58
Scanning the Post Thyroidectomy Neck Teresa M Bieker, MBA, RDMS, RDCS, RVT Lead Sonographer University of Colorado Hospital
| Date post: | 18-Dec-2015 |
| Category: |
Documents |
| Upload: | winfred-francis |
| View: | 220 times |
| Download: | 1 times |

Scanning the Post Thyroidectomy Neck
Teresa M Bieker, MBA, RDMS, RDCS, RVTLead Sonographer
University of Colorado Hospital

Appearance of Normal Cervical Lymph Nodes
Appearance of Abnormal Cervical Lymph Nodes
Identifying Zones/Levels of the Neck
Scanning Technique and Protocol

Thyroid cancer is the most common endocrine cancer
In 2011, there where 48,020 new cases (26,550 women, 11,470 men) and 1,740 deaths
For 2013, American Cancer Society estimates 60,220 new cases (46,970 women, 13,250 men) and 1,850 deaths
Two thirds of patients are between 20-55 with a mean age of 45
Causes include:
occupational risks
dietlifestyleparityfamily history
Well Differentiated Thyroid Cancer:
Papillary
Follicular
Arise from thyroid follicular cells
Account for 80-90% of all thyroid cancers
Poorly Differentiated Thyroid Cancer:
Medullary (5-10%)
Anaplastic (1-2%)

Thyroid cancer is treatable; however, outcome is dependent on stage (I-IV)
Five year survival rates:
Papillary: 51% to >99%
Follicular: 50% to >99%
Medullary: 28% to near 100%
Anaplastic: 7%
Age
Distant metastasis
Local invasiveness
Cervical lymph node metastasis
Tumor size
Multifocality
Tumor subtype

T = Tumor
N = Node
M = Distal Metastasis

TX: Primary tumor cannot be assessed
T0: No evidence of primary tumor.
T1: Tumor ≤2 cm in greatest dimension limited to the thyroid.T1a: Tumor ≤1 cm, limited to the thyroid.T1b: Tumor >1 cm but ≤2 cm in greatest dimension, limited to the thyroid.
T2: Tumor >2 cm but ≤4 cm in greatest dimension, limited to the thyroid.
T3: Tumor >4 cm in greatest dimension limited to the thyroid or any tumor with minimal extrathyroid extension (e.g., extension to sternothyroid muscle or perithyroid soft tissues).
T4a: Moderately advanced disease.Tumor of any size extending beyond the thyroid capsule to invade subcutaneous soft tissues, larynx, trachea, esophagus, or recurrent laryngeal nerve.
T4b: Very advanced disease.Tumor invades prevertebral fascia or encases carotid artery or mediastinal vessels

NX: Regional lymph nodes cannot be assessed.
N0: No regional lymph node metastasis.
N1: Regional lymph node metastasis.
N1a: Metastases to Level VI (pretracheal, paratracheal, and
prelaryngeal/Delphian lymph nodes).
N1b: Metastases to unilateral, bilateral, or contralateral cervical
(Levels I, II, III, IV, or V) or retropharyngeal or superior
mediastinal lymph nodes (Level VII)

M0: No Distant metastasis
M1: Distant metastasis

Stage T N M
Younger then 45 years
I any T any N MO
II any T any N M1
45 years and older
I T1 N0 M0
II T2 N0 M0
III T3 N0 M0
T1 N1a M0
T2 N1a M0
T3 N1a M0
IVA T4A N0 M0
T4A N1a M0
T1 N1b M0
T2 N1b M0
T3 N1a M0

For well differentiated thyroid cancer, there is a 9-30% recurrence rate within the first decade after diagnosis
Most recurrences occur within the thyroid bed or cervical lymph nodes
60-75% occur in Z3 or Z4
20% occur in Z6
Tend to affect the ipsilateral neck

Total or near total thyroidectomy is the standard treatment for thyroid cancer. Z6 lymph nodes can also be removed at this time
If the lateral/cervical lymph nodes are involved, a neck dissection is also performed
Ultrasound and FNA are essential for surgical management

Physical palpation exam by endocrinologist/surgeon
Depending on extent of disease:
Iodine 131 whole body scan
Radioactive iodine ablation therapy
Chest x-ray
CT/MRI/PET
Neck ultrasound/Labwork (6-12 months)

Typically drawn every 6-12 months
Thyroglobulin (Tg)
Specific protein secreted from thyroid tissue
Tg levels should be undetectable in disease free patients
If Tg increases, it is likely caused by recurrent tumor
Tg Antibodies
Present in 20-25% of thyroid cancer patients
If antibodies are positive, Tg levels are falsely decreased
Tg antibodies typically decrease over several years
When disease in present, antibodies can increase
Thyroid Stimulating Hormone (TSH) - suppressed by medication

There are approximately 300 lymph nodes in the neck
Normal nodes have a cortex and medulla covered by a fibrous capsule
Cortex: contains lymphocytes packed together forming spherical lymphoid follicles
Medulla: contains trabeculae and medullary cords and sinuses. Multiple medullary sinuses form the echogenic hilum
A main artery and vein enter/exit the node at the hilum


training.seer.cancer.gov

Common Locations
Normal Appearance
Abnormal Appearance

Arranged in chains
Commonly visualized along:
Jugular chain
Submandibular gland
Supraclavicular region
Thyroid bed

ATA recommends U/S pre and post thyroidectomy
More sensitive in detecting lymph nodes and determining benign vs malignant
More cost effective
Quicker, non-invasive
No radiation
Can detect disease as small as 2-3mm (often before palpated or detected by Tg)
FNA
Very operator dependent

12-15 MHz, 8MHz curved
Patient Position
Supine with neck extended
Elevating the head 20o in obese patients may help
Neck rotation
Image optimization


Indications: Routine screening Elevated TG Follow-upCorrelation with NM, CT, PET
Zones 1-7 are evaluated and imaged
Residual thyroid tissueRecurrent thyroid tumorAbnormal lymph nodes


ZONES LANDMARKS NODAL GROUP
IA Midline. Anterior to the digastric muscle and superior to the hyoid bone Submental
IB Lateral to zone IA, but medial or anterior to the submandibular gland Submandibular nodes
IIAAnterior or medial to the interior jugular vein but Lateral/posterior to the submandibular gland. Superior to the hyoid bone
Upper internal jugular chain. More superiorly, the parotid nodes.
IIB Posterior to the interior jugular veinUpper internal jugular chain. More superiorly, the parotid nodes.
IIIFrom the level of the hyoid bone inferiorly to the cricoid arch. Lateral to the common carotid artery.
Middle internal jugular chain
IVFrom the level of the cricoid arch inferiorly to the level of the clavicle. Lateral to the common carotid artery.
Lower internal jugular chain
VAPosterior to the sternocleidomastoid muscle, from the base of the skull to the cricoid arch
Supraclavicular fossa/posterior triangle (spinal accessory chain and transverse cervical chain
VBPosterior to the sternocleidomastoid muscle from the croicoid arch to the level of the clavicle
Supraclavicular fossa/posterior triangle (spinal accessory chain and transverse cervical chain
VIAnterior/medial to the common carotid arteries from the level of the hyoid to the manubrium
Anterior cervical nodes, pre and paratracheal
VIIAnterior/medial to the common carotid arteries, inferior to the sternal notch
Anterior, upper mediastinal nodes
Sup Clav Lateral to the common carotid artery. At or inferior to the clavicle Supraclavicular nodes

It is not unusual to see multiple normal nodes in the neck
The number of normal nodes visualized increases with age
Characterized by:
Location
Shape
Size
Echogenicity
Vascular pattern
Presence of echogenic hilum

Hypoechoic cortex
Echogenic hilumStrong predictor of a normal nodeMaybe difficult to visualize in small nodes
One feeder vessel (hilar flow)
Cylindrical or cigar shape

Lose elliptical shape and become more rounded
Malignant cells invade the node, disrupting the hilum
96% of malignant nodes lack a fatty hilum
Become hyperechoic with papillary invasion but hypoechoic with medullary and lymphoma.
Increase in echogenicity due to the presence of Tg within the lymph node
Microcalcifications
Mixed or peripherial flow
Cystic in advanced disease




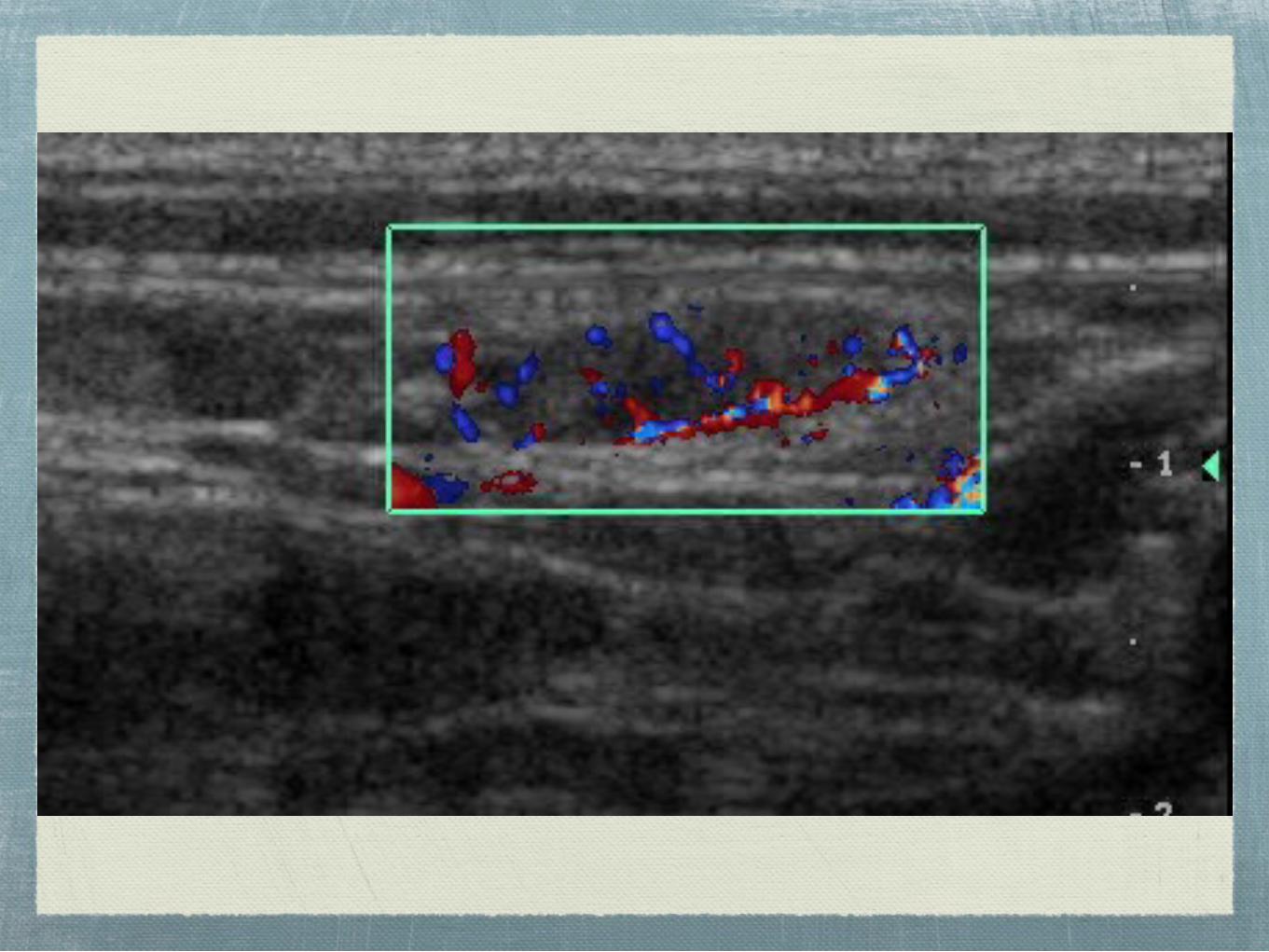
Hilar: flow branches radially from the hilum
Peripheral: flow is present along the periphery of the node but does not arise from the hilar vessels
Mixed: hilar and peripheral flow
Absence of flow despite optimal Doppler settings
Literature is inconsistent on benefit of color and pulsed Doppler



Following thyroidectomy, the paratracheal region should be homogeneous
Z6 masses can include:
Postoperative scarring
Muscle
Necrosing fat
Suture granulomas
Parathyroid gland
Lymph node
Remnant tissue
Metastasis




Medial or anterior to the SMG
Midline/superior to hyoid bone
Nodal group: submental/submandibular
Unusual to have papillary involvement in Zone 1
Often see reactive nodes

Anterior/medial to the CCA
From the hyoid inferiorly to the manubrium
Nodal group: anterior cervical nodes, pre and para tracheal
20% of recurrences are in Zone 6

Lateral/posterior to the SMG
Superior to the hyoid bone (CCA bifurcation)
Nodal group: upper IJ chain, parotid nodes
Reactive nodes can be seen in Zone 2
Uncommon for PTC, but can occur

From the level of the hyoid (CCA bifurcation) to the cricoid cartilage (level of expected thyroid bed)
Lateral to CCA
Nodal group: middle IJ chain
60-75% of recurrences are in Zone 3 or 4

From the cricoid arch to the level of the clavicle (thyroid bed level)
Lateral to the CCA
Nodal group: lower IJ chain
60-75% of recurrences are in Zone 3 or 4

Anterior/ medial to CCA
At or inferior to the sternal notch
Nodal group: anterior, upper mediastinal nodes
Zone 7 vs Notch:Zone 7 is inferior to the subclavian
This changes surgical management. “Notch” nodes can be removed during standard thyroidectomy. Zone 7 nodes requires a more extensive surgery

Lateral to the CCA
At or inferior to the clavicle
Nodal group: supraclavicular nodes

Posterior to sternocleidomastoid, superior to clavicle
Nodal group: supraclavicular fossa, posterior triangle
Uncommon location for PTC recurrence

We do not label A or B for Zones 1, 2, 5
Evaluate Zone 5 only if palpable
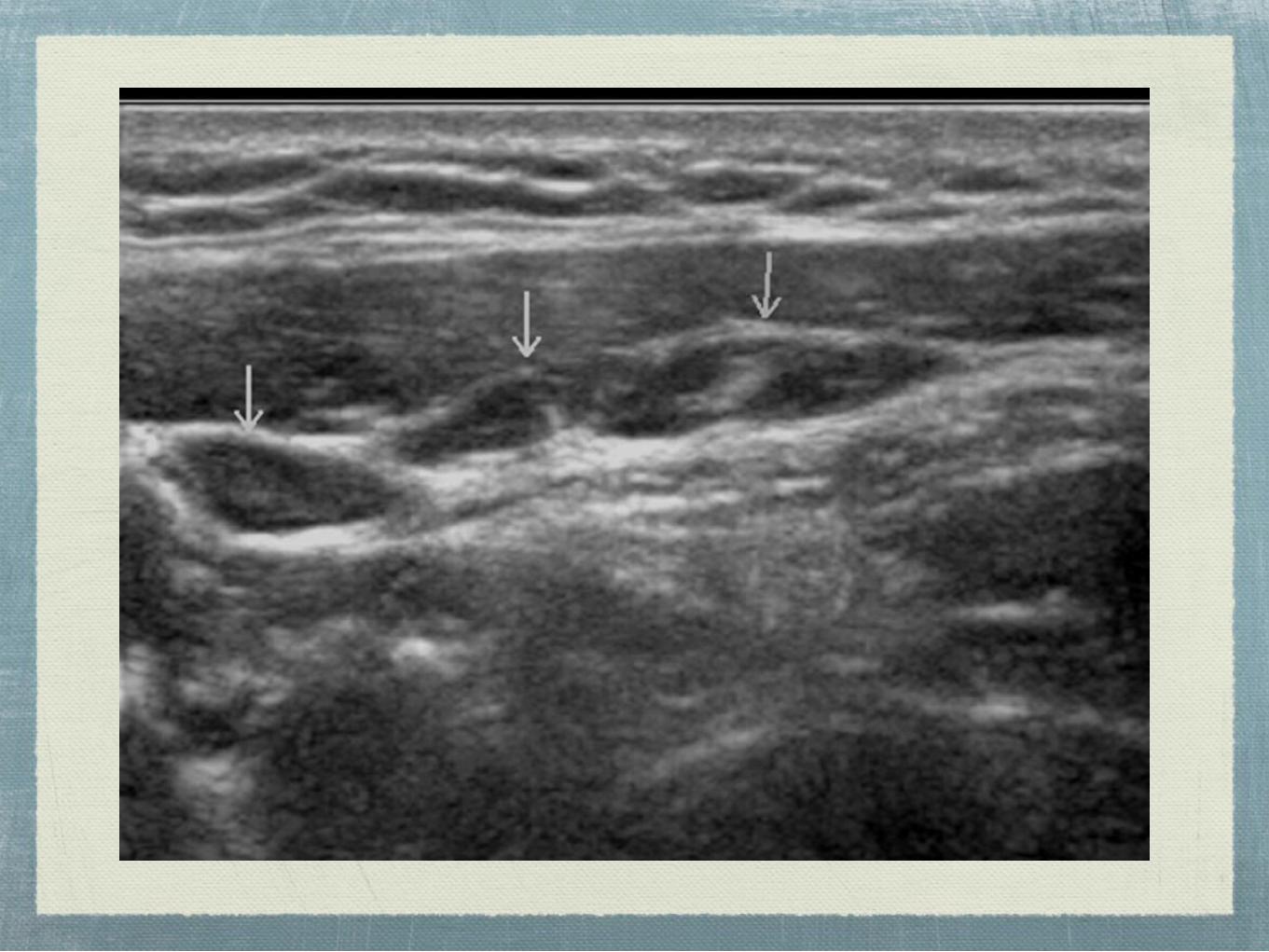
Arrow normal nodes
If no nodes are seen, take image labeled “lateral neck”
Zone 2 is lateral to SMG only. It does not extend midline.
Measure largest or most worrisome node in each zone, can number others
Measure largest or most worrisome thyroid nodule
Take cine if unsure




If less then 5mm, nodes are difficult to track
Is the abnormality in Zone 6 reproduceable in all 3 planes? If not, don’t measure
Can this be biopsied?
To determine Zone 3/4 vs Zone 6, put the patient in a neutral position
Thyroid bed vs Zone 6 labeling: Use Z6 after thyroidectomy or to measure abnormality superior or inferior to the thyroid


Additional Reference: Bieker T. Scanning the Post-Thyroidectomy Neck:
Appearance and Technique. Journal of Diagnostic Medical Sonography.
2010. 26(5): 215-223.

















