40
Respiratory viruses (other than influenza virus)
| Date post: | 03-Jan-2016 |
| Category: |
Documents |
| Upload: | sharleen-richard |
| View: | 226 times |
| Download: | 1 times |
Respiratory viruses(other than influenza virus)

CDC/James Gathany

CDC/James Gathany
COMMON COLD
MOST COMMON CAUSES
RHINOVIRUSES
(MEMBERS OF THE PICORNAVIRIDAE)
- many other viruses as well

Respiratory viruses
• Paramyxoviridae (paramyxovirus family)
• HPIV 1-4– human parainfluenza virus
• RSV– respiratory syncytial virus
• hMPV– Human metapneumovirus
• Adenoviridae (adenovirus family)
• adenoviruses

GENUS GLYCOPROTEINS TYPICAL MEMBERS
Paramyxovirus HN, F HPIV1, HPIV3Rubulavirus HN, F HPIV2, HPIV4, mumps virusMorbillivirus H, F measles virus
Pneumovirus G, F respiratory syncytial virusMetapneumovirus G, F human metapneumovirus
PARAMYXOVIRUS SUBFAMILY
PNEUMOVIRUS SUBFAMILY
Paramyxoviruses – surface glycoproteins

M protein
helical nucleocapsid (RNA plusNP protein)
HN/H/G glycoprotein SPIKES
polymerasecomplex
lipid bilayer membrane
F glycoprotein SPIKES
Paramyxovirusespleomorphic

Parainfluenza Virus
• SS (-) RNA virus (15kb)
• 4 serotypes: 1, 2, 3, 4 (type 4 – 4a and 4b)

HPIV 1, 2, 3 and 4
• Infection– aerosol, person to person and fomites
• unstable, but can survive on surfaces for a few hrs
– highly contagious
– susceptible to soap and water /alcohol
– incubation 1-5 days

HPIV -disease
• URI - one of causes ‘common cold’ - congestion, headache, runny nose, fever, pharyngitis, croup
• LRI– Croup, bronchitis, bronchiolitis, pneumonia – serious disease due to HPIV in young children
• Elderly and IC – severe LRI• viremia is rare in HPIV.

Airway narrowing in croup

HPIV and croup
• laryngotracheitis or
laryngotracheobronchitis
• primarily in young - usually <6 yrs
• HPIV is most common cause of croup
• fever, cough, hoarseness
• outbreaks most often associated with
HPIV1 and HPIV2
• HPIV3 /4 – sporadic cases

HPIV – Lab diagnosis
• viral culture
- detect with IF
• Direct detection Ag /nucleic acids in resp. secretions– ELISAs or PCR
HPIV -Rx
• no antiviral therapy
• supportive
• usually self-limited

Epidemiology ”Iceberg phenomenon”
Classical disease presentation
Mild clinical disease
Asymptomatic infection but infectivity (+)

HPIV – Epidemiology
• restricted to humans, ubiquitous– most people have had all types of HPIV by 5yrs of
age
• reinfections throughout life– usually milder, may be symptomatic or asymptomatic
• antigenically stable

HPIV – prevention
• No vaccine
• Passive maternal antibodies may help in first few months
• Hand and surface hygiene

Respiratory syncytial virus

Respiratory syncytial virus
GENUS GLYCOPROTEINS TYPICAL MEMBERS
Paramyxovirus HN, F HPIV1, HPIV3Rubulavirus HN, F HPIV2, HPIV4, mumps virusMorbillivirus H, F measles virus
Pneumovirus G, F respiratory syncytial virusMetapneumovirus G, F human metapneumovirus
PARAMYXOVIRUS FAMILY SURFACE GLYCOPROTEINS
PARAMYXOVIRUS SUBFAMILY
PNEUMOVIRUS SUBFAMILY

• 2 major strains
– group A and group B (G protein differences)
Respiratory syncytial virus (RSV)

• infections– aerosol, person-to-person and fomites
• Can survive on inanimate surfaces for a few hrs
– virtually all children have been infected by 2yrs of age
• incubation period– a few days to a week
• infects respiratory epithelial cells – cell to cell spread
RSV infections

RSV- disease• common cause upper respiratory tract
infections– runny nose, cough, sore throat, headache, fever– co-infection with bacteria - rare – complications - otitis media (up to 40%)
• 25% of primary infections result in LRI
– bronchiolitis, viral pneumonia
RSV- risk factors for severe disease
• Age (especially if less than 6 months)
• Pre-term birth
• Preexisting respiratory conditions
• Immunodeficiency

RSV – Lab diagnosis
• rapid antigen assay – ICT
• Virus isolation – cell culture
• PCR – especially useful in older children and adults when
viral load is usually lower and so antigen detection or viral isolation less reliable
• serology– used for epidemiology ; not diagnosis

RSV- Rx
• no specific antivirals
-ribavirin- not used routinely, may be considered in life threatening situations
• supportive care

RSV- prevention
• No vaccine
• Passive immunization– for high-risk children – monoclonal antibody against F protein– monthly IM injections during the RSV season– not effective in treatment of infection
RSV- prevention
• Hand and surface hygiene
• Nosocomial infections common– need to be especially rigorous when high risk patients
involved • pediatric wards, neonatal units, transplantation
units, etc.• gloves, gowns, masks, goggles; isolation

Human metapneumovirus (hMPV)
GENUS GLYCOPROTEINS TYPICAL MEMBERS
Paramyxovirus HN, F HPIV1, HPIV3Rubulavirus HN, F HPIV2, HPIV4, mumps virusMorbillivirus H, F measles virus
Pneumovirus G, F respiratory syncytial virusMetapneumovirus G, F human metapneumovirus
PARAMYXOVIRUS FAMILY SURFACE GLYCOPROTEINS
PARAMYXOVIRUS SUBFAMILY
PNEUMOVIRUS SUBFAMILY

Human metapneumovirus (hMPV)
• only recently (2001) recognized
• common – probably 15% of childhood colds– commercial tests only recently available

hMPV- Disease
• Disease - similar to RSV/ HPIV
• most children infected by age 5
• reinfections common
• upper respiratory tract - common cold, croup• lower respiratory tract - bronchiolitis /pneumonia
(especially in infants)

hMPV - epidemiology
• Worldwide
• humans only source of infection
• Not fully understood
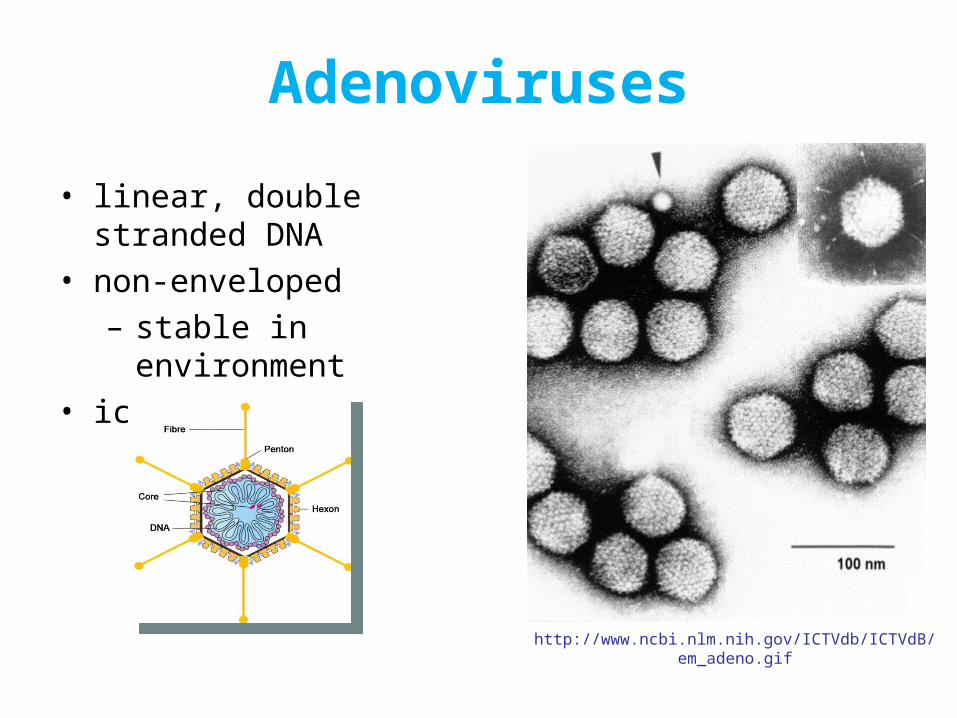
Adenoviruses
http://www.ncbi.nlm.nih.gov/ICTVdb/ICTVdB/em_adeno.gif
• linear, double stranded DNA • non-enveloped
– stable in environment• icosahedral
• Fiber protein – virus attachment protein
- determines host cell specificity
• Infect epithelial cells lining the mucus membranes– respiratory, GI, urinary tract– enter via epithelium, replicate and spread to lymphoid
tissue
• Viremia occurs• Secondary involvement of viscera
Adenoviruses - pathogenesis

• Acute infection
• latent/occult– virus remains in cell – seen in lymphoid tissue
• oncogenic transformation (animals only)
Adenoviruses - pathogenesis

Human Adenoviruses
• 51 human serotypes (1-51)
• Classified into six subgroups (A-F)
• members of a subgroup often cause similar spectrum of disease
– enteric adenoviruses are in subgroup F (40,41)
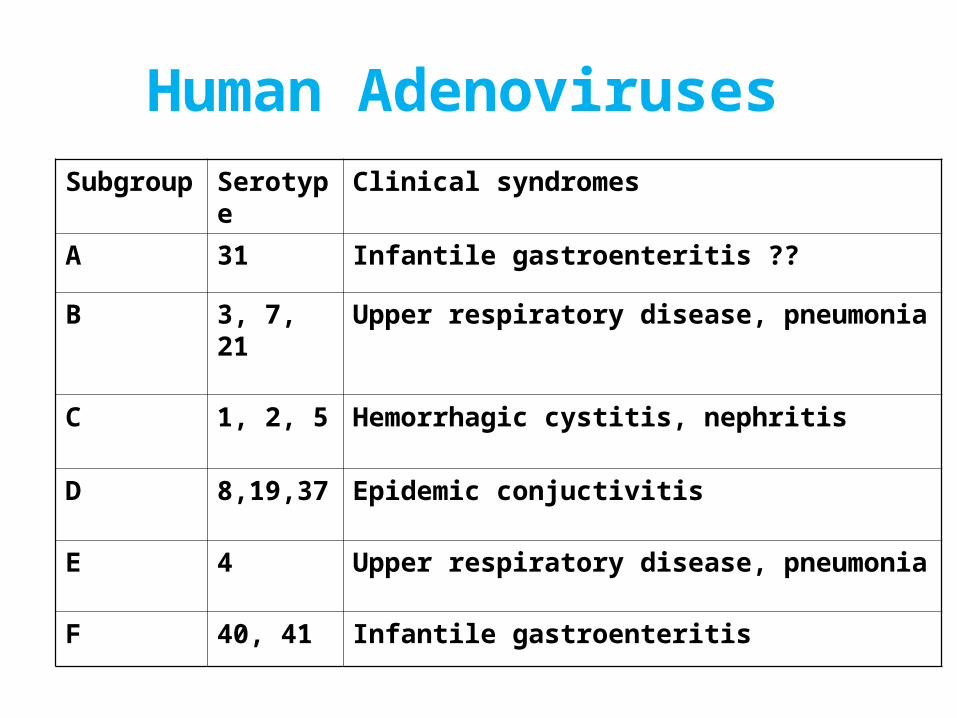
Human AdenovirusesSubgroup Serotype Clinical syndromes
A 31 Infantile gastroenteritis ??
B 3, 7, 21 Upper respiratory disease, pneumonia
C 1, 2, 5 Hemorrhagic cystitis, nephritis
D 8,19,37 Epidemic conjuctivitis
E 4 Upper respiratory disease, pneumonia
F 40, 41 Infantile gastroenteritis

Human adenoviruses Transmission
• aerosols, fomites
• Secretions – respiratory, tears, fecal/oral

Human adenoviruses- infection and virus shedding
• incubation – up to a couple of weeks
• virus shedding usually highest during acute phase– may continue to shed at lower levels for a long
time (months)– high rate of transmission to other family members
(up to 50%)

Human adenovirusesDisease
• LRI
• URI
• Diarrhea
• Conjunctivitis
• Cystitis

Adenovirus infections in Immunocompromised hosts
• Disseminated, severe and often fatal infections
• New infection
• Reactivation of latent virus
• Prolonged infections with prolonged viremia and
viral shedding

Human adenoviruses Lab diagnosis
• antigen testing in body fluids - very rapid
• cell culture
• PCR

















