Respiratory System Melissa Gonzales McNeal 1 1 Respiratory System Respiration - Definition The exchange of oxygen and carbon dioxide between the atmosphere and the cells of an organism External respiration: exchange of gases between atmosphere and blood Internal respiration: exchange of gases between blood and interstitial fluid The utilization of oxygen in the mitochondria of cells for the production of energy (ATP) Cellular respiration 2 Functions of Respiratory System 3 Moves air to and from the exchange surfaces of the lungs Provides extensive area for gas exchange between air and circulating blood Protects and conditions respiratory surfaces Produces sounds Senses odors Assists in regulation of Blood volume and pressure Angiotensin I to angiotensin II pH balance (CO 2 ) Pressure gradients between thorax and abdomen promoting lymph and venous blood flow Filters blood clots Valsava maneuver helps expel abdominal contents during urination, defecation, and childbirth THE TOTAL SURFACE AREA OF THE LUNG IS ABOUT 80 METERS SQUARE ~ ABOUT THE SIZE OF A TENNIS COURT 4 Respiratory Anatomy
Transcript
Respiratory System
Melissa Gonzales McNeal 1
1
Respiratory System
Respiration - Definition
The exchange of oxygen and carbon dioxide between the atmosphere and the cells of an organism
External respiration: exchange of gases between atmosphere and blood
Internal respiration: exchange of gases between blood and interstitial fluid
The utilization of oxygen in the mitochondria of cells for the production of energy (ATP)
Cellular respiration
2
Functions of Respiratory System
3
Moves air to and from the exchange surfaces of the lungs Provides extensive area for gas exchange between air and
circulating blood
Protects and conditions respiratory surfaces
Produces sounds
Senses odors
Assists in regulation of Blood volume and pressure
Angiotensin I to angiotensin II
pH balance (CO2)
Pressure gradients between thorax and abdomen promoting lymph and venous blood flow
Filters blood clots
Valsava maneuver helps expel abdominal contents during urination, defecation, and childbirth
T H E T O TAL S U R FAC E A R E A O F T H E L U N G I S A B OUT 8 0 M E TE RS S Q U A RE
a. Alveolar (intrapulmonary) pressure: inside alveoli
b. Intrapleural pressure: inside pleural cavity
4. Compliance of lungs
5. Clinical applications
79
Forces that keep lungs against the cavity walls
80
1. Pressure difference
a. Intrapleural pressure is less than alveolar pressure
2. Surface tension
a. Present in pleural cavity
b. Decreased due to surfactant in alveoli
Respiratory System
Melissa Gonzales McNeal 21
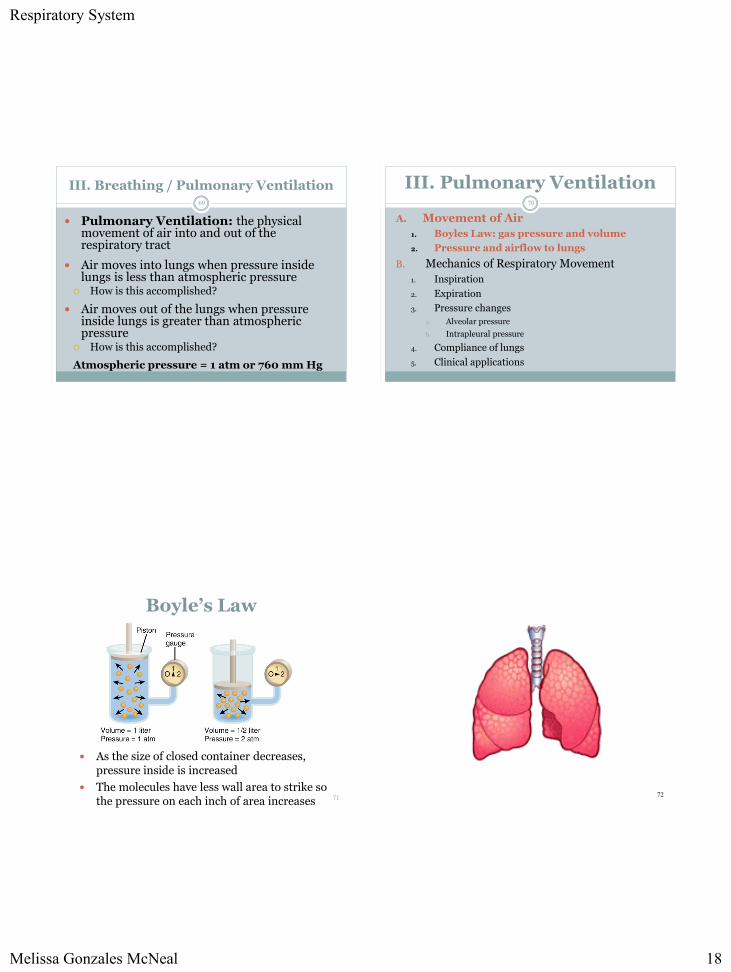
III. Pulmonary Ventilation81
A. Movement of Air
1. Boyles Law: gas pressure and volume
2. Pressure and airflow to lungs
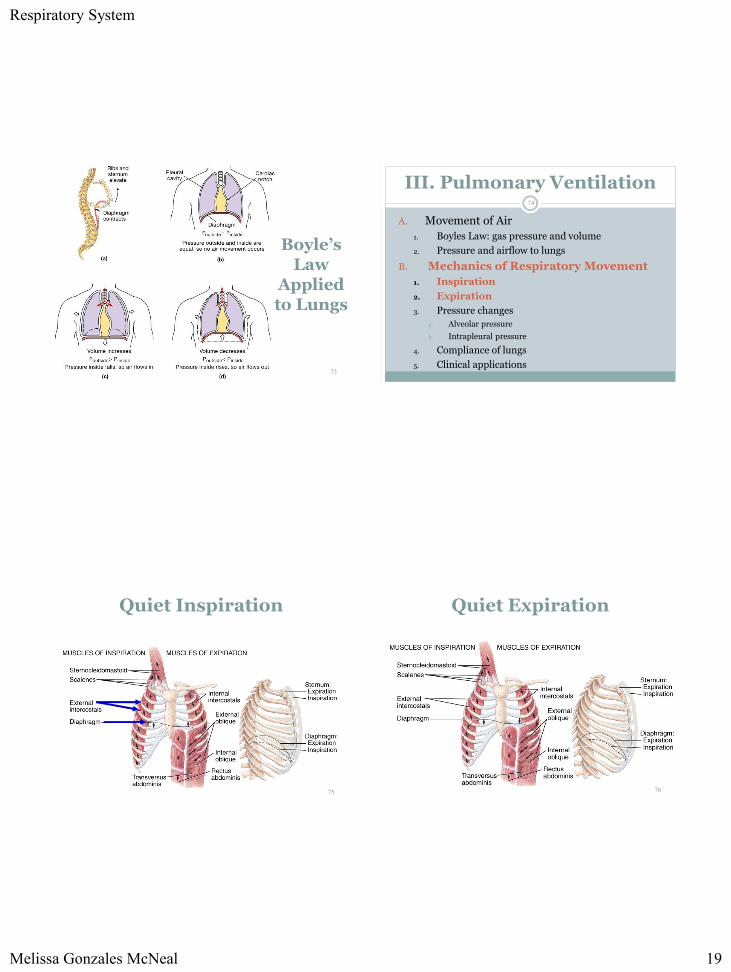
B. Mechanics of Respiratory Movement
1. Inspiration
2. Expiration
3. Pressure changes
a. Alveolar pressure
b. Intrapleural pressure
4. Compliance of lungs
5. Clinical applications
Compliance of the Lungs
Ease with which lungs & chest wall expand
Elasticity of lungs Surface tension
Some diseases reduce compliance Scar tissue Tuberculosis Rheumatoid arthritis
Pulmonary edema --- fluid in lungs & reduced surfactant
Pneumonia Paralysis
82
III. Pulmonary Ventilation83
A. Movement of Air
1. Boyles Law: gas pressure and volume
2. Pressure and airflow to lungs
B. Mechanics of Respiratory Movement
1. Inspiration
2. Expiration
3. Pressure changes
a. Alveolar pressure
b. Intrapleural pressure
4. Compliance of lungs
5. Clinical applications
Pneumothorax
Pleural cavities are sealed cavities not open to the outside
Injuries to the chest wall that let air enter the intrapleuralspace
Causes a pneumothorax
Collapsed lung on same side as injury
Surface tension and recoil of elastic fibers causes the lung to collapse 84
Respiratory System
Melissa Gonzales McNeal 22
III. Pulmonary Ventilation85
C. Respiratory volumes and rates
1. Volumes and capacities
a. Tidal Volume
b. Inspiratory/expiratory capacity
c. Inspiratory/expiratory reserve volume
d. Vital capacity
e. Residual volume
f. Functional residual capacity
g. Total lung capacity
2. Rates
a. Respiratory rate
b. Respiratory minute volume
3. Alveolar ventilation and anatomic dead space
Lung Volumes and Capacities
EXPIRATORY
CAPACITY
1,700 mL
86
III. Pulmonary Ventilation87
C. Respiratory volumes and rates1. Volumes and capacities
a. Tidal Volume (TV)
b. Inspiratory capacity (IC)
c. Inspiratory reserve volume (IRV)
d. Vital capacity (VC)
e. Residual volume (RV)
f. Functional residual capacity (FRV)
g. Total lung capacity (TLC)
h. Expiratory capacity (EC)
i. Expiratory reserve volume (ERV)
2. Rates
a. Respiratory rate
b. Respiratory minute volume
3. Alveolar ventilation and anatomic dead space
Respiratory Rates and Volumes
Tidal volume (VT): amount air moved during quiet breathing
Respiratory rate (ƒ): number of breaths per minute
Respiratory minute volume (VE)
VE = ƒ X VT
88
Respiratory System
Melissa Gonzales McNeal 23
89
If your tidal volume is 475 ml per breath and your respiratory rate is 12 breaths per minute, what is your Respiratory Minute Volume?
VE = ƒ X VT
= 12 breaths/minute X 475 ml/breaths
= 5700 ml/minute
Alveolar Ventilation (VA): amount of air reaching alveoli each minute
VA = ƒ x (VT – VD)
Anatomic dead space (VD): volume of air in the conducting passages
90
91
If your respiratory rate is 12 breaths per minute, your tidal volume is 475 ml per breath, and your anatomical dead space is 150 ml, what is the amount of air reaching your alveoli each minute (Alveolar Ventilation)?
VA = ƒ x (VT – VD)
= 12 breaths/minute X (475 ml/breath – 150 ml)
= 3900 ml
Conducting Zone
Respiratory Zone
Total Lung Capacity: 5,000 mls
~ 150 mls
~ 4,850 mls
Tidal Volume: 500 ml
150 mls 350 mls
Atmosphere
Air in the RoomAlveoli
150 mls350 mls
Respiratory System
Melissa Gonzales McNeal 24
Conducting Zone
Respiratory Zone
Total Lung Capacity: 5,000 mls
~ 150 mls
~ 4,850 mls
Tidal Volume: 75 ml
75 mls
Alveoli
75 mlsAtmosphere
Air in the Room
What happens if the tidal volume drops lower
than the conducting zone volume?
PART 4
GAS EXCHANGE
94
Respiratory Physiology
IV. Gas Exchange95
A. The Gas Laws
B. Diffusion and Respiratory Function
C. Gas Pickup and Delivery
IV. Gas Exchange96
A. The Gas Laws
1. Dalton’s Law: partial pressures
2. Henry’s Law: diffusion between liquids and gases
a. Hyperbaric oxygenation
B. Diffusion and Respiratory Function
C. Gas Pickup and Delivery
Respiratory System
Melissa Gonzales McNeal 25
Dalton’s Law
Each gas in a mixture of gases exerts its own pressure
As if all other gases were not present
Partial pressures denoted as p
Total pressure is sum of all partial pressures
Atmospheric pressure
(760 mm Hg) = pO2 + pCO2 + pN2 + pH2O
To determine partial pressure of O2-- multiply 760 by % of air that is O2 (21%) = 160 mm Hg
97
What is Composition of Air?
Air = 21% O2, 79% N2 and .04% CO2
Alveolar air = 14% O2, 79% N2 and 5.2% CO2
Expired air = 16% O2, 79% N2 and 4.5% CO2
Observations alveolar air has less O2 since absorbed by blood
Mystery??? expired air has more O2 & less CO2 than alveolar air?
98
Henry’s Law
Quantity of a gas that will dissolve in a liquid depends upon the amount of gas present and its solubility coefficient
explains why you can breathe compressed air while scuba diving despite 79% Nitrogen
N2 has very low solubility unlike CO2 (soda cans)
dive deep & increased pressure forces more N2 to dissolve in the blood (nitrogen narcosis)
decompression sickness if come back to surface too fast or stay deep too long
Breathing O2 under pressure dissolves more O2 in blood 99
Hyperbaric Oxygenation
Clinical application of Henry’s law
Use of pressure to dissolve more O2 in the blood
treatment for patients with anaerobic bacterial infections (tetanus and gangrene)
anaerobic bacteria die in the presence of O2
Hyperbaric chamber pressure raised to 3 to 4 atmospheres so that tissues absorb more O2
Used to treat heart disorders, carbon monoxide poisoning, cerebral edema, bone infections, gas embolisms & crush injuries
100
Respiratory System
Melissa Gonzales McNeal 26
101
102
IV. Gas Exchange103
A. The Gas Laws
B. Diffusion and Respiratory Function
1. External Respiration
2. Internal Respiration
3. Efficiency of diffusion
C. Gas Pickup and Delivery
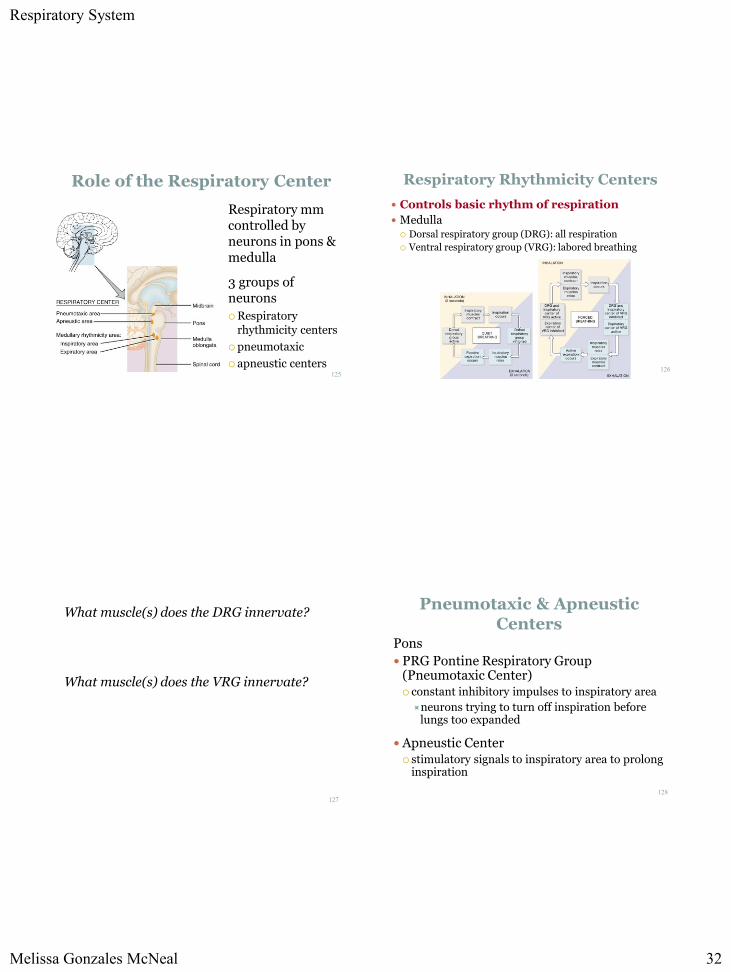
External Respiration
Diffusion Across Respiratory Membrane
Gases diffuse from areas of high partial pressure to areas of low partial pressure
Deoxygenated blood becomes saturated
104
Respiratory System
Melissa Gonzales McNeal 27
Internal Respiration
Exchange of gases between blood & tissues
Conversion of oxygenated blood into deoxygenated
Diffusion of O2 inward at rest 25% of available O2
enters cells
during exercise more O2 is absorbed
Diffusion of CO2 outward105
Efficiency of Diffusion
Depends upon partial pressure of gases in air pO2 at sea level is 160 mm Hg
10,000 feet is 110 mm Hg / 50,000 feet is 18 mm Hg