559 growth. Hot sterile ’ Vaseline ’ was run on to the surface to a depth of — in. to exclude air. The tube was then incubated at 37° C. After incubation for about 60 hours acne bacilli were perceptible, and there was a copious growth in 4 days. This method was followed in a number of cases as a routine, and in all a pure primary growth of acne bacilli was obtained in penicillin-glucose broth, whereas in glucose broth without penicillin the staphylococci when present outgrew the acne bacilli and usually inhibited their growth. ‘ Results obtained are shown in table I. TABLE I-CULTURES OBTAINED FROM ACNE LESIONS IN GLUCOSE BROTH WITH AND WITHOUT PENICILLIN This procedure requires no special apparatus, and enables autogenous vaccines of the acne bacillus to be prepared in 3-4 days after the material has been collected. Such vaccines also can be made from the primary cultures, so that changes in antigenic structure due to cultivation on artificial medium are reduced to a minimum. The penicillin used was a simple filtrate of Penicillium notatum, and, since the concentration of the antibacterial active principle in such filtrates is not always the same, it is not possible to give a definite dilution of the penicillin which will stop the growth of staphylococci without interfering with the growth of the acne bacillus. The penicillin used must have been previously titrated against staphylococcus and the concentration used in glucose broth should be twice that which completely inhibits staphylococcal growth. TYPES OF ACNE BACILLUS When the primary cultures of acne bacilli were plated anaerobically two types of colony were noted. Type I gave a large heaped-up colony which had a yellowish buff colour and on blood agar was surrounded with a large zone of haemolysis. The individual bacilli were short, thick, irregular in shape, and often clubbed. Type II gave small flat colonies and the individual bacilli were longer, thinner and often curved. These two types often occurred together in the same specimen of pus, but in 8 cases out of 24 only type n was present. In the, indolent pustules often seen in some cases of acne type II is usually found in pure culture. The sugar reactions were not quite constant, but in most cases both types fermented glucose, saccharose and glycerin, while type I also fermented maltose. Rabbits were immunised with the two types of acne bacillus and the agglutination reactions of these immune rabbits were tested against cultures of the different types (table 11). TABLE II-AGGLUTINATION OF DIFFERENT TYPES OF ACNE BACILLUS WITH IMMUNE RABBIT SERUM i t . The tests show that the two types of acne bacillus are antigenically distinct. . SUMMARY Pure cultures of acne bacilli were obtained from 47 specimens of acne material in glucose broth containing penicillin in double the concentration which inhibited staphylococcal growth. Two types of colony of acne bacillus were noted. These two types were antigenically distinct. I am indebted to Prof. Alexander Fleming for his help. Medical Societies ROYAL SOCIETY OF MEDICINE AT a meeting of the section of State Medicine on April 24, with Dr. E. H. R. HARRIES, the president, in the chair, a discussion on the Future of Public Health Nursing was opened by Miss M. E. FLAMBERT, deputy chief nursing officer to the Ministry of Health. Public health nursing, she said, depends on the future development of the medical and social services. The term covers health visiting, midwifery, and district, school and industrial nursing. All these services have grown with the growth of maternity and child welfare work. Today most health visitors are general-trained nurses with a mid- wifery qualification who have taken a health visitor’s course and have thus spent some 4-5 years in prepara- tion for their career. She doubted whether general training at present is sufficiently comprehensive : it’ should contain more of the fundamentals of public health nursing. At present comprehensive service is being given by those district nurses who are also doing midwifery and health visiting. All Queen’s nurses, for example, are state registered and must take a six months’ course in district nursing. Many .nurses, however, are unable to afford a health visitor’s course before under- taking district nursing, and are thus not able to make full use of a fine opportunity for teaching hygiene. Much health visiting still falls on voluntary organisa- tions, and in many districts these organisations cannot afford fully trained women, but employ nurse-midwives who have had 2 years’ training in midwifery without a nursing qualification. The number of Queen’s nurses employed, however, is steadily increasing, although it is still an open question whether one nurse should combine the duties of health visitor, midwife and district nurse, or whether the work should be divided among specialists. Miss Flambert felt that people must become much more health-conscious before they will readily tolerate more than one visitor. A medical officer of health had told her that he had tried both methods, and that though the single visitor was more acceptable to the public, a service of specialist nurses was easier to administer. The aim in training women for public health nursing must be to educate them in preventive medicine. As it stands district nursing does not necessarily attract the women most fitted for it, but rather those who wish to escape from the petty restrictions of hospital life. More must be done to improve standards in public health work and so to attract the right type of girl. Those entering at present have their outlook focused on the care of the sick. Matrons and sister tutors could do much, she thinks, to shift the emphasis to preventive work. The scope of school nursing could be extended, and she would like to see all health teaching in schools given by trained public health nurses who have been taught to teach. The prospects of promotion should also be greater : better candidates will be attracted if there is a ladder to climb. Thus there should be more posts for superintendent health visitors, she considers, and more non-medical supervisors of midwives. Many feel that the combined post of superintendent of mid- wives and health visitors should be abolished because it excludes able women who have only specialised in one branch. Industrial nursing is a branch of public health nursing which has grown rapidly: in 1939 there’ were 1500 industrial nurses, and this number is believed to have been trebled in the last 2 years ; and industrial nurses can give much health teaching to workers in factories. AMERICAN EXPERIENCE _ Miss E. C. PHILLIPS, associate chief nurse in the American Red Cross, serving with the Harvard Field Unit, said that public health nursing in America has had an erratic childhood, labouring under three difficulties : the job has never been defined ; there have been too few nurses to carry it out; and the preparation of the nurse has not kept pace with her developing oppor- tunities. Before the last war, growth was sporadic, but in 1912 the National Organisation for Public Health Nursing was established, with the aim of improving performance. At the beginning of the century there. T3
Transcript
559
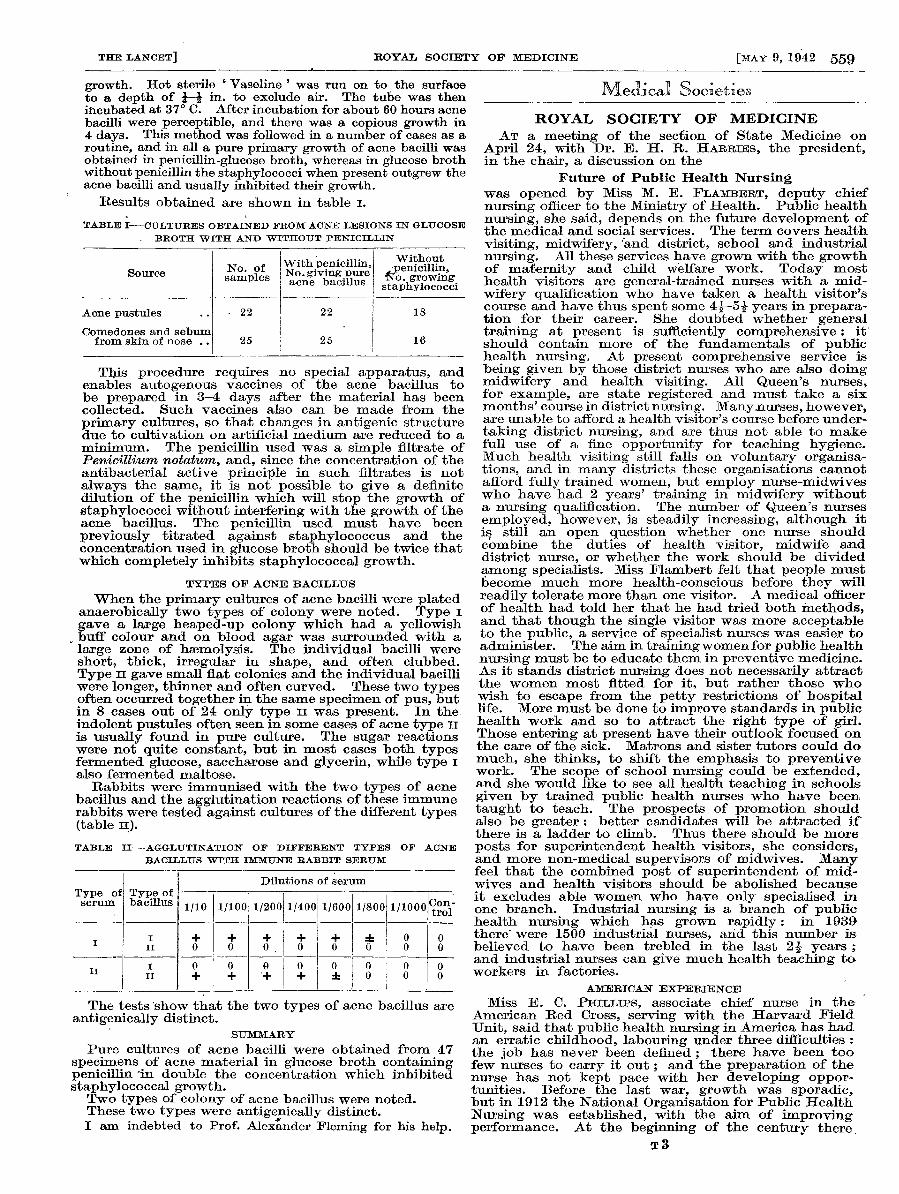
growth. Hot sterile ’ Vaseline ’ was run on to the surfaceto a depth of — in. to exclude air. The tube was thenincubated at 37° C. After incubation for about 60 hours acnebacilli were perceptible, and there was a copious growth in4 days. This method was followed in a number of cases as aroutine, and in all a pure primary growth of acne bacilli wasobtained in penicillin-glucose broth, whereas in glucose brothwithout penicillin the staphylococci when present outgrew theacne bacilli and usually inhibited their growth.
‘ Results obtained are shown in table I.
TABLE I-CULTURES OBTAINED FROM ACNE LESIONS IN GLUCOSE
BROTH WITH AND WITHOUT PENICILLIN
This procedure requires no special apparatus, andenables autogenous vaccines of the acne bacillus tobe prepared in 3-4 days after the material has beencollected. Such vaccines also can be made from the
primary cultures, so that changes in antigenic structuredue to cultivation on artificial medium are reduced to aminimum. The penicillin used was a simple filtrate ofPenicillium notatum, and, since the concentration of theantibacterial active principle in such filtrates is notalways the same, it is not possible to give a definitedilution of the penicillin which will stop the growth ofstaphylococci without interfering with the growth of theacne bacillus. The penicillin used must have beenpreviously titrated against staphylococcus and theconcentration used in glucose broth should be twice thatwhich completely inhibits staphylococcal growth.
TYPES OF ACNE BACILLUS
When the primary cultures of acne bacilli were platedanaerobically two types of colony were noted. Type I
gave a large heaped-up colony which had a yellowishbuff colour and on blood agar was surrounded with alarge zone of haemolysis. The individual bacilli wereshort, thick, irregular in shape, and often clubbed.Type II gave small flat colonies and the individual bacilliwere longer, thinner and often curved. These two typesoften occurred together in the same specimen of pus, butin 8 cases out of 24 only type n was present. In the,indolent pustules often seen in some cases of acne type IIis usually found in pure culture. The sugar reactionswere not quite constant, but in most cases both typesfermented glucose, saccharose and glycerin, while type Ialso fermented maltose.
Rabbits were immunised with the two types of acnebacillus and the agglutination reactions of these immunerabbits were tested against cultures of the different types(table 11).
TABLE II-AGGLUTINATION OF DIFFERENT TYPES OF ACNE
BACILLUS WITH IMMUNE RABBIT SERUM
i t .
The tests show that the two types of acne bacillus areantigenically distinct.
.
SUMMARY
Pure cultures of acne bacilli were obtained from 47specimens of acne material in glucose broth containingpenicillin in double the concentration which inhibitedstaphylococcal growth.Two types of colony of acne bacillus were noted.These two types were antigenically distinct.I am indebted to Prof. Alexander Fleming for his help.
Medical Societies
ROYAL SOCIETY OF MEDICINEAT a meeting of the section of State Medicine on
April 24, with Dr. E. H. R. HARRIES, the president,in the chair, a discussion on the
Future of Public Health Nursingwas opened by Miss M. E. FLAMBERT, deputy chiefnursing officer to the Ministry of Health. Public healthnursing, she said, depends on the future development ofthe medical and social services. The term covers healthvisiting, midwifery, and district, school and industrialnursing. All these services have grown with the growthof maternity and child welfare work. Today mosthealth visitors are general-trained nurses with a mid-wifery qualification who have taken a health visitor’scourse and have thus spent some 4-5 years in prepara-tion for their career. She doubted whether generaltraining at present is sufficiently comprehensive : it’should contain more of the fundamentals of publichealth nursing. At present comprehensive service isbeing given by those district nurses who are also doingmidwifery and health visiting. All Queen’s nurses,for example, are state registered and must take a sixmonths’ course in district nursing. Many .nurses, however,are unable to afford a health visitor’s course before under-taking district nursing, and are thus not able to makefull use of a fine opportunity for teaching hygiene.Much health visiting still falls on voluntary organisa-tions, and in many districts these organisations cannotafford fully trained women, but employ nurse-midwiveswho have had 2 years’ training in midwifery withouta nursing qualification. The number of Queen’s nursesemployed, however, is steadily increasing, although itis still an open question whether one nurse shouldcombine the duties of health visitor, midwife anddistrict nurse, or whether the work should be dividedamong specialists. Miss Flambert felt that people mustbecome much more health-conscious before they willreadily tolerate more than one visitor. A medical officerof health had told her that he had tried both methods,and that though the single visitor was more acceptableto the public, a service of specialist nurses was easier toadminister. The aim in training women for public healthnursing must be to educate them in preventive medicine.As it stands district nursing does not necessarily attractthe women most fitted for it, but rather those whowish to escape from the petty restrictions of hospitallife. More must be done to improve standards in publichealth work and so to attract the right type of girl.Those entering at present have their outlook focused onthe care of the sick. Matrons and sister tutors could domuch, she thinks, to shift the emphasis to preventivework. The scope of school nursing could be extended,and she would like to see all health teaching in schoolsgiven by trained public health nurses who have beentaught to teach. The prospects of promotion shouldalso be greater : better candidates will be attracted ifthere is a ladder to climb. Thus there should be moreposts for superintendent health visitors, she considers,and more non-medical supervisors of midwives. Manyfeel that the combined post of superintendent of mid-wives and health visitors should be abolished becauseit excludes able women who have only specialised inone branch. Industrial nursing is a branch of publichealth nursing which has grown rapidly: in 1939there’ were 1500 industrial nurses, and this number isbelieved to have been trebled in the last 2 years ;and industrial nurses can give much health teaching toworkers in factories.
AMERICAN EXPERIENCE _
Miss E. C. PHILLIPS, associate chief nurse in theAmerican Red Cross, serving with the Harvard FieldUnit, said that public health nursing in America has hadan erratic childhood, labouring under three difficulties :the job has never been defined ; there have been toofew nurses to carry it out; and the preparation of thenurse has not kept pace with her developing oppor-tunities. Before the last war, growth was sporadic,but in 1912 the National Organisation for Public HealthNursing was established, with the aim of improvingperformance. At the beginning of the century there.
T3
560
were only 130 public health nurses in the United States,employed by 58 agencies ; by 1920 the number hadincreased to 9000, employed by 4000 agencies ; andin the last 20 years the figure has increased to 24,000,employed by 6000 agencies. Yet the figure of one toevery 2000 population, set up by the American PublicHealth Association, would require a total of 65,000public health nurses today, and only one state has sofar approached it. The average at present is one nurseto 7000 population. The federal government hopes toadd 10,000 new public health nurses to the field in thecoming year. About £312,000 last year and probablyabout 500,000 this year is being allotted by Congressto nursing, and will chiefly be spent on expanding under-graduate and graduate courses. A typical plan for train-ing public health nurses is designed for graduates ofapproved schools of nursing who qualify for a universitycourse. They spend 4 months on a combined programmeof college and field work, and receive an allowance ofabout £112 to cover tuition and maintenance. In returneach nurse agrees to give two years service on a minimumsalary as a junior public health nurse, and to completea year’s programme of study in public health nursing.Basic courses for all nurses in the better schools alreadyinclude psediatric nursing, care of children with ortho-paedic and cardiac conditions, and experience at nurseryschools when possible ; and efforts are made to developin the student a deep appreciation of the social and healthaspect of nursing. The public health nurse worksunder four kinds of organisation : official agencies ;non-official or voluntary agencies ; boards of education ;and commercial companies. In 1941, about 4% of the23,533 public health nurses were in State agencies,41% in local health departments, 25% under non-
official agencies, 15% under boards of education and15% in industrial companies. The numbers have grownmost rapidly in the factories, increasing by more than athird in the last 5 years. Americans, she said, believedthat the goal of public health nursing was a compre-hensive community programme, to be achieved byrepresentatives of all the agencies sitting round a tableand planning together; it will then probably becomeclear that fewer agencies are needed. The public healthnurse can give adequate care to the whole family.She works under a doctor who may be the private doctorof the patient, or the doctor at the health department,hospital, school or factory. If she finds a patient notunder medical care she gets him under the doctor. Sheis primarily an educator. Scholarships and grantsfit her for the task ; in 1941, 62% of all supervisingnurses had had a year or more of public health educationand over a third of them held university degrees. Thoughthe service is still fluid, eight trends can now be recog-nised : bedside nursing is becoming a part of programmeswhere it never was before ; teaching given by the publichealth nurse is accompanied by practical demonstration ;the family is being recognised as a unit for health care ;the school nurse is working more with the teachers thandirectly with the children ; the preschool, adolescent andsenescent years are receiving more attention ; the careof the chronically ill is being improved ; emphasis isbeing placed on those aspects of the public health workwhich require great nursing skill, such as the care of thepremature, the pneumonia patient or the child withcardiac disease; and industry is using public health nurses,not only in factories but in the homes of the workers.The leaders of public health nursing are helping to recruitand select the right kind of girls as students for schoolsof nursing.
AND IN THE DOMINIONS
Miss I. S. HAWKINS explained that in New Zealandthe population was only 3,000,000, and there were noreal, though some potential, slums. The problem,she said, is how to cover the scattered population econo-mically and efficiently. She believed that the house-wife should have some say about the number of visitorscalling on her ; we help her most by giving her one soundfriend and adviser, rather than several specialists.The Plunket nursing service, founded by Truby King,has reduced the New Zealand infant mortality from 75to 30 per 1000. The hospitals are not elaboratelyequipped, but are made to approximate to the averagehome so that the nurse can teach the mother to handleproperly the materials she will be using on her discharge.
New Zealand is the only country in the Empire where thenatives are accepted as the equals of the whites. TheMaori are a fine race with whom fitness and strengthwere almost a religion before white settlers came.
They have received the advantage of easier living,and with it the disadvantages of tuberculosis and dentalcaries. For a time they seemed to be a dying race, inconsequence, but now, thanks to public health measures,their numbers are slowly increasing again. They areintensely superstitious, and a man dying in hospital withtuberculosis is always taken back to expire among hisfriends, so that infection is kept alight. Yet it wouldbe’ a mistake to be highhanded with them : their mis-trust and fear is slowly being overcome by public healthteaching. Over here, where everyone is working hardand wanting to keep fit, and where we have had practicaldemonstration, in the shelters, of the importance ofdrainage and sanitation, now is the time, she believes, toinstil ideals of public health.
Miss ELEANOR JONES described the three yearsuniversity course in combined hospital and publichealth nursing given at the Toronto School of Nursing,of which she is a graduate. Those entering are aged19, must have had a secondary school education witha good grounding in science. The first year is spent inthe study of the principles of public health nursingand preventive medicine and in laboratory work;the remaining two years are spent in hospital doingbedside nursing; during the third year the student alsoundertakes social case work, child hygiene and field work.Only six classes have graduated so far, but all the graduateshold responsible positions.
OUTLOOK AT HOME
Dr. NICOLAS GEBBIE, medical officer of health to Hull,said that the forerunner of the public health nurse wasthe female sanitary inspector, who did pioneer work insupervising the health of women and girls in factories.The activities of public health nurses began in 1906-07,and it. says much for the tact of the pioneers that thenurse has become a welcome visitor and that knock-knees and bow-legs have gone out. The school nurse,known affectionately as the " nit nurse," resolutelytries to raise the standard of cleanliness, and the midwifeplays her own important part. The public health nurseshould have a sound general training including experiencein the care of the chronic sick. She should be essentiallya teacher, and should have, he considered, the samestandard of education as teachers in elementary schools.At Hull, the public health course for nurses lasts a year.Enrolments should be sufficient to attract the best inthe profession ; there is no shortage of health visitors,he said, in places which offer a minimum salary of over£200 and a maximum of over £250. As to the retiringage, 60 is old enough, in his view, for anyone to bebicycling about in all weathers. Refresher courses
should be provided and the amenities and rewards offeredto the public health nurse should be commensurate withthe importance of her work to the nation.
Sir WiLSON JAMESON agreed that it is impossible toattract the right women unless they can be given adecent status. The new section of nursing in the Ministryof Health has the same status as any medical sectionin the department. He believes that it is better for onenurse to be responsible for the health of the family, andthis can possibly be done by extending the service ofQueen’s district nurses who have had public healthtraining. Miss Russell’s school in Toronto, describedby Miss Jones, shows what can be done ; her nurses aretrained as students, and not made use of as cheap nursesfor hospitals.
Dr. J. A. H. BRINCKER spoke of the internationalcourse in social science which has been successful atBedford College. He thought the education in hygieneof children in elementary schools could be improved.-Dr. T. 0. GARLAND said that in nursing, as in medicine,the emphasis during training was largely on the treatmentof the sick. This bias will remain until the early asso-ciations of the student are with the influence of socialconditions on health.-Miss G. E. STEPHENS mentioneda Royal College of Nursing survey which shows that50 % of nurses in a northern city are doing public healthwork ; in the country as a whole the figure is about14%.-Sir WELDON DALRYMPLE-CHAMPNEYS pointed
561
out that the break up of family life brought about by thewar had led people to depend more on the public services,and this was a great opportunity for the public healthnurse.
MEDICAL SOCIETY FOR THE STUDY OFVENEREAL DISEASES
Compulsory PowersAT a meeting of this society in London on April 25,
with Colonel L. W. HARRISON, F.R.C.P., the president,in the chair, a discussion on the need for further powersto deal with sources of infection, contacts and defaulterswas opened by Major S. M. LAIRD, R.A.M.C. In describ-ing existing legislation he pointed out that any person isfree to have VD and to communicate it as much as hechooses ; he is not obliged to be treated or to continuetreatment until cured -or rendered non-infectious ; he isunder no legal obligation to assist in tracing his infectiveconsort and the latter is free to refuse examination andtreatment. In the absence of notification no accurateknowledge of the incidence of these diseases exists. Heemphasised the diagnostic difficulties in female gonor-rhcea and the need for a greater index of suspicion on thepart of the medical profession. The control of infectionrequires a knowledge of the causative organism, themethod of spread, efficient diagnosis and treatment ofthe individual case, and the discovery of the source ofinfection and all other contacts. In relation to gonor-rhœa and syphilis the first two requirements are fullymet ; the third may fail in practice from diagnostic delayor inadequate treatment; but the fourth requirement isinfrequently met in this country. Control is sabotagedin this country by three factors : the technical imperfec-tions of the medical profession ; the defaulting patient;and’ the untraced source of infection and contacts.Failure to suspect and diagnose VD contributes to thelack of success in the control of these diseases, and MajorLaird suggested that they should only be dealt with bypractitioners who have successfully passed throughpostgraduate instruction in this specialty. A patientmay default before the completion of treatment or he maycease to attend after treatment but before cure can bepronounced. The latter imperils his future health ; theformer, in addition, imperils the public health. Bothcategories are important ; the inadequately treatedpatient may be incapacitated by the later complicationsof VD and, with his dependents, become liabilities to thestate ; the infectious defaulter, particularly if a woman,may infect others of the same and the next generation.The defaulter-rate is high in this country ; in England in1935 only 17-5% of patients at the treatment centrescompleted treatment and tests of cure. The correspond-ing figure for Sweden was 97-5%. Factors encouragingdefaulting are manifold and many are avoidable. Thedefaulter-rate can be lowered by attention to such factorsas suitable clinic hours, a sympathetic and skilful staff,taking trouble to establish and maintain a close under-standing and harmony between patient and clinic officer,and the services of an almoner. Some defaulters maybe brought back by a suitable written reminder or by acall from a health visitor. In spite of attention to allthese points a certain hard core persists which wouldonly be controlled by the threat or actual use of com-pulsion. The position with regard to sources of infectionand contacts is still worse, and Major Laird submittedthat the methods of control in use in this country are notsatisfactory. He thought it significant that the NewYork Commission which in 1936 studied the. antivenerealmeasures employed in Britain and the Scandinaviancountries reported in favour of the compulsory powers inuse in Scandinavia. The Swedish law of 1918, underwhich the present antivenereal measures are carried on,applies to syphilis, gonorrhoea and soft sore in an infec-tious form. It provides for confidential notification ;compulsory treatment and obedience to instructionscalculated to prevent the infection of others ; ascertain-ment of the source of infection and the compulsoryexamination and treatment of the source ; a comprehen-sive mechanism for dealing with defaulters ; compulsoryremoval to hospital of patients who might otherwisecause other persons to become infected, and of defaultersand sources of infection who fail to carry out the instruc-tions of the inspector of health. The order for removal
to hospital is normally issued by the health authority,against whose decision there is a right of appeal to higherauthority. The decision already given must be observeduntil countermanded by higher authority. A doctor whofails in any of his statutory duties is liable to a fine.Major Laird then quoted from the British Mission’sReport (H.M. Stationery Office, No. 83, 1938) to indicatethat the Swedish measures do not lead to concealmentor malicious complaint and are well received by thepeople. Persons called on to undergo medical examina-tion seldom raise objection and appeals are rare. Themission was told by the Swedish doctors that it was ofassistance to have the penal provisions of the law behindthem, but that it was rarely necessary to use them. Therates per 10,000 of the population for primary andsecondary syphilis in 1935 were : Stockholm, 1-8 ; therest of Sweden, 0-57; and all Sweden, 0-67. Tlie ratesin 1935 were respectively 4-1%, 7.5% and 6.6% of therates for 1919. Major Laird emphasised that Stockholm,in spite of density of population and a high proportionof imported infections (31-7% of all early syphilis inmales), had a rate similar to that of the whole of Englandand Wales. The number of cases of all stages of acquiredand congenital syphilis reporting for the first time inStockholm in 1935 was 5% of what it was in 1919. InLiverpool the corresponding total in 1935 was 37% ofthe 1919 total. Sweden has far outstripped this countryin reducing the incidence of congenital syphilis. MajorLaird concluded that compulsory powers have contri-buted to the success of the Swedish antivenereal measuresand was of the opinion that the Minister of Healthshould arrange, without delay, for a survey of the VDproblem in this country with a view to the trial of noti-fication and compulsory measures. Notification mustbe by number only unless and until the patient defaults,and compulsory measures must be applied withoutdiscrimination to both sexes and all sections of thecommunity. He emphasised the need for intensive
education of the public and thought it time that the manin the street was told the truth about VD in this country ;otherwise he could not be expected to cooperate insolving the problem. The medical profession requirefurther education especially in the epidemiologicalaspects of VD, and expert legal and political advice mustbe sought in drafting the necessary measures. He urgedthe Government to avoid complacency.
Dr. E. W. ASSINDER (Birmingham) said he had neverunderstood why the venereal diseases were not on thelist of notifiable infectious diseases ; he was in favour ofnotification and compulsory powers.
Dr. A. M. STUART (Portsmouth) emphasised the needfor education of the medical profession and mentionedthat home-visiting of defaulters by health visitors hadrecently been introduced in Portsmouth.
Dr. J L. BURN (Barnsley) described the resultsachieved by home visiting in Barnsley and Salford andreminded the meeting that Salford some years ago askedfor a local trial of compulsion.
Mrs. NEVILLE-ROLFE (secretary-general, British SocialHygiene Council) attributed the greater success of theSwedish measures to the better undergraduate and post-graduate training of the doctors treating VD in thatcountry and to the education of the school-children insocial hygiene including VD. She asked for the morethorough application of the voluntary method, and inparticular for more adequate facilities for diagnosis andtreatment, especially for women working in industry.She urged the setting up of ailments-of-women clinics toattract cases which would not attend the ad-hoc clinic.She agreed that compulsion would often be necessary tocontrol the professional prostitute and the regularlypromiscuous girl and that these two categories wouldrequire adequate inpatient treatment facilities.
Dr. W. G. BOOTH (Boston, Lines) had found that ademand for more effective control already existed amongthe laity, particularly among the council members oflocal authorities. He was impressed- by the case forcompulsion.
Dr. ROBERT FoRGAN (Central Council fdr HealthEducation), who said he expressed the views of theScottish committee of the society in addition to his own,mentioned previous Scottish attempts to promote legis-lation and asked why the compulsion used in the Servicesshould not also be applied to the civilian population.