REVIEW ––––––––––––––––––––––––––––––––––––––––– Robot-assisted ophthalmic surgery Howard F. Fine,* { MD, MHSc; Wei Wei, { PhD; Roger E. Goldman, { PhD; Nabil Simaan, {§ PhD ABSTRACT N RE ´ SUME ´ Surgical robots have revolutionized a number of surgical subspecialties, including laparoscopic surgery, urology, gynecology, and orthopedics. Robots offer a number of potential improvements over unassisted human hands, such as tremor filtration, scaling of motion, enhanced dexterity in confined spaces, and extremely high precision. Several designs and prototypes have recently been introduced for use in ophthalmic surgery and they have been tested in animal models. Ophthalmic surgical robots have the potential to expand our treatment armamentarium, reduce complication rates, and hold future promise to treat surgical conditions that remain incurable today. La chirurgie robotique a re ´volutionne ´ plusieurs sous-spe ´cialite ´s, notamment la chirurgie laparoscopique, l’urologie, la gyne ´cologie, et l’orthope ´die. La robotique offre plusieurs possibilite ´s d’ame ´lioration par rapport a ` la main humaine sans aide, tels le traitement du tremblement par la filtration, la mise a ` l’e ´chelle du mouvement, l’ame ´lioration de la dexte ´rite ´ dans les espaces limite ´s, et le besoin d’une pre ´cision extre ˆme. Plusieurs concepts et prototypes, introduits re ´cemment pour utilisation en chirurgie ophtalmique, ont fait l’objet de tests chez des mode `les animaux. La chirurgie robotique ophtalmique permet d’e ´tendre notre arsenal the ´rapeutique, de re ´duire les taux de complication, et de maintenir la promesse de traiter chirurgicalement des maladies aujourd’hui incurables. T he introduction of robots in the operating room has revolutionized a number of surgical fields including laparoscopic surgery, gynecologic surgery, urology, cardi- othoracic surgery, and orthopedics. Robotic surgical assist- ance represents a major paradigm shift in the operating room and the list of surgical indications is growing rapidly as the technology becomes more accessible. Usage is in- creasing almost exponentially. For example, the percentage of robot-assisted radical prostatectomies performed in the United States grew from 0% prior to 2000, to 40% in 2006, to over 80% by 2008, with reported complication rates of incontinence and impotence far lower than with traditional laparoscopic techniques. 1 SURGICAL ROBOT ADVANTAGES The stunning growth rate of robot-assisted surgery is due to the number of advantages it offers over traditional surgical techniques. Tremor filtration can reduce or elim- inate an inherent human flaw. Scaling of motion allows unprecedented precision that is not possible with unassis- ted human hands. Dexterity in confined anatomic spaces can be enhanced, as can maneuverability without direct visualization. 2 Robots can protect surgeons from hazardous exposures and tele-operation of robotic systems can afford patients access to specialized procedures without necessit- ating travel. 3 In fact, all of these advantages have already been achieved. The da Vinci Surgical System (Intuitive Surgical, Sunnyvale, Calif.) is currently the most commonly utilized surgical robot (Fig. 1). Surgeons are seated at a console (master) where they can stereoscopically visualize the oper- ative field. Hand manipulators and foot pedals control the instruments and the endoscopic camera. Movements are translated by the computer to scale motion and to filter or eliminate tremor in real time without any detectable lag to the surgical instruments. The surgical cart, containing up to 4 robotic arms, docks to laparoscopic robotic tools and a 12 mm endoscopic camera provides a 3-dimensional view. A number of modular surgical instruments are available for a wide variety of applications. 4 There are also other commercial robots available for spe- cialized purposes. Examples include the Sansei X Robotic Catheter System (Hansen Medical, Mountain View, Calif.) which allows cardiac electrophysiologists to guide a catheter- based robot with great dexterity and without exposure to fluoroscopy, 5 and the Robotic Arm Interactive Orthopedic System (Mako Surgical Corp, Ft. Lauderdale, Fla.), which is capable of high-precision joint replacement and resurfacing based on pre-operative CT scans. 6 From *Department of Ophthalmology, Robert Wood Johnson University Hospital, New Brunswick, N.J.; { Edward Harkness Eye Institute, Department of Ophthalmology, Columbia University Medical Center, New York, N.Y.; { Advanced Robotics and Mechanism Applications (ARMA) Laboratory, Dept. of Mechanical Engineering, Columbia University, New York, N.Y.; and § Vanderbilt University, Department of Mechanical Engineering PMB, Nashville, Tenn. Presented in part at the Next Generation Eye Surgery, Device and Drug Delivery Symposium in Toronto, Ont., October 17, 2009. Originally received Oct. 20, 2010 Accepted Oct. 29, 2010 Published online Nov. 16, 2010 Correspondence to Howard F. Fine, MD, Department of Ophthalmology, Robert Wood Johnson University Hospital, 10 Plum St., Suite 600, New Brunswick, N.J. 08901; [email protected]This article has been peer reviewed. Cet article a e ´te ´e ´value ´e par les pairs. Can J Ophthalmol 2010;45:581–4 doi:10.3129/i10-106 CAN J OPHTHALMOL—VOL. 45, NO. 6, 2010 581
Transcript
REVIEW –––––––––––––––––––––––––––––––––––––––––
Robot-assisted ophthalmic surgeryHoward F. Fine,*{ MD, MHSc; Wei Wei,{ PhD; Roger E. Goldman,{ PhD; Nabil Simaan,{§ PhD
ABSTRACT N RESUME
Surgical robots have revolutionized a number of surgical subspecialties, including laparoscopic surgery, urology,gynecology, and orthopedics. Robots offer a number of potential improvements over unassisted human hands, suchas tremor filtration, scaling of motion, enhanced dexterity in confined spaces, and extremely high precision. Severaldesigns and prototypes have recently been introduced for use in ophthalmic surgery and they have been tested in animalmodels. Ophthalmic surgical robots have the potential to expand our treatment armamentarium, reduce complicationrates, and hold future promise to treat surgical conditions that remain incurable today.
La chirurgie robotique a revolutionne plusieurs sous-specialites, notamment la chirurgie laparoscopique, l’urologie, lagynecologie, et l’orthopedie. La robotique offre plusieurs possibilites d’amelioration par rapport a la main humaine sansaide, tels le traitement du tremblement par la filtration, la mise a l’echelle du mouvement, l’amelioration de la dexteritedans les espaces limites, et le besoin d’une precision extreme. Plusieurs concepts et prototypes, introduits recemmentpour utilisation en chirurgie ophtalmique, ont fait l’objet de tests chez des modeles animaux. La chirurgie robotiqueophtalmique permet d’etendre notre arsenal therapeutique, de reduire les taux de complication, et de maintenir lapromesse de traiter chirurgicalement des maladies aujourd’hui incurables.
The introduction of robots in the operating room hasrevolutionized a number of surgical fields including
laparoscopic surgery, gynecologic surgery, urology, cardi-othoracic surgery, and orthopedics. Robotic surgical assist-ance represents a major paradigm shift in the operatingroom and the list of surgical indications is growing rapidlyas the technology becomes more accessible. Usage is in-creasing almost exponentially. For example, the percentageof robot-assisted radical prostatectomies performed in theUnited States grew from 0% prior to 2000, to 40% in2006, to over 80% by 2008, with reported complicationrates of incontinence and impotence far lower than withtraditional laparoscopic techniques.1
SURGICAL ROBOT ADVANTAGES
The stunning growth rate of robot-assisted surgery isdue to the number of advantages it offers over traditionalsurgical techniques. Tremor filtration can reduce or elim-inate an inherent human flaw. Scaling of motion allowsunprecedented precision that is not possible with unassis-ted human hands. Dexterity in confined anatomic spacescan be enhanced, as can maneuverability without directvisualization.2 Robots can protect surgeons from hazardousexposures and tele-operation of robotic systems can afford
patients access to specialized procedures without necessit-ating travel.3
In fact, all of these advantages have already beenachieved. The da Vinci Surgical System (Intuitive Surgical,Sunnyvale, Calif.) is currently the most commonly utilizedsurgical robot (Fig. 1). Surgeons are seated at a console(master) where they can stereoscopically visualize the oper-ative field. Hand manipulators and foot pedals control theinstruments and the endoscopic camera. Movements aretranslated by the computer to scale motion and to filter oreliminate tremor in real time without any detectable lag tothe surgical instruments. The surgical cart, containing upto 4 robotic arms, docks to laparoscopic robotic tools and a12 mm endoscopic camera provides a 3-dimensional view.A number of modular surgical instruments are available fora wide variety of applications.4
There are also other commercial robots available for spe-cialized purposes. Examples include the Sansei X RoboticCatheter System (HansenMedical, Mountain View, Calif.)which allows cardiac electrophysiologists to guide a catheter-based robot with great dexterity and without exposure tofluoroscopy,5 and the Robotic Arm Interactive OrthopedicSystem (Mako Surgical Corp, Ft. Lauderdale, Fla.), which iscapable of high-precision joint replacement and resurfacingbased on pre-operative CT scans.6
From *Department of Ophthalmology, Robert Wood Johnson UniversityHospital, New Brunswick, N.J.; {Edward Harkness Eye Institute, Departmentof Ophthalmology, Columbia University Medical Center, New York, N.Y.;{Advanced Robotics and Mechanism Applications (ARMA) Laboratory,Dept. of Mechanical Engineering, Columbia University, New York, N.Y.;and §Vanderbilt University, Department of Mechanical Engineering PMB,Nashville, Tenn.
Presented in part at the Next Generation Eye Surgery, Device and DrugDelivery Symposium in Toronto, Ont., October 17, 2009.
Originally received Oct. 20, 2010Accepted Oct. 29, 2010Published online Nov. 16, 2010
Correspondence to Howard F. Fine, MD, Department of Ophthalmology,Robert Wood Johnson University Hospital, 10 Plum St., Suite 600, NewBrunswick, N.J. 08901; [email protected]
This article has been peer reviewed. Cet article a ete evaluee par les pairs.
Can J Ophthalmol 2010;45:581–4
doi:10.3129/i10-106
CAN J OPHTHALMOL—VOL. 45, NO. 6, 2010 581
SURGICAL ROBOT DISADVANTAGES
There are a number of drawbacks to robots in the oper-ating room. Not surprisingly, expense is a major limitingfactor. The da Vinci Surgical System carries a price tag thatexceeds US$1million. Annual maintenance and service con-tracts, combined with the cost of disposables, can add wellover $100000 to the annual cost of operating the device.Operating room setup time can be significantly longer
with da Vinci assisted cases, over 20 minutes have beendocumented in some studies.7 Predominantly outpatientsurgical sub-specialties, such as ophthalmology, are trend-ing toward shorter duration procedures, faster room turn-over, and overall increased efficiency. These trends may beat odds with the introduction of robotic assistance.Lastly, there exists a learning curve associated with using
new surgical tools, and the complexity of surgical robotsoften presents a challenge both for physicians and oper-ating room support staff alike.
EXAPTATION
Ophthalmic surgeons might reasonably question thevalue of a robotic system in the operating room whencurrent procedures can be performed efficiently and have
low complication rates. Similar questions were posed byurologists, laparoscopic surgeons, gynecologic surgeons,and other surgical subspecialists when robots were firstintroduced to their operating rooms. Yet history hasdemonstrated that once the tool was available, the advan-tages became apparent for select cases and surgical innova-tors applied the tool in creative, and unforeseen, ways.What drives a surgical tool to be adopted?Merely repro-
ducing what surgeons can already do well is unlikely topromote use of robots for ophthalmic surgery. A ‘‘killerapplication’’ is required such as, enabling surgeons to treata condition that is currently untreatable. Significantlyimproving outcomes or lowering complications rates arealso compelling arguments.
OPHTHALMIC SURGICAL ROBOTS
The majority of ophthalmic surgical innovations inrecent years is largely due to engineering breakthroughs.
Fig. 1—da Vinci Surgical System.
Fig. 2—Use of the da Vinci robot to suture a corneal laceration in a
porcine eye. Reprinted with permission.14
Fig. 3—Cannulation of porcine retinal vessels with a 20 mglass micro-
pipette tip. Reprinted with permission: figure was published in Ophthal-
mology, 116, T. Ueta, Y. Yamaguchi, Y. Shirakawa et al., Robot-assisted
vitreoretinal surgery: development of a prototype and feasibility stud-
ies in an animal model, 1538–43, Copyright Elsevier (2009).
Robot-assisted ophthalmic surgery—Fine et al.
582 CAN J OPHTHALMOL—VOL. 45, NO. 6, 2010
In anterior segment surgery, for example, the excimer andnow femtosecond lasers offer precise reshaping of the cor-nea, and new indications include automated capsulorhexisand lens-softening procedures prior to cataract extrac-tion.8,9 In vitreoretinal surgery, small-gauge instrumenta-tion, high-speed cutters, and panoramic-visualizationsystems have made major advances.10 Could robot-assistedsurgery represent an upcoming revolution in our field?Ophthalmic surgery poses a number of unique engin-
eering challenges for robot development. The precisionrequired is great: epiretinal membrane peeling and othertechniques require tolerances on the order of microns, notmillimetres. Visualization is unlike other surgical fields,with not only an operating microscope but often also withspecialized lens systems in the case of vitreoretinal surgery.The pivot point (remote centre of motion) differs fromtypical laparoscopic surgery, making adaptation of com-mercial laparoscopic robots problematic.
Several ophthalmologists have worked to introducerobotic systems for ophthalmic and (or) vitreoretinal sur-gery. Taylor et al.11 developed a ‘‘steady-hand’’ robot cap-able of tremor filtration. Charles et al.12 developed atelerobotic system for eye surgery. Charles foundedMicro-Dexterity Systems, which is currently focused on orthope-dics and neurosurgery.13 Tsirbas et al.14 utilized the daVinci system to suture corneal lacerations in an animalmodel (Fig. 2). As they noted, however, the da Vinci robotsuffered because of a lack of precision and difficultiesresulting from the use of endoscopic rather than micro-scopic visualization. Additionally, the remote centre ofmotion is above the wrist to avoid skin tension duringlaparoscopy rather than below the wrist to maximize intra-ocular manipulation and rotation of the eyeball. Ueta15
demonstrated vascular cannulation in an animal model(Fig. 3). Hubschman et al.16 described a hexapod systemthat works in conjunction with the da Vinci robot. Ourgroup designed a novel dual-arm ophthalmic surgicalrobot (Fig. 4) capable of high precision (, 5 m) and pre-sented both vascular cannulation and stent deployment inanimal models (Fig. 5).17
CONCLUSIONS
Robot-assisted surgery has revolutionized many surgicalsubspecialties. While a number of obstacles exist for oph-thalmic surgical robots, interest appears to be growing,as highlighted by a number of recent presentations andpublications. Robotic assistance for ophthalmic surgeryhas the potential to expand our treatment armamentarium,reduce complication rates, and treat conditions that re-main incurable today.
Disclosure(s): The authors have made the following disclosures:
Howard F. Fine, MD, MHSc: Auris Surgical Robotics, Inc–patent,equity, consultant; Allergan, Inc–consultant, speaker; Bausch & Lomb,Inc–speaker; EyeTech, Inc–consultant; Genentech, Inc–consultant,speaker; NuMe Health LLC–equity; Ophthotech Corp–consultant.
Patents concerning this work are governed by a licensing agreementbetween Columbia University and Auris Surgical Robotics, Inc.
1. Systems, devices, andmethods for surgery on a hollow anatomicallysuspended organ. Simaan N, Fine HF, Chang S. Cross-reference UnitedStates Provisional Patent Applicaions No. 60/845,688, filed on 9/19/2006 and 60/920,848 filed on 3/30/2007.
2. Systems, devices, and methods for retinal vascular access andstent deployment. Fine HF, Simaan N, Chang S, Wei W, GoldmanR. International patent WO/2008/036304, 2007, United Statespatent pending.
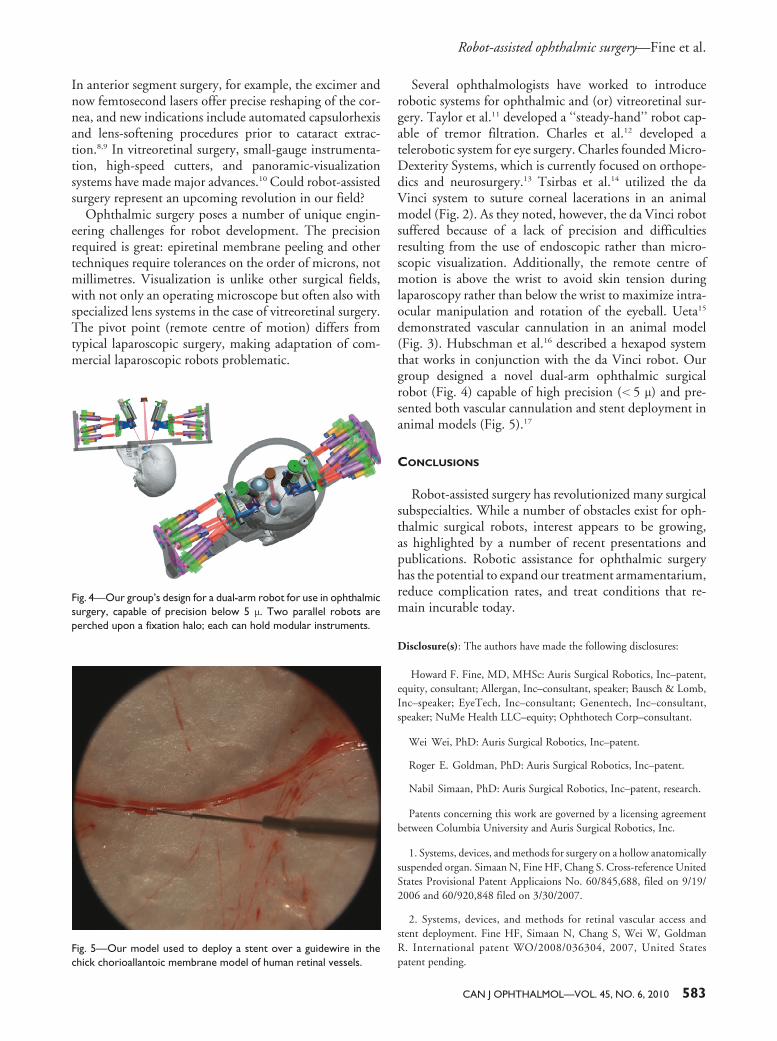
Fig. 4—Our group’s design for a dual-arm robot for use in ophthalmic
surgery, capable of precision below 5 m. Two parallel robots are
perched upon a fixation halo; each can hold modular instruments.
Fig. 5—Our model used to deploy a stent over a guidewire in the
chick chorioallantoic membrane model of human retinal vessels.
3. Marescaux J, Leroy J, Rubino F, Smith M, Vix M, Simone M,Mutter D. Transcontinental robot-assisted remote telesurgery:feasibility and potential applications.Ann Surg 2002;235:487–92.
4. da Vinci Surgical System. Intuitive Surgical, Sunnyvale, Calif.www.davincisurgery.com. Accessed October 1, 2010.
5. SalibaW,ReddyVY,WazniO, et al. Atrial fibrillation ablationusing a robotic catheter remote control system: initial humanexperience and long-term follow-up results. J Am Coll Cardiol2008;51:2407–11.
6. Pearle AD, Kendoff D, Stueber V, Musahl V, Repicci JA.Perioperative management of unicompartmental knee arthro-plasty using the MAKO robotic arm system (MAKOplasty).Am J Orthop 2009;38:16–9.
7. Iranmanesh P,Morel P,Wagner OJ, Inan I, Pugin F,HagenME.Set-up and docking of the da Vinci surgical system: prospectiveanalysis of initial experience. Int J Med Robot 2010;6:57–60.
8. Salomao MQ, Wilson SE. Femtosecond laser in laser in situkeratomileusis. J Cataract Refract Surg 2010;36:1024–32.
9. Masket S, Sarayba M, Ignacio T, Fram N. Femtosecond laser-assisted cataract incisions: architectural stability and repro-ducibility. J Cataract Refract Surg 2010;36:1048–9.
10. Bhatnagar P, Fine HF, Ho I. Evolutionary and RevolutionaryTrends in Vitreoretinal Surgery. Retinal Physician, November2006. Available at www.retinalphysician.com/article.aspx?article5100272. Accessed October 1, 2010.
11. Taylor R, Jensen P, Whitcomb L, et al. Steady-hand roboticsystem for microsurgical augmentation. International Journalof Robotics Research 1999;18:1201–10.
12. Charles S, Das H, Ohm T, Boswell C, Rodriguez, Steele R,Istrade D. Dexterity-enhanced telerobotic microsurgery. 19978th International Conference on Advanced Robotics. Proceed-ings. ICAR’97 Monterey, Calif. 1997;5–10.
13. Charles Retina Institute.Memphis, Tenn. www.charles-retina.com. Accessed October 1, 2010.
14. Tsirbas A, Mango C, Dutson E. Robotic ocular surgery. Br JOphthalmol 2007;91:18–21.
15. Ueta T, Yamaguchi Y, Shirakawa Y, et al. Robot-assisted vitreor-etinal surgery: development of a prototype and feasibility studiesin an animal model. Ophthalmology 2009;116:1538–43.
16. Hubschman JP, Bourges JL, Wilson J, et al. Evaluation of theHexapod Surgical System. American Academy of Ophthal-mology, San Francisco, October 2009.
17. Fine HF, Simaan N, Wei W, et al. A novel dual-arm dexterousophthalmic microsurgical robot: applications for retinal vascularcannulation and stent deployment. Retina Congress, New York,October 2009.