206
Manual for community-based rehabilitation workers Version 2.0

Manualforcommunity-based
rehabilitationworkers
Version2.0

2
RehabilitationInterventionforpeoplewithSchizophreniainEthiopia(RISE):A
manualforcommunity-basedrehabilitationworkers
August2017
Authors:LauraAsher,CharlotteHanlon,JulianEaton,MaryDeSilva,Sudipto
Chatterjee,RahelBirhane,AtalayAlem,VikramPatel,AbebawFekadu
TheRISEmanualwascreatedfollowinganextensiveinterventiondevelopmentprocessin
collaborationbetweentheDepartmentofPsychiatry,CollegeofHealthSciences,Addis
AbabaUniversity,EthiopiaandtheDepartmentofPopulationHealth,LondonSchoolof
HygieneandTropicalMedicine,London,UK.Forfurtherinformationpleasesee:
http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0143572.TheRISE
interventionwasevaluatedinaclusterrandomisedtrial(ClinicalTrials.govNCT02160249)
Contact:[email protected]
Acknowledgements:Theauthorswouldliketogratefullyacknowledgeseveralsource
materialsthatwereusedtodeveloptheRISEmanual,including‘TheCOPSIManual:Manual
forWorkingwithPeoplewithSchizophreniaandtheirFamilies’(Sangath,Goa,India
http://www.sangath.in/copsi/);the‘MentalHealthPocketGuideforHealthExtension
Workers’(FederalDemocraticRepublicofEthiopiaMinistryofHealth);‘CommunityBased
RehabilitationGuidelines’(WorldHealthOrganisation);‘Facilitator’sGuideforPsychosocial
RehabilitationSupportGroups’(CarrieBrooke-Sumner,PRIMESouthAfrica),‘MentalHealth
andHumanRightsResourcePack’(AmaudoUK,2007),and‘Wherethereisnopsychiatrist:A
mentalhealthcaremanual’(VikramPatel).
Funding:TheRISEprojectwasfundedbytheWellcomeTrust.TheRISEprojectwaspartof
the PRogramme for Improving Mental health carE (PRIME), which is funded by the UK
DepartmentforInternationalDevelopment.
Thismanualbelongsto:
Telephonenumber:

3
Contents
INTRODUCTIONTOTHECBRMANUAL.....................................................................................6
SECTIONA:UNDERSTANDWHATSCHIZOPHRENIAISANDTHEPROBLEMSITCAUSES.............7
1 WHATISMENTALILLNESS?..............................................................................................8
2 WHATISSCHIZOPHRENIA?.............................................................................................13
3 MEDICATIONFORSCHIZOPHRENIA................................................................................18
4 DISABILITIESRELATEDTOSCHIZOPHRENIA.....................................................................21
5 IMPACTOFSCHIZOPHRENIAONTHEFAMILY.................................................................23
6 STIGMAANDDISCRIMINATION......................................................................................26
7 HUMANRIGHTS.............................................................................................................29
8 THEIMPORTANCEOFTHECOMMUNITY.........................................................................31
SECTION B: LEARN HOW TO HELP PEOPLE WITH SCHIZOPHRENIA AND THEIR FAMILIES
THROUGHCBR.......................................................................................................................34
9 OVERVIEWOFCBRDELIVERY.........................................................................................35
10 COMMUNICATIONSKILLSANDPROBLEMSOLVING........................................................50
11 CREATINGATRUSTINGRELATIONSHIP...........................................................................55
12 NEEDSASSESSMENT.......................................................................................................58
13 GOALSETTING................................................................................................................62
14 RISKASSESSMENT..........................................................................................................68

4
15 BEINGAWAREOFTHECAREGIVER’SNEEDS...................................................................73
16 MODULE:UNDERSTANDINGSCHIZOPHRENIAANDITSTREATMENT...............................75
17 MODULE:IMPROVINGACCESSTOHEALTHSERVICES.....................................................81
18 MODULE:PREPARINGFORACRISIS...............................................................................85
19 MODULE:DEALINGWITHHUMANRIGHTSPROBLEMS...................................................89
20 MODULE:SUPPORTINGINDIVIDUALSTOTAKETHEIRMEDICATION...............................96
21 MODULE:IMPROVINGPHYSICALHEALTH.....................................................................106
22 MODULE:DEALINGWITHDISTRESSINGSYMPTOMS.....................................................112
23 MODULE:MANAGINGSTRESSANDANGER..................................................................116
24 MODULE:IMPROVINGDAYTODAYFUNCTIONING......................................................122
25 MODULE:IMPROVINGTHEFAMILYENVIRONMENT.....................................................128
26 MODULE:TAKINGPARTINCOMMUNITYLIFE..............................................................134
27 MODULE:GETTINGBACKTOWORK.............................................................................140
28 MODULE:DEALINGWITHSTIGMAANDDISCRIMINATION............................................146
29 MODULE:IMPROVINGLITERACY..................................................................................150
30 MODULE:TAKINGCONTROLOFYOURHEALTH............................................................152
31 COMMUNITYENGAGEMENT........................................................................................158
32 FAMILYSUPPORTGROUPS...........................................................................................167

5
SECTIONC:KNOWHOWYOUWILLBESUPPORTEDTODELIVERCBR...................................172
33 CBRWORKERWELLBEING............................................................................................173
34 SUPERVISION...............................................................................................................177
35 DEALINGWITHDIFFICULTSITUATIONS.........................................................................182
36 LINKSTOHEALTHSERVICES..........................................................................................195
37 GOODDOCUMENTATION.............................................................................................198
38 HOWTODEALWITHOTHERPEOPLEWITHPROBLEMS.................................................200
39 SUPPORTINGPEOPLEWITHINTELLECTUALDISABILITYANDSCHIZOPHRENIA...............204

6
IntroductiontotheCBRmanual
Whatiscommunity-basedrehabilitation(CBR)forschizophrenia?
Schizophrenia is a long-term illness, which can lead to severe disability in the individual,
especiallyifthecommunitydoesnotacceptthem.Theillnesscanalsoplaceaheavyburdenon
thefamily.Peoplewithschizophreniausuallyneedaperiodofrehabilitationandfamilysupport.
Rehabilitation is where people are helped to regain skills and to return to their usual life
activities.
Community-basedrehabilitation isawaytohelppeoplewithdisabilitiestobe included inthe
lifeof theircommunities. Itaddressesallareasofaperson’s life includinghealth, inclusion in
social lifeandactivitiesofthecommunity, livelihoodandwork,educationandempowerment.
Empowermentmeansthattheindividualhastheabilitytomakedecisionsabouttheirownlife.
Thefocus isalwaysontheneedsandwishesofthe individual.AsaCBRworkeryouwillwork
withindividualswithschizophrenia,theirfamiliesandtheircommunitiestohelptheindividual
togetbacktotheirusualactivitiesandbeacceptedfullyintosociety.
Whoisthismanualfor?
Thismanual is for community-based rehabilitationworkers,whowill beworkingwith people
withschizophrenia.
Howtousethismanual
Thismanualisdesignedtohelpyou:
Understandwhatschizophreniaisandtheproblemsitcauses
àthisiscoveredinSectionA
LearnhowtohelppeopleschizophreniaandtheirfamiliesthroughCBR
àthisiscoveredinSectionB
KnowhowyouwillbesupportedtodeliverCBR
àthisiscoveredinSectionC
ThroughoutthemanualyouwillfollowtheexperiencesofYosefandSara,peoplewith
schizophrenia,andtheirfamilies.YosefandSaraarenotrealpeople,buttheirstoriesinclude
situationsandeventsthatrealpeoplewithschizophreniahaveexperienced.

7
SECTIONA:Understandwhatschizophrenia
isandtheproblemsitcauses
RISE

8
1 Whatismentalillness?
1.1 Whatdoestheminddo?
Theminddoesthefollowingtasks:
• Perceiving:thismeanssight,hearing,smell,tasteandtouch
• Thinking:thismeansmemory,judgementanddecision-making
• Feeling:thismeansemotionssuchassadnessandhappiness
• Behaviour:thismeanshowweact
1.2 Whatismentalhealth?
Mentalhealthmeansthemindisworkingwellandweareproductive,wehavegood
relationshipswithothersandweareabletocopewellwhenproblemshappen.
1.3 Whatismentalillness?
Mental illness is any illness experiencedby a person that affects their emotions, thoughts or
behaviour,andhasanegativeeffectontheirlifeorthelivesoftheirfamily.
1.4 Whatisdisability?
Disability iswhere people have difficulty doing their normal activities andbeing part of their
community.Manypeoplewithmentalillnessexperiencedisability.
1.5 Whydopeoplesometimesbecomementallyill?
Likeinotherpartsofthebody,themindcanhaveproblemsandnotworkperfectlyallthetime.
Mentalillnessesarecausedbyproblemswiththewaythemindworks,especiallywhenweare
affectedbystressesoflife.Mentalillnesscancauseproblemswiththefourtasksofthemind:
perceiving,thinking,feelingandbehaviour.
1.6 Canpeoplewithmentalillnessrecover?
Itisimportanttorememberthatallpeoplewithmentalillnesshavethepossibilityofrecovery.
Recoverydoesnotalwaysmeanthattheillnesswillbecuredcompletely.Insteaditmeansthat
thingshaveimproved,anddisabilityisreduced,inawaythatisimportanttotheindividual.In
ordertomakesureindividualshavethepossibilitytorecover,itisimportanttoalwaysfocuson
theirownneedsandwishes.

9
1.7 Whattypesofmentalillnessarethere?
There are two main groups of mental illnesses: severe mental illness and common mental
illness. Severe mental illness includes schizophrenia or psychosis. Common mental illness
includesanxiety,depressionandalcoholproblems.Severementalillnessisusuallymoreserious
anddisablingthancommonmentalillness.Individualsmayhavemorethanonethanonetype
ofmentalillness.Forexample,peoplewithschizophreniamayalsohaveanalcoholproblem.In
thismanualyouwilllearnlotsmoreaboutpeoplewithschizophrenia,andhowyoucansupport
themthroughCBR.
1.8 Howcanwerecognisementalillness?
Whenpeoplehavementalillnesstheyoftenbehaveincertainwaysthathelpsustorecognise
thattheillnessisthere.
Psychosisorschizophrenia
SomeonewhohasANYofthefollowing: Mayhave:
• Talks alone, saysmeaninglesswords or speaks in a strange language, talks
veryfast
Psychosis or
schizophreni
a or ‘severe
mental
illness’
• Isoftenveryrestless;hasmoodswingsfromveryhappyorirritabletofeeling
verysad
• Hasfalsebeliefsorsuspicions,e.g.thatsomeoneistryingtoharmthem,or
thattheyhavespecialpowers
• Showsself-neglect(e.g.dirty,untidyappearance)
• Ishearingvoicesorseeingthingsthatarenotthere
• Neglectsorhasdifficulties in carryingoutusualwork, schoolperformance,
domesticorsocialactivities
• Behavesstrangelye.g.runningoutofthehouse,runningnaked

10
Seizures
SomeonewhohasANYofthefollowing: Mayhave:
• Suddenlyfallsdownandhassharp,shakybodymovements(seizures)
Epilepsy
• Duringtheseizure,heorshe:
–losesconsciousnessordoesnotrespondnormally
–hasstiffbody,armsandlegs
–maybitetheirowntongue,injurethemselves,andwetorsoiltheirclothes
• After the seizure: the person may feel very tired, sleepy, confused, and
complainofheadache,muscleaches
Excessivesadnessorworry
SomeonewhohasANYofthefollowing: Mayhave:
• Complainsofmanyphysicalsymptomsbutnophysicalcausehasbeenfound
(e.g.headache,burningsensations,achesandpains)
Depression
oranxiety
• Haslowenergy;isalwaystired;hassleepproblemsordoesnotwanttoeat
• Alwaysseemssadoranxiousorirritable;feelshopelessorhelplessorguilty
• Haslowinterestorpleasureinactivitiesthatusedtobeenjoyable
• Worriesorthinksaboutday-to-dayproblemstoomuch
• Isnotableormotivatedtodotheirusualjob,houseworkorsocialactivities
• Hasbeenthinkingofharmingthemselves,e.g.endingtheirlife

11
Alcoholproblems
SomeonewhohasANYofthefollowing: Mayhave:
• Often appears to be affected by alcohol (e.g. smells of alcohol, looks
intoxicated,staggerswhenwalking,slurredspeech)
Alcohol use
disorder
• Becauseofalcohol,often injures themselves,e.g. fromfallingdown, fights,
orwalkingintraffic
• Has physical symptoms from excessive alcohol use (e.g. can’t sleep, very
tired,can’teat,vomits,complainsofbadstomach,diarrhoea)
• Hasfinancialdifficultiesorcrime-relatedordomesticproblems
• Has difficulties in carrying out usual work, school, domestic or social
activities;doesnotattendoroftenarriveslate
Khatproblems
SomeonewhohasANYofthefollowing: Mayhave:
• Oftenappearsdrug-affected (e.g. lowenergyor agitated, fidgeting, slurred
speech,suspicious,mayseeorhearthingsthatarenotreal)
Khatorother
druguse
disorder
• Shows signs of drug use, e.g. skin infection, unkempt appearance, burned
lips,badorwornteeth,hasdukak(unpleasantdreams)
• Hasfinancialdifficultiesorcrime-relatedlegalordomesticproblems
• Has difficulties in carrying out their usual work, school, domestic or social
activities;doesnotattendoroftenarriveslate
Problemswithforgetfulness
AnolderpersonwhohasANYofthefollowing: Mayhave:
• Can’t tell the timeofday,or forgetswhere theyare, forgets thenamesof
objectsormaynotrecognisefamiliarpeople
Dementia
• Getslostwhenoutsidethehome
• Hasdifficultorembarrassingbehaviour
• Oftenlosesemotionalcontrol,iseasilyupset,irritableortearful
• Lackofattentiontopersonalhygiene,incontinence
• Hasdifficultiesincarryingouttheirusualwork,domesticorsocialactivities
12
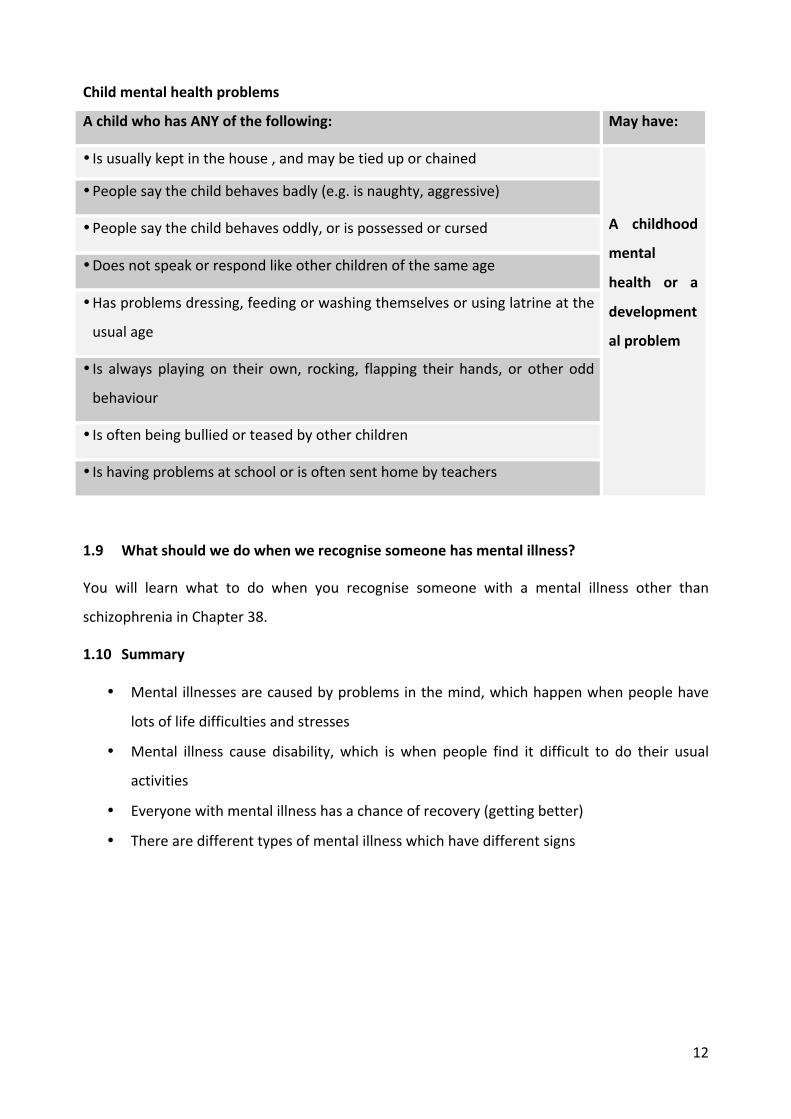
Childmentalhealthproblems
AchildwhohasANYofthefollowing: Mayhave:
• Isusuallykeptinthehouse,andmaybetieduporchained
A childhood
mental
health or a
development
alproblem
• Peoplesaythechildbehavesbadly(e.g.isnaughty,aggressive)
• Peoplesaythechildbehavesoddly,orispossessedorcursed
• Doesnotspeakorrespondlikeotherchildrenofthesameage
• Hasproblemsdressing,feedingorwashingthemselvesorusinglatrineatthe
usualage
• Is always playing on their own, rocking, flapping their hands, or other odd
behaviour
• Isoftenbeingbulliedorteasedbyotherchildren
• Ishavingproblemsatschoolorisoftensenthomebyteachers
1.9 Whatshouldwedowhenwerecognisesomeonehasmentalillness?
You will learn what to do when you recognise someone with a mental illness other than
schizophreniainChapter38.
1.10 Summary
• Mental illnessesarecausedbyproblemsinthemind,whichhappenwhenpeoplehave
lotsoflifedifficultiesandstresses
• Mental illness cause disability, which iswhen people find it difficult to do their usual
activities
• Everyonewithmentalillnesshasachanceofrecovery(gettingbetter)
• Therearedifferenttypesofmentalillnesswhichhavedifferentsigns

13
2 Whatisschizophrenia?
2.1 Whatkindofillnessisschizophrenia?
Schizophreniaisatypeofmentalillness.Peoplewithschizophreniahaveproblemswiththeway
theirmindworksinthefollowingareas:
• Perceiving:Topeoplewithschizophreniathingsthatarenotrealmightseemasifthey
arereal
• Thinking: People with schizophrenia have confused or strange thinking. They believe
thingsthatarenottrue.
• Feeling: People with schizophrenia have fewer emotions or stronger emotions than
usual
• Behaviour:Peoplewithschizophreniamaybehaveinastrangeway.
2.2 Whatarethesymptomsofschizophrenia?
Therearefourgroupsofsymptomsofschizophrenia.
1. Hallucinationsanddelusions
Hallucinationsarewhenapersonexperiencessomethingthatisnotreallyhappening.Theymay
hearsoundsthatarenotreallythere, forexampleavoicetellingthemtodosomething.They
mayseethings,feelthingsorsmellthingsthatarenotreallythere.
Delusionsarewhenapersonbelievessomethingthatisnotreallytrue.Forexample,theymay
believethattheyhavespecialpowers.Ortheymaybelievethatpeoplearetryingtopoisontheir
food.
Hallucinationsanddelusionsmaymakepeoplebehaveinastrangeway.Forexample,theymay
talktothemselves,saymeaninglesswords,speakinastrangelanguageorspeakveryfast.They
mayalsohavemoodswings,fromveryhappyorirritabletofeelingverysad.
2. Problemswithmotivation
Peoplewith schizophrenia often have low levels ofmotivation. They often do things slower,
includingthinking,talkingandmoving.Theymayfeeltheyhavenoenergytodoanything.They
maynotbotherwashingordressingproperly. Theymaynotbe interested in talking toother
people.Theymaynotshowanyemotions.

14
3. Problemswiththinkingclearly
Peoplewithschizophreniaoftenhaveproblemsconcentratingonatask,orrememberingthings.
Thismeansitisdifficulttofollowaconversationordohouseholdtaskssuchascooking.
4. Lackofawarenessofillness
Oftenpeoplewithschizophreniadounderstandorbelievethattheyareunwell.Theymaynot
realisethattheyarebehavingstrangely.
2.3 Whatcausesschizophrenia?
There is not one thing that causes schizophrenia and you cannot catch schizophrenia from
someone else. Schizophrenia is usually caused by a combination of vulnerability and life
stress.Protectivefactorscanstopschizophrenia fromdevelopingorgettingworseevenwhen
vulnerabilityandlifestressarethere.Wedon’talwaysknowwhyapersongetsschizophrenia.
Vulnerability
Vulnerabilitymeansthingsthathappenbeforeapersonisbornorearlyinlife.Itincludes:
Yosef’sstory
Yosef isa24yearoldmanwho lives ina ruralkebelewithhismother,Addis, father,Solomon
andyounger siblings.About fiveyearsagohewasworkinghardonhis family’s farm.He had
friendsinvillagewhohewenttothealcoholshopswith,ordrankcoffee.Hewasn’twealthybut
wasseenassuccessfulinthekebele.Healwayswenttothekebelemeetingsandcontributedto
Edir.Hismotherhopedhewouldgetmarriedsoon.
AboutfiveyearsagoYosefbegantobehaveinastrangeway.Peopleinthekebelenoticedthat
he talked to himself and laughed to himself. He confided in hismother that SaintMarywas
communicatingwithhimandtoldhimthathehadtodospecialtasks.Sometimesheranaway
forseveraldays.Hebegantobelievethattheneighbourshatedhimandweretryingtoruinhis
crops.Sometimesheshoutedattheneighboursandthreatenedthem.
Astimehasgoneon,hehasstoppedtalkingabouthisstrangebeliefsmostofthetimeandheno
longerrunsaway.Butheisstillnotbacktohisusualself.Hehasstoppedworkingonthefarm
andspendsthedaysbyhimself.Hestoppedwashinganddressingproperly.Thingsdon’tseemto
be improving for Yosef. Every fewmonths he becomes much more unwell again. When this
happensheseemstobeverydistressedandshoutsattheneighboursagain.

15
• Aperson’smotherhavingproblemsduringherpregnancy,forexampleaninfection.
• Havingadifficultbirthduringwhichthebabyisinjured.
• Havingaheadinjury.
• Usingkhatfromanearlyage.
• Beingabusedduringchildhood.
• Whensomeonehasschizophreniainthefamilymostofthefamilymemberswillnotdevelop
schizophrenia,butthereismorechanceofithappening.
Lifestress
Lifestressmeanseventsorcircumstancesinaperson’slifethatputalotofpressureonthem.
Theymightleadthemtofeelangry,anxiousorsad.Thesemightinclude:
• Beingdisappointedaboutabigthing.Forexample,arelationshiporinwork.
• Movingtoanareawheretheydon’tknowanyone
• Familyconflict
• Illness
• Bereavement
• Havingchildren
Noneofthesethingsalonemeanthatapersonwillgetschizophrenia.Itonlyhappenswhen
thepersonhasatleastonetypeofvulnerabilityandatleastonetypeoflifestress.
Preventativefactors
Preventativefactorsarethingsthathelptostopapersonbecomingunwellwithschizophrenia,
orstopitfromgettingworse.Theyinclude:
• Goodsocialsupport
• Goodcopingstrategies
• Regularanti-psychoticmedication
Yosef’sstory
Yosef’sfamilybelievethathisproblemsareduetobeingpossessedbyspirits.Hisproblems
allseemedtostartwhenhebecameverydisappointedthathedidnotmarrythewomanhe
expected to. In the years before Yosef’s problems started life had been stressful for the
family.Someofhisyoungersiblingshaddiedandtherehadbeenapoorharvestafewyears
inarow.

16
2.4 Whatbeliefsdopeoplehaveaboutschizophrenia?
Peoplewithschizophrenia,theirfamiliesandotherpeopleinthecommunitymayhavebeliefs
about what causes schizophrenia which are different from the explanation given here. In
Ethiopiathemostcommonbeliefsarethatschizophreniaiscausedbyspiritpossession,evileye
orpossessionbythedevil.Thesamepersonmayevenhavelotsofdifferentideasaboutwhat
causes it. Having different beliefs is not always a bad thing by itself. Having different beliefs
becomesaproblemwhenitresultsin:
• Peoplewithschizophrenianotgettingtreatmentthatworks,forexamplenotbeingtakento
thehealthcentreorhospitaltogetmedication
• Peoplewith schizophrenia being treated badly, for example being beaten to exorcise the
devil
2.5 Howlongdoesschizophrenialast?
Schizophreniacaneitherlastashorttime(evenoneepisode),butusuallylastslonger,evenfor
manyyears.Therearetwomainwaysthatpeoplecanbeaffectedtoschizophrenia:
• Short-term,moresevereillness:Duringthisphasethepersoncanbeverydisturbed.They
oftenhaveproblemswithhallucinationsanddelusions.Thismayleadthepersontobehave
strangely.Theymayspeakandthinkinastrangeway,andmaybecomeangry.It isusually
duringthisphasethatthefamilyofthepersontryandgethelp,forexamplebygoingtoholy
waterorthehospital.Theacutephaseusuallylastsfromweekstomonths.
• Long-term,established illness:Duringthisphasethepersonmaystopbehavingstrangely,
but they still have problems with motivation and with thinking clearly. They may have
problemswithdoingusualactivities,suchasgettingdressedordoingfarmwork.Theymay
finditdifficulttotalktootherpeopleorsocialise.Thisphasecanlastformonths,yearsor
canbelife-long.
Mostpeoplewithschizophreniahaveashort-term,moresevereillnessatthebeginning.What
happensnextvariesalotfrompersontoperson.
• A fewpeopledonot have anymore severe illness. Theymayormaynot have some less
severeillness.
• Mostpeoplewithschizophreniahave repeatedepisodesofmoresevere illness.Theseare
knownasrelapses.Inbetweentheyusuallyhavesomelesssevereillness.
• Afewpeoplestayunwellwithmoresevereillnessallthetime

17
2.6 Canpeoplerecoverfromschizophrenia?
The important thing to remember is that everyone with schizophrenia has a chance to get
betterandtorecover.Evenifanindividualdoesnotgetridofalltheirsymptoms,theyhavea
goodchanceofgettingback to theirnormalactivities.Recovery canmeandifferent things to
differentpeople.Itdoesn’tusuallymeanthatanindividualis‘cured’ofschizophrenia.Insteadit
means that things have improved in a way that is important to that person. Getting lots of
support,takingmedicationandnotusingalcoholorkhatmakeitmorelikelythiswillhappen.
Evenifapersonwithschizophrenia isfeelingmuchbetter,theymaysuddenlybecomeunwell
againwitha relapse.Relapsesmayhappendue tonot takingmedication,physical illness, life
stress or for no particular reason. The signs that a relapse is coming include problems with
sleep,beingisolatedfrompeople,beingangryoranxiousandstoppingmedication.InChapter
30youwilllearnhowtopreventandmanagerelapses.Havingarelapsedoesn’tmeantheywill
be unwell forever and it is important for the individual and family not to give up hope that
thingswillimprove.
2.7 Howisschizophreniadiagnosed?
There is no test for schizophrenia. The doctor or nurse decides whether someone has
schizophreniaornotbylisteningtotheirproblemsandhowlongtheyhavelasted.
2.8 Howcommonisschizophrenia?
Schizophreniaisnotaverycommondisease.Inakebeleof5000people,theremightbearound
10peoplewithsevereschizophrenia.
2.9 Howdowegiveinformationaboutschizophrenia?
YouwilllearnhowtogiveinformationaboutschizophreniainChapter16.
2.10 Summary
• People with schizophrenia have hallucinations, delusions, problems with motivation,
problemswiththinkingclearly,andusuallydonotunderstandthattheyareunwell
• Schizophreniaiscausedbyacombinationofvulnerability(earlyevents)andlifestress
• Peoplewithschizophreniacanhaveperiodsofshortterm,severeillnessandlong-termless
severeillness
• Allpeoplewithschizophreniahavethechanceofrecovery(gettingbacktousualactivities)
• Schizophreniaisnotverycommon

18
3 Medicationforschizophrenia
3.1 Whatisanti-psychoticmedication?
Takingregularanti-psychoticmedication isan importantpartof treatment forallpeoplewith
schizophrenia.
3.2 Whyisitimportanttotakeanti-psychoticmedication?
Taking anti-psychotic medication may improve the chances of recovery. Anti-psychotic
medicationisgoodatreducingthefollowingsymptomsofschizophrenia:
• Hallucinations(seeingorhearingthingsthataren’treallythere)
• Delusions(believingthingsthataren’ttrue)
Anti-psychoticmedicationislesshelpfulforthefollowingsymptomsofschizophrenia:
• Problemswithmotivation,includingshowingemotions
• Problemswiththinkingclearly,includingconcentratingandbeingorganised
3.3 Whenisanti-psychoticmedicationneeded?
• Whenapersonwithschizophreniaisunwell,anti-psychoticmedicationisneededtoreduce
thesymptoms
• Evenwhenthepersonhasbecomebetterandhasnosymptoms,medicationisstillneeded
topreventrelapse(i.e.preventthepersonbecomingunwellagain).
• Antipsychoticmedicationworksbestwhentakenregularlybutitcanbedifficultforpatients
tokeeptakingmedication.
3.4 Whattypesofanti-psychoticmedicationarethere?
Anti-psychoticmedicationsareavailable in tabletand injection forms (seeTable1). Injections
arenormallygivenwhenthepersonwithschizophreniahasdifficultyrememberingtotaketheir
tablets or has experienced lots of relapses (when the severe illness comes back).

19
Table1Medicationsforschizophrenia
Nameofmedication Brandname Typeofdrug How often it should betaken
Haloperidol Haloperidol Tablet OnceortwiceadayChlorpromazine CPZ Tablet OnceortwiceadayFluphenazine Modecate Injection Fortnightlytomonthly
3.5 Whatsideeffectsdoanti-psychoticmedicationshave?
Medicationcansometimescauseproblems(sideeffects)aswellashelp(SeeTable2).Theside-
effects fromanti-psychoticmedication are common so it is important that you knowhow to
recognise them.Despite these problems, formanypeople their quality of life is betterwhen
takingthemedicationcomparedtowhennottakingit.
Table2Sideeffectsofanti-psychoticmedications
CommonThepersonfeelsrestlessandcannotsitstillThehead,neckorbodybecomesstuckinanunusualpositionbecauseofmusclestiffnessThehandsshakeThepersonmovesveryslowlyThepersonissleepyduringthedayThemouthisdryAlotofsalivaisproducedConstipationThepersonfeelsdizzywhentheystanduptooquicklyfromlyingdownorsitting.ThepersonwantstoeatmorethanusualUnusualmovementsofthehead,neck,armsorlegsLesscommonSeizuresSuddenlydevelopingstiffmuscles,fever,andconfusionSexualproblemsSkinrashThepersoncannotpassurine
3.6 Canpregnantandbreastfeedingwomentakeanti-psychoticmedication?
Dependingonthewoman,pregnantandbreastfeedingwomenmayneedtostoporreduceanti-
psychoticmedication.

20
3.7 Howdowehelppeoplewithschizophreniatotaketheirmedication?
You will learn how to help people with schizophrenia to take their medication regularly in
Chapter20,includinghowyoucanhelpwithsideeffects.
3.8 Summary
• Anti-psychoticmedicationisoftenneededtohelppeoplewithschizophreniatorecover
• Itisimportanttotakemedicationwhentheindividualisunwell,andtocarryontakingthe
medicationwhentheindividualiswell(tostoptheillnesscomingback)
• Anti-psychoticmedicationcanbegivenintabletsorinjections
• Anti-psychoticmedicationcancauseside-effects
Yosef’sstory
Afterseveralyearsofbeingunwell,Yosef’sparentstookhimtothe localhealthcentreasthey
hadheardhemightbeabletogethelpthere.Hereanursediagnosedhimwithschizophrenia.
The nurse gave him anti-psychotic medication, called haloperidol. He was told to take the
medicationtwiceaday.YoseffoundthattakingthemedicationstoppedthevoiceofSaintMary
inhishead.Hisparentsnoticedthathestoppedshoutingattheneighboursandrunningaway.
HoweverthemedicationalsogaveYosefsomeproblems.Heisoftenverytiredanddrowsyand
hishandsoftenshake.Thesethingsmakeithardtodofarmwork.

21
4 Disabilitiesrelatedtoschizophrenia
4.1 Whatisdisability?
Disabilityiswhenapersoncannotdotheactivitiesthatwewouldnormallyexpectthemtodo,
giventheirageandsocialcircumstances.Disabilitycaninclude:
• Problemswiththebody,forexampleblindness
• Problemswithdoingphysicalactivities,forexamplewalking
• Problemsdoingusualworkandsocialactivities,forexamplegoingtomarket.
4.2 Whatcausesdisabilities?
Disabilitiesinpeoplewithschizophreniaarecausedbyacombinationofthesocialenvironment
inwhichthepersonlivesandtheillnessitself.Forexample,
• An individual may not be allowed to vote at the kebele meeting because of stigma and
discriminationinthecommunity(seeChapter6).
• Apersonwhodoesn’thaveanyfamilymaynotworkbecausetheyarenotbeingencouraged
todoso.
• Problemswithself-caremayresultfromlackofmotivation,asymptomoftheillness.
4.3 Whatlimitationsdopeoplewithschizophreniahave?
Peoplewithschizophreniausuallyexperiencemanytypesofdisability.Theseinclude:
1. Problemswithself-care
Thisincludesproblemswithwashing,dressing,brushinghairandeatingattherighttime.
2. Problemsdoinghouseholdtasks
Thisincludesproblemswithcooking,washingclothes,choppingwoodorfetchingwater.
3. Problemswithsocialinteractionsandparticipatingincommunitylife
Thisincludesproblemswithhavingconversationswithpeopleandproblemsattendingchurch,
funeralsorEdirmeetings.
4. Problemsinworking
Thisincludesproblemsdoingfarmwork,tradingorbusiness.
5. Problemsinlookingafterchildren
Thisincludesproblemsgivingchildrenlove,feedingandclothingthem.
6. Problemswithmaritalrelationships
Thisincludesnotgettingonwellandarguingalot.

22
4.4 Whatistheimpactofhavingdisabilities?
Disabilitymaybemoreupsettingtotheindividualthanthesymptomsthemselves.Forexample,
finding it difficult to drink coffee with others may be more distressing than simply hearing
voices.Disabilitiesmayresultinproblemswithmoney.Forexample,havingproblemswithfarm
workislikelytomeantheindividualhaslessmoney.Disabilitiesmayalsohaveabigimpacton
therestofthefamily.Forexampleifamotherwithschizophreniafindsitdifficulttolookafter
her children, other familymembersmay need to help out. These familymembersmay then
havetroublelookingaftertheirownfarmproperly(seeChapter5).
4.5 Howdoweassessdisabilities?
Youwilllearnhowtoassesswhatkindsofdisabilitiespeoplewithschizophreniahaveaspartof
theNeedsAssessment(seeChapter12).
4.6 Howdoweworkwithindividualstoimprovetheirsituation?
Theaimofrehabilitationistoworkwithindividualstoimprovetheirsituationsotheyareless
disabled and can get back to their usual activities. Rehabilitation should be an empowering
process. This means the needs and wishes of the individual are at the centre of the work.
Rehabilitation isn’tabout ‘doingthings’ toor forpeoplewhoaredisabled. It isaboutworking
togethertoimprovetheir lifeandworktowardsrecovery.Recoverycanmeandifferentthings
to different people. It doesn’t usually mean that an individual is ‘cured’ of schizophrenia.
Insteaditmeansthatthingshaveimprovedinawaythatisimportanttothatperson.Youwill
seethatallofCBRisfocusedtowardsrehabilitation.
4.7 Summary
• Disabilityiswhenanindividualcannotdotheactivitieswewouldnormallyexpect
• Disabilityiscausedbyacombinationofthesocialenvironmentandtheillness
• Peoplewithschizophreniacanhaveproblemswith:self-care,householdtasks,participating
incommunitylife,working,lookingafterchildrenandmaritalrelationships
• Rehabilitation involves work with the individual to reduce disability.
Yosef’sstory
Yosefdoesnotoftenwashordresshimself.Heno longerhelpsonthefamily’s farm.Hedoes
notcontributetoEdiranymore,insteadhereliesonhisparent’scontributions.Hedoesn’thave
anyfriendsanymoreanddoesnotgotoChurch.

23
5 Impactofschizophreniaonthefamily
Aswellashavingabigimpactontheindividual,whenapersonhasschizophreniaitalsohasa
bigeffectonthewholefamily.Thisisbecausethefamilyareusuallytheirmaincarers.Theseare
someoftheeffectstheillnesscanhaveonthefamily.
5.1 Comingtotermswiththeillness
Notmanyfamilies immediatelyknoworbelievethattheirrelativehasamentalillness.When
the individual is very unwell, the family members may be scared by what is happening.
When the episode is over, everyone wants to forget this painful time and focus on the
future.Familiesmayalsolookforotheranswers,hopingthatthesymptomswerecausedbya
physicalproblem orstressfuleventsthatcanberemoved.
5.2 Stigmaanddiscrimination
Even when families knowthattheirrelativehasamental illness, theymay notwant to talk
with others about it, because they fear other people’s reactionsormightbeembarrassed.
Otherpeople in thecommunitymay suggest that there is somethingwrongwith the family to
cause the illness.The family may notwant to invite anyone to the home.Or theymaybe
anxious about leaving the individual athome alone.Peoplewithschizophreniaoftenfindit
difficult togetmarried.This issometimesbecauseof thestigmatowardsthem,whichmay
continueeveniftheybecomewell.Thisputsanextraburdenontheparents.SeeChapterfor
moreaboutstigmaanddiscrimination.
5.3 Heavyresponsibilityofcaring
Familymembersmayspendalotoftheirtimelookingafterthepersonwithschizophrenia.Itis
often female caregivers, either the individual’s mother or wife, who take on most of the
responsibilities. Their household routine may be disrupted and it may be difficult to attend
social gatherings such as weddings. Sometimes caregivers, for example brothers and sisters,
evendecidenottomarrysothattheycantakecareofapersonwithschizophrenia.Intheend
thefamilymaybecomeisolatedfromthecommunity.Somefamiliesmayfeeltheydonotget
enoughsupport fromwider familymembersandthecommunity.Familiesmaybeconcerned
that the individual will run away, harm their neighbours’ property, or other people or get
hurtthemselves.Thismaymeanthat,asa lastresort,familieschainortieuptheindividual

24
toprotectthemandotherpeople.Alloftheseissuesmeanthefamilymembersoftenbecome
stressed,fullofworryandexhausted.
5.4 Economicimpact
People with schizophrenia usually need to take medication everyday for many months or
years.Thecostofthis,alongwiththecostofseeinganurseordoctor,andcostoftransportto
thehealthcentreorhospital,meansthefamilyhastospendalotofmoneyontheindividual.
The person with schizophreniamay find it difficult to do their own farmwork, day to day
labouringorbusiness.Thismeansthattheotherfamilymembershavemoreworktodo,and,
theremaybelessmoneycomingintothefamily.Alsothefamilymembersmaybeabletodo
lessworkthemselves,becausetheyarecarers.
5.5 Familyconflict
Family members may not understand the illness and blame the individual for their bad
behaviourandfornotworking.Theymaybecomefrustratedandangrythattheindividualisnot
gettingbetter.Conflictinfamiliestendstomakeschizophreniaworse,anditisimportanttotry
toreducethis.Theindividualthemselvesmayfeelbadaboutallthemoneyspentbythefamily
ontreatment.
5.6 Howdowehelpthefamiliesofpeoplewithschizophrenia?
The whole of CBR aims to improve the situation of families, by helping individuals with
schizophreniagetbacktotheirusualactivities.Inparticular,youwilllearnhowtoimprovethe
familyenvironmentinChapter25.
Yosef’sstory
ThelivingconditionofYosef’swholefamilyhasgotworsebecauseYosefcannotwork.Addisis
oftenscaredtoleaveYosefaloneincaseherunsawayagain.Thismakesitdifficultforhertodo
herusualwork likegoing tomarket.Hisparents can’tgo to funeralsorweddingsunlesshe is
asleep.TheydonothaveanyvisitorsatthehousebecausetheyareashamedofYosef.Theyfeel
thatnobody in the community helps them. Sometimes thewhole family has argumentsabout
Yosef.Theyargueaboutwhyheisnotgettinganybetter.

25
5.7 Summary
• Theremaybeextracosts tothefamilyofapersonwithschizophreniaandtheymayhave
problemsdoingusualactivities
• Thefamilymayexperiencestigma
• Theremaybeconflictwithinthefamily
26
6 Stigmaanddiscrimination
6.1 Whatisstigma?
Stigmaiswhenpeopleautomaticallythinkbadthingsaboutapersonjustbecausetheyhavea
mental illness.Stigma fromotherpeople towardspeoplewithschizophreniaconsistsof three
problems.
• Theproblemofknowledge.Thisiscalledignorance.
• Theproblemofattitudes.Thisiscalledprejudice.
• Theproblemofbehaviour.Thisiscalleddiscrimination.
All these types of stigma can be found in familymembers, communitymembers and health
workers.Stigmafromthepersonwithschizophreniatowardshimorherself,becausetheystart
to believe the negative things that other people say, is called self-stigma. Stigma and
discriminationisalsoexperiencedbyotherpeople,forexamplepeoplewithphysicaldisabilities,
albinism,HIVorepilepsy.
6.2 Whattypesofstigmadopeoplewithschizophreniaexperience?
Ignorance
Mostpeopleinthecommunityandsomehealthworkersdonothaveagoodunderstandingof
schizophrenia.Thismeanstheycanhavesomeofthefollowingfalsebeliefs:
• Nobodyrecoversfromschizophrenia
• Thereisnotreatmentforschizophrenia
• Peoplewithschizophreniaareviolentanddangerous
• Peoplewithschizophreniaarelazyandyoucannottrustthem
• Schizophreniaistheresultofspiritpossession
• Schizophreniaistheresultofaweakcharacter
• Everythingpeoplewithschizophreniasayisnonsense
• Peoplewithschizophreniacannotmakedecisionsabouttheirownlives
Prejudice
Prejudice is when people feel emotions such as anxiety, anger, hostility or disgust towards
peoplewithschizophrenia,aswellashavingignorantthoughts.Forexample,aneighbourmay
feelscaredwhilsttalkingtoapersonwithschizophrenia,evenifthepersonisnotactinginan
aggressiveway.

27
Discrimination
Discrimination iswhenpeoplebehavedifferently towardspeoplewithschizophrenia,because
oftheirignoranceandprejudice.Thiscanmeanthatindividualsarenotabletodotheactivities
that they used to when they were well. People with schizophrenia may continue to be
discriminatedagainsteven though theyhave recovered.Theyoften feel thatdiscrimination is
moredistressingthanthesymptomsoftheillness.
Herearesomeexamplesofdiscriminationwhichpeoplewithschizophreniaexperience:
• Communitymembersdonotgreettheindividualintheneighbourhood
• Communitymemberscalltheindividualrudenames,laughorgossipaboutthem
• Friendsdonotwanttotalkordrinkcoffeewiththeindividual
• Community members do not listen to the individual when they try to contribute at
communitymeetings,suchaskebelemeetingsoredirmeetings
• The individual cannot get a job or cannot be involved in a microfinance group because
employersorgroupmembersthinktheyarelazyandunreliable
• Theindividualfindsitdifficulttogetmarried
• Thefamilyaskstheindividualtohidewhenrelativesvisitthehouse
• Familymembersmaytieupthepersonwithschizophrenia.Thisisusuallydonebecausethe
person is veryunwell and the family cannot control them.However sometimes it is done
becausethefamilybelievestheindividualispossessedbyspiritsorthedevil.
Self-stigma
Somepeoplewithschizophreniastarttobelievethenegativeattitudesthatothershavetowards
them.Thiscanresultin:
• Lowself-esteem
• Feelingcriticaltowardsthemselves
• Feelinghopeless
• Depression
• Beingisolated
Peoplewithschizophreniamaystopthemselvesdoingactivitiesbecausetheyexpectpeopleto
berudetothem,laughatthem,ortreatthemdifferently.
28
6.3 Whattypesofstigmadofamiliesexperience?
Thefamilymembersofpeoplewithschizophreniacommonlyexperiencestigmatoo.Thewhole
familymaybetreatedwithlessrespectorpeoplemayavoidthem.Theymayalsobeblamedfor
theillnessintheindividual.
6.4 Howdowereduceexperiencesofstigma?
YouwilllearnhowCBRcanreduceexperiencesofstigmaanddiscriminationinChapter28.
6.5 Summary
• Stigma includes problems of knowledge (ignorance), attitudes (prejudice) and behaviour
(discrimination).
• Manypeoplewithschizophrenia,andalsotheirfamilies,experiencestigma
• Experiencesofstigmamayinclude:beinglaughedatorcallednames,beingexcludedfrom
communityactivitiesorwork,andbeingkepthiddenortiedup
Yosef’sstory
Sometimes people laugh and gossip about Yosef when he goes outside. Sometimes children
throwstonesathim.Yosefdoesn’thaveany friends anymore.His family doesn’t thinkhewill
evergetmarriednowhehasbecome ill.Oncewhenhewasfeelingbetterhewenttoakebele
meetingandtried toadd to thediscussion.Theotherpeopletheredidn’t sayanythingbadto
him,buttheyignoredhim.ThismadeYoseffeelbadandhedidn’tgothemeetingagain.Hehas
startedtobelieveotherpeopleandthinksheisworthless.
29
7 Humanrights
7.1 Whatarehumanrights?
Theterm‘humanrights’describesthebeliefthatallpeoplehavebasicrights,includingtheright
tolife,freedomofspeech,beliefandfreedomfromfear.TheEthiopianconstitutionstatesthat
humanrightsandfreedomareinourhumannature(Ethiopianconstitution,chapter10,No1).
Allpeoplehavehumanrights,regardlessofage,sex,ethnicityorreligion.Theserightsenablea
person to live their lifewithworthanddignity. TheEthiopianConstitution states thathuman
rightsshouldnotbeviolated.
7.2 Whathumanrightsdopeoplewithmentalillnesshave?
PeoplewithmentalhealthproblemshaveequalrightslikeanyotherEthiopiancitizen;theyhave
the sameneed for respectandcare.The following rightsapply topeoplewithmental illness,
justlikeallotherpeople:
• Theyshouldnotbechained,suffer,orbelockedupathomebecauseoftheirillness
• Theyshouldnotbeheldbypolicejustbecausetheyareill
• Theyhavetherighttohaveafamilyoftheirown,getmarriedandhavechildren;
• Theyhavetherighttowork
• Theyhavebasicrightsforfood,clothing,housingandmedicalservices;theyshouldnotbe
lefttostarve,orbehomeless.
• Theyshouldnotbeabused,disrespectedorcalledbadnames,orbeaten todriveoutbad
sprits.
Itisquitecommonforpeoplewithmentalillnesstobedeniedtheirhumanrights.
7.3 Howdowedealwithhumanrightsproblemsinpeoplewithschizophrenia?
InChapter19youwilllearnhowtohelpprotectthehumanrightsofindividuals.
Yosef’sstory
WhenYosefbecomesveryunwellhisparentssometimeschainhimtothewalloftheirhouse.
Theydothisbecausetheyareworriedhewill runawayandhurtsomeone,orgeteatenby
hyenasordrownintheriver.

30
7.4 Summary
• All peoplehave the sameHuman rights including the right to life, freedomof speech,
beliefandfreedomfromfear.
• Itisquitecommonforpeoplewithschizophreniatobedeniedtheirhumanrights
31
8 Theimportanceofthecommunity
8.1 Whatisthecommunity?
Everybodyliveswithinacommunityofsomekind.Whenwesaycommunitywemean:
• Agroupofpeoplelivinginthesameplace,forexamplethekebele
• Afeelingofsharedattitudesandinterests
Forpeoplewithschizophreniatheircommunitymightinclude:
• Theirfriends,neighboursandrelatives
• Communitymembersthatliveinthesamekebele,eveniftheydonotknowthem
• Communityleaderssuchaskebeleleaders,priestsortheheadteacher
Therearemanycommunityresourcesineverykebele.Theseinclude:
• Churchesandmosques,includingpriests
• Edirgroups
• Religiousgroupssuchasmahaber,tsewaandlika
• Primaryschool
• Women’sAssociationsandYouthAssociations
• Kebeleadministration
• Markets
• Traditionalhealers,forexampletanqwayorherbalists,andholywatersitesandholywater
priests
8.2 Whatproblemsdopeoplewithschizophreniahaveincommunitylife?
Peoplewith schizophreniaoften find theyhaveproblemsaccessing the community resources
anddoingtheirusualcommunityactivities(seeChapter26).Thesemightinclude:
• Notsocialisingwithfriendsandneighbours,forexampledrinkingcoffee
• Notattendingchurchormosque
• Notparticipatinginreligiousgroupssuchasmahaber
• NotparticipatinginEdir
• Not attending community groups such as the Women’s or Youth Association

32
8.3 Whatroledoesthecommunityhaveinthelifeofthepersonwithschizophrenia?
Positiveinfluences
Thecommunitycanhaveapositiveorsupportive influenceonthepersonwithschizophrenia,
suchas:
• Makingtheindividualfeelwelcomewhentheyparticipateincommunityactivities
• Helpingtheindividualandfamilywithfoodorotherpracticalsupportwhentheyarehaving
aparticularlydifficulttime
• Givingemotionalsupporttothefamily,forexamplelisteningtotheirproblems
• Organisingcommunityactivitiesthatthepersonwithschizophreniamaywishtobepartof.
Thisincludesgovernmentschemes,suchasadultliteracygroups,andlocalgroups,suchas
Edir.
• Helpingthefamilyintransportingtheindividualtothehealthcentreorhospital
Negativeinfluences
The community can also have a negative influence on the person with schizophrenia. The
community may make it even more difficult for the individual to participate in their usual
activities.Thisisusuallyduetostigmaanddiscrimination.SeeChapter6formoredetail.
8.4 WhatistheroleofthecommunityinCBR?
CBR aims to increase the positive influences of the community, and reduce the negative
influences. Italsoaimstohelppeoplewithschizophreniatoaccessthecommunityresources.
Thecommunityalsohasanimportantroleinmakingsurethepositivechangesthathavebeen
madeduringCBRarecontinuedaftertheCBRworkerhasleft(seeChapter31).Thecommunity
alsobenefits throughCBR.Once the individual isback todoing theirusualactivities, theyare
likelytobeamoreproductiveandactivecommunitymember.
8.5 Summary
• Peoplewithschizophreniaoftenhaveproblemstakingpartincommunitylife
• Thecommunitycanhaveapositiveornegativeinfluenceonthepersonwithschizophrenia
Yosef’sstory
Yosefusedtobeanactivememberofhiskebele.Thekebelechairpersonthinksthecommunity
hasbeenaffectedbyhisillness,andifYosefcouldgetbetterthecommunitywouldbenefit.

33
• TheaimofCBRistoincreasethepositiveinfluencesandreducethenegativeinfluencesof
thecommunity.
• CBR helps individuals to become more productive and active, so the community also
benefits

34
SECTIONB:Learnhowtohelppeoplewith
schizophreniaandtheirfamiliesthroughCBR
RISE
35
9 OverviewofCBRdelivery
9.1 Whatiscommunity-basedrehabilitation?
Community-basedrehabilitation isawaytohelppeoplewithdisabilitiestobe included inthe
lifeoftheircommunities.Itaimstoimprovethequalityofallareasofaperson’slife.Thefocus
isalwayson theneedsandwishesof the individual.CBRbenefits the family,by reducing the
burdenuponthem.Italsobenefitsthewholecommunity,byhelpingtheindividualtobeamore
activeandproductivecommunitymember.Sometimes ittakesa longtimetoseethepositive
impactsofCBR,soitisimportantthateveryoneinvolvedispatientandstayspositive.
9.2 WhataretheprinciplesofCBR?
1. Useaholisticapproach
CBRaddressesallaspectsoftheperson’slifeincluding:
• Social
• Livelihood
• Health
• Education
• Empowerment(aperson’sabilitytomakedecisionabouttheirownlife)
TheseareallareaswheretheindividualmightbehavingproblemsandwhereCBRcanmakea
positivechange.
2. Workwiththefamilyandthecommunity.
Thefamilyarethemaincarersforpeoplewithschizophreniaandtheaimistohandovercareto
family at the end of your involvement. The community also has an important role in the
individual’slife.Workingwiththecommunityisrequiredtomaximisetheimpactofthefamily
workandtoensurethepositiveimpactofCBRstaysafteryouhavegone.
3. Encouragerespectforhumanrights
AllofCBR,whetherworkwith the individual, familyorcommunity, shouldencourage respect
for the human rights of the individual. Treating people with schizophrenia with dignity and
respectisempoweringandwillmakeitmorelikelytheywillgetbacktotheirusualactivities.
4. Linktoexistingservices
Where possible, should involve linking the individual to existing services, for example the
governmentrunadultliteracyscheme.
36
9.3 WhoisinvolvedinCBR?
Thepersonwithschizophrenia
Thepersonwith schizophrenia should alwaysbe at the centreofCBR.By always focusingon
theirconcerns,needsandwishesyouwillbemorelikelytohelpthemtorecoverinawaythatis
importanttothem.Inthismanualwewillusuallyrefertothepersonwithschizophreniaas‘the
individual’.
Primarycaregiver
Theprimarycaregiver is themainpersonwho looksafter thepersonwithschizophrenia.This
maybeaspouse,parent,siblingorotherrelative.Veryoccasionallytheprimarycaregivermay
beaneighbour,friendorothercommunitymember.Theprimarycaregivershouldbeyourmain
pointofcontactwithinthefamily.Theyshouldalsobepresentatallhomevisits.Theywillhave
beenidentifiedbeforeyoustarttheCBR.
Otherfamilymembers
At your first visit you should find out which othermembers are involved in the care of the
person with schizophrenia. This may include a spouse, parent, sibling, child or grandparent.
Dependingontheindividualcircumstances,otherfamilymembersmaybeinvolvedinmanyof
thehomevisitsoronlyafew.Themanualwilltellyouwhenit isparticularlyusefultoinvolve
other familymembers. In thismanualwewill often refer to theprimary caregiver andother
familymembersas‘thefamily’.
You,theCBRworker
Youwillarrangeandleadallthehomevisitstothefamilyanddoallofthecommunitywork.
Yoursupervisor
Youwillbesupportedbyyoursupervisor.Yoursupervisorwillcomewithyouatcertainhome
visits,forexamplefortheneedsassessmentandgoalsetting.Youwillalsomeetregularlywith
themtodiscusstheprogressofeachindividual(seeChapter34).
HealthCentrestaff
Youwillbelinkedtoonehealthcentre,whereallthepeoplewithschizophreniayouareworking
withwillreceivetheirmedicalcare.Youwillneedtogowiththeindividualtothehealthcentre
everyfewmonths,aroundthetimeofeachCBRReview.Thereareseveralsituationswhenyou
shouldsendtheindividualforareviewatthehealthcentre(seeChapter37).
Trialpsychiatricnurse
37
Incertaincircumstancesyouoryoursupervisormayneedtocontactthepsychiatricnurse.This
will usually bewhen a serious event has occurred, such as the individual attempting suicide.
ThereismoredetailonwhentocontactthepsychiatricnurseinChapter35.
Communityleaders
Communityleaderswillbeinvitedtoattendawareness-raisingmeetings.Youmayalsoneedto
haveindividualmeetingswithcertaincommunityleaderstohelpwithpartsofCBR.
Communitymembers
Communitymemberswillbeinvitedtoattendpublicawarenessraisingevents.
9.4 WhereandwhendoesCBRtakeplace?
Most of CBR takes place through home visits, where you will meet with the individual and
family.Youshouldtrytofitthelocation,durationandfrequencyofthehomevisitsaroundthe
needsandwishesoftheindividualandfamily.Thesevisitswillusuallylastbetween30and90
minutes,butmaybeshorter ifnecessary. Insomecases the individualor familymaynot feel
comfortableforyoutovisitthemathome.Atthefirstvisityoushouldoffertoseethematthe
healthpost instead, if theywish.Whereveryoumeet the individual, thecaregiveroranother
familymembershouldalwaysbepresentornearby.Howoftenyoumakethehomevisitsare
dependsonthephase.YouwilllearnaboutthePhasesinsection9.7.Wesuggestthefollowing,
butthismayvarybetweenfamiliesorduringharvesttimeorfestivals:
PhaseI:Everyweekorevery15days
PhaseII:Every15days
PhaseIII:Everymonth.
The communityworkwill take place at different places in the kebele. For example, youmay
meetthekebeleleaderatthekebeleoffice.
9.5 HowlongdoesCBRlast?
Youwillworkwitheachindividualfor12months.Evenifthe individualbecomesmuchbetter
whilstyouareworkingwiththem,youshouldstillcontinuetovisitthemduringthe12-month
period.Thiswillhelpthemtokeepwellanddevelopmoreskills.
9.6 HowdowestartCBR(initialvisit)?
Yoursupervisorwillgiveyouthenameandcontactdetailsoftheindividualsyouwillbeworking
with. You will arrange the first home visit by phone or in person. You can ask the Health
38
ExtensionWorkertohelpyoutofindthehomeoftheindividual.Overthefirstoneortwovisits
youshouldgivethefollowinginformation:
• Introduceyourself
• Describe thestructureandpurposeofCBR (seesection9.1and9.7).Explain thatyou
arenotabletooffermoney,aloanorajob.Explainthatthefamilydonotneedtopay
youorgiveyougifts.
• Describethemodulesyoumightcover(seesection9.7)
• Discussconfidentiality(seeChapter10,section10.6)
• Explainthatthecaregiveroranotherfamilymembershouldbepresentornearbywhen
youdothevisits
Youshouldalsogatherthefollowinginformation:
• AskwhytheydecidedtoparticipateinCBR
• Askhowlongtheyhavebeenunwellandwhentheyfirstsoughthelp
• Askiftheyaregenerallywellorunwellatthemoment.Askwhatproblemstheillnessis
causingatthemomente.g.behavingstrangely,beingunmotivated.
• Relationshipofprimarycaregivertoindividual
• OtherfamilymemberswhowillalsobeinvolvedinCBR.Inparticularthinkaboutwhich
familymember/shavemostpowerandinfluence.Thismaybeanolder,malerelative.
• Homeenvironmentincludingwholivesinthehome,thetypeandconditionofthehome,
positionof the homeand any issueswith access, and incomeand landownedby the
family.
• Preferredlocationofvisits(homeorhealthpost)
• Iftheindividualiscurrentlychained
• Iftheindividualiscurrentlyaccessingthehealthcentre
• Iftheindividualiscurrentlyaccessingmedication
• Contactdetailsoftheprimarycaregiver
• Urgent needs which need addressing immediately, before the next home visit. For
example,theindividualissuicidalorseriouslyillwithaphysicalhealthproblem.
• Theparticularstrengths,opportunitiesandchallengesforthatfamily.
YoushouldrecordthisinformationontheInitialAssessmentform(Form1).

39
9.7 WhatarethephasesofCBR?
This CBR is divided into three phases. At each phase you will be helping the individual in
differentways.Thisisbecauseastimepassespeoplewithschizophreniawillusuallyhavesome
improvement,sotheirneedswillchange.AtthebeginningofeachPhaseyouwillconductaCBR
Reviewtogetherwithyoursupervisor.Thekeyareas foreachphasearedescribedbelowand
summarisedinTable3.
PhaseI
During Phase I the aim is to get to know the individual and family and to develop a trusting
relationshipwiththem.YouwillcompletethefourPhaseImoduleswithall individuals.These
modulesareimportantforallpeoplewithschizophreniaastheyaddressbasicneeds:
• Understandingschizophreniaanditstreatment
• Improvingaccesstohealthservices
• Dealingwithhumanrightsissues,whentheyarise
• Preparingforacrisis
CBR Review I, at the beginning of Phase I, helps to decide which order to address these
modules.ThelengthofPhaseIdependsontheparticularcircumstancesoftheindividual.Itmay
lastforaroundthreemonths,butitmaybemuchshorterormuchlonger.AttheendofPhaseI
youmaywishtorevisethemainissuesyouhavecoveredbeforemovingtoPhaseII.
PhaseII
AsidefromthebasicneedsaddressedinPhaseI,peoplewithschizophreniahaveverydifferent
disabilities and needs. In CBRReview II, at the beginning of Phase II, youwill therefore do a
NeedsAssessment.Thishelpsyoutodecidewhichareastofocuson.TheNeedsAssessmentis
describedinChapter12.OnthebasisoftheNeedsAssessmentandthewishesoftheindividual
and family, you will set goals to work towards during Phase II. Goal Setting is described in
Chapter13.Tomakesurewearetakingactionstoachievethesegoals,youwillthendelivera
seriesof linkedModules.Theexactmodules thatyoudeliver to the individualwilldependon
whichproblemshavebeenidentifiedintheNeedsAssessment.Dependingontheneedsofthe
individualPhaseIImayincludethefollowingmodules:
• Supportingindividualstotakemedication
• Improvingdaytodayfunctioning
• Improvingthefamilyenvironment
• Managingstressandanger

40
• Takingpartincommunitylife
• Gettingbacktowork
• Dealingwithstigmaanddiscrimination
• Dealingwithdistressingsymptoms
• Improvingliteracy
• Improvingphysicalhealth
• Takingcontrolofyourhealth
In Phase II youwill also set up a Family SupportGroup in each kebele. All caregivers, and in
somecasespeoplewithschizophrenia,areinvitedtotheseGroups(seeChapter32).Thelength
ofPhaseIIdependsontheparticularcircumstancesoftheindividual.Itmaylastforaround4to
6months,butitmaybemuchshorterormuchlonger.AttheendofPhaseIIyoumaywishto
revisethemainissuesyouhavecoveredbeforemovingtoPhaseIII.
PhaseIII
ThenewfocusinPhaseIIIispreventionofrelapse(stoppingtheillnessreturning).Thereforethe
ModulethatwecoverwitheveryoneinPhaseIIIis:
• Takingcontrolofyourhealth
ThemainpurposeofPhaseIIIistomaintaintheprogressmadeinPhaseII.However,individuals
will still have different needs, and thesemay have changed over time since Phase II. In CBR
Review III at the beginning of Phase III you will therefore do another Needs Assessment.
Dependingontheneedsoftheindividual,andthegoalsthatareset,PhaseIIImayincludeany
of the Phase II modules. The Family Support Groups should continue through Phase III. The
length of Phase III depends on the particular circumstances of the individual. Itmay last for
around3to6months,butitmaybemuchshorterormuchlonger.

Table1OverviewofRISECBRstructure
Phase CBRReview Goals Modules Communityengagementtasks Family SupportGroup
I CBRReviewI:• Initial
Assessment• Needs
Assessment• Goalsettingfor
PhaseI• RiskAssessment• Accompanyto
healthcentre• Rehabilitation
plan
Individualandcaregiverhavebeeninformedofwhatschizophreniais,availabletreatments,andthepotentialforrecovery
Understandingschizophreniaanditstreatment
Task1:Meetwithhealthextensionworker/sTask2:IdentifykeycommunityleadersTask3:IdentifykeycommunityresourcesTask4:AscertainwhatcommunityengagementrelatingtomentalillnesshasalreadytakenplaceorisplannedTask5:MeetwithkeycommunityleadersTask6:Communityawareness-raisingTask7:Identifypotentialemploymentopportunitiesinthekebele
Individualisabletoaccessmedicationandattendhealthcentreformentalhealthasindicatedbyclinicalstatus
Improvingaccesstohealthservices
Crisismanagementplanisinplace PreparingforacrisisPersonwithschizophreniaisnotchainedorrestrained
Dealingwithhumanrightsissues
II CBRReviewII:• Needs
Assessment• Goalsettingfor
PhaseII• RiskAssessment• Accompanyto
healthcentre• InvitetoFamily
SupportGroup• Rehabilitation
plan
Individualiswillingtotakemedication Supportingindividualstotakemedication
Task8:IndividualmeetingswithKebeleleadersTask9:IndividualmeetingswithEdirleadersTask10:IndividualmeetingswithreligiousleadersTask11:Individualmeetingswithtraditionalhealer/holywaterpriest/attendant
SupportgroupactiveIndividualhasstrategiestoremember
totakemedicationIndividualfeelssideeffectsareimprovingIndividualfeelshallucinationsanddelusionsareimproving
Dealingwithdistressingsymptoms
IndividualfeelsproblemswithmotivationandthinkingclearlyareimprovingIndividualisabletoaccesshealthservicesforphysicalandsexualhealthneedsandcontraceptionwhen
Improvingaccesstohealthservices

required Task12:Demonstrateprogressofclient/stocommunityleaders/widercommunityTask13:CommunityawarenessraisingconsolidationTask14:FacilitateemploymentopportunitiesinthekebeleTask15:Individualmeetingswithliteracygroupleader
Individualhasstrategiestodealwithstressandanger
Managingstressandanger
Individualhasinformationtomakedecisionsabouthealth-relatedbehaviours
ImprovingPhysicalHealth
Individualhasgoodphysical,sexualandreproductivehealthIndividualisnotmalnourishedIndividualparticipatesincommunitylife
Takingpartincommunitylife
IndividualparticipatesinreligiousactivitiesiftheyareimportanttotheindividualPersonwithschizophreniaisabletointeractsociallywithneighboursandfriendsIndividualhasimprovingabilitytodoparentingactivities
Improvingthefamilyenvironment
IndividualcancarryoutusualfamilyroleIndividualhasimprovedrelationshipwithfamilymembersCaregiverhasimprovedabilitytocopeIndividualhasimprovingself-care Improvingdaytoday
functioningIndividualhasimprovingabilitytodohouseholdtasksIndividualhasimprovingself-esteem Dealingwithstigmaand

Individualdoesnotfeeldiscriminatedagainst
discrimination
Individualisnotthevictimofphysical,sexualoremotionalabuse
Dealingwithhumanrightsissues
Individualhasrestoredparticipationinlivelihoodactivities,includingfarmwork
Gettingbacktowork
Individualhasbasicliteracyskills Improvingliteracy3 CBRReviewIII:
• NeedsAssessment
• GoalsettingforPhaseIII
• RiskAssessment• Accompanyto
healthcentre• Rehabilitation
Plan
Individualhasrelapsepreventionplan Takingcontrolofyourhealth
AnyPhase2CommunityEngagementtask
Supportgroupactive
AnyPhase2goal AnyPhase2module

9.8 WhataretheCBRReviews?
TheCBRReviewsareachanceforyoutodiscussthe individual’sprogresswiththe individual,
thefamilyandyoursupervisor.TheytakeplaceatthebeginningofeachPhase.Whatyoucover
intheCBRReviewdependsonthePhase.JustbeforeoraroundthetimeofeachCBRReview
you should go with the individual to the health centre. By doing this you will get more
information about the progress the individual is making and any problems they are having.
EverytimeyouaccompanyanindividualtothehealthcentreyoushouldrecorditontheHealth
CentreContactForm(Form2).EachCBRReviewwillusuallytakemorethanonehomevisitto
complete. You should complete the CBR Review Form (Form 3) to ensure you have done
everythingforthatCBRReview.
CBRReviewI:BeginningofPhaseI
InitialAssessment(seesection9.6andForm1)
NeedsAssessment(seeChapter12andForm4)
Accompanytohealthcentre(seeForm2)
PrioritisePhaseIGoals(seeSection13.5andForm5)
RiskAssessment(seeChapter14andForm7)
RehabilitationPlan(seeForm8)
CBRReviewII:BeginningofPhaseII
NeedsAssessment(seeChapter12andForm4)
GoalsettingforPhaseII(seeSection13.5andForm6)
RiskAssessment
Accompanytohealthcentre
InvitetoFamilySupportGroup(seeChapter32)
RehabilitationPlan
CBRReviewIII:BeginningofPhaseIII
NeedsAssessment
GoalsettingforPhaseIII(seeSection13.5andForm6)
RiskAssessment
Accompanytohealthcentre
RehabilitationPlan
CBRReviewIV:At10-11months
ContinuingCareAssessment(seeSection9.12andForm9)
45
Accompanytohealthcentre
9.9 Whatcommunityworkisinvolved?
Ineverykebele, youneed to conduct the samecore tasks tomake linkswith thecommunity
(community engagement tasks). These should be completed around the time when the
individualsareinPhaseI(aroundthefirstthreemonths):
• Task1:Meetwithhealthextensionworker/s
• Task2:Identifykeycommunityleaders
• Task3:Identifykeycommunityresources
• Task4:Findoutwhatcommunityworkrelatingtomentalillnesshasalreadytakenplaceor
isplanned
• Task5:Meetingswithkeycommunityleaders
• Task6:Communityawareness-raisingevent/s
• Task7:Identifypotentialemploymentopportunitiesinthekebele
Dependingontheneedsof thepeoplewithschizophrenia,youmayalsoneedtoconductthe
followingtaskswhentheindividualsareinPhasesIIandIII:
• Task8:IndividualmeetingwithKebeleleaders
• Task9:IndividualmeetingwithEdirleaders
• Task10:Individualmeetingwithreligiousleaders
• Task11:Individualmeetingwithtraditionalhealer/holywaterpriest/attendant
• Task12:Individualmeetingwithliteracygroupleader
• Task13:Demonstrateprogressofclient/stocommunityleaders/widercommunity
• Task14:Communityawarenessraisingconsolidation
• Task15:Facilitateemploymentopportunitiesinthekebele
ThecommunityengagementworkshouldberecordedintheKebeleLogbook(Form10)
Yosef’sstory
BerhanisaCBRworkerwhoisaskedtolookafterYosefandhisfamily.Sherecordsherfirstvisit
toYosefontheInitialAssessmentForm.AtthenextvisitsheconductstheNeedsAssessmentto
gettoknowhissituationbetter.AspartofCBRReviewI,Berhanalsogoestothehealthcentre
withYosefandAddisa fewdays laterandsits inwhilstYosefseesthenurse.Thishelpsherto
understandhisillness.SherecordstheinformationontheHealthCentreContactForm.

46
9.10 HowdoyoudeliverCBR?
CBRManual
The rest of themanualwill tell youhow todeliver eachmoduleof CBR. Each chapter in the
manual covers a differentmodule. In each chapter youwill find the following questions are
answered:
• Whatistheproblem?
• Whydoesthisproblemhappen?
• Whyisitimportanttohelpwiththisproblem?
• Howcanwehelp?
Chapter31alsotellsyouhowtoconducttheCommunityEngagementtasks.
Step-by-stepguide
Thereisashortstep-by-stepguidetodeliveringeachmodule.Thesearedesignedtotakeonthe
homevisitstoremindyouofthemainthingstosayanddoforthemodule.
Structureofhomevisits
Eachhomevisitshouldcoverthefollowing
o Checktheirgeneralhealthandsymptoms
o Checkandrecordprogressrelatingtoongoinggoals
o Problemsolvingforongoinggoals
o Delivermodule/s:selectedonthebasisoftheremaininggoals
o Checkwhethertheyaretakingmedicationregularly
o Dobriefriskassessment(seeChapter14)
o Taskstocompletebeforethenextsession
o Plandateandcontentofnextsession
Recordinghomevisits
AllhomevisitsshouldberecordedontheHomeVisitForm(Form11).Youshouldalsocomplete
theVisit SummaryForm (Form12),whichasks for informationabout thepractical aspectsof
yourvisit,forexamplehowlongittookyoutogetthere.
Completingmodules
Youcan takeusemore thanonehomevisit tocompleteamodule.Sometimes,youmayalso
covermorethanonemoduleinonehomevisit.
Workload

47
Youshouldusuallydotwotaskseveryday.Forexampletwohomevisits,oronehomevisitand
onemeetingwithcommunityleaders.SeeForm13foranexampleofhowyourtimetablemight
look.
9.11 HowdoyouencourageindividualstotakepartinCBR?
Whenyouaregoingtomakeahomevisit,ifpossiblecallaheadthedaybeforeorwhenyouare
on your way to remind the individual or caregiver. During Phase III you should also call the
individualorcaregivertochecktheirprogresseverytwoweeks.Iftheindividualgoesmissingfor
a long period you should encourage the family and community members to look for the
individual,butyoushouldnotnormallysearchforthemyourself.
9.12 HowdoyouendCBR(continuingcareassessment)?
Ataround10or11monthsyoushouldconductCBRReviewIV.AtthisCBRReviewyoushould
discussthefactthatCBRwillsoonendwiththeindividualandfamily.Youshouldlookbackto
theGoalSettingFormsfromeachPhaseanddiscusstheprogressthathasbeenmadeoneach
goal. This should be a positive exercise, which focuses on the individual’s strengths and
achievements. It should not be a chance to make the individual feel that they have failed.
Around this timeyou shouldalsoattend thehealth centrewith the individual. Togetherwith
yoursupervisoryoushouldcompletetheContinuingCareAssessment(seeForm9).Theaimis
to identifyongoingneedsandto formulateanongoingplantoaddresstheseneedsonceyou
haveleft.Youshouldpreparetheindividualandfamilyforthepossibilitythatoldproblemswill
comebackorthatnewproblemsmayappear.Reassurethemthatthehealthcentrestaffwill
continue to look after the individual. At the final session theContinuingCare Plan should be
reviewedwiththe individualandtheircaregiver.Theymayfeelangryorupsetthatthehome
visitsareending.Remindthemthattheyhavelearnttodealwiththeirownproblemswhilstyou
havebeenworkingwiththem.
9.13 WhatdoyoudoifCBRisnotwanted?
Rarelytheindividualand/orfamilymaywishtostopparticipatinginCBRbeforetheendof12
months. This may make you feel shocked, upset or rejected. However we should not force
anyonetobeinvolvedinCBRiftheydonotwanttobe.Herearesomewaystodealwiththe
situation:
• Acceptwhatthefamilysaysanddon’ttrytoarguewiththem
48
• Checkwhatthefamilyisunhappywithandtrytochangeit.Forexample,offertomeetthem
atthehealthpostinsteadofathome.
• ConsiderinvitinganindividualwhohasreceivedorisreceivingCBRtodiscussthebenefitsof
participatingwiththeindividualandfamily.
• Alwaysdiscussthesituationwithyoursupervisor
• Leaveyourcontactdetailswiththefamily.Sayyouarehappytocontinuewhenevertheyare
ready.
• Trytoarrangeafinalsessiontosaygoodbyeanddosomefinalwork-forexamplereminding
themwhattodoinanemergencysituation.
InsomecasesonlythecaregiverdoesnotwishtoparticipateinCBRoristoobusy,butthe
individual wishes to continue. When this happens you may continue to support the
individual,butonlyifyouandyoursupervisorhavenoconcernsaboutyoursafety.
9.14 Summary
• CBRaimstoimprovethelivesofpeoplewithschizophreniaandinvolvethemincommunity
life.Theprinciplesare:employaholisticapproach,workwiththefamilyandthecommunity,
encouragerespectforhumanrightsandlinktoexistingservices.
• ThefollowingpeopleareinvolvedinCBR:thepersonwithschizophrenia,thecaregiverand
family, theCBRworker, theCBR supervisor, thehealth centre staff, thepsychiatricnurse,
thecommunityleaderandcommunitymembers.
• CBRlasts12monthsforeachindividualandtakesplacethroughhomevisitsandmeetingsin
thecommunity
• CBRhas3phases.InPhaseItheaimistobuildarelationshipwiththeindividualandcover
the same Modules with everyone: Understanding Schizophrenia and its treatment,
Improvingaccesstohealthservices,Dealingwithhumanrightsissues,Preparingforacrisis.
• InPhasesIIandIIItheModulesdifferbetweenindividualsdependingontheirneeds.They
might include: supportwith takingmedication, improvingdaily functioning, improving the
family environment, getting back to work and community life, Dealing with stigma and
distressingsymptoms,improvingphysicalhealthandliteracy.
• The Community Engagement Work involves: Identifying community resources, engaging
with the health extension worker and community leaders, doing community awareness-
raisingandarrangingemploymentopportunities.
• YouwillsetupaFamilySupportGroupforfamiliestoprovidemutualsupport

49
• TheCBRmanualandStepbyStepGuidetellyouhowtodeliverCBR

50
10 Communicationskillsandproblemsolving
10.1 Whydoweneedcommunicationskills?
A lotofCBRtakesplace in the familyhomethroughdiscussionsbetweenyouandtheperson
withschizophreniaandtheirfamily.Forthesediscussionstogowellandbeusefulyouwillneed
certain skills in listeningand communicating.Although itmay sometimesbemoredifficult to
communicateclearlywithapersonwhohasschizophrenia,itisimportantthatyoualwaystreat
thepersonasaresponsibleandrespectedindividual.
10.2 Howtocommunicatewellwithfamilies
1. Befriendlyandunderstanding
Itisimportanttobewarmandfriendlytowardstheindividualsandfamily.Trytoputyourselfin
the place of the person you are talking to and feel what he or she could be feeling at the
moment,forexamplefrustrationoranger.The process willhelpyouto understandbetter the
situationof theperson.Youcanalso letthepersonknowthattheirfeelingsarecommonand
expectedforsomeoneintheirsituation.This isdifferentfromexpressingpitywhereyou only
expressthe factthatyoufeelbad fortheperson.Thisdoesnotmake theperson feel thathe
or she is being genuinely understood. Some ways to be understanding include: “I can
understandhowthewaypeoplehavebeentreatingyoumakesyoufeelangry”and“Youseem
tofeelupsettoday.”
2. Benon-judgemental
Youshould accept the person forwhoheor she is irrespective of religionandethnicgroup.
Thepersonhastherighttohisorherownviewsandfeelings.Evenwhenyoudonotagreeyou
shouldnot judgethepersonnegatively.
3. Berespectful
Beawareof theperson’sage,genderandculture.Youshouldmake them feel respected.Use
words that are easily understandable, and that the individual does not find distressing or
offensive,torefertoschizophreniaormentalillness.
4. Bepatient
51
The individual and the familymay take a lot of time to understand informationor tochange
theirbehaviour.
5. Encouragetrust
Respond sensitively if the individual or family tell you private or distressing information (for
example,regardingsexualviolence),andreassurethemthatyouwillnotdiscussthiswithother
membersofthecommunity.
10.3 Whatskillscanyouusewhencommunicating?
1. Showthepersonthatyouarelisteningtothem
Listencarefullytowhatthepersonwithschizophreniaissaying.Ifyoushowthepersonthatyou
arelisteningtheyaremorelikelytofeelcomfortabletosayhowtheyfeel.Youcandothisby:
• Keepingappropriateeyecontactwiththeperson
• Use body language.Make encouraging facial expressions and gestures. Sit facing the
personwithyourarmsunfolded.
• Don’tkeepcheckingyourwatchorphone.
• Keepyourphoneonsilentmode.Don’tansweritunlessitisyoursupervisor.Don’tread
orrespondtotextmessages.
• Keepyourvoicegentle.Speakslowlyandclearly.
• Don’tinterruptthepersonorignorewhattheyaresaying
2. Usequestioningskills
‘Open ended’ questions can be useful in getting the person to talk. They are questions that
cannotbeansweredinafewwordsorsentences.Forexample,“Couldyoutellmemoreabout
that?”and “How did you feelwhen that happened?”Trynottoputyourownviewintothe
question.Forexample,“Don’tyouthinkitwouldbehelpfulifyougotbacktowork?”Thismay
sounds judgemental and threatening. Instead you could say, “What do you think would be
helpfulforyou?”
3. Beobservant
Youshould be observant of the body languagethattheindividualuses.Forexample, if the
personhas a smile onher facebut hasher fists clenched or twisting her fingers vigorously
thismay indicateabuild-upof tension.
52
4. Useencouragement
Usewordtoencouragethepersontocarryontalking,forexample“um”,“really”or“ahha”.
Nod your headandsmileattheperson. Sometimes just the repetition of a word leads to
the person giving further details. If the person says “My life is amess” you could reply “A
mess?”. This encourages the persontosay what she means.Youcanalso repeatback the
person’sstoryinyourownwords.Thisisusefultomakesureyouhaveunderstoodcorrectly,
andtoencouragethepersontotalkabouttheproblemindetail.
5. Noticethefeelingsoftheperson
Itcanbeusefultonoticethefeelingsofthepersonandshowthemwhatyouhavenoticed.This
helpsthemtofeelunderstood.Youmightnoticefeelingsthroughwhatthepersonsaysorhow
theyact.Forexample,ifthepersonsays“Iwassoangry thatI felt likehittinghim”,youcould
reply “Youmusthave been really angry”.Orifthepersonisbitingherlips,youcouldsay “You
seemvery worried today”.
6. Noticethepositivethings
Noticing the positive things and how the individual is improvingwill help to improve their
self-esteem. Forexample“You sayyouare unhappyaboutyourdaughter-inlawbeingrudeto
you... but it is good to hear that you have been enjoying time playingwith your grandson.”
However,trynottobeunrealisticortogivefalsehopeforthingsthatdefinitelywon’thappen.
10.4 Whatapproachesarenothelpfulwhenworkingwithfamilies?
• Tellingthepersonwhat tothinkordoormakingdecisions for them,withoutaskingthem
abouttheirexperiencesorideas
• Makingjudgementsonwhetherthepersonis‘good’or‘bad’
• Blamingthepersoniftheyhavedifficultychangingtheirbehaviour
• Makingpromisesthatyoucannotkeep
• Pretendingtounderstandwhattheymeanwhenyoudon’t
• Notrespondingwhenthepersontellsyousomethingsadordifficult
• Tellingthepersonaboutyourpersonalexperiences
• Usingoffensivewordsforschizophreniaormentalillness

53
10.5 Problemsolving
Sometimespeoplewith schizophreniaand their caregivers find theirproblemsoverwhelming.
Worryingor thinking toomuchabout theirproblemscanmake them feel stress (seeChapter
23).Thisstressmayevenmaketheillnessworseorcausearelapse(seeSection2.4).Youcan
use problem solving to help individuals find ways around their problems. You can use this
methodfordifferenttypesofproblems,forexampledealingwithstigmaanddiscrimination(see
Chapter 28) or planning how to get back to farm work (see Chapter 27). People with
schizophreniamayhavemanyworriesorproblems.Trytofocusononeatatime.Picktheone
that relates to the module you are covering, or the one which is most important to the
individualatthattime.Onceyouhavedecidedwhichproblemyouaregoingtofocuson,follow
thesesteps:
1. Describetheproblem
• Discusstogetherwhattheproblemis
• Trytodescribeitintheclearestway
2. Thinkofpossiblesolutions
• Together,listasmanysolutionsaspossibletosolvingtheproblem.Sometimesyoumayneedyour
supervisor’shelptothinkaboutpossiblesolutions.
• Trynottothinkaboutwhetherthesearegoodorbadsuggestions
3. Discussthepossiblesolutions
• Discusseachpossiblesolutioninturn
• Foreachone,nowdecidetogetherwhetheritisagoodsuggestionornotuseful
• Foreachofthegoodsuggestions,discusstogetherthegoodandbadthingsaboutit.
4. Decideonasolution
• Decidewhichofthepossiblesolutionsisthebest.Alwayschecktheindividualishappywith
thissolution.
• Discussthestepbystepactionswhichareneededtocarryoutthesolution.
• Thinkaboutwhowillbeinvolvedandwhattheirroleswillbe
5. Carryoutthesolution
• Supporttheindividualandfamilytocarryoutthesolutionasyouhavediscussed
• Checkontheirprogressatlatersessions

54
10.6 Confidentiality
Information that you gather during your workmust be kept secret from other people, even
fromthepatient’srelatives,unless:
• Thepatientgivespermissionforyoutodiscussitwiththem
• Itisessentialthatyoutellotherpeopleinordertoprotecttheperson.Forexample,ifyou
areworriedthepersonisatriskofsuicide(seeChapter14).
Theplaceswhereyoutalktopeoplewithschizophreniaandtheircaregiversshouldbearranged
insuchawaythatno-onecanlistentoyourprivatediscussions.Explainthatyouwon’ttellother
peopleaboutthethingsthattheytellyouunlessitisnecessaryforhelpingthem.Rememberto
askpermissionoftheindividualandcaregiverbeforediscussinganindividualwithacommunity
leaderorcommunitymember.Thiswillhelpinbuildingtrustbetweenyouandtheindividuals
youworkwith.
10.7 Summary
• GoodcommunicationbetweenyouandtheindividualandfamilyisessentialforCBR
• When working with families you should be: understanding, non-judgemental, respectful,
patientandencouragetrust
• The skills you can use include: listening and questioning skills, being observant, using
encouragement,noticingfeelingsandnoticingpositivethings.
• You can use Problem Solving to help individuals find practical ways around their problems
55
11 Creatingatrustingrelationship
11.1 Whatisatrustingrelationship?
A trusting relationshipmeans that there is a bondbetween you, the individual and family. It
meanstheindividualandfamilyspeakfreelyandsharetheirideasandconcerns.
11.2 Whyisitimportanttohaveatrustingrelationship?
Itisveryimportanttohaveatrustingrelationshipwiththeindividualandfamily.Thiswillhelp
theCBRinthefollowingways:
• Theindividualandfamilymembersaremorelikelytotellyoutheinformationyouneed
tohelpthem.Forexample,worriesaboutmoneyorfamilyconflict.
• Theyaremorelikelytolistentotheinformationyougivethem
• Theyaremorelikelytotrytheactivitieswhichyousuggest
• Theyaremorelikelytotaketheirmedicationregularly
• Theyaremorelikelytokeepreturningtothehealthcentre
• Theyhaveawayofexpressingtheiremotions
• Theyaremorelikelytobehopefulthatthingscanimprove
11.3 Howtoformatrustingrelationship
1. Introduceyourself
Whenyoufirstmeettheindividualandfamily,introduceyourself.Introduceyourselftoanynew
familymembersyoumeetatlatersessions.
2. Learnaboutthefamily
Try to learnasmuchaspossibleabout the individualandtheir familybeforeyoumeet them.
Findout fromthehealthcentrestafforHealthExtensionWorkerhow longthe individualhas
beenunwellandwhatproblemstheyhavehad.Whenyoumeetthefamily,trytounderstand
whoisinvolvedinthecareoftheindividualandwhohaspowerandinfluence.Youmayneedto
workwiththisfamilymember/stochangehowthefamilytreatstheindividual.
3. Focusontheproblemsthatareimportanttotheindividual
Listentowhattheindividualwantstochangeandhelpthemtoachieveit(seeChapter13).

56
4. Keepeachsessionfocusedontheindividual
Nearthebeginningofeachsession,asktheindividual“Whatwouldmakethisahelpfulvisit?”or
“Whatwouldyou like to seedifferentafterourmeeting?” It isnotusuallyhelpful to refer to
yourownexperiences.
5. Getdetailedinformationfromtheindividual
Trytogetasmuchinformationaspossibleaboutthecurrentsituation,andanydifficultiesthey
have.Forexample,anindividualmaybedrinkingalotofalcohol.Onaskinghimforthereasons
fordrinking,hemaysaythisisduetofrequentquarrelsathome.Youcanthendiscusshowto
reducethequarrels,insteadofdrinkingtodealwiththeproblem.
6. Listentoideas,beliefsandconcerns
Listentothe ideasandbeliefsofthe individualwithout judgingthemortellingthemtheyare
wrong.Forexample,theindividualmayfindithelpfultomakeregularvisitstoholywater.Ifthis
isnotcausingharmyoushouldsupportthemtocontinue,evenifyoudonotbelievethatholy
watercancuretheillness.Youshould listentotheirconcerns.Forexample,eveniftheyhave
worriesaboutsideeffectsthatyouthinkaren’timportant,youshouldnotsimplydismissthem.
7. Treattheindividualwithdignityandrespect
Maketheindividualthecentreofyourattentionatalltimes.Treatthemwiththerespectyou
wouldwithanyotherperson,duringthesessionsandifyoumeettheminthekebele.Don’tuse
stigmatizing words like ‘mental’. Use non-stigmatizing words like problem and illness. These
actionswillhelptoimprovetheself-esteemoftheindividual.Theyalsohelptoreducestigma
anddiscriminationfromthefamilyandcommunitytowardstheindividual.
8. Stayneutralduringfamilydiscussions
Theremaybedisagreementswithinthefamilyonthebestwaytodothings.Trytostayneutral.
9. Keepclearboundaries
Youareaimingforacloseworkingrelationshipwiththeindividualandfamily.However,itisnot
appropriateforthemtointrudeonyourpersonallife.Thefamilyshouldnotvisityouathome.
However,itisfinetogreetthefamilyifyouseethemoutsidetheirhome.Itisfineforthefamily

57
togiveyouteaorcoffeewhenyouvisit,butitisnotnormallyallowedforyoutoreceivegifts.
Youshouldalsonotpayfortheindividual’sfoodormedicationyourself.
11.4 Challengeswithformingatrustingrelationship
Due to their illness people with schizophrenia sometimes find it more difficult to form a
relationshiporbondwithotherpeople.Youshouldalwayskeep trying.But this ispartof the
reasonwhyitisimportanttoalsomakeagoodrelationshipwiththefamily.
11.5 Summary
• Creating a trusting relationship between you, the individual and the family makes it more
likelythatCBRwillbehelpful.
• You can form a trusting relationship by: finding out about the family, keeping the sessions
focusedontheindividualandtreatingthemwithdignityandrespect,listeningtobeliefsand
concerns,andstayingneutralduringfamilydiscussions.

58
12 NeedsAssessment
12.1 WhatistheNeedsAssessment?
Peoplewithschizophreniahavemanydifferentsortsofproblems.Someproblemswillbemore
importantforparticularindividualsandfamilies.Manyoftheseproblemscanbehelpedthrough
CBR.TheNeedsAssessment isanorganisedwayoffindingoutwhatproblemseachindividual
andfamilyarefacing.
12.2 Whydowedotheneedsassessment?
• TheNeedsAssessmenttellsuswhatproblemstheindividualandfamilyhave,andwhichare
themost important problems at that time. This helps us decidewhat improvements the
personwith schizophreniaand their familywould like towork towards first. This is called
GoalSetting(seeChapter13).ThishelpsustodecidewhichModulesofCBRtostartwith,
andwhichtoleaveuntillater.
• Doing the Needs Assessmentwill help the individual and family understand that you are
interestedintheirproblems.Thiswillhelpbuildatrustingrelationship(seeChapter11).
• It isalsousefultolookbackattheNeedsAssessmentattheendeachPhase.Thenwecan
seewhethertheproblemsthatthefamilyhadatthebeginningarestillthere,andwhatstill
needstobedone.
12.3 Whoisinvolvedintheneedsassessment?
TheNeedsAssessment should always involve you, , the individual and theprimary caregiver.
YoursupervisorshouldbeinvolvedatthebeginningofPhaseIandmaybeinvolvedinPhaseII
andIII.Youmayincludeothermembersofthefamilywhoareinvolvedintheindividual’scare.
AroundthetimeoftheNeedsAssessment,youshouldaccompanytheindividualtothehealth
centreforareviewbythenurseorhealthofficer.Byobservingwhatthenurseorhealthofficer
saysyouwill getextra informationabout theneedsof the individual. Theremaybedifferent
viewsaboutwhatthemostimportantneedsare.Forexample,theindividualmayfeelthemost
urgentneed is to getback to farmwork. The familymay feel that the symptomsneed tobe
underbettercontrolfirst.Atthisstageitisimportanttogetallthepointsofview.InChapter13
youwilllearnhowtosetgoalsfortheindividualtogetherwiththefamily.
12.4 Whenistheneedsassessmentdone?
TheNeedsAssessmentisdonethreetimesduringCBR,atCBRReviewsI,IIandIII.

59
12.5 Howdowedotheneedsassessment?
You will use a detailed checklist to assess whether there are problems in the areas where
peoplewithschizophreniausuallyhavedifficulties.
UsingtheNeedsAssessmentform
TheNeedsAssessmentForm(Form4)coversthefollowingareas:
• Understandingschizophrenia
• Accessinghealthservices
• Preparingforacrisis
• Humanrightsissues
• Symptoms
• Takingmedication
• Sociallife
• Familylife
• Dailyfunctioning
• Work
• Empowerment
• Literacy
Youshouldgothrougheachpotentialneed in turnandask the individualand familywhether
theyhaveanyproblemsinthisarea.Forexampletoassesssociallifeyoucouldsay,“Sometimes
peoplewithschizophreniahaveproblemsdoingtheactivitiesinthecommunitythattheyusedto
do,orthatotherpeopletheiragedo.Forexample,beingpartofanEdirgroup,goingtokebele
meetingsorbeingpartofamahabergroup.Haveyouhadanyproblemswithdoingthesesorts
ofactivities?”
Usingobservations
Youandthesupervisorcanalsouseyourownobservationsaboutwhattheproblemsare.For
example, youmay notice that the individual is very drowsy (whichmight be a side effect of
medication),orthatafamilymemberoftenshoutsattheindividual.
Recordingtheneedsassessment
Markontheassessmentformwhethereachpossibleneedis:
60
• Not a problem for this person (everyone agrees there arenoproblems). For example, an
individualrememberstotaketheirmedicationeverydaywithoutbeingreminded.
• A partially met need (there are a few small problems). For example, an individual
occasionallydoesnotgotochurch,eventhoughtheywouldliketo.
• An unmet need (there are problems). For example the individual does not do any of the
farmworkthattheyusedtodo.
For each need write some comments about what you have been told and what you have
observed.Include:
• Detailedinformationontheneed.Forexample,whattypeofworktheindividualwouldlike
todoorwhatself-caretasksaremostdifficult.
• How long this has been a problem. For example, the individual may have had difficulty
socialisingforalongtime,buttheremaybenewmedicationsideeffects.
• Howimportantthisneedisfortheindividual.Thiswillhelplaterwhengoalsetting.
• If this is the second Needs Assessment, record what progress has been made since the
previousneedsassessment.
Assessingpersonalneeds
Inadditiontothechecklistyoushouldalsoasktheindividualandfamilytotellyouaboutany
otherproblemsorneedsthathavenotbeencovered.Theseareknownas‘personalneeds’and
youshouldrecordthemontheneedsassessmentform.
12.6 Tipsforcompletingtheneedsassessment
• Someindividualsandfamilymembersmaystartbysayingthattheyhavenoproblems.Itis
importanttogentlycontinueaskingfordifficulties.Youmayneedtocomebacktosections
onthechecklist.Sometimesyouwillneedmorethanonehomevisittocompletetheneeds
assessment.
• Whenyouaskeachquestion,thinkaboutwhat is likelytobeusualforthat individual.For
example, if youngwomendonotusually attend the kebelemeetings, then itmaynotbe
appropriatetoaskaboutproblemswiththis.
Yosef’sstory
AtReviewII,BerhandoestheNeedsAssessmentwithYosefandhisfamily.Haile,hersupervisor,
isalsothere.SherecordseverythingontheNeedsAssessmentForm.
61
• It is likelythatthe individualandfamilywillaskyouquestionsaboutthe illnesswhilstyou
aredoingtheneedsassessment.Youshouldbereadytoanswersomequestions,butremind
themtherewillbeachancetodiscussthesethingsinmoredetaillater.
12.7 Whatdowedowiththeinformationfromtheneedsassessment?
InPhaseI,wedotheNeedsAssessmenttohelptogettoknowtheindividualandthefamily.In
PhasesIIandIIIweusetheinformationforGoalSetting(seeChapter13).
12.8 Summary
• WedoaNeedsAssessmenttounderstandwhatproblemstheindividualhasandtodecide
whichpartsofCBRtostartwith
• Weconducttheneedsassessmentbyaskingquestionstotheindividualandfamily,making
observations,andattendingthehealthcentrewiththeindividual
• On the Needs Assessment Form you should record whether each possible need is not a
problem for this person, an unmet or partially met need.

62
13 GoalSetting
13.1 WhatisGoalSetting?
Goalsettingisaboutdecidingtogetherwhichneedstoaddressandinwhichorder.Itshouldbe
apositiveprocess,notonethatmakestheindividualfeelhelplessorafailure.
13.2 WhydoweneedtodoGoalSetting?
Goalsettingis importantsothattheindividual,family,youandyoursupervisorallknowwhat
youareworkingtowards.Thiscanhelpindividualstorecovermorequickly.Goalsettingmakes
surethattheCBRModulesthatyoudowitheachindividualaretherightonesforhimorher.
Goalsettingalsogivesasenseofachievementandprogresswhenagoalisachieved.
13.3 WhoisinvolvedinGoalSetting?
Goal setting should always involve you, the individual and the primary caregiver. You may
involveothermembersofthefamilywhoareinvolvedintheindividual’scare.Yoursupervisor
shouldbeinvolvedatthebeginningofPhaseIandmaybeinvolvedinPhaseIIandIII.
13.4 WhendowedoGoalSetting?
WedoGoal Setting as part of theCBRReviews at thebeginningof eachPhase.Goal Setting
shouldalwayscomeaftertheNeedsAssessment.
13.5 HowdowedoGoalSetting?
PhaseI
PhaseIisaboutmakingsureallindividualshavetheirbasicneedsmet.Eventhoughyoumight
havefoundoutaboutlotsofdifferentproblemsontheNeedsAssessment,duringPhaseIyou
shouldfocusonbasicneeds.ThepotentialgoalsforPhaseIaretherefore:
• Individualandcaregiverhavebeeninformedofwhatschizophreniais,availabletreatments,
andthepotentialforrecovery
• Individualisabletoaccessmedicationandattendhealthcentreformentalhealthas
indicatedbyclinicalstatus
• Crisismanagementplanisinplace
• Individualisnotchainedorrestrained
Notallindividualswillhaveproblemswiththesebasicneeds,sonoteveryonewillneedtoseta
goalaroundallofthem.TheorderinwhichyouaddressthePhaseIgoalswillalsodependon

63
the situation of the individual. For example if an individual is currently chained, you should
usually address the goal ‘Personwith schizophrenia is not chainedor restrained’ first, before
going on to the other goals. You should work together with the individual, family and your
supervisortodecidethebestordertoaddressthegoals.OnthePhaseIGoalSettingform(Form
5),youshouldmakenotesaboutthemostimportantgoalstoaddressfirst.Addatimeframefor
howlongyouexpect ittotaketoachievethegoal. Inadditiontothesecoregoalsyoushould
also ask the individual if they would like to set a personal goal. You should fill in the
RehabilitationPlan(Form8)tosummarisetheinformationfromtheInitialAssessmentandGoal
Setting. This form should be filled in using simple language that the family can understand.
Makeacopyoftheformfortheindividualandfamilytokeep.
PhaseII
In Phase II, all the goals are based on the particular needs of the individual and family. This
means they will differ from individual to individual. To set the Phase II goals you should go
through the list of needs that you marked as ‘Partially met’ or ‘Unmet met’ on the Needs
AssessmentyoucompleteaspartofCBRReviewII.Thenumberofgoals forPhase IIwillvary
betweenindividualsbutshouldnotbemorethanfiveorsix.Thedecisionaboutwhichgoalsto
focus on should bemade together with the individual, family, you and your supervisor. You
shouldalsodecidewhichgoalstofocusonfirst,andhowlongyouexpectitwilltaketoachieve
each goal. You can continueworking on Phase I goals if you feel ongoingwork is needed to
maintainthesituation.Youshouldencouragediscussionaboutthefollowing:
• Whichgoalsaremostimportanttotheindividualandwhy?
• Whichgoalsaremostimportanttothefamilywhy?
• Whichgoalsneedtobeachievedfirstbeforeothergoalscanbeachieved?Forexample,the
individualmayhaveproblemsrememberingtotaketheirmedication.Astheystillhave
manysymptomsthismaybethereasonwhytheyalsohavedifficultieswithself-careand
sociallife.Youmayagreethatitisimportantforthepersontostarttakingtheirmedication
regularly,beforemovingontoaddressingself-care.
• Whichgoalsarerealistic?
Yosef’sstory
AtReview I, Berhan doesGoal SettingwithYosef andhis family.Haile, her supervisor, is also
there.SherecordseverythingontheGoalSettingForm.
64
OnthePhaseIIGoalSettingform(Form6),youshouldtickoffthegoalsyouhavechosen,and
makenotes about themost important goals to address first. Include informationonwhy the
familywantstofocusonthosegoalsfirst.Youshouldadddetailsonwhatyouhopetoachieve.
Forexample,ifthegoalis‘Individualhasgoodself-care’youcouldaddtheparticulartasksyou
aretryingtoimprove,suchasgettingwashed.Atanytimeyoumaybeworkingtowardsseveral
goals at once. You should also discuss the personal goal set in Phase I, and either continue
workingtowardsthisorsetanewpersonalgoal.Recordanypersonalgoalsontheform.Once
again,youshouldsummarisethe informationfromgoalsettingbyupdatingtheRehabilitation
Plan(Form8).Makeacopyoftheformfortheindividualandfamilytokeep.
PhaseIII
SettingandprioritisinggoalsinPhaseIIIshouldfollowthesameprocessasPhaseII.However,in
Phase III you should focus on maintaining the improvements made in Phase III, rather than
starting to work on lots of new areas. The number of goals for Phase III will vary between
individualsbutshouldnotbemore thanthree.Unless theyhavealreadyachievedthegoal in
PhaseII,allindividualsshouldhavethefollowinggoal:
• Individualhasrelapsepreventionplaninplace
OnthePhaseIIIGoalSettingform(Form6),youshouldtickoffthegoalsyouhavechosen,and
makenotesaboutthemostimportantgoalstoaddressfirst.Summarisetheinformationonthe
RehabilitationPlan(Form8).
13.6 WhatdowedowiththeinformationfromGoalSetting?
EachgoalhasaspecificModuleconnectedtoit.Ifanindividualisworkingtowardsagoal,then
you should complete the connectedModule at somepointduring thePhase.More thanone
goal may be addressed by the same module, so you can try to work on these linked goals
aroundthesametime.Evenifyouareonlytryingtoachieveonegoallinkedtoamodule,you
shouldnormally complete thewholemodule.However, you should tailor themodule tohelp
with the specific problems that the individual faces. Remember the focus is on supporting
individualstoachievethegoals,notjusttocompletethemoduleasfastaspossible.
Yosef’sstory
AtReview II,BerhandoesGoal SettingwithYosefandhis family.Haile,her supervisor, isalso
there.SherecordseverythingontheGoalSettingForm.

65
PhaseI
InPhaseIeveryoneshouldcompletethesameModules,eveniftheyhaven’tsetaspecificgoal
relatingtothemodule.Thesemodulesare:
• Understandingschizophreniaanditstreatment
• Improvingaccesstohealthservices
• Addressinghumanrightsissues
• Preparingforacrisis
However the order of the Modules should be decided depending on the situation of the
individual. The Initial Assessment will help you to decide this. How long you spend on each
Module will also depend on the individual. For example, if an individual has a good
understandingofschizophrenia,isnotchainedortiedup,andregularlyaccesshealthservices,
theymayonlyneedoneortwohomevisitstocompletealltheseModules.Oryoumayneedto
spendmanymorehomevisitswithsomeonewhodoesnotaccesshealthservicesandwho is
currentlysufferingseveresymptoms.
PhasesIIandIII
OnceyouhavedecidedwhichgoalstofocusoninPhasesIIorIII,andinwhichorder,youshould
thennoteanddiscusswhichmodulesareneededtoachievethesegoals.Thisshouldbeeasy,as
eachgoalhasarecommendedmodulelinkedtoit.ThesearelistedonthePhaseIIandIIIGoal
Setting forms. On the forms you can also write other actions that you think might help to
achievethegoal,butwhicharen’tinthemodule.AsinPhaseIthelengthoftimetocomplete
eachModulewillvarybetweenindividuals.
13.7 Howdoweknowifgoalsareachieved?
Youshouldalwaysbethinkingaboutwhichgoalstheindividualisworkingonatthemoment.At
eachhomevisityouwillcheckandrecordtheprogressofeachofthecurrentgoalsusingthe
HomeVisitForm(Form11).Onthisformforeachgoalyourecord:
• Themodule/syouarecurrentlyworkingonwhichrelatetothatgoal
• Anycommunityengagementworkorotheractionsunderwaywhichrelatetothatgoal
• Anyissuesorproblemsrelatingtothegoal
• Whetherthegoal isachieved,partiallyachievedornotachievedbytheendofthehome
visit.

66
InPhases II and III agoal isnormallyonlyachievedwhen there isa change in thebehaviour,
actions or experiences of the individual or family. You should ask the individual and family
whether they feel thegoalhasbeenachieved. Youwill alsomeetwith your supervisorevery
twoweekstodiscusstheprogressofeach individual (seeChapter34).At thesemeetingsyou
shoulddiscusswhethereachof thegoalsyouareworkingonhasbeenachievedyet.There is
not a fixed timewhen any of the goals should be achieved by. In your discussions with the
family you should focuson thepositive things. Trynot tomake the individual feel theyhave
failedif ittakesalongtimetoachievethegoal.OnceagoalisachievedtickitoffontheGoal
SettingForm.
13.8 Whendowemovetothenextphase?
MovingfromPhaseItoPhaseII
Once all the Phase I goals have been achieved, you should arrange CBR Review II with the
individual, family, youandyour supervisor. If the individual isnot ready forCBRReview IIby
about2months,youandyoursupervisorwillreviewthesituationtogether.Theremaybeone
ormoregoalthatyou,yoursupervisor,theindividualandfamilyagreemayneverbeachieved
despitethebesteffortsofyouall. Ifthishappens,withthepermissionofyoursupervisor,the
individualcanmoveontoPhaseIIwithouthavingachievedthatgoal.Youshouldhoweverstill
continuetosupporttheindividualtoachievethegoalduringPhaseII.Itisnotnecessarytohave
achievedthepersonalgoalbeforemovingontoPhaseII.Yoursupervisorwillbemonitoringthe
progressofeachindividual.
MovingfromPhaseIItoPhaseIII
Once all the Phase II goals have been achieved, you should arrange CBR Review III with the
individual,family,youandyoursupervisor.IftheindividualisnotreadytomovetoPhaseIIIby
about8months,youandyour supervisorwill review thesituation together. If there isagoal
thatyouagreemayneverbeachieved,youcanmoveontoPhase IIIwithouthavingachieved
thatgoal.
Yosef’sstoryAteachvisitBerhanfills inahomevisit form,whichkeeps trackof thegoalsYosef isworkingtowards.

67
13.9 TipsforGoalSetting
• Remember to choose realistic goals with the individual and family. For example, if the
individual is still unwell at the beginning of Phase II, it may be better to choose ‘Taking
medication’insteadof‘Gettingbacktowork’asagoalatthisstage.
• Remindthe individualthat justbecauseagoalhasnotbeenchosenatthisstagedoesnot
meanitwillneverbeaddressed.Youcanaddgoalslater,forexampleinPhaseIII.
• Ifaparticulargoalhasnotbeenachievedyet,keepfocusingontheprogressmade.
• Remember that if you, your supervisor, the individual and family agree that a goal may
neverbeachieved,itisacceptabletomoveontothenextPhaseanyway.
13.10 Summary
• WedoGoalSettingtodecidewhichneedstoaddressandinwhichorder,andtofollowthe
progressoftheindividual
• In Phase I the Goals are the same for everyone. You should decide the order to address
thembydiscussingwiththefamilyandrecordingonthePhaseIGoalSettingForm
InPhases IIand III theGoalsaredifferent foreach individual.Youshouldchoosenomore
thanfiveorsixgoalstofocusonineachPhaseandrecordthemonthePhaseIIorIIIGoal
SettingForm
• ThegoalsyouchoosewilltellyouwhichModulestodeliver

68
14 Riskassessment
14.1 Whatrisksdopeoplewithschizophreniaface?
Suicide
Peoplewithschizophreniaareabouttentimesmore likely tocommitsuicide (kill themselves)
than other people. Suicide is therefore quite a common cause of death in people with
schizophrenia. Themost commonways people commit suicide in rural Ethiopia are hanging,
drowningandswallowingpesticidesorchemicals.
Attemptedsuicide
Attempted suicide iswhere someone tries to kill themselves but does not succeed. This is a
serious warning sign that the person needs urgent help. Suicide attempts are much more
common than suicide, where people succeed in killing themselves. Young women are most
likely to attempt suicide in Ethiopia. People who have attempted suicide are more likely to
commitsuicidelater.
Chainingandtyingup
Peoplewith schizophreniaarequitecommonly tieduporchainedup fromtime to time.This
may take place at the family home, or sometimes at a holywater site or traditional healer’s
home.Thepersonmaybetiedupforaperiodofdaystoweeks,orsometimesmonthstoyears.
SeeChapter7.
Physicalabuse
Peoplewithschizophreniamaybebeatenby familymembers.Sometimes theyarebeatenby
holywaterpriestsorattendantsortraditionalhealersaspartofthetreatment.SeeChapter7.
Emotionalabuse
People with schizophrenia may be treated badly even without being physically abused. For
example,theymaybeshoutedatortreatedinanundignifiedway.Thismaytakeplacewithin
thehomeoroutside.
Sexualviolence
Peoplewithschizophreniaareparticularlyvulnerabletosexualviolence,forexamplerape.This
mayhappenwithinoroutsidethefamilyhome.
Neglect
Sometimespeoplewith schizophrenia are not given enough food, or don’twear any clothes.
Sometimestheyarehomelessandhavenoshelter.SeeChapter7.

69
Riskstochildren
Children who live in a household where a person has schizophrenia may be vulnerable to
neglectorabuse.Thismayhappenbecauseaparent (eitherwith the illnessoracaregiver) is
unabletolookafterthechildproperlyduetoburdenonthefamilyduetotheillness.
Environmentalrisks
Sometimespeoplewithschizophreniaarenotabletolookafterthemselvesaswellasnormal.
Thiscanresultinthembeinghitbycars,fallingoffbuildingsorbeingattackedbywildanimals.
Imprisonment
Somepeoplewithschizophreniagetinvolvedwiththepolice,particularlyiftheyarebehavingin
adisruptiveway,andmayendupimprisonedinajail.
14.2 Whydoweneedtoassessriskinpeoplewithschizophrenia?
Onceweknowthe risks individualsare facingwecan takeaction to try to reduce the risk. In
somecaseswemaysaveanindividual’slife.Inothercases,wemayimprovetheirsituationso
theyhaveabetterqualityof lifeandfinditeasiertogetbacktousualactivities. It isnottrue
that asking about suicidal ideas introduces the idea in the person’s mind. Instead, asking
whetherthepersonhasexperiencedsuicidal ideas is theonlyway to identify risk andprovide
thenecessaryhelptopreventsuicide.
14.3 Howdoweassessriskinpeoplewithschizophrenia?
Inyourworkwithindividualsandfamiliesyoumaybecomeawarethattheindividualisatriskin
differentways,justbylisteningtothemandobservingtheirsituation.Belowyouwillfindsome
specificthingsthatwillhelpyouknowthattheindividual isatrisk. Inaddition,ateveryhome
visityoushouldsensitivelyaskquestionstocheckforsuicideriskandchainingorrestraint.At
each CBR Review your supervisor will do a full risk assessment by asking questions to the
individualandfamily.Youshouldalsobepresentandcontributewhereyoucan.Itmayfeelvery
sensitivetoaskaboutthesetopics.Youcanstartbysaying,“Ineedtoaskyousomequestions
whichmight be difficult or sensitive. Before we start I want to let you know that these are
routinequestionthatweasktoeveryone.”
Suicide
Youshouldasksomequestionstoassesssuicideriskateveryhomevisit.Onewaytostartasking

70
about this is: “How do you feel about life at the moment?” If the individual does not say
anythingverynegative,youcancarryonwiththehomevisitasusual.Iftheindividualsaysthat
they are feeling very negative, or things are going very badly, you should ask some more
questions, such as “I can see you are going through a very difficult period. In your situation,
somepeoplemightfeelthatitisnotworthcarryingonwithlife.Haveyoueverfeltlikethatsince
Ilastsawyou?”
Oryoucanuseotherwaysofaskingthequestion,forexample,
“Haveyoufeltitwouldbebetterifyoudidnotwakeupinthemorning?”
“Haveyoufeltitisnotworthcarryingonwithlife?”
“Have you felt that yourproblems in lifeare toodifficult tobe solvedand that youwouldbe
betteroffdead?”
Iftheindividualsaysyestoanyofthesequestionsyoushouldaskthem,“Have youmade any
plansforharmingyourself?”Thiswillhelpyouknowhowserioustheriskis.
Thefollowingthingsmayalsoindicatetheindividualisatriskofsuicide:
• Anyreferencetodeathordying,inverbalorwrittenexpressionorastrongfocusonan
individualwhocommittedsuicide
• Notbeingwillingtodiscussthetopicandseemingdistressed
• Anystatementsthat“lifeisnotworthliving”
• Impulsiveandpotentiallydangerousbehaviour.Forexampledrinkingalcoholorusingkhat.
Iftheindividualtellsyoutheyhavethoughtaboutsuicide,listencarefullyandrespond
sensitivelyusingyourcommunicationskills(Chapter10).
Chaining
You should assess for chaining at every home visit. It may be obvious that the individual is
chainedoryoumaynoticewoundsorsoresontheindividual.Ifitisnotobviousyoucancheck
byasking:“SinceIlastsawhaveyoubeenchainedorrestrainedathome,ataholywatersite,or
byatraditionalhealerorbyanyoneelse?”
Physical,emotionalorsexualabuseinsideoroutsidethehome
Youmaynoticesignsofphysicalinjurysuchasbruisesorcuts.Youmaynoticethatafamily
membertreatstheindividualinanabusiveway.

71
Neglectandnoteatingordrinking
Youmaynoticetheindividuallooksverythinormalnourished,orthattheyarenotwearingany
clothes.
14.4 Howdowerespondwhenwefindtherearerisks?
RecordanyrisksyoufindontheHomeVisitForm.Followthesesteps.
1. Findoutiftherewereanyparticularcircumstancesorfactorsleadingtotherisk.
2. Discusswithyoursupervisor,thefamilyandindividualimmediateactionsthatwouldbe
helpful.
3. Followtheflowchart(Chapter35)forthesituation.Itwilltellyouthespecificstepsyou
needtotake.Thestepsforsuicideriskandchainingarealsogivenbelow(section14.5).
4. Discusswithyoursupervisor,thefamilyandindividualstepstoreducetheriskinfuture.
5. Followupateveryvisittocheckthesestepshavebeentaken,andiftherehavebeenany
furtherproblems.
14.5 Howdowedealwithsuiciderisk?
Inadditiontothegeneralsteps(Section14.4),ifyouidentifyariskofsuicideyoushouldalways
followthesesteps:
• Checktheindividualistakingtheirmedicationandifnotencouragethemtodoso
• Facilitateaccesstothehealthcentreassoonaspossibleforareview.FillinaHealthCentre
ReferralForm(Form14).
• Informyoursupervisorimmediately,iftheyarenotalreadyaware.
• Iftheindividualdoesnotattendedthehealthcentreafteroneday,makeajointhomevisit
withyoursupervisor.
• Atthishomevisityouandyoursupervisorshoulddiscusswiththefamilyandtheindividual
(ifpossible)thereasonswhytheyhavenotattended.
• Trytoaddressthesereasons,forexample:
o Reiteratetheimportanceofreceivingtreatmentforimprovingsymptoms
o Mobilisecommunityleaderstohelptheindividualtraveltothehealthcentre
o AlsoseeChapter17AccessingHealthServices
• Yoursupervisorwilldoamorein-depthassessmentofsuiciderisk
• YoursupervisorwillthengivediscusstheriskassessmentwiththePsychiatricNurse
72
• Iftheindividualstillhasnotattendedthehealthcentrewithin2days,andtheTrial
PsychiatricNursethinkstheindividualisathighrisktheywillthendoahomevisittoreview
thesituationandimprovethetreatment.
14.6 Howdowedealwithriskofchainingorrestraint?
Inadditiontothegeneralsteps(14.4), ifyou identifyan individualwho ischainedyoushould
followthesesteps(seeChapter19formoredetail):
• Tellyoursupervisorimmediately.
• Checktheindividualistakingtheirmedicationandifnotencouragethemtodoso
• Facilitateimmediateaccesstothehealthcentreforaclinicalreview.FillinaHealthCentre
ReferralForm(FormU).
• Iftheindividualisstillchainedandtheyhavenotattendedthehealthcentreafteroneweek,
makeajointhomevisitwithyoursupervisor.
• Atthishomevisityouandyoursupervisorshoulddiscusswiththefamilyandtheindividual
(ifpossible)thereasonswhytheyhavenotattended.
• Trytoaddressthesereasons
• Iftheindividualisstillchainedandtheyhavenotattendedthehealthcentreafteroneweek,
youshouldinformtheTrialPsychiatricNurse.Theymaydoahomevisittoreviewthe
situationandimprovethetreatment.
14.7 Summary
• Weassessriskstofindoutwhatrisksanindividualfaces,sowecantakeactiontoprotect
them
• YoursupervisorwilldoafullriskassessmentateveryCBRReview.Youshouldasksensitive
questionsaboutsuicideriskandchainingateveryhomevisit
• Whenariskisidentifiedtherearecertainstepsyoushouldfollow.Usuallythisisreferringto
the health centre and informing your supervisor, if they are not aware yet.

73
15 Beingawareofthecaregiver’sneeds
15.1 Whatproblemsdocaregivershave?
AswelearntinChapter5,whensomeonehasschizophreniathiscanputaburdenonthewhole
family.Often theburden fallsononeperson inparticular.Thismaybe the spouse,parentor
child.Itisoften,butnotalways,afemalecaregiverwhotakesmostoftheresponsibility.Female
caregivers may be less likely to get support from other family members or people in the
community. Sometime the stress on this person is so great that they become unwell
themselves.Thecaregivermaydevelopdistress,depressionoranxiety.Someofthesignsofthis
arewhenthecaregiver:
• Complains of many physical symptoms but no physical cause has been found (e.g.
headache,burningsensations,achesandpains)
• Haslowenergy;isalwaystired;hassleepproblemsordoesnotwanttoeat
• Alwaysseemssadoranxiousorirritable;feelshopelessorhelplessorguilty
• Haslowinterestorpleasureinactivitiesthatusedtobeenjoyable
• Worriesorthinksaboutday-to-dayproblemstoomuch
• Isnotableormotivatedtodotheirusualjob,houseworkorsocialactivities
• Hasbeenthinkingofharmingthemselves,e.g.endingtheirlife
15.2 Whyisitimportanttothinkaboutthecaregiversneeds?
Caregivershavetherighttobehealthy,justlikepeoplewithschizophrenia.Also,ifthecaregiver
becomesunwelltheywillnotbeabletolookafterthepersonwithschizophreniaverywell.
15.3 Howshouldwestayawareofthecaregiver’sneeds?
Unlikeforthepersonwithschizophrenia,youdonotneedtodoafullneedsassessmentwith
thecaregiver.However,ateveryhomevisityoushouldthinkabouthowthecaregiverseemsto
begettingon.Caregiverswhoare female,elderly, isolatedor suffering fromaphysical illness
aremorelikelytosufferfromthestressofcaregiving.Lookoutforanyofthesignsthattheyare
distressedordepressed(section15.1).Ifyounoticeanyofthesesignstakethesesteps:
• Ifpossible,trytotalktothecaregiverbythemselves,withouttheindividualpresent.Ifyou
do this, you may need to explain to the individual that you are not talking about them
behindtheirback.Explainthatyoujustwanttocheckhowthecaregiverisdoing.

74
• Askthecaregiverhowtheyfeeltheyarecopingandlistentotheirexperiences.Askifthey
haveanybodytheycanturntoforsupport,forexamplearelativeorneighbour.
• Tellthemitissometimesusefultodiscusstheirproblemswithsomebodyelse.Justbydoing
this,thingscanfeeleasier.
• Iftheyarenotalreadydoingso,encouragethemtojointheFamilySupportGroup(Chapter
32)
• Ifpossible,involvetheothermembersofthefamily.Speaktothemandshareyourconcerns
aboutthestressonthecaregiver.Discusshowtheycantakesomeoftheresponsibilities
• Ifyouareveryworriedaboutthecaregiver,youshouldsuggestthattheygotothehealth
centreforareviewwiththenurseorhealthofficer.Youshouldalsotellyoursupervisor.
15.4 Summary
• Caregivers can become unwell through the stress of looking after a person with
schizophrenia.Itisoftenfemalecaregiverswhotakeonmoreresponsibility.
• They may have physical symptoms, low energy, be very worried, or consider harming
themselves
• Ask the caregiverhow theyare coping. If youare concerned try toensure theygetmore
support, for example from friends and family.
Yosef’sstory
Berhannotices thatAddis sometimes seemssadanddistressed. Sheoften soundshopeless
aboutYosef’ssituation.AddisagreestotalktoBerhanalone.TheybothreassureYosefthat
they are not talking about him behind his back. Addis tells her problems to Berhan. She
admitssheoften feelsunhappyandstressed.Addisagrees to shareherproblemswithher
cousin,whoshetrusts.Addis isalsointerestedinjoiningtheFamilySupportGroupwhenit
getssetup.
75
16 Module:Understandingschizophreniaanditstreatment
16.1 What problems do people with schizophrenia and their families have with
understandingschizophrenia?
Manypeoplewith schizophreniaand their familiesdonot knowverymuchabout the illness.
Somecommonbeliefs,whicharenottrue,include:
• Noonewithschizophreniawillimproveorgetwell
• Medicationcancompletelycuretheillness
• Schizophreniaiscausedbyspiritpossessionorevileye
Mostoftheseincorrectbeliefsarenotharmfulbythemselves.However,somecanbeunhelpful.
Forexample,iftheindividualandfamilybelievetheillnesswillneverimprove,theymaymake
less effort to support the person. On the other hand, if they believe the medication will
completely cure the illness, they may be disappointed when it takes a while to see
improvements.Theindividualmaythenstoptakingthemedicationaltogether.
16.2 Whydopeoplewithschizophreniaandtheirfamilieshaveproblemswithunderstanding
schizophrenia?
People with schizophrenia and their families may have little understanding of schizophrenia
because there was no information available to them. Even if they have been to the health
centre,thenurseorhealthofficermaynothavehadtimetogivetheinformationproperly.
Peoplemayfindtraditionalbeliefsmakesenseandthattraditionalpracticesarehelpful.
16.3 Whyisitimportanttogiveinformationaboutschizophrenia?
Peoplewithschizophreniaandtheirfamilieshavearighttohaveinformationabouttheirillness.
However,thisdoesnotmeanweshouldforcethemtobelieveallofthe informationtheyare
given.Peoplecanhavelotsofdifferentbeliefsatonce.Havingacertainbelief,suchasthatthe
illness iscausedby thedevil,doesnotalwaysstoppeople takingcertainactions, forexample
takingmedication.
Ifpeoplehavemoreinformationaboutschizophrenia,theymayfeelmorepositiveabouttheir
illnessandthatthingsmayimprove.Withthisattitude,theindividualandfamilymaybemore
likelytotakeactivestepstohelprecovery,includingparticipatinginCBRmorefully.Themore
active steps individualsand familiesmake, themore likely theyare togetback to theirusual
activities.

76
16.4 Howdowegiveinformationaboutschizophrenia?
1. Usetheseprinciplesforgivinginformation
Giving information about schizophrenia is an ongoing process. You will need to remind the
individual and family about information you have already given them. Also, the issues the
personfaces,andthereforetheinformationtheyneed,willchangeastimegoeson.Itislikely
thatyouwillinvolveotherfamilymembersapartfromtheindividualandtheprimarycaregiver
whenyougive informationaboutschizophrenia.Whoyouinvolveshouldbedecidedbetween
you,theindividualandthecaregiver.Trytoincludethosefamilymembersthathavepowerand
influencewithinthefamily,alongwiththosewhoarehelpingtolookaftertheindividual.Here
aresomegeneraltipsongivinginformationaboutschizophrenia:
• Givetheindividualandfamilytimetoaskquestionsandpauseaftereachsection
• Encouragethefamilytotellyouiftheydisagreewiththe information
• Bepreparedtodiscussandclarifythe informationwiththefamily.
• Avoidover-loadingthefamilywithtoomuchinformationormedicalterms.
• Use examples fromwhatyouknowaboutthe individual
• Listenandunderstandthefamily’sviewof the illness.
• Besensitivetoanydistressingexperiencesofthefamilymembers
• Tellthefamilyifyoudonotknowtheanswerstotheirquestions.Beforethenextsession,
makesureyoufindouttheanswerbytalkingtoyoursupervisororlookingupthe
informationinthismanual.
2. Explainwhyyouaredoingthismodule
Tellthemwhywouldliketogivetheminformationaboutschizophrenia
3. Assessunderstandingaboutschizophrenia
• Tobeginwith,askwhethertheythinksomethingiswrongwiththeindividual ornot.
• Ifso,askthemwhatdotheythinkthatiswrongwithhim/her?Theyareunlikelytoreport
problems with “hallucinations” or “delusions”. They may instead report the effect of
hallucinationsordelusionsontheindividual’sbehavior. Forexample,thatheorshe laughs
and talks to himself, says things that do not make sense, is not doing well in work or
school, ordoesnotwanttospendtimewithotherpeople.
• Ask if they know what illness the individual has. They may not have been told the

77
diagnosis,oriftheyhave,theymaynotunderstandthedetails.
• Find out about their knowledge about medications. Do they know why medicines are
given?What is the relationship between themedications and the symptoms?What are
thesideeffects of themedication?
• Askiftheythinkmedicationcanmakethembetterorworse.
• Askwhatthey thinkabouthowlongthe illnesslasts. Somefamilies expect the illness to
becuredwithmedication.Theymaynotbeawarethattheremaybemanyepisodes.
• Finally,askwhatthey thinkabout thecauses ofthe illness.Most familymemberswillnot
consider mind problems as being themain cause. They may wonder if they are being
punished for something they didwrong, and therefore feel guilty, angry or responsible.
Some family members may think that “evilspirits”causeit.Parentsmaywonder ifithas
been inherited andmay blame the other spouse if they have a relative with a mental
illness.
4. Giveinformationabouttypicalsymptomsofschizophrenia
• Explaineachsymptomgroupinturn(hallucinationsanddelusions,problemswith
motivation,problemswiththinkingclearlyandnotunderstandingtheyareunwell)
• Useexamplesfromthe individual’sbehaviour tohelpexplain
• Tell the family that each individual has a different symptom pattern and will have
different symptoms at different times. This is important, as family members may not
listentoyouwhenyoudescribesymptomsthattheindividualdoesnothave.
• Emphasizethatthehallucinationsanddelusionscannotbeeasilyunderstood.Theyare
thoughts, ideas,andvoicesthatgo in insidethe individual’shead.Thefamilycanon ly
seetheireffects throughthe individual’sbehavior.
• Emphasize that the symptoms are real to the individualand they cannot control them.
Forexample,theycannothelpbutanswerthevoicestheyhear.
• Emphasize thatproblemsofmotivationandproblemswiththinkingclearly cannotbe
easily overcomebythe individual.
5. Thecausesofschizophrenia
• Explainthatbothstressandvulnerabilityareusuallyneededforapersontodevelop
schizophrenia,butsometimeswedon’tknowwhyapersondevelopstheillness.Give
78
examplesofstressandvulnerability.Whendiscussingvulnerability,donotemphasisethat
havingaclosefamilymemberwithschizophreniaincreasestherisk,asthismaybe
stigmatising.Instead,focusondifficultearlylifeexperiences.
• Familiesusuallyhavetheirownbeliefsaboutthecauseoftheillness.Youshouldlistento
theseideas.Itispossibletohavemorethanonebeliefaboutthecause.
• Familymembersmay thinktheycausedor couldhavepreventedthe illness insome
way. Theseideasmakethefamilyfeel guiltyanddepressed.Youshouldreassurethe
familythattheydidnotcausetheillness.
• Ifthefamilyasksyou,youcantellthemthattheirchildrenwillmostlikelyNOTdevelopthe
illnesstoo.
6. Courseofschizophrenia
• Inform them that there are good chances individual can recover from an episode and
have anearnormallife.
• Alsotellthemthattheillnessmaycomeback(relapse),evenoncetheyhavestartedtofeel
better.Describesomeofthesignsthatarelapseiscoming(e.g.problemswithsleep,
feelingangryoranxious).Totryandstopthishappeningtheyshouldcontinuemedication
allthetime.Howeversometimesthingsoutoftheindividual’scontrolwillhappene.g.
physicalillnessorlifestress,whichmaytriggertheillnesstocomeback.Iftheillnessdoes
comebackitisimportantnottogiveuphope.
7. Howcommonisschizophrenia
• Tellthemabout10peoplehaveschizophreniainanaveragekebele.Youdon’tneedtogive
themtheexactnumberforthekebeletheylivein.
8. Medication
• Whatarethemedicinesfor
Tell them medication may reduce symptoms, prevent relapse and improve the chances of
recovery.
• Howdo theywork
Tell them the medication works by improving theway themindworks and prevents it from
gettingsickagain.Theresultofthiswillbefewer hallucinationsanddelusions.
79
• Whatisthenameofthemedicationthathasbeenprescribed?
• Whatarethecommonsideeffects
• Regularmedication
Discusswith the familyandemphasize the need for takingmedication regularly.Thereis
aseparatemoduleforsupportwithtakingmedication(Chapter20).
• Continuingmedication
Emphasize thatmedication will need to be taken for a long period of one to two years or
evenforever. Thedurationofthetreatmentdependsonhowwelltheindividualisrecovering
andnotonhowlongthe illnesswastherebefore the treatmentstarted.
• Addressconcerns
Some families think that the medications are addictive if used for a long time. The family
maythendecidethattheindividualshouldlearntocopewithoutthemedication.Thisviewis
notcorrect.Beclearthatthemedicinesarenotaddictive.
9. Stress-vulnerabilitymodel
• Explainthatbothreducingstressandtakingmedicationcanhelpreducerelapsesandhelp
thepersontorecover
• ExplainthatotherpartsofCBRcanhelpreducestress,forexampleimprovingthefamily
environment,reducingstigmaanddiscrimination
Followup
• Bepreparedtoremindthefamilyoftheinformationatlaterhomevisits
• Lookuporaskyoursupervisoranyquestionsthatyoudidnotknowtheanswerto.Givethe
individualandfamilytheinformationatthenexthomevisit
Yosef’sstory
Berhanexplainswhatthesymptomsofschizophreniaare,referringbacktoYosef’sproblems.
Sheexplainsthecausesofschizophreniaandtheimportanceofmedication.Addisisstillsure
thatYosef’sillnesswascausedbyspiritpossession,butshecanalsoseethatthemedication
isuseful.Addisdoesnot trytochangeAddis’beliefsaboutspiritpossession.Yosef’s family
havelotsofquestionssoittakestwovisitstocoveralltheinformation.

80
16.5 Summary
• Manypeoplewithschizophreniaandtheirfamiliesdonotknowmuchabouttheillness
• If people with schizophrenia knowmore about their illness they are more likely to take
positivestepstowardsrecovery
• You shouldgive the following informationabout schizophrenia: typical symptoms, causes,
course,howcommon it is,medication(names,sideeffects, importanceof takingregularly
and continuing once well) and the stress-vulnerability model.

81
17 Module:Improvingaccesstohealthservices
17.1 Whatproblemsdopeoplewithschizophreniahaveaccessinghealthservices?
Therearethreelevelsofhealthservicesthatareavailableforpeoplewithschizophrenia.
1. Healthcentre
NursesandhealthofficersinSodoworedaaretrainedtolookafterpeoplewithschizophrenia.
Nearlyallthemedicalcareforindividualstakesplaceinhealthcentres
2. ButajiraOutpatientClinic
Psychiatric nurses at Butajira have expert knowledge about schizophrenia. Sometimes health
centrestaffwillsendindividualsherewhentheyareveryunwell.
3. AmmanuelHospitalinAddisAbaba
Psychiatrists (doctors with expert knowledge on mental illness) look after people with
schizophreniaatAmmanuelHospital.Rarely,anindividualwillbesentherewhentheyarevery
unwell.
Problemsaccessinghealthservices
Sometimespeoplewithschizophreniahavedifficultygettingtothehealthcentreorhospitalto
getthetreatmenttheyneed.Thismaymeanthateventhoughtheindividualiswillingtoseethe
nurseorhealthofficerandtotakethemedication,theyarenotableto.
17.2 Whydopeoplewithschizophreniahaveproblemsaccessinghealthservices?
There are various reasons why people with schizophrenia have problems accessing health
services.Theseinclude:
• Thefamilycannotaffordthemedication
• Thefamilycannotaffordtotraveltothehealthcentre
• Thereisnobodytogowiththeindividual
• Itisdifficulttotaketheindividualtothehealthcentrebecausetheyareunwelloritisfar.
• Themedicationisnotalwaysavailableatthehealthcentre
• Theindividualischainedupathome
Insomecasestheindividualisabletoaccesshealthservicesbutchoosesnottobecausetheydo
notwanttoreceivetreatment.

82
17.3 Whydoweneedtoimproveaccesstohealthservices?
Gettingaccesstothehealthcentre isessential forrecoveryfromschizophrenia.Atthehealth
centretheindividualisreviewedbyanurseorhealthofficerwhowill:
• Checkoverallprogress
• Prescribethemedicationorgivetheinjection.Peoplewithschizophrenianeedtotaketheir
medicationregularlyinordertofeelbetterandgetbacktousualactivities(seeChapter20)
• Checkforandtrytoimprovesideeffects
• Changethedoseofthemedicationifitisnotenoughortoomuch
• ReferthemtoButajiraoutpatientcliniciftheycannotmeetallindividual’sneeds
Howoftenpeoplewith schizophrenianeed to attend thehealth centredependsonhowbad
their illnessisatthattime.Usuallytheyneedtoseeanurseorhealthofficerandcollecttheir
medicationevery1-3months.
17.4 Howcanweimproveaccesstohealthservicesforpeoplewithschizophrenia?
1. Informthefamilywhathealthservicesareavailable
2. Explainwhyyouaredoingthismodule
Explaintheimportanceofaccessinghealthservices.
3. Assessproblemswithaccessinghealthservices
Findoutwhatthecurrentarrangementsforaccessingmedication.Thenassessanyreasonswhy
the individual has problems accessing health services, or might do in the future. Use the
potential reasons above (Section 17.2) as a starting point. If the individual is able to access
services but does notwant to, youmayneed to completeModule: Supporting Individuals to
TakeMedication(Chapter20).
4. Useproblemsolvingtoimproveaccesstohealthservices
You should then discuss each reason or problem in turn with the individual and caregiver.
Encouragethemtothinkofideasforhowtogetaroundtheproblemusingtheproblemsolving
approach (Section10.5).Discuss the approaches theyhavealready tried.Buildon their ideas
and then suggest some of your own if everything has not been covered. Some or all of the
followingmethodscanbeused.

83
a. Exploreaccessingfreemedication
Acertificateforfreemedicationcanbegivenbythekebeleadministrationtothe‘poorestofthe
poor’.Only5 inevery1000 families can receive this certificate, thereforenotall peoplewith
schizophreniawillbeeligible.However,ifyouthinkthatthefamilyisamongstthepoorestinthe
kebeleand theydonotalreadyhave the certificate, you should take someaction. Firstof all
encouragethefamilytoapproachthekebeleleadersandrequestthiscertificateforthemselves.
Discusswiththecaregiversthekindofthingstheymightsay.Ifthisisunsuccessful,youshould
approach the kebele leader yourself and request that the family receives the certificate. See
Task8intheCommunityEngagementchapter.
b. Maketravellingtothehealthcentreeasier
Discusspotentialsourcesofhelpfortravellingtothehealthcentre.Thismayincludeextended
familymembers, neighbours or community leaders. Theymaybe able to givemoney for the
transport costs, or help to accompany the individual, along with family members, on the
journey. If the family is unable to find additional support themselves, you couldmeetwith a
communityleaderandaskfortheirhelp.SeeTasks8,9and10intheCommunityEngagement
chapter. You are not normally expected to accompany the individual to the health centre
yourself,exceptforaroundthetimeoftheCBRReviews.
c. Addressfinancialproblems
Poverty is a long-term problem, which may to be difficult to improve over the course of
receiving CBR.However, financial problemsmaybe addressed to someextent by getting the
personwithschizophreniabacktowork(SeeChapter27).Rememberyoushouldnotpayforthe
individual’smedicationyourself.
5. Discussdeliveringmedicationtotheindividual’shome
Youshouldonlydiscussthis iftheindividualorfamilysuggests it.YouortheHealthExtension
Worker taking themedicine from thehealth centre to the individual’shome shouldbea last
resortwhenalltheotherrelevantmethodshavebeentried.Thereasonforthisisthatitisnot
anempoweringorsustainablewaytoensurethepersontakesmedication.Fordeliverytothe
home to be considered, the individual should be very unwell and not attending the health
centre.Discussthiswithyoursupervisor.

84
6. Monitorwhethertheindividualattendsthehealthcentre
Eachindividualshouldgotothehealthcentreevery1to3months.Youshouldbeawareofall
the appointments they have, and check if they have attended. If they have missed an
appointment,evenifyouarenotdueforahomevisit,youshouldmakeahomevisittocheck
foranyproblemsandremindthemtoattend.Iftheindividualchoosesnottoattendthehealth
centre you should discuss the potential benefits of treatment but also listen to their own
wishes.
7. Makeaplan
Attheendofthediscussion,makesurethateverybodyknowswhatinputtheyareexpectedto
have.
Followup
Remembertocheckwhatprogresshasbeenmadebythenexthomevisit.
If you agreed to do so, discuss free medication certificate with kebele leader or support
travellingtothehealthcentrewithcommunityleader/s.
17.5 Summary
• Someindividualsdonotaccesshealthservicesduetomoneyortransportproblems
• Itisimportanttoaccessthehealthcentretogettreatment,asthismayimprovethechance
ofrecovery
• Waystoimproveaccessinclude:exploringthepossibilityoffreemedication,makingtravel
to the health centre easier, and improving financial problems.
Yosef’sstory
Addis tells Berhan that sometimes they can’t get to health centre because Yosef is too
unwelltowalkthere.Thismakesthingsworseasthenhecan’tgetthemedication.They
agreethattogetoverthisproblemtheyneedhelptogettothehealthcentre.Theydiscuss
whocouldhelp.AddisagreestoaskherunclesandcousinstohelpwalkorcarryYosefto
mainroad.Theywillthengetagariusingsmallamountofmoneyborrowedfromuncle
85
18 Module:Preparingforacrisis
18.1 Whatkindsofcrisesdopeoplewithschizophreniahave?
AswelearntinChapter14,peoplewithschizophreniaarevulnerabletomanysortsofrisks.A
crisisiswhendangerousorworryingincidentshappenasaresultoftheserisks.Somecommon
typesofcrisisinclude:
• Theindividualtalksaboutortriestocommitsuicide
• Theindividualisthevictimofphysical,emotionalorsexualabuse
• The individual behaves in a dangerous way. For example they consume poisonous fluid
thinkingitwouldn’thurtthem,ortheyjumpoffaroof.
• Theindividualthinksthefamilyorhealthworkeristryingtoharmthemandtriestoprotect
themselvesinanaggressiveway.
• Theindividualdoesnotwanttoeatordrink
Theindividualmayfeelscaredandalone.Thefamilymaynotknowhowthebestwayto look
aftertheindividual,andmayfinditdifficulttocope.
18.2 Whydopeoplewithschizophreniahavecrises?
Manytypesofcrisishappenduetotheillness.Forexample,behavinginanunpredictableway
or thinking others are trying to harm them may be due to hallucinations or delusions
(experiencing or believing things that aren’t true). These are all likely to beworsewhen the
individualishavingarelapse(whentheillnessgetsmuchworse).Othertypesofcrisisaredueto
stigmaorotherexternalfactors.Forexample,beingbeatenattheholywater.Althoughthese
thingscanhappenatanytime,theyarealsomorelikelytohappenwhentheindividualisvery
unwell.
18.3 Whyisitimportanttoprepareforacrisis?
InChapter14youlearnthowyoushouldrespondwhenyouidentifytheindividualisatrisk.We
alsoneedtogivefamiliesadviceonhowtodealwithacrisiswhenoneoccurs.Itisgoodtogive
thefamilyskillstodothisbecausetheyarethemaincarers,andtheyneedtoknowhowtocope
whenyouarenolongervisitingthem.Beingwellpreparedforacrisishelpstoavoidaseriousor
undesirableoutcome,forexampletheindividualhurtingthemselvesorsomeoneelse,orbeing
chainedup.
86
18.4 Howdowehelpindividualsandfamiliestoprepareforacrisis?
Principles
It isgoodtostartpreparing foracrisiswhenthe individual iswellenoughtotakepart in the
discussions. This gives the individual more control over the situation. Be aware that talking
aboutfutureorpastcrisesmaybeupsettingfortheindividualandfamily.
1. Discusswhatkindsofcrisisarelikely
Asktheindividualandfamilytothinkofcrisesthathavealreadyhappenedormighthappenin
thefuture.Usetheexamples inSection18.1tohelpthemtothinkabout it.Discusshowthey
willknowifacrisisishappeninge.g.theindividualstopstakingmedicationorbecomesangryor
upset.
2. Explainwhyyouaredoingthismodule
Explainwhyyouwouldliketohelpthemtoprepareforacrisis.
3. Decidewhotoaskforhelp
Asktheindividualandfamilytodecidethreepeopletocallforsupportinacrisis.Tellthem
tokeep their phone numbers in morethanoneplacesotheydon’tlosethem.Thepeople
mightinclude:
• Arelative
• Aneighbour
• Acommunityorreligiousleader
• TheCBRworker.Remindthemthatthiswon’tbepossibleonceCBRhasfinished
4. Makeacrisisplan
Decidetogetherwhatactionsthefamilyshouldtakewhenthereisacrisisandrecordthese
ontheCrisisManagementPlan(Form22).Thismightincludethefollowing:
a) Trytomakesuretheindividualistakingthemedication
b) Taketheindividualtothehealthcentreforareview.Tellthefamilytomakesuretheyare
clearaboutwhattheplanisandwhattodonext.Tellthefamilytoinformyouorthehealth
centrestaffaboutviolentbehaviour,discussionaboutdeathorsuicideandanybeliefsthat
otherpeoplearetryingtoharmthem
87
c) Contacttherelative/neighbour/leader.Justbringingsomeoneelseintothehometoassessthe
situationmaybeuseful.Theymayalsohelpwithgettingtothehealthcentreifthisisdifficult.
d) Removeaccesstoweaponsandpotentiallypoisonousmaterials
e) Maketheenvironmentsafeandcomforting.Givetheindividuallotsofspace.
f) Removeallaccesstoalcoholandkhat.
g) Encouragetheindividualtoputstrongfeelingsandenergyintosafeactivitiestheyenjoy,
suchaslisteningtotheradio
h) Suggesttheindividualtriesrelaxationtechniques(SeeSection23.4)
5. Discusshowthefamilyshouldtreattheindividualduringacrisis
• Useacalm,positivebutfirmtoneofvoice.
• Usesimplelanguage
• Givetheindividualextratimetorespondandtocalmdown
• Reduceexpectationsaboutworkorhouseholdtasks
6. Discusswhatactionsarenotusuallyhelpful
• Thefamilyshouldtrynottoarguewiththeindividual.Thiswillonlymaketheperson
confusedand frustrated.Insteadthefamilyshouldbeloving.Thefamilyshouldn’tdisagree
with delusions.It’soktotellthepersontheydon’tseethingsthesamewayandleaveitat
that.
• Thefamilyshouldnotacceptviolencefromthe individual.The individualshouldbeclearly
toldthatthisbehaviourisunacceptable.
• Theyfamilyshouldnotbeviolenttowardstheindividualandshouldtrytoavoidrestraining
them.
7. Makeaplantodealwiththecurrentcrisis,ifthereisone
Followup
If there iscurrentlyacrisis,makesureyoufollowuponwhathashappenedandwhetherthe
stepshelpedatthenexthomevisit.
88
18.5 Summary
• It iscommonforpeoplewithschizophreniatohavecrisessuchasdangerousbehaviouror
thinkingaboutsuicide
• Itisimportanttoprepareforacrisistoavoidseriousoutcomessuchasgettinghurtorbeing
chained
• Waystoprepareforacrisis include:decidingwhotoaskforsupport,makingacrisisplan,
andthinkingaboutwaystotreattheindividualduringthecrisis.
Yosef’sstory
YosefandAddisagree that themost likely crisis is that Yosefwill becomeunwell and run
away, like hashappened in the past. They agree that if a crisis happensSolomon (Yosef’s
father)willasktheiruncleforhelp.Theymightalsoaskthelocalpriest,whoseopinionthey
respect. Berhan writes down the crisis plan. The family cannot read but they appreciate
Berhanhavingtheplanwrittendown.ThismeanstheycanlookbackatitlaterwithBerhan.
Yosef’sCrisisManagementPlan
• CheckifYosefistakingthemedication.Gentlyencouragehimtostarttakingitagainifhehasstopped.
• Gotothehealthcentreforareview,withthehelpoftheuncle.• TellthelocalpriestifYosefhasrunaway,incasehecanhelptofindhimandbring
himhome.• IfYosefisstillathome,makesurehehassomespacetohimself.• Makesurethereisnoalcoholorkhatinthehouse.
89
19 Module:Dealingwithhumanrightsproblems
19.1 Whathumanrightsproblemsdopeoplewithschizophreniaexperience?
All people, including all people with schizophrenia, have the same human rights. Quite
commonly peoplewith schizophrenia are denied their human rights.We have already learnt
aboutsomehumanrightsproblems inChapter7,and inChapter14as theyarealso typesof
risksandcrises.Thehumanrightsproblemsexperiencedbypeoplewithschizophreniainclude:
• Chainingandrestraint
• Neglect
• Physicalabuse
• Sexualviolence
• Notaccessinghealthservices
Manypeoplewithschizophreniafinditdifficulttoaccesshealthserviceseitherfortheirmental
illness or for physical health problems (see Chapter 17). On some occasions people with
schizophreniaareactuallyexcludedfromgettingthesamelevelofhealthcareaspeoplewhodo
nothavementalillness.
• Notbeingabletoworkorgetmarried
Sometimespeoplewithschizophreniacannotdousuallifeactivitiessuchasworkingorgetting
marriedbecausetheyaretoounwell.Justasoften,individualsfinditdifficulttodothesethings
duetostigmaanddiscrimination(seeChapter6).
19.2 Whydopeoplewithschizophreniaexperiencehumanrightsproblems?
• Duetobeingunwellandthefamilynothavingenoughsupport
Peoplewithschizophreniamaygetmentallyunwellfromtimetotime.Thiscanhappenbecause
theyarenotaccessingtreatmentorbecausethemedicationisnotsufficienttohelpthem.
Duringthesetimes,ifthefamilyhaslittlesupporttheymayfeeltheyhavenochoicebutto
restraintheindividual.Usually,theyaretryingtoprotecttheirfamilymemberfromrunning
awayandbeingharmedinanaccident,orbyotherpeople.Oftentheyarealsoconcernedthat
theindividualmayharmotherpeopleordamageproperty.Whenapersonisunwellwith
schizophreniaandthefamilydoesnothaveenoughsupportitalsobecomesmoredifficultfor
thefamilytolookafterthemproperly.Itbecomesdifficulttokeeptheindividualfedand
clothed.Itcanthenbecomemoredifficulttogetthemtothehealthcentre,whichmakesallthe
problemsworse.

90
• Nottakingmedication
When a person with schizophrenia is not taking their medication, the family may resort to
secretlygivingthemedication(forexamplemixedintofood),tyinguporphysicallyforcingthe
individualtomakethemtaketheirmedication.Thepersonmayalsobetiedupinordertomake
thejourneytothehealthcentreorhospital.
• Stigmaanddiscrimination
Manypeopledon’t knowverymuchabout schizophrenia. Theymaybelieve thatpeoplewith
schizophreniaarealwaysviolent,orthattheyarepossessedbythedevil.Thesekindsofbeliefs
can leadpeople to treat thosewith schizophreniabadly, suchasbybeating themor keeping
themtiedupevenwhentheyarewell(SeeChapter6).
• Traditionalandreligioushealing
Most traditional and religious healing does not harm people with schizophrenia. However,
sometimeswhenaperson refuses to takeholywater, theymaybebeatenor tiedupso that
they can be forced to take thewater or bathe in it. Also, some traditional healing practices
include physical abuse such as branding, beating and fumigation. All of these things make
schizophreniaworse,andareanabuseofhumanrights.
• Nohealthservicesavailable
Oftenthereasonwhypeopledonotgetmedicalcareforschizophreniaisbecausethereisnone
availablelocally,oritistoofarortooexpensiveforthemtouse.
19.3 Whyisitimportanttoreducehumanrightsproblemsinpeoplewithschizophrenia?
Peoplewithschizophreniahavethesamehumanrightsasallpeople,soweshouldensurethey
areprotected.Reducinghumanrightsissuesisalsoanimportantwaytohelptherehabilitation.
Whilsttheyaretiedup, individualscannotbegintoundertakeusual lifeactivities likewashing
and dressing, drinking coffee and doing farmwork. Treating people with schizophrenia with
dignityandrespectwillimprovetheirself-esteemandconfidenceandmakeitmorelikelythey
willgetbacktotheirusualactivities.Thisinturnreducestheburdenonthefamily.
19.4 Howcanwereducehumanrightsproblemsinpeoplewithschizophrenia?
Principles
OneofthemainaimsofCBRistoreducehumanrightsproblems.CBRcandothisby:
• Improvingaccesstohealthservicesforphysicalandmentalhealth(seeChapter17)
91
• Improvingunderstandingaboutschizophreniaandchangingnegativeandincorrectbeliefs
amongstthefamily(seeChapter16)andcommunity(seeChapter31)
• Improvingself-care(Chapter24)andnutrition(seeChapter21)
• Improvingthefamilyenvironment(seeChapter25)thereforereducingthelikelihoodof
emotionalandphysicalabuse.
Therearealsospecificstepswecantaketoreducehumanrightsproblems.Rememberthat
discussinghumanrightsproblemsmaybeupsettingfortheindividualandfamily.Besensitiveto
thisandbereadytotakeabreakfromthediscussionsifnecessary.
1. Explainwhyyouaredoingthismodule
Explainwhathumanrightsare,andthatpeoplewithschizophreniahavethesamerightsas
otherpeople.Explainwhyitisimportanttoprotectthehumanrightsofpeoplewith
schizophrenia.
• Theindividualcannotbegintogetbacktousualactivitieswhilsttiedup
• Treatingtheindividualinadignifiedwaywillimproveself-esteemandmakeitmorelikely
theywilldousualactivitiesagain
2. Assesshumanrightsproblems
Youshouldbeginbydiscussingwhathumanrightsissuestheindividualhasfacedinthepast,or
present ormay face in the future. You should also refer back to the risk assessment,where
humanrightsissuesmayhavebeenidentified(seeChapter14).
3. Educatethefamilyaboutchainingandphysicalabuse
Advisethefamilythatchainingisnotdesirable,evenifthishasn’thappenedtotheindividual.
Usethereasonsgivenabove(seeSection19.3)forwhyitshouldbeavoided.
4. Useproblemsolvingtoreducehumanrightsproblems
You should then discuss each human rights issue in turn with the individual and caregiver.
Encouragethemtothinkofideasforhowtoavoidtheissueinfutureusingtheproblemsolving
approach(seeSection10.5).Discusstheapproachestheyhavealreadytried.Buildontheirideas
and then suggest some of your own if everything has not been covered. Some or all of the
followingmethodscanbeused.

92
a. Helpindividualstotaketheirmedicationandreducerelapse
UsethestrategiesinChapters20and30tosupportindividualstotakemedicationandreduce
relapse.Thesewillhelpavoidsituationswheretheindividualbecomesunwellandthefamily
turntochaining.
b. Helpfamiliestodealwithviolenceandcrises
Givingthefamilystrategiestodealwithviolencefromthepersonwithschizophrenia,andother
crisessituations,willhelpthemtoavoidresortingtochaining.SeeChapter18.
c. Educatecommunitymembersandcommunityleaders
Partoftheawareness-raisingforcommunitymembersandcommunityleadersshouldbethat
restraintshouldnotbeusedexceptinanemergency(seeTasks5and6intheCommunity
Engagementchapter31).Askthefamilyifthereisanyparticularindividualwhowouldbenefit
fromeducationaboutchainingorphysicalabuse.
d. Educatingholywaterpriests,attendantsandtraditionalhealers
Holy water priests and attendants and traditional healers may be involved in your general
communityawarenessraising.Ifnot,andyoufeelthereareparticularproblemswithpriestsor
attendants you have identified, you may need to undertake specific meetings with these
individuals.Askthefamilyifthereisanyparticularindividualwhowouldbenefitfromeducation
aboutchainingorphysicalabuse.Theaim is toencourage themtoavoidchainingorphysical
abuseduringtheirhealingpractices.SeeTask11inCommunityEngagementChapter31.
5. Whattodoifsomeoneischained(seealsoChapter14)
Ifanindividualischainedwhilstyouareworkingwiththefamilyfollowthesesteps:
• Tellyoursupervisorimmediately.
• Facilitateaccesstothehealthcentreforaclinicalreview.Askthefamilytotakethe
individualassoonaspossible.
• Iftheindividualisstillchainedandtheyhavenotattendedthehealthcentreafteroneweek,
makeajointhomevisitwithyoursupervisor.
• Atthishomevisityouandyoursupervisorshoulddiscusswiththefamilyandtheindividual
(ifpossible)thereasonswhytheyhavenotattended.

93
• Trytoaddressthesereasons,forexample:
o Repeattheimportanceofreceivingtreatmentforimprovingsymptoms
o Mobilisecommunityleaderstohelptheindividualtraveltothehealthcentre
o AlsoseeChapter17
• Iftheindividualisstillchainedandtheyhavenotattendedthehealthcentreafteroneweek,
youshouldinformtheTrialPsychiatricNurse.
Unchaining
Donottellthefamilytounchaintheindividualwithoutsupportfromyoursupervisorandthe
healthcentre.Thedecisiontounchainshouldbemadebythefamily,preferablyindiscussions
withthehealthcentre.
6. Reducingharmfromchainingwhenitoccurs
Despite the best efforts of you, the family and the individual, sometimes the individualmay
becomesounwellthatthefamilystillfeelsthebestoptionistotieuptheindividual.Youshould
informyoursupervisorandfacilitatetheindividualtoattendthehealthcentreforareview.You
should not encourage chaining, however you can offer the following advice to the family to
ensurethatchainingisassafeanddignifiedaspossiblewhenitdoesoccur.
• Makesuretheindividualisinashelteredpositionnotexposedtothesunandrain.
• Makesuretheindividualhassomeclothingand/orblanketstokeepwarm
• Makesuretheindividualisofferedregularfoodandwater.Helpandencouragementshould
begiventoeatanddrink.
• Ifpossible,allowtheindividualtobeunchainedeverydaytowalkaround
• Changethepositionofthechains/restraintasoftenaspossible,toensuretheindividualis
notalwayssittingorlyinginthesameposition
• Checkregularlyforwoundsorsorescausedbythechains/restraint,orbylyinginthesame
positionforalongtime.Carefullywashanywoundsorsoreswithcleanwater.Changethe
positionofthechainstoallowthewoundstoheal.
• Continueinteractingwiththeindividualandinvolvingtheminconversation
• Iftheindividualbecomesphysicallyunwell,takethemtothehealthcentre
7. Whattodowhenotherhumanrightsabusesoccur
94
• Neglect.SeeChapter35.
• Physicalabuse.SeeChapter35.
• Sexualviolence.SeeChapter35.
• Notaccessinghealthservices.CompleteModule:ImprovingAccesstoHealthServices
(Chapter17).
• Notbeingabletoworkorgetmarried.ConsidercompletingModules:Gettingbacktowork
(Chapter27),Takingpartincommunitylife(Chapter26)orDealingwithStigmaand
Discrimination(Chapter28)dependingonthesituation.
8. Makeaplan
Attheendofthediscussion,makesurethateverybodyknowswhatinputtheyareexpectedto
havebeforethenextsession.
Followup
Checkwhatprogresshasbeenmaderelatingtohumanrightsproblemsatthenexthomevisit.
19.5 Summary
• Quitecommonlypeoplewithschizophreniaaredeniedtheirhumanrights,forexamplethey
arechainedorphysicallyabused.
Yosef’sstory
InthepastwhenYosefwasveryunwellAddisandSolomonfeltitwasnecessarytochain
Yoseftothehouse.Thekebelechairpersonalsotoldthemitwastheirresponsibilitytothis,to
protectotherpeopleandpropertyinthekebele.YosefandAddisfinditupsettingtotalk
abouthimbeingchainedup.Berhantellsthefamilythatsheunderstandsthattheywereonly
tryingtohelpYosefandprotectotherpeoplewhentheychainedhimupinthepast.
However,itisimportanttotrytopreventthishappeninginthefuture.Thefamilyagreethat
themainwaytoavoidchainingistoensureYoseftakeshismedicationregularly.Theyagree
thatinthefuturetheywillcompletetheModule:Supportingindividualstotakemedication.
SolomonandAddisfeeltheycannothaveanyinfluenceonthekebelechairperson.Berhan
agreestodiscusstheissuewithhim.Berhanalsogivesthefamilyadviceonhowtochain
Yosefinawaywhichisasdignifiedassafeaspossible,incasetheyeverneedtodoitasa
lastresort.

95
• Respectingthehumanrightsofpeoplewithschizophreniaisempoweringandmakesitmore
likelytheywillgetbacktousualactivities.
• You can reduce human rights problems by: educating the family, supporting adherence,
helping families to deal with crises, and educating community leaders and traditional
healers.
• Therearewaystoreducetheharmfromchainingwhenitdoesoccur.
.
96
20 Module:Supportingindividualstotaketheirmedication
20.1 Whatproblemsdopeoplewithschizophreniahaveintakingtheirmedication?
Some people with schizophrenia refuse to take any treatment from the beginning. More
commonly,peoplestartthemedicationbutthenstoptaking itregularly,orstop italtogether,
overaperiodoftime.
20.2 Whydosomepeoplewithschizophrenianottaketheirmedication?
Individualfactors
• Insufficientsupportfromthefamily
• Theindividualfeelsshameorstigmafromtakingthemedication,especiallyiftheynolonger
havesymptomsandwishtobeseenaswell
• Theindividualand/ortheirfamilybelievethattheillnessisduetospiritpossessionorother
causes,andthatmedicationwillnothelpthis.
• Theindividualand/ortheirfamilyunderstandthatmedicationhelpstorelievesymptomsin
theshorttermbutdonotunderstandthe importanceofmedicationtopreventthe illness
comingback.
• Holy water priests or attendants or traditional healers tell the individual that it is not
needed,orevenharmful,totakemedicationwhilstreceivingtraditionaltreatment
Illnessfactors
• People with schizophrenia may not understand that they have an illness that needs
treatment.Becauseoftheirillness,theymayevenbelievethatthetreatmentisbeinggiven
tothemtoharmthem.
• Peoplewithschizophreniaoftenhavelowlevelsofmotivation
• Peoplewithschizophreniaoftenhavelowlevelsofattentionandconcentration
• Thepersonmayalsobeusingkhatoralcohol.Thismaymake them lessorganisedor less
interestedintakingmedication.
Treatmentfactors
• Themedicationcausesunpleasantsideeffectsinthepersonwithschizophrenia
• Thepersonwithschizophreniadoesnothaveenoughfoodtocopewithfeelingmorehungry
thanusualasaresultofthesideeffectsofthemedication
• Thepersonwithschizophreniadoesnothaveagood,trustingrelationshipwiththenurseor
doctorprescribingthemedication

97
• Themedicationhastobetakenonacomplicatedschedulesothepersonwithschizophrenia
forgetstotakethemedication.
• Themedicationdoesnotcompletelycuretheillnesssotheindividualdoesnotseethepoint
intakingit.
Practicalfactors(seeChapter17)
• Thefamilycannotaffordthemedication
• Thefamilycannotaffordtotraveltothehealthcentre
• Itisdifficulttotaketheindividualtothehealthcentrebecausetheyareunwelland/oritis
toofar.
• Thereisnoonefreetotaketheindividualtothehealthcentre.
• Themedicationisnotalwaysavailableatthehealthcentre
20.3 Whyisitimportanttotakemedicationregularly?
It is important to take medication regularly to treat the illness so that the person with
schizophreniastartsfeelingbetter.Whenindividualstakemedicationtheyaremorelikelytobe
abletogetbacktousualactivitieslikefarmworkandhousework.Oncetakingthemedication,it
also ismuch less likely that the individualwill be so unwell that the family needs to restrain
them up. It is very important to continue to take medication, even after the person with
schizophreniaisfeelingwellagain.Thisistopreventtheillnessfromcomingback.Iftheillness
comesbacktheindividualmaystopbeingabletoworkandsocialiseagain.Eventhoughthere
are somedisadvantages to takingmedication, forexample the sideeffects,mostpeoplewith
schizophreniafeelonbalancethatlifeisbetterwhentakingthemedication.
20.4 Howcanwesupportpeoplewithschizophreniatotaketheirmedication?
Principles
• Thereisnotonesingleapproachtohelpingpeopletotaketheirmedication.Oftenarange
ofmethodsisneededforeachindividual.
• Whichmethodsyouusedependsontheirsocialandpersonalcircumstances
• Whensomebodydoesnottakehisorhermedication,itisusuallynotaproblemthatcanbe
quickly ‘solved’. Thismeansongoing input isneeded,usually for thedurationof receiving
CBR.
• You should not hassle or force the individual to take medication. The individual should
continueCBReveniftheyarenottakingmedicationforanyreason.
98
1. Revisetheinformationaboutmedication
Revisethefollowinginformationaboutmedication.
• Whatisanti-psychoticmedication
• Sideeffectsofanti-psychoticmedication
2. Explainwhyyouaredoingthemodule
Explainwhy it is important to takemedication regularly andwhy is it important to continue
takingmedicationwhenfeelingwell.
3. Assessingproblemswithtakingmedication
Findoutwhatthecurrentarrangementsarefortakingmedication.Whendotheytakeit?Does
anyone remind them? Then assess the reasons why the individual has problems taking the
medication,ormighthaveproblemsinthefuture.Askwhattheirattitudetowardsmedication
is.Havetheyfoundituseful?TheChecklistforproblemstakingmedication(Form15)shouldbe
used.ThiscoversthereasonsinSection20.2.
4. Problemsolvingtoimprovetakingmedicationregularly
You should then discuss each reason or problem in turn with the individual and caregiver.
Encouragethemtothinkofideasforhowtogetaroundtheproblemusingtheproblemsolving
approach (Section10.5).Discuss the approaches theyhavealready tried.Buildon their ideas
andthensuggestsomeoralloftheonesbelow,iftheyhavenotbeencovered:
a. Involvethefamily
The individual’s immediate family are the most important people to help them take
medicationregularly.Youshould:
• Trytounderstandthefamilymember’sviewpointand attitudes towardsmedicines
• Involve them in understanding the reasons for not taking medicines and deciding the
bestmethodstoimprovethesituation
• Provide themwith informationon thebenefitsandsideeffectsof medicines.
• Involvemembers of the extended family (uncles, aunts, cousins, etc)who liveoutside
99
the home. They may have a significant role to play in ensuring individuals take
medication regularly. Find out who the important individuals are and consider meeting
withthemtogaintheirsupport.
• Getthefamilytousepositivefeedback
• Givethe family skills todealamicablywithsituationswhere thefamilymembers andthe
individualhavedifferentviewsonadherence(seeChapter25)
• Consideraskingthefamilytoobservethe individualeverytimetheytakethemedication.
However thismaynothelp the individual to feel independent, so try thisonly if this the
otherideasdonotwork.
b. Reinforceinformationaboutmedication
Giveorreviseinformationaboutmedications,theirbenefitsandsideeffects.Youmayneedto
giveinformationtootherfamilymembersaswellastheindividualandcaregiver.
c. Addresssideeffects
Discussconcernsaboutsideeffects.Therearesomesideeffectsyoucanhelpwithandothers
thatneedtobereviewedatthehealthcentre(seeTable4).

100
Table4Howtohelpwithsideeffects
Whathappens? HowyoucanhelpThemouthisverydry Try putting a clove in the mouth or sipping
waterAlotofsalivaisproduced Advisethemtoputaclothnexttotheirmouth
atnightConstipation Advisethemtodrinklotsofwaterandeathigh
fibrefoodse.g.lentilsandvegetablesThe person feels dizzy when they gofromlyingdownorsittingtostanding
Advise person to get up slowly and wigglefingersandtoesbeforegettingup
The person wants to eat more thanusual
Advise that the individual probably does notneedmorefood,thisisjustasideeffectofthemedication.Tryeatingsmallamountsregularlyandincludingmorebulkyfoode.g.vegetables.Refer to health centre- for changeof doseorpossiblymedication.
Thepersonfeelsrestlessandcannotsitstill.
Refertohealthcentre
Thehead,neckorbodybecomesstuckinanunusualposition.
Refertohealthcentre
Thehandsshake RefertohealthcentreThe person moves very slowly andfeelstheirmusclesareverystiff
Refertohealthcentre
Thepersonisverydrowsy Refer to the health centre- the amount ofmedication may need to be changed, or thetime of day they take it. Drowsiness mayreduce when the person gets used to themedication
Writhing movements of the head,neck,armsorlegs.
Refertohealthcentre
Seizures RefertohealthcentreSexualproblems RefertohealthcentreSkinrash RefertohealthcentreThepersoncannotpassurine RefertohealthcentreSuddenly developing stiff muscles,fever,andconfusion
Taketohospitalimmediately
d. Getadailyroutine
Buildmedicationintothedailyroutine.Suggestthepersonwithschizophreniaalwaystakesthe
medicationafterdoingadailytaske.g.gettingwashedinthemorningorhavingbreakfast.
e. Usepositivefeedback
Peoplewith schizophreniahaveproblemswithmotivation.Theyneedfrequentandconsistent
101
feedback and appreciation from family members and you for continuing to take the
medication. Tobegin, the family can reward the individual taking his medication with clear
signsof appreciation (bytellingthemtheyaredoingwellorcooking his favouritedish).Make
itclearthatthisis linkedtothefact thatthe individualhasbeentaking themedicines.
f. Improverelationshipwiththenurse
Whenyouattend thehealth centrewith the individual around the timeofeachCBRReview,
oneofyourrolesistohelpimprovethecommunicationandrelationshipwiththenurse.Ifthere
isanyobviousmisunderstandingduringtheconsultation,trytoclarifythisatthetime.Youcan
also help the individual to raise any issues, for example that themedication schedule is too
complicated. After the consultation, check the individual and the caregiver understood
everythingandfillinanygaps.
g. Arrangeamedicationreviewatthehealthcentre
Takingthemedicationoncedailyislikelytobeeasiertoremember.If the individual feelsthat
the schedule is too complicated, they can discuss this with the nurse at the health centre.
Havingtheinjectioninsteadoftabletsusuallymakesitmorelikelytheindividualwilltakethe
medication,astheydon’thavetoremembereveryday.Ontheotherhandsomepeoplewith
schizophreniaarelesswillingtohaveinjectionsthantotaketablets.Itisnotyourdecisionto
changeto injections.However, ifothermethodshavebeentriedbutarenotsuccessful,and
theindividualiswillingtotryinjections,youcanencouragehimorhertospeak tothenurse
aboutthisatthehealthcentre.
h. Engagewithtraditionalandreligioushealers
Tryto findoutwhothehealer is.Youmayhavealreadymadecontactwiththemduringyour
initial community engagement (see Task 5 in Community Engagement Chapter 31).With the
permissionofthefamily,trytoarrangeameetingwiththehealer.Givetheminformationabout
schizophrenia, includingthatmedicationcanhelptoreducesymptomsandpreventtheillness
from returning. Tell them that the individual does not need to stop receiving holy water or
traditionalpractices,butthattheycanusemedicationalongsideit(seeTask11inCommunity
EngagementChapter31).

102
i. Exploreaccessingfreemedication
SeeChapter17.
j. Maketravellingtothehealthcentreeasier
SeeChapter17.
k. Addressfinancialproblems
SeeChapter17.
Table5canbeusedasaguideforwhichmethodstouse:
Table5Approachesforsupportingindividualstotakemedication
Problem Approach/sInsufficientfamilysupport InvolvethefamilyShameorstigma Giveinformation
InvolvethefamilyDifferingbeliefs Giveinformation
InvolvethefamilyLack of understanding about preventingrelapse
GiveinformationInvolvethefamily
Discouraged to take medication at holywater
GiveinformationEngagewithtraditionalandreligioushealersInvolvethefamily
Lackofawareness(duetoillness) GiveinformationInvolvethefamily
Lackofmotivationand/orconcentration PositivefeedbackDailyroutineInvolvethefamilyMedicationreviewathealthcentre
Khatoralcoholuse ReferraltohealthcentrePositive feedback when khat or alcohol isavoidedGetadailyroutineInvolvethefamily
Sideeffects AddresssideeffectsInsufficientfoodforincreasedappetite SmallregularmealsincludingvegetablesPoor relationship/communication withnurse
Improverelationshipwithnurse
Complicatedmedicationschedule MedicationreviewathealthcentreCannotaffordmedication Explorefreemedication
AddresseconomicproblemsCannotaffordtraveltohealthcentre Maketravellingtothehealthcentreeasier
AddresseconomicproblemsPractical issues travelling to healthcentre
Maketravellingtothehealthcentreeasier
103
5. Difficultsituations
Whattodowhentheindividualrefusestotakethemedication
If the individual refuses to take themedication you should listen carefully and respect their
point of view. You should try the approaches above. However, sometimes the individualwill
continue to refuse. If this happens you should not hassle themor force them to take it, but
should refer them to the health centre for a review. It is important to remember that you
shouldcontinuewithCBReveniftheindividualisunableorunwillingtotakethemedication.
Givingtheindividualmedicationwithouttheirknowledge
Thecaregiversmayhavepreviouslygiventhemedicationwithouttheknowledgeoftheperson
withschizophrenia,forexamplebymixingitinfoodortea.Thefamilymayalsosuggestthisasa
methodfordealingwiththemnottakingthemedicationinthefuture.Thisisadifficultsituation
as the individual’s basic right to decidewhat treatment they receive is not respected. It also
meansthatiftheindividualgetsbettertheydonotrealisethatitisduetothemedication.This
makesitevenlesslikelytheywilltakethemedicationoutofchoicelateron.Inaddition,ifthe
individualfindsoutlateronthattheywerebeinggiventhemedicationinsecret,theymayfindit
difficulttotrustpeople.Thismightmaketheillnessworse.
Ontheotherhand,itisusuallyunderstandablewhenfamiliestakethisstep,iftheyfeelthereis
nootherwaytogetthepersontotakethemedication,andthereforegetwell.Youshouldnot
encouragethefamilytogivetheindividualmedicationwithouttheirknowledge.Ifthisisdone
orsuggested,youshouldexplaintothefamilywhythismethodshouldbeavoidedifpossible,
withoutappearingtobejudgemental.Yourroleisthentoensurethatalltheothermethodsfor
helpingtheindividualtotakemedicationareusedfirst.Tellyoursupervisorifyouareawareifit
ishappening.
Forcingindividualstotakemedication
Thecaregiversmayhavepreviouslyusedphysicalforcetogetthepersonwithschizophreniato
takethemedication,forexample,bytyinguptheindividualandforcingthemedicationintohis
orhermouth.Othersmaysuggestthisasamethodforfutureuse.
Youshouldencouragefamiliesnevertoforceindividualstotakemedicationinthisway.Aswell
asbeingdisempowering,itmaymakethepersonmoreagitated,ortheymayevengetharmed.
Tellyoursupervisorifyouareawareifitishappening.

104
6. Makeaplan
Attheendofthediscussion,makesurethateverybodyknowswhatinputtheyareexpectedto
have.Setsomespecifictasksfortheindividualandfamilytocompletebythenexthomevisit.
Forexample:
• Thepersonwithschizophreniaagreestotakethemedicationwithbreakfasteveryday
• The caregiver agrees to remind the individual to takemedicationwith breakfast, observe
whethertheytakeitornotandtogiveencouragementifheorshetakesit
• The CBR worker agrees to meet with the holy water priest and attendant and give
informationabouttheimportanceoftakingmedicationwhilstreceivingholywater
7. Monitoringmedication
You should assesswhethermedication is being taken at somepoint during everyhomevisit,
even if you are not currently working through this module. Ask both the individual and the
caregiver if therehavebeenanyproblems.Be sensitiveand respectful anddonothassle the
individualtotakethemedication.Useproblemsolvingtoaddressanyproblems,orcompleteor
repeatthismodule.RecordissueswithmedicationontheHomeVisitForm(Form11).
Yosef’sstory
Yosef says even when he is well he often has problems remembering to take his
medication.Themedicationmakeshimfeeltired,droolsalivaandmakeshishandsshake.
SometimesYosefgoestoholywater.Theholywaterattendantstellhimheshouldn’tuse
medicationatthesametimeasthiswillmeantheholywaterwillnotwork.
Addis and Yosef agree that Yosef needs the family’s help to remember to take the
medication. TheyagreeAddiswill remindhimandwatch him take it at breakfastevery
day.Whenhe takes itsheandSolomonwillgive lotsofencouragement.Berhanadvises
Yoseftotryputtingaclothnexttohismouthatnight,tohelpwiththedrooling.Shealso
askshimtogotothehealthcentreincasetheamountofmedicationcanbereduced,or
hecantakeitatnight.Berhanagreestodiscusstheimportanceofcontinuingmedication
withtheholywaterpriestandattendant.Shediscussesthiswithhersupervisor,Haile,and
theygotogethertotheholywatersite.IttakesBerhanandthefamilytwohomevisitsto
discussmedicationandcreatetheplan.

105
Followup
Remembertocheckwhatprogresshasbeenmadeatthenexthomevisit. Ifrelevant,referto
the health centre, or meet with community leader, kebele leader or traditional or religious
healer.
20.5 Summary
• Manypeoplewith schizophreniahaveproblems taking theirmedicationdue to: individual
reasons (for example, not enough family support), illness factors (for example, not being
organised),treatmentfactors(forexample,sideeffects)andsystemicfactors(forexample,
cannotaffordtraveltohealthcentre)
• Takingmedicationisimportantforgettingwellandstayingwell
• Ways to help individuals takemedication include: involve family, give information, get a
dailyroutine,usepositivefeedback,educatetraditionalhealers,arrangemedicationreview
atthehealthcentreandaddresssideeffects.
106
21 Module:Improvingphysicalhealth
21.1 Whatproblemswithphysicalhealthdopeoplewithschizophreniahave?
• Usualhealthproblems
Peoplewithschizophreniaexperiencethesamephysicalhealthproblemsasotherpeople.For
example,theymaygetmalaria,acoughorabrokenbonefromanaccident.However,people
withschizophreniaarelesslikelythanotherpeopletogetmedicalhelpforanyphysicalhealth
problemstheyhave.
• Otherdisabilities
Peoplewithschizophreniaarejustaslikelytohaveotherdisabilitiesasotherpeople.For
exampletheymaybeblindorhaveproblemswalkingduetochildhoodpoliooranaccident.
• Beingunderweightorunderweight
In Ethiopia, people with schizophrenia are commonly underweight. Much less commonly in
Ethiopia,peoplewithschizophreniamaybecomeoverweight.
• Reproductivehealthandsexualhealthproblems,needforfamilyplanningandantenatal
care
Like anyone else, people with schizophrenia have sexual relationships. Women with
schizophreniamayalsobesexuallyexploited.Theythereforeneedaccesstoadviceaboutsafe
sex,familyplanningandantenatalcarejustlikeotherpeople.
• Chewingkhat,drinkingalcoholorsmoking
• Physicalinjuries
Peoplewithschizophreniamaydevelopwoundsandsoresfrombeingbeatenorbeingchained
up.Theirmusclesmaystopworkingproperlyiftheyarechainedupforalongtime.
• Heartdiseaseanddiabetes
Peoplewithschizophreniaaremore likelytogetheartdiseaseanddiabetes(highbloodsugar
levels)thanotherpeople.
21.2 Whydopeoplewithschizophreniahaveproblemswithphysicalhealth?
There are a number of reasons why people with schizophrenia have more physical health
problemsthanotherpeople.
• Difficultyaccessingthehealthcentre
Itmaybedifficultforfamiliestotaketheindividualwithschizophreniatothehealthcentre,
eitherbecausetheyhavedifficultbehaviourorbecausetheyaretiedup.

107
• Difficultypayingforhealthcare
Familiesmayhaveproblemspayingforhealthcare,particularlyiftheindividualissounwellthat
theyorthecaregiverhavedifficultyworking.
• Sideeffectsofmedication
Medicationcancauseproblemssuchasgainingweightandsexualproblems.Sometimespeople
dounhealthybehaviours, such as chewing khat or drinking alcohol, to try to reduce the side
effectsofmedication.
• Notenoughfood
Peoplewithschizophreniamaybecomeunderweightbecausethefamilyispoorandtheydonot
haveenoughfood.
• Stigmaanddiscrimination
Sometimesthefamilyorcommunitybelievestheindividualdoesnotneedordeservethesame
nutritionorphysicalhealthcareasotherpeople.Sometimeshealthworkersdon’t takepeople
withschizophreniaseriouslyanddismisstheirphysicalcomplaints.
• Individualnotwillingorabletoeatregularly
Sometimesduetotheillnesstheindividualdoesnotwanttoeatordoesn’tfindtimetoeat
• Beinginactive
Manypeoplewithschizophreniabecomeinactive.Thiscanbeonereasonforweightgain.
• Tryingtoescapeproblemsorsocialise
People with schizophrenia may drink alcohol, chew khat or smoke to try to escape their
problemsandsocialise.
21.3 Whyisitimportanttoimprovephysicalhealthinpeoplewithschizophrenia?
Peoplewithschizophreniaaremuchmore likelytodieyoungthanotherpeople.This ispartly
due to people with schizophrenia committing suicide. However, it is mainly due to physical
healthproblemssuchasinfectionsandmalnutrition.Havingphysicalhealthproblemsmaystop
people recovering fromschizophrenia.Whenpeoplehavephysicalhealthproblems itmaybe
more difficult to get to the health centre for anti-psychoticmedication, or to return to farm
work. It istherefore importanttotryto improvephysicalhealth inpeoplewithschizophrenia.
Chewingkhatcanresultindecayoftheteeth,heartproblems,cancer,anxietyanddepression.
Both khat and alcohol make the symptoms of schizophrenia worse and make it harder to
recover.Itisthereforeimportanttosupportpeopletostopusingkhatandalcohol.
108
21.4 Howcanweimprovephysicalhealthinpeoplewithschizophrenia?
1. Explainwhyyouaredoingthismodule
Explaintotheindividualandfamilywhatphysicalhealthproblemsarecommoninpeoplewith
schizophrenia.Givereasonswhypeoplewithschizophreniahavetheseproblems.
2. Assessphysicalhealthproblems
Assesswhatphysicalhealthproblemsorunhealthybehaviourstheindividualhasormighthave
inthefuture.
3. Problemsolvingtoimprovephysicalhealth
Youshouldthendiscusseachprobleminturnwiththeindividualandcaregiver.Encouragethem
tothinkof ideas forhowtogetaroundtheproblemusingtheproblemsolvingapproach(see
Chapter 10). Discuss the approaches they have already tried. Build on their ideas and then
suggestsomeoralloftheonesbelow,iftheyhavenotbeencovered:
a. Ensureaccesstohealthcare
Ensurethattheindividualisaccessingthehealthcentreorhospitalforphysicalhealthproblems
whentheyarise,forexampleinfectionsoraccidents.SeeChapter17.
b. Avoidalcohol,cigarettesandkhat
Encouragetheindividualnottodrinkalcohol,smokeorchewkhat.Explainthatthiswill
probablymaketheillnessworse.Askthefamilytotrytoavoidgivingtheindividualmoneyfor
alcohol,khatorcigarettes,ifpossible.Discusswiththeindividualwhethertheyneedhelptocut
downorstop.
c. Gethelpforproblemswithalcoholorkhat
Iftheindividualhasseriousproblemswithalcoholorkhatuse,thenyoushouldreferthemto
thehealthcentre.Apersonhasaseriousproblemif:
• Theyoftenappeartobeaffectedbyalcoholorkhat.Forexample,smellsofalcohol,looks
intoxicated,staggerswhenwalking,slurredspeech.

109
• Becauseofalcohol,theyofteninjurethemselves,forexamplefromfallingdown,fights,or
walkingintraffic
• Theyhavephysicalsymptomsfromexcessivealcoholuse.Forexamplecan’tsleep,very
tired,can’teat,nauseatedbyfoodsmells,vomits,complainsofabadstomach,diarrhoea,
headaches.
• Theyshowsignsofdruguse.Forexample,skininfection,unkemptappearance,drymouth,
burnedlips,badorwornteeth,complainsofdukak(vividunpleasantdreams)
d. Encourageahealthydiet
Encouragetheindividualtoeatahealthydietasmuchaspossible.Beawarethatmanyfamilies
willhaveverylimitedchoiceaboutwhattheyeat.Ahealthydietconsistsofamixtureof:
• Cereals,suchasteff(injera),barleyandwheat
• Pulses,suchaslentils
• Fruits
• Vegetables
• Smallamountsofmilk,cheeseandyogurt
• Smallamountsofmeat
Makesurethepersonwithschizophreniaeatsthesameamountandtypeoffoodastherestof
the family (SeeChapter24). If youare concerned theperson is veryunderweightyou should
referthemtothehealthcentre.
e. Encourageappropriatephysicalactivity
Encouragetheindividualtodosomephysicalactivityasitisnotgoodforthemtositathomeall
day.Mostpeoplecandothisaspartoftheirday-to-dayactivities,forexamplegoingtofetch
water.However,peoplewithschizophreniashouldnotdoexcessiveexerciseasthismay
contributetowardsthembecomingunderweight.
f. Refertothehealthcentreforproblemswithsideeffectsofmedication
Youshouldreferbacktothehealthcentreiftheindividualsideeffectswhichareaffectingthe
individuals’physicalhealth.Forexample,problemswithmenstrualperiods.
110
g. Refertothehealthcentreformalnutrition
Refertheindividualtothehealthcentre,andfacilitatethemtoattend,iftheyappearvery
underweightormalnourished(seeChapter14).
h. Attendtophysicalinjuries
Iftheindividualhasanywoundsorsoresmakesurethesearewashedwithcleanwater.Ifyou
areworriedaboutthewound,forexampleifitisnothealing,refertheindividualtothehealth
centre.Iftheindividualhasproblemsmovingtheirarmsorlegsproperlybecausetheyhave
beenchainedupforalongtimeyoushouldreferthemtothehealthcentre.Youmaybeasked
tohelpthemexercisetheirarmsandlegs.
i. Attendtophysicaldisabilities
Iftheindividualhasaphysicaldisabilitydiscusswithyoursupervisorthebestwaytosupport
them.
j. Ensureaccesstothehealthextensionprogramme
TheHealthExtensionWorkershouldmakeroutinevisitstothehouseholdtocover
contraception,protectionagainstHIV,sanitation,malariaprevention,childnutritionand
antenatalcare.Iftheindividualasksforhelpwithanyoftheseissues,orifyouknowthatthe
HealthExtensionWorkerhasnotmaderoutinevisitstothehousehold,contacttheHealth
ExtensionWorker.Askhertomakearoutinevisittotheindividualtodiscusstheseissues.
4. Makeaplan
Attheendofthediscussion,makesurethateverybodyknowswhatinputtheyareexpectedto
have.Setsomespecifictasksfortheindividualandfamilytocomplete.

111
Followup
Makesureyourefertothehealthcentreorhealthextensionworkerifthisisrelevant.Ifyoudo
makeareferralmakesurethattheindividualattendsfortheinitialvisitandanyfollowupthat
is needed. At later visits ask about progress with healthy behaviours. If there are physical
disabilities,discusswithyoursupervisor.
21.5 Summary
• Peoplewith schizophrenia have physical health problems such as being underweight and
usingkhatandalcohol
• Physicalhealthproblemsmaybedangerous,andmakeitmoredifficulttogetwell
• Wecan improvephysicalhealthby:ensuringaccesstohealthcentreandhealthextension
worker, and giving advice about diet, exercise, alcohol and khat.
Yosef’sstory
BerhanobservesthatYosef isquiteunderweight.Yosefsayssometimesheis tootiredto
eat.BerhantellsAddisaboutthedifferentpartsofahealthydiet.Addisexplainsthatoften
theycannotgroworaffordtobuydifferenttypesofgrainsandvegetablesandtheyrarely
eatmeat.BerhantellsAddissheunderstandstheyhave limitedchoices.Theyagreethat
Yosefneedsmoresupportandencouragementatmealtimes.Berhandiscussesthe issue
withHaile.TheyagreethatYosefdoesnotneedtogotothehealthcentreatthemoment,
butifhelosesmoreweightthiswillbenecessary.

112
22 Module:Dealingwithdistressingsymptoms
22.1 Whatdistressingsymptomsdopeoplewithschizophreniahave?
AswediscussedinChapter2peoplewithschizophreniacanhavefourgroupsofsymptoms:
a. Hallucinations(seeingorhearingthingsthataren’treallythere)anddelusions(believing
thingsthataren’ttrue)
b. Problemswithmotivation
c. Problemswiththinkingclearly
d. Personnotbeingawarethattheyhaveanillness
All of these symptoms can be very distressing for individuals. The extent to which they are
distressingvariesfrompersontoperson.
22.2 Whydopeoplewithschizophreniahavedistressingsymptoms?
Distressing symptoms are part of the illness of schizophrenia. Medication usually helps to
reducehallucinationsanddelusions,butsometimestheycancontinueevenwhenanindividual
is taking themedication regularly. It is common for problemswithmotivation and problems
withthinkingclearlytocontinueevenwhenanindividualistakingtheirmedicationregularly.
22.3 Whyisitimportanttoreducedistressingsymptoms?
Aswellasbeingdistressingfortheindividual,thesesymptomscanbedisabling.SeeChapter4.
Havingsymptomscanmakegettingbacktousualactivitiesmoredifficult.
22.4 Howcanwehelptoreducedistressingsymptoms?
Principles
Atalltimes,thefocusshouldbeonempoweringtheindividualtotakechargeofmanagingtheir
ownillness.Thegeneralapproachtoreducingsymptomsis:
• Supportingtheindividualtotakemedication(seeChapter20)
• Reducingstressbyimprovingtheenvironment,forexampledealingwithhumanrights
problems(SeeChapter19),orimprovingcopingstrategies(seeChapter23)
However,peoplewithschizophreniaoftencontinuetoexperiencedistressingsymptomsdespite
takingthesesteps.Itisthereforeimportanttohavespecificwaystohelptocopewiththem.To
dothis,followthesesteps.
113
1. Reviseinformationaboutsymptoms
Revise what kinds of symptoms people with schizophrenia experience, relating them to the
symptomstheindividualhas
2. Explainwhyyouaredoingthismodule
Explainwhyitisimportanttoreducedistressingsymptoms.Emphasisethatthisisachancefor
theindividualtofeelbetter.Highlightthatproblemswithmotivationandthinkingclearlycanbe
difficulttoovercome.
3. Assesssymptoms
Findoutwhichisthemostdistressingsymptomandfocusonthatfirst.Discussthefollowing
issuesrelatingtothatsymptom:
• Howoftenithappens
• Howitaffectstheperson
• Whatmakesitworse,forexamplehavinganargumentwithparents
• Whatmakesitbetter,forexampletalkingtoabrotherorsister
4. Suggestpotentialcopingstrategies
a. Hallucinations
• Changethelevelofactivity
Tryrelaxation(seeChapter23),ortakingawalk
• Doadistractingactivity
Talktofamilymembersorneighbours,listentotheradioorsingasongorhum
• Talktoyourselfinapositiveway
Forexample,‘Icancopewiththis’
• Ignorethehallucinationasmuchaspossible
b. Delusions
• Suggestthattheindividualcheckstheirideasofrealitywithsomeonetheytrust,forexample
thecaregiver
• Iftheindividualdiscussestheirdelusionswiththecaregiver,thecaregivershouldlistento
them.Thecaregivershouldnottrytoargueorreasonwiththem.
c. Problemswithmotivation

114
• Remindthefamilythatthepersonisnotlazyoruseless,buthasanillnessthatmakesit
difficulttofindtheenergyorwillpowertodotheirusualactivities.
• Encouragetheindividualtohavearegularroutine,e.g.gettingupataregulartime,eating
whenotherseat(seeSection24.4formoredetail)
• Encouragethefamilytoinvolvetheindividualinsocialandcommunityactivities,for
exampleattendingchurch(seeChapter26)
• Encouragetheindividualandfamilytothinkaboutthefuturewithhope.Askthemtothink
abouttheprogressthattheindividualhasalreadymade.
d. Problemswiththinkingclearly
• Whenthepersonwithschizophreniaisdoingsomething,forexamplepreparingfoodor
havingaconversation,trytoreducedistractions.Forexampleturnofftheradioandreduce
backgroundconversations.
• Tryactivitiesthatimproveconcentration,forexampleweavingorpraying
• Remindthefamilytogivetheindividuallotsoftimetodosmalltasksandnottobecome
impatient.
• Practiceactivitiesmanytimesuntiltheybecomeeasier
5. Discusscopingstrategiesthatareunlikelytobehelpful.
Theseinclude:Angrilytellingthevoicestogoaway;Drinkingalcoholorchewingkhat;Sleepinga
lot;AvoidingcontactwithotherpeopleandStoppingmedication.
6. Makeaplan
Helptheindividualtoselectacopingstrategyorstrategies,involvingthecaregiverinthe
discussion.Youcanalsouseaproblemsolvingapproach(seeSection10.5).Asktheindividualto
practicethecopingstrategytheyhavechosenafewtimes.Asktothemtothinkabouttimes
whenitispossibleornotpossibletousethestrategy.

115
Followup
Followupprogresseverytimeyouseetheindividual.Askwhetheritishelpingornot.Ifitisnot
helping,makechangestothestrategyortryadifferentstrategy.
22.5 Summary
• Manypeoplewithschizophreniafindtheirsymptomsdistressing,evenwhentheyaretaking
medicationregularly.
• Havingdistressingsymptomscanmakeitmoredifficulttogetbacktousualactivities
• We can try to reduce distressing symptoms by supporting individuals to takemedication,
andreducinglifestress.
• We can also suggest coping strategies such as: doing a distracting activity (for
hallucinations), discussing ideas with a trusted person (for delusions), having a regular
routine (for motivation problems) and reducing background noise (for problems thinking
clearly)
Sara’sstory
Saraisayoungwomanwhobecameunwellwithschizophreniaoneyearago.Shecanstill
hearvoicesthatcommandhertodothings.Sometimesshebelievesshehasspecialpowers
toreadotherpeople’sminds.Herhusband,Alemu,usuallytellsSarathatsheisstupidor
madwhenshetalksaboutthis.Theseproblemsareabitbettersinceshestartedtakingthe
medication,buttheyhavenevercompletelygoneaway.BerhanasksSaratodescribethese
problemsandtotellherhowoftentheyhappen.SaratellsBerhanthattheproblemsget
worsewhenshedoesn’ttakethemedicationandwhenshegetsstressed.Aftersome
discussion,Saraagreestotrylisteningtotheradiowhenthevoicesnextbecomeverybad.
Alemuagreesthatitdoesn’tseemtohelpwhenheinsultsSaraortellsheroffwhenshetalks
aboutherspecialpowers.Alemuagreestotrynottodothisinfuture.BerhanasksSaraand
Alemutotrytheseideasandthattheywilldiscusshowitwentatthenexthomevisit.
116
23 Module:Managingstressandanger
23.1 Whatproblemsdopeoplewithschizophreniahavewithstressandanger?
Stressiswhatpeopleexperiencewhentheyfeeloverwhelmedbythethingshappeninginlife.
Itmakespeople feel tenseandanxiousand that they cannot copewith thedifficulties they
face.Weallexperiencestressinourdailylives.Howeverwhensomeonehasschizophreniathis
will increase the stress of the individual and their family members. Stress can have many
effects on people,includingchangesinthebody,emotions,andbehaviour.Inparticularstress
can sometimes cause people with schizophrenia to become angry. Anger can sometimes
causeanindividualtoharmotherpeopleorthemselvesordamageproperty.
23.2 Whydopeoplewithschizophreniahaveproblemswithstressandanger?
Differentpeoplefinddifferentthingsstressful.Stresscanbecausedby:
• Importantlifeeventsthathappensuddenly,forexampleadeathinthefamily,
• Ongoingdifficultsituations,forexamplefinancialproblemsorfamilyconflict.Thesethings
maybemorecommonwhensomeoneinthefamilyhasschizophrenia.
23.3 Whyisitimportanttoreduceproblemswithstress?
Stress,alongwithvulnerability, isoneofthefactorsthatdetermineshowsevere the illness is
andhowmanyrelapses thereare (seeSection2.3). Learning to manage stress is therefore
important for thewellbeingof the individualand tohelp themto recover.Angercancause
relationshipproblemswithin the family. If a personwith schizophrenia becomes aggressive,
the family may feel it necessary to tie them up in order to protect other people and the
individual.Inordertopreventthishappeningitisimportanttolearnhowtopreventanddeal
withanger.
23.4 Howcanwehelptoreduceproblemswithstressandanger?
Principles
Problemswithstressandangercanbereducedby:
• Preventingstressandangerhappeninginthefirstplace
• Givingwaystodealwithstressandangerwhenitdoeshappen
1. Giveinformationaboutstressandanger
Explainwhatstressandangerareandwhytheyhappen

117
2. Explainwhyyouaredoingthismodule
Explainwhyitisimportanttoreducestressandanger
3. Assessproblemswithstress
Discusswhatsituationswerestressfulinthepastormightbestressfulinthefuture.
4. Discusswaystopreventstress
Discuss how the individual can avoid feeling stressed in the future. Use the individual and
families’ideasandsuggestthefollowingiftheyhavenotbeencovered:
a. Avoidortrytochangesituationsthatwerestressfulinthepast
If a situation was stressful before, it is likely to cause problems for the person when
they are in the same situation again. Suggest to the individual that they avoid these if
possible. For example if the individual finds it difficult to attend a wedding, they could
avoid going to the ceremony. Or suggest that they change the situation to make it less
stressful.Forexample,theycouldmeetthebrideandgroomatadifferenttime.
b. Haveregularactivities
Stress canbereduced if the person has the right balance of activityandrest.Peoplewith
schizophrenia usually find it helpful to have some structure to the day. Try to involve the
individualinmeaningfulactivities,suchashousework,farmworkordrinkingcoffeewithothers.
SeealsoChapter24.
c. Haveahealthylifestyle
Eatingenoughnutritiousfood,gettingenoughsleep,doingexerciseandnotdrinkingalcoholor
usingkhatcanallhelptoreducestress.SeealsoChapter21.
d. Havereasonableexpectations
Havinghighexpectationsoftheindividualcanbestressfulforhimorher.Encouragethefamily
tohavereasonableexpectationsandforrealisticgoalstobeset.
e. Trynottobecritical
It is importantnotbecriticalof the individualand forthemnottobe criticalofthemselves.

118
Encouragementshouldbegiven forany task that the individualdoesandanysmall changes
should be acknowledged. Think of positive things about the person and remind them of
these when theyare feelingnegative.Askthefamilytodothesame.
5. Discusswaystodealwithstress
Discuss how the individual deals with stress when it does happen- is it helpful? Use the
individualandfamilies’ideasandsuggestthefollowingiftheyhavenotbeencovered:
a. Allowtheindividualtodiscusstheirfeelings
Letting theperson talk about their feelings oftenprovides some immediate relief and can
keep stress from buildingup.Stressmaybeanearlywarningsignofarelapse.Iftheperson
withschizophreniacantellyouorarelativewhenhe/sheisfeelingstressed,therelapsemay
beprevented.SeeChapter30.
b. Allowthefamilytodiscussthesituation
Discuss the situation with the family and try to find possible solutions to the problem
causing thestress.Usetheproblemsolvingapproach(seeSection10.5).
c. Userelaxationtechniques
Relaxation techniques can help in reducing stressandsleepingwell.Youcanteachboththe
individualandfamilythesetechniques.Itisbesttopracticeeveryday.
ControlledBreathing
• Explain that when we become stressed our breathing rate often speeds up. Slowing
downourbreathingcanhelpusto feelmorecomfortable.
• Showthe individualandfamilyhowtobreathe in for4counts,hold for2countsand
breatheoutfor6counts.Youcancloseyoureyesifyouwish.
• Practicethisexerciseinthesessionfor5or10minutes.
• Askforfeedbackfromtheclientandfamilyabouthowtheyfoundtheexperience
anddiscussanydifficulties.
• Discuss that learning a slow breathing technique ismore difficult than it first seems,
and requires a lot of practice. You could also suggest some ways of making the
processeasier,forexample:

119
o Initially,onlypracticethebreathingexercisewhenyou’renotfeelingstressed
o Explainthatsomepeopledescribefeelingmorestressedwhentheyfirstbeginusing
controlledbreathing.Itis importanttocarryonwiththetechnique,becausethis
feelingofstresswilldecreasewithpractice
o Practiceinacomfortableenvironment.Lyingdowniseasier thansittinginachair.
Chooseaquietdimly litroom,andtrytopracticeata timewhentheywillnotbe
disturbed
o Thebreathingpatternmaybehardforsomepeoplesoyoumightneedtoadjustit
(e.g.breatheinfor3counts,holdfor1andbreatheoutfor5,orbreatheinfor3
counts,holdfor1andbreatheoutfor3counts)
Muscle relaxation
The aim of this form of relaxation technique is to help the person relax by releasing
muscle tension with each outward breath. It builds on the controlled breathing
techniquedescribedabove.Thisiswhatyoushouldsay:
“Focus on your breathing…Just focus on each breath, in and out...As you breathe in,
tensethemusclesinyourfeetastightasyoucan.Asyoubreatheoutrelaxyourfeetand
letgoofthetension”
You then go through each specific areas of the body in turn, continuing with the
ankles and working upwards. Repeat the instruction to tense the particular area as
you breathe in and release any tension as you breathe out. Continuethisexercisefor
10-15minutes.
d. Religion
Formany people religion gives comfort anddirection to their lives. Religious beliefs,prayer
andattendingchurchormosquecanhelppeoplecopewithstress.Also, religiousgroups,for
examplemahaber,canbea sourceofsocialsupport,whichcanreduce feelingsofisolation
andstress.
e. Encouragetheindividualtotalkaboutthemselvesinapositiveway
Encourage the person with schizophrenia to stop talking to themselves ina negativeway,
forexample“This is awful”.Encouragethemtotrytalkingtothemselvesinapositiveway,
forexample“ThisisachallengebutIcanhandleit”or“Iamgoingtodo thebest I can”.

120
f. Keepasenseofhumour
Many peoplewith schizophreniahave agood senseof humour.Whenastressful situation
happens, try to say something thatwillmake the individual smile, toavoid them being
totallyoverwhelmedbythesituation.
g. Exercise
Physical activity has a positive effect on reducing stress, lifting mood and improving sleep
patterns.Peoplewithschizophreniashouldtry todosome lightphysicalactivityeveryday, for
examplewalking.Howevertheyshouldnotdostrenuousactivitiesorexerciseforlongperiodsas
thismaycontributetoweightloss(seeSection21.2).
6. Discussunhelpfulwaystodealwithstress
These include: smoking,drinkingalcohol, chewingkhat,notspending timewithotherpeople,
beingverybusyandgettingangrywithotherpeople.
7. Discussproblemswithanger
Discusswhatsituationshavemadetheindividualfeelangryorwhatmightdointhefuture.
8. Discusswaystopreventanger
Somewaystopreventangerinclude:
• Trytounderstandwhatmakestheindividualangryandtrytoaddressthisproblem
• Preventanddealwithstress(seeabove)
• Developself-confidenceintheindividual(seeChapter28)
• Makesuretheindividualisaccessingthehealthcentreandtakingtheirmedication
• Trytoavoiddrinkingalcoholorusingkhat;thesecanreducepeople’sangercontrol.
9. Discusswaystodealwithangerwhenithappens
Suggesttheindividualtriessomeorallofthefollowingtechniqueswhentheyfeelangry:
• Leavethesituationwhichiscausinghimorhertofeelangryassoonaspossible
• Noticethefactthatheorsheisangry.Stopdoingwhatevertheyweredoingandeitherwalk
aroundorsitcalmlyforafewminutes.

121
• Release the stress in away inwhich there is least possible harm to self, others, and the
environment,forexamplepunchingapillow.
• Dorelaxationtechniques,forexamplecontrolledbreathing.
• Ifpossibledosomethingdistracting,likewateringthekitchengarden
• Talktosomeoneaboutwhatismakingthemfeelangry.
If he or she became aggressive, after the situation has passed, suggest that individual:
Apologisestoanyoneinvolvedandtriestotidyuporfixanythingthatwasdisturbed
10. Makeaplan
Help the individual toselect strategies forpreventingwithanddealingwithstressandanger.
Involvethecaregiverinthediscussion.
Followup
Remembertoreviewwhichofthesewaystodealwithstressorangerwerehelpful,andwhich
werenot.Suggesttotheindividualandfamilytofocusonthehelpfulonesinfuture.
23.5 Summary
• Everyone experiences stress sometimes, but it is more common in people with
schizophrenia.Stresscanleadtoanger.
• Stresscanmakesymptomsworseandmakerelapsemorelikely
• Waystopreventstressinclude:avoidstressfulsituations,healthylifestyle,havereasonable
expectations
• Waystodealwithstressinclude:relaxation,religionandtalkingaboutproblems
• Ways to prevent and deal with anger include: developing self-confidence, leaving the
situation that ismaking themangry, and releasing theanger in away that isnotharmful
122
24 Module:Improvingdaytodayfunctioning
24.1 Whatproblemsdopeoplewithschizophreniahavewithday-to-dayfunctioning?
Peoplewithschizophreniamayspendthedaydoingnothinginparticular.Thiscanbedistressing
forfamilymembersandtheymayseethepersonasbeing‘lazy’.Peoplewithschizophreniamay
also have problems doing specific tasks. They may have problems with self-care, including:
Cleaning teeth,Washing theirbodyandhair,Eating food inapropermanner,Washinghands
beforeandaftereating,CuttingnailsandUsingthetoiletproperly.
Theymayalsohaveproblemswithhouseholdtasks,including:Preparingfood,Preparingcoffee,
Cleaningthecookingandservingutensils,Fetchingwater,Goingtothemillhousetogetgrain
ground,Washingclothes,Cleaningtheanimalarea,Preparinglocalbeverages,forexampletella,
forthehousehold,fencingandrepairingthehouse.
24.2 Whydopeoplewithschizophreniahaveproblemswithdaytodayfunctioning?
Peoplewithschizophreniamayhaveproblemsdoingthesetasksforavarietyofreasons:
• Theillnessgivesthemproblemswithmotivation
• Theillnessgivesthemproblemswiththinkingclearly
• Medicationsideeffects,suchasdrowsinessorshakinghands,makesometasksdifficult
• Thefamilydoesnotletthemdotasks,forexamplepreparingthecoffee,becausetheyare
worriedtheywilldoitwrong.
24.3 Whyisitimportanttoimprovedaytodayfunctioning?
• Keepthepersonengaged inuseful tasks
• Improvememory,attentionandconcentration
• Distract fromtroublesomesymptoms likehallucinationsanddelusions.
• Improve their self-confidence
• Reducestigmatowardsthem
• Improvesocialinteractions
24.4 Howtoimproveproblemswithdaytodayfunctioning?
Principles
• Establishwhatisnormalforthehousehold.Forexample,checkhowoftenotherfamily
membersgetwashed,andwhethersoapisused.

123
• Establishwhatisnormalfortheindividual.Forexample,checkwhetherfetchingwaterwas
expectedofthemwhentheywerewell.
• Setrealisticgoalsandaimforgradualimprovement.Theindividualwillneedmoretimethan
usualtodothetasks
• Involvethefamilyateverystageoftheprocess.Theaimisforthemtobeabletosupport
theindividualtodothetaskwhenyouarenotthere.
• Theindividualwilloftenknowhowtodothetask,butmayhaveproblemsrememberingor
beingmotivatedtodoit.Focusongettingtheindividualbackintoaroutine.
• Askthefamilymemberstogiveencouragementwhenanyofthetasksaredone
• Youmaynoticethatthereareproblemswithhygieneandsanitationwithinthehousehold
thatarenotonlyrelatedtotheindividuals’illness.Ifthisisthecaseyoucoulddirectsomeof
youradvice,forexampleabouttheimportanceofwashing,towardsotherfamilymembers
too.Youcanalsoconsideraskingthehealthextensionworkertovisittodiscusssanitation,if
theyhavenotalreadydoneso.
1. Explainwhyyouaredoingthismodule
Explaintotheindividualandfamilythatproblemswithdaytodayfunctioningarecommonin
peoplewithschizophrenia.Givesomeofthereasonswhypeoplehaveproblemsandwhyitis
importanttoimprovethesituation.
2. Assessforproblemswithselfcare
Askwhatproblemstheindividualhaswithdaytodayfunctioning,usingtheDaytoDay
functioningProgressForm(Form16).Asktheindividualwhytheyarehavingdifficulty.Focuson
thetaskswherethereisaproblem.
3. Giveadviceonhowtoimproveeachselfcaretask
Foreachtask:
• Discusswhyitisimportanttodothetask.Sayitishealthytokeepyourteethandbody
clean.Alsoitwillmakeiteasiertosocialisewithfriendsandfamily.
• Checkwhatthefamilynormallydoesandwhatisexpectedoftheindividual
• Agreeatimewhentheindividualwilldothetaske.g.cleanteethstraightafterwaking

124
• Iftheindividualisverydisorganisedyoumayneedtotalkthrough,ordemonstrate,the
stagesinthetask.Ifappropriate,asktheindividualtohaveagoatdoingthetask
• Tobeginwiththecaregivermayneedtowatchtheindividualdoingthetask
Tasksmayinclude:
a. Cleaningteeth
b. Washing
c. Groominge.g.braidinghair,cuttingnails.Thefamilyshouldsupervisethefirst few
attemptsatcuttingnailstoensurethathe/shecutsit safelyandneatly.
d. Usingthetoilet,washinghandsandmenstrualhygiene.Thisisasensitiveissueandyou
mustbecarefulwhenyoudiscussthistopicsoasnottooffendtheindividualorthe
family.Discussthedisposalandwashingofsoiledclothes.
e. Dressingandtakingcareofclothes.E.g.notwearingtoofewortoomanyclothes.
f. Healthyeatinghabits.Ensuretheindividualisbeinginvolvedinmealtimeswiththerestof
thefamily.Discusstheimportantthingstodoandnotdowhilsteatinge.g.
o Washhandsbeforeeating
o Onlyeatwiththerighthand
o Donotlickfingers
o Donotreachacrossotherpeople
o Washhandsaftereating
4. Assessforproblemswithhouseholdtasks
Askwhathouseholdtaskstheindividualfindsdifficult.Referbacktoanyproblemshighlightedin
theneedsassessment.Trytounderstandfromtheindividualwhytheyarenotdoingthetask.
5. Giveadviceonhowtoimprovehouseholdtasks
Foreachhouseholdtaskwherethereisaproblem,gothroughthefollowingsteps
• Discusswhatisexpectedoftheindividual
• Talkthrough,ordemonstrate,thestagesinthetask
• Ifappropriate,asktheindividualtohaveagoatdoingthetask
Thehouseholdtasksmightinclude:
• Tidyingthesleepingarea,andfoldingtheblanket

125
• Keepingtheroomtidy.Theyshouldbeencouraged to pick up fallen items and
replacethem.Theyshouldcleanthefloorifsomethinghasbeenspilt.
• Sweeptheroom everyday.
• Cleaningand cuttingvegetables
• Fetchingthewater
• Preparingcoffee
• Lightingthefire
6. Encouragementandpositivefeedback
Foreachself-careandhouseholdtask,askthefamilytoencouragetheindividualtodothetask
andgivethempositivefeedbackwhenit isdone.Tellthefamilytheindividualwillneedmore
timethanusualandwillneedbreakswhilstdoingthetasks.
7. Creatingadailyroutine
Once the individualhas someability todo the individual tasks, you shouldhelp them toget
intoadailyroutine.Thedailyroutine shouldbea combinationofwork,rest,leisure,self-care
andsleep.Thefollowingisanexampleofadailyroutine.
12:00:Wakeup,attendtotoilet,washface,brushhair
12:15:Tidybed
12:30:Sayprayers
1:00:Eatbreakfast
1:15:Washplateandglass,tidytable
1:30:Milkthecowsandfeedthem
2:30:Fetchwater
3:30:Restortea/coffeebreak
4:00:Householdactivitieslikecooking,tidyingrooms
6:30:Lunch
6:45:Washplate,glassandtidytable
7:00:Rest
8:00:Washclothes
9:00:Weavingcloth
10:00:Tea/coffeeandconversewithfamily,friendsorneighbours
126
11:00:Feedthecows
12:00:Householdtaskslikecooking
2:00:Eatdinner
2:30:Washplateandglassandtidytable
3:00:Listeningradioortalkingwithfamilymembers
4:00:Sleep
You canmake a similar routine for the person you are working with after consideringtheir
age, sex, needs andwishes.Give the individual guidanceonhow todo all the tasks.Ask the
caregivertobe involvedandencourage thepersonstickto theroutineas faraspossible.Itis
usuallyhelpful towrite itdown for future reference,even if the individualand family cannot
read.
8. Giveadviceonmanagingmoney
• Thefamilymayneedtohelptheindividualtorecognizethetypesofcoinsandnotes.
• Familymembersshouldencouragethepersontopurchasethingsrequiredforthefamily
byinitiallygiving theexactamounttobespent.Later,thepersonshouldbeencouraged
topaytheappropriateamount, collectthecorrectbalanceandreturnhomewiththe
items.
9. Makeaplan
Decidewhich task the individualand familywill trybefore thenext session.Agreewhateach
person’sroleis.Iftherearemanytasksthatarecurrentlydifficult,focusontheonesthatarea
priorityfortheindividualandfamilye.g.gettingdressed.
Followup
Remembertoreviewprogressatthenexthomevisits,referringtotheDaytoDayFunctioning
progressForm.
127
24.5 Summary
• People with schizophrenia often have problems with day to day functioning, such as
washingthemselvesortidyingthehouse
• Problemsareduetotheillness,themedicationandlowexpectationsofthefamily
• Wecanimprovedaytodayfunctioningbybreakingdowntasksintosmallsteps,asking
thefamilytogivelotsofencouragement,andmakingadailyroutine
Yosef’sstory
YosefandAddistellBerhanthatYosefdoesnotwashandsometimesdoesn’tdressproperly.
BerhandiscusseswithYoseftheimportanceofwashinganddressingproperly.Yosefagrees
thismightbestoppinghimmakingfriendsagain.WithAddis’help,Berhanbreaksdownthe
stepsofwashinganddressingintosimplesteps.TheyagreethatAddiswillprompthimtodo
these steps every morning, and will give him lots of praise if he does them by himself.
Together they thinkofadaily routine that Yosefwill try to follow.Berhandoesn’twrite it
downasthefamilycannotread,buttheyagreetotryandrememberit.

128
25 Module:Improvingthefamilyenvironment
25.1 Whatproblemsdopeoplewithschizophreniahavewiththefamilyenvironment?
Problemswithinthefamilyarecommonwhenapersonhasschizophrenia.Theremaybemany
argumentsorevenviolencebetweenfamilymembers.Sometimesthefamilyareverycriticalof
thepersonwithschizophrenia.Orcertain familymembersmaybe involved ineverythingthat
the individualdoesbecausetheyareworriedtheycannotdoitalone.Thismeansneitherone
hastimetothemselves.Alltheseproblemssometimesmeanthatthefamilybecomeslessgood
at caring for the individual. It can also be very stressful for the caregiver, who may find it
difficulttocope.Lookingafterchildrencanbestressfulandtiringforanyparent,butespecially
whentheparenthasschizophrenia.Theymayfeeltheyarenotabletolookafterthechildren
properly.
25.2 Whydopeoplewithschizophreniahaveproblemswiththefamilyenvironment?
Thefamilyarethemaincarerswhenapersonhasschizophrenia.Thiscanputalotofstresson
the family.The individualmayhavedisruptivebehaviours,whicharedifficult tocontrol.They
mayalsonotbeworking,whichputsextrastrainonthefamily.Thecostsoftreatmentmayalso
beasourceofstress.Thefamilymaynotunderstandwhytheindividualcannotworkandhas
not recovered. All these problems can mean the family environment becomes stressful and
unpleasant(SeeChapter5).Parentswithschizophreniamayhaveproblemslookingaftertheir
childrenbecause theyhavemanysymptomsorbecauseof sideeffectsof themedication (for
exampledrowsiness).
25.3 Whyisitimportanttoimprovethefamilyenvironment?
When there areproblemswith the family environment it usually takes longer for theperson
with schizophrenia to recover. It is therefore important to help the family to support the
individualbetter.Also,improvingthefamilyenvironmentmeansthefamilyhaslessstressand
worry.It isempoweringfortheindividualtostartlookingaftertheirchildrenagain.Doingthis
mightimprovetheirself-esteemandmakethemfeelhappythattheyareparticipatinginfamily
life.It isalsobetterforthechildren’sdevelopmentiftheparentsgiveproperloveandcareto
thechildren.
129
25.4 Howcanwehelptoimprovethefamilyenvironment?
Principles
Before you can start improving the family environment it is important to have a good
relationshipwith the family (seeChapter 11). Be awareof the fact thatdiscussing the family
environmentmaybeupsettingfortheindividualandfamily.
1. Explainwhyyouaredoingthismodule
Explain why it is important for the person with schizophrenia to have a good family
environment.
2. Understandproblemsinthefamilyenvironment
Discusswiththeindividualandfamilywhatproblemsthereareinthefamilyenvironment.For
examplewhether there are oftendisagreements or conflict. You should also check the latest
needsassessment.
3. Considerhowwellthecaregiveriscoping
SeeChapter15forhowtosupportthecaregiveriftheyarenotcopingwell.
4. Giveadviceonhowtoimprovethefamilyenvironment.
Tryandcoverallthefollowingpointswiththefamily.Relatethepointstothespecificissuesthe
familyhasraised.
a. Haveappropriateexpectations
Oncetheworstsymptomshavegone,thefamilymayexpectthepersonwithschizophreniato
getbacktotheirusualactivitiesstraightaway.The family oftenfeels disappointed when the
individual is unable todo so.Theindividualmayinactive,unmotivatedandmayneedtosleep
morethanusual.Ortheymayberestlessandunabletoconcentrateonsmall tasks.Givethe
familythefollowingadvice:
• Encouragethemtohaverealisticexpectationsofwhattheindividualcando.
• Encouragethemtoviewtheindividualashavingaseriousphysicalillness,which requires
alongtimeforresting.Howevertheycaneventuallyrecover.
• Discouragethemfromthinkingtheindividualisjustbeinglazy.

130
• Encouragethemtocomparethe individual’scurrentbehaviorwithhow itwasamonthor
moreago.Thishelpsthefamilymemberstoseethepositivechanges.
b. Setlimits
Tell the familythat justbecausethe individual is ill, the familydoesnotneedtodowhatever
theyask. Instead,helpthemtoset limitsontheunacceptablebehaviors.
• Help them to decide which behaviors are intolerable (for example violence) and which
are irritating but tolerable (for example, not eating in the correct way). When the
intolerablebehavioroccurs, theymust immediately lettheindividualknowthatthisisnot
acceptable.Theaimistostopapatternofbehaviorsfromstarting.
• Advisethefamilynottodiscusswiththeindividual thereasonsforsettingthe limitorhow
they feel about it. Tell them to only state that the behavior is unacceptable, without
explainingwhy.
• Advise the family that the individualshouldbeencouraged to behave inaway that is
usualfortheirage.Forexample,anadultshouldnothave tantrums.
• Tell the family thatitwillbedifficultatfirsttosetlimits.Itmaytakeanumberofweeks.
Encouragethemnottogiveuptrying.
• Tell the family that they shouldnot ignore behaviors such as suicidal threats or violence.
SeeChapter18forhowtoaddressthesesituations.
• When the individual behaveswell, advise the family to reward them. This can be through
givingfood,allowingthemtodoafavouriteactivity,orthroughsmiling,pattingandpraising
them.Askthefamilytothinkaboutwhichrewardisthemostuseful.
• Whenthe individualdoesnotbehavewell, the familyshouldstoprewardinghimorher. If
possible, the individual should be taken away from the others for a short period and
returned when the individual is behaving well again. For example, when the individual
disturbs others by shouting, then he or she should be taken to another room and not
spokentountilhestops it.Howeveritmaybedifficulttodothiswhentheindividualisvery
unwell.
c. Reducestress
Remindthefamily thattheindividualshouldnotbeputunderalotofstress.Use thestress-
vulnerabilitymodel tohelpexplain(seeSection2.3).

131
• Tell the family to try and reduce arguments and nagging behaviours (e.g. constantly
commentingnegativelyaboutwhatthepersonisdoing).
• Tellthefamilynottobeverycriticaloftheindividualorhostiletowardsthem.
• Advise familymembers against talking about complex and emotional topicswhilst the
individualisthere,forexamplediscussingproblemswithmoney.
• Advisethemthatbeingveryenthusiasticorshowinglotsofconcerncanbeupsettingfor
theindividual.Askthemtotryandreducethesebehaviours.
• Advise them that iftheindividualwantstobealone the family shouldallow it.Theydo
notneedtobeinvolvedineverythingtheindividualdoes.
d. Improvecommunication
• People with schizophrenia often do not reply straight away when they are spoken to.
Advisethefamilymemberstoavoidspeakingontheindividual’s behalfwhenthisoccurs.
Advisethemtowaitfortheindividualtorespond.
• Advisethefamilytoavoiddetailedconversations,whichtheindividualmay findconfusing.
e. Getthefamilyroutinebacktonormal
Discuss with the family the problems that comewhen the individual is the centre of their
lives. Tell them that since schizophrenia is a long-term illness, after some time they may
becometoostressedtobeabletolookafter the individual.Theymayalsodevelopproblems
of their own.As far as possible, encourage them to startagain the daily routines that they
hadbefore the illness. Advise them to thinkabout the needsof other familymembers, for
examplechildrenorsiblings.
f. Strengthensocialnetworks
Sometimes family members think that they should not worry other people with their
problems. Theymayalsoworryaboutthereactionsofothers.
• Discuss with the family the benefits of discussing their problems with others like
relatives, friends, neighbours, religious or community groups. This may help to reduce
theirdistress. Italsohelpsthemtothinkofnewandbettersolutionstotheirproblems.
• Tell the familymembers that theywill notbe able tocare for the individual for a long
timeunlesstheylookafterthemselvesaswell.
132
g. Treattheindividualwithrespect
Discuss the importance of respecting the individual as an adult who can make decision for
themselves
5. Discussunhelpfulcopingstrategies
Sometimes family members do things that are not helpful or may even make the family
environmentworse.Theseinclude:
• Thefamilymaytrytopersuadetheindividualthattheirunusualideasarenottrue.This
mayleadtoargumentsand angryresponsesfrombothsides.
• Evenwhenitisclearthattheindividualdoesnotmakesense,familymembersmaytryto
findameaningfulmessageinwhatthepersonissaying.
• Sometimes the family members ignore the symptoms and pretend the illness is not
important.Thisisunhelpfulwhenthesymptomsareverybad.
• Familymembersmayconstantlysupervisetheindividual,astheyarenotsurewhatthey
willdonext.Thismakesthefamilymemberfeelmoreincontrol.However, it isdifficult
forthefamilytomaintain this constantsupervisionfora longtime.
• Theneedsofotherfamilymembersareignoredbecausetheneedsoftheindividualareso
great. This may mean that other family members feel uncared for and problems with
familyrelationshipshappen.
6. Giveadviceonhowtoimproveparenting
• Whentheindividualiswell,encouragethemtospendtimewiththechildrenandtotakeon
theirusualparentingtasks.Forexample,helpingthechildrentodressandwash.
• Discusswiththefamilyhowtheycansupporttheindividualtogetbacktotheseactivities.
Askthefamilytogiveencouragementwhentheindividualdoestheactivities.
• Ifyouareconcernedaboutthesafetyofthechild, informyoursupervisor(seeChapter14
andChapter35).
7. Makeaplan
Askthefamilytoconsiderwhatspecificthingstheywilltrytododifferently.
133
Followup
Check how for progress at the next home visit. Ask what the family tried, and how easy or
difficultthiswas.Asktheindividualandfamilyifthefamilyenvironmentfeelsanydifferent.
25.5 Summary
• Sometimesthereareproblemswith inthefamilywhenapersonhasschizophrenia.These
includethefamilybeingtoocriticalorover-involvedintheindividual,ortherebeinglotsof
conflict
• Problemsinthefamilyenvironmentworsenillnessandcausestressforcaregivers
• Ways to improve the family environment include: setting limits, having appropriate
expectations,reducingstress,improvingcommunicationandgettingthefamilyroutineand
sociallifebacktonormal
• Waysto improveparenting include:whentheyarewellencouragethe individualtospend
time with the children and ask the family to support the individual with this
Yosef’sstory
YosefandAddisagreethatthereare lotsofargumentswithinthehousehold.Theyusually
argueaboutthefactthatYosefisstillnotworking,eventhoughinsomewaysheisbetter.
Yosefalsocomplainsthatheneverhasanytimealone.
Berhanhelpsthemtodiscussthistogetherinacalmway.Shesuggeststhatthefamilyneed
tohaverealisticexpectationsofYosefandthatitmighttakealongtimeforhimtogetback
to his previouswork. Addis agrees that shewill try not to nag Yosef. They discuss that it
might be useful for Yosef to spendmore time alone during the day, at least whilst he is
feelingwell.
134
26 Module:Takingpartincommunitylife
26.1 Whatproblemsdopeoplewithschizophreniahavetakingpartincommunitylife?
It iscommonforpeoplewithschizophreniatohaveproblemsdoingtheusualactivities inthe
community.Peoplemayhaveproblemswith:
• Attendingweddingsandfunerals
• Drinkingcoffeewithfriendsandneighbours
• Visitingrelatives
• TakingpartinEdirmeetings
• ParticipatinginthepracticalactivitiesofEdir
• Participatinginkebelemeetings
• Attendingchurchormosque
• Participatinginreligiousgroups,suchasmahaberorlika
• Goingtomarket
• Participatinginothercommunityorganisations,suchastheWomen’sassociation
26.2 Whydopeoplewithschizophreniahaveproblemstakingpartincommunitylife?
• Theillnessmakesthemunmotivatedtogooutside
• Theillnessgivesthemproblemswithsocialskills,suchasdifficultiesstartingaconversation
ortakingturnstospeak
• Medicationsideeffects,suchasdrowsiness,makeitdifficulttogettheenergytowalk
somewhereandsocialise.
• Thefamilydoesnotlettheindividualattendcommunityeventsbecausetheyareworried
theywillbehavestrangelyordosomethingembarrassing
• Communitymembersmayhavestigmatisingattitudestowardspeoplewithschizophrenia.
Thismeanstheymayignoretheindividual,notallowthemtoparticipateinactivities,not
respecttheiropinionorevenshoutnamesatthem.
26.3 Whyisitimportanttotakepartincommunitylife?
• Tofeelpartofthecommunity
• Improvetheirsenseofwell-being
• Improvetheirself-confidence
• Reducestigmatowardsthem

135
• Reducedburdenonthefamily
• Keepthepersonengaged inuseful tasks
• Distract fromdistressingsymptoms likehallucinationsanddelusions.
26.4 Whatcanwedotohelppeoplewithschizophreniatakepartincommunitylife?
Principles
• Focusontheareaswherethereareproblems,andwhichareimportanttotheindividualto
change
• Establishwhatisnormalforthehouseholdandtheindividual
• Involvethefamilyateverystageoftheprocess.Theaimisforthemtobeabletosupport
theindividualtodotheactivitieswhenyouarenotthere.
1. Explainwhyyouaredoingthismodule
Explaintotheindividualandfamilythatproblemstakingpartincommunitylifearecommonin
peoplewithschizophrenia.Givereasonswhypeoplewithschizophreniahavetheseproblems.
2. Discusswhatproblemstheindividualhas
Discusswhatproblemstheindividualhashadtakingpartincommunitylife
3. Identifytheactivitiestheindividualwantstodo
Findoutwhichcommunityactivitiestheindividualwouldliketodobutishavingdifficultywith
atthemoment.Youshouldreferbacktothelatestneedsassessment.
4. Identifybarriersandsuggestwaystoovercomethem
You should discuss with the individual and their caregiver why they think they are having
problemstakingpartinthesecommunityactivities.Lookatthesection26.2forsuggestions.The
mostappropriateapproachforhelpingindividualstotakepartincommunitylifewilldependon
thetypesofbarriers.Youshouldalsousetheproblemsolvingapproachtohelpyou(seeSection
10.5).Youcansuggestsomeorallofthefollowing:
a. Improvesocialskills
• Asktheindividualandfamilymembertothinkaboutwhatsocialskillstheyneedtodothe
communityactivitiestheywouldliketobeinvolvedin.Thesemightinclude:
o Greetingothers
136
o Listeningtoothers
o Askingforinformation
o Expressinganopinion,forexampleabouttheirowntreatment.
o Sayingsorrywhenthisisneeded
o Eatingwithothersinapoliteway
Nowdiscusswith the individual and caregiverwhich things the individual hasproblemswith.
Focusonthesethings.
• Asktheindividualtopracticetheseskillswithyou.Forexample,
o Askthemtoshowyouhowtheywouldgreetaneighbourtheymetatchurch.
o Askthemtoshowyouhowtheywouldaskthepriceofsomethings,forexample
cabbageatthemarket
• Giveencouragement,includingsmilesandpraise,whentheindividualshowstheycandothe
skill
• Asktheindividualtotrytheskillsinareallifesituation
b. Inviteneighboursorrelativeforcoffee
Suggestthatthefamilyinviteneighboursorrelativestothehometodrinkcoffee.Thiscanbea
chancetopracticetalkingtofamiliarpeopleinafamiliarenvironment.
c. Familymemberaccompaniesthepersontocommunityactivities
Suggest thata familymembergoeswith the individual to thecommunityactivity for the first
few times. Thiswill give the individualmoremotivation and confidence. The familymember
maybeworriedthattheindividualwillbehaveinanembarrassingway.Suggestthattheystart
withactivitiesthatareclosetothehouseandinvolvefewerpeople.Forexampleitmaybeless
stressfultogotothegrainmilltogether,thantoattendafuneralwithmanyguests.
d. Engagewithcommunityleaders
Withthehelpoftheindividualandthecaregiver,identifykeypeoplewithinthecommunitywho
maybeabletohelptheindividualtogetbacktousualactivities.Consider:
o Religiousleaders,whomaybeabletohelpthepersongotochurch,mosqueora
religiousgroup(mahaberorlika)
137
o Edirleaders,whomaybeabletohelpthepersoncontributetoEdirandparticipatein
theEdiractivities
o LeadersofYouthAssociation,Women’sAssociationorkebeleleaders,whomaybeable
tohelpthepersonattendmeetingsandcontributetokebeleaffairs
Ifyouhavenotalreadydoneso,itmaybeappropriateforyoutomeetwiththeleadertogive
theminformationaboutschizophreniaandtoseehowtheycanhelp.SeeTasks8,9and10in
CommunityEngagementChapter31.Alternativelythecaregivermaybewillingtoapproachthe
leaderindependently.
e. Useapproachesfromothermodules
Someoftheapproachesfromothermodulesmayalsocontributetowardshelpingindividualsto
takepartincommunitylife,forexample:
• Community-awarenessraising(seeChapter31),whichaimstoreducestigmaand
discriminationtowardspeoplewithschizophrenia
• Improvingadherenceandimprovingsideeffects(seeChapter20)
• Givingtheindividualstrategiestodealwithstigmatisingattitudes(seeChapter28)
• Improvingtheattitudeofthefamilytowardstheindividual(seeChapter25)
• Dealingwithdistressingsymptomssuchashallucinations,lackofmotivationandproblems
withorganisation(seeChapter22)
f. Actingasarolemodel
Thewayyoubehaveinthekebelecanhaveabigimpactonotherpeople’sattitudes.Whenyou
seetheindividualoutsidewhilstnotinahomevisit,greetthem,asyouwoulddoanyoneelse.
Showingthecommunitythattheindividualisjustlikeotherpeoplemaybeonewaytoreduce
stigma.
YoucanuseTable6asaguideforwhichapproachtouseinwhichcircumstances:
138
Table6Approachestosupportindividualstotakepartincommunitylife
Problem ApproachLackofmotivation • Familymemberaccompanies
• Inviteneighboursorrelatives• Dealingwithdistressingsymptoms
Medicationsideeffects • AddresssideeffectsProblemswithholdingaconversation • Practicesocialskills
• InviteneighboursorrelativesThe family does not let the individualattendcommunityevents
• Improvingthefamilyenvironment• Inviteneighboursorrelatives
Stigmaanddiscriminationfromcommunity • Engagewithcommunityleaders• Actingasarolemodel• Dealingwithstigmaanddiscrimination• Communityawarenessraising
5. Makeaplan
Discusswith the individualwhich specific community activity to focus on first, and agree the
stepstostartparticipatingagain.Makesureeveryoneknowswhattheirroleis.
Followup
Make sure you followup progress on participating in community activities at the next home
visit.Discusswhatstrategiesweretriedandwhichoneshelped.Practicesocialskillsagainifyou
agreethismayhelp.Ifrelevant,makecontactwithcommunityleadertofacilitateengagement
incommunityactivities
Sara’sstory
Since she became unwell Sara has had problems visiting her sisters in the neighbouring
kebele.Thisissomethingsheusedtoenjoyalot.Oftenshedoesn’tgobecauseshedoesn’t
havetheenergy to leavethehouse.She isalsoworried that shedoesn’thaveanything to
say. Berhan discusses with Sara and Alemu, Sara’s husband, how they can change the
situation. Sara suggests that she could invite her sisters to visit her first of all as this will
requirelessenergy.Thenifthisgoeswell,Alemucantrytosupporthertovisitthem.Berhan
helpsSaratopracticehowtogreetpeopleandhowtostartaconversation.Theyallagreeto
tryandinvitethesisterswithinthenexttwoweeks,whichiswhenBerhanwillvisitagain.
139
26.5 Summary
• Many people with schizophrenia have problems taking part in community life such as
attendingchurchorfunerals.
• Helping individuals take part in community life is good for improving self confidence,
reducingstigma,andreducingtheburdenonthefamily
• Waystohelpindividualstakepartincommunitylife:improvesocialskills,inviteneighbours
for coffee, family member accompanies, and engaging community leaders
140
27 Module:Gettingbacktowork
27.1 Whatproblemsdopeoplewithschizophreniahavewithwork?
When we talk about work, it might mean different things depending on the individual and
whethertheyareamanorawoman.Workcaninclude:
• Farmworkonthefamilyfarm
• Dailylabouringonotherpeople’sfarms
• Householdworke.g.fetchingwood,fetchingwaterandpreparingfood
• Paidemploymentforexampleinashop
• Tradingatmarket
Manypeoplewith schizophrenia have problemswithwork. Theymay find they canwork for
shorterperiodsoronlyonsimpletasks.Someindividualsfinditdifficulttoworkatall.
27.2 Whydopeoplewithschizophreniahaveproblemswithwork?
• Theyareunwellandhavelotsofsymptoms
• Theillnessmakesitdifficulttoconcentrateandbeorganised.Forexample,handlingmoney
atmarketmaybecomedifficult.
• Medicationsideeffects,suchasdrowsinessandshakinghands,makeitdifficulttowork,
particularlyifitinvolvesphysicallabour
• Theillnessgivesthemproblemswithsocialskills
• Thefamilydoesnotlettheindividualdotheirusualworktasksastheyareconcernedthey
willdoitwrong
• Communitymembersmayhavestigmatisingattitudestowardspeoplewithschizophrenia.
Thismeansitmaybedifficulttogetpaidwork,forexampledailylabouring,withinthe
community.
• Theyarerestrainedathomesocannotwork.
• Inbetweenperiodsofbeingwellandabletowork,theindividualhasrelapses,duringwhich
timeitisnotpossible.Thiscanmaketheindividualseemunreliable.
• Whilsttheywereunwelltheymayhavelosttheirfarmlandorcattle.Thismaybebecause
theyhadtosellthemtogetmoneyformedicationorbecausetheywereunabletowork.Or
thelandorcattlemayhavebeengiventoanotherfamilymembertolookafter.
• Theillnessmakesthemunmotivated.

141
27.3 Whyisitimportanttogetpeoplewithschizophreniabacktowork?
• Helpstoimprovetheeconomicstatusofthefamily
• Improvesself-esteemandconfidence
• Helpstostoptheindividualfromthinkingabouttheirsymptoms
• Reducesisolationandimprovessocialskills
• Ifthepersoncanworkalone,thismeansthecaregiverdoesnothavetostaywiththem,and
theycandotheirownusualactivities
• Improvesrelationshipwithfamily
27.4 Howcanwehelppeoplewithschizophreniatogetbacktowork?
Principles
• Focusontheareaswherethereareproblems
• Establishwhatisnormalfortheindividual
• Goslowlyandsteadily;theyshouldn’ttakeontoomuchworktoosoon.
• Involvethefamilyateverystageoftheprocess.Theaimisforthemtobeabletosupport
theindividualtoworkwhenyouarenotthere.
1. Explainwhyyouaredoingthismodule
2. Discusswhatproblemstheindividualhashadwithwork
Discusswhatproblemstheindividualhashadwithworkandwhytheyhavehadthem.
3. Identifytheworktheindividualwantstodo
Establishwhatwasworkwas normally done by the individual before they became unwell. If
theyusedtodoseveraltypesofwork,forexamplegoingtomarket,lookingafterthehousehold
anddoingfarmwork,discusswiththeindividualandfamilywhichtypeofworktostartwith.It
isusuallysensibletostartwiththesimplesttypeofwork.
4. Considerwhatpreparationisneeded
This will depend on the type of work and the wishes of the individual and family. If the
individual needs to engage with people outside the family during work, for example daily
labouring, theirneedsmaybedifferent. Itmightbenecessary toensure theyhavegoodself-

142
care, improved social skills and the symptoms are under control. If the person plans only to
workonthefamilyfarm,itmightbelessimportanttoachievethesethingspriortodoingwork.
5. Tryspecifictasks
• Onceyouhavedecidedthetypeofwork,askthefamilytoselectonespecifictaskwithin
this.Forexample,ifthefocusisonfarmworkthefirsttaskselectedmightbelookingafter
thecattle.Askthefamilyandindividualtoselectataskthatis:
• Somethingtheindividualusedtodo,orisexpectedtodo
• Somethingwhichtheindividualfeelsreadytotry
• Withthefamily,breakdownthespecifictaskintoindividualsteps.Forexample,thesteps
involvedinlookingafterthecattleare:
• Untyingthecattle
• Takingthemtothefield
• Watchingthemwhilsttheygraze
• Asktheindividualtotrydoingthetaskwithafamilymemberpresent.Theyshoulddecidein
advancewhichoftheindividualstepsthefamilymemberwilldo,andwhichtheindividual
willdo.Theyshouldgraduallyworktowardstheindividualdoingallsteps.Evenifthe
individualmakesamistakethefamilyshouldgiveencouragementtocontinue.
• Discussthattheindividualwillprobablyonlybeabletoworkforshortperiodsatthe
beginning.Theymayneedtolotsofrestswhilstdoingwork.
• Oncetheindividualisabletodosomeofortheentirespecifictask,chooseanothertask
togetherandrepeatstepsatocagain.
6. Encourageindependentworking
As the individualbecomesmoreconfidentandable tocomplete thespecific tasks, the family
membersshouldencouragethemtoworkindependently.
7. ConsideraskingcommunitymembersoranNGOfortheirinput
In somecasesyoumayneed thehelpof community leadersandothercommunitymembers.
Any meetings with other community members should be done with the permission of the
individualandfamily.
143
• Inyourinitialmeetingswithcommunityleadersyoushouldhavefoundoutthepotentialfor
daily labouringandotherpaidemploymentopportunitieswithin thekebele (seeTask7 in
CommunityEngagementChapter31).Ifyoufoundtherewereanyopportunities,youshould
nowdiscussthemwiththe individualandfamily.FollowTask15 inChapter31forhowto
followuptheseopportunities.
• If they lost their farmlandor cattlewhilstunwell, youmayalsoneed toaska community
leaderforinput.
• DiscusswithyoursupervisorifthereisalocalNGOwhocanoffersomelivelihoodsupportor
skilldevelopment.
8. Identifyingbarriers
You should discuss with the individual and their caregiver why they think they have had
problemsdoingtheworksofar,andwhatpotentialproblemsmightariseiftheytrytodothe
worknow.LookattheSection27.2forsomesuggestions.Youcanalsouseaproblemsolving
approach (see Section 10.5). Try to address these barriers alongside trying the specific tasks
(step 4). This will increase the chances of the person being able to work.

144
Table7Approachestosupportindividualstogetbacktowork
Barrier ApproachUnwellandlotsofsymptoms • Module:Supportingindividualstotake
medicationLacksconfidence • Encouragementandsupportfromyou
andfamilyProblemswithmotivation • Module:Dealingwithdistressing
symptomsProblemswithorganisation • Module:Dealingwithdistressing
symptomsMedicationsideeffects • Module:Supportingindividualstotake
medicationProblemswithholdingaconversation • Practicesocialskills(Module:Takingpart
incommunitylife)The family does not let the individualwork
• Module:Improvingthefamilyenvironment
Stigma and discrimination fromcommunity
• Engagewithcommunityleaders• Module:Dealingwithstigmaand
discrimination• Communityawarenessraising• Actingasarolemodel
Relapse • Module:TakingcontrolofyourillnessFarm land has been taken by kebeleadministration
• Engagewithcommunityleaders
Farmlandhasbeentakenbyotherfamily • Identifywhohasdecision-makingpowerwithinfamilyanddiscusswiththemthebenefitsofindividualstartingtoworkonorlookafterownlandorcattleagain
• Module:Improvingthefamilyenvironment
Farmlandlostduetopoverty • Engagewithcommunityleaders• EngagewithNGO
9. Difficultsituations
Theindividualorfamilymayaskyouforfinancialhelp,foraloanorforajob.Ifthishappensyou
shouldexplainthatunfortunatelyyouarenotabletoprovideanyofthesethingstothemor
indeedtoanyofthepeopleyouareworkingwith.Tellyousupervisoriftheindividualorfamily
continuetoaskyouaboutthis,andconsiderdiscussingtogether.
10. Makeaplan
Makesureeveryoneknowswhatstepstheywilltakebeforethenexthomevisit.

145
Followup
Onceyouhavestartedhelpingtheindividualtogetbacktoworkitisimportantthatyoufollow
thisupeverytimeyouseethem.
• Checkwhatprogresshasbeenmadewithspecifictasks.
• Checkwhatprogresshasbeenmadeoverall.Forexample,howmuchofthedaydoesthe
individualspenddoingfarmwork?Howdoesthiscomparetowhentheywereveryunwell?
Howdoesthiscomparetowhentheywerewell?
• Checkforanyproblems.Inparticularwhethertheworkistoostressfulortheindividualfeels
theyarenotbeinggivenenoughresponsibility.Trytochangetheplantofitbetterwiththe
individual’sneeds.
• Checktheprogresswithanylinksmadewithcommunitymembers
• Reviewanybarriersthatarestillpresentandtrytoaddressthemusingthesuggestions
above.
27.5 Summary
• Manypeoplewithschizophreniahaveproblemswithwork.Thismaybeduetotheillness,
medicationsideeffectsandstigma
• Gettingbacktowork is importantas ithelpsto improveconfidenceandsocialskills,bring
moneyintothefamilyandreducestigma
• Tohelptheindividualgetbacktowork:decidewhatpreparationisneededthentryspecific
tasksbrokendownintosteps.
• Consider working with community leaders to help find work within the community
Yosef’sstory
Yosefnolongerdoesanyfarmwork.Beforehebecameunwellhedidallthenecessarytasks.
Hesaysthereasonhedoesn’tdotheworkisbecauseheusuallyfeelstiredandunmotivated,
andtheworkseemsoverwhelming.YosefandhisfamilyagreeYosefisreadytostarttrying
toworkagainashissymptomsarequitewellcontrolled.Theyagreehewillstartbyhelping
hisfathertothreshthewheat.Beforehestartstheydiscussthespecificstepsinvolved,and
agreethatYosefshouldonlyworkforashorttimeinitially,beforehavingarest.

146
28 Module:Dealingwithstigmaanddiscrimination
28.1 Whatproblemsdopeoplewithschizophreniahavewithstigmaanddiscrimination?
InChapter6you learntabout theproblems thatpeoplewith schizophreniahavewith stigma
anddiscrimination.
28.2 Whydopeoplewithschizophreniahaveproblemswithstigmaanddiscrimination?
Stigma can be found in familymembers, communitymembers and healthworkers. A person
mayalsostarttobelievethestigmatisingthingsthatpeoplesay–thatiscalledself-stigma.
28.3 Whyisitimportanttoreduceexperiencesofstigmaanddiscrimination?
Stigma and discrimination can mean that individuals find it more difficult to return to the
activitiesthattheyusedtodowhentheywerewell.Peoplewithschizophreniamaycontinueto
bediscriminatedagainsteventhoughtheyhaverecovered.Itcanbeupsettingtofeelseparate
anddifferentfromfamily,neighboursandcommunity.Peoplewithschizophreniaoftenfeelthat
stigma and discrimination is even more distressing than the symptoms of the illness. It is
therefore important to reduce stigma and discrimination. Individuals may get back to usual
activitiesfasteriftheseproblemsareaddressed.
28.4 Howcanwereduceexperiencesofstigmaanddiscrimination?
1. Explainwhatstigmaanddiscriminationis
Explainwhatyoumeanbystigmaanddiscrimination
2. Explainwhyyouaredoingthismodule
Explainwhyitisimportanttoreduceexperiencesofstigmaanddiscrimination.
3. Discussexperiencesofnegativecommentsanddiscrimination
Firstofall,discusswhatexperiencesofstigmaanddiscriminationtheindividualhashad.Discuss
whathappenedandhowitmadethemfeelaboutthemselves.Iftheindividualhastrouble
thinkingofanyexperiences,youcanyouuseSection6.2topromptthem.Rememberthismight
beupsettingfortheindividualandfamily.
4. Encouragetheindividualtothinkaboutthemselvesinapositiveway

147
Discusswiththeindividualthatevenifwecannotcontrolthewayotherpeopleseethem,they
should still see themselves as a valuableperson. Tell the individual that the illness is not the
onlyimportantthingaboutthem,andthattheycanrecoverandhaveameaningfullife.
5. Discusshowtodealwithnegativecommentsanddiscrimination
a. Discusshowtheindividualdealtwiththesituationatthetime.Forexample,whattheydid
whensomeonecalledthemaninsultingname.Discusswhetherthewaytheyresponded
wasusefulornot.
b. Discussotherwaystheindividualcouldrespond.Forexample,itmaybeusefultopractice
explainingtheillnesstoothers.Youcouldsuggestthattheindividualtriessaying,“Ihavean
illnesslikeotherillnesses.Iamtakingthemedication,whichmakesmebetter“or“This
illnesscouldhavehappenedtoanyone.”
6. Discusswhichwaysofrespondingwouldnotbeuseful.
Forexample,gettingintoafight.
7. Discussthecaregiver’sexperiencesstigmaanddiscrimination.
Youcanrepeatthesestepswiththecaregiver.
8. Discusswhatotherapproachesmayreducestigma
TherearemanypartsofCBRthathelptoreducestigmaanddiscrimination.Theseinclude:
a. Giveinformationaboutschizophreniatothepersonwithschizophreniaandtheirfamily(see
Chapter16).Inparticular,focusonthepossibilityofpositiveoutcomes.
b. Awareness-raisingamongstcommunitymembersandcommunityleaders(seeChapter31).
Oncepeoplehavemoreinformationtheyarelesslikelytohavenegativeattitudestowards
peoplewithschizophrenia.
c. Supportingindividualstoimproveself-care,togetbacktotheirusualactivitieswithinthe
communityandtogetbacktofarmworkoremployment(seeChapter26and27).When
peopleinthecommunityseetheindividualdoingusualactivitiesagain,thiswillhelpto
reducetheirignoranceandprejudicetowardspeoplewithschizophrenia.

148
d. Supportingaccesstotreatmentandsupporttakingmedicationswillhopefullyimprove
symptoms(seeChapters17and20).Thismakesitmorelikelythefamilyandcommunitywill
treattheindividualasnormal,andalsoshowspeoplethatschizophreniaistreatable.
e. Iftheindividualortheirfamilyisworriedthathomevisitsbyyoumaybringnegative
attentiontothehousehold,suggestyouholdthesessionselsewhere,forexampleatthe
healthpost.
f. SetupaFamilySupportGroupsothatthepersonandtheirfamilycansharetheir
experiences,includingwaystodealwithstigma.Thegroupscanalsobeawaytoimprove
self-esteem(seeChapter32).
g. Encouragethefamilytoaccepttheperson’sillnessandtreattheindividualinadignifiedway
(seeChapters19and25)
h. Treattheindividualwithrespectanddignityyourself(seeChapter11).
9. Makeaplan
Agreewhatactionstheindividualandfamilywilltakebeforethenextsession
Followup
Atthenextsessioncheckiftherehavebeenanynewexperiencesofstigmaordiscrimination
andifsohowtheindividualdealtwithit.Askwhetherthestrategieswereuseful.Discusshowto
changethestrategyfornexttimeithappens.
Sara’sstory
Sometimes children in the kebele shout at Sara that she is mad. They laugh at her and
sometimes throw stones. Sara finds this very upsetting and itmakes her want to stay at
homeallthetime.Whenithappensusuallysheignoresthechildren,whichisquitehelpful.
However,shetellsBerhanthatshewouldfeelmoreconfidenttogooutsideifshehadsome
wayofresponding.SaraandBerhanpracticehelpfulthingsthatSaracansayinacalmway
tothechildrennexttime.Theyagreethatitisnothelpfultothrowstonesback.Alemuagrees
thatitisalsonothelpfulwhenhecallsSaranames.SaraandAlemuagreetotrytheseideas
before they next see Berhan in one month’s time. Berhan tells Sara that she is doing
awareness-raising in the kebele, which hopefully will improve the attitudes of community
members,includingthechildren.

149
28.5 Summary
• Stigmaanddiscriminationisacommonexperienceforpeoplewithschizophrenia
• Itisimportanttoreducestigmabecauseitisabarriertoreturningtousualactivities
• Ways to reduce stigma include: helping the family and community to understand
schizophreniabetter,supporting individualstogetbacktousualactivitiesandgivingthem
strategiestodealwithnegativecomments

150
29 Module:Improvingliteracy
29.1 Whatproblemsdopeoplewithschizophreniahavewithliteracy?
Likemanypeople in rural Ethiopia,oftenpeoplewith schizophreniaarenotable to readand
write.Thisismorecommoninwomen.
29.2 Whydopeoplewithschizophreniahaveproblemswithliteracy?
Peoplewithschizophreniamayhavemoreproblemswithliteracythanotherpeopleiftheyhad
toleaveschoolearlyduetotheillness.Peoplewithschizophreniamayalsofinditmoredifficult
toaccesstheadultliteracytrainingthatisavailableineverykebele.Thismaybebecauseof:
• Beingtoounwelltotakepart
• Havingproblemswithmotivationorproblemsthinkingclearly
• Stigmaanddiscriminationmeaningpeoplewithschizophreniaareexcludedsimplybecause
oftheirillness.
29.3 Whyisitimportanttoimproveliteracy?
Improvingliteracyinpeoplewithschizophreniamayhavethefollowingbenefits:
• Improveself-esteemandconfidence
• Providesameaningfulactivity,whichmaydistractfromsymptomsandsideeffects
• Helpstogetbacktousualactivitiesforwhichithelpstoreadandwrite,forexample
participatinginkebeleorediractivities,orconductingbusiness
29.4 Howcanwehelptoimproveliteracyinpeoplewithschizophrenia?
Principles
It isnotyour role to teach the individual to readandwrite. Insteadyoushouldhelp themto
accessexisting facilitiesusing the following steps.Beforeyouundertake thismodule, confirm
thatthereisadultliteracytrainingoraschool(iftheindividualisschoolage)inthekebelethat
isacceptingstudents.Discusswiththeco-ordinatororheadteacherwhetherthereisanyreason
whyaneligiblepersonwith schizophreniacouldnotattend, if theywished to.SeeTask15 in
CommunityEngagementchapter.Ifthereisafacilityavailable,continuethefollowingsteps.
1. Explainwhyyouaredoingthismodule
Explainwhyitmaybeimportantforsomepeoplewithschizophreniatoimproveliteracy

151
2. Findoutthelevelofliteracyoftheindividual
• Howmanyyearsdidtheygotoschoolfor?
• Howlongagoweretheyatschool?
• Cantheywritetheirname?
• Cantheyreadshopsigns?
3. Confirmtheindividualisinterested
Confirmthattheyareinterestedinlearningtoreadandwrite.
4. Arrangeattendanceatfacility
Asktheindividualandfamilymembertoapproachtheliteracygrouporschooltoarrange
attendance.Iftheindividualandfamilyarenotwillingorabletomaketheinitiallink,arrangea
meetingwiththeco-ordinatororheadteacheryourself.Discussthepotentialbenefitsforthe
group/schoolandfortheindividual.
5. Helptheindividualtoattend
Facilitatetheindividualtoattendthegroup/schoolifthishasbeenarranged.Forexample,
discusswiththefamilywhowilltakethemtothefacility.Itmaybepossibleforafamilymember
tositinthegroupinitially.
Followup
Followupprogresseachtimeyouseetheindividual.Askthefollowingquestions:
• Hastheindividualattendedthegroup/school?
• Werethereanyproblems?Ifsotrytouseaproblemsolvingapproachtoaddressthem.
• Istheindividualnoticinganybenefits?
29.5 Summary
• ManypeopleinruralEthiopiaareunabletoreadandwrite,butthismaybemorecommon
inpeoplewithschizophrenia
• Learning to read and write may help with confidence, and getting back to work or
communityactivities
• You should not teach the individual to read and write but you can help them to access
existing services
152
30 Module:Takingcontrolofyourhealth
30.1 Whatproblemsdopeoplewithschizophreniahavewithrelapse?
Most people with schizophrenia have an ‘up and down’ course of the illness. This means
sometimes they feel well and have no symptoms, while at other times they experience a
return of symptoms.When symptoms return in away that is problematic and distressing,
thisisknownasarelapse.
30.2 Whydopeoplewithschizophreniahaverelapses?
Different people experience relapses due to particular reasons and the time between
relapses also varies a lots. Most often relapses develop gradually over a period of a few
weeks. But some people experience a relapse very quickly, in a matter of days. Not taking
medicationmakesitmorelikelythatarelapsewillhappen.Somestressfulsituationscantrigger
arelapse,including:
• Illnessordeath in thefamily
• Change indailyroutineor livingarrangement
• Argumentorrelationshipproblemwithfamilymemberorneighbour
• Newresponsibilities,forexampleduetofamily illnessorrelativesvisiting
• Physicalillness
• Khatoralcoholuse
Whataretheearlywarningsignsofrelapse?
Duringthetimebefore the relapse, there are changes inthepersonwithschizophreniathat
are called ‘early warning signs’. Thesewarning signs are often unique to each person.The
personwithschizophreniaandfamily memberscanoften identify themsince theyhaveseen
this happen a few times. These early signs of a relapse are important to recognize and
respond to, since this can be a timewhen something can be done to stop the person from
sufferingtheseriousconsequencesofa relapse.Themostcommonearlywarningsignsare:
• Tensionandnervousness
Individualsmay report feeling anxious,nervousor tenseabout small things that theywould
not usual ly worry about. People feel worried,walk around the house excessively, and are
unabletorestbysitting inoneplace for long.
• Sleepdisturbances
Manypeople with schizophrenia experience changes in their sleeping habits. They either

153
have difficulty insleepingor startsleepingmorethannormal.
• Feelingsadandangry
Individualsmay feel sad all the time. This can lead the person feeling hopeless and having
suicidal ideas. Family member may notice that the person is talking less, hardly smiles,
looks worriedandisoftentearful.
• Becomingisolatedfromothers
Manypeoplewillbecomewithdrawnandlessinterestedintalkingtopeople. This isoften
noticed firstby familymembers as theperson becomesquieter, doesnotmeetguests,and
avoids going out of the house. There can bemany reasons for the social isolation. Some
people feel tense and anxious if they have to talk to someone, while others can start
feeling suspicious of people and decide the best way to deal with it is by reducing social
interactions.
• Difficulty inconcentration:
Individualsmay find itmore difficult to concentrate and pay attention to something for a
period of time. This leads to difficulty in following a conversation, cooking a meal, or
rememberingtogetthingsfromashop.
• Reducingorstoppingmedicines
Sometimes the personwith schizophrenia does not realize that they are going to have a
relapse.Becauseofthistheymaydecidetoreduceorstopthemedication.Theymayalso
refusetogotothehealthcentreorrefusetoseeyou.
• Changeinappetite
Beforearelapsepeopleoftenchangetheireatinghabits.Usuallythereisalossofappetite.
This can sometimes lead toa loss ofweightand to ageneral senseof tirednessand lackof
energy.Lesscommonly,peoplemaystartwantingalotoffoodseveraltimes aday.
• Uniquesignsofrelapse
Quite often, family memberswill be able to describe particular signs of a relapse that are
uniquetotheindividual and tend tooccuronly in suchsituations.
30.3 Whyisitimportanttopreventrelapse?
During a relapse, most people are too unwell to do farm work, housework or other usual
activities.Evenafterthesymptomsstop,itcantakeafewweeksormonthsfortheperson to
return to the previous level of functioning. Some people may even feel that they want to
commitsuicideduringthis timeduetoconstantlyhearingvoicetellingthemnegativethingsor

154
becausetheyhavedevelopeddepression.Others canbecome very suspicious and frightened.
This is also the timewhen some people become irritated andeasily angry; rarely, there can
beariskofharmfromthe persontoothersinthefamilyorcommunity.Thefamilymayfeel
they have no choice but to tie up the person with schizophrenia. After a relapse the
individualmayalsohaveasenseof failure (‘Thishappened inspite oftryingsohardtostay
well’). Theymayalso feelmorestigmaanddiscrimination from their family, neighbours and
community. Having a serious relapse is a setback for everyone and preventing this from
happening isoneofthemostimportantgoalsofCBR.
30.4 Howcanwepreventrelapse?
Principles
Relapse prevention involves helping the person with schizophrenia and the family to
recognizetheearlysignsofarelapseandputting inplaceaplantodealwith the situation.It
is a jointeffort involvingyou, thepersonwith schizophrenia and the family.Thefocusshould
beonhelpingtheindividualtotakecontroloftheirownhealth. Theaimsofrelapseprevention
are:
• Topreventa relapsefromhappening.Unfortunatelythisisnotalwayspossible.
• Tominimizetheseverityoftherelapsesothatthetimetorecoveryisshortened.
Topreventrelapseweshoulddotwomainthings:
• Firstly,weshouldsupportindividualstotakemedication.
• Secondly,weshouldtryandreducelifestressbyhelpingindividualstocopebetterwith
theirproblems.
Before undertaking thismodule, decidewho to involve. The personwith schizophrenia must
alwaysbeinvolved,aswellastheprimarycaregiverandanyotherkeyfamilymemberswho
the person trusts and is comfortable with.Thegroupshouldbebetween3and5peopleand
will usually involve parents, spouses and in some cases adult children or more distant
relatives.Gatherthegrouptogethertocarryoutthefollowingsteps:
1. Explainwhyyouaredoingthismodule
Give information about what relapse is, what problems it causes and why it is important to
preventit.

155
2. Discusstheproblemsofrelapse
Discusswhat happened during themost recent relapse, for examplewhich symptomswere
mostprominentandwhatusualtasksthepersoncouldnolongerdo.Allmembersofthegroup
shouldbeencouragedtojointhediscussion.
3. Discusstheearlywarningsigns
Explainwhatearlywarningsignsareandaskthegroupwhethertheyusuallynoticeany. Use
theEarlyWarningsignsChecklist(Form17)tomakesureyouhaven’tmissedany.Agreeon3to
5importantsignsfortheindividual.
4. Discussstressfultriggers
Explainthatrelapsecanbecausedbycertainstressfulsituations.Askthegroupwhetherthey
can remember anywhich came before the person’s relapse. Explain that it is useful to think
aboutthesesotheycanbeavoidedinthefuture,wherepossible.
5. Discusstherelapsemanagementplan
Explainthatthepurposeoftheplanistodecideinadvancehowyouwillallrespondtoearly
warning signs.Having aplanmayhelpus toprevent a serious relapse, or help it to resolve
quicker.Theplanshouldbemadejointlywiththegroupmembers.Inparticularthewishesof
the personwith schizophrenia should be sought and included in the plan. They should feel
theyhavesomecontroloverwhathappenstothemduringtherelapse.Recordtheplanonthe
RelapseManagementForm(Form18).Eachmembershouldbeclearonwhattheirrole is. If
appropriate,giveacopyoftheplantoeachmemberofthegroup.Thedetailedpartsofthe
planwill be different for each individual.However formost families the following elements
shouldbeincluded.
a. Familymeeting
Ifearlywarningsignsarenoticedbythepersonwithschizophreniaorfamilymembers,afamily
meeting should be held. Concerns should be discussedopenly and aplan isagreedon. This
process should help everyone, including the person with schizophrenia, to participate as
equals in trying to improve the situation. This process also helps the person with
schizophrenia and family take on responsibility for managing the illness and improve their
senseofcontrol.
156
b. Reviewwhethertheindividualistakingmedicationregularly
Not takingmedication is often an important factor in a relapse. Find out the person’s
reasons forstoppingthemedicine.Takethestepsintheadherencesupportchaptertoensure
theindividualstartsthemedicationagainassoonaspossible.
c. Clinical review
Arrange for a review at the health centre as soon as possible. Inform the person with
schizophrenia and familywhen the appointment is. Check if there are anymajor barriers to
attendingthehealthcentreandtrytoresolvethem.Ifyoufeel theyareunlikelytoattend,you
might need to accompany the person to the health centre. After the review, check if
everyonehasunderstoodtheadvice f romthe nurse .
d. Reducestress
Identify anyobviousstressful situation thattheperson has experienced recently.Ifpossible
try to removeor reduce thestress.Suggest stress management activities,particularly those
thathavebeenusefulinthepast(seeChapter23).
e. Reducealcoholorkhat
Usingalcoholorkhatmaymaketherelapseworse.Youandthefamilyshouldhelptheperson
toreduceorstopusingalcoholorkhat.Forexample,byremovinganybottlesfromthehouse,
providing lessmoney to buy it and by reinforcing any steps taken by him to reduce alcohol
use.
f. Activatesocialandpracticalsupport
Identify relatives, friends and community leaders who may be able to provide social and
practical support. In particular, the caregivermay needmore support during a relapse. For
example,neighboursmaybeabletohelpwiththefarmworkwhilstthepersonisunwell.
g. Monitorthesituation
Yourroleistocloselymonitorthesituation.Ateachvisitcheckwhethertheearlywarningsigns
haveimproved.

157
6. Maketheplan
Ensureeachmemberisclearonwhathisorherroleintheplanis.
Followup
It is a good idea to review the plan every 6 months, to ensure that everyone involved
rememberstheissuesclearlyand anyupdatescanbemade.
30.5 Summary
• Whensymptomsreturn inawaythat isproblematicanddistressing, this isknownasa
relapse.Relapsesareacommonpartoftheillness
• Relapsesmaybetriggeredbystressfulevents
• Youshouldhelpthefamilytodeveloprecognisetheearlywarningsignsandknowthelikely
stressfultriggers
• Youshouldhelpthefamilytomakearelapsepreventionplanwhichusuallyincludes:family
meeting, check medication, review at the health centre and reduce stress
158
31 Communityengagement
31.1 Whyisitimportanttodocommunityengagementwork?
Thecommunitycanhaveapowerfulimpact-bothpositiveandnegative-ontheexperiencesof
thepersonwithschizophrenia.CBRaimstoincreasethepositiveinfluencesofthecommunity,
andreducethenegativeinfluences.Therearemanycommunityresourcesineverykebele(see
Chapter8). It isyour role toensure that thepersoncando thesamecommunityactivitiesas
otherpeopleoftheirageandgender.Thecommunityalsohasanimportantroleinmakingsure
thepositivechangesmadeduringCBRarecontinuedafteryouhaveleft.
31.2 Whatcommunityengagementworkdowedo?
PhaseI
DuringPhase I you shoulddo the following tasks ineachkebelewhereyouareworking. You
shoulddothesetasksatthesametimeasyouaredoingthehomevisitstoeachindividualyou
workwith.Youdon’tneedtodo these tasks in theordersetoutbelow; lotsof the taskswill
overlap. Rememberwhen you talk to community leaders or other communitymembers you
shouldnotrevealthenameorproblemsoftheindividualyouarecaringfor,unlessyouhavegot
theirpermissiontodoso.
Task1:Meetwithhealthextensionworker/s(HEW)
How?
• GettheHEWcontactdetailsfromthehealthcentreandarrangeameeting.Youmayneedto
spendbetween2hoursandawholedaywiththeHEW.
• CheckwhethertheHEWisawareofthepeoplewithschizophreniatowhomyouhavebeen
allocated.Iftheyare,askiftheyarewillingtoshowyouwheretheylive.Askwhatthey
knowaboutthemandwhatproblemstheyareawareof.
• Askthemwhotheimportantcommunityleadersare(seeTask2)andiftheHEWwouldbe
willingtomakeinitialintroductions
• Askwhattheimportantcommunityresourcesare(seeTask3)
• Explainwhatyourrolewillbeintermsofhomevisitsandcommunityengagement
• Explainhowyouwouldlikethemtobeinvolved:supportthemessagesyouwillgiveabout
reducingstigmaanddiscriminationandtheimportanceofaccessingtreatment;dotheir
159
usualhomevisitandofferthecaretheyusuallyprovidetopeoplewithschizophreniae.g.
familyplanning.
• Giveyourcontactdetailsincasetheyhaveanyquestions
Task 2: Identify important community leaders e.g. kebele leader/s, Edir leaders, religious
leaders,traditionalhealers,women’sassociationleader.
How?
• FirstasktheHEWtohelpyou.Iftheydonothavetheinformationuse:HealthCentreof
DistrictHealthBureau(DHB)records;church/mosque;othercommunityleaders
• Getthenames/address/telephonenumber
Task3:Identifykeycommunityresourcese.g.churches/mosque,Edir,adultliteracygroup,
schools,Mahaber/tsewa/likagroups,informalsocialnetworks,women/youthassociations,
NGOs
How?
• AsktheHEWs,kebeleleaderandcommunityleaders
• Iftheydonothavetheinformationuse:HealthCentreorDHBrecordsandchurch/mosque
Task4:Ascertainwhatcommunityworkrelatingtomentalillnesshasalreadytakenplaceoris
plannede.g.communityconversations,engagement/trainingoftraditionalheaders
How?
• AsktheHEWs
• This will help you to plan meetings with community leaders (Task 7) and community
awarenessraising(Task6)
Task5:Meetingswithimportantcommunityleaders
How?
• AsktheHEWstointroduceyoutocommunityleadersifpossible
• Meetwithandintroduceyourselfto5-10importantcommunityleadersfromacrossall
sectors.
• Trytospeaktothesecommunityleadersatameetingoreventthatisalreadyplanned,for
exampleakebelemeeting.Thiswillmakeiteasiertoreachthem.Ifthatisnotpossible,

160
invitethesecommunityleaderstoameeting,eitherinonegrouporsmallgroupsdepending
onthelocalcircumstances.Discusswithyoursupervisor.
• Themeetingmaytakeupto2hours,butcouldbemuchless.
• Atthemeeting,coverthefollowing:
o PurposeofCBRprogramme(brieflydescribeseverementalillness;thepossiblyof
recovering;importanceofmedication;theneedforhelpwithrehabilitationtoo;get
moreproductivecommunitymemberattheend,benefitswholecommunity),
o AuthorisationgiventoCBRprogramme(linkstodistricthealthbureauandAddisAbaba
University)
o GiveoutlineofCBRactivities,includinghomevisitsandtypesofmodules
o Giveoutlineofcommunityengagementactivities(communityawarenessraisingevents,
furtherindividualmeetingswithcommunityleadersaccordingtoneedsofindividuals)
o Giveoutlineofhowyouwantthecommunityleaderstobeinvolved(helparrange
communityawareness-raisingevents;generalsupporte.g.encouragingindividualto
keepusingmedication;encourageinclusioninEdirtasksforthepersonwith
schizophrenia;encouraginginclusioninkebelemeetings;makingsurepeoplearenot
excludedfromchurch)
o Giveoutlineofhowyouwantgeneralcommunitymemberstobeinvolved(general
support;encouragegeneralsocialinclusion)
o Askwhatisthebestplaceforacommunityawareness-raisingevent
o Askaboutcommunityresources(SeeTask3)
o Gatherinformationonpotentialpaidemploymentinthekebelee.g.farmlabouring(see
Task7)
o Arrangeasubsequentmeetingifthecommunityleader/swouldlikemoretimeto
discuss
Task6:Communityawareness-raisingevent/s
How?
• Youshouldholdtheeventatacommunitymeetingthatisalreadyplanned.Utilisetheplace
suggestedbythecommunityleaderse.g.kebeleorEdirmeeting
• Pre-arrangethedate,starttimeandtheamountoftimeyouhavetospeak.Themeeting
maytake30minutesto2hoursdependingonwhereitisheldandthetopicsyoucover

161
• Youmaywishtoarrange2or3meetingstogiveyoutimetocoverallthetopics.Thisisa
suggestionforhowtodivideupthetopics.
• Meeting1topics
o Introduceyourselfandexplainthatyouareworkinginthekebeletotryandsupport
peoplewithschizophrenia
o Describehowschizophreniaisaminddiseasethatcanimprovewithmedication
o Peopledevelopschizophreniaduetostressfuleventsthathappeninlife.
• Meeting2topics
o Explainthatwithtimeandsupportpeoplewithschizophreniacangetbacktousual
activities,suchasworkandsocialising
o Peoplewithschizophreniacangetmedicationatthehealthcentre.Thiswillmake
thembetter.
• Meeting3topics
o Togetbetterpeoplewithschizophrenianeedthesupportofpeopleinthecommunity
o Itisimportantnottotreatpeoplewithschizophreniadifferently,forexamplewith
disrespect,callingthemnames,orignoringthemjustbecausetheyhavethisillness.
o Thiskindofbehaviourwillstopthemfromgettingbacktotheirusualactivities
o Itisalsoimportantnottobeatpeoplewithschizophrenia.Thiswillnothelpthemget
better.
o Gettingmedicationwillreducetheneedforindividualstobechained.Weshouldavoid
chainingifpossible,andinsteadhelppeoplewithschizophreniagettreatment.
• Explaintheinformationsimplyandclearly
• Listencarefullytotheresponsesfromthoseattending.Berespectfulofanydifferencesin
beliefsordifferingopinions.
• Thankattendeesfortheirtime.
Task7:Identifypotentialemploymentopportunitiesinthekebele
How?
• Identifypotentialpaidemploymentopportunitiese.g.farmlabouringbyconsulting:
communityleaders,thepersonwithschizophreniaandHEWs.Thismaybeonaone-offor
ongoingbasis.
• Arrangeameetingwiththepotentialemployer

162
• Discusspotentialbenefitsfortheemployer,community,individualandcaregiverofoffering
paidemployment
• Addressanyconcernsthepotentialemployerhas
PhasesIIandIII
InPhasesIIandIIIyoumayormaynotneedtoconductthefollowingactivitiesdependingon:
• Needsofindividualandcaregivers.ItisindicatedinthemoduleswhenaCommunity
Engagementtaskislikelytobeuseful.
• Availablecommunityresources,whichyouidentifiedinTask3.
• Whatthepersonortheirfamilyiswillingorabletodothemselves(thereforenotrequiring
yourinput).
• Whotheindividualandfamilyarehappyforyoutotalktointhecommunity
• Youshouldalwaysdiscusswithyoursupervisorwhichonestoundertake.
Task8:IndividualmeetingswithKebeleleaders
Inwhatcircumstances?
• IftheindividualisnotreceivingfreemedicationbutmaybeeligibleAND/OR
• Iftheindividualand/orcaregiverisnotengagedinkebeleactivitiesbutwouldliketobe,and
familyhavebeenunsuccessfulingettinginvolvedwithoutyourhelp
How?
• ArrangemeetingwithKebeleleader
• DiscussthepossibilityoflettersupportingfreemedicationAND/OR
• Discussthefactthattheindividualorcaregiverfindsitdifficulttoparticipateinkebele
activities
• Discussthebenefitsofthemparticipatinge.g.contributetodevelopmentofkebele
• Discusshowtofacilitatetheirincreasedparticipation
Task9:IndividualmeetingswithEdirleaders
Inwhatcircumstances?
• IftheindividualorcaregiverisnotengagedinEdiractivitiesbutwouldliketobe,andfamily
havebeenunsuccessfulingettinginvolvedwithoutyourhelpAND/OR

163
• Thehealthextensionworkerorcommunity leaderssuggest that theEdirgroupcouldgive
financialorpracticalsupporttotheindividualandfamily
How?
• ArrangemeetingwithEdirleader
• DiscussthefactthattheindividualorcaregiverfindsitdifficulttoparticipateinEdir
activities
• Discussthebenefitsofthemparticipatinge.gcontributetoEdirwork,reduceworkof
others.
• DiscusshowtohelpthemparticipatemoreAND/OR
• Discuss that in a crisis situation the individualmay come to Edir for financial or practical
support
Task10:Individualmeetingswithreligiousleader
Inwhatcircumstances?
• Theindividual,caregiverorHEWidentifiesreligiousleaderasimportantsourceofsupport
AND/OR
• Theindividualhashaddifficultiesattendingchurchorreligiousgroups,andfamilyhavebeen
unsuccessfulingettinginvolvedwithoutyourhelpAND/OR
• Theindividual,caregiverorHEWidentifiespriestascurrentlygivingincorrectorconflicting
messagesabouttreatment,includingmedication
How?
• Arrangemeetingwithreligiousleader
• Discusshowthereligiousleadercansupporttheindividualandcaregivere.g.reinforce
importanceofaccessingcare,notchainingunlessabsolutelynecessaryAND/OR
• Giveinformationabouttheimportanceoftakingmedicationforrecovery.Berespectfuland
donotdisagreewiththeirbeliefsAND/OR
• Discussthefactthattheindividualorcaregiverfindsitdifficulttoparticipatein
church/mosque/religiousgroups
• Discussthebenefitsofthemparticipating
• Discussnextstepsforinvolvingthem,ifpossiblee.g.priestiswelcomingtoindividual;priest
makesadaptationsorspecialarrangementstoencourageindividualtoattend.

164
Task11Individualmeetingswithtraditionalhealer/holywaterattendant
Inwhatcircumstances?
The individual, caregiver or HEW identifies traditional healer or holy water attendant as
importantsourceofreinforcementorcurrentlygivesincorrectmessagesabouttreatment
How?
• Arrangemeetingwithtraditionalhealerorholywaterpriestorattendant
• Discusshowthetraditionalhealerorholywaterattendantcansupporttheindividualand
caregivere.g.reinforceimportanceoftakingmedicationwhilstatholywater
• Berespectfulanddonotdisagreewiththeirbeliefs
Task12Individualmeetingswithliteracygroupleaderorheadteacher
Inwhatcircumstances?
If the individualorcaregiver isnotengaged in literacygrouporschool(and isschoolage)but
wouldliketobe,andfamilyhavebeenunsuccessfulinarrangingthiswithoutyourhelp.
How?
• Arrangemeetingwithliteracygroupleader
• Discussthefactthattheindividualorcaregiverwouldliketoparticipateintheliteracygroup
• Discussthebenefitsofthemparticipating
• Discussnextstepsforinvolvingthem,ifpossible
Task13Demonstrateprogressofindividualstocommunityleaders/widercommunity
Inwhatcircumstances?
• Personwithschizophreniawhoisrecoveredandhasgoodfunctioningisavailableandwilling
tospeaktogeneralcommunityAND
• ThereisasuitableplaceinacommunitysettingwherethisindividualcanspeakAND
• You and your supervisor assess that the community has a good level of awareness and
speakingtocommunitymembersisunlikelytobringadditionalstigmaanddiscriminationto
theindividual.
How?
• Workwithsupervisortoidentifypersonwithschizophreniawhoissuitableforthistask,
eitherthroughRISEortheButajirastudy
• Discussexpectationswiththeindividuale.g.anyfearsaboutstigma

165
• Takeconsentfromtheindividual
• Arrangewithcommunityleaderforindividualtospeakatpublicmeetinge.g.FamilySupport
Groupmeeting,kebelemeeting,Edirmeeting.
• Ensuretheindividualreceivescompensationfortheirtime,transportetc.Discusswithyour
supervisor
Task14Communityawarenessraisingconsolidation
Inwhatcircumstances?
Communityleadersarewillingtoreceivefurthercommunityawarenessraisingactivities
How?
RepeatTask6inthesameordifferentcommunitymeetings
Task15Facilitateemploymentopportunitiesinthekebele
• Arrangejointmeetingwiththeindividual,caregiverandemployerpreviouslyidentifiedas
abletoofferemployment
• Iftheemploymentgoesahead,keepinregularcontactwiththeemployertodiscuss
progressandconcerns.
31.3 Howdowedealwithdifficultsituations?
Whenmeetingwithcommunityandreligious leadersyoumayfindtheyhavedifferentbeliefs
aboutschizophrenia,forexamplethatit iscausedbyspiritpossessionorevileye,orthatholy
waterwillnotworkiftheindividualtakesmedication.Youshouldnottellthemtheirbeliefsare
wrong. You may find it useful to say there may be many different reasons why someone
becomesunwellwithschizophrenia,andoftenwedon’tknowthecause.Alsorememberthat
you are not suggesting that people should stop going to holy water, unless they are being
harmedthere.Youshouldbeworkingtowardstheindividualusingmedicationandholywaterat
thesametime.
Occasionally,community leadersmaynotbe interestedtomeetwithyou. If thishappensyou
shouldworkonbuildingyourrelationshipgradually,insteadofinsistingthattheyworkwithyou.
You could try asking others for help building the relationship, such as the HEW, or another
community leader who is more interested in CBR. If you are having lots of problems with
community engagementwork you should discuss this with your supervisor andmake a plan
togetherforhowtoimprovethesituation.

166
31.4 Howdowedocumentthecommunityengagementwork?
ForeachkebeleyouareworkinginyouwillhaveaseparateKebeleLogbook(seeForm10).In
theLogbookyouwillrecordinformationallthecommunityengagementworkyouundertake.
31.5 Howdowemonitortheprogressofthecommunityengagementwork?
You will discuss at the community engagement work in each kebele at your Face-to-Face
Discussionswithyoursupervisor,andalsoattheGroupSupervisionsessions.
31.6 Summary
• Itisimportanttodocommunityengagementworktotrytoincreasethepositiveinfluences
ofthecommunityontheindividual,andtoreducethenegativeinfluences.
• InPhaseIyoushould:meetwiththehealthextensionworker,identifyimportantcommunity
leaders and resources, find out what mental health awareness raising has already taken
place,meetwiththecommunityleaders,doacommunityawareness-raisingevent,andfind
outaboutpotentialemploymentopportunities.
• InPhases IIand IIIyoumayormaynotneedtodothe followingsteps,dependingonthe
needs of the individual: individualmeetingswith the kebele leader, religious leader, Edir
leader, Traditional healer andholywaterpriestor literacy group leader; demonstrate the
progressofindividualstothecommunity;andfacilitateemploymentopportunities
• YoushoulddocumentthecommunityengagementworkintheKebeleLogbook
• Your supervisor will monitor the progress of community engagement work at your
supervisionmeetings

167
32 Familysupportgroups
32.1 Whatarefamilysupportgroups?
Family support groupsarewhere the caregiversofpeoplewith schizophreniawho live in the
samekebelemeetregularly.Sometimespeoplewithschizophreniathemselvesarealsopartof
the groups. The aim is to share experiences and information and provide one another with
support.Thetypeofsupportisusuallyemotionalsupport,butcansometimesbepractical.
32.2 Whyarefamilysupportgroupsimportant?
Caregiversofpeoplewithschizophreniaareoftenisolatedfromotherpeopleinthecommunity.
Theymay feel alone with their problems and that no one understands what they are going
through. Many caregivers, and sometimes also people with schizophrenia, find it useful to
discusstheirexperienceswithotherpeopleinthesamesituation.Thiscan:
• Beempoweringas ithelps caregiversandpeoplewith schizophrenia feel theyareable to
helpthemselves
• Reducefeelingsofisolationbyseeingotherpeopleinthesameposition
• Helptoworkthroughproblems,suchasdifficultiesreturningtofarmwork,bysharingideas
• Reducestressbytalkingaboutproblems
• Helptogiveideasabouthowtodealwithstigmaanddiscrimination
• Improveconfidenceandself-esteem
• Improvesocialskillsbyhavingachancetomeetwithothersinasafesetting
FamilysupportgroupsmayalsocontinueafteryouhavestoppeddoingCBRinthekebele.This
mayhelpthepositiveeffectsofCBRtocontinueafteryouhaveleft.
32.3 Howtowesetupfamilysupportgroups?
Whocanparticipateinthefamilysupportgroups?
There should usually be one family support group in each kebele. The caregivers of all the
individualsyouareworkingwithandanyotherkeyfamilymembershouldbeinvitedtojoin.In
addition,youwillbeaskedtoinvitethecaregiversofanyotherpeoplewithschizophreniainthe
kebele,butwhoarenotparticipating inCBR.Your supervisorwill giveyou informationabout
theseindividuals.YouwillnotbeaskedtoprovideanyothercomponentsofCBR(forexample,
home visits) to these additional individuals. Family support groupsmay vary a lot in size. In
somekebelestheymaybeverysmall,forexample3members.Familymembersaremorelikely

168
tobenefit if thegroup isnot toobige.g.more than10people (althoughtyoucanbe flexible
dependingontheneedsofthefamilies).Insomekebelestheremaybeanetworkorgroupof
caregiversalready.Ifsoyoushouldtrytobuildonthisratherthanstartinganewgroup.
People with schizophrenia who are unwell or very disabled will usually find it difficult to
participateinthegroup.Howeversomeindividualsmayfinditusefultobeinvolved,especially
when they are getting better. Discuss with your supervisor, the family and the individual, if
possible,aboutwhethertheyshouldbe involved. If theyaretoounwellat thebeginning, this
shouldbereviewedastimegoeson.
Whendowestartthefamilysupportgroups?
Youwill invite caregivers toparticipate in the family support grouparound the time that the
familiesyouareworkingwitharemovingfromPhaseItoPhaseII.Thiswillusuallybeabout2
monthsafteryoustartworkinginthekebele,butthismayvary.Thereasonforstartingaround
PhaseIIisthatyouaremorelikelytohaveagoodrelationshipwiththefamilybythen,andyou
shouldhaveaddressedthemostimportantproblems.Howeveryoushouldinviteallfamiliesto
participate at the same time, even if some of them haven’t reached Phase II yet. Aswell as
inviting the families you are already working with, you should invite the other people with
schizophrenialivinginthekebeleataroundthistime.
Howdoweinvitefamiliestoparticipate?
Youcouldsaysomethingsimilartothistoinviteindividualsandfamiliestojoin:
‘‘Weareplanningtostarta familysupportgroupin yourkebelewhichwillallowyoutomeet
withpeoplehavingsimilar problemsasyouareexperiencing.Thiswillgiveyouopportunityto
expressyourdifficulties,gainsupportbysharing personal experiences and will help to learn
different waysoftacklingyourproblems.Wewillnotbeabletoprovideanyloans,butwestill
hopethegroupwillbehelpful.Willyoube interestedtobeapartof the group?’’
32.4 Howdoweorganisethefamilysupportgroups?
Wherewillthefamilysupportgroupsbeheld?
Thefamilysupportgroupshouldtakeplacewithinthekebele,usuallyinthehealthpost.They
couldalsotakeplaceinoneofthefamilies’homes,ifthisissuggestedbymembersofthegroup.
Thelocationshouldbeeasilyaccessibleonfootforallthemembers.

169
Howoftenwillthefamilysupportgroupsmeet?
Howoftenthegroupmeetsshouldbedecidedtogetherwiththegroupmembersatoneofthe
first meetings. It should usually be about every month. Once decided, the group members
shouldagreetotryandattendallthemeetings.
Whenwillthemeetingsbeheld?
Whenthegroupmeetsshouldbedecidedtogetherwiththegroup.Itisusuallyhelpfultomeet
atthesametimeeachmonth,forexampleatearlyonthe1stSaturdayeachmonth.
Howlongwillthefamilysupportgroupmeetingslast?
Themeetingsmightlast60to90minutes,butthisshouldbedecidedbythegroupmembers.
Willweprovidecoffeeorteaatthemeetings?
Youwillnotbegivenanymoney tobuycoffeeor tea for thegroup.However thegroupmay
decidetoeachcontributeasmallamounteachmonthtobuycoffeeortea.
HowdowerecordthedetailsoftheFamilySupportGroup?
YoushouldrecordthedetailsofeachfamilysupportgroupontheFamilySupportGroupDetails
Form(Form19).
32.5 Whatdowedointhefamilysupportgroupmeetings?
Wholeadsthemeetings?
Inthebeginningyoushouldberesponsibleforleadingthemeeting.Afterseveralmeetingshave
takenplaceyoushouldtrytoidentifyagroupleaderwhocantakeoverafteryouhaveleft.The
group should decide together who the leader will be. Different group members can be the
leaderatdifferenttime.
Whatisthestructureofthemeetings?
Whoeverisleadingthegroup-youoragroupmember-isresponsibleforkeepingthestructure
ofthemeetings.Meetingsshouldnormallyfollowthesesteps:
• Welcomeallmembers,andintroducenewmemberstotherestofthegroup
• Remindthegroupwhattopicyouwilldiscussatthismeeting
• Askinggroupmemberstosharetheirexperiences,concernsandideasonthetopic

170
• Attheendsummarisingthemainpointswhichwereraisedinthediscussion
• Agreewhichtopicyouwilldiscussatthenextmeetingandconfirmthetime,dateandplace
ofthemeeting
Verysmallgroupsmaybemoreinformalandnotnecessarilyfollowthesesteps.
Whatdowediscussinthemeetings?
The group members should decide what you discuss in the meetings, but you can give
suggestions. It is usually a good idea to keep to one or two topics at eachmeeting. Decide
togetherwhichtopicyouwilldiscussnextweek.Topicsmightinclude:
• Sharingproblemswithtakingmedicationandhowtoovercomethem.
• Sharingexperiencesofnegativecommentsorothertypesofdiscriminationfromcommunity
members,andhowtodealwiththesesituations
• Discussing how to improve participation in community life. Caregivers or people with
schizophreniafromdifferentfamiliesmayagreetogotogethertosocialevents
Whatshouldthebasicrulesofthemeetingsbe?
Atoneofthefirstmeetingsyoushouldagreeonthebasicrules,usingtheideasfromthegroup.
Theseshouldnormallyinclude:
• Everythingdiscussedinthegroupshouldbeconfidential
• Everyoneshouldlistentotheothergroupmembersandsharetheirownexperiences
• Nooneshouldmakejudgementsorcriticisetheothermembers
• Everyonemustrespecttheothermember’ssituation.Whatisrightforonepersondoesnot
havetoberightfortheothers.
Howdowedocumentthemeetings?
The group leader should recordwho attends andwhatwas discussed on the Family Support
GroupMeetingForm(Form20).
Whatshouldwedoifthegroupasksforaloanorequipment?
Thegroupmembersmayaskyouforfinancialhelp,foraloan,forstationaryorotherequipment
orfortraining.Ifthishappensyoushouldencouragethegrouptothinkofhowtheycanuse
theirownstrengths,skillsandresources.Explainthatunfortunatelyyouarenotabletoprovide
171
anyofthesethingstothemorindeedtoanyofthegroupsyouareworkingwith.Tellyour
supervisorifthegroupcontinuetoaskyouaboutthis,andconsiderdiscussingtogether.
32.6 Howdowemakesurethefamilysupportgroupscarryonafterwehaveleft?
Fromthebeginningofthesupportgroupmeetingsyoushouldbethinkingabouthowtomake
suretheycarryonafteryouhaveleftthekebele.Herearesomewaystodothis:
• Make sure the group discusses topics that are important to the members. If they are
benefittingfromthegroupitismorelikelytocontinue.
• Tellthegroupthatyouwillsupporttheminthebeginningbutthatyouhopetheywillrunit
bythemselveslateron,oncetheyareready.
• Findagroupleaderfromwithinthegroupafterthefirstfewsessions.
• Bepreparedforthegrouptotakealongtimetogetstartedandtorunbyitself.
32.7 Summary
• Family support groups are where caregivers of individuals, and sometimes people with
schizophreniathemselves,providesupporttooneanother
• Theyareempoweringfortheparticipants,andreducefeelingsofstressandisolation
• Thegroupsshouldhave5-10membersandshouldmeetaboutevery15days.
• Youshouldleadthegroupinitiallythenlateragroupmembershouldlead.Youshouldtryto
ensurethegroupcarriesonafteryouhaveleft
• Discussion topics can include: sharing problems, sharing experiences, improving
participationincommunitylife

172
SECTIONC:Knowhowyouwillbesupported
todeliverCBR
RISE

173
33 CBRworkerwellbeing
33.1 WhatproblemswithwellbeingmightCBRfieldworkershave?
Working with people with mental illness is often rewarding but you may sometimes find it
stressful.Stressisn’talwaysbad,butitcancauseproblems.Theseproblemsinclude:
• Worryingallthetime
• Sleepingbadly
• Beingirritable
• Drinkingtoomuchalcoholorchewingkhat
• Notwantingtobewithpeople
• Physicalhealthproblems(highbloodpressure,pepticulcerdisease)
• Conflictswithyourworkcolleaguesoversmallthings
• Problemswithrelationshipsathome
• Developingdepressionorananxietydisorder
33.2 WhymightCBRfieldworkershaveproblemswithwellbeing?
Herearesomeofthereasonswhyyoumighthaveproblemswithyourwellbeing:
• Youfeelyouhavetoomuchtodo
• Youareworriedaboutyourpersonalsafety.
• Youfeeltherearehighexpectationsfromothersortheindividualsaren’tmakingenough
progress
• Youhavetomakedifficultdecisions
• Youdon’thaveenoughsupport
• Workingwithpeoplewithmanyproblems,youmaytakeontheirworriesasyourown
33.3 WhyisitimportantforCBRworkerstolookafterthemselves?
Itisveryimportantforyoutolookafteryourself.Itwillbedifficulttohelpthepeopleyouare
workingwithifyouarenotlookingafteryourselfandfeelingwell.Youmightfeelthatadmitting
youfeelstressedorunhappyisasignofweaknessorlackofcommitmenttoyourwork.Thisis
nottrue.
33.4 Howcanyoumaintainyourwellbeing?
1.Reducingstress
174
Herearesomeideastomakesurestressdoesn’tcauseproblemsforyou:
• Don’tworkallthetime–inyourresttimes,meetupwithfamilyandfriends,dothings
youenjoyandtrytorelax
• Eatadequately
• Trytomaintainaroutine
• Discussworkproblemswithanotherperson,forexampleyourspouseorafriend
• Don’tbeafraidtoaskformoresupport.
• TrytherelaxationtechniquesinChapter23.
2.Discussyourwork
Youshouldhavelotsofopportunitytodiscusshowyourworkisgoing,andanyproblemsyou
arefacing(seeChapter34).Theseinclude:
• Meetingwithyoursupervisoronceeverytwoweeks
• MonthlygroupsupervisionwithotherCBRworkers
• Youcancallyoursupervisoratanytimeifyouarefacingdifficulties.
Rememberthatitmighttakealongtimetoseepositivechangesintheindividualsyouare
workingwith.Trytostaypositiveandthinkaboutthesmallchangeswhichhavehappenedsince
youstarted.
3.Seekhelp
TherearetwosituationswhereyoushouldlookforhelpSTRAIGHTAWAY:
• Suicidalfeelings.Ifyoufeelsohopelessthatyouarethinkingthatlifeisnotworthliving,or
even thinking about ending your life it is very important to discuss these feelings with
someoneyoutrust.
• Problemswithalcoholorkhat.Ifyouareconcernedthatyouhaveaproblemwithalcohol
orkhatoryourfriendsorrelativestellyoutheyareconcerned,youshouldtrytogethelp.
Togethelpyoucanalsotalktoyoursupervisororgotothehealthcentre.
4.Keepsafe
Thefollowingstepsaredesignedtoensureyoufeelsafewhilstatwork:
• Yoursupervisorshouldaccompanyyouonfirsttwohomevisitstoeachindividual
175
• Foreachindividual,yoursupervisorwillundertakeaCBRworkersafetyassessmentofthe
risktoyouandthesupervisor
• Youshouldalwayscarryamobilephone.Youwillbeprovidedwithcredit.
• Youshouldensurethatthereisafamilymemberpresentatallhomevisits.Thisshouldbe
emphasisedtothecaregiverduringyourfirstvisits.
• Ifthereisahighrisktoyoursafety,yoursupervisorwillaccompanyyouonthehomevisits
• Ifthereisamediumrisktoyoursafety,youshouldcallyoursupervisoratthebeginningand
theendofeachvisit
5.Knowhowtodealwithaviolentoraggressiveperson
• Beawareofthesignsthatsomeoneisgoingtobecomeviolent.Theseinclude:
o Talkinglouderorbecomingthreatening
o Fistsopeningandclosing
o Breathingfast
o Fidgeting
o Tapping,punchingorslappingtables,wallsorthefloor
• Beawareiftheindividualsmellsofalcohol,islosingtheirbalanceorhasslurredspeech.This
mightmeantheindividualisdrunkandismorelikelytobeviolent
• Thinkaboutyourownfeelings.Ifyoufeelscaredyoushouldstopthehomevisitandleave
thehouse.
• Makesurethatbothyouandtheindividualcanreachthedoorofthehouseeasily.
• Speakinaclearandcalmvoice.Donotshouttotryandcalmtheindividual.
• Lettheindividualknowthatyouwanttohelpthem.
• Don’ttellthemthattheycan’treallyhearvoicesorthattheirbeliefsarewrong.
• Donotthreatentheindividualorcorrecttheirswearing.Thiswillonlymakeitworse.
• Iftheindividualhasaweapon,reassurethemthatyouareheretohelpthemandthereisno
needforaweapon.Iftheyrefusetoputdownorhandovertheweapon,youshouldstop
thehomevisitandleavethehouse.
• Iftheindividualbecomesviolenttellhimtocalmdownbyfirmreassurance.Ifthisisnot
possibleyoushouldstopthehomevisitandleavethehouse.
• Aftertheincidentcallyoursupervisortotellthemwhathashappenedandagreetogether
anystepsyouneedtotakenow.
176
33.5 Summary
• WhilstworkingasaCBRworkeryoumaysometimesfeelstressedorunhappy
• Thismayhappenifyoufeelyoudonothaveenoughsupportoryouareworriedaboutyour
safetyorhaveotherproblemsinyourlifetodealwith
• Itisimportantforyoutostaywellsothatyoucanhelptheindividualsyouareworkingwith
properly
• Ways to stay well and happy include: reducing stress, discussing your work with others,
seekinghelp if youneed to, keeping safeandknowinghow todealwitha violentperson

177
34 Supervision
34.1 Whatissupervision?
Supervision is where somebody else supports you in your work and gives advice on how to
improvethewayyouareworking.
34.2 Whyissupervisionimportant?
Itisimportantthatyouaresupervisedforthefollowingreasons:
• Tomakesurethatalltherightstepsaretakenforeachindividual,forexamplethatreferrals
tothehealthcentrearemadeattherighttime.
• TomakesurealltheindividualsreceivingCBRaresupportedinasimilarway.Eventhough
eachindividualwillreceiveadifferentversionofCBR,dependingontheirneedsandgoals,
there are some things that should be the same for everybody. These include your
relationshipwiththeindividualandhowwellyoudocumenttheirprogress.
• Tomakesureallthekebeleshavesimilarcommunityengagement,forexamplecommunity
awarenessraising.
• Tomakesuregapsinyourknowledgeareidentified,sothatyoucanreceiveextratraining
andsupportifyouneedit.
• TomakesureyouaresafeandwellwhilstdeliveringCBR
34.3 Whoisinvolvedinsupervision
YouandtheotherCBRworkers
You and the other CBR workers will get lots of experience with working with people with
schizophreniawhilstdeliveringCBR.Youwillprobablyfinditusefultosharetheseexperiences
andhearabouthowothershaveovercomedifficulties.
Yoursupervisor
Your supervisorwill be yourmain sourceof supervision. Theyhaveexperience in supervising
CBRworkers.
Theinterventionco-ordinator
Theinterventionco-ordinatorwillsuperviseyourfieldsupervisor.Youwillnothaveverymuch
contactwiththeinterventionco-ordinator.
34.4 Howwillyoubesupervised?
Therearefourwaysinwhichyouwillbesupervised.
178
1. Facetofacediscussion
Who?Youandyoursupervisor
When?Every15daysatapre-arrangedmeeting
Where?Atthehealthcentreorahealthpost
What?• UsingthemostrecentHomeVisitForms(Form11)andthelogbooksyouwilldiscussthe
progressofeachindividualyouareworkingwith,including:
o Generalhealthandsymptoms
o Whethertheyaretakingmedication
o Whetheranyriskshavebeenidentified,particularlysuiciderisk
o Modulesyouareworkingonandmodulesyouhavecompleted
o Progressoncurrentgoals
o Anyproblemsordifficultiesachievingthegoals
o Practicalissues
o Safetyissues
• YouwillrecordanyactionsthatyoursupervisorsuggestsonthemostrecentHomeVisit
Form.Youwillneedtomakesureyouusethesesuggestionsinyournexthomevisit.Atthe
nextFacetoFaceDiscussionyoursupervisorwillcheckwhetheryouusedthesuggestions.
• Usingyourkebelelogbooksyouwilldiscusstheprogressofthecommunityengagement,
including:
o Communityengagementactivitiescarriedoutandplanned
o Anyproblemswithcommunityengagement
• Youwilldiscussyourtimetableforthenextfortnight.Bothyouandyoursupervisorwillthen
havearecordofwhichindividualsyouplantovisit,andwhatcommunityengagement
activitiesyouplantodo,oneachday.SeeForm13.
• Yoursupervisorwillidentifyanytrainingneedsthatyouhaveandupdateyourknowledgeor
skillsifneeded.YoushouldrecordthispartofyourdiscussionontheSupervisionRecord
Form(Form21).
• Youwillarrangeyournextsupervisionmeetingandanyjointhomevisitswhichareneeded
2. PhonecontactWho?Youandyoursupervisor
When?Wheneveryouneedadviceorsupport
179
Where?Bymobilephone
What?
• Youcancallyoursupervisoratanytimetodiscussproblemsorquestionswhichariseduring
yourwork
• Therearecertainsituationswhereyoushouldalwayscallyoursupervisor.Theseinclude:
o Individualisatriskofsuicide,chaining,neglect,physicaloremotionalabuseinsideor
outsidethehome,orsexualviolence(seeChapter14andChapter35)
o Youhavemadeanurgentreferralfortheindividualtoattendthehealthcentre(see
Chapter36)
• YouwillrecordanysuggestionsthatyoursupervisormakesonthemostrecentHomeVisit
Form,ifitrelatestoanindividual,orontheSupervisionRecordFormifitrelatestoyour
owntrainingneeds.Youwillneedtomakesureyouusethesesuggestionsinyournext
homevisit.
3. Unannouncedobservedhomevisits
Who?Youandyoursupervisor
When?Abouteverymonthtotwomonths,butyouwillnotknowthetimeordayinadvance
Where?Atanindividual’shome
What?
• Youwillcarryoutthehomevisitasnormal,butyoursupervisorwillalsocometothehome
andobserveyouworking.Theywillbelookingat:
o Howgoodyourrelationshipiswiththeindividualandfamily
o Howwellyoulistenandexplainthingstotheindividualandfamily
o Whetheryoudomodulesortaskswhichseemrightfortheindividualatthattime
o Howwellyouwritedownwhathappenedduringthehomevisit
• Afterthehomevisit,usuallyatthehealthpostorhealthcentre,thesupervisorwilltellyou
howwelltheythinkyouareworking.Theywillalwaysgiveyousomepositivefeedback,as
wellastellingyouaboutanyproblems.
• Youwilldiscusstogetherhowyoucanimprovethingsifthereareanyproblems.Your
supervisormaygiveyoumoretrainingifyouneedit.
• YouwillrecordanysuggestionsthatyoursupervisormakesonthecurrentHomeVisitForm
ifitrelatestotheindividual,oronaSupervisionRecordFormifitrelatestoyourown
180
trainingneeds.Youwillneedtomakesureyouusethesesuggestionsinyournexthome
visit.
4. Groupsupervision
Who?You,alltheotherCBRworkersandbothfieldsupervisors
When?Everymonth
Where?Atahealthcentre
What?
• Priortothemeetingyoushouldtrytothinkofoneortwospecificproblemsorissuesthat
youhavefacedthatyouwouldlikesomesupportwith.Thesemightberelatedto:
o Issueswithdeliveringthemodulese.g.thebestwaytogiveadviceaboutselfcare
o Issueswithworkingwithpeoplewithschizophreniae.g.Howtoreactwhenan
individualisunwellandhallucinating
o Issueswithcommunityengagementworke.g.howtoworkwithanobstructive
communityelder
o Practicalissuese.g.howtousepublictransporttogettoaparticularlocation
o Yourownwellbeinge.g.howtobalanceworkandhomelife
• Duringthesessionthesupervisorwillfacilitatethediscussion.Theywillaskoneofyouto
brieflypresentyourproblemorquestion.TheotherCBRWswillthenhaveachancetoask
youquestionstomakesureeveryoneunderstandswhatyourissueis.
• ThesupervisorwillthenaskforideasandadvicefromyouandtheotherCBRworkersfor
howtoovercometheproblem.ItmaybeusefulforotherCBRworkerstodescribehowthey
respondedtoasimilarsituation.
• YouwillrecordanysuggestionsthatthegroupmakesonaSupervisionRecordForm.You
willneedtomakesureyouusethesesuggestions,forexampleatyournexthomevisit.
• ThesupervisorwillthenaskthenextCBRworkertopresenttheirproblem.Ineachsession
aroundhalfoftheCBRworkerswillhavechancetopresenttheirissue.
• Thesupervisorswillalsoupdateyourknowledgeorskillsbasedonissuesthatcomeup
duringthegroupdiscussion,orwhichtheyhavenoticedfromfacetofacediscussionsor
observedhomevisits.
181
34.5 Summary
• It is importantthatyouaresupervisedtomakesurealltherightthingsarebeingdonefor
eachindividual;tomakesureyourskillsareuptodateandthatyouaresafe
• Every15daysyouwillhaveaFacetoFaceDiscussionwithyoursupervisortodiscusseach
individualandkebeleyouarelookingafter,yourtimetable,andanytrainingneeds
• Youcancall your supervisoratany time for support.Youshouldalsocall themwhenyou
identifycertainrisksorifyouhavemadeareferraltothehealthcentre
• Yoursupervisorwillmakeanunannouncedhomevisitaboutonceamonth
• Youwill have a Group Supervision session everymonth to discuss issueswith other CBR
workersandshareideas.
• You should record any supervision on themost recent HomeVisit Form or a Supervision
RecordForm
182
35 Dealingwithdifficultsituations
35.1 Whatdifficultsituationsmightyoucomeacross?
Asyou learnt inChapter14,peoplewithschizophreniaarevulnerable tomany typesof risks.
These include: suicide attempt or suicide risk, chaining, neglect, physical abuse outside the
home,physicaloremotionalabuseinsidethehomeandsexualviolence.
Otherdifficultsituationsyoumightcomeacrossinclude:
• Theindividualcommitssuicideordiesfromanothercause
• The individual is admitted tohospital due to a serious side effect from the anti-psychotic
medication,orduetoanyotherseriousmedicalemergency
• Theindividualisviolentoraggressivetowardsyouorothers
35.2 Whyisitimportanttoknowhowtodealwithdifficultsituations?
Itisimportantthatyouknowhowtodealwithdifficultsituationssothattheindividualcanget
thebestcareandsupportavailableassoonaspossible.Thiswill leadtoabetteroutcomefor
theindividual,familyandthecommunity.
35.3 Howshouldyoudealwithdifficultsituations?
In this section there is a summary of what you should do for each difficult situation. Your
prioritieswhendealingwithdifficult situationsarealways toensureyourownsafetyand the
safetyof the individual.Wheneveryou send the individual to thehealth centre,writeon the
Health Centre Referral Form (Form 14) the reason for the referral and ask the individual or
caregiver to show the form to the nurse or health officer. Keep a copy of the form for the
participant logbook. You shouldonly call thepolice if you stronglybelieve the individual is in
immediatedangerofbeingseriouslyhurtbysomeone.
Solidarrow:alwayscontinuetothenextstep
Dashedarrow:continuetothenextstepiftheredwritingistrueinthissituation
KEY

183
Figure1Attemptedsuicideflowchart
Youoryoursupervisorfindouttheindividualhasa3emptedsuicide
Addressreasonfornota,endinghealthcentre.Thismayincludeeduca7ngthefamilyand/orge9ngfinancialorprac7cal
communitysupport
Nurseorclinicalofficerwillcarryoutclinicalassessment
Immediatelyinformyoursupervisor,iftheyarenotaware
Arrangeajointhomevisitwithyoursupervisor.Iftheyhavenota,endedthehealthcentre,atthevisitsfindoutwhynot.
Iftheindividualdoesnota,endhealthcentrewithin1week
Checktheindividualistakingmedica7onandencouragefamilytotakeindividualtohealthcentreimmediately
Informthetrialco-ordinator
Immediatelyinformthetrialpsychiatricnurse,whowilldoahomevisit
Advisethefamilynottoleavetheindividualunaccompaniedandtoremoveanyitemswhichcouldbeusedforsuicidea,empt

184
Figure2Riskofsuicideflowchart
Youoryoursupervisoriden.fyindividualisatriskofsuicide
Addressreasonfornota,endinghealthcentre.Thismayinclude
educa7ngthefamilyand/orge9ngfinancialorprac7cal
communitysupport
Yoursupervisorwillarrangeareviewathomebytrialpsychiatric
nurse
Nurseorclinicalofficerwill
carryoutclinicalassessmentInformyoursupervisorassoonaspossible,iftheyarenotaware
Arrangeajointhomevisitwithyoursupervisor.Iftheyhavenot
a,endedthehealthcentre,atthevisitsfindoutwhynot.
Iftheindividualdoesnota,endhealthcentre
within1day
Checktheindividualistakingmedica7onandencouragethe
familytotakeindividualtohealthcentreimmediately
Ifthepsychiatricnurseassessestheindividualis
mediumorhighrisk
Yoursupervisorwilldoariskassessment
Yoursupervisorwilldiscusstheriskassessmentwiththe
psychiatricnurse
Advisethefamilynottoleavetheindividualunaccompaniedand
toremoveanyitemswhichcouldbeusedforsuicidea,empt
Iftheindividual
a,endshealth
centrebutthere
areon-going
suicidalthoughts

185
Figure3VIolentoraggressiveindividualflowchart
Theindividualisviolentoraggressive
Takestepstoensureyourownsafety:• Makesurethatbothyouandtheindividualcanreachthedoorofthehouse.• Iftheindividualhasaweapon,reassurethemthatyouareheretohelpthemandthereisnoneedforaweapon• Ifyoufeelscaredyoushouldstopthehomevisitandleavethehouse.
Informyoursupervisora=ertheincidentandagreetogetheranystepsyouneedtotakenow.Donotvisitthehomeun@lyouhavepermissionfromyoursupervisor
Checktheindividualistakingmedica@onandencouragethemtodoso
Encouragefamilytotakeindividualtohealthcentre
Takestepstocalmtheindividual:• Speakinaclearandcalmvoice.Donotshouttotryandcalmtheindividual.• Lettheindividualknowthatyouwanttohelpthem.• Don’ttellthemthattheycan’treallyhearvoicesorthattheirbeliefsarewrong.• Donotthreatentheindividualorcorrecttheirswearing.
Yoursupervisormayarrangeforreviewathomebytrialpsychiatricnurse
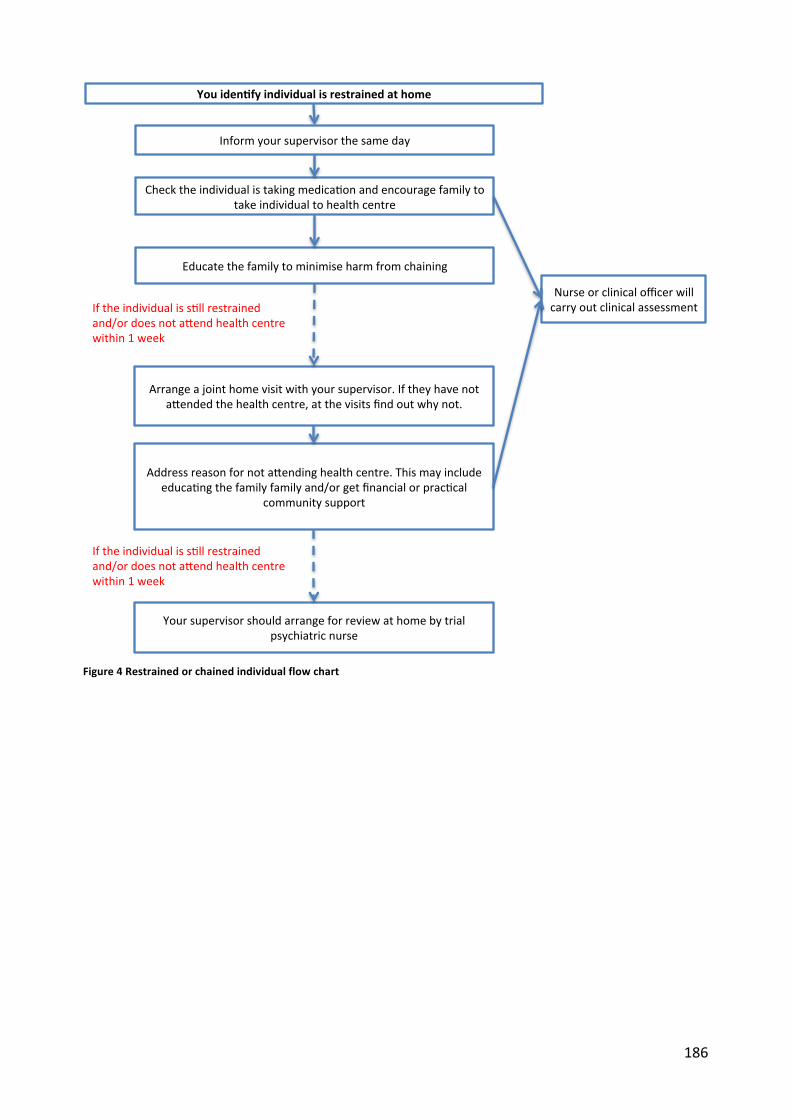
186
Figure4Restrainedorchainedindividualflowchart
Youiden)fyindividualisrestrainedathome
Addressreasonfornota,endinghealthcentre.Thismayincludeeduca7ngthefamilyfamilyand/orgetfinancialorprac7cal
communitysupport
Yoursupervisorshouldarrangeforreviewathomebytrialpsychiatricnurse
Nurseorclinicalofficerwillcarryoutclinicalassessment
Checktheindividualistakingmedica7onandencouragefamilytotakeindividualtohealthcentre
Arrangeajointhomevisitwithyoursupervisor.Iftheyhavenota,endedthehealthcentre,atthevisitsfindoutwhynot.
Iftheindividualiss7llrestrainedand/ordoesnota,endhealthcentrewithin1week
Educatethefamilytominimiseharmfromchaining
Informyoursupervisorthesameday
Iftheindividualiss7llrestrainedand/ordoesnota,endhealthcentrewithin1week

187
Figure5Physicalabuseoutsidethehomeflowchart
Youiden)fyindividualisvic)mofphysicalabuseoutsidethehome
Addressreasonfornota,endinghealthcentre.Thismayincludeeduca7ngthefamilyfamilyand/orgetfinancialorprac7cal
communitysupport
Yoursupervisorshouldarrangeforreviewathomebytrialpsychiatricnurse
Nurseorclinicalofficerwillcarryoutclinicalassessment
Checktheindividualistakingmedica7onandencouragefamilytotakeindividualtohealthcentreifunwell/notreviewedrecently
Arrangeajointhomevisitwithyoursupervisor.Iftheyhavenota,endedthehealthcentre,atthevisitsfindoutwhynot.
Iftheabusecon7nuesand/ortheindividualdoesnota,endhealthcentrewithin1week
Informyoursupervisorthesameday
Iftheabusecon7nuesand/ortheindividualdoesnota,endhealthcentrewithin1week
Ifthereisareligiousortradi7onalhealerinvolved,educatetradi7onalorreligioushealeraboutpoten7alharm

188
Figure6Physicaloremotionalabuseinsidethehomeflowchart
Youiden)fyindividualisvic)mofphysicaloremo)onalabuseinsidethehome
Addressreasonfornota,endinghealthcentre.Thismayincludeeduca7ngthefamilyfamilyand/orgetfinancialorprac7calcommunitysupport
Yoursupervisorshouldarrangeforreviewathomebytrialpsychiatricnurse
Nurseorclinicalofficerwillcarryoutclinicalassessment
Checktheindividualistakingmedica7onandencouragefamilytotakeindividualtohealthcentreifunwell/notreviewedrecently
Arrangeajointhomevisitwithyoursupervisor.Iftheyhavenota,endedthehealthcentre,atthevisitsfindoutwhynot.
Informyoursupervisorthesameday
Speakwithapersontrustedbytheindividual,orneighbours,orlocalcommunityleadertofindasolu7on
Provideindividualwithdetailsofrelevantorganisa7onsandwhattheycandotohelp
WorkthroughModule:Improvingthefamilyenvironment
Domes7cviolencepersistsandindividualwantshelpORdoesnothavecapacity
Domes7cviolencepersistsandindividualwantshelpORdoesnothavecapacity
Discussstrategiesforindividualtofollowifabusehappensagaine.g.seekingrefugeatneighbourshouse
IfDomes7cviolencepersistsand/ortheindividualhasnota,endedthehealthcentrewithin1week
Callthepolice
Iftheindividualisatimmediateriskofseriousharm

189
Figure7Sexualviolenceflowchart
Youiden)fytheindividualisavic)mofsexualviolence
Nurseorclinicalofficerwill
carryoutclinicalassessment
and,ifappropriateoffer:
• emergencyfamilyplanning
• treatmentforsexually
transmi:eddiseases
• aHIVtest
Encouragefamilytotakeindividualtohealthcentre
Informyoursupervisorthesameday
Helptheindividualdecidewhethertocallthepolice
ProvideindividualwithdetailsofrelevantorganisaConsandwhatthey
candotohelp
Reassuretheindividualitisnotherfault
Encouragetheindividualtoshareherexperiencewithafamilymemberor
friend
Increasethefrequencyofhomevisits
Supporttheindividualtoinformthepoliceifthisisherdecision
Iftheindividualdoesnot
wishtoinformthepoliceor
familyyoursupervisor
shouldarrangeforreviewat
homebytrialpsychiatric
nurse.Trialpsychiatricnurse
decideswhetherthe
individualiswellenoughto
maketheirowndecisions.If
theyarenotwellenough
thenyoursupervisormay
decidetotellthefamilyor
police.
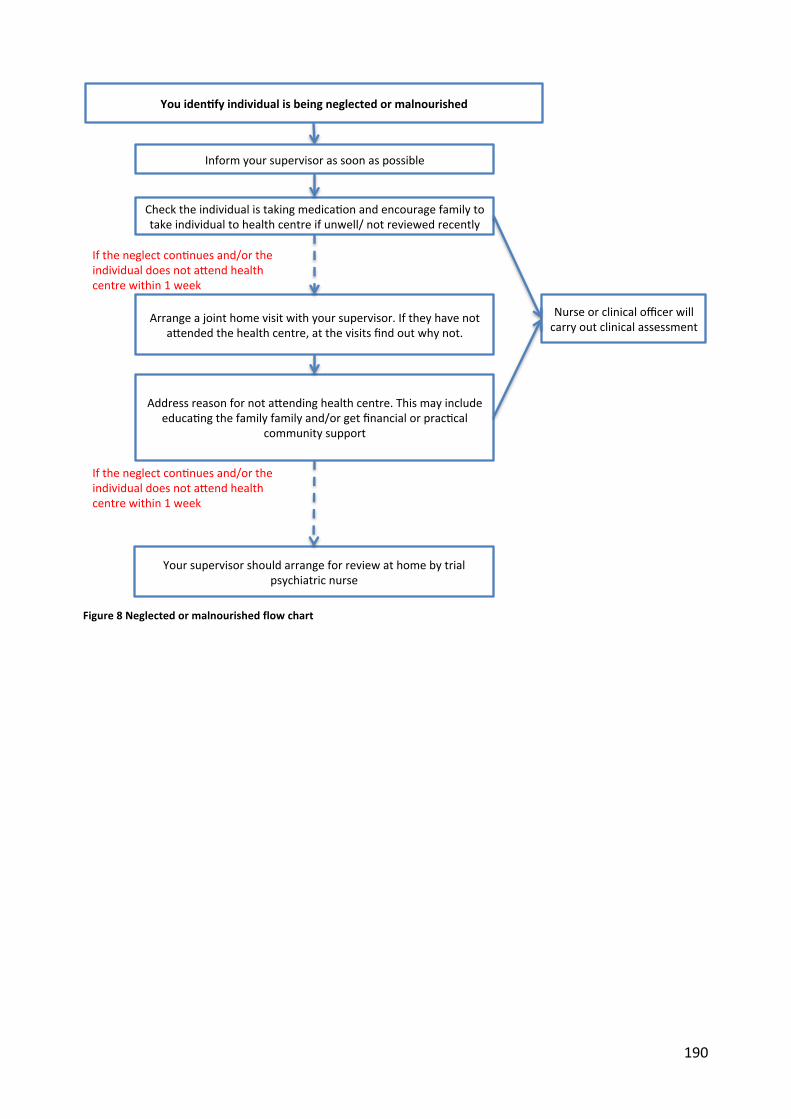
190
Figure8Neglectedormalnourishedflowchart
Youiden)fyindividualisbeingneglectedormalnourished
Addressreasonfornota,endinghealthcentre.Thismayincludeeduca7ngthefamilyfamilyand/orgetfinancialorprac7cal
communitysupport
Yoursupervisorshouldarrangeforreviewathomebytrialpsychiatricnurse
Nurseorclinicalofficerwillcarryoutclinicalassessment
Checktheindividualistakingmedica7onandencouragefamilytotakeindividualtohealthcentreifunwell/notreviewedrecently
Arrangeajointhomevisitwithyoursupervisor.Iftheyhavenota,endedthehealthcentre,atthevisitsfindoutwhynot.
Iftheneglectcon7nuesand/ortheindividualdoesnota,endhealthcentrewithin1week
Informyoursupervisorassoonaspossible
Iftheneglectcon7nuesand/ortheindividualdoesnota,endhealthcentrewithin1week
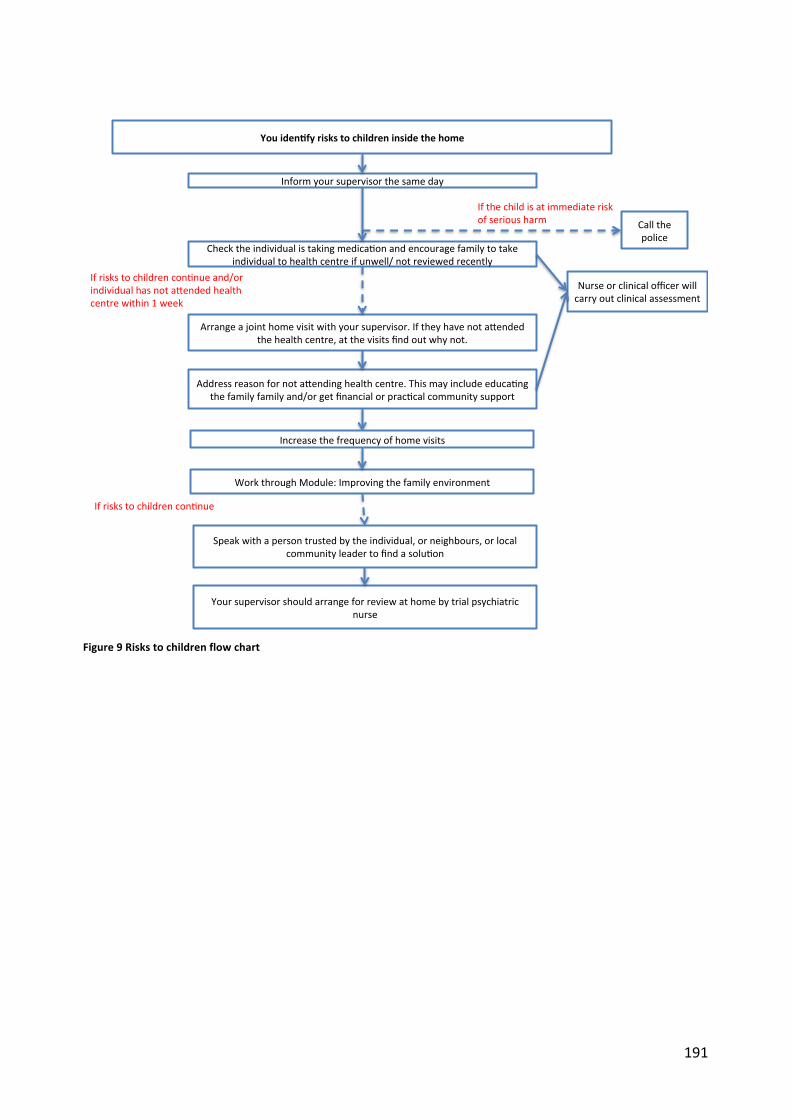
191
Figure9Riskstochildrenflowchart
Youiden)fyriskstochildreninsidethehome
Addressreasonfornota,endinghealthcentre.Thismayincludeeduca7ngthefamilyfamilyand/orgetfinancialorprac7calcommunitysupport
Yoursupervisorshouldarrangeforreviewathomebytrialpsychiatricnurse
Nurseorclinicalofficerwillcarryoutclinicalassessment
Checktheindividualistakingmedica7onandencouragefamilytotakeindividualtohealthcentreifunwell/notreviewedrecently
Arrangeajointhomevisitwithyoursupervisor.Iftheyhavenota,endedthehealthcentre,atthevisitsfindoutwhynot.
Informyoursupervisorthesameday
Speakwithapersontrustedbytheindividual,orneighbours,orlocalcommunityleadertofindasolu7on
WorkthroughModule:Improvingthefamilyenvironment
Ifriskstochildrencon7nue
Increasethefrequencyofhomevisits
Ifriskstochildrencon7nueand/orindividualhasnota,endedhealthcentrewithin1week
Callthepolice
Ifthechildisatimmediateriskofseriousharm

192
Figure10Hospitalisationflowchart
Figure11Suicideordeathfromothercauseflowchart
Youoryoursupervisorfindouttheindividualhasbeenadmi5edtohospitalduetoasideeffectofan9-psycho9cmedica9onoranotherseriousmedicalemergency
Informyoursupervisorassoonaspossible,iftheyarenotaware
Youencouragetheindividualtoa:endthehealthcentre
Informthetrialco-ordinator
Youandyoursupervisordoajointreviewathomea=ertheindividualisdischarged
Nurseorclinicalofficerwillcarryoutclinicalassessment
Youoryoursupervisorfindouttheindividualhascommi5edsuicideordiedofanothercause
Informyoursupervisorassoonaspossible,iftheyarenotaware
Ifassessedtobeappropriatebysupervisor,CBRWandsupervisormakehomevisittofamily.Assessongoingneeds.
Informthetrialco-ordinator
Informthehealthcentre

193
Figure12Individualisunwellorgettingworse
Youiden)fyindividualisunwellorge3ngworse
Addressreasonfornota,endinghealthcentre.Thismayincludeeduca7ngthefamilyfamilyand/orgetfinancialorprac7cal
communitysupport
Yoursupervisorshouldarrangeforreviewathomebytrialpsychiatricnurse
Nurseorclinicalofficerwillcarryoutclinicalassessment
Checktheindividualistakingmedica7onandencouragefamilytotakeindividualtohealthcentre
Arrangeajointhomevisitwithyoursupervisor.Iftheyhavenota,endedthehealthcentre,atthevisitsfindoutwhynot.
Iftheindividualiss7llunwelland/ordoesnota,endhealthcentrewithin1week
Informyoursupervisorthesameday
Iftheindividualiss7llunwelland/ordoesnota,endhealthcentrewithin1week

194
35.4 Summary
• It is important you knowhow todealwithdifficult situations tomake sure the individual
getsthebestcarepossible
• Thereisasetofactionsyoushouldtakeforeachdifficultsituation
195
36 Linkstohealthservices
36.1 Whatarelinkstohealthservices?
Linkstohealthservicesareanycommunicationthatyouhavewith:
• Thehealthcentre
• Thehealthextensionworkers
36.2 Whyisitimportanttohavelinkstohealthservices?
All the individuals youareworkingwithhaveaccess tomedical care for schizophrenia at the
health centre. It is part of your role to ensure that the individual attends the health centre
regularly,asthiswillhelpthemtorecover(seeChapter17).Therearesomesituationsthatare
too complicated for you todealwith, forwhich you should send the individual to thehealth
centre.Thereareothertypesofwork,forexamplegivingadviceaboutfamilyplanning,which
youhavenotbeentrainedfor,soyoushouldinvolvethehealthextensionworker.Keepinglinks
withhealthserviceswillensuretheindividualcangetthebestpossiblecare.
36.3 Howdoyoukeeplinkstohealthservices?
Introduceyourselfatthehealthcentre
AtthebeginningoftheCBRprogrammeyouandyoursupervisorwillintroduceyourselftothe
healthcentreheadandthenursesandclinicalofficers.TheywillalreadybeawareoftheCBR
programmebutyoucanremindthemofyourrole.
Regularappointmentsatthehealthcentre
Eachindividualshouldgotothehealthcentreevery1to3months.Youshouldbeawareofall
the appointments they have, and check if they have attended. If they have missed an
appointment,evenifyouarenotdueforahomevisit,youshouldmakeahomevisittocheck
foranyproblemsandremindthemtoattend.
Specialsituations
Youshouldsendtheindividualtothehealthcentreinanyofthefollowingsituations:
• Youthinktheindividualisatriskofcommittingsuicide(SeeChapter14and35)
• Youareworriedthattheindividualisnoteatingordrinking(SeeChapter35)
196
• Youareworriedthatchildrenmaybeatriskofharmfromtheindividual(SeeChapter35)
• Theindividualhasharmedsomeoneelseoryouareworriedthisisgoingtohappen
• Theindividualhasarelapsei.e.isveryunwellwithsymptomsofschizophrenia(Chapter30)
• Theindividualbecomepregnant.Youshouldalsoinformthepsychiatricnurse.
• Theindividualhasanewphysicalhealthproblemorphysicalinjury(Chapter21)
• Theindividualhasaseriousproblemwithalcoholorkhat(Chapter21)
• Theindividualhasseriousside-effectsoftheanti-psychoticmedication(seeChapter20for
descriptionofsideeffects).
• You would like the nurse to review the medication schedule or consider the injection
(Chapter20)
Youshouldtellyoursupervisorifanyofthesesituationshappen.Advisethefamilytotakethe
individualtothehealthcentreassoonaspossibleandgivethemsupportinmakingthejourney.
Thismayincludefindingothercommunitymemberswhocanhelpthefamily(seeChapter31).
Recordonthehomevisitformthatyouhavereferredtothehealthcentre.WriteontheHealth
CentreReferralForm(Form14)thereasonforthereferralandasktheindividualorcaregiverto
show the form to the nurse or health officer. Keep a copy of the form for the participant
logbook.Youcangoto thehealthcentrewith the individual. Ifyouaccompanythe individual
youshouldcompleteaHealthCentreContactForm(seeForm2).Oncetheyhavereturnedfrom
thehealthcentreyoushouldcontinuetodeliverCBRasnormal.Ifyoufindthatthecaregiveris
verydistressedyoucansuggesttheygotothehealthcentre(seeChapter15).
HealthExtensionProgramme
Thehealthextensionworkersshouldbecontinuingtoprovidetheirusualcaretotheindividuals
youareworkingwith.Youshouldaskthehealthextensionworkertovisittheindividualifthey
needsupportwithcontraception, sanitationadvice,ormalariaprevention,and theyhavenot
received a home visit. Health extension workers are not expected to assist with CBR, for
examplehelpwithself-care.
36.4 Summary
• It is importanttohave linkswiththehealthcentreandhealthextensionworkertoensure
theindividualhasthebestcarepossible.
• You should send the individual to thehealth centrewhen: they are at risk of committing
suicide, they are not eating or drinking, they have harmed someone else, they are very

197
unwellwithschizophrenia,theyarepregnant,theyhaveaphysicalhealthproblemorthey
haveserioussideeffectsofanti-psychoticmedication.
• YoushouldasktheHEWtovisitiftheyhavenotdeliveredtheirusualcaretotheindividual
• Ifanindividualmissesaroutineappointmentatthehealthcentreyoushouldremindthem
toattend
198
37 Gooddocumentation
37.1 Whatisgooddocumentation?
Gooddocumentationmeansthatyouwritethingsdown,forexampleaboutahomevisit, ina
waythat:
• Youareabletolookbackandrememberwhathappened.
• Otherpeople,forexampleyoursupervisor,canunderstandwhathappenedwithouthaving
toaskyou
• The individual and family can read what you have written and they think it is a good
descriptionofwhathappenedduringthevisit
37.2 Whyisitimportanttohavegooddocumentation?
WhenyouaredoingCBRwithmanyfamiliesatthesametimeitmaybedifficulttoremember
thedetailsofwhathappenedevery timeyou seea family.Bykeepingagood recordofeach
individual’sprogress,youwillbemuchbetterathelpingthemeachtimeyouseethem. Itwill
alsobeeasierforyoursupervisortocheckthatyouarelookingafterindividualsintherightway,
andgiveyouadviceonhowtoimprovethewaythatyouareworking.Theindividualandfamily
youareworkingwithmayasktoseewhatyouhavewritten.Itisfineforyoutoshowthem.
37.3 Whatdoweneedtodocument?
Foreach individualyouare lookingafteryouwillkeepan individual logbook.Thiswill include
thefollowingforms:
• Initialcontactform(Form1)
• HealthCentreContactForm(Form2)
• CBRReviewForm(Form3)
• NeedsAssessmentForm(Form4)
• GoalssettingForms(Forms5and6)
• RiskassessmentForm(Form7)
• Rehabilitationplan(Form8)
• ContinuingCareForm(Form9)
• Homevisitformsforeachvisit(Form11)
• VisitSummaryForms(Form12)
• HealthCentreReferralForm(Form14)
199
• Medicationchecklist(Form15)
• DaytoDayfunctioningProgressForm(Form16)
• EarlyWarningsignschecklist(Form17)
• RelapseManagementPlan(Form18)
• SupervisionRecordForms(Form21)
Foreachkebele youareworking in youwill keepa kebele logbook (Form I). Youhave learnt
aboutwhatinformationtorecordintheselogbooksinothersectionsofthemanual.
37.4 Howdowemakesurewehavegooddocumentation?
Thesearethethingsyoucandotomakesureyouhavegooddocumentation:
• Writeinaclearandlegibleway
• WriteinAmharic
• Writedownenoughdetailsothatyouandsomeoneelsewillbeabletounderstanditlater
• Make sure youwould be happy for the individual and family to readwhatever youwrite
down.
• Useapeninsteadofapencil
• Keep all your logbookswith you at all timeswhen you areworking in the field. At other
timeskeeptheminasafeplace.
• Keepyourlogbooksdryandclean
• Yoursupervisorwillcheckyourdocumentationeverysooftenandwillgiveadviceonhowto
improveitifnecessary
37.5 Summary
• Gooddocumentationiswhereyourecordthingsinawayitiseasytounderstandlater
• It is important to make sure you and your supervisor can easily follow the progress of
individuals
• Youwillkeepanlogbookforeachindividualandeachkebele
• You can ensure good documentation by:writing clearly, keeping logbooks dry and clean,
writinginpenandwritingenoughdetail

200
38 Howtodealwithotherpeoplewithproblems
38.1 Whatotherproblemsmightyoucomeacross?
DuringyourCBRworkyoumaycomeacrosspeople,apartfromtheindividualsyouareworking
with,whohaveproblems.Thesemightinclude:
• Peoplewith schizophreniawhohavebeenoffered care at thehealth centrebutwhoyou
havenotbeenasked to lookafter.Theymight live inakebelewhereyouareworking,or
anotherkebelewhereyouarenotworking.
• Peoplewhoyouthinkmayhaveschizophreniabutwhoarenotreceivingcareatthehealth
centre
• Peoplewithothersortsofmentalhealthproblems,forexamplealcoholproblemsinadults,
ordevelopmentaldelayinchildren
• Peoplewith other sorts of disabilities, for example blindness or problemswalking due to
polio
• Community members or community leaders may ask you to do community engagement
workinanotherkebele
38.2 Whymightyoucomeacrossotherpeoplewithproblems?
Inmost kebeles therewill bepeoplewith schizophreniawhoare receiving careat thehealth
centrebutwhoyouhavenotbeenaskedtolookafter.Thereasonsforthiswillbe:
• TheyaregenerallymorewellorlessdisabledsodonotneedtheextrasupportofCBR
• TheywereofferedCBRbuttheydidnotwanttoparticipate
• ThereisanotherreasonwhytheycouldnotreceiveCBR,forexampletherewasnocaregiver
abletoparticipate,ortheyhaveplanstoleavethekebelesoon.
You may be asked by the individual, family or community members to offer CBR or extra
support to these individuals. Itmay be difficult for people to understandwhy you are giving
extrasupporttosomepeoplewithschizophreniabutnotothers.
You will become good at recognising schizophrenia, and you may notice the symptoms in
peoplewhohavenotbeendiagnosedbyanurseatthehealthcentre.Orcommunitymembers
mighttellyouaboutindividualswhoarechainedupbecausetheyareunwell.
When you areworkingwithin the kebele youmight also notice other sorts of problems, for
examplephysicaldisabilities,justbyobservingthepeopleyoumeet.Thefamilyyouareworking
withmight tell youaboutproblemswithother familymembers. Community leadersorother
201
communitymembersmayseeyouasasourceofsupportandmaytellyouaboutproblemsthat
otherpeoplehave,evenifyoudon’taskthemto.
Communitymembers or community leaders from kebeles which have not been allocated to
receiveCBRmayaskyou todocommunityengagementwork in their kebele.Theymayhave
seenorheardaboutyoudoingthisworkinthekebeleswhereyouareworking.
38.3 Whyisitimportanttoknowwhattodoifyoucomeacrossotherpeoplewithproblems?
InthisCBRprogrammeyourroleistosupportthepeoplewithschizophreniathatyouhavebeen
asked to look after. However, it is important that you knowwhat to do if you come across
peoplewithotherproblems.This is tomakesurethat thesepeoplegetanycareandsupport
thatisavailable.Itwillalsohelptheindividual,familyandcommunitytotrustyoumoreifyou
knowwhattodowhenyoucomeacrosspeoplewithotherproblems.
38.4 Whatshouldyoudoifyoucomeacrosspeoplewithotherproblems?
Whatyoushoulddowhenyoucomeacrossotherpeoplewithproblemsdependsonthetypeof
problem.But thegeneral rule is toask someoneelse tohelp, rather thanhelping theperson
yourself.
1. Peoplewithschizophreniawhohavebeenofferedcareatthehealthcentrebutwhomyou
havenotbeenaskedtolookafter
• Suggestthattheyvisitthehealthcentreiftheyhavenotbeenrecently
• Explainthatunfortunatelyyoucannotofferhomevisitstothemandthatthisisoutofyour
control.
• AsktheHealthExtensionWorkertosupportthe individual, forexampleencouragingthem
toattendthehealthcentre.
• Iftheindividual livesinkebelewhereyouareworking(i.e. inakebeleallocatedtoreceive
CBR),considerinvitingthemtotheFamilySupportGroup,ifthishasalreadystarted.
• Iftheindividuallivesinkebelewhereyouarenotworking(i.e.inakebelenotallocatedto
receiveCBR),itisimportantthatyoudonotinvitethemtotheFamilySupportGroup.
• Informyoursupervisorofyourdiscussions
2. Peoplewhoyouthinkmayhaveschizophreniabutwhomhavenotyetbeenofferedcare
atthehealthcentre
202
• Suggesttotheindividualandfamilytotaketheindividualtothehealthcentre
• AsktheHealthExtensionWorkertoalsoencouragethemtoattendthehealthcentreandto
followupontheirprogress.
• Informthehealthcentrethatyouhaveaskedtheindividualtoattend
• Informyoursupervisor
3. Peoplewithothersortsofmentalhealthproblems
• Suggesttotheindividualandfamilytotaketheindividualtothehealthcentre
• Ask the Health ExtensionWorker to encourage them to attend the health centre and to
followupontheirprogress.
• Informthehealthcentrethatyouhaveaskedtheindividualtoattend
• Informyoursupervisor
4. Peoplewithothersortsofdisabilities
• Suggesttotheindividualandfamilytotaketheindividualtothehealthcentre
• AsktheHealthExtensionWorkertoencouragethemtoattendthehealthcentre
• Informthehealthcentrethatyouhaveaskedtheindividualtoattend
• Informyoursupervisor
• RefertheindividualtoanyrelevantNGOs
5. Communitymembersorcommunityleaderswhowantyoutodocommunityengagement
workinanotherkebele
• ItisveryimportantthatyoudoNOTdoanycommunityengagementworkinkebeleswhere
youarenotalreadyworking(i.einkebelesnotallocatedtoCBR).
• Explain that unfortunately you cannot offer community engagementwork in their kebele
andthatthisisoutofyourcontrol.
• Explainthatmedicalcareforpeoplewithschizophreniaisavailableatthehealthcentreand
thatanyonewithschizophreniawhoisnotalreadydoingsoshouldseekhelpthere.
• Givethemthenumberofthetrialco-ordinatorincasetheywishtodiscussthisfurther
• Informyoursupervisorofyourdiscussions.
203
38.5 Summary
• During CBRwork youmay come across other peoplewith problems, for example people
withmentalhealthproblems,orpeoplewithphysicaldisabilities
• Itisimportanttoknowwhattodosothatthesepeoplecangetthebestcarepossible
• Generally,youshouldnottrytolookafterthesepeopleyourself,butyoushouldtellthem
how to get help

204
39 Supportingpeoplewithintellectualdisabilityandschizophrenia
39.1 Whatisintellectualdisability?
Intellectual disability affectsthe waya personunderstands information and how they
communicate.Thismeanstheycanhavedifficulty:
• understandingneworcomplexinformation• developingasfastasotherpeople• learningnewskills• livingindependently
Someintellectualdisabilitiesarediagnosedatbirth,suchasDown'ssyndrome.Othersmightnot
be discovered until the child is old enough to talk or walk. It is possible to have both
schizophrenia and an intellectual disability. Someof the individuals you support throughCBR
mayhavebothschizophreniaandanintellectualdisability.
39.2 Whatcausesintellectualdisability?
Anintellectualdisabilityhappenswhenaperson'sbraindevelopmentisaffected,eitherbefore
they are born, during their birth or in early childhood. Severalfactors can affect brain
development,including:
• themotherbecomingillinpregnancy• problemsduringthebirththatstopenoughoxygengettingtothebrain• illness,suchasmeningitis,orinjuryinearlychildhood
Sometimesthereisnoknowncauseforanintellectualdisability.Intellectualdisabilityisnotdue
toGodpunishingchildrenorparents forsins,orduetocursesorbewitchment.Neglectingor
punishingthepersonforbeingsloworhavingdifficultbehaviourislikelytomakethingsworse.
39.3 Whatproblemsdopeoplewithintellectualdisabilityhave?
Justlikepeoplewithschizophrenia,peoplewithintellectualdisabilitiescanhavedifferentkinds
ofdisabilities.An intellectualdisability canbemild,moderateor severe. Somepeoplewith a
mild intellectual disability can talk easily and look after themselves, but take a bit longer
thanusual to learnnew skills.Othersmaynotbe able to communicate at all andhavemore
thanonedisability.
205
Somepeoplewithintellectualdisabilitiescanbequiteindependent,whileothersneedhelpwith
everyday tasks, such aswashing or getting dressed, for theirwhole lives. It depends on their
abilities. People with intellectual disability are more likely to have the following problems
comparedtootherpeople
• Physicalproblems,forexampleproblemsmovingandwalking;problemswithhearing,speechandsight;epilepsy
• Mentalhealthproblem,includingschizophrenia.• Problemssleeping• Behaviourproblems,includingdoingthingsthatthreatentheirownsafety,orthesafety
ofotherpeople;andtantrums
People with intellectual disabilities may also experience stigma and discrimination, or be
vulnerabletoexploitationandabuse.
39.4 Howshouldwecommunicatewithpeoplewithintellectualdisability?
1. Ensureyouhavetheperson’sattention.Usetheirnameanduseeyecontact2. Aperson’sabilitytounderstandmayvary,forexampleitmaybeworsewhentheyare
tiredorupset.Whenyou’renotsureoftheperson’sabilitytounderstand,itismorerespectfultoassumetheyDOunderstandratherthantheyDON’T
3. Ifyou’renotsure,checkwiththecaregiverhowtheindividualcommunicatese.g.howdotheysayyes/no?
4. Whenyouspeaktotheperson,usesimpleandclearwordsandshortsentences.5. Speaktothepersonwiththesamerespectthatyouwouldanyotheradult,ratherthan
talkingtothemlikeyouwouldtalktoachild.6. Givethepersonlotsoftimetounderstandwhatyouhavesaidandtorespond.7. Checktheperson’sunderstandingintheirownwords.8. Ifyoudon’tunderstandtheperson,youshouldsayso.Don’tpretendtounderstand.
Keepingtryingtounderstande.g.couldyouuseanotherwordtoexplain?Canyoushowme?
9. Ifthepersondoesn’tunderstandwhatyouaresaying,don’tgiveup.Keeptrying,butsayitinadifferentway.Tryusingpicturesoractionstoexplain.
10. Involvethecaregivertohelpyoutocommunicate-butfirstofallaskthepersonifthat’sok.
39.5 Whatisthetreatmentforintellectualdisability?
Thereisnospecifictreatmentforintellectualdisability,unlikeforschizophrenia.Ifapersonhas
both schizophrenia and intellectual disability they will usually be given anti-psychotic

206
medication. If a person has only intellectual disability, they will not usually be given any
medication, as this is unlikely to help. However, if they also have another condition, such as
epilepsy,theymaybegivenmedicationforthis.
39.6 Canpeoplewithintellectualdisabilityrecover?
Intellectual disability is usually lifelong, but some problems may improve. People with
intellectualdisabilitymaycontinuedevelopingand learningbutata slower ratecompared to
other people. Supporting the individual and their family you can help increase the different
kindsofactivitiestheindividualdoesandtoincreasetheirqualityoflife.
39.7 Which RISE CBR modules should we use for people with intellectual disabilities and
schizophrenia?
Ifan individualhasboth intellectualdisabilityandschizophrenia,manyof theirneedsmaybe
thesameas for individualswithonlyschizophrenia.Howevertheremaybesomedifferences.
For example, there may be more need to focus on the module ‘Improving day to day
functioning’. Progressmaybe slower amongst individualswith intellectual disabilities, so you
shouldmake sure familymembersdonot expect to see rapid changes in the individual.Also
whencoveringthemodule‘Improvingthefamilyenvironment’,thefamilymayneedparticular
supportincopingwithchallengingbehaviour.

















