16
Royal Columbian Hospital Intensive Care Unit Delirium Quality Improvement Initiative Breakout session #G8 Sandy White, RN BSN Sharon Hickin, RN BSc, CNCC(C)
| Date post: | 17-Feb-2017 |
| Category: |
Healthcare |
| Upload: | bcpsqc |
| View: | 291 times |
| Download: | 0 times |

Royal Columbian Hospital Intensive Care Unit Delirium Quality
Improvement Initiative
Breakout session #G8 Sandy White, RN BSN Sharon Hickin, RN BSc, CNCC(C)
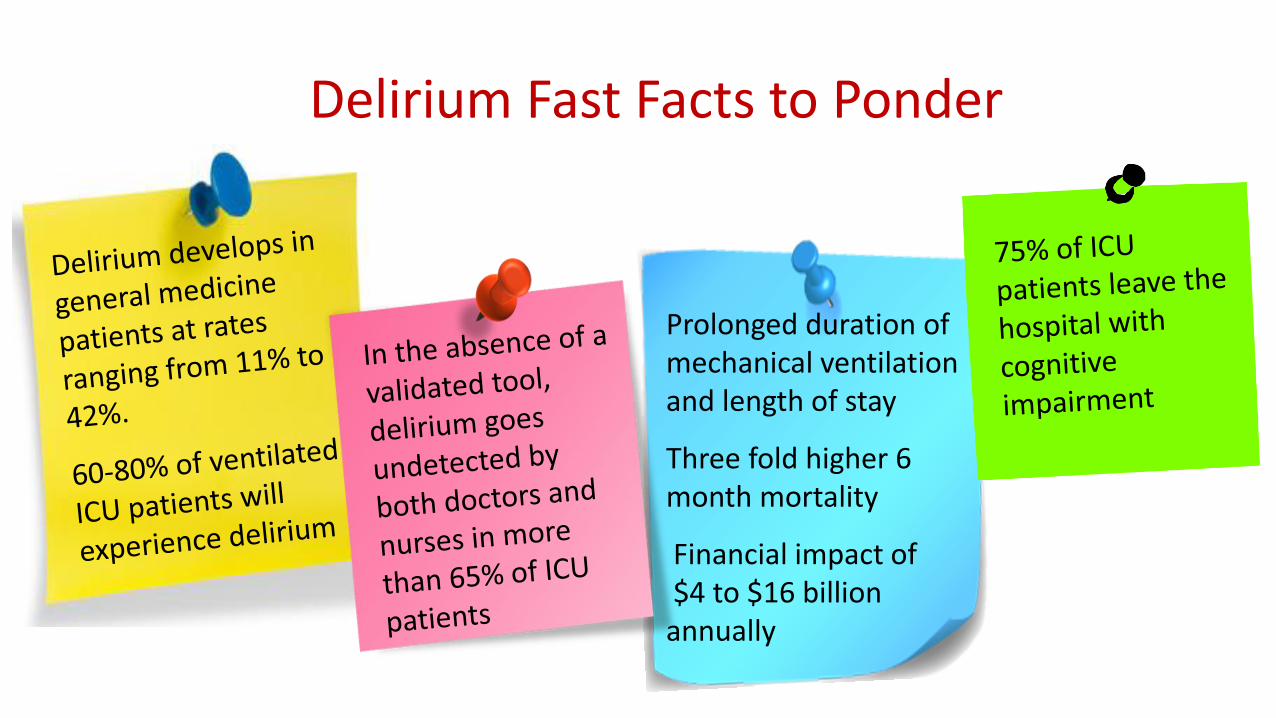
Prolonged duration of mechanical ventilation and length of stay
Three fold higher 6 month mortality
Financial impact of $4 to $16 billion annually
Delirium Fast Facts to Ponder

“Is a syndrome characterized by the acute onset of cerebral dysfunction with a change or fluctuation in baseline mental status, inattention, and either disorganized thinking or an altered level of consciousness”(Barr et al. 2013, p282)
Whatever the cause, delirium is an ACUTE and WIDE-SPREAD BRAIN DYSFUNCTION
Delirium

Pain, Agitation, Delirium (PAD) Why Care?
Understanding the impact that delirium can have on hospitalized patients makes prevention and optimal treatment
of this organ dysfunction a priority

Our Mission:
To develop a cohesive interdisciplinary delirium mitigation strategy aimed at improving patient
outcomes.

Analyzing Assumptions
1. Everyone understood delirium and the impact it had on patient outcomes
2. Delirium management relied primarily on pharmacological interventions
3. Providing education would help ICU staff recognise the significance of delirium and thus lead to a change in practice
The Starting Point: Needs Assessment of Delirium
Created ICU Delirium Working Team
Explore current research and gold standards of practices
Review current RCH ICU delirium management and gaps in practice
Assess/measure baseline knowledge of ICU RNs
Dual-pronged Approach
Multifaceted Education Roll-out
Development of discipline specific Clinical Practice Guidelines (CPG) for non-pharmacological aspects of delirium management

Team Rounds: Communication is Key in Delirium Management
Differentiate Analgesic versus
Sedation
Use Objective Language
Report & discuss Pain, Agitation & Delirium using Validated Scoring
Tools

Sleep Habits
Date: RN: RT: Physio: Doctor:
Understanding Delirium Brings Change in Culture
Pet Therapy
Family Engagement
Routines
Early Mobility
ICU Nursing Kardex

Spring 2012- Fall 2013:
• Whiteboards in rooms
• Family journals
• Ear plugs at bedside
• Encourage sensory aids
• Using proper language
• Delirium added to rounds
checklist
Spring 2012: Delirium
Management Working Group
formed
Dec 2012: First draft of
Interdisciplinary CPG
Baseline
Assessment
October 2013: Nursing
Education Roll Out
Follow-Up
Assessment
May 2014: Regional CC
Ed Days
Winter Surge Winter Surge
Sustained Education Gap Analysis Engagement
Family Empowerment
December 2014
Program team
approval of CPG
Winter 2014/ Spring 2015
• Brain Cards
• Quiet signs
• Quick ref for Doctors
• Ed Roll Out CPG/PAD
Long-term
Follow-Up
Education Matters Most

• Engagement: Delirium champions, families • Sustained Education: Incorporate into unit
orientation for all disciplines including students and residents
• Interdisciplinary Delirium QI Team: New
initiative to examine rates of delirium within unit • Leadership: Commitment to action plan Health
Authority wide
What Lies Ahead

Self Preservation… Understanding the Impact of Delirium

Take-Away Delirium Fast Facts
34% experience cognitive impairment similar in severity to patients with moderate traumatic brain injury
Pandharipande PP, et al. N Engl J Med. 2013 Oct 3;369(14):1306-16

References Barr, J., Fraser, J., Puntillo, K., Ely, E., Gélinas, C., Dasta, J., . . . Jaeschke, R. (2013). Clinical practice guidelines for the management of pain, agitation, and delirium in
adult patients in the intensive care unit. Critical Care Medicine, 41(1), 263-306. doi:10.1097/CCM.0b013e3182783b72
Bergeron, N., Dubois, M.-J., Dumont, M., Dial, S., & Skrobik, Y. (2001). Intensive care delirium screening checklist: evaluation of a new screening tool. Intensive
Care Medicine, 27, 859-864. doi:10.1007/s001340100909
Brummel, N., Vasilevskis, E., Han, J., Boehm, L., Pun, B., & Ely, E. (2013). Implementing delirium screening in the ICU: Secrets to success. Critical Care Medicine,
41(9), 2196-2208. doi:10.1097/CCM.0b013e31829a6f1e
Carolinas Medical Center. (2008). Evaluation of delirium in critically ill patients at Carolinas Healthcare System: Nursing education.
Devlin, J., Brummel, N., & Al-Qadheeb, N. (2012). Optimising the recognition of delirium in the intensive care unit. Best Practice & Research Clinical
Anaesthesiology, 26, 385-393. doi:10.1016/j.bpa.2012.08.002
Ely, E., Siegel, M., & Inouye, S. (2001). Delirium in the intensive care unit: An under-recognized syndrome of organ dysfunction. Seminars in Respiratory and Critical
Care Medicine, 22(2), 115-126.
Gesin, G. R. (2012). Impact of a delirium screening tool and multifaceted education on nurses’ knowledge of delirium and ability to evaluate it correctly. American
Journal of Critical Care, 21(1), e1-e11. doi:10.4037/ajcc2012605
Girard TD, Jackson JC, Pandharipande PP, et al. Delirium as a predictor of long-term cognitive impairment in survivors of critical illness. Crit Care Med.
2010;38(7):1513-1520.
Law, T., Leistikow, N., Hoofring, L., Krumm, S., Neufeld, K., & Needham, D. (2012). A survey of nurses' perceptions of the intensive care delirium screening checklist.
Dynamics, 23(4), 18-24.
Macfarlane, K. (2012, Feb). The wakeful brain: Analgesia, sedation & delirium.
Pandharipande PP1, Girard TD, Jackson JC, Morandi A, Thompson JL, Pun BT, Brummel NE, Hughes CG, Vasilevskis EE, Shintani AK, Moons KG, Geevarghese SK,
Canonico A, Hopkins RO, Bernard GR, Dittus RS, Ely EW; BRAIN-ICU Study Investigators. (2013, Oct) N Engl J Med; 369(14):1306-16. doi:
10.1056/NEJMoa1301372.Long-term cognitive impairment after critical illness.
Pun, B., & Ely, E. (2007). The importance of diagnosing and managing ICU delirium. Chest, 132, 624-636. doi:10.1378/chest.06-1795
Pun, B., Gordon, S., Peterson, J., Shintani, A., Jackson, J., Bernard, G., . . . Ely, E. (2005). Large-scale implementation of sedation and delirium monitoring in the
intensive care medical centers. Critical care Medicine, 33(6), 1199-1205. doi:10.1097/01.CCM.0000166867.78320.AC

















