52
SAMPLE PRESENTATION Christopher Hurst M.Ed., Office of Resident Wellness Fatigue Management
SAMPLE PRESENTATION
Christopher Hurst MEd
Office of Resident Wellness
Fatigue Management
Objectives
Describe signs and symptoms of fatigue
Discuss the effects of fatigue and sleep
deprivation on well-being and performance and
Identify strategies for managing fatigue and sleep
debt
ldquoThe best decision makers are the ones who know
when not to trust themselvesrdquo
Dr R Baumeister
Basic Message
Fatigue and sleep deprivation are significant risk
factors for diminished performance and reduced
well-being
The anti-dote is active self-monitoring for fatigue
and sleep debt and
Choosing to make rest sleep and self-care a key
priority in daily activities
Self-Monitoring
Physical Sensation
ThinkingAttention
FeelingMotivation
Performance Indicators
Fatigue
Fatigue is a protective physiological function
signaling that the margin of effective performance
has been reached
People cannot reliably self-judge their level of
fatigue-related impairment
St Pierre et al 2011
Fatigue Demands Rest
People often react to tiredness only when their
performance has already decreased This is one of
the reasons why breaks are often taken too late
Recovery then takes more time compared with
situations when breaks are taken early
St Pierre et al 2011
Fatigue
ldquoFatiguerdquo can be thought of as the combined
influence of sleep homeostasis circadian rhythm
and time on task on performance capability
Van Dongen amp Hursh 2011
Other Conditions Linked with Fatigue
Fatigue can be related to anxiety depression
stress thyroid disease other medical conditions
medication side effects or career dissatisfaction
Residents may have a primary undiagnosed
sleep disorder such as obstructive sleep apnea
narcolepsy restless leg syndrome or insomnia
What creates fatigue in residency
training
FT = Total resident fatigue
FT =
FT = FSS + Few + Fpf FT = Total resident fatigue
FSS = Fatigue related to system design (circadian
rhythm disruption sleep deprivation fragmented sleep)
Few = Fatigue related to work and environmental
factors (task requirements physical work loads
workstation design physical factors team factors) and
Fpf = Fatigue related to the operatorrsquos personal
factors (health status nutritional status social and
domestic dictates)
Adapted from Schutte (2009)
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Primary
Sleep Disorders
(sleep apnea etc)
Fragmented Sleep
(pager phone calls)
Circadian Rhythm
Disruption
(night float rotating
shifts)
Insufficient Sleep
(on call sleep lossinadequate
recovery sleep)
EXCESSIVE DAYTIME SLEEPINESS
Fatigue amp Burnout
The characteristic symptoms of burnout are
persistent and excessive fatigue emotional
exhaustion and cognitive dysfunction Frequently
the condition also includes components of
depersonalization or cynicism toward
clientspatients and reduced personal efficacy with
a tendency to evaluate oneself negatively
Aringkerstedt (2011)
Burnout in Residency
Prevalence estimates range between 40ndash76
among internal medicine and pediatric residents
and 47ndash70 among surgery residents
McCray (2008)
Burnout and Sleep Deprivation
It has recently been demonstrated that burnout
scores are closely related to reports of disturbed
sleep
Aringkerstedt (2011)
Ego Depletion Decision Fatigue
and Task Performance
We find that the percentage of favorable rulings
drops gradually from 65 to nearly zero within
each decision session and returns abruptly to
65 after a break Danzigera (2011)
These studies demonstrated that ego depletion
coincides with decreases in blood glucose and
glucose supplementation attenuates the ego-
depletion effect relative to a sweetened placebo
Hagger (2010)
Fatigue Effects Alertness attention and vigilance are reduced People are able to sustain
concentration on a task for a shorter than usual period of time
Reduced motor performance (fine motor skills and eyendashhand coordination)
and a decrease effectiveness of motor tasks (speed and accuracy are
reduced)
Slowed reaction time and decision-making In order to reduce effort rule-
based decisions are preferred over knowledge-based decision-making
(principle of economy)
Impaired memory function manifested as a reduced ability both to learn and
to recall items
Motivational alteration of the thinking process people become careless in
the formation of opinion increasingly tolerant of their own mistakes and
prone to hasty decisions
Change in social behavior with disrupted communications uncontrolled
affects and a reduced willingness to share information with team members
The degree of resolution of perception can decrease which may lead to
important details being missed
St Pierre (2011)
Fatigue and Perceived Medical Error
Higher levels of fatigue and distress are
independently associated with self-perceived
medical error
West (2009)
Fatigue Surgery and Complications
Surgeons who had limited opportunity for sleep had
significantly higher rates of complications than
those who had a longer sleep opportunity We did
not observe an increased rate of complication
among obstetriciansgynecologists who had limited
opportunity for sleep
Rothschild (2009)
Surgical Resident Fatigue
Residents were fatigued during 48 and impaired during 27 of their time awake Among all residents the mean amount of daily sleep was 53 hours Overall residents fatigue levels were predicted to increase the risk of medical error by 22 compared with well-rested historical control subjects Night-float residents were more impaired (P = 02) with an increased risk of medical error (P = 045)
McCormick (2012)
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun
First day of Residency
Working on-call and weekends
Lack of vacation causing burnout
Took vacation but tired from previous rotations
Holiday spirit and relaxation
Uncertainty about knowledge-base responsibility future plans
Improving weather more daylight
Vacation time in summer
Ready to start 2nd year more confident and knowing what to expect
Well
Being
Feel
Good
Okay
Distress
Despair
Orientation
Feel Good
Well-rested
OK
Feel
Fatigued
Sleepy
Well Being
Time
Fatigue and Sleep Deprivation Graph
Times of Increased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
What was most helpful
Times of Decreased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
How Does Fatigue Come Into Play in
the OR
How Do You Manage Fatigue in the
OR
Posture Wauben et al reported a high prevalence rate (80)
of discomfort in the neck shoulders and back areas
among 280 surgeons in Europe Liberman et al
reported a high prevalence rate of lsquolsquoinjuriesrsquorsquo in the
hands fingers (42) and 107 in the neck among
colorectal surgeons
A recent study in Hong Kong found high prevalence
rates of neck and back musculoskeletal symptoms
among general surgeons The 12-month prevalence
rate was 829 for neck symptoms 578 for the
shoulder and 681 in the lower back
Szeto et al A study of surgeonsrsquo postural muscle activity during open laparoscopic and
endovascular surgery Surg Endosc (2010) 241712ndash1721
McDonald (1998)
Attention and Pacing You do drift Its human nature but thats when the risk factor increases Of course your attention span is decent the first hour or two then it gradually decreases I think the peak is between an hour and four hours After four hours your attention span starts to lessen You have to be aware of your attention span As the operation gets lengthy you have to be careful that you dont start losing your patience because you want to finish You have to say to yourself No I should not rush I should take my time You have to tell yourself and remind yourself that when you start to rush you get into trouble You say I should slow down because its better for the patient and its better for merdquo
- Elite neurosurgeon
Sleep Deprivation
Sleep Deprivation
ldquoSleep loss creates sleepiness which can be
associated with decrements in vigilance reaction
time psychomotor co-ordination information
processing decision making (eg fixation on
certain aspects of a situation to the neglect of other
information)rdquo
Rosekind MR et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Recognizing Sleep Deprivation in
Residency and Fellowship
Repeatedly yawning and ldquonodding offrdquo during
conferences or other sedentary activities (driving)
Loss of ability to perform usual activities quickly
Poor memory concentration judgment
Irritability moodiness depression
Dozing off while writing notesorders or while
reviewing medicationslabs
Repeatedly checking your work
Tisha Wang MD UCLA The Effects of Sleep Deprivation and Implications for Residency Training
Sleepiness in residents is equivalent to that found in patients
with serious sleep disorders Mustafa and Strohl unpublished data Papp 2002
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Epworth Sleepiness Scale
Normal
Insomnia
Sleep Apnea
Residents
Narcolepsy
0
5
10
15
20
Mean 590 220 1170 1470 1750
Normal InsomniaSleep
ApneaResidents Narcolepsy
Some Individuals are More Fatigue
Resistant Than Others
People who prefer to be active early in the day
(ldquomorningnessrdquo) are often more affected by sleep
deprivation than people who are most alert in the
late evening hours (ldquoeveningnessrdquo)
Thus personal characteristics of being ldquolarksrdquo or
ldquoowlsrdquo seem to affect psychomotor performance
in the work environment
St Pierre (2011)
Sleep Inertia and the Pager
Sleep inertia refers to the cognitive
impairment present immediately on
awakening from sleep
The first 15-30 min after waking are a
vulnerable period and performance
decrements can exceed those after 24 hrs of
continuous wakefulness
Highlights risk of residents committing
fatigue-related errors when woken from sleep
by a page
Lockley (2007)
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
Objectives
Describe signs and symptoms of fatigue
Discuss the effects of fatigue and sleep
deprivation on well-being and performance and
Identify strategies for managing fatigue and sleep
debt
ldquoThe best decision makers are the ones who know
when not to trust themselvesrdquo
Dr R Baumeister
Basic Message
Fatigue and sleep deprivation are significant risk
factors for diminished performance and reduced
well-being
The anti-dote is active self-monitoring for fatigue
and sleep debt and
Choosing to make rest sleep and self-care a key
priority in daily activities
Self-Monitoring
Physical Sensation
ThinkingAttention
FeelingMotivation
Performance Indicators
Fatigue
Fatigue is a protective physiological function
signaling that the margin of effective performance
has been reached
People cannot reliably self-judge their level of
fatigue-related impairment
St Pierre et al 2011
Fatigue Demands Rest
People often react to tiredness only when their
performance has already decreased This is one of
the reasons why breaks are often taken too late
Recovery then takes more time compared with
situations when breaks are taken early
St Pierre et al 2011
Fatigue
ldquoFatiguerdquo can be thought of as the combined
influence of sleep homeostasis circadian rhythm
and time on task on performance capability
Van Dongen amp Hursh 2011
Other Conditions Linked with Fatigue
Fatigue can be related to anxiety depression
stress thyroid disease other medical conditions
medication side effects or career dissatisfaction
Residents may have a primary undiagnosed
sleep disorder such as obstructive sleep apnea
narcolepsy restless leg syndrome or insomnia
What creates fatigue in residency
training
FT = Total resident fatigue
FT =
FT = FSS + Few + Fpf FT = Total resident fatigue
FSS = Fatigue related to system design (circadian
rhythm disruption sleep deprivation fragmented sleep)
Few = Fatigue related to work and environmental
factors (task requirements physical work loads
workstation design physical factors team factors) and
Fpf = Fatigue related to the operatorrsquos personal
factors (health status nutritional status social and
domestic dictates)
Adapted from Schutte (2009)
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Primary
Sleep Disorders
(sleep apnea etc)
Fragmented Sleep
(pager phone calls)
Circadian Rhythm
Disruption
(night float rotating
shifts)
Insufficient Sleep
(on call sleep lossinadequate
recovery sleep)
EXCESSIVE DAYTIME SLEEPINESS
Fatigue amp Burnout
The characteristic symptoms of burnout are
persistent and excessive fatigue emotional
exhaustion and cognitive dysfunction Frequently
the condition also includes components of
depersonalization or cynicism toward
clientspatients and reduced personal efficacy with
a tendency to evaluate oneself negatively
Aringkerstedt (2011)
Burnout in Residency
Prevalence estimates range between 40ndash76
among internal medicine and pediatric residents
and 47ndash70 among surgery residents
McCray (2008)
Burnout and Sleep Deprivation
It has recently been demonstrated that burnout
scores are closely related to reports of disturbed
sleep
Aringkerstedt (2011)
Ego Depletion Decision Fatigue
and Task Performance
We find that the percentage of favorable rulings
drops gradually from 65 to nearly zero within
each decision session and returns abruptly to
65 after a break Danzigera (2011)
These studies demonstrated that ego depletion
coincides with decreases in blood glucose and
glucose supplementation attenuates the ego-
depletion effect relative to a sweetened placebo
Hagger (2010)
Fatigue Effects Alertness attention and vigilance are reduced People are able to sustain
concentration on a task for a shorter than usual period of time
Reduced motor performance (fine motor skills and eyendashhand coordination)
and a decrease effectiveness of motor tasks (speed and accuracy are
reduced)
Slowed reaction time and decision-making In order to reduce effort rule-
based decisions are preferred over knowledge-based decision-making
(principle of economy)
Impaired memory function manifested as a reduced ability both to learn and
to recall items
Motivational alteration of the thinking process people become careless in
the formation of opinion increasingly tolerant of their own mistakes and
prone to hasty decisions
Change in social behavior with disrupted communications uncontrolled
affects and a reduced willingness to share information with team members
The degree of resolution of perception can decrease which may lead to
important details being missed
St Pierre (2011)
Fatigue and Perceived Medical Error
Higher levels of fatigue and distress are
independently associated with self-perceived
medical error
West (2009)
Fatigue Surgery and Complications
Surgeons who had limited opportunity for sleep had
significantly higher rates of complications than
those who had a longer sleep opportunity We did
not observe an increased rate of complication
among obstetriciansgynecologists who had limited
opportunity for sleep
Rothschild (2009)
Surgical Resident Fatigue
Residents were fatigued during 48 and impaired during 27 of their time awake Among all residents the mean amount of daily sleep was 53 hours Overall residents fatigue levels were predicted to increase the risk of medical error by 22 compared with well-rested historical control subjects Night-float residents were more impaired (P = 02) with an increased risk of medical error (P = 045)
McCormick (2012)
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun
First day of Residency
Working on-call and weekends
Lack of vacation causing burnout
Took vacation but tired from previous rotations
Holiday spirit and relaxation
Uncertainty about knowledge-base responsibility future plans
Improving weather more daylight
Vacation time in summer
Ready to start 2nd year more confident and knowing what to expect
Well
Being
Feel
Good
Okay
Distress
Despair
Orientation
Feel Good
Well-rested
OK
Feel
Fatigued
Sleepy
Well Being
Time
Fatigue and Sleep Deprivation Graph
Times of Increased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
What was most helpful
Times of Decreased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
How Does Fatigue Come Into Play in
the OR
How Do You Manage Fatigue in the
OR
Posture Wauben et al reported a high prevalence rate (80)
of discomfort in the neck shoulders and back areas
among 280 surgeons in Europe Liberman et al
reported a high prevalence rate of lsquolsquoinjuriesrsquorsquo in the
hands fingers (42) and 107 in the neck among
colorectal surgeons
A recent study in Hong Kong found high prevalence
rates of neck and back musculoskeletal symptoms
among general surgeons The 12-month prevalence
rate was 829 for neck symptoms 578 for the
shoulder and 681 in the lower back
Szeto et al A study of surgeonsrsquo postural muscle activity during open laparoscopic and
endovascular surgery Surg Endosc (2010) 241712ndash1721
McDonald (1998)
Attention and Pacing You do drift Its human nature but thats when the risk factor increases Of course your attention span is decent the first hour or two then it gradually decreases I think the peak is between an hour and four hours After four hours your attention span starts to lessen You have to be aware of your attention span As the operation gets lengthy you have to be careful that you dont start losing your patience because you want to finish You have to say to yourself No I should not rush I should take my time You have to tell yourself and remind yourself that when you start to rush you get into trouble You say I should slow down because its better for the patient and its better for merdquo
- Elite neurosurgeon
Sleep Deprivation
Sleep Deprivation
ldquoSleep loss creates sleepiness which can be
associated with decrements in vigilance reaction
time psychomotor co-ordination information
processing decision making (eg fixation on
certain aspects of a situation to the neglect of other
information)rdquo
Rosekind MR et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Recognizing Sleep Deprivation in
Residency and Fellowship
Repeatedly yawning and ldquonodding offrdquo during
conferences or other sedentary activities (driving)
Loss of ability to perform usual activities quickly
Poor memory concentration judgment
Irritability moodiness depression
Dozing off while writing notesorders or while
reviewing medicationslabs
Repeatedly checking your work
Tisha Wang MD UCLA The Effects of Sleep Deprivation and Implications for Residency Training
Sleepiness in residents is equivalent to that found in patients
with serious sleep disorders Mustafa and Strohl unpublished data Papp 2002
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Epworth Sleepiness Scale
Normal
Insomnia
Sleep Apnea
Residents
Narcolepsy
0
5
10
15
20
Mean 590 220 1170 1470 1750
Normal InsomniaSleep
ApneaResidents Narcolepsy
Some Individuals are More Fatigue
Resistant Than Others
People who prefer to be active early in the day
(ldquomorningnessrdquo) are often more affected by sleep
deprivation than people who are most alert in the
late evening hours (ldquoeveningnessrdquo)
Thus personal characteristics of being ldquolarksrdquo or
ldquoowlsrdquo seem to affect psychomotor performance
in the work environment
St Pierre (2011)
Sleep Inertia and the Pager
Sleep inertia refers to the cognitive
impairment present immediately on
awakening from sleep
The first 15-30 min after waking are a
vulnerable period and performance
decrements can exceed those after 24 hrs of
continuous wakefulness
Highlights risk of residents committing
fatigue-related errors when woken from sleep
by a page
Lockley (2007)
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
ldquoThe best decision makers are the ones who know
when not to trust themselvesrdquo
Dr R Baumeister
Basic Message
Fatigue and sleep deprivation are significant risk
factors for diminished performance and reduced
well-being
The anti-dote is active self-monitoring for fatigue
and sleep debt and
Choosing to make rest sleep and self-care a key
priority in daily activities
Self-Monitoring
Physical Sensation
ThinkingAttention
FeelingMotivation
Performance Indicators
Fatigue
Fatigue is a protective physiological function
signaling that the margin of effective performance
has been reached
People cannot reliably self-judge their level of
fatigue-related impairment
St Pierre et al 2011
Fatigue Demands Rest
People often react to tiredness only when their
performance has already decreased This is one of
the reasons why breaks are often taken too late
Recovery then takes more time compared with
situations when breaks are taken early
St Pierre et al 2011
Fatigue
ldquoFatiguerdquo can be thought of as the combined
influence of sleep homeostasis circadian rhythm
and time on task on performance capability
Van Dongen amp Hursh 2011
Other Conditions Linked with Fatigue
Fatigue can be related to anxiety depression
stress thyroid disease other medical conditions
medication side effects or career dissatisfaction
Residents may have a primary undiagnosed
sleep disorder such as obstructive sleep apnea
narcolepsy restless leg syndrome or insomnia
What creates fatigue in residency
training
FT = Total resident fatigue
FT =
FT = FSS + Few + Fpf FT = Total resident fatigue
FSS = Fatigue related to system design (circadian
rhythm disruption sleep deprivation fragmented sleep)
Few = Fatigue related to work and environmental
factors (task requirements physical work loads
workstation design physical factors team factors) and
Fpf = Fatigue related to the operatorrsquos personal
factors (health status nutritional status social and
domestic dictates)
Adapted from Schutte (2009)
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Primary
Sleep Disorders
(sleep apnea etc)
Fragmented Sleep
(pager phone calls)
Circadian Rhythm
Disruption
(night float rotating
shifts)
Insufficient Sleep
(on call sleep lossinadequate
recovery sleep)
EXCESSIVE DAYTIME SLEEPINESS
Fatigue amp Burnout
The characteristic symptoms of burnout are
persistent and excessive fatigue emotional
exhaustion and cognitive dysfunction Frequently
the condition also includes components of
depersonalization or cynicism toward
clientspatients and reduced personal efficacy with
a tendency to evaluate oneself negatively
Aringkerstedt (2011)
Burnout in Residency
Prevalence estimates range between 40ndash76
among internal medicine and pediatric residents
and 47ndash70 among surgery residents
McCray (2008)
Burnout and Sleep Deprivation
It has recently been demonstrated that burnout
scores are closely related to reports of disturbed
sleep
Aringkerstedt (2011)
Ego Depletion Decision Fatigue
and Task Performance
We find that the percentage of favorable rulings
drops gradually from 65 to nearly zero within
each decision session and returns abruptly to
65 after a break Danzigera (2011)
These studies demonstrated that ego depletion
coincides with decreases in blood glucose and
glucose supplementation attenuates the ego-
depletion effect relative to a sweetened placebo
Hagger (2010)
Fatigue Effects Alertness attention and vigilance are reduced People are able to sustain
concentration on a task for a shorter than usual period of time
Reduced motor performance (fine motor skills and eyendashhand coordination)
and a decrease effectiveness of motor tasks (speed and accuracy are
reduced)
Slowed reaction time and decision-making In order to reduce effort rule-
based decisions are preferred over knowledge-based decision-making
(principle of economy)
Impaired memory function manifested as a reduced ability both to learn and
to recall items
Motivational alteration of the thinking process people become careless in
the formation of opinion increasingly tolerant of their own mistakes and
prone to hasty decisions
Change in social behavior with disrupted communications uncontrolled
affects and a reduced willingness to share information with team members
The degree of resolution of perception can decrease which may lead to
important details being missed
St Pierre (2011)
Fatigue and Perceived Medical Error
Higher levels of fatigue and distress are
independently associated with self-perceived
medical error
West (2009)
Fatigue Surgery and Complications
Surgeons who had limited opportunity for sleep had
significantly higher rates of complications than
those who had a longer sleep opportunity We did
not observe an increased rate of complication
among obstetriciansgynecologists who had limited
opportunity for sleep
Rothschild (2009)
Surgical Resident Fatigue
Residents were fatigued during 48 and impaired during 27 of their time awake Among all residents the mean amount of daily sleep was 53 hours Overall residents fatigue levels were predicted to increase the risk of medical error by 22 compared with well-rested historical control subjects Night-float residents were more impaired (P = 02) with an increased risk of medical error (P = 045)
McCormick (2012)
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun
First day of Residency
Working on-call and weekends
Lack of vacation causing burnout
Took vacation but tired from previous rotations
Holiday spirit and relaxation
Uncertainty about knowledge-base responsibility future plans
Improving weather more daylight
Vacation time in summer
Ready to start 2nd year more confident and knowing what to expect
Well
Being
Feel
Good
Okay
Distress
Despair
Orientation
Feel Good
Well-rested
OK
Feel
Fatigued
Sleepy
Well Being
Time
Fatigue and Sleep Deprivation Graph
Times of Increased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
What was most helpful
Times of Decreased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
How Does Fatigue Come Into Play in
the OR
How Do You Manage Fatigue in the
OR
Posture Wauben et al reported a high prevalence rate (80)
of discomfort in the neck shoulders and back areas
among 280 surgeons in Europe Liberman et al
reported a high prevalence rate of lsquolsquoinjuriesrsquorsquo in the
hands fingers (42) and 107 in the neck among
colorectal surgeons
A recent study in Hong Kong found high prevalence
rates of neck and back musculoskeletal symptoms
among general surgeons The 12-month prevalence
rate was 829 for neck symptoms 578 for the
shoulder and 681 in the lower back
Szeto et al A study of surgeonsrsquo postural muscle activity during open laparoscopic and
endovascular surgery Surg Endosc (2010) 241712ndash1721
McDonald (1998)
Attention and Pacing You do drift Its human nature but thats when the risk factor increases Of course your attention span is decent the first hour or two then it gradually decreases I think the peak is between an hour and four hours After four hours your attention span starts to lessen You have to be aware of your attention span As the operation gets lengthy you have to be careful that you dont start losing your patience because you want to finish You have to say to yourself No I should not rush I should take my time You have to tell yourself and remind yourself that when you start to rush you get into trouble You say I should slow down because its better for the patient and its better for merdquo
- Elite neurosurgeon
Sleep Deprivation
Sleep Deprivation
ldquoSleep loss creates sleepiness which can be
associated with decrements in vigilance reaction
time psychomotor co-ordination information
processing decision making (eg fixation on
certain aspects of a situation to the neglect of other
information)rdquo
Rosekind MR et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Recognizing Sleep Deprivation in
Residency and Fellowship
Repeatedly yawning and ldquonodding offrdquo during
conferences or other sedentary activities (driving)
Loss of ability to perform usual activities quickly
Poor memory concentration judgment
Irritability moodiness depression
Dozing off while writing notesorders or while
reviewing medicationslabs
Repeatedly checking your work
Tisha Wang MD UCLA The Effects of Sleep Deprivation and Implications for Residency Training
Sleepiness in residents is equivalent to that found in patients
with serious sleep disorders Mustafa and Strohl unpublished data Papp 2002
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Epworth Sleepiness Scale
Normal
Insomnia
Sleep Apnea
Residents
Narcolepsy
0
5
10
15
20
Mean 590 220 1170 1470 1750
Normal InsomniaSleep
ApneaResidents Narcolepsy
Some Individuals are More Fatigue
Resistant Than Others
People who prefer to be active early in the day
(ldquomorningnessrdquo) are often more affected by sleep
deprivation than people who are most alert in the
late evening hours (ldquoeveningnessrdquo)
Thus personal characteristics of being ldquolarksrdquo or
ldquoowlsrdquo seem to affect psychomotor performance
in the work environment
St Pierre (2011)
Sleep Inertia and the Pager
Sleep inertia refers to the cognitive
impairment present immediately on
awakening from sleep
The first 15-30 min after waking are a
vulnerable period and performance
decrements can exceed those after 24 hrs of
continuous wakefulness
Highlights risk of residents committing
fatigue-related errors when woken from sleep
by a page
Lockley (2007)
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300

Basic Message
Fatigue and sleep deprivation are significant risk
factors for diminished performance and reduced
well-being
The anti-dote is active self-monitoring for fatigue
and sleep debt and
Choosing to make rest sleep and self-care a key
priority in daily activities
Self-Monitoring
Physical Sensation
ThinkingAttention
FeelingMotivation
Performance Indicators
Fatigue
Fatigue is a protective physiological function
signaling that the margin of effective performance
has been reached
People cannot reliably self-judge their level of
fatigue-related impairment
St Pierre et al 2011
Fatigue Demands Rest
People often react to tiredness only when their
performance has already decreased This is one of
the reasons why breaks are often taken too late
Recovery then takes more time compared with
situations when breaks are taken early
St Pierre et al 2011
Fatigue
ldquoFatiguerdquo can be thought of as the combined
influence of sleep homeostasis circadian rhythm
and time on task on performance capability
Van Dongen amp Hursh 2011
Other Conditions Linked with Fatigue
Fatigue can be related to anxiety depression
stress thyroid disease other medical conditions
medication side effects or career dissatisfaction
Residents may have a primary undiagnosed
sleep disorder such as obstructive sleep apnea
narcolepsy restless leg syndrome or insomnia
What creates fatigue in residency
training
FT = Total resident fatigue
FT =
FT = FSS + Few + Fpf FT = Total resident fatigue
FSS = Fatigue related to system design (circadian
rhythm disruption sleep deprivation fragmented sleep)
Few = Fatigue related to work and environmental
factors (task requirements physical work loads
workstation design physical factors team factors) and
Fpf = Fatigue related to the operatorrsquos personal
factors (health status nutritional status social and
domestic dictates)
Adapted from Schutte (2009)
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Primary
Sleep Disorders
(sleep apnea etc)
Fragmented Sleep
(pager phone calls)
Circadian Rhythm
Disruption
(night float rotating
shifts)
Insufficient Sleep
(on call sleep lossinadequate
recovery sleep)
EXCESSIVE DAYTIME SLEEPINESS
Fatigue amp Burnout
The characteristic symptoms of burnout are
persistent and excessive fatigue emotional
exhaustion and cognitive dysfunction Frequently
the condition also includes components of
depersonalization or cynicism toward
clientspatients and reduced personal efficacy with
a tendency to evaluate oneself negatively
Aringkerstedt (2011)
Burnout in Residency
Prevalence estimates range between 40ndash76
among internal medicine and pediatric residents
and 47ndash70 among surgery residents
McCray (2008)
Burnout and Sleep Deprivation
It has recently been demonstrated that burnout
scores are closely related to reports of disturbed
sleep
Aringkerstedt (2011)
Ego Depletion Decision Fatigue
and Task Performance
We find that the percentage of favorable rulings
drops gradually from 65 to nearly zero within
each decision session and returns abruptly to
65 after a break Danzigera (2011)
These studies demonstrated that ego depletion
coincides with decreases in blood glucose and
glucose supplementation attenuates the ego-
depletion effect relative to a sweetened placebo
Hagger (2010)
Fatigue Effects Alertness attention and vigilance are reduced People are able to sustain
concentration on a task for a shorter than usual period of time
Reduced motor performance (fine motor skills and eyendashhand coordination)
and a decrease effectiveness of motor tasks (speed and accuracy are
reduced)
Slowed reaction time and decision-making In order to reduce effort rule-
based decisions are preferred over knowledge-based decision-making
(principle of economy)
Impaired memory function manifested as a reduced ability both to learn and
to recall items
Motivational alteration of the thinking process people become careless in
the formation of opinion increasingly tolerant of their own mistakes and
prone to hasty decisions
Change in social behavior with disrupted communications uncontrolled
affects and a reduced willingness to share information with team members
The degree of resolution of perception can decrease which may lead to
important details being missed
St Pierre (2011)
Fatigue and Perceived Medical Error
Higher levels of fatigue and distress are
independently associated with self-perceived
medical error
West (2009)
Fatigue Surgery and Complications
Surgeons who had limited opportunity for sleep had
significantly higher rates of complications than
those who had a longer sleep opportunity We did
not observe an increased rate of complication
among obstetriciansgynecologists who had limited
opportunity for sleep
Rothschild (2009)
Surgical Resident Fatigue
Residents were fatigued during 48 and impaired during 27 of their time awake Among all residents the mean amount of daily sleep was 53 hours Overall residents fatigue levels were predicted to increase the risk of medical error by 22 compared with well-rested historical control subjects Night-float residents were more impaired (P = 02) with an increased risk of medical error (P = 045)
McCormick (2012)
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun
First day of Residency
Working on-call and weekends
Lack of vacation causing burnout
Took vacation but tired from previous rotations
Holiday spirit and relaxation
Uncertainty about knowledge-base responsibility future plans
Improving weather more daylight
Vacation time in summer
Ready to start 2nd year more confident and knowing what to expect
Well
Being
Feel
Good
Okay
Distress
Despair
Orientation
Feel Good
Well-rested
OK
Feel
Fatigued
Sleepy
Well Being
Time
Fatigue and Sleep Deprivation Graph
Times of Increased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
What was most helpful
Times of Decreased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
How Does Fatigue Come Into Play in
the OR
How Do You Manage Fatigue in the
OR
Posture Wauben et al reported a high prevalence rate (80)
of discomfort in the neck shoulders and back areas
among 280 surgeons in Europe Liberman et al
reported a high prevalence rate of lsquolsquoinjuriesrsquorsquo in the
hands fingers (42) and 107 in the neck among
colorectal surgeons
A recent study in Hong Kong found high prevalence
rates of neck and back musculoskeletal symptoms
among general surgeons The 12-month prevalence
rate was 829 for neck symptoms 578 for the
shoulder and 681 in the lower back
Szeto et al A study of surgeonsrsquo postural muscle activity during open laparoscopic and
endovascular surgery Surg Endosc (2010) 241712ndash1721
McDonald (1998)
Attention and Pacing You do drift Its human nature but thats when the risk factor increases Of course your attention span is decent the first hour or two then it gradually decreases I think the peak is between an hour and four hours After four hours your attention span starts to lessen You have to be aware of your attention span As the operation gets lengthy you have to be careful that you dont start losing your patience because you want to finish You have to say to yourself No I should not rush I should take my time You have to tell yourself and remind yourself that when you start to rush you get into trouble You say I should slow down because its better for the patient and its better for merdquo
- Elite neurosurgeon
Sleep Deprivation
Sleep Deprivation
ldquoSleep loss creates sleepiness which can be
associated with decrements in vigilance reaction
time psychomotor co-ordination information
processing decision making (eg fixation on
certain aspects of a situation to the neglect of other
information)rdquo
Rosekind MR et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Recognizing Sleep Deprivation in
Residency and Fellowship
Repeatedly yawning and ldquonodding offrdquo during
conferences or other sedentary activities (driving)
Loss of ability to perform usual activities quickly
Poor memory concentration judgment
Irritability moodiness depression
Dozing off while writing notesorders or while
reviewing medicationslabs
Repeatedly checking your work
Tisha Wang MD UCLA The Effects of Sleep Deprivation and Implications for Residency Training
Sleepiness in residents is equivalent to that found in patients
with serious sleep disorders Mustafa and Strohl unpublished data Papp 2002
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Epworth Sleepiness Scale
Normal
Insomnia
Sleep Apnea
Residents
Narcolepsy
0
5
10
15
20
Mean 590 220 1170 1470 1750
Normal InsomniaSleep
ApneaResidents Narcolepsy
Some Individuals are More Fatigue
Resistant Than Others
People who prefer to be active early in the day
(ldquomorningnessrdquo) are often more affected by sleep
deprivation than people who are most alert in the
late evening hours (ldquoeveningnessrdquo)
Thus personal characteristics of being ldquolarksrdquo or
ldquoowlsrdquo seem to affect psychomotor performance
in the work environment
St Pierre (2011)
Sleep Inertia and the Pager
Sleep inertia refers to the cognitive
impairment present immediately on
awakening from sleep
The first 15-30 min after waking are a
vulnerable period and performance
decrements can exceed those after 24 hrs of
continuous wakefulness
Highlights risk of residents committing
fatigue-related errors when woken from sleep
by a page
Lockley (2007)
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
Self-Monitoring
Physical Sensation
ThinkingAttention
FeelingMotivation
Performance Indicators
Fatigue
Fatigue is a protective physiological function
signaling that the margin of effective performance
has been reached
People cannot reliably self-judge their level of
fatigue-related impairment
St Pierre et al 2011
Fatigue Demands Rest
People often react to tiredness only when their
performance has already decreased This is one of
the reasons why breaks are often taken too late
Recovery then takes more time compared with
situations when breaks are taken early
St Pierre et al 2011
Fatigue
ldquoFatiguerdquo can be thought of as the combined
influence of sleep homeostasis circadian rhythm
and time on task on performance capability
Van Dongen amp Hursh 2011
Other Conditions Linked with Fatigue
Fatigue can be related to anxiety depression
stress thyroid disease other medical conditions
medication side effects or career dissatisfaction
Residents may have a primary undiagnosed
sleep disorder such as obstructive sleep apnea
narcolepsy restless leg syndrome or insomnia
What creates fatigue in residency
training
FT = Total resident fatigue
FT =
FT = FSS + Few + Fpf FT = Total resident fatigue
FSS = Fatigue related to system design (circadian
rhythm disruption sleep deprivation fragmented sleep)
Few = Fatigue related to work and environmental
factors (task requirements physical work loads
workstation design physical factors team factors) and
Fpf = Fatigue related to the operatorrsquos personal
factors (health status nutritional status social and
domestic dictates)
Adapted from Schutte (2009)
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Primary
Sleep Disorders
(sleep apnea etc)
Fragmented Sleep
(pager phone calls)
Circadian Rhythm
Disruption
(night float rotating
shifts)
Insufficient Sleep
(on call sleep lossinadequate
recovery sleep)
EXCESSIVE DAYTIME SLEEPINESS
Fatigue amp Burnout
The characteristic symptoms of burnout are
persistent and excessive fatigue emotional
exhaustion and cognitive dysfunction Frequently
the condition also includes components of
depersonalization or cynicism toward
clientspatients and reduced personal efficacy with
a tendency to evaluate oneself negatively
Aringkerstedt (2011)
Burnout in Residency
Prevalence estimates range between 40ndash76
among internal medicine and pediatric residents
and 47ndash70 among surgery residents
McCray (2008)
Burnout and Sleep Deprivation
It has recently been demonstrated that burnout
scores are closely related to reports of disturbed
sleep
Aringkerstedt (2011)
Ego Depletion Decision Fatigue
and Task Performance
We find that the percentage of favorable rulings
drops gradually from 65 to nearly zero within
each decision session and returns abruptly to
65 after a break Danzigera (2011)
These studies demonstrated that ego depletion
coincides with decreases in blood glucose and
glucose supplementation attenuates the ego-
depletion effect relative to a sweetened placebo
Hagger (2010)
Fatigue Effects Alertness attention and vigilance are reduced People are able to sustain
concentration on a task for a shorter than usual period of time
Reduced motor performance (fine motor skills and eyendashhand coordination)
and a decrease effectiveness of motor tasks (speed and accuracy are
reduced)
Slowed reaction time and decision-making In order to reduce effort rule-
based decisions are preferred over knowledge-based decision-making
(principle of economy)
Impaired memory function manifested as a reduced ability both to learn and
to recall items
Motivational alteration of the thinking process people become careless in
the formation of opinion increasingly tolerant of their own mistakes and
prone to hasty decisions
Change in social behavior with disrupted communications uncontrolled
affects and a reduced willingness to share information with team members
The degree of resolution of perception can decrease which may lead to
important details being missed
St Pierre (2011)
Fatigue and Perceived Medical Error
Higher levels of fatigue and distress are
independently associated with self-perceived
medical error
West (2009)
Fatigue Surgery and Complications
Surgeons who had limited opportunity for sleep had
significantly higher rates of complications than
those who had a longer sleep opportunity We did
not observe an increased rate of complication
among obstetriciansgynecologists who had limited
opportunity for sleep
Rothschild (2009)
Surgical Resident Fatigue
Residents were fatigued during 48 and impaired during 27 of their time awake Among all residents the mean amount of daily sleep was 53 hours Overall residents fatigue levels were predicted to increase the risk of medical error by 22 compared with well-rested historical control subjects Night-float residents were more impaired (P = 02) with an increased risk of medical error (P = 045)
McCormick (2012)
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun
First day of Residency
Working on-call and weekends
Lack of vacation causing burnout
Took vacation but tired from previous rotations
Holiday spirit and relaxation
Uncertainty about knowledge-base responsibility future plans
Improving weather more daylight
Vacation time in summer
Ready to start 2nd year more confident and knowing what to expect
Well
Being
Feel
Good
Okay
Distress
Despair
Orientation
Feel Good
Well-rested
OK
Feel
Fatigued
Sleepy
Well Being
Time
Fatigue and Sleep Deprivation Graph
Times of Increased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
What was most helpful
Times of Decreased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
How Does Fatigue Come Into Play in
the OR
How Do You Manage Fatigue in the
OR
Posture Wauben et al reported a high prevalence rate (80)
of discomfort in the neck shoulders and back areas
among 280 surgeons in Europe Liberman et al
reported a high prevalence rate of lsquolsquoinjuriesrsquorsquo in the
hands fingers (42) and 107 in the neck among
colorectal surgeons
A recent study in Hong Kong found high prevalence
rates of neck and back musculoskeletal symptoms
among general surgeons The 12-month prevalence
rate was 829 for neck symptoms 578 for the
shoulder and 681 in the lower back
Szeto et al A study of surgeonsrsquo postural muscle activity during open laparoscopic and
endovascular surgery Surg Endosc (2010) 241712ndash1721
McDonald (1998)
Attention and Pacing You do drift Its human nature but thats when the risk factor increases Of course your attention span is decent the first hour or two then it gradually decreases I think the peak is between an hour and four hours After four hours your attention span starts to lessen You have to be aware of your attention span As the operation gets lengthy you have to be careful that you dont start losing your patience because you want to finish You have to say to yourself No I should not rush I should take my time You have to tell yourself and remind yourself that when you start to rush you get into trouble You say I should slow down because its better for the patient and its better for merdquo
- Elite neurosurgeon
Sleep Deprivation
Sleep Deprivation
ldquoSleep loss creates sleepiness which can be
associated with decrements in vigilance reaction
time psychomotor co-ordination information
processing decision making (eg fixation on
certain aspects of a situation to the neglect of other
information)rdquo
Rosekind MR et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Recognizing Sleep Deprivation in
Residency and Fellowship
Repeatedly yawning and ldquonodding offrdquo during
conferences or other sedentary activities (driving)
Loss of ability to perform usual activities quickly
Poor memory concentration judgment
Irritability moodiness depression
Dozing off while writing notesorders or while
reviewing medicationslabs
Repeatedly checking your work
Tisha Wang MD UCLA The Effects of Sleep Deprivation and Implications for Residency Training
Sleepiness in residents is equivalent to that found in patients
with serious sleep disorders Mustafa and Strohl unpublished data Papp 2002
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Epworth Sleepiness Scale
Normal
Insomnia
Sleep Apnea
Residents
Narcolepsy
0
5
10
15
20
Mean 590 220 1170 1470 1750
Normal InsomniaSleep
ApneaResidents Narcolepsy
Some Individuals are More Fatigue
Resistant Than Others
People who prefer to be active early in the day
(ldquomorningnessrdquo) are often more affected by sleep
deprivation than people who are most alert in the
late evening hours (ldquoeveningnessrdquo)
Thus personal characteristics of being ldquolarksrdquo or
ldquoowlsrdquo seem to affect psychomotor performance
in the work environment
St Pierre (2011)
Sleep Inertia and the Pager
Sleep inertia refers to the cognitive
impairment present immediately on
awakening from sleep
The first 15-30 min after waking are a
vulnerable period and performance
decrements can exceed those after 24 hrs of
continuous wakefulness
Highlights risk of residents committing
fatigue-related errors when woken from sleep
by a page
Lockley (2007)
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
Fatigue
Fatigue is a protective physiological function
signaling that the margin of effective performance
has been reached
People cannot reliably self-judge their level of
fatigue-related impairment
St Pierre et al 2011
Fatigue Demands Rest
People often react to tiredness only when their
performance has already decreased This is one of
the reasons why breaks are often taken too late
Recovery then takes more time compared with
situations when breaks are taken early
St Pierre et al 2011
Fatigue
ldquoFatiguerdquo can be thought of as the combined
influence of sleep homeostasis circadian rhythm
and time on task on performance capability
Van Dongen amp Hursh 2011
Other Conditions Linked with Fatigue
Fatigue can be related to anxiety depression
stress thyroid disease other medical conditions
medication side effects or career dissatisfaction
Residents may have a primary undiagnosed
sleep disorder such as obstructive sleep apnea
narcolepsy restless leg syndrome or insomnia
What creates fatigue in residency
training
FT = Total resident fatigue
FT =
FT = FSS + Few + Fpf FT = Total resident fatigue
FSS = Fatigue related to system design (circadian
rhythm disruption sleep deprivation fragmented sleep)
Few = Fatigue related to work and environmental
factors (task requirements physical work loads
workstation design physical factors team factors) and
Fpf = Fatigue related to the operatorrsquos personal
factors (health status nutritional status social and
domestic dictates)
Adapted from Schutte (2009)
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Primary
Sleep Disorders
(sleep apnea etc)
Fragmented Sleep
(pager phone calls)
Circadian Rhythm
Disruption
(night float rotating
shifts)
Insufficient Sleep
(on call sleep lossinadequate
recovery sleep)
EXCESSIVE DAYTIME SLEEPINESS
Fatigue amp Burnout
The characteristic symptoms of burnout are
persistent and excessive fatigue emotional
exhaustion and cognitive dysfunction Frequently
the condition also includes components of
depersonalization or cynicism toward
clientspatients and reduced personal efficacy with
a tendency to evaluate oneself negatively
Aringkerstedt (2011)
Burnout in Residency
Prevalence estimates range between 40ndash76
among internal medicine and pediatric residents
and 47ndash70 among surgery residents
McCray (2008)
Burnout and Sleep Deprivation
It has recently been demonstrated that burnout
scores are closely related to reports of disturbed
sleep
Aringkerstedt (2011)
Ego Depletion Decision Fatigue
and Task Performance
We find that the percentage of favorable rulings
drops gradually from 65 to nearly zero within
each decision session and returns abruptly to
65 after a break Danzigera (2011)
These studies demonstrated that ego depletion
coincides with decreases in blood glucose and
glucose supplementation attenuates the ego-
depletion effect relative to a sweetened placebo
Hagger (2010)
Fatigue Effects Alertness attention and vigilance are reduced People are able to sustain
concentration on a task for a shorter than usual period of time
Reduced motor performance (fine motor skills and eyendashhand coordination)
and a decrease effectiveness of motor tasks (speed and accuracy are
reduced)
Slowed reaction time and decision-making In order to reduce effort rule-
based decisions are preferred over knowledge-based decision-making
(principle of economy)
Impaired memory function manifested as a reduced ability both to learn and
to recall items
Motivational alteration of the thinking process people become careless in
the formation of opinion increasingly tolerant of their own mistakes and
prone to hasty decisions
Change in social behavior with disrupted communications uncontrolled
affects and a reduced willingness to share information with team members
The degree of resolution of perception can decrease which may lead to
important details being missed
St Pierre (2011)
Fatigue and Perceived Medical Error
Higher levels of fatigue and distress are
independently associated with self-perceived
medical error
West (2009)
Fatigue Surgery and Complications
Surgeons who had limited opportunity for sleep had
significantly higher rates of complications than
those who had a longer sleep opportunity We did
not observe an increased rate of complication
among obstetriciansgynecologists who had limited
opportunity for sleep
Rothschild (2009)
Surgical Resident Fatigue
Residents were fatigued during 48 and impaired during 27 of their time awake Among all residents the mean amount of daily sleep was 53 hours Overall residents fatigue levels were predicted to increase the risk of medical error by 22 compared with well-rested historical control subjects Night-float residents were more impaired (P = 02) with an increased risk of medical error (P = 045)
McCormick (2012)
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun
First day of Residency
Working on-call and weekends
Lack of vacation causing burnout
Took vacation but tired from previous rotations
Holiday spirit and relaxation
Uncertainty about knowledge-base responsibility future plans
Improving weather more daylight
Vacation time in summer
Ready to start 2nd year more confident and knowing what to expect
Well
Being
Feel
Good
Okay
Distress
Despair
Orientation
Feel Good
Well-rested
OK
Feel
Fatigued
Sleepy
Well Being
Time
Fatigue and Sleep Deprivation Graph
Times of Increased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
What was most helpful
Times of Decreased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
How Does Fatigue Come Into Play in
the OR
How Do You Manage Fatigue in the
OR
Posture Wauben et al reported a high prevalence rate (80)
of discomfort in the neck shoulders and back areas
among 280 surgeons in Europe Liberman et al
reported a high prevalence rate of lsquolsquoinjuriesrsquorsquo in the
hands fingers (42) and 107 in the neck among
colorectal surgeons
A recent study in Hong Kong found high prevalence
rates of neck and back musculoskeletal symptoms
among general surgeons The 12-month prevalence
rate was 829 for neck symptoms 578 for the
shoulder and 681 in the lower back
Szeto et al A study of surgeonsrsquo postural muscle activity during open laparoscopic and
endovascular surgery Surg Endosc (2010) 241712ndash1721
McDonald (1998)
Attention and Pacing You do drift Its human nature but thats when the risk factor increases Of course your attention span is decent the first hour or two then it gradually decreases I think the peak is between an hour and four hours After four hours your attention span starts to lessen You have to be aware of your attention span As the operation gets lengthy you have to be careful that you dont start losing your patience because you want to finish You have to say to yourself No I should not rush I should take my time You have to tell yourself and remind yourself that when you start to rush you get into trouble You say I should slow down because its better for the patient and its better for merdquo
- Elite neurosurgeon
Sleep Deprivation
Sleep Deprivation
ldquoSleep loss creates sleepiness which can be
associated with decrements in vigilance reaction
time psychomotor co-ordination information
processing decision making (eg fixation on
certain aspects of a situation to the neglect of other
information)rdquo
Rosekind MR et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Recognizing Sleep Deprivation in
Residency and Fellowship
Repeatedly yawning and ldquonodding offrdquo during
conferences or other sedentary activities (driving)
Loss of ability to perform usual activities quickly
Poor memory concentration judgment
Irritability moodiness depression
Dozing off while writing notesorders or while
reviewing medicationslabs
Repeatedly checking your work
Tisha Wang MD UCLA The Effects of Sleep Deprivation and Implications for Residency Training
Sleepiness in residents is equivalent to that found in patients
with serious sleep disorders Mustafa and Strohl unpublished data Papp 2002
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Epworth Sleepiness Scale
Normal
Insomnia
Sleep Apnea
Residents
Narcolepsy
0
5
10
15
20
Mean 590 220 1170 1470 1750
Normal InsomniaSleep
ApneaResidents Narcolepsy
Some Individuals are More Fatigue
Resistant Than Others
People who prefer to be active early in the day
(ldquomorningnessrdquo) are often more affected by sleep
deprivation than people who are most alert in the
late evening hours (ldquoeveningnessrdquo)
Thus personal characteristics of being ldquolarksrdquo or
ldquoowlsrdquo seem to affect psychomotor performance
in the work environment
St Pierre (2011)
Sleep Inertia and the Pager
Sleep inertia refers to the cognitive
impairment present immediately on
awakening from sleep
The first 15-30 min after waking are a
vulnerable period and performance
decrements can exceed those after 24 hrs of
continuous wakefulness
Highlights risk of residents committing
fatigue-related errors when woken from sleep
by a page
Lockley (2007)
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
Fatigue Demands Rest
People often react to tiredness only when their
performance has already decreased This is one of
the reasons why breaks are often taken too late
Recovery then takes more time compared with
situations when breaks are taken early
St Pierre et al 2011
Fatigue
ldquoFatiguerdquo can be thought of as the combined
influence of sleep homeostasis circadian rhythm
and time on task on performance capability
Van Dongen amp Hursh 2011
Other Conditions Linked with Fatigue
Fatigue can be related to anxiety depression
stress thyroid disease other medical conditions
medication side effects or career dissatisfaction
Residents may have a primary undiagnosed
sleep disorder such as obstructive sleep apnea
narcolepsy restless leg syndrome or insomnia
What creates fatigue in residency
training
FT = Total resident fatigue
FT =
FT = FSS + Few + Fpf FT = Total resident fatigue
FSS = Fatigue related to system design (circadian
rhythm disruption sleep deprivation fragmented sleep)
Few = Fatigue related to work and environmental
factors (task requirements physical work loads
workstation design physical factors team factors) and
Fpf = Fatigue related to the operatorrsquos personal
factors (health status nutritional status social and
domestic dictates)
Adapted from Schutte (2009)
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Primary
Sleep Disorders
(sleep apnea etc)
Fragmented Sleep
(pager phone calls)
Circadian Rhythm
Disruption
(night float rotating
shifts)
Insufficient Sleep
(on call sleep lossinadequate
recovery sleep)
EXCESSIVE DAYTIME SLEEPINESS
Fatigue amp Burnout
The characteristic symptoms of burnout are
persistent and excessive fatigue emotional
exhaustion and cognitive dysfunction Frequently
the condition also includes components of
depersonalization or cynicism toward
clientspatients and reduced personal efficacy with
a tendency to evaluate oneself negatively
Aringkerstedt (2011)
Burnout in Residency
Prevalence estimates range between 40ndash76
among internal medicine and pediatric residents
and 47ndash70 among surgery residents
McCray (2008)
Burnout and Sleep Deprivation
It has recently been demonstrated that burnout
scores are closely related to reports of disturbed
sleep
Aringkerstedt (2011)
Ego Depletion Decision Fatigue
and Task Performance
We find that the percentage of favorable rulings
drops gradually from 65 to nearly zero within
each decision session and returns abruptly to
65 after a break Danzigera (2011)
These studies demonstrated that ego depletion
coincides with decreases in blood glucose and
glucose supplementation attenuates the ego-
depletion effect relative to a sweetened placebo
Hagger (2010)
Fatigue Effects Alertness attention and vigilance are reduced People are able to sustain
concentration on a task for a shorter than usual period of time
Reduced motor performance (fine motor skills and eyendashhand coordination)
and a decrease effectiveness of motor tasks (speed and accuracy are
reduced)
Slowed reaction time and decision-making In order to reduce effort rule-
based decisions are preferred over knowledge-based decision-making
(principle of economy)
Impaired memory function manifested as a reduced ability both to learn and
to recall items
Motivational alteration of the thinking process people become careless in
the formation of opinion increasingly tolerant of their own mistakes and
prone to hasty decisions
Change in social behavior with disrupted communications uncontrolled
affects and a reduced willingness to share information with team members
The degree of resolution of perception can decrease which may lead to
important details being missed
St Pierre (2011)
Fatigue and Perceived Medical Error
Higher levels of fatigue and distress are
independently associated with self-perceived
medical error
West (2009)
Fatigue Surgery and Complications
Surgeons who had limited opportunity for sleep had
significantly higher rates of complications than
those who had a longer sleep opportunity We did
not observe an increased rate of complication
among obstetriciansgynecologists who had limited
opportunity for sleep
Rothschild (2009)
Surgical Resident Fatigue
Residents were fatigued during 48 and impaired during 27 of their time awake Among all residents the mean amount of daily sleep was 53 hours Overall residents fatigue levels were predicted to increase the risk of medical error by 22 compared with well-rested historical control subjects Night-float residents were more impaired (P = 02) with an increased risk of medical error (P = 045)
McCormick (2012)
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun
First day of Residency
Working on-call and weekends
Lack of vacation causing burnout
Took vacation but tired from previous rotations
Holiday spirit and relaxation
Uncertainty about knowledge-base responsibility future plans
Improving weather more daylight
Vacation time in summer
Ready to start 2nd year more confident and knowing what to expect
Well
Being
Feel
Good
Okay
Distress
Despair
Orientation
Feel Good
Well-rested
OK
Feel
Fatigued
Sleepy
Well Being
Time
Fatigue and Sleep Deprivation Graph
Times of Increased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
What was most helpful
Times of Decreased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
How Does Fatigue Come Into Play in
the OR
How Do You Manage Fatigue in the
OR
Posture Wauben et al reported a high prevalence rate (80)
of discomfort in the neck shoulders and back areas
among 280 surgeons in Europe Liberman et al
reported a high prevalence rate of lsquolsquoinjuriesrsquorsquo in the
hands fingers (42) and 107 in the neck among
colorectal surgeons
A recent study in Hong Kong found high prevalence
rates of neck and back musculoskeletal symptoms
among general surgeons The 12-month prevalence
rate was 829 for neck symptoms 578 for the
shoulder and 681 in the lower back
Szeto et al A study of surgeonsrsquo postural muscle activity during open laparoscopic and
endovascular surgery Surg Endosc (2010) 241712ndash1721
McDonald (1998)
Attention and Pacing You do drift Its human nature but thats when the risk factor increases Of course your attention span is decent the first hour or two then it gradually decreases I think the peak is between an hour and four hours After four hours your attention span starts to lessen You have to be aware of your attention span As the operation gets lengthy you have to be careful that you dont start losing your patience because you want to finish You have to say to yourself No I should not rush I should take my time You have to tell yourself and remind yourself that when you start to rush you get into trouble You say I should slow down because its better for the patient and its better for merdquo
- Elite neurosurgeon
Sleep Deprivation
Sleep Deprivation
ldquoSleep loss creates sleepiness which can be
associated with decrements in vigilance reaction
time psychomotor co-ordination information
processing decision making (eg fixation on
certain aspects of a situation to the neglect of other
information)rdquo
Rosekind MR et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Recognizing Sleep Deprivation in
Residency and Fellowship
Repeatedly yawning and ldquonodding offrdquo during
conferences or other sedentary activities (driving)
Loss of ability to perform usual activities quickly
Poor memory concentration judgment
Irritability moodiness depression
Dozing off while writing notesorders or while
reviewing medicationslabs
Repeatedly checking your work
Tisha Wang MD UCLA The Effects of Sleep Deprivation and Implications for Residency Training
Sleepiness in residents is equivalent to that found in patients
with serious sleep disorders Mustafa and Strohl unpublished data Papp 2002
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Epworth Sleepiness Scale
Normal
Insomnia
Sleep Apnea
Residents
Narcolepsy
0
5
10
15
20
Mean 590 220 1170 1470 1750
Normal InsomniaSleep
ApneaResidents Narcolepsy
Some Individuals are More Fatigue
Resistant Than Others
People who prefer to be active early in the day
(ldquomorningnessrdquo) are often more affected by sleep
deprivation than people who are most alert in the
late evening hours (ldquoeveningnessrdquo)
Thus personal characteristics of being ldquolarksrdquo or
ldquoowlsrdquo seem to affect psychomotor performance
in the work environment
St Pierre (2011)
Sleep Inertia and the Pager
Sleep inertia refers to the cognitive
impairment present immediately on
awakening from sleep
The first 15-30 min after waking are a
vulnerable period and performance
decrements can exceed those after 24 hrs of
continuous wakefulness
Highlights risk of residents committing
fatigue-related errors when woken from sleep
by a page
Lockley (2007)
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
Fatigue
ldquoFatiguerdquo can be thought of as the combined
influence of sleep homeostasis circadian rhythm
and time on task on performance capability
Van Dongen amp Hursh 2011
Other Conditions Linked with Fatigue
Fatigue can be related to anxiety depression
stress thyroid disease other medical conditions
medication side effects or career dissatisfaction
Residents may have a primary undiagnosed
sleep disorder such as obstructive sleep apnea
narcolepsy restless leg syndrome or insomnia
What creates fatigue in residency
training
FT = Total resident fatigue
FT =
FT = FSS + Few + Fpf FT = Total resident fatigue
FSS = Fatigue related to system design (circadian
rhythm disruption sleep deprivation fragmented sleep)
Few = Fatigue related to work and environmental
factors (task requirements physical work loads
workstation design physical factors team factors) and
Fpf = Fatigue related to the operatorrsquos personal
factors (health status nutritional status social and
domestic dictates)
Adapted from Schutte (2009)
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Primary
Sleep Disorders
(sleep apnea etc)
Fragmented Sleep
(pager phone calls)
Circadian Rhythm
Disruption
(night float rotating
shifts)
Insufficient Sleep
(on call sleep lossinadequate
recovery sleep)
EXCESSIVE DAYTIME SLEEPINESS
Fatigue amp Burnout
The characteristic symptoms of burnout are
persistent and excessive fatigue emotional
exhaustion and cognitive dysfunction Frequently
the condition also includes components of
depersonalization or cynicism toward
clientspatients and reduced personal efficacy with
a tendency to evaluate oneself negatively
Aringkerstedt (2011)
Burnout in Residency
Prevalence estimates range between 40ndash76
among internal medicine and pediatric residents
and 47ndash70 among surgery residents
McCray (2008)
Burnout and Sleep Deprivation
It has recently been demonstrated that burnout
scores are closely related to reports of disturbed
sleep
Aringkerstedt (2011)
Ego Depletion Decision Fatigue
and Task Performance
We find that the percentage of favorable rulings
drops gradually from 65 to nearly zero within
each decision session and returns abruptly to
65 after a break Danzigera (2011)
These studies demonstrated that ego depletion
coincides with decreases in blood glucose and
glucose supplementation attenuates the ego-
depletion effect relative to a sweetened placebo
Hagger (2010)
Fatigue Effects Alertness attention and vigilance are reduced People are able to sustain
concentration on a task for a shorter than usual period of time
Reduced motor performance (fine motor skills and eyendashhand coordination)
and a decrease effectiveness of motor tasks (speed and accuracy are
reduced)
Slowed reaction time and decision-making In order to reduce effort rule-
based decisions are preferred over knowledge-based decision-making
(principle of economy)
Impaired memory function manifested as a reduced ability both to learn and
to recall items
Motivational alteration of the thinking process people become careless in
the formation of opinion increasingly tolerant of their own mistakes and
prone to hasty decisions
Change in social behavior with disrupted communications uncontrolled
affects and a reduced willingness to share information with team members
The degree of resolution of perception can decrease which may lead to
important details being missed
St Pierre (2011)
Fatigue and Perceived Medical Error
Higher levels of fatigue and distress are
independently associated with self-perceived
medical error
West (2009)
Fatigue Surgery and Complications
Surgeons who had limited opportunity for sleep had
significantly higher rates of complications than
those who had a longer sleep opportunity We did
not observe an increased rate of complication
among obstetriciansgynecologists who had limited
opportunity for sleep
Rothschild (2009)
Surgical Resident Fatigue
Residents were fatigued during 48 and impaired during 27 of their time awake Among all residents the mean amount of daily sleep was 53 hours Overall residents fatigue levels were predicted to increase the risk of medical error by 22 compared with well-rested historical control subjects Night-float residents were more impaired (P = 02) with an increased risk of medical error (P = 045)
McCormick (2012)
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun
First day of Residency
Working on-call and weekends
Lack of vacation causing burnout
Took vacation but tired from previous rotations
Holiday spirit and relaxation
Uncertainty about knowledge-base responsibility future plans
Improving weather more daylight
Vacation time in summer
Ready to start 2nd year more confident and knowing what to expect
Well
Being
Feel
Good
Okay
Distress
Despair
Orientation
Feel Good
Well-rested
OK
Feel
Fatigued
Sleepy
Well Being
Time
Fatigue and Sleep Deprivation Graph
Times of Increased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
What was most helpful
Times of Decreased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
How Does Fatigue Come Into Play in
the OR
How Do You Manage Fatigue in the
OR
Posture Wauben et al reported a high prevalence rate (80)
of discomfort in the neck shoulders and back areas
among 280 surgeons in Europe Liberman et al
reported a high prevalence rate of lsquolsquoinjuriesrsquorsquo in the
hands fingers (42) and 107 in the neck among
colorectal surgeons
A recent study in Hong Kong found high prevalence
rates of neck and back musculoskeletal symptoms
among general surgeons The 12-month prevalence
rate was 829 for neck symptoms 578 for the
shoulder and 681 in the lower back
Szeto et al A study of surgeonsrsquo postural muscle activity during open laparoscopic and
endovascular surgery Surg Endosc (2010) 241712ndash1721
McDonald (1998)
Attention and Pacing You do drift Its human nature but thats when the risk factor increases Of course your attention span is decent the first hour or two then it gradually decreases I think the peak is between an hour and four hours After four hours your attention span starts to lessen You have to be aware of your attention span As the operation gets lengthy you have to be careful that you dont start losing your patience because you want to finish You have to say to yourself No I should not rush I should take my time You have to tell yourself and remind yourself that when you start to rush you get into trouble You say I should slow down because its better for the patient and its better for merdquo
- Elite neurosurgeon
Sleep Deprivation
Sleep Deprivation
ldquoSleep loss creates sleepiness which can be
associated with decrements in vigilance reaction
time psychomotor co-ordination information
processing decision making (eg fixation on
certain aspects of a situation to the neglect of other
information)rdquo
Rosekind MR et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Recognizing Sleep Deprivation in
Residency and Fellowship
Repeatedly yawning and ldquonodding offrdquo during
conferences or other sedentary activities (driving)
Loss of ability to perform usual activities quickly
Poor memory concentration judgment
Irritability moodiness depression
Dozing off while writing notesorders or while
reviewing medicationslabs
Repeatedly checking your work
Tisha Wang MD UCLA The Effects of Sleep Deprivation and Implications for Residency Training
Sleepiness in residents is equivalent to that found in patients
with serious sleep disorders Mustafa and Strohl unpublished data Papp 2002
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Epworth Sleepiness Scale
Normal
Insomnia
Sleep Apnea
Residents
Narcolepsy
0
5
10
15
20
Mean 590 220 1170 1470 1750
Normal InsomniaSleep
ApneaResidents Narcolepsy
Some Individuals are More Fatigue
Resistant Than Others
People who prefer to be active early in the day
(ldquomorningnessrdquo) are often more affected by sleep
deprivation than people who are most alert in the
late evening hours (ldquoeveningnessrdquo)
Thus personal characteristics of being ldquolarksrdquo or
ldquoowlsrdquo seem to affect psychomotor performance
in the work environment
St Pierre (2011)
Sleep Inertia and the Pager
Sleep inertia refers to the cognitive
impairment present immediately on
awakening from sleep
The first 15-30 min after waking are a
vulnerable period and performance
decrements can exceed those after 24 hrs of
continuous wakefulness
Highlights risk of residents committing
fatigue-related errors when woken from sleep
by a page
Lockley (2007)
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
Other Conditions Linked with Fatigue
Fatigue can be related to anxiety depression
stress thyroid disease other medical conditions
medication side effects or career dissatisfaction
Residents may have a primary undiagnosed
sleep disorder such as obstructive sleep apnea
narcolepsy restless leg syndrome or insomnia
What creates fatigue in residency
training
FT = Total resident fatigue
FT =
FT = FSS + Few + Fpf FT = Total resident fatigue
FSS = Fatigue related to system design (circadian
rhythm disruption sleep deprivation fragmented sleep)
Few = Fatigue related to work and environmental
factors (task requirements physical work loads
workstation design physical factors team factors) and
Fpf = Fatigue related to the operatorrsquos personal
factors (health status nutritional status social and
domestic dictates)
Adapted from Schutte (2009)
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Primary
Sleep Disorders
(sleep apnea etc)
Fragmented Sleep
(pager phone calls)
Circadian Rhythm
Disruption
(night float rotating
shifts)
Insufficient Sleep
(on call sleep lossinadequate
recovery sleep)
EXCESSIVE DAYTIME SLEEPINESS
Fatigue amp Burnout
The characteristic symptoms of burnout are
persistent and excessive fatigue emotional
exhaustion and cognitive dysfunction Frequently
the condition also includes components of
depersonalization or cynicism toward
clientspatients and reduced personal efficacy with
a tendency to evaluate oneself negatively
Aringkerstedt (2011)
Burnout in Residency
Prevalence estimates range between 40ndash76
among internal medicine and pediatric residents
and 47ndash70 among surgery residents
McCray (2008)
Burnout and Sleep Deprivation
It has recently been demonstrated that burnout
scores are closely related to reports of disturbed
sleep
Aringkerstedt (2011)
Ego Depletion Decision Fatigue
and Task Performance
We find that the percentage of favorable rulings
drops gradually from 65 to nearly zero within
each decision session and returns abruptly to
65 after a break Danzigera (2011)
These studies demonstrated that ego depletion
coincides with decreases in blood glucose and
glucose supplementation attenuates the ego-
depletion effect relative to a sweetened placebo
Hagger (2010)
Fatigue Effects Alertness attention and vigilance are reduced People are able to sustain
concentration on a task for a shorter than usual period of time
Reduced motor performance (fine motor skills and eyendashhand coordination)
and a decrease effectiveness of motor tasks (speed and accuracy are
reduced)
Slowed reaction time and decision-making In order to reduce effort rule-
based decisions are preferred over knowledge-based decision-making
(principle of economy)
Impaired memory function manifested as a reduced ability both to learn and
to recall items
Motivational alteration of the thinking process people become careless in
the formation of opinion increasingly tolerant of their own mistakes and
prone to hasty decisions
Change in social behavior with disrupted communications uncontrolled
affects and a reduced willingness to share information with team members
The degree of resolution of perception can decrease which may lead to
important details being missed
St Pierre (2011)
Fatigue and Perceived Medical Error
Higher levels of fatigue and distress are
independently associated with self-perceived
medical error
West (2009)
Fatigue Surgery and Complications
Surgeons who had limited opportunity for sleep had
significantly higher rates of complications than
those who had a longer sleep opportunity We did
not observe an increased rate of complication
among obstetriciansgynecologists who had limited
opportunity for sleep
Rothschild (2009)
Surgical Resident Fatigue
Residents were fatigued during 48 and impaired during 27 of their time awake Among all residents the mean amount of daily sleep was 53 hours Overall residents fatigue levels were predicted to increase the risk of medical error by 22 compared with well-rested historical control subjects Night-float residents were more impaired (P = 02) with an increased risk of medical error (P = 045)
McCormick (2012)
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun
First day of Residency
Working on-call and weekends
Lack of vacation causing burnout
Took vacation but tired from previous rotations
Holiday spirit and relaxation
Uncertainty about knowledge-base responsibility future plans
Improving weather more daylight
Vacation time in summer
Ready to start 2nd year more confident and knowing what to expect
Well
Being
Feel
Good
Okay
Distress
Despair
Orientation
Feel Good
Well-rested
OK
Feel
Fatigued
Sleepy
Well Being
Time
Fatigue and Sleep Deprivation Graph
Times of Increased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
What was most helpful
Times of Decreased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
How Does Fatigue Come Into Play in
the OR
How Do You Manage Fatigue in the
OR
Posture Wauben et al reported a high prevalence rate (80)
of discomfort in the neck shoulders and back areas
among 280 surgeons in Europe Liberman et al
reported a high prevalence rate of lsquolsquoinjuriesrsquorsquo in the
hands fingers (42) and 107 in the neck among
colorectal surgeons
A recent study in Hong Kong found high prevalence
rates of neck and back musculoskeletal symptoms
among general surgeons The 12-month prevalence
rate was 829 for neck symptoms 578 for the
shoulder and 681 in the lower back
Szeto et al A study of surgeonsrsquo postural muscle activity during open laparoscopic and
endovascular surgery Surg Endosc (2010) 241712ndash1721
McDonald (1998)
Attention and Pacing You do drift Its human nature but thats when the risk factor increases Of course your attention span is decent the first hour or two then it gradually decreases I think the peak is between an hour and four hours After four hours your attention span starts to lessen You have to be aware of your attention span As the operation gets lengthy you have to be careful that you dont start losing your patience because you want to finish You have to say to yourself No I should not rush I should take my time You have to tell yourself and remind yourself that when you start to rush you get into trouble You say I should slow down because its better for the patient and its better for merdquo
- Elite neurosurgeon
Sleep Deprivation
Sleep Deprivation
ldquoSleep loss creates sleepiness which can be
associated with decrements in vigilance reaction
time psychomotor co-ordination information
processing decision making (eg fixation on
certain aspects of a situation to the neglect of other
information)rdquo
Rosekind MR et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Recognizing Sleep Deprivation in
Residency and Fellowship
Repeatedly yawning and ldquonodding offrdquo during
conferences or other sedentary activities (driving)
Loss of ability to perform usual activities quickly
Poor memory concentration judgment
Irritability moodiness depression
Dozing off while writing notesorders or while
reviewing medicationslabs
Repeatedly checking your work
Tisha Wang MD UCLA The Effects of Sleep Deprivation and Implications for Residency Training
Sleepiness in residents is equivalent to that found in patients
with serious sleep disorders Mustafa and Strohl unpublished data Papp 2002
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Epworth Sleepiness Scale
Normal
Insomnia
Sleep Apnea
Residents
Narcolepsy
0
5
10
15
20
Mean 590 220 1170 1470 1750
Normal InsomniaSleep
ApneaResidents Narcolepsy
Some Individuals are More Fatigue
Resistant Than Others
People who prefer to be active early in the day
(ldquomorningnessrdquo) are often more affected by sleep
deprivation than people who are most alert in the
late evening hours (ldquoeveningnessrdquo)
Thus personal characteristics of being ldquolarksrdquo or
ldquoowlsrdquo seem to affect psychomotor performance
in the work environment
St Pierre (2011)
Sleep Inertia and the Pager
Sleep inertia refers to the cognitive
impairment present immediately on
awakening from sleep
The first 15-30 min after waking are a
vulnerable period and performance
decrements can exceed those after 24 hrs of
continuous wakefulness
Highlights risk of residents committing
fatigue-related errors when woken from sleep
by a page
Lockley (2007)
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
What creates fatigue in residency
training
FT = Total resident fatigue
FT =
FT = FSS + Few + Fpf FT = Total resident fatigue
FSS = Fatigue related to system design (circadian
rhythm disruption sleep deprivation fragmented sleep)
Few = Fatigue related to work and environmental
factors (task requirements physical work loads
workstation design physical factors team factors) and
Fpf = Fatigue related to the operatorrsquos personal
factors (health status nutritional status social and
domestic dictates)
Adapted from Schutte (2009)
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Primary
Sleep Disorders
(sleep apnea etc)
Fragmented Sleep
(pager phone calls)
Circadian Rhythm
Disruption
(night float rotating
shifts)
Insufficient Sleep
(on call sleep lossinadequate
recovery sleep)
EXCESSIVE DAYTIME SLEEPINESS
Fatigue amp Burnout
The characteristic symptoms of burnout are
persistent and excessive fatigue emotional
exhaustion and cognitive dysfunction Frequently
the condition also includes components of
depersonalization or cynicism toward
clientspatients and reduced personal efficacy with
a tendency to evaluate oneself negatively
Aringkerstedt (2011)
Burnout in Residency
Prevalence estimates range between 40ndash76
among internal medicine and pediatric residents
and 47ndash70 among surgery residents
McCray (2008)
Burnout and Sleep Deprivation
It has recently been demonstrated that burnout
scores are closely related to reports of disturbed
sleep
Aringkerstedt (2011)
Ego Depletion Decision Fatigue
and Task Performance
We find that the percentage of favorable rulings
drops gradually from 65 to nearly zero within
each decision session and returns abruptly to
65 after a break Danzigera (2011)
These studies demonstrated that ego depletion
coincides with decreases in blood glucose and
glucose supplementation attenuates the ego-
depletion effect relative to a sweetened placebo
Hagger (2010)
Fatigue Effects Alertness attention and vigilance are reduced People are able to sustain
concentration on a task for a shorter than usual period of time
Reduced motor performance (fine motor skills and eyendashhand coordination)
and a decrease effectiveness of motor tasks (speed and accuracy are
reduced)
Slowed reaction time and decision-making In order to reduce effort rule-
based decisions are preferred over knowledge-based decision-making
(principle of economy)
Impaired memory function manifested as a reduced ability both to learn and
to recall items
Motivational alteration of the thinking process people become careless in
the formation of opinion increasingly tolerant of their own mistakes and
prone to hasty decisions
Change in social behavior with disrupted communications uncontrolled
affects and a reduced willingness to share information with team members
The degree of resolution of perception can decrease which may lead to
important details being missed
St Pierre (2011)
Fatigue and Perceived Medical Error
Higher levels of fatigue and distress are
independently associated with self-perceived
medical error
West (2009)
Fatigue Surgery and Complications
Surgeons who had limited opportunity for sleep had
significantly higher rates of complications than
those who had a longer sleep opportunity We did
not observe an increased rate of complication
among obstetriciansgynecologists who had limited
opportunity for sleep
Rothschild (2009)
Surgical Resident Fatigue
Residents were fatigued during 48 and impaired during 27 of their time awake Among all residents the mean amount of daily sleep was 53 hours Overall residents fatigue levels were predicted to increase the risk of medical error by 22 compared with well-rested historical control subjects Night-float residents were more impaired (P = 02) with an increased risk of medical error (P = 045)
McCormick (2012)
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun
First day of Residency
Working on-call and weekends
Lack of vacation causing burnout
Took vacation but tired from previous rotations
Holiday spirit and relaxation
Uncertainty about knowledge-base responsibility future plans
Improving weather more daylight
Vacation time in summer
Ready to start 2nd year more confident and knowing what to expect
Well
Being
Feel
Good
Okay
Distress
Despair
Orientation
Feel Good
Well-rested
OK
Feel
Fatigued
Sleepy
Well Being
Time
Fatigue and Sleep Deprivation Graph
Times of Increased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
What was most helpful
Times of Decreased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
How Does Fatigue Come Into Play in
the OR
How Do You Manage Fatigue in the
OR
Posture Wauben et al reported a high prevalence rate (80)
of discomfort in the neck shoulders and back areas
among 280 surgeons in Europe Liberman et al
reported a high prevalence rate of lsquolsquoinjuriesrsquorsquo in the
hands fingers (42) and 107 in the neck among
colorectal surgeons
A recent study in Hong Kong found high prevalence
rates of neck and back musculoskeletal symptoms
among general surgeons The 12-month prevalence
rate was 829 for neck symptoms 578 for the
shoulder and 681 in the lower back
Szeto et al A study of surgeonsrsquo postural muscle activity during open laparoscopic and
endovascular surgery Surg Endosc (2010) 241712ndash1721
McDonald (1998)
Attention and Pacing You do drift Its human nature but thats when the risk factor increases Of course your attention span is decent the first hour or two then it gradually decreases I think the peak is between an hour and four hours After four hours your attention span starts to lessen You have to be aware of your attention span As the operation gets lengthy you have to be careful that you dont start losing your patience because you want to finish You have to say to yourself No I should not rush I should take my time You have to tell yourself and remind yourself that when you start to rush you get into trouble You say I should slow down because its better for the patient and its better for merdquo
- Elite neurosurgeon
Sleep Deprivation
Sleep Deprivation
ldquoSleep loss creates sleepiness which can be
associated with decrements in vigilance reaction
time psychomotor co-ordination information
processing decision making (eg fixation on
certain aspects of a situation to the neglect of other
information)rdquo
Rosekind MR et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Recognizing Sleep Deprivation in
Residency and Fellowship
Repeatedly yawning and ldquonodding offrdquo during
conferences or other sedentary activities (driving)
Loss of ability to perform usual activities quickly
Poor memory concentration judgment
Irritability moodiness depression
Dozing off while writing notesorders or while
reviewing medicationslabs
Repeatedly checking your work
Tisha Wang MD UCLA The Effects of Sleep Deprivation and Implications for Residency Training
Sleepiness in residents is equivalent to that found in patients
with serious sleep disorders Mustafa and Strohl unpublished data Papp 2002
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Epworth Sleepiness Scale
Normal
Insomnia
Sleep Apnea
Residents
Narcolepsy
0
5
10
15
20
Mean 590 220 1170 1470 1750
Normal InsomniaSleep
ApneaResidents Narcolepsy
Some Individuals are More Fatigue
Resistant Than Others
People who prefer to be active early in the day
(ldquomorningnessrdquo) are often more affected by sleep
deprivation than people who are most alert in the
late evening hours (ldquoeveningnessrdquo)
Thus personal characteristics of being ldquolarksrdquo or
ldquoowlsrdquo seem to affect psychomotor performance
in the work environment
St Pierre (2011)
Sleep Inertia and the Pager
Sleep inertia refers to the cognitive
impairment present immediately on
awakening from sleep
The first 15-30 min after waking are a
vulnerable period and performance
decrements can exceed those after 24 hrs of
continuous wakefulness
Highlights risk of residents committing
fatigue-related errors when woken from sleep
by a page
Lockley (2007)
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300

FT = FSS + Few + Fpf FT = Total resident fatigue
FSS = Fatigue related to system design (circadian
rhythm disruption sleep deprivation fragmented sleep)
Few = Fatigue related to work and environmental
factors (task requirements physical work loads
workstation design physical factors team factors) and
Fpf = Fatigue related to the operatorrsquos personal
factors (health status nutritional status social and
domestic dictates)
Adapted from Schutte (2009)
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Primary
Sleep Disorders
(sleep apnea etc)
Fragmented Sleep
(pager phone calls)
Circadian Rhythm
Disruption
(night float rotating
shifts)
Insufficient Sleep
(on call sleep lossinadequate
recovery sleep)
EXCESSIVE DAYTIME SLEEPINESS
Fatigue amp Burnout
The characteristic symptoms of burnout are
persistent and excessive fatigue emotional
exhaustion and cognitive dysfunction Frequently
the condition also includes components of
depersonalization or cynicism toward
clientspatients and reduced personal efficacy with
a tendency to evaluate oneself negatively
Aringkerstedt (2011)
Burnout in Residency
Prevalence estimates range between 40ndash76
among internal medicine and pediatric residents
and 47ndash70 among surgery residents
McCray (2008)
Burnout and Sleep Deprivation
It has recently been demonstrated that burnout
scores are closely related to reports of disturbed
sleep
Aringkerstedt (2011)
Ego Depletion Decision Fatigue
and Task Performance
We find that the percentage of favorable rulings
drops gradually from 65 to nearly zero within
each decision session and returns abruptly to
65 after a break Danzigera (2011)
These studies demonstrated that ego depletion
coincides with decreases in blood glucose and
glucose supplementation attenuates the ego-
depletion effect relative to a sweetened placebo
Hagger (2010)
Fatigue Effects Alertness attention and vigilance are reduced People are able to sustain
concentration on a task for a shorter than usual period of time
Reduced motor performance (fine motor skills and eyendashhand coordination)
and a decrease effectiveness of motor tasks (speed and accuracy are
reduced)
Slowed reaction time and decision-making In order to reduce effort rule-
based decisions are preferred over knowledge-based decision-making
(principle of economy)
Impaired memory function manifested as a reduced ability both to learn and
to recall items
Motivational alteration of the thinking process people become careless in
the formation of opinion increasingly tolerant of their own mistakes and
prone to hasty decisions
Change in social behavior with disrupted communications uncontrolled
affects and a reduced willingness to share information with team members
The degree of resolution of perception can decrease which may lead to
important details being missed
St Pierre (2011)
Fatigue and Perceived Medical Error
Higher levels of fatigue and distress are
independently associated with self-perceived
medical error
West (2009)
Fatigue Surgery and Complications
Surgeons who had limited opportunity for sleep had
significantly higher rates of complications than
those who had a longer sleep opportunity We did
not observe an increased rate of complication
among obstetriciansgynecologists who had limited
opportunity for sleep
Rothschild (2009)
Surgical Resident Fatigue
Residents were fatigued during 48 and impaired during 27 of their time awake Among all residents the mean amount of daily sleep was 53 hours Overall residents fatigue levels were predicted to increase the risk of medical error by 22 compared with well-rested historical control subjects Night-float residents were more impaired (P = 02) with an increased risk of medical error (P = 045)
McCormick (2012)
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun
First day of Residency
Working on-call and weekends
Lack of vacation causing burnout
Took vacation but tired from previous rotations
Holiday spirit and relaxation
Uncertainty about knowledge-base responsibility future plans
Improving weather more daylight
Vacation time in summer
Ready to start 2nd year more confident and knowing what to expect
Well
Being
Feel
Good
Okay
Distress
Despair
Orientation
Feel Good
Well-rested
OK
Feel
Fatigued
Sleepy
Well Being
Time
Fatigue and Sleep Deprivation Graph
Times of Increased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
What was most helpful
Times of Decreased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
How Does Fatigue Come Into Play in
the OR
How Do You Manage Fatigue in the
OR
Posture Wauben et al reported a high prevalence rate (80)
of discomfort in the neck shoulders and back areas
among 280 surgeons in Europe Liberman et al
reported a high prevalence rate of lsquolsquoinjuriesrsquorsquo in the
hands fingers (42) and 107 in the neck among
colorectal surgeons
A recent study in Hong Kong found high prevalence
rates of neck and back musculoskeletal symptoms
among general surgeons The 12-month prevalence
rate was 829 for neck symptoms 578 for the
shoulder and 681 in the lower back
Szeto et al A study of surgeonsrsquo postural muscle activity during open laparoscopic and
endovascular surgery Surg Endosc (2010) 241712ndash1721
McDonald (1998)
Attention and Pacing You do drift Its human nature but thats when the risk factor increases Of course your attention span is decent the first hour or two then it gradually decreases I think the peak is between an hour and four hours After four hours your attention span starts to lessen You have to be aware of your attention span As the operation gets lengthy you have to be careful that you dont start losing your patience because you want to finish You have to say to yourself No I should not rush I should take my time You have to tell yourself and remind yourself that when you start to rush you get into trouble You say I should slow down because its better for the patient and its better for merdquo
- Elite neurosurgeon
Sleep Deprivation
Sleep Deprivation
ldquoSleep loss creates sleepiness which can be
associated with decrements in vigilance reaction
time psychomotor co-ordination information
processing decision making (eg fixation on
certain aspects of a situation to the neglect of other
information)rdquo
Rosekind MR et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Recognizing Sleep Deprivation in
Residency and Fellowship
Repeatedly yawning and ldquonodding offrdquo during
conferences or other sedentary activities (driving)
Loss of ability to perform usual activities quickly
Poor memory concentration judgment
Irritability moodiness depression
Dozing off while writing notesorders or while
reviewing medicationslabs
Repeatedly checking your work
Tisha Wang MD UCLA The Effects of Sleep Deprivation and Implications for Residency Training
Sleepiness in residents is equivalent to that found in patients
with serious sleep disorders Mustafa and Strohl unpublished data Papp 2002
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Epworth Sleepiness Scale
Normal
Insomnia
Sleep Apnea
Residents
Narcolepsy
0
5
10
15
20
Mean 590 220 1170 1470 1750
Normal InsomniaSleep
ApneaResidents Narcolepsy
Some Individuals are More Fatigue
Resistant Than Others
People who prefer to be active early in the day
(ldquomorningnessrdquo) are often more affected by sleep
deprivation than people who are most alert in the
late evening hours (ldquoeveningnessrdquo)
Thus personal characteristics of being ldquolarksrdquo or
ldquoowlsrdquo seem to affect psychomotor performance
in the work environment
St Pierre (2011)
Sleep Inertia and the Pager
Sleep inertia refers to the cognitive
impairment present immediately on
awakening from sleep
The first 15-30 min after waking are a
vulnerable period and performance
decrements can exceed those after 24 hrs of
continuous wakefulness
Highlights risk of residents committing
fatigue-related errors when woken from sleep
by a page
Lockley (2007)
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300

copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Primary
Sleep Disorders
(sleep apnea etc)
Fragmented Sleep
(pager phone calls)
Circadian Rhythm
Disruption
(night float rotating
shifts)
Insufficient Sleep
(on call sleep lossinadequate
recovery sleep)
EXCESSIVE DAYTIME SLEEPINESS
Fatigue amp Burnout
The characteristic symptoms of burnout are
persistent and excessive fatigue emotional
exhaustion and cognitive dysfunction Frequently
the condition also includes components of
depersonalization or cynicism toward
clientspatients and reduced personal efficacy with
a tendency to evaluate oneself negatively
Aringkerstedt (2011)
Burnout in Residency
Prevalence estimates range between 40ndash76
among internal medicine and pediatric residents
and 47ndash70 among surgery residents
McCray (2008)
Burnout and Sleep Deprivation
It has recently been demonstrated that burnout
scores are closely related to reports of disturbed
sleep
Aringkerstedt (2011)
Ego Depletion Decision Fatigue
and Task Performance
We find that the percentage of favorable rulings
drops gradually from 65 to nearly zero within
each decision session and returns abruptly to
65 after a break Danzigera (2011)
These studies demonstrated that ego depletion
coincides with decreases in blood glucose and
glucose supplementation attenuates the ego-
depletion effect relative to a sweetened placebo
Hagger (2010)
Fatigue Effects Alertness attention and vigilance are reduced People are able to sustain
concentration on a task for a shorter than usual period of time
Reduced motor performance (fine motor skills and eyendashhand coordination)
and a decrease effectiveness of motor tasks (speed and accuracy are
reduced)
Slowed reaction time and decision-making In order to reduce effort rule-
based decisions are preferred over knowledge-based decision-making
(principle of economy)
Impaired memory function manifested as a reduced ability both to learn and
to recall items
Motivational alteration of the thinking process people become careless in
the formation of opinion increasingly tolerant of their own mistakes and
prone to hasty decisions
Change in social behavior with disrupted communications uncontrolled
affects and a reduced willingness to share information with team members
The degree of resolution of perception can decrease which may lead to
important details being missed
St Pierre (2011)
Fatigue and Perceived Medical Error
Higher levels of fatigue and distress are
independently associated with self-perceived
medical error
West (2009)
Fatigue Surgery and Complications
Surgeons who had limited opportunity for sleep had
significantly higher rates of complications than
those who had a longer sleep opportunity We did
not observe an increased rate of complication
among obstetriciansgynecologists who had limited
opportunity for sleep
Rothschild (2009)
Surgical Resident Fatigue
Residents were fatigued during 48 and impaired during 27 of their time awake Among all residents the mean amount of daily sleep was 53 hours Overall residents fatigue levels were predicted to increase the risk of medical error by 22 compared with well-rested historical control subjects Night-float residents were more impaired (P = 02) with an increased risk of medical error (P = 045)
McCormick (2012)
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun
First day of Residency
Working on-call and weekends
Lack of vacation causing burnout
Took vacation but tired from previous rotations
Holiday spirit and relaxation
Uncertainty about knowledge-base responsibility future plans
Improving weather more daylight
Vacation time in summer
Ready to start 2nd year more confident and knowing what to expect
Well
Being
Feel
Good
Okay
Distress
Despair
Orientation
Feel Good
Well-rested
OK
Feel
Fatigued
Sleepy
Well Being
Time
Fatigue and Sleep Deprivation Graph
Times of Increased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
What was most helpful
Times of Decreased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
How Does Fatigue Come Into Play in
the OR
How Do You Manage Fatigue in the
OR
Posture Wauben et al reported a high prevalence rate (80)
of discomfort in the neck shoulders and back areas
among 280 surgeons in Europe Liberman et al
reported a high prevalence rate of lsquolsquoinjuriesrsquorsquo in the
hands fingers (42) and 107 in the neck among
colorectal surgeons
A recent study in Hong Kong found high prevalence
rates of neck and back musculoskeletal symptoms
among general surgeons The 12-month prevalence
rate was 829 for neck symptoms 578 for the
shoulder and 681 in the lower back
Szeto et al A study of surgeonsrsquo postural muscle activity during open laparoscopic and
endovascular surgery Surg Endosc (2010) 241712ndash1721
McDonald (1998)
Attention and Pacing You do drift Its human nature but thats when the risk factor increases Of course your attention span is decent the first hour or two then it gradually decreases I think the peak is between an hour and four hours After four hours your attention span starts to lessen You have to be aware of your attention span As the operation gets lengthy you have to be careful that you dont start losing your patience because you want to finish You have to say to yourself No I should not rush I should take my time You have to tell yourself and remind yourself that when you start to rush you get into trouble You say I should slow down because its better for the patient and its better for merdquo
- Elite neurosurgeon
Sleep Deprivation
Sleep Deprivation
ldquoSleep loss creates sleepiness which can be
associated with decrements in vigilance reaction
time psychomotor co-ordination information
processing decision making (eg fixation on
certain aspects of a situation to the neglect of other
information)rdquo
Rosekind MR et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Recognizing Sleep Deprivation in
Residency and Fellowship
Repeatedly yawning and ldquonodding offrdquo during
conferences or other sedentary activities (driving)
Loss of ability to perform usual activities quickly
Poor memory concentration judgment
Irritability moodiness depression
Dozing off while writing notesorders or while
reviewing medicationslabs
Repeatedly checking your work
Tisha Wang MD UCLA The Effects of Sleep Deprivation and Implications for Residency Training
Sleepiness in residents is equivalent to that found in patients
with serious sleep disorders Mustafa and Strohl unpublished data Papp 2002
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Epworth Sleepiness Scale
Normal
Insomnia
Sleep Apnea
Residents
Narcolepsy
0
5
10
15
20
Mean 590 220 1170 1470 1750
Normal InsomniaSleep
ApneaResidents Narcolepsy
Some Individuals are More Fatigue
Resistant Than Others
People who prefer to be active early in the day
(ldquomorningnessrdquo) are often more affected by sleep
deprivation than people who are most alert in the
late evening hours (ldquoeveningnessrdquo)
Thus personal characteristics of being ldquolarksrdquo or
ldquoowlsrdquo seem to affect psychomotor performance
in the work environment
St Pierre (2011)
Sleep Inertia and the Pager
Sleep inertia refers to the cognitive
impairment present immediately on
awakening from sleep
The first 15-30 min after waking are a
vulnerable period and performance
decrements can exceed those after 24 hrs of
continuous wakefulness
Highlights risk of residents committing
fatigue-related errors when woken from sleep
by a page
Lockley (2007)
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300

Fatigue amp Burnout
The characteristic symptoms of burnout are
persistent and excessive fatigue emotional
exhaustion and cognitive dysfunction Frequently
the condition also includes components of
depersonalization or cynicism toward
clientspatients and reduced personal efficacy with
a tendency to evaluate oneself negatively
Aringkerstedt (2011)
Burnout in Residency
Prevalence estimates range between 40ndash76
among internal medicine and pediatric residents
and 47ndash70 among surgery residents
McCray (2008)
Burnout and Sleep Deprivation
It has recently been demonstrated that burnout
scores are closely related to reports of disturbed
sleep
Aringkerstedt (2011)
Ego Depletion Decision Fatigue
and Task Performance
We find that the percentage of favorable rulings
drops gradually from 65 to nearly zero within
each decision session and returns abruptly to
65 after a break Danzigera (2011)
These studies demonstrated that ego depletion
coincides with decreases in blood glucose and
glucose supplementation attenuates the ego-
depletion effect relative to a sweetened placebo
Hagger (2010)
Fatigue Effects Alertness attention and vigilance are reduced People are able to sustain
concentration on a task for a shorter than usual period of time
Reduced motor performance (fine motor skills and eyendashhand coordination)
and a decrease effectiveness of motor tasks (speed and accuracy are
reduced)
Slowed reaction time and decision-making In order to reduce effort rule-
based decisions are preferred over knowledge-based decision-making
(principle of economy)
Impaired memory function manifested as a reduced ability both to learn and
to recall items
Motivational alteration of the thinking process people become careless in
the formation of opinion increasingly tolerant of their own mistakes and
prone to hasty decisions
Change in social behavior with disrupted communications uncontrolled
affects and a reduced willingness to share information with team members
The degree of resolution of perception can decrease which may lead to
important details being missed
St Pierre (2011)
Fatigue and Perceived Medical Error
Higher levels of fatigue and distress are
independently associated with self-perceived
medical error
West (2009)
Fatigue Surgery and Complications
Surgeons who had limited opportunity for sleep had
significantly higher rates of complications than
those who had a longer sleep opportunity We did
not observe an increased rate of complication
among obstetriciansgynecologists who had limited
opportunity for sleep
Rothschild (2009)
Surgical Resident Fatigue
Residents were fatigued during 48 and impaired during 27 of their time awake Among all residents the mean amount of daily sleep was 53 hours Overall residents fatigue levels were predicted to increase the risk of medical error by 22 compared with well-rested historical control subjects Night-float residents were more impaired (P = 02) with an increased risk of medical error (P = 045)
McCormick (2012)
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun
First day of Residency
Working on-call and weekends
Lack of vacation causing burnout
Took vacation but tired from previous rotations
Holiday spirit and relaxation
Uncertainty about knowledge-base responsibility future plans
Improving weather more daylight
Vacation time in summer
Ready to start 2nd year more confident and knowing what to expect
Well
Being
Feel
Good
Okay
Distress
Despair
Orientation
Feel Good
Well-rested
OK
Feel
Fatigued
Sleepy
Well Being
Time
Fatigue and Sleep Deprivation Graph
Times of Increased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
What was most helpful
Times of Decreased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
How Does Fatigue Come Into Play in
the OR
How Do You Manage Fatigue in the
OR
Posture Wauben et al reported a high prevalence rate (80)
of discomfort in the neck shoulders and back areas
among 280 surgeons in Europe Liberman et al
reported a high prevalence rate of lsquolsquoinjuriesrsquorsquo in the
hands fingers (42) and 107 in the neck among
colorectal surgeons
A recent study in Hong Kong found high prevalence
rates of neck and back musculoskeletal symptoms
among general surgeons The 12-month prevalence
rate was 829 for neck symptoms 578 for the
shoulder and 681 in the lower back
Szeto et al A study of surgeonsrsquo postural muscle activity during open laparoscopic and
endovascular surgery Surg Endosc (2010) 241712ndash1721
McDonald (1998)
Attention and Pacing You do drift Its human nature but thats when the risk factor increases Of course your attention span is decent the first hour or two then it gradually decreases I think the peak is between an hour and four hours After four hours your attention span starts to lessen You have to be aware of your attention span As the operation gets lengthy you have to be careful that you dont start losing your patience because you want to finish You have to say to yourself No I should not rush I should take my time You have to tell yourself and remind yourself that when you start to rush you get into trouble You say I should slow down because its better for the patient and its better for merdquo
- Elite neurosurgeon
Sleep Deprivation
Sleep Deprivation
ldquoSleep loss creates sleepiness which can be
associated with decrements in vigilance reaction
time psychomotor co-ordination information
processing decision making (eg fixation on
certain aspects of a situation to the neglect of other
information)rdquo
Rosekind MR et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Recognizing Sleep Deprivation in
Residency and Fellowship
Repeatedly yawning and ldquonodding offrdquo during
conferences or other sedentary activities (driving)
Loss of ability to perform usual activities quickly
Poor memory concentration judgment
Irritability moodiness depression
Dozing off while writing notesorders or while
reviewing medicationslabs
Repeatedly checking your work
Tisha Wang MD UCLA The Effects of Sleep Deprivation and Implications for Residency Training
Sleepiness in residents is equivalent to that found in patients
with serious sleep disorders Mustafa and Strohl unpublished data Papp 2002
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Epworth Sleepiness Scale
Normal
Insomnia
Sleep Apnea
Residents
Narcolepsy
0
5
10
15
20
Mean 590 220 1170 1470 1750
Normal InsomniaSleep
ApneaResidents Narcolepsy
Some Individuals are More Fatigue
Resistant Than Others
People who prefer to be active early in the day
(ldquomorningnessrdquo) are often more affected by sleep
deprivation than people who are most alert in the
late evening hours (ldquoeveningnessrdquo)
Thus personal characteristics of being ldquolarksrdquo or
ldquoowlsrdquo seem to affect psychomotor performance
in the work environment
St Pierre (2011)
Sleep Inertia and the Pager
Sleep inertia refers to the cognitive
impairment present immediately on
awakening from sleep
The first 15-30 min after waking are a
vulnerable period and performance
decrements can exceed those after 24 hrs of
continuous wakefulness
Highlights risk of residents committing
fatigue-related errors when woken from sleep
by a page
Lockley (2007)
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
Burnout in Residency
Prevalence estimates range between 40ndash76
among internal medicine and pediatric residents
and 47ndash70 among surgery residents
McCray (2008)
Burnout and Sleep Deprivation
It has recently been demonstrated that burnout
scores are closely related to reports of disturbed
sleep
Aringkerstedt (2011)
Ego Depletion Decision Fatigue
and Task Performance
We find that the percentage of favorable rulings
drops gradually from 65 to nearly zero within
each decision session and returns abruptly to
65 after a break Danzigera (2011)
These studies demonstrated that ego depletion
coincides with decreases in blood glucose and
glucose supplementation attenuates the ego-
depletion effect relative to a sweetened placebo
Hagger (2010)
Fatigue Effects Alertness attention and vigilance are reduced People are able to sustain
concentration on a task for a shorter than usual period of time
Reduced motor performance (fine motor skills and eyendashhand coordination)
and a decrease effectiveness of motor tasks (speed and accuracy are
reduced)
Slowed reaction time and decision-making In order to reduce effort rule-
based decisions are preferred over knowledge-based decision-making
(principle of economy)
Impaired memory function manifested as a reduced ability both to learn and
to recall items
Motivational alteration of the thinking process people become careless in
the formation of opinion increasingly tolerant of their own mistakes and
prone to hasty decisions
Change in social behavior with disrupted communications uncontrolled
affects and a reduced willingness to share information with team members
The degree of resolution of perception can decrease which may lead to
important details being missed
St Pierre (2011)
Fatigue and Perceived Medical Error
Higher levels of fatigue and distress are
independently associated with self-perceived
medical error
West (2009)
Fatigue Surgery and Complications
Surgeons who had limited opportunity for sleep had
significantly higher rates of complications than
those who had a longer sleep opportunity We did
not observe an increased rate of complication
among obstetriciansgynecologists who had limited
opportunity for sleep
Rothschild (2009)
Surgical Resident Fatigue
Residents were fatigued during 48 and impaired during 27 of their time awake Among all residents the mean amount of daily sleep was 53 hours Overall residents fatigue levels were predicted to increase the risk of medical error by 22 compared with well-rested historical control subjects Night-float residents were more impaired (P = 02) with an increased risk of medical error (P = 045)
McCormick (2012)
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun
First day of Residency
Working on-call and weekends
Lack of vacation causing burnout
Took vacation but tired from previous rotations
Holiday spirit and relaxation
Uncertainty about knowledge-base responsibility future plans
Improving weather more daylight
Vacation time in summer
Ready to start 2nd year more confident and knowing what to expect
Well
Being
Feel
Good
Okay
Distress
Despair
Orientation
Feel Good
Well-rested
OK
Feel
Fatigued
Sleepy
Well Being
Time
Fatigue and Sleep Deprivation Graph
Times of Increased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
What was most helpful
Times of Decreased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
How Does Fatigue Come Into Play in
the OR
How Do You Manage Fatigue in the
OR
Posture Wauben et al reported a high prevalence rate (80)
of discomfort in the neck shoulders and back areas
among 280 surgeons in Europe Liberman et al
reported a high prevalence rate of lsquolsquoinjuriesrsquorsquo in the
hands fingers (42) and 107 in the neck among
colorectal surgeons
A recent study in Hong Kong found high prevalence
rates of neck and back musculoskeletal symptoms
among general surgeons The 12-month prevalence
rate was 829 for neck symptoms 578 for the
shoulder and 681 in the lower back
Szeto et al A study of surgeonsrsquo postural muscle activity during open laparoscopic and
endovascular surgery Surg Endosc (2010) 241712ndash1721
McDonald (1998)
Attention and Pacing You do drift Its human nature but thats when the risk factor increases Of course your attention span is decent the first hour or two then it gradually decreases I think the peak is between an hour and four hours After four hours your attention span starts to lessen You have to be aware of your attention span As the operation gets lengthy you have to be careful that you dont start losing your patience because you want to finish You have to say to yourself No I should not rush I should take my time You have to tell yourself and remind yourself that when you start to rush you get into trouble You say I should slow down because its better for the patient and its better for merdquo
- Elite neurosurgeon
Sleep Deprivation
Sleep Deprivation
ldquoSleep loss creates sleepiness which can be
associated with decrements in vigilance reaction
time psychomotor co-ordination information
processing decision making (eg fixation on
certain aspects of a situation to the neglect of other
information)rdquo
Rosekind MR et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Recognizing Sleep Deprivation in
Residency and Fellowship
Repeatedly yawning and ldquonodding offrdquo during
conferences or other sedentary activities (driving)
Loss of ability to perform usual activities quickly
Poor memory concentration judgment
Irritability moodiness depression
Dozing off while writing notesorders or while
reviewing medicationslabs
Repeatedly checking your work
Tisha Wang MD UCLA The Effects of Sleep Deprivation and Implications for Residency Training
Sleepiness in residents is equivalent to that found in patients
with serious sleep disorders Mustafa and Strohl unpublished data Papp 2002
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Epworth Sleepiness Scale
Normal
Insomnia
Sleep Apnea
Residents
Narcolepsy
0
5
10
15
20
Mean 590 220 1170 1470 1750
Normal InsomniaSleep
ApneaResidents Narcolepsy
Some Individuals are More Fatigue
Resistant Than Others
People who prefer to be active early in the day
(ldquomorningnessrdquo) are often more affected by sleep
deprivation than people who are most alert in the
late evening hours (ldquoeveningnessrdquo)
Thus personal characteristics of being ldquolarksrdquo or
ldquoowlsrdquo seem to affect psychomotor performance
in the work environment
St Pierre (2011)
Sleep Inertia and the Pager
Sleep inertia refers to the cognitive
impairment present immediately on
awakening from sleep
The first 15-30 min after waking are a
vulnerable period and performance
decrements can exceed those after 24 hrs of
continuous wakefulness
Highlights risk of residents committing
fatigue-related errors when woken from sleep
by a page
Lockley (2007)
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
Burnout and Sleep Deprivation
It has recently been demonstrated that burnout
scores are closely related to reports of disturbed
sleep
Aringkerstedt (2011)
Ego Depletion Decision Fatigue
and Task Performance
We find that the percentage of favorable rulings
drops gradually from 65 to nearly zero within
each decision session and returns abruptly to
65 after a break Danzigera (2011)
These studies demonstrated that ego depletion
coincides with decreases in blood glucose and
glucose supplementation attenuates the ego-
depletion effect relative to a sweetened placebo
Hagger (2010)
Fatigue Effects Alertness attention and vigilance are reduced People are able to sustain
concentration on a task for a shorter than usual period of time
Reduced motor performance (fine motor skills and eyendashhand coordination)
and a decrease effectiveness of motor tasks (speed and accuracy are
reduced)
Slowed reaction time and decision-making In order to reduce effort rule-
based decisions are preferred over knowledge-based decision-making
(principle of economy)
Impaired memory function manifested as a reduced ability both to learn and
to recall items
Motivational alteration of the thinking process people become careless in
the formation of opinion increasingly tolerant of their own mistakes and
prone to hasty decisions
Change in social behavior with disrupted communications uncontrolled
affects and a reduced willingness to share information with team members
The degree of resolution of perception can decrease which may lead to
important details being missed
St Pierre (2011)
Fatigue and Perceived Medical Error
Higher levels of fatigue and distress are
independently associated with self-perceived
medical error
West (2009)
Fatigue Surgery and Complications
Surgeons who had limited opportunity for sleep had
significantly higher rates of complications than
those who had a longer sleep opportunity We did
not observe an increased rate of complication
among obstetriciansgynecologists who had limited
opportunity for sleep
Rothschild (2009)
Surgical Resident Fatigue
Residents were fatigued during 48 and impaired during 27 of their time awake Among all residents the mean amount of daily sleep was 53 hours Overall residents fatigue levels were predicted to increase the risk of medical error by 22 compared with well-rested historical control subjects Night-float residents were more impaired (P = 02) with an increased risk of medical error (P = 045)
McCormick (2012)
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun
First day of Residency
Working on-call and weekends
Lack of vacation causing burnout
Took vacation but tired from previous rotations
Holiday spirit and relaxation
Uncertainty about knowledge-base responsibility future plans
Improving weather more daylight
Vacation time in summer
Ready to start 2nd year more confident and knowing what to expect
Well
Being
Feel
Good
Okay
Distress
Despair
Orientation
Feel Good
Well-rested
OK
Feel
Fatigued
Sleepy
Well Being
Time
Fatigue and Sleep Deprivation Graph
Times of Increased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
What was most helpful
Times of Decreased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
How Does Fatigue Come Into Play in
the OR
How Do You Manage Fatigue in the
OR
Posture Wauben et al reported a high prevalence rate (80)
of discomfort in the neck shoulders and back areas
among 280 surgeons in Europe Liberman et al
reported a high prevalence rate of lsquolsquoinjuriesrsquorsquo in the
hands fingers (42) and 107 in the neck among
colorectal surgeons
A recent study in Hong Kong found high prevalence
rates of neck and back musculoskeletal symptoms
among general surgeons The 12-month prevalence
rate was 829 for neck symptoms 578 for the
shoulder and 681 in the lower back
Szeto et al A study of surgeonsrsquo postural muscle activity during open laparoscopic and
endovascular surgery Surg Endosc (2010) 241712ndash1721
McDonald (1998)
Attention and Pacing You do drift Its human nature but thats when the risk factor increases Of course your attention span is decent the first hour or two then it gradually decreases I think the peak is between an hour and four hours After four hours your attention span starts to lessen You have to be aware of your attention span As the operation gets lengthy you have to be careful that you dont start losing your patience because you want to finish You have to say to yourself No I should not rush I should take my time You have to tell yourself and remind yourself that when you start to rush you get into trouble You say I should slow down because its better for the patient and its better for merdquo
- Elite neurosurgeon
Sleep Deprivation
Sleep Deprivation
ldquoSleep loss creates sleepiness which can be
associated with decrements in vigilance reaction
time psychomotor co-ordination information
processing decision making (eg fixation on
certain aspects of a situation to the neglect of other
information)rdquo
Rosekind MR et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Recognizing Sleep Deprivation in
Residency and Fellowship
Repeatedly yawning and ldquonodding offrdquo during
conferences or other sedentary activities (driving)
Loss of ability to perform usual activities quickly
Poor memory concentration judgment
Irritability moodiness depression
Dozing off while writing notesorders or while
reviewing medicationslabs
Repeatedly checking your work
Tisha Wang MD UCLA The Effects of Sleep Deprivation and Implications for Residency Training
Sleepiness in residents is equivalent to that found in patients
with serious sleep disorders Mustafa and Strohl unpublished data Papp 2002
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Epworth Sleepiness Scale
Normal
Insomnia
Sleep Apnea
Residents
Narcolepsy
0
5
10
15
20
Mean 590 220 1170 1470 1750
Normal InsomniaSleep
ApneaResidents Narcolepsy
Some Individuals are More Fatigue
Resistant Than Others
People who prefer to be active early in the day
(ldquomorningnessrdquo) are often more affected by sleep
deprivation than people who are most alert in the
late evening hours (ldquoeveningnessrdquo)
Thus personal characteristics of being ldquolarksrdquo or
ldquoowlsrdquo seem to affect psychomotor performance
in the work environment
St Pierre (2011)
Sleep Inertia and the Pager
Sleep inertia refers to the cognitive
impairment present immediately on
awakening from sleep
The first 15-30 min after waking are a
vulnerable period and performance
decrements can exceed those after 24 hrs of
continuous wakefulness
Highlights risk of residents committing
fatigue-related errors when woken from sleep
by a page
Lockley (2007)
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
Ego Depletion Decision Fatigue
and Task Performance
We find that the percentage of favorable rulings
drops gradually from 65 to nearly zero within
each decision session and returns abruptly to
65 after a break Danzigera (2011)
These studies demonstrated that ego depletion
coincides with decreases in blood glucose and
glucose supplementation attenuates the ego-
depletion effect relative to a sweetened placebo
Hagger (2010)
Fatigue Effects Alertness attention and vigilance are reduced People are able to sustain
concentration on a task for a shorter than usual period of time
Reduced motor performance (fine motor skills and eyendashhand coordination)
and a decrease effectiveness of motor tasks (speed and accuracy are
reduced)
Slowed reaction time and decision-making In order to reduce effort rule-
based decisions are preferred over knowledge-based decision-making
(principle of economy)
Impaired memory function manifested as a reduced ability both to learn and
to recall items
Motivational alteration of the thinking process people become careless in
the formation of opinion increasingly tolerant of their own mistakes and
prone to hasty decisions
Change in social behavior with disrupted communications uncontrolled
affects and a reduced willingness to share information with team members
The degree of resolution of perception can decrease which may lead to
important details being missed
St Pierre (2011)
Fatigue and Perceived Medical Error
Higher levels of fatigue and distress are
independently associated with self-perceived
medical error
West (2009)
Fatigue Surgery and Complications
Surgeons who had limited opportunity for sleep had
significantly higher rates of complications than
those who had a longer sleep opportunity We did
not observe an increased rate of complication
among obstetriciansgynecologists who had limited
opportunity for sleep
Rothschild (2009)
Surgical Resident Fatigue
Residents were fatigued during 48 and impaired during 27 of their time awake Among all residents the mean amount of daily sleep was 53 hours Overall residents fatigue levels were predicted to increase the risk of medical error by 22 compared with well-rested historical control subjects Night-float residents were more impaired (P = 02) with an increased risk of medical error (P = 045)
McCormick (2012)
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun
First day of Residency
Working on-call and weekends
Lack of vacation causing burnout
Took vacation but tired from previous rotations
Holiday spirit and relaxation
Uncertainty about knowledge-base responsibility future plans
Improving weather more daylight
Vacation time in summer
Ready to start 2nd year more confident and knowing what to expect
Well
Being
Feel
Good
Okay
Distress
Despair
Orientation
Feel Good
Well-rested
OK
Feel
Fatigued
Sleepy
Well Being
Time
Fatigue and Sleep Deprivation Graph
Times of Increased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
What was most helpful
Times of Decreased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
How Does Fatigue Come Into Play in
the OR
How Do You Manage Fatigue in the
OR
Posture Wauben et al reported a high prevalence rate (80)
of discomfort in the neck shoulders and back areas
among 280 surgeons in Europe Liberman et al
reported a high prevalence rate of lsquolsquoinjuriesrsquorsquo in the
hands fingers (42) and 107 in the neck among
colorectal surgeons
A recent study in Hong Kong found high prevalence
rates of neck and back musculoskeletal symptoms
among general surgeons The 12-month prevalence
rate was 829 for neck symptoms 578 for the
shoulder and 681 in the lower back
Szeto et al A study of surgeonsrsquo postural muscle activity during open laparoscopic and
endovascular surgery Surg Endosc (2010) 241712ndash1721
McDonald (1998)
Attention and Pacing You do drift Its human nature but thats when the risk factor increases Of course your attention span is decent the first hour or two then it gradually decreases I think the peak is between an hour and four hours After four hours your attention span starts to lessen You have to be aware of your attention span As the operation gets lengthy you have to be careful that you dont start losing your patience because you want to finish You have to say to yourself No I should not rush I should take my time You have to tell yourself and remind yourself that when you start to rush you get into trouble You say I should slow down because its better for the patient and its better for merdquo
- Elite neurosurgeon
Sleep Deprivation
Sleep Deprivation
ldquoSleep loss creates sleepiness which can be
associated with decrements in vigilance reaction
time psychomotor co-ordination information
processing decision making (eg fixation on
certain aspects of a situation to the neglect of other
information)rdquo
Rosekind MR et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Recognizing Sleep Deprivation in
Residency and Fellowship
Repeatedly yawning and ldquonodding offrdquo during
conferences or other sedentary activities (driving)
Loss of ability to perform usual activities quickly
Poor memory concentration judgment
Irritability moodiness depression
Dozing off while writing notesorders or while
reviewing medicationslabs
Repeatedly checking your work
Tisha Wang MD UCLA The Effects of Sleep Deprivation and Implications for Residency Training
Sleepiness in residents is equivalent to that found in patients
with serious sleep disorders Mustafa and Strohl unpublished data Papp 2002
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Epworth Sleepiness Scale
Normal
Insomnia
Sleep Apnea
Residents
Narcolepsy
0
5
10
15
20
Mean 590 220 1170 1470 1750
Normal InsomniaSleep
ApneaResidents Narcolepsy
Some Individuals are More Fatigue
Resistant Than Others
People who prefer to be active early in the day
(ldquomorningnessrdquo) are often more affected by sleep
deprivation than people who are most alert in the
late evening hours (ldquoeveningnessrdquo)
Thus personal characteristics of being ldquolarksrdquo or
ldquoowlsrdquo seem to affect psychomotor performance
in the work environment
St Pierre (2011)
Sleep Inertia and the Pager
Sleep inertia refers to the cognitive
impairment present immediately on
awakening from sleep
The first 15-30 min after waking are a
vulnerable period and performance
decrements can exceed those after 24 hrs of
continuous wakefulness
Highlights risk of residents committing
fatigue-related errors when woken from sleep
by a page
Lockley (2007)
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
Fatigue Effects Alertness attention and vigilance are reduced People are able to sustain
concentration on a task for a shorter than usual period of time
Reduced motor performance (fine motor skills and eyendashhand coordination)
and a decrease effectiveness of motor tasks (speed and accuracy are
reduced)
Slowed reaction time and decision-making In order to reduce effort rule-
based decisions are preferred over knowledge-based decision-making
(principle of economy)
Impaired memory function manifested as a reduced ability both to learn and
to recall items
Motivational alteration of the thinking process people become careless in
the formation of opinion increasingly tolerant of their own mistakes and
prone to hasty decisions
Change in social behavior with disrupted communications uncontrolled
affects and a reduced willingness to share information with team members
The degree of resolution of perception can decrease which may lead to
important details being missed
St Pierre (2011)
Fatigue and Perceived Medical Error
Higher levels of fatigue and distress are
independently associated with self-perceived
medical error
West (2009)
Fatigue Surgery and Complications
Surgeons who had limited opportunity for sleep had
significantly higher rates of complications than
those who had a longer sleep opportunity We did
not observe an increased rate of complication
among obstetriciansgynecologists who had limited
opportunity for sleep
Rothschild (2009)
Surgical Resident Fatigue
Residents were fatigued during 48 and impaired during 27 of their time awake Among all residents the mean amount of daily sleep was 53 hours Overall residents fatigue levels were predicted to increase the risk of medical error by 22 compared with well-rested historical control subjects Night-float residents were more impaired (P = 02) with an increased risk of medical error (P = 045)
McCormick (2012)
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun
First day of Residency
Working on-call and weekends
Lack of vacation causing burnout
Took vacation but tired from previous rotations
Holiday spirit and relaxation
Uncertainty about knowledge-base responsibility future plans
Improving weather more daylight
Vacation time in summer
Ready to start 2nd year more confident and knowing what to expect
Well
Being
Feel
Good
Okay
Distress
Despair
Orientation
Feel Good
Well-rested
OK
Feel
Fatigued
Sleepy
Well Being
Time
Fatigue and Sleep Deprivation Graph
Times of Increased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
What was most helpful
Times of Decreased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
How Does Fatigue Come Into Play in
the OR
How Do You Manage Fatigue in the
OR
Posture Wauben et al reported a high prevalence rate (80)
of discomfort in the neck shoulders and back areas
among 280 surgeons in Europe Liberman et al
reported a high prevalence rate of lsquolsquoinjuriesrsquorsquo in the
hands fingers (42) and 107 in the neck among
colorectal surgeons
A recent study in Hong Kong found high prevalence
rates of neck and back musculoskeletal symptoms
among general surgeons The 12-month prevalence
rate was 829 for neck symptoms 578 for the
shoulder and 681 in the lower back
Szeto et al A study of surgeonsrsquo postural muscle activity during open laparoscopic and
endovascular surgery Surg Endosc (2010) 241712ndash1721
McDonald (1998)
Attention and Pacing You do drift Its human nature but thats when the risk factor increases Of course your attention span is decent the first hour or two then it gradually decreases I think the peak is between an hour and four hours After four hours your attention span starts to lessen You have to be aware of your attention span As the operation gets lengthy you have to be careful that you dont start losing your patience because you want to finish You have to say to yourself No I should not rush I should take my time You have to tell yourself and remind yourself that when you start to rush you get into trouble You say I should slow down because its better for the patient and its better for merdquo
- Elite neurosurgeon
Sleep Deprivation
Sleep Deprivation
ldquoSleep loss creates sleepiness which can be
associated with decrements in vigilance reaction
time psychomotor co-ordination information
processing decision making (eg fixation on
certain aspects of a situation to the neglect of other
information)rdquo
Rosekind MR et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Recognizing Sleep Deprivation in
Residency and Fellowship
Repeatedly yawning and ldquonodding offrdquo during
conferences or other sedentary activities (driving)
Loss of ability to perform usual activities quickly
Poor memory concentration judgment
Irritability moodiness depression
Dozing off while writing notesorders or while
reviewing medicationslabs
Repeatedly checking your work
Tisha Wang MD UCLA The Effects of Sleep Deprivation and Implications for Residency Training
Sleepiness in residents is equivalent to that found in patients
with serious sleep disorders Mustafa and Strohl unpublished data Papp 2002
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Epworth Sleepiness Scale
Normal
Insomnia
Sleep Apnea
Residents
Narcolepsy
0
5
10
15
20
Mean 590 220 1170 1470 1750
Normal InsomniaSleep
ApneaResidents Narcolepsy
Some Individuals are More Fatigue
Resistant Than Others
People who prefer to be active early in the day
(ldquomorningnessrdquo) are often more affected by sleep
deprivation than people who are most alert in the
late evening hours (ldquoeveningnessrdquo)
Thus personal characteristics of being ldquolarksrdquo or
ldquoowlsrdquo seem to affect psychomotor performance
in the work environment
St Pierre (2011)
Sleep Inertia and the Pager
Sleep inertia refers to the cognitive
impairment present immediately on
awakening from sleep
The first 15-30 min after waking are a
vulnerable period and performance
decrements can exceed those after 24 hrs of
continuous wakefulness
Highlights risk of residents committing
fatigue-related errors when woken from sleep
by a page
Lockley (2007)
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
Fatigue and Perceived Medical Error
Higher levels of fatigue and distress are
independently associated with self-perceived
medical error
West (2009)
Fatigue Surgery and Complications
Surgeons who had limited opportunity for sleep had
significantly higher rates of complications than
those who had a longer sleep opportunity We did
not observe an increased rate of complication
among obstetriciansgynecologists who had limited
opportunity for sleep
Rothschild (2009)
Surgical Resident Fatigue
Residents were fatigued during 48 and impaired during 27 of their time awake Among all residents the mean amount of daily sleep was 53 hours Overall residents fatigue levels were predicted to increase the risk of medical error by 22 compared with well-rested historical control subjects Night-float residents were more impaired (P = 02) with an increased risk of medical error (P = 045)
McCormick (2012)
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun
First day of Residency
Working on-call and weekends
Lack of vacation causing burnout
Took vacation but tired from previous rotations
Holiday spirit and relaxation
Uncertainty about knowledge-base responsibility future plans
Improving weather more daylight
Vacation time in summer
Ready to start 2nd year more confident and knowing what to expect
Well
Being
Feel
Good
Okay
Distress
Despair
Orientation
Feel Good
Well-rested
OK
Feel
Fatigued
Sleepy
Well Being
Time
Fatigue and Sleep Deprivation Graph
Times of Increased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
What was most helpful
Times of Decreased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
How Does Fatigue Come Into Play in
the OR
How Do You Manage Fatigue in the
OR
Posture Wauben et al reported a high prevalence rate (80)
of discomfort in the neck shoulders and back areas
among 280 surgeons in Europe Liberman et al
reported a high prevalence rate of lsquolsquoinjuriesrsquorsquo in the
hands fingers (42) and 107 in the neck among
colorectal surgeons
A recent study in Hong Kong found high prevalence
rates of neck and back musculoskeletal symptoms
among general surgeons The 12-month prevalence
rate was 829 for neck symptoms 578 for the
shoulder and 681 in the lower back
Szeto et al A study of surgeonsrsquo postural muscle activity during open laparoscopic and
endovascular surgery Surg Endosc (2010) 241712ndash1721
McDonald (1998)
Attention and Pacing You do drift Its human nature but thats when the risk factor increases Of course your attention span is decent the first hour or two then it gradually decreases I think the peak is between an hour and four hours After four hours your attention span starts to lessen You have to be aware of your attention span As the operation gets lengthy you have to be careful that you dont start losing your patience because you want to finish You have to say to yourself No I should not rush I should take my time You have to tell yourself and remind yourself that when you start to rush you get into trouble You say I should slow down because its better for the patient and its better for merdquo
- Elite neurosurgeon
Sleep Deprivation
Sleep Deprivation
ldquoSleep loss creates sleepiness which can be
associated with decrements in vigilance reaction
time psychomotor co-ordination information
processing decision making (eg fixation on
certain aspects of a situation to the neglect of other
information)rdquo
Rosekind MR et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Recognizing Sleep Deprivation in
Residency and Fellowship
Repeatedly yawning and ldquonodding offrdquo during
conferences or other sedentary activities (driving)
Loss of ability to perform usual activities quickly
Poor memory concentration judgment
Irritability moodiness depression
Dozing off while writing notesorders or while
reviewing medicationslabs
Repeatedly checking your work
Tisha Wang MD UCLA The Effects of Sleep Deprivation and Implications for Residency Training
Sleepiness in residents is equivalent to that found in patients
with serious sleep disorders Mustafa and Strohl unpublished data Papp 2002
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Epworth Sleepiness Scale
Normal
Insomnia
Sleep Apnea
Residents
Narcolepsy
0
5
10
15
20
Mean 590 220 1170 1470 1750
Normal InsomniaSleep
ApneaResidents Narcolepsy
Some Individuals are More Fatigue
Resistant Than Others
People who prefer to be active early in the day
(ldquomorningnessrdquo) are often more affected by sleep
deprivation than people who are most alert in the
late evening hours (ldquoeveningnessrdquo)
Thus personal characteristics of being ldquolarksrdquo or
ldquoowlsrdquo seem to affect psychomotor performance
in the work environment
St Pierre (2011)
Sleep Inertia and the Pager
Sleep inertia refers to the cognitive
impairment present immediately on
awakening from sleep
The first 15-30 min after waking are a
vulnerable period and performance
decrements can exceed those after 24 hrs of
continuous wakefulness
Highlights risk of residents committing
fatigue-related errors when woken from sleep
by a page
Lockley (2007)
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
Fatigue Surgery and Complications
Surgeons who had limited opportunity for sleep had
significantly higher rates of complications than
those who had a longer sleep opportunity We did
not observe an increased rate of complication
among obstetriciansgynecologists who had limited
opportunity for sleep
Rothschild (2009)
Surgical Resident Fatigue
Residents were fatigued during 48 and impaired during 27 of their time awake Among all residents the mean amount of daily sleep was 53 hours Overall residents fatigue levels were predicted to increase the risk of medical error by 22 compared with well-rested historical control subjects Night-float residents were more impaired (P = 02) with an increased risk of medical error (P = 045)
McCormick (2012)
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun
First day of Residency
Working on-call and weekends
Lack of vacation causing burnout
Took vacation but tired from previous rotations
Holiday spirit and relaxation
Uncertainty about knowledge-base responsibility future plans
Improving weather more daylight
Vacation time in summer
Ready to start 2nd year more confident and knowing what to expect
Well
Being
Feel
Good
Okay
Distress
Despair
Orientation
Feel Good
Well-rested
OK
Feel
Fatigued
Sleepy
Well Being
Time
Fatigue and Sleep Deprivation Graph
Times of Increased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
What was most helpful
Times of Decreased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
How Does Fatigue Come Into Play in
the OR
How Do You Manage Fatigue in the
OR
Posture Wauben et al reported a high prevalence rate (80)
of discomfort in the neck shoulders and back areas
among 280 surgeons in Europe Liberman et al
reported a high prevalence rate of lsquolsquoinjuriesrsquorsquo in the
hands fingers (42) and 107 in the neck among
colorectal surgeons
A recent study in Hong Kong found high prevalence
rates of neck and back musculoskeletal symptoms
among general surgeons The 12-month prevalence
rate was 829 for neck symptoms 578 for the
shoulder and 681 in the lower back
Szeto et al A study of surgeonsrsquo postural muscle activity during open laparoscopic and
endovascular surgery Surg Endosc (2010) 241712ndash1721
McDonald (1998)
Attention and Pacing You do drift Its human nature but thats when the risk factor increases Of course your attention span is decent the first hour or two then it gradually decreases I think the peak is between an hour and four hours After four hours your attention span starts to lessen You have to be aware of your attention span As the operation gets lengthy you have to be careful that you dont start losing your patience because you want to finish You have to say to yourself No I should not rush I should take my time You have to tell yourself and remind yourself that when you start to rush you get into trouble You say I should slow down because its better for the patient and its better for merdquo
- Elite neurosurgeon
Sleep Deprivation
Sleep Deprivation
ldquoSleep loss creates sleepiness which can be
associated with decrements in vigilance reaction
time psychomotor co-ordination information
processing decision making (eg fixation on
certain aspects of a situation to the neglect of other
information)rdquo
Rosekind MR et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Recognizing Sleep Deprivation in
Residency and Fellowship
Repeatedly yawning and ldquonodding offrdquo during
conferences or other sedentary activities (driving)
Loss of ability to perform usual activities quickly
Poor memory concentration judgment
Irritability moodiness depression
Dozing off while writing notesorders or while
reviewing medicationslabs
Repeatedly checking your work
Tisha Wang MD UCLA The Effects of Sleep Deprivation and Implications for Residency Training
Sleepiness in residents is equivalent to that found in patients
with serious sleep disorders Mustafa and Strohl unpublished data Papp 2002
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Epworth Sleepiness Scale
Normal
Insomnia
Sleep Apnea
Residents
Narcolepsy
0
5
10
15
20
Mean 590 220 1170 1470 1750
Normal InsomniaSleep
ApneaResidents Narcolepsy
Some Individuals are More Fatigue
Resistant Than Others
People who prefer to be active early in the day
(ldquomorningnessrdquo) are often more affected by sleep
deprivation than people who are most alert in the
late evening hours (ldquoeveningnessrdquo)
Thus personal characteristics of being ldquolarksrdquo or
ldquoowlsrdquo seem to affect psychomotor performance
in the work environment
St Pierre (2011)
Sleep Inertia and the Pager
Sleep inertia refers to the cognitive
impairment present immediately on
awakening from sleep
The first 15-30 min after waking are a
vulnerable period and performance
decrements can exceed those after 24 hrs of
continuous wakefulness
Highlights risk of residents committing
fatigue-related errors when woken from sleep
by a page
Lockley (2007)
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
Surgical Resident Fatigue
Residents were fatigued during 48 and impaired during 27 of their time awake Among all residents the mean amount of daily sleep was 53 hours Overall residents fatigue levels were predicted to increase the risk of medical error by 22 compared with well-rested historical control subjects Night-float residents were more impaired (P = 02) with an increased risk of medical error (P = 045)
McCormick (2012)
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun
First day of Residency
Working on-call and weekends
Lack of vacation causing burnout
Took vacation but tired from previous rotations
Holiday spirit and relaxation
Uncertainty about knowledge-base responsibility future plans
Improving weather more daylight
Vacation time in summer
Ready to start 2nd year more confident and knowing what to expect
Well
Being
Feel
Good
Okay
Distress
Despair
Orientation
Feel Good
Well-rested
OK
Feel
Fatigued
Sleepy
Well Being
Time
Fatigue and Sleep Deprivation Graph
Times of Increased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
What was most helpful
Times of Decreased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
How Does Fatigue Come Into Play in
the OR
How Do You Manage Fatigue in the
OR
Posture Wauben et al reported a high prevalence rate (80)
of discomfort in the neck shoulders and back areas
among 280 surgeons in Europe Liberman et al
reported a high prevalence rate of lsquolsquoinjuriesrsquorsquo in the
hands fingers (42) and 107 in the neck among
colorectal surgeons
A recent study in Hong Kong found high prevalence
rates of neck and back musculoskeletal symptoms
among general surgeons The 12-month prevalence
rate was 829 for neck symptoms 578 for the
shoulder and 681 in the lower back
Szeto et al A study of surgeonsrsquo postural muscle activity during open laparoscopic and
endovascular surgery Surg Endosc (2010) 241712ndash1721
McDonald (1998)
Attention and Pacing You do drift Its human nature but thats when the risk factor increases Of course your attention span is decent the first hour or two then it gradually decreases I think the peak is between an hour and four hours After four hours your attention span starts to lessen You have to be aware of your attention span As the operation gets lengthy you have to be careful that you dont start losing your patience because you want to finish You have to say to yourself No I should not rush I should take my time You have to tell yourself and remind yourself that when you start to rush you get into trouble You say I should slow down because its better for the patient and its better for merdquo
- Elite neurosurgeon
Sleep Deprivation
Sleep Deprivation
ldquoSleep loss creates sleepiness which can be
associated with decrements in vigilance reaction
time psychomotor co-ordination information
processing decision making (eg fixation on
certain aspects of a situation to the neglect of other
information)rdquo
Rosekind MR et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Recognizing Sleep Deprivation in
Residency and Fellowship
Repeatedly yawning and ldquonodding offrdquo during
conferences or other sedentary activities (driving)
Loss of ability to perform usual activities quickly
Poor memory concentration judgment
Irritability moodiness depression
Dozing off while writing notesorders or while
reviewing medicationslabs
Repeatedly checking your work
Tisha Wang MD UCLA The Effects of Sleep Deprivation and Implications for Residency Training
Sleepiness in residents is equivalent to that found in patients
with serious sleep disorders Mustafa and Strohl unpublished data Papp 2002
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Epworth Sleepiness Scale
Normal
Insomnia
Sleep Apnea
Residents
Narcolepsy
0
5
10
15
20
Mean 590 220 1170 1470 1750
Normal InsomniaSleep
ApneaResidents Narcolepsy
Some Individuals are More Fatigue
Resistant Than Others
People who prefer to be active early in the day
(ldquomorningnessrdquo) are often more affected by sleep
deprivation than people who are most alert in the
late evening hours (ldquoeveningnessrdquo)
Thus personal characteristics of being ldquolarksrdquo or
ldquoowlsrdquo seem to affect psychomotor performance
in the work environment
St Pierre (2011)
Sleep Inertia and the Pager
Sleep inertia refers to the cognitive
impairment present immediately on
awakening from sleep
The first 15-30 min after waking are a
vulnerable period and performance
decrements can exceed those after 24 hrs of
continuous wakefulness
Highlights risk of residents committing
fatigue-related errors when woken from sleep
by a page
Lockley (2007)
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
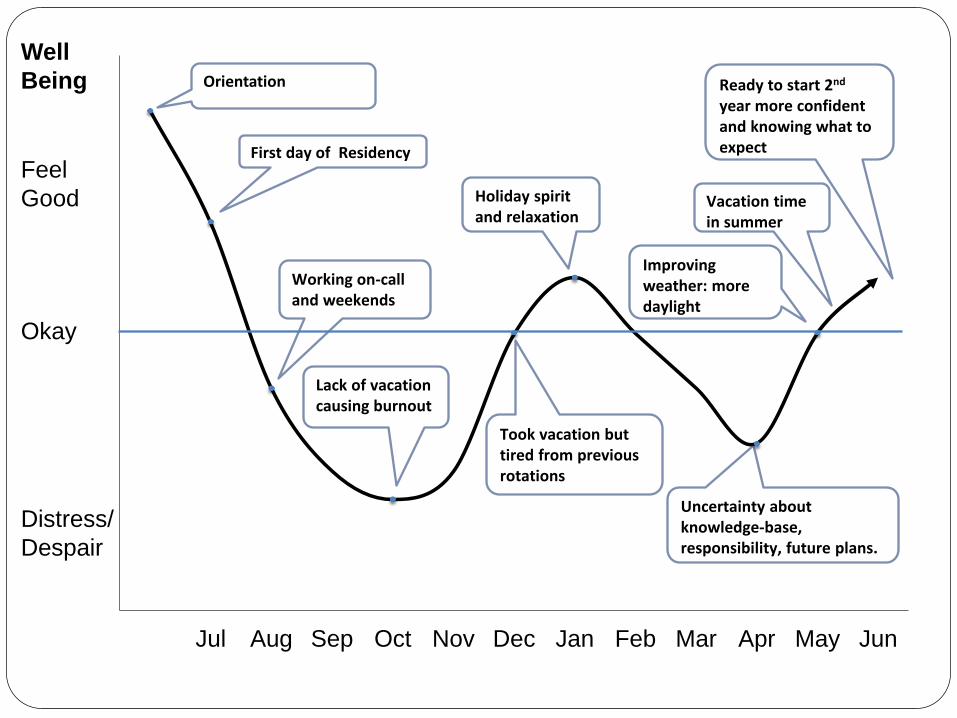
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun
First day of Residency
Working on-call and weekends
Lack of vacation causing burnout
Took vacation but tired from previous rotations
Holiday spirit and relaxation
Uncertainty about knowledge-base responsibility future plans
Improving weather more daylight
Vacation time in summer
Ready to start 2nd year more confident and knowing what to expect
Well
Being
Feel
Good
Okay
Distress
Despair
Orientation
Feel Good
Well-rested
OK
Feel
Fatigued
Sleepy
Well Being
Time
Fatigue and Sleep Deprivation Graph
Times of Increased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
What was most helpful
Times of Decreased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
How Does Fatigue Come Into Play in
the OR
How Do You Manage Fatigue in the
OR
Posture Wauben et al reported a high prevalence rate (80)
of discomfort in the neck shoulders and back areas
among 280 surgeons in Europe Liberman et al
reported a high prevalence rate of lsquolsquoinjuriesrsquorsquo in the
hands fingers (42) and 107 in the neck among
colorectal surgeons
A recent study in Hong Kong found high prevalence
rates of neck and back musculoskeletal symptoms
among general surgeons The 12-month prevalence
rate was 829 for neck symptoms 578 for the
shoulder and 681 in the lower back
Szeto et al A study of surgeonsrsquo postural muscle activity during open laparoscopic and
endovascular surgery Surg Endosc (2010) 241712ndash1721
McDonald (1998)
Attention and Pacing You do drift Its human nature but thats when the risk factor increases Of course your attention span is decent the first hour or two then it gradually decreases I think the peak is between an hour and four hours After four hours your attention span starts to lessen You have to be aware of your attention span As the operation gets lengthy you have to be careful that you dont start losing your patience because you want to finish You have to say to yourself No I should not rush I should take my time You have to tell yourself and remind yourself that when you start to rush you get into trouble You say I should slow down because its better for the patient and its better for merdquo
- Elite neurosurgeon
Sleep Deprivation
Sleep Deprivation
ldquoSleep loss creates sleepiness which can be
associated with decrements in vigilance reaction
time psychomotor co-ordination information
processing decision making (eg fixation on
certain aspects of a situation to the neglect of other
information)rdquo
Rosekind MR et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Recognizing Sleep Deprivation in
Residency and Fellowship
Repeatedly yawning and ldquonodding offrdquo during
conferences or other sedentary activities (driving)
Loss of ability to perform usual activities quickly
Poor memory concentration judgment
Irritability moodiness depression
Dozing off while writing notesorders or while
reviewing medicationslabs
Repeatedly checking your work
Tisha Wang MD UCLA The Effects of Sleep Deprivation and Implications for Residency Training
Sleepiness in residents is equivalent to that found in patients
with serious sleep disorders Mustafa and Strohl unpublished data Papp 2002
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Epworth Sleepiness Scale
Normal
Insomnia
Sleep Apnea
Residents
Narcolepsy
0
5
10
15
20
Mean 590 220 1170 1470 1750
Normal InsomniaSleep
ApneaResidents Narcolepsy
Some Individuals are More Fatigue
Resistant Than Others
People who prefer to be active early in the day
(ldquomorningnessrdquo) are often more affected by sleep
deprivation than people who are most alert in the
late evening hours (ldquoeveningnessrdquo)
Thus personal characteristics of being ldquolarksrdquo or
ldquoowlsrdquo seem to affect psychomotor performance
in the work environment
St Pierre (2011)
Sleep Inertia and the Pager
Sleep inertia refers to the cognitive
impairment present immediately on
awakening from sleep
The first 15-30 min after waking are a
vulnerable period and performance
decrements can exceed those after 24 hrs of
continuous wakefulness
Highlights risk of residents committing
fatigue-related errors when woken from sleep
by a page
Lockley (2007)
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300

Feel Good
Well-rested
OK
Feel
Fatigued
Sleepy
Well Being
Time
Fatigue and Sleep Deprivation Graph
Times of Increased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
What was most helpful
Times of Decreased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
How Does Fatigue Come Into Play in
the OR
How Do You Manage Fatigue in the
OR
Posture Wauben et al reported a high prevalence rate (80)
of discomfort in the neck shoulders and back areas
among 280 surgeons in Europe Liberman et al
reported a high prevalence rate of lsquolsquoinjuriesrsquorsquo in the
hands fingers (42) and 107 in the neck among
colorectal surgeons
A recent study in Hong Kong found high prevalence
rates of neck and back musculoskeletal symptoms
among general surgeons The 12-month prevalence
rate was 829 for neck symptoms 578 for the
shoulder and 681 in the lower back
Szeto et al A study of surgeonsrsquo postural muscle activity during open laparoscopic and
endovascular surgery Surg Endosc (2010) 241712ndash1721
McDonald (1998)
Attention and Pacing You do drift Its human nature but thats when the risk factor increases Of course your attention span is decent the first hour or two then it gradually decreases I think the peak is between an hour and four hours After four hours your attention span starts to lessen You have to be aware of your attention span As the operation gets lengthy you have to be careful that you dont start losing your patience because you want to finish You have to say to yourself No I should not rush I should take my time You have to tell yourself and remind yourself that when you start to rush you get into trouble You say I should slow down because its better for the patient and its better for merdquo
- Elite neurosurgeon
Sleep Deprivation
Sleep Deprivation
ldquoSleep loss creates sleepiness which can be
associated with decrements in vigilance reaction
time psychomotor co-ordination information
processing decision making (eg fixation on
certain aspects of a situation to the neglect of other
information)rdquo
Rosekind MR et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Recognizing Sleep Deprivation in
Residency and Fellowship
Repeatedly yawning and ldquonodding offrdquo during
conferences or other sedentary activities (driving)
Loss of ability to perform usual activities quickly
Poor memory concentration judgment
Irritability moodiness depression
Dozing off while writing notesorders or while
reviewing medicationslabs
Repeatedly checking your work
Tisha Wang MD UCLA The Effects of Sleep Deprivation and Implications for Residency Training
Sleepiness in residents is equivalent to that found in patients
with serious sleep disorders Mustafa and Strohl unpublished data Papp 2002
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Epworth Sleepiness Scale
Normal
Insomnia
Sleep Apnea
Residents
Narcolepsy
0
5
10
15
20
Mean 590 220 1170 1470 1750
Normal InsomniaSleep
ApneaResidents Narcolepsy
Some Individuals are More Fatigue
Resistant Than Others
People who prefer to be active early in the day
(ldquomorningnessrdquo) are often more affected by sleep
deprivation than people who are most alert in the
late evening hours (ldquoeveningnessrdquo)
Thus personal characteristics of being ldquolarksrdquo or
ldquoowlsrdquo seem to affect psychomotor performance
in the work environment
St Pierre (2011)
Sleep Inertia and the Pager
Sleep inertia refers to the cognitive
impairment present immediately on
awakening from sleep
The first 15-30 min after waking are a
vulnerable period and performance
decrements can exceed those after 24 hrs of
continuous wakefulness
Highlights risk of residents committing
fatigue-related errors when woken from sleep
by a page
Lockley (2007)
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300

Times of Increased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
What was most helpful
Times of Decreased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
How Does Fatigue Come Into Play in
the OR
How Do You Manage Fatigue in the
OR
Posture Wauben et al reported a high prevalence rate (80)
of discomfort in the neck shoulders and back areas
among 280 surgeons in Europe Liberman et al
reported a high prevalence rate of lsquolsquoinjuriesrsquorsquo in the
hands fingers (42) and 107 in the neck among
colorectal surgeons
A recent study in Hong Kong found high prevalence
rates of neck and back musculoskeletal symptoms
among general surgeons The 12-month prevalence
rate was 829 for neck symptoms 578 for the
shoulder and 681 in the lower back
Szeto et al A study of surgeonsrsquo postural muscle activity during open laparoscopic and
endovascular surgery Surg Endosc (2010) 241712ndash1721
McDonald (1998)
Attention and Pacing You do drift Its human nature but thats when the risk factor increases Of course your attention span is decent the first hour or two then it gradually decreases I think the peak is between an hour and four hours After four hours your attention span starts to lessen You have to be aware of your attention span As the operation gets lengthy you have to be careful that you dont start losing your patience because you want to finish You have to say to yourself No I should not rush I should take my time You have to tell yourself and remind yourself that when you start to rush you get into trouble You say I should slow down because its better for the patient and its better for merdquo
- Elite neurosurgeon
Sleep Deprivation
Sleep Deprivation
ldquoSleep loss creates sleepiness which can be
associated with decrements in vigilance reaction
time psychomotor co-ordination information
processing decision making (eg fixation on
certain aspects of a situation to the neglect of other
information)rdquo
Rosekind MR et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Recognizing Sleep Deprivation in
Residency and Fellowship
Repeatedly yawning and ldquonodding offrdquo during
conferences or other sedentary activities (driving)
Loss of ability to perform usual activities quickly
Poor memory concentration judgment
Irritability moodiness depression
Dozing off while writing notesorders or while
reviewing medicationslabs
Repeatedly checking your work
Tisha Wang MD UCLA The Effects of Sleep Deprivation and Implications for Residency Training
Sleepiness in residents is equivalent to that found in patients
with serious sleep disorders Mustafa and Strohl unpublished data Papp 2002
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Epworth Sleepiness Scale
Normal
Insomnia
Sleep Apnea
Residents
Narcolepsy
0
5
10
15
20
Mean 590 220 1170 1470 1750
Normal InsomniaSleep
ApneaResidents Narcolepsy
Some Individuals are More Fatigue
Resistant Than Others
People who prefer to be active early in the day
(ldquomorningnessrdquo) are often more affected by sleep
deprivation than people who are most alert in the
late evening hours (ldquoeveningnessrdquo)
Thus personal characteristics of being ldquolarksrdquo or
ldquoowlsrdquo seem to affect psychomotor performance
in the work environment
St Pierre (2011)
Sleep Inertia and the Pager
Sleep inertia refers to the cognitive
impairment present immediately on
awakening from sleep
The first 15-30 min after waking are a
vulnerable period and performance
decrements can exceed those after 24 hrs of
continuous wakefulness
Highlights risk of residents committing
fatigue-related errors when woken from sleep
by a page
Lockley (2007)
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300

Times of Decreased Fatigue
What were you able to do to look after the fatigue
andor sleep deprivation
How effective were your strategies
How Does Fatigue Come Into Play in
the OR
How Do You Manage Fatigue in the
OR
Posture Wauben et al reported a high prevalence rate (80)
of discomfort in the neck shoulders and back areas
among 280 surgeons in Europe Liberman et al
reported a high prevalence rate of lsquolsquoinjuriesrsquorsquo in the
hands fingers (42) and 107 in the neck among
colorectal surgeons
A recent study in Hong Kong found high prevalence
rates of neck and back musculoskeletal symptoms
among general surgeons The 12-month prevalence
rate was 829 for neck symptoms 578 for the
shoulder and 681 in the lower back
Szeto et al A study of surgeonsrsquo postural muscle activity during open laparoscopic and
endovascular surgery Surg Endosc (2010) 241712ndash1721
McDonald (1998)
Attention and Pacing You do drift Its human nature but thats when the risk factor increases Of course your attention span is decent the first hour or two then it gradually decreases I think the peak is between an hour and four hours After four hours your attention span starts to lessen You have to be aware of your attention span As the operation gets lengthy you have to be careful that you dont start losing your patience because you want to finish You have to say to yourself No I should not rush I should take my time You have to tell yourself and remind yourself that when you start to rush you get into trouble You say I should slow down because its better for the patient and its better for merdquo
- Elite neurosurgeon
Sleep Deprivation
Sleep Deprivation
ldquoSleep loss creates sleepiness which can be
associated with decrements in vigilance reaction
time psychomotor co-ordination information
processing decision making (eg fixation on
certain aspects of a situation to the neglect of other
information)rdquo
Rosekind MR et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Recognizing Sleep Deprivation in
Residency and Fellowship
Repeatedly yawning and ldquonodding offrdquo during
conferences or other sedentary activities (driving)
Loss of ability to perform usual activities quickly
Poor memory concentration judgment
Irritability moodiness depression
Dozing off while writing notesorders or while
reviewing medicationslabs
Repeatedly checking your work
Tisha Wang MD UCLA The Effects of Sleep Deprivation and Implications for Residency Training
Sleepiness in residents is equivalent to that found in patients
with serious sleep disorders Mustafa and Strohl unpublished data Papp 2002
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Epworth Sleepiness Scale
Normal
Insomnia
Sleep Apnea
Residents
Narcolepsy
0
5
10
15
20
Mean 590 220 1170 1470 1750
Normal InsomniaSleep
ApneaResidents Narcolepsy
Some Individuals are More Fatigue
Resistant Than Others
People who prefer to be active early in the day
(ldquomorningnessrdquo) are often more affected by sleep
deprivation than people who are most alert in the
late evening hours (ldquoeveningnessrdquo)
Thus personal characteristics of being ldquolarksrdquo or
ldquoowlsrdquo seem to affect psychomotor performance
in the work environment
St Pierre (2011)
Sleep Inertia and the Pager
Sleep inertia refers to the cognitive
impairment present immediately on
awakening from sleep
The first 15-30 min after waking are a
vulnerable period and performance
decrements can exceed those after 24 hrs of
continuous wakefulness
Highlights risk of residents committing
fatigue-related errors when woken from sleep
by a page
Lockley (2007)
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
How Does Fatigue Come Into Play in
the OR
How Do You Manage Fatigue in the
OR
Posture Wauben et al reported a high prevalence rate (80)
of discomfort in the neck shoulders and back areas
among 280 surgeons in Europe Liberman et al
reported a high prevalence rate of lsquolsquoinjuriesrsquorsquo in the
hands fingers (42) and 107 in the neck among
colorectal surgeons
A recent study in Hong Kong found high prevalence
rates of neck and back musculoskeletal symptoms
among general surgeons The 12-month prevalence
rate was 829 for neck symptoms 578 for the
shoulder and 681 in the lower back
Szeto et al A study of surgeonsrsquo postural muscle activity during open laparoscopic and
endovascular surgery Surg Endosc (2010) 241712ndash1721
McDonald (1998)
Attention and Pacing You do drift Its human nature but thats when the risk factor increases Of course your attention span is decent the first hour or two then it gradually decreases I think the peak is between an hour and four hours After four hours your attention span starts to lessen You have to be aware of your attention span As the operation gets lengthy you have to be careful that you dont start losing your patience because you want to finish You have to say to yourself No I should not rush I should take my time You have to tell yourself and remind yourself that when you start to rush you get into trouble You say I should slow down because its better for the patient and its better for merdquo
- Elite neurosurgeon
Sleep Deprivation
Sleep Deprivation
ldquoSleep loss creates sleepiness which can be
associated with decrements in vigilance reaction
time psychomotor co-ordination information
processing decision making (eg fixation on
certain aspects of a situation to the neglect of other
information)rdquo
Rosekind MR et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Recognizing Sleep Deprivation in
Residency and Fellowship
Repeatedly yawning and ldquonodding offrdquo during
conferences or other sedentary activities (driving)
Loss of ability to perform usual activities quickly
Poor memory concentration judgment
Irritability moodiness depression
Dozing off while writing notesorders or while
reviewing medicationslabs
Repeatedly checking your work
Tisha Wang MD UCLA The Effects of Sleep Deprivation and Implications for Residency Training
Sleepiness in residents is equivalent to that found in patients
with serious sleep disorders Mustafa and Strohl unpublished data Papp 2002
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Epworth Sleepiness Scale
Normal
Insomnia
Sleep Apnea
Residents
Narcolepsy
0
5
10
15
20
Mean 590 220 1170 1470 1750
Normal InsomniaSleep
ApneaResidents Narcolepsy
Some Individuals are More Fatigue
Resistant Than Others
People who prefer to be active early in the day
(ldquomorningnessrdquo) are often more affected by sleep
deprivation than people who are most alert in the
late evening hours (ldquoeveningnessrdquo)
Thus personal characteristics of being ldquolarksrdquo or
ldquoowlsrdquo seem to affect psychomotor performance
in the work environment
St Pierre (2011)
Sleep Inertia and the Pager
Sleep inertia refers to the cognitive
impairment present immediately on
awakening from sleep
The first 15-30 min after waking are a
vulnerable period and performance
decrements can exceed those after 24 hrs of
continuous wakefulness
Highlights risk of residents committing
fatigue-related errors when woken from sleep
by a page
Lockley (2007)
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
How Do You Manage Fatigue in the
OR
Posture Wauben et al reported a high prevalence rate (80)
of discomfort in the neck shoulders and back areas
among 280 surgeons in Europe Liberman et al
reported a high prevalence rate of lsquolsquoinjuriesrsquorsquo in the
hands fingers (42) and 107 in the neck among
colorectal surgeons
A recent study in Hong Kong found high prevalence
rates of neck and back musculoskeletal symptoms
among general surgeons The 12-month prevalence
rate was 829 for neck symptoms 578 for the
shoulder and 681 in the lower back
Szeto et al A study of surgeonsrsquo postural muscle activity during open laparoscopic and
endovascular surgery Surg Endosc (2010) 241712ndash1721
McDonald (1998)
Attention and Pacing You do drift Its human nature but thats when the risk factor increases Of course your attention span is decent the first hour or two then it gradually decreases I think the peak is between an hour and four hours After four hours your attention span starts to lessen You have to be aware of your attention span As the operation gets lengthy you have to be careful that you dont start losing your patience because you want to finish You have to say to yourself No I should not rush I should take my time You have to tell yourself and remind yourself that when you start to rush you get into trouble You say I should slow down because its better for the patient and its better for merdquo
- Elite neurosurgeon
Sleep Deprivation
Sleep Deprivation
ldquoSleep loss creates sleepiness which can be
associated with decrements in vigilance reaction
time psychomotor co-ordination information
processing decision making (eg fixation on
certain aspects of a situation to the neglect of other
information)rdquo
Rosekind MR et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Recognizing Sleep Deprivation in
Residency and Fellowship
Repeatedly yawning and ldquonodding offrdquo during
conferences or other sedentary activities (driving)
Loss of ability to perform usual activities quickly
Poor memory concentration judgment
Irritability moodiness depression
Dozing off while writing notesorders or while
reviewing medicationslabs
Repeatedly checking your work
Tisha Wang MD UCLA The Effects of Sleep Deprivation and Implications for Residency Training
Sleepiness in residents is equivalent to that found in patients
with serious sleep disorders Mustafa and Strohl unpublished data Papp 2002
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Epworth Sleepiness Scale
Normal
Insomnia
Sleep Apnea
Residents
Narcolepsy
0
5
10
15
20
Mean 590 220 1170 1470 1750
Normal InsomniaSleep
ApneaResidents Narcolepsy
Some Individuals are More Fatigue
Resistant Than Others
People who prefer to be active early in the day
(ldquomorningnessrdquo) are often more affected by sleep
deprivation than people who are most alert in the
late evening hours (ldquoeveningnessrdquo)
Thus personal characteristics of being ldquolarksrdquo or
ldquoowlsrdquo seem to affect psychomotor performance
in the work environment
St Pierre (2011)
Sleep Inertia and the Pager
Sleep inertia refers to the cognitive
impairment present immediately on
awakening from sleep
The first 15-30 min after waking are a
vulnerable period and performance
decrements can exceed those after 24 hrs of
continuous wakefulness
Highlights risk of residents committing
fatigue-related errors when woken from sleep
by a page
Lockley (2007)
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
Posture Wauben et al reported a high prevalence rate (80)
of discomfort in the neck shoulders and back areas
among 280 surgeons in Europe Liberman et al
reported a high prevalence rate of lsquolsquoinjuriesrsquorsquo in the
hands fingers (42) and 107 in the neck among
colorectal surgeons
A recent study in Hong Kong found high prevalence
rates of neck and back musculoskeletal symptoms
among general surgeons The 12-month prevalence
rate was 829 for neck symptoms 578 for the
shoulder and 681 in the lower back
Szeto et al A study of surgeonsrsquo postural muscle activity during open laparoscopic and
endovascular surgery Surg Endosc (2010) 241712ndash1721
McDonald (1998)
Attention and Pacing You do drift Its human nature but thats when the risk factor increases Of course your attention span is decent the first hour or two then it gradually decreases I think the peak is between an hour and four hours After four hours your attention span starts to lessen You have to be aware of your attention span As the operation gets lengthy you have to be careful that you dont start losing your patience because you want to finish You have to say to yourself No I should not rush I should take my time You have to tell yourself and remind yourself that when you start to rush you get into trouble You say I should slow down because its better for the patient and its better for merdquo
- Elite neurosurgeon
Sleep Deprivation
Sleep Deprivation
ldquoSleep loss creates sleepiness which can be
associated with decrements in vigilance reaction
time psychomotor co-ordination information
processing decision making (eg fixation on
certain aspects of a situation to the neglect of other
information)rdquo
Rosekind MR et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Recognizing Sleep Deprivation in
Residency and Fellowship
Repeatedly yawning and ldquonodding offrdquo during
conferences or other sedentary activities (driving)
Loss of ability to perform usual activities quickly
Poor memory concentration judgment
Irritability moodiness depression
Dozing off while writing notesorders or while
reviewing medicationslabs
Repeatedly checking your work
Tisha Wang MD UCLA The Effects of Sleep Deprivation and Implications for Residency Training
Sleepiness in residents is equivalent to that found in patients
with serious sleep disorders Mustafa and Strohl unpublished data Papp 2002
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Epworth Sleepiness Scale
Normal
Insomnia
Sleep Apnea
Residents
Narcolepsy
0
5
10
15
20
Mean 590 220 1170 1470 1750
Normal InsomniaSleep
ApneaResidents Narcolepsy
Some Individuals are More Fatigue
Resistant Than Others
People who prefer to be active early in the day
(ldquomorningnessrdquo) are often more affected by sleep
deprivation than people who are most alert in the
late evening hours (ldquoeveningnessrdquo)
Thus personal characteristics of being ldquolarksrdquo or
ldquoowlsrdquo seem to affect psychomotor performance
in the work environment
St Pierre (2011)
Sleep Inertia and the Pager
Sleep inertia refers to the cognitive
impairment present immediately on
awakening from sleep
The first 15-30 min after waking are a
vulnerable period and performance
decrements can exceed those after 24 hrs of
continuous wakefulness
Highlights risk of residents committing
fatigue-related errors when woken from sleep
by a page
Lockley (2007)
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
McDonald (1998)
Attention and Pacing You do drift Its human nature but thats when the risk factor increases Of course your attention span is decent the first hour or two then it gradually decreases I think the peak is between an hour and four hours After four hours your attention span starts to lessen You have to be aware of your attention span As the operation gets lengthy you have to be careful that you dont start losing your patience because you want to finish You have to say to yourself No I should not rush I should take my time You have to tell yourself and remind yourself that when you start to rush you get into trouble You say I should slow down because its better for the patient and its better for merdquo
- Elite neurosurgeon
Sleep Deprivation
Sleep Deprivation
ldquoSleep loss creates sleepiness which can be
associated with decrements in vigilance reaction
time psychomotor co-ordination information
processing decision making (eg fixation on
certain aspects of a situation to the neglect of other
information)rdquo
Rosekind MR et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Recognizing Sleep Deprivation in
Residency and Fellowship
Repeatedly yawning and ldquonodding offrdquo during
conferences or other sedentary activities (driving)
Loss of ability to perform usual activities quickly
Poor memory concentration judgment
Irritability moodiness depression
Dozing off while writing notesorders or while
reviewing medicationslabs
Repeatedly checking your work
Tisha Wang MD UCLA The Effects of Sleep Deprivation and Implications for Residency Training
Sleepiness in residents is equivalent to that found in patients
with serious sleep disorders Mustafa and Strohl unpublished data Papp 2002
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Epworth Sleepiness Scale
Normal
Insomnia
Sleep Apnea
Residents
Narcolepsy
0
5
10
15
20
Mean 590 220 1170 1470 1750
Normal InsomniaSleep
ApneaResidents Narcolepsy
Some Individuals are More Fatigue
Resistant Than Others
People who prefer to be active early in the day
(ldquomorningnessrdquo) are often more affected by sleep
deprivation than people who are most alert in the
late evening hours (ldquoeveningnessrdquo)
Thus personal characteristics of being ldquolarksrdquo or
ldquoowlsrdquo seem to affect psychomotor performance
in the work environment
St Pierre (2011)
Sleep Inertia and the Pager
Sleep inertia refers to the cognitive
impairment present immediately on
awakening from sleep
The first 15-30 min after waking are a
vulnerable period and performance
decrements can exceed those after 24 hrs of
continuous wakefulness
Highlights risk of residents committing
fatigue-related errors when woken from sleep
by a page
Lockley (2007)
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300

Sleep Deprivation
Sleep Deprivation
ldquoSleep loss creates sleepiness which can be
associated with decrements in vigilance reaction
time psychomotor co-ordination information
processing decision making (eg fixation on
certain aspects of a situation to the neglect of other
information)rdquo
Rosekind MR et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Recognizing Sleep Deprivation in
Residency and Fellowship
Repeatedly yawning and ldquonodding offrdquo during
conferences or other sedentary activities (driving)
Loss of ability to perform usual activities quickly
Poor memory concentration judgment
Irritability moodiness depression
Dozing off while writing notesorders or while
reviewing medicationslabs
Repeatedly checking your work
Tisha Wang MD UCLA The Effects of Sleep Deprivation and Implications for Residency Training
Sleepiness in residents is equivalent to that found in patients
with serious sleep disorders Mustafa and Strohl unpublished data Papp 2002
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Epworth Sleepiness Scale
Normal
Insomnia
Sleep Apnea
Residents
Narcolepsy
0
5
10
15
20
Mean 590 220 1170 1470 1750
Normal InsomniaSleep
ApneaResidents Narcolepsy
Some Individuals are More Fatigue
Resistant Than Others
People who prefer to be active early in the day
(ldquomorningnessrdquo) are often more affected by sleep
deprivation than people who are most alert in the
late evening hours (ldquoeveningnessrdquo)
Thus personal characteristics of being ldquolarksrdquo or
ldquoowlsrdquo seem to affect psychomotor performance
in the work environment
St Pierre (2011)
Sleep Inertia and the Pager
Sleep inertia refers to the cognitive
impairment present immediately on
awakening from sleep
The first 15-30 min after waking are a
vulnerable period and performance
decrements can exceed those after 24 hrs of
continuous wakefulness
Highlights risk of residents committing
fatigue-related errors when woken from sleep
by a page
Lockley (2007)
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300

Sleep Deprivation
ldquoSleep loss creates sleepiness which can be
associated with decrements in vigilance reaction
time psychomotor co-ordination information
processing decision making (eg fixation on
certain aspects of a situation to the neglect of other
information)rdquo
Rosekind MR et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Recognizing Sleep Deprivation in
Residency and Fellowship
Repeatedly yawning and ldquonodding offrdquo during
conferences or other sedentary activities (driving)
Loss of ability to perform usual activities quickly
Poor memory concentration judgment
Irritability moodiness depression
Dozing off while writing notesorders or while
reviewing medicationslabs
Repeatedly checking your work
Tisha Wang MD UCLA The Effects of Sleep Deprivation and Implications for Residency Training
Sleepiness in residents is equivalent to that found in patients
with serious sleep disorders Mustafa and Strohl unpublished data Papp 2002
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Epworth Sleepiness Scale
Normal
Insomnia
Sleep Apnea
Residents
Narcolepsy
0
5
10
15
20
Mean 590 220 1170 1470 1750
Normal InsomniaSleep
ApneaResidents Narcolepsy
Some Individuals are More Fatigue
Resistant Than Others
People who prefer to be active early in the day
(ldquomorningnessrdquo) are often more affected by sleep
deprivation than people who are most alert in the
late evening hours (ldquoeveningnessrdquo)
Thus personal characteristics of being ldquolarksrdquo or
ldquoowlsrdquo seem to affect psychomotor performance
in the work environment
St Pierre (2011)
Sleep Inertia and the Pager
Sleep inertia refers to the cognitive
impairment present immediately on
awakening from sleep
The first 15-30 min after waking are a
vulnerable period and performance
decrements can exceed those after 24 hrs of
continuous wakefulness
Highlights risk of residents committing
fatigue-related errors when woken from sleep
by a page
Lockley (2007)
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
Recognizing Sleep Deprivation in
Residency and Fellowship
Repeatedly yawning and ldquonodding offrdquo during
conferences or other sedentary activities (driving)
Loss of ability to perform usual activities quickly
Poor memory concentration judgment
Irritability moodiness depression
Dozing off while writing notesorders or while
reviewing medicationslabs
Repeatedly checking your work
Tisha Wang MD UCLA The Effects of Sleep Deprivation and Implications for Residency Training
Sleepiness in residents is equivalent to that found in patients
with serious sleep disorders Mustafa and Strohl unpublished data Papp 2002
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Epworth Sleepiness Scale
Normal
Insomnia
Sleep Apnea
Residents
Narcolepsy
0
5
10
15
20
Mean 590 220 1170 1470 1750
Normal InsomniaSleep
ApneaResidents Narcolepsy
Some Individuals are More Fatigue
Resistant Than Others
People who prefer to be active early in the day
(ldquomorningnessrdquo) are often more affected by sleep
deprivation than people who are most alert in the
late evening hours (ldquoeveningnessrdquo)
Thus personal characteristics of being ldquolarksrdquo or
ldquoowlsrdquo seem to affect psychomotor performance
in the work environment
St Pierre (2011)
Sleep Inertia and the Pager
Sleep inertia refers to the cognitive
impairment present immediately on
awakening from sleep
The first 15-30 min after waking are a
vulnerable period and performance
decrements can exceed those after 24 hrs of
continuous wakefulness
Highlights risk of residents committing
fatigue-related errors when woken from sleep
by a page
Lockley (2007)
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
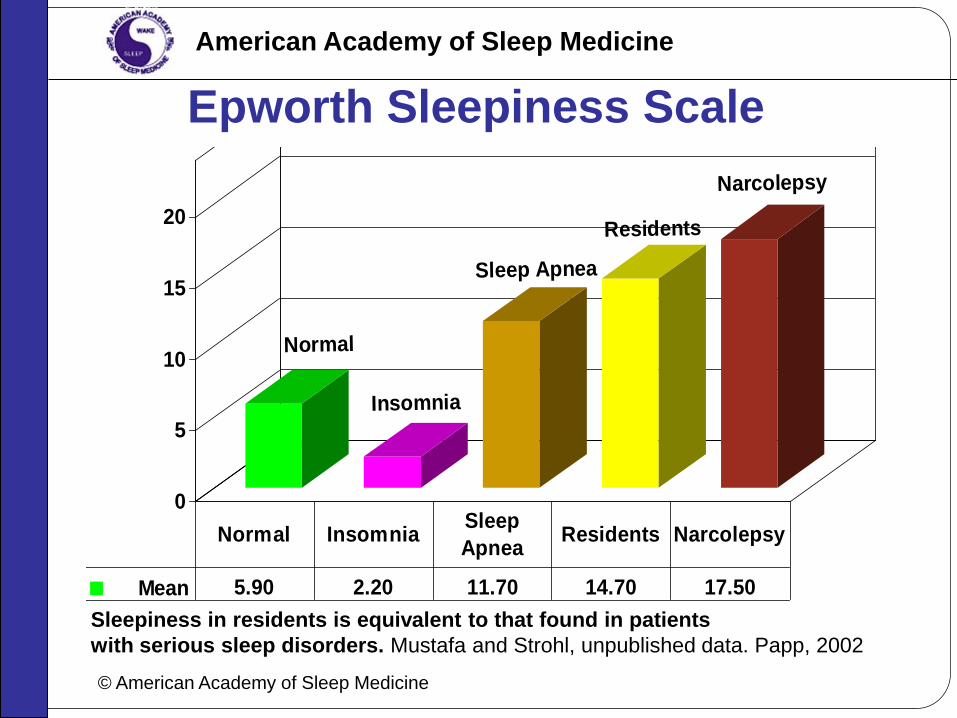
Sleepiness in residents is equivalent to that found in patients
with serious sleep disorders Mustafa and Strohl unpublished data Papp 2002
copy American Academy of Sleep Medicine
American Academy of Sleep Medicine
Epworth Sleepiness Scale
Normal
Insomnia
Sleep Apnea
Residents
Narcolepsy
0
5
10
15
20
Mean 590 220 1170 1470 1750
Normal InsomniaSleep
ApneaResidents Narcolepsy
Some Individuals are More Fatigue
Resistant Than Others
People who prefer to be active early in the day
(ldquomorningnessrdquo) are often more affected by sleep
deprivation than people who are most alert in the
late evening hours (ldquoeveningnessrdquo)
Thus personal characteristics of being ldquolarksrdquo or
ldquoowlsrdquo seem to affect psychomotor performance
in the work environment
St Pierre (2011)
Sleep Inertia and the Pager
Sleep inertia refers to the cognitive
impairment present immediately on
awakening from sleep
The first 15-30 min after waking are a
vulnerable period and performance
decrements can exceed those after 24 hrs of
continuous wakefulness
Highlights risk of residents committing
fatigue-related errors when woken from sleep
by a page
Lockley (2007)
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
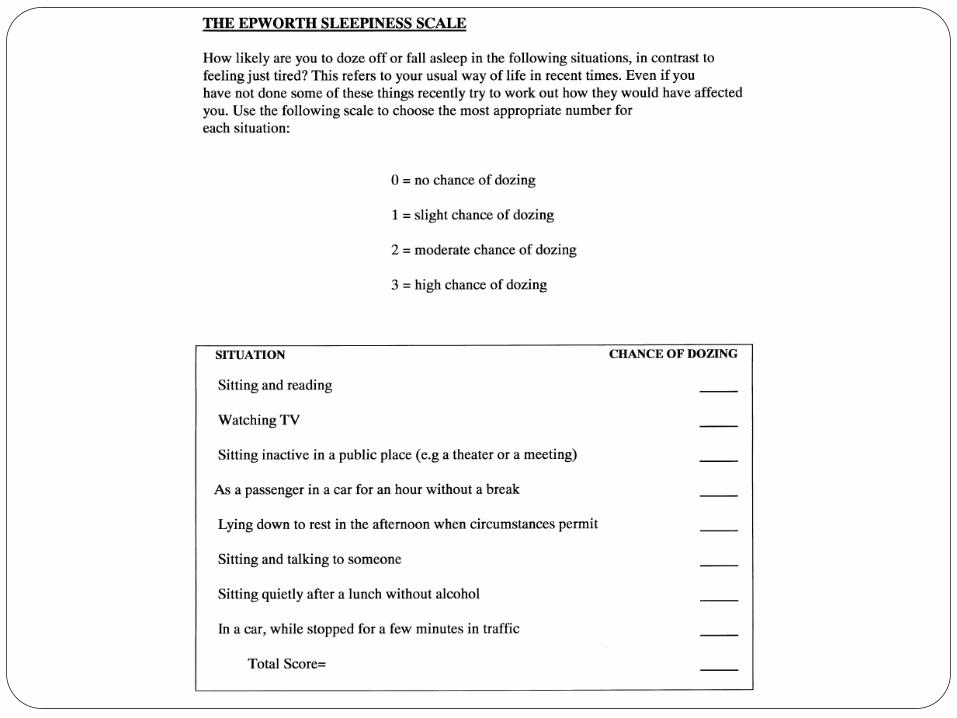
Some Individuals are More Fatigue
Resistant Than Others
People who prefer to be active early in the day
(ldquomorningnessrdquo) are often more affected by sleep
deprivation than people who are most alert in the
late evening hours (ldquoeveningnessrdquo)
Thus personal characteristics of being ldquolarksrdquo or
ldquoowlsrdquo seem to affect psychomotor performance
in the work environment
St Pierre (2011)
Sleep Inertia and the Pager
Sleep inertia refers to the cognitive
impairment present immediately on
awakening from sleep
The first 15-30 min after waking are a
vulnerable period and performance
decrements can exceed those after 24 hrs of
continuous wakefulness
Highlights risk of residents committing
fatigue-related errors when woken from sleep
by a page
Lockley (2007)
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
Sleep Inertia and the Pager
Sleep inertia refers to the cognitive
impairment present immediately on
awakening from sleep
The first 15-30 min after waking are a
vulnerable period and performance
decrements can exceed those after 24 hrs of
continuous wakefulness
Highlights risk of residents committing
fatigue-related errors when woken from sleep
by a page
Lockley (2007)
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
What Helps
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
How do You Get More Sleep
What choices can you make to increasepreserve
your sleep
When can you try and pay off your sleep debt
Do you rationalize lack of sleep in a way that
might create further problems
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
What Helps
Be sure to get adequate sleep before anticipated
sleep loss ndash donrsquot start out with a sleep debt
Plan for adequate recovery sleep Data indicates
that is takes two nights of extended sleep to
restore alertness after a night of total sleep loss
Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300

Try to stay active during on-call shifts (eg take a walk during breaks or climb stairs between floors)
Strategic caffeine use includes avoiding it when you are alert-at the beginning of a work period or just after a nap Consumption should begin about an hour before expected times of decreased alertness (eg 3am ndash 5am)
What Helps During On-call
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
What Helps During On-call
Brief (1-2 hours) napping prior to prolonged
period of sleep loss such as 24 hours on call
can enhance alertness
To be therapeutic during a shift naps should
ideally be frequent (every 2-3 hours) and brief
(15-30 minutes)
If you can pick just one nap get it as early in the
period of sleep deprivation as possible
Time naps during circadian window of
opportunity between 2-5 am and 2-5 pm
A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300

A Nap Intervention in a Group of
Physicians and Nurses During Actual
Night Shifts in the ED
ldquoSubjects who napped had faster reaction times and
fewer vigilance lapses at 730 am and rated themselves
as less fatigued more vigorous and less sleepy at the
end of their night shiftFinally subjects who napped
started a simulated intravenous catheter more quickly
than controlsrdquo
Smith-Coggins (2006)
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
What Helps Post-on-call
On the days following your time ldquoon callrdquo and
particularly your 24 hour period per week off
make sure yoursquore getting sufficient catch up
sleep
There is evidence that melatonin has a soporific
effect when taken outside the normal sleep
period particularly when taken to phase-advance
the sleep period
Arnedt (2005)
Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300

Sleep Hygiene Develop rituals that help you relax each night before bed
Keep a regular sleep schedule as much as possible
Protect your sleep time enlist your family and friends
Donrsquot go to bed unless you are sleepy
Limit late day caffeine intake
Limit alcohol intake within six hours of your bedtime
Do not go to bed hungry but no heavy meals within 3 hours of
sleep
Optimize you sleeping environment Cooler temperature Dark
(eye shades room darkening shades) Quiet (unplug phone turn
off pager use ear plugs white noise
If you are not asleep after 30 minutes then get out of the bed
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
Sleep Deprivation and Driving ldquoThe odds that interns will have a documented motor vehicle crash on the commute after an extended work shift were more than double the odds after a non-extended shift Near-miss incidents were more than five times as likely to occur after an extended work shift as they were after a non-extended shiftrdquo
Barger (2005)
What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300

What Else do You Need to Know
About Sleep Deprivation and Fatigue
Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300

Resident Wellness
Resource Booklet
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
E-couch
A self-help interactive program with modules for depression generalized anxiety and worry social anxiety relationship breakdown and loss and grief It provides evidence- based information and teaches strategies drawn from cognitive behavioral and interpersonal therapies as well as relaxation and physical activity techniques
wwwecouchanueduauwelcome
MoodGym
An innovative interactive web program designed to prevent depression It consists of five modules an interactive game anxiety and depression assessments downloadable relaxation audio a workbook and feedback assessment
httpmoodgymanueduauwelcome
Overcoming Perfectionism
This information package is designed to help you understand what is helpful and unhelpful about being a perfectionist The goal is not for you to give up your high standards altogether but to learn to pursue healthy high standards rather than unrelenting high standards that negatively impact your life This Infopax is organized into modules that are designed to be worked through in sequence We recommend that you complete one module before going on to the next Each module includes information worksheets and suggested exercises or activities
wwwccihealthwagovauresourcesinfopaxcfmInfo_ID=52
CALM
Computer Assisted Learning for the Mind contains podcasts and audio files that can be easily uploaded to mobile devices The tunes included within this website are geared towards mental resilience managing stressors healthy relationships and meaning in life
httpwwwcalmaucklandacnz18html
Resident Wellness Resources
Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300

Where to Go For Help Office of Resident Wellness
Dr Susan Edwards Director Resident Wellness Available Tuesdays and Thursdays 416-946-4015 Susanedwardsutorontoca Christopher Hurst M Ed Wellness Consultant Available for consult on Tuesdays and Thursdays 416-978-6861 christopherhurstutorontoca Diana Nuss Assistant To Dr Susan Edwards and Christopher Hurst Available Monday to Friday 416-946-3074 pgwellnessutorontoca
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
What Can the Office of Resident
Wellness Do For Me
Appointment with the Director of Resident Wellness
Advice
Advocacy
Referrals to appropriate providers for stress and other
issues
Speak to resident groups
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
Where to Go For Help Physician Health Program OMA
Confidential assessment and triage for all physicians
experiencing difficulty with stress mental health or
substance use issues
wwwphpomaorg or 1 800 851-6606
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
Thanks
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300
References Aringkerstedt T Perski A Kecklund G Sleep stress and burnout In Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011
Arnedt J Melatonin characteristics concerns and prospectsJ Biol Rhythms 200520291ndash303
Barger LK Cade BE Ayas NT Cronin JW Rosner B Speizer FE Czeisler CA Extended Work Shifts and the Risk of Motor Vehicle Crashes among Interns N Engl J Med 2005 352125-134
Hagger MS Wood C Stiff C Chatzisarantis NL Ego depletion and the strength model of self-control a meta-analysis Psychol Bull 2010 Jul136(4)495ndash525
Lockley SW Barger LK Ayas NT Rothschild JM Czeisler CA Landrigan CP Effects of health care provider work hours and sleep deprivation on safety and performance Jt Comm J Qual Patient Saf 2007 Nov33(11 Suppl)7-18
McCray LW Cronholm PF Bogner HR Gallo JJ Neill RAMcCray LW Cronholm PF Bogner HR Gallo JJ Neill RAResident Physician Burnout Is There Hope Fam Med 200840(9)626-32
McCormick F Kadzielski J Landrigan C Evans B Herndon J Rubash H Prospective Analysis of the Incidence Risk and Intervals of Predicted Fatigue-Related Impairment in Residents Arch Surg 2012147(5)430-435 doi101001archsurg201284
McDonald J Orlick T Excellence in Surgery Psychological Considerations The Sport Psychologist1994 7 31-48
Rosekind MR Gander PH Gregory KB et al Managing Fatigue in Operational Settings 1 Physiological Considerations and Countermeasures Behavioral Medicine 1996 21 157-165
Rothschild JM Keohane CA Rogers S et al Risks of Complications by Attending Physicians After Performing Nighttime Procedures JAMA 2009302(14)1565-1572
P C Schutte Fatigue Risk Management Charting a path to a safer workplace Human Factors Research Group CSIR Centre for Mining Innovation 2009
Danzigera S LevavJAvnaim-Pessoa L (11 April 2011) Extraneous factors in judicial decisions Proceedings of the National Academy of Sciences of the United States of America
Smith-Coggins R Howard SK Mac ST Wang C et al Improving Alertness and Performance in Emergency Department Physicians and Nurses The Use of Planned Naps Annals of Emergency Medicine Volume 48 Issue 5 November 2006 596-604e3
StPierre M Hofinger G Simon R BuerschaperC Attention The Focus of Consciouness In Crisis Management in Acute Care Settings Human Factors Team Psychology and Patient Safety in a High Stakes Environment Springer-Verlag Berlin Heidelberg 2011
Szeto G P Y Ho P Ting A C W Poon J T C Tsang R C C Cheng S W K A study of surgeonsrsquo postural muscle activity during open laparoscopic and endovascular surgery Surg Endosc (2010) 241712ndash1721
Van Dongen H Hursh R Fatigue Performance Errors and AccidentsIn Principle and Practice of Sleep Medicine St Louise Elsevier Saunders 2011 p 753-759
Wang T The Effects of Sleep Deprivation and Implications for Residency Training
West CP Tan AD Habermann TM Sloan JA Shanafelt TD ldquoAssociation of resident fatigue and distress with perceived medical errorsldquo JAMA 2009 Sep 23302(12)1294‐300

















