4
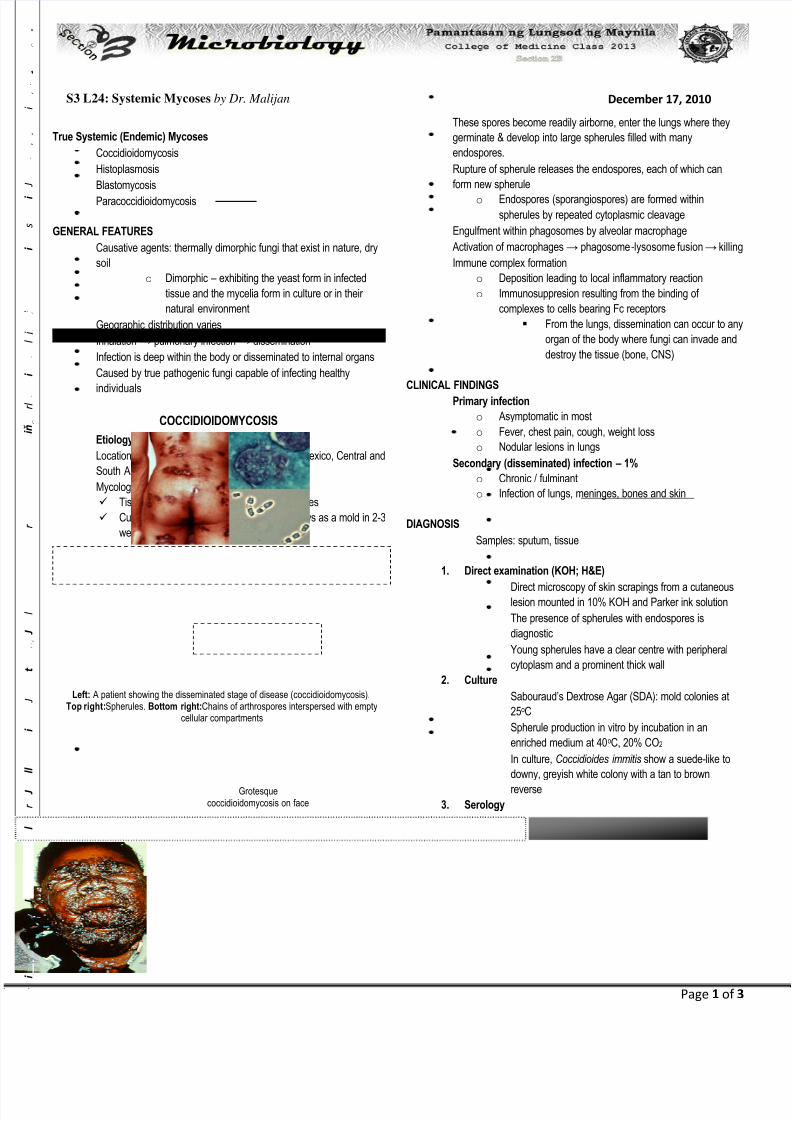
Page 1 of 3 S3 L24: Systemic Mycoses by Dr. Malijan December 17, 2010 True Systemic (Endemic) Mycoses Coccidioidomycosis Histoplasmosis Blastomycosis Paracoccidioidomycosis GENERAL FEATURES Causative agents: thermally dimorphic fungi that exist in nature, dry soil o Dimorphic – exhibiting the yeast form in infected tissue and the mycelia form in culture or in their natural environment Geographic distribution varies Inhalation → pulmonary infection → dissemination Infection is deep within the body or disseminated to internal organs Caused by true pathogenic fungi capable of infecting healthy individuals Etiology: Coccidioides immitis Location: confined to southwestern US, northern Mexico, Central and South America Mycology: Tissue (37 o C): spherules filled with endospores Cultured on Sabouraud’s agar at 25 o C: grows as a mold in 2-3 weeks; hyphae, barrel-shaped arthroconidia PATHOGENESIS In the soil, the fungus generates spores by septation of hyphal filaments (arthrospores / arthroconidia) These spores become readily airborne, enter the lungs where they germinate & develop into large spherules filled with many endospores. Rupture of spherule releases the endospores, each of which can form new spherule o Endospores (sporangiospores) are formed within spherules by repeated cytoplasmic cleavage Engulfment within phagosomes by alveolar macrophage Activation of macrophages → phagosome -lysosome fusion → killing Immune complex formation o Deposition leading to local inflammatory reaction o Immunosuppresion resulting from the binding of complexes to cells bearing Fc receptors From the lungs, dissemination can occur to any organ of the body where fungi can invade and destroy the tissue (bone, CNS) CLINICAL FINDINGS Primary infection o Asymptomatic in most o Fever, chest pain, cough, weight loss o Nodular lesions in lungs Secondary (disseminated) infection – 1% o Chronic / fulminant o Infection of lungs, meninges, bones and skin DIAGNOSIS Samples: sputum, tissue 1. Direct examination (KOH; H&E) Direct microscopy of skin scrapings from a cutaneous lesion mounted in 10% KOH and Parker ink solution The presence of spherules with endospores is diagnostic Young spherules have a clear centre with peripheral cytoplasm and a prominent thick wall 2. Culture Sabouraud’s Dextrose Agar (SDA): mold colonies at 25 o C Spherule production in vitro by incubation in an enriched medium at 40 o C, 20% CO2 In culture, Coccidioides immitis show a suede-like to downy, greyish white colony with a tan to brown reverse 3. Serology Latex agglutination Complement fixation 4. Skin test (coccidioidin and spheruline antigens) TREATMENT Symptomatic treatment only (primary infection) Severe disease: o Amphotericin B o Itraconazole o Fluconazole (particularly for meningitis) Grotesque coccidioidomycosis on face Left: A patient showing the disseminated stage of disease (coccidioidomycosis). Top right:Spherules. Bottom right:Chains of arthrospores interspersed with empty cellular compartments COCCIDIOIDOMYCOSIS i i I J l r J l l i J t J l i i i r i ň r l i l i i . i s i J i