8 Role of the midwife and the obstetrician in obstetric critical care – a case study from the James Cook University Hospital Helen Simpson * BM BS BMed Sci MRCOG Consultant Obstetrician Debbie Barker BSc (Hons)midwifery Critical Care Midwife The James Cook University Hospital, Marton Road, Middlesbrough TS4 3BW, UK The role of the obstetrician and the midwife are fundamental to the successful antenatal management, delivery and postpartum management of the critically ill obstetric patient. How- ever, there is a dearth of published literature on the integrated management of these roles. This chapter addresses these issues by reporting on experiences at James Cook University Hospital in developing a more holistic approach to patient management and critical care through appraisal of these roles, and resulting extension of the role of the midwife to encompass phys- iological assessment, understanding the effects of pregnancy on disease, interpretation of, and acting on, blood results including arterial gases, and development of the service through the development of guidelines and undertaking audits. The role of the midwife has been extended taking an overview of critical care of the mother, baby and family. The resulting development of the role of the obstetrician encompasses leadership, clinical knowledge, documentation, guide- line development, risk management and the communication functions of debrief, audit and education. Development of the roles has reduced admissions to intensive care and increased patient satisfaction and adherence to policies at James Cook University Hospital. This paper provides a critical appraisal of this role development and discusses some of the lessons learned. Key words: critical care; obstetrics; maternity; obstetrician; midwife; role. The aim of this chapter is to discuss the roles of both the midwife and the obstetrician within critical care. Very limited research is available, especially regarding the role of the obstetrician. This chapter will consider the reasoning behind setting up a critical * Corresponding author. Tel.: þ44 (0) 1642 282777; Fax: þ44 (0) 1642 854874. E-mail address: [email protected](H. Simpson). 1521-6934/$ - see front matter ª 2008 Elsevier Ltd. All rights reserved. Best Practice & Research Clinical Obstetrics and Gynaecology Vol. 22, No. 5, pp. 899–916, 2008 doi:10.1016/j.bpobgyn.2008.06.007 available online at http://www.sciencedirect.com
Transcript
Best Practice & Research Clinical Obstetrics and GynaecologyVol. 22, No. 5, pp. 899–916, 2008
doi:10.1016/j.bpobgyn.2008.06.007
available online at http://www.sciencedirect.com
8
Role of the midwife and the obstetrician
in obstetric critical care – a case study
from the James Cook University Hospital
Helen Simpson* BM BS BMed Sci MRCOG
Consultant Obstetrician
Debbie Barker BSc (Hons)midwifery
Critical Care Midwife
The James Cook University Hospital, Marton Road, Middlesbrough TS4 3BW, UK
The role of the obstetrician and the midwife are fundamental to the successful antenatalmanagement, delivery and postpartum management of the critically ill obstetric patient. How-ever, there is a dearth of published literature on the integrated management of these roles.This chapter addresses these issues by reporting on experiences at James Cook UniversityHospital in developing a more holistic approach to patient management and critical care throughappraisal of these roles, and resulting extension of the role of the midwife to encompass phys-iological assessment, understanding the effects of pregnancy on disease, interpretation of, andacting on, blood results including arterial gases, and development of the service through thedevelopment of guidelines and undertaking audits. The role of the midwife has been extendedtaking an overview of critical care of the mother, baby and family. The resulting development ofthe role of the obstetrician encompasses leadership, clinical knowledge, documentation, guide-line development, risk management and the communication functions of debrief, audit andeducation. Development of the roles has reduced admissions to intensive care and increasedpatient satisfaction and adherence to policies at James Cook University Hospital. This paperprovides a critical appraisal of this role development and discusses some of the lessons learned.
The aim of this chapter is to discuss the roles of both the midwife and the obstetricianwithin critical care. Very limited research is available, especially regarding the role ofthe obstetrician. This chapter will consider the reasoning behind setting up a critical
care team of midwives, what barriers arise in midwifery care of the critically ill woman,the need for education and competencies. It will also discuss the role of team workingand communication, and clinical roles and limitations. Extension of the roles into policydevelopment, risk management, debriefs and leadership are also discussed.
THE ROLE OF THE MIDWIFE IN OBSTETRIC CRITICAL CARE
Setting up an obstetric critical care team is not merely a question of calling a group ofindividual midwives a ‘team’. Midwives must be suitably trained and appropriatelyorganized for the service they provide. The following discussion provides an overviewof the features which underpinned the development of an obstetric critical care teamat the James Cook University Hospital (JCUH), and further discusses the factors whichare essential to the team’s continued development and success.
Management of the high-risk obstetric patient, cared for in high-dependencysettings (HDU) by professionals with a commitment to obstetrics, is a recent phenom-enon, with countries such as the UK failing to recognize HDU in obstetrics as anindependent specialty for a number of years.1 However, several reports publishedover the last decade emphasized the need for a suitably trained multidisciplinaryteam to be developed within nationwide consultant-led units, with a vision for improv-ing the overall management of the critically ill obstetric patient.2–5 These reportsprovided a template for midwives to develop new ways in which to work interdepen-dently within the National Health Service, forging a path for partnerships and alliancesto be formed amongst all healthcare providers.5 This approach to multidisciplinaryteamwork was welcomed by both the medical and midwifery professions, as itfostered and developed women-centered care within a high-technology environment,creating positive clinical and emotional outcomes for women.
Several reports published by the Confidential Enquiry into Maternal and ChildHealth (CEMACH) over the last decade have highlighted areas of concern in obstetriccritical care. Several CEMACH reports suggest that although maternal mortality in theUK is low, many of the mortality cases reported were preventable.2,6,7 CEMACH iden-tified that over 50% of maternal deaths received some level of suboptimal care withinboth the direct and indirect pathologies.2,6,7 CEMACH further suggests that factorswhich contributed to substandard care included conditions which were ineffectivelydiagnosed, conditions which received ineffective or wrong treatment, failure of staffto recognize or act upon the severity of critical illness, care which was not consistentwith agreed guidelines, and poor communication amongst cross-disciplines.6 From theevidence available, this appears to be the result of a lack of a sound knowledge base onspecific medical conditions which warranted the involvement of the wider multidisci-plinary team, and lack of specific knowledge in critical complications with staff failing toimplement protocols or even appreciate their relevance in the care of the critically illwomen.2,6,7 It has also been identified within the CEMACH reports that midwiferystaff fail to call upon the relevant senior medical professionals capable of managingcritical situations, with junior doctors attending women and, at times, misdiagnosingconditions.2,6,7
A study undertaken within a large London trust addressed the numerous issuesexperienced by midwifery staff caring for high-risk obstetric women, and the findingswere similar to those of the CEMACH report.8 This small-scale qualitative studyinvolved 11 midwives whose responses were generated by semi-structured interviewsand a questionnaire involving simulated exercise scenarios. Although small, the study
Role of the midwife and the obstetrician in obstetric critical care 901
findings were adequately supported by a large systematic literature review of criticalcare in obstetrics, providing the study with credibility. The study explored midwives’recognition and management of critical illness, and addressed some of the difficultiesfacing midwives managing the care of the critically ill obstetric woman. Many importantissues were raised within the study, each of which warrants a more in-depth analysisindependent of this article. Issues raised included the following.
� Pattern recognition: Findings suggest that more experienced midwives seemed tobe more able to apply pattern recognition when recognizing early signs of deterio-ration in sick patients. This appeared to be more evident amongst midwives withprevious nursing experience and less evident in midwives entering the professionvia the direct entry route.� Poor continuity of care from consultants across various disciplines, including
obstetrics.� Inconsistency in care and poor communication between all disciplines.� Lack of support for midwives, resulting in discrepancies being made during observa-
tion, monitoring and communication.� Staffing levels and skill mix.� Midwives relied on direct guidance from medical personal without understanding
the implications of what they were asked.� Midwives made little reference to the clinical significance of certain vital signs and
how to apply these correctly to practice.
Midwives within the study felt that learning came from experience, and that eachsituation presented to them offered a new learning opportunity. In this regard, theless-frequent critical care experience that midwives gained was perceived as problem-atic, inhibiting the ongoing development necessary to gain the repertoire of skillsrequired to practice safely. Midwives felt more positive and in control whilst caringfor high-risk women when they were supported by the presence of a more experi-enced midwife, equipped with knowledge and intelligence in critical care.8 Anaesthe-tists were also viewed quite positively within the study, and recognized as a greatand indeed valuable source of support to staff. Lack of adequate support during a crisiscan provoke feelings of overwhelming anxiety which, in turn, can influence a midwife’sability to cope with the stress of managing critically ill women; findings which wereidentified and supported within the study.8
Other issues raised by this study include the reluctance displayed by medicalpersonal from various disciplines to transfer obstetric patients to a more appropriateenvironment when the labour ward setting was neither equipped with the staff nor theresources to afford the care required. The reasons for this were not disclosed. TheCEMACH report identified that some maternal deaths would have been avoided ifthere had not been a delay in transfer of care to intensive care (ITU) or HDU areassupported by a clinician who specialized in high-risk obstetric care.7
Another area of grave concern to arise from the study was that some junior mid-wives acted upon the orders given by doctors without having an understanding of whatthey were doing, why they were doing it and what the implications of their actionsmight be. A recipe for disaster in terms of professional accountability! Midwives, unlikeother healthcare professionals, are not limited to their practice by legislation, but maypractice and develop in various areas provided that the midwife has the skill andcompetence to do so.9 When midwives embark upon a new extension in their role,as they do when caring for high-risk obstetric women requiring invasive monitoring
902 H. Simpson and D. Barker
and intervention, it increases their accountability and responsibility fundamentally,deeming them answerable for any actions or decisions taken. Midwives must ensurethat they are adequately prepared, trained and competent to care for high-risk womenwho require specialist care, as failure to do so will result in a breach of professionalconduct and duty of care.
In 1997, the issues raised in CEMACH (1996), Changing Childbirth (1993) andTowards a Safer Childbirth (1999) were addressed at local level within the authors’client group, and the need to establish a critical care service was identified. Whenassessing the needs of the patient group, factors taken into account included the avail-ability of resources such as:
� funding for training and development;� feasibility for the provision of staffing a core critical care team 24 hours per day, 365
days per year;� availability of a consultant lead;� availability of assistance from cross-disciplines;� availability of ITU beds;� availability of neonatal unit (NNU) intensive care cots; and� audit of the number and severity of obstetric complications presenting in the unit
for the year preceding team development.
Implementation of the critical care project at JCUH was based on the DevelopingExcellence Model, and the success of the project was based on strong leadership fromthe ward manager. A sum of £28 000 was secured from the Working Paper 10 trainingmonies, which assisted with the initial secondment and training of staff. Additionalfunding has been generated through the kind generosity of the local Women’s RoyalVoluntary Service, public donations, participation in the Magpie Trial, 2002 winnerof the Trust Team of the Year Award and the production of a regional study day atJCUH entitled ‘Critical care in obstetrics’. The day was produced and presented bythe critical care midwives with grateful assistance from various cross-disciplines, whichpromoted the sharing of good practice. The key note being ‘A multidisciplinaryapproach to the development of critical care in obstetrics’.
Staff members working within the critical care team were and remain chosen asa result of their interest in critical care and their past experience. All staff undertakea 10-week rotation to ITU within both the surgical and medical disciplines, cardiacthoracic theatres, coronary care, renal and medicine units and have periodic yearlyupdates in the same. As well as clinical development, all staff undertake academic train-ing and complete a module at the University of Teesside entitled ‘Care of the criticallyill obstetric patient’. The module has been developed to cover both the physiology andpathophysiology of diseases of pregnancy, and includes medical complications exagger-ated by pregnancy, which are on the increase within the pregnant population.10
Education is pivotal in the development of the midwife.11 Prior to the full establish-ment of the critical care team, original members completed a general ITU academicmodule at level 2 with very little obstetric input. However, through the evolution ofthe team since its instigation in 1999, an academic training module has been developedat level 3, which has been the result of joint collaboration between academic tutorsfrom the University of Teesside and critical care midwives from JCUH. Midwivesthroughout the Northern Region now access the course. A member of the criticalcare team whose subspecialty is education regularly participates in the teaching ofnovice critical care midwives on the course, and a course lecturer regularly attends
Role of the midwife and the obstetrician in obstetric critical care 903
critical care team meetings, providing a valuable link between practice and theory. Thecontent of the course focuses on physiological and pathophysiological changes withinthe organ systems during pregnancy, and includes the psychosocial impact on thefamily unit. Inclusion of an in-depth obstetric element provides novice critical caremidwives with the knowledge to care for this pregnant population.
Novice critical care midwives need to be suitably prepared for this extension withintheir role via the attainment of academic and clinical competencies in order to providecompetent high-dependency care. The critical care training pathway at JCUH effec-tively links theory to practice as it has been jointly agreed to meet both women’sand midwives’ needs. These competencies are initially validated by academic tutors,delivery suite leads and critical care mentors, whose role it is to work alongside,support and guide novice critical care midwives whilst they achieve clinical compe-tence. Periodic validation of acquired skills is achieved in accordance with Nursingand Midwifery Council guidelines through the active use of annual supervisoryreviews.12–14 Midwives by virtue of their status have a legal, contractual and profes-sional obligation to provide evidence in various forms which reflects that changesand advances in their practice is for the benefit and safety of the women they serve.This is supported by statutory midwifery supervision, knowledge and skills framework,and professional practice development reviews.15 Critical care midwives must provethat the care they provide is evidence based, and they must be able to demonstratethat they have the necessary repertoire of skills and competence to perform thetask. Supervisors of midwives can assist in assessing and implementing professionalstandards that assess individual team member’s qualities and clinical ability requiredfor safe practice when providing critical care. Active use of the above resources duringthe process of practice development will enhance a pro-active and supportive environ-ment, where both novice and experienced members of the critical care team will beencouraged to evaluate each stage of their practice in accordance with contractual andprofessional responsibilities.
When assessing suitability for the formation of an obstetric critical care team,smaller units may not be equipped with the necessary resources for the developmentof a specialized team, or may not encounter enough critically ill women in order tomaintain competency skills; factors which have been proven to contribute to mortalityand morbidity in the UK.11 In this instance, optimal care may be provided in the formof an outreach service, by combining the expertise of clinical subspecialists from thevarious cross-disciplines, supported by midwives who have been provided with aca-demic education in obstetric critical care and clinical training in ITU settings. Midwiferystaff will require the support of their managers when providing an outreach service (arecent recommendation for service provision within critical care areas) in order tomanage conditions collaboratively. However, it will not prevent mother and infantseparation, or foster and promote women-centered care within suitable environ-ments16 if women are admitted to general critical care units. The development ofan outreach service is currently under review at JCUH. This service will target areassuch as accident and emergency departments and medical admissions, where womencan and often do present with life-threatening conditions.
Units that have a limited number of annual admissions of critically ill women with noobstetric HDU facilities often rely on professionals from cross-disciplines to care forpatients away from the labour ward setting, as was the regime previously at JCUH.1
Maintenance of maternal health by professionals from different disciplines can posea unique medical and ethical challenge; pregnancy induces changes in every organ ofthe pregnant women, each of which is intended to provide the best outcome for
904 H. Simpson and D. Barker
the mother and fetus. However, when deviations from the normal state of pregnancyoccur, a catastrophic cascade of events can develop which requires an effectiveresponse.17 Healthcare professionals from cross-disciplines working in isolation mayfail to appreciate the adverse effects on the maternal–fetal unit of obstetric emergen-cies such as haemolysis–elevated liver enzymes–low platelets (HELLP) syndrome, pre-eclampsia and sepsis, and subsequently fail to recognize secondary complications asa result of this. They may not have available the resources, skills or staff to monitorwomen with appropriate technology, or interpret findings correctly in the pregnantpopulation.
Since the critical care team was established at JCUH, the authors have developeda close alliance with various divisions, with critical care team members often takingthe lead in liaising with ITU staff and physicians from numerous disciplines in thecare of women with complex and complicated pregnancies. It is suggested that thesharing of knowledge and experience that takes place between staff from variousdisciplines enhances the development of mutual trust and respect, with staff readilyand comfortably collaborating and communicating with one another in the manage-ment of the critically ill women.18
Communication and lack of uncoordinated teamwork was discussed as beinga major contributory factor pertaining to substandard care, and appears to havebeen a recurring theme in numerous CEMACH reports.2,6,8 Highlighted within thecurrent CEMACH report was midwives’ reluctance to refer across different specialties(horizontal communication) when caring for high-risk clients, even when thereappeared to be a serious risk to health or deterioration in a condition.6 Midwivesshould possess the ability and skills to be able to make decisions to refer clients aboutwhom they are concerned, which may at times involve challenging less-experiencedmedical staff. Development of horizontal communication skills involves the develop-ment of certain interaction skills such as negotiation and assertiveness (communicatingon a macro level).19 Midwives’ ability to achieve this depends upon their awareness inthe areas of knowledge of complications, guidelines and protocols, current researchand past experience (reflection). Lack of assertiveness and unwillingness to beassertive may be the result of decreased confidence and insecurity in oneself due toinadequate knowledge or experience and inability to interpret findings.20 The deci-sion-making process is described as being both beneficial and progressive in nature,especially in critical or life-threatening situations.21
Numerous theorists have explored and developed models to assist in the decision-making process, and many of them have compared novice with expert.22 Benner’s(1982–1984) Skills of Acquisition Model stresses the significance of experience ratherthan knowledge as being the most effective prerequisite to the decision-makingprocess.22 This model focuses on the process by which ‘expert’ health professionalsreach clinical decisions within their practice by acting upon ‘cues’ in a clinical situationthat ‘non-experienced’ health professionals may miss.23 Several arguments have beenput forward which dispute Benner’s model, suggesting that intuition alone does notmake for a defence against negligence or support for clinical excellence. Other writerson the subject state that a sound knowledge base must be developed which incorpo-rates both the analysis and synthesis of empirical research in supporting professionalintuitive feelings. These skills are achievable by individuals attending educationalprogrammes that support and encourage the use of both semantic and episodicdevelopment (theoretical and clinical experience).24 An effective multidisciplinaryapproach achieved through positive communication channels has been proven to bepivotal to both midwife and client well-being.
Role of the midwife and the obstetrician in obstetric critical care 905
The work of the midwives within the critical care team at JCUH involves assistancein diagnosing, coordinating and managing women’s care in consultation with obstetri-cians, anaesthetists and physicians from various disciplines, with the aim of developinga robust plan of care. CEMACH supports this approach, outlining strategies forimproving the overall management of the critically ill obstetric woman. These include:referral to a practitioner specializing in obstetric high-risk care would prevent a delayin the treatment of the critically ill obstetric woman and have positive effects on theoverall outcome.6 Women requiring high-dependency care at JCUH usually requireassistance with haemodynamic and cardiac monitoring due to hypertensive, renal,cardiac or systemic disorders related to or exaggerated by pregnancy. It is the roleof the critical care midwife at JCUH to provide further support by:
� the administration and maintenance of arterial and central venous pressure lines;� developing in-depth knowledge and understanding of the impact that disease has on
fluid shifts within the compromised system, and administering the correct fluidsaccordingly;� displaying a sound knowledge base in the interpretation of blood gas analysis includ-
ing metabolic/respiratory acidosis and its impact on maternal and fetal health;� interpreting haemoglobin, electrolytes, liver and kidney function tests and coagula-
tion studies, and being vigilant with respect to pathological results, acting promptlyupon findings, liaising with haematologists and biochemists when required;� displaying knowledge regarding the physiological effect that pregnancy has on the
cardiovascular system, and being able to recognize abnormal electrocardiogrampatterns and initiate a correct response;� displaying a sound knowledge base regarding the effects of systemic maternal
disease upon the fetus;� initiating the administration of intravenous antihypertensives and anticonvulsants in
the absence of a obstetrician when the situation calls for a rapid response; and� the team is self-rostering and provides this service to all women working across the
consortium of antenatal, intranatal and postnatal care 24 hours per day, 365 daysper year.
The critical care team at JCUH supports and encourages all general midwives totake the lead with high-dependency clients in a number of cases, offering supportwith interpretation of vital signs, fluid replacement, interpretation of blood resultsand assistance with quick routes of referral to the wider multidisciplinary teamwhen rapid investigation and treatment is required. General midwives also have theopportunity to shadow and work with a critical care midwife when staffing levelsand workload allow. The critical care team provides further support with regularteaching regarding the recognition and management of ill women, which includes anoverview of protocols and algorithms, and the role that various disciplines can beexpected to take. These teaching sessions are open to all midwifery and medical staffwishing to participate. Critical care midwives at JCUH have a diverse mix of compli-mentary skills including education, midwifery supervision, breastfeeding key worker,subspecialist in diabetes, and intermediate and advanced life support practitioners.Team members also undertake the role of delivery suite shift team leader. To furthersupport staff development, consultant leads from various disciplines lead trainingsessions in both obstetric and medical conditions which afflict the pregnant population,and include the recognition and management of a pathological crisis and multidisciplin-ary involvement.
906 H. Simpson and D. Barker
It is suggested that where specialist midwifery teams exist, problems and conflictbetween staff can manifest. Lack of communication and team involvement can leadto a ‘them and us’ scenario, with general midwives feeling deskilled in the area ofhigh-dependency care. Literature suggests that midwives working in specialist areasneed to develop a cultural awareness of the differences between various healthcareprofessionals and their attributes in order to value the contribution of others posi-tively, with specialist midwives striving at all times to educate staff in high-risk carerather than to deskill them.25 Critical care midwives at JCUH identified this issuethrough the distribution and audit of a staff questionnaire, and tailored staff needsaccordingly following evaluation of the results. Understanding the boundaries andsphere of each others’ practice and the degree of both autonomy and authority thiscreates can alleviate conflict to a great extent. Conflict per se has been describedas neither good nor bad but neutral; rather, it is an individual’s interpretation ofconflict that gives it a negative connotation.26
Conflict is not only present amongst general staff but has the ability to manifestbetween the team itself.26 If a team is supportive regarding the contribution madeby each member, conflict can be channelled as a motivator and stimulator for thedevelopment of concepts within the team. However, teams may develop a demotiva-tion effect amongst staff, with the team relying on certain members within the groupto do the necessary work. By working collectively, communicating, planning anddeveloping with a set and agreed agenda, teams can identify gaps in the service byencouraging cooperative learning, problem solving, evaluation and auditing, andenhancing the service that the team provides to its users.26 The critical care teamat JCUH has a set agenda which is developed in conjunction with analysing patients’needs generated through regular audit of complex cases, reviews of complex casesand recommendations from CEMACH reports which encompass the introductionof evidence-based care.6 This gives midwives working within the critical care teamthe opportunity to keep up to date in profession-specific skills and knowledge, encour-aging cooperative learning in an environment where confidentiality, trust and opennessis assured. Supporting this approach, leading analysts on team development suggestthat teams have a tendency to positively utilize resources to maximum effect.22
One such resource is the development of policies and strategies applicable to criticalcare, which is evidence based and updated regularly by team members. Any new de-velopments in research are presented to the team by members in formal meetings.22
Within a team, there will be both dominant and quiet members, and it is importantthat all members identify this. The role of critical care coordinator at JCUH is under-taken annually on a rotational basis amongst all team members, which encouragesleadership development and equal participation of all team members to join in discus-sion and share ideas. Workload amongst the team is evenly balanced betweenmembers, and discussion is undertaken regularly at meetings regarding the planningand appraisal of what needs to be done, again with duties undertaken on a rotationalbasis, and with each member allocated their equal share.
At JCUH, the critical care team has the benefit of strong leadership and directionfrom an obstetric consultant lead, anaesthetic consultant and delivery suite managerwith an interest in obstetric critical care. This has contributed greatly to the motiva-tion of the team and has assisted in equipping the team to provide the highest possiblestandards of care. The team’s consultant lead provides assistance and guidance onquality, safety and the appropriateness of care; an important contribution to high-dependency care which appears to be nationally supported.11 The consultant rolewithin the team involves the following.
Role of the midwife and the obstetrician in obstetric critical care 907
Development of policies and procedures, which are influenced by regular auditswithin the client group, National Institute for Health and Clinical Excellence guidanceandup-to-date evidence-based research. It has been identified that unambiguous guidelinesandprotocols are an effectivewayof enhancing multidisciplinary care of critically ill women.
Recognition, management and treatment of diseases of pregnancy as a result ofthe above, and dissemination of these amongst the multidisciplinary team includingaccident and emergency departments and general practitioners’ surgeries.
Development of criteria for the admission, discharge and transfer of women tocritical care area on labour ward and ITU areas.
Provision of assistance to critical care midwives with the formation of appropriatedocumentation such as specific obstetric ITU charts, patient information leaflets,discharge proformas to postnatal areas, patient satisfaction questionnaires etc.
Monthly case reviews of women admitted to critical care take place between theconsultant lead, critical care midwives and risk management, which supports therecommendations in accordance with clinical governance and Clinical NegligenceScheme for Trusts (CNST) strategies.
Presentation and review of cases at the monthly multidisciplinary obstetric andgynaecology audit meeting.
Development of an on-call obstetric consultant’s protocol within HDU, whichensures routine review of all critically ill women at periodic intervals.
Management of high-risk women requiring critical care at JCUH is initiated on thecentral delivery suite, where there is a single-bedded high-dependency room whichhas been designed to provide care that is in someway similar to an ITU setting, forinstance haemodynamic monitoring and drug and equipment stock. However, theroom is provided with soft lighting, and equipment is hidden within suitable bedroomfurniture. The room also has the facilities to accommodate partners or family, and thewoman’s need for privacy is advocated at all times, with interruptions from medicalstaff kept to an agreed limit unless clinical condition dictates otherwise. Psychosocialwell-being and the maternal–infant bonding process is a huge concern for midwiveswithin the critical care team. Women requiring high-dependency care quite oftenhave very challenging and unique emotional needs, which always falls within themidwives’ realm of practice. Research indicates that psychological distress in womenduring a crisis period can have lingering effects on the overall family unit, and theseeffects can then manifest and inhibit the family’s ability to incorporate the birth expe-rience positively into their lives, making it difficult to move forward into productiveparenthood. Research undertaken within a special care baby unit identified significantbarriers to the psychosocial well-being of women and the maternal–infant bondingprocess, which can be applied to a mother’s ability to cope and interact with her new-born infant and significant others within a critical care environment. These include27:
� Physical environmentTechnology of monitorsVentilators
� Mechanical barriersAlarmsEquipment
� Psychosocial barriersLack of privacyFeelings of guiltFeelings of helplessness
908 H. Simpson and D. Barker
Shock of event� Nurse barriers
Policies and proceduresTechnology-focused careInadequate staffingEmotions and values of the nurseVisitation policies
The critical care team at JCUH is flexible with regards to visitation for partners, sib-lings and significant family members when clinical conditions allow, and strives to provideaccommodation for partners when required. Breastfeeding is encouraged, assistance isprovided, and a breast pump is supplied when needed. Referral to a breastfeeding keyworker is also facilitated, which is of great benefit if the infant is cared for on the neonatalunit. The neonatal unit is located within close proximity of the central delivery suite, andcommunication between the neonatal unit and a woman requiring critical care is excel-lent. The neonatal unit communicates the status of the infant at all times, providingPolaroid photos when necessary, and facilitates visits to the ill mother when possible.
Upon completion of their stay in critical care, women are transferred to a postnatalarea along with a critical care discharge summary and robust plan of care thatpromotes continuity of care. Members of the team visit the women prior to discharge,and a discharge proforma is completed which affords women the opportunity todiscuss and debrief on the condition which led to their admission, management andtreatment, and their interpretation and understanding of it, obtaining a referral forcounselling when required. A 6-week follow-up appointment is also facilitated withthe woman’s named consultant, and a patient satisfaction survey is sent annually toall patients admitted to critical care which directs improvements in service provision.
This discussion has hopefully identified some of the barriers and skills required todevelop an effective specialist team of midwives practising within high-risk obstetriccare. The aims and objectives should focus upon reducing the risk of patients receivingsuboptimal care, diminish the rates of admission to ITU areas, and ensure that womenand their families remain together. The inclusion in the discussion of a well-establishedteam of specialist midwives at JCUH may serve as a template for maternity units wish-ing to develop this level of service. When developing a team of midwives who special-ize in caring for critically ill patients, there can be a number of successes. Firstly, andmost importantly, is an awareness of the factors which have brought about this recentchange to care in the high-risk obstetric patient group and includes the findings andrecommendations of the CEMACH reports which target a reduction in maternal mor-tality and morbidity. The needs of local client groups, which serve to direct serviceprovision, must also be considered and should include recognition of risk factorsamongst the local population that could result in indirect pathologies. The availabilityof an educational programme, which supports clinical development, is a necessity asmidwives practising without a suitable repertoire of contemporaneous skills mayfind themselves clinically, professionally and contractually at risk. Open levels anddevelopment of interpersonal skills amongst midwives serves to promote effectiveinterdependent working relationships across the various disciplines required to safe-guard care. The importance of working together in a pleasant, supportive environmentand having colleagues to discuss and debrief with regarding patient care are vitallyimportant for staff working within complex situations, as it helps to reduce anxietyand stress whilst sharing knowledge and recent developments in care. It does appearthat critically ill patients are best cared for by a well-educated team of midwives, who
Role of the midwife and the obstetrician in obstetric critical care 909
strive at all times to promote and enhance the quality of care they provide, as caringand treating clients with life-threatening conditions can be beyond the scope of prac-tice for many midwives. The commitment and dedication of an enthusiastic midwiferyteam in high-dependency settings ensures that women and babies remain together,which is vital to the mother–infant relationship.
THE ROLE OF THE OBSTETRICIAN IN OBSTETRIC CRITICAL CARE
Between 0.2% and 1.0% of pregnant women will require critical care during or aftertheir pregnancy. Even in units with over 5000 deliveries per year, less than one womanper week will require critical care. Any published series are small and there is limited, ifany, research available on the role of the obstetrician in critical care. It is difficult for allobstetricians and gynaecologists to have a complete understanding of invasive moni-toring, but equally it is difficult for intensivists to have a complete understanding ofmaternal physiology and pregnancy-specific conditions. It is therefore necessary towork as a team, with each member providing their own area of expertise.
Due to the limited research into the role of the obstetrician in critical care, much ofthis discussion is based on professional opinion and should be used as a template todiscuss and develop the role further. The role can be divided into the following areas:leadership; clinical knowledge and skills; documentation; guideline development; riskmanagement and debrief; audit; and education.
Leadership
Northwick Park Enquiry28 highlighted ‘a lack of clinical leadership, poor relationshipsbetween staff, inadequate cover of consultants who were responsible for overseeingcare on the labour ward’ as key issues involved in the women’s deaths. ‘Consultant ob-stetricians did not routinely carry out ward rounds on the delivery suite and teamworkbetween midwives and obstetricians was not as effective as it should have been’, and thiswas particularly apparent when managing critically ill women. ‘Deficiencies in care in-clude a lack of input from consultants at crucial times. There was too much relianceon junior staff to manage complex and difficult situations with little guidance or support.’
Similarly, the most recent CEMACH report7 found that ‘many women were notseen by an appropriately trained senior or consultant doctor in time, and a few neversaw a consultant doctor at all, despite, in some cases, being in a critical care unit. Thereasons for this were, generally, a lack of awareness of the severity of the woman’sillness by more junior or locum maternity staff, both doctors and midwives. Ina few cases, but in smaller numbers than in previous reports, the consultant(s) didnot attend in person until too late and relied on giving advice over the phone.’
All women in critical care should be reviewed regularly by a consultant obstetrician;an example of a suggested standard is given in Table 1. This should be an auditablestandard of care. At other times, a woman in critical care should be reviewed ona 4-hourly basis by a senior trainee (ST 3 or above).
Ideally, ward rounds should reflect the multidisciplinary team involved in the care,i.e. obstetrician, midwife, anaesthetist (or intensivist) etc. All aspects of care should becovered including physiotherapy, thromboprophylaxis, bereavement counselling if indi-cated, debrief of all the family and more normal midwifery care. A holistic pathway ofcare should be developed. However, it is vital that one person takes the lead and thatcontinuity of care is maintained. If the woman is on ITU, it may be more appropriate
Table 1. Consultant review standard for critical care.
1. There should be a consultant review of all obstetric critical care patients weekdays at 08.30, 13.00
and 17.00 h.
2. A telephone update should be obtained at a minimum at approximately 22.00 h.
3. At the weekend or on bank holidays, a minimum standard of one in person review by a consultant with
telephone updates throughout the day at approximately 13.00, 17.00 and 22.00 h.
4. In the recovery period, it may be appropriate to decrease consultant review to daily.
5. All visits should be clearly documented in the notes by the consultant or a member of the medical
staff, clearly stating that the consultant was present.
6. In the event of deterioration in clinical condition, further care should be discussed with a consultant. If
there is no response to treatment, a personal review by a consultant is indicated.
910 H. Simpson and D. Barker
for the lead to be taken by the intensivist, but when the woman is cared for on thedelivery suite, this role is more likely to be taken by the consultant obstetrician.Continuity of care can be encouraged with the development of guidelines and clearcare planning.
One of the learning points in the midwifery chapter of Saving Mothers’ Lives7 high-lights the problems some midwives faced in either feeling able to refer directly toa consultant or to ask for a second medical opinion. If a midwife remains worriedfollowing a medical opinion, they should have no qualms about contacting relevant se-nior medical personnel directly, such as the obstetric consultant on call. It is vital thatthere are clear lines of communication at all levels; Figure 1 gives a simple example.
Figure 1. Flow chart of communication.
Role of the midwife and the obstetrician in obstetric critical care 911
Clinical knowledge
Although it is vital that all obstetricians and gynaecologists maintain a thorough under-standing of the management of critically ill obstetric women, it may be that one individ-ual needs to take on the main role of developing the service within each unit; this couldbe the labour ward lead. Regular multidisciplinary case discussion of recent cases allowsopen discussion of good and poor aspects of care, allowing learning by experience.
It is vital that all those involved in critical care obstetrics update their knowledge ondevelopments in care on a regular basis. The recent CEMACH7 report highlights thechanges in our population (increasing maternal age, increasing migrant population,increasing twining rate) and the shift in the causes of maternal death, with cardiacdeath now being the leading cause of maternal death (thrombosis continues as theleading cause of direct death).
All those involved with the care of obstetric patients should be aware of thephysiological changes that occur during pregnancy and the puerperieum, and theeffects on the disease processes that are either directly caused or altered by preg-nancy. These are covered in other chapters within this issue.
Appropriate referral and identification of the high-risk woman within each unit andalso across disciplines, and if necessary to other centres, is paramount for the safeassessment and management of the more complicated women. Clear criteria foranaesthetic referral at a relevant point in pregnancy should be developed.
Documentation
In the Northwick Park Enquiry28, some of the cases had poor documentation by themidwifery and obstetric staff, an absence of documentation for surgical procedures bythe obstetric staff, and an absence of contemporaneous documentation. Standards ofclear documentation should be maintained as shown in Table 2. All obstetriciansshould ensure that they maintain these standards.
The standard of documentation within critical care notes should be audited regularly.It is even more important not to use abbreviations when differing specialities areinvolved, as it is all to easy to misinterpret what has been requested. Even simple abbre-viations can lead to confusion: is an FBS a fetal blood sample or a fasting blood sugar?
Accurate clinical information is important in some situations, and the developmentof proformas may be useful. One example in critical care would be eclampsia, which isnow rare but very easily fits into a simple management proforma/aide memoire asillustrated in Figure 2.
Although audits of this particular proforma are not available as the numbers are toosmall, a similar proforma for ventouse delivery has been audited29 prior to (60 cases)
Table 2. Standards of documentation.
- Date and time
- Sign
- Print name and grade
- Write in black
- Legible
- No abbreviations.
912 H. Simpson and D. Barker
and after (140 cases) its introduction, and showed a significant improvement indocumentation.
All notes should be multidisciplinary and contemporaneous. Early warning scorecharts have been discussed elsewhere in this issue, and it is vital that a nationallyacceptable chart is developed. Specific intensive care charts may also be useful.
Clinical guidelines
It is essential that the lead for critical care ensures that there are guidelines available,and that these are reviewed regularly (at least every 3 years). The Royal College of
Procedure: ECLAMPSIA
Date and time of writing……………………….Staff present:
Date of Fit:…………………………… Time of Fit:…………………………. Location of Fit:…………………………………………………………………….
Fit witnessed by:…………………………………………………………………..
Time fit stopped:…………………………………
Second Fit: No Yes Time:……………………………
Initial action
Left lateral: Yes No Airway maintained: Yes No Facial oxygen: Yes NoSuction required: Yes No Gudel airway required: Yes No
CTG commenced: Yes No Time:…………………….
IV access: Yes No
Bloods: FBC LFT’s U&E Urate Clotting Group & Save
Magnesium Sulphate (See guideline A7):Loading dose: Yes No Time:…………………….
(4 g = 40 mL of 10% MgSO4 over 15 min – ideally through syringe driver)
Maintenance dose: Yes No Time:…………………….(1g/h = 50 mL of 10% MgSO4 over 5 h via pump)
2nd
loading dose (after 2nd fit):Yes No Time:………… (2 g = 20 mL of 10% MgSO4)
Labetalol required (see guideline A14): Yes No Time 1st bolus (40 mg):…………………….. Time 2nd bolus (40 mg):…………………….. Time 3rd bolus (80 mg):…………………….. Time 4th bolus (80 mg):……………………..
Infusion: Yes No Time:………………………… Start at 8 mL/h (40 mg), double every 30 min as per protocol to max 32 mL/h (160 mg)
Hydralazine required (see guideline A14): Yes No Time 1st bolus:…………………….. Time 2nd bolus:…………………….. Time 3rd bolus:…………………….. (5 mg bolus, repeat x3 every 15 min until diastolic <100)
Infusion required: Yes No Time:………………………… (40 mg in 40mL N.Saline commence at 10 mL/h, increase every 30 min to max of 40 mL/h, titrate against BP 160/100)
Mode delivery:
Suitable for ARM For caesarean section
Time of transfer to CDS/critical care room:…………………………………
Signature:…………………………………………………………….
Print Name:………………………………………………………….
Figure 2. (Continued)
Role of the midwife and the obstetrician in obstetric critical care 913
Obstetricans and Gynaecologists’ guidelines are available at www.rcog.org.uk on thefollowing subjects:
� eclampsia;� severe pre-eclampsia and eclampsia;� thromboembolic disease; and� the role of emergency and elective interventional radiology in postpartum
haemorrhage.
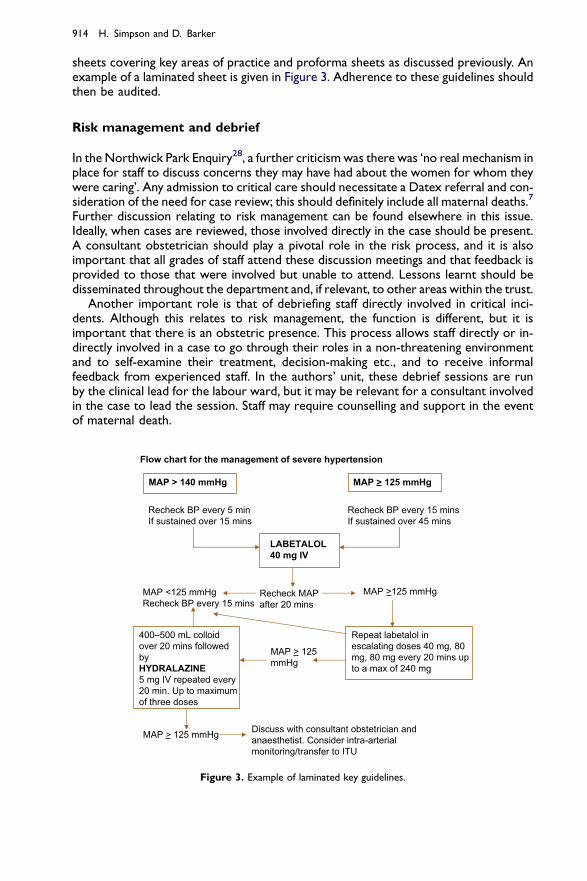
Guidelines should be clear and cover the acute phase and longer term management.They should contain clear instructions on who should be contacted and at what stage.They should be simple to follow with flowcharts where appropriate; it may be worthhaving laminated key sheets readily available. In the authors’ unit, emergency trolleysare set up containing some key drugs, intravenous access (including arterial and longlines), fluids, equipment for intubation etc. On the top of the trolley are laminated
sheets covering key areas of practice and proforma sheets as discussed previously. Anexample of a laminated sheet is given in Figure 3. Adherence to these guidelines shouldthen be audited.
Risk management and debrief
In the Northwick Park Enquiry28, a further criticism was there was ‘no real mechanism inplace for staff to discuss concerns they may have had about the women for whom theywere caring’. Any admission to critical care should necessitate a Datex referral and con-sideration of the need for case review; this should definitely include all maternal deaths.7
Further discussion relating to risk management can be found elsewhere in this issue.Ideally, when cases are reviewed, those involved directly in the case should be present.A consultant obstetrician should play a pivotal role in the risk process, and it is alsoimportant that all grades of staff attend these discussion meetings and that feedback isprovided to those that were involved but unable to attend. Lessons learnt should bedisseminated throughout the department and, if relevant, to other areas within the trust.
Another important role is that of debriefing staff directly involved in critical inci-dents. Although this relates to risk management, the function is different, but it isimportant that there is an obstetric presence. This process allows staff directly or in-directly involved in a case to go through their roles in a non-threatening environmentand to self-examine their treatment, decision-making etc., and to receive informalfeedback from experienced staff. In the authors’ unit, these debrief sessions are runby the clinical lead for the labour ward, but it may be relevant for a consultant involvedin the case to lead the session. Staff may require counselling and support in the eventof maternal death.
Flow chart for the management of severe hypertension
MAP > 140 mmHg MAP > 125 mmHg
Recheck BP every 5 minIf sustained over 15 mins
LABETALOL
40 mg IV
Recheck BP every 15 minsIf sustained over 45 mins
MAP <125 mmHgRecheck BP every 15 mins
Recheck MAPafter 20 mins
MAP >125 mmHg
400–500 mL colloidover 20 mins followedbyHYDRALAZINE
5 mg IV repeated every20 min. Up to maximumof three doses
Repeat labetalol inescalating doses 40 mg, 80mg, 80 mg every 20 mins upto a max of 240 mg
MAP > 125mmHg
MAP > 125 mmHg Discuss with consultant obstetrician andanaesthetist. Consider intra-arterialmonitoring/transfer to ITU
Figure 3. Example of laminated key guidelines.
Role of the midwife and the obstetrician in obstetric critical care 915
Audit
A further important role of the obstetrician is ensuring that all guidelines and manage-ment pathways including documentation are audited regularly. This allows analysis ofguidelines to ensure that they function and allow appropriate management for women.It also allows assessment regarding whether staff are following the guidelines, or mayidentify areas that require changes or updates. Feedback should be in a multidisciplinaryformat allowing open discussion. Standards should be clearly set within the guidelineand audit. Re-audit on a regular cycle is imperative to ensure that any changes producethe appropriate improvement in patient management.
Education
The role of training in critical care is discussed elsewhere in this issue. The continu-ing education of all staff is at the heart of good management and can be achieved inseveral ways. In-house training sessions, regional training programmes and nationalcourses are all useful tools to deliver updated information. On a week-by-weekbasis, regular case review and discussion is often one of the most productiveways of learning.
SUMMARY
In summary, the roles of the midwife and the obstetrician overlap a great deal, anda well-functioning team relies on both working together and liaising with otherdisciplines as and when required – particularly with the anaesthetist. In simpleterms, their roles can be divided into the following areas: leadership; clinical knowl-edge and skills; documentation; guideline development; risk management anddebrief; audit; and education. All of this should enable a holistic approach to thewoman and the family.
Practice points
� set auditable standards of review� consider identifying one consultant to take a lead/interest in critical care� ensure that the roles are clearly defined and include development of guidelines,
documentation, involvement in risk management and audit
Research agenda
� impact of a well-structured critical care team working on the care of pregnant/delivered women and their families� how this role can be developed in smaller units versus the need to centralize
such teams and the issues that this raises
916 H. Simpson and D. Barker
REFERENCES
*1. Lee B. Life threatened by birth: mothers in high dependency obstetric care. RCM Midwives J 2000; 3:
282–285.
2. Lewis G. Why Mothers Die 1997–1999. the fifth report of the confidential enquiry into maternal deaths in the
UK. London: RCOG, 2001.
3. Walton I, Hamilton M & Ashton R. Midwives and changing childbirth. Royal Collage of Midwives, 2004.
4. Royal College of Obstetricians & Gynecologists and Royal College of Midwives. Towards a safer childbirth
– minimum standards for the organization of labour wards. Report of a joint working party. London: RCOG,
1999.
5. Department of Health. The NHS Plan – a Plan for Investment, a Plan for Reform. London: DoH, 2000.
*6. Lewis G. Why Mothers Die 2000–2002. The sixth report of the confidential enquiry into maternal and child
health in the UK. London: RCOG, 2004.
*7. Lewis G. Saving Mothers’ Lives 2003–2005. The seventh report of the confidential enquiry into maternal and
child health in the UK. London: RCOG, 2007.
*8. Bench S. Recognition and management of critical illness by midwives: implications for service provision.
J Nurs Manag 2007; 15: 348–356.
9. Dimond B. The midwife and her caseload: the legal issues. BMJ 1999; 7: 141–143.
10. Naylor D & Olson M. Critical care obstetrics and gynecology. Crit Care Clin 2003; 19: 127–149.
*11. Zeeman G, Wendal G & Cunningham F. A blueprint for obstetric care. Am J Obstetr Gynecol 2003; 188:
532–536.
12. Nursing & Midwifery Council. The NMC code of professional conduct: standards for conduct, performance
and ethics. NMC, 2004.
13. Nursing & Midwifery Council. The PREP handbook. NMC, 2004.