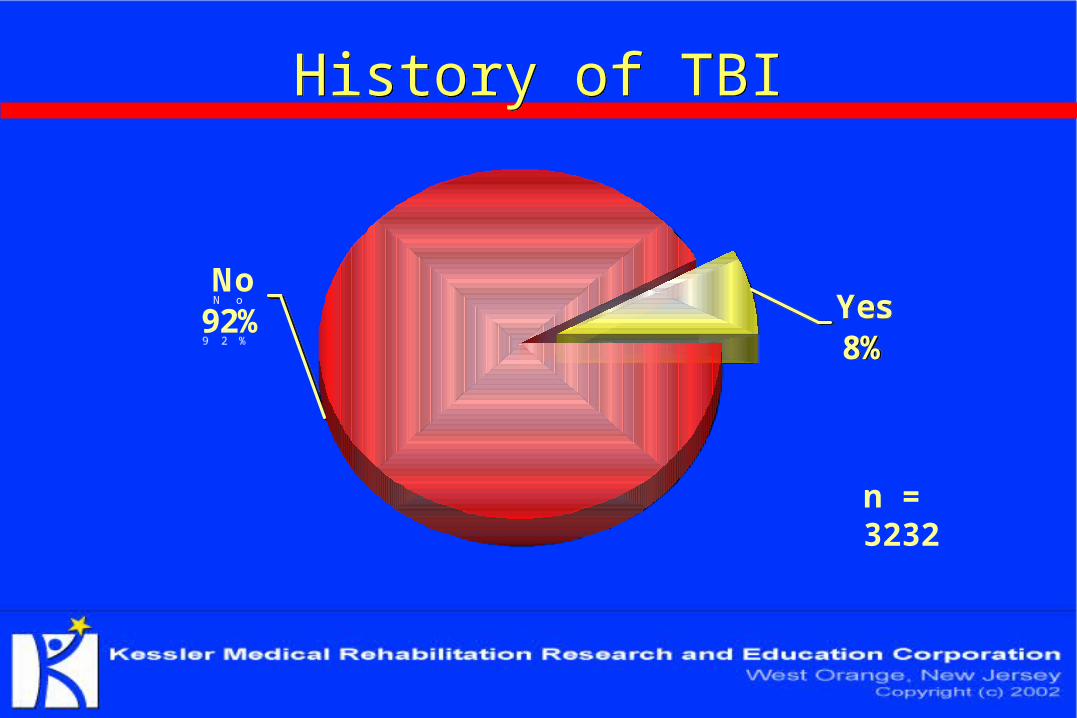
History of TBIHistory of TBI
Yes8%
No92% Yes
8%
No92%
n = 3232
Associated InjuriesAssociated Injuries
75%
17%
17%
14%
4%
2%
2%
1%
0% 10% 20% 30% 40% 50% 60% 70% 80%
Amputation
Brachial Plexus
Peripheral Nerve
Spinal Cord
Intra-abdominal
Pneumo/hemothorax
Cranial Nerve
Fracture
Percentage of Patients
75%
17%
17%
14%
4%
2%
2%
1%
0% 10% 20% 30% 40% 50% 60% 70% 80%
Amputation
Brachial Plexus
Peripheral Nerve
Spinal Cord
Intra-abdominal
Pneumo/hemothorax
Cranial Nerve
Fracture
Percentage of Patients
SummarySummary
Severity of Injury:
• Few have previous TBI (8%)
• Majority have severe TBI (66%)
• Majority experience LOC (97%) with an average duration of 3.8 days
• Most experience PTA (97%)
• The majority have at least one bone fracture (75%)
Severity of Injury:
• Few have previous TBI (8%)
• Majority have severe TBI (66%)
• Majority experience LOC (97%) with an average duration of 3.8 days
• Most experience PTA (97%)
• The majority have at least one bone fracture (75%)
SummarySummary
Costs of Treatment:
• Average charge is $5,169 per day for acute care and $1,455 per day for inpatient rehabilitation
• LOS decreased 28% for acute care and 29% for inpatient rehabilitation (1993-2002)
• 38% have government-sponsored care (Medicaid/Medicare) which is higher than that for the general population (26%)
Costs of Treatment:
• Average charge is $5,169 per day for acute care and $1,455 per day for inpatient rehabilitation
• LOS decreased 28% for acute care and 29% for inpatient rehabilitation (1993-2002)
• 38% have government-sponsored care (Medicaid/Medicare) which is higher than that for the general population (26%)
SummarySummary
Disability Outcomes:
• DRS indicates improvement in level of disability from SEVERE DISABILITY at rehab. admission to PARTIAL DISABILITY at 1 and 2 yrs. post-injury
• FIM indicates improvement in functional ability from level requiring MODERATE ASSISTANCE at rehab. admission to MODIFIED INDEPENDENCE at 1 and 2 yrs. post-injury
Disability Outcomes:
• DRS indicates improvement in level of disability from SEVERE DISABILITY at rehab. admission to PARTIAL DISABILITY at 1 and 2 yrs. post-injury
• FIM indicates improvement in functional ability from level requiring MODERATE ASSISTANCE at rehab. admission to MODIFIED INDEPENDENCE at 1 and 2 yrs. post-injury
SummarySummary
Disability Outcomes (cont.):
• Most improvement in level of disability and functional ability occurs during inpatient rehabilitation
• Continued improvement is seen at 1 yr. post-injury
• Level of disability and functional ability appear to plateau between 1 and 2 yrs. post-injury
Disability Outcomes (cont.):
• Most improvement in level of disability and functional ability occurs during inpatient rehabilitation
• Continued improvement is seen at 1 yr. post-injury
• Level of disability and functional ability appear to plateau between 1 and 2 yrs. post-injury
SummarySummary
Handicap Outcomes:
• Most live in a private residence following rehab. discharge (85%)
• Few live alone at rehab. discharge (3%), with the highest proportion living with parent(s) (38%), or other relatives, friends or caregivers (35%)
• 28% are employed at 1 yr. post-injury (60%employed at injury)
Handicap Outcomes:
• Most live in a private residence following rehab. discharge (85%)
• Few live alone at rehab. discharge (3%), with the highest proportion living with parent(s) (38%), or other relatives, friends or caregivers (35%)
• 28% are employed at 1 yr. post-injury (60%employed at injury)
ConclusionsConclusions
Large Minority Population:
• % violence-related injuries is higher than other studies
• Majority have severe TBI
• Rehab. length of stay deceased 28% in the past ninth yrs.
• Functional ability improves from a level requiring MODERATE ASSISTANCE at rehab. admission to MODIFIED INDEPENDENCE at 1 and 2 yrs. post-injury
Large Minority Population:
• % violence-related injuries is higher than other studies
• Majority have severe TBI
• Rehab. length of stay deceased 28% in the past ninth yrs.
• Functional ability improves from a level requiring MODERATE ASSISTANCE at rehab. admission to MODIFIED INDEPENDENCE at 1 and 2 yrs. post-injury
Conclusions (cont.)Conclusions (cont.)
• Functional ability improves most during rehab.; continued improvement at 1 yr. post-injury; plateau between 1 and 2 yrs. post-injury
• Most return to private residences at rehab. discharge with few living alone
• Less community integration than persons without TBI
• Functional ability improves most during rehab.; continued improvement at 1 yr. post-injury; plateau between 1 and 2 yrs. post-injury
• Most return to private residences at rehab. discharge with few living alone
• Less community integration than persons without TBI
Accessible NIDRR Web Pages Accessible NIDRR Web Pages
NIDRR Home page:
www.ed.gov/offices/OSERS/NIDRR
National Center for the Dissemination of Disability Research Home page:
www.ncddr.org
National Rehabilitation Information Center Home page:
www.naric.com/naric
NIDRR Home page:
www.ed.gov/offices/OSERS/NIDRR
National Center for the Dissemination of Disability Research Home page:
www.ncddr.org
National Rehabilitation Information Center Home page:
www.naric.com/naric
For additional informationFor additional information