31
Schizophrenia David Soskin, M.D. Medical Director, MCBH Chief of Psychiatry, NMC
| Date post: | 13-Dec-2015 |
| Category: |
Documents |
| Upload: | alexis-ross |
| View: | 217 times |
| Download: | 0 times |
Schizophrenia
David Soskin, M.D.Medical Director, MCBHChief of Psychiatry, NMC
Objectives
• Schizophrenia:– Defining features– Phenomenology of schizophrenia– Diagnosis

What is Psychosis?
• Impairment in reality-testing

What is Schizophrenia?

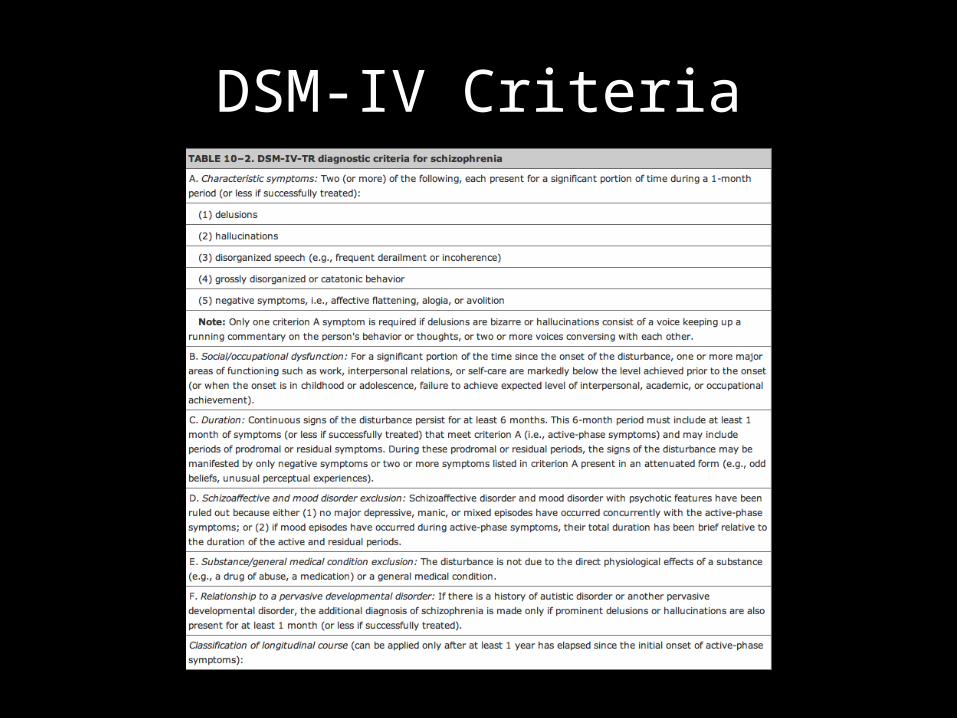
DSM-IV Criteria
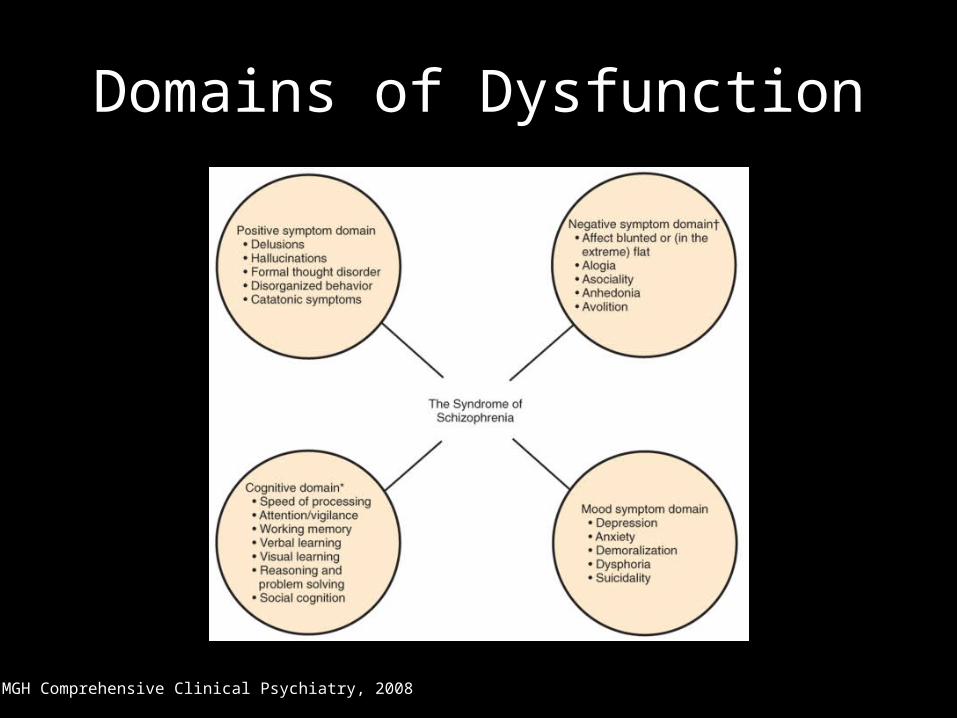
Domains of Dysfunction
MGH Comprehensive Clinical Psychiatry, 2008

Positive Symptoms
MGH Comprehensive Clinical Psychiatry, 2008

Positive Symptoms
MGH Comprehensive Clinical Psychiatry, 2008
Disorganization• Yet here, Laertes! aboard, aboard, for shame! The wind sits in the shoulder of your sail,
And you are stay’d for. There; my blessing with thee! And these few precepts in thy memory. See thou character. Give thy thoughts no tongue, Nor any unproportioned thought his act. Be thou familiar, but by no means vulgar. Those friends thou hast, and their adoption tried, Grapple them to thy soul with hoops of steel; But do not dull thy palm with entertainment. Of each new-hatch’d, unfledged comrade. Beware of entrance to a quarrel, but being in, Bear’t that the opposed may beware of thee. Give every man thy ear, but few thy voice; Take each man’s censure, but reserve thy judgment. Costly thy habit as thy purse can buy, But not express’d in fancy; rich, not gaudy; For the apparel oft proclaims the man, And they in France of the best rank and station, Are of a most select and generous chief in that. Neither a borrower nor a lender be; For loan oft loses both itself and friend, And borrowing dulls the edge of husbandry. This above all: to thine ownself be true, And it must follow, as the night the day, Thou canst not then be false to any man. Farewell: my blessing season this in thee. (Shakesepare, Hamlet)
• Circumstantial

Disorganization• The fall (bababadalgharaghtakamminarronnkonnbronntonner
ronntuonnthunntrovarrhounawnskawntoohoohoordenenthur nuk!) of a once wall strait oldparr is retaled early in bed and later on life down through all christian minstrelsy. The great fall of the off wall entailed at such short notice the pftjschute of Finnegan, erse solid man, that the humptyhillhead of humself prumptly sends an unquiring one well to the west in quest of his tumptytumtoes: and their upturnpikepointandplace is at the knock out in the park where oranges have been laid to rust upon the green since dev-lins first loved livvy. (Joyce, Finnegan’s Wake)
• Loose, tangential, neologisms, alliteration/clanging

Disorganization• So, nat by night by naught by naket, in those good old lousy days gone by, the days,
shall we say? of Whom shall we say while kinderwardens minded their twinsbed, therenow they stood, the sycomores, all four of them, in their quartan agues, the majorchy, the minorchy, the everso and the fermentarian with their ballyhooric blowreaper, titranicht by tetranoxst, at their pussycorners, and that old time pallyollogass, playing copers fearsome, with Gus Walker, the cuddy, and his poor old dying boosy cough, esker, newcsle, saggard, crumlin, dell me, donk, the way to wumblin. Follow me beeline and you're bumblin, esker, newcsle, saggard, crumlin. And listening. So gladdied up when nicechild Kevin Mary (who was going to be commandeering chief of the choirboys' brigade the moment he grew up under all the auspices) irishsmiled in his milky way of creamdwibble and onage tustard and dessed tabbage, frighted out when badbrat Jerry Godolphing (who was hurrying to be cardinal scullion in a night refuge as bald as he was cured enough unerr all the hospitals) furrinfrowned down his wrinklywaste of methylated spirits, ick, and lemoncholy lees, ick, and pulverised rhubarbarorum, icky waste of methylated. (Joyce, Finnean’s Wake)
• Word Salad

Subjective vs. Objective
Kring, Psychiatry Res, 2005
Cognitive
• Cognitive deficits include:– Attention– Memory– Language– Executive function– Information processing– Social cognition
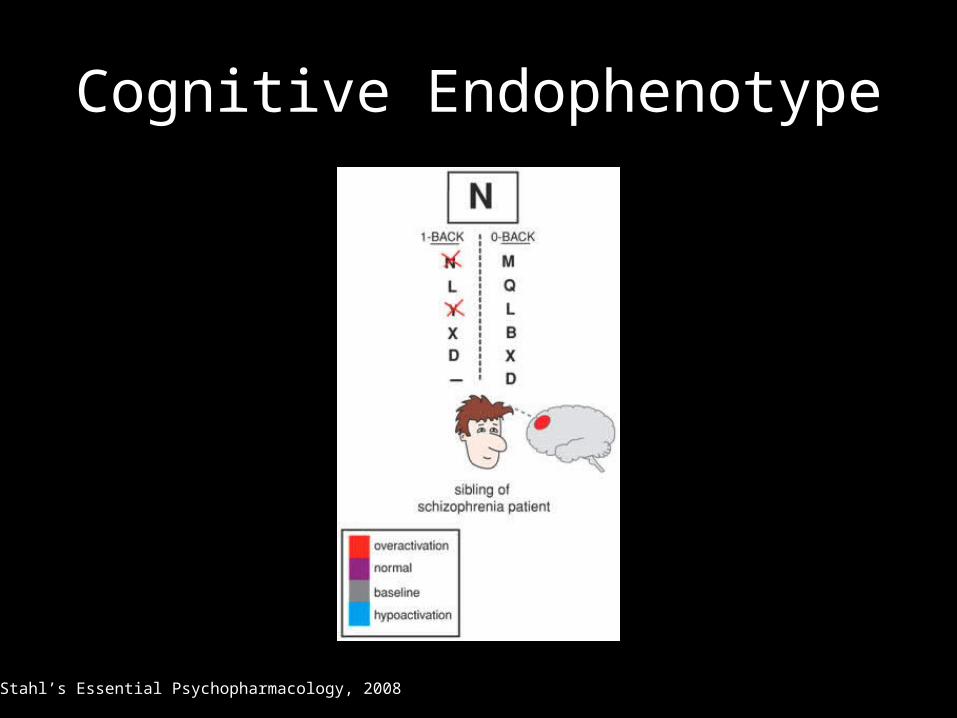
Cognitive Endophenotype
Stahl’s Essential Psychopharmacology, 2008
Epidemiology
• Prevalence?– 1% lifetime prevalence
• Gender differences?– Males 30-40% higher lifetime risk (McGrath, 2004)– Age of onset 3-4 years later for females (Aleman, 2003)
• Economic Burden?– 50% of all inpatient admissions (Geller, 92)– $62.7 billion in U.S. in 2002 (Wu, 2005)
• Genetics:– Heritability coefficient 0.25-0.50
APA Textbook of Psychiatry, 2008
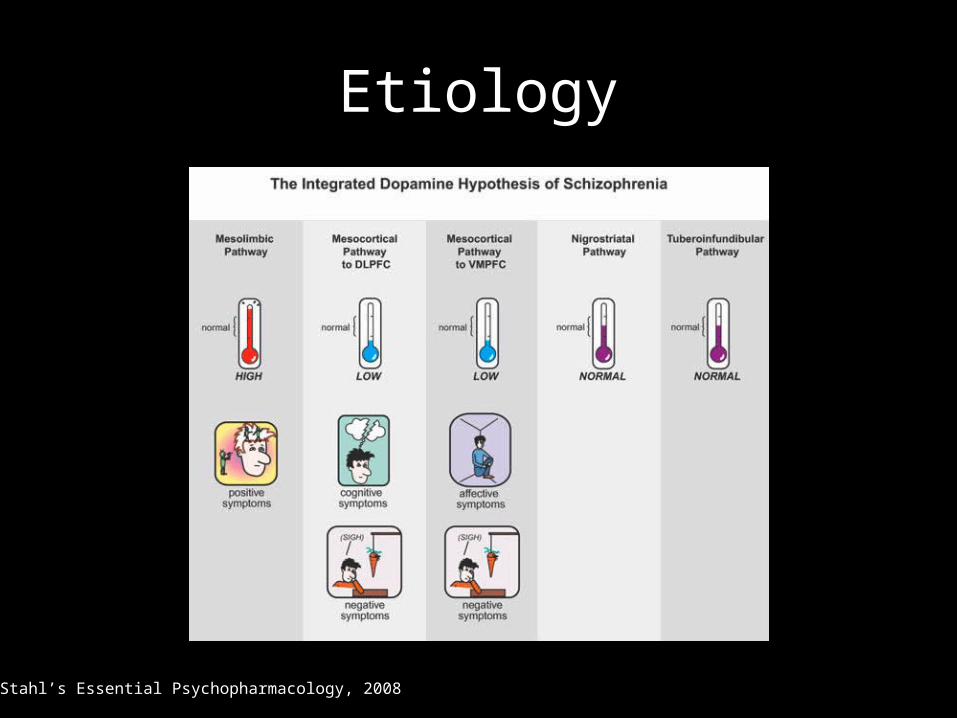
Etiology
Stahl’s Essential Psychopharmacology, 2008

Etiology
• Multiple Neurotransmitter Systems?– Serotonin– Acetylcholine– GABA– Glutamate

Stahl’s Essential Psychopharmacology, 2008

MGH Comprehensive Clinical Psychiatry, 2008
Diathesis Model
• Prenatal infection (rubella and infection)• Obstetric complicatons• Season of birth (winter)• Immigration• Head injury• Drug use (LSD, cannabis, and amphetamines)
MGH Comprehensive Clinical Psychiatry, 2008

Neurodevelopmental Model
APA Textbook of Psychiatry, 2008
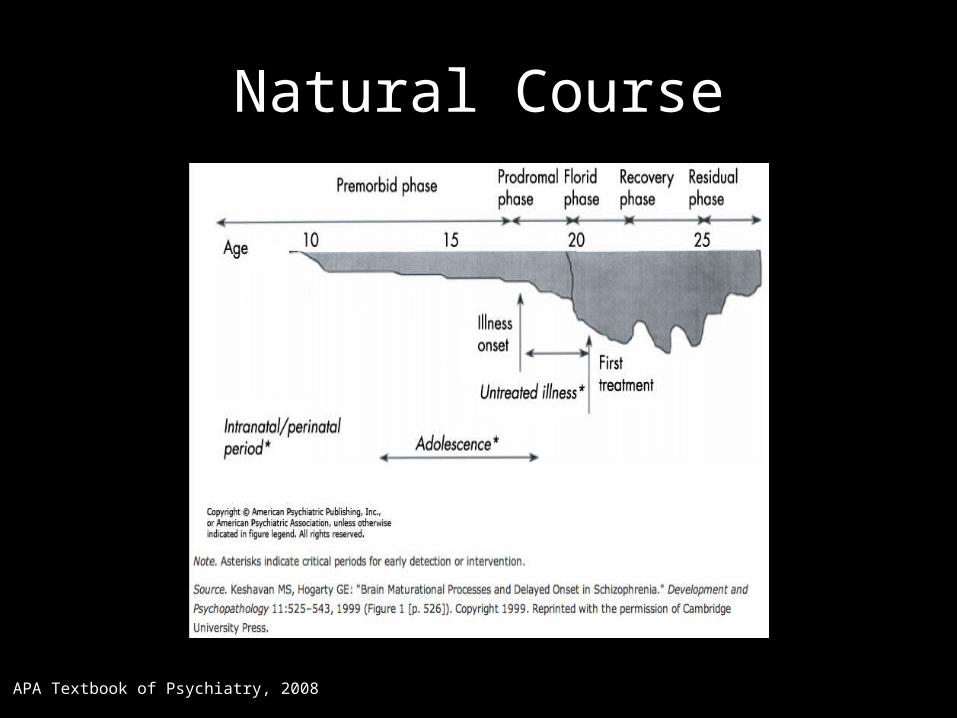
Natural Course
APA Textbook of Psychiatry, 2008
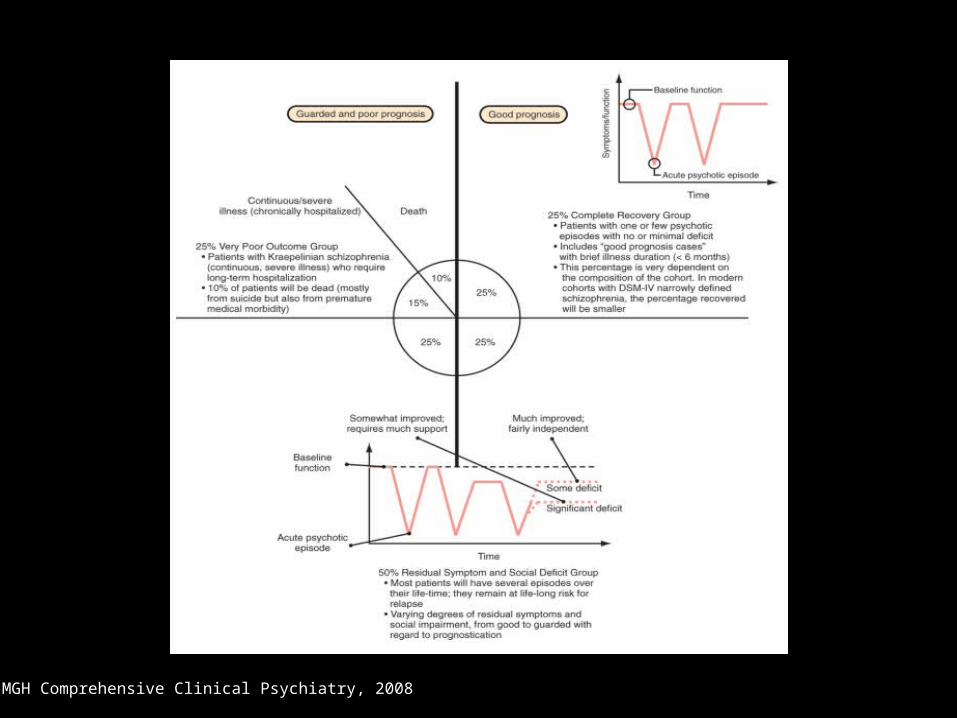
MGH Comprehensive Clinical Psychiatry, 2008

Clinical Integration
• Are there things that have happened to you recently that you can’t explain?
• Have you had any problems with your mind playing tricks on you?
• Have you seen or heard things that other people haven’t?
• Do you have any concerns that people are bothering you or trying to harm you?
• What about people on the radio or TV giving you special messages?

Differential Diagnosis
• Medical:– Delirium, CNS infections, dementia, other degenerative
CNS, structural CNS, metabolic, endocrine• Substance:
– Stimulants, sedatives, cannabis, hallucinogens, steroids, opioids, anticholinergic agents, anesthetics, antiinfectious agents
• Psychiatric:– Bipolar, MDE with psychotic features, episodic psychosis,
SAD, BPD or borderline personality structure, cluster A
“Though this be madness, yet there is method in it.”
• Suspect malingering psychosis if:– Hallucinations continuous rather than intermittent– Vague or inaudible AH– Hallucinations not associated with delusions– Abrupt onset or termination of delusions– Eagerness to call attention to delusions– Conduct not consistent with delusions– Bizarre content without disordered thinking– Inconsistency on cognitive testing– Symptom inconsistency– Inability to identify alleviating or exacerbating factors
Resnick, Psychiatric Clinics of North America, 1999

Diagnostic Studies
• Laboratory:– CBC, chemistry 10, urine toxicology, liver function
tests, UA, TSH, B12, folate, RPR, HIV, ceruloplasmin
• Imaging:– MRI
• If clinically indicated:– CXR, EEG, LP, neuropsychiatric testing

Prognostic Questions
• Acute versus insidious onset?– Acute
• Childhood versus adult onset?– Adult
• Predominance of positive versus negative versus cognitive symptoms at onset?– Positive • Living in a developing versus industrialized country?– Developing

















