Role of Bariatric Surgery in Obesity and Diabetes Cleveland Clinic Bariatric and Metabolic Institute Endocrinology, Diabetes and Metabolism Philip R. Schauer, MD Professor of Surgery, Cleveland Clinic Lerner College of Medicine Director: Bariatric and Metabolic Institute (BMI) [email protected]
Transcript
Role of Bariatric Surgery in Obesity and Diabetes
Cleveland Clinic Bariatric and Metabolic Institute Endocrinology, Diabetes and Metabolism
Philip R. Schauer, MD Professor of Surgery, Cleveland Clinic Lerner College of Medicine
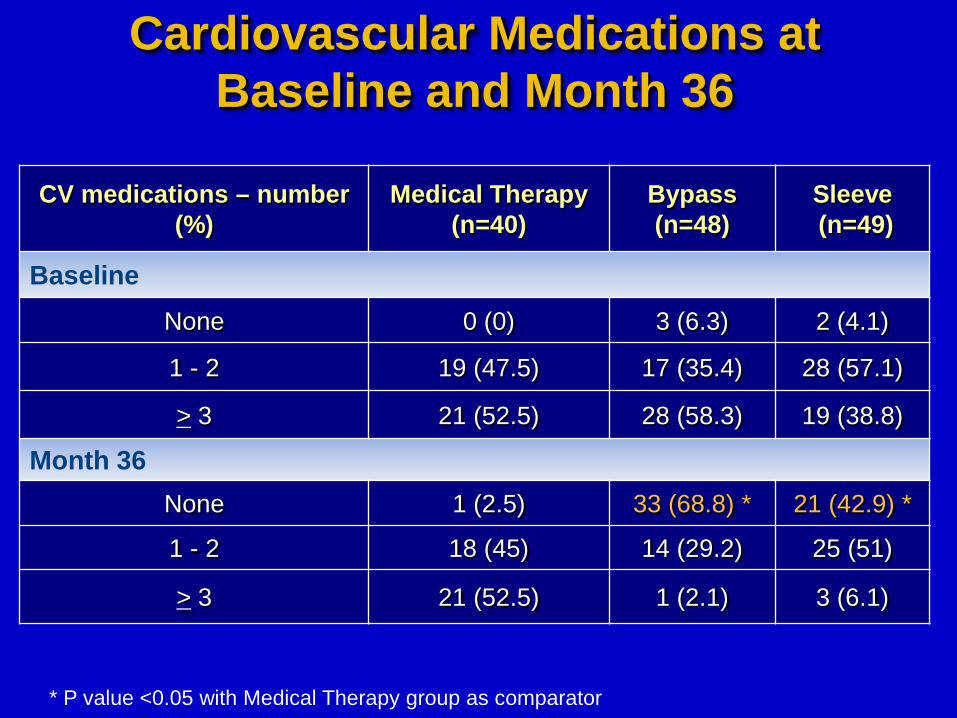
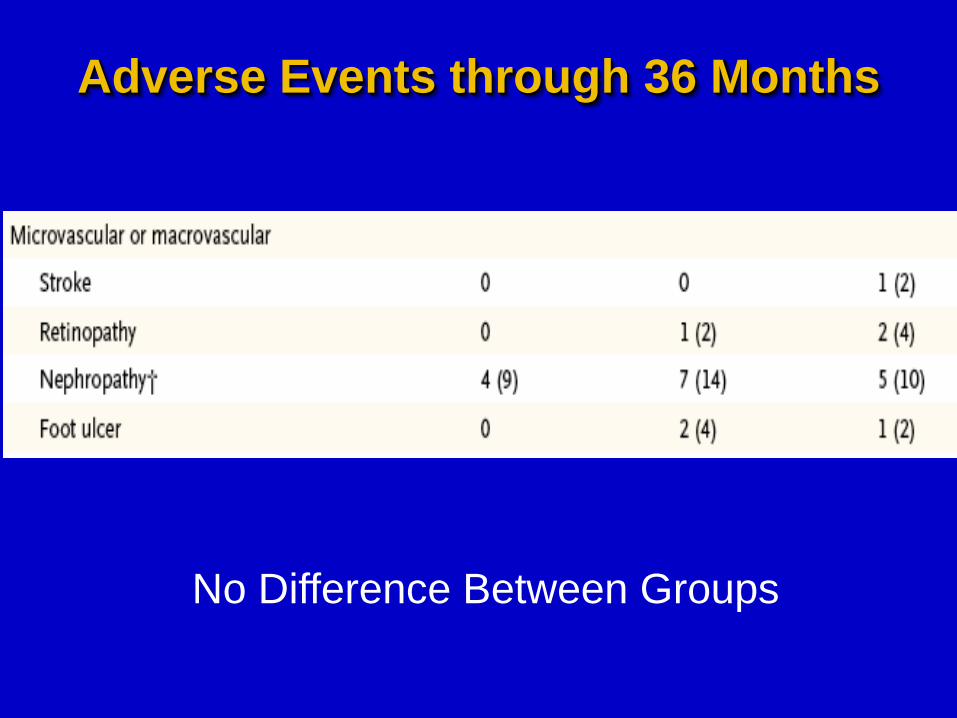
• No difference in BP or LDL • No CV events or death after surgery • Anemia (15%), Reoperation (8%)
Surgical vs Medical Treatments for Type 2 Diabetes Mellitus: A Randomized Clinical Trial
Anita P. Courcoulas, MD, MPH; Bret H. Goodpaster, PhD; Jessie K Eagleton, MPH; Steven H. Belle, PhD, MScHyg; Melissa A. Kalarchian, PhD; Wei Lang, PhD; Frederico G.
S. Toledo, MD; John M. Jakicic, PhD
Roux-en-Y Gastric Bypass Surgery or Lifestyle With Intensive Medical Management in Patients With Type 2 Diabetes Feasibility
and 1-Year Results of a Randomized Clinical Trial Florencia Halperin, MD; Su-Ann Ding, MD; Donald C. Simonson, MD, MPH, ScD;
Jennifer Panosian, BA; Ann Goebel-Fabbri, PhD; Marlene Wewalka, MD; Osama Hamdy, MD, PhD; Martin Abrahamson, MD; Kerri Clancy, RN;
Kathleen Foster, RN; David Lautz, MD; Ashley Vernon, MD; Allison B. Goldfine, MD
2 More Recent RCT’s JAMA Surgery June 4, 2014
Both Show Superiority of Surgery vs. Intensive Medical RX
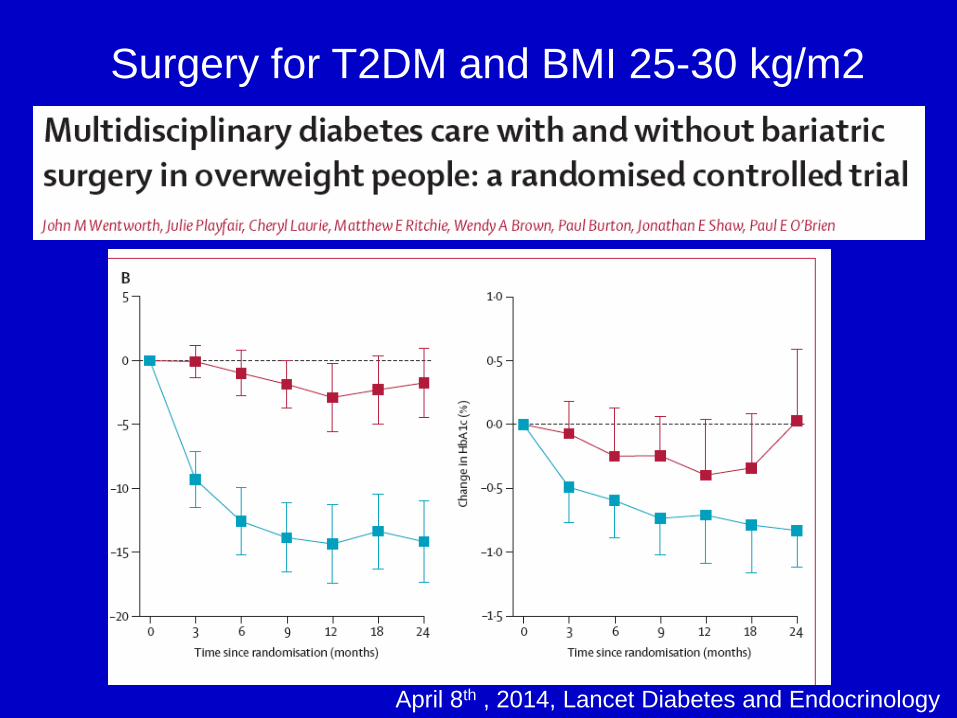
April 8th , 2014, Lancet Diabetes and Endocrinology
Surgery for T2DM and BMI 25-30 kg/m2
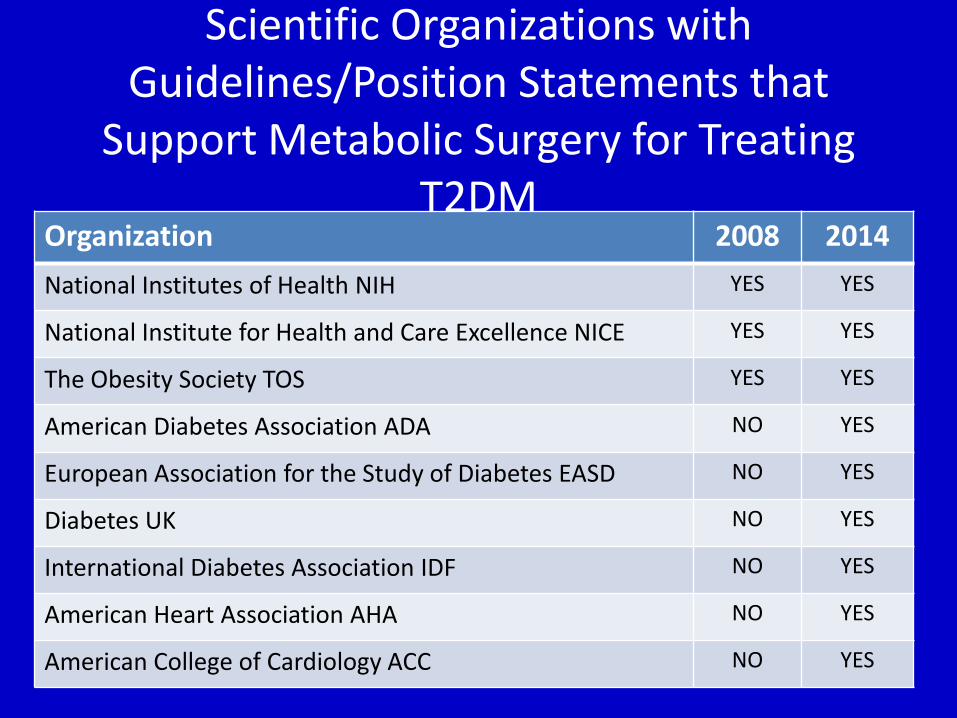
Scientific Organizations with Guidelines/Position Statements that
Support Metabolic Surgery for Treating T2DM
Organization 2008 2014 National Institutes of Health NIH YES YES
National Institute for Health and Care Excellence NICE YES YES
The Obesity Society TOS YES YES
American Diabetes Association ADA NO YES
European Association for the Study of Diabetes EASD NO YES
Diabetes UK NO YES
International Diabetes Association IDF NO YES
American Heart Association AHA NO YES
American College of Cardiology ACC NO YES
International Diabetes Federation Guidelines
• Surgery should be an accepted option in people who have type 2 diabetes and BMI of 35 or more
• Surgery should also be considered as an alternative treatment option in persons with BMI 30 to 35 when diabetes cannot be adequately controlled by optimal medical regimen, especially in the presence of other major cardiovascular disease risk factors
• In Asian, and some other ethnicities of increased risk, BMI action points may be lower e.g. BMI 27.5 to 32.5
Bariatric Surgical and Procedural Interventions in the Treatment of Obese Patients with Type 2 Diabetes
Download at www.idf.org
Summary Bariatric Surgery for T2DM
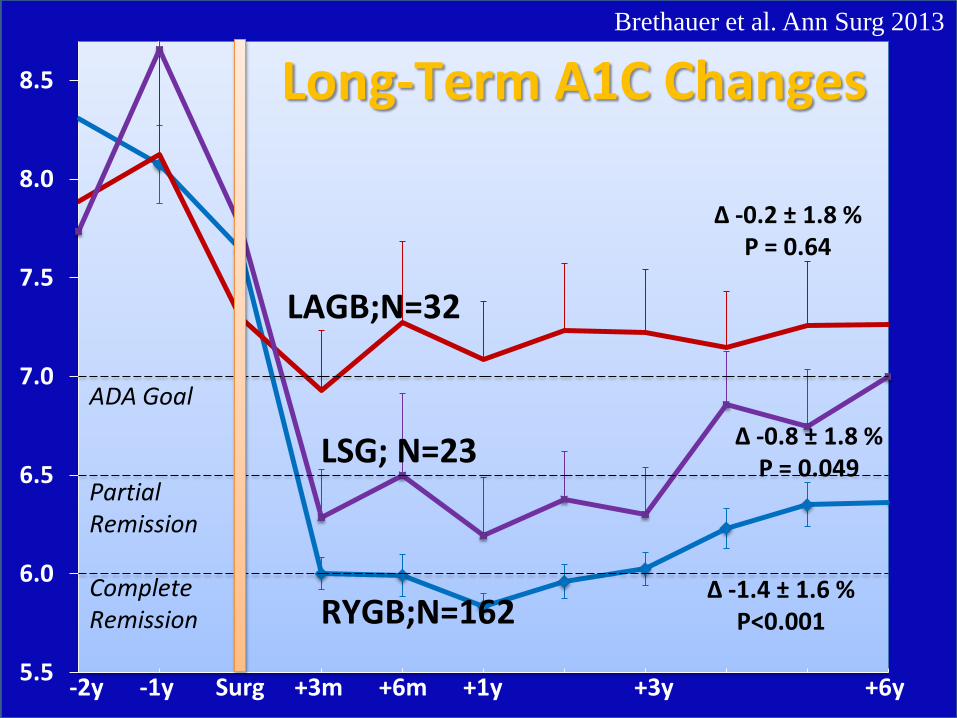
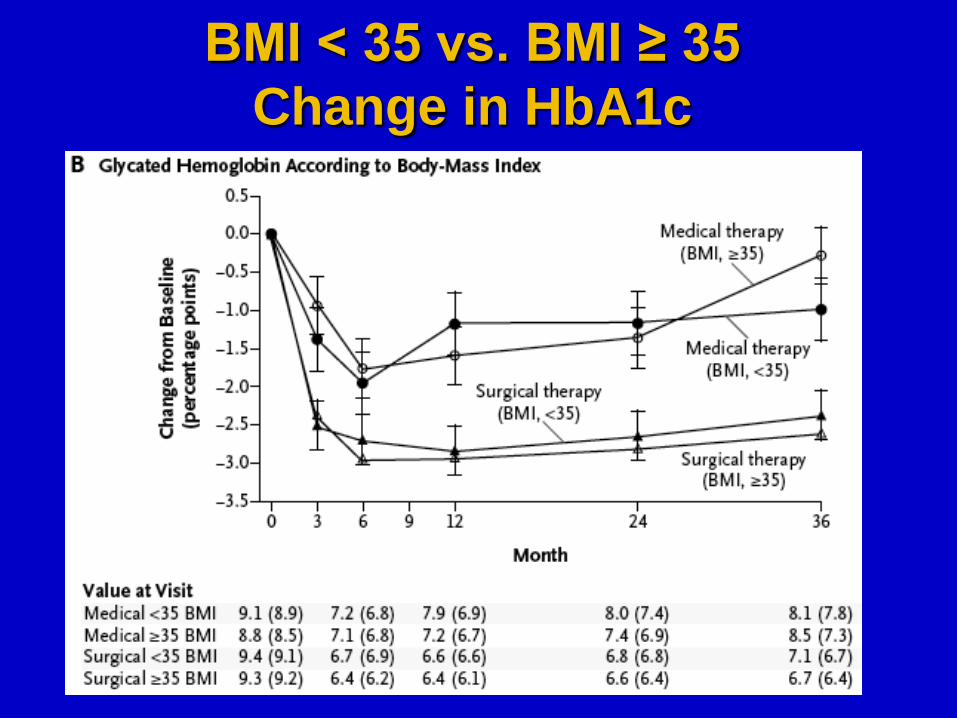
• 14 RCT’s (>950 patients, BMI 25-52) show that surgery results in superior glycemic control compared to medical Rx ( up to 3 year follow-up)
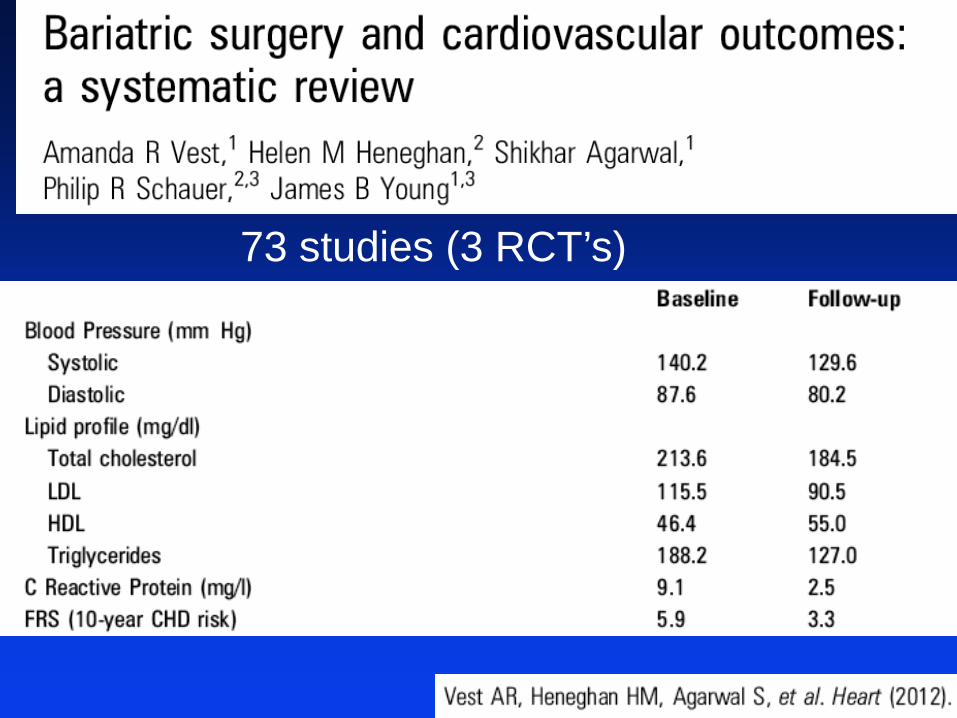
• CV risk factors improved with surgery
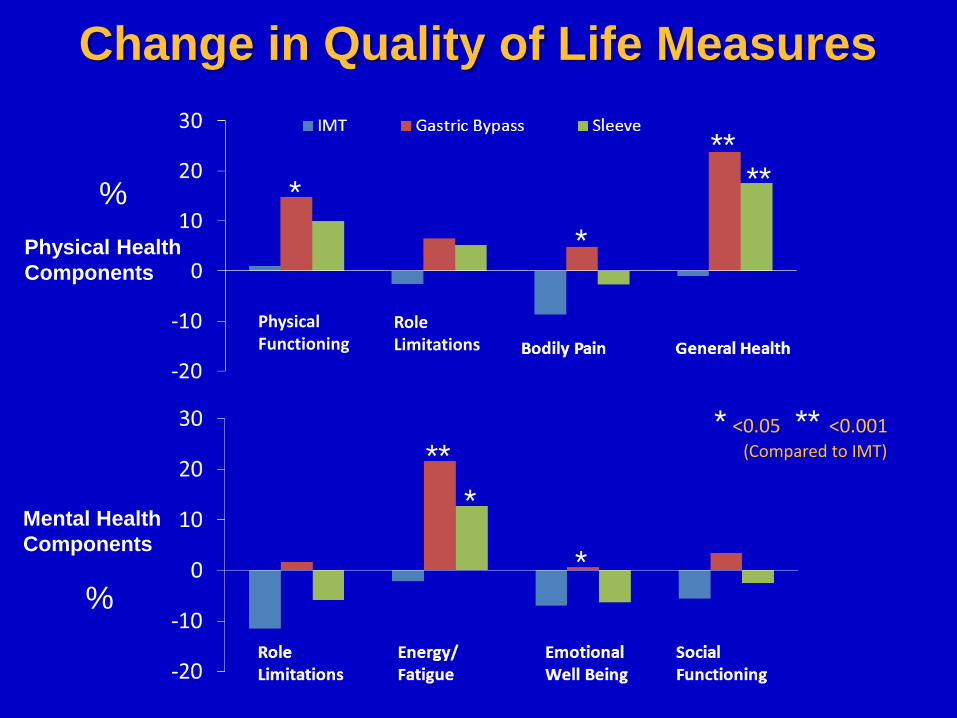
• Surgery significantly improves quality of life
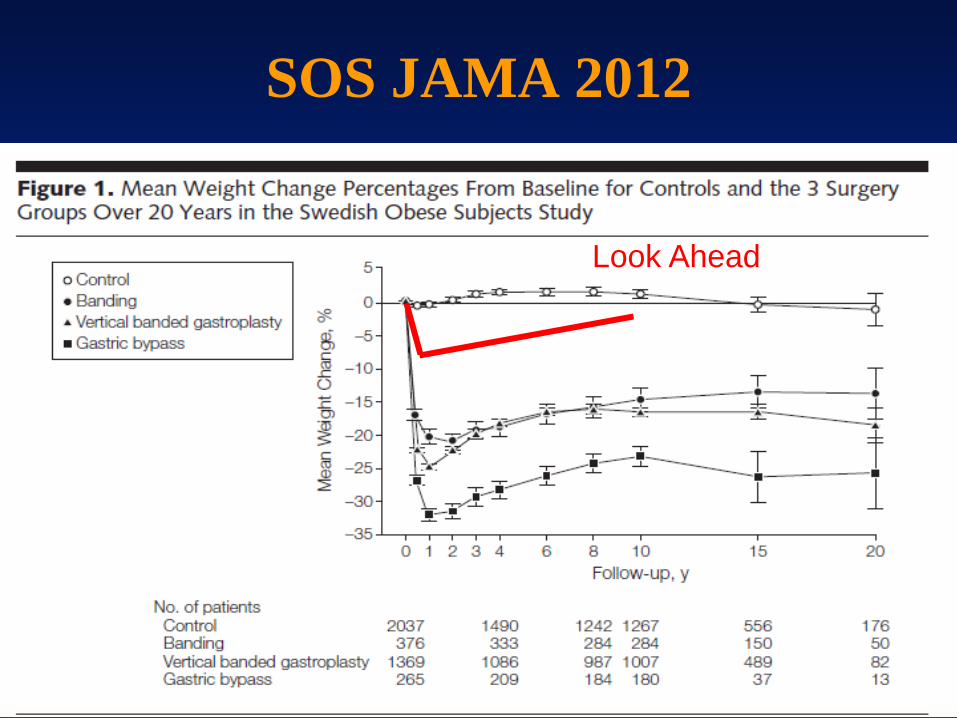
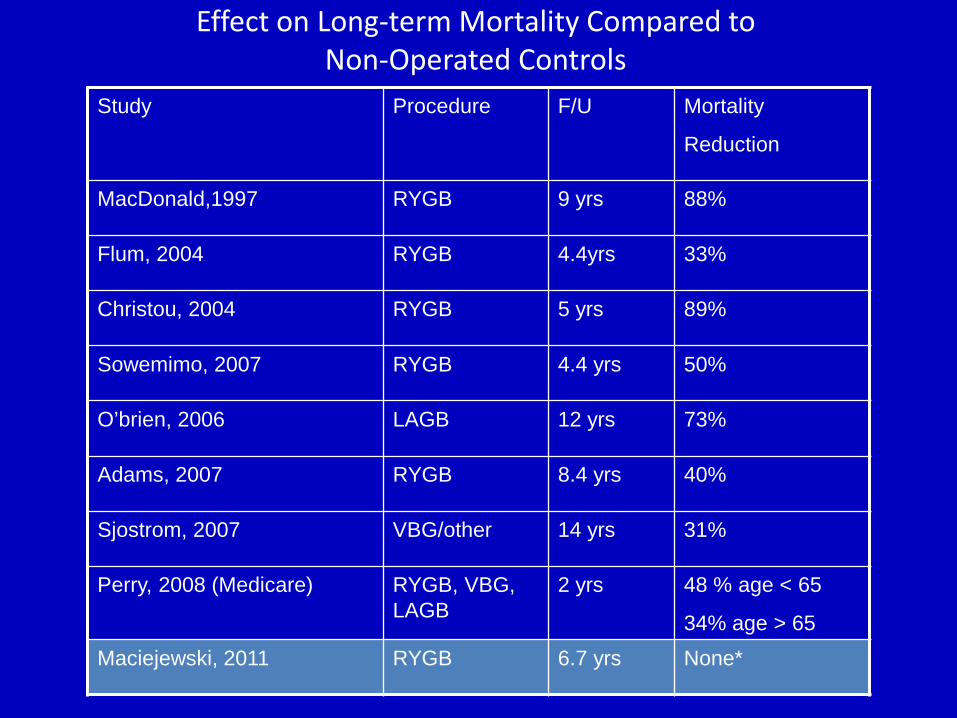
• Surgery reduces mortality/CV events (non-RCT, SOS)
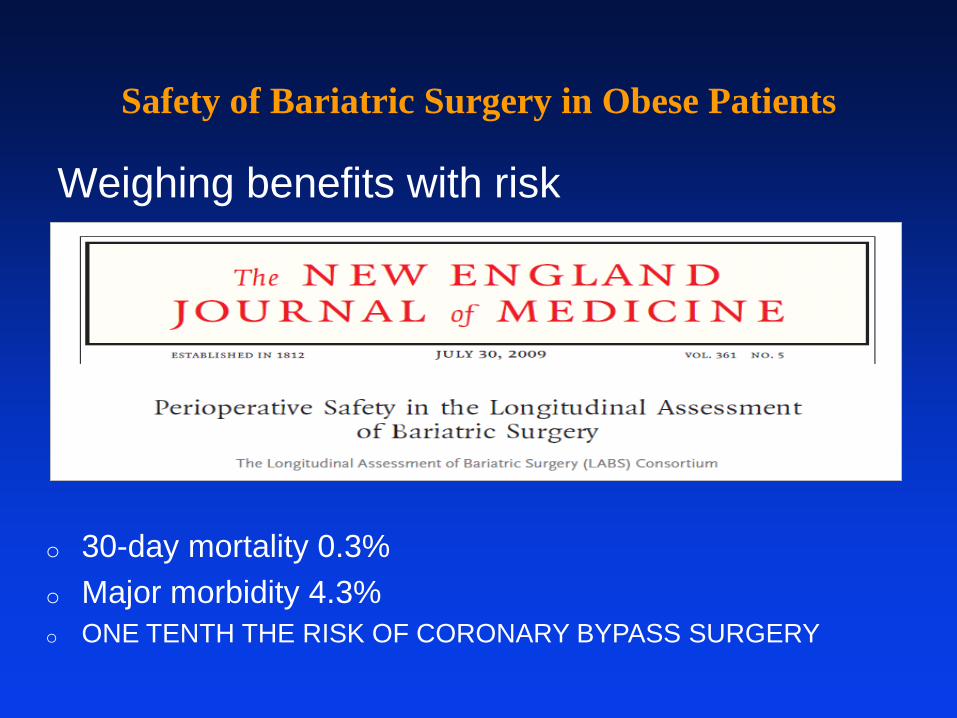
• Perioperative morbidity <5%, mortality < 0.3%
Conclusion Bariatric Surgery for T2DM
Patients with uncontrolled T2DM (HbA1c >7.0%) and Obesity (BMI > 30) should be considered for bariatric surgery
THANK YOU! Role of Bariatric Surgery in
Obesity and Diabetes
Cleveland Clinic Bariatric and Metabolic Institute Endocrinology, Diabetes and Metabolism
Philip R. Schauer, MD Professor of Surgery, Cleveland Clinic Lerner College of Medicine