45
. . rickets Osteomalacia
| Date post: | 16-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | monther-alkhawlany |
| View: | 83 times |
| Download: | 2 times |

..
rickets Osteomalacia

Rickets is a childhood disorder involving softening and weakening of the bones.
It is primarily caused by lack of vitamin D, calcium, or phosphate.

Sunlight as a source of vitamin D
Lack of vitamin D production by the skin may occur if a person is confined indoors, or works indoors
during the daylight hours, or lives in climates with
little exposure to sunlight.
Sunlight is important to skin production of
vitamin D and environmental conditions where sunlight exposure
is limited may reduce this source of vitamin D.

Sunlight as a source of vitamin D
Adequate supplies of vitamin D3 can be
synthesized with sufficient exposure to solar
ultraviolet B radiation
Melanin, clothing or sunscreens that absorb
UVB will reduce cutaneous production of vitamin D3

Rickets In rickets, another mechanism in the body works to increase
the blood calcium level. The parathyroid gland may increase its functioning rate to compensate for decreased levels of calcium in the bloodstream.
To increase the level of calcium in the blood the hormone destroys the calcium present in the bones of the body and this results in further loss of calcium and phosphorous from the bones. In severe cases, cysts may develop in the bones.
Vitamin D deficiency could be caused due to numerous
reasons

• What are the causes for deficiency of Vitamin D?

Etiology
• . * Vitamin D–deficient conditions :-
– Dietary lack of vitamin D – Insufficient exposure to sunlight – Vitamin D deficiency of

Etiology
. Diseases and drug:
• Liver diseases, renal diseases
• Gastrointestinal diseases
• Antiepileptic
• Glucocorticosteroid

Cholecalciferol (vitamin D-3) is formed in the skin from 7-dihydrotachysterol. This steroid undergoes hydroxylation in 2 steps.
- Metabolism of vitamin D
• The first hydroxylation occurs at position 25 in the liver, producing calcidiol (25-hydroxycholecalciferol), which circulates in the plasma as the most abundant of the vitamin D metabolites and is thought to be a good indicator of overall vitamin D status.

• Cholecalciferol (vitamin D-3) is formed in the skin from 7-dihydrotachysterol. This steroid undergoes hydroxylation in 2 steps.
Pathophysiology
• The second hydroxylation step occurs in the kidney at the 1 position, where it undergoes hydroxylation to the active metabolite calcitriol (1,25-dihydroxycholecalciferol - DHC). This cholecalciferol is not a vitamin, but a hormone.

Vitamin D: The Sunshine Vitamin

Pathway of Vitamin D Production

Calcitriol acts on regulation of calcium metabolism:
• Calcitriol promotes absorption of calcium and phosphorus from the intestine,
• increases reabsorption of phosphate in the kidney,
• acts on bone to release calcium and phosphate;
• Calcitriol may also directly facilitate calcification.
Calcitriol (1,25-DHC) – acts as a hormone rather than a vitamin, endocrine and paracrine properties
CLASSIFICATION• vitamin D deficiency rickets :-
– hypocalcemic rickets– Poor vitamin D intake
– avoidance of sunlight
• pseudo-vitamin D–deficiency rickets :- – familial hypophosphatemic rickets– this syndrome present in the first year of life.
• growth retardation
• Rickets
• hypocalcemic seizures

Pathogenesis
• Vitamin D deficiency
• Absorption of Ca, P
• Serum Ca
• Function of Parathyroid

Pathogenesis PTH High secretion
P in urine Decalcification of old bone
P in blood Ca in blood normal or low slightly
Ca, P product
Rickets

Pathogenesis
• Low secretion of PTH
• Failure of decalcification of bone
• Low serum Ca level
• Rachitic tetany(Spasmophylia)


Causes and types
• 1/vit d defcincy –most common-duto
• 1-ditary diffcincy
• 2-lack exposure sun light
• 3-increase damened
• 2-defective vit d absorbation
• 3-defective activation
• 1- liver and renel dz

• 2-difcincy 1 alpha hydroxlyase enzyme this called vit d depended rickets type 1
• 3-end organ rsistance to vit d this called type 2
• 4-hypophsphatemia called vitamine d resistant rickets
• 5-drugs
Clinical picture
Early rickets :
1- anorexia,irritabilit ,sweating of forhead
2- craniotabese
s (areas of thinning and softening of bones of
the skull).
3- knobby deformities called rachitic rosary
along the costochondral junctions :firstly
palpable not visible

• Advanced rackets• A- Skeletal manifestation • large head ::thickening of the skull develops. This
produces frontal bossing and delays the closure of the anterior fontanelle
depression of nasal bridge
• Delay eruption of
primary teeth
Clinical signs
Frontal bossing

Protruding foreheadasymmetrical or odd-shaped skull

Clinical signs
• In the chest knobby deformities results in the rachitic rosary along the costochondral junctions.• The weakened ribs pulled by muscles also produce flaring over the diaphragm, which is known as Harrison groove. • Forward projection of the breastbone - pigeon chest or pectus carinatum),

Pathway of Vitamin D Production
Rib beading (rachitic rosary)

• Spine deformities (spine curves abnormally, including scoliosis or kyphosis). • In more severe instances in children older than 2 years, vertebral softening leads to kyphoscoliosis
Clinical signs

Knock knee deformity (genu valgum)
Bowleg deformity (genu varum)

Bowlegs and knock-knees
Pelvic deformities

Thikening and enlargment of the wrist and ankleDistal Tibial bowing

Pelvic deformities
Bowlegs and knock-knees
Clinical signs
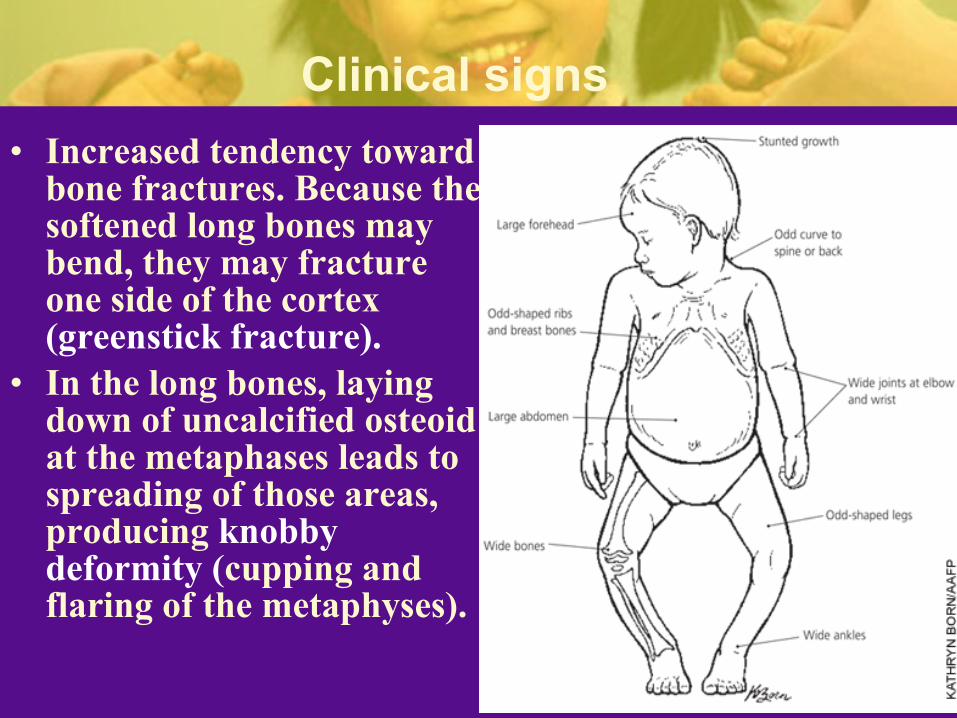
• Increased tendency toward bone fractures. Because the softened long bones may bend, they may fracture one side of the cortex (greenstick fracture).
• In the long bones, laying down of uncalcified osteoid at the metaphases leads to spreading of those areas, producing knobby deformity (cupping and flaring of the metaphyses).
•Extraskeletal manifsetation Progressive weakness•Decreased muscle tone (loss of muscle strength)•Delayed of motor development (( in rickets developing in infancy •Protuberant abdomen ( due to hypotonia of skeletal muscle of abdomen•Fever or restlessness, especially at night•Muscle cramps
•
Clinical signs


investigation• Biochemical findings Calciumdecrease or normal due to
compensatory mechanism *Phosphatedecreas *Alkaline phosphataseincrease
*Serum parathyroid hormone typically is ↑in hypocalcemic rickets, in contrast it is N in hypophosphatemic rickets
Decreases
in serum calcium, serum phosphorus, calcidiol, calcitriol, urinary calcium.
The most common laboratory findings in nutritional rickets are:
Parathyroid hormone, alkaline phosphatase,
urinary phosphorus levels are elevated.

• Classic radiographic findings include:
widening of the distal epyphysis, fraying and widening of the metaphysis, and angular deformities of the arm and leg bones.

Classic radiographic findings include
Anteroposterior and lateral radiographs of the wrist of an 8-year-old boy with rickets demonstrates cupping and fraying of the
metaphyseal region

• Classic radiographic findings include:
Radiographs of the knee of a 3-year-old girl with hypophosphatemia depict severe fraying of the metaphysis.

Radiographic image of wrist and forearm showing pathologic fractures of radius and ulna with rachitic changes of distal end of radius and ulna.

X-ray in rickets


Prevention
**Sun exposure (5_10 min per day)
**Eat food high in vitamin Dfish, , milk and egg,.
**Take supplements of vitamin D and calcium.
Sun exposureSun exposure

Treatment:-
**Vitamine D daily 50-150 mg(calciferol 2000-6000 I.U per day ) after healing reduce dose to400 iu per day **Adequate dietary Calcium & phosphorus provided by milk, formula & other dairy products. Sun exposure .Bony deformities may require bracing or osteotomy .

1. Exposure to sunlight.
2. Daily enough taken vitamin D & Calcium.
3. Good exposure and vitamin D taken for mothers

develop signs of rickets.

















