RTOG1106: Randomized Phase RTOG1106: Randomized Phase IIR Trial of Personalized IIR Trial of Personalized Adaptive Radiotherapy Based Adaptive Radiotherapy Based on Mid-treatment FDG-PET in on Mid-treatment FDG-PET in Locally Advanced NSCLC Locally Advanced NSCLC P.I.: Feng-Ming (Spring) Kong, M.D., Ph.D. Study Team Mitchell Machtay, M.D. Jeffrey D. Bradley, M.D. Jean Moran, Ph.D. Vera Hirsh, M.D. Barry Siegel, M.D.
Transcript
RTOG1106: Randomized Phase IIR Trial of RTOG1106: Randomized Phase IIR Trial of Personalized Adaptive Radiotherapy Based Personalized Adaptive Radiotherapy Based
on Mid-treatment FDG-PET in Locally on Mid-treatment FDG-PET in Locally Advanced NSCLCAdvanced NSCLC
P.I.: Feng-Ming (Spring) Kong, M.D., Ph.D.
Study TeamMitchell Machtay, M.D.Jeffrey D. Bradley, M.D.
Jean Moran, Ph.D.Vera Hirsh, M.D.
Barry Siegel, M.D.
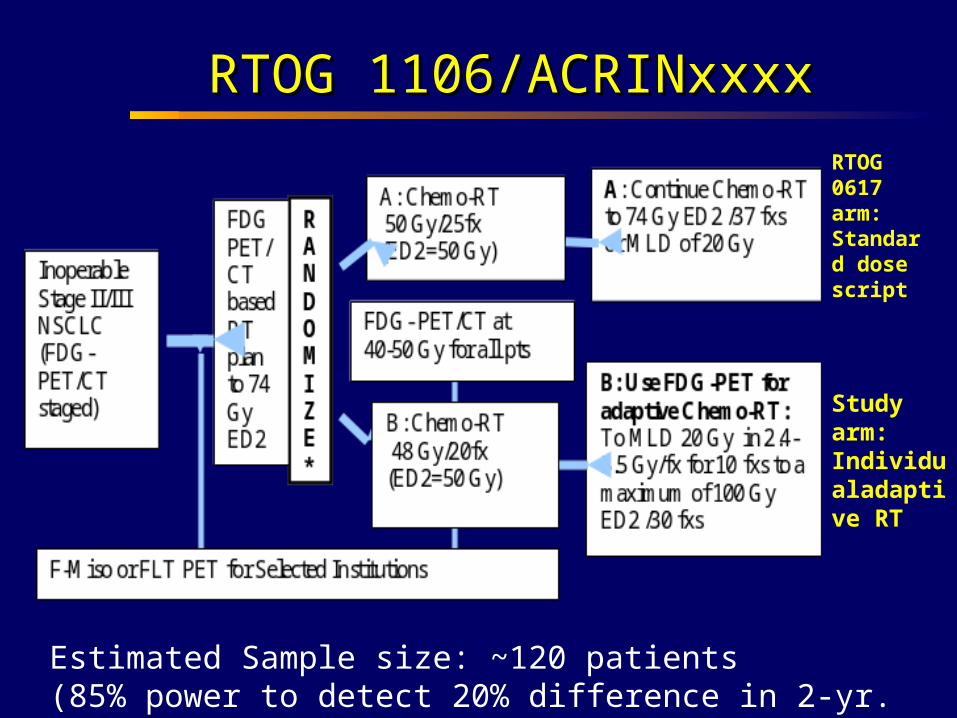
RTOG 1106/ACRINxxxxRTOG 1106/ACRINxxxx
Estimated Sample size: ~120 patients(85% power to detect 20% difference in 2-yr. local PFS)
Weeks to monthsWeeks to months Months Months to yearsto years
The Traditional ApproachThe Traditional ApproachCTCT
PETPET1-3 months1-3 months
Background - 1Background - 1
ACRIN 6668/RTOG 0235: FDG-PET
REGISTER
FDG-PET with SUV
Chemo-RT +/- ‘adjuvant’
chemo
Eligibility
Stage III NSCLC plan for conc. chemo-RT
PS 0-1
Primary Endpoint: Survival as a function of post-RT SUV
Sample Size: 250
FDG-PET with SUV
2-3 months after XRT
ACRIN 6668/RTOG 0235 Update
Activation Date: 3/1/2005.
Closed to Accrual: 5/15/2009.
Total Accrual: 251 pts.236 verified eligible (94%).
Total # Participating Sites: 37.
Central Review in Process.Qualitative, SUVpeak, MTV
Primary Outcome Analysis in Early/mid 2011.
RTOG 0515 Results
Exploratory trial of pre-Tx FDG-PET for XRT planningN=47
Variable CT Only PET/CT Difference p
Mean GTV (cc) 98.7 86.2 -12.5% <0.0001
Mean # involved nodes
2.1 2.4 14% 0.41
Mean Lung dose (Gy)
19 Gy 17.8 Gy -6% 0.06
Mean esophageal dose (Gy)
28.7 Gy 27.1 Gy -6% 0.30
Bradley et al. ASTRO 2009
HypothesesHypotheses
Use of mid-treatment FDG-PET is as useful or more useful than pre-RT FDG-PET and/or 3-month post-RT PET.Mid treatment PET can be used to individualize (and escalate) XRT dose will result in improved outcomes (2-yr. LPFS) compared with standard XRT.
Weeks to monthsWeeks to months Months Months to yearsto years
The Traditional ApproachThe Traditional ApproachCTCT
PETPET1-3 months1-3 months
•Post-RT PET response is highly correlated with pathologic response.•Post-RT PET is predictive of long term survival and pattern of failure(Mac Manus et al, 2003)RTOG235/Acrin688 results awaited.
However, post-RT PET tumor response does not provide an opportunity to change the treatment plan.
When should PET be done?When should PET be done?
PET during RT?PET during RT?
PET scan can be performed during-RT University of Michigan study, ASTRO 2005 MAASTRO study, ASTRO 2005 Stanford study, ASTRO 2007 Princess Margaret Hospital, ASTRO 2008
UM has demonstrated that PET response at 45 Gy during-RT was highly correlated with post-RT response in a small pilot study.
The above finding has been recently validated in another 50+ patients from Michigan.
Kong et al, JCO, 2007Kong et al, JCO, 2007
Individualized RT Escalation Is Feasible
Michigan trial usees PET-MTV guided isotoxicity adaptive plan to escalate tumor dose: 30 daily treatments, 2.2-3.8 Gy per fraction, 66 Gy~85.5 Gy To NTCP of 17% (mean lung dose 20 Gy), with concurrent and
adjuvant carbo and taxol, maximum at102 Gy in 2 Gy equivalent dose for lung (=ED2) (92 Gy ED2 for tumor).
14 patients completed treatments per study, all patients treated >74 Gy ED2 (median=92 Gy for tumor), majority of them received the maximum dose.
6 patients followed up for 1.5 years, no local failure thus far, 2 brain mets, only 1 death thus far from GI bleeding (gastric and esophageal ulcers).
Tumor Response During-RTTumor Response During-RT
Pre- RTPre- RT
HeartHeart
HeartHeart
TumorTumor TumorTumor
TumorTumor TumorTumorDuring-RT at 45 GyDuring-RT at 45 Gy
Example-1
CT-lunGwindow CT-mediastinum window FDGPET
Pre-RT
During-RT
3 mo post
9 mo post
16 mo post
UM002
MTV: 353 cm3GTV: 468 cm3
GTV: 402 cm3MTV: 268 cm3
GTV: 174 cm3
MTV: 12 cm3
This 48 YO male received 85.5 Gy(120 Gy BED) had grade 0 clinical toxicity thus far.He works full time now with heavy duty.
Patient-2
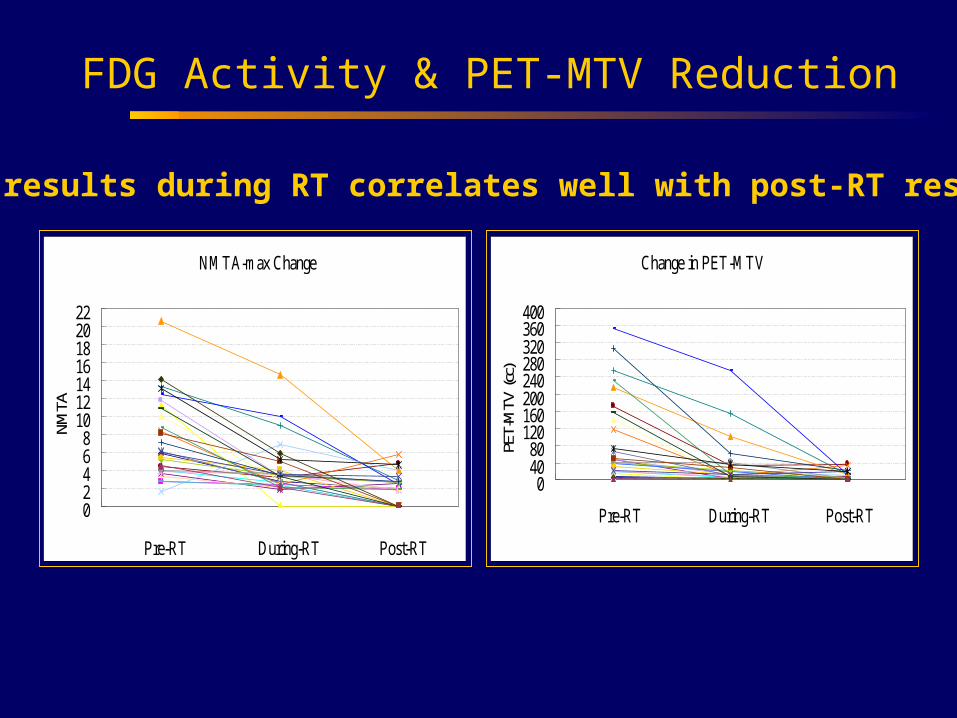
FDG Activity & PET-MTV Reduction
NMTA-max Change
02468
10121416182022
Pre-RT During-RT Post-RT
NMTA
Change in PET-MTV
04080
120160200240280320360400
Pre-RT During-RT Post-RTPE
T-M
TV (c
c)
PET results during RT correlates well with post-RT results
PET-MTV Decreased More than CT-GTVPET-MTV Decreased More than CT-GTV
CTCTPETPET
Pre-RTPre-RT
During-RTDuring-RT
During-RTDuring-RT
50 pts 88 tumors50 pts 88 tumors
Mid-course FDG-PET and PFSMid-course FDG-PET and PFS1 Year Progression-Free Survival1 Year Progression-Free Survival
(Kong et al, ASTRO 2009)(Kong et al, ASTRO 2009)
Mid-course FDG-PET and SurvivalMid-course FDG-PET and Survival
Followup to ACRIN 6668/RTOG 0235.FDG-PET during RTValidate UM resultsStudy adaptive RT/dose escalationRandomization to assess the efficacy of
mid-treatment FDG-PET
Opportunity to study a novel tracer (e.g. F-Miso) in limited institution sub-study.
RTOG 1106/ACRINxxxxRTOG 1106/ACRINxxxx
Estimated Sample size: ~120 patients(85% power to detect 20% difference in 2-yr. local PFS)
RTOG 0617 arm:Standard dose script
Study arm:Individualadaptive RT
Secondary AimsSecondary Aims
To compare toxicity between such a PET image-guided adaptive dose escalation and conventional RT.
To validate recent findings from a single institution that a tumor metabolic response during-RT predicts long term local tumor control, LPFS and overall survival.
To perform a pilot study to assess whether a novel PET tracer (F-Miso) is more predictive than FDG-PET.
To obtain blood and tissue samples to explore relationships between imaging findings, biomarkers and outcomes (both anti-tumor efficacy and toxicity).
FLT versus F-Miso
FLT F-Miso
Ease of use √ √
Sensitivity relative to FDG
Specificity relative to FDG √
Relevance to Radioresistance √
Which is the ‘better’ exploratory agent?
Other Issues Still to be Resolved
ACRIN Co-PI TBA.
Radiotherapy Fractionation issues.
Randomization, stratification issues.
Sample size for FLT/FMISO sub-study.
Insurance company reimbursement for mid course PET.