Int J Clin Exp Med 2019;12(5):4528-4539 www.ijcem.com /ISSN:1940-5901/IJCEM0086007 Review Article Loss of dominance of ticagrelor over clopidogrel in East Asian patients with acute coronary syndrome Bo Li 1 , Xiaodong Jin 1 , Linlin Wang 4 , Lifang Cui 2 , Yunhe Zhao 1 , Bin Meng 1 , Bo Yin 1 , Jingbin Yu 1 , Chenglong Bi 1 , Tongtong Zhang 3 , Zhiyong Wang 5 Departments of 1 Cardiology, 2 Hyperbaric Oxygen, 3 Clinical Laboratory, Central Hospital of Zibo, NO. 54, Gong Qing Tuan Xi Road, Zibo 255036, Shandong, PR China; 4 Department of Internal Medicine, Zibo Municipal Hospital, NO. 24-3, Ren Min Xi Road, Zibo 255036, Shandong, PR China; 5 Department of Emergency Surgery, Qilu Hospital of Shandong University, Ji’nan 250012, Shandong, PR China Received May 9, 2018; Accepted February 11, 2019; Epub May 15, 2019; Published May 30, 2019 Abstract: Objectives: The superiority of ticagrelor in acute coronary syndrome (ACS) has been challenged in East Asian patients. The aim of this analysis is to determine whether ticagrelor is superior to clopidogrel in East Asian patients with ACS. Methods: A meta-analysis that compared ticagrelor with clopidogrel in East Asian patients with ACS was performed. Embase, PubMed, and the Cochrane Library were searched for relevant trials with data on the primary efficacy endpoints and adverse effects. Results: A total of 4 randomized trials, 1 prospective cohort study, and 2 retrospective pilot studies with 5,360 subjects were included in this analysis. Although there was no statisti- cal significance regarding the primary efficacy endpoints and cardiovascular death (CV death) among the RCTs, the superiorities of ticagrelor were shown in combination with the non-RCTs. No difference was found in all-causes of death and myocardial infarction (MI), whether regarding the RCT results or the integrated results. There was no difference in major bleeding between the 2 agents among the RCTs, but after combination with the non-RCTs, clopi- dogrel seemed to be better than ticagrelor. Clopidogrel was markedly superior to ticagrelor in terms of all bleeding and dyspnea. Conclusions: Ticagrelor did not show an absolute advantage in East Asian patients according to the current data from RCTs but seemed to be marginally better than clopidogrel when taking all the trials into account. Clopidogrel also did not show a marked superiority in major bleeding in East Asian patients, but significantly de- creased the incidences of all-cause bleeding and dyspnea. Keywords: Ticagrelor, clopidogrel, acute coronary syndrome, East Asian patients Introduction The new class of adenosine diphosphate (ADP) receptor, the antagonist ticagrelor, has shown its characteristic of reversible, direct and fast onset of action, and it provides faster, greater, and more consistent P2Y12 inhibition [1-3]. In the PLATO study [3], treatment with ticagrelor (180 mg loading dose and 90 mg twice daily) significantly reduced the death rate from vas- cular causes, myocardial infarction, and stroke in patients with acute coronary syndrome, com- pared with clopidogrel (300 to 600 mg loading dose and 75 mg daily). From then on, ticagrelor has been recommended as superior to clopido- grel by several clinical management guidelines for P2Y12 inhibition in patients with ACS [4-6]. In China, both the guidelines for percutaneous coronary intervention and the emergency rapid diagnosis and treatment guidelines for acute coronary syndrome have also recommended ticagrelor over clopidogrel in patients undergo- ing PCI and in patients with ACS. However, more and more data suggest that al- though East Asian patients have a higher level of platelet reactivity, they seem to have a lower rate of ischemic events after PCI compared with Caucasians, which is known as the “East Asian paradox” [7]. Therefore, the efficacy and safety of antiplatelet agents may differ between Asian and Caucasian patients. Although the PLATO study has shown the tremendous superi- ority of ticagrelor, only 6% of those enrolled in the study were patients from Asia, so it is diffi- cult to apply the results to other individual
Transcript
Int J Clin Exp Med 2019;12(5):4528-4539www.ijcem.com /ISSN:1940-5901/IJCEM0086007
Review ArticleLoss of dominance of ticagrelor over clopidogrel in East Asian patients with acute coronary syndrome
Bo Li1, Xiaodong Jin1, Linlin Wang4, Lifang Cui2, Yunhe Zhao1, Bin Meng1, Bo Yin1, Jingbin Yu1, Chenglong Bi1, Tongtong Zhang3, Zhiyong Wang5
Departments of 1Cardiology, 2Hyperbaric Oxygen, 3Clinical Laboratory, Central Hospital of Zibo, NO. 54, Gong Qing Tuan Xi Road, Zibo 255036, Shandong, PR China; 4Department of Internal Medicine, Zibo Municipal Hospital, NO. 24-3, Ren Min Xi Road, Zibo 255036, Shandong, PR China; 5Department of Emergency Surgery, Qilu Hospital of Shandong University, Ji’nan 250012, Shandong, PR China
Received May 9, 2018; Accepted February 11, 2019; Epub May 15, 2019; Published May 30, 2019
Abstract: Objectives: The superiority of ticagrelor in acute coronary syndrome (ACS) has been challenged in East Asian patients. The aim of this analysis is to determine whether ticagrelor is superior to clopidogrel in East Asian patients with ACS. Methods: A meta-analysis that compared ticagrelor with clopidogrel in East Asian patients with ACS was performed. Embase, PubMed, and the Cochrane Library were searched for relevant trials with data on the primary efficacy endpoints and adverse effects. Results: A total of 4 randomized trials, 1 prospective cohort study, and 2 retrospective pilot studies with 5,360 subjects were included in this analysis. Although there was no statisti-cal significance regarding the primary efficacy endpoints and cardiovascular death (CV death) among the RCTs, the superiorities of ticagrelor were shown in combination with the non-RCTs. No difference was found in all-causes of death and myocardial infarction (MI), whether regarding the RCT results or the integrated results. There was no difference in major bleeding between the 2 agents among the RCTs, but after combination with the non-RCTs, clopi-dogrel seemed to be better than ticagrelor. Clopidogrel was markedly superior to ticagrelor in terms of all bleeding and dyspnea. Conclusions: Ticagrelor did not show an absolute advantage in East Asian patients according to the current data from RCTs but seemed to be marginally better than clopidogrel when taking all the trials into account. Clopidogrel also did not show a marked superiority in major bleeding in East Asian patients, but significantly de-creased the incidences of all-cause bleeding and dyspnea.
Keywords: Ticagrelor, clopidogrel, acute coronary syndrome, East Asian patients
Introduction
The new class of adenosine diphosphate (ADP) receptor, the antagonist ticagrelor, has shown its characteristic of reversible, direct and fast onset of action, and it provides faster, greater, and more consistent P2Y12 inhibition [1-3]. In the PLATO study [3], treatment with ticagrelor (180 mg loading dose and 90 mg twice daily) significantly reduced the death rate from vas-cular causes, myocardial infarction, and stroke in patients with acute coronary syndrome, com-pared with clopidogrel (300 to 600 mg loading dose and 75 mg daily). From then on, ticagrelor has been recommended as superior to clopido-grel by several clinical management guidelines for P2Y12 inhibition in patients with ACS [4-6]. In China, both the guidelines for percutaneous
coronary intervention and the emergency rapid diagnosis and treatment guidelines for acute coronary syndrome have also recommended ticagrelor over clopidogrel in patients undergo-ing PCI and in patients with ACS.
However, more and more data suggest that al- though East Asian patients have a higher level of platelet reactivity, they seem to have a lower rate of ischemic events after PCI compared with Caucasians, which is known as the “East Asian paradox” [7]. Therefore, the efficacy and safety of antiplatelet agents may differ between Asian and Caucasian patients. Although the PLATO study has shown the tremendous superi-ority of ticagrelor, only 6% of those enrolled in the study were patients from Asia, so it is diffi-cult to apply the results to other individual
Ticagrelor vs. clopidogrel in East Asian patients with ACS
4529 Int J Clin Exp Med 2019;12(5):4528-4539
national regions, especially East Asia. In the PHILO study [8], the investigators enrolled ACS patients from Japan, Taiwan and South Korea, and the results showed that the rate of the composite endpoints (myocardial infarction, stroke or death from vascular causes) were slightly higher, albeit without statistical signifi-cance, in the ticagrelor group compared with the clopidogrel group. In Chen’s multicenter ret-rospective pilot study [9], during the half-year follow-up, ticagrelor did not show a significant effect on the primary efficacy endpoint in the overall cohort, but only in the matched cohort, ticagrelor showed a lower incidence of primary endpoint. Moreover, the study from Korea Acu- te Myocardial Infarction Registry-National Ins- titute of Health also showed that ticagrelor not only didn’t reduce ischemic events, but it incr- eased the risk of bleeding complications com-pared with clopidogrel [10]. Accordingly, it is essential for us to pool all of the currently avail-able comparative data to determine whether ticagrelor is superior to clopidogrel in East Asi- an patients with ACS.
Methods
The preferred Reporting Items for systematic reviews and meta-analyses of individual partici-pant data (the PRISMA-IPD) statement was fol-lowed for the conduct and reporting of this meta-analysis [11].
Data source, search strategy, and inclusion criteria
In order to identify all the studies comparing the efficacy and safety of ticagrelor versus clop-idogrel, EMBASE, PubMed, and the Cochrane Library of Trials were carefully searched for articles published from January 2009 to May 2017. The following search terms or key words were used alone or in combination: ‘ticagrelor’, ‘clopidogrel’, ‘AR C124910XX’, ‘P2Y12 inhibi-tor’, ‘acute coronary syndrome’, ‘myocardial in- farction’, ‘Non-ST-elevation myocardial infarc-tion’, and ‘unstable angina’.
The inclusion criteria were as follows: (1) com-parative studies: randomized controlled trials RCTs or non-RCTs published in English; (2) study population: more than 100 participants were included in the study, and the participants were from East Asian countries or regions; (3) study intervention: the patients in the treat-ment group received ticagrelor, and the patients
in the control group received clopidogrel; (4) parameters: the primary outcome of major ad- verse cardiovascular events (MACE) and adver- se events should be given. (5) treatment dura-tion: no shorter than 6 months. Case reports, nonhuman studies, studies without adequate information, studies lacking a control group, and studies without East Asia patient data were excluded in the present meta analysis.
Data extraction and study quality assessment
Two investigators (BL and YZ) individually revi- ewed the full articles that met the inclusion cri-teria and extracted the data. The following items were extracted from the included stud-ies: (1) general data: the titles of the included articles, first author, publication names, year of publication; (2) study design: patient character-istics, sample size, duration, and methods of intervention, type of control, drug dose; (3) out-come index: mortality rate, and adverse events. The Cochrane Collaboration’s tool was followed to assess the risk of bias, including: random sequence generation, allocation concealment, the blinding of the participants and the person-nel, the blinding of the outcome assessment, incomplete outcome data, selective reporting, and other sources of bias.
Data synthesis and statistical analysis
All analyses were performed using RevMan software version 5.3. Pooled risk ratios (RR) with 95% CIs were presented for dichotomous outcomes (e.g. the composite endpoints: death from vascular causes, myocardial infarction, or stroke, and adverse effects, such as bleeding). The results of the included studies were per-formed with fixed-effect models (Mantel-Haen- szel method) [12] or random-effect models in cases of significant heterogeneity between es- timates [13]. We used the I2 statistics to assess the magnitude of heterogeneity: 25%, 50%, and 75% represented low, moderate, and high degrees of heterogeneity, respectively. The ch- oice of the proper effect model was based on the analysis results: the fixed effect model was used if I2 < 50%, and the random effect model was used if I2 ≥ 50% [14].
Results
Selected studies and baseline characteristics
After initially identifying 11084 potential trials, 3573 duplicate documents were identified. Of
Ticagrelor vs. clopidogrel in East Asian patients with ACS
4530 Int J Clin Exp Med 2019;12(5):4528-4539
Figure 1. Flow diagram of the study selection process.
Ticagrelor vs. clopidogrel in East Asian patients with ACS
4531 Int J Clin Exp Med 2019;12(5):4528-4539
Table 1. Baselines characteristics of the 7 included trials
Study Type of study Follow-up Population
Drug DoseMACEs definitions Major bleeding definitions
Ticagrelor ClopidogrelPHILO 2015 RCT 12 months Patients from
Japanese, Taiwanese and South Korean
180 mg loading dose and 90 mg twice daily
300 mg loading dose and 75 mg once daily
The composite endpoint of spontaneous MI, stroke, or CV death
Fatal bleeding, intracranial bleeding, intrapericardial bleeding with cardiac tamponade, hypovolemic shock or severe hypotension due to bleeding and requiring vasopressors or surgery, decline in hemoglobin ≥ 5.0 g/dl, or the need for transfusion of at least 4 units of whole blood or packed red blood cells.
PLATO 2015 RCT 12 months East Asian patients from South Korea, China, and Hong Kong
180 mg loading dose and 90 mg twice daily
300 mg loading dose and 75 mg once daily
The composite of death from vascular causes, MI, or stroke
The safety end points consisted of bleeding (PLATO-defined major bleeding, non-CABG related major bleeding, and fatal bleeding).
Tang 2016 RCT 6 months Patients from China A loading dose of 180 mg prior to PPCI followed by 90 mg twice daily for one years post-PPCI
A loading dose of 600 mg prior to PPCI followed by 75 mg once daily for one year post-PPCI
The composite of overall death, MI, unplanned revascularization or stroke
Bleeding events defined by the Thrombolysis in Myocardial Infarction (TIMI) criteria.
Wang 2016 RCT 12 months Patients older than 65 years from China
180 mg loading dose and 90 mg twice daily
300 mg loading dose and 75 mg once daily
The composite of MI, stroke, or CV death
PLATO major bleeding (life-threatening and others).
Chen 2016 A multicenter retrospective pilot study
164.3 ± 116.4 days
Patients from Taiwan - - The primary PLATO composite efficacy endpoints: death from vascular causes, MI, or stroke
The first PLATO-defined and PLATO-adjudicated major bleeding event.
Park 2016 A prospective, multicenter, cohort study
6 months Patients from Korea 180 mg loading dose and 90 mg twice daily
300-600 mg loading dose and 75 mg once daily
The composite of cardiac death, non-fatal MI, stroke, and clinically-driven target vessel revascularization
Thrombolysis in Myocardial Infarction (TIMI) major bleeding.
Xin 2017 A retrospective study
6 months Patients from China 180 mg loading dose and 90 mg twice daily
300 mg loading dose and 75 mg or 150 mg daily
A composite of death from cardiovascular diseases, nonfatal myocardial infarction, nonfatal stroke, in-stent thrombosis and target vessel revascularization
TIMI major bleeding: (1) fatal bleeding; (2)intra-cranial bleeding; (3) intrapericardial bleeding with cardiac tamponade; (4) hypovolemic shock or severe hypotension due to bleeding and requiring pressors or surgery, a decline in the hemoglobin level of 5.0 g per deciliter or more.
Ticagrelor vs. clopidogrel in East Asian patients with ACS
4532 Int J Clin Exp Med 2019;12(5):4528-4539
endpoints between the treatment of ticagrelor and clopidogrel. The heterogeneity test result of the 7 studies was calculated as I2 = 52%. Therefore, the random effect model was used for further analyses. The total results from all of the 7 included studies (with a total amount of 5360 patients) showed that the incidence of the primary efficacy endpoints was statistically significantly lower in patients with ticagrelor compared to patients with clopidogrel [RR = 0.68, 95% CI (0.49, 0.95), Z = 2.26, P = 0.02] (Figure 4). The meta-analysis of the 3 non-RCTs (3408 patients) also showed a statistically sig-nificant reduction in patients with ticagrelor compared to patients with clopidogrel [RR = 0.61, 95% CI (0.44, 0.83), Z = 3.12, P = 0.002], but the results of the 4 RCTs (1952 patients) did not show the same effect [RR = 0.73, 95%CI (0.40, 1.31), Z = 1.06, P = 0.29] (Figure 4).
Then we respectively compared the differences of all-causes of death, cardiovascular death, and myocardial infarction. With respect to all-
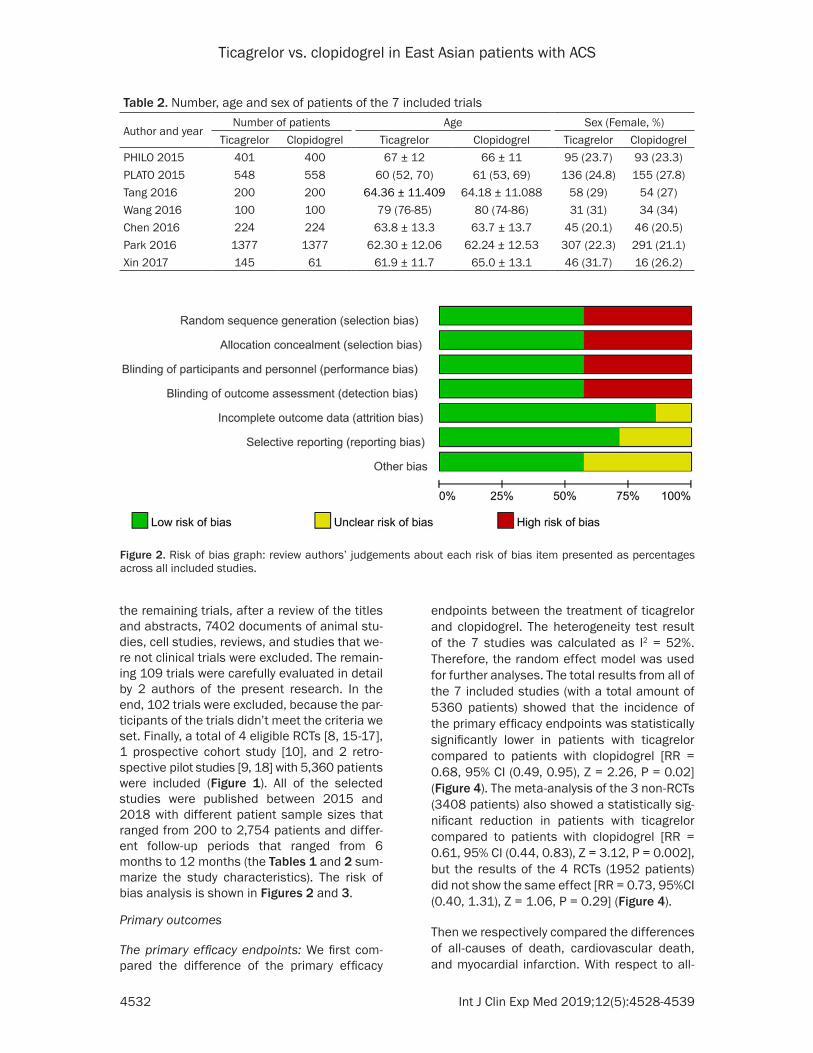
the remaining trials, after a review of the titles and abstracts, 7402 documents of animal stu- dies, cell studies, reviews, and studies that we- re not clinical trials were excluded. The remain-ing 109 trials were carefully evaluated in detail by 2 authors of the present research. In the end, 102 trials were excluded, because the par-ticipants of the trials didn’t meet the criteria we set. Finally, a total of 4 eligible RCTs [8, 15-17], 1 prospective cohort study [10], and 2 retro-spective pilot studies [9, 18] with 5,360 patients were included (Figure 1). All of the selected studies were published between 2015 and 2018 with different patient sample sizes that ranged from 200 to 2,754 patients and differ-ent follow-up periods that ranged from 6 months to 12 months (the Tables 1 and 2 sum-marize the study characteristics). The risk of bias analysis is shown in Figures 2 and 3.
Primary outcomes
The primary efficacy endpoints: We first com-pared the difference of the primary efficacy
Table 2. Number, age and sex of patients of the 7 included trials
Author and yearNumber of patients Age Sex (Female, %)
Figure 2. Risk of bias graph: review authors’ judgements about each risk of bias item presented as percentages across all included studies.
Ticagrelor vs. clopidogrel in East Asian patients with ACS
4533 Int J Clin Exp Med 2019;12(5):4528-4539
causes of death, the fixed effect model that was used for the heterogeneity of the 7 studies was calculated as I2 = 0%. The total result inclu- ded in all of the 7 studies revealed that there was no significant difference in the incidence of all-causes of death between ticagrelor and clopidogrel [RR = 0.76, 95% CI (0.57, 1.02), Z = 1.81, P = 0.07] (Figure 5A). The same results were also shown in the 3 non-RCTs [RR = 0.78, 95% CI (0.53, 1.15), Z = 1.25, P = 0.21] and the 2 RCTs meta-analysis [RR = 0.73, 95% CI (0.46, 1.16), Z = 1.32, P = 0.19], respectively.
The incidence of cardiovascular death evaluat-ed in all of the 7 studies was found to have a significant difference [RR = 0.68, 95% CI (0.48, 0.97), Z = 2.13, P = 0.03] (the fixed effect model was used for the heterogeneity of the 7 studies and was calculated as I2 = 0%), even if the data from the RCTs [RR = 0.66, 95% CI
(0.41, 1.09), Z = 1.63, P = 0.10] and non-RCTs [RR = 0.70, 95% CI (0.43, 1.16), Z = 1.38, P = 0.17] were barely significant (Figure 5B).
The incidence of another important end point, myocardial infarction, was also evaluated in 7 studies, and the random effect model used for the heterogeneity of the 4 RCTs was calculated as I2 = 62%. There was no statistically signifi-cant difference between ticagrelor and clopido-grel in the total result of the 7 studies [RR = 0.73, 95% CI (0.44, 1.22), Z = 1.20, P = 0.23], as were in RCTs [RR = 0.75, 95% CI (0.33, 1.70), Z = 0.69, P = 0.49] and in non-RCTs [RR = 0.66, 95% CI (0.35, 1.23), Z = 1.30, P = 0.19] (Figure 5C).
Safety endpoints: Among all of the studies, the primary safety endpoints were determined as total major bleeding and all bleeding, and dys-pnea received more attention among all of the adverse effects. When we analyzed the data of all bleeding, all of the total 7 included studies [RR = 1.71, 95% CI (1.39, 2.09), Z = 5.16, P < 0.00001], 4 RCTs [RR = 1.75, 95% CI (1.28, 2.39), Z = 3.53, P = 0.0004] and 3 non-RCTs [RR = 1.68, 95% CI (1.28, 2.19), Z = 3.773, P = 0.0002], showed the same result: ticagrelor significantly increased the incidences of bleed-ing compared to clopidogrel (Figure 6A). The meta-analysis of all the 6 included studies showed that the incidence of major bleeding was statistically significantly lower in patients with clopidogrel compared to patients with ticagrelor [RR = 1.52, 95% CI (1.08, 2.15), Z = 2.38, P = 0.02]. However, neither the 4 RCTs [RR = 1.47, 95% CI (1.01, 2.16), Z = 1.99, P = 0.05] nor the 2 non-RCTs [RR = 1.2, 95% CI (0.3, 4.79), Z = 0.25, P = 0.80] showed the sa- me significant difference (Figure 6B). In accor-dance with the expectation, both the total re- sult and the 2 RCTs result showed that ticagre-lor significantly increased the incidence of dys-pnea compared to clopidogrel [respectively: OR = 2.26, 95% CI (1.58, 3.21), Z = 4.51, P < 0.00001; OR = 2.47, 95% CI (1.52, 4.01), Z = 3.66, P = 0.0002] (Figure 6C).
Discussion
Clopidogrel resistance is considered to exist widely in patients with ACS or those undergoing PCI treatment. As reported, 22% of patients undergoing PCI treatment were shown to be clopidogrel nonresponders (platelet aggrega-
Figure 3. Risk of bias summary: review authors’ judgements about each risk of bias item for each in-cluded study.
Ticagrelor vs. clopidogrel in East Asian patients with ACS
4534 Int J Clin Exp Med 2019;12(5):4528-4539
tion of < 10% after administrated with clopido-grel), 32% were low responders (platelet aggre-gation of < 30%), and 47% were responders (platelet aggregation of ≥ 30%) [19]. And the pa- tients with clopidogrel resistance had increased risks for recurrent cardiovascular events [20]. The studies that adjusted the dose of clopido-grel to a high-dose according to CYP2C19*2 alleles demonstrated that high-dose clopido-grel still could not overcome clopidogrel resis-tance in the CYP2C19*2 carriers [21].
Then, with the appearance of ticagrelor, it dis-played a reversible, direct-acting characteristic and could provide a faster, greater, and more consistent platelet inhibitory effect. In the Plato study, ticagrelor was proven to be the favored choice compared with clopidogrel in ACS pati- ents, for it significantly decreased the incidenc-es of both the primary and the secondary end points (P < 0.001 and P = 0.005, respectively), without any significant differences in major bleeding. Based on the study, ticagrelor is rec-ommended by several clinical management guidelines for P2Y12 inhibition in patients with ACS, as well as the guidelines in China. However, in March 2015, in the subgroup analysis of East Asian patients, a series of different results were published: the rates of efficacy end points (ticagrelor vs. clopidogrel: 8.3% and 10.3%), major bleeding (ticagrelor vs. clopidogrel: 8.0% and 5.6%) and net clinical benefit (ticagrelor vs.
clopidogrel: 12.2% and 15%). Although ticagre-lor decreased the incidence of primary efficacy end points, it increased the hazard of major bleeding and seemingly decreased the net clini-cal benefit. Then, in November 2015, another randomized, double-blind PHILO study was published, and the results also suggested that ticagrelor treatment increased the primary effi-cacy end points (ticagrelor vs. clopidogrel: 9.0% and 6.3%) and major bleeding (ticagrelor vs. clopidogrel: 10.3% and 6.8%), albeit not signifi-cantly. Both the results above reminded us that differences in thrombogenesis as well as the responses to anti platelet agents according to ethnicity should not be ignored. Lately, with the institution of the concept of the “East Asian Paradox” [7], ample evidence has been accu-mulated and suggests that although more East Asians carry the CYP2C19 loss-of-function allele and have a higher level of platelet reactiv-ity compared with Caucasians [22], East Asians may have similar or even lower rates of post-PCI ischemic event occurrence [23, 24]. Alth- ough we still have no idea of the underlying mechanisms, we have found that the degree of platelet inhibition with P2Y12 inhibitors is high-er in East Asian patients than in white patients. After the administration of ticagrelor, the expo-sure of ticagrelor and its major active metabo-lite (AR-C124910XX) was 40% and 48% higher in Japanese volunteers than in white volun-
Figure 4. Forest plots depicting the comparison of ticagrelor and clopidogrel on the primary efficacy endpoints.
Ticagrelor vs. clopidogrel in East Asian patients with ACS
4535 Int J Clin Exp Med 2019;12(5):4528-4539
Ticagrelor vs. clopidogrel in East Asian patients with ACS
4536 Int J Clin Exp Med 2019;12(5):4528-4539
teers, which correlated with a higher level of platelet inhibition.
Recently, 2 meta-analyses were published co- mparing the efficacy and safety of ticagrelor with clopidogrel in East Asian patients with ACS, which only enrolled 2 and 3 studies res- pectively [25, 26]. Compared with these stud-ies, the present meta-analysis, which enrolled 4 RCTs, 2 retrospective studies and 1 perspec-tive study, was comprised of both randomized controlled trials and real world studies and cov-ered all of the current, relevant studies. The pri-mary efficacy endpoints, mainly including the composite endpoints of MI, stroke, or CV death, were chosen as the primary outcome measure in our meta-analysis. Generally, the confirma-tion of the conclusion mainly depends on the results from the enrolled RCT. We did not find a significant difference in the reduction on MA- CEs of ticagrelor in the pooled analysis of RCT. However, there were signals towards a poten-tial benefit of ticagrelor over clopidogrel if we also considered the non-randomized data. Simultaneously, the data on the topic of cardio-vascular death revealed a similar result that although neither the RCTs nor the non-RCTs showed a significant difference between ticag- relor and clopidogrel, the merged result showed a statistical significance. As for the incidences of MI and all-causes of death, no statistical sig-nificance was shown in either the the segrega-tive analysis of the RCTs or the non-RCTs, nor in the merged analysis. To our surprise, the results from the 2 RCTs from China seemed to have the opposite propensity in contrast to the re- sults of the PLATO and PHILO trials. Although we don’t believe that there is still a marked dif-ference of ticagrelor treatment among the East Asian countries, the results at least reminded us that there is a great deal of controversy and larger trials comparing ticagrelor and clopido-grel are needed.
Bleeding was seen as the most important adverse complication of DAPT, and the differ-ences in the propensity for bleeding between the East Asian and white populations have also drawn our attention. In contrast to ischemic
events after PCI, the risk incidence of serious bleeding in East Asian patients seems to be more serious [27]. In a study comparing throm-botic and thrombolytic status in Japanese and Western populations, marked differences were found, with the Japanese being less prothrom-botic but having a less thrombolytic profile [28]. In another study to assess the association of high-responsiveness to antiplatelet therapy and bleeding risk, they found that major bleeding occurred more frequently in high-responders with no reduction in adverse cardiac events [29]. The present analysis summarized all of the studies and found that all of the results showed a trend that ticagrelor increased the bleeding risk, with the P value < 0.00001 (all bl- eeding) and = 0.02 (major bleeding). Meanwhile, the complication of dyspnea was also markedly increased and it might be another limitation of ticagrelor.
Our main findings can be summarized as fol-lows: 1. Although no difference in the primary efficacy end points between ticagrelor and clopidogrel treatments was found in the RCTs, ticagrelor was better when pooled the other observational studies. 2. The incidences of MI, all-causes of death and CV death still showed no difference between the ticagrelor and clopi-dogrel treatments. Only after combining the RCTs and non-RCTs did ticagrelor show superi-ority in CV death. 3. Ticagrelor significantly increased the risk of bleeding and dyspnea. 4. In consideration of the underlying trend of ticagrelor vs. clopidogrel in the primary efficacy end points and the slight change of the P value of major bleeding, larger trials enrolling more East Asian patients should be undertaken.
Acknowledgements
This study was supported by the Natural Sci- ence Foundation of China (no. 81700321), the Natural Science Foundation of Shandong Pro- vince (ZR2014HP005 and ZR201702140357), the Key Research and Development Plan of Shandong Province (2018GSF118140), the Key Science and Technology Program of Shandong Province (2015GSF118054), and the Medical and Health Science and Technology Develop-
Figure 5. Forest plots depicting the comparisons of ticagrelor and clopidogrel on all-causes of death, cardiovascular death, and myocardial infarction. A. Forest plot of all-cause death comparison: Ticagrelor vs. Clopidogrel. B. Forest plot of cardiovascular death comparison: Ticagrelor vs. Clopidogrel. C. Forest plot of myocardial infarction compari-son: Ticagrelor vs. Clopidogrel.
Ticagrelor vs. clopidogrel in East Asian patients with ACS
4537 Int J Clin Exp Med 2019;12(5):4528-4539
Figure 6. Forest plots depicting the comparisons of ticagrelor and clopidogrel on all bleeding, major bleeding, and dyspnea. A. Forest plot of all bleeding comparison: Ticagrelor vs. Clopidogrel. B. Forest plot of major bleeding com-parison: Ticagrelor vs. Clopidogrel. C. Forest plot of despnea comparison: Ticagrelor vs. Clopidogrel.
Ticagrelor vs. clopidogrel in East Asian patients with ACS
4538 Int J Clin Exp Med 2019;12(5):4528-4539
ment Project of Shandong Province (2017WS- 043).
Disclosure of conflict of interest
None.
Address correspondence to: Zhiyong Wang, Depart- ment of Emergency Surgery, Qilu Hospital of Shan- dong University, No. 107, Wen Hua Xi Road, Jinan 250012, Shandong, PR China. Tel: +86 1856008- 3156; E-mail: [email protected]
References
[1] Husted S, Emanuelsson H, Heptinstall S, Sand- set PM, Wickens M, Peters G. Pharmacodyna- mics, pharmacokinetics, and safety of the oral reversible P2Y12 antagonist AZD6140 with as-pirin in patients with atherosclerosis: a double-blind comparison to clopidogrel with aspirin. Eur Heart J 2006; 27: 1038-47.
[2] Storey RF, Husted S, Harrington RA, Heptinstall S, Wilcox RG, Peters G, Wickens M, Emanue- lsson H, Gurbel P, Grande P, Cannon CP. Inhibi- tion of platelet aggregation by AZD6140, a re-versible oral P2Y12 receptor antagonist, com-pared with clopidogrel in patients with acute coronary syndromes. J Am Coll Cardiol 2007; 50: 1852-6.
[3] Wallentin L, Becker RC, Budaj A, Cannon CP, Emanuelsson H, Held C, Horrow J, Husted S, James S, Katus H, Mahaffey KW, Scirica BM, Skene A, Steg PG, Storey RF, Harrington RA, Freij A, Thorsen M. Ticagrelor versus clopido-grel in patients with acute coronary syndromes. N Engl J Med 2009; 361: 1045-57.
[4] Task Force on the management of ST-segment elevation acute myocardial infarction of the Eu-ropean Society of Cardiology (ESC), Steg PG, James SK, Atar D, Badano LP, Blömstrom-Lun-dqvist C, Borger MA, Di Mario C, Dickstein K, Ducrocq G, Fernandez-Aviles F, Gershlick AH, Giannuzzi P, Halvorsen S, Huber K, Juni P, Kas-trati A, Knuuti J, Lenzen MJ, Mahaffey KW, Val-gimigli M, van ‘t Hof A, Widimsky P, Zahger D. ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur Heart J 2012; 33: 2569-619.
[5] Levine GN, Bates ER, Bittl JA, Brindis RG, Fihn SD, Fleisher LA, Granger CB, Lange RA, Mack MJ, Mauri L, Mehran R, Mukherjee D, Newby LK, O’Gara PT, Sabatine MS, Smith PK, Smith SC Jr. 2016 ACC/AHA guideline focused up-date on duration of dual antiplatelet therapy in patients with coronary artery disease: a report of the American college of cardiology/Ameri-can heart association task force on clinical
practice guidelines: an update of the 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention, 2011 ACCF/AHA guide-line for coronary artery bypass graft surgery, 2012 ACC/AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis and management of patients with stable ischemic heart disease, 2013 ACCF/AHA guideline for the manage-ment of ST-elevation myocardial infarction, 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coro-nary syndromes, and 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing non-cardiac surgery. Circulation 2016; 134: e123-55.
[6] Amsterdam EA, Wenger NK, Brindis RG, Casey DE Jr, Ganiats TG, Holmes DR Jr, Jaffe AS, Jneid H, Kelly RF, Kontos MC, Levine GN, Liebson PR, Mukherjee D, Peterson ED, Sabatine MS, Sma- lling RW, Zieman SJ. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American college of cardiology/Ameri-can heart association task force on practice guidelines. J Am Coll Cardiol 2014; 64: e139-e228.
[7] Jeong YH. “East asian paradox”: challenge for the current antiplatelet strategy of “one-guide-line-fits-all races” in acute coronary syndrome. Curr Cardiol Rep 2014; 16: 485.
[8] Goto S, Huang CH, Park SJ, Emanuelsson H, Kimura T. Ticagrelor vs. clopidogrel in Japane- se, Korean and Taiwanese patients with acute coronary syndrome -- randomized, double-blind, phase III PHILO study. Circ J 2015; 79: 2452-60.
[9] Chen IC, Lee CH, Fang CC, Chao TH, Cheng CL, Chen Y, Yu CL, Lin CC, Lin CY, Li YH. Efficacy and safety of ticagrelor versus clopidogrel in acute coronary syndrome in Taiwan: a multi-center retrospective pilot study. J Chin Med As-soc 2016; 79: 521-30.
[10] Park KH, Jeong MH, Ahn Y, Ahn TH, Seung KB, Oh DJ, Choi DJ, Kim HS, Gwon HC, Seong IW, Hwang KK, Chae SC, Kim KB, Kim YJ, Cha KS, Oh SK, Chae JK. Comparison of short-term clinical outcomes between ticagrelor versus clopidogrel in patients with acute myocardial infarction undergoing successful revascular-ization; from Korea acute myocardial infarction registry-national institute of health. Int J Cardi-ol 2016; 215: 193-200.
[11] Stewart LA, Clarke M, Rovers M, Riley RD, Sim-monds M, Stewart G, Tierney JF. Preferred re-porting items for systematic review and meta-analyses of individual participant data: the PRISMA-IPD statement. JAMA 2015; 313: 1657-65.
Ticagrelor vs. clopidogrel in East Asian patients with ACS
4539 Int J Clin Exp Med 2019;12(5):4528-4539
[12] Greenland S. Quantitative methods in the re-view of epidemiologic literature. Epidemiol Rev 1987; 9: 1-30.
[13] DerSimonian R, Laird N. Meta-analysis in clini-cal trials. Control Clin Trials 1986; 7: 177-88.
[14] Zhang Z, Wu P, Zhang J, Wang S, Zhang G. The effect of statins on microalbuminuria, protein-uria, progression of kidney function, and all-cause mortality in patients with non-end stage chronic kidney disease: a meta-analysis. Phar- macol Res 2016; 105: 74-83.
[15] Kang HJ, Clare RM, Gao R, Held C, Himmel-mann A, James SK, Lim ST, Santoso A, Yu CM, Wallentin L, Becker RC; PLATO Investigators. Ticagrelor versus clopidogrel in Asian patients with acute coronary syndrome: a retrospective analysis from the platelet inhibition and pa-tient outcomes (PLATO) trial. Am Heart J 2015; 169: 899-905, e1.
[16] Wang H, Wang X. Efficacy and safety outcomes of ticagrelor compared with clopidogrel in el-derly Chinese patients with acute coronary syndrome. Ther Clin Risk Manag 2016; 12: 1101-5.
[17] Tang X, Li R, Jing Q, Wang Q, Liu P, Zhang P, Liu Y. Assessment of ticagrelor versus clopidogrel treatment in patients with ST-elevation myo-cardial infarction undergoing primary percuta-neous coronary intervention. J Cardiovasc Pharmacol 2016; 68: 115-20.
[18] Xin YG, Zhang HS, Li YZ, Guan QG, Guo L, Gao Y, Yu HJ, Zhang XG, Xu F, Zhang YL, Jia DL, Sun YX, Qi GX, Tian W. Efficacy and safety of ticagre-lor versus clopidogrel with different dosage in high-risk patients with acute coronary syn-drome. Int J Cardiol 2017; 228: 275-9.
[19] Lau WC, Gurbel PA, Watkins PB, Neer CJ, Hopp AS, Carville DG, Guyer KE, Tait AR, Bates ER. Contribution of hepatic cytochrome P450 3A4 metabolic activity to the phenomenon of clopi-dogrel resistance. Circulation 2004; 109: 166-71.
[20] Matetzky S, Shenkman B, Guetta V, Shechter M, Beinart R, Goldenberg I, Novikov I, Pres H, Savion N, Varon D, Hod H. Clopidogrel resis-tance is associated with increased risk of re-current atherothrombotic events in patients with acute myocardial infarction. Circulation 2004; 109: 3171-5.
[21] Zhang L, Yang J, Zhu X, Wang X, Peng L, Li X, Cheng P, Yin T. Effect of high-dose clopidogrel according to CYP2C19*2 genotype in patients undergoing percutaneous coronary interven-tion- a systematic review and meta-analysis. Thromb Res 2015; 135: 449-58.
[22] Margolis JR, Hirshfeld JW Jr, McNeer JF, Starm-er CF, Rosati RA, Peter RH, Behar VS, Kong Y. Sudden death due to coronary artery disease. A clinical, hemodynamic, and angiographic profile. Circulation 1975; 52: III180-8.
[23] Goto S, Toda E. Antiplatelet therapy after coro-nary intervention in Asia and Japan: the Asian perspective of antiplatelet intervention. Hamo- staseologie 2009; 29: 321-5.
[24] Mak KH, Bhatt DL, Shao M, Hankey GJ, Easton JD, Fox KA, Topol EJ. Ethnic variation in ad-verse cardiovascular outcomes and bleeding complications in the clopidogrel for high ath-erothrombotic risk and ischemic stabilization, management, and avoidance (CHARISMA) stu- dy. Am Heart J 2009; 157: 658-65.
[25] Wu B, Lin H, Tobe RG, Zhang L, He B. Ticagrelor versus clopidogrel in East-Asian patients with acute coronary syndromes: a meta-analysis of randomized trials. J Comp Eff Res 2018; 7: 281-91.
[26] Misumida N, Aoi S, Kim SM, Ziada KM, Abdel-Latif A. Ticagrelor versus clopidogrel in East Asian patients with acute coronary syndrome: systematic review and meta-analysis. Cardio-vasc Revasc Med 2018; 19: 689-694.
[27] Levine GN, Jeong YH, Goto S, Anderson JL, Huo Y, Mega JL, Taubert K, Smith SC Jr. World heart federation expert consensus statement on an-tiplatelet therapy in east asian patients with ACS or undergoing PCI. Glob Heart 2014; 9: 457-67.
[28] Gorog DA, Yamamoto J, Saraf S, Ishii H, Ijiri Y, Ikarugi H, Wellsted DM, Mori M, Yamori Y. First direct comparison of platelet reactivity and thr- ombolytic status between Japanese and Wes- tern volunteers: possible relationship to the “Japanese paradox”. Int J Cardiol 2011; 152: 43-8.
[29] Tsukahara K, Kimura K, Morita S, Ebina T, Ko- suge M, Hibi K, Okuda J, Iwahashi N, Maejima N, Nakachi T, Ohtsuka F, Hashiba K, Tahara Y, Sugano T, Umemura S. Impact of high-respon-siveness to dual antiplatelet therapy on bleed-ing complications in patients receiving drug-eluting stents. Int J Cardiol 2010; 74: 679-85.