Allison Ross Eckard, MD Professor of Pediatrics and Medicine, Divisions of Infectious Diseases Division Director, Pediatric Infectious Diseases February 23, 2021 SCHOOL RE-OPENING IN THE TIME OF COVID-19: An Overview of What We Know & Current Best Practices
Transcript
Allison Ross Eckard, MDProfessor of Pediatrics and Medicine, Divisions of Infectious Diseases
SCHOOL RE-OPENING IN THE TIME OF COVID-19:An Overview of What We Know & Current Best Practices
The Bottom Line…▸ Children (in general) should be attending school
in person.▸ In-person school is safe for students and
teachers if appropriate multi-layered risk mitigation strategies are in place.
▸ In-person school with appropriate risk mitigation is not risk free, but activities outside of school pose a much higher risk to individuals.
▸ In-person learning in this modified setting is not ideal, but ▸ is essential for the greater good and▸ is superior to virtual learning.▸ Children are resilient; no evidence that mitigation
strategies are adversely affecting their well-being
Facts about COVID-19
▸ South Carolina has been hit hard by COVID-19, especially when you consider case rate and death rate per 100k population.
▸ Much of South Carolina is rural and not necessarily equipped to handle this type of public health/medical crisis.
▸ Many hospitals in SC are struggling to keep up with the many demands that COVID-19 has created.
COVID-19 is serious, and the pandemic has caused catastrophic morbidity and mortality in the U.S. and worldwide.
COVID-19 in South Carolina & by Region
(as of 2/23/2021)
Facts about COVID-19
▸ CDC list of underlying conditions (independent of age) that increase or might increase your risk of severe disease is extensive & includes many common conditions:▸ Obesity (42.4% of Americans)▸ Diabetes (10.5% of Americans)▸ Hypertension (45% of Americans) ▸ Smoking (14% of Americans)
Source: CDC
While statistically it is true that older people & people with underlying conditions die more often from COVID-19, many “underlying conditions” are very common and people often live normal lives for many decades with many of these chronic conditions.
▸ Most people recover completely from COVID-19 within a few weeks.
▸ But some people continue to have symptoms for weeks to months, even those with mild symptoms and those without underlying medical conditions (including young adults and children).
▸ A recent systematic review of published studies found >50 described long-term effects of COVID-19. ▸ Most common were fatigue, headache, attention
disorder, hair loss, and dyspnea (trouble breathing)▸ There is still much to learn about how COVID-19
may increase the risk of long-term health problems, including in children and those with mild symptoms.
82 Children Admitted to MUSC with Acute COVID-19 in the Last Year (0-21 years old)*
02468
1012141618
Healthy Misc.Med.Cond.
Healthy Diabetes SickleCell
Disease
Asthma SpecialNeeds
ImmuneSystemCond.
Misc.Med.Cond.
<2 years old >2 years old
• Some admitted b/c COVID-19 worsened their underlying condition• A few developed serious disease from COVID-19; all survived • 3 healthy children presented w/ new Type 1 diabetes related to COVID
*Excludes those with a positive COVID test found incidentally on admission
African-American Children and <2 Years Old Have Been Hit Hardest by COVID-19 at MUSC
48
9137
21
50
1020304050
ALL CHILDREN HEALTHY CHILDREN
# Admissions by Race/Ethnicity
African American HispanicCaucasian/Other
25
47 7
1316
82
-3
2
7
12
17
22
27
# Admissions by Age Range (Years)
*Excludes those with a positive COVID test found incidentally on admission
COVID-19 poses a greater risk to many of the same children who obtain essential services at school (e.g., OT/PT/speech therapy, medical and mental health treatment, nutrition, etc.) and/or are most at risk for educational disparities w/ virtual learning.
We have the responsibility to provide a safe in-person school environment for these at risk and disadvantaged children.
Rare Complications in Healthy Children
▸ Myocarditis (heart inflammation) ▸ “Cardiovascular Magnetic
Resonance Findings in Competitive Athletes Recovering From COVID-19 Infection”
▸Rajpal et al, JAMA, Sept 2020▸26 competitive college athletes w/
COVID-19 at OSU▸4 (15%) had MRI findings
suggestive of myocarditis▸2 w/ mild COVID-19
symptoms, 2 w/ no symptoms
• 2060 cases and 30 deaths so far in U.S.
Multi-System Inflammatory Syndrome in Children (MIS-C)
Source: SC DHEC & CDC
A rare but very serious and often life-threatening post-infectious inflammatory syndrome in children (0-21 yrs) that occurs 2-4 weeks after having COVID-19.
Most families do not know their children had COVID-19 or even were exposed to the virus.
Most children with MIS-C were completely healthy before.
Most common symptoms = fever, vomiting/diarrhea, fatigue (can include rash and/or red eyes)
Oher Facts about COVID-19 in Children▸ Children can transmit SARS-CoV-2 even if asymptomatic.▸ Evidence does suggest that younger children (particularly ≤5
years old) are not as likely to get infected or transmit the virus. ▸ But, there are many variables that matter….
School Closures: Wide-Reaching Negative Impact on Students & Families▸ Decreases in educational performance
▸ “COVID-19 slide”: 70% of SC students in grades 3-8 projected not to meet grade level proficiency standards in math and English language arts in Spring 2021 (SC Education Oversight Committee)
▸ Increase in community-based gun violence; increase in weekday home-based gun violence with a larger proportion involving children (Liou, et al)
▸ Increase in suicidal behavior among youths (Hill RM, et al)▸ Decreases in emergency dept visits related to child/abuse
neglect but % requiring hospitalization increased (MMWR)▸ Additional potential consequences:
▸ Poorer nutrition and health, socio-emotional growth; add’lburdens on families; disproportionately affect vulnerable & disadvantaged children
MUSC-CCSD-DHEC Partnership for Safer School Re-opening▸ CCSD contracted with MUSC’s Back2Business to help assess schools,
implement wide-reaching mitigation strategies & troubleshoot/adjust strategies as needed.
▸ Intensive, coordinated team of 8 full-time CCSD nurse liaisons trained by DHEC on contact tracing.
▸ MUSC established in-school saliva testing for symptomatic students/staff.▸ We hosted multiple live-streamed discussions for families and community
leaders to get feedback, address concerns, and reinforce safety precautions.
Charleston County School District Opened for 5-Day/Week In-Person School on 9/8/2020
SC DHEC
Situation at Time of Re-opening
*Excludes charter schools; **Includes only staff with direct student contact and/or staff regularly present on school property (3,470 teachers, 210 substitute teachers, 1,507 support staff, 451 bus driver contractors, 269 daytime part-time/full-time custodial staff, 421 nutrition service contractors); °One 9-12th grade school also includes early head start children
37,065 total in-person staff/students*
• 30,737 in-person students (~70% of total)• 6,328 in-person staff**
COVID-19 Cases Among In-Person Students and Staff During First Semester
▸ Case Inclusion▸ DHEC reports every positive case
among school-aged children to appropriate school district + self reporting by staff/families.
▸ COVID cases/associated information are centrally compiled by DHEC-trained CCSD contact tracers.
▸ Data presented include every CCSD COVID-19 case among in-person students/staff from 9/8-12/18 + students/staff with positive tests and/or symptoms from 12/19-12/20 who attended school while potentially infectious.
▸ All additional cases with symptom onset or positive tests from 12/19-1/1 were reviewed for in-school transmission potential and included in data where deemed appropriate.
497 in-person cases (1.3% of total in-person students/staff)
294 students (0.96% of total in-person students)
• 74 schools w/ ≤13 total positive students at each school (19 schools w/ no cases)
• 2 largest high schools w/ 19 and 39 positive students each
202 staff (3.2% of total in-person staff)• 76 schools w/ ≤10 positive staff at
each school (9 schools w/ no cases) • 6 bus drivers • 1 from a center for advanced studies • 1 substitute teacher, school unknown
*if person at multiple locations, primary location used for data compilation but all locations considered for contact tracing
Number of Daily COVID-19 Cases by Group
0
2
4
6
8
10
12
14
16
18
20
22
9/8/
2020
9/10
/202
09/
12/2
020
9/14
/202
09/
16/2
020
9/18
/202
09/
20/2
020
9/22
/202
09/
24/2
020
9/26
/202
09/
28/2
020
9/30
/202
010
/2/2
020
10/4
/202
010
/6/2
020
10/8
/202
010
/10/
2020
10/1
2/20
2010
/14/
2020
10/1
6/20
2010
/18/
2020
10/2
0/20
2010
/22/
2020
10/2
4/20
2010
/26/
2020
10/2
8/20
2010
/30/
2020
11/1
/202
011
/3/2
020
11/5
/202
011
/7/2
020
11/9
/202
011
/11/
2020
11/1
3/20
2011
/15/
2020
11/1
7/20
2011
/19/
2020
11/2
1/20
2011
/23/
2020
11/2
5/20
2011
/27/
2020
11/2
9/20
2012
/1/2
020
12/3
/202
012
/5/2
020
12/7
/202
012
/9/2
020
12/1
1/20
2012
/13/
2020
12/1
5/20
2012
/17/
2020
12/1
9/20
2012
/21/
2020
Students Staff
Characteristics Among Students and Staff with COVID-19 Attending School In-Person
Frequency (%) unless otherwise noted Students(N=295)
Staff(N=202)
Total(N=497)
Median age in years (range) 12 (1-18) -- --Symptoms reported 193 (65.4%) 182 (90.0%) 375 (75.5%)Developed symptoms after quarantine
Developed symptoms >48h after quarantined35 (11.9%)24 (8.1%)
16 (7.9%)10 (5.0%)
51 (20.3%)34 (6.8%)
Day of symptom onset = last day at school 46 (15.6%) 69 (3.4%) 115 (23.1%)Person at school ≥2 days after symptom onset
Median no. of days (range)34 (11.5%)
3 (2-9)35 (17.3%)
3 (2-7)69 (13.9%)
3 (2-9)Person at school while test results pending 10 (3.4%) 3 (1.5%) 13 (2.6%)Person at school while infectious
YesPossible/Unknown
125 (42.4%)113 (38.3%)
143 (70.8%)29 (14.4%)
268 (53.9%)142 (28.6%)
Person reported close contacts at schoolYesNoUnclear if close contact occurred/unknown
50 (16.9%)225 (76.0%)
20 (6.8%)
37 (18.3%)142 (70.3%)23 (11.4%)
87 (17.5%)367 (73.8%)
43 (8.7%)Breakdown of close contacts at school reported by person
StudentsStaffStudents and StaffUnknown
N=5032 (64%)7 (14.0%)9 (18.0%)2 (4.0%)
N=379 (24.3%)21 (10.4%)7 (18.9%)0 (0.0%)
N=8741 (47.1%)28 (32.2%)16 (18.4%)
2 (2.3%)
Frequency (%) unless otherwise noted Students(N=295)
Staff(N=202)
Total(N=497)
Subject developed symptoms after 7-day quarantine period 3 (1.0%) 3 (1.5%) 6 (1.2%)Subject with ≥1 relative or household member among cases 175 (59%) 34 (16.8%) 209 (42.1%)Source of infection
Infection acquired outside of schoolInfection likely acquired outside of schoolPossible but unlikely school acquisitionPossible school acquisitionLikely school acquisition Unknown but no evidence of school acquisition
75 (25.4%)61 (20.7%)
5 (1.7%)2 (0.7%)4 (1.3%)
148 (50.2%)
42 (20.8%)15 (7.4%)1 (0.5%)1 (0.5%)1 (0.5%)
142 (70.3%)
117 (23.5%)76 (15.3%)
6 (1.2%)3 (0.6%)5 (1.0%)
290 (58.4%)Nature of out-of-school exposures
Close contact exposure within household Close contact w/ co-worker/schoolmate outside of schoolExtra-curricular sport-related close contact exposureOther non-household close contactOther cases w/in household at same time as subject Close contact w/ non-school/non-household positive cases Unknown but school source excluded
Nature of in-school exposuresLikely acquisition after close contact w/ symptomatic studentLikely acquisition after close contact w/ symptomatic teacher*
School cluster 1School cluster 2
N=110 (0%)
2 (18.2%)2 (18.2%)7 (63.6%)
N=31 (33.3%)
0 (0%)1 (33.3%) 1 (33.3%)
N=141 (7.1%)
2 (14.3%)3 (21.4%)8 (57.1%)
*One teacher developed symptoms after returning to school following a shortened quarantine period of 7 days w/ a negative PCR test at day 5
School Cluster 1Symptomatic teacher who floated between classrooms & had close contact w/ 2 asymptomatic 2 year olds from 2 different classrooms; teacher also had asymptomatic household members w/ positive tests at same time; index case/directionality of transmission could not be definitively established
5 classrooms with positive cases
Classroom 1(1&2 shared recess)
1 student(first case reported;
household contact)
Classroom 2(1&2 shared recess)
1 Student(likely from school?)
Classroom 3*
(3&4 shared recess)
5 students w/ close contact
outside of school (possible but
unlikely classroom transmission)
2 students(developed
symptoms after positive cases;
likely from school)
3 students reported over
break (possibly related to school)
Teacher #1 attended school/outside of school party when
symptomatic
Classroom 4(3&4 shared recess)
Teacher #2
1 student reported over break; close contact w/ student in classroom 3 w/
reported symptoms over break but no
test
Classroom 5
2 students (reported over break; outside
sources identified)
Close contact outside of school
*Close contact occurred among all students in classroom 3
School Cluster 2
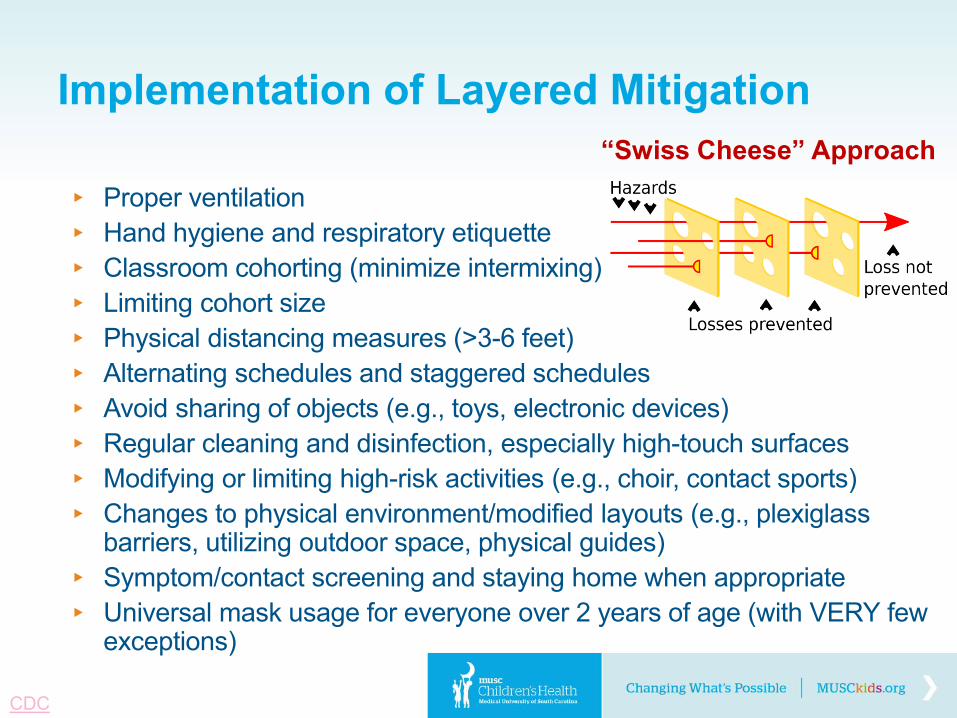
Implementation of Layered Mitigation
▸ Proper ventilation▸ Hand hygiene and respiratory etiquette▸ Classroom cohorting (minimize intermixing)▸ Limiting cohort size▸ Physical distancing measures (>3-6 feet)▸ Alternating schedules and staggered schedules▸ Avoid sharing of objects (e.g., toys, electronic devices)▸ Regular cleaning and disinfection, especially high-touch surfaces▸ Modifying or limiting high-risk activities (e.g., choir, contact sports)▸ Changes to physical environment/modified layouts (e.g., plexiglass
barriers, utilizing outdoor space, physical guides)▸ Symptom/contact screening and staying home when appropriate▸ Universal mask usage for everyone over 2 years of age (with VERY few
▸ Cut, constructed and installed more than 60 miles of plexiglass dividers and 3,400 sneeze guards for teachers and guidance counselors.
▸ Optimized indoor air quality by: review of all fresh air equipment and maximizing fresh air intake; extending system run times before and after school; and upgrading filters.
▸ Installed automatic drinking water bottle fillers in all schools.▸ Purchased personal water bottles for all children.▸ Acquired fogging machines for all schools and fogging 20% of each
facility with a hydrogen peroxide product every week night.▸ Disinfecting all school bathrooms and school buses twice per day.▸ Disinfecting common touch surfaces in schools throughout the day.▸ Developed and distributed pocket action cards with cleaning tasks for
both day and night janitor crews.▸ Installed COVID-19 awareness signage at all school entrances and
common bathrooms.▸ Posted safe COVID-19 capacities for all elevators and bathrooms.
The Power of Masks
▸ 6 feet = distance most large respiratory droplets travel from sneeze/cough travel before settling on to surfaces (based on pre-COVID studies)
▸ More recent simulationshows 12 feet (tracer droplets suspended midair for 3 min)
▸ Droplet spread decreased significantly w/ face coverings: ▸ Bandana = 3 ft., 7 in. ▸ Folded cotton handkerchief
= 1 ft., 3 in. ▸ Stitched quilted cotton
mask = 2.5 in. ▸ Cone-style mask = 8 in.
Masks decrease spread of virus-containing respiratory DROPLETS,the primary mode of SARS-CoV-2 transmission.
▸ Children suffer when not attending in-person school.
▸ Transmission in schools is low for both students and staff when appropriate risk mitigation strategies are in place.
▸ Activities outside of school are the main driver of transmission & cases in schools.
▸ On-going community education and “buy in” needed to alter behaviors outside of school.
Dr. Carolyn Styles: As infectious disease pediatricians, name the one point that you would have us remain cognizant of (during this pandemic) as we advocate for our students, teachers, staff, and community?
Ms. Michelle Goodwin-Calwile: There seems to be a correlation between the community spread being high and the student, faculties and staffs contracting it. Why should we not go back to Attendance Plan 0 or 2? The students, faculties and staffs live in the communities and if they are partaking in activities that are risky, isn't that risky for our district spread?
Mr. Derek Lewis:It seems that much of the evidence supports the idea that children are less likely to spread the virus than adults. Much of the precautions we put in place were to help protect the staff who were uncomfortable returning to confined spaces. Educators are currently in Vaccine group 1B, which could ensure staff receive the vaccine this spring. If those vaccinations go well, would you support lifting of any of the following COVID protocols for Fall 2021?• Class Size reductions: Classes are currently 'at capacity" based on number of people who can be socially
distanced in a room • Mask/Plexiglass usage: Every classroom (2nd to 12th) has plexiglass dividers, and all students are required to
wear masks • Bus capacity: Currently capped at numbers that allow for 6ft social distancing on buses • Restrictions on performances: band, theater groups have audience restrictions that make public performances
difficult • Student gatherings: Currently assemblies, students eating in cafeterias is prohibited unless where 6ft social
distancing occurs
How well will the vaccine protect staff and does it offer protection against any spread as well?
Mr. Charles Saylors:
Ms. Sarah Dulin: I'd like to hear what the reason is that students are not transmitting Covid to each other or their teachers. If it were only masks and plexiglass, then we would expect to see similar numbers of transmission across all school age groups, and this doesn't appear to be the case per all the studies we've seen recently. And if the younger a person is (or the smaller their physical self is) then are they less likely to transmit? If this could be true, then are we doing more harm than good by keeping them masked all day behind plexiglass?
Ms. Angie Mosley: I understand that you are both pediatric infectious disease doctors, but with depression and anxiety hitting peak levels in our student populations, my larger concern is with mental health. Many in our community have expressed concerns that the excessive masking of children and setting up plexiglass barriers that prevent natural developmental stages from occurring is far more harmful to children long term … an example in our adolescent student population would be relationship building/bonding stage that's critical during that 9th grade transition year (studies have actually shown that there’s a direct correlation to 9th grade experiences and drop-out/graduation rates). How much emphasis should be placed on mental health during our decision making and who do you believe we should be collaborating with to ensure that we are providing developmentally appropriate environments that keep our children emotionally and mentally healthy?