2Provide brief skills for clinicians using behavioral techniques for smoking cessation, including the 5 A's and pharmacologic cessation aids in psychiatry.
3Be able to access RxforChange, a web based curriculum to disseminate tobacco treatment training for health care professionals, including specific training for psychiatric settings.
4
For even more slides, handouts and resources (free of charge), visit RxForChange.ucsf.edu
Smoking, Substance Use Disorders (SUD) and Mental Illness
n 20% of the population uses a tobacco productn Cigarettes (13.7%), cigars (3.9%), e-cigarettes (3.2%)
n Individuals with mental illness and/or SUD n 2-4 fold higher rates of smokingn Consume 44-46% of cigarettes sold in the USn Account for 200,000 of the 480,000 premature deaths annually n Die on average 25 years earlier (treatable conditions related to
tobacco use)n Smoking accounts for more morbidity than alcohol and all
other drugs combined, even among individuals with SUD
https://www.cdc.gov/mmwr/volumes/68/wr/mm6845a2.htm Grant, et al, Arch Gen Psych, 2004 Colton, Manderscheid, Prev Chronic Disease 2006Lasser, et al, JAMA, 2000 Schroeder, Morris, Ann Review Pub Health, 2010Surgeon General’s Report, 2014
Department of Health, Education, and Welfare National Institute of Mental Health
Washington, DC August 4, 1980
I am writing to request a donation of cigarettes for long-term psychiatric patients…because of recent changes in the DHHS regulations, Saint Elizabeth Hospital can no longer purchase cigarettes for them.
I am therefore requesting a donation of approximately 5,000 cigarettes a week (8 per day for each of the 100 patients without funds).
Slide from Judith J. Prochaska, PhD, MPH
10
LD 463 - An Act to Exempt Substance Abuse and Psychiatric Patients from the Prohibition against Smoking in Hospitals
Slide from Judith J. Prochaska, PhD, MPH
11
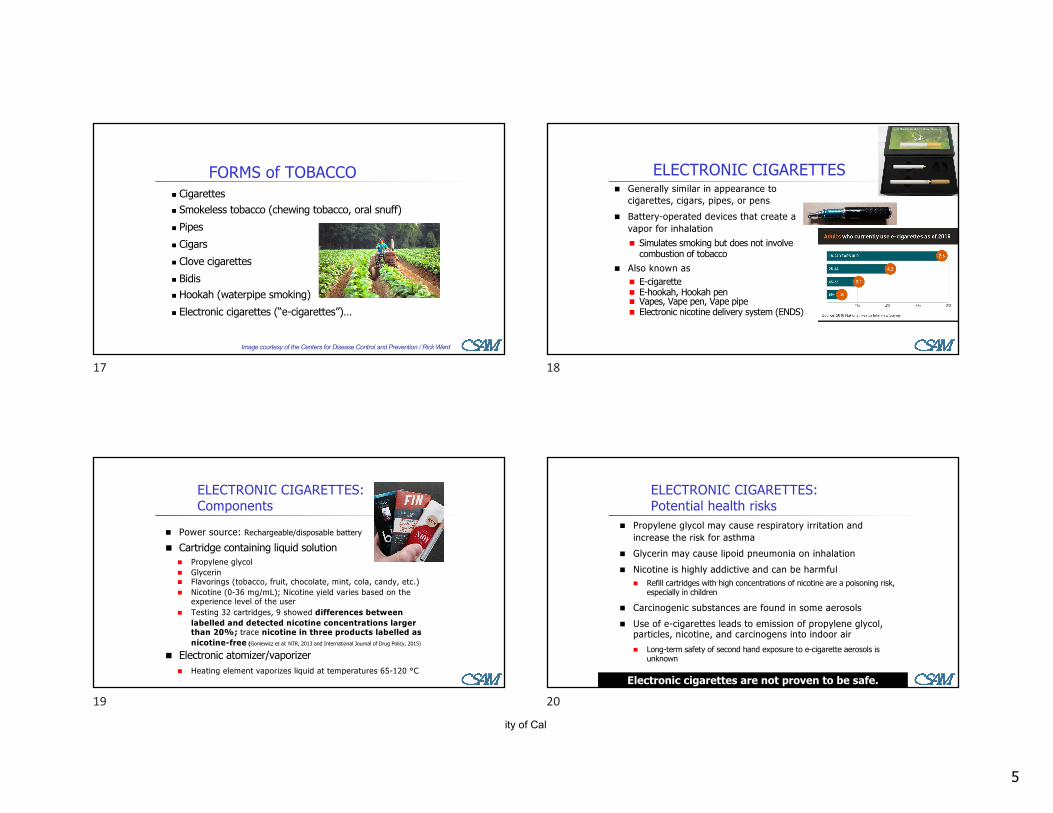
ANNUAL U.S. DEATHS ATTRIBUTABLE to SMOKING, 2005–2009
33%27%23%
9%7%
<1%
Cardiovascular & metabolic diseases 160,600Lung cancer 130,659Pulmonary diseases 113,100Second-hand smoke 41,280Cancers other than lung 36,000Other 1,633
Percent of all smoking-attributable deaths
TOTAL: >480,000 deaths annuallyU.S. Department of Health and Human Services (USDHHS). (2014).
The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General.
FORMS of TOBACCO n Cigarettesn Smokeless tobacco (chewing tobacco, oral snuff)n Pipesn Cigarsn Clove cigarettesn Bidisn Hookah (waterpipe smoking)n Electronic cigarettes (“e-cigarettes”)…
Image courtesy of the Centers for Disease Control and Prevention / Rick Ward
17
n Generally similar in appearance to cigarettes, cigars, pipes, or pens
n Battery-operated devices that create a vapor for inhalationn Simulates smoking but does not involve
combustion of tobaccon Also known as
n E-cigaretten E-hookah, Hookah pen n Vapes, Vape pen, Vape pipen Electronic nicotine delivery system (ENDS)
ELECTRONIC CIGARETTES
18
n Power source: Rechargeable/disposable battery
n Cartridge containing liquid solutionn Propylene glycoln Glycerinn Flavorings (tobacco, fruit, chocolate, mint, cola, candy, etc.)n Nicotine (0-36 mg/mL); Nicotine yield varies based on the
experience level of the usern Testing 32 cartridges, 9 showed differences between
labelled and detected nicotine concentrations larger than 20%; trace nicotine in three products labelled as nicotine-free (Goniewicz et al: NTR, 2013 and International Journal of Drug Policy, 2015)
n Electronic atomizer/vaporizern Heating element vaporizes liquid at temperatures 65-120 °C
ELECTRONIC CIGARETTES: Components
19
n Propylene glycol may cause respiratory irritation and increase the risk for asthma
n Glycerin may cause lipoid pneumonia on inhalationn Nicotine is highly addictive and can be harmful
n Refill cartridges with high concentrations of nicotine are a poisoning risk, especially in children
n Carcinogenic substances are found in some aerosolsn Use of e-cigarettes leads to emission of propylene glycol,
particles, nicotine, and carcinogens into indoor airn Long-term safety of second hand exposure to e-cigarette aerosols is
E-cigarettes: Youthn LA HS student study: Ever users compared with nonusers more likely
initiate combustible tobacco use over next year n 1/5 e-cigarette using adolescents use device to smoke cannabis oiln "Nicotine acts as a gateway drug on the brain, and this effect is likely to
occur whether the exposure is from smoking tobacco, passive tobacco smoke, or e-cigarettes" and concern that behavior is outpacing science (Kandel and Kandel NEJM 2014)
Morean et al., 2015 Pediatrics Rigotti, Jama 2015
21
Use routinely for cessation? Not based on current evidencen One Cochrane review investigating e-
cigarette for cessationn Combined, 2 studies suggest e-cigarette vs placebo
does have an effect on cessation BUT low gradeevidence (“Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate”)
n No difference in e-cigarette versus NRTn 2019 study in NEJM: 886 smokers randomized to e-
cigs or NRT; 1 year abstinence was 18.0% in e-cig compared to 9.9% NRT.
Bullen et al, Lancet 2013; Caponnetto et la, Plos One 2013; McRobbie, Cochrane Database 2015; Hajek P, et al. N Engl J Med. 2019
22
National Academies of Sciences, Engineering, and Medicine : Public Health Consequences of E-Cigarettes
There is conclusive evidence that:n E-cigarette use increases airborne concentrations of particulate matter and
nicotinen Exposure to nicotine from e-cigarettes is highly variablen Most e-cigarette products contain and emit numerous potentially toxic
substances… other than nicotine, the number, quantity, and characteristics of potentially toxic substances emitted from e-cigarettes are highly variable
n E-cigarette devices can explode and cause burns and projectile injuries. Such risk is significantly increased when batteries are of poor quality, stored improperly, or modified by users.
n Intentional or accidental exposure to e-liquids…can result in adverse health effects including…seizures, anoxic brain injury, vomiting, and lactic acidosis.
n Intentionally or unintentionally drinking or injecting e-liquids can be fatal. n Completely substituting e-cigarettes for combustible tobacco cigarettes reduces users’
exposure to toxicants and carcinogens present in combustible tobacco cigarettes.
23
Recommendationsn Newly regulated: FDA proposed to subject e-cigarettes to
regulatory oversight like other tobacco productsn FDA safety reports by consumers and health care professionals
have reported pneumonia, congestive heart failure, seizures, and hypertension in connection with use of these products
n >20 countries have banned e-cigarettesn AHA Summary Statement:
n Clinicians should not recommend e-cigarettes as primary cessation aidsn Also if patient has tried evidence based methods, it “is reasonable to
support the attempt.”n If a smoker is using e-cigarettes, consider quit date
n While harm reduction is still being researched, concern about youth, new users is very concerning
n Irritability/frustration/angernAnxietynDifficulty concentratingnRestlessness/impatiencenDepressed mood/depressionn Insomnian Impaired performancen Increased appetite/weight gainnCravings
NICOTINE PHARMACODYNAMICS: WITHDRAWAL EFFECTS
Hughes. (2007). Nicotine Tob Res 9:315–327.
Most symptoms manifest within the first 1–2 days,
peak within the first week, and subside within
2–4 weeks.
29
NICOTINE ADDICTION CYCLE
Reprinted with permission. Benowitz. (1992). Med Clin N Am 2:415–437.
30
ASSESSINGNICOTINE DEPENDENCE
Fagerström Test for Nicotine Dependence (FTND)n Developed in 1978 (8 items); revised in 1991 (6 items)
n Most common research measure of nicotine dependence; sometimes used in clinical practice
n Responses coded such that higher scores indicate higher levels of dependence
n Scores range from 0 to 10; score of greater than 5 indicates substantial dependence
Heatherton et al. (1991). British Journal of Addiction 86:1119–1127.
31
PHARMACOKINETIC DRUG INTERACTIONS with SMOKING
Drugs that may have a decreased effect due to induction of CYP1A2:§ Bendamustine § Haloperidol § Tasimelteon§ Caffeine § Olanzapine § Theophylline§ Clozapine § Riociguat§ Erlotinib § Ropinirole§ Fluvoxamine § Tacrine§ Irinotecan (clearance increased and systemic exposure decreased,
due to increased glucuronidation of its active metabolite)n HANDOUT ON RxForChange website
n Tobacco products are effective delivery systems for the drug nicotine.
n Nicotine is a highly addictive drug that induces a constellation of pharmacologic effects, including activation of the dopamine reward pathway in the brain.
n Clinically significant interactions result the combustion products of tobacco smoke, not from nicotine. Drug interactions should be considered clinically.
n Tobacco use is complex, involving the interplay of a wide range of factors.
n Treatment of tobacco use and dependence requires a multifaceted treatment approach.
33
ASSISTING PATIENTS with QUITTING
CLINICAL PRACTICE GUIDELINE for TREATING TOBACCO USE and DEPENDENCE
Sponsored by the U.S. Department of Health and Human Services, Public Heath Service with:
n Agency for Healthcare Research and Qualityn National Heart, Lung, & Blood Instituten National Institute on Drug Abusen Centers for Disease Control and Preventionn National Cancer Institute
34
EFFECTS of CLINICIAN INTERVENTIONS
0
10
20
30
No clinician Self-helpmaterial
Nonphysicianclinician
Physicianclinician
Type of Clinician
Estim
ated
abs
tinen
ce a
t 5+
mon
ths
1.0 1.11.7
2.2
n = 29 studies
Fiore et al. (2008). Treating Tobacco Use and Dependence: 2008 Update. Clinical Practice Guideline. Rockville, MD: USDHHS, PHS, May 2008.
With help from a clinician, the odds of quitting approximately doubles.
Compared to patients who receive no assistance from a clinician, patients who receive assistance are 1.7–2.2 times as likely to quit successfully for 5 or more months.
35
Esti
mat
ed a
bsti
nenc
e ra
te
at 5
+ m
onth
s0
10
20
30
None One Two Three or more
Number of Clinician Types
1.0
1.82.5 2.4
n = 37 studies
The NUMBER of CLINICIAN TYPES CAN MAKE a DIFFERENCE, too
Compared to smokers who receive assistance from no clinicians, smokers who receive assistance from two or more clinician types are 2.4–2.5 times as likely to quit successfully for 5 or more months.
Fiore et al. (2008). Treating Tobacco Use and Dependence: 2008 Update. Clinical Practice Guideline. Rockville, MD: USDHHS, PHS, May 2008.
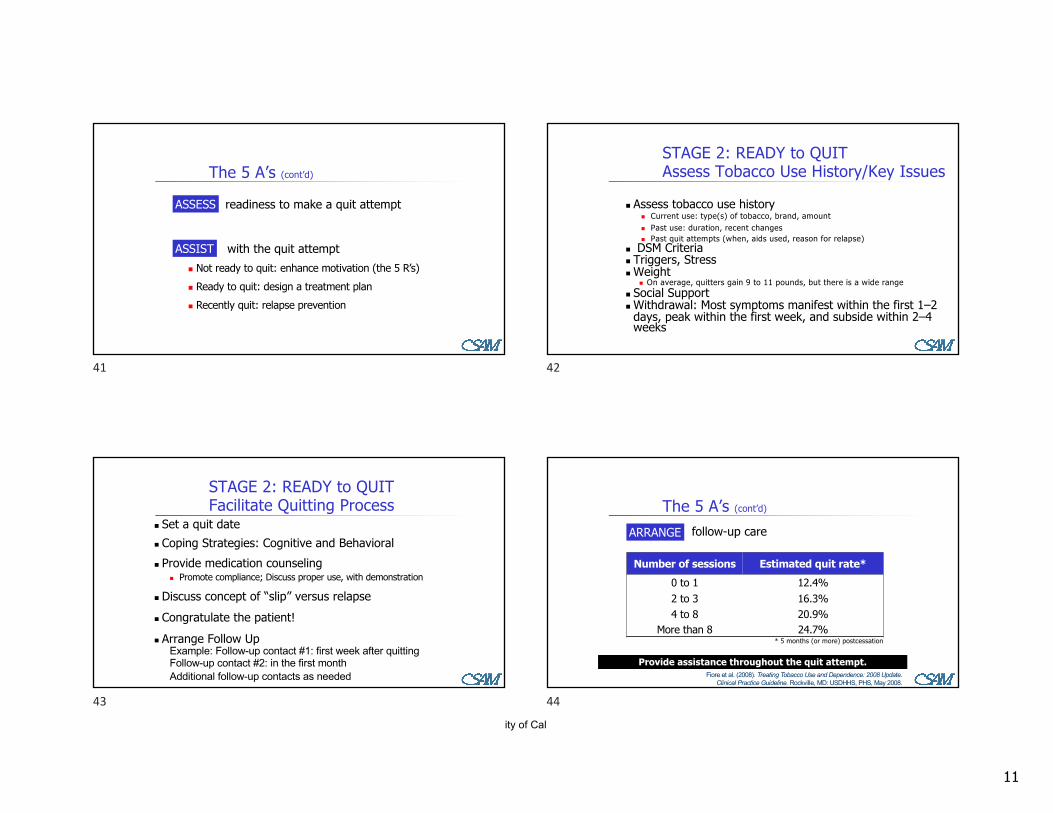
with the quit attemptn Not ready to quit: enhance motivation (the 5 R’s)n Ready to quit: design a treatment plann Recently quit: relapse prevention
ASSIST
41
STAGE 2: READY to QUITAssess Tobacco Use History/Key Issues
n Assess tobacco use historyn Current use: type(s) of tobacco, brand, amountn Past use: duration, recent changesn Past quit attempts (when, aids used, reason for relapse)
n DSM Criterian Triggers, Stressn Weight
n On average, quitters gain 9 to 11 pounds, but there is a wide rangen Social Supportn Withdrawal: Most symptoms manifest within the first 1–2
days, peak within the first week, and subside within 2–4 weeks
42
n Set a quit daten Coping Strategies: Cognitive and Behavioraln Provide medication counseling
n Promote compliance; Discuss proper use, with demonstration
n Discuss concept of “slip” versus relapsen Congratulate the patient! n Arrange Follow Up
Example: Follow-up contact #1: first week after quittingFollow-up contact #2: in the first monthAdditional follow-up contacts as needed
STAGE 2: READY to QUITFacilitate Quitting Process
43
follow-up careARRANGE
The 5 A’s (cont’d)
Number of sessions Estimated quit rate*0 to 1 12.4%2 to 3 16.3%4 to 8 20.9%
More than 8 24.7%* 5 months (or more) postcessation
Provide assistance throughout the quit attempt.Fiore et al. (2008). Treating Tobacco Use and Dependence: 2008 Update.
Clinical Practice Guideline. Rockville, MD: USDHHS, PHS, May 2008.
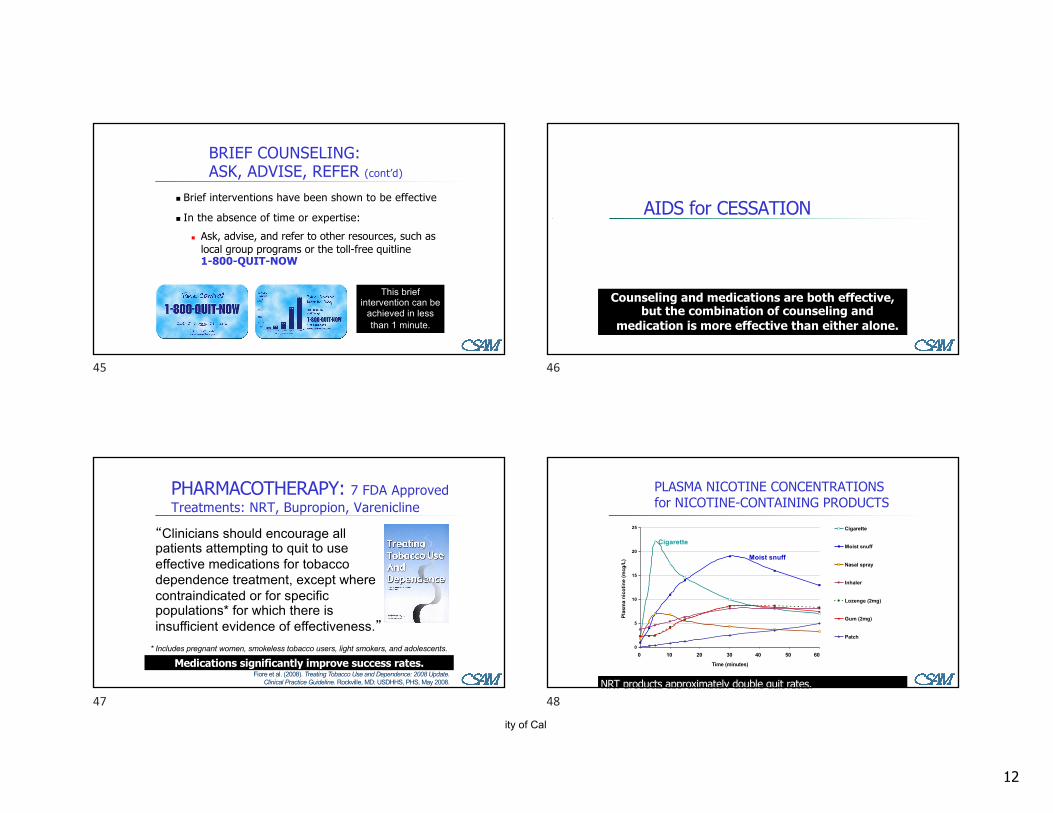
n Brief interventions have been shown to be effective
n In the absence of time or expertise:n Ask, advise, and refer to other resources, such as
local group programs or the toll-free quitline1-800-QUIT-NOW
BRIEF COUNSELING: ASK, ADVISE, REFER (cont’d)
This brief intervention can be
achieved in less than 1 minute.
45
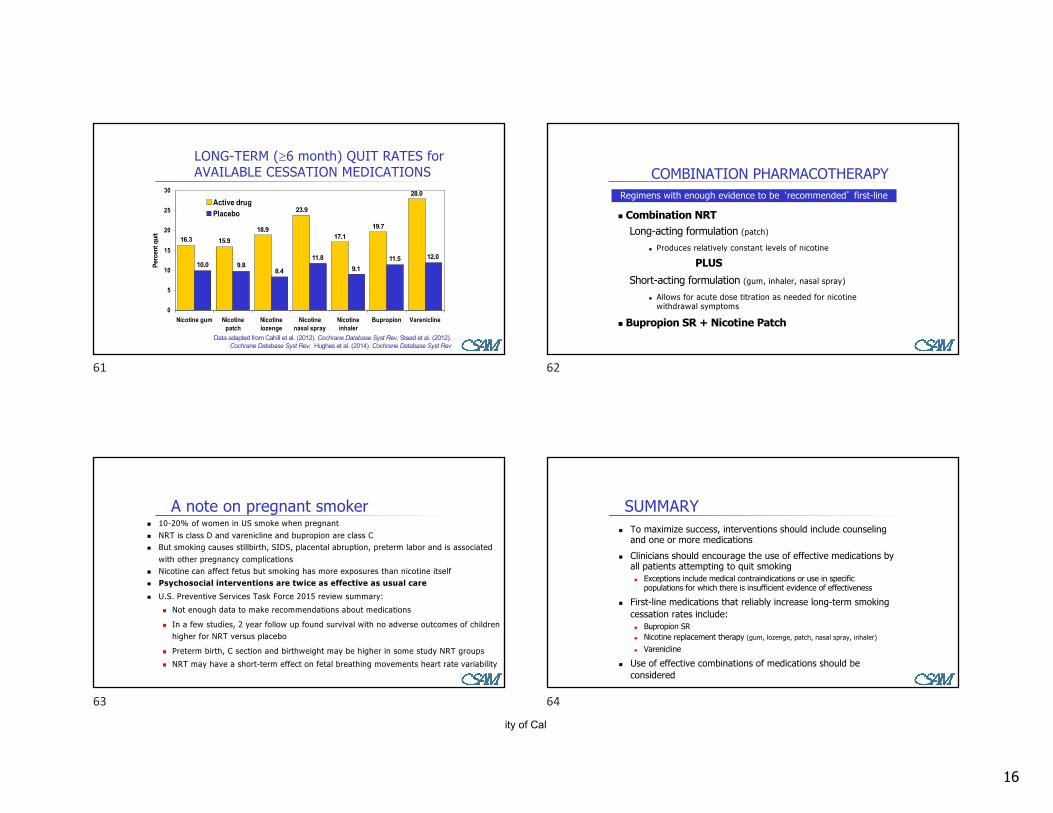
AIDS for CESSATION
Counseling and medications are both effective, but the combination of counseling and
medication is more effective than either alone.
46
PHARMACOTHERAPY: 7 FDA Approved Treatments: NRT, Bupropion, Varenicline
Fiore et al. (2008). Treating Tobacco Use and Dependence: 2008 Update. Clinical Practice Guideline. Rockville, MD: USDHHS, PHS, May 2008.
Medications significantly improve success rates.* Includes pregnant women, smokeless tobacco users, light smokers, and adolescents.
“Clinicians should encourage all patients attempting to quit to use effective medications for tobacco dependence treatment, except where contraindicated or for specific populations* for which there is insufficient evidence of effectiveness.”
47
PLASMA NICOTINE CONCENTRATIONS for NICOTINE-CONTAINING PRODUCTS
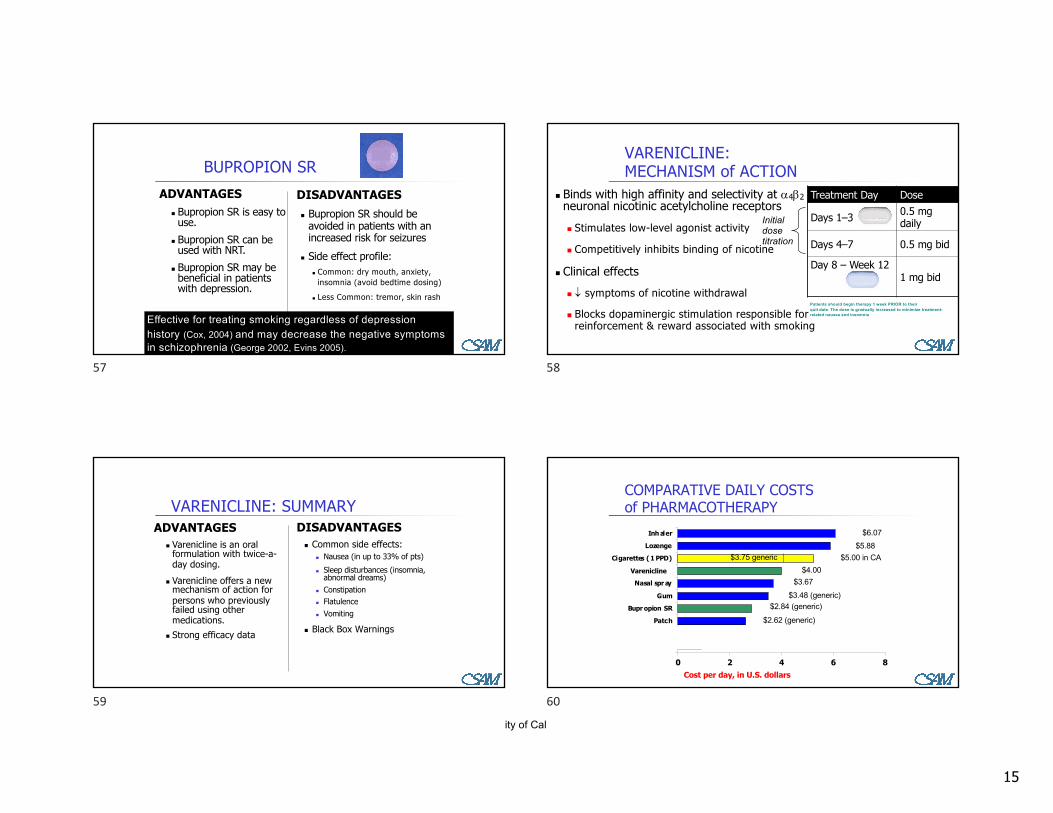
avoided in patients with an increased risk for seizures
n Side effect profile:n Common: dry mouth, anxiety,
insomnia (avoid bedtime dosing)
n Less Common: tremor, skin rash
ADVANTAGESn Bupropion SR is easy to use.
n Bupropion SR can be used with NRT.
n Bupropion SR may be beneficial in patients with depression.
Effective for treating smoking regardless of depression history (Cox, 2004) and may decrease the negative symptoms in schizophrenia (George 2002, Evins 2005).
57
VARENICLINE:MECHANISM of ACTION
n Binds with high affinity and selectivity at a4b2neuronal nicotinic acetylcholine receptorsn Stimulates low-level agonist activity
n Competitively inhibits binding of nicotine
n Clinical effectsn ¯ symptoms of nicotine withdrawal
n Blocks dopaminergic stimulation responsible for reinforcement & reward associated with smoking
Treatment Day Dose
Days 1–3 0.5 mg daily
Days 4–7 0.5 mg bid
Day 8 – Week 121 mg bid
Initial dose titration
Patients should begin therapy 1 week PRIOR to theirquit date. The dose is gradually increased to minimize treatment-related nausea and insomnia
58
VARENICLINE: SUMMARYDISADVANTAGES
n Common side effects:n Nausea (in up to 33% of pts)n Sleep disturbances (insomnia,
n Allows for acute dose titration as needed for nicotine withdrawal symptoms
n Bupropion SR + Nicotine Patch
Regimens with enough evidence to be ‘recommended’ first-line
62
A note on pregnant smokern 10-20% of women in US smoke when pregnantn NRT is class D and varenicline and bupropion are class Cn But smoking causes stillbirth, SIDS, placental abruption, preterm labor and is associated
with other pregnancy complicationsn Nicotine can affect fetus but smoking has more exposures than nicotine itselfn Psychosocial interventions are twice as effective as usual caren U.S. Preventive Services Task Force 2015 review summary:
n Not enough data to make recommendations about medications
n In a few studies, 2 year follow up found survival with no adverse outcomes of children higher for NRT versus placebo
n Preterm birth, C section and birthweight may be higher in some study NRT groupsn NRT may have a short-term effect on fetal breathing movements heart rate variability
63
SUMMARYn To maximize success, interventions should include counseling
and one or more medicationsn Clinicians should encourage the use of effective medications by
all patients attempting to quit smokingn Exceptions include medical contraindications or use in specific
populations for which there is insufficient evidence of effectiveness