Thirty-second Session of WHO South-East Asia Advisory Committee on Health Research Bangkok, Thailand 11-13 October 2011 SEA/ACHR/32/2.7 8 October 2011 Agenda Item 2.7 By Dr Monir Islam Review of the Regional Policy on Research Aspect of Immunization
Transcript
Thirty-second Session of WHO South-East Asia
Advisory Committee on Health Research Bangkok, Thailand 11-13 October 2011
SEA/ACHR/32/2.78 October 2011
Agenda Item 2.7
By Dr Monir Islam
Review of the Regional Policy on Research Aspect of Immunization
1. BACKGROUND
Global efforts to achieve MDG 4 have resulted in the reduction of under five mortality from 11.9 million deaths in 1990 to 7.7 million deaths in 20101 with immunization being a major contributor to this effort. The EPI programme was established more than 30 years ago initially with 6 antigens BCG, Diphtheria Pertussis and Tetanus (DTP), Polio and Measles. In 2000, new initiatives were launched with the financial support of the Global Alliance for Vaccine & Immunization (GAVI) to introduce Hepatitis B vaccine followed five years later with the introduction of DTP containing combination vaccine with Hepatitis B and Haemophilus Influenzae type b [Hib] vaccine altogether in a single jab. Today, immunization against 8 childhood infections (tuberculosis, diphtheria, tetanus pertussis, polio, measles, hepatitis B and hib) are preventing more than 2.5 million child deaths every year. According to WHO estimates, raising the vaccination coverage with these vaccines to 90% would result in averting an additional two million deaths a year3.
The South East Asia region includes major manufacturers of vaccines located mostly in India and in Indonesia. These producers from both private and public sectors play a significant role in ensuring vaccine availability in the region and on a global scale. The WHO regional office for South East Asia has encouraged the Member Countries to develop long term policies not only to maintain the current level of vaccine production but also to stimulate research and development for vaccines to prevent tropical diseases i.e.; Dengue, Japanese Encephalitis and Malaria. In 2003, SEARO/IVD published the first regional vaccine policy for the South East Asia region with the broad objective to provide a framework for decision makers on issues related to vaccine research, production availability and distribution.
Since 2003, the EPI programme in countries of the SEA region have undergone many changes and transformed its character to a great extent. During this period, new vaccines and new combinations of established vaccines have been introduced. This change has been initiated subsequent to observations by the immunization stakeholders at the global level that the uptake of vaccines which were available in the developed countries was slow in the developing world . For an example, Hepatitis B vaccine had not been able to be used in developing countries even 20 years after its extensive use in developed countries. Recognizing the reasons for slow up take, the GAVI was created by immunization stakeholders to support introducing Hepatitis B and Auto Disabled (AD) syringes in developing countries. This eventually led to an increase in uptake of Hepatitis B vaccine.
1
Riding on the success of the introduction of the Hepatitis B vaccine in developing countries, the immunization stakeholders continued research on developing low cost new vaccines and technologies and provided these research findings to the vaccine manufacturers including in developing countries. Parallel to these developments, countries were identified based on Gross National Income (GNI) for prioritization of support. The measure of defining eligibility for support was aimed at increasing the uptake of underutilized new vaccines in least affordable countries. In order to enhance the country responsibility in vaccine procurement, subsequently a co-financing mechanism was introduced. In addition to these interventions small groups were identified in focussing on specific vaccines. As a result of these activities, low cost vaccines such as live attenuated Japanese Encephalitis Vaccine SA-14-14-2 were available for introduction in lower income countries.
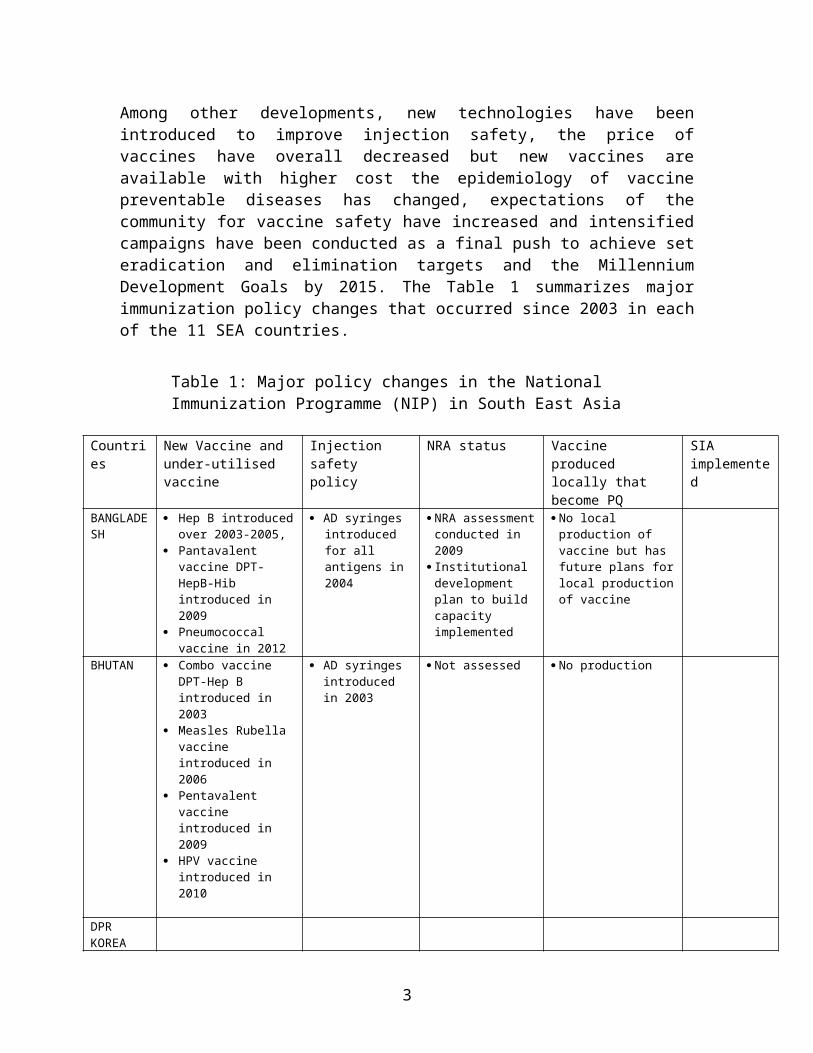
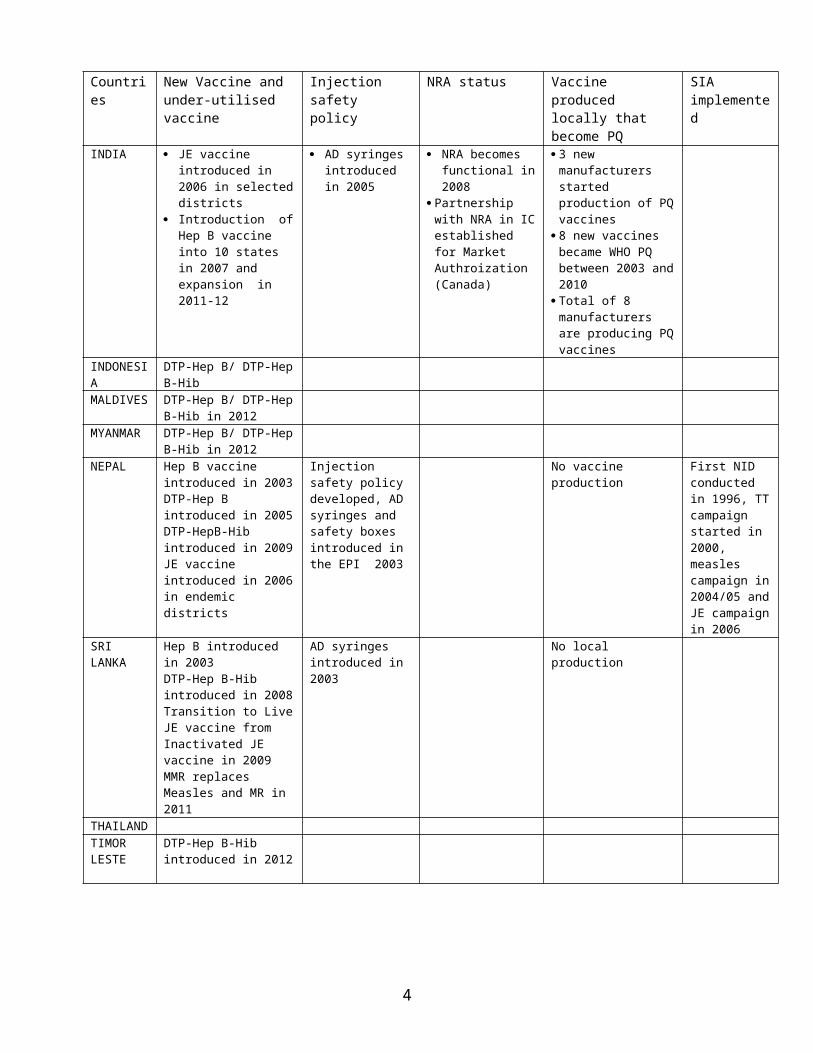
Among other developments, new technologies have been introduced to improve injection safety, the price of vaccines have overall decreased but new vaccines are available with higher cost the epidemiology of vaccine preventable diseases has changed, expectations of the community for vaccine safety have increased and intensified campaigns have been conducted as a final push to achieve set eradication and elimination targets and the Millennium Development Goals by 2015. The Table 1 summarizes major immunization policy changes that occurred since 2003 in each of the 11 SEA countries.
Table 1: Major policy changes in the National Immunization Programme (NIP) in South East Asia
Countries New Vaccine and under-utilised vaccine
Injection safety policy
NRA status Vaccine produced locally that become PQ
SIA implemented
BANGLADESH
Hep B introduced over 2003-2005,
Pantavalent vaccine DPT-HepB-Hib introduced in 2009
Pneumococcal vaccine in 2012
AD syringes introduced for all antigens in 2004
NRA assessment conducted in 2009
Institutional development plan to build capacity implemented
No local production of vaccine but has future plans for local production of vaccine
BHUTAN Combo vaccine DPT-Hep B introduced in 2003
Measles Rubella vaccine introduced in 2006
Pentavalent vaccine introduced in 2009
HPV vaccine introduced in 2010
AD syringes introduced in 2003
Not assessed No production
DPR KOREAINDIA JE vaccine introduced in
2006 in selected districts Introduction of Hep B
vaccine into 10 states in 2007 and expansion in 2011-12
AD syringes introduced in 2005
NRA becomes functional in 2008
Partnership with NRA in IC established for Market Authroization (Canada)
3 new manufacturers started production of PQ vaccines
8 new vaccines became WHO PQ between 2003 and 2010
Total of 8 manufacturers are producing PQ vaccines
INDONESIA DTP-Hep B/ DTP-Hep B-HibMALDIVES DTP-Hep B/ DTP-Hep B-Hib
2
Countries New Vaccine and under-utilised vaccine
Injection safety policy
NRA status Vaccine produced locally that become PQ
SIA implemented
in 2012MYANMAR DTP-Hep B/ DTP-Hep B-Hib
in 2012NEPAL Hep B vaccine introduced in
2003DTP-Hep B introduced in 2005DTP-HepB-Hib introduced in 2009JE vaccine introduced in 2006 in endemic districts
Injection safety policy developed, AD syringes and safety boxes introduced in the EPI 2003
No vaccine production First NID conducted in 1996, TT campaign started in 2000, measles campaign in 2004/05 and JE campaign in 2006
SRI LANKA Hep B introduced in 2003DTP-Hep B-Hib introduced in 2008Transition to Live JE vaccine from Inactivated JE vaccine in 2009 MMR replaces Measles and MR in 2011
AD syringes introduced in 2003
No local production
THAILANDTIMOR LESTE
DTP-Hep B-Hib introduced in 2012
In 2005, the WHO and UNICEF jointly prepared a Global Immunization Vision and Strategy 2006-2015 (GIVS) to meet the challenges in global immunization. GIVS goal by 2010 or earlier is for countries to reach at least 90% national vaccination coverage and at least 80% vaccination coverage in every district or equivalent administrative unit. By 2015, the GIVS aims to sustain vaccination coverage goal reached in 2010 and to reduce morbidity and mortality due to vaccine preventable diseases by at least two thirds compared to 2000 levels. It further aims gradual introduction of new vaccines to reach full scale availability for all eligible population within 5 years of the introduction of these new vaccines in national programmes, ensuring capacity for surveillance and monitoring, strengthen health systems and assure financial sustainability4. Introduction of new vaccines will also be an important contributor to achieving Millennium Development Goal 4. The challenge to develop immunization policy is to take advantages of achievements and to understand and utilize the opportunities created by vaccine market forces that will drive vaccine prices to affordable levels for developing countries.
In the last decade, the vaccine market has grown at an annual rate of 10% from $2.9 bn to 6bn. This growth is forecast to continue. The market remains characterized by strong value /volume skews. High income country demand represents 82% of industry revenue but only 12% of volume (Mercier Management consulting; Lessons Learned: New procurement Strategies for vaccines Final report to the GAVI Board). For the multinational targeting high income country markets (USA, Western Europe and Japan), the profitability has
3
risen significantly driven by patented products. As a consequence, Reasearch and Development (R&D) initiatives and investments have also risen significantly to reach pharmaceutical industry levels.
In the low and middle income countries the paradigm is different. Vaccines used to vaccinate children and adults in the national immunization programmes are non-patented products. The Developing Country Vaccine Manufacturers Network (DCVMN1), a non-profit public health driven alliance of vaccine manufacturers which are located in developing countries, estimated that 2 out of every 3 children born in the world get immunized with at least one vaccine come from a manufacturer of the DCVMN. This further demonstrates the critical role vaccine manufacturers in developing countries have taken to ensure the global supply of most needed vaccines. However, these vaccines are sold at very low prices yielding less profit than patented products and thus generating less financial opportunity to invest in R&D. Out of the 28 members of the DCVMN, 10 are located in the SEA region including India, Indonesia and Thailand. India has become a major vaccine producing country manufacturing more than 80% of the total DTP group of vaccines produced by the DCVMN members.
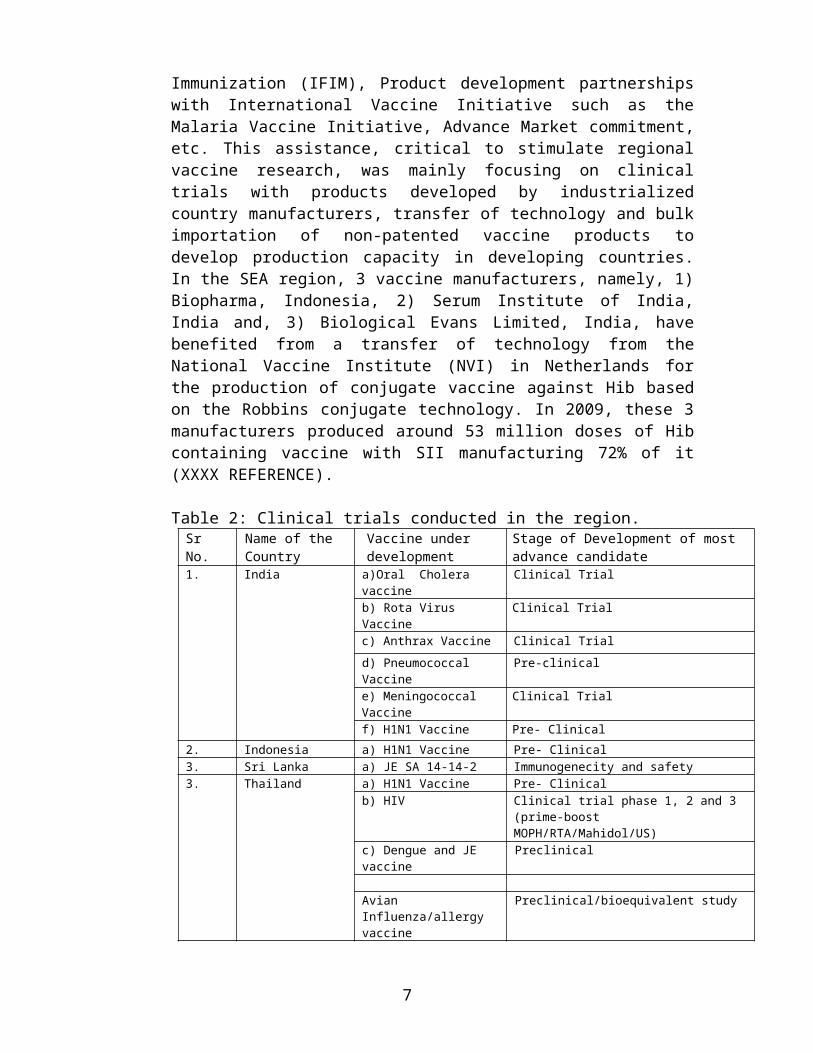
Since 2000, R&D for vaccine in developing countries has received substantial financial support from international funding sources and initiatives including the International Finance Facility for Immunization (IFIM), Product development partnerships with International Vaccine Initiative such as the Malaria Vaccine Initiative, Advance Market commitment, etc. This assistance, critical to stimulate regional vaccine research, was mainly focusing on clinical trials with products developed by industrialized country manufacturers, transfer of technology and bulk importation of non-patented vaccine products to develop production capacity in developing countries. In the SEA region, 3 vaccine manufacturers, namely, 1) Biopharma, Indonesia, 2) Serum Institute of India, India and, 3) Biological Evans Limited, India, have benefited from a transfer of technology from the National Vaccine Institute (NVI) in Netherlands for the production of conjugate vaccine against Hib based on the Robbins conjugate technology. In 2009, these 3 manufacturers produced around 53 million doses of Hib containing vaccine with SII manufacturing 72% of it (XXXX REFERENCE).
Table 2: Clinical trials conducted in the region.Sr No. Name of the Country Vaccine under
developmentStage of Development of most advance candidate
1 DCVMN membrs includes: 1) Bharat Immunologicals & Biologicals Corp’n India, 2) Bharat biotech Intl, India, 3) Bio farma Indonesia, 4) Biological Evans Ld India, 5) BIRMEX Mexico, 6) China Natl Biotech corp’n china, 7) CGEB Cuba, 8) Fiocruz/BioManguinhos Brazil, 9) Finlay Institute Cuba, 10) Hafkine Bio-Pharmaceutical copr’n India, 11) India Immunologicals lts india, 12) Instituto Butantan Brazil, 13) Institute Pasteur d’Iran Iran, 14) Institu Pasteur de Dakar Senegal, 15) Institut Pasteur de Tunis Tunisia, 16) Institute of Virology of Belgrade Yugoslavia, 17) Queen Saovabba institute (QSMI) Thailand; 18) LG Life science South Korea; 19) National Institute of Vaccine and Biologicals (IVAC) Vietnam; 20) Panacea Biotech Ltd india; 21) Razi Institute for serums and Vaccine Iran; 22) serum Institute of India Ltd India; 23) Vabiotech, National Institute of Hygiene and Epidemiology (NIHE) Vietnam, 24) VACSERA, Egypt; 25) Zhengzhou Kangtai Pharmaceutical Co Ltd China; 26) Zydus Cadilla India; 27) The Biovac South Africa; 28) Xiamen YST Biotec China
2. Indonesia a) H1N1 Vaccine Pre- Clinical3. Sri Lanka a) JE SA 14-14-2 Immunogenecity and safety3. Thailand a) H1N1 Vaccine Pre- Clinical
b) HIV Clinical trial phase 1, 2 and 3 (prime-boost MOPH/RTA/Mahidol/US)
c) Dengue and JE vaccine Preclinical
Avian Influenza/allergy vaccine Preclinical/bioequivalent study
The region has a large community of well qualified scientists especially in vaccine producing countries with sophisticated laboratory facilities in some countries. However, the lack of interest , incentives and support of governments for R&D in producing countries, the challenges posed by Intellectual Property Rights (IPR) , regulatory compliance, the limited coordination between research institutes, manufacturers, National Regulatory Authorities and national immunization programmes have hampered the development of novel vaccines needed for the South East Asia region i.e.; Cholera, Japanese Encephalitis (JE), Malaria, dengue, Diarrhoeal diseases, etc. There is a need to develop an immunization policy for the SEA region that would foster Government leadership for vaccine R&D, and stimulate greater synergy between research institutes and universities, National Regulatory Authorities, manufacturers and national EPI programmes to define vaccine research and development priorities.
A national policy on immunization will rationalize the decision making process, provide a vision with priority interventions and estimate financial requirements in the short- and medium-term perspectives. It would also send a clear signal to vaccine production units within the country, within the region and globally to plan and coordinate production to meet the global needs of vaccines. Rather than developing national policies from scratch, it would be more beneficial to adapt a regional policy to the national needs. This will also enable some degree of similarity of the national policies of different countries in the region which share common characteristics with regard to the epidemiology of vaccine preventable diseases and socio-economic considerations.
2. PURPOSE OF THE POLICY
The need for a regional vaccine policy was first articulated by the South-East Asia Regional Advisory Committee for Health Research (ACHR) in April 1999. A task force was formed and a policy document was developed covering the period 2003 to 20107. This policy document is for the five year period of 2010-2015.
5
This policy does not intend to cover all aspects of the service delivery of immunization programmes or detailed guidelines on specific vaccines that are included in other global and regional documents8. Rather, its primary purpose is to provide a framework for decision-making on wide-ranging issues related to research, production, availability, and distribution of vaccines and the sustainability of the immunisation programmes in the countries of the region. The ultimate aim of this document is to develop regional priorities for sustainable vaccine initiatives and immunisation strategies that support the goals of national immunization programmes of Member Countries. By providing direction for vaccine initiatives and immunization strategies, the policy can serve as an advocacy tool to increase government and donor commitment and to encourage greater cooperation among countries.
In retrospect, SEA members states immunization programmes have achieved a great deal since the first regional policy was introduced in terms of vaccine safety, vaccine quality and its regulations, vaccine coverage and Supplementary Immunization Activities for Polio eradication , measles mortality reduction and Measles-Neonatal Tetanus elimination . This regional policy aims to take advantages of the past lessons learnt and to move countries of the region towards vaccine security with quality products alongside a greater visibility and mobilization of the regional and country vaccine scientists’ communities and governments to address needs of vaccine R&D to prevent tropical diseases.
CONTEXTS
3.1 Currently Used Routine EPI VaccinesRoutine vaccination is an effective, safe, and economical intervention that has brought about dramatic improvements in reducing childhood morbidity and mortality and overall in health. In the South-East Asia Region (SEAR) childhood immunizations against polio, diphtheria, pertussis, tetanus, measles and tuberculosis have been given since the 1970s and every child has a right to receive these vaccines. In 2010, except for India, and Timor Leste, all other countries in the region have over 80% coverage with DTP39.
Currently, member countries have different immunization schedules (refer Table 1). Nevertheless, during the last decade a number of new vaccines have been introduced in all countries which have now become routine. These include vaccines against Hepatitis B, Japanese Encephalitis (JE) and Haemophilus influenzae type B.
Countries must have the capacity to forecast their vaccine supply needs and procure and have necessary funding to meet these needs. Of the countries in the SEA Region, India, Indonesia and to some extent Thailand produce substantial quantities of routine vaccines. Other non vaccine producing countries purchase their vaccines either directly through WHO pre-qualified vaccine manufacturers in the global market or through international group procurement systems such as through UNICEF Supply Division or PAHO revolving funds.
6
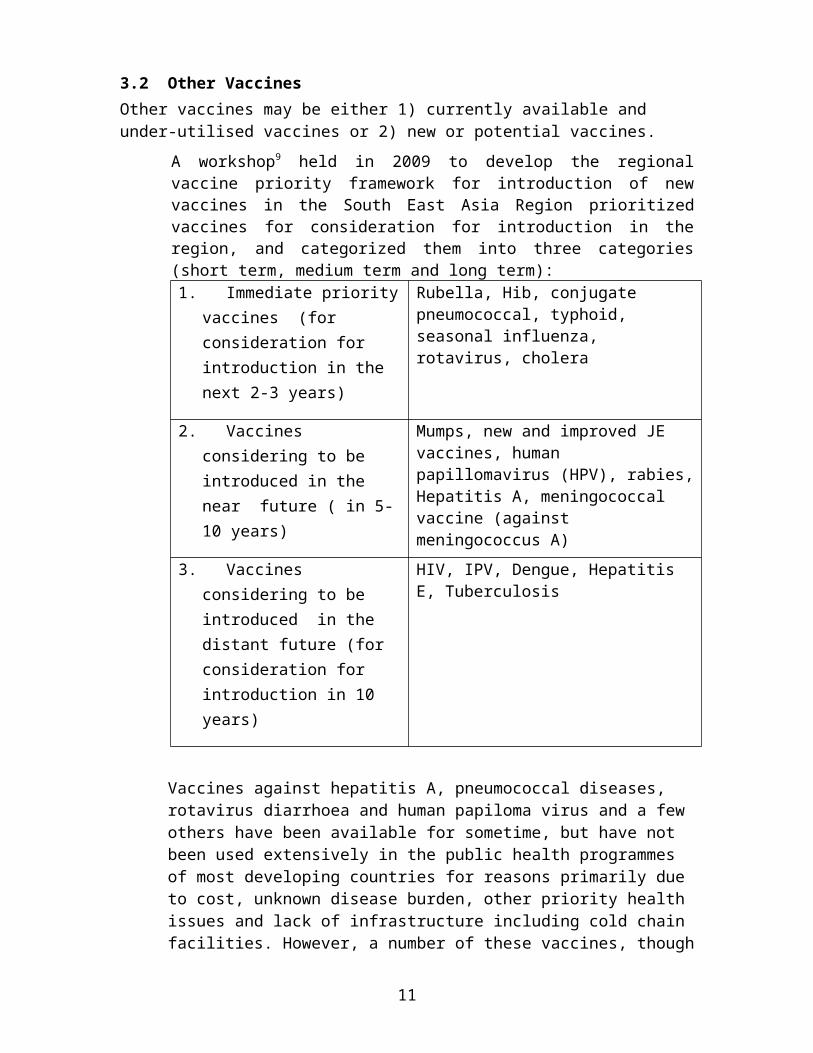
3.2 Other VaccinesOther vaccines may be either 1) currently available and under-utilised vaccines or 2) new or potential vaccines.
A workshop9 held in 2009 to develop the regional vaccine priority framework for introduction of new vaccines in the South East Asia Region prioritized vaccines for consideration for introduction in the region, and categorized them into three categories (short term, medium term and long term):1. Immediate priority
vaccines (for consideration for introduction in the next 2-3 years)
2. Vaccines considering to be introduced in the near future ( in 5-10 years)
Mumps, new and improved JE vaccines, human papillomavirus (HPV), rabies, Hepatitis A, meningococcal vaccine (against meningococcus A)
3. Vaccines considering to be introduced in the distant future (for consideration for introduction in 10 years)
HIV, IPV, Dengue, Hepatitis E, Tuberculosis
Vaccines against hepatitis A, pneumococcal diseases, rotavirus diarrhoea and human papiloma virus and a few others have been available for sometime, but have not been used extensively in the public health programmes of most developing countries for reasons primarily due to cost, unknown disease burden, other priority health issues and lack of infrastructure including cold chain facilities. However, a number of these vaccines, though poorly regulated and controlled, are available in the private sector in all countries of the region.
There are other diseases such as malaria, dengue and tuberculosis prevalent in the countries of the region that take a huge toll on productive lives for which no safe, effective, and economical vaccine yet exist. HIV/AIDS has a wider global prevalence, but still has a much deeper impact in developing countries. Due to resource constraints and multiple competing health problems and lack of clear health policies and strategies, drugs and even low-cost prevention measures are less available in developing countries.
Most of the research and progress in developing new vaccines has taken place in the industrialized countries10. Until recently, comparatively little effort has been made to develop new vaccines for diseases that are priorities in the developing countries. Further compounding this disparity is the reality that developing countries have limited access to new technologies for vaccine development and
7
production. Consequently, developing countries primarily produce only the “traditional” vaccines and limited work takes place to address the needs of the third world. In response to these concerns, the Developing Countries Vaccine Manufacturers’ Network was established in November 2000. Strategies recommended by this group to promote vaccine research and production in developing countries should be considered in formulating a regional vaccine policy 11.
Vaccine research in the SEA should focus on improving regional capacity for the following: to carry out basic science research, conduct clinical trials, to transfer research into viable products, to support immunization programme implementation and evaluation, and to facilitate introduction of new research techniques and methodologies. Clear policy statements will enable relevant regional bodies (such as the Regional Committee and the Technical Consultative Group on Immunizations) and Member Countries to establish a strong network of resources and develop a research agenda based on local priorities.
3.3 Vaccine QualitySince the last publication of the regional Vaccine Policy for the South East Asia Region in September 2003, the vaccine regulatory context in South East Asia has significantly improved among the eleven member states. The 3 vaccine producing countries, namely, India, Indonesia and Thailand, now have a fully functioning NRA in compliance with WHO set of criteria to regulate vaccine safety, quality and efficacy. All countries including those that are procuring vaccine directly or through UN procurement agencies have established monitoring system for Adverse Events Following Immunization (AEFI). A network of vaccine regulatory experts was expanded to include specialists from industrialized countries and emerging countries in other WHO regions. This network of regulatory specialists was instrumental to conduct WHO formal NRA assessments with international teams of highly specialized technicians, to foster innovative partnerships to implement Institutional Development Plans including development of training material to facilitate in-countries training courses on Vaccine Quality with WHO. A regional vaccine policy can set the goal and strategy to further promote partnerships among vaccine regulatory institutions and specialists, to harmonize and to standardize procedures allowing countries with limited regulatory capacity to benefit from NRA with expertise to assess the vaccine dossier. The regional vaccine policy provides the framework for a country to establish fast track licensing procedures for vaccine and support mechanisms for mutual recognition of regulatory pathways with NRA from countries with assessed regulatory capacity. The regional vaccine policy should encourage the integration and the standardization of WHO PQ procedures with existing regional fora and task forces activities such as “the vaccine chapter” for clinical evaluation of vaccines in the Association of South East Asian Nations (ASEAN). Finally, the regional vaccine policy is in line with on-going policy to decentralize WHO support to bring expertise closer to countries in need.
3.4 Context of overall health policy
8
Implementation of any immunization programme must be put in the perspective of ongoing public heath policy. Health sector reform is sweeping through many countries in the world, including Bangladesh, Indonesia, Sri Lanka and Thailand in the SEA Region. The opportunities and challenges presented by these reforms need to be evaluated in the context of vaccine security, research and development, and vaccine regulation.
The EPI programme has contributed in many ways in strengthening of health systems and its acceptance by the community. In addition to providing immunization services, the EPI programme has been used to complement other programmes such as the vitamin A supplementation programme by providing an opportunity for their initiation and implementation. The EPI programme has also trained many health care workers in various aspects of programme management and implementation. Some aspects of these training programmes are applicable to other programmes as well and there are many lessons that could be learnt from this experience. In short, it can be concluded that the EPI programme has helped in strengthening the health system.
As much as the EPI programme has helped in strengthening the health system, immunization programmes cannot function in isolation. Consequently, the capacity to integrate with other programmes needs to be developed. A regional immunization policy should provide broad guidance to countries on how to address this challenge.
4. GUIDING PRINCIPLES The regional immunization policy is based on five guiding principles that underscore the tenets of immunization:
(1) Immunization is the most cost-effective public health interventions. Hence every child in the target age group should have equal access to immunization services regardless of its social determinants of health (religion, caste, or economic status etc).
(2) Immunization is a public good. That is, immunization produces group benefits far greater than the sum of individual benefits obtained by those immunized. Therefore, governments should allocate sufficient funds in ensuring adequate vaccines of assured quality for immunization programmes .
(3) Immunization services are only one modality for health promotion and disease prevention. Immunization services should complement other methods of health promotion or disease prevention.
(4) Immunization services should complement and be integrated with other health care services. This is best achieved through primary health care approaches that provide the best opportunity to reduce inequities.
(5) The Region should strive for vaccine self-sufficiency for all countries. This is broadly defined as:
Access to all nationally adopted vaccines either through procurement from the global market or through domestic production overseen by a
9
competent national regulatory authority. Mechanisms to finance vaccines should be developed in close collaboration with governments, donor agencies, and vaccine manufacturers to ensure sustainability.
There are three important approaches which serve as the premises for implementing the policy itself:
(6) Based on the primary principles of equity, sustainability, and regional solidarity, the regional immunisation policy will complement and support the development of a national immunisation policy in each country.
(7) The process of policy development should be guided by technical experts and related stakeholders in the field and it should be an interactive process with Member Countries. Good practices and desirable standards must be balanced with country needs and realities.
(8) Development of the current policy will be based on the best available evidence/knowledge with the understanding that this is a dynamic process incorporating multiple issues both directly and indirectly related to immunization services. To take this into account, the Task Force should periodically review the policy.
5. POLICY OBJECTIVESWithin the broad purpose of providing a framework for decision-making, the immunization policy has nine policy objectives:
(1) To ensure political and administrative commitment at the highest level to ensure sustainable immunization services in member countries;
(2) To provide guidance to member countries to ensure an adequate, safe and equitable immunization service;
(3) To provide guidance to member countries to improve and expand existing immunization services;
(4) To provide criteria for countries to select new vaccines for National Immunization Programmes;
(5) To provide a coordinated approach to establishing regional vaccine needs, including evaluation of current vaccine production capacity and suggested initiatives for determining the burden of vaccine preventable diseases;
(6) To assist countries in assessing the options for attaining and sustaining financial self-sufficiency for existing and expanded immunization services;
(7) To provide support and direct global and bilateral inputs to the countries in the Region, and facilitating public-private partnerships in vaccine development and immunization services;
(8) To provide guidance on establishing regional vaccine research and development (R&D) priorities in the global context and to determine
10
steps necessary to strengthen regional R&D, production, and necessary regulatory oversight capacity; and
(9) To broadly support the implementation of national immunization programmes within the framework of the health systems based on primary health care/PHC in member countries.
6. POLICY FRAMEWORK
6.1 Political and administrative commitment at the highest level to ensure sustainable immunization services
In most countries in the region, the management of the EPI programme has been done as a vertical programme with integration of services at the client level. The management of, and the logistic support for, the EPI programme at the Central level requires a high level of political and administrative commitment
6.2 Adequate, safe and equitable immunization servicesIn the region, the challenge for WHO remains providing guidance to member countries to ensure an adequate, safe and equitable immunization services. Hence, this policy objective will be key for ensuring the accessibility, the availability and the uninterrupted supply of quality vaccines that has been widely accepted by the community in all countries.
6.3 Improve and expand existing immunization services Seven member states (Bangladesh, Bhutan, DPR Korea, Maldives, Myanmar and Sri Lanka) have already achieved >90% coverage for DTP3 at the national level. Nepal and Indonesia have a DTP3 coverage > 80% at national level. India and Timor Leste are the only countries in the region that have not achieved 80% coverage of DTP3. However, there are wide differences in immunization coverage across Member States as well as within countries between states, provinces, districts or equivalent administrative areas. When countries reach immunization coverage of 80%, the push to improve coverages beyond what has already been achieved becomes difficult. At this stage, it is essential to assess coverage at sub national / district or even local level to identify pockets of low coverage and unimmunized children and take appropriate actions to improve coverage and reach the unimmunized. As indicated by the District Level Health Survey III (2007-08) in India, 90% of children who did not receive DTP3 resided in 11 states (Uttar Pradesh, Bihar, Rajasthan, Madhya Pradesh, Maharasthra, West Bengal, Assam, Jharkhand, Gujarat Andhra Pradesh, and chattsgarh). Out of these states Maharasthra, West Bengal, Gujarat and Andhra Pradesh are medium performing states with DTP3 coverage of at least 70%. This evidence very clearly stress the need for providing guidance to member countries to improve and expand existing immunization services. There is evidence from Indonesia to suggest that the post financial crisis of the late 1990s and the decentralization of immunization services have led to a decline in access and quality of immunization services in the country. However,
11
strenuous efforts have been undertaken to enhance coverage in Indonesia and as a result the current, DTP3 coverage in Indonesia is > 80% at the national level. .Based on existing knowledge and experience, interventional framework is being suggested for six key determinants that has been identified for low routine immunization coverage in the SEA Region.
1. Improving access:
Using social mobilization and advocacy campaigns to publicize time, date and location of immunization services
Increasing opportunities for immunization by using community information to design context specific delivery mechanisms to reach every community
Increasing the range of settings in which immunization services are provided
Reducing the opportunity costs for immunization (decreasing waiting time/community pooling of transport services )
2. Ensuring resource availability & utilization:
Mapping and addressing gaps in resource positions including finances, infrastructure, human resources, vaccine supply and cold chain
Advocating governments for financing immunization as an investment Developing financial sustainability plans Adopting different mechanisms to support existing staff until new staff is
recruited Ensuring availability of an adequate number of trained vaccinators Advocating for filling vacancy positions and reducing the workload of
the overburdened staff Introducing a coordination network of all field level staff who can be
mobilized for immunization activities
3. Strengthening immunization service delivery:
Improving utilization of available immunization services through improvement of quality of service delivery,
Strengthening cold chain ( vaccine Supply chain) systems, effective vaccine management ensuring assured quality of vaccines and other logistics distributed timely to all levels of immunization programme
Strengthen collaboration and integration with other primary health care services
Using maternal health delivery mechanisms to increase awareness and establish early linkages for compliance to immunization schedules and follow up on children who have missed vaccinations.
12
4. Information Use:
Strengthen recording, reporting, improving data quality; analysis, interpretation, use and exchange of data for programme planning at all levels
Sharing of data, using common platforms for monitoring and evaluation
5. Management of AEFI:
Strengthening of AEFI surveillance Investigation of serious AEFI cases Implementation of a plan for effective management of AEFI and risk
communication. Exploring ways to encourage parents to be partners in maintaining up to date
vaccination records and reporting AEFI. .
6. Enhancing managerial capacity: Using Middle Level Managerial training modules to address training needs at
different levels and scaling up training of key managers. Reorganizing monitoring and supervision systems to improve performance Task based Standard Operating Procedures for Immunization service
providers and supervisors; incentives / rewards for teams achieving outlined targets.
Introducing quarterly monitoring of immunization coverage at all levels with standard denominators.
6.4 Introduction of new vaccines for National Immunization Programmes The introduction of new vaccines in routine immunization programmes is a lengthy and complex process. Ideally, vaccine development should be guided by the extent of disease burden, but market forces often dictate other directions. On a regional or global basis, the disease burden should determine research and development priorities.
However, for the introduction of new vaccines the major criterion appears to be the availability of a vaccine. Subsequent to the availability of the vaccine, disease burden studies are carried out that may not necessarily reflect the relative burden of disease in measurable terms such as the attributable fraction. When studies to estimate the burden of disease of a specific disease are conducted singularly, it is likely that exaggerated estimates are obtained unless the entire surveillance process is enhanced to encompass all preventable infectious diseases.
13
Individual countries must use the same data as measured in the same way as other diseases as one of the criteria to select which, if any, of available vaccines to add to their routine EPI or offer through other mechanisms. This is important as there is a tendency to target the assessment of the burden of disease of diseases for which vaccines are available irrespective of the relative burden of disease. If decisions are based solely on the absolute burden of disease, there is the theoretical possibility of a member country not being able to finance a new vaccine that is cost-effective, affordable and sustainable if found in the near future (say in the short term of 2-5 years) due to commitment of the introduction of a new vaccine that may not have been relatively that important.
Norms and standards for new vaccines are set by national authorities in vaccine producing countries and, globally, by WHO Expert Committees. National Regulatory Authorities (NRA), in both exporting and importing countries, are responsible for ensuring the quality of all vaccines used to vaccinate populations. Countries also have to determine whether to produce locally or procure globally and how they will continue to finance vaccine purchases. Selected vaccines are introduced in routine immunization programmes with appropriate safety precautions. Ultimately, it is the role of the NRA to monitor quality and safety but it has to rely on the NIP capacity to collect quality AEFI data.
6.5 Establishing regional vaccine needs including evaluation of current vaccine production capacity
Forcasting regional vaccine needs is a priority for the region. This is grounded not only on the enhancement of the forecasting capacity of the countries, but also in new innovative cost saving manoeuvres such as pooel procurement of vaccines. To determine the regional vaccine needs,, appraisal of the current vaccine production capacity of the region is also important. This may be relevant for production capacity of vaccines such as JE which is produced outside the region. Hence, the policy framework promotes providing a coordinated approach to establishing regional vaccine needs.
6.6 Assesing the options for attaining and sustaining financial self-sufficiency for immunization services
Attainment and sustenance of self-sufficiency is important based on the fact that all member states fund their immunization programmes through allocations of national budgets or through donor funds. Various circumstances in different countries in the region will stretch finaincail resources. Hence, the policy framework suggests the assessment of options for financial self-sufficiency
6.7 Support and direct global and bi-lateral inputs to regional countries and facilitation of public private partnerships The South East Asian region is characterised by the need for global and bi-lateral input for aspects ranging from vaccine manufacturing to new vaccines introduction. The same is essential in terms of mobilizing public and private partnerships for vaccine
14
manufacturing, introduction of new vaccines and delivery of vaccines to end recipients in the country level. Hence, the policy frame work requires supporting access to global inputs and facilitating public private partnerships
6.8 Establishing regional vaccine resreach and development priorities
Given the availability of s a large scientific community especially in vaccine producing countries with sophisticated laboratory facilities in some countries and non-availability of a strong link with medical institutes, NRAs, manufacturers and the national EPI programmes to define research priorities, policy framework highlights the need for providing guidance on establishing regional vaccine research and development priorities in the global context and to determine steps necessary to strengthen regional R&D, production and necessary regulatory oversight capacity.
6.9 Implementation of the National immunization Programmes within the framework of the health system
The regional policy framework is advocates that the implementation of the National Immunization Programme should be carried out within the framework of the health system. The suggested approach should be the time tested Primary Health Care approach.
As these policy objectives are health system related, to further improve immunization coverage, strengthening health system is critical. The relationship between the improvement of the immunization services and the health system may be depicted as shown in Figure 1.
15
Figure 1. Relationship between immunization services and the health system
7. POLICY ISSUESBased on the framework of improving the management of existing immunization services and introduction of new vaccines, specific regional goals, policy approaches and activities to assist in meeting these goals have been identified.
7.1 Political and administrative commitment7.1.1 Regional goalTo ensure maximum political and administrative commitment at the highest level to sustain, strengthen and expand existing immunisation services.
7.1.2 StatusThe regional growth of political, administrative commitment and patronage since the introduction of the EPI programme is best exemplified by the procurement of vaccines by all member countries with funds allocated from their country’s regular budget or donor funds.
16
7.1.3 Issues Ensuring political and administrative commitment and support for a
country-wide programme such as the EPI. Competing priorities in resource limited settings in member countries. Requirement of much advocacy at the highest level for ensuring maximum
political and administrative commitment and support Political and administrative support in vaccine producing countries to
enforce the vaccine regulatory system to ensure that vaccines domestically produced and used are equivalent or of higher safety and quality standards than those which are WHO PQ.
7.1.4 Policy approaches and activitiesMost politicians and administrators are cognizant of the benefits of immunization services and view immunization as an intervention that serves the people. In order to maintain this commitment at the highest level in the midst of competing priorities, the following policy approaches need to be identified as priorities:
advocacy at the highest level to be maintained and strengthened. reviewing activities at regular intervals and sharing the findings with all
concerned to ensure EPI programme continue to be a national priority sufficient financial allocations made for the strengthening and expansion
of immunization services.
7.2 Strengthening and expanding existing immunization services7.2.1 Regional goalTo strengthen and expand existing immunization services to reduce inequities and to provide better services ensuring safe and effective vaccines and immunization services in an integrated health system.
7.2.2 StatusIn the South-East Asia Region (SEAR), childhood immunizations against polio, diphtheria, pertussis, tetanus, measles and tuberculosis have been included in the immunization programmes since the 1970s and every child has a right to receive them. Except for India, Indonesia, Nepal and Timor Leste, all other countries in the region have over 90% coverage with DTP3.
During the last decade a number of new vaccines have been introduced in different countries. These include vaccines against Hepatitis B (Hep B), Japanese Encephalitis (JE) and Hemophilus influenzae type B (Hib).
7.2.3 Issues Need for strengthening of the health system. to increase coverage over
and above levels achieved currently and to develop capacity for the introduction of new vaccines
17
Challenge of providing immunization services to hard-to-reach populations and marginalised communities.
Policy approaches and activites
With regard to the schedule of routine immunization, the region recommends the following policy approaches:
a. to ensure an opportunity for children to receive the 4th dose of DTPw before they reach 5 years of age,
b. to ensure an opportunity for a dose of Td in the immunization schedules to prevent diphtheria in adulthood, and
c. to ensure the delivery of a 2nd dose of measles in the respective immunization schedules either as a 2nd routine dose or through routine immunization or periodic SIAs. The countries may provide opportunities for either MR or MMR depending on the epidemiology of rubella and mumps in the respective country
The issues pertinent to strengthening and expanding immunization services are interrelated and overarching. Hence some of the policy approaches and activities are addressed separately under separate headings below. Client perspectives are addressed in section 7.7.
7.2.3.1 Access to safe and effective vaccines7.2.3.1.1 Regional Goal
To ensure equitable access to immunization services and availability of safe and effective vaccines to all children in all member states in the region
7.2.3.1.2 StatusCurrently, most of the SEA countries are using vaccines of assured quality as per WHO definition. India is using a mix of vaccines from PQ sources and from public sector domestic manufacturers that have not submitted their products for WHO Pre-Qualification. All vaccines used in India for the National Immunization Programme are domestically produced except JE which is manufactured in China. Thailand also procures vaccines out of the WHO list of PQ products but mostly from producers in Industrialized Countries with functioning NRAs. In all SEA vaccine producing countries, including India, Indonesia and Thailand, the NRAs were recently assessed; after the implementation of the Institutional Development Plan all were found functioning to regulate vaccine safety, quality and efficacy. All the other countries use WHO PQ vaccines that are procured directly through their national procurement agencies or through UNICEF. The priority for countries that do not produce vaccines is to establish vaccine licensing procedures that comply with fast track guidelines for registration of WHO
18
PQ vaccines (REFRENCE) and/or other harmonized and standardized registration procedures agreed upon among member states. A country in the region with a strong NRA could conduct part of the pre-clinical assessment of the product dossier and its manufacturing process that is required for a full vaccine licensure and be endorsed by countries with limited regulatory capacity.
7.2.3.1.3 Issues/Challenges Future challenge of overstretched capacities of countries to provide an
efficient regulatory framework to entry of more vaccine producers and newer vaccines in the market
Hard-to-reach populations and marginalized communities where immunization coverage is low as compared to national figures. for special attention
Issues emerging from the lucrative immunization market offering a
plethora of vaccines not available in the public sector in all member countries
o Using various scheduleso Mostly not being regulated and monitored properlyo Not reporting immunization coverage in routine returns compiled
by the public sector. o Affecting the coverage reported by the public sector as more
clients would avail of private sector services and would not be counted in the returns of the public sector.
7.2.3.1.4 Policy approaches and activities. Continuation with the current practice of pre-qualification and facilitating a dialogue to ensure the availability of safe and effective vaccines between countries in the region and, between countries and vaccine producers
o Assigning responsibility of regulation to the NRA of the country in which the vaccine is produced and the NRA in the country in which the vaccine is supplied.
o Providing assistance to enhance capacity of NRAo ,
Removal of all potential barriers to immunization services o Establishing an adequate number of vaccination centers to cover
all populations with proper infrastructure facilities
Increasing immunization coverage of hard-to reach marginalized communities with low immunization coverage by strengthening the health system, raising community awareness and promoting community participation.
19
o Providing regular services including outreach sessions in “hard to access areas”.
o Providing additional financial resources to improve infrastructure and train additional human resources.
Operating immunization services within hours convenient for the access of service users to increase immunization coverage
o Need to look at this aspect with a view to enhancing utilization of immunization services by all member states.
Private Sector
Monitoring immunization services provided by the privates sector and incorporating their statistics in national returns as a strategy for overall programme monitoring to ensure that national goals are achieved.
o Using novel methods to coax the private sector to be partners in the surveillance and reporting systems.
o Promulgation of legislation where the private sector will have to account for all vaccines imported or purchased from local manufacturers.
o Encouraging, the National Immunization Programme to offer the vaccine free of charge to private practitioners, private clinics in return that coverage data are provided to the NIP.
o Monitoring vaccines that are provided in the private sector by the NRA that grants licenses to vaccines that may not be used in the NIP.
o Establishing provisions in the vaccine licensing procedures to make compulsory reporting of data as for a post-licensure clinical trial (Phase IV) by The NRAs with the NIPs.
7.2.3.2 Vaccine management, logistics and cold chain infrastructure
7.2.3.2.1 Regional GoalTo establish an un-interrupted effective delivery mechanism for and maintain vaccines and supplies with suitable cold storage facilities and management practices for the delivery of an effective immunization service
7.2.3.2.2 StatusThe success of the EPI programme has been largely due to the maintenance of the cold chain. Improvements in technology have contributed tremendously to this effort. Member states have established a good system for the maintenance of the cold chain as is evident from the impact of the immunization programme.
20
In 2010, WHO IVB/EPI in Geneva compiled data on vaccine storage capacity availability and requirements from 66 countries representing all WHO regions. The finding shows that present vaccine storage capacity in SEA member states is adequate. However, the storage requirement will increase in a couple of years with the introduction of new vaccines.
7.2.3.2.3 Issues/Challenges
Requirement for upgrading and expansion of the cold chain in most member states to increase coverage and introduce new vaccines. The upgrading requires increased infrastructure in terms of physical space as well as additional equipment.
Requirement for additional vaccine storage volume for introducing pre-filled vaccine syringes and new vaccines in containers of less than 5 doses. Pre-filled vaccine syringes may require up to 10 times more storage space.
Accurate forecasting of cold chain requirements where new vaccines are to be introduced
Additional requirements will include infrastructure in terms of physical space, necessary equipment, sites for proper storage facilities and plans for development of these sites
Increased global demand for vaccine cold chain equipment that may exceed the production capacity worldwide in next 5 years with the introduction of New and under-utilized vaccines in many countries
Requirement of important recurrent equipment needs just to maintain the existing cold chain infrastructure in large countries such as India and Indonesia
7.2.3.2.4 Policy approaches and activities
Establishing optimal, overarching infra-structures including cold storage facilities to provide immunization services for the successful implementation of an effective immunization programme.
Upgrading and modernization and expansion of the existing clod chain infrastructure system.
Updating of the inventory of existing cold chain infrastructure to determine the extent of the resources needed for upgrading and expansion
Commitment of the governments of member states , donor agencies, other financing schemes such as co-financing and involvement of the
21
private sector for large scale funding required for expansion of the cold chain facilities
Building on the WHO supported laboratory testing units established in India and Singapore to promote regional production of cold chain equipment suitable for vaccines. Tested and pre-qualified cold chain equipment listings can be found on the WHO website http://www.who.int/immunization_standards/vaccine_quality/pqs/en/
Strengthening and organization of health system for sustainable and, continued supply of vaccines and other logistics
o Establishing well organized systems to procure, manage and distribute vaccines and other logistics.
Oversight of vaccine safety and quality not only within vaccine production facilities and during the lot release by NCL but also throughout the distribution and storage phases in health facilities until the vaccine is administered to the person by the National Regulatory Authorities.
Prioritizing supporting activities to reinforce the regulatory role over the storage and distribution of vaccines within the country in vaccine producing countries and subsequent expansion to all countries of the region.
Incorporating good management practices to effectively deliver vaccines and supplies to the service delivery points in the grass root levels.
Promoting co-ordination of immunization services with the private sector to ensure an un-interrupted effective delivery mechanism for vaccines and supplies with suitable storage facilities
7.2.3.3 VPD Surveillance
7.2.3.3.1 Regional GoalTo enhance VPD surveillance to assist immunization programmes in achieving goals and targets
7.2.3.3.2 StatusEffective Vaccine Preventable Disease (VPD) surveillance is essential for guiding immunization strategies, monitoring programme performance, and allocating resources.
Since 2005, substantial progress has been made in accelerating and integrating surveillance of VPDs with existing AFP surveillance systems in the region. The polio eradication program in SEAR continues to be a
22
model for using data effectively to support AFP surveillance and control polio and other vaccine-preventable diseases8. The polio Surveillance Medical Officer (SMO) network in Bangladesh, India, Myanmar and Nepal and the Surveillance Officer (SO) structure in provinces in Indonesia have proven to be an essential component of effective AFP surveillance for polio eradication.
The AFP surveillance performance indicators of most countries have exceeded global and regional targets. Sub national indicators have been used as benchmarks to identify areas of concern and to prioritize surveillance reviews.
There is an effective system in place where member country surveillance systems notify AFP cases to SEARO/IVD which, in turn, cross-notifies countries within and outside the region in order to shorten response times.
Nepal, Bangladesh, Indonesia and Myanmar submit measles case-based data2 on a monthly basis from their integrated VPD surveillance systems. With the aim of obtaining information to determine the progress of countries in achieving measles elimination, since 2009, the data collection tools of SEAR were modified to capture information on suspected measles cases, outbreaks and classification of outbreaks.
A comprehensive laboratory network supports field surveillance. The SEAR laboratory network consists of 17 polio, 22 measles and 14 JE laboratories supporting field surveillance. Laboratory data and field data are merged electronically to give the final “picture” of the Vaccine Preventable Diseases in the region.
7.2.3.3.3 Issues/Challenges
Expansion of case based surveillance especially for measles to ensure that all indicators and targets towards elimination are achieved at national and sub-national levels.
Requirement of greater government support for expansion of surveillance networks including case-based surveillance and investigation of case
Varying quality of the annual data provided in WHO/UNICEF Joint Reporting Form (JRF) and Annual EPI Reporting Form (AERF) by country and inconsistency with the year-end surveillance data provided through the aggregate monthly reporting system
Need for commencing surveillance of the diseases targeted by the introduction of new and underutilized vaccines.
2
23
7.2.3.3.4 Policy approaches and activities:.
Surveillance of VPDs before vaccine introduction
Demonstrating the disease burden to justify vaccine introduction, identifying circulating strains of the organism and establishing a system to measure vaccine impact when the vaccine is introduced.
o Currently, targeted syndromes are diarrhoeas and pneumonias targeting Hib and pneumococcus, meningococcus, rotavirus and typhoid organisms.
o In general, sentinel hospital based surveillance is being carried out for some of these diseases among children less than five years.
Where potential vaccines have been identified for introduction, commencing surveillance of the respective diseases while strengthening the overall surveillance system.
o This ensures that correct estimates of the attributable faction are obtained for decision making.
o Concentrating only on the disease for which a potential vaccine has been identified leads to erroneous exaggeration of the disease burden
o Although starting such surveillance activities will be costly initially, in the long term, it provides benefits of the investment for the introduction of a new vaccine that will far outweigh the negative impacts in the short term.
Surveillance of VPDs after vaccine introduction
In line with the guiding principles of the Global Immunization Vision and Strategy - GIVS (2006-2015)12 to pursue policies and strategies based on evidence and best practices, the SEA Region is encouraging Member States to ensure that, by 2015 or earlier, all countries will have developed the capacity at all levels to conduct case-based surveillance of vaccine-preventable diseases, supported by laboratory confirmation where necessary.
Where this may not be possible for all VPDs, starting case-based surveillance and investigation at least for diseases targeted for elimination; and carrying out routine surveillance for all other diseases at all levels.
24
prioritizing diseases for which case based surveillance systems should be established by Member countries
Considering measles which is targeted for elimination as a priority
Strengthening of the existing system and its expansion of VPD surveillance.
o Recruiting and providing adequate training to selected personnel
o Considering funding of these activities a priority by both governments and donor agencies.
Reviewing the discrepancies between the annual data provided by JRF and AERF and the monthly surveillance data in detail.
o Periodic reviews at closer intervals such as quarterly intervals to reconcile inconsistent data.
o The introduction of immunization registers maintained by health care workers that record all immunizations given would help in minimising data discrepancies.
Expansion and integration of the VPD surveillance laboratory network with surveillance of other communicable diseases.
7.2.3.4 Adverse Events Following Immunization (AEFI) Surveillance, causality assessment and management
7.2.3.4.1 Regional GoalTo eestablish and sustain effective systems for monitoring adverse events following immunization, their management and communicating the investigation results with all stakeholders
7.2.3.4.2 Status
As the incidence of vaccine-preventable diseases is reduced or even close to elimination due to high routine immunization coverage, Supplementary Immunization Activities (SIA), the use of vaccine of assured quality, and the rate of adverse events associated with immunization become relatively more apparent with better surveillance systems able to detect and report AEFI which before were unnoticed. This conjunction of factors consequently has led to increased public concerns about vaccine safety. In the SEA region, MoHs had to temporally suspend immunization services following clusters of deaths temporally associated with AEFI (e.g. with the use of Measles vaccines in Myanmar in 2005-2006 and in India in 2008 and 2010, and with Rubella vaccine in Sri-Lanka in 2009). The MoHs with the technical assistance of WHO, conducted causality
25
assessments and scientifically demonstrated that the quality of the vaccine was not related to the causes of the deaths reported as AEFI.
AEFI surveillance is an important aspect of immunization services. While all member countries have some sort of AEFI surveillance system in place, there are wide variations in its practice, both between and within countries. Where surveillance systems are in place, causality assessment is done when serious events occur. Management of potential AEFI are done at the peripheral level based on guidelines issued by the nationalprogrammes.
7.2.3.4.3 Issues/Challenges Improving AEFI surveillance and causal investigation with view to
improving immunization services as well as maintaining client confidence in the programme.
Causality assessment and reassurance of the public to counter adverse media reports following the occurrence of adverse events.
Non-allocation of funds by many MoHs to the national AEFI
committee to conduct vaccine post-licensure studies or to conduct periodic meetings for causality assessment and providing feed back.
Though very well documented vaccine safety profiles which have facilitated AEFI causality assessment are available for traditional EPI vaccines, changing paradigm for the introduction of under-utilized and new vaccines possessing regulatory challenges to the NRA in the SEA countries
o Pentavalent vaccine is manufactured by four manufacturers in four countries including 2 in the SEA region.
o The vaccine although licensed in all the producing countries, is not used in the National Immunization Programm as it is produced to supply developing countries mostly with no AEFI system.
o Consequently very limited post-licensure safety data are available constraining the comparison of AEFI rates among the countries using the vaccine.
7.2.3.4.4 Policy approaches and activities
Establishing functional expert committees on monitoring AEFI in all Member States-
Operationalizing mechanisms of adequate monitoring and timely management of AEFI along with establishing effective communicating channels with all stakeholders.
26
Countries being open on this issue and sharing the information with immunization stakeholders including WHO and national AEFI committees to avoid crisis situations resulting from inaccurate and adverse media reports based on false allegations of vaccine sub-quality.
o Keeping the media informed by EPI managers not only at the time AEFI occurs but each time a major policy change occurs such as the introduction of a new vaccine in the NIP, major upgrading of the cold chain infrastructures, Supplementary Immunization Activities, etc…
Including a secretariat and having a budget to fulfill their duties and responsibilities by National AEFI committees.
Striving to raise funds in novel ways by member countries to support AEFI surveillance including mobilization of the support of vaccine industry, the AEFI surveillance role of which has been limited. Due to perceived conflicts of interest, lack of credibility, and vaccination promotion by public health institutions.
Ensuring that the role of the National Regulatory Authority and the National Control Laboratory in overseeing the safety, quality and efficacy of the vaccines is well understood especially in the countries that do not produce vaccines.
o Establishing the role of the NRA/NCL from the moment the vaccine specifications are developed and tenders are issued for their procurement.
o Then checking compliance with specifications and release the lot for use in the NIPs by NRAs.
o Contacting manufacturers to verify if similar incidents have occurred in other countries where the vaccine was distributed and also to conduct testing procedures when AEFI occurs
o Adopting WHO developed guidelines for fast track licensing that include simple procedures to be undertaken by the NRA when WHO pre-Qualified vaccines are delivered to countries13.
Providing WHO’s technical support to strengthen procedures established by countries to respond to serous AEFI cases by empowering national AEFI committees and advocacy for greater involvement of NRAs/NCLs in investigations.
Promoting the capacity of assessing the causality assessment between an AEFI and a vaccine using a three-pronged strategy:
27
a. To enhance regional networking of AEFI experts to share AEFI data in order to document vaccine safety profiles especially for vaccines that have recently been introduced and for which limited data is available in the region.
b. To streamline and standardize procedures for field and laboratory investigations. This includes completeness and timeliness of the investigation.
c. To prepare a regional guideline by the WHO to utilize laboratory investigations to verify causal hypothesis, post mortem investigations when they can be undertaken to verify a hypothesis for the benefit of National AEFI committees
Ensuring access to vaccine regulatory experts from 10 different member countries of the global PMS network, gain experience in conducting AEFI investigation and causality assessment, develop and field test models to establish a system for post-marketing safety surveillance of vaccine.
o SEARO/IVD/VSQ strategy to strengthen surveillance of vaccine safety is in line with WHO global strategy that promotes cross-country cooperation and establishment of networks
o Participation of member states in WHO established Global Network for Post-marketing surveillance of newly Pre-Qualified vaccines
Management of AEFIs and counseling of clients to boost public confidence in immunization services.
o Developing proper guidelines for the management of AEFIs and counseling services for the region having taking into consideration the vaccines used in the region.
o Making this a part of all refresher training programs for all categories of health care personnel involved in providing immunization services.
7.2.3.5 Human resources7.2.3.5.1 Regional Goal
To make available adequate trained and competent human resources with necessary skills and facilities for their mobility to provide an effective and quality immunization services
7.2.3.5.2 Status
28
For the EPI programme to be effective an adequate number of competent personnel at all levels is required. Personnel should have the basic prerequisites, core knowledge, specific skills and competencies to accomplish the given task. However, inadequate human resource availability is a problem in all member countries. Human resource capacity is not adequate to cover all the target population. As a result of inadequate human resources, the existing workforce is overburdened and it will reflect in their performance of the duties.
7.2.3.5.3 Issues/Challenges
Lack of an adequate number of competent personnel to increase immunization services to pockets of hard-to reach populations and marginalized communities identified in member countries.
Lack of adequate human resources in clinic centers due to the poor mobility of existing health workforce especially in hard to reach areas.
Ensuring the availability of a critical mass of competent personnel in all member states with the need to improve current immunization services in general and the possibility of introduction of new and under-utilized vaccines in the short- and mid-term
7.2.3.5.4 Policy approaches and activities
Mapping existing health workforce required for maintaining equitable immunization by countries
Filling vacancies of the workforce in providing immunization services based on the gaps detected
Providing relevant facilities for mobility by the health workforce to provide an equitably accessible, quality immunization service
o In many pockets of hard to reach populations, the lack of mobility of the workforce further affects the access to immunization services
Providing training opportunities to enhance the skills of the immunization workforce
o There is an abundance of literature and training materials that have been developed by WHO and other agencies for public use
o Currently training programmes at different levels are been carried out in all member states.
o There is a need to train additional personnel to improve existing immunization programmes as well as to cater to the increased demand envisaged with the introduction of new vaccines.
Considering translation and modification of generic training material to suit the demands of member countries without compromising the
29
essential knowledge, skills and competencies required by personnel working in immunization programmes.
Enhancement of basic training and in-service training programmes for all categories of health care personnel at all levels both in quality and quantity with attendance of a critical mass.
. Considering a system of certification especially in places where sectors other than the public sector are heavily involved in immunization services. Where possible, this would have to be tailor made for individual member states.
Considering appropriate attractive incentive schemes based on performance to retain trained personnel to ensure that services of the highest quality are delivered.
7.2.3.6 Good governance and management capacity7.2.3.6.1 Regional Goal
To Invest in strengthening effective management of immunization
services with a view to promoting good governance, accountability of quality services and effective decision making
7.2.3.6.2 StatusAll programmes have to be managed efficiently to be effective. Management of EPI programmes have to be done at different levels viz, national, sub-national, field level etc. At each of these levels, the skills and competencies required of managers vary. Although materials for training of managers are available, training of managers are not carried out on a regular basis in member states for different reasons. Governance relates to decisions that define expectations, grant power, or verify performance as a separate process or part of management process. Governance remains an integral component in provision of immunization services in terms of both the coverage and quality. All member states in the region have governing mechanisms consolidated within their Expanded Programs Of immunization. However, the governance types, degree of execution and effectiveness of the governing methods are so variable that they have been reflected in output indicators of immunization programs. For example, all countries in the region tend to have areas with low immunization coverage. Nevertheless, only seven countries in the region have successful in reaching immunization coverage of over 90%. The success of these countries lies in the fact that they have been able to identify barriers leading to low immunization coverage and address them proactively. Meanwhile the inability to address these issues proactively in other countries has hampered the success in achieving the GIVS target of over 90% coverage at national level. This has occurred against the background of the availability of evidence on further improvability of immunization coverage with a proactive approach and the continued
30
failure to demonstrate results indicate existing governance issues that attribute to management failures in these countries
7.2.3.6.3 Issues/Challenges
Non consideration of qualifications and experience in appointment lower level EPI managers though it is considered in appointing higher level managers.
o Sometimes, even at higher levels of management, experience in the EPI programme itself may not be considered with deleterious effects on the programme itself.
Inability of the managers to adequately conduct situational analysis, monitor processes and take corrective actions.
Inaction in relation to coordinating and capitalizing on strengthening immunization through health system strengthening mechanisms due to inadequate managerial capacities
Ensuring that lower level managers of the EPI programme have the necessary management skills to function efficiently to ensure an effective immunization service.
Introducing and sustenance of good governance in immunization programs to make effective decisions directed at improving access to immunization services, creating demand in areas where the coverage is low, strengthening immunization service delivery, information use and overall improvement in management capacity.
7.2.3.6.4 Policy approaches and activities
Intensive focus of member countries on improving the overall management process.
o commitment of member states to ensure managers at higher levels of the EPI programme have the necessary technical knowledge and management skills to manage immunization programmes efficiently
o Regular programmes not necessarily be specific to immunization services for managers to improve their skills and competencies
o Training of lower levels managers done periodically especially at junior levels where there is a regular turnover of personnel.
Requirement of the commitment of governments of member states and funding agencies such as WHO to ensure adequate funding of these programmes that would have ripple effects on the entire health system
Investment in training and supporting good managers to strengthen their managerial skills for effective management of immunization services to provide quality immunization service.
Promoting Middle Level Management (MLM) training to consolidate management process through enhancing managerial skills in following areas
31
o partnering with the community, logistic management, ensuring vaccine safety, annual planning for EPI related activities, ensuring proper function of the disease surveillance system, conducting EPI coverage surveys, engaged in supportive supervisions and monitoring the EPI activities.
Supporting the mangers too be responsive and accountable for situations affecting immunization
services and adoptive in taking corrective actions.o innovatively strategize for emerging new situations which may be
challenging for the sustainability of immunization services
Setting priorities and based on priority activities setting targets Supervision and monitoring activities to appraise if these targets
have been reachedo Regular reviews of immunization services where good and bad
management practices are highlighted would help to relinquish bad practices and adopt good practices that would ensure accountability and quality of the immunization service in general.
o Improve performance through reorganizing monitoring and supervision systems
o Establish Standard Operative Procedures (SOP) for streamlining the purview of activities more efficiently
7.3 New Vaccines7.3.1 Regional goal
To ensure that the introduction of new and under-utilized vaccines into immunization programmes in the region are evidence based, affordable to member countries, and done in an equitable manner without affecting the effectiveness of existing programmes so that limited resources are used in a manner that helps achieve optimum outcomes in terms of reduction of the disease burden in the region.
7.3.2 StatusVaccines not included in the EPI programme have been available for some time and some of them are available in the private sector. A safe and effective Hepatitis B vaccine has been available for many years now but SEAR has still not completed its introduction. Except India, all countries in the region have introduced the Hepatitis B vaccine within the last 10 years; in India, 25 of 35 states are still to introduce it. Sri Lanka introduced the pentavalent vaccine within 2 years of its introduction; currently 4 countries in the region have introduced the pentavalent vaccine into their national immunization programmes. Bhutan has successfully negotiated with donors and introduced the relatively expensive HPV vaccine in its EPI in May 2010.
32
7.3.3 Issues Complexity of the introduction of new vaccines especially when the country’s
immunization systems are weak and routine immunization coverage are low.o Recommendation of one school of thought that countries that have not
been able to provide the six basic EPI antigens in hard to reach areas should strengthen the immunization systems before introducing new vaccines.
o Recommendation of the other school of thought that countries with weak systems have a better chance of improving their performance when faced with new challenges and, hence, introducing new vaccines will be a great opportunity for them to strengthen their existing weak systems.
o The availability of new vaccines in the private sector
Consideration of following aspects in the introduction of new vaccines as an important intervention to achieve MDG 4
o The demand, vaccine characteristics, system capacity and vaccine financing based on sound evidence.
o Programmatic issues, vaccine strategies for general and specific populations, legal and regulatory frameworks and ethical issues.
Issues related to graduation as a result of the improving socioeconomic
conditions of the countries of the region
o Promotion of five more countries in the region to the low middle income country group in 2011
o Only Bangladesh, DPRK, Myanmar India and Nepal as GAVI eligible countries in the region.
A rational approach to deal with AEFIs and gain the confidence of the medical profession and the public. with the introduction of new vaccines,
7.3.4 Policy approaches and activitiesCriteria for introduction of new vaccines in the Region have been clearly spelt out in the Regional Vaccine Policy for South East Asia12 and the Report of the South East Asia Regional Vaccine Prioritization Workshop13. These criteria are currently applicable. A checklist of criteria for introduction of new vaccines is given below:
33
CHECKLIST OF CRITERIA FOR INTRODUCTION OF NEW VACCINEA. Demand
Burden of disease: Is the disease a public health problem? How does this burden compare to that of other diseases?
Epidemiological features of disease: Is the disease epidemic or endemic? What is the age distribution of cases? What is the phenotype of the infecting organism?
Community demand/acceptance: Does the population generally feel the need for another vaccine?
Availability and effectiveness of alternative/complementary measures for disease control: Is immunization the best strategy for ameliorating this disease?
B. Vaccine characteristics Availability of the vaccine: Is there an adequate global supply of quality vaccine
available? Are the sources WHO pre-qualified? Protective characteristics of the vaccine: What is the vaccine efficacy? How
long does immunity persist? What are the adverse events associated with the vaccine?
Implications on local production: Will a new, imported vaccine threaten local production? Is it feasible to produce the vaccine locally?
C. System capacity Strength of current EPI system to absorb a new vaccine: Is it logistically
feasible to add a new vaccine? How well is the current immunization programme working? What are the programmatic implications (e.g. Will it require an additional visit?)
Available information on practical effectiveness of the vaccine: What is the realistic performance in target populations?
D. Financing Balance between costs and benefits: What are the direct and indirect costs of
adding a new vaccine? How will benefits be calculated? Will the introduction of the vaccine increase the equity of health services?
Sustainability of financing: How will the vaccine and any other necessary resources (e.g. syringes) be funded in the long term?
Source: WHO Regional Vaccine Policy for South-East Asia Region, New Delhi 2003 (SEA-Vaccines-133)
Focusing on estimation of the disease burden, which is an important consideration in the introduction of a new vaccine, relative to all diseases by improving the surveillance system, in general, rather than targeting an improvement of surveillance of a single disease entity.
34
Not disregarding other effective preventive measures with the introduction of a new vaccine, although immunization may be the most cost effective strategy to control the spread of a disease and its consequences.
Introduction of new vaccines is at the sole discretion of member states considering factors such as the availability and production of the vaccine, and the affordability and the capacity of the routine immunization programme to accommodate the new vaccine.
Requirement of in- and inter-country meetings and plans to identify gaps for delaying NUVIs including risk communication plans, country support teams to ensure coordinated response from partners and strengthening AEFI surveillance systems for the introduction of new vaccines into routine immunization programmes.
Promoting phased introduction of new vaccines or targeting high risk groups as suitable alternatives in countries with inadequate capacities for introducing a new vaccine on a country wide basis.
Ensuring that only safe and effective vaccines are made available to populations in member countries through enhancing and empowering the legal and regulatory framework of member states as described in section 7.4.4 to counter challenges posed by the availability of new vaccines in the private sector.
Stockpiling vaccines at the regional level, preferably by WHO, to be used in any emergency such as pandemic situations.
7.4 Legal and regulatory framework of countries of the Region7.4.1 Regional goal
To enhance and empower country level legal and regulatory frameworks to ensure the access and availability of safe effective and quality vaccines to populations in member countries of the Region under the purview of a fully functioning, competent national regulatory authority (NRA) backed by an appropriate national control laboratory (NCL) and research institutions .
7.4.2 StatusWHO included a fully functioning NRA as a pre-requisite to Pre-Qualify vaccines in 2002. WHO recommended six functions for NRAs in vaccine producing countries and assessment tools to evaluate the NRAs were developed in consultation with experts from developing countries and industrialized countries. In SEARO, vaccine producing countries were assessed and institutional development plans including training on vaccine quality through the
35
Global Training Network were implemented and progress monitored through periodic re-assessments of the NRA. In 2009, all the NRAs in the vaccine producing countries of the SEA region were functional regulating vaccine safety, quality and efficacy.
It is well recognized that the WHO pre-qualification procedures for vaccines and the NRA capacity building programme were successful in building national regulatory authority capacities in member states and assuring the availability of quality vaccines in developing countries. In the SEA region, it has enabled several countries to procure quality vaccines from other sources after cessation of procurement through UN agencies. In the vaccine producing countries, the enforcement of WHO recommended safety and quality standards for vaccines through capacity building of local NRAs have enabled local manufacturers to expand their market beyond the NIP, to invest to upscale production and to access novel technologies for vaccine production through joint ventures with manufacturers in developing and industrialized countries.
In the developing countries with limited NRA capacity, the WHO PQ mechanism has enabled local manufacturers to submit their vaccines to an independent review process. Once the product is WHO PQ, the vaccine manufacturers may gain access to international markets through UN procurement agencies. This regulated environment has significantly increased availability of vaccines of assured quality in the region and globally, fostered a more competitive market, contributed to reduced prices and provided better access to high quality vaccines including pentavalent vaccines which, currently, are still relatively expensive but have become more accessible for low and middle income countries.
7.4.3 Issues/challenges
Urgent need to strengthen the sustainability of national vaccine regulatory systems at the regional level giving priority to WHO PQ vaccine producing countries in the region, namely, India, Indonesia and Thailand with the increased demand for under-utilized and novel vaccines, the increasing complexity of vaccine formulation and the limited capacity of WHO to review and assess all manufacturers applications to PQ vaccines.
Challenges to capacities of countries in the region to develop production plans posed by the emerging pandemics and the need to rapidly upscale production of seasonal and pandemic vaccines
The need to increase regional cooperation to develop and manufacture vaccines and for early involvement of NRAs in the pre-licensure phase of vaccine development to minimize delays in commercial production of the vaccine and its introduction into the population when required.
7.4.4 Policy approaches and activities
36
Overall policy of building sustainable regulatory systems with financial and expertise capacity to regulate vaccines giving priority to vaccine producing countries and countries procuring vaccines directly from the international market.
o Ensuring following line with the WHO strategy to decentralize expertise to regions and countries.
o Anticipated transfer of some of the PQ activities to NRAs in regions and country in a phased manner. by the WHO as NRAs have better capacity to regulate vaccines currently
o Providing greater responsibility in the PQ process to NRAs as they gain experience and maturity in regulating vaccine safety, quality and efficacy
o Developing SOPs to assess the acceptability of vaccine for procurement through UN agencies.
Training through the WHO Global Learning Opportunity (GLO) or through in-country training workshops
The regional policy is to support initiatives that involve global and regional fora, such as the Developing Country Vaccine Regulatory Network (DCVRN3), the Developing Country Vaccine Manufacturers Network (DVCMN4) and the Association of South East Asian Nations (ASEAN) Vaccine Chapter, to harmonize and standardize vaccine regulatory requirements across the region
Establishment of a regional network of NRAs to assist countries which may not be able to develop ideal NRAs leading to greater inter-country cooperation, granting reciprocal recognition and assisting countries in introducing new vaccines.
3 The DCVRN was established in 2004 with the mission to promote and support the strengthening of regulatory capacities of NRAs of emerging and developing countries for evaluation of clinical trial proposals (including preclinical data and product development processes) and clinical trial data through expertise and exchange of relevant information. The member countries include the Republic of South Africa, India, Indonesia, Thailand, South Korea, China, Russia, Cuba and Brazil. The DCVRN is a strong coordinating network which has already met to address regulatory issues on HIV, Rotavirus, HPV (Nov 2005), Typhoid (May 2006) and regulatory monitoring of Clinical trials (Nov 2006). The regional policy is to promote harmonized procedures for clinical trials and will continue to engage DCVRN in the discussions and elaboration of CT procedures for the region.
4 The DCVMN is a network of emerging vaccine manufacturers in developing countries including the Republic of South Africa, India, Indonesia, Thailand, South Korea, China, Russia, Cuba and Brazil. The network goals are: to promote transfer of vaccine conjugation technology from the Netherlands Vaccine Institute (NVI) to produce DTP containing vaccine including DTP-Hep B and DTP-Hep B and Hib vaccines and, to foster the development of the members to attain WHO Pre-Qualification criteria, to encourage continuation of research and development efforts to facilitate emerging vaccine needs in developing countries. Members of this network are all in demand for WHO PQ status and for a strong NRA in their country to enable them to export their vaccines. The DCVMN network represents a strong advocacy partner to strengthen NRA capacity.
37
o Enabling licensing of vaccines based on evidence provided by other NRAs.
o Elimination of the need to conduct fresh trials in the recipient country
7.5 Research and Development7.5.1 Regional goal
To establish and implement a research and development plan to ensure safe and effective immunization services including vaccines of assured quality for all vaccine preventable diseases prevalent in the region.
7.5.2 StatusResearch and development of vaccines and immunization services in the region are minimal due to poor infrastructure and limited funding for such activities given other pressing problems faced by countries of the region. Currently, the region is dependent on vaccines that have originated in developed countries. With bilateral and global agreements such as the TRIPS agreement, technology transfer is restricted and new vaccines are costly that some countries could ill afford to introduce them into their routine immunization programmes.
The National Vaccine Committee Office (NVCO) established in 2003 by Thailand is the only country in the region that has a committee which actively promotes vaccine research and development
7.5.3 Issues/challenges
Despite financial support from international funding and initiatives since 2000, the focus of this assistance which is critical to stimulate regional vaccine research, was mainly focusing on clinical trials of products being developed by industrialized manufacturers and on transfer of technology or importing bulk to develop production capacity in developing countries of existing non-patented vaccine products.
Hampering of the development of novel vaccines needed for the South East Asia by
o the lack of interest, incentives and support from governments in producing countries,
o the challenges posed by Intellectual Property Rights (IPR) and regulatory compliance,
o limited coordination with research institutes, manufacturers, National Regulatory Authorities and national immunization programmes
Despite the availability of a large regional scientific community especially in
vaccine producing countries with sophisticated laboratory facilities in some countries, non-existence of a strong link with medical institutes, NRAs, manufacturers and the national EPI programmes to define research priorities.
38
7.5.4 Policy approaches and activities
Sustenance of the system established in SEA countries to register and monitor the number of vaccine clinical trials conducted in WHO member states by the WHO supported NRA capacity building programme. This enables the NRAs to regulate safety, quality and efficacy of vaccine from seeds to the mass production of the final product.
Requirement of Vaccine Research and Development for strong coordination among the stakeholders especially, with new vaccine products becoming increasingly sophisticated in their preparation, formulation and production technology.
o Conducting a review of vaccine R&D and developing a road map to bring vaccine research to the final product and mass production by all the vaccine producing countries
o Establishing coordinating bodies that would ensure the synergy among stakeholders including the NRAs, the medical research institutes, the manufacturers and the national immunization programmes by . Member state governments
o Inclusion of a secretariat and budget to conduct product research reviews, establish Scientific Technical Advisory Groups (STAG) to review progress and to advise on steps to further develop the product in the coordinating body
o Empowering the coordinating body to develop a vaccine policy based on the disease burden, status of research, financial feasibility, and R&D and production capacity
Encouraging the establishment of vaccine research and development coordinating
bodies similar to NVCO in Thailand to coordinate reviews of country-specific vaccine research projects through Scientific Technical Advisory Groups (STAG) established in compliance with WHO agreement on conflict of interest and confidentiality
o Reviewing outcomes of STAG, communication to the international research community through publications and presentations at international peer meetings.
Promoting the networking of in-country coordinating bodies with existing trans-regional networks like the Developing Country Vaccine Manufacturers Network (DCVMN) and other networks of international experts on vaccine development
To ensure sustainability for immunization programmes in all member countries through assured funding from either national or international resources.
39
7.6.2 StatusAll member states fund their immunization programmes through allocations of national budgets or through donor funds for country programmes. The highest percentage of budgets of public/preventive health programmes is spent on immunization services. Immunization services have also proved to be cost-effective investments in controlling vaccine preventable diseases and reducing childhood morbidity and mortality in the quest to achieve MDG 4.
7.6.3 Issues/challenges Adequate funding for sustainability of all effective programmes.
o Additional investments in terms of infrastructure development such as the cold chain and purchase of the vaccines which are usually more expansive than the vaccines used in routine immunization programmes for the introduction
o Long term commitment for sustenance of a new vaccine , once introduced, for many decades
Serious funding issues regarding funding of immunization programmes arising as a result of cessation of funding from agencies such as GAVI parallel to moving or likelihood of moving of a few countries of the region ahead in the socio-economic ladder as low middle income countries
7.6.4 Policy approaches and activities Assurance of adequate funding by individual governments through dedicated
allocations from national budgets. o Inclusion of costs of vaccines and all other aspects of immunization
services including the use of auto-disable syringes in allocations o Allocations being a central function even in a decentralised systemo Development of an immunization policy for each country incorporating
sustained funding for the immunization programme.
Encouragement of national governments to increase their spending on immunization, in general, as a cost-effective intervention that is a primary responsibility of the public sector.
Approaches which can help move in this direction include:
o Use of cost-effectiveness and public finance principles to allocate funding;o Establishment of legal mandates for baseline funding (e.g. budget line
item for vaccines);o Establishment of trust funds o Use of immunization coverage and measures of programme performance
as indicators of public sector involvement;o Taking steps to ensure efficient use of funds;
40
o Working with donors to determine strategic interventions so that external support does not displace domestic investment (7)
o Policy-makers should determine their national plan for financing immunization based on a mix of the four basic sources of finance for immunization in any country:
Domestic public (e.g. tax revenues or social health insurance) Domestic private (e.g. user fees) External public (e.g. bilateral development assistance) External private (e.g. the Vaccine Fund)
o Evaluation of the options based on the following criteria in choosing optimum sources for financing by countries : Promote equity, achieves efficiency, provides resources in an adequate, timely, and reliable manner, engenders accountability, and encourages the highest level of self-sufficiency.
o Consideration for sustaining the administration of the vaccine over many decades when a decision to introduce a new vaccine is taken
o Reliable budgetary projections for consideration in the short-, the medium- and the long-term
o Novel mechanisms of funding such as using the pentavalent vaccine instead of monovalent vaccines enabling a decrease in the cost of immunization programmes and cost-saving to the country.
o Then channelling these funds for improving the existing immunization services and/or purchase of other antigens.
o Local manufacture of vaccines and AD syringes to reduce costs. - this may not be financially viable for small countries and is not advisable unless other infrastructure such as a NRA and a NCL are in place
o Facilitating the purchase of quality vaccines at cheaper rates especially if bulk purchases of pre-Qualified vaccines are done and negotiating with countries on pricing structures by the WHO
o WHO’s assistance to member countries in finding funding options for immunization programmes and striving to convince GAVI and other donor agencies to extend benefits to low middle income countries as well.
o Coordinating donor supply, pooling of resources and exploring possibility of pool procurement are some other policy approaches that deserve attention in this context
41
7.7 Client satisfaction and community participation7.7.1 Regional goal
To attain the highest possible levels of client satisfaction and community participation in immunization programmes in all countries of the region.
7.7.2 StatusClient satisfaction and acceptance has generally not been addressed in immunization programmes which, in the past, have been supplier driven. High vaccine coverages and low drop-out rates are an indirect indication of client acceptance and satisfaction.With advances in the education sector and improvement in literacy in the countries of the region, expectations of clients have also increased. The ready availability of information on the internet and ready access to it has compounded the knowledge of the public.
7.7.3 Issues/challenges The way communities view and respond to health services including
immunization services as a result of client expectations and access to information are changing. Contrast to the past where immunization services were supply driven, more demand driven nature of the health system and immunization services today with the private sector playing a leading role in delivery of immunization services are seen.
Considering client satisfaction as a prerequisite for community participation that would eventually lead to wide immunization coverage and an effective immunization campaign client satisfaction also needs to be addressed. The issues such as counselling and prompt and effective management of AEFIs should be effectively managed.
Neglecting accountability to clients especially with regard to the occurrence of serious AEFIs and the fact that clients have the right to know the reasons for the possible AEFI.
7.7.4 Policy approaches and activities Acknowledging that client satisfaction is a key to a successful immunization
programme, Strengthening ability of health care workers to communicate and interact
effectively with clients, providing counselling services in a people friendly manner to gain the confidence of clients on immunization services. Ensuring consistency in the messages given when dealing with the public especially in dealing with serious AEFIs that may be misreported by the press.
o Setting up a public relations unit for this purpose within the immunization programme to deal with these issues and to keep the public well informed. This service may also be used as a hot line to provide current information on vaccines and the immunization programme.
Improving client satisfaction and community participation. This requires enormous amounts of attitudinal changes from staff. Special programmes will
42
have to be conducted and measurable reward systems set in place to achieve these changes. The concept of certification as a “people friendly facility” may be considered to boost public confidence.
7.8 Strengthening Health Systems by Augmenting Immunization Services in Primary Health Care Services7.8.1 Regional goal
To strengthen health systems in member countries of the region by revitalising primary health care through immunizations programmes
7.8.2 StatusPrimary Health Care (PHC) that was adopted by all member countries with the Alma Ata Declaration of 1978 is the main strategy in provision of public health/preventive care services in the region. Immunization service is a principal component of that strategy and has been a success story in the health sector. High immunization coverages in all member countries indicate the accessibility to, and acceptability of, the PHC approach by the community. During last decade, the concept of the PHC approach has lost momentum, but there are attempts to revive the concept.
7.8.3 Issues/Challengeso Inability to disintegrate immunization services and PHC (see figure 1) from the
health system. The benefit of this is that improvements in the immunization services improve the health system and vice versa.
o The need to revitalise the PHC system not only to strengthen the health system to provide basic services to populations to reduce morbidity and mortality but also to reduce health care budgets which are increasing exponentially for a variety of reasons.
7.8.4 Policy approaches and activities Utilizing all the overarching and inter-related policy approaches and activities to
achieve the goal for health for all. Liaising with other sectors and tacit coercion by WHO to build a strong political
commitment and inspired leadership to revitalise PHC. .Strengthening immunization services and increasing immunization coverage to
strengthen the PHC approach Making the health system popular by extending the immunization
services to cover hard-to-reach populations and marginalised communities
Encouraging national governments to invest in primary health care to achieve equity in health care.
1. Making PHC an integral part of the Health sector reforms process.2. Increasing resources for PHC
43
3. Involving the private sector in such reforms so as enabling opening an avenue for the regulation and monitoring private sector immunization services
4. Training and re-training of staff at all levels and expansion of services to improve immunization services and to strengthen the health system. This in turn will increase patient satisfaction and lead to a demand driven health system.
Table 1. Vaccines used in Member Countries - 2009
Vaccine Ban
glad
esh
Bhu
tan
DPR
K
Indi
a
Indo
nesi
a
Mal
dive
s
Mya
nmar
Nep
al
Sri L
anka
Tha
iland
Tim
or L
este
BCG OPV DTP DTP+Hep B DTP+Hep B+Hib Measles MR MMR TT Td YF Vit A HPV Hep B DT IPV JE Rubella
44
References
1 Rajatatnam JK, Marcus JK, Flaxman AD, Wang H, Rector AL, Dwyer DM, Costa M, Lopez AD, Murray CL. Neonatal, postneonatal, childhood, under -5 mortality for 187 countries, 1970-2010: a systematic analysis of progress towards Millennium Development Goal 4. Lancet 2010; 375:1988-2008. 2 Copenhagen Consensus 2008. http://www.copenhagenconsensus.com/default.aspx?ID=953, accessed 9th June 2010. 3 WHO, UNICEF and World Bank. State of world’s vaccines and Immunization 3rd ed. Geneva. WHO 2009.4 Global Vision and Immunization Vision and Strategy. WHO and UNICEF, 2005.5 The World Bank. World development report 1993: Investing in health. New York, Oxford University Press, 1993.
6 Walker DG, Hutubessy R, Beutels P. WHO Guide for standardisation of economic evaluations of immunization programmes. Vaccine 2010;28(11):2356-9
7 WHO Task Force for Development of a Regional Vaccine Policy. Regional Vaccine Policy for South-East Asia Region. New Delhi, World Health Organization Regional Office for South-East Asia, 2003.
8 WHO. Core information for development of Immunization Policy. Geneva: 2002 (WHO/V&B//02.28)9 Andrus JK, Thapa AB, Withana N, Fitzsimmons JW, Abeykoon P, Aylward B. A new paradigm for international disease control: lessons learned from polio eradication in Southeast Asia. American Journal of Public Health. 2001;91(1):146-50
10 WHO/VAB and GAVI. Assessing the global needs for vaccine research and development: results of a Joint GAVI/WHO meeting, Geneva, 4-5 November 1999. Geneva: April 2000 (WHO/V&B/00.18 & GAVI/00.02)11 Report of the Meeting of Vaccine Producers for Developing Countries. Bilthoven, The Netherlands, November 2000.
12 WHO. Regional Vaccine Policy for South-East Asia Region. New Delhi 2003 (SEA-Vaccines-133)
13 WHO. Report of the South East Asia Regional Vaccine Prioritization Workshop- Bangkok, Thailand. 11-13 May 2009. WHO Regional Office for South East Asia.