299 pulling the fingers towards the radial side, all together or separately. The condition was distinctly bilateral, being more marked in the right hand. Complete correction was not possible even under ansisthesia, during which the dragging on the palmar fascia was more marked. In spite of the application of splints and vigorous treat- ment by massage and electricity, no change, except perhaps for the worse, was noticed for over three months. The essential question was whether the case was organic or functional. In favour of functional origin were the circumstances leading up to it; no history of a definite injury to the hands; loss of memory by patient once, soon after admission. Finally, the unusual and symmetrical deformity of hands FIG, 1.-Condition of hands on admission August, 1917. (Maximum extension.) Note marked ulnar deflection. had led several surgeons to support its functional nature. On the other hand, there was a complete absence of the usual concomitants of functional disorders, such as sensory disturbances, wasting of muscles (except in the face), and it was evident that the voluntary efforts were genuine. The symmetrical disposition is known in cases of hallux valgus, hammer-toe, and camptodactylia has been described amongst organic disorders. Yet there was no hypothermia nor acrocyanosis to indicate trophic disturbances. The sole disorder known to be associated with the palmar fascia resulting in a contracture of the fingers was first described by Baron Dupuytren. This, however, results in a more or less complete flexion of the digits, mostly of the ring finger, without lateral deflection. Why the process of shortening should have in our case chosen just the ulnar fascicles and be symmetrical is difficult to answer. Perhaps the slight arthritic affection determined the course to a certain extent ; for the appearance at the height of the FiG. 2.-Condition of hands in July, 1918. (Maximum extension.) Note absence of ulnar deflection. Two crucial scars in the left and three in the right palm can be seen in relation to and above the lower palmar crease. contracture was not unlike the deformity met with in advanced arthritis deformans. The interdigital folds (webs) were very marked. Whatever the origin, the deformity must have resulted from a progressive fibrosis of the ulnar portions of the palmar fascia. The finer anatomical studies of the fascia reveal its intimate relations with the skin of the palm, with which it is connected by perpendicular fibres of great firmness. Operation was resorted to in November, 1917. Under general anaesthesia I put the affected portion of the palmar fascia of the left hand on the stretch by reducing the ulnar deflection. A fine scalpel was introduced, first parallel to the fine prominent cord on the ulnar aspect and then at right angles to the original incision, severing the strings. At once the fingers could be easily straightened out and the deflection undone. The bleeding was (compara- tively) not inconsiderable, despite care to avoid vessels and nerves. Dressing was applied and a specially constructed splint firmly tied on. Massage was resumed directly the incisions were lightly united. The result was very good. After a few months I attacked the right hand. Both hands can now be used freely, without even a suggestion of ulnar deflection. The splint is still worn at night on the right hand. The grip is steadily improving and there is not the slightest sign of relapse. It took exactly 12 months to cure the case. This case reminds one strongly of the type of reflex nervous disorders described by Babinski and Froment, though I could not find anything resembling it amongst their pictures. Also, according to them such a contracture should be easily undone in deep anaesthesia. In conclusion, I wish to express my thanks to Lieutenant-Colonel Sir Nestor Tirard, Commanding Officer of the 4th London General Hospital, for his permission to publish the case. I am also much indebted to Captain E. B. Clayton for his untiring efforts in the massage depart- ment, and to Miss Berry for the execution of an ingenious splint. St. John’s Wood, -B,W. Medical Societies. ROYAL SOCIETY OF MEDICINE. SECTION OF OPHTHALMOLOGY. A :&bgr;IEETING of this section was held on Feb. 5th, Mr. W. T. Hor.ntES SPICER, the President, being in the chair. Retiraol, Degenendion.-Ivo’l’Y Exostosis of Orbit. Mr. A. C. HUDSON exhibited a case of Retinal Degenera- tion following Intraocular Foreign Body. The ophthalmo- scopic picture was that of folds in the internal limiting membrane of the retina, probably resulting from contusion of the eye. There were double contour reflex lines radiating from the macular region and having certain peculiarities, one of them being that they passed in front of certain of the retinal vessels and another that they were faintly stippled. He regarded the condition as pathological: there appeared to have been cejema of the whole retina and optic disc. Similar appearances have been seen by the exhibitor in a case of retinitis pigmentosa, resulting, in that patient, from traction on the retina. The lines were analogous to those seen in some posterior capsules after cataract extraction.- Mr. J. H. FISHER thought the history and appearance sug- gested that the lines were caused by some new formation, probably in the fundus oculi.-Mr. A. W. ORMOND considered that the amount of swelling was much greater in the upper than in the lower part of the disc and that it was patho- logical. Mr. W. LAXG and Colonel DONALD ARMOUR, exhibited a youth from whom an Ivory Exostosis of the Orbit had been removed by Colonel Armour through the cranium. The patient attended at the Royal London Ophthalmic Hospital, where the members of the staff agreed it was a case for a general surgeon. Colonel Armour did the operation of removal. His problem was to remove the growth completely without doing damage to the cranial or orbital contents, and to leave as little facial disfigurement as possible. The skiagram led to his decision to use an osteoplastic flap turned over the frontal region, with its base at the supra-orbital margin, turning down bone and scalp together. That displayed the cranial portion of the tumour, which was found to be indenting the under surface of the frontal lobe. By pushing the dura and brain gently back over the summit of the tumour, be was able to see the whole extent of its cranial portion. Removal was effected in the main by means of hammer and chisel, the small portion of the orbital roof being attacked with cutting forceps. The recovery was practically uninterrupted and complete ; there was very little external to indicate that an operation had been carried out. The growth must, he said, have originated in the frontal sinus, judging by the fact that the lower portion of the tumour was covered with mucous
Transcript
299
pulling the fingers towards the radial side, all together orseparately. The condition was distinctly bilateral, beingmore marked in the right hand. Complete correction wasnot possible even under ansisthesia, during which thedragging on the palmar fascia was more marked.In spite of the application of splints and vigorous treat-
ment by massage and electricity, no change, except perhapsfor the worse, was noticed for over three months.The essential question was whether the case was organic
or functional.In favour of functional origin were the circumstances
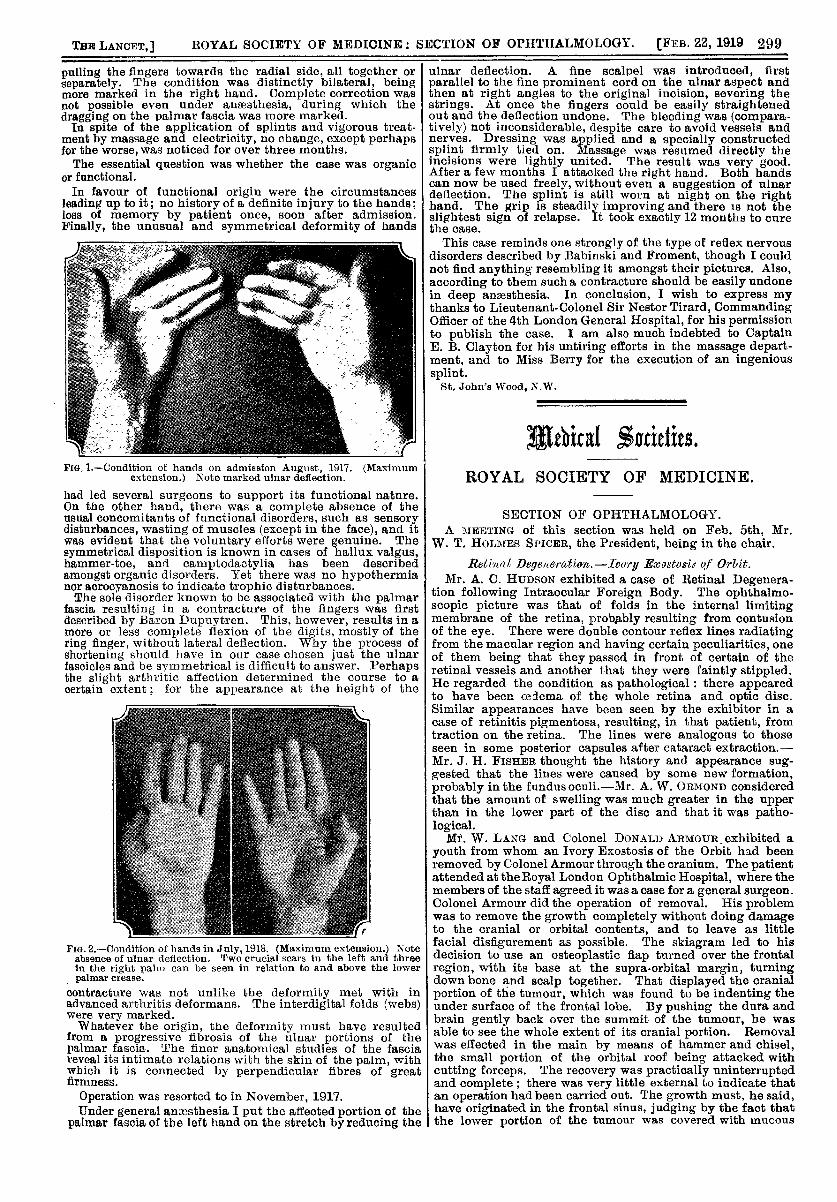
leading up to it; no history of a definite injury to the hands;loss of memory by patient once, soon after admission.Finally, the unusual and symmetrical deformity of hands
FIG, 1.-Condition of hands on admission August, 1917. (Maximumextension.) Note marked ulnar deflection.
had led several surgeons to support its functional nature.On the other hand, there was a complete absence of theusual concomitants of functional disorders, such as sensorydisturbances, wasting of muscles (except in the face), and itwas evident that the voluntary efforts were genuine. Thesymmetrical disposition is known in cases of hallux valgus,hammer-toe, and camptodactylia has been describedamongst organic disorders. Yet there was no hypothermianor acrocyanosis to indicate trophic disturbances.The sole disorder known to be associated with the palmar
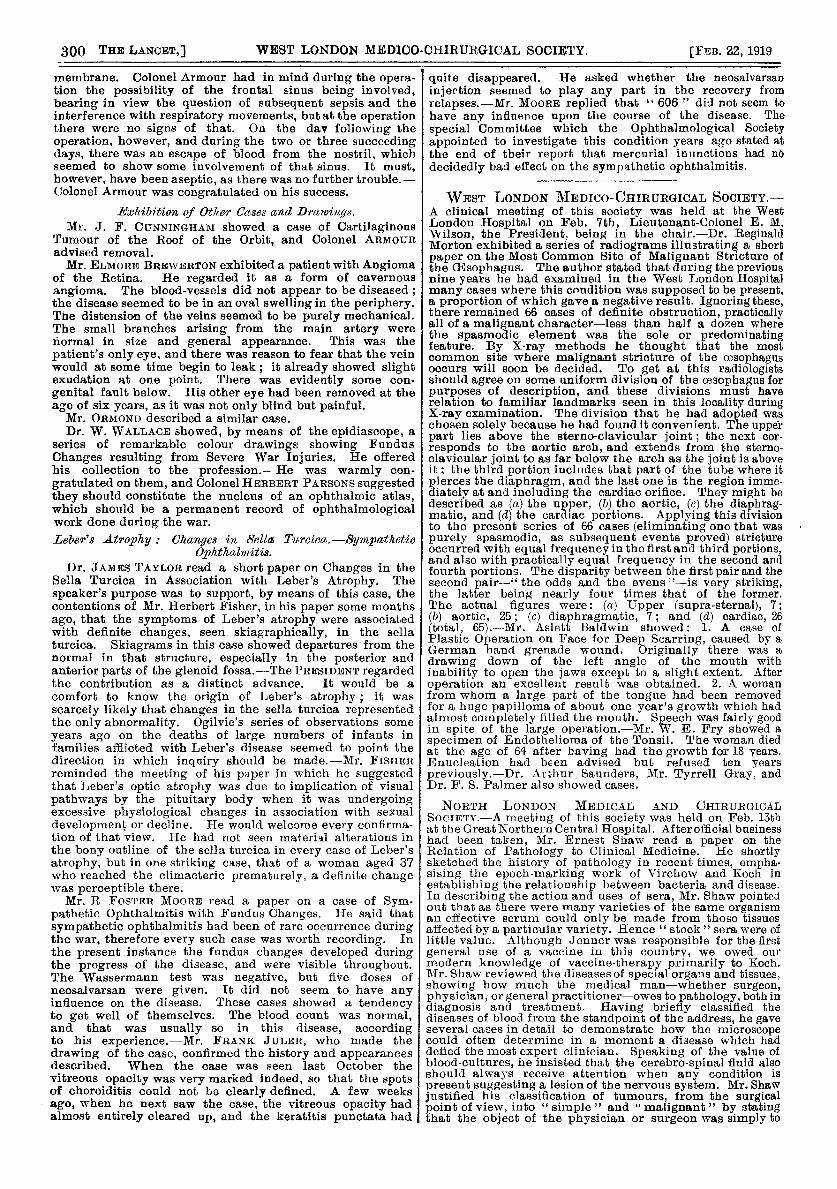
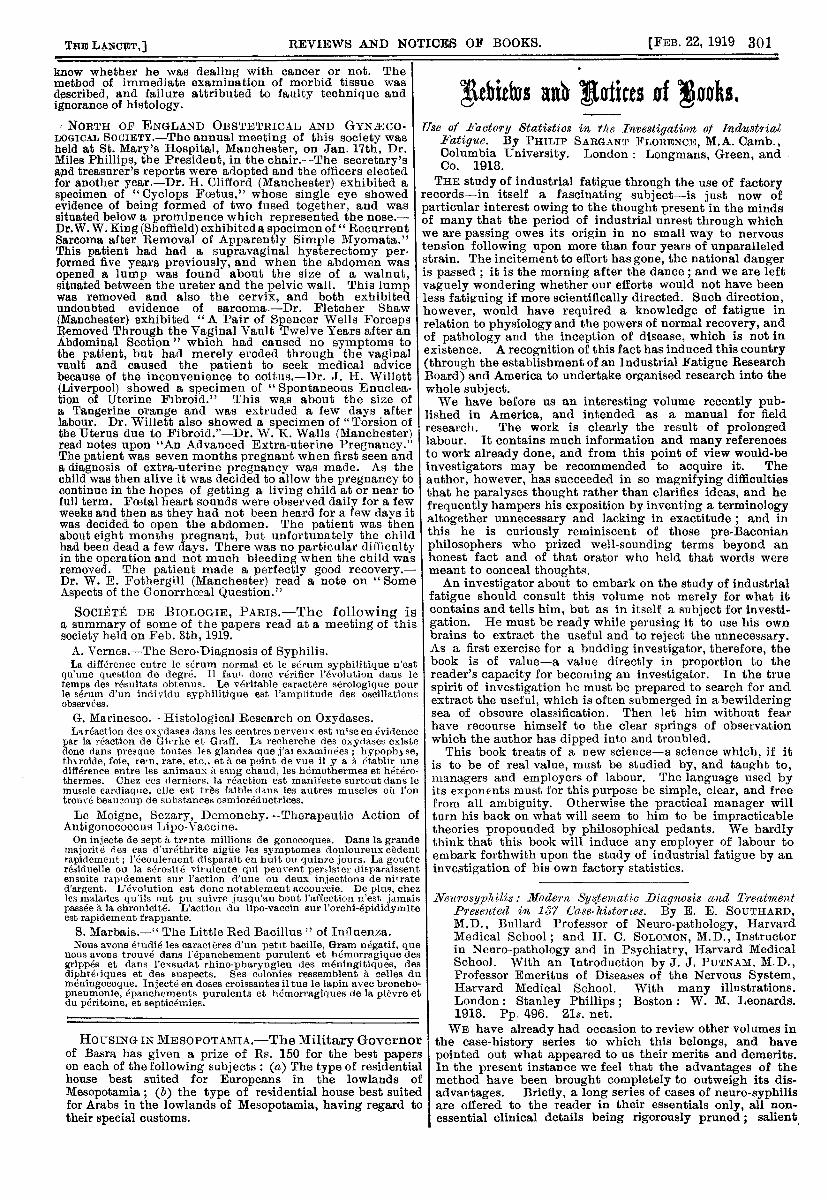
fascia resulting in a contracture of the fingers was firstdescribed by Baron Dupuytren. This, however, results in amore or less complete flexion of the digits, mostly of thering finger, without lateral deflection. Why the process ofshortening should have in our case chosen just the ulnarfascicles and be symmetrical is difficult to answer. Perhapsthe slight arthritic affection determined the course to acertain extent ; for the appearance at the height of the
FiG. 2.-Condition of hands in July, 1918. (Maximum extension.) Noteabsence of ulnar deflection. Two crucial scars in the left and threein the right palm can be seen in relation to and above the lowerpalmar crease.
contracture was not unlike the deformity met with inadvanced arthritis deformans. The interdigital folds (webs)were very marked.Whatever the origin, the deformity must have resulted
from a progressive fibrosis of the ulnar portions of thepalmar fascia. The finer anatomical studies of the fasciareveal its intimate relations with the skin of the palm, withwhich it is connected by perpendicular fibres of greatfirmness.
Operation was resorted to in November, 1917.Under general anaesthesia I put the affected portion of the
palmar fascia of the left hand on the stretch by reducing the
ulnar deflection. A fine scalpel was introduced, firstparallel to the fine prominent cord on the ulnar aspect andthen at right angles to the original incision, severing thestrings. At once the fingers could be easily straightenedout and the deflection undone. The bleeding was (compara-tively) not inconsiderable, despite care to avoid vessels andnerves. Dressing was applied and a specially constructedsplint firmly tied on. Massage was resumed directly theincisions were lightly united. The result was very good.After a few months I attacked the right hand. Both handscan now be used freely, without even a suggestion of ulnardeflection. The splint is still worn at night on the righthand. The grip is steadily improving and there is not theslightest sign of relapse. It took exactly 12 months to curethe case.
This case reminds one strongly of the type of reflex nervousdisorders described by Babinski and Froment, though I couldnot find anything resembling it amongst their pictures. Also,according to them such a contracture should be easily undonein deep anaesthesia. In conclusion, I wish to express mythanks to Lieutenant-Colonel Sir Nestor Tirard, CommandingOfficer of the 4th London General Hospital, for his permissionto publish the case. I am also much indebted to CaptainE. B. Clayton for his untiring efforts in the massage depart-ment, and to Miss Berry for the execution of an ingenioussplint.
St. John’s Wood, -B,W.
Medical Societies.ROYAL SOCIETY OF MEDICINE.
SECTION OF OPHTHALMOLOGY.A :&bgr;IEETING of this section was held on Feb. 5th, Mr.
W. T. Hor.ntES SPICER, the President, being in the chair.
Retiraol, Degenendion.-Ivo’l’Y Exostosis of Orbit.Mr. A. C. HUDSON exhibited a case of Retinal Degenera-
tion following Intraocular Foreign Body. The ophthalmo-scopic picture was that of folds in the internal limitingmembrane of the retina, probably resulting from contusionof the eye. There were double contour reflex lines radiatingfrom the macular region and having certain peculiarities, oneof them being that they passed in front of certain of theretinal vessels and another that they were faintly stippled.He regarded the condition as pathological: there appearedto have been cejema of the whole retina and optic disc.Similar appearances have been seen by the exhibitor in acase of retinitis pigmentosa, resulting, in that patient, fromtraction on the retina. The lines were analogous to thoseseen in some posterior capsules after cataract extraction.-Mr. J. H. FISHER thought the history and appearance sug-gested that the lines were caused by some new formation,probably in the fundus oculi.-Mr. A. W. ORMOND consideredthat the amount of swelling was much greater in the upperthan in the lower part of the disc and that it was patho-logical.
Mr. W. LAXG and Colonel DONALD ARMOUR, exhibited ayouth from whom an Ivory Exostosis of the Orbit had beenremoved by Colonel Armour through the cranium. The patientattended at the Royal London Ophthalmic Hospital, where themembers of the staff agreed it was a case for a general surgeon.Colonel Armour did the operation of removal. His problemwas to remove the growth completely without doing damageto the cranial or orbital contents, and to leave as littlefacial disfigurement as possible. The skiagram led to hisdecision to use an osteoplastic flap turned over the frontalregion, with its base at the supra-orbital margin, turningdown bone and scalp together. That displayed the cranialportion of the tumour, which was found to be indenting theunder surface of the frontal lobe. By pushing the dura andbrain gently back over the summit of the tumour, be wasable to see the whole extent of its cranial portion. Removalwas effected in the main by means of hammer and chisel,the small portion of the orbital roof being attacked withcutting forceps. The recovery was practically uninterruptedand complete ; there was very little external to indicate thatan operation had been carried out. The growth must, he said,have originated in the frontal sinus, judging by the fact thatthe lower portion of the tumour was covered with mucous
300
membrane. Colonel Armour had in mind during the opera-tion the possibility of the frontal sinus being involved,bearing in view the question of subsequent sepsis and theinterference with respiratory movements, but at the operationthere were no signs of that. On the day following theoperation, however, and during the two or three succeedingdays, there was an escape of blood from the nostril, whichseemed to show some involvement of that sinus. It must,however, have been aseptic, as there was no further trouble.-Colonel Armour was congratulated on his success.
L’xhibition of Other Cases and D]’{twings.Mr. J. F. CUNNINGHAM showed a case of Cartilaginous
Tumour of the Roof of the Orbit, and Colonel ARMOURadvised removal.Mr. ELMORE BREWERTON exhibited a patient with Angioma
of the Retina. He regarded it as a form of cavernous
angioma. The blood-vessels did not appear to be diseased ;the disease seemed to be in an oval swelling in the periphery.The distension of the veins seemed to be purely mechanical.The small branches arising from the main artery werenormal in size and general appearance. This was the
patient’s only eye, and there was reason to fear that the veinwould at some time begin to leak ; it already showed slightexudation at one point. There was evidently some con-genital fault below. His other eye had been removed at theage of six years, as it was not only blind but painful.
Mr. ORMOND described a similar case.Dr. W. WALLACE showed, by means of the epidiascope, a
series of remarkable colour drawings showing FundusChanges resulting from Severe War Injuries. He offeredhis collection to the profession.- He was warmly con-gratulated on them, and Colonel HERBERT PARSONS suggestedthey should constitute the nucleus of an ophthalmic atlas,which should be a permanent record of ophthalmologicalwork done during the war.Leber’s Atrophy: : Changes in &lla Ticreiec.-Sympathetio
6/MKM.Dr. JAMES TAYLOR read a short paper on Changes in the
Sella Turcica in Association with Leber’s Atrophy. The
speaker’s purpose was to support, by means of this case, thecontentions of Mr. Herbert Fisher, in his paper some monthsago, that the symptoms of Leber’s atrophy were associatedwith definite changes, seen skiagraphically, in the sellaturcica. Skiagrams in this case showed departures from thenormal in that structure, especially in the posterior andanterior parts of the glenoid fossa.-The PRESIDENT regardedthe contribution as a distinct advance. It would be acomfort to know the origin of Leber’s atrophy ; it was
scarcely likely that changes in the sella turcica representedthe only abnormality. Ogilvie’s series of observations some
years ago on the deaths of large numbers of infants infamilies afflicted with Leber’s disease seemed to point thedirection in which inquiry should be made.-Mr. FISHERreminded the meeting of his paper in which he suggestedthat Leber’s optic atrophy was due to implica,tion of visualpathways by the pituitary body when it was undergoingexcessive physiological changes in association with sexualdevelopment or decline. He would welcome every confirma-tion of that view. He had not seen material alterations inthe bony outline of the sella turcica in every case of Leber’satrophy, but in one striking case, that of a woman aged 37who reached the climacteric prematurely, a definite changewas perceptible there.
Mr. R FOSTER MooRE read a paper on a case of Sym-pathetic Ophthalmitis with Fundus Changes. He said that
sympathetic ophthalmitis had been of rare occurrence duringthe war, therefore every such case was worth recording. Inthe present instance the fundus changes developed duringthe progress of the disease, and were visible throughout.The Wassermann test was negative, but five doses ofneosalvarsan were given. It did not seem to have anyinfluence on the disease. These cases showed a tendencyto get well of themselves. The blood count was normal,and that was usually so in this disease, accordingto his experience.-Mr. FRANK JULER, who made thedrawing of the case, confirmed the history and appearancesdescribed. When the case was seen last October thevitreous opacity was very marked indeed, so that the spotsof choroiditis could not be clearly defined. A few weeks
Iago, when he next saw the case, the vitreous opacity hadalmost entirely cleared up, and the keratitis punctata had
quite disappeared. He asked whether the neosalvarsan
injection seemed to play any part in the recovery from
relapses.-Mr. MOORE replied that " 606 " did not seem to
have any influence upon the course of the disease. The
special Committee which the Ophthalmological Societyappointed to investigate this condition years ago stated atthe end of their report that mercurial inunctions had nodecidedly bad effect on the sympathetic ophthalmitis.
WEST LONDON MEDICO-CHIRURGICAL SOCIETY.-A clinical meeting of this society was held at the WestLondon Hospital on Feb. 7th, Lieutenant-Colonel E. M.B’ilson, the President, being in the chair.-Dr. ReginaldMorton exhibited a series of radiograms illustrating a shortpaper on the Most Common Site of Malignant Stricture ofthe (Esophagus. The author stated that during the previousnine years he had examined in the West London Hospitalmany cases where this condition was supposed to be present,a proportion of which gave a negative result. Ignoring these,there remained 66 cases of definite obstruction, practicallyall of a malignant character-less than half a dozen wherethe spasmodic element was the sole or predominatingfeature. By X-ray methods he thought that the mostcommon site where malignant stricture of the oesophagusoccurs will soon be decided. To get at this radiologistsshould agree on some uniform division of the oesophagus forpurposes of description, and these divisions must haverelation to familiar landmarks seen in this locality duringX-ray examination. The division that he had adopted waschosen solely because he had found it convenient. The upperpart lies above the sterno-clavicular joint; the next cor-
responds to the aortic arch, and extends from the sterno-clavicular joint to as far below the arch as the joint is aboveit ; the third portion includes that part of the tube where itpierces the diaphragm, and the last one is the region imme-diately at and including the cardiac orifice. They might bedescribed as (a) the upper, (b) the aortic, (c) the diaphrag-matic, and (d) the cardiac portions. Applying this divisionto the present series of 66 cases (eliminating one that waspurely spasmodic, as subsequent events proved) strictureoccurred with equal frequency in the first and third portions,and also with practically equal frequency in the second andfourth portions. The disparity between the first pair and thesecond pair-" the odds and the evens "-is very striking,the latter being nearly four times that of the former.The actual figures were: (a) Upper (supra-sternal), 7;(b) aortic, 25; (c) diaphragmatic, 7; and (d) cardiac, 26(total, 65).--Mr. Aslett Baldwin showed: 1. A case ofPlastic Operation on Face for Deep Scarring, caused by aGerman hand grenade wound. Originally there was a
drawing down of the left angle of the mouth withinability to open the jaws except to a slight extent. Afteroperation an excellent result was obtained. 2. A womanfrom whom a large part of the tongue had been removedfor a huge papilloma of about one year’s growth which hadalmost completely filled the mouth. Speech was fairly goodin spite of the large operation.-Mr. W. E. Fry showed aspecimen of Endothelioma of the Tonsil. The woman diedat the age of 64 after having had the growth for 18 years.Enucleation had been advised but refused ten yearspreviously.-Dr. Arthur Saunders, Mr. Tyrrell Gray, andDr. F. S. Palmer also showed cases.
NORTH LONDON MEDICAL AND CHIRURGICALSOCIETY.-A meeting of this society was held on Feb. 13that the Great Northern Central Hospital. After official businesshad been taken, Mr. Ernest Shaw read a paper on theRelation of Pathology to Clinical Medicine. He shortlysketched the history of pathology in recent times, empha-sising the epoch-marking work of Virchow and Koch inestablishing the relationship between bacteria and disease.In describing the action and uses of sera, Mr. Shaw pointedout that as there were many varieties of the same organisman effective serum could only be made from those tissuesaffected by a particular variety. Hence " stock " sera were oflittle value. Although Jenner was responsible for the firstgeneral use of a vaccine in this country, we owed ourmodern knowledge of vaccine-therapy primarily to Koch.Mr. Shaw reviewed the diseases of special organs and tissues,showing how much the medical man-whether surgeon,physician, or general practitioner-owes to pathology, both indiagnosis and treatment. Having briefly classified thediseases of blood from the standpoint of the address, he gaveseveral cases in detail to demonstrate how the microscopecould often determine in a moment a disease which haddefied the most expert clinician. Speaking of the value ofblood-cultures, he insisted that the cerebro-spinal fluid alsoshould always receive attention when any condition ispresent suggesting a lesion of the nervous system. Mr. Shawjustified his classification of tumours, from the surgicalpoint of view, into simple" and malignant" by statingthat the object of the physician or surgeon was simply to
301
know whether he was dealing with cancer or not. Themethod of immediate examination of morbid tissue wasdescribed, and failure attributed to faulty technique andignorance of histology.
, NORTH OF ENGLAND OBSTETRICAL AND GYNFCO-LOGICAL SOCIETY.-The annual meeting of this society washeld at St. Mary’s Hospital, Manchester, on Jan. 17th, Dr.Miles Phillips, the President, in the chair.-The secretary’sapd treasurer’s reports were adopted and the officers electedfor another year.-Dr. H. Clifford (Manchester) exhibited aspecimen of "Cyclops Foetus," whose single eye showedevidence of being formed of two fused together, and wassituated below a prominence which represented the nose.-Dr. W. W. King (Sheffield) exhibited a specimen of " RecurrentSarcoma after Removal of Apparently Simple Myomata."This patient had had a supravaginal hysterectomy per-formed five years previously, and when the abdomen wasopened a lump was found about the size of a walnut,situated between the ureter and the pelvic wall. This lumpwas removed and also the cervix, and both exhibitedundoubted evidence of sarcoma.-Dr. Fletcher Shaw(Manchester) exhibited "A Pair of Spencer Wells ForcepsRemoved Through the Vaginal Vault Twelve Years after anAbdominal Section" which had caused no symptoms tothe patient, but had merely eroded through the vaginalvault and caused the patient to seek medical advicebecause of the inconvenience to coitus.-Dr. J. H. Willett(Liverpool) showed a specimen of " Spontaneous Enuclea-tion of Uterine Fibroid." This was about the size ofa Tangerine orange and was extruded a few days afterlabour. Dr. Willett also showed a specimen of " Torsion of Ithe Uterus due to Fibroid."-Dr. W. K. Walls (Manchester)read notes upon "An Advanced Extra-uterine Pregnancy."The patient was seven months pregnant when first seen anda diagnosis of extra-uterine pregnancy was made. As thechild was then alive it was decided to allow the pregnancy tocontinue in the hopes of getting a living child at or near tofull term. Foetal heart sounds were observed daily for a fewweeks and then as they had not been heard for a few days itwas decided to open the abdomen. The patient was thenabout eight months pregnant, but unfortunately the childhad been dead a few days. There was no particular difficultyin the operation and not much bleeding when the child wasremoved. The patient made a perfectly good recovery.-Dr. W. E. Fothergill (Manchester) read a note on " SomeAspects of the Gonorrhoeal Question."SOCIBTE DE BIOLOGIE, PARIS.-The following is
a summary of some of the papers read at a meeting of thissociety held on Feb. 8th, 1919.A. Vernes.-The Sero-Diagnosis of Syphilis.La difference entre le serum normal et le serum syphilitique n’est
qu’une question de degre. 11 faut, done vérifier revolution dans letemps des r6sultats obtenus. Le veritable caractère sérologique pourle serum d’un individu syphilitique est 1’amplitude des oscillationsobservees.
G. Marinesco.-Histoloical Research on Oxvdases.Lt reaction des oxydases dans les centres nerveux est miseen evidence
par la reaction de Gierke et Graff. La recherche des oxydases existedone dans presque tontes les glandes que j’ai examinees ; hypoph3, se,throide, foie, re-n. rate, etc., et à ce point de vue il y a a 6tablir unedifference entre les animaux à sang chaud, les hémothermes et hetero-thermes. Chez ces derniers. la reaction est manifeste surtout dans Iemuscle cardiaque, elle est très faible dans les autres muscles oit l’ontrouve beau coup de substances osmioréductrices. I
Le Moigne, Sezary, Demonchy.-Therapeutic Action ofAntigonococcus Lipo-Vaccine.On injecte de sept a trpnte millions de gonocoques. Dans la grande
majorite des cas d’urethrite aigiie les symptomes douloureux cedentrapidement; l’écoulement disparait en huit ou quinze jours. La goutterésiduelle ou la sérosité virulente qui peuvent persist er disparaissentensuite rap’dement sur 1’action d’une ou deux injections de nirrated’argent. L’évolution est done notablement accourcie. De plus, chezles malades qu’ils ont pu suivre jusqu’au bout l’affection n’est jamaispassee a la chronicité. L’action du lipo-vaccin sur 1’orchi-epididymiteest rapidement frappante.
S. Marbais.-" The Little Red Bacillus " of Influenza.Nous avons etudie les caractères d’un pattt bacille, Gram negatif. que
nous avons trouve dans l’épanchement purulent et hemorragique desgrippes et dans 1’exsudat rhino-pharyngien des meningitiques, desdiphtériques et des suspects. Ses colonies ressemblent a celles dumeningocoque. Injecté en doses croissantes il tue le lapin avec broncho-pneumonie, epanchements purulents et hemorragiques de la plèvre etdu péritoine. et septicemies.
HOUSING IN MESOPOTAMIA.-The Military Governorof Basra has given a prize of Rs. 150 for the best paperson each of the following subjects : (a) The type of residentialhouse best suited for Europeans in the lowlands ofMesopotamia ; (b) the type of residential house best suitedfor Arabs in the lowlands of Mesopotamia, having regard totheir special customs.
Reviews and Notices of Books.Use of 11’actor,y Statistics in the Investigation ot Industrial
Fatigue. By PHILIP SARGANT FLORENCE, M.A. Camb.,Columbia University. London : Longmans, Green, andCo. 1918.THE study of industrial fatigue through the use of factory
records-in itself a fascinating subject-is just now ofparticular interest owing to the thought present in the mindsof many that the period of industrial unrest through whichwe are passing owes its origin in no small way to nervoustension following upon more than four years of unparalleledstrain. The incitement to effort has gone, the national dangeris passed ; it is the morning after the dance ; and we are leftvaguely wondering whether our efforts would not have beenless fatiguing if more scientifically directed. Such direction,however, would have required a knowledge of fatigue inrelation to physiology and the powers of normal recovery, andof pathology and the inception of disease, which is not inexistence. A recognition of this fact has induced this country(through the establishment of an Industrial Fatigue ResearchBoard) and America to undertake organised research into thewhole subject.We have before us an interesting volume recently pub-
lished in America, and intended as a manual for fieldresearch. The work is clearly the result of prolongedlabour. It contains much information and many referencesto work already done, and from this point of view would-beinvestigators may be recommended to acquire it. Theauthor, however, has succeeded in so magnifying difficultiesthat he paralyses thought rather than clarifies ideas, and hefrequently hampers his exposition by inventing a terminologyaltogether unnecessary and lacking in exactitude ; and inthis he is curiously reminiscent of those pre-Baconianphilosophers who prized well-sounding terms beyond anhonest fact and of that orator who held that words weremeant to conceal thoughts.An investigator about to embark on the study of industrial
fatigue should consult this volume not merely for what itcontains and tells him, but as in itself a subject for investi-
, gation. He must be ready while perusing it to use his ownbrains to extract the useful and to reject the unnecessary.As a first exercise for a budding investigator, therefore, the
, book is of value-a value directly in proportion to thereader’s capacity for becoming an investigator. In the true
spirit of investigation he must be prepared to search for and,
extract the useful, which is often submerged in a bewilderingsea of obscure classification. Then let him without fear
have recourse himself to the clear springs of observation; which the author has dipped into and troubled., This book treats of a new science-a science which, if itJ is to be of real value, must be studied by, and taught to,J managers and employers of labour. The language used by1 its exponents must for this purpose be simple, clear, and free
from all ambiguity. Otherwise the practical manager will r
f turn his back on what will seem to him to be impracticabletheories propounded by philosophical pedants. We hardly
3 think that this book will induce any employer of labour to Lt embark forthwith upon the study of industrial fatigue by an
investigation of his own factory statistics.
s Neurosyp7e £ lis: Modern Systematic Diagnosis and Treatment,e Presented in 137 Case-ki6tories. By E. E. SOUTHARD,
M.D., Bullard Professor of Neuro-pathology, HarvardMedical School; and H. C. SOLOMON, M.D., Instructorin Neuro-pathology and in Psychiatry, Harvard Medical
s School. With an Introduction by J. J. PuTNAM, M.D.,Professor Emeritus of Diseases of the Nervous System,
3t 31- Harvard Medical School. With many illustrations.London: Stanley Phillips; Boston : W. M. Leonards.
_
1918. Pp. 496. 21s. net.WE have already had occasion to review other volumes in
the case-history series to which this belongs, and haves pointed out what appeared to us their merits and demerits.vl In the present instance we feel that the advantages of thef method have been brought completely to outweigh its dis-d advantages. Briefly, a long series of cases of neuro-syphiliso are offered to the reader in their essentials only, all non-
essential clinical details being rigorously pruned; salient.