Third-Party Payer Track Rx Drugs and Urine Testing: Knowing What’s Too Much, Too Little and Just Right Presenters: • Michael Gavin, President, PRIUM • Jo-Ellen Abou Nader, CFE, CIA, CRMA, Senior Director, Drug Waste Solutions, Express Scripts, Inc. • Elaine Jeter, MD, MolDX Medical Director, Palmetto GBA Moderator: Daniel Blaney-Koen, JD, Senior Legislative Attorney, American Medical Association Advocacy Resource Center, and Member, Rx Summit National Advisory Board
Transcript
Third-Party Payer Track
Rx Drugs and Urine Testing:Knowing What’s Too Much, Too
Drug Waste Solutions, Express Scripts, Inc.• Elaine Jeter, MD, MolDX Medical Director, Palmetto GBA
Moderator: Daniel Blaney-Koen, JD, Senior Legislative Attorney, American Medical Association Advocacy Resource Center, and Member, Rx Summit National Advisory Board
Disclosures
• Michael Gavin has disclosed no relevant, real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services.
• Jo-Ellen Abou Nader, CFE, CIA, CRMA, has disclosed no relevant, real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services.
• Elaine Jeter, MD, has disclosed no relevant, real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services.
• Daniel Blaney-Koen, JD, has disclosed no relevant, real or apparent personal or professional financial relationships with proprietary entities that produce health care goods and services.
Disclosures
• All planners/managers hereby state that they or their spouse/life partner do not have any financial relationships or relationships to products or devices with any commercial interest related to the content of this activity of any amount during the past 12 months.
• The following planners/managers have the following to disclose:– Kelly Clark – Employment: Publicis Touchpoint Solutions;
Consultant: Grunenthal US– Robert DuPont – Employment: Bensinger, DuPont &
Associates-Prescription Drug Research Center– Carla Saunders – Speaker’s bureau: Abbott Nutrition
Learning Objectives
1. Describe how the PBM identifies, investigates and resolves Rx fraud, waste and abuse.
2. Compare appropriate with fraudulent and wasteful usage of UDT.
3. Advocate strategies that optimize usage of UDT.
Urine Drug Monitoring
Too Much or Too Little
Michael Gavin wishes to disclose he is the President of PRIUM, a wholly-owned subsidiary of Ameritox. He will present this content in a fair and balanced manner.
Disclosure 6
This presentation:
1. Outlines the care settings and technologies used for urine drug monitoring
2. Illustrates the clinical rationale for urine drug monitoring
3. Examines why appropriate testing does not always occur
Learning
Objectives
7
• Industry Context
• Data and Observations
• Best Practices
Agenda8
Societal
BurdenMisuse and abuse of prescription drugs is hugely expensive from a financial and socioeconomic perspective
• In the United States, prescription opioid abuse costs were about $55.7 billion in 2007.1 Of this amount, 46% was attributable to workplace costs, 45% to healthcare costs, and 9% to criminal justice costs.
• Drug overdose was the leading cause of injury death in 2012. Among people 25 to 64 years old, drug overdose caused more deaths than motor vehicle traffic crashes.2
• The drug overdose death rate has more than doubled from 1999 through 2013.3
1. Birnbaum HG, White AG, Schiller M, Waldman T, Cleveland JM, and Roland CL. Societal costs of prescription opioid abuse, dependence, and misuse in the United
States. Pain Medicine 2011; 12: 657-667
2. Centers for Disease Control and Prevention. Web-based Injury Statistics Query and Reporting System (WISQARS) [online]. (2014) Available from URL:
http://www.cdc.gov/injury/wisqars/fatal.html.
3. Centers for Disease Control and Prevention. National Vital Statistics System mortality data. (2015) Available from URL: http://www.cdc.gov/nchs/deaths.htm.
Est. Device Cost <$10 <$30,000 ~$295,000-$690,000 ~$200,000 - $400,000
Results & Reliability Qualitative result
Detects drug class
Low to moderate degree
of reliability(1)
Qualitative result
Typically detects drug
class(2)
Moderate to high degree
of reliability
Quality highly variable
Qualitative results
Detects drug class
High degree of reliability
FDA approve Reagent
kits
95% confidence level
Quantitative (ng / mL)
result
Detects specific
compound
High degree of reliability
Lab Certification CLIA-waiver CLIA certificate –
Moderate complexity lab
CLIA certificate –
Moderate complexity lab
Rigorous lab audits
Requires moderate to
highly trained personnel
CLIA certificate – High
complexity lab
Rigorous lab audits
Requires highly trained
personnel1. In a recent comparison of POCT and confirmation results performed by Ameritox POCT devices produced an incorrect result over 50% of the time.
2. Assays exist for some specific compounds.
Not Created
EqualNot all testing technologies and settings are created equal; the quality and quantity of data differs by setting.
6
Why Monitor?Urine drug monitoring informs clinical decision making by prompting new conversations between doctors and patients.
What Drug Monitoring Tells Us
• Presence of prescribed substances• Identification of non-prescribed
substances• Identification of illicits• Uncover possible misuse/abuse and
cross-reactivity risk
What Drug Monitoring Doesn’t Tell Us
• The amount of drug ingested or taken
• When last dose was taken• Source of the medication.• Proof of misuse/abuse
11
Longitudinal
AnalysisThe availability of information to assist with assessing likely adherence over time is of critical importance in light of chronic opioid therapy.
12
MEDs1 Rx Spend2
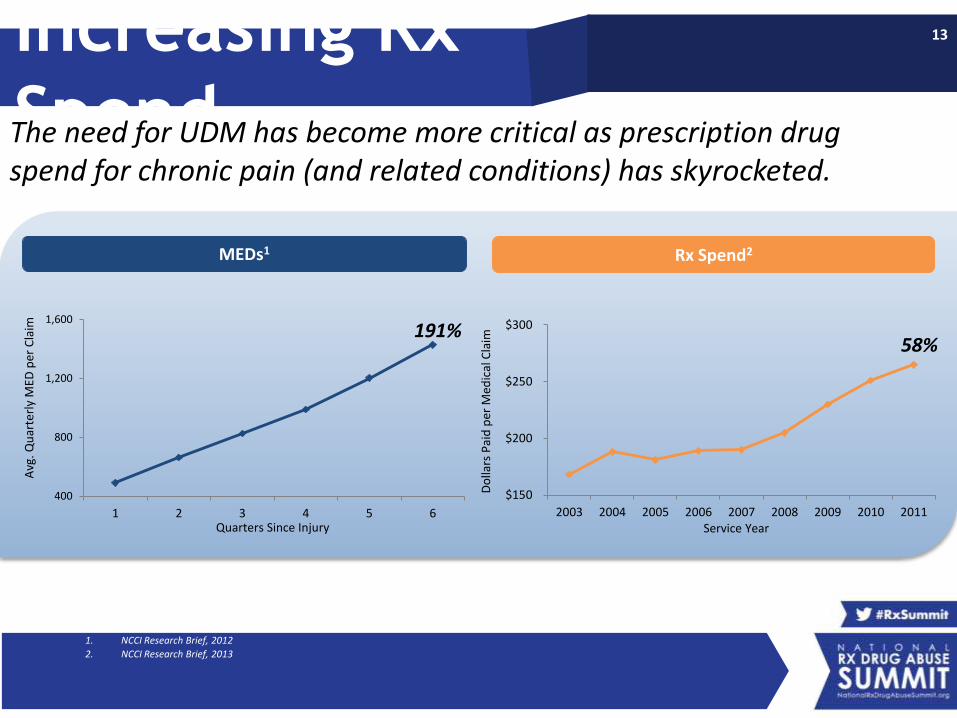
191%
400
800
1,200
1,600
1 2 3 4 5 6
Avg
. Qu
arte
rly
MED
per
Cla
im
Quarters Since Injury
58%
$150
$200
$250
$300
2003 2004 2005 2006 2007 2008 2009 2010 2011
Do
llars
Pai
d p
er M
edic
al C
laim
Service Year
Increasing Rx
SpendThe need for UDM has become more critical as prescription drug spend for chronic pain (and related conditions) has skyrocketed.
1. NCCI Research Brief, 2012
2. NCCI Research Brief, 2013
13
Observations
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%
40.00%
45.00%
Illicits Found Rx Not Found Found, No Rx
Overall Testing Results Over Time
2006 2007 2008 2009 2010 2011 2012 2013 2014
Many samples show multiple issues; just 33.9% of samples show no abnormalities.
14
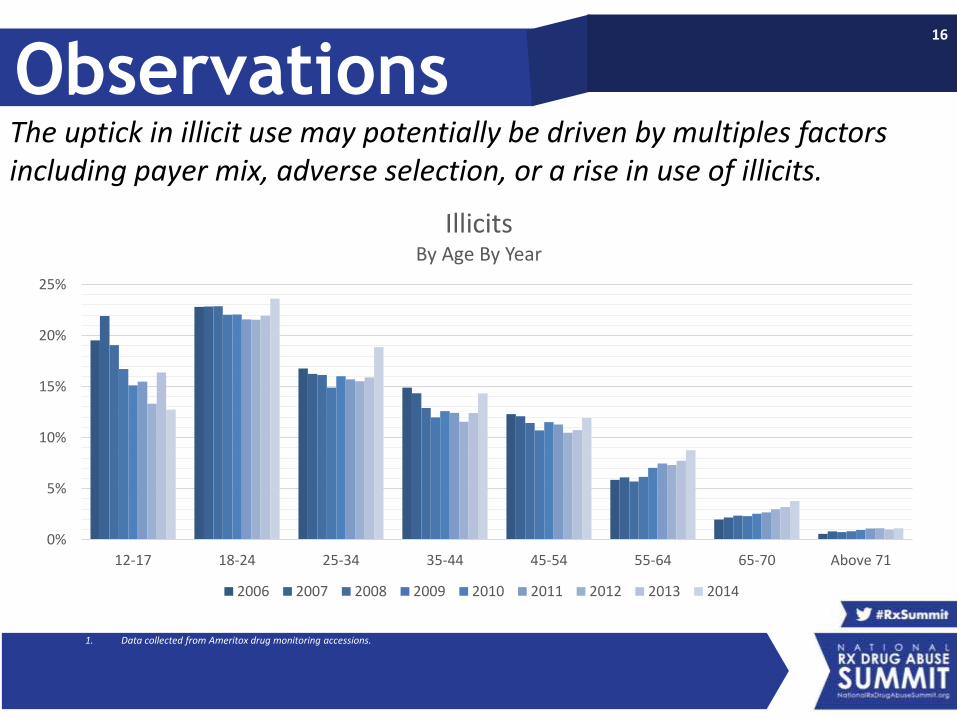
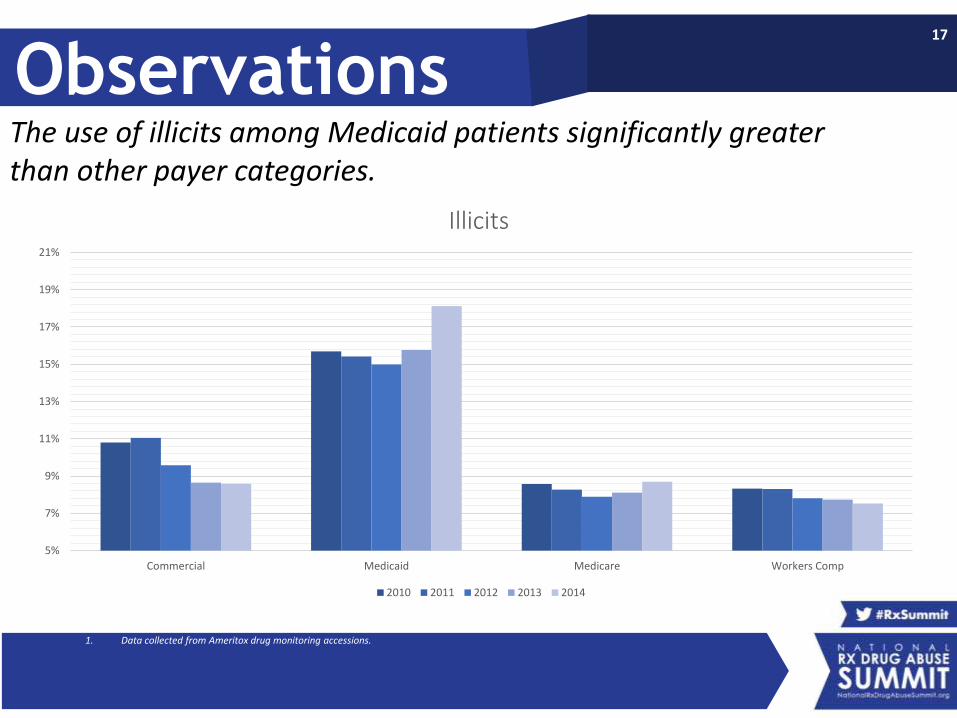
1. Data collected from Ameritox drug monitoring accessions.
Observations
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%
40.00%
Illicits Rx Not Found Found, No Rx
Overall Testing Results by Age
12-17 18-24 25-34 35-44 45-54 55-64 Above 65
Despite the declination of illicit medications with age, adherence does not follow this same trend – even beyond 65.
15
1. Data collected from Ameritox drug monitoring accessions.
ObservationsThe uptick in illicit use may potentially be driven by multiples factors including payer mix, adverse selection, or a rise in use of illicits.
MediumArkansas, Illinois, Kentucky, Louisiana, Massachusetts, Montana, Nevada, New York, North Dakota, Ohio, Oklahoma,Utah, Washington, West Virginia, Wyoming
WeakColorado, Connecticut, DC, Delaware, Georgia, Indiana,Maine, New Hampshire, New Mexico, North Carolina, Pennsylvania
None
Alaska, Arizona, Hawaii, Idaho, Iowa, Kansas, Maryland, Michigan, Minnesota, Missouri, Nebraska, New Jersey, Oregon, Rhode Island, South Carolina, South Dakota, Vermont, Virginia, Wisconsin
Utilization review is the evaluation of medical necessity, appropriateness, and reasonableness of medical treatment.
27
Coordinated
InterventionsManaged care tools are all essential components to ensuring compliance with medication regimens.
Drug Waste Solutions, Express Scripts, Inc.• Elaine Jeter, MD, MolDX Medical Director, Palmetto GBA
Moderator: Daniel Blaney-Koen, JD, Senior Legislative Attorney, American Medical Association Advocacy Resource Center, and Member, Rx Summit National Advisory Board