58
Safe and Calm August 12, 2020

Safe and CalmAugust 12, 2020

Agenda
Advocacy
Situation Update
Resources and Guidance

Advocacy Agenda
• SB 899
• CON Appointments
• Michigan Updates
• Possible Strike
• Stimulus Updates

Leadership Institute 9/09-9/10
• Fully virtual conference• State and legislative updates• Finance and reimbursement trends• Regulations and guidance• Strategic planning• Innovative programs• Networking
Overcome Persevere Continue

LeadingAge Line-UP
• Dr. Robert Gordon (invited), Director MDHHS
• Larry Horvath, Director LARA BCHS
• Dr. Alexis Travis, Senior Deputy Director AASA
• Mary Ann Cleary, Director House Fiscal Agency
• Go to LeadingAgeMI.org to register!!!

Michigan Updates
SB 899 Vetoed by Governor Whitmer• This bill would have provided liability protections for a variety of health care facilities
New CON commissioners appointed • Justin B. Dimick,. is a staff physician and the chair of the Department of Surgery at the University of Michigan Health System. To
represent physicians licensed under part 170 or 175 representing a school of medicine or osteopathic medicine, for a term commencing August 7, 2020 and expiring April 9, 2023. He succeeds Stewart Wang whose term expired April 9, 2020.
• Amy Engelhardt-Kalbfleisch is a chief medical officer-associate at Henry Ford Hospital. Appointed to represent physicians licensed under part 175 to engage in the practice of osteopathic medicine and surgery, for a term commencing August 7, 2020 and expiring April 9, 2023. She succeeds Tressa Gardner whose term expired April 9, 2020.
• James B. Falahee, Jr. is the senior vice president of legal and legislative affairs for Bronson Healthcare Group. Mr. Falahee is reappointed to represent hospitals for a term commencing August 7, 2020 and expiring April 9, 2022.
• Ashok Kondur is a physician with Dearborn Cardiology, program director for the Garden City Hospital Cardiology Fellowship, and the director of Mechanical Circulatory Support & Complex and High-risk PCI at Ascension Providence Hospital. Dr. Kondur is appointed to represent hospitals for a term commencing August 7, 2020 and expiring April 9, 2022. He succeeds Denise Brooks-Williams whose term expired April 9, 2019.
• Lorissa MacAllister is the president and founder of Enviah, a healthcare consulting firm appointed to represent a company that is not self-insured for health coverage for a term commencing August 7, 2020 and expiring January 1, 2023. She succeeds Robert L. Hughes whose term expired January 1, 2020.

Michigan Legislative Updates
This week the legislature is focused primarily back to school issues.• There will be a joint legislative panel on Thursday with MDHHS director
Robert Gordon• Final planned session day for the month is on Saturday
The house has been working on an education package that would• Allow schools to conduct E-learning days as long as they stay within
curriculum requirements • Requirements for in-person learning for K -5 were included in the original
package• Require Parental consent for e learning• Waive the required minimum amount of days/hours of education• Submit school plans to the state• Schools would have to test their students to receive funding
Other options are being considered and negotiations are ongoing between the senate, governor and house
• Education pods

Detroit Union Workers Threaten to Strike
• On Aug. 17, around 1,600 Detroit nursing home workers plan to go on strike • Citing “unfair labor practices that illustrate the industry’s failure to keep workers and
residents safe”
• The workers represent 18 homes across Metro Detroit -- all but two of which are represented by for-profit nursing home chains Villa, Ciena, Charles and Dunn
• “We’re called essential, but we’re treated like we’re expendable. We’re calling on nursing home owners to pay us a living wage so we can afford to get healthcare just like we provide it, and put in place proper safety protocols and guarantee PPE throughout the pandemic.”
• https://www.mlive.com/news/ann-arbor/2020/08/1600-detroit-nursing-home-workers-to-strike-over-covid-19-safety-pay.html

Stimulus Update
• Negotiations still ongoing
• Presidential executive orders• Details still being released• May meet legal challenges• Extended the $400 million dollar unemployment benefit
• States will have to cover 25% of the costs• Defers student loan payments• Defers the employee portion of the federal payroll taxes from April 1 to the end of
the year• Right now the taxes would have to be paid back
• Efforts to halt evictions• Asks treasury to look at the costs of paying for rent for those who can’t afford it

Next Stimulus Package – What’s at Stake• $175 billion in healthcare provider relief funds – not all
distributed. $100 billion more requested for physicians and hospitals
• Medicare Loans – pay backs due starting in August. Relaxations in repayment conditions
• Liability protections
• Telehealth policy extensions
• COVID Testing funds by commercial insurers
• State and local funding to insulate budgets – Medicaid rates
• Hazard Pay and child care subsidies requested by hospitals and healthcare providers (new)
• COBRA subsidies (new)
• Funding for FQHCs (new)

360careAdvanced Satellite Communications, Inc.All Med Medical Supply, LLCBaker TillyBasic American Medical ProductsCompass Communications Group,Concept Rehab, Inc.Creative Dining ServicesDermaRite IndustriesEZ Way, Inc.FOX RehabilitationFunctional Pathways
Furnishings By Design, LLCFusco, Shaffer & Pappas, Inc.Genesis Rehabilitation ServicesGMB Architecture & EngineeringHealthPRO HeritageHoekstra TransportationHomeTown Pharmacy LTCHooker DeJong, Inc.HPSHPSIIn Touch Pharmaceuticals
Thank You Exhibitors

Situation Update

Weekly New Case Trends - Global

United States
Michigan
Illinois
Indiana
Wisconsin
1000
Ohio
50000
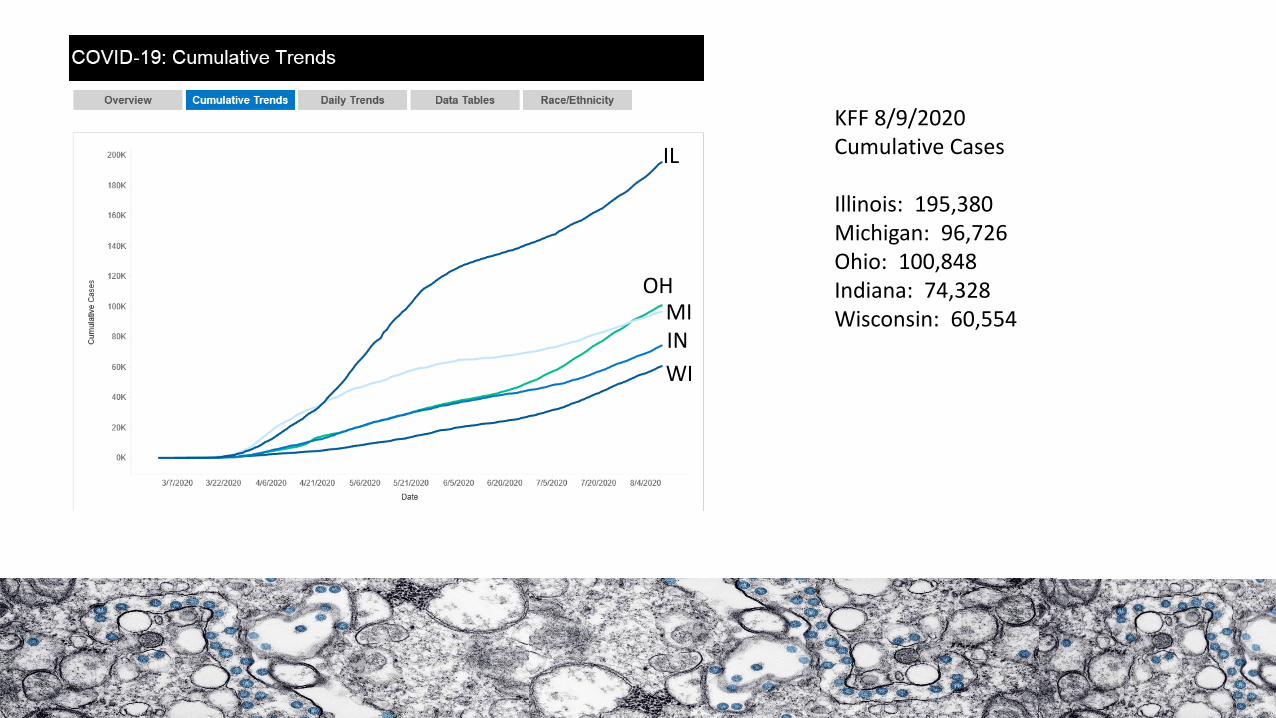
KFF 8/9/2020Cumulative Cases
Illinois: 195,380Michigan: 96,726Ohio: 100,848Indiana: 74,328Wisconsin: 60,554
IL
OHMIIN
WI

KFF 8/9/2020Cumulative Deaths
Illinois: 7845Michigan: 6519Ohio: 3668Indiana: 3041Wisconsin: 998
IL
MI
OH
IN
WI

0.00
2,000.00
4,000.00
6,000.00
8,000.00
10,000.00
12,000.00
14,000.00
16,000.00
18,000.00
US Illinois Michigan Ohio Indiana Wisconsin
Cumulative Cases per Million Population 8/9/2020

Seven Day Rolling Average Daily New Cases 8/9/2020
0
200
400
600
800
1000
1200
1400
1600
1800
2000
Illinois Michigan Ohio Indiana Wisconsin

• Share of adults under age 65 at risk: 21% across US
• Share of adults under age 65 at risk: 25% in Michigan• Seven states have higher percentages – all southeastern US
• Oklahoma – 25%
• Older adults, as a share of all at risk adults: 55% across US
• Older adults, as a share of all at risk adults: 53% in Michigan
• At risk adults, as a share of all adults 18+: 38% in US/ 41% Michigan
https://www.kff.org/coronavirus-covid-19/issue-brief/what-share-of-people-who-have-died-of-covid-19-are-65-and-older-and-how-does-it-vary-by-state/?utm_campaign=KFF-2020-The-Latest&utm_medium=email&_hsmi=91992161&_hsenc=p2ANqtz-90U-wnL2iOkdZvWU4N6oM8MomkxLc2g9Hjbr1E8srFrEd9OtujrUbWeTK3NSK3Vs3eHcYUGN2ieTkfVh9Hyfx_xEm37w&utm_content=91992161&utm_source=hs_email
KFF

The number of adults 65 and older who have died of COVID-19 is considerably higher in some states than others, with 61% of all adults 65 and older who died of COVID-19 as of July 15, residing in just 7 states: New York, New Jersey, Massachusetts, Pennsylvania, Illinois, California, and Michigan.
Kaiser Family Foundation,
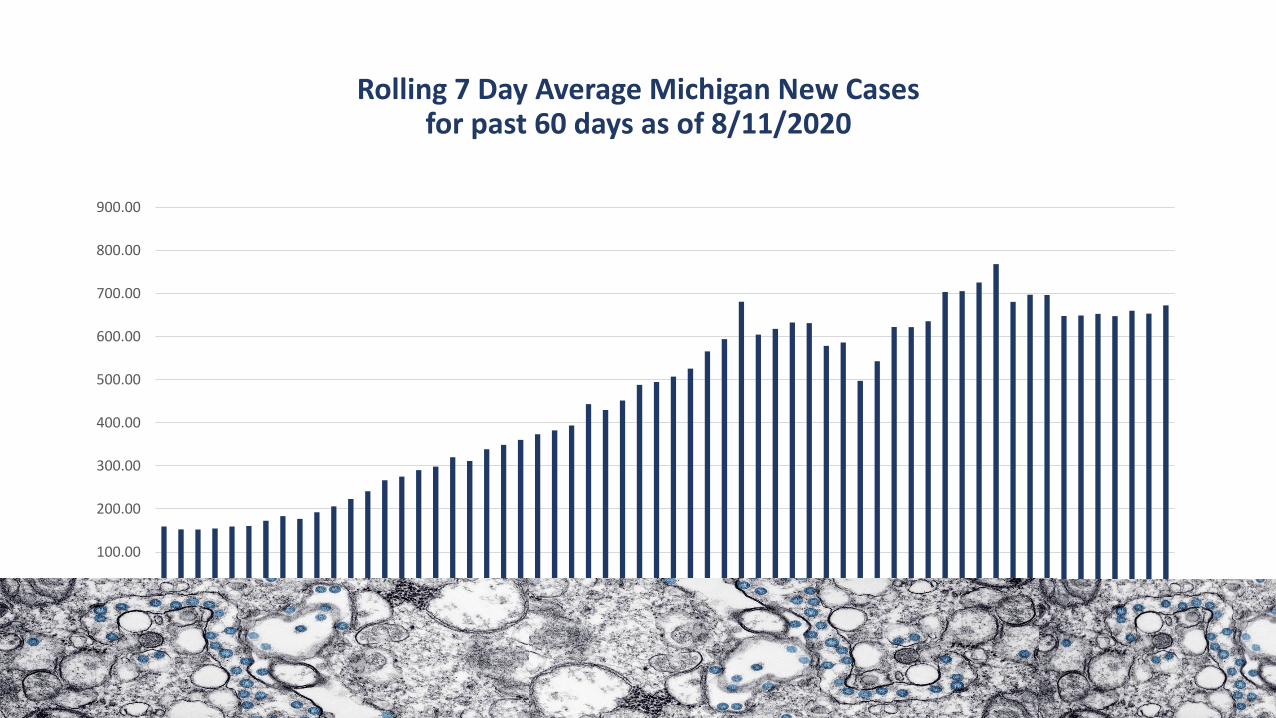
Rolling 7 Day Average Michigan New Cases for past 60 days as of 8/11/2020
0.00
100.00
200.00
300.00
400.00
500.00
600.00
700.00
800.00
900.00
Series 1

Rolling 7 Day Average Daily Michigan Deaths for past 60 days as of 8/11/2020
0.00
2.00
4.00
6.00
8.00
10.00
12.00
14.00
16.00
18.00
Series 1

MI Safe Start – 8/11/2020 Update
As of 8/9/2020

Resources and Guidance
August 12, 2020

Executive Orders
• EO 2020-163: Black Leadership Advisory Council
• EO 2020-164: Requiring Masks at Childcare Centers
• EO 2020-165: Declaration of State of Emergency –9/4/2020
• EO 2020-166: Protecting Workers who stay home/stay safe – No end date
• EO 2020-167: Food Security Council
• EO 2020-168: Temporary Measures for Food Sellers
• EO 2020-169: Enhanced Protections for Residents and Staff – 9/7/2020

Executive Order 2020-166
• Employers cannot discharge, discipline, or retaliate for staying at home when he or she is at risk of infecting others
• Must treat employees as if taking medical leave
• If no leave, leave may be unpaid. Employers are permitted but not required to debit any hours from accrued leave
• Length of leave is not limited by amount of leave and must extend, whether paid or unpaid as long as they employee remains away from work within time periods described below
• Employers can discharge/discipline for declining to come to work when allowed to do so, with employee consent, other unlawful reasons
• Complaints can be made to associated licensing authority
• Which employees does this pertain to? All individuals who test positive for COVID or who display one or more principal symptoms, until 24 hours following resolution of fever without meds, 10 days since first symptoms appear or tested positive, and other symptoms improved.

Executive Order 2020-166• Any and all persons who have had close contact with a person who tests positive or who has
displayed symptoms should remain in their home until 14 days have passed since exposure or the person displaying symptoms has a negative test
• Exceptions to requirements for persons with close contact include: healthcare professionals, healthcare workers, first responders, childcare workers, workers at AFCs, workers at correctional facilities
• Anyone who voluntarily returns to work prior to these quarantine periods are not entitled to protections
• Persons suspected/confirmed/or in close contact should leave home only to the extent necessary and should remain out of public buildings, for outdoor activities with social distancing
• Principle symptoms are fever, sore throat, new uncontrolled cough that causes difficulty breathing, diarrhea, vomiting, abdominal pain, new onset severe headache, new loss of taste or smell
• Close contact means within 6 feet for at least fifteen minutes

Executive Order 169: Protecting Residents and Staff
• Extension of EO 148 to 9/7/2020
• We originally called this order the Regional Hub Order
• Protections for residents of LTCFs: evictions, readmissions, right to return, promote telemedicine
• Protections for employees and residents: COVID positive employees must stay home, facilities must cancel all communal dining, disinfection, PPE, notify employees, report cases and PPE
• Transfers and discharges: NH must make reasonable efforts to create dedicated unit (provide PPE, maintain infection control)
• Transfer residents to a dedicated unit; attempt to transfer to a regional hub, alternate care facility or swing bed, or hospital with bed capacity
• Hospital must conduct testing aligned with CDC best practices; discharge to a hub, the facility where resident resided, alternate care facility, or a swing bed
• Discharge destination with CDC guidelines, considering safety of residents, wishes, local health department guidance. Can only discharge to a facility capable of isolating the resident consistent with CDC and MDHHS guidelines
• Or remain in hospital
• Covers nursing homes, adult foster care, homes for the aged and assisted living

Toolkit on State Actions to Mitigate COVID Prevalence in Nursing HomesJuly 2020 – Version 6
• https://www.cms.gov/files/document/covid-toolkit-states-mitigate-covid-19-nursing-homes.pdf
• Cleaning and Disinfection
• Reporting
• Testing
• Workforce and Staffing
• Cohorting
• Infection Control Strike Teams
• Infection Control Surveys
• Nursing Home Communications
• Access to PPE
• Utilization of PPE
• Housing and Sheltering
• Transportation Needs
• Patient Transfer
• Resources
• Screening Visitors
• Tellehealth

CMS Counseling Checklist
• https://www.cms.gov/files/document/covid-provider-patient-counseling-checklist.pdf
• Provides education and guidance to persons who are being tested routinely or for symptoms
• Anticipates actions if results are positive
• Includes a set of resources for more information and tools
• Includes information about health department follow up in case of positive findings

Provider Relief Grants: General Distribution – Phase 1
• First distributions included $30 million of $50 million available
• Additional distributions if first payment did not equal 2% of total patient care revenue (not just Medicare revenue). Financial information was due June 3 for this second run which would use the remaining $20 million.
• This could apply to providers who primarily served Medicaid, but had low Medicare revenues.
• Extended deadline starting August 10 through August 28
https://cares.linkhealth.com/#/

General Distribution Funding – Phase 2
• Eligibility (Press Release)• Providers who were ineligible for Phase
1 funding because of CHOW in 2019-2020
• Providers who did not have Medicare FFS revenue during 2019
• Providers who received a payment but missed the June 3 deadline to submit revenue information to gain the entire 2% payment of total revenues
• Providers who previously received funds and returned them, but now have changed their minds
• Providers will only receive 2% of total revenue regardless
• Must accept HHS terms and conditions
https://cares.linkhealth.com/#/
Eligibility Website (Steps)• Received no payment from Phase 1 General
Distribution• Billed Medicaid for health-related services in
CY2018-CY2019• Filed income tax for 2017, 2018, 2019 or exempt• Provided patient care after January 1• Did not permanently cease operationsValidate TINApply for FundingReceive PaymentAttest to PaymentReport on use of Funds

Reporting on Use of Funds
Funds must be used to cover lost revenue attributable to COVID or health related expenses needed to prevent, prepare for, and respond to coronavirus including but not limited to…
• Supplies
• Equipment
• Workforce training
• Test reporting
• Building temporary structures
• Acquiring additional resources
https://www.hhs.gov/sites/default/files/provider-post-payment-notice-of-reporting-requirements.pdf
• Reporting system will become available on October 1
• All recipients have within 45 days of the end of the calendar year 2020 to report on expenditures through 12/31/2020
• Recipients who expended all funds by 12/31/2020 can submit anytime after 10/1 but no later than February 15, 2021
• Recipients expending funds after January 1 have until 7/31/2021
• Detailed reporting requirements will be available along with a template by 8/17/2020

CARES Act Relief Fund for Nursing Homes – 8/7/2020
• Distribution total is $5 billion
• ‘…Linking funds to performance in controlling COVID-19
• AHRQ will oversee the implementation of specialized learning networks/ expected to be some training requirements
• $2.5 billion in upfront funding for increased testing, staffing, and PPE needs based on bed count and whether or not POC testing has been received
• Funding will also be available for establishing COVID isolation facilities
• Balance will be linked to nursing home performance with a focus on providers who perform average or better than average when reviewing the number of new facility-acquired COVID cases in their community –using NHSN data with rewards distributed each month between September and December. Formula has not yet been developed

CARES Act Relief Fund for Nursing Homes – 8/7/2020• 40% of all COVID related deaths occur in nursing homes
• Ensure that the government is paying for better outcomes
• Evaluation of performance will consider local transmission, and will be based on facility ability to minimize COVID spread
• Consistent with Principles from June 2019 Quality Roadmap/Pronovost-Cleveland Clinic
• Project ECHO – a consortium of 250 health system hubs partnering with AHRQ to pilot nursing home infection control learning network
• Initial $2.5 billion distribution should occur in August and additional performance based distributions in the Fall.

Provider Relief Grants
Webinar on Provider Relief Funds
August 13, 3:00 PM ET
https://webex.webcasts.com/starthere.jsp?ei=1354695&tp_key=b56041b5d4
• www.HHS.gov/providerrelief for updates

Health Care Workers Lost to COVID• 922 persons have died to date
• Many worked in facilities with shortages of PPE such as gowns, masks, gloves, and face shields
• Persons of color account for a disproportionate share of deaths
• KFF database and 167 profiles• 31% had inadequate PPE• 62% were persons of color• 64% were nurses, but also included physicians, pharmacists, first responders• 46% > 60; • 32% were born outside the US https://khn.org/news/exclusive-over-900-health-workers-have-
died-of-covid-19-and-the-toll-is-rising/

HUD – Physical Inspection Update
• 8/7/2020- HUD announced Real Estate Assessment Center inspections for HUD multifamily and public housing properties will restart in October
• Inspections will be conducted using strict safety protocols
• Standard 14-day physical inspections will resume after 9/21/2020 with first inspections expected on October 5.
• Inspections will be prioritized based on local transmission rates as well as previous scores: low score + low risk area
• HUD has developed a HEAT Map that categorize regions by risk
• LeadingAge has asked to avoid inspections of senior facilities and asked for waivers from fault if inspections are cancelled because of COVID

HUD Heat Map Green – LowYellow – Moderately lowGold – Moderately HighRed * High

Learning Opportunities
CMS Nursing Home Call
Wednesday, August 12th 4:30 – 5:00 PM Eastern
Toll Free Attendee Dial-In: 833-614-0820;
Access Passcode: 7857618
Audio Webcast Link
JPST – COVID Related
Virtual Meeting: 9/29/2020
Register by 9/21
http://www.michigan.gov/lara/0,4601,7-154-63294-290587--,00.html
LeadingAge Housing Calls
During the next two scheduled LeadingAge Housing calls, HUD will be available to discuss recent updates
August 17, 12:30 PM ET: NSPIRE Demonstration Pilot
August 24, 12:30 PM ET: Fair Housing
Join Skype Meeting
Or Join by phone
1 (240) 669-5802 (United States)
Conference ID: 537899

Learning Opportunities
• CMS – Transparency, Resident and Family Notification, Department of Health and other Notifications
• Date: Thursday, August 13, 2020
• Time: 4:00 – 5:00 PM ET
• Advance Registration Required: https://zoom.us/webinar/register/WN_w16sb6o8TBa-PR7oAFNg2g

42
Exclusive Sponsors
Gold Sponsors
Silver Sponsors
Bronze Sponsors
Thank you to our Sponsors!!

CDC and Personal Protective Equipment
• Healthcare personnel must adhere to standard and transmission based precautions for COVID suspected or positive residents
• Universal Source Control Measures• Cloth face coverings or face masks to cover mouth and nose
• Potential for asymptomatic and pre-symptomatic transmission
• Source control measures are for EVERYONE in the facility
• Residents must wear face coverings while outside of room but replace when around others or staff are in the room
• Staff must wear a facemask at all times in the facility, including in breakrooms; facemasks are preferred over cloth face coverings.
• Consider wearing the same face mask throughout the shift to reduce the number of times staff must touch their face and risk contamination. Should not switch back to cloth face covering.
https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-recommendations.html

Implement Universal Use of Personal Protective Equipment
• Staff working in areas with moderate to substantial transmission should follow standard precautions
• Transmission based precautions must be followed if required based on suspected diagnosis
• Staff must wear eye protection in addition to facemask to ensure eyes, nose and mouth are completely protected
• Wear an N95 or higher respirator for aerosol generating procedures
• Staff working in areas with minimal or no transmission -same

Aerosol Generating Procedures
• Open suctioning of airways
• Sputum induction
• Collection of respiratory specimens/unless respirators not readily available
• Cardiopulmonary resuscitation
• Nebulizer administration*
• High O2 delivery*

Residents with Suspected or Confirmed COVID
• Evaluate need for hospitalization
• Place in single room with door closed and dedicated bathroom
• Airborne Infection Isolation Rooms should reserved for persons undergoing aerosol generating procedures
• Only residents with the same respiratory pathogen may be housed in the same room
• If possible, suspected or confirmed positive persons should be housed continuously in same room
• Limit transport and movement of the resident outside of the room to medically essential activities
• After vacating the room, sufficient time for enough air changes to remove infectious particles should elapse before cleaning

Use of PPE for Suspected or Confirmed COVID• Staff who enter the room should adhere to standard precautions and use an
N95 mask or higher/or a facemask if a respirator is not available, gown, gloves, and eye protection
• Respirators are preferred, but should be prioritized when respiratory protection is most important and for care of persons requiring airborne precautions (TB, measles, varicella).
• Hand hygiene before and after all resident contact, contact with any potentially infectious material, before donning and doffing PPE, including changes in gloves
• Hand hygiene is especially important after removing PPE
• Facilities should select appropriate PPE in accordance with OSHA PPE Standards https://www.osha.gov/laws-regs/regulations/standardnumber/1910
• Training and demonstration: when to use PPE, what PPE is needed, donning and doffing, how to dispose or disinfect and maintain PPE, and the limitations of PPE

Use of PPE for Suspected or Confirmed COVID
• Cloth face coverings are not PPE and should not be worn for resident care or any time a facemask or respirator is recommended
• Put on N95 masks before entry into the resident room if not already wearing (as part of extended use strategy).
• Disposable respirators and facemasks should be removed and discarded after exiting the resident room unless implementing extended use or reuse. (dedicated staff?)
• When supply chain is restored, facilities with a respiratory protection program should return to use of respirators for persons with suspected or confirmed COVID
• Eye protection must be donned upon entry to the room unless working under extended use.
• Safety glasses, eye glasses with gaps around the face do not protect eyes from all splashes and sprays
• Ensure eye wear does not interfere with positioning of face mask
• Gloves and gowns should be donned and doffed and disposed after each use.

Transmission Based Precautions
• Additional precautions for persons with suspected transmission risk
• Contact, droplet, and airborne precautions
• If unsure of diagnosis, use highest level of necessary precautions until confirmed

Long Term Care Guidelines
• https://www.cdc.gov/coronavirus/2019-ncov/hcp/long-term-care.html
• ICAR – infection prevention and control assessment tool for nursing homes
• Facemasks are required for all staff while in the facility.
• Residents should wear a cloth covering or facemasks whenever out of their room.
• Depending on prevalence of COVID in the community, place new admissions in a single room or in a separate observation area to monitor for COVID. HCP should wear an N95 or higher level respirator (or a facemask if a respirator is not available), eye protection (goggles or a face shield that covers the front and sides of the face), gowns and gloves when caring for these residents.
• Residents can transfer out of the observation area to the main facility if they remain afebrile and without symptoms for 14 days after their admission. Testing AFTER this time can be considered to increase certainty that the resident is not affected (it does not replace the 14 day quarantine)

Long Term Care Guidelines
• Fever/chills
• Cough
• Shortness of breath and difficulty breathing
• Fatigue
• Muscle or body aches
• Headache
• New loss of taste or smell
• Sore throat
• Congestion or runny nose
• Nausea or vomiting
• diarrhea
https://www.cdc.gov/coronavirus/2019-ncov/hcp/long-term-care.htmlMonitor all residents upon admission and at least daily for fever (T>100.0oF) and symptoms consistent with COVID

LTC Specific Guidance
• Ideally, place residents with COVID in a private room and/or move to dedicated unit
• Roommates should be isolated for 14 days after exposure, assuming they have no symptoms
• Residents with known or suspected COVID should be cared for using all recommended PPE, including N95 or facemask if extending use or not available, eye protection, gloves, and gown.
• Increase monitoring of ill residents, including assessment for symptoms, vital signs, oxygen saturation, respiratory exam to at least three times daily to identify and quickly manage serious infection. Consider increasing monitoring of asymptomatic residents from daily to every shift to more rapidly detect any with new symptoms
• Universal use of all PPE for care of all residents on any unit with COVID positive resident. Or facility wide use of all PPE is recommended when even a single case among residents or staff is newly identified in the community. This should also be considered when there is sustained transmission in the community.
• Discontinuation of transmission based precautions.

Long Term Care Specific Guidance
• Visitation Restrictions: restrict non-essential healthcare personnel, such as those providing elective consultations and providing non-essential services (barbers and hair stylists) and volunteers from entering the building

MSA 20-57: COVID 19 Specimen Collection • Effective March 10
• Assessment and specimen collection to support testing will require extraordinary and resource intensive measures
• Temporary policy changes for outpatient hospitals, labs, physicians and other practitioners
• Includes appropriate codes for billing
• Nursing Facilities: Drawing, collecting, and delivery of laboratory specimens are routine nursing services. As such, they are included in the nursing facility’s per diem rate regardless of who performs the service (i.e., nursing facility or ancillary laboratory provider). COVID-19 specimen collection will not be reimbursed separately in these instances.
• Home Health Agencies: If a beneficiary is receiving home health nursing services, the home health nurse, during an otherwise covered visit, may obtain the sample to send to the laboratory for COVID-19 diagnostic testing. Specimen collection will not be reimbursed separately in these instances.

Nursing Home Point of Care Testing
• Point of Care Testing has now reached Michigan as 16 facilities have been included in the most recent priority list from CMS. Nursing homes are not required to use the equipment or testing but those that do must hold a CLIA certificate of waiver and must also comply with the HHS Lab Data Reporting Guidance. On August 4, the CDC released updated guidance that helps explain these requirements.
• Three LeadingAge Michigan members are in the group.
• Conference call with MDHHS today to discuss protocols and reporting requirements

Nursing Home Testing / Learning Opportunities
• NHSN Data Quality Webinar
• Wednesday, August 12, 1:00pm ET:
• CDC has updated its reporting requirements for nursing home reporting to NHSN. MDHHS informed us that they will be working to align the data elements with EMResource. These updates were not announced but were noted on the NHSN instruction page. Members are encouraged to review this asap and to check for updates routinely.
• Webinar Link
• NHSN COVID-19 Module:
The NHSN Module now asks about barriers to perform or obtain resources for testing, what report response times are for results, and facilities are conducting any facility wide testing
https://www.cdc.gov/nhsn/pdfs/covid19/ltcf/57.144-toi-508.pdf

PointClickCareProSure Fund, ThePS of MIReliant RehabilitationRemedi SeniorCarePharmacySelect RehabilitationService Care Industries Inc.Spartan ChemicalThe Compliance StoreTherapy Management, Inc.TMCValue FirstZiegler
Interstate Restoration
It ’s Never 2 Late, LLC
Kalamazoo Long Term Care
Pharmacy
Kingscott Associates
Marcus & Millichap
McKesson Medical Surgical
Midwest Juice, Inc.
Mobile Care Group
Omnicare
PCA Pharmacy
PharMerica
Thank You To Our Exhibitors!


















