56
1 REVALIDATION GUIDANCE FOR PSYCHIATRISTS Version 2 Dr Laurence Mynors-Wallis Registrar December 2011
1
REVALIDATION GUIDANCE
FOR
PSYCHIATRISTS
Version 2
Dr Laurence Mynors-Wallis Registrar
December 2011
2
The Royal College of Psychiatrists is the professional and educational body for psychiatrists in the United Kingdom. It has been in existence in some form since
1841, receiving a Supplemental Charter to become the "Royal College of Psychiatrists" in 1971.
The College has some 15000 members worldwide. The majority of members are based in the UK where there are six psychiatric specialties and three sub-
specialties.
Trainees in psychiatry are the third largest group of medical trainees in the UK; they will revalidate through the Deanery processes. Psychiatrists not in training in the UK will need to follow the guidance in this report.
Psychiatrists working outside the UK will need to revalidate if they wish to retain
their licence to practise. They will need to follow the recommendations in this report but should consult the General Medical Council about who their
Responsible Officer will be.
Citation for this document: Royal College of Psychiatrists. Revalidation
Guidance for Psychiatrists. London: Royal College of Psychiatrists, 2011.
Royal College of Psychiatrists
17 Belgrave Square, London SW1X 8PG
www.rcpsych.ac.uk
3
Contents
Introduction 4
College Aims of Revalidation 4 How Psychiatrists will be able to evidence meeting revalidation standards 5
Evidence that will be reviewed at appraisal
- General information 9 - Quality improvement activity 11 - Case based discussion 12
- Clinical audit 13 - Clinical outcome measures 14
- Multisource feedback – colleagues 15 - Patient feedback 16 - Continuing professional development 17
- Review of significant events 18 - Review of complaints and compliments 19
Other Revalidation Issues
- Non-clinical Practice 21 - Academic Practice 22 - Research 23
- Teaching 23 - Private and Independent Practice 24
Responsible Officers 25
Remediation 28
Electronic Portfolio 29 Frequently asked questions 30
Summary of process 33
References 34
Appendix A – Summary of Supporting Information 36 Appendix B – Case Based Discussion Sheet 48
Appendix C – Guidance for Case Based Discussion 50 Appendix D – Criteria and Indicators of Best Practice in Clinical Audit 51 Appendix E – Audit Proforma 52
Appendix F – Multisource Feedback Colleague Structured Reflective Template 53 Appendix G – Multisource Feedback Patient Structured Reflective Template 54
Appendix H – Significant Event Structured Reflective Template 55 Appendix I – Complaint Report Structured Reflective Template 56
4
Introduction
Revalidation is the process by which licensed doctors will demonstrate to the
General Medical Council (GMC) that they are up to date and fit to practise and
that they are complying with the relevant professional standards. This
document has been updated from Version 1 to reflect current GMC Guidance1.
revalidation is expected to begin in late 2012.
College Aims of Revalidation
The College aims of revalidation are:-
Revalidation must command the confidence of patients, the public and
the profession.
Revalidation should facilitate improved practice for all members and
fellows.
The process should identify those whose practice falls below acceptable
standards and give advice and monitoring to allow revalidation to be
reconsidered. There should be early warning of potential failure so
remedial action can be taken.
The process should allow those who are working to college standards
to revalidate without undue difficulty or stress.
There must be equity across the specialty, independent of differing
areas of practice, working environments and geographical location.
Revalidation should be affordable and flexible, starting simple to allow
further development.
The process should incorporate as far as possible information already
being collected in clinical work and use existing tools and standards
where available.
At the time of writing this document some aspects of revalidation are still being
considered by the GMC and other bodies and will no doubt be altered over time.
5
How Psychiatrists will be able to Evidence Meeting Revalidation
Standards
All doctors will be required to collect a portfolio of evidence that will be reviewed
at appraisal on an annual basis. Generic standards which apply to all doctors are
set out in Good Medical Practice2. Specialty standards for psychiatrists are set
out in Good Psychiatric Practice Version 33. Revalidation is planned to take place
on a 5 yearly cycle and hence the necessary evidence to provide assurance
about keeping up to date and fit to practise can be gathered over a 5 year
period.
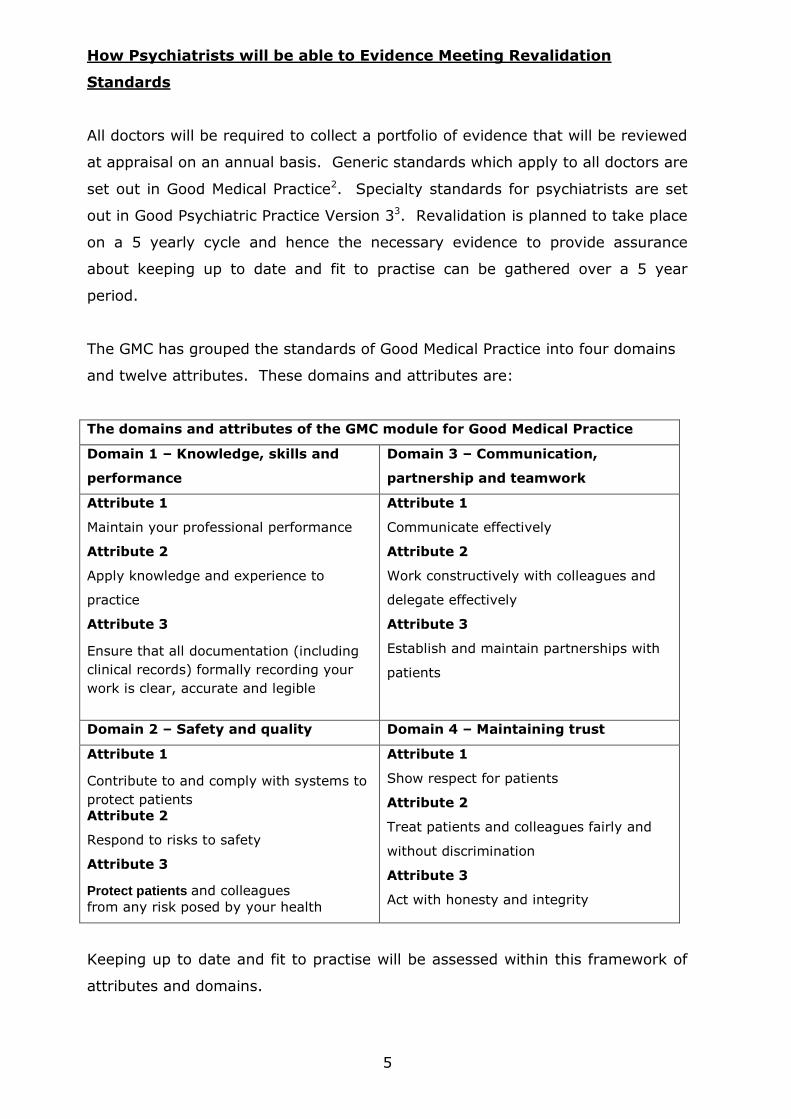
The GMC has grouped the standards of Good Medical Practice into four domains
and twelve attributes. These domains and attributes are:
The domains and attributes of the GMC module for Good Medical Practice
Domain 1 – Knowledge, skills and
performance
Domain 3 – Communication,
partnership and teamwork
Attribute 1
Maintain your professional performance
Attribute 2
Apply knowledge and experience to
practice
Attribute 3
Ensure that all documentation (including
clinical records) formally recording your
work is clear, accurate and legible
Attribute 1
Communicate effectively
Attribute 2
Work constructively with colleagues and
delegate effectively
Attribute 3
Establish and maintain partnerships with
patients
Domain 2 – Safety and quality Domain 4 – Maintaining trust
Attribute 1
Contribute to and comply with systems to
protect patients
Attribute 2
Respond to risks to safety
Attribute 3
Protect patients and colleagues
from any risk posed by your health
Attribute 1
Show respect for patients
Attribute 2
Treat patients and colleagues fairly and
without discrimination
Attribute 3
Act with honesty and integrity
Keeping up to date and fit to practise will be assessed within this framework of
attributes and domains.
6
The key process through which revalidation standards will be evidenced is
appraisal. The NHS is piloting an enhanced appraisal process which will have
both a summative and a formative component. The summative component of
appraisal will involve looking back at what has been achieved and the formative
part will be the agreeing of a Personal Development Plan as to the way forward.
There is an expectation that appraisers will have been trained to ensure that
appraisal is delivered in a professional, fair and transparent manner. The Royal
College of Psychiatrists has established appraisal training, providing an
opportunity for psychiatrists to train, not only using the recommended appraisal
system, but also to know how the specialist standards for psychiatry can be
evidenced. The College has produced Good Practice Guidelines for Appraisal to
assist both appraisers and appraisees in meeting best practice standards4.
This document sets out guidance about the evidence that psychiatrists will be
expected to collect in order to meet the requirements for Revalidation. The
examples given are not exclusive. The decision as to the appropriateness of
evidence will be taken in discussion at appraisal between the appraiser and the
appraisee. At the completion of a 5 year cycle a Responsible Officer will need to
be assured that evidence collected is sufficient to ensure that the doctor meets
the revalidation requirements. If a particular standard has not been met, for a
valid reason, agreed at appraisal between the appraiser and the psychiatrist
being appraised, this should be documented so that the Responsible Officer will
understand why decisions were made.
Supporting Information
All doctors will bring to their appraisal supporting information that provides
evidence about the GMC twelve attributes. The supporting information that you
will need to bring to your appraisal will fall under four broad headings:-
i) General information – providing context about what you do in all
aspects of your work.
ii) Keeping up to date – maintaining and enhancing the quality of your
professional work.
7
iii) Review of your practice – evaluating the quality of your professional
work.
iv) Feedback on your practice – how others perceive the quality of your
professional work.
There are six types of supporting information over and above general
information that you will be expected to provide and discuss at your appraisal at
least once in each five year cycle. These are:
i) Quality improvement activity.
ii) Feedback from colleagues.
iii) Feedback from patients (where applicable).
iv) Continuing professional development.
v) Significant events.
vi) Review of complaints and compliments.
The nature of the supporting information will reflect your particular practice and
your other professional roles.
By providing all six types of supporting information over the revalidation cycle
each psychiatrist should, through reflection and discussion at appraisal, have
demonstrated practice against all 12 attributes outlined in the GMC separate
guidance, Good Medical Practice Framework for Appraisal and Revalidation5. This
will make it easier for the appraiser to complete the appraisal and for the
Responsible Officer to make a recommendation to the GMC about revalidation.
It is not necessary to structure the appraisal formally around the GMC
Framework, or to map supporting information directly against each attribute.
However, some doctors may prefer to do this and some appraisers may find it
useful to structure the appraisal interview in this way.
8
The purpose of collecting the evidence for appraisals over the five year cycle is
not to tick boxes showing that a particular standard has been met, but rather to
enable the psychiatrist to collect a body of meaningful information that will
demonstrate continuing fitness to practise. It is expected that this process will
facilitate ongoing professional development, the aim of which is to improve the
standard of care that each psychiatrist provides for patients.
Appendix A provides a summary of the supporting information requirements.
9
Evidence that will be Reviewed at Appraisal
1. General Information
a) Personal details (including your GMC reference number)
b) Scope of work
This will include the organisations and locations where you have
undertaken work as a doctor. You will also need to provide a description
of the scope and nature of your practice.
c) Record of annual appraisals
d) Personal development plans and their review
e) Probity
Probity is at the heart of medical professionalism. Probity means being
honest and trustworthy and acting with integrity.
A statement of probity is a declaration that you accept the professional
obligations placed on you in Good Medical Practice in relation to probity. It
also includes the requirement to inform the GMC without delay if,
anywhere in the world, you have accepted a caution, been charged with or
found guilty of a criminal offence, or if another professional body has made
a finding against your registration as a result of fitness to practise
procedures.
If you are suspended from a medical post, or have restrictions placed on
your practice you must, without delay, informed any other organisations
for which you undertake medical work and any patients you see
independently.
Good Medical Practice provides guidance on issues of probity as follows:
Being honest and trustworthy (paragraphs 56-59).
Providing and publishing information about your services (paragraphs
60-62).
Writing reports and CVs, giving evidence and signing documents
(paragraphs 63-69).
Research (paragraphs 70-71).
Financial and commercial dealings (paragraphs 72-73).
Conflicts of interest (paragraphs 74-76).
10
f) Health
A statement of health is a declaration that you accept the professional
obligations place on you in Good Medical Practice about your personal
health.
Good Medical Practice provides the following guidance:
Registration with a GP – You should be registered with a general
practitioner outside your family to ensure that you have access to
independent and objective medical care. You should not treat yourself
(paragraph 77).
Immunisation – You should protect your patients, your colleagues and
yourself by being immunised against common serious communicable
diseases where vaccines are available (paragraph 78).
A serious condition that could pose a risk to patients – If you know
that you have, or think you might have, a serious condition that you
could pass on to patients, or if your judgement or performance could
be affected by a condition or its treatment, you must consult a suitably
qualified colleague. You must ask for and follow their advice about
investigations, treatment and changes to your practice that they
consider necessary. You must not rely on your own assessment of the
risk you pose to patients (paragraph 79).
11
2. Quality Improvement Activity
For the purposes of revalidation, you will have to demonstrate that you regularly
participate in activities that review and evaluate the quality of your work.
Quality improvement activities should be robust, systematic and relevant to your
work. They should include an element of evaluation and action, and where
possible, demonstrate an outcome or change.
Quality improvement activities could take many forms depending on the role you
undertake and the work that you do. If you work in a non-clinical environment,
you should participate in quality improvement activities relevant to your work.
Examples of quality improvement activities include:
i) Clinical audit – evidence of effective participation in clinical audit or
an equivalent quality improvement exercise that measures the care
with which an individual doctor has been directly involved.
ii) Review of clinical outcomes – where robust, attributable and
validated data are available.
iii) Case review or discussion – a documented account of interesting or
challenging cases that a doctor has discussed with a peer, another
specialist or within a multi-disciplinary team.
iv) Audit and monitor the effectiveness of a teaching programme.
v) Evaluate the impact and effectiveness of a piece of health policy or
management practice.
The College is recommending three key quality improvement activities:-
i) Case based discussion.
ii) Clinical audit.
iii) Clinical outcomes.
12
Case Based Discussion
The College is recommending that the case based discussion6 technique is used
as a key plank of appraisal. The system being proposed for those not in training
has been adapted from that used by trainees to meet the different requirements
of more experienced doctors.
Case based discussion provides the opportunity for a specialist psychiatrist to
discuss the care of a real case with a colleague. It provides an opportunity for
the colleague to make an assessment of key clinical care standards set out in
Good Psychiatric Practice. Case based discussion evaluates what the doctor has
done in practise. It has the advantage over a simple review of case notes in that
the doctor being appraised has the opportunity to explain and clarify the
information that is contained in the clinical records and provide appropriate
clinical background. A summary case based discussion sheet (Appendix B)
records the relevant information.
The expectation is that at each case based discussion, a discussion will occur as
to whether the psychiatrist has satisfactorily met the standards being evaluated
from Good Psychiatric Practice. Good points in the clinical care will be
highlighted together with the identification of areas of improvement. Each area
for improvement will then link to a Personal Development Plan which will be
followed up at appraisal.
The College recommends that a minimum of 10 case based discussions be
undertaken over a 5 year period (2 per year). It will be the responsibility of
each psychiatrist to ensure that an appropriate sample of the patients whom
they are looking after are included in case based discussion. In order to achieve
this, approximately two thirds of case based discussions should be chosen at
random and the other third should be chosen by the psychiatrist being
appraised. The purpose of random selection is to provide reassurance that care
provided is satisfactory for cases that the psychiatrist has not particularly
selected. The purpose of allowing a proportion of cases to be selected is to
ensure that over a five year cycle, cases discussed broadly reflect the diagnostic
case mix of the psychiatrist‟s workload. Selection also allows the psychiatrist to
13
discuss the management of complex cases that they consider would be of value
for their own personal development.
Guidance as to how to conduct a case based discussion is given in Appendix C.
Case based discussion may occur in a one to one format but could involve more
than one colleague and occur, for example, in the context of a peer group. Case
based discussion could also occur in the context of supervision. If more than
one colleague is involved in the case based discussion, it will be the
responsibility of one person to complete the case discussion summary sheet with
the ratings and action plans.
Case based discussion is not the only workplace assessment that might be of
value in Revalidation. If psychiatrists wish to use other techniques, for example,
direct observation of practice by a colleague, this information can be included in
the evidence set out at appraisal and would be a reasonable alternative to a case
based discussion.
Standard
Undertake 10 case based discussions over a 5 year cycle and incorporate
identified action points in a personal development plan.
Clinical Audit
It is expected that each psychiatrist will provide an audit over a 5 year cycle in
at least two significant clinical areas of their practice with standards, based on
best practice guidelines, re-audit, evidence of discussion in appraisal and
appropriate action. It is important that the audits reflect the care provided by
the individual doctor and focuses on key areas of clinical practice. The
importance of audit is not the audit process itself but the evidence it provides
that the psychiatrist is working to improve patient care. In discussion with an
appraiser, a non-audit quality improvement process could be agreed in place of
one of the audits, for example, a research project.
It will often be the case that the psychiatrist will work with others to undertake
the audit. The participation of the psychiatrist will most importantly occur in the
setting of standards and the drawing up and implementation of appropriate
action. Participation in national audits (where individual or team results can be
14
determined) eg. the Prescribing Observatory of Mental Health can be used as
evidence of clinical audit as long as there is evidence of action plans, change
implementation and re-audit.
The College intends to identify and approve (kite mark) audits in key areas of
psychiatric practice that colleagues can use if considering an audit. It is hoped
that this will provide an opportunity to benchmark practice with colleagues. It is
recognised that the meeting of standards in many areas of psychiatry involves
the practice of colleagues and also the availability of appropriate resources. The
development of action plans following audit may, therefore, be used as an
example of working with clinical and managerial colleagues to bring about
improvement in patient care.
HQIP (Healthcare Quality Improvement Partnership) have set out criteria and
indicators of best practice in clinical audit (Appendix D). The audit form
(Appendix E) will provide the summary of the audit data for the revalidation
portfolio.
Standard
To complete two audits of significant clinical areas of practice over a 5 year
cycle.
Clinical Outcome Measures
The College is not recommending specific outcome measures to be used for
revalidation at this stage. It is the College‟s view, however, that psychiatrists
should be considering, with colleagues, the use of appropriate outcome
measures as a way of working with patients to determine the benefit or
otherwise of interventions chosen.
The College has published a report on the use of clinical outcome measures to
assist in the choice of relevant measures7. The National Institute for Mental
Health in England has produced an outcomes compendium8 of potentially
relevant measures. Using structured outcome measures to look at, not only
clinical progress, but also outcomes relevant to patients is an example of good
practice and a significant quality improvement activity.
15
Psychiatrists in managed care organisations should work with managers to
ensure that organisation collected outcomes are made available for use in
revalidation.
Standard
Demonstrate the use of appropriate outcome measures in clinical practice.
3. Multisource Feedback – Colleagues
It is a GMC requirement that colleague multisource feedback is obtained for all
doctors. The expectation is that each doctor obtain feedback using standard
questionnaires that comply with GMC principles5. These principles are that the
questionnaire:-
a) be consistent with the principles, values and responsibilities set out
in the GMC‟s core guidance, Good Medical Practice.
b) be piloted on the appropriate population, and demonstrate that they
are reliable and valid.
c) reflects and measures the whole practice of the doctor.
d) be evaluated and administered independently from the doctor and
appraiser to ensure an objective review of the information.
e) provides appropriate and useful information to the doctor that can
be used in discussions with a supervisor or mentor, or through
appraisal.
f) helps the doctor reflect on his or her practice and identify
opportunities for professional development and improvement.
The GMC has also produced checklists for the development, administration and
implementation of questionnaires.
It is recommended that colleague multisource feedback occurs at least once
every 5 years. The feedback should then be discussed with a colleague, either
at or outside appraisal and an appropriate Personal Development Plan drawn up
to address any issues that arise.
16
The requirement for multisource feedback is a minimum of one per 5 years and
assumes that no significant concerns have arisen. If significant concerns have
been picked up by multisource feedback, a second multisource feedback should
be undertaken in the 5 year cycle, following appropriate action by the doctor
concerned.
You should be able to demonstrate that you have reflected on the feedback.
Your appraiser will be interested in what actions you took as a result of the
feedback, not just that you collected it.
The discussion at appraisal should highlight areas of good performance and help
you to identify any areas that might require further development. This should
be reflected in your personal development plan and your choices for continuing
professional development.
Multisource feedback from colleagues allows psychiatrists to meet several of the
standards for Good Psychiatric Practice concerned with teamwork and working
with colleagues. The College ACP360 has been designed specifically for
psychiatrists9. Using this tool enables psychiatrists to be compared with their UK
colleagues and provides a useful benchmark against which to draw up
appropriate actions.
A summary of the MSF findings to be included in appraisal documentation is
provided in Appendix F.
Standard
Undertake one MSF from colleagues using a tool meeting GMC standards at
least once in a 5 year cycle and take appropriate action.
4. Patient Feedback
As with colleague multisource feedback, it is a requirement that there will be
patient feedback (where applicable) using a questionnaire that meets GMC
standards (agreed by appraiser) once in 5 year cycle. As with multisource
feedback from colleagues, it is expected that any issues that arise from patient
17
feedback will be subject to action points in a Personal Development Plan and be
reviewed at appraisal.
Many colleagues may wish to collect patient feedback in a variety of formats,
providing evidence over and above the minimum requirement. This is to be
encouraged. Those doctors working in managed care systems should endeavour
to work with managers to facilitate the routine collection of patient experience
data that could then be used as part of the supporting evidence for appraisal.
You should be able to demonstrate that you have reflected on the feedback.
Your appraiser will be interested in what actions you took as a result of the
feedback, not just that you collected it.
The discussion at appraisal should highlight areas of good performance and help
you to identify any areas that might require further development. This should
be reflected in your personal development plan and your choices for continuing
professional development.
A summary of patient feedback information to be included in appraisal
documentation is given in Appendix G.
Standard
Obtain patient feedback using a tool meeting GMC standards at least once in a
5 year cycle and take appropriate action.
The College recognises the important role carers play and recommends that,
where possible, psychiatrists obtain feedback from carers.
5. Continuing Professional Development
It is a requirement for revalidation that psychiatrists keep their knowledge and
skills up to date; they are encouraged to take part in educational activities that
maintain and further develop their competence and performance. The College
recommends that psychiatrists are in good standing with the College for
Continuing Professional Development (or have done equivalent CPD). The
College has produced clear guidance for Continuing Professional Development
18
which reflects and is in line with the recommendations of the other medical
Royal Colleges10.
The requirements for CPD can be summarised as follows:-
i) Minimum of 50 hours per year (250 hours over a 5 year cycle).
ii) The content of CPD will reflect the job of the psychiatrist and
include an appropriate mixture of clinical, managerial, and
professional activities. CPD should equip the doctor to meet the
changing nature of their practice.
iii) The meeting of the CPD requirements will be validated by a peer
group chosen by the psychiatrist. If this is not possible this will
occur at appraisal by the appraiser.
The GMC advice for CPD emphasises the need for CPD to focus on outcomes or
outputs rather than time served.
A certificate of good standing for CPD in each of the 5 years should meet the
GMC and College requirements for revalidation. The evidence supporting such a
certificate can be held electronically for review if necessary. It is not expected
that an appraiser will need to review the evidence in detail as this will have been
examined via a peer group process.
Standard
Remain in good standing with the College for CPD in each of the 5 years or
have done the equivalent professional development.
6. Review of Significant Events
It is expected that psychiatrists will reflect upon significant events or serious
untoward incidents involving patients in their care and identify, not only good
practice, but also areas for improvement. The areas for improvement should be
incorporated into a Personal Development Plan and be reviewed through the
appraisal process.
19
A significant event (also known as an untoward or critical incident) is any
unintended or unexpected event, which could or did lead to harm of one or more
patients. This includes incidents which did not cause harm but could have done,
or where the event should have been prevented. These events should be
collected routinely by your employer, where you are directly employed by an
organisation. If you are self-employed, you should make note of any such
events or incidents and undertake a review.
You should discuss significant events involving you at appraisal with a particular
emphasis on those that have led to a specific change in practice or demonstrate
learning.
The numbers of significant events may vary across different specialities and it is
the content and what you learnt, rather than the number that should be the
focus in appraisal.
A structured format for documenting reflection on serious untoward incidents is
provided in Appendix H.
Standard
Reflect on each significant event and discuss learning and appropriate action
at appraisal.
7. Review of Complaints and Compliments
A complaint is a formal expression of dissatisfaction or grievance. It can be
about an individual doctor, the team or about the care of patients where a doctor
could be expected to have had influence or responsibility.
Complaints should be seen as another type of feedback, allowing doctors and
organisations to review and further develop their practice and to make patient-
centred improvements.
You might also choose to bring any compliments you have received to appraisal.
20
You should discuss any change in your practice that you have made as a result
of any complaints or compliments you have received since your last appraisal.
You may not have any complaints made about you or your team in a given
appraisal period.
The numbers of complaints may vary across different specialities and it is how
you dealt with the complaint, rather than the number, that should be the focus
of discussion in appraisal.
A structured format for documenting reflection on complaints is given in
Appendix I.
Standard
Reflect on each complaint and discuss learning and appropriate action at
appraisal.
21
Other Revalidation Issues
Non-clinical Practice
Many psychiatrists spend a significant proportion of their time in non-clinical
practice including academic work, both teaching and research, management
activities, and medico-legal work. There is a range of supporting information
that can be provided at appraisal to demonstrate good practice in these areas.
Teaching – Evidence to show that psychiatrists involved in teaching are
meeting the standards of Good Psychiatric Practice could include
information about the content of a teaching course together with
feedback from students. A useful set of standards for medical
educators11 is provided by the Academy of Medical Educators.
Research - Evidence of compliance with Good Medical and Psychiatric
Practice would include information about meeting national and local
research governance arrangements. The GMC has produced specific
guidance for the roles and responsibilities of doctors in research12.
Medical Management and Clinical Leadership – The GMC has produced
guidance13 and the former British Association of Medical Managers
produced standards14 for medical managers.
Expert Advice – Evidence of compliance in medico-legal work could
include providing evidence of compliance with ensuring patients and
psychiatrists understand the confidentiality issues and that the
psychiatrist has ensured that their training has been kept up to date in
the areas in which they are providing expert knowledge. The GMC and
the BMA have provided guidance15,16 for those acting as an expert
witness.
Standard
Provide supporting information that teaching, research, management and
expert advice activities meet standards set in Good Medical and Good
Psychiatric Practice.
22
Academic Practice
Academic Psychiatrists will be expected, as part of revalidation, to provide at
appraisal supporting evidence covering both the clinical and academic aspects of
the work they undertake. As with revalidation in general, Academic Psychiatrists
will be expected to provide evidence to support meeting the standards of Good
Medical and Good Psychiatric Practice for the roles they undertake, reflecting for
many individuals specialised and expert areas of practice.
The Follett principles of whole practice appraisal will continue to apply. There
should be a jointly agreed appraisal scheme between the educational and clinical
provider. Only one appraisal should be undertaken each year which will be
structured so as to review both the clinical and academic work of the appraisee.
The General Medical Council have published a report on non-clinical work and
revalidation from the Non-Clinical Work Group of the Academy of Medical Royal
Colleges (click here http://www.gmc-
uk.org/Item_6e_AoMRC_progress_update.pdf_28990378.pdf). This report sets
out standards for medical research and medical education together with
supporting evidence that could be provided at appraisal. This report should be
viewed as providing a menu of ideas about supporting information that could be
brought to appraisal with regard to non-clinical work.
There is no expectation that academics will be expected to provide any particular
evidence over and above the standards of Good Medical Practice and Good
Psychiatric Practice. It is also recognised that academic psychiatrists have widely
differing job descriptions for both their clinical and academic roles, for example
in terms of the nature and relative amounts of clinical work, research, teaching,
and of management and leadership roles. As such, the process and content of
appraisal should be similarly flexible, and proportionate, whilst remaining fully
consistent with the principles of revalidation.
23
Research
In the GMC core guidance, Good Medical Practice, doctors who are involved in
research are advised that:-
If you are involved in designing, organising or carrying out research, you
must put the protection of participants‟ interests first, act with honesty
and integrity and follow the appropriate national research governance
guidelines.
More detailed guidance (32 points) are set out in the GMC Guidance Good
Psychiatric Practice in Research (click here http://www.gmc-
uk.org/guidance/ethical_guidance/5991.asp). This Guidance also includes
relevant confidentiality guidance. It is expected that academic psychiatrists
involved in research will provide supporting evidence that the GMC standards are
met.
Point 4, and the related GMC guidance, applies primarily to clinical research with
patients. Some academic psychiatrists may be engaging in „preclinical‟ research
– e.g. research with animals or cells, which falls outside the remit of
revalidation. Nevertheless, it is still appropriate for such research to be included
in the appraisal, with that component of the appraisal being led by the University
appraiser.
Teaching
Key Teaching Standards for Medical Education set out by the Academy of Medical
Royal Colleges include:-
Use observation, feedback, up to date educational knowledge and
research as sources for active reflection, evaluation and revision of your
practice.
Routinely audit and monitor the effectiveness of your programme.
Ensure that assessment decisions are recorded and documented
accurately and systematically.
Develop a variety of clear, accurate presentations and representations of
concepts, using alternative explanations to assist learners‟ understanding
and presenting diverse perspectives to encourage critical thinking.
24
Record and report results accurately and in a way that is transparent and
open to audit.
Teaching issues and standards fall equally within the University and NHS
domains of appraisal. For example, educational training, and ongoing evaluation
of teaching activities, will usually be a standard part of the academic‟s job
description. The documentation and discussion of teaching activities during the
appraisal should be conducted in a single and integrated fashion, avoiding
duplication.
Private and Independent Practice
Those psychiatrists undertaking private work will revalidate to the same
standard as those in NHS work.
This guidance is for all psychiatrists and may need to be adapted according to
the circumstances of each doctor e.g. if a psychiatrist is not seeing patients in a
clinical context it is not expected that they provide feedback from patients using
the standardised GMC appraisal tools.
It remains unclear at the time of preparing this guidance who will be the
Responsible Officer for those psychiatrists who have no links with managed care
organisations.
At present there is no legal requirement that doctors doing no other medical
work except sitting on Mental Health Review Tribunals will be required to
revalidate. It is the view of the College that psychiatrists in this situation
maintain their licence to practise through revalidation.
25
Responsible Officers
Responsible Officers will have a key role in revalidation. They will make a
recommendation to the GMC, usually every five years, about whether an
individual doctor should be revalidated. The Responsible Officer will also be
responsible for ensuring that systems of clinical governance and appraisal in
their organisation are working and are appropriate for revalidation.
The Responsible Officer Regulations came into force in Northern Ireland on 1
October 2010 and in England, Scotland and Wales on 1 January 2011.
The regulations specify the organisations or bodies which are “designated
bodies” and which must appoint or nominate a Responsible Officer. Responsible
Officers must be licensed medical practitioners, such as a Medical Director within
a healthcare organisation. The designation of such bodies or organisations and
the associated requirement to nominate or appoint a Responsible Officer will
ensure that the vast majority of doctors, and particularly those whose work
affects the safety of patients, will link to a Responsible Officer.
Responsible Officers will be responsible for the doctors employed by, or
contracted to, the designated body or organisation. Doctors will only link to one
Responsible Officer.
One of the key duties of a Responsible Officer will be to ensure that systems and
processes are in place so that doctors within the organisation can meet
revalidation requirements. Such systems will include a robust appraisal process
in which all doctors are enrolled.
At the end of each 5 year cycle, the Responsible Officer will be required to make
a recommendation to the GMC as to whether the doctor has met the standards
for revalidation. In areas where the decision to make a revalidation
recommendation is uncertain it is likely that Responsible Officers will seek advice
from College Advisors in making a revalidation recommendation. Responsible
Officers may or may not be psychiatrists. The role of the College Advisor in
assisting Responsible Officers has yet to be set out. The College has alongside
26
other Medical Royal Colleges agreed the following principles for the giving of
specialty advice:-
Consistency: advice given to ROs, appraisers and individual doctors must be
consistent with guidance from other key revalidation partners, based on the
standards and guidance already published by colleges and faculties, and
consistent between different individuals providing advice.
Commonality: common processes across all specialties should be agreed as
far as possible in order to avoid inconsistency in methods of acquiring and
providing advice.
Legality: colleges and Faculties must not become involved in the decision-
making process regarding the recommendation for revalidation, and work
within the legal considerations (Appendix 2).
Impartiality: advisors providing guidance/advice must be impartial and must
not have any conflict of interest or vested interest in the individuals
concerned. If locally sought, this may require the adviser to come from
outside the area/region in which the doctor is employed.
Generality: requests for advice must be in relation to a situation or set of
circumstances and not to an individual doctor or appraiser.
The final decision about making a revalidation recommendation will rest with the
Responsible Officer.
The Department of Health (England) has produced guidance about the
Responsible Officer role, including how doctors can find out who their
Responsible Officer is. Relevant extracts from the Responsible Officer Guidance,
DH (England) July 2010 includes:-
1.6
The responsible officer, following the appropriate or necessary consultations with
Medical Royal College representatives and where necessary the National Clinical
Assessment Service (NCAS), will decide whether the necessary standards are
met and if not will refer the doctor to the GMC on fitness to practise grounds.
27
3.10
The responsible officer should be informed by the appraiser about any significant
concerns that arise, i.e. those of a sufficiently serious nature to call into question
the doctor's fitness to practise, as these are likely to require specialist input from
the appropriate Medical Royal College or Faculty, NCAS or other relevant body.
Arrangements for remediation, supervision or suspension may also need to be
put in place.
3.11
At the time of revalidation, the responsible officer, having assessed all the
information and, if appropriate, consulted the relevant Medical Royal College or
Faculty, will make a recommendation to the GMC regarding the doctor‟s fitness
to practise.
4.7
Medical Royal Colleges and Faculties will offer support to responsible officers in
evaluating the specialist practice of doctors. The responsible officer will want to
ensure that there is appropriate liaison between their organisation and the
relevant Medical Royal Colleges and Faculties to seek their input to the appraisal
process as required, in terms of specialist practice. The responsible officer will
decide when he or she needs advice on specialist practice. In cases where there
are concerns relating to general practice or specialist clinical practice advice may
be available from the Medical Royal Colleges.
4.9
The responsible officer will also be expected to liaise with the appropriate
Medical Royal College or Faculty, where appropriate, through the College
Regional Advisors or identified college contacts for independent advice on the
relevant specialist practice and also, in cases of concern, for advice on the
performance of the doctor.
4.11
The responsible officer is unlikely to make the decision to refer a doctor to the
GMC in isolation; he or she will want to seek advice from appropriate sources,
for example from the medical Royal Colleges and Faculties or the National
28
Clinical Assessment Service (NCAS) or other relevant body. The responsible
officer must also ensure that remediation and disciplinary procedures, where
appropriate, are followed.
4.31
The responsible officer will liaise, where appropriate, with the Medical Royal
Colleges and Faculties for information and support regarding specialist and GP
practice and potential recommendations.
The guidance and further information about the Responsible Officer role is
available on the Department of Health (England) website.
The Department of Health, Social Services and Public Safety (DHSSPS) has
published the regulations and guidance that apply to Responsible Officers in
Northern Ireland. These can be viewed on the DHSSPS website.
In Scotland the Executive Medical Directors of Health Boards (including special
Boards such as the State Hospital Board) will be the responsible Officers within
the NHS. Further information about this can be found at
http://www.scotland.gov.uk/Topics/Health/NHS-
Scotland/paper/Revalidation/Officers
Remediation
There will be some psychiatrists for whom the revalidation process identifies the
need for remediation. In these cases employers, the National Clinical
Assessment Service (NCAS), the Deanery (for trainees) and the Responsible
Officer may need to be involved in order to draw up a plan for remediation and
assessment.
The College was involved in the drawing up and supports the recommendation of
remediation report produced for the Department of Health in England by the
steering group on remediation17.
29
Electronic Portfolio
Each of the four UK devolved health departments have taken a different
approach to standardising the documentation to be used in appraisal.
England
No standardised documentation to be recommended. It will be the responsibility
of individual employers and Responsible Officers to determine what best meets
their requirements.
The College is examining, with other Medical Royal Colleges, the feasibility of
recommending a cross specialty electronic portfolio to be used in England.
Scotland
Standardised portfolio based on SOAR which may be found at
http://www.scottishappraisal.scot.nhs.uk/what%27s-this/about-
appraisal/confidentiality.aspx
Wales
Standardised portfolio based on GP appraisal documentation which may be found
at https://nhswalesappraisal.org.uk/
Northern Ireland
The appraisal documentation for psychiatrists working in Northern Ireland may
be found at http://www.dhsspsni.gov.uk/public_health-appraisal
30
Frequently Asked Questions
1. What is revalidation?
Revalidation is the process by which doctors will have to demonstrate to the GMC, normally
every five years, that they are up to date and fit to practise.
2. What is the purpose of revalidation?
The purpose of revalidation is to assure patients and the public, employers and other
healthcare professionals that licensed doctors are up to date and fit to practise.
Revalidation is a new way of regulating the medical profession that will provide a focus for
doctors' efforts to maintain and improve their practice; facilitate the organisations in which
doctors' work to support them in keeping their practice up to date; and encourage patients
and the public to provide feedback about the medical care they receive from doctors. In
these ways, revalidation will contribute to the ongoing improvement in the quality of medical
care delivered to patients throughout the UK.
3. How will revalidation work?
Revalidation will be based on a local evaluation of doctors' performance through appraisal.
Doctors will be expected to participate in annual appraisal in the workplace and will need to
maintain a folder or portfolio of supporting information to bring to their appraisals as a basis
for discussion. There will be some types of supporting information that all doctors will be
expected to provide at appraisal over a revalidation cycle. However, doctors can take any
other additional information to demonstrate their practice at appraisal.
For more information, please see our guidance on supporting information for appraisal and
revalidation.
Information from the appraisal will be provided to a Responsible Officer who will make a
recommendation to the GMC, normally every five years, on whether to revalidate a doctor.
In order to revalidate a doctor, the GMC will require assurance that a doctor is fit to practise.
4. What has happened to recertification?
When the Government published its proposals for revalidation in 2007, it divided revalidation
into two elements - relicensing and recertification. We have now moved to a single system of
revalidation, which incorporates both of these elements into a simpler, more effective and
more efficient process than the two separate strands originally proposed.
5. How often must I revalidate?
For most doctors, revalidation will be a five year cycle. Every five years the GMC will require
confirmation from a doctor's Responsible Officer that they are up to date and fit to practise
and that there are no significant unresolved concerns about their practice.
The GMC may vary the frequency of this cycle where the circumstances of the individual
doctor require it. One example is where a doctor has taken a career-break and their
31
revalidation may be postponed for a period of time to allow them time to gather sufficient
supporting information for the appraisal and revalidation.
6. How will patients, carers and the public be involved in revalidation?
One of the aims of revalidation is to assure patients and the public that licensed doctors are
up to date and fit to practise. Patients will need to have confidence in the way that
revalidation will work.
Our consultation, Revalidation: The Way Ahead, explored a number of ways in which patients
and the public might be involved in revalidation. Following the consultation, we have agreed
that the information that doctors will discuss at appraisal will include feedback from patients,
through patient questionnaires, complaints and compliments. It may also be appropriate for
patient feedback received through other mechanisms, for instance through engagement with
Patient Advice and Liaison Services (www.pals.nhs.uk), to be included in appraisal discussions
where it is available.
7. What should I be doing now to prepare for revalidation?
Revalidation is not expected to roll out until 2012. In the meantime, you need to ensure that
you are participating in annual appraisal. If you cannot access appraisal through your
workplace, you should contact your Responsible Officer or relevant health board.
Information about what psychiatrists will be expected to bring to their appraisal is in this
document.
You should ensure that you know who your Responsible Officer is. Guidance and further
information about the Responsible Officer role is available on the Department of Health
(England) website and the Department of Health, Social Services and Public Safety
(DHSSPS) website.
Responsible Officers have been in place since 1 January 2011. They will have a legal duty to
ensure the local systems and processes which underpin revalidation are in place, including
clinical governance systems and a system of annual appraisals. Doctors who have queries
about finding their Responsible Officer should contact the DHSSPS or the Department of
Health (England) for more information. Doctors may also wish to contact the organisations
that employ or contract their services to confirm arrangements for linking with a Responsible
Officer based in those organisations.
In order to stay up to date with developments in revalidation and guidance that we are
publishing you can sign up to the GMC Revalidation Update, a regular e-bulletin sent on
behalf of the UK Revalidation Programme Board by the General Medical Council. In order to
do this, please send an email requesting addition to our mailing list to revalidation@gmc-
uk.org.
For more information about appraisals and revalidation in your country, you can visit:
The NHS Revalidation Support Team website:
www.revalidationsupport.nhs.uk (England)
32
The Health in Wales website: www.wales.nhs.uk (Wales)
The Scotland NHS website: www.show.scot.nhs.uk (Scotland)
The Health and Social care in Northern Ireland website: www.n-i.nhs.uk (Northern
Ireland)
8. What will happen if I do not engage in appraisal and revalidation?
The GMC expect that the majority of doctors will have no problem meeting the requirements
for revalidation if they engage with the appraisal and local clinical governance processes.
If you choose not to engage, by not providing evidence to support your revalidation or failing
to participate in an annual appraisal process, you cannot be revalidated and you risk having
your licence to practise withdrawn.
9. If serious concerns are raised about a doctor's practise what will be the consequences for their revalidation?
If concerns are identified about a doctor's practice that are sufficiently serious to raise
questions about whether they should have a licence to practise and the Responsible Officer is
therefore unable to recommend them for revalidation, the doctor will be referred to the GMC's
Fitness to Practice processes.
Where concerns about a doctor's practise exist these should be identified early and, where
possible, addressed through relevant local clinical governance processes including appraisal.
The identification of, and action on, concerns should not wait until they are due to be
revalidated but be dealt with through usual day to day systems or at appraisal. The
Responsible Officer might also want to immediately engage with the National Clinical
Assessment Service (www.ncas.npsa.nhs.uk) or refer the doctor to the GMC if the concerns
raised are sufficiently serious.
Where a doctor is referred to the GMC's Fitness to Practise department for investigation their
revalidation will be deferred until the outcome of that investigation is known.
10. Will there be a required minimum number of clinical sessions that doctors must undertake in order to revalidate?
The GMC will not require doctors to undertake a set minimum number of hours or clinical
sessions for revalidation as it is based on what a doctor's practice consists of on a day-to-day
basis and different fields of practise have different requirements.
Before making a recommendation, a Responsible Officer will need to be satisfied that a doctor
is up to date and fit to practise, based on the information and discussions at appraisal.
If you have any further questions about revalidation, please email the College at
33
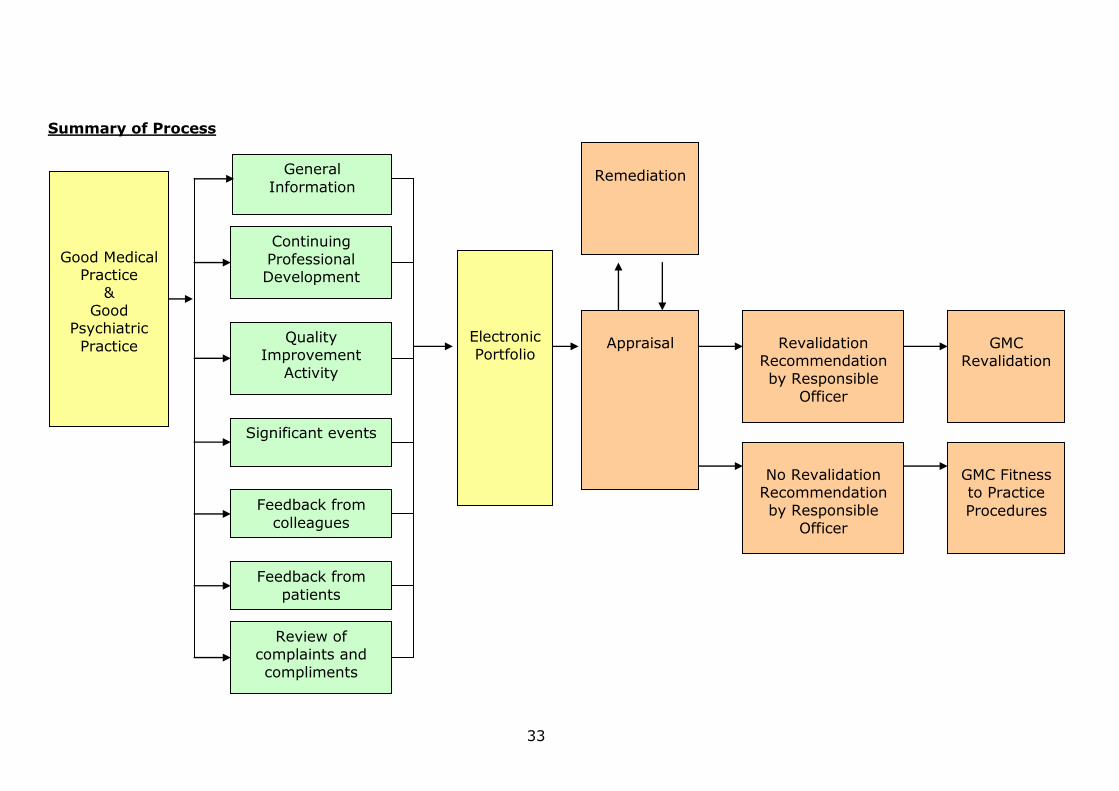
Summary of Process
Good Medical Practice
& Good
Psychiatric
Practice
General
Information
Continuing
Professional Development
Quality
Improvement
Activity
Significant events
Electronic
Portfolio
Appraisal
Revalidation Recommendation
by Responsible
Officer
Remediation
Feedback from
colleagues
No Revalidation Recommendation
by Responsible
Officer
GMC
Revalidation
GMC Fitness to Practice
Procedures
Feedback from
patients
Review of
complaints and
compliments
34
References
1. Revalidation: A Statement of Intent. GMC, 2010.
2. General Medical Council (2006). Good Medical Practice.
3. Good Psychiatric Practice. Royal College of Psychiatrists, 3rd Edition.
February 2009.
4. Good Practice Guidelines for Appraisal (2010). Royal College of
Psychiatrists.
5. Good Medical Practice Framework for Appraisal and Revalidation.
(http://www.gmc-
uk.org/doctors/revalidation/revalidation_gmp_framework.asp).
6. Case Based Discussion: A Useful Tool for Revalidation. Mynors-Wallis L et
al. The Psychiatrist (2011)35;230-234.
7. Outcome Measures Recommended for Use in Adult Psychiatry. Hampson M,
Killaspy H, Mynors-Wallis L, Meier R. Occasional Paper OP78. London,
Royal College of Psychiatrists, 2011.
8. Outcomes Compendium: Helping you select the right tools for best mental
healthcare practice in your field. National Institute of Mental Health in
England. Department of Health, October 2008.
[http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/Publication
sPolicyAndGuidance/DH_093316]
9. Questionnaires for 360 degree assessment of Consultant Psychiatrists:
Development and Psychometric Prospectus. Lelliott P, Williams K, Mears A
et al. British Journal of Psychiatry (2008)193;156-160.
10. Good Psychiatric Practice – CPD. Royal College of Psychiatrists, 2nd Edition.
October 2009.
11. Academy of Medical Educators (2008). Interim Professional Development
Standards. AME.
12. General Medical Council (2002). Research: The role and responsibilities of
doctors. London, GMC.
13. Management of Doctors – GMC Guidance.
14. Standards for Clinical Leadership and Management. The British Association
of Medical Managers.
35
15. General Medical Council (2008). Acting as an expert witness. London,
GMC.
16. British Medical Association (2009). Expert Witness Guide.
17. Remediation Report (2011). Department of Health, England.
36
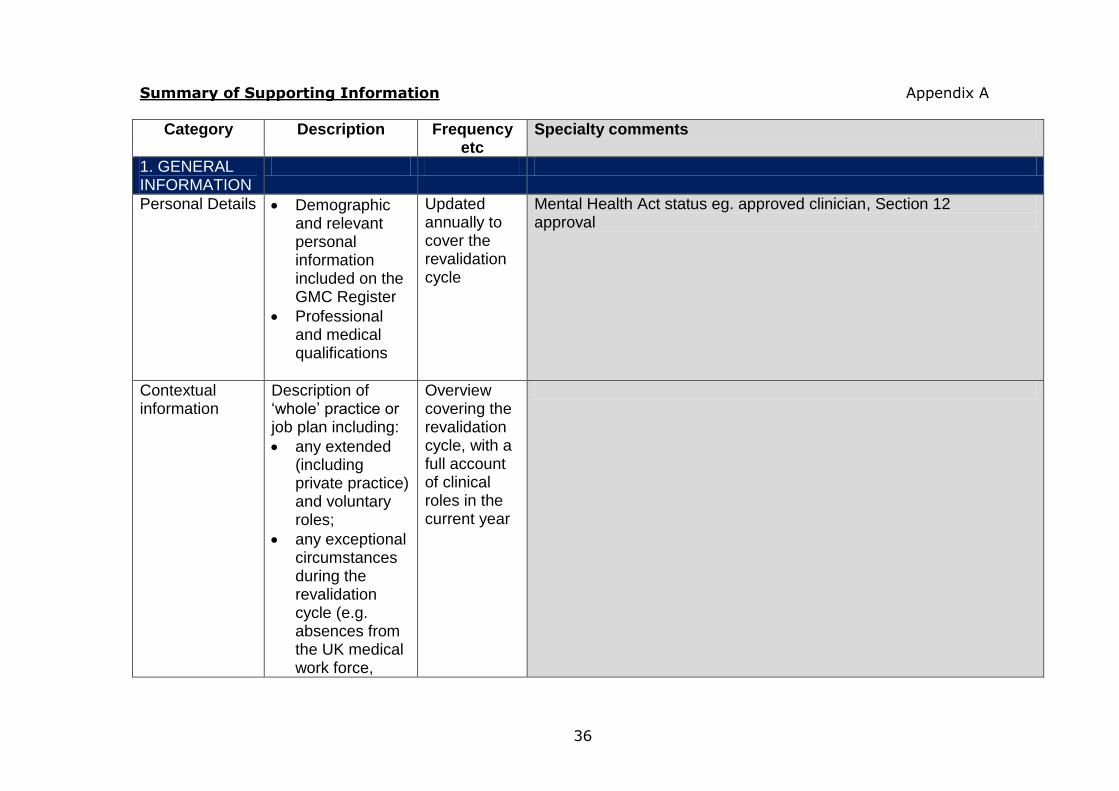
Summary of Supporting Information Appendix A
Category Description Frequency etc
Specialty comments
1. GENERAL INFORMATION
Personal Details Demographic and relevant personal information included on the GMC Register
Professional and medical qualifications
Updated annually to cover the revalidation cycle
Mental Health Act status eg. approved clinician, Section 12 approval
Contextual information
Description of ‘whole’ practice or job plan including:
any extended (including private practice) and voluntary roles;
any exceptional circumstances during the revalidation cycle (e.g. absences from the UK medical work force,
Overview covering the revalidation cycle, with a full account of clinical roles in the current year
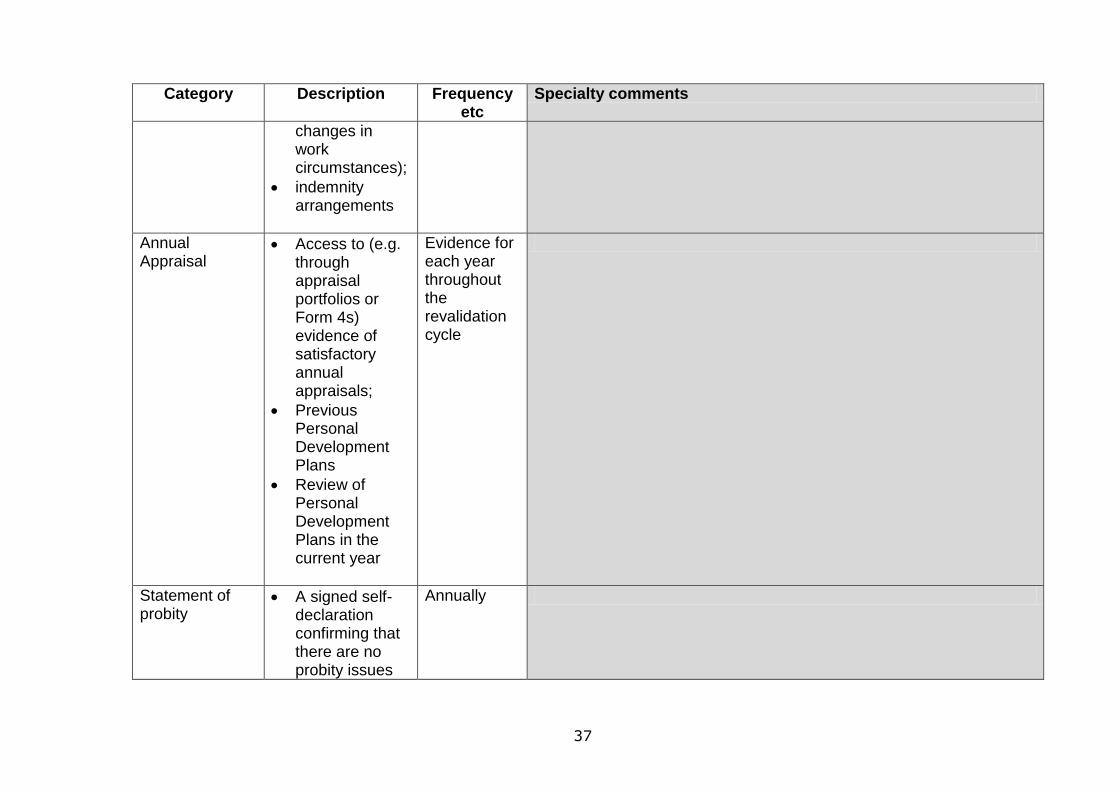
37
Category Description Frequency etc
Specialty comments
changes in work circumstances);
indemnity arrangements
Annual Appraisal
Access to (e.g. through appraisal portfolios or Form 4s) evidence of satisfactory annual appraisals;
Previous Personal Development Plans
Review of Personal Development Plans in the current year
Evidence for each year throughout the revalidation cycle
Statement of probity
A signed self-declaration confirming that there are no probity issues
Annually
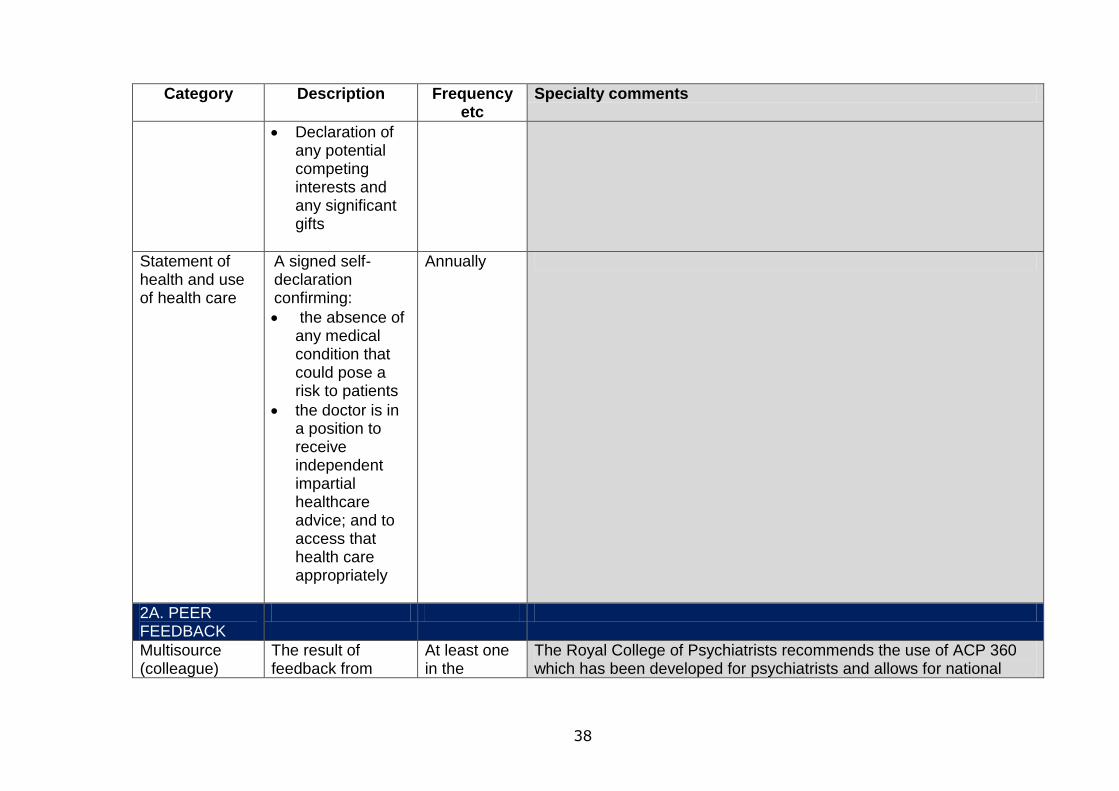
38
Category Description Frequency etc
Specialty comments
Declaration of any potential competing interests and any significant gifts
Statement of health and use of health care
A signed self-declaration confirming:
the absence of any medical condition that could pose a risk to patients
the doctor is in a position to receive independent impartial healthcare advice; and to access that health care appropriately
Annually
2A. PEER FEEDBACK
Multisource (colleague)
The result of feedback from
At least one in the
The Royal College of Psychiatrists recommends the use of ACP 360 which has been developed for psychiatrists and allows for national
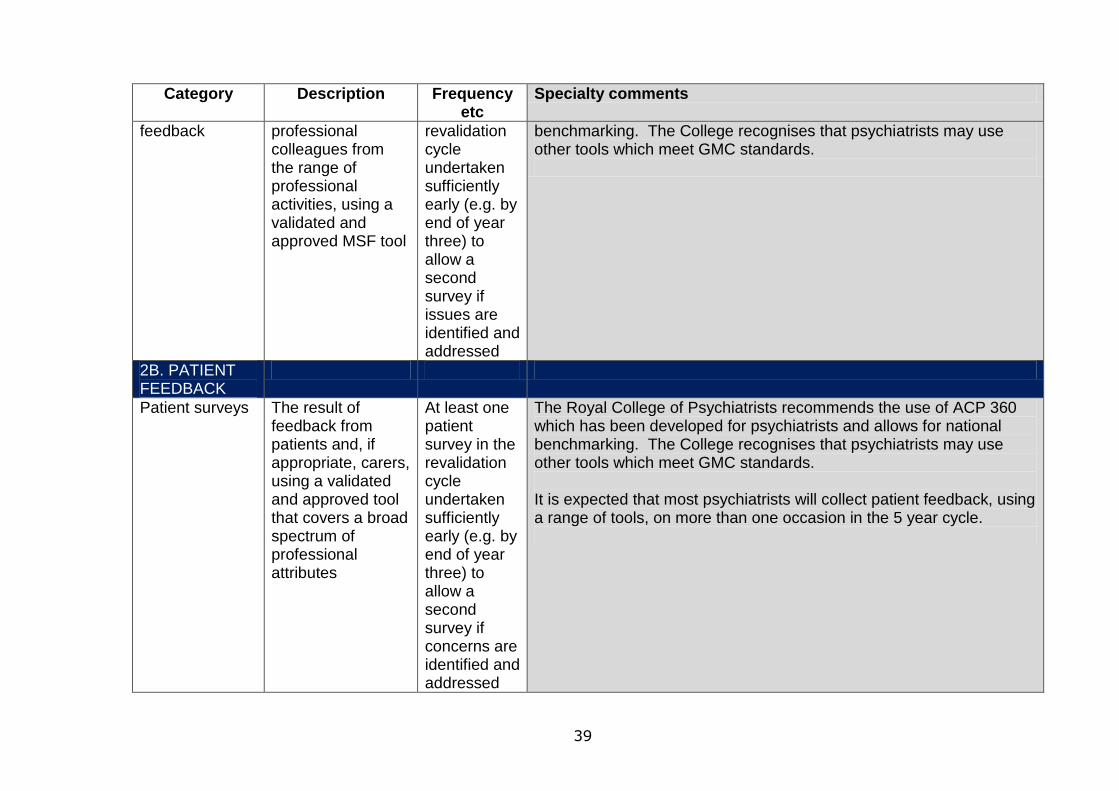
39
Category Description Frequency etc
Specialty comments
feedback professional colleagues from the range of professional activities, using a validated and approved MSF tool
revalidation cycle undertaken sufficiently early (e.g. by end of year three) to allow a second survey if issues are identified and addressed
benchmarking. The College recognises that psychiatrists may use other tools which meet GMC standards.
2B. PATIENT FEEDBACK
Patient surveys
The result of feedback from patients and, if appropriate, carers, using a validated and approved tool that covers a broad spectrum of professional attributes
At least one patient survey in the revalidation cycle undertaken sufficiently early (e.g. by end of year three) to allow a second survey if concerns are identified and addressed
The Royal College of Psychiatrists recommends the use of ACP 360 which has been developed for psychiatrists and allows for national benchmarking. The College recognises that psychiatrists may use other tools which meet GMC standards. It is expected that most psychiatrists will collect patient feedback, using a range of tools, on more than one occasion in the 5 year cycle.
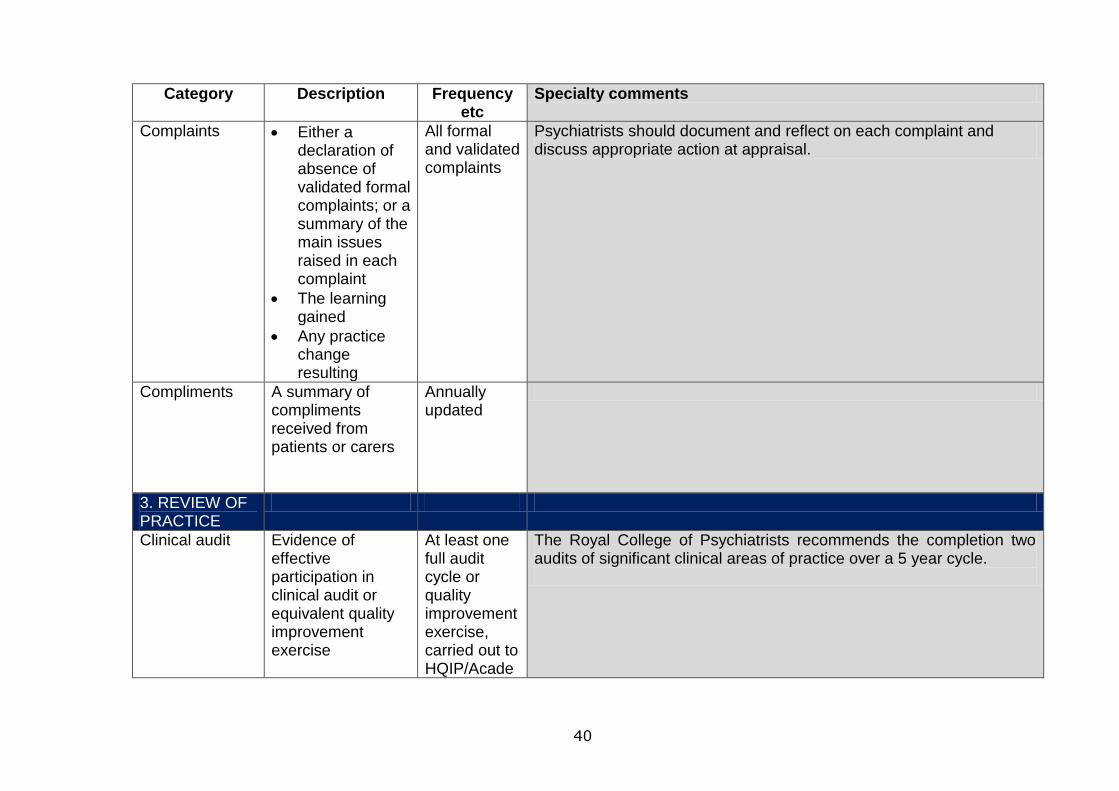
40
Category Description Frequency etc
Specialty comments
Complaints Either a declaration of absence of validated formal complaints; or a summary of the main issues raised in each complaint
The learning gained
Any practice change resulting
All formal and validated complaints
Psychiatrists should document and reflect on each complaint and discuss appropriate action at appraisal.
Compliments A summary of compliments received from patients or carers
Annually updated
3. REVIEW OF PRACTICE
Clinical audit
Evidence of effective participation in clinical audit or equivalent quality improvement exercise
At least one full audit cycle or quality improvement exercise, carried out to HQIP/Acade
The Royal College of Psychiatrists recommends the completion two audits of significant clinical areas of practice over a 5 year cycle.
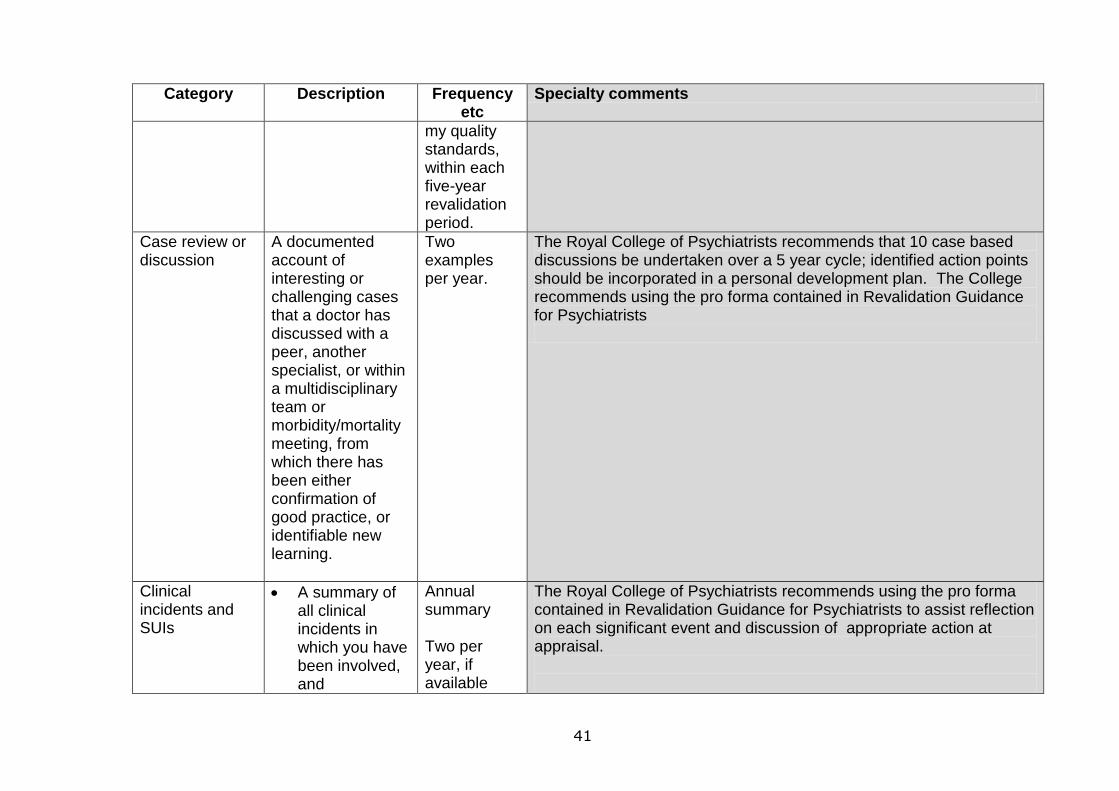
41
Category Description Frequency etc
Specialty comments
my quality standards, within each five-year revalidation period.
Case review or discussion
A documented account of interesting or challenging cases that a doctor has discussed with a peer, another specialist, or within a multidisciplinary team or morbidity/mortality meeting, from which there has been either confirmation of good practice, or identifiable new learning.
Two examples per year.
The Royal College of Psychiatrists recommends that 10 case based discussions be undertaken over a 5 year cycle; identified action points should be incorporated in a personal development plan. The College recommends using the pro forma contained in Revalidation Guidance for Psychiatrists
Clinical incidents and SUIs
A summary of all clinical incidents in which you have been involved, and
Annual summary Two per year, if available
The Royal College of Psychiatrists recommends using the pro forma contained in Revalidation Guidance for Psychiatrists to assist reflection on each significant event and discussion of appropriate action at appraisal.
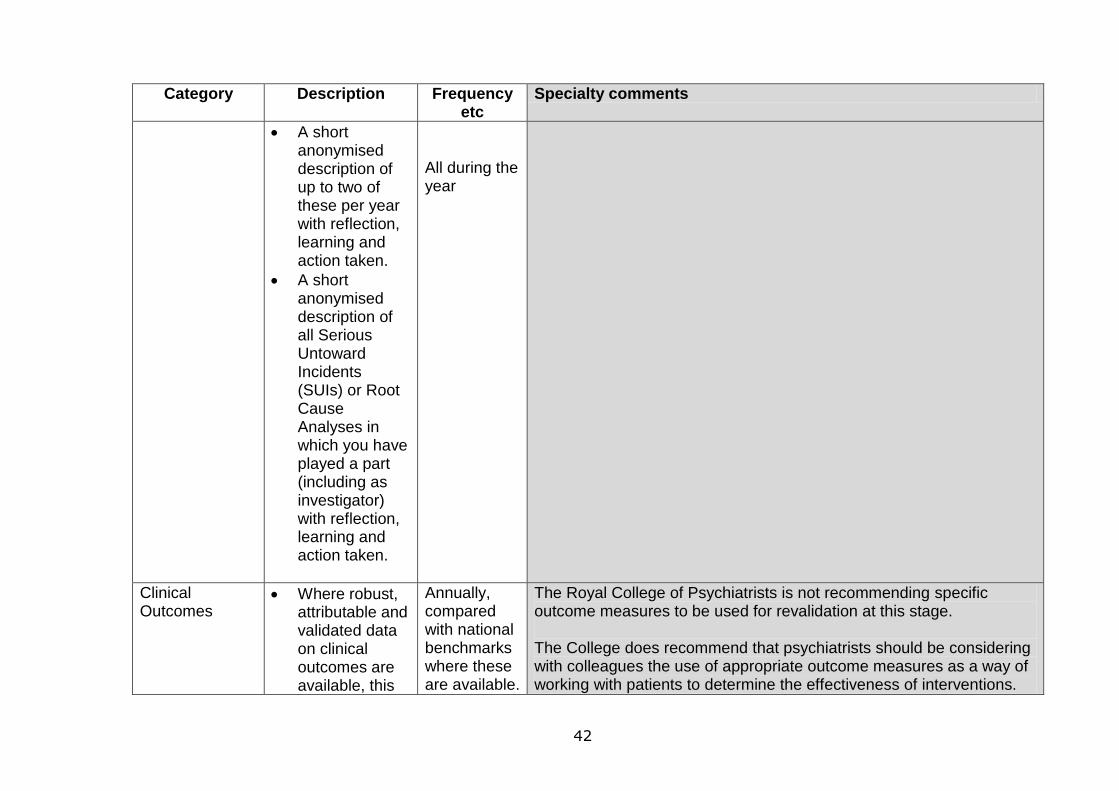
42
Category Description Frequency etc
Specialty comments
A short anonymised description of up to two of these per year with reflection, learning and action taken.
A short anonymised description of all Serious Untoward Incidents (SUIs) or Root Cause Analyses in which you have played a part (including as investigator) with reflection, learning and action taken.
All during the year
Clinical Outcomes
Where robust, attributable and validated data on clinical outcomes are available, this
Annually, compared with national benchmarks where these are available.
The Royal College of Psychiatrists is not recommending specific outcome measures to be used for revalidation at this stage. The College does recommend that psychiatrists should be considering with colleagues the use of appropriate outcome measures as a way of working with patients to determine the effectiveness of interventions.
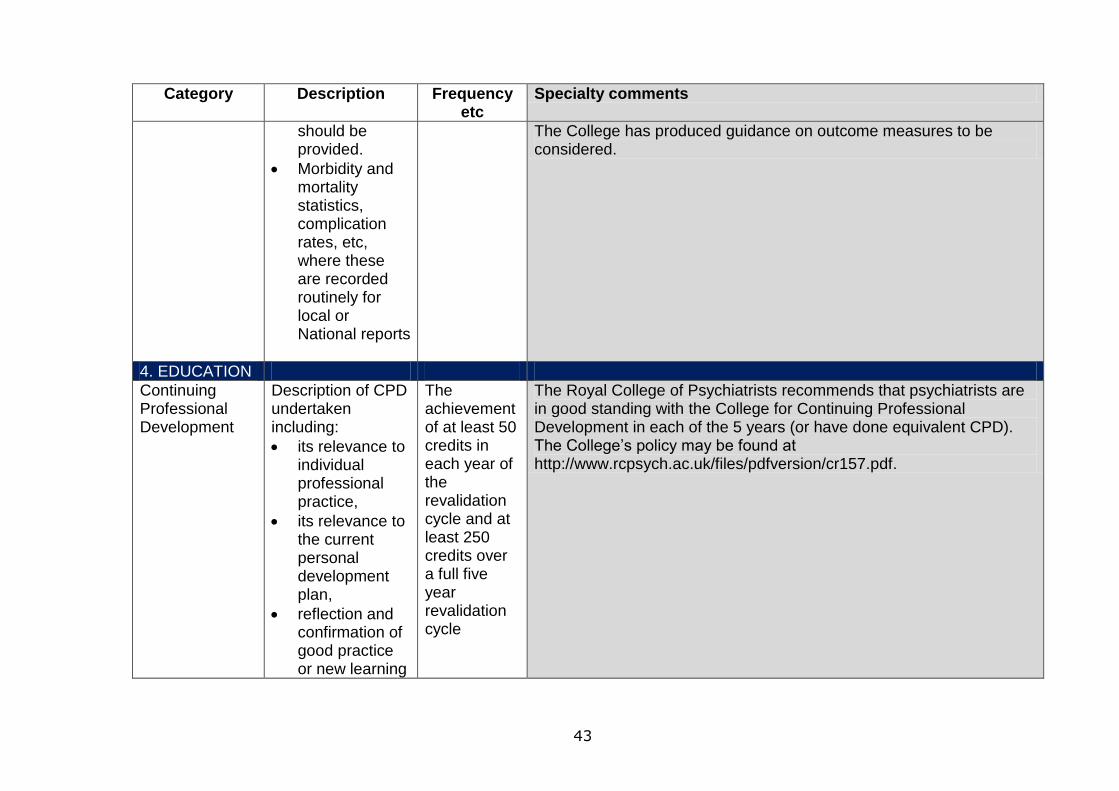
43
Category Description Frequency etc
Specialty comments
should be provided.
Morbidity and mortality statistics, complication rates, etc, where these are recorded routinely for local or National reports
The College has produced guidance on outcome measures to be considered.
4. EDUCATION
Continuing Professional Development
Description of CPD undertaken including:
its relevance to individual professional practice,
its relevance to the current personal development plan,
reflection and confirmation of good practice or new learning
The achievement of at least 50 credits in each year of the revalidation cycle and at least 250 credits over a full five year revalidation cycle
The Royal College of Psychiatrists recommends that psychiatrists are in good standing with the College for Continuing Professional Development in each of the 5 years (or have done equivalent CPD). The College’s policy may be found at http://www.rcpsych.ac.uk/files/pdfversion/cr157.pdf.
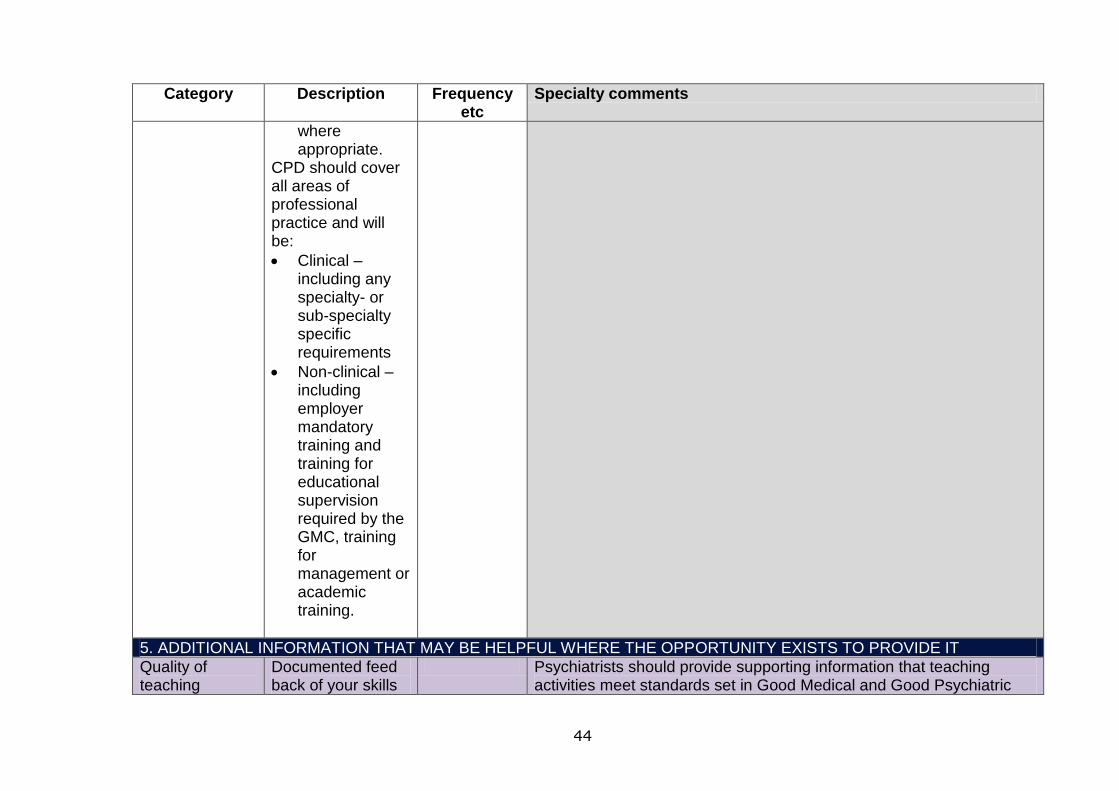
44
Category Description Frequency etc
Specialty comments
where appropriate.
CPD should cover all areas of professional practice and will be:
Clinical – including any specialty- or sub-specialty specific requirements
Non-clinical – including employer mandatory training and training for educational supervision required by the GMC, training for management or academic training.
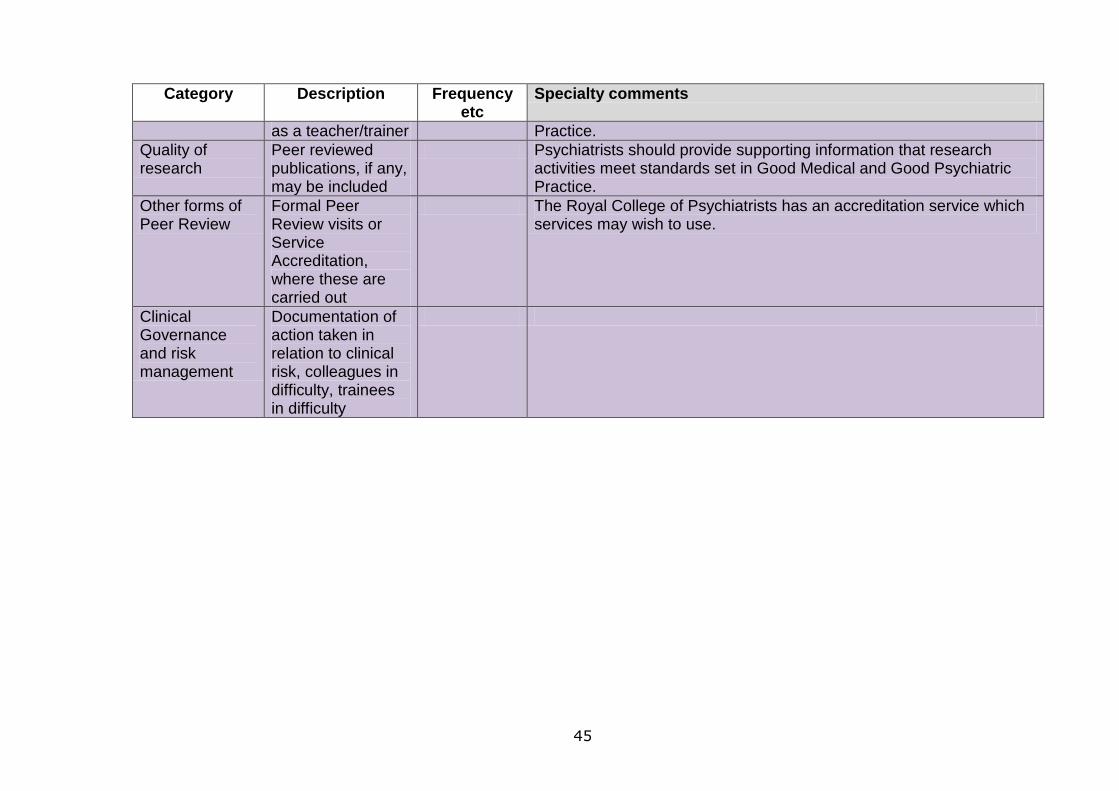
5. ADDITIONAL INFORMATION THAT MAY BE HELPFUL WHERE THE OPPORTUNITY EXISTS TO PROVIDE IT
Quality of teaching
Documented feed back of your skills
Psychiatrists should provide supporting information that teaching activities meet standards set in Good Medical and Good Psychiatric
45
Category Description Frequency etc
Specialty comments
as a teacher/trainer Practice.
Quality of research
Peer reviewed publications, if any, may be included
Psychiatrists should provide supporting information that research activities meet standards set in Good Medical and Good Psychiatric Practice.
Other forms of Peer Review
Formal Peer Review visits or Service Accreditation, where these are carried out
The Royal College of Psychiatrists has an accreditation service which services may wish to use.
Clinical Governance and risk management
Documentation of action taken in relation to clinical risk, colleagues in difficulty, trainees in difficulty
46
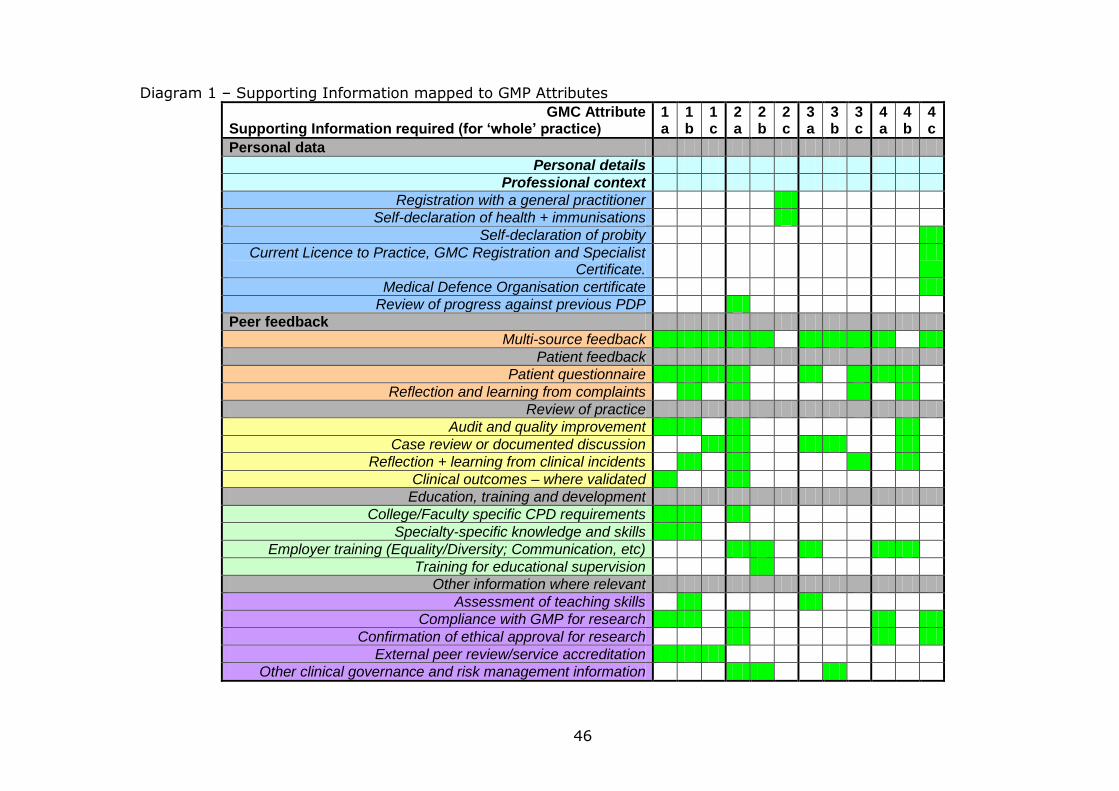
Diagram 1 – Supporting Information mapped to GMP Attributes
GMC Attribute Supporting Information required (for ‘whole’ practice)
1a
1b
1c
2a
2b
2c
3a
3b
3c
4a
4b
4c
Personal data
Personal details
Professional context
Registration with a general practitioner
Self-declaration of health + immunisations
Self-declaration of probity
Current Licence to Practice, GMC Registration and Specialist Certificate.
Medical Defence Organisation certificate
Review of progress against previous PDP
Peer feedback
Multi-source feedback
Patient feedback
Patient questionnaire
Reflection and learning from complaints
Review of practice
Audit and quality improvement
Case review or documented discussion
Reflection + learning from clinical incidents
Clinical outcomes – where validated
Education, training and development
College/Faculty specific CPD requirements
Specialty-specific knowledge and skills
Employer training (Equality/Diversity; Communication, etc)
Training for educational supervision
Other information where relevant
Assessment of teaching skills
Compliance with GMP for research
Confirmation of ethical approval for research
External peer review/service accreditation
Other clinical governance and risk management information
47
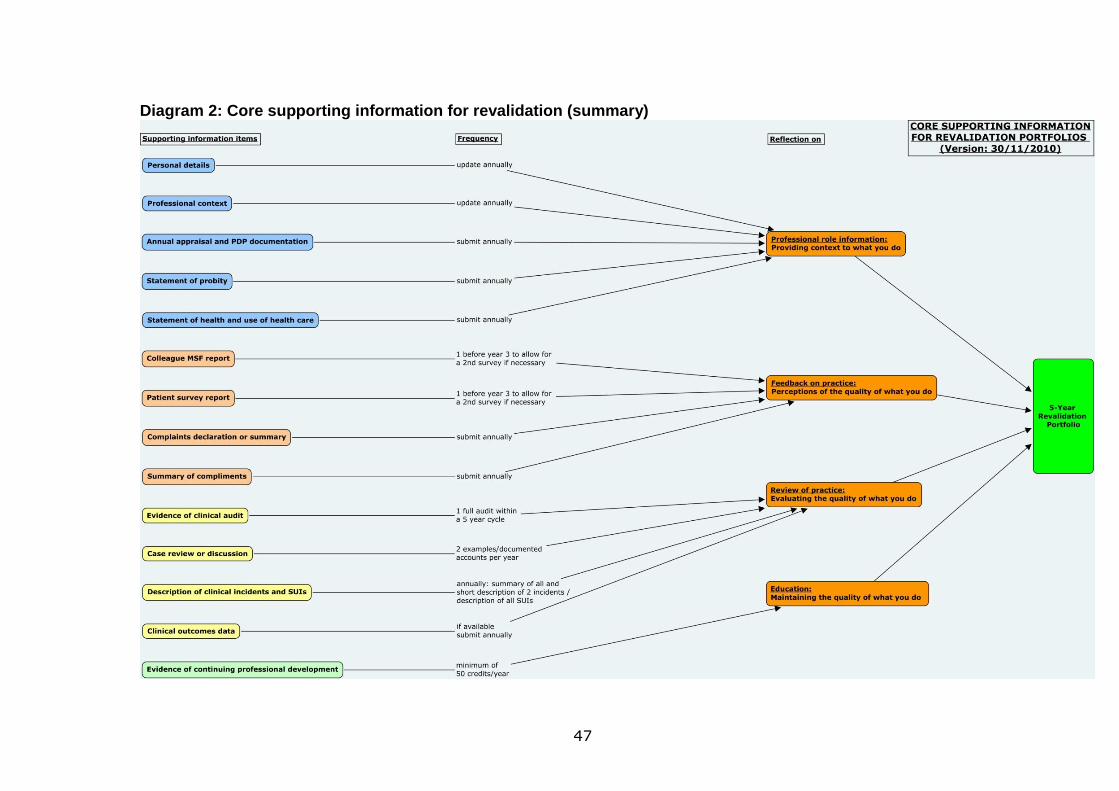
Diagram 2: Core supporting information for revalidation (summary)
48
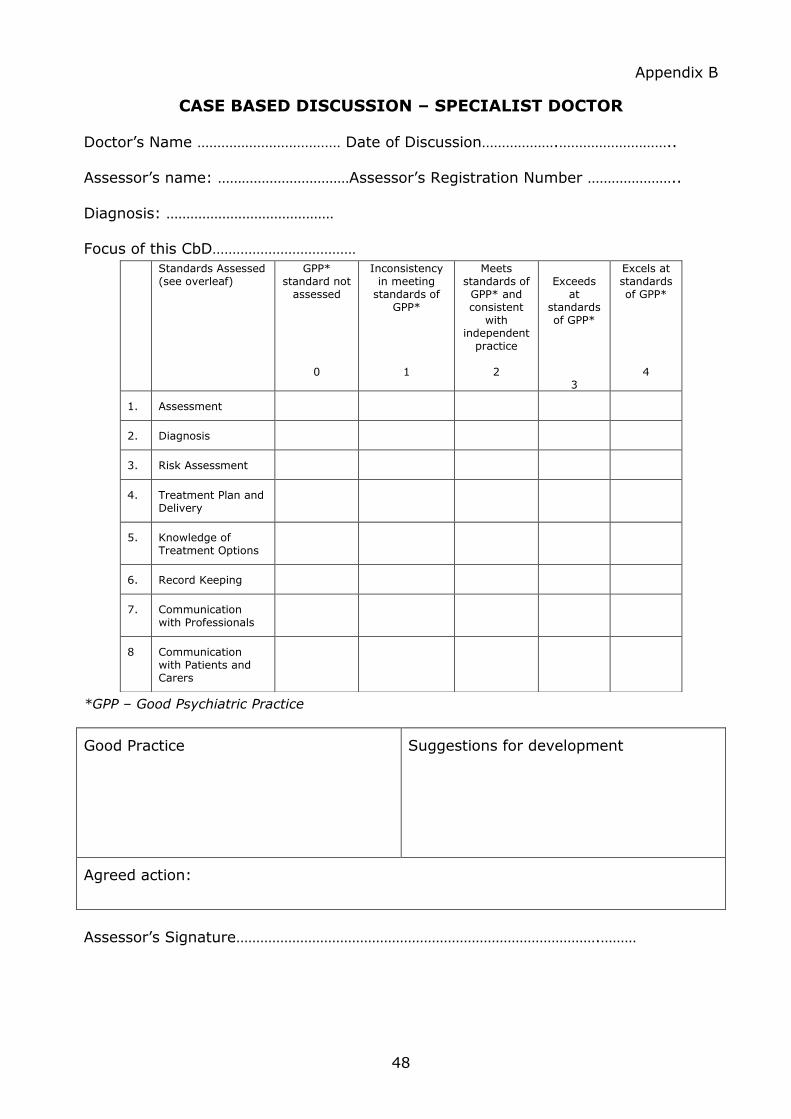
Appendix B
CASE BASED DISCUSSION – SPECIALIST DOCTOR
Doctor‟s Name ……………………………… Date of Discussion……………….………………………..
Assessor‟s name: ……………………………Assessor‟s Registration Number …………………..
Diagnosis: …………………………………… Focus of this CbD………………………………
*GPP – Good Psychiatric Practice
Good Practice Suggestions for development
Agreed action:
Assessor‟s Signature……………………………………………………………………………….………
Standards Assessed (see overleaf)
GPP* standard not
assessed 0
Inconsistency in meeting
standards of GPP*
1
Meets standards of GPP* and consistent
with independent
practice 2
Exceeds
at standards of GPP*
3
Excels at standards of GPP*
4
1. Assessment
2. Diagnosis
3. Risk Assessment
4. Treatment Plan and Delivery
5. Knowledge of Treatment Options
6. Record Keeping
7. Communication with Professionals
8 Communication with Patients and Carers
49
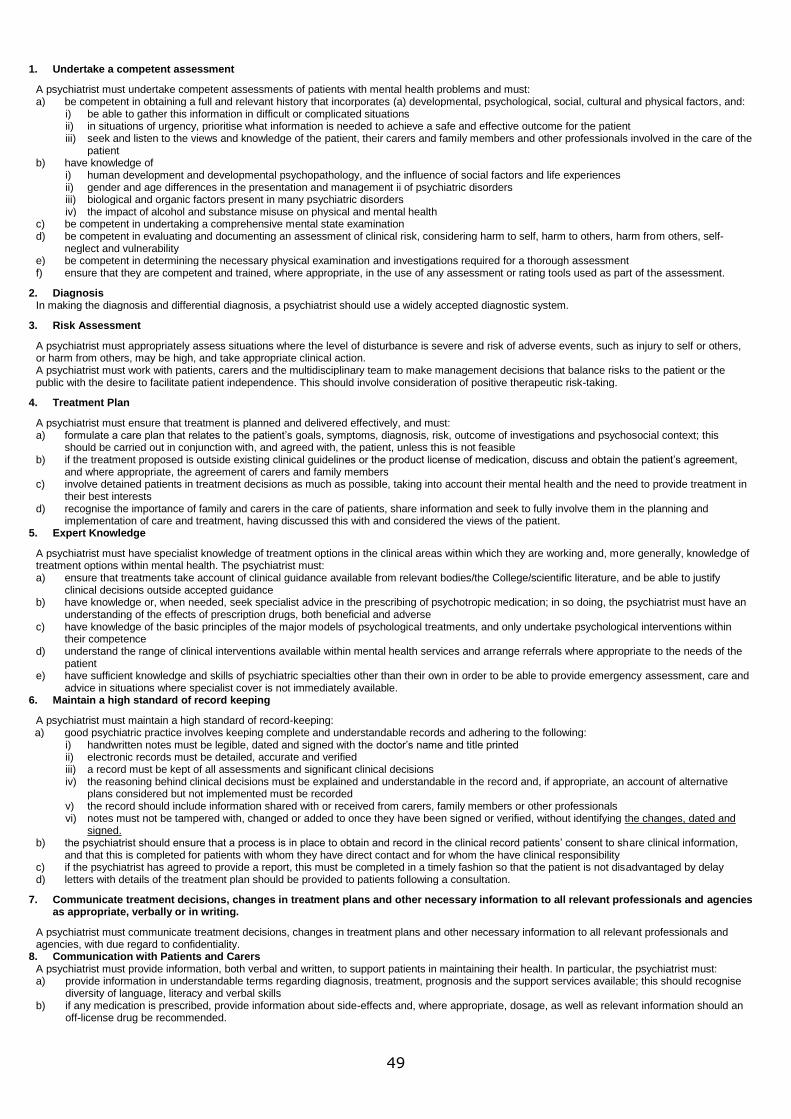
1. Undertake a competent assessment
A psychiatrist must undertake competent assessments of patients with mental health problems and must: a) be competent in obtaining a full and relevant history that incorporates (a) developmental, psychological, social, cultural and physical factors, and:
i) be able to gather this information in difficult or complicated situations ii) in situations of urgency, prioritise what information is needed to achieve a safe and effective outcome for the patient iii) seek and listen to the views and knowledge of the patient, their carers and family members and other professionals involved in the care of the
patient b) have knowledge of
i) human development and developmental psychopathology, and the influence of social factors and life experiences ii) gender and age differences in the presentation and management ii of psychiatric disorders iii) biological and organic factors present in many psychiatric disorders iv) the impact of alcohol and substance misuse on physical and mental health
c) be competent in undertaking a comprehensive mental state examination d) be competent in evaluating and documenting an assessment of clinical risk, considering harm to self, harm to others, harm from others, self-
neglect and vulnerability e) be competent in determining the necessary physical examination and investigations required for a thorough assessment f) ensure that they are competent and trained, where appropriate, in the use of any assessment or rating tools used as part of the assessment.
2. Diagnosis In making the diagnosis and differential diagnosis, a psychiatrist should use a widely accepted diagnostic system.
3. Risk Assessment
A psychiatrist must appropriately assess situations where the level of disturbance is severe and risk of adverse events, such as injury to self or others, or harm from others, may be high, and take appropriate clinical action. A psychiatrist must work with patients, carers and the multidisciplinary team to make management decisions that balance risks to the patient or the public with the desire to facilitate patient independence. This should involve consideration of positive therapeutic risk-taking.
4. Treatment Plan
A psychiatrist must ensure that treatment is planned and delivered effectively, and must: a) formulate a care plan that relates to the patient’s goals, symptoms, diagnosis, risk, outcome of investigations and psychosocial context; this
should be carried out in conjunction with, and agreed with, the patient, unless this is not feasible b) if the treatment proposed is outside existing clinical guidelines or the product license of medication, discuss and obtain the patient’s agreement,
and where appropriate, the agreement of carers and family members c) involve detained patients in treatment decisions as much as possible, taking into account their mental health and the need to provide treatment in
their best interests d) recognise the importance of family and carers in the care of patients, share information and seek to fully involve them in the planning and
implementation of care and treatment, having discussed this with and considered the views of the patient. 5. Expert Knowledge
A psychiatrist must have specialist knowledge of treatment options in the clinical areas within which they are working and, more generally, knowledge of treatment options within mental health. The psychiatrist must: a) ensure that treatments take account of clinical guidance available from relevant bodies/the College/scientific literature, and be able to justify
clinical decisions outside accepted guidance b) have knowledge or, when needed, seek specialist advice in the prescribing of psychotropic medication; in so doing, the psychiatrist must have an
understanding of the effects of prescription drugs, both beneficial and adverse c) have knowledge of the basic principles of the major models of psychological treatments, and only undertake psychological interventions within
their competence d) understand the range of clinical interventions available within mental health services and arrange referrals where appropriate to the needs of the
patient e) have sufficient knowledge and skills of psychiatric specialties other than their own in order to be able to provide emergency assessment, care and
advice in situations where specialist cover is not immediately available. 6. Maintain a high standard of record keeping
A psychiatrist must maintain a high standard of record-keeping: a) good psychiatric practice involves keeping complete and understandable records and adhering to the following:
i) handwritten notes must be legible, dated and signed with the doctor’s name and title printed ii) electronic records must be detailed, accurate and verified iii) a record must be kept of all assessments and significant clinical decisions iv) the reasoning behind clinical decisions must be explained and understandable in the record and, if appropriate, an account of alternative
plans considered but not implemented must be recorded v) the record should include information shared with or received from carers, family members or other professionals vi) notes must not be tampered with, changed or added to once they have been signed or verified, without identifying the changes, dated and
signed. b) the psychiatrist should ensure that a process is in place to obtain and record in the clinical record patients’ consent to share clinical information,
and that this is completed for patients with whom they have direct contact and for whom the have clinical responsibility c) if the psychiatrist has agreed to provide a report, this must be completed in a timely fashion so that the patient is not disadvantaged by delay d) letters with details of the treatment plan should be provided to patients following a consultation.
7. Communicate treatment decisions, changes in treatment plans and other necessary information to all relevant professionals and agencies as appropriate, verbally or in writing.
A psychiatrist must communicate treatment decisions, changes in treatment plans and other necessary information to all relevant professionals and agencies, with due regard to confidentiality.
8. Communication with Patients and Carers A psychiatrist must provide information, both verbal and written, to support patients in maintaining their health. In particular, the psychiatrist must: a) provide information in understandable terms regarding diagnosis, treatment, prognosis and the support services available; this should recognise
diversity of language, literacy and verbal skills b) if any medication is prescribed, provide information about side-effects and, where appropriate, dosage, as well as relevant information should an
off-license drug be recommended.
50
Appendix C
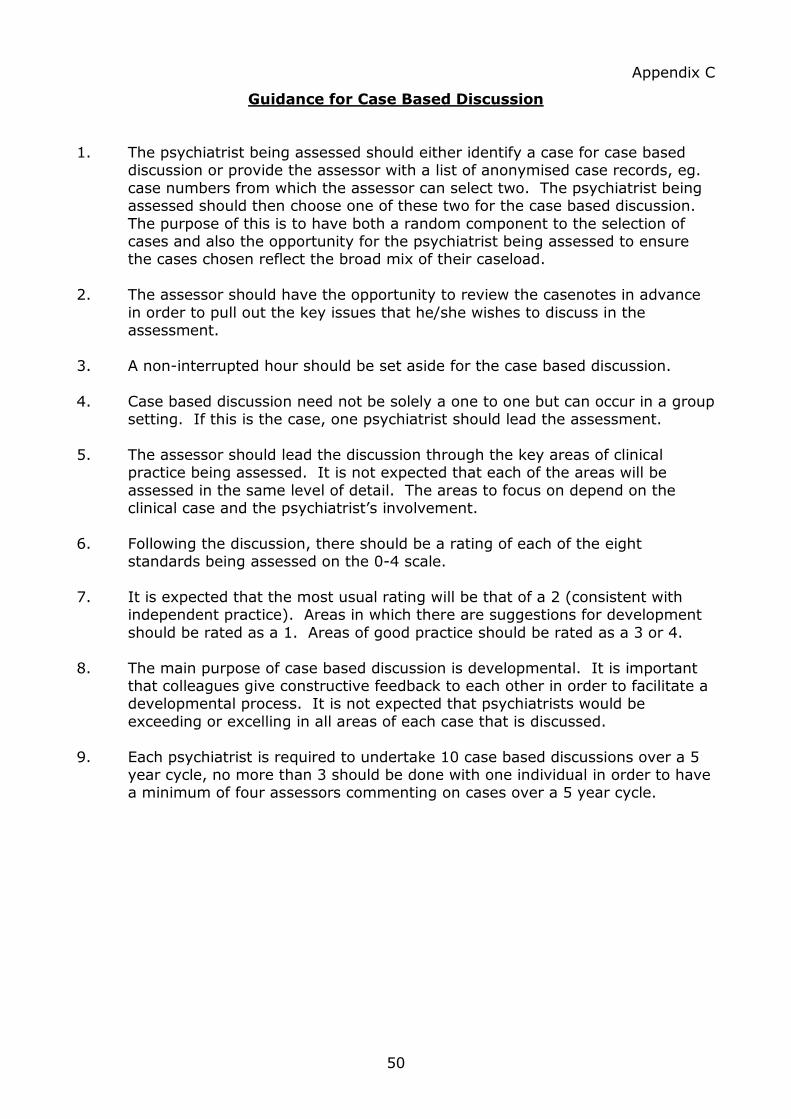
Guidance for Case Based Discussion
1. The psychiatrist being assessed should either identify a case for case based discussion or provide the assessor with a list of anonymised case records, eg.
case numbers from which the assessor can select two. The psychiatrist being assessed should then choose one of these two for the case based discussion.
The purpose of this is to have both a random component to the selection of cases and also the opportunity for the psychiatrist being assessed to ensure the cases chosen reflect the broad mix of their caseload.
2. The assessor should have the opportunity to review the casenotes in advance
in order to pull out the key issues that he/she wishes to discuss in the assessment.
3. A non-interrupted hour should be set aside for the case based discussion.
4. Case based discussion need not be solely a one to one but can occur in a group setting. If this is the case, one psychiatrist should lead the assessment.
5. The assessor should lead the discussion through the key areas of clinical practice being assessed. It is not expected that each of the areas will be
assessed in the same level of detail. The areas to focus on depend on the clinical case and the psychiatrist‟s involvement.
6. Following the discussion, there should be a rating of each of the eight standards being assessed on the 0-4 scale.
7. It is expected that the most usual rating will be that of a 2 (consistent with
independent practice). Areas in which there are suggestions for development
should be rated as a 1. Areas of good practice should be rated as a 3 or 4.
8. The main purpose of case based discussion is developmental. It is important that colleagues give constructive feedback to each other in order to facilitate a developmental process. It is not expected that psychiatrists would be
exceeding or excelling in all areas of each case that is discussed.
9. Each psychiatrist is required to undertake 10 case based discussions over a 5 year cycle, no more than 3 should be done with one individual in order to have a minimum of four assessors commenting on cases over a 5 year cycle.
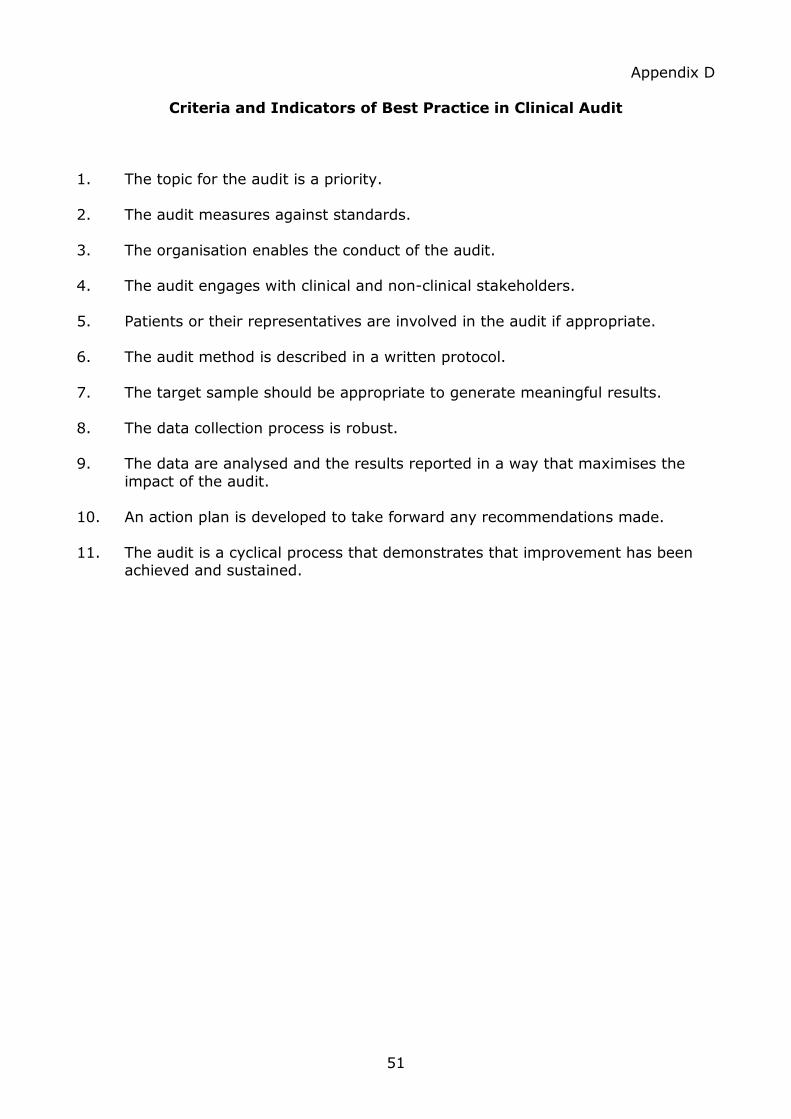
51
Appendix D
Criteria and Indicators of Best Practice in Clinical Audit
1. The topic for the audit is a priority.
2. The audit measures against standards.
3. The organisation enables the conduct of the audit. 4. The audit engages with clinical and non-clinical stakeholders.
5. Patients or their representatives are involved in the audit if appropriate.
6. The audit method is described in a written protocol.
7. The target sample should be appropriate to generate meaningful results.
8. The data collection process is robust. 9. The data are analysed and the results reported in a way that maximises the
impact of the audit.
10. An action plan is developed to take forward any recommendations made.
11. The audit is a cyclical process that demonstrates that improvement has been achieved and sustained.
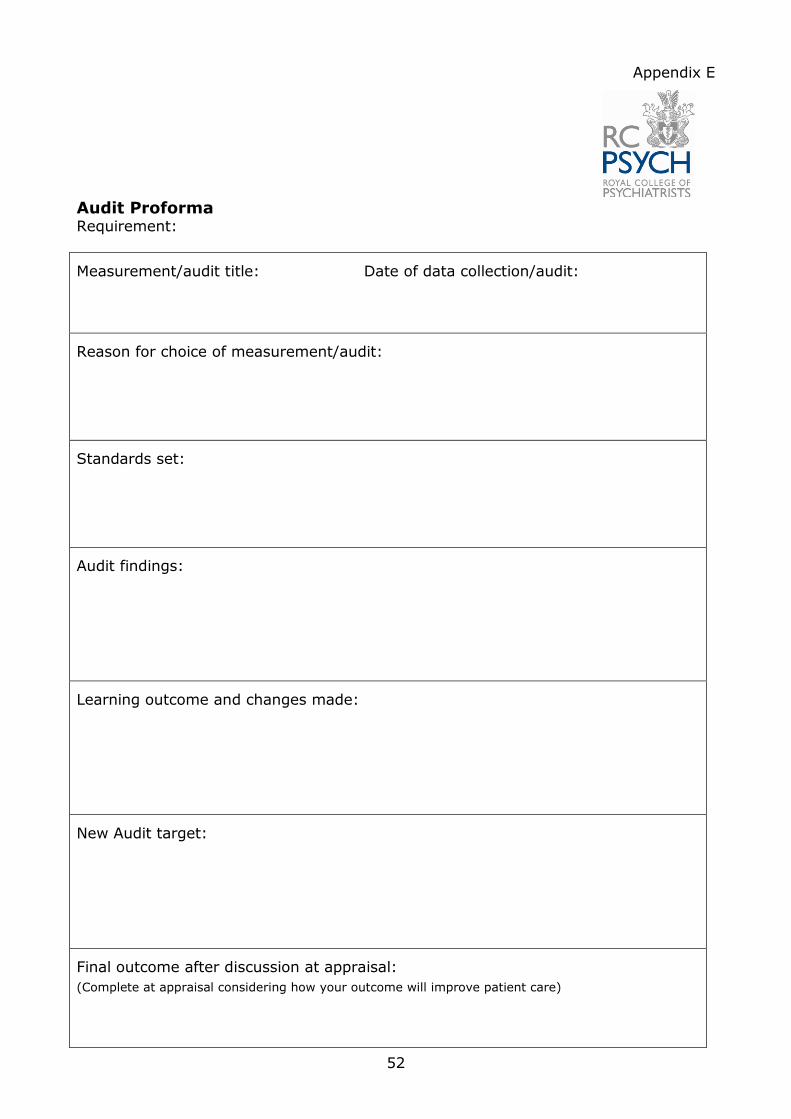
52
Appendix E
Audit Proforma Requirement:
Measurement/audit title: Date of data collection/audit:
Reason for choice of measurement/audit:
Standards set:
Audit findings:
Learning outcome and changes made:
New Audit target:
Final outcome after discussion at appraisal:
(Complete at appraisal considering how your outcome will improve patient care)
53
Appendix F
Multi-source Feedback Colleague Structured Reflective Template Requirement: one every five years
Date of feedback:
Feedback scheme used:
Number of colleagues giving feedback:
Name and designation of person who collated and gave feedback:
Main outcomes of feedback:
Hints: Look at positive outcomes, as well as learning needs:
What learning might I undertake?
Hint: It may help to separate learning from changing your behaviour. So, rather than “I will show
more respect to nursing colleagues”, it might be more productive to undertake learning which
develops your understanding of the benefits of the diversity of teams. Your ideas in this section can
be discussed further with your appraiser.
Final outcome after discussion at appraisal:
(Complete at appraisal considering how your outcome will improve patient care)
54
Appendix G
Multi-source Feedback Patient/Carer Structured Reflective Template Requirement: one every five years
Date of feedback:
Feedback scheme used:
Number of patients giving feedback:
Name and designation of person who collated and gave feedback:
Main outcomes of feedback:
Hints: Look at positive outcomes, as well as learning needs:
What learning might I undertake?
Hint: To think about feedback from patients from marginalised groups. To consider involvement with
a local patient or carer group.
Final outcome after discussion at appraisal:
(Complete at appraisal considering how your outcome will improve patient care)
55
Appendix H
Significant Event Structured Reflective Template Requirement: one for each significant event
Date of incident:
Description of events:
What went well?
What could have been done better?
What changes have been agreed?
Personally:
For the team:
Final outcome after discussion at appraisal:
(Complete at appraisal considering how your outcome will improve patient care)
56
Appendix I
Complaint Report Structured Reflective Template
Requirement: one for each complaint you have received.
Date of Complaint:
Key Issues of Complaint:
Involvement of other bodies: Responsible organisation / SHA / NCAA / GMC /
Other
If resolved, what were the findings:
What did I learn from this complaint:
How will my practice change?
Final outcome after discussion at appraisal:
(Complete at appraisal considering how your outcome will improve patient care)

















