40
San Diego Long Term Care Integration Project (LTCIP) Mental Health & Substance Abuse Workgroup September 23, 2003
| Date post: | 03-Jan-2016 |
| Category: |
Documents |
| Upload: | mark-maxwell |
| View: | 216 times |
| Download: | 2 times |

San Diego Long Term Care Integration Project (LTCIP)
Mental Health & Substance Abuse Workgroup
September 23, 2003

Community Planning Process
Grass-roots effort to improve system of care for long term care consumers and providers
From 50 to 550+ key stakeholders over past 4 years: 10,000+ hours
Agreement to use existing providers, assure fair compensation
Planning within state LTCIP authorization, AB 1040 (form follows funding)

San Diego County Board of Supervisors&
State Office of Long Term Care
Rodger G. Lum, Ph.D, DirectorCounty of San Diego, Health & Human Services
Agency, (HHSA)
Advisory Group:Goal: Make final decisions and
recommendations for inclusion in the plan.
Planning Committee:Goal: Guide the LTCIP planning process.
Suspended Workgroups pending service delivery
model decision
Suspended Workgroups pending service delivery
model decisionHealth Plan Workgroup
Health Plan Workgroup Finance/Data
Workgroup
Finance/DataWorkgroup Options Workgroup
Options Workgroup
Internet• Facilitates
communication• Provides broad public
education
Pamela B. Smith, Project DirectorEvalyn Greb, Project ManagerAging & Independence Services
Lead County Agency
Mental HealthWorkgroup
Mental HealthWorkgroup
Explore use of the Healthy SanDiego model for potentialService delivery system for LTCIP.
Determine the financialfeasibility of the proposedLTCIP for San Diego County.
Make recommendation to Planning Committee re: inclusion of mentalhealth and substance abuse services in LTCIP.
Incremental LTCI Strategies:1) Network of Care2) Physician Strategy3) Health Plan Pilots
Governance-Case Management-Info/Technology-Quality Assurance-Scope of Services-Workforce Issues-Community Network Development
Developmental DisabilitiesWorkgroup
Developmental DisabilitiesWorkgroup
Make recommendation to PC re: inclusion of persons with developmental disabilities in LTCIP.
Long Term Care Integration Project
Organizational Chart & Decision Tree
8/2003

Legislative Authority
AB 1040 in 1995 (revised in 1998) State Office of LTC:
– provides planning $$– provides “Center” resources– provides liaison with other state programs– approves local activity toward LTCI– will assist in procuring federal waivers

San Diego LTCIP Stakeholder Vision for Elderly & Disabled Develop “system” that:
– provides continuum of all health, social and support services that “wrap around consumer” w/prevention & early intervention focus
– pools associated (categorical) funding– is consumer driven and responsive– expands access to/options for care

Stakeholder Vision (continued)
– Fairly compensates all providers w/rate structure developed locally
– Engages MD as pivotal team member– Decreases fragmentation/duplication
w/single point of entry, single plan of care– Improves quality & is budget neutral– Implements Olmstead Decision locally– Maximizes federal and state funding

Why change?
Impact of demographics Cost containment vs. care management Consumer/outcomes not current focus Incentives for optimum care not aligned Health & support service fragmentation

Client Referral Patterns

From Vision to Service Delivery Model…
CUSTOMER ACCESS w ith LTCIP
Customer At Home/Community
Care Manager w/ Network of Care
IncomeAsst.
SeniorCntr.
In-homecare
HICAP
MedicalClinic/Health
Care
BloodPressure
Cks
ShoppingAsst. Mental
Health
Transp.
Escort
housingRehab
Intake Worker InformationProvided

From Vision to Service Delivery Model… Explore Healthy San Diego due to:
– Access, education, prevention– Advocacy– Cost-effectiveness– Population-based– Existing infrastructure– Stakeholder-designed, BUT

HSD Currently Does NOT…
Tailor the program for chronic care or aged and disabled persons
Provide “wraparound” services Provide chronic care management on a
population basis Receive adequate reimbursement for
chronic care Have much info on “duals”

Where are we now?
BOS: “come back with 3 options” Dr. Mark Meiners strategies/looking for
“consortium of funding”:– Network of Care– Physician Strategy – HSD Health Plan/Pilot Projects
Administrative Action Plan for FY 2003-04 State Development Grant
Establishment of Mental Health Workgroup

Why should mental health stakeholders get involved?
To influence planning and decisions To impact delivery of acute & LTC
needs of individuals (support+services) To recommend to include mental health
and substance abuse service integrated with primary, acute, and social support

Mental Health Today Current Medi-Cal carve-out (UBH) Limited Medicare reimbursement LTCIP stakeholders want no carve-outs Mental health problems under-diagnosed &
under-treated Quality of life and cost impact of untreated
mental illness/substance abuse is huge Most state integration projects do not enroll
disabled w/primary MH diagnosis Seniors do not self-identify as having MH
need; don’t use MH Centers

Mental Health and LTCIP
Establishment of Mental Health Workgroup to:– hear from broad array of stakeholders (132 invited!)– focus on consumer as “whole” in system– develop plan specific to San Diego and LTCIP
How do we “mainstream” mental health services for aged and disabled?– parity w/physical health for treatment– age-, disease-specific treatment– delivered as “part of the whole”– viewed within greater context of health

LTCIP Mental Health Workgroup Goal Process… Make recommendation to Planning
Committee on inclusion of mental health programs, populations, and services
Importance of consensus on a recommendation
Forward to Planning Committee by February 2004

Why do we even talk about Integrating primary medical care
and mental health care?
Margaret E. McCahill, M.D.
Clinical Professor, UCSD School of Medicine
Director of Clinical Services, St. Vincent de Paul Village
Diplomate, American Board of Family Practice
Diplomate, American Board of Psychiatry and Neurology

How do we think about diagnoses?
Axis-I: what major mental illness does the patient have?
Axis-II: what kind of patient has the illness? (P.D.’s, developmental disorders, etc.)
Axis-III: what general medical conditions does the patient have?
Axis-IV and Axis-V: interesting, and have some prognostic value, but not generally used by primary care practitioners

It takes awareness of the proper treatment of all THREE axes to treat the patient effectively The personality-disordered patient will act
out more if the major depression is not treated
The diabetic will be out of control if the personality disorder or psychosis is not managed
The psychosis will be worse if the asthma, diabetes, pneumonia, etc., is not treated

Multidisciplinary teams Bring a wealth of comprehensive
skills and service to the patient are essential in many settings to be
sure that the patient is receiving the correct treatment that he/she needs
However…they need to be well coordinated, and someone needs to be aware of the big picture…the overall view of the patient’s health care needs--all 3 axes.

Integration is not new:From the AAFP, 11/94:
“White Paper on the Provision of Mental Health Care Services by Family Physicians” AAFP Reprint no. 714
“After replacing its managed care firm (i.e., a “carve-out” model) with a collaborative mental health care model, a large health care delivery system reduced by 33% its overall medical and mental health costs, while retaining high consumer and provider satisfaction.”

Expertise in psychiatric diagnosis Most primary care physicians can
recognize most mood disorders, anxiety disorders, psychoses
personality disorders and substance use disorders can be more difficult to recognize at first
but remember...

Even for the “experts:” Psychiatric diagnosis is always a work in progress
For example, major depression is only major depression until the first episode of mania, and now its bipolar disorder
“Schizophrenia” may be an initial impression until the UDS comes back positive for amphetamines…
The challenge: how to treat the patient when the diagnosis might change…


Is this our field of expertise? Who treats patients for depression? (Rx only)
general and family physicians ? %
internists ? % other specialists ? %
psychiatrists ? %

Is this our field of expertise?
Who treats patients for depression? (Rx only)
general and family physicians 56%
internists 11% other specialists 10%
psychiatrists 23%

Kroenke and Price. Kroenke and Price. Arch Intern MedArch Intern Med. 1993;153:2474.. 1993;153:2474.
0 20 40 60 80 100
Insomnia
Fatigue
Constipation
Fainting
Headache
Palpitations
0 20 40 60 80 100
Insomnia
Fatigue
Constipation
Fainting
Headache
Palpitations
Physical Symptoms often attributed to Psychiatric illness

Kroenke et al. Kroenke et al. Arch Fam MedArch Fam Med. 1994;3:774.. 1994;3:774.
0 10 20 30 40 50 60 70
Fainting
Insomnia
Chest Pain
Abdominal Pain
Headache
Fatigue
Mood Disorder Anxiety Disorder
0 10 20 30 40 50 60 70
Fainting
Insomnia
Chest Pain
Abdominal Pain
Headache
Fatigue
Mood Disorder Anxiety Disorder
Somatic Symptoms In Mood And Anxiety Disorders

0
20
40
60
80
100
0 to 1 2 to 3 4 to 5 6 to 8 >9
Anxiety Disorder Mood Disorder Any Phychiatric Disorder
0
20
40
60
80
100
0 to 1 2 to 3 4 to 5 6 to 8 >9
Anxiety Disorder Mood Disorder Any Phychiatric Disorder
%%
Kroenke et al. Kroenke et al. Arch Fam MedArch Fam Med. 1994;3:774.. 1994;3:774.
Physical Symptoms (#)Physical Symptoms (#)
Physical Symptoms & Risk of Psychiatric Disorder


0
10
20
30
40
50
60
Any Anxiety Depression Somatoform Multiple
0
10
20
30
40
50
60
Any Anxiety Depression Somatoform Multiple
Prev.Prev.(%)(%)
**PP<.05<.05O’Malley et al. O’Malley et al. Arch Intern MedArch Intern Med. 1998;158:2357.. 1998;158:2357.
Psychiatric DisorderPsychiatric Disorder
**
**
ConnectiveConnective Articular orArticular orPeriarticularPeriarticular
Nonarticular orNonarticular orOtherOther
Psychiatric Disorders In Rheumatology Referrals

Cumulative Mortality For Depressed And Non-depressed Patients Following Heart Attack
Frasure-Smith et al. Frasure-Smith et al. JAMAJAMA. 1993;270:1819.. 1993;270:1819.
0
5
10
15
20
25
30
0 1 2 3 4 5 6
Months After Heart Attack
Mortality(%)
Depressed (N = 35)
Nondepressed (N = 187)
0
5
10
15
20
25
30
0 1 2 3 4 5 6
Months After Heart Attack
Mortality(%)
Depressed (N = 35)
Nondepressed (N = 187)
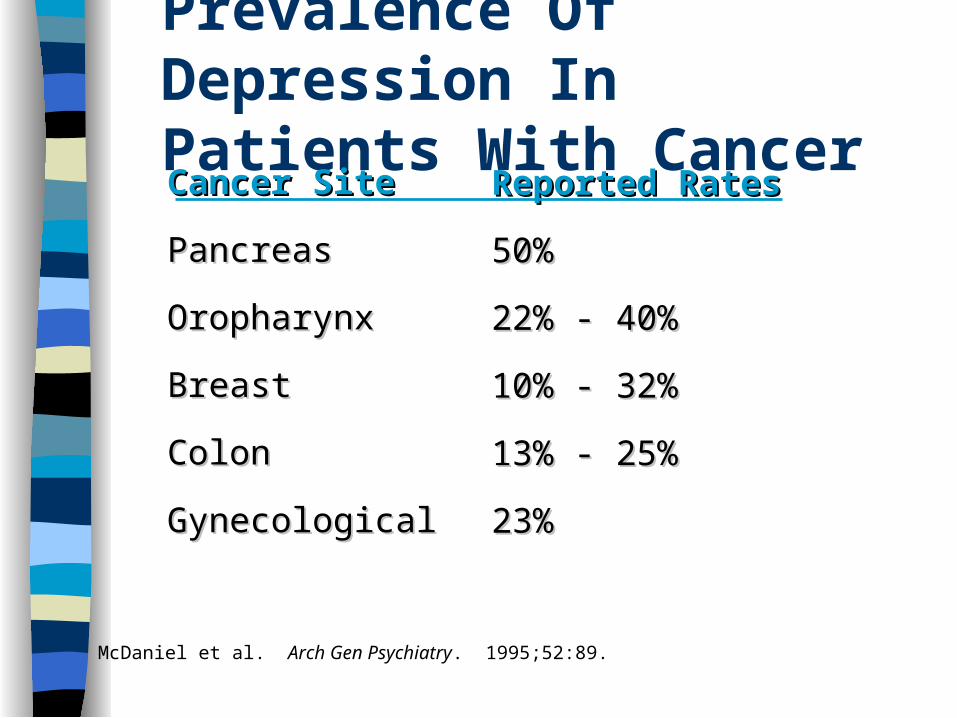
Prevalence Of Depression In Patients With Cancer
McDaniel et al. Arch Gen Psychiatry. 1995;52:89.
Cancer SiteCancer Site
PancreasPancreas
OropharynxOropharynx
BreastBreast
ColonColon
GynecologicalGynecological
Reported RatesReported Rates
50%50%
22% - 40%22% - 40%
10% - 32%10% - 32%
13% - 25%13% - 25%
23%23%
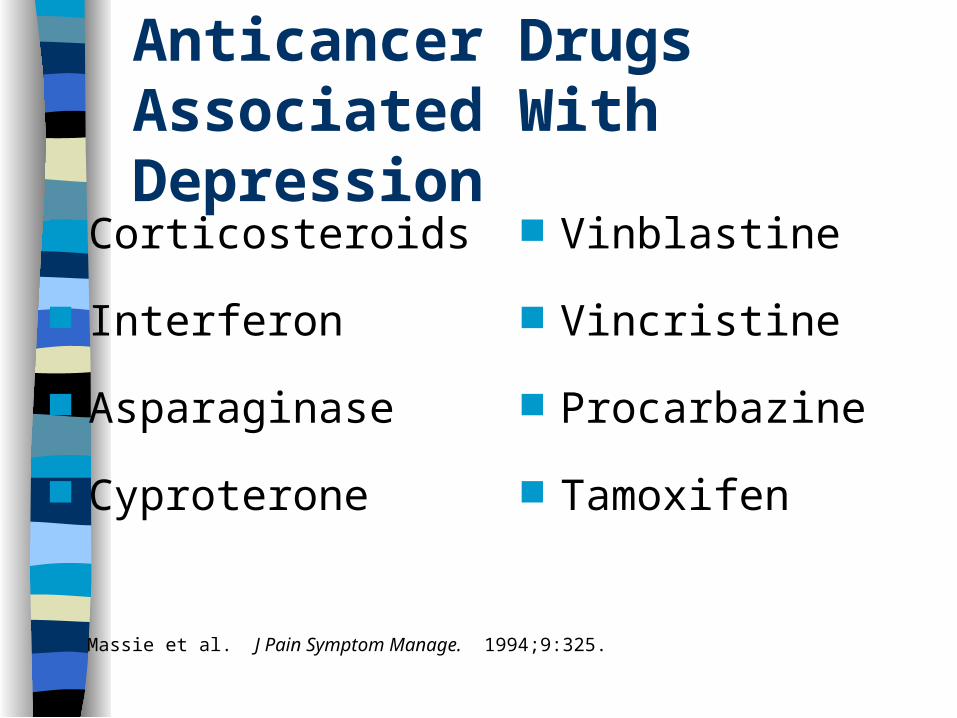
Anticancer Drugs Associated With Depression
Massie et al. J Pain Symptom Manage. 1994;9:325.
Corticosteroids
Interferon
Asparaginase
Cyproterone
Vinblastine
Vincristine
Procarbazine
Tamoxifen

HIV Disease
Initial presentation of illness may be psychiatric symptoms
Untreated mental disorders worsen the primary illness
The medications used in treatment of HIV disease may exacerbate/cause mental illness
A presentation unto itself

Katon et al. Katon et al. Gen Hosp PsychiatryGen Hosp Psychiatry. 1990;12:355.. 1990;12:355.
PatientsPatients(%)(%)
0
25
50
75
100
MajorDepression
PanicDisorder
GeneralizedAnxiety
Disorder
SomatizationDisorder
AlcoholAbuse/
Dependence
0
25
50
75
100
MajorDepression
PanicDisorder
GeneralizedAnxiety
Disorder
SomatizationDisorder
AlcoholAbuse/
Dependence
Psychiatric Disorders &High Medical Utilizers (n=119)

Special problems:
Drug interactions abuse potential of medications compliance issues diversion of medications follow-up issues interaction between mental illness
and general medical conditions—both current and those that develop with time…..others…

Next Steps Sign-up to be considered for smaller
stakeholder work committee 15 stakeholders will be selected by
LTCIP staff and Dr. McCahill Formal invitation to participate in
working committee by October 10 First meeting: Oct. 21, 2003 from 2:30-
4:00 at Aging & Independence Services
November 2003 Mental Health Workgroup Meeting Staff and committee work to-date presented Option discussion by full group Ideas for further option development Refer back to staff and committee Consensus development at January MH
Workgroup meeting Forward recommendation to LTCIP Planning
Committee

How can you influence planning?
Get on LTCIP mailing list for updates
Participate in Planning Committee and Mental Health Workgroup meetings
Log onto website for background & info: www.sdcounty.ca.gov/cnty/cntydepts/health/ais/ltc/
Call 858-495-5428 or e-mail on-going input/ideas: [email protected]

















