Rethinking the Tools in the Toolbox? Evidence-Based Strategies to "Move Forward" in Neurological Rehabilitation T. George Hornby, PT, PhD, Indiana University, Indianapolis, IN Lindsay H. Shoger, PT, Rehabilitation Hospital of Indiana Jennifer K. Lotter, PT, Rehabilitation Hospital of Indiana
Transcript
Rethinking the Tools in the Toolbox? Evidence-Based Strategies to "Move
Forward" in Neurological Rehabilitation
T. George Hornby, PT, PhD, Indiana University, Indianapolis, IN
Lindsay H. Shoger, PT, Rehabilitation Hospital of Indiana
Jennifer K. Lotter, PT, Rehabilitation Hospital of Indiana
Neuropt list-serve - when to integrate traditional techniques/derivatives (Neuro-IFRAH) into PT neurologic education
2009 – JNPT President’s Perspective
Initial translation of early scientific work was important in development of neurological PT (NDT, PNF, Brunstromm)
Evolution of neurologic PT influenced by scientific advances –STEP conferences - how current science influences practice??
Continued use of traditional theories without considering more recent findings would not be exemplar of evidence-based practice
… time to let go . . .
III Step Roadmap - Apply neuroplastic
principles - Define dosage
parameters- Use relevant
outcomes- Translate science to
practice
“Why do we need to change our approaches? . . . current approaches are not adequate. . . assumptions do not fit current knowledge”
“Therapist are dissatisfied with traditional models …. . . looking for new models based on more recent
discoveries/new understandings of motor control”
1990’s - Challenging traditional models of neurologic physical therapy
“Why do we need to change our approaches? . . . current approaches are not adequate. . . assumptions do not fit current knowledge”
“Therapist are dissatisfied with traditional models …. . . looking for new models based on more recent
discoveries/new understandings of motor control”
1990’s - Challenging traditional models of neurologic physical therapy
We can facilitate normal movement by applying specific
sensory stimulation.
Common assumptions?
Need to inhibit abnormal movement/abnormal reflexes
Recovery follows predictable sequence . . . mimics normal
development
“Why do we need to change our approaches? . . . current approaches are not adequate. . . assumptions do not fit current knowledge”
“Therapist are dissatisfied with traditional models …. . . looking for new models based on more recent
discoveries/new understandings of motor control”
1990’s - Challenging traditional models of neurologic physical therapy
Increasing importance of neurologic rehabilitation
Why change? Why the dissatisfaction?
Advances in science
Lack of functional carry-over of facilitation approaches
Normal science
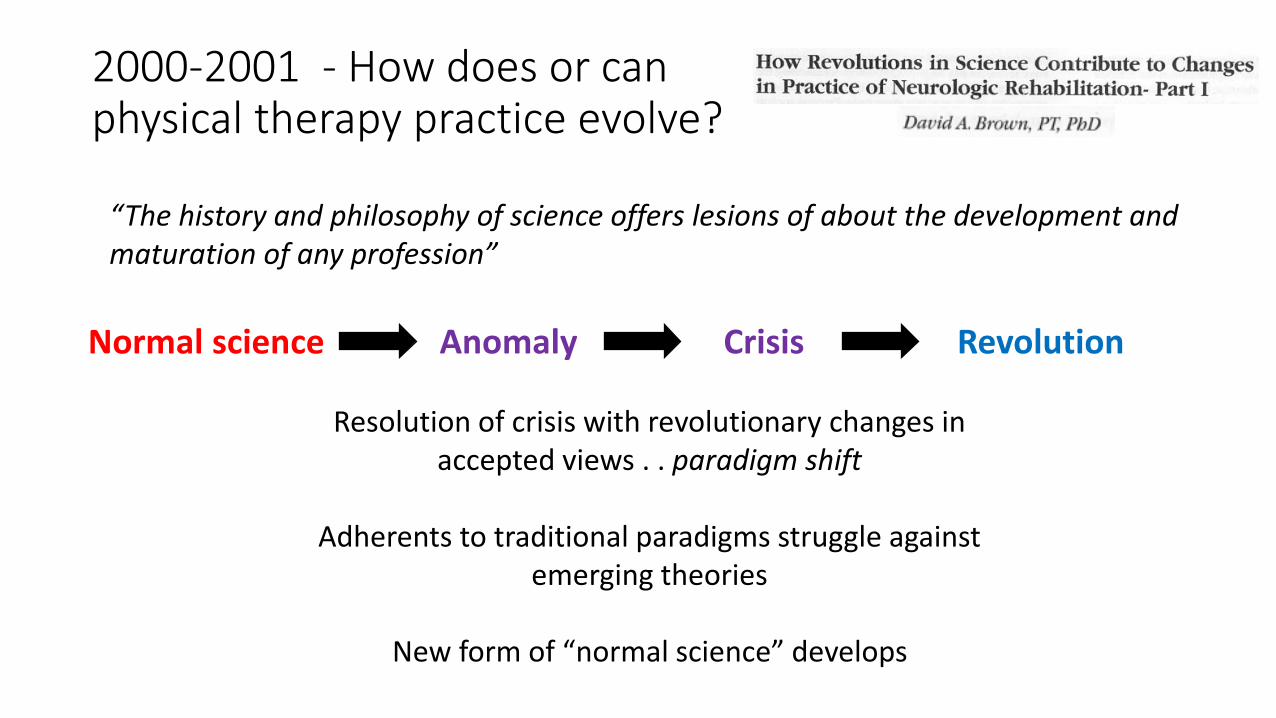
2000-2001 - How does or can physical therapy practice evolve?
Research based on past achievements . . . agreement about basic foundations for practical application
Research accumulates to validate specific theoretical foundations/paradigms
Characterized by adherent supporters for prevailing views/against competing alternative views
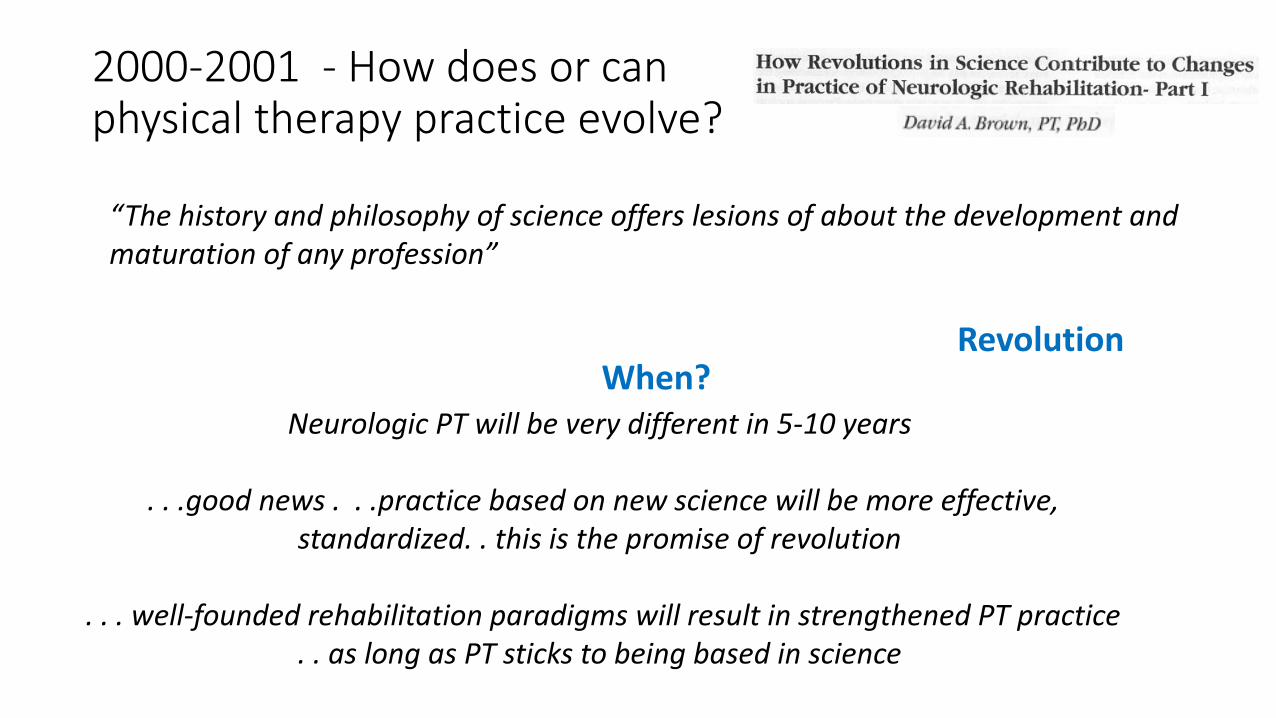
“The history and philosophy of science offers lesions of about the development and maturation of any profession”
Normal science Anomaly
2000-2001 - How does or can physical therapy practice evolve?
Discovery of violations to accepted paradigms, testing/violating prevailing views
Encounters significant resistance from adherents to existing paradigms
“The history and philosophy of science offers lesions of about the development and maturation of any profession”
CrisisNormal science Anomaly
Repeated occurrence of anomalous observations
Professional insecurity/failure of existing paradigms prelude to search for new ones
Proliferation of versions of theories
Crisis
2000-2001 - How does or can physical therapy practice evolve?
“The history and philosophy of science offers lesions of about the development and maturation of any profession”
Crisis
Resolution of crisis with revolutionary changes in accepted views . . paradigm shift
Adherents to traditional paradigms struggle against emerging theories
New form of “normal science” develops
2000-2001 - How does or can physical therapy practice evolve?
“The history and philosophy of science offers lesions of about the development and maturation of any profession”
RevolutionCrisisNormal science Anomaly
Revolution
Neurologic PT will be very different in 5-10 years
. . .good news . . .practice based on new science will be more effective, standardized. . this is the promise of revolution
. . . well-founded rehabilitation paradigms will result in strengthened PT practice . . as long as PT sticks to being based in science
When?
2000-2001 - How does or can physical therapy practice evolve?
“The history and philosophy of science offers lesions of about the development and maturation of any profession”
In 5-10 years . . .
Response?
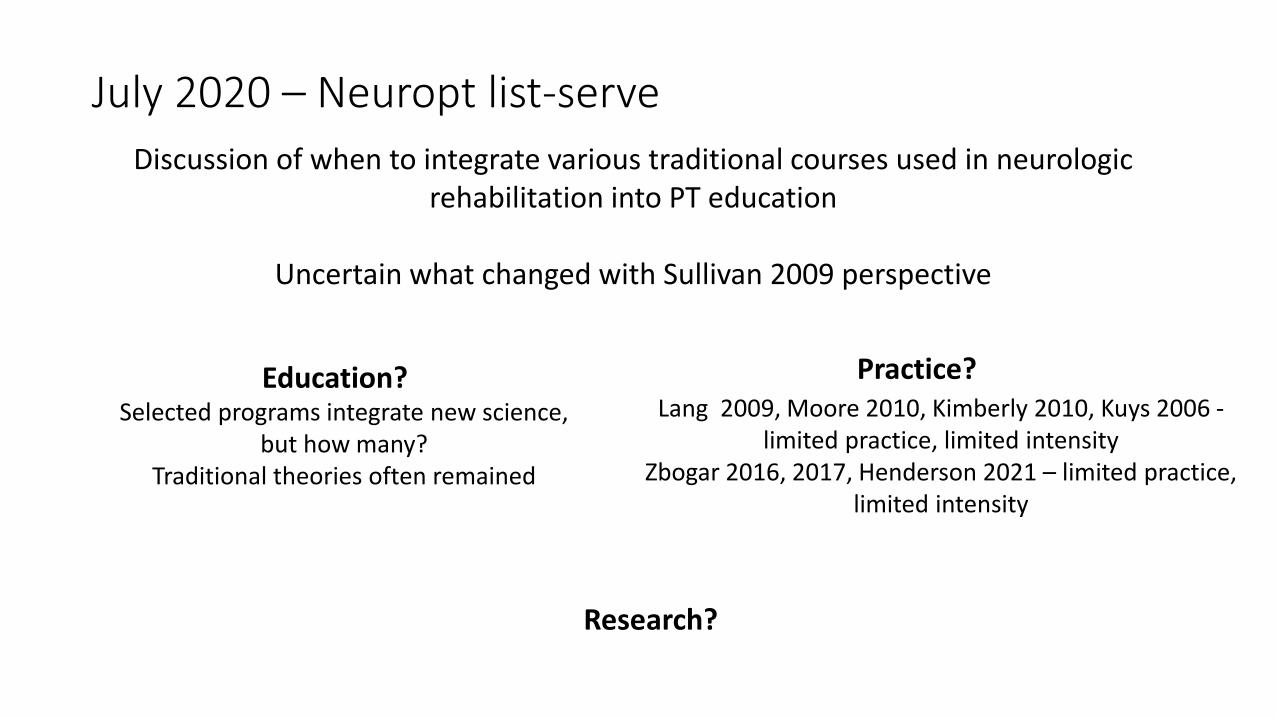
Discussion of when to integrate various traditional courses used in neurologic rehabilitation into PT education
Uncertain what changed with Sullivan 2009 perspective
July 2020 – Neuropt list-serve
Education? Selected programs integrate new science,
but how many? Traditional theories often remained
Practice? Lang 2009, Moore 2010, Kimberly 2010, Kuys 2006 -
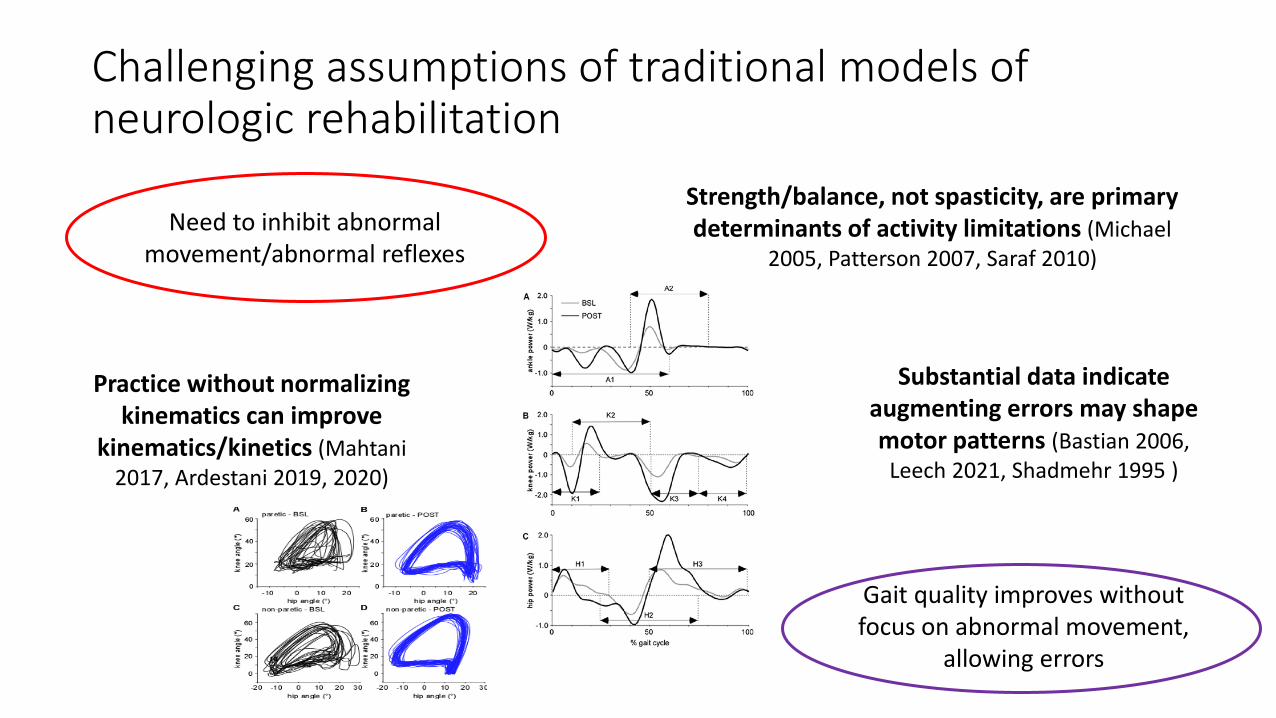
Substantial data indicate augmenting errors may shape motor patterns (Bastian 2006,
Leech 2021, Shadmehr 1995 )
Gait quality improves without focus on abnormal movement,
allowing errors
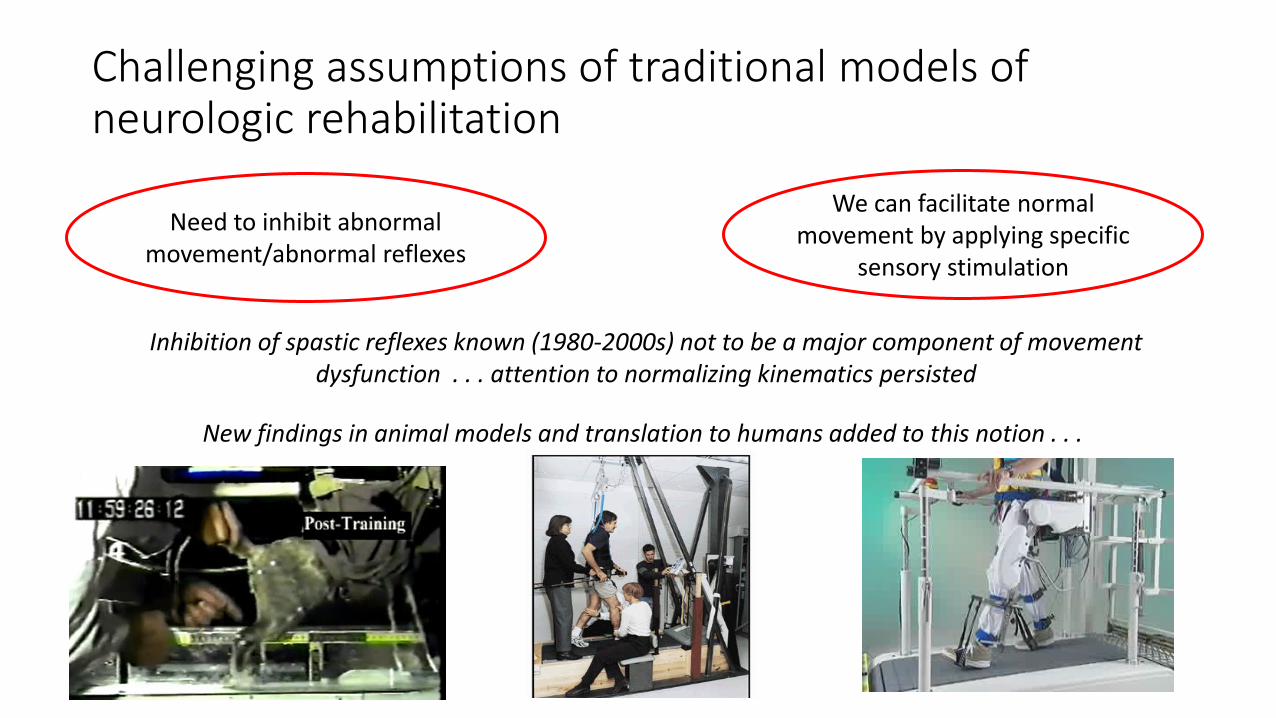
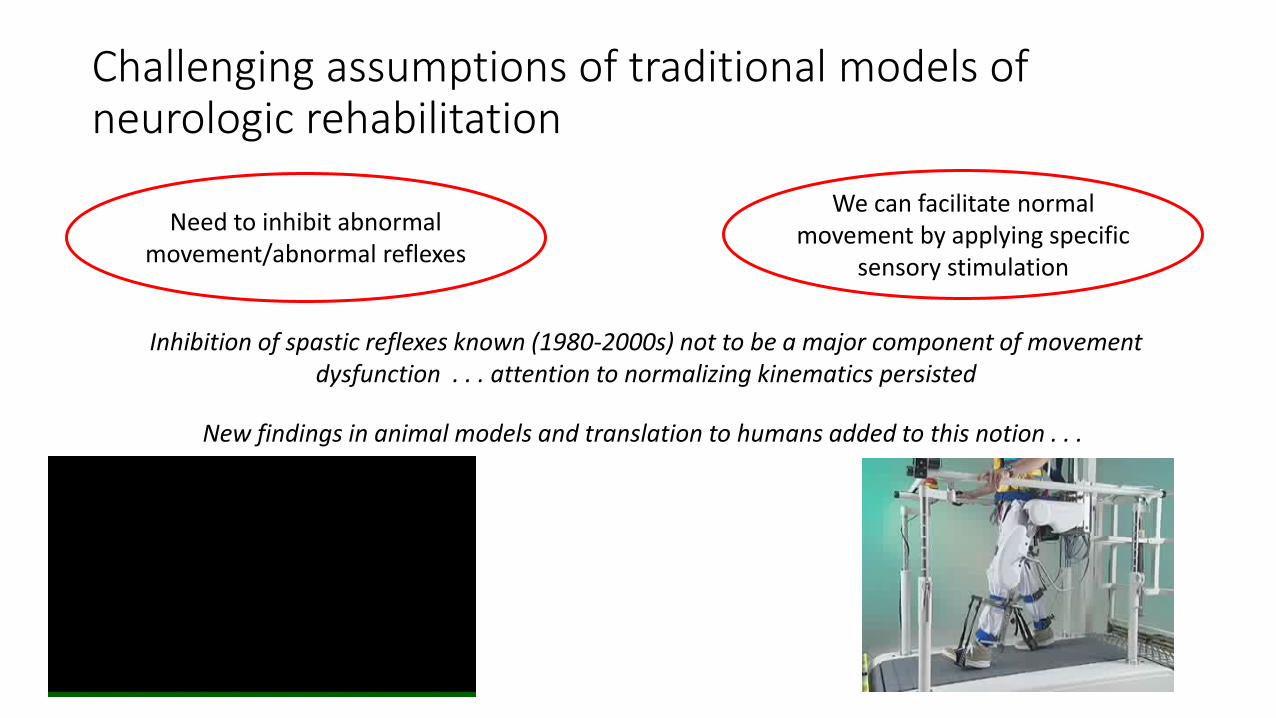
Need to inhibit abnormal movement/abnormal reflexes
Challenging assumptions of traditional models of neurologic rehabilitation
We can facilitate normal movement by applying specific
sensory stimulation
Inhibition of spastic reflexes known (1980-2000s) not to be a major component of movement dysfunction . . . attention to normalizing kinematics persisted
New findings in animal models and translation to humans added to this notion . . .
Need to inhibit abnormal movement/abnormal reflexes
Challenging assumptions of traditional models of neurologic rehabilitation
We can facilitate normal movement by applying specific
sensory stimulation
Inhibition of spastic reflexes known (1980-2000s) not to be a major component of movement dysfunction . . . attention to normalizing kinematics persisted
New findings in animal models and translation to humans added to this notion . . .










![RETHINKING EXPERT OPINION EVIDENCE...2017] Rethinking Expert Opinion Evidence 971 secondly, the opinion must be ‘wholly or substantially based on that knowledge’.18 Despite the](https://static.documents.pub/doc/80x56/5e5617ee1945e55d0a3aded9/rethinking-expert-opinion-evidence-2017-rethinking-expert-opinion-evidence.jpg)
















