108
Respiratory System Respiratory System Pathology 91 Pathology 91 Spring 2012 Spring 2012
| Date post: | 02-Jan-2016 |
| Category: |
Documents |
| Upload: | buck-lester |
| View: | 231 times |
| Download: | 1 times |

Respiratory SystemRespiratory System
Pathology 91Pathology 91Spring 2012Spring 2012
22
Respiratory System AnatomyRespiratory System Anatomy1.1. Divided into:Divided into:
1.1. Upper respiratory tractUpper respiratory tract2.2. Lower respiratory tractLower respiratory tract
2.2. Thoracic cavityThoracic cavity1.1. RT & LT pleural cavitiesRT & LT pleural cavities2.2. MediastinumMediastinum3.3. Lined by parietal pleuraLined by parietal pleura
3.3. Visceral pleura Visceral pleura adheresadheres to the lung tissue to the lung tissue4.4. Bones of thorax assist in iBones of thorax assist in inspirationnspiration & & expirationexpiration5.5. Sinuses Sinuses
1.1. are lined with respiratory epithelium are lined with respiratory epithelium 2.2. communicate with visceral cavitiescommunicate with visceral cavities
33
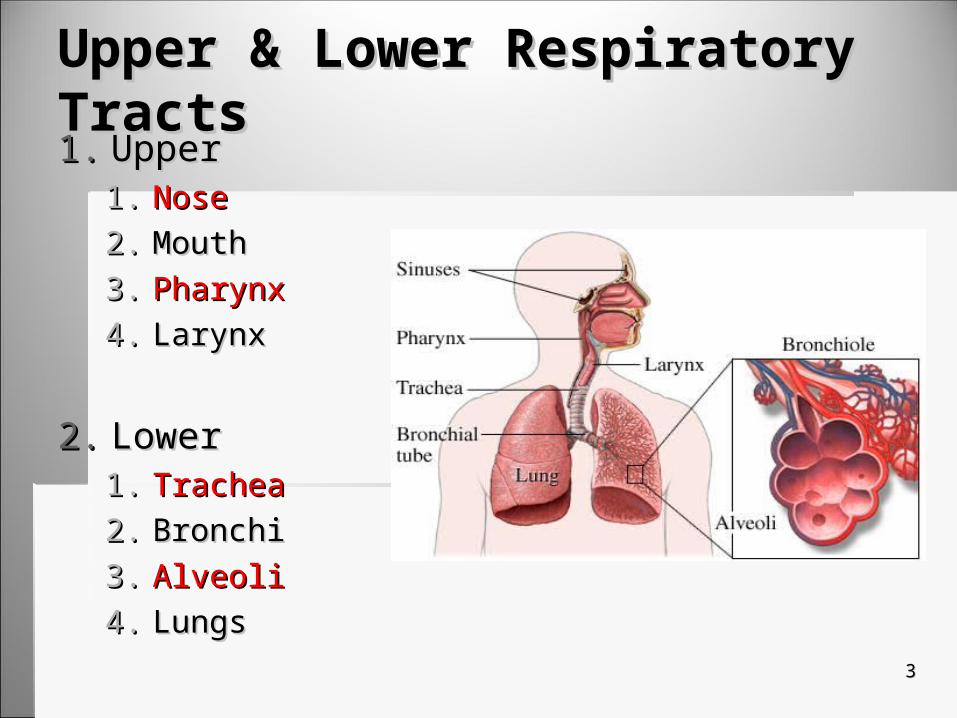
Upper & Lower Respiratory TractsUpper & Lower Respiratory Tracts1.1. UpperUpper
1.1. NoseNose2.2. MouthMouth3.3. PharynxPharynx4.4. LarynxLarynx
2.2. LowerLower1.1. TracheaTrachea2.2. BronchiBronchi3.3. AlveoliAlveoli4.4. LungsLungs

44
MediastinumMediastinum
1.1. AnteriorAnterior1.1. Thyroid & thymus Thyroid & thymus
glandsglands
2.2. MiddleMiddle1.1. HeartHeart2.2. Great vesselsGreat vessels3.3. Esophagus & tracheaEsophagus & trachea
3.3. PosteriorPosterior1.1. Descending aortaDescending aorta
55
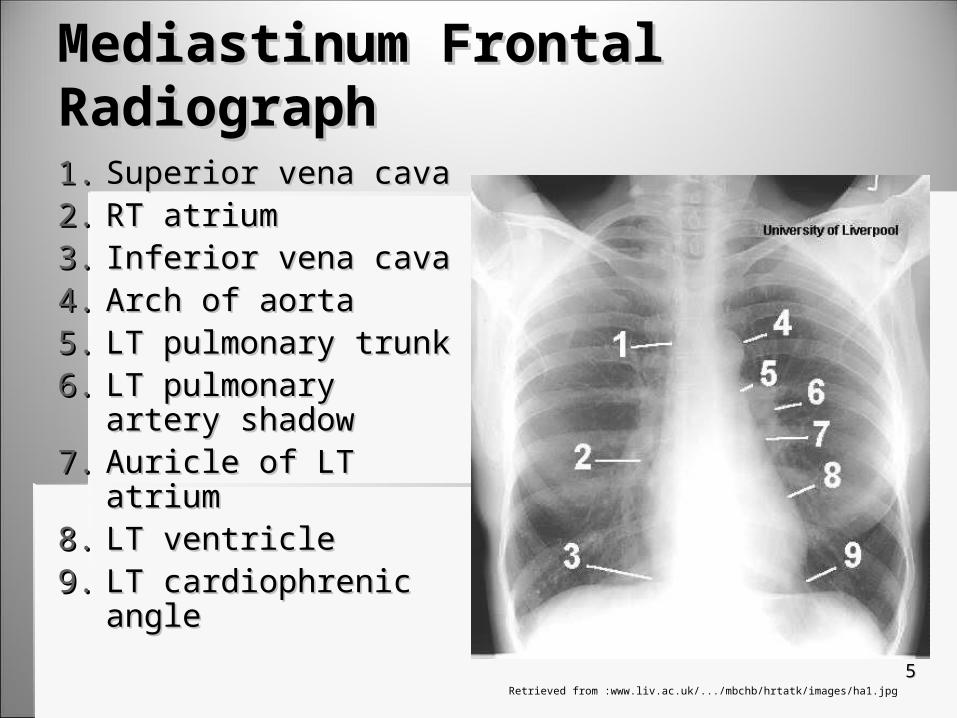
Mediastinum Frontal RadiographMediastinum Frontal Radiograph
1.1. Superior vena cavaSuperior vena cava2.2. RT atriumRT atrium3.3. Inferior vena cavaInferior vena cava4.4. Arch of aortaArch of aorta5.5. LT pulmonary trunkLT pulmonary trunk6.6. LT pulmonary artery LT pulmonary artery
shadowshadow7.7. Auricle of LT atriumAuricle of LT atrium8.8. LT ventricleLT ventricle9.9. LT cardiophrenic angleLT cardiophrenic angle
Retrieved from :www.liv.ac.uk/.../mbchb/hrtatk/images/ha1.jpg

66
The Importance of CXR’sThe Importance of CXR’s
1.1. It is the It is the most common most common diagnostic examdiagnostic exam
2.2. It becomes It becomes routineroutine
3.3. ImproperImproper techniques techniques
77
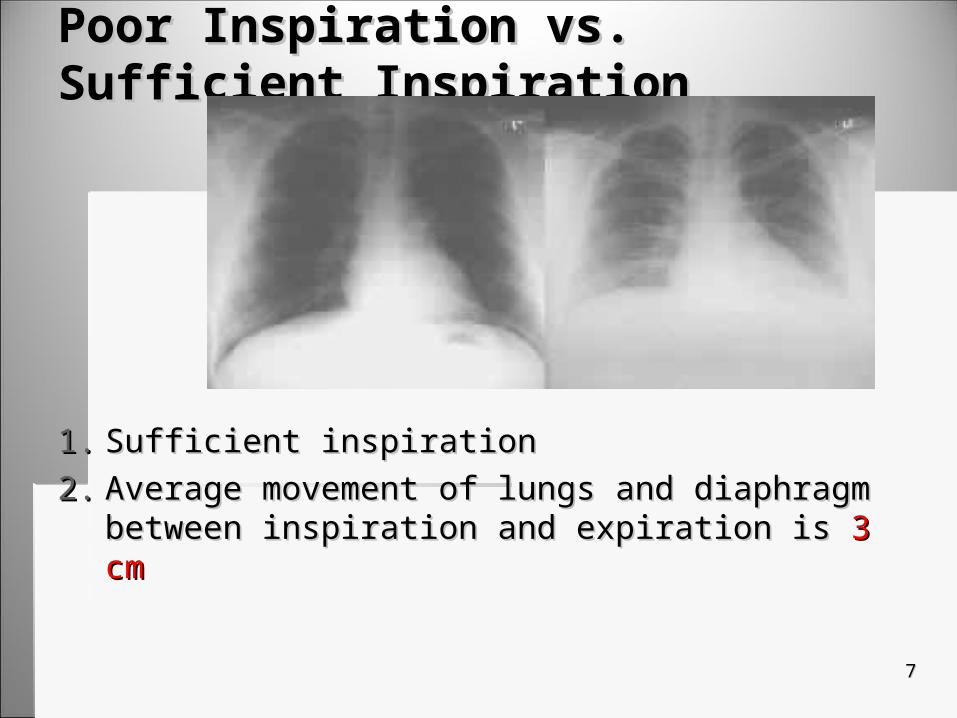
Poor Inspiration vs. Sufficient InspirationPoor Inspiration vs. Sufficient Inspiration
1.1. Sufficient inspiration Sufficient inspiration 2.2. Average movement of lungs and diaphragm Average movement of lungs and diaphragm
between inspiration and expiration isbetween inspiration and expiration is 3 cm 3 cm
88
Film Screen vs. CR / DRFilm Screen vs. CR / DRand Technique Considerationsand Technique Considerations
1.1. Manual Manual techniques techniques 1.1. Consistent TechniquesConsistent Techniques
2.2. Daily radiographsDaily radiographs1.1. Analyze changes in Analyze changes in
pathology after treatmentpathology after treatment2.2. Or the progression the Or the progression the
diseasedisease
3.3. Must have optimal Must have optimal kVpkVp and and mAsmAs
1.1. Use PSP plates Use PSP plates 1.1. They offer a wider latitudeThey offer a wider latitude
2.2. KVpKVp is increased to is increased to decrease PT dosedecrease PT dose

99
Additive & Subtractive PathologiesAdditive & Subtractive Pathologies
1.1. Additive-Additive-1.1. harder than normal to harder than normal to
penetratepenetrate
2.2. Requires an Requires an increaseincrease in in exposure factorsexposure factors
3.3. These are pathologies These are pathologies that that add fluid or tissue add fluid or tissue to normal aerated chestto normal aerated chest1.1. EX: pneumoniaEX: pneumonia
1.1. Subtractive- Subtractive- 1.1. easier than normal to easier than normal to
penetratepenetrate
2.2. These pathologies These pathologies increase increase aerationaeration in the in the chestchest
1.1. EX: emphysemaEX: emphysema
3.3. ReducesReduces exposure exposure factors requiredfactors required

1010
Additive and Subtractive ExamplesAdditive and Subtractive Examples
1111
Technique Adjustments for Different Technique Adjustments for Different Image ReceptorsImage Receptors
1.1. Film ScreenFilm Screen1.1. mAs adjustmentmAs adjustment2.2. kVp adjustments changes kVp adjustments changes contrastcontrast
2.2. With a digital systemWith a digital system1.1. kVpkVp should be adjusted should be adjusted2.2. To To reducereduce PT dose PT dose
1212
AEC Sensors and PathologiesAEC Sensors and Pathologies1.1. AEC requires careful thought in regards to where AEC requires careful thought in regards to where
pathology is in relation to sensorspathology is in relation to sensors
2.2. Portable AEC Portable AEC 1.1. consistent exposure accuracyconsistent exposure accuracy2.2. less sensorsless sensors
3.3. Sensors should be carefully selectedSensors should be carefully selected

CXR ProjectionsCXR Projections

1414
PA: Upright vs. RecumbentPA: Upright vs. Recumbent
1.1. Upright:Upright:
2.2. Recumbent:Recumbent:

1515
AP CXR’sAP CXR’s Usually seen in Portable examsUsually seen in Portable exams Best to be performed upright to demonstrate Best to be performed upright to demonstrate
air/fluid levelsair/fluid levels
Maintain beam perpendicular to plane of IR Maintain beam perpendicular to plane of IR To prevent foreshortening of the heartTo prevent foreshortening of the heart
Use 72” Use 72” To reduce heart magnificationTo reduce heart magnification Longer SID reduces magnificationLonger SID reduces magnification Short OID reduces magnification (this is why PA is Short OID reduces magnification (this is why PA is
preferred)preferred)
1616
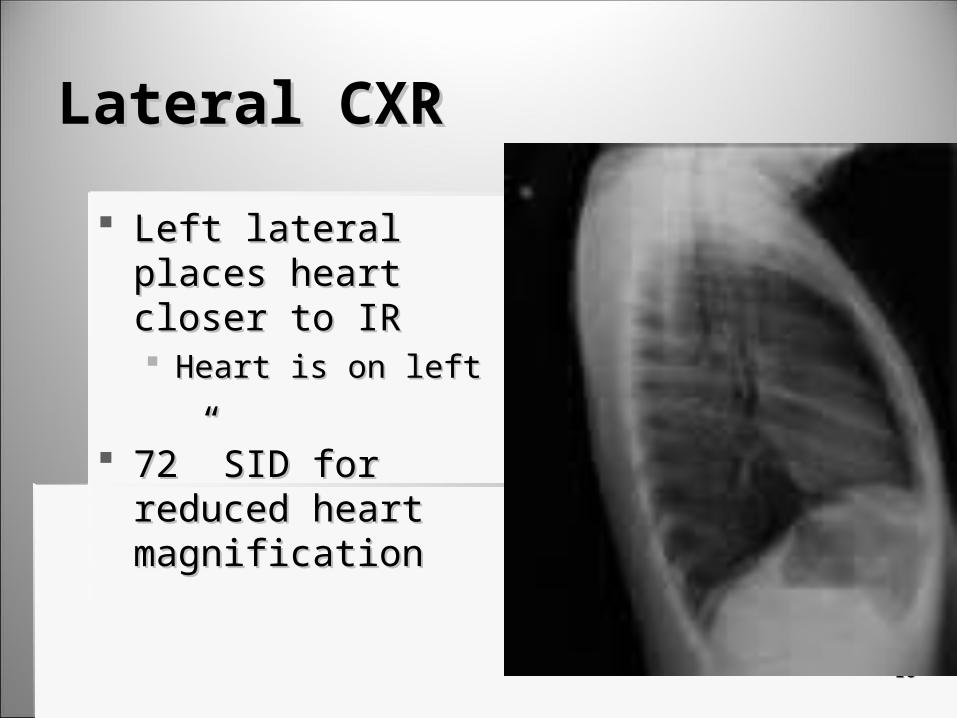
Lateral CXRLateral CXR
Left lateral places heart Left lateral places heart closer to IR closer to IR Heart is on leftHeart is on left
72” SID for reduced 72” SID for reduced heart magnificationheart magnification
1717
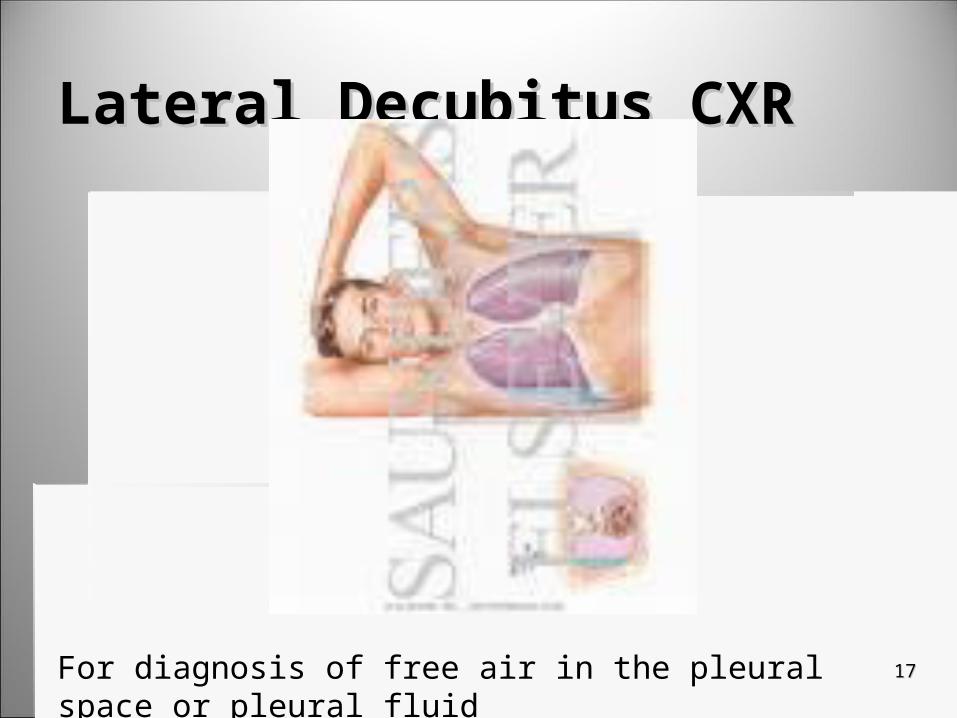
Lateral Decubitus CXRLateral Decubitus CXR
For diagnosis of free air in the pleural space or pleural fluid

1818
Lordotic ChestLordotic Chest
Useful in demonstrating Useful in demonstrating apical regions of the lungapical regions of the lung
Apices are normally Apices are normally obscured by bony obscured by bony structuresstructures
TB likes to reside in apicesTB likes to reside in apices
1919
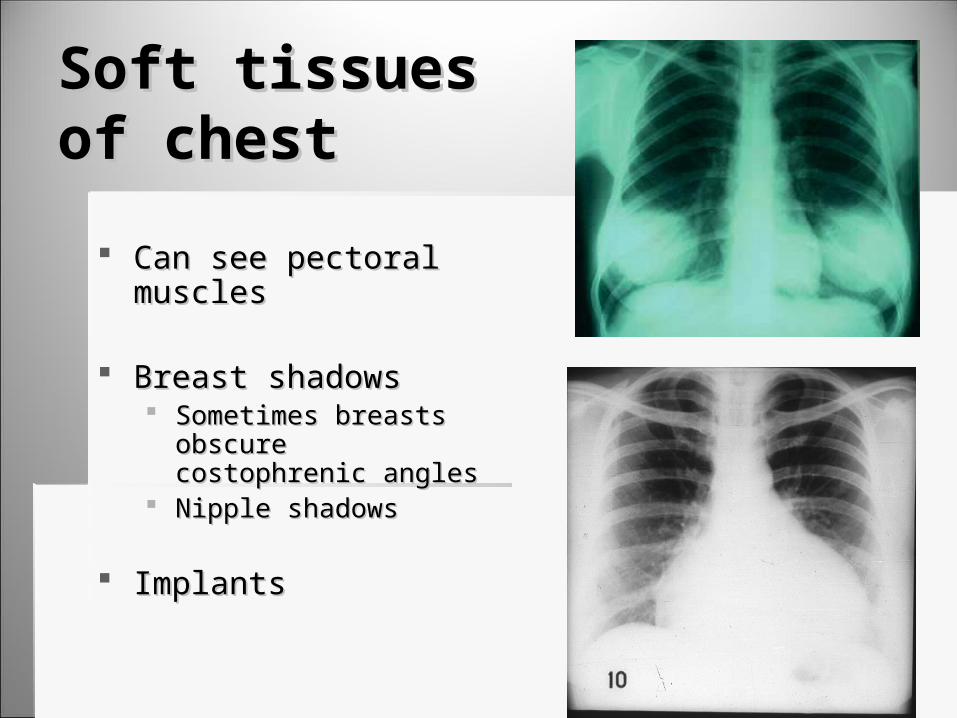
Soft tissuesSoft tissuesof chestof chest
Can see pectoral musclesCan see pectoral muscles
Breast shadowsBreast shadows Sometimes breasts obscure Sometimes breasts obscure
costophrenic anglescostophrenic angles Nipple shadowsNipple shadows
ImplantsImplants
Mediastinal Radiographs Mediastinal Radiographs and Pathologiesand Pathologies
2121
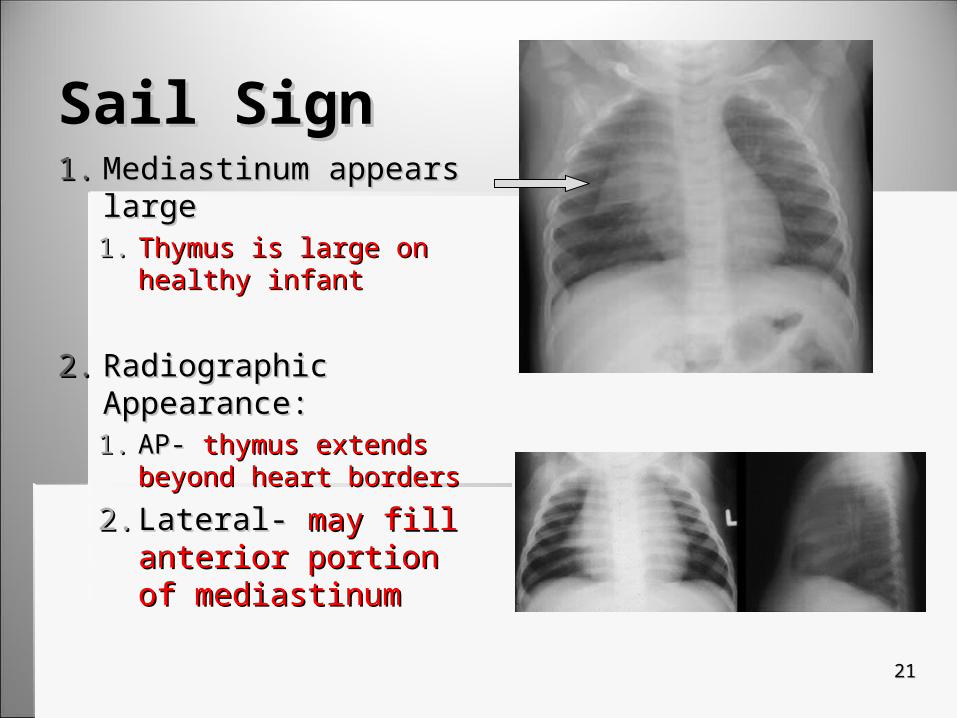
Sail SignSail Sign1.1. Mediastinum appears Mediastinum appears
largelarge1.1. Thymus is large on Thymus is large on
healthy infanthealthy infant
2.2. Radiographic Radiographic Appearance:Appearance:1.1. AP- AP- thymus extends thymus extends
beyond heart bordersbeyond heart borders
2.2. Lateral- Lateral- may fill may fill anterior portion of anterior portion of mediastinummediastinum
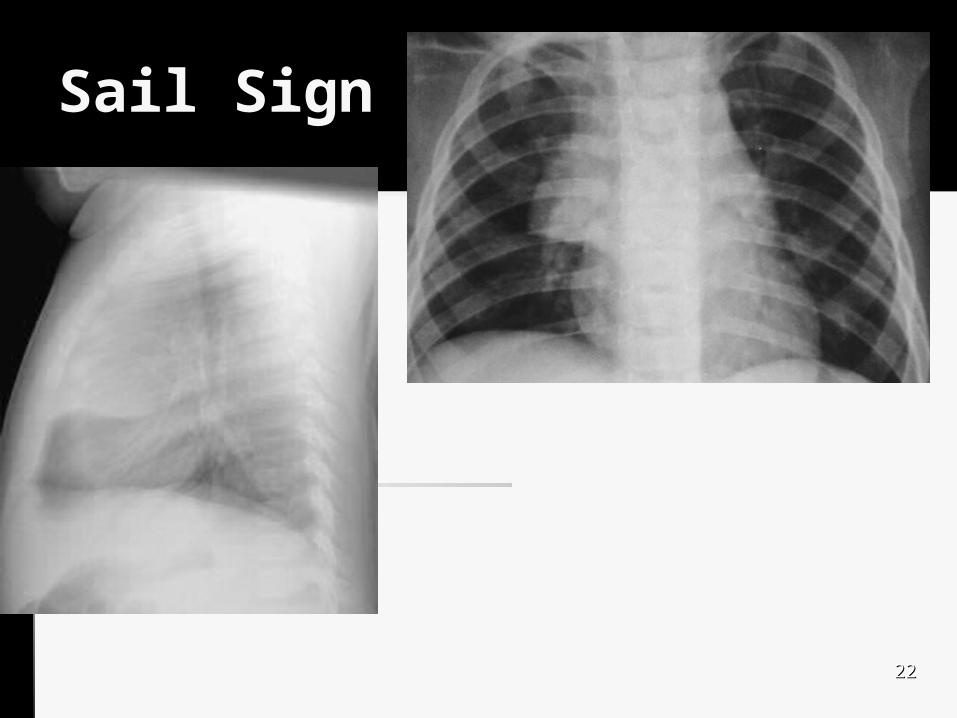
Sail SignSail Sign
2222
2323
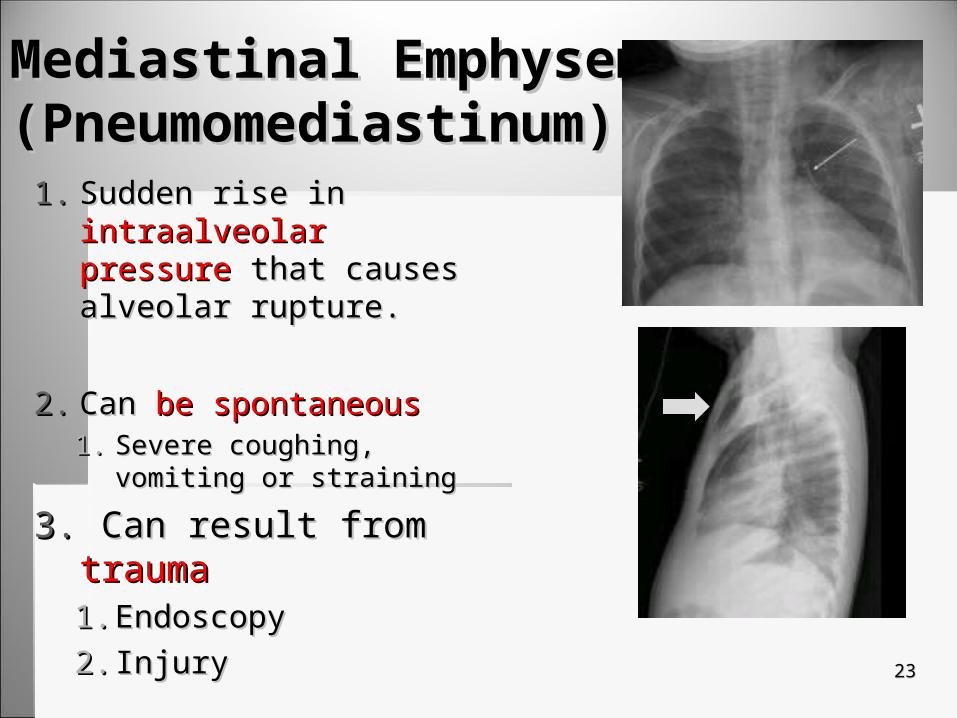
Mediastinal EmphysemaMediastinal Emphysema(Pneumomediastinum)(Pneumomediastinum)
1.1. Sudden rise in Sudden rise in intraalveolar intraalveolar pressure pressure that causes that causes alveolar rupture.alveolar rupture.
2.2. Can Can be spontaneousbe spontaneous1.1. Severe coughing, vomiting or Severe coughing, vomiting or
strainingstraining
3.3. Can result from Can result from traumatrauma1.1. EndoscopyEndoscopy2.2. InjuryInjury
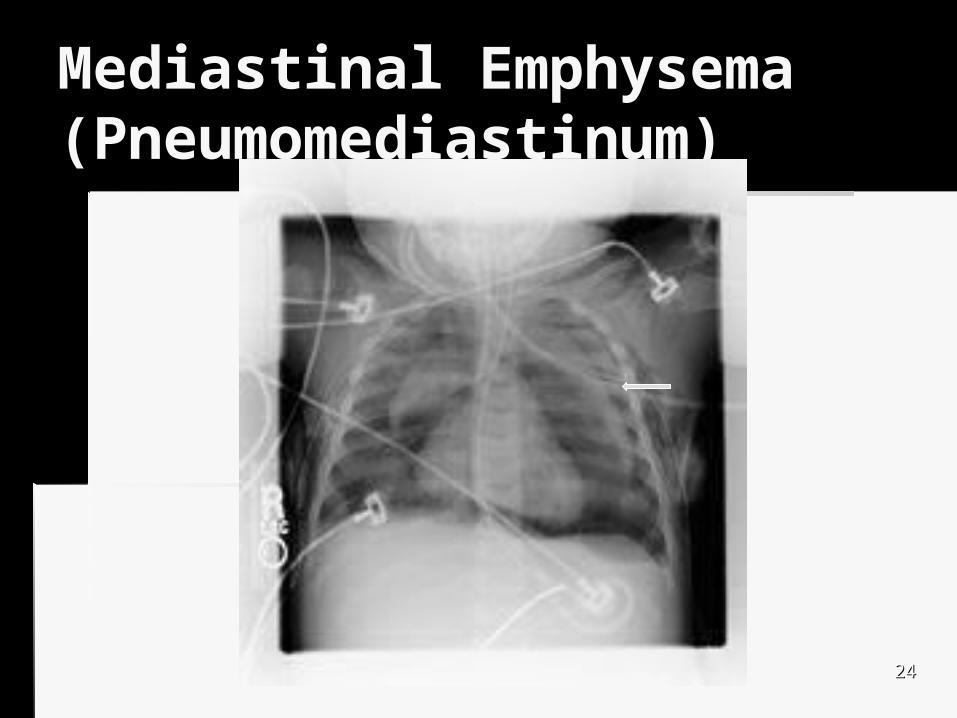
Mediastinal EmphysemaMediastinal Emphysema(Pneumomediastinum)(Pneumomediastinum)
2424
2525
Treatment of Mediastinal Treatment of Mediastinal EmphysemaEmphysema
Spontaneous:Spontaneous: If there is no If there is no
pneumothorax, no pneumothorax, no treatment is necessarytreatment is necessary
Usually resolves in a Usually resolves in a few days without few days without complicationscomplications
Other than Other than spontaneous: spontaneous: Rupture in esophagus Rupture in esophagus
(usually from vomiting)(usually from vomiting) Major bronchus trauma Major bronchus trauma
(trauma)(trauma) Both need prompt Both need prompt
diagnosis & surgical diagnosis & surgical interventionintervention
Esophogram can verify a Esophogram can verify a leak has not occurred.leak has not occurred.

2626
Subcutaneous Subcutaneous EmphysemaEmphysema
1.1. Can be caused by:Can be caused by:1.1. Severe Severe
pneumomediastinumpneumomediastinum 2.2. Penetrating or blunt Penetrating or blunt
injuriesinjuries
2.2. Usually in Usually in chestchest and/or and/or neckneck
3.3. Crackling sound or Crackling sound or sensationsensation
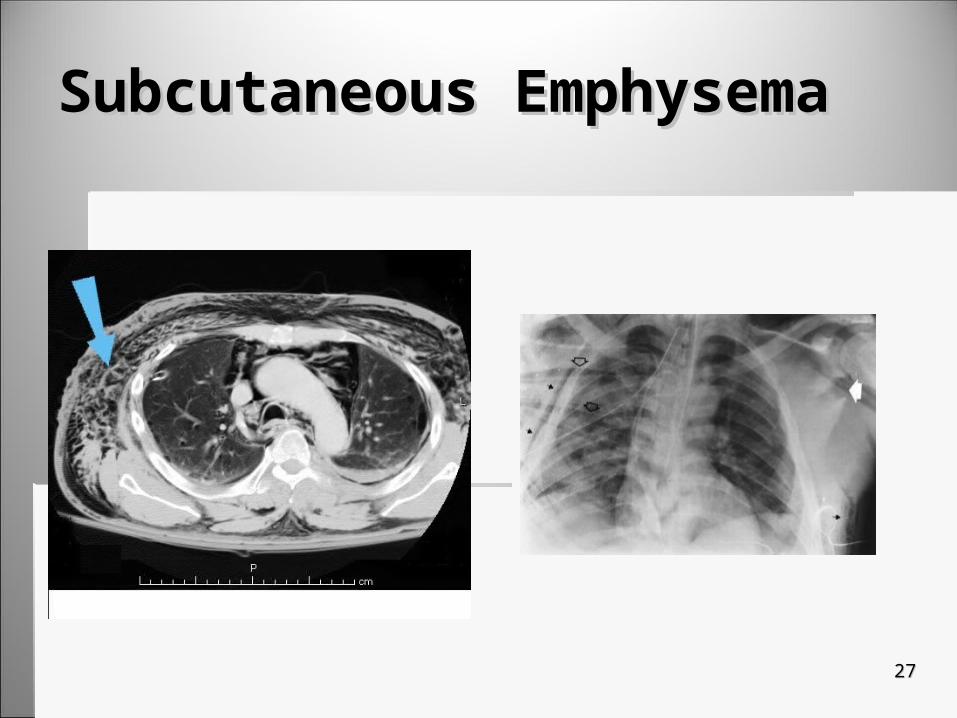
Subcutaneous EmphysemaSubcutaneous Emphysema
2727
Congenital and Hereditary Congenital and Hereditary DiseasesDiseasesCystic FibrosisCystic FibrosisHyaline Membrane DiseaseHyaline Membrane Disease

2929
Cystic FibrosisCystic Fibrosis Generalized disorder from a genetic defect that affects the Generalized disorder from a genetic defect that affects the
function of the exocrine glandsfunction of the exocrine glands
Involves many organs & nearly all exocrine glandsInvolves many organs & nearly all exocrine glands
Other organs affectedOther organs affected Salivary glandsSalivary glands Small bowelSmall bowel PancreasPancreas Biliary tractBiliary tract Female cervixFemale cervix Male genital organsMale genital organs
Most lethal genetic disease of white childrenMost lethal genetic disease of white children
3030
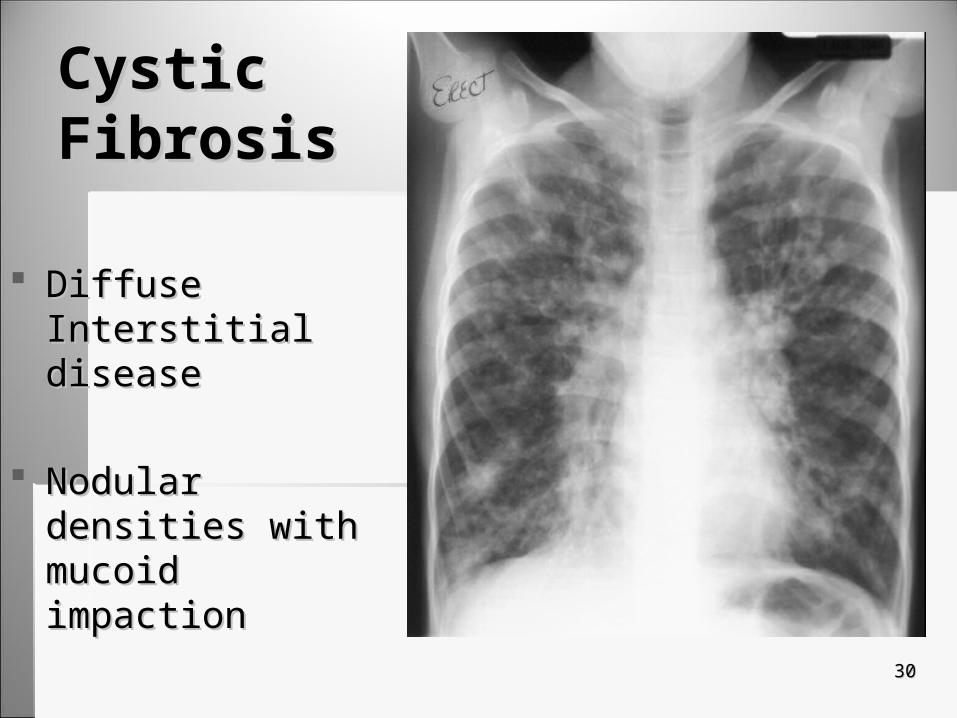
Cystic Cystic FibrosisFibrosis
Diffuse Interstitial Diffuse Interstitial diseasedisease
Nodular densities with Nodular densities with mucoid impactionmucoid impaction

3131
Progression of Cystic FibrosisProgression of Cystic Fibrosis At birth lungs are normalAt birth lungs are normal
Progression:Progression: Increased secretions from bronchial glandsIncreased secretions from bronchial glands Leads to obstruction of the bronchial glandsLeads to obstruction of the bronchial glands Obstruction leads to staph infections,Obstruction leads to staph infections, Followed by tissue damage:Followed by tissue damage:
atelectasis,(collapsed lung) and emphysemaatelectasis,(collapsed lung) and emphysema
Once progression is in motion it is hard to stopOnce progression is in motion it is hard to stop
3232
Cystic Cystic FibrosisFibrosis
SymptomsSymptoms Chronic couthChronic couth
With sputum, vomiting & With sputum, vomiting & disturbed sleepdisturbed sleep
WheezingWheezing
Recurrent Pulmonary Recurrent Pulmonary infectionsinfections
Role of Radiography:Role of Radiography:
CXR aid in diagnosisCXR aid in diagnosis Early: bronchial thickening Early: bronchial thickening
and hyperinflationand hyperinflation Progression: brochiectasis, Progression: brochiectasis,
cyst, atelectasis, scarring, cyst, atelectasis, scarring, enlargement of pulmonary enlargement of pulmonary artery and RT ventricle, artery and RT ventricle, overflation of lungs and chest overflation of lungs and chest wallwall

Cystic Fibrosis SinusesCystic Fibrosis Sinuses
Sinus x-rays & CT will demonstrate persistent Sinus x-rays & CT will demonstrate persistent opacification of sinusesopacification of sinuses
3333
3434
Cystic FibrosisCystic Fibrosis Prognosis:Prognosis:
Determined by degree of Determined by degree of respiratory involvementrespiratory involvement
Respiratory failure is Respiratory failure is inevitable inevitable
Death 20-30 years of ageDeath 20-30 years of age
Treatment:Treatment:
Antimicrobial drugsAntimicrobial drugs BronchodilatorsBronchodilators Respiratory P.T.Respiratory P.T. With pneumothorax- With pneumothorax-
chest tubechest tube With hemoptysis- With hemoptysis-
embolizing involved embolizing involved brachial arteriesbrachial arteries
PsychotherapyPsychotherapy

3535
Cystic FibrosisCystic Fibrosis
3636
Hyaline Membrane Disease Hyaline Membrane Disease Respiratory Distress Syndrome (RDS)Respiratory Distress Syndrome (RDS)
Affects Affects Premature infantsPremature infants
Caused by immature surfactant producing Caused by immature surfactant producing systemsystem
What is surfactant?What is surfactant? AnswerAnswer

3737
RDS : Signs and SymptomsRDS : Signs and Symptoms
1.1. Signs:Signs:1.1. Rapid & labored breathing Rapid & labored breathing 2.2. Respiratory distress Respiratory distress 3.3. Atelectasis worseningAtelectasis worsening
2.2. In severe cases acidosis occursIn severe cases acidosis occurs
3.3. What is acidosis? What is acidosis? 1.1. AnswerAnswer
3838
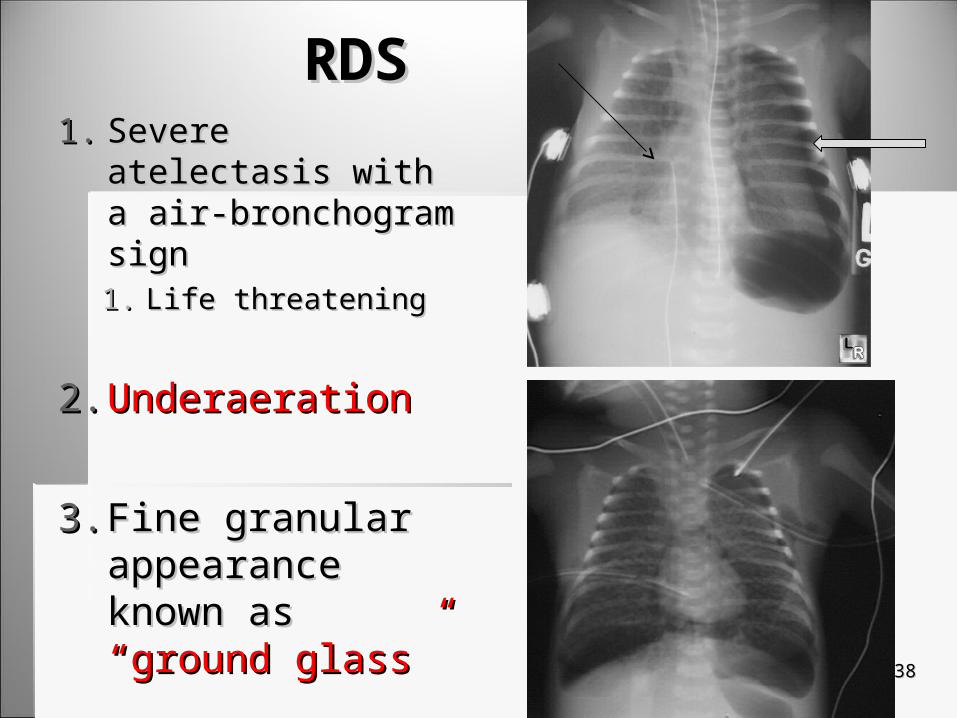
RDSRDS1.1. Severe atelectasis with Severe atelectasis with
a air-bronchogram signa air-bronchogram sign1.1. Life threateningLife threatening
2.2. UnderaerationUnderaeration
3.3. Fine granular Fine granular appearance known appearance known as as “ground glass”“ground glass”
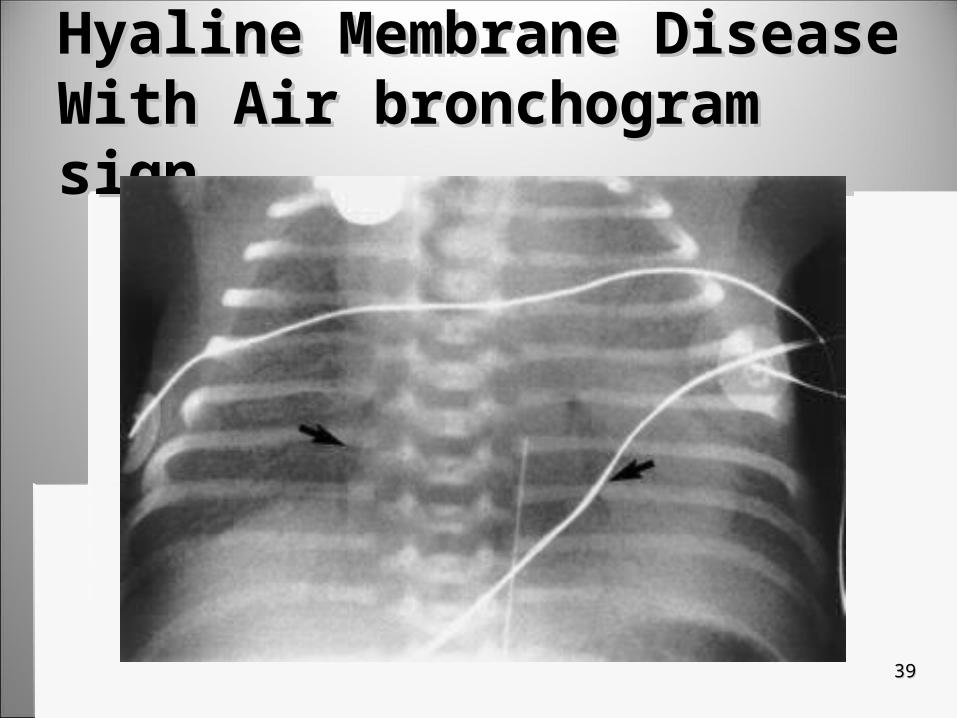
Hyaline Membrane Disease With Hyaline Membrane Disease With Air bronchogram signAir bronchogram sign
3939

4040
Treatment for RDSTreatment for RDS
1.1. Proper Proper thermalthermal environment environment
2.2. Satisfactory tissue Satisfactory tissue oxygenationoxygenation1.1. Monitored by arterial blood gasMonitored by arterial blood gas
3.3. Artificial surfactant Artificial surfactant
Inflammatory DiseasesInflammatory Diseases
4242
PneumoniaPneumonia1.1. 66thth leading cause of death in U.S. leading cause of death in U.S.
1.1. Most common lethal noscomial infectionMost common lethal noscomial infection
2.2. Most frequent type of inflammation in the Most frequent type of inflammation in the lung compromising pulmonary functionlung compromising pulmonary function
3.3. Causes include:Causes include:1.1. BacteriaBacteria2.2. VirusVirus3.3. mycoplasmasmycoplasmas

4343
Pneumonia: Age relatedPneumonia: Age related
Infants & childrenInfants & children Most common caused Most common caused
by viral pathogensby viral pathogens
In adolescents & young In adolescents & young adultsadults Most common causesMost common causes
Bacterial organisms Bacterial organisms termed mycoplasma termed mycoplasma pneumoniaepneumoniae
In adultsIn adults Most common causes:Most common causes:
StreptococcusStreptococcus StaphylococcusStaphylococcus PneumococcusPneumococcus Haemophilus influenzaHaemophilus influenza Chlamydia pneumoniaeChlamydia pneumoniae Legionella pneumophilaLegionella pneumophila
4444
Pneumonia: Pneumonia: Classification by locationClassification by location
1.1. Lobar pneumoniaLobar pneumonia1.1. The inflammation effects entire lobeThe inflammation effects entire lobe
2.2. Segmental pneumoniaSegmental pneumonia1.1. A segment of the lungA segment of the lung
3.3. BronchopneumoniaBronchopneumonia1.1. Bronchi and alveoliBronchi and alveoli
4.4. Interstitial pneumoniaInterstitial pneumonia1.1. Interstitial lung tissueInterstitial lung tissue

4545
Lobar Lobar PneumoniaPneumonia
Right sided lobar Right sided lobar pneumoniapneumonia

4646
Segmental pneumoniaSegmental pneumonia
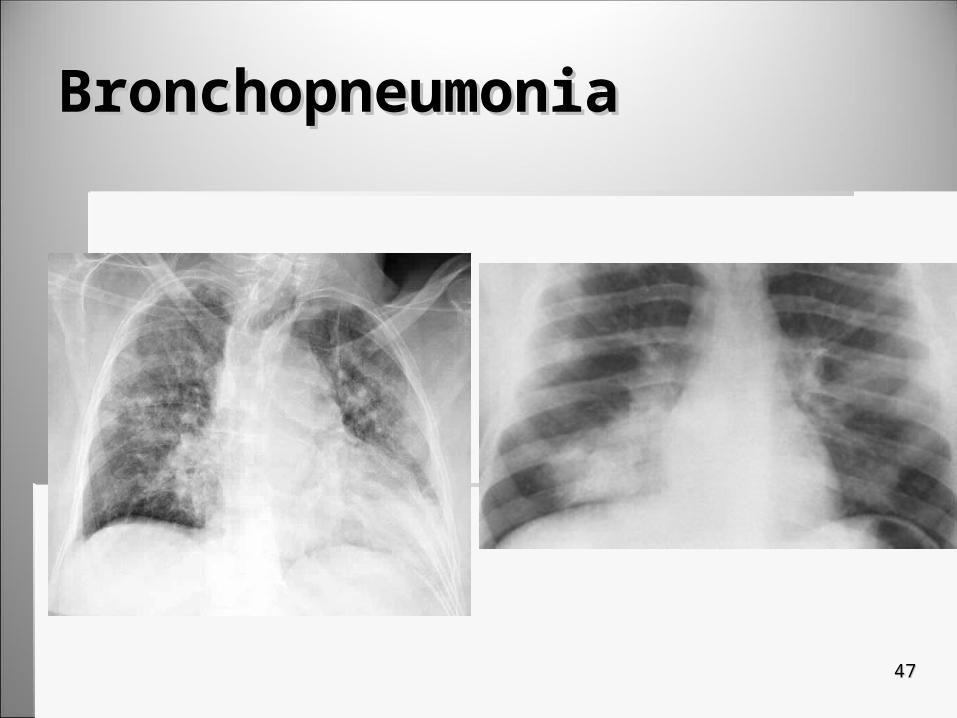
BronchopneumoniaBronchopneumonia
4747

4848
Interstitial PneumoniaInterstitial Pneumonia
4949
CXR’s for PneumoniaCXR’s for Pneumonia
Important in determining location of Important in determining location of pneumoniapneumonia
Appears as soft-patchy, ill defined alveolar Appears as soft-patchy, ill defined alveolar infiltrates and pulmonary densitiesinfiltrates and pulmonary densities Alveolar infiltration results when alveolar air Alveolar infiltration results when alveolar air
spaces are filled with fluid or cellsspaces are filled with fluid or cells

5050
Generalized Symptoms Generalized Symptoms of Pneumoniaof Pneumonia CoughCough
FeverFever
Sputum production (develops over days)Sputum production (develops over days)
TachypneaTachypnea
Crackles during clinical examinationCrackles during clinical examination
5151
Types of Bacterial PneumoniaTypes of Bacterial Pneumonia Most commonMost common
Pneumococcal (lobar) pneumoniaPneumococcal (lobar) pneumonia
Less commonLess common StaphylococcalStaphylococcal
Occurs sporadically with epidemics of influenzaOccurs sporadically with epidemics of influenza StreptpcoccalStreptpcoccal
Less than 1% of bacterial pneumoniasLess than 1% of bacterial pneumonias LegionnairesLegionnaires
Occurs in late summer- early fallOccurs in late summer- early fall Severe bacterial pneumoniaSevere bacterial pneumonia Occurs in LG buildings such as hotels and hospitalsOccurs in LG buildings such as hotels and hospitals

5252
Pneumococcal (lobar) PneumoniaPneumococcal (lobar) Pneumonia
Caused by a bacteria present in healthy Caused by a bacteria present in healthy throatsthroats Making it most common bacterial pneumoniaMaking it most common bacterial pneumonia When immune system weak bacteria multiplies When immune system weak bacteria multiplies
and spreads to lung, causing inflammation to and spreads to lung, causing inflammation to alveolialveoli
Usually in lobular without affecting bronchus Usually in lobular without affecting bronchus themselvesthemselves

5353
Pneumococcal (lobar) PneumoniaPneumococcal (lobar) Pneumonia
Demonstrates a collection of fluid on one or more lessDemonstrates a collection of fluid on one or more less Lateral view serving to identify segmental involvementLateral view serving to identify segmental involvement In a LLD pleural fluid is evidentIn a LLD pleural fluid is evident
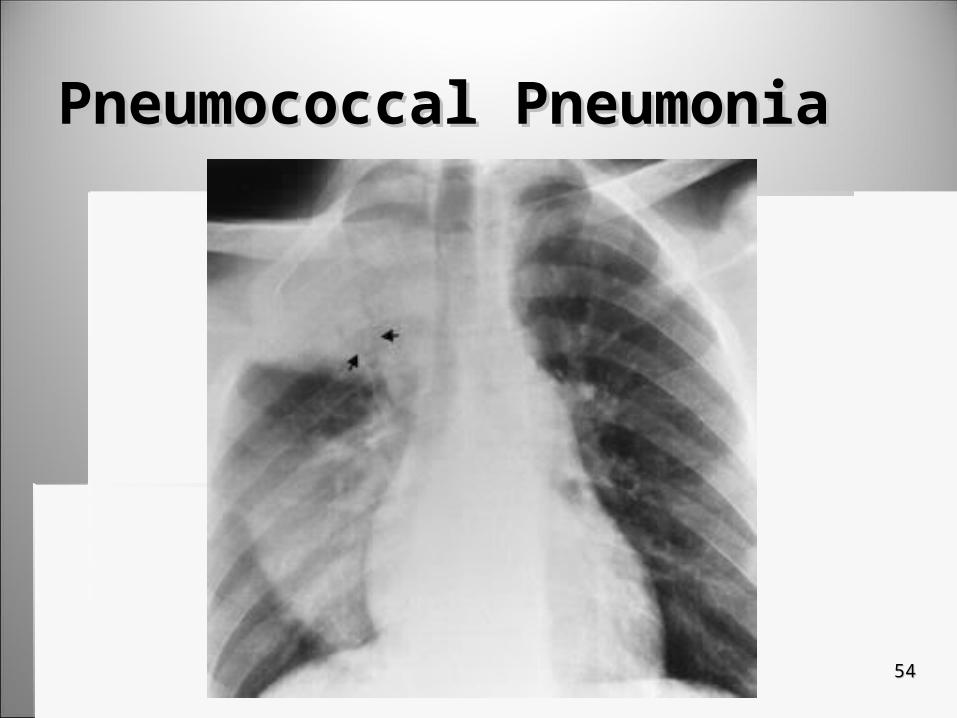
Pneumococcal PneumoniaPneumococcal Pneumonia
5454

Air- Bronchogram signAir- Bronchogram sign
5555
5656
Treatment of Treatment of Pneumococcal (lobar) PneumoniaPneumococcal (lobar) Pneumonia
Bed restBed rest
AntibioticsAntibiotics Based on lab resultsBased on lab results AgeAge
Usually resolves in 1 weekUsually resolves in 1 week
5757
Aspiration PneumoniaAspiration Pneumonia
Caused by acid vomitus aspirated by lower Caused by acid vomitus aspirated by lower respiratory tractrespiratory tract
May follow May follow anesthesia anesthesia alcoholic intoxication alcoholic intoxication strokestroke
5858
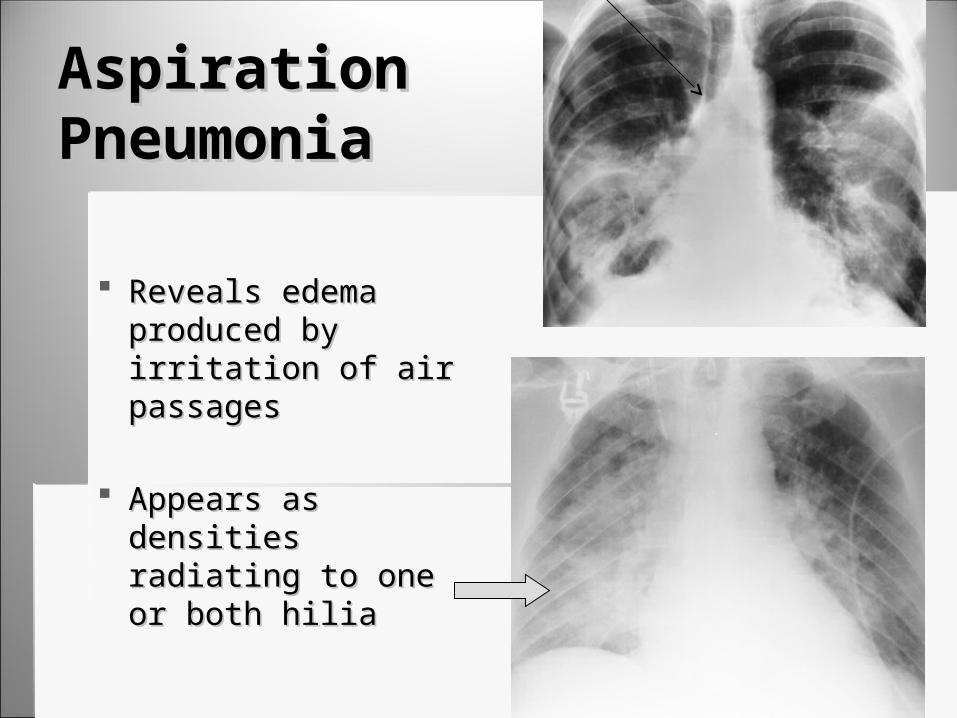
Aspiration Aspiration PneumoniaPneumonia
Reveals edema Reveals edema produced by irritation produced by irritation of air passagesof air passages
Appears as densities Appears as densities radiating to one or radiating to one or both hilia both hilia
5959
Treatment of Treatment of Aspiration PneumoniaAspiration Pneumonia Strictly supportiveStrictly supportive
Control of hypoxia and secretionsControl of hypoxia and secretions
Replacement of fluids (speech therapist)Replacement of fluids (speech therapist)
Antimicrobial drugs if infection has occurred Antimicrobial drugs if infection has occurred Based on lab resultsBased on lab results
6060
Viral (interstitial) PneumoniaViral (interstitial) Pneumonia Can be caused by various virusesCan be caused by various viruses
Mostly influenza A & BMostly influenza A & B
Spreads by infected person spreading virus to Spreads by infected person spreading virus to a non-immune persona non-immune person
Most cases are mild and x-ray findings are Most cases are mild and x-ray findings are minimalminimal Diagnosis is based on clinical findings and Diagnosis is based on clinical findings and
serologic testsserologic tests

6161
Viral (interstitial) PneumoniaViral (interstitial) Pneumonia Symptoms:Symptoms:
Dry coughDry cough FeverFever
Complications:Complications: Secondary to bacterial infections as a result of low Secondary to bacterial infections as a result of low
resistanceresistance Brought on by inflammatory process to the virusBrought on by inflammatory process to the virus
Treatment:Treatment: Relief of symptomsRelief of symptoms Does not respond to antibioticsDoes not respond to antibiotics
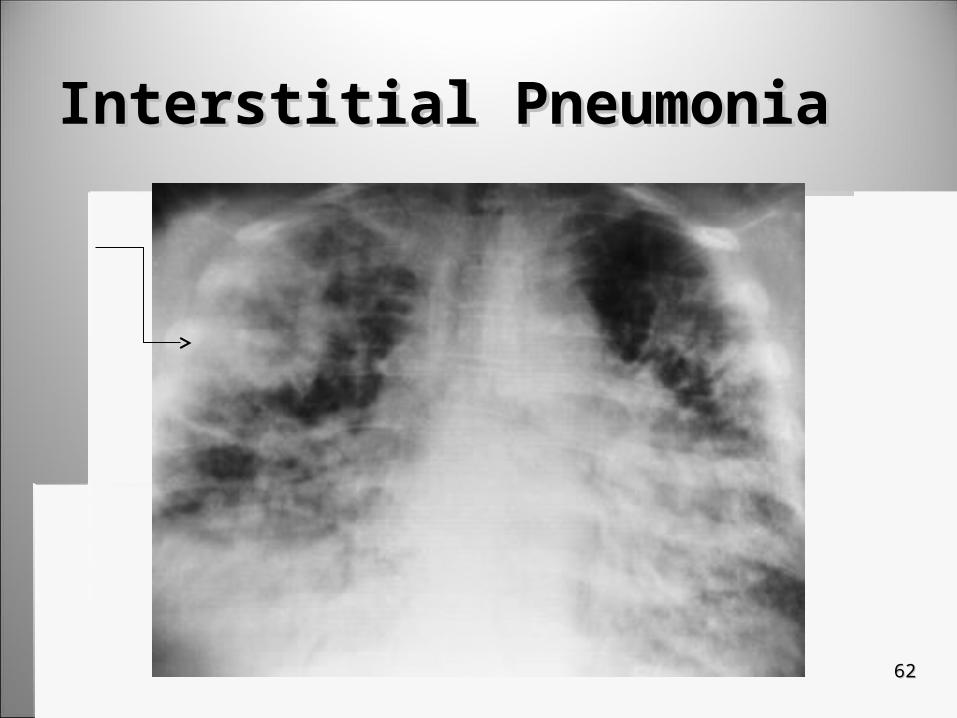
Interstitial PneumoniaInterstitial Pneumonia
6262
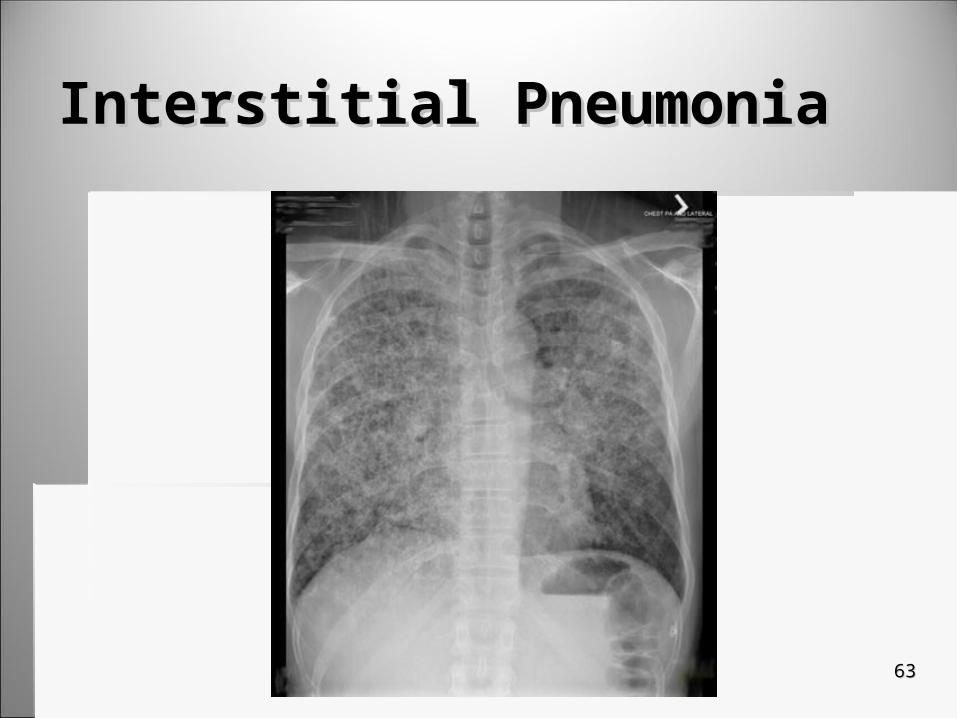
Interstitial PneumoniaInterstitial Pneumonia
6363
6464
BronchiectasisBronchiectasis Permanent dilatation of 1 or more of the large Permanent dilatation of 1 or more of the large
bronchibronchi A result of destruction of the elastic & muscular A result of destruction of the elastic & muscular
components of the bronchial wallcomponents of the bronchial wall
Can be congenital or acquiredCan be congenital or acquired Typically following and inflammation of the bronchial Typically following and inflammation of the bronchial
walls due to bacterial or viral infectionswalls due to bacterial or viral infections

6565
Progression of BronchiectasisProgression of Bronchiectasis1.1. Early stages:Early stages:
1.1. Chronic coughChronic cough2.2. Can be asymptomaticCan be asymptomatic
2.2. Progresses:Progresses:1.1. Into a productive cough as bronchial a weakened a Into a productive cough as bronchial a weakened a
dilateddilated2.2. Forms a sac-like structure which is a haven for infectionsForms a sac-like structure which is a haven for infections
3.3. Later:Later:1.1. Infection grow and bronchial walls destroyed,Infection grow and bronchial walls destroyed,2.2. Results in an abscessResults in an abscess3.3. Pt’s may complain of pain, recurrent fevers and SOBPt’s may complain of pain, recurrent fevers and SOB

6666
BronchiectasisBronchiectasis
Demonstrated increased bronchovascular markings and parallel lines Demonstrated increased bronchovascular markings and parallel lines outlining the bronchi (Tram lines)outlining the bronchi (Tram lines)
Occasionally Occasionally honeycombinghoneycombing and cystic areas are present and cystic areas are present
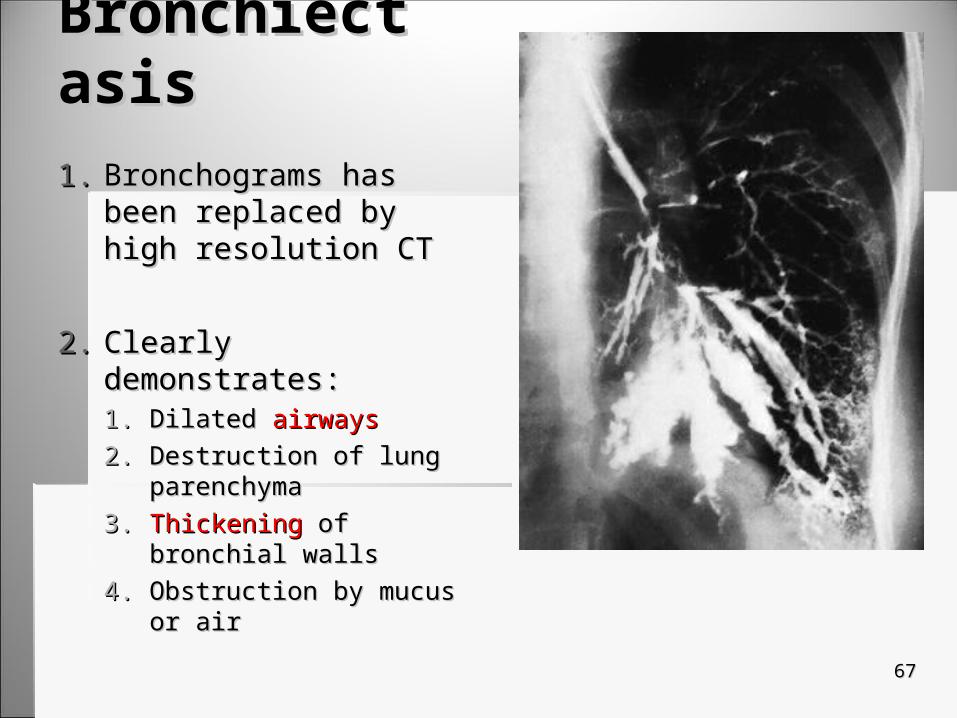
BronchiectasisBronchiectasis1.1. Bronchograms has been Bronchograms has been
replaced by high resolution replaced by high resolution CTCT
2.2. Clearly demonstrates:Clearly demonstrates:1.1. DilatedDilated airways airways2.2. Destruction of lung Destruction of lung
parenchymaparenchyma3.3. ThickeningThickening of bronchial walls of bronchial walls4.4. Obstruction by mucus or airObstruction by mucus or air
6767
6868
CT and BronchiectasisCT and Bronchiectasis CT has replaced BronchographyCT has replaced Bronchography
High resolution CTHigh resolution CT With 1-2 mm slicesWith 1-2 mm slices With or without contrastWith or without contrast Clearly demonstrates dilated airways of 1.5 times larger Clearly demonstrates dilated airways of 1.5 times larger
than adjacent vesselsthan adjacent vessels Thickening of bronchial walls & obstruction of airways by Thickening of bronchial walls & obstruction of airways by
mucous or airmucous or air
Helical or spiral CTHelical or spiral CT Can offer additional information regarding the extent of Can offer additional information regarding the extent of
disease & its distribution within the segment of the lungdisease & its distribution within the segment of the lung
6969
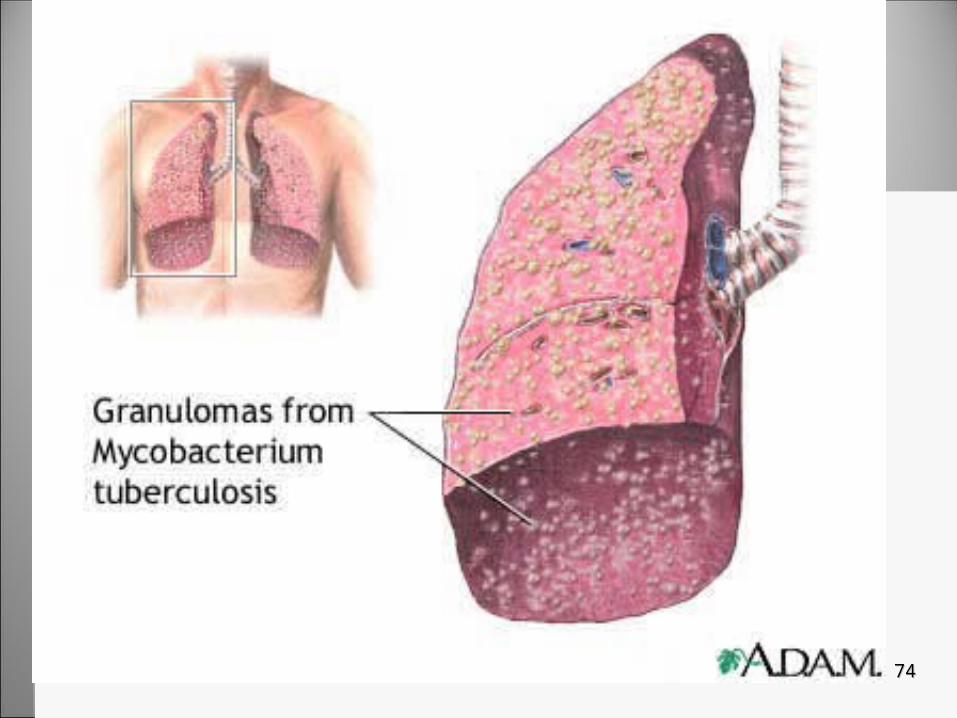
Pulmonary TBPulmonary TB Is an infection caused by inhalation of myobacterium Is an infection caused by inhalation of myobacterium
tuberculosistuberculosis Generally virus affects lungs but can affect other areas of Generally virus affects lungs but can affect other areas of
the bodythe body PT’s contagious through sputum & air dropletsPT’s contagious through sputum & air droplets Respiratory isolation indicatedRespiratory isolation indicated
More prevalent in blacks than whitesMore prevalent in blacks than whites Increase in black & Hispanic IV drug usersIncrease in black & Hispanic IV drug users
Approximately 8 in 100,000 people in the U.S. Approximately 8 in 100,000 people in the U.S. developed TB in late 1990’sdeveloped TB in late 1990’s 1.7 million people worldwide and 10 million in U.S.1.7 million people worldwide and 10 million in U.S.
7070
Progression of TBProgression of TB
Early stages are asymptomatic (90-95%). Early stages are asymptomatic (90-95%). Only identified in mantoux skin testOnly identified in mantoux skin test Primary means of diagnosis but if positive other Primary means of diagnosis but if positive other
tests are performed because of false positivestests are performed because of false positives
Lung lesions begin to appear (apices)Lung lesions begin to appear (apices) Lordotic views of chest for diagnosisLordotic views of chest for diagnosis

7171
TBTB

7272
TBTB
SymptomsSymptoms Most common- morning Most common- morning
productive cough productive cough producing minimal mucous producing minimal mucous
As disease progresses As disease progresses cough becomes more cough becomes more productiveproductive Pts complain of dyspnea, Pts complain of dyspnea,
spontaneous spontaneous pneumothorax, and pleural pneumothorax, and pleural effusioneffusion
TreatmentTreatment Chemotherapeutic Chemotherapeutic
agentsagents
Must be treated with 2 Must be treated with 2 antituberculosis drugsantituberculosis drugs
In extreme cases where In extreme cases where TB is resistant to drug TB is resistant to drug therapy, surgical therapy, surgical resection of may be resection of may be performedperformed
7373
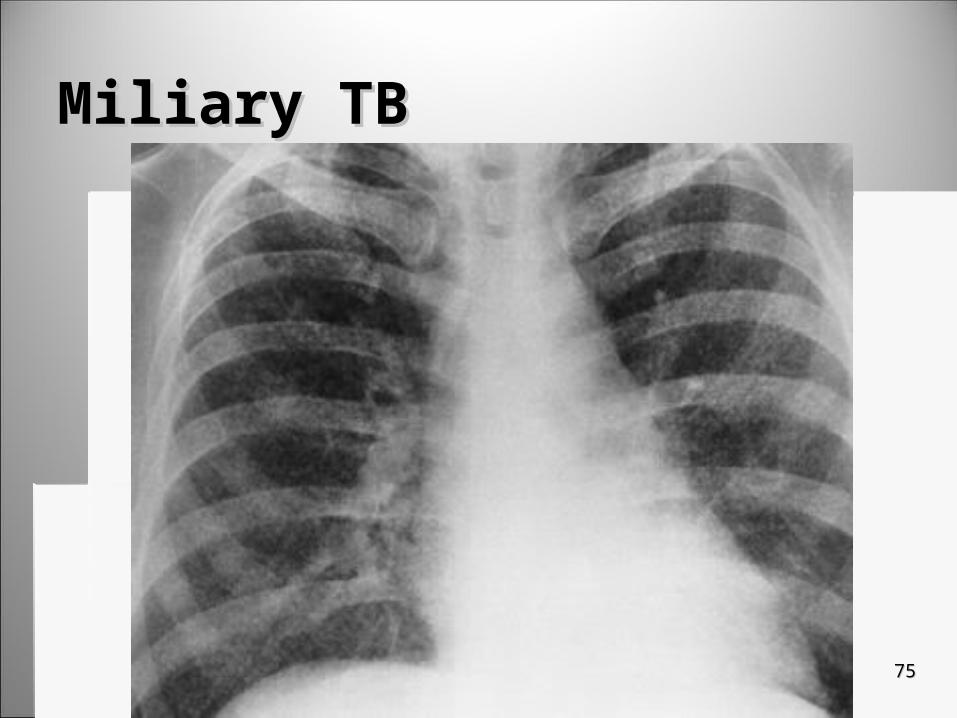
Miliary TBMiliary TB
1.1. Initially miliary TB is not identifiable on filmsInitially miliary TB is not identifiable on films2.2. Immunosuppressed PT’s infection is much more Immunosuppressed PT’s infection is much more
aggressiveaggressive1.1. Overwhelms immune system & spreads through lungs Overwhelms immune system & spreads through lungs
causing pneumoniacausing pneumonia2.2. Spreads through bloodSpreads through blood
3.3. Grows very rapidlyGrows very rapidly1.1. Without treatment TB pneumonia with result in death Without treatment TB pneumonia with result in death
in a few in a few monthsmonths2.2. If resistant to drug therapy If resistant to drug therapy 50% 50% will die in will die in 6060 days days
7474
Miliary TBMiliary TB
7575
7676
COPD- Chronic Obstructive COPD- Chronic Obstructive Pulmonary DisorderPulmonary Disorder1.1. Group of disorder that case chronic airway Group of disorder that case chronic airway
obstructionobstruction1.1. 2 most common are 2 most common are bronchitis & emphysemabronchitis & emphysema2.2. Others are Others are asthma & brochiectasisasthma & brochiectasis
2.2. It is irreversible & results in limited air flowIt is irreversible & results in limited air flow
3.3. Mortality rate has increased in the past 20 years Mortality rate has increased in the past 20 years due to cigarette smoking.due to cigarette smoking.1.1. It is the top It is the top fivefive most common causes of death in U.S. most common causes of death in U.S.2.2. # of people diagnosed has increased # of people diagnosed has increased 60%60% since the 80’s since the 80’s
7777
Chronic BronchitisChronic Bronchitis
Often associated with long term smoking and Often associated with long term smoking and exposure to high levels of industrial air exposure to high levels of industrial air pollutionpollution
Chronic exposure leads to hyperplasia of Chronic exposure leads to hyperplasia of mucous glands, hypertrophy of smooth mucous glands, hypertrophy of smooth muscle & thickening of the bronchial wallmuscle & thickening of the bronchial wall
CXR demonstrates hyperinflation of lungsCXR demonstrates hyperinflation of lungs

7878
Chronic BronchitisChronic Bronchitis Disease progresses slowly over months and Disease progresses slowly over months and
yearsyears
Symptoms:Symptoms: Persistent cough & exportation of phlegm & Persistent cough & exportation of phlegm &
mucousmucous Wheezing, SOB, & arterial hypoxiaWheezing, SOB, & arterial hypoxia
Lungs become hyperinflated and more air is Lungs become hyperinflated and more air is inhaled than exhaledinhaled than exhaled
7979
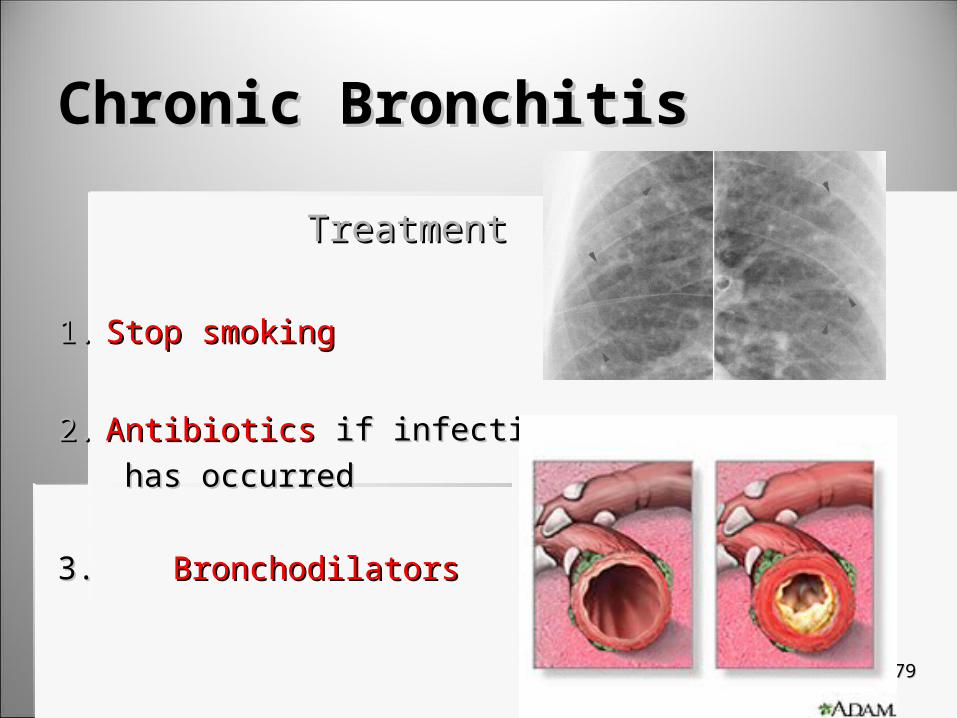
Chronic BronchitisChronic Bronchitis
TreatmentTreatment
1.1. Stop smokingStop smoking
2.2. AntibioticsAntibiotics if infection if infection has occurredhas occurred
3. 3. BronchodilatorsBronchodilators
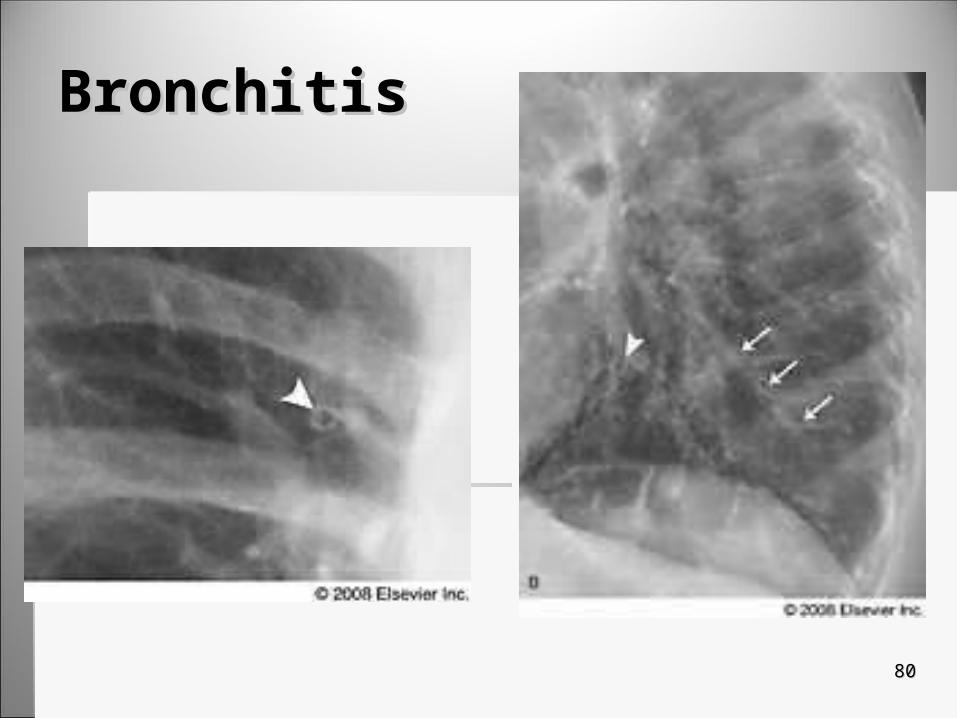
BronchitisBronchitis
8080
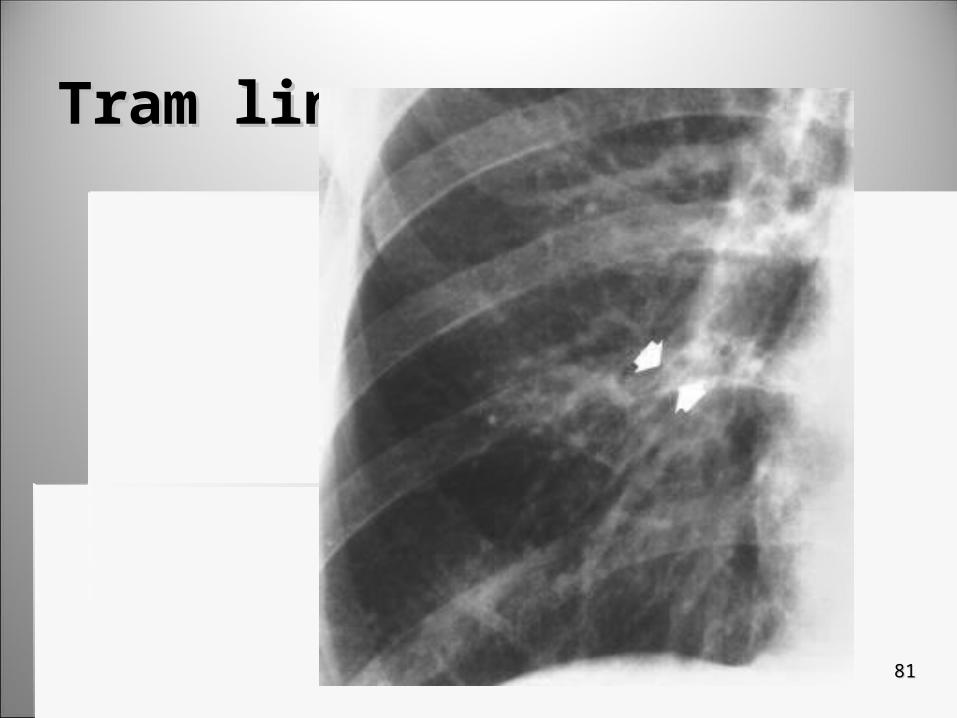
Tram linesTram lines
8181
8282
EmphysemaEmphysema1.1. Lung’s alveoli lose Lung’s alveoli lose elasticity elasticity
2.2. Interference with Interference with expirationexpiration
3.3. Increase in air spaces distal to the Increase in air spaces distal to the terminalterminal bronchioles bronchioles
4.4. Destruction of the alveolar Destruction of the alveolar wallswalls
5.5. Symptoms include Symptoms include dyspneadyspnea (most common). (most common).

8383
EmphysemaEmphysema
1.1. Appears as Appears as depresseddepressed or or flattenedflattened diaphragm diaphragm
2.2. RadiolucentRadiolucent lungs lungs
3.3. BarrelBarrel shaped chest shaped chest
4.4. CXR helps differentiate CXR helps differentiate this disease from others this disease from others that have similar that have similar symptomssymptoms

EmphysemaEmphysema
8484

EmphysemaEmphysema
8585
8686
AsthmaAsthma1.1. Widespread Widespread narrowing narrowing of airways developof airways develop
1.1. Due to Due to increasedincreased responsiveness to various responsiveness to various allergensallergens
2.2. Allergens include:Allergens include:1.1. House dust, pollen, molds, animal dander, foods House dust, pollen, molds, animal dander, foods
fabrics (fabrics (extrinsic extrinsic asthma)asthma)2.2. Exercise, cold, heat, and emotional upset (Exercise, cold, heat, and emotional upset (intrinsicintrinsic
asthma)asthma)
8787
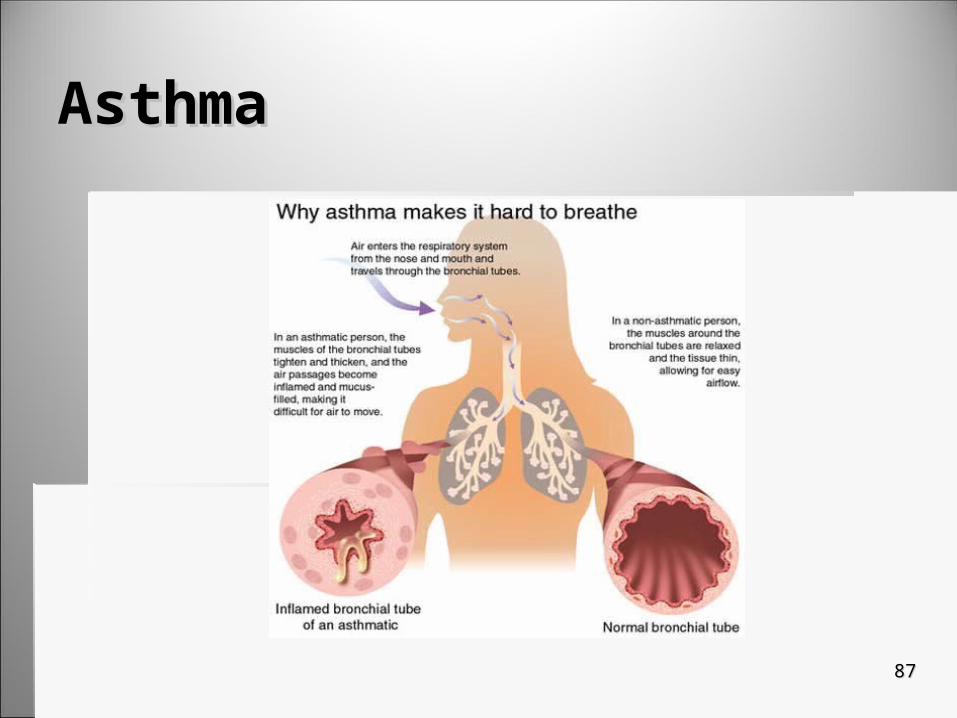
AsthmaAsthma
AsthmaAsthma
8888
8989
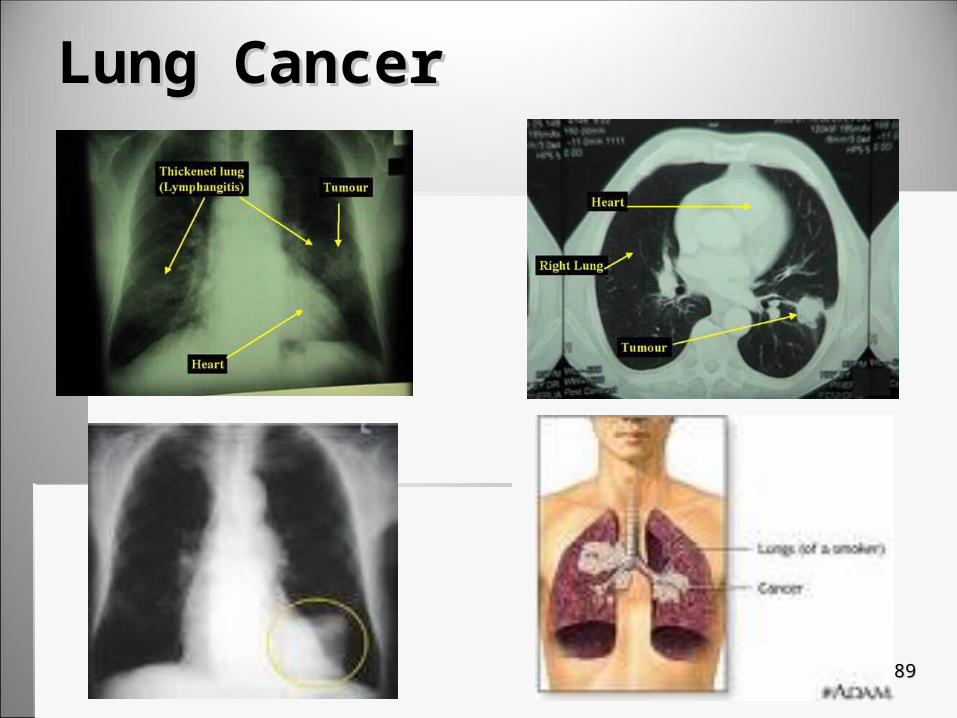
Lung CancerLung Cancer
9090
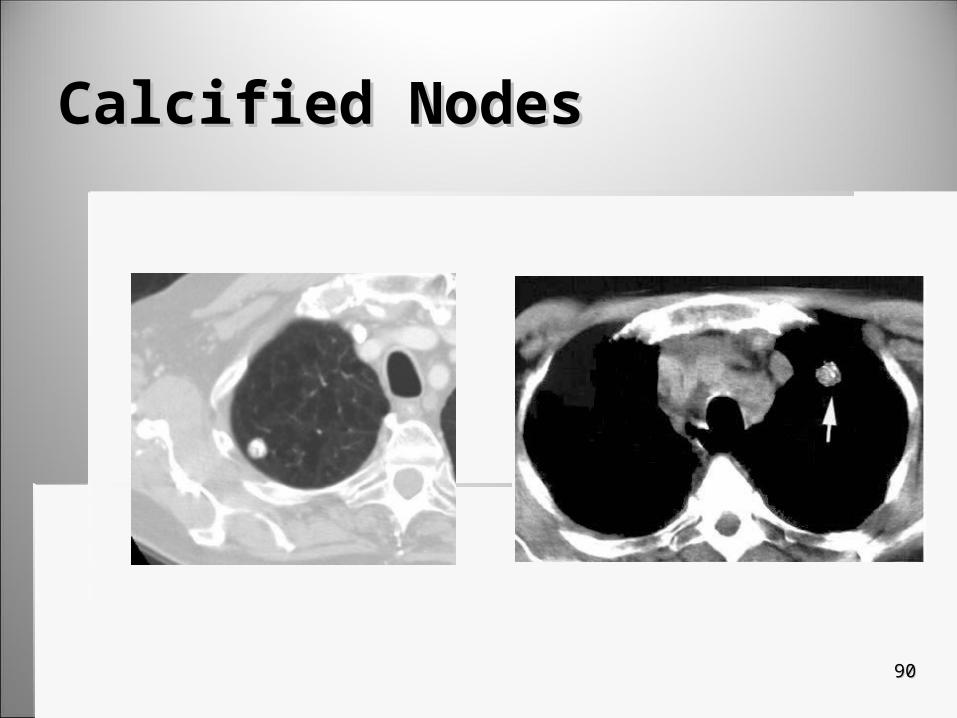
Calcified NodesCalcified Nodes

9191
CroupCroup
Primarily a viral infection of Primarily a viral infection of young children young children Produces inflammatory Produces inflammatory
swelling at the subglottic swelling at the subglottic portion of the tracheaportion of the trachea
Causes a stricture that Causes a stricture that causes a barking coughcauses a barking cough

9292
CroupCroup
9393
Lung AbscessLung Abscess Localized area of dead lung tissue surrounded Localized area of dead lung tissue surrounded
by inflammatory debrisby inflammatory debris
May result from periodontal disease, May result from periodontal disease, neoplasms, pneumonia, or other organisms that neoplasms, pneumonia, or other organisms that invade lunginvade lung More common in RT lungMore common in RT lung
9494
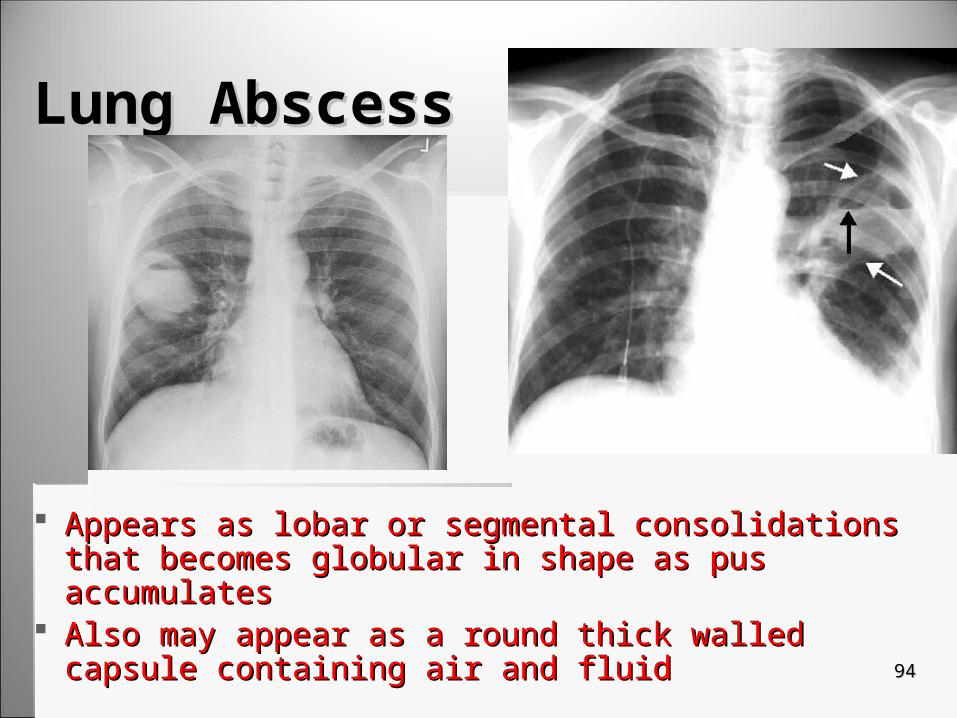
Lung AbscessLung Abscess
Appears as lobar or segmental consolidations that Appears as lobar or segmental consolidations that becomes globular in shape as pus accumulatesbecomes globular in shape as pus accumulates
Also may appear as a round thick walled capsule Also may appear as a round thick walled capsule containing air and fluid containing air and fluid
9595
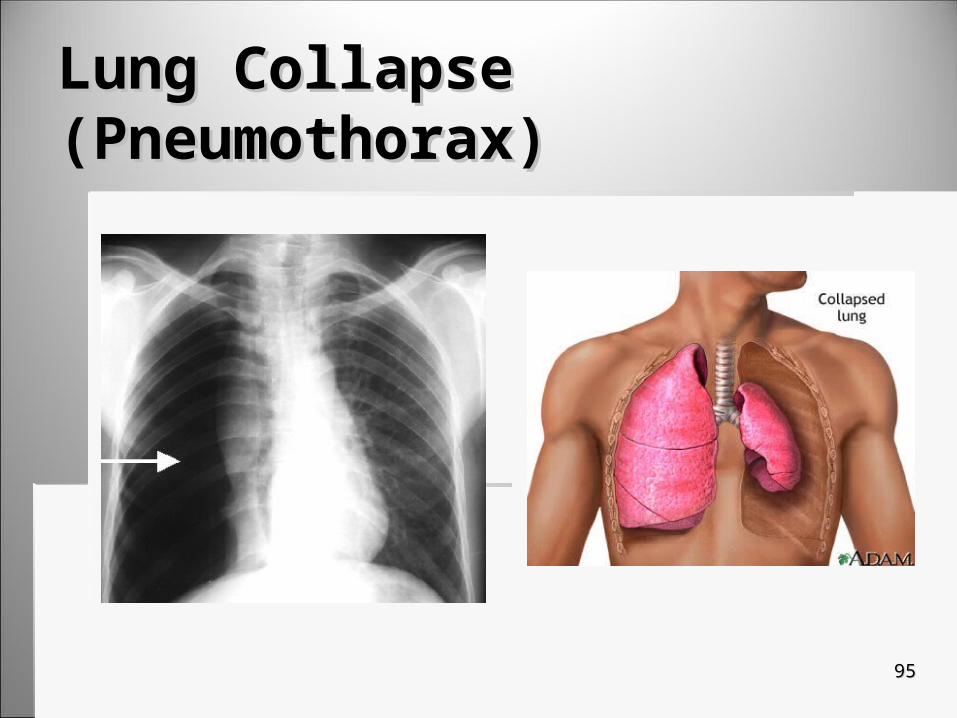
Lung Collapse (Pneumothorax)Lung Collapse (Pneumothorax)

9696
AtelectasisAtelectasis

9797
Foreign BodyForeign Body
9898
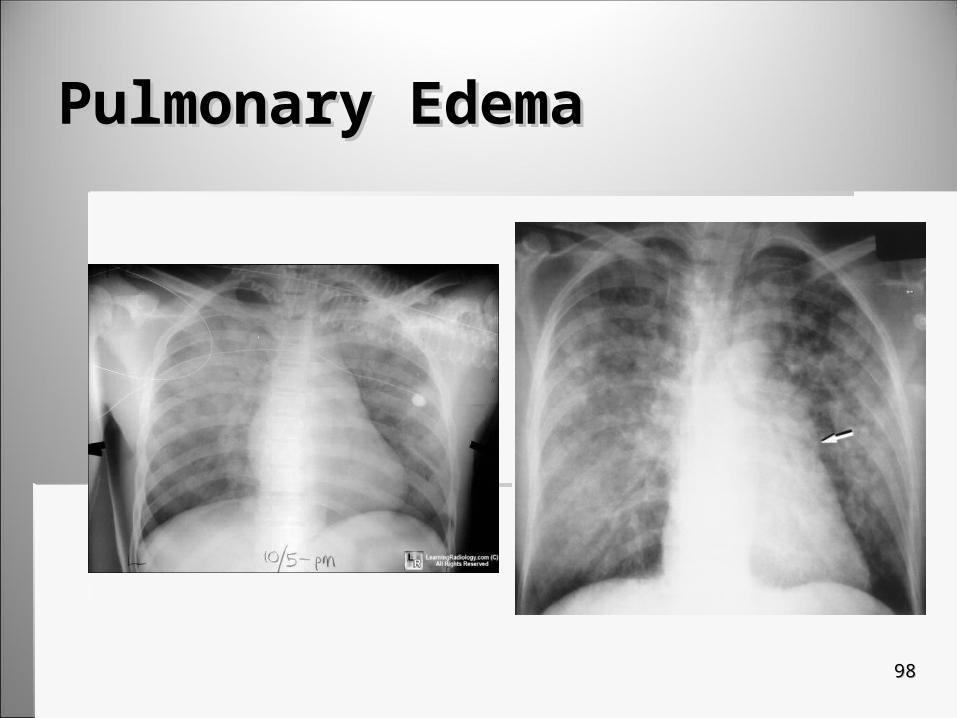
Pulmonary EdemaPulmonary Edema
9999
HistoplasmosisHistoplasmosis Systemic fungal infection caused by a fungus that Systemic fungal infection caused by a fungus that
thrives in soilthrives in soil Especially by bird or bat excretaEspecially by bird or bat excreta Particularly endemic in Ohio Particularly endemic in Ohio
Most cases are acute and mild so they are not Most cases are acute and mild so they are not diagnoseddiagnosed
More severe case: Progressive disseminated More severe case: Progressive disseminated histoplasmosishistoplasmosis It spreads to lungs and leads to cavitory formationsIt spreads to lungs and leads to cavitory formations Cavities resemble TB & are also in apicesCavities resemble TB & are also in apices It is an opportunistic infection for AIDs PT’s & leads to acute It is an opportunistic infection for AIDs PT’s & leads to acute
pneumoniapneumonia
100100
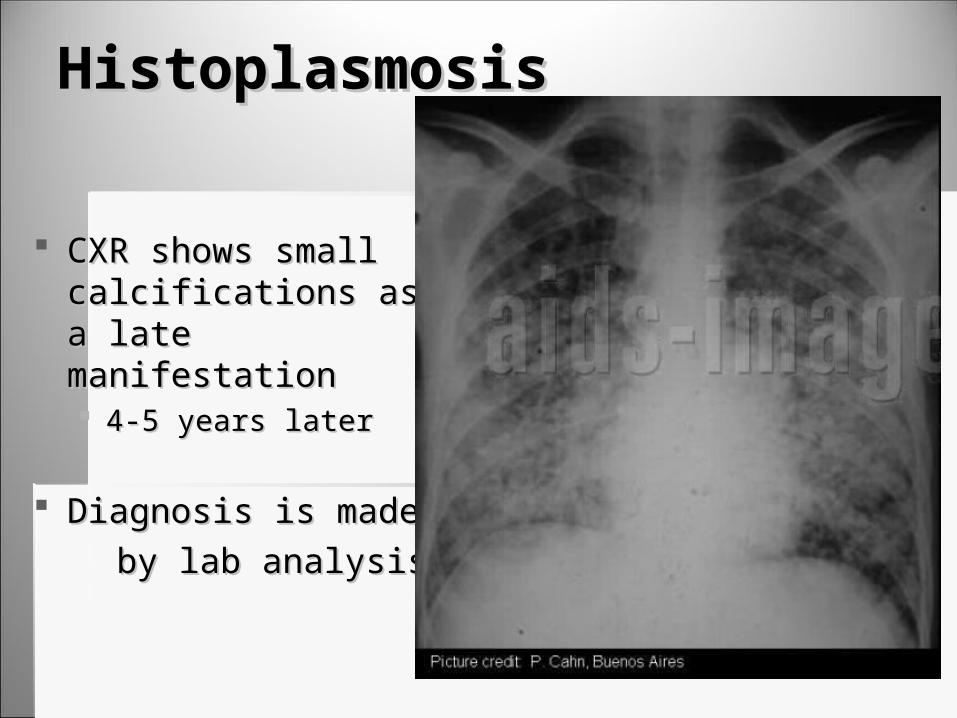
HistoplasmosisHistoplasmosis
CXR shows small CXR shows small calcifications as a late calcifications as a late manifestationmanifestation 4-5 years later4-5 years later
Diagnosis is madeDiagnosis is made by lab analysis by lab analysis
101101
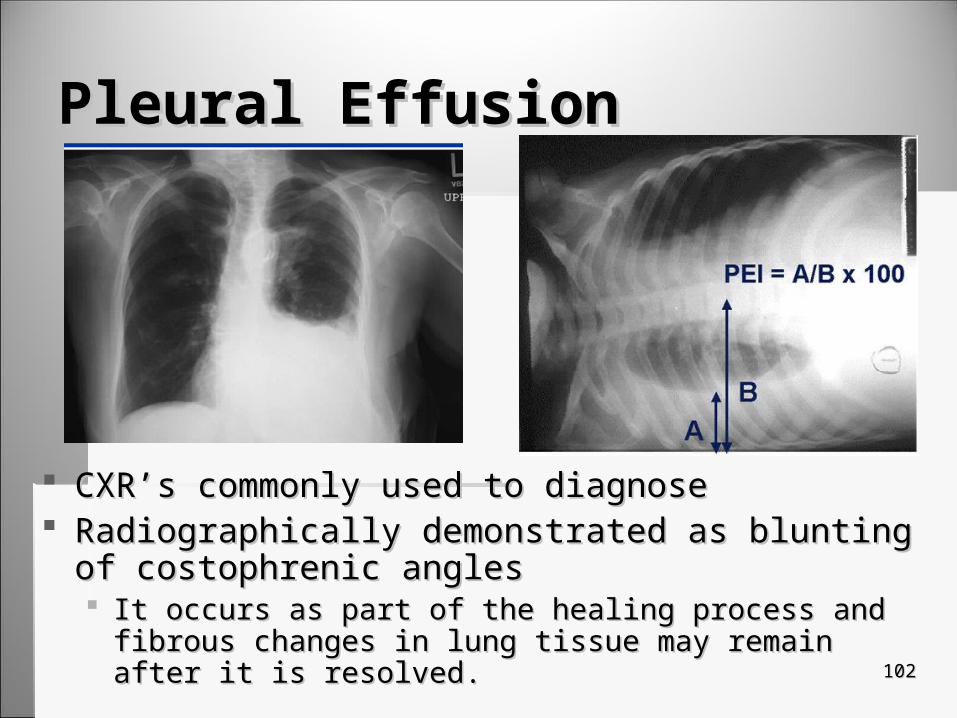
Pleural EffusionPleural Effusion
Results when excess fluid collects on pleural Results when excess fluid collects on pleural cavitycavity
Frequent manifestation of serious thoracic Frequent manifestation of serious thoracic diseasedisease Usually pulmonary or cardiacUsually pulmonary or cardiac It is a sign on an underlying conditionIt is a sign on an underlying condition
102102
Pleural EffusionPleural Effusion
CXR’s commonly used to diagnose CXR’s commonly used to diagnose Radiographically demonstrated as blunting of Radiographically demonstrated as blunting of
costophrenic anglescostophrenic angles It occurs as part of the healing process and fibrous changes in It occurs as part of the healing process and fibrous changes in
lung tissue may remain after it is resolved.lung tissue may remain after it is resolved.

103103
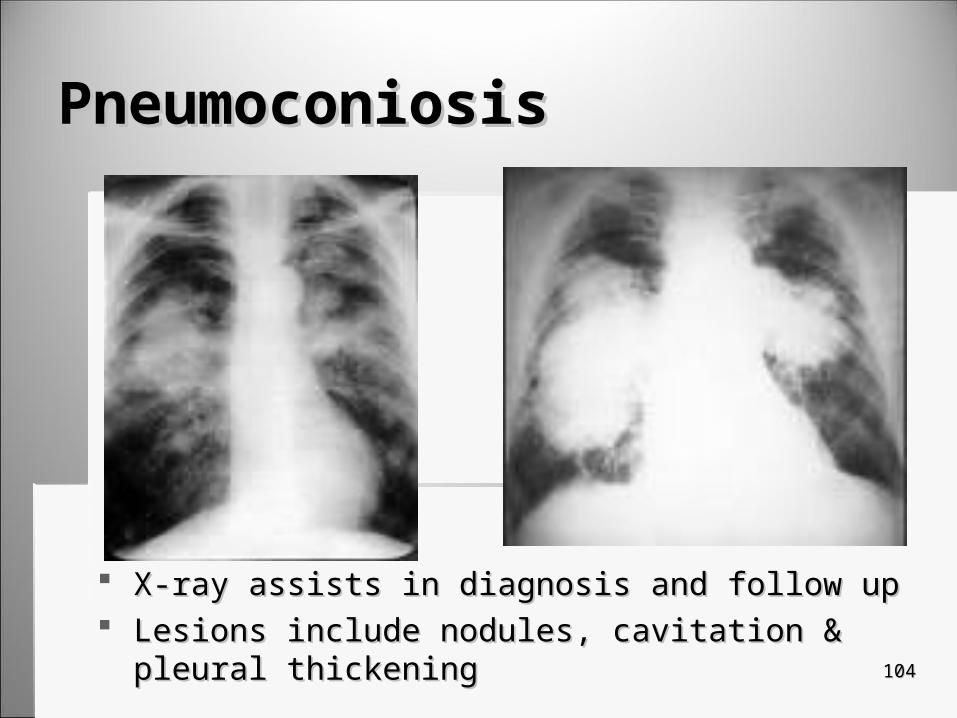
PneumoconiosisPneumoconiosis1.1. Occupational diseases in which inhalation of dust Occupational diseases in which inhalation of dust
in work environment causes pulmonary fibrosisin work environment causes pulmonary fibrosis
2.2. Exposure to substance must be in sufficient Exposure to substance must be in sufficient duration & host must be susceptibleduration & host must be susceptible
3.3. 3 types of pneumoconiosis:3 types of pneumoconiosis:1.1. SilicosisSilicosis2.2. AnthracosisAnthracosis3.3. AsbestosisAsbestosis
104104
PneumoconiosisPneumoconiosis
X-ray assists in diagnosis and follow upX-ray assists in diagnosis and follow up Lesions include nodules, cavitation & pleural thickeningLesions include nodules, cavitation & pleural thickening

105105
Asbestos PlaquesAsbestos Plaques
106106
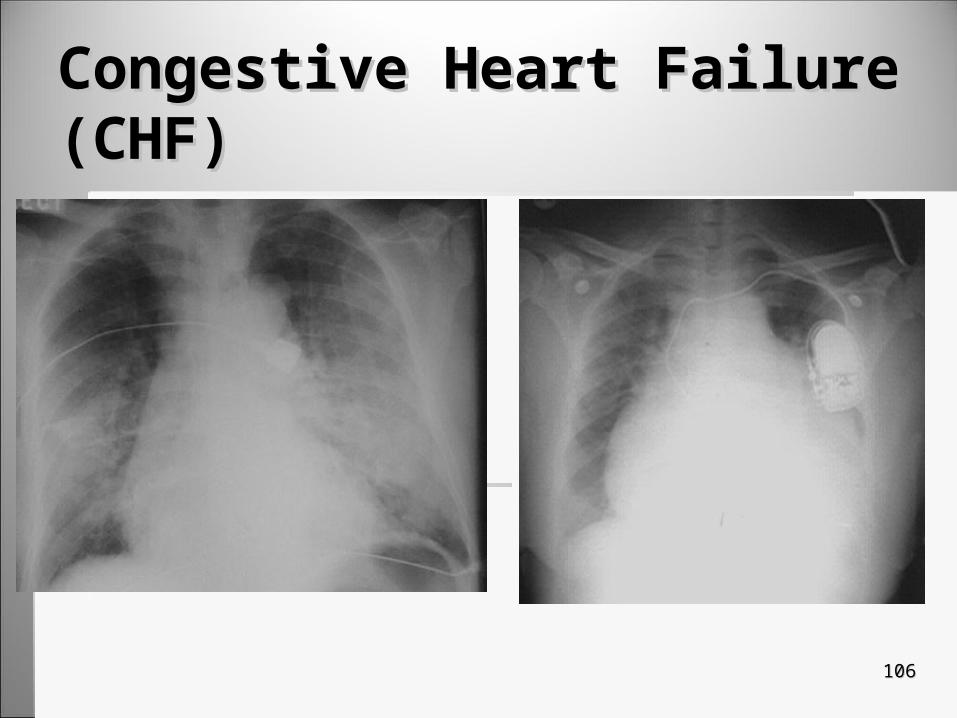
Congestive Heart Failure (CHF)Congestive Heart Failure (CHF)

107107
CTCT
Spiral CT has the advantage of imaging the entire Spiral CT has the advantage of imaging the entire chest with one breath holdchest with one breath hold Allows for better evaluation of the chest including Allows for better evaluation of the chest including
emboli detection.emboli detection.
Advances it CT allow high resolution, thin slices (1-Advances it CT allow high resolution, thin slices (1-1.5 mm), faster scan times in combination with 1.5 mm), faster scan times in combination with dynamic scanning. dynamic scanning.
Needle aspirations is commonly performed under Needle aspirations is commonly performed under CT guidance.CT guidance.

108108
Nuclear MedicineNuclear Medicine
Perfusion and ventilation scans are useful in Perfusion and ventilation scans are useful in evaluating chest disease in the case of obstructive evaluating chest disease in the case of obstructive disease and pulmonary embolidisease and pulmonary emboli
PET captures info regarding metabolic activityPET captures info regarding metabolic activity Because of cost constraints, PET is not currently Because of cost constraints, PET is not currently
consistently used in the staging of early ling cancersconsistently used in the staging of early ling cancers
Promising modality for the future especially when Promising modality for the future especially when combined with CTcombined with CT

















