Safe and Appropriate Use of Opiates David Wensel, DO, FAAHPM Medical Director, Midland Care [email protected]Kevin T. Bain, PharmD, MPH, BCPS, BCGP, CPH, FASCP Vice President of Medication Risk Mitigation, CareKinesis [email protected]Robert Alesiani, PharmD, BCGP Chief Pharmacotherapy Officer, CareKinesis [email protected]NPA Annual Conference 2017 October 18, 2017
At the end of this webinar, participants should be able to:• Understand the risks associated with opiate drug therapy in
the elderly population• Learn and understand safe and effective pain management
practices with opiates• Ascertain best practice for starting and ending opiate therapy
using evidence-based tools• Know which medications are available for older adults, which
may have pharmacogenomic implications, and how to utilize pharmacogenomic information to assure medication safety and effectiveness
• Access resources to guide clinicians2
Opioid-Related Drug InteractionsEpidemic
“The crisis of opioid addiction is a public health tragedy of enormous proportions. We need to confront it like any explosive epidemic.”- Remarks by Scott Gottlieb, MD, U.S. FDA Commissioner on
July 10, 2017 during the FDA’s Scientific Meeting on Opioids
Opioid Epidemic
Volkow ND, et al. N Engl J Med. 2014;370(22):2063-6.Jones CM, et al. JAMA. 2013;309(7):657-9.
4
The rate of death from ODs of prescription opioids in the United
States more than quadrupled between 1999 and 2010, far
exceeding the combined death toll from cocaine & heroin ODs
It is estimated that almost 80% of opioid-related overdose deaths are
considered accidental or unintentional
Due, in part, to DRUG INTERACTIONS
Case VignetteIntroduction
Opioid Pain Management CaseBackground
J.D. is an 84-year old male with post-surgical repair of spinal stenosis (L1-L2).
His PMH includes chronic, non-cancer pain with comorbid depression, HTN, COPD, and Diabetes Type II. He has NKDA.
Following surgery, he was started on tramadol by the pain management specialist• Tramadol 50mg: Take 1 to 2 tablets every 4 to 6 hours as
needed for pain
8
Opioid Pain Management CaseBackground
During his follow-up visit with PACE (PCP) approximately a week later, it was evident that he failed to achieve an adequate response and exhibited intolerable side effects with tramadol
• J.D. stated that he tried tramadol 50mg for 2 days but has been taking tramadol 100mg every 4 hours while awake for the past 5 days with only a small reduction in his pain (7/10 at best)
• He also expressed that he has been experiencing nausea, constipation, and dizziness
9
Opioid Pain Management CaseCurrent Medication History
His PCP changes tramadol to hydrocodone/APAPHis current medication profile is as follows:• Hydrocodone/acetaminophen 5/325 mg every 4 hours PRN
pain – NEW
• Senna-S 2 tablets daily – NEW
• Sertraline 50 mg/day
• Metoprolol succinate 50 mg/day
• Hydrochlorothiazide 25 mg/day
• Beclomethasone 80 mcg/inhalation twice daily
• Albuterol MDI 2 puffs every 4 hours as needed10
Unchanged
To Be Continued…
Opioid Pain Management
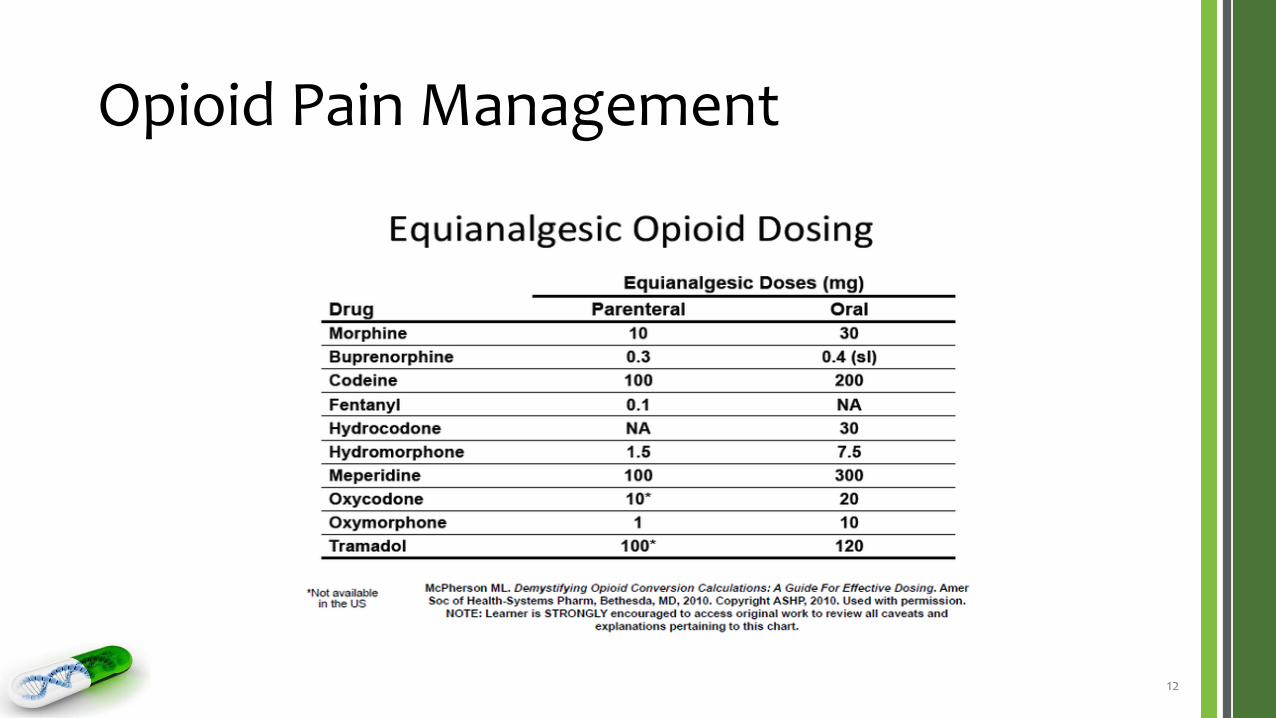
• How potent is Hydrocodone compared to other opioids?
• Look for Equianalgesic table
• When switching from one opioid to another, reduce dose by 25% to account for cross tolerance
• Always start low and go slow
11
Opioid Pain Management
12
Opioid Pain Management
• Need to consider how the opioid will be metabolized and excreted
• Opioids are primarily metabolized by CYP2D6
• 2 exceptions are Fentanyl and Methadone
• Both are highly lipophilic
• Need to consider medications that compete for the same enzymes
13
Opioid Pain Management
• The number one side effect of all Opioids is
• CONSTIPATION not respiratory suppression
• Always write a prescription for Senna when you prescribe any opioid
• Must think of improving peristalsis to treat constipation
14
Opioid-Related Drug InteractionsPharmacodynamic Mechanisms
Respiratory Depression & Sedation
• Action-related (respiratory effects)• Concomitant administration with drugs that cause respiratory depression
• Exemplar drugs that cause respiratory depression:• Benzodiazepines (e.g. Diazepam [Valium®])
• Use of opioids in patients with conditions accompanied by hypoxia, hypercapnia, or decreased respiratory reserve• COPD, cor pulmonale, morbid obesity
• Action-related (CNS effects)• Concomitant administration with drugs that cause CNS depression
Opioid-Related Drug InteractionsPharmacogenomic (PGx) Mechanisms
28
Impact of Genetic VariationsDrug-Gene Interactions
How genetic variations affect drug disposition & response
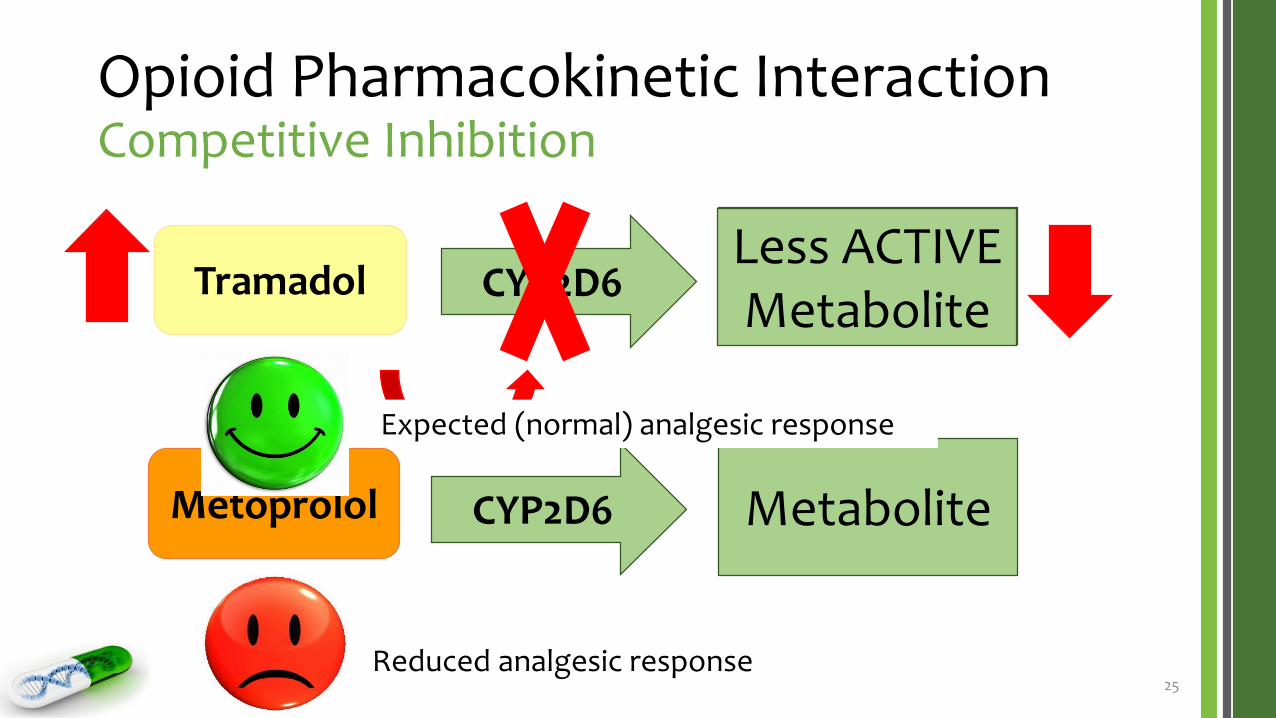
PhenoconversionCompetitive Inhibition
29
Metabolite
Drug D CYP2D6 Metabolite
Drug X CYP2D6
PhenoconversionNon-Competitive Inhibition
30
Drug XLess Active Metabolite
CYP2D6
Paroxetine
*1|*1 = Normal Metabolizer (NM)*1|*1 = Poor Metabolizer (PM)
Patients treated with both Paroxetine and Drug X may be phenoconverted into a poor
metabolizer of Drug X.
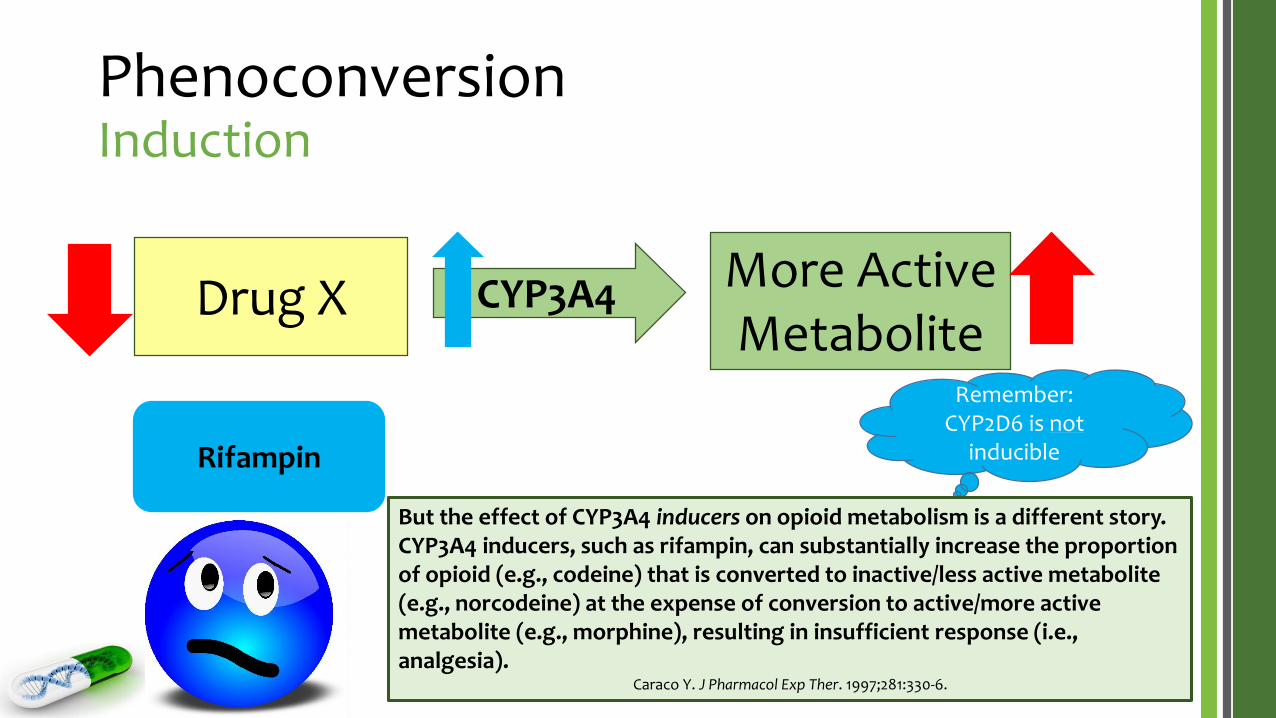
PhenoconversionInduction
31
Drug XMore Active Metabolite
CYP3A4
Rifampin
*1|*1 = Normal Metabolizer (NM)*1|*1 = Ultra-rapid Metabolizer (UM)
Patients treated with both Rifampin and Drug X may be phenoconverted into an ultra-rapid
metabolizer of Drug X.
Remember: CYP2D6 is not
inducible
But the effect of CYP3A4 inducers on opioid metabolism is a different story. CYP3A4 inducers, such as rifampin, can substantially increase the proportion of opioid (e.g., codeine) that is converted to inactive/less active metabolite (e.g., norcodeine) at the expense of conversion to active/more active metabolite (e.g., morphine), resulting in insufficient response (i.e., analgesia).
Caraco Y. J Pharmacol Exp Ther. 1997;281:330-6.
32
Drug-Gene Interaction Examples
Clinical Relevance Citations:Poulsen L. Eur J Clin Pharmacol. 1996;51:289-95.Gasche Y. N Engl J Med. 2004;351:2827-31.Ciszkowski C. N Engl J Med. 2009;361:827-8. Argoff CE. Clin J Pain. 2010;26:S16-S20.Lurcott G. Anesth Prog. 1998;45:154-6.
Opioids
33
Opioid CYP2D6 CYP3A4 CYP2B6
Codeine 5%* 10%
Morphine NON P450
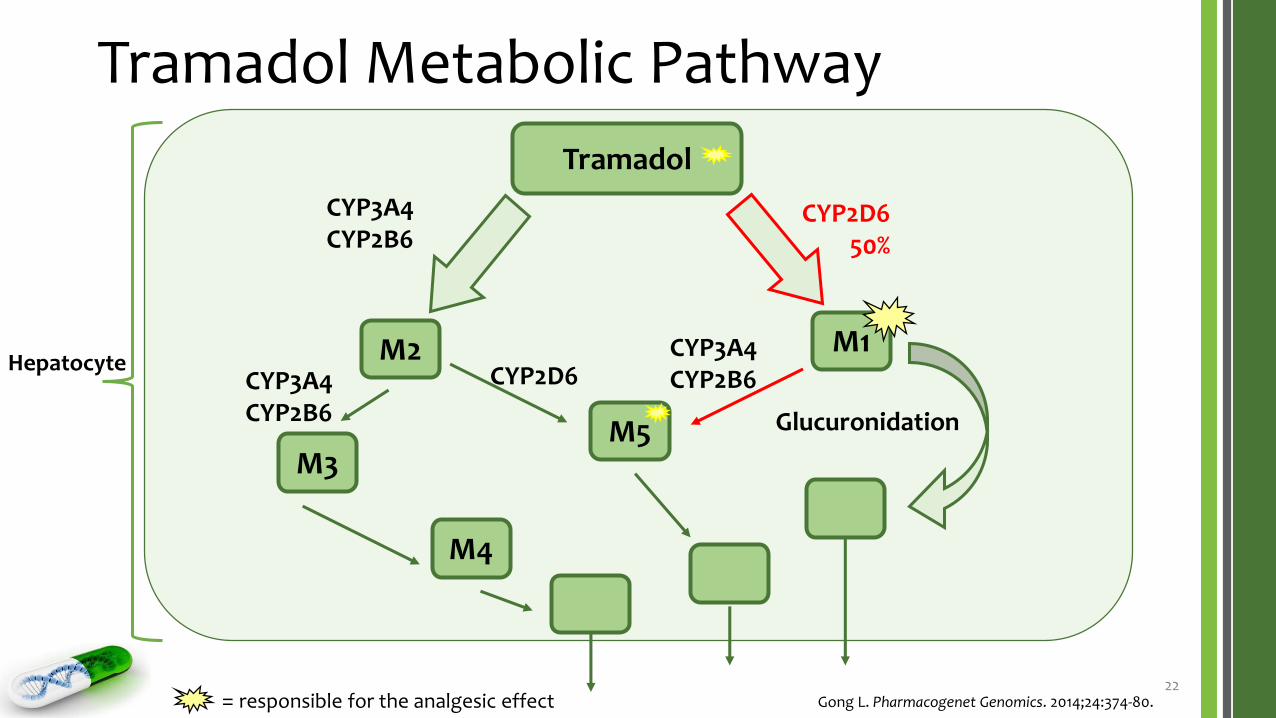
Tramadol 50% 10% 10%
Oxycodone 15%* 30%
Oxymorphone NON P450
Hydrocodone 10%* 55%
Hydromorphone NON P450
Fentanyl 90%
Methadone 10% 50%
Tapentadol 25%
Dihydrocodeine 25%
https://www.intermedrx.com/* = Pro-drug or drug that is converted to a more active metabolite
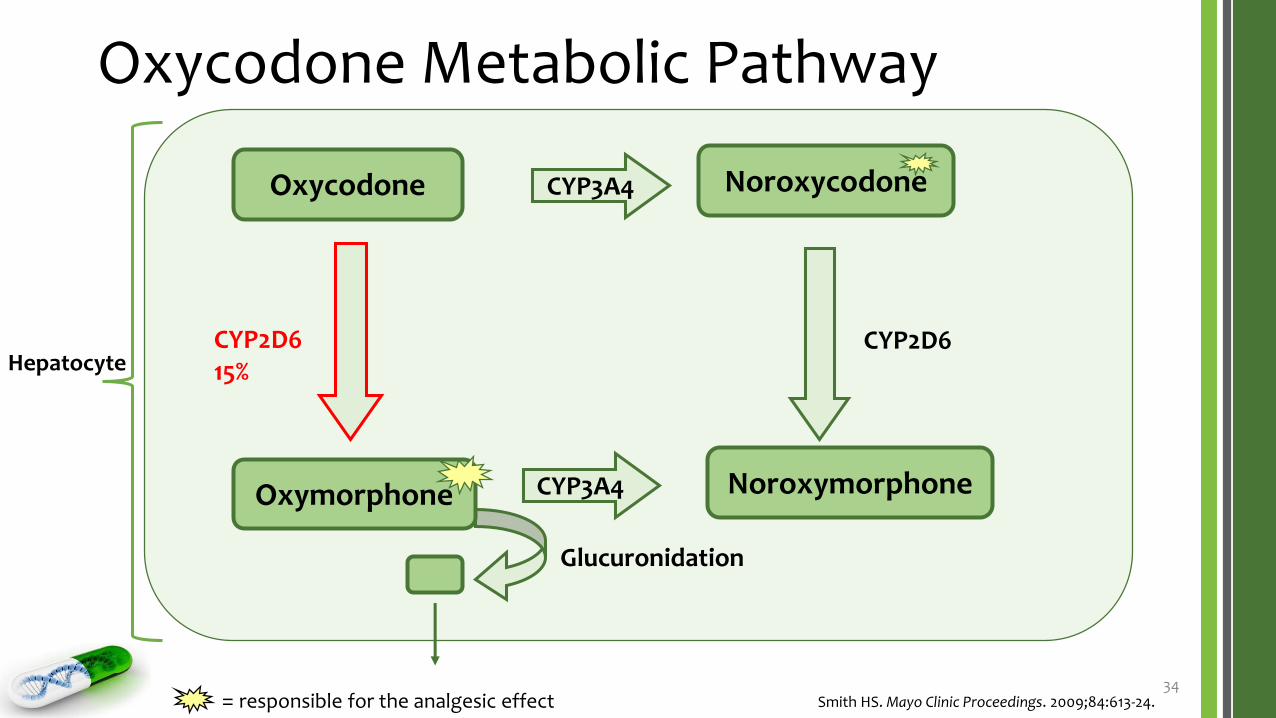
Oxycodone Metabolic Pathway
34
Oxycodone
CYP2D615%
Glucuronidation
Hepatocyte
Smith HS. Mayo Clinic Proceedings. 2009;84:613-24.
CYP3A4 Noroxycodone
NoroxymorphoneOxymorphone
CYP2D6
CYP3A4
= responsible for the analgesic effect
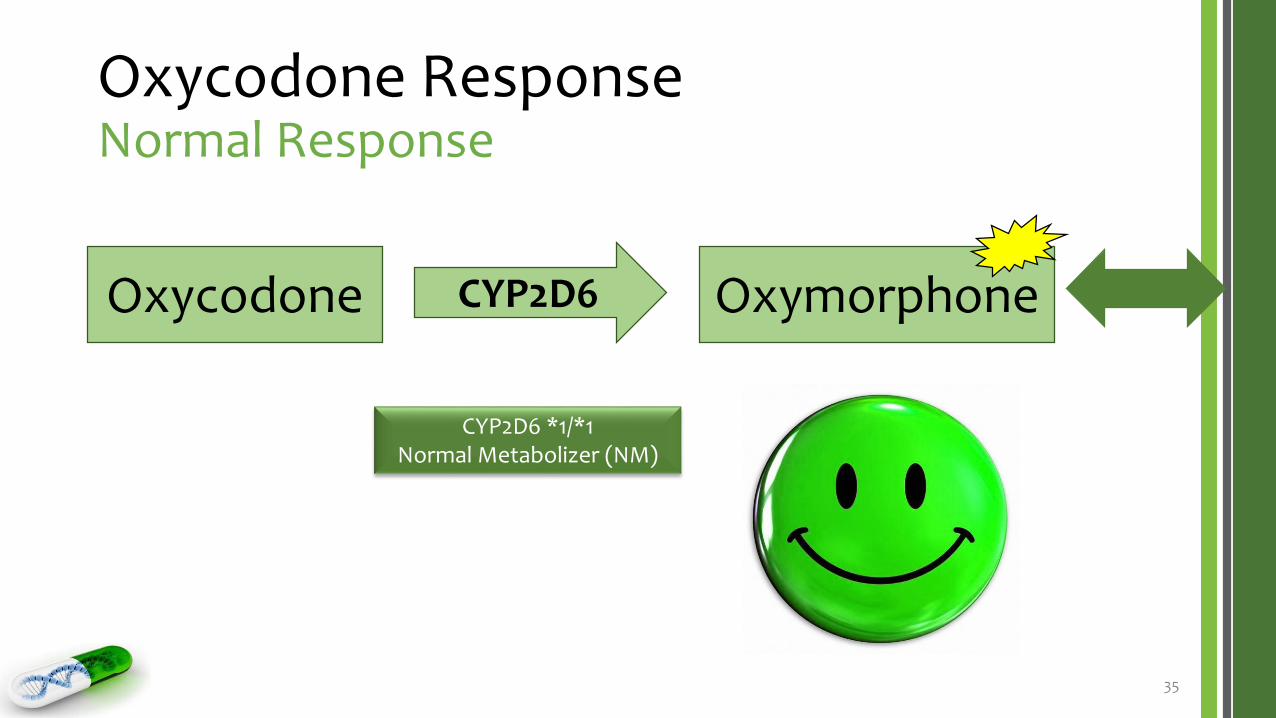
Oxycodone ResponseNormal Response
35
Oxycodone OxymorphoneCYP2D6
CYP2D6 *1/*1Normal Metabolizer (NM)
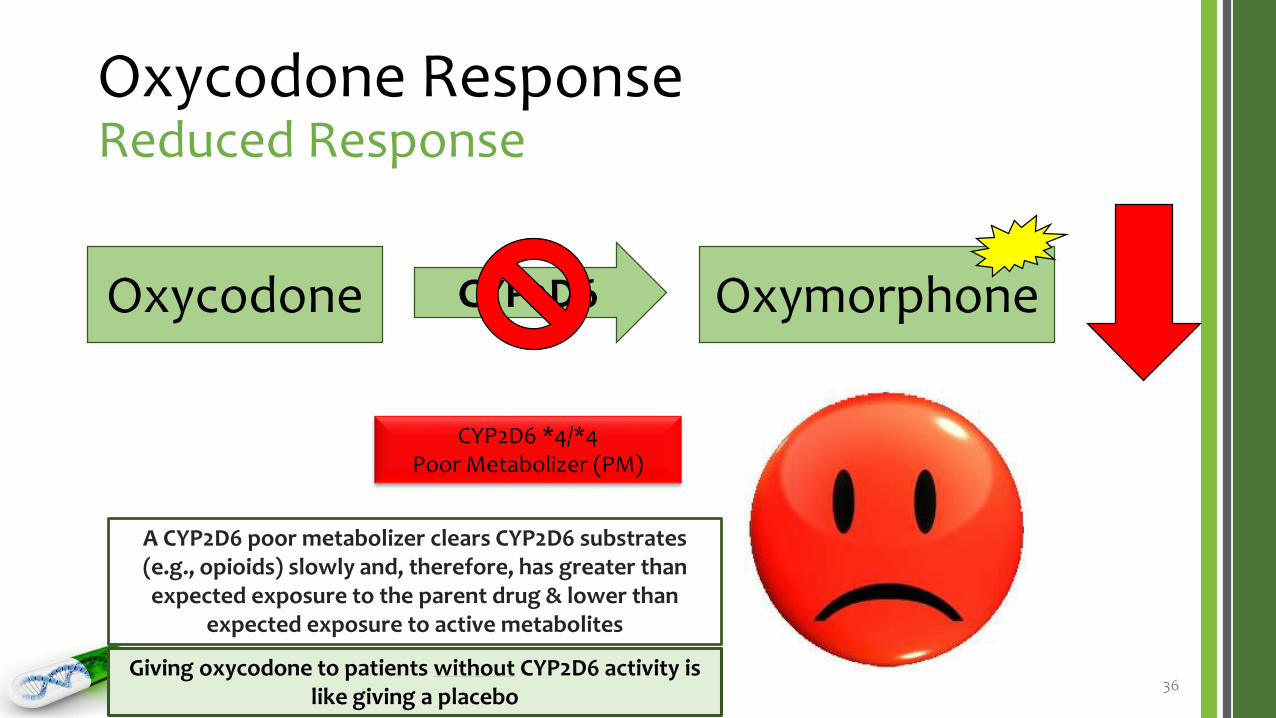
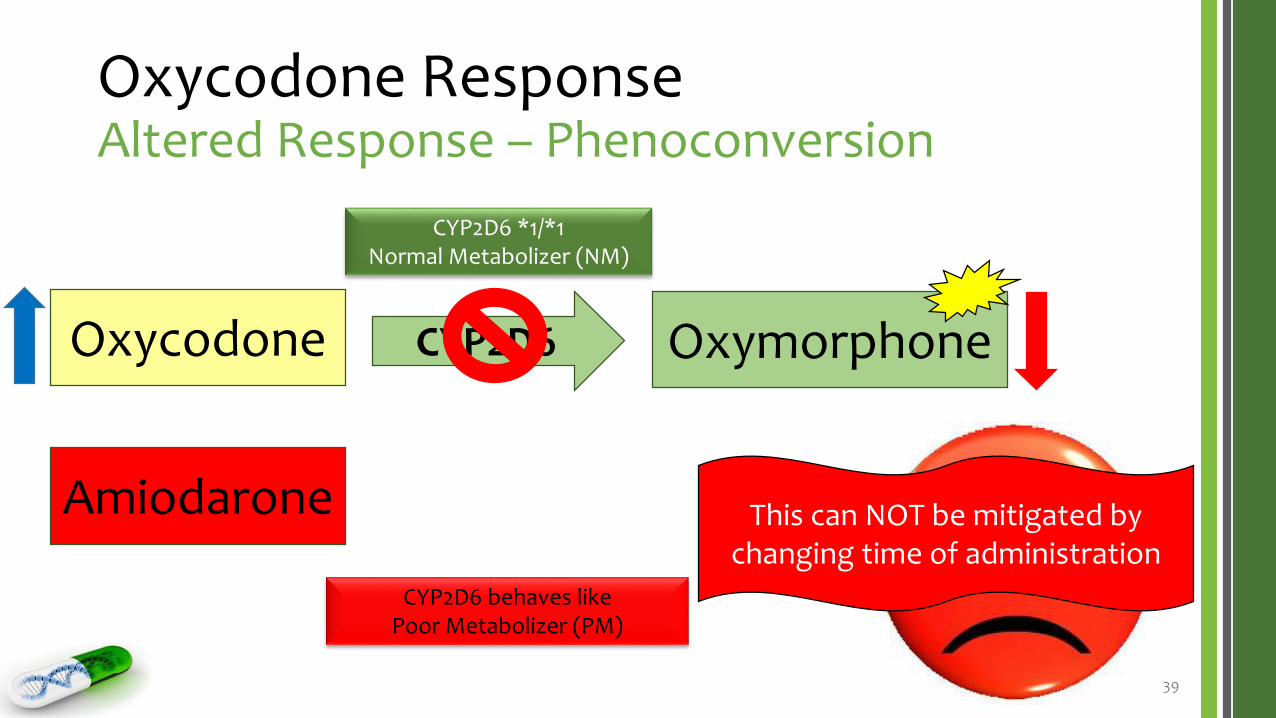
Oxycodone ResponseReduced Response
36
Oxycodone OxymorphoneCYP2D6
CYP2D6 *4/*4Poor Metabolizer (PM)
A CYP2D6 poor metabolizer clears CYP2D6 substrates (e.g., opioids) slowly and, therefore, has greater than expected exposure to the parent drug & lower than
expected exposure to active metabolites
Giving oxycodone to patients without CYP2D6 activity is like giving a placebo
Opioid Pain Management CaseScenario 1J.D. continues taking the hydrocodone/acetaminophen 10/325 mg as prescribed, with mild to modest analgesic response• Takes 1 tablet 4-5 times per day
• Best 4-5/10 pain score on Likert scale
• Most improvement at night
After several days, he calls his PCP to report that his analgesic response, and reports that his nausea & constipation is mitigated & his dizziness has improved
Unsuspecting of a drug-drug interaction, his PCP orders a PGx test to determine his CYP2D6 genotype-phenotype status• His result comes back as follows: CYP2D6*1/*1 – normal metabolizer (NM)
• Oxycodone immediate-release 5 mg every 4 to 6 hours PRN breakthrough pain
The PCP also adds pregabalin for potential nerve pain
• Pregabalin 50 mg at bedtime x 3 days then 50 mg twice daily
J.D. begins taking his new prescriptions the following day46
What should we expect?
Opioid Pain Management CaseExplained – Oxycodone
47To Be Continued…
Case VignetteApplied Mitigating Strategies
Opioid Pain Management CaseScenario 3A week and a half later, J.D. calls his PCP to report that his pain control is relatively unchanged & that he tried taking the pregabalin twice daily but could not tolerate it because of fogginess & daytime sleepiness
After consulting with the pharmacist that rotates in his practice, the PCP recognizes that J.D. is suffering from multiple drug interactions• Oxycodone & pregabalin – sedation
He also realizes that J.D. has become physically & possibly psychologically addicted to opioids
The PCP decides to stop the pregabalin and switch the metoprolol to atenolol• Atenolol 50 mg/day
49What should we expect?
Opioid Pain Management CaseExplained – Oxycodone
50To Be Continued…
Opioid Pain Management CaseScenario 4
Several days after changing from metoprolol to atenolol, J.D.’s wife calls 9-11
• She found J.D. slumped over in his chair and difficult to arouse
J.D. is brought to the emergency department for urgent care
51
What could have been done differently?
Opioid Pain Management CaseScenario 4 (cont.)
When changing to atenolol, the PCP should have reduced the oxycodone dosage
• J.D. was not fully metabolizing the previous opioids and, therefore, the concentrations were lower than expected
• However, when the competitive inhibition was mitigated, the opioid concentrations rose, and this occurred over several days (due to relatively high bioavailability of oxycodone)
52
What could have been done differently?
Why?
Opioid Pain Management CaseScenario 4 (cont.)
Instead of changing metoprolol to atenolol, the PCP could have changed the oxycodone to morphine or oxymorphone
• These opioids do not undergo metabolism by the CYP2D6 isoenzyme
• In doing so, still, the estimated conversion should be significantly reduced (50-75%) to account for incomplete cross-tolerance (i.e., treat J.D. like he is opioid naïve)
53
What could have been done differently?
Why?
Improving Opioid PrescribingTreatment of Opioid-Use Disorder (OUD)
A psychiatric diagnosis that involves use despite negative consequences and/or loss of control over
use, compulsion, and cravings
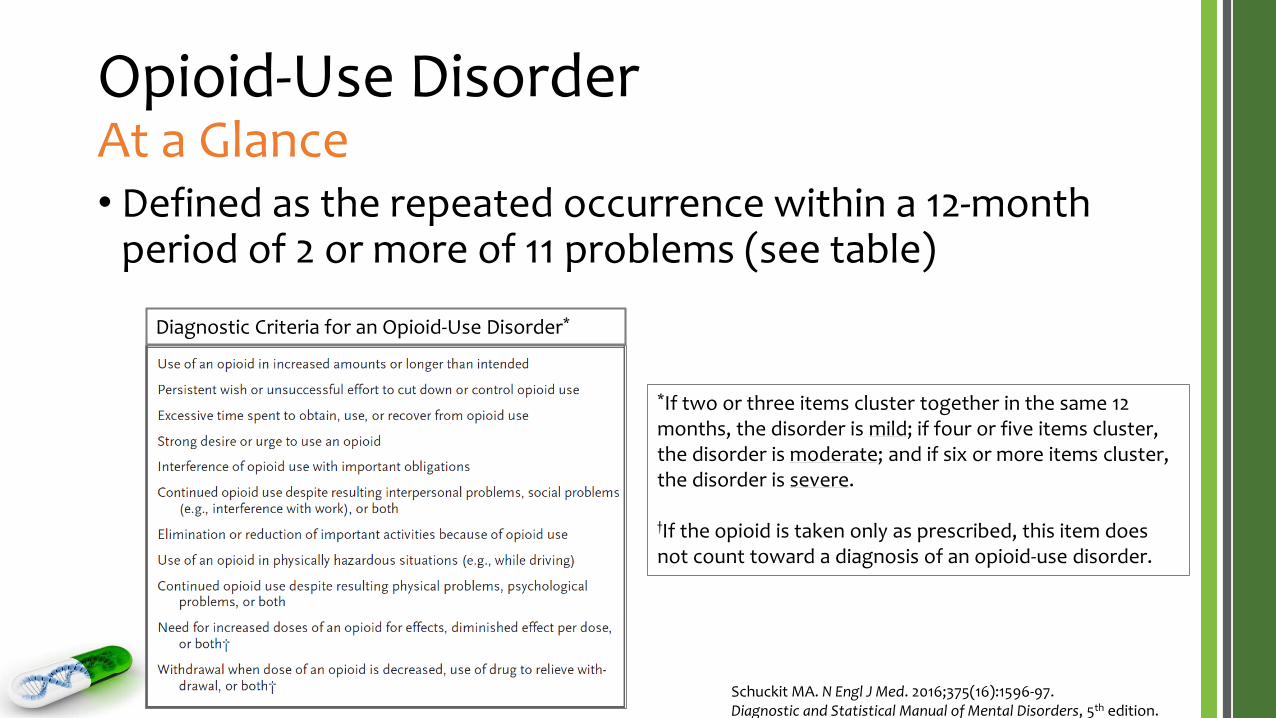
Opioid-Use DisorderAt a Glance• Defined as the repeated occurrence within a 12-month
period of 2 or more of 11 problems (see table)
Diagnostic Criteria for an Opioid-Use Disorder*
Schuckit MA. N Engl J Med. 2016;375(16):1596-97.Diagnostic and Statistical Manual of Mental Disorders, 5th edition.
*If two or three items cluster together in the same 12 months, the disorder is mild; if four or five items cluster, the disorder is moderate; and if six or more items cluster, the disorder is severe.
†If the opioid is taken only as prescribed, this item does not count toward a diagnosis of an opioid-use disorder.
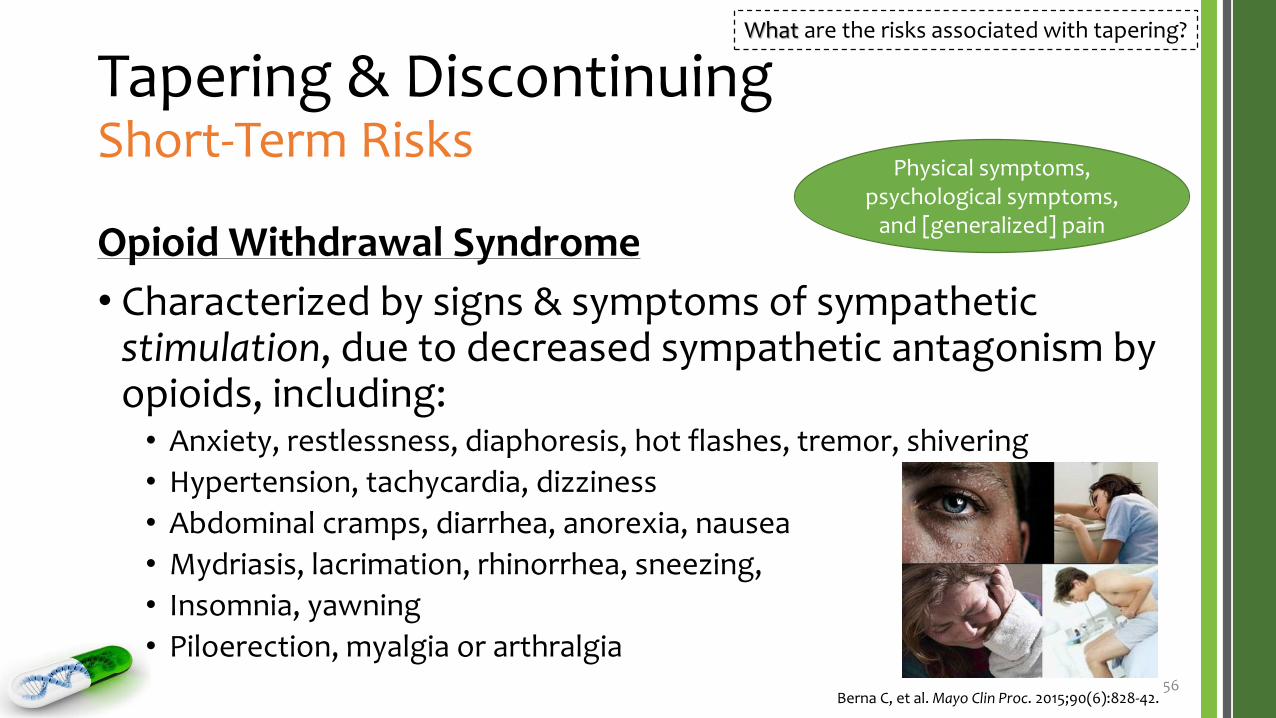
Tapering & DiscontinuingShort-Term Risks
Opioid Withdrawal Syndrome
• Characterized by signs & symptoms of sympathetic stimulation, due to decreased sympathetic antagonism by opioids, including:• Anxiety, restlessness, diaphoresis, hot flashes, tremor, shivering
• Hypertension, tachycardia, dizziness
• Abdominal cramps, diarrhea, anorexia, nausea
• Mydriasis, lacrimation, rhinorrhea, sneezing,
• Insomnia, yawning
• Piloerection, myalgia or arthralgia56
Berna C, et al. Mayo Clin Proc. 2015;90(6):828-42.
What are the risks associated with tapering?
Physical symptoms, psychological symptoms,
and [generalized] pain
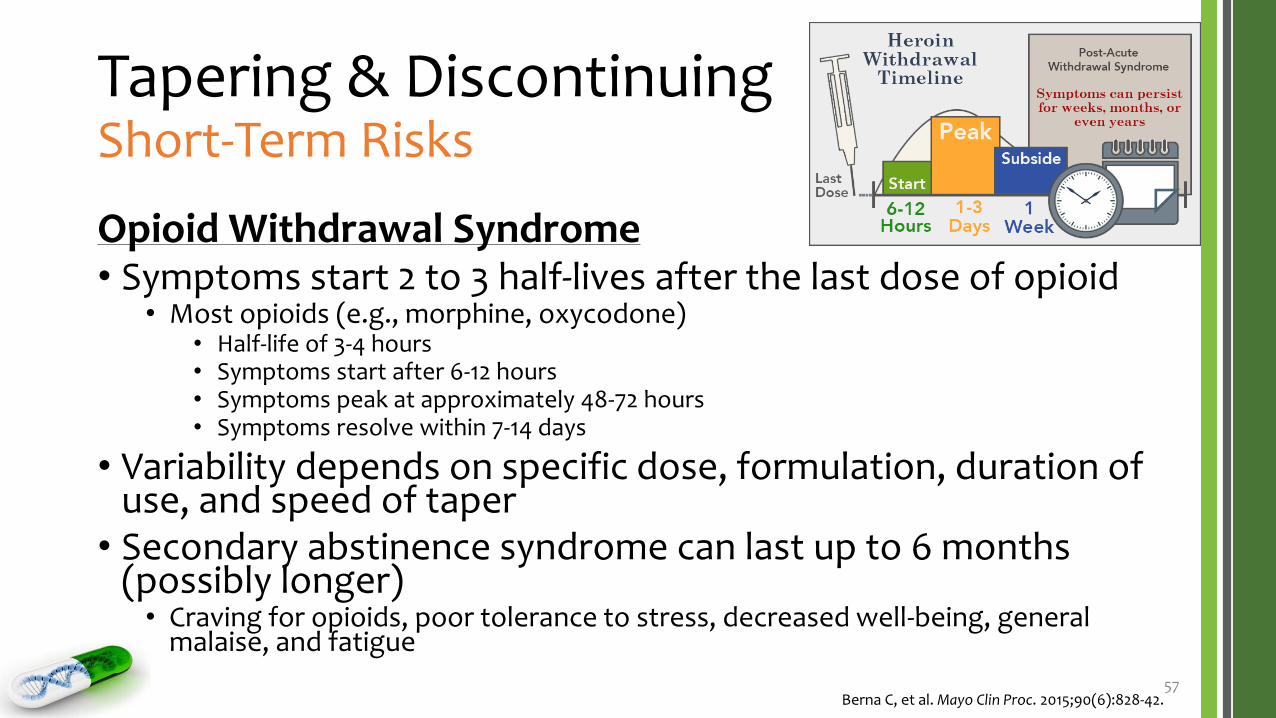
Tapering & DiscontinuingShort-Term Risks
Opioid Withdrawal Syndrome• Symptoms start 2 to 3 half-lives after the last dose of opioid
• Most opioids (e.g., morphine, oxycodone)• Half-life of 3-4 hours• Symptoms start after 6-12 hours• Symptoms peak at approximately 48-72 hours• Symptoms resolve within 7-14 days
• Variability depends on specific dose, formulation, duration of use, and speed of taper
• Secondary abstinence syndrome can last up to 6 months (possibly longer)• Craving for opioids, poor tolerance to stress, decreased well-being, general
malaise, and fatigue
57Berna C, et al. Mayo Clin Proc. 2015;90(6):828-42.
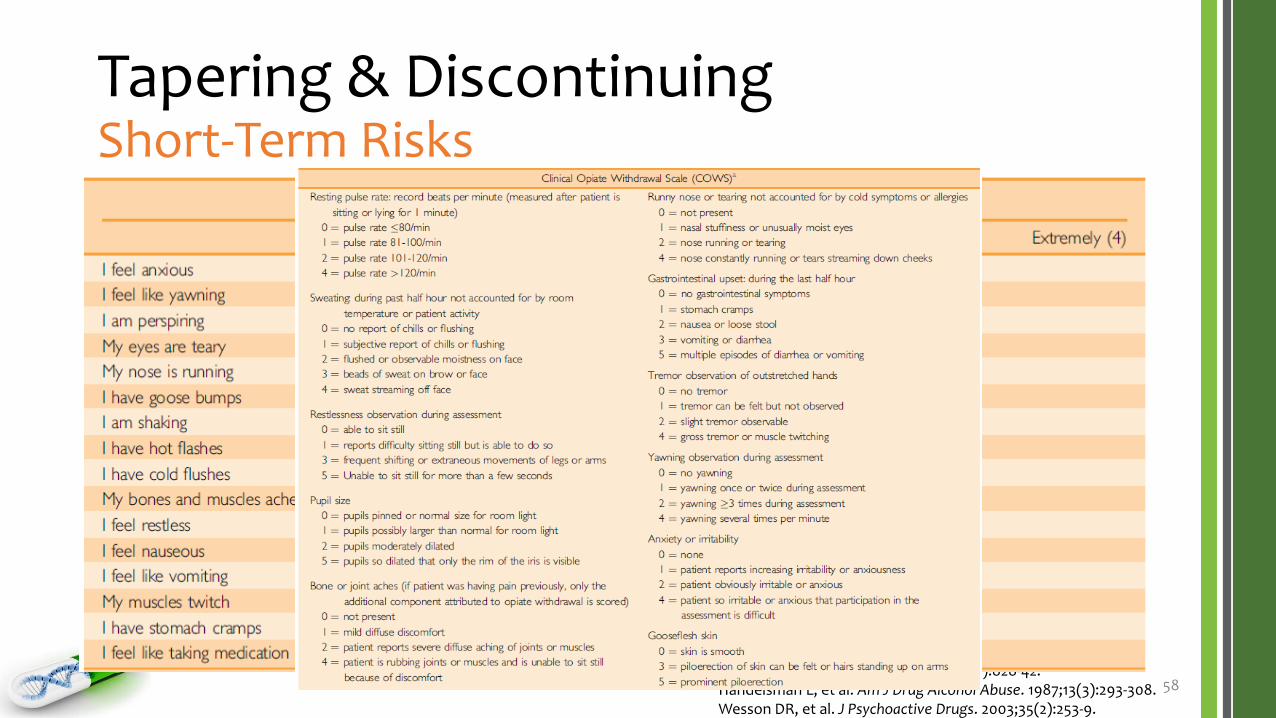
Tapering & DiscontinuingShort-Term Risks
Opioid Withdrawal Syndrome
• Tools allow clinicians to measure withdrawal symptoms
58Berna C, et al. Mayo Clin Proc. 2015;90(6):828-42.Handelsman L, et al. Am J Drug Alcohol Abuse. 1987;13(3):293-308.Wesson DR, et al. J Psychoactive Drugs. 2003;35(2):253-9.
Tapering & DiscontinuingShort-Term Risks
Rebound (Increased) Pain
• According to studies of long-term opioid therapy tapers, overall, patients report improvements in function without associated worsening in pain or even decreased pain levels
• Rebound pain following opioid taper & discontinuation appears to be a brief, time-limited phenomenon• Studies indicate that hyperalgesia may appear immediately after
discontinuation of long-term opioid therapy
• Similarly, hyperalgesia has been described postoperatively, when the use of short-acting opioids is abruptly discontinued at the end of surgery
59Berna C, et al. Mayo Clin Proc. 2015;90(6):828-42.
Opportunity to reduce patients’ fear
Tapering & DiscontinuingShort-Term Risks
Dropout
• There is legitimate concern for the following:• A patient will refuse to taper or discontinue opioids; or
• A patient will resume long-term opioid treatment, often with a different prescriber; and/or
• A patient will display aggressive behavior
• Dropout more commonly occurs when there is no plan• In other words, patients without an opioid maintenance treatment option,
in case of taper failure or following discontinuation, are more likely to quit
60Berna C, et al. Mayo Clin Proc. 2015;90(6):828-42.
Opportunity to reduce patients’ fear
Tapering & DiscontinuingLong-Term Risks
Relapse
• Ultimately, the goal is to maintain reduced opioid consumption or abstinence
• Relapse after a full opioid taper is influenced or predicted by:• Higher pain scores at initiation & conclusion of taper
• Conversely, low pain scores at the end of an opioid taper is predictive of long-term abstinence from opioids
• Depressive symptoms at initiation of tapering
• It may also be influenced by the speed of opioid taper & coping strategies of the patient
61Berna C, et al. Mayo Clin Proc. 2015;90(6):828-42.Heiwe S, et al. Eur J Pain. 2011;15(9):966-70.
What are the risks associated with tapering?
Tapering & DiscontinuingManaging Risks
Preventing Taper Failure (Dropout & Relapse)• Appropriate management of depression
• Comparative studies have not found one to be superior• Therefore, the choice is based on pharmacologic particularities of the
different drugs
• Examples• Clonidine 0.1-0.2 mg orally every 6 hours or transdermally once weekly• Tizanidine 2 mg orally at bedtime, titrated by 2-4 mg every day up to 8 mg
every 8 hours• Side effects common to both include hypotension, dry mouth, & sedation
63Berna C, et al. Mayo Clin Proc. 2015;90(6):828-42.Gowing L, et al. Cochrane Database Syst Rev. 2014.
How can the risks associated with tapering be managed?
Tapering & DiscontinuingManaging Risks – Other Therapies
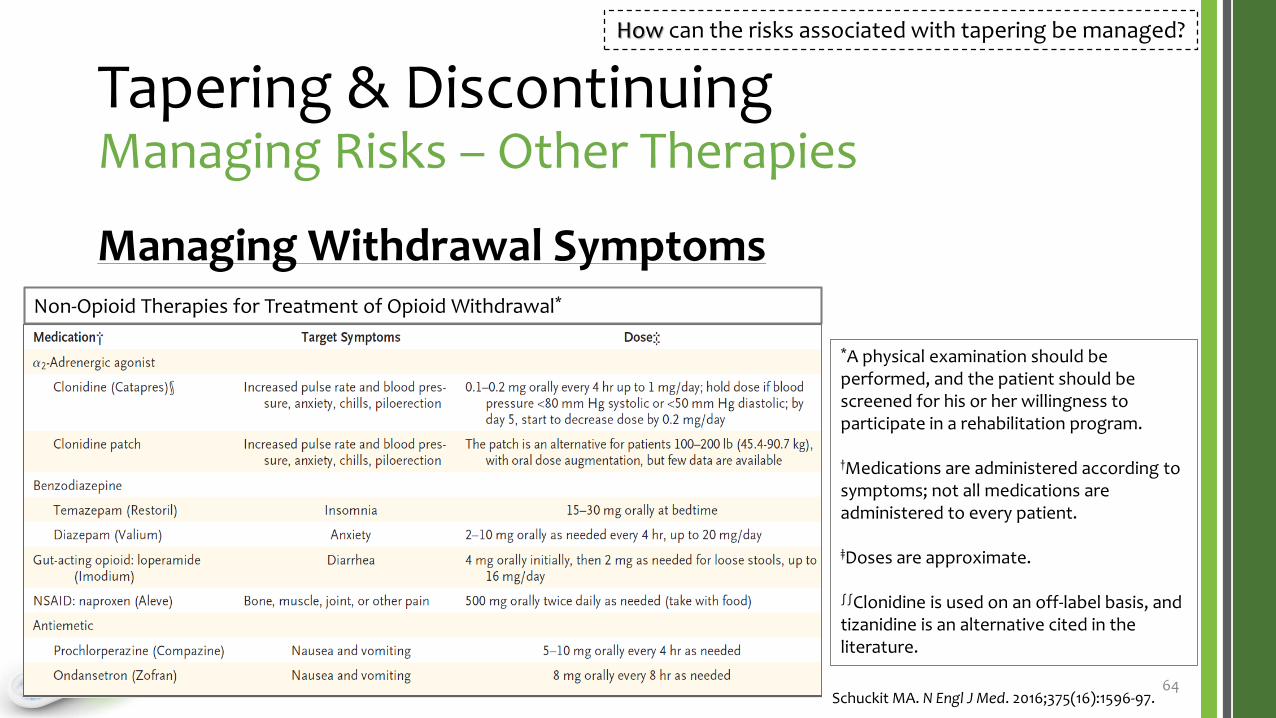
Managing Withdrawal Symptoms
64Schuckit MA. N Engl J Med. 2016;375(16):1596-97.
How can the risks associated with tapering be managed?
*A physical examination should be performed, and the patient should be screened for his or her willingness to participate in a rehabilitation program.
†Medications are administered according to symptoms; not all medications are administered to every patient.
‡Doses are approximate.
∫∫Clonidine is used on an off-label basis, and tizanidine is an alternative cited in the literature.
Non-Opioid Therapies for Treatment of Opioid Withdrawal*
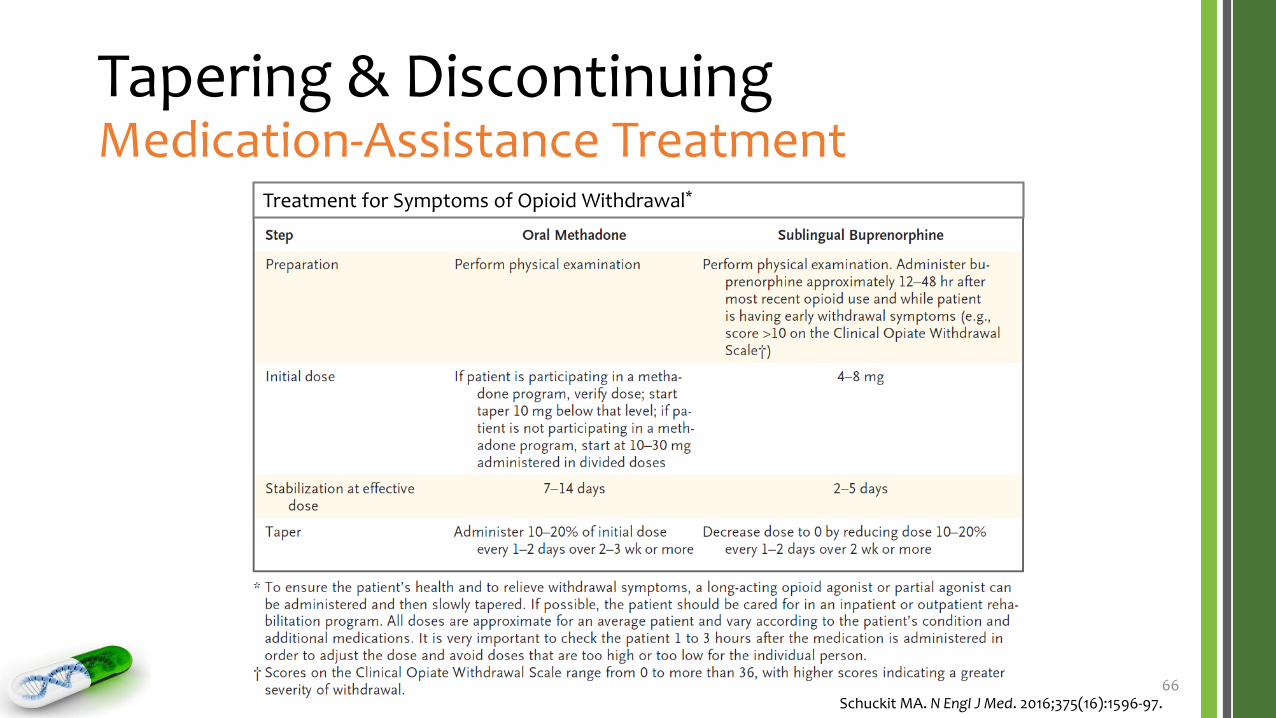
66Schuckit MA. N Engl J Med. 2016;375(16):1596-97.
Treatment for Symptoms of Opioid Withdrawal*
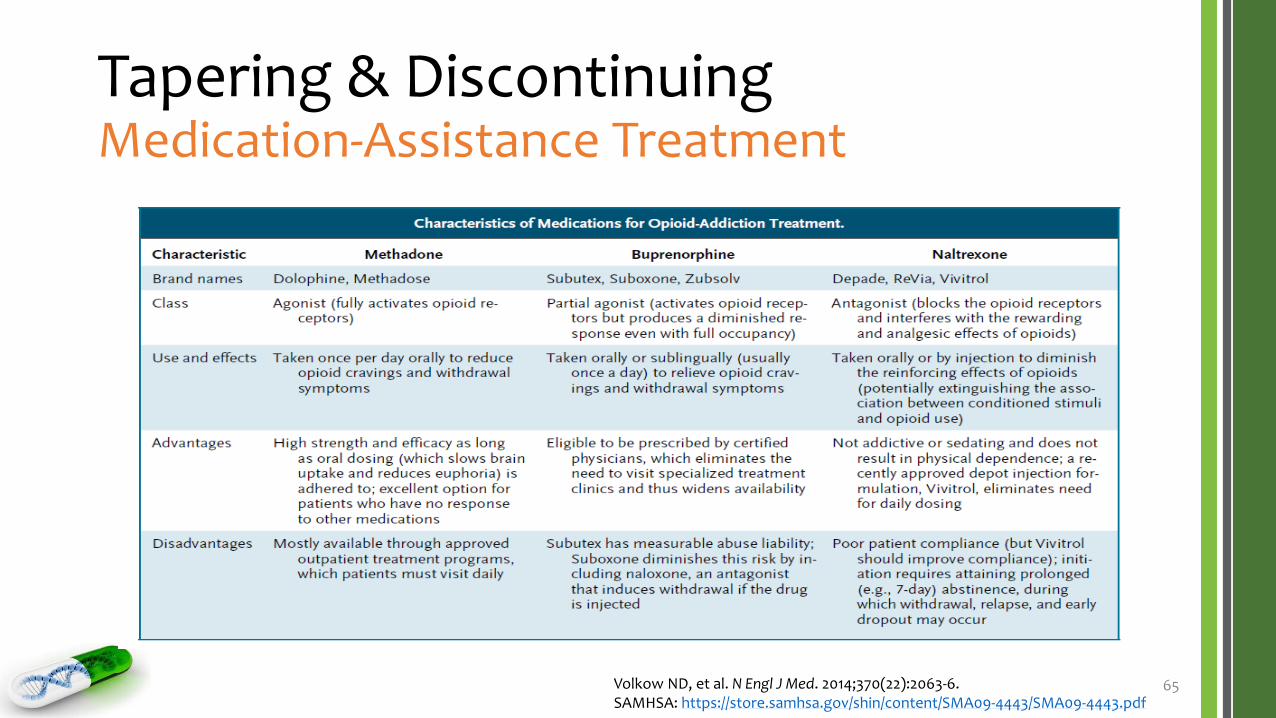
Medication-Assistance TreatmentClinical Pearls
Methadone
• A long-acting full µ-opioid receptor agonist that can be safely taken at the start of recovery
• It has a long & variable half-life (i.e., 15 to 40 hours)
• If initiated during withdrawal (i.e., added to opioid therapy during taper), need to be vigilant about dosing • Risk for respiratory depression and/or sedation• Risk of OD if the dose is increased too quickly
• A baseline ECG should be obtained before prescribing • Risk of QT interval prolongation, especially at doses > 100 mg/day and/or • Also keep in mind DRUG INTERACTIONS
67Berna C, et al. Mayo Clin Proc. 2015;90(6):828-42.Volkow ND, et al. N Engl J Med. 2014;370(22):2063-6.
Pharmacodynamic drug interaction
Medication-Assistance TreatmentClinical Pearls
Buprenorphine +/- naloxone
• A µ-opioid receptor partial agonist • Competitively antagonizes concomitantly administered full opioid agonists
• Introduced to patients in mild to moderate withdrawalbecause adding buprenorphine to a full opioid agonist can precipitate withdrawal• Initiate 12-18 hours after last short-acting opioid; 48 hours after long-acting
• Naloxone becomes available only if the medication is dissolved & injected, blocking the effect of buprenorphine• In which case, the withdrawal symptoms can be sudden & severe
68Berna C, et al. Mayo Clin Proc. 2015;90(6):828-42.Volkow ND, et al. N Engl J Med. 2014;370(22):2063-6.
• Cannot be taken until opioids are completely out of the body, usually 7 to 10 days after withdrawal begins / abstinence
• A good choice for preventing relapse because it takes away the “high” if the problem opioid(s) is used again
69Berna C, et al. Mayo Clin Proc. 2015;90(6):828-42.Volkow ND, et al. N Engl J Med. 2014;370(22):2063-6.
Safe & Appropriate Use of OpiatesClosing
Summary
• The CYP2D6 enzyme is responsible for metabolizing many commonly used opioids to more active metabolites• These opioids are weak substrates and, therefore, can be competitively
inhibited by moderate to strong substrates (e.g., antidepressants)
• This will result in reduced analgesic effect and potentially side effects
• Clinically, we tend to increase the opioid dosage to improve analgesic effect, which may result in opioid addiction, abuse, and/or misuse
• The CYP2D6 enzyme also is highly polymorphic• Genetic variations and drug-gene interactions resulting in
phenoconversion can significantly alter opioid response as well 71
Summary
• Inappropriate prescribing of opioids, entailing drug interactions, is a key upstream driver of the opioid epidemic
• Mitigating strategies are multifaceted and require careful consideration of the nature & extent of drug interactions involving the patient’s complete drug regimen
72
Summary
• Efforts to address the opioid epidemic need to simultaneously reduce opioid abuse & safeguard legitimate & appropriate access to opioids
• Expanding access to addiction-treatment services & MATs is a crucial component of the effort to help patients recover