Rethinking the Way We Deliver Addiction Treatment to Women Fostering Recovery through Empowerment and a Customer Focus Carla A. Green, Ph.D., MPH Center for Health Research, Kaiser Permanente Northwest Women’s Alliance to Strengthen Treatment and Retention Substance Abuse Treatment and Recovery Conference September 17, 2007
Transcript
Rethinking the Way We Deliver Addiction Treatment to Women Fostering Recovery through Empowerment
and a Customer FocusCarla A. Green, Ph.D., MPH
Center for Health Research, Kaiser Permanente NorthwestWomen’s Alliance to Strengthen Treatment and Retention Substance Abuse Treatment and Recovery Conference
September 17, 2007
2
Background: What we know about women and substance abuse treatment
Over their lifetimes, women with substance problems are less likely to seek treatment than men
Women experience more barriers to treatment entry and to staying clean and sober than men because they: Lack social support from those in their networks Experience more negative influences from drug-using
romantic partners Are more likely to live in poverty Have more responsibilities for children and childcare Have more mental health problems Have greater needs for weekend and evening services
Greenfield, S.F., Brooks, A.J., Gordon, S.M., Green, C.A., Kropp, F., McHugh, R.K., Lincoln, M., Hien, D, & Miele, G.M. (2007). Substance abuse treatment entry, retention, and outcome in women: A review of the literature. Drug & Alcohol Dependence, 86, 1-21
3
What we know about women and substance abuse treatment (continued)
Women are more likely to seek treatment in non-specialty addiction treatment settings
Some subgroups of women may need specially designed services Older women Women from specific ethnic or minority groups Women in the perinatal period Women with eating disorders Women who are victims of violence
Once in treatment, women do as well as or better than men For these reasons getting them in is critical
4
Background: Myths(1) that Affect Approaches to Substance Abuse Treatment for Women
Myth: Drug addiction is voluntary Reality: Because drug use starts as a voluntary activity
we forget that substances change us physiologically What was once voluntary becomes involuntary and
compulsive Reality: Environment is critical in acquiring addictions
and in the relapse process Stresses and strains can affect use and relapse
Women experience more because of poverty and child-rearing Drug use in social networks can be hard to resist
Women are influenced more than men by loved ones who use or continue to use
Women have less social support for entering and continuing in treatment
(1)Adapted from Leshner, A.I. (1999) Principles of Drug Addiction Treatment: A Research-Based Guide. National Institute on Drug Abuse, National Institute of Health
5
Effects of believing, even in small ways, that addiction is voluntary
We treat people with addictions differently than we treat people with other conditionsThis is stigmatizing
We blame them for relapsing We deny treatment following relapseWe deny treatment because of poor treatment
complianceWomen may be more sensitive to these
stigmatizing experiences
6
Myths & Their Effects (continued)
Myth: Drug addiction results from poor character
Reality: Addiction changes behavior because it changes brain functioning We perceive these changes as changes in
character that are permanent, but character is not fixed
Current character is not past character, nor is it future character
Negative effects in treatment settings Punitive approaches, including shaming for past
behaviors and for relapses Again, women may be more sensitive to these
experiences
7
Myths & Their Effects (continued)
Myth: You have to want drug treatment for it to be effective
Reality: People who are pressured to attend treatment do at
least as well, if not better, than others in treatment Many who are not sure about treatment can be
engaged and will enter treatment if properly approached
Forcing people to overcome barriers to accessing treatment does produce a group that is selected for the greatest motivation, BUT
Keeps others out of treatment—many of them women Those who are less assertive Those who have more life-related barriers to overcome
8
Myths & Their Effects (continued)
Negative effects in treatment settingsWe deny treatment unless people prove that
they “really” want it (e.g., we make them call every day or every week until an opening is available)
We don’t design treatment programs to draw people in, rather
We make it difficult to find out about services (what is your program’s telephone system like?)
We limit access (how long is your waiting list?)
9
Results of these myths on women
Women seek care in settings that aren’t equipped to treat addictions (e.g., psychiatric settings)
Women avoid treatment overall Women who try to seek care may not be able to
attend because Care is not available when they are Services that meet their needs are not available
Child care Transportation Mental health services
10
An Alternative Approach?
Focus on the customer and personal empowerment Person-centered, collaborative care improves
outcomes for chronic conditions Empowering women in clinical settings may help
them develop better control and power in the rest of their lives
As women’s personal control and power increase, women will be more likely to
Overcome the barriers they experience to staying clean and sober
Improve their quality of life, thus reducing the risk of relapse
11
An Alternative Approach (continued)
Learning from other fields and areas to inform our approach and improve treatment access and treatment experiences:
Stress processes and stress management Happiness and quality of life research Effects of environment on behavior Developmental processes, including adult learning Identity, healing, and adaptation to chronic illness Motivation Consumer empowerment and collaborative care Process improvement for businesses
Normal growth & development can be disrupted by substance abuse and mental health problems, but they still continue Individuals are learning and adapting, even
when it doesn’t seem that they arePeople often need to learn from multiple
modalities (from others, visually, by trying it out, from books)
People often need to try things multiple times—each episode of treatment, each relapse, is an opportunity for learning
Adaptation is the behavioral manifestation of learning, development, and personal growth In addiction treatment
We are teaching methods for adapting to and maintaining a drug-free lifestyle
But if this is all, it isn’t enough Life must be more than the absence of addiction
We need to help people catch up when their development has been disrupted and to move toward a life that is rewarding to them
17
Processes of Adaptation to Chronic Illnesses
Can research on adapting to chronic illness inform our understanding of recovery from addictions? Common responses to initial illness symptoms,
receiving diagnoses, and functional limitations/impairments results in complicated processes of:
DenialAcceptance IdentificationAdaptation
18
Adapting to chronic illness People with chronic illnesses often:*
Distance themselves from their illness and diagnoses Deny that they have a serious illness Deny that their illness is chronic Begin to recognize that their bodies are altered and accept their illness
as real, allowing them to account for symptoms and life changes Feel estranged from the person they have become, betrayed by their
own bodies, or guilty for not meeting normal standards for activities, functioning or appearance.
Learn about the chronicity of their illness and its effects on daily life as they deal with symptoms and repeated acute crises
Compare their present condition with their past condition, weigh the risks of continuing regular activities, then alter those activities
Become immersed in their illness Eventually find ways to take stock, embrace their illness, recover a
sense of a valuable self, and achieve a better quality of life
*from Charmaz,1991;1994;1995;1999;2000)
19
Implications for Substance Abuse Treatment
Treatment may need to target specific developmental tasks Particularly if substance abuse began before reasonable adult
functioning was established
Denial may be a normal part of the process of adaptation to having a chronic, stigmatized problem Helping clinicians and families reframe denial as a normal part of
adaptation may reduce stigma and negative assessments
“Addict” or “alcoholic” identities may be a critical step in learning about what it means to have a chronic substance abuse problem We can recognize this as an important step in the healing
process, then help people move beyond this stage
20
Implications for Substance Abuse Treatment
Timing of particular treatment efforts should depend on where an individual is in this (non-linear) adaptation process We do this to some extent with:
Motivational enhancement Stage of change approaches, and Stepped care, but
More comprehensive, whole-person, approaches could help us target individuals’ specific needs when they are needed
For example, if a woman can’t leave an unhealthy home environment without a job, the most important way to support recovery might be vocational rehabilitation
21
Facilitating Adaptation: Sources of Motivation
Environment
Resources Strains
Recovery Processes:Development
Learning Healing
Adaptation
Sources of Motivation:
HopeOptimism Meaning
Capacity:Competence Dysfunction
Prerequisites for Action:
AgencyControl
Autonomy
22
Hope, Optimism, Meaning
People need to have hope that they can recoverbe optimistic that they can build, rebuild, and
maintain a meaningful lifehave some source of meaning in their lives
SpiritualClose relationships (often disrupted by substance
abuse)Activities—work, school, volunteer, family,
hobbies
23
Implications for Substance Abuse Treatment Current system characteristics can undermine
hope and optimism Long waiting lists Poor coordination of care for those with medical or
mental health problems, or those transitioning from detox
The more complex the problems, the more likely care will be fragmented
The more fragmented the care, the more likely these most vulnerable people will fall through the cracks
High staff turnover/low continuity of care Continuity of care is critical in developing the kind of collaborative
clinician-client alliances that are necessary to foster the kind of trust and hope that support good disease management
24
Implications for Substance Abuse Treatment
To foster hope for recovery, we need toLearn to coordinate services for people who
need them Improve access to careWork to keep treatment staff to improve
continuity of care so that clients can build relationships with clinicians
Help clients carefully time the introduction or reintroduction of meaningful activities to improve their quality of life
25
Prerequisites for Action
Environment
Resources Strains
Recovery Processes:Development
Learning Healing
Adaptation
Sources of Motivation:
HopeOptimism Meaning
Capacity:Competence Dysfunction
Prerequisites for Action:
AgencyControl
Autonomy
26
Agency, Control & Autonomy To recover, each person must be able to
Envision a goal Set priorities among possible actions and goals Plan methods of achieving those actions or goals Act in concert with those plans
Substance abuse problems interfere with agency—the ability to progress through these steps
Incarceration, legal or other mandates, and strict treatment program regulations, can interfere with the control & autonomy necessary for action
Agency is also necessary for managing any chronic illness
27
Agency
Agency should be seen as a strength that can be developed, or attenuated, over time Agency is affected by experiences and outcomes
Successes increase agency (and hope) Lack of control, autonomy, or opportunity can Failures interfere with agency (and hope)
Thwart the best-constructed plans of a motivated actor Reduce hope and optimism for the future
Agency can be rebuilt, even if a person starts with responsibility for only micro-level decisions
(from Davidson & Strauss)
28
Implications for Substance Abuse Treatment & Research
Collaborative relationships with clinicians & counselors provide the foundation for developing agency These relationships require
client empowerment consumer involvement in program development and
evaluation
We also need to find ways to reconcile client-centered and client-directed treatment with evidence based practices and manualized approaches
29
Capacity: Competence & Dysfunction
Environment
Resources Strains
Recovery Processes:Development
Learning Healing
Adaptation
Sources of Motivation:
HopeOptimism Meaning
Capacity:Competence Dysfunction
Prerequisites for Action:
AgencyControl
Autonomy
30
Competence & Dysfunction
Recovery must build on competencies Taking stock of strengths and weaknesses is part
of the process of adapting to chronic illness
When functioning is limited, clinicians & clients can become overly focused on dysfunction and risk, missing strengths & desires that: Improve motivation Increase hope Lead to meaningful activities
31
Competence & Dysfunction
Balancing risks while continuing to progress is difficult work People often overextend, relapse, then
try againUsing a chronic disease, collaborative,
framework facilitates learning, personal empowerment, and return to treatment following relapse
32
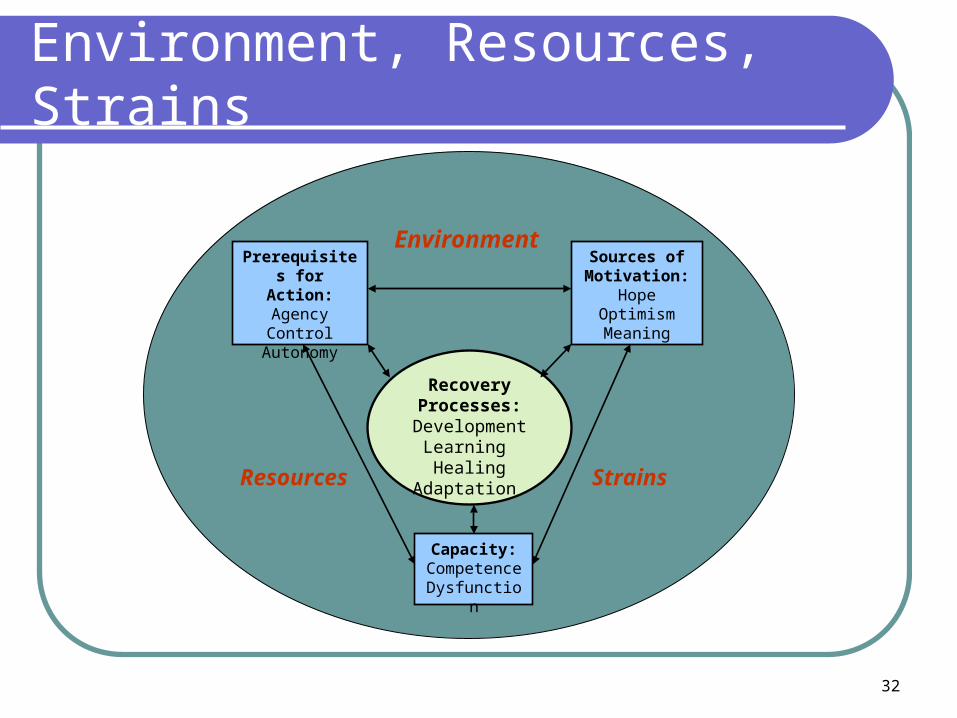
Environment, Resources, Strains
Environment
Resources Strains
Recovery Processes:Development
Learning Healing
Adaptation
Sources of Motivation:
HopeOptimism Meaning
Capacity:Competence Dysfunction
Prerequisites for Action:
AgencyControl
Autonomy
33
Environment, Resources, Strains
Provide the context in which recovery occursBroad & pervasive
Financial Emotional OpportunitiesStigma & discriminationSubstance abuse treatment & mental health care
can be resources or strains This depends on how care is organized, delivered, and
financed
34
Resources & Strains Strains result from resource loss Stress resistance is bolstered by resources &
resource gains Resources of one kind can offset resource loss of
another kind Loss spirals can occur when resources are so low
that stores aren’t adequate to offset losses Losses, and investments that do not pay off, can
lead to demoralization, low self-esteem, depression, loss of hope
(adapted from Hobfall)
35
Implications for Substance Abuse Treatment & Research Individuals with substance abuse and mental
health problems are at increased risk of resource loss
We know little about preventing resource loss, or helping people to maintain resources We often rely on “low turning points” or “hitting bottom”
to enhance motivation Need to learn how to intervene effectively before
devastating losses occur Addressing other strains may free up energy for
recovery
36
Implications for Substance Abuse Research & Treatment
Early treatment could include resource loss prevention to:Help to engage the client in treatment by
addressing issues that s/he sees as important
Employment problemsFamily problems etc.
Prevent losses that make recovery more difficult
Increase resources that facilitate recovery
37
Learning from process improvement
Personal empowerment, agency, and control can also be enhanced when treatment agencies adopt a customer focus
Process improvement techniques, including walk-through exercises can: help identify agency characteristics and processes that are
cumbersome, frustrating, or demoralizing for clients and staff help agencies streamline procedures to reduce staff workload
and improve client experiences improve the work environment and staff worklife, reducing
turnover improve client access and retention, and therefore, the bottom
line
38
Conclusions
Adopting an approach that focuses on empowering clients and addressing their individual needs has the potential to: Improve access and retention in treatment,
particularly for women Improve long-term outcomes Increase treatment agency capacity Improve the quality of staff’s work and the