Spinal Conditioning for Athletes With Lumbar Spondylolysis and Spondylolisthesis Erin Nau, ATC, 1 William J. Hanney, PT, DPT, ATC, CSCS, 1 and Morey J. Kolber, PT, PhD, CSCS 2 1 University of Central Florida, Orlando, Florida; 2 Nova Southeastern University, Fort Lauderdale, Florida SUMMARY LOW BACK PAIN IS A COMMON CONDITION IN ATHLETIC POPULATIONS. PARTICIPATION IN ATHLETICS HAS BEEN LINKED TO SPECIFIC ANATOMICAL CHANGES TO THE LUMBER SPINE (SPONDYLOLYSIS AND SPONDYLOLISTHESIS). PRACTICAL GUIDELINES FOR STRENGTH AND CONDITIONING PROFESSIONALS SHOULD RECOGNIZE THE BIOMECHANICAL STRESSES ASSOCIATED WITH ATHLETIC PARTICIPATION IN THIS POPULATION. PROGRAM MODIFICATIONS CAN BE MADE IN ATHLETES WITH SPONDYLOLITIC DISORDERS. CONDITIONING ROUTINES SHOULD EMPHASIZE SPINAL STABILIZATION AND SPORT-SPECIFIC FLEXIBILITY. THIS ARTICLE MAKES RECOMMENDA- TIONS FOR ATHLETES WITH SPONDYLOLITIC DISORDERS THAT SHOULD ALLOW PARTICIPATION IN LUMBAR CONDITIONING WHILE PROTECTING THE BACK FROM UNDUE STRESS. INTRODUCTION L ow back pain (LBP) is a preva- lent condition in the athletic population (10,19). Among athletes, LBP accounts for up to 40% of documented injuries (2,9,25). Al- though LBP is not the most frequent disorder encountered among the ath- letic population, it is one of the most challenging to treat, perhaps as a result of training demands. Although the etiology of LBP is multifactorial, epi- demiological data have suggested that athletes are more prone to degenera- tive and spondylolytic related injuries when compared with the general population (2,5,8,10,13,16,26). The purpose of this article is to present a brief overview of spondylolitic dis- orders and to provide a comprehensive spinal-conditioning program designed to achieve the dual benefit of improved spinal conditioning while protecting the spondylolitic region from undue stress. Spondylolitic disorders among athletes typically comprise the diagnosis of either a spondylolysis or a spondylolis- thesis. The term spondylolisthesis comes from the derivative of ‘‘spondy- lo,’’ which means vertebrae, and ‘‘lis- thesis’’ which means forward slippage (34). Therefore, a spondylolisthesis is essentially a forward slippage of one vertebra on another (Figure 1) (10,34). Spondylolisthesis often are attributed to degenerative changes and/or a de- fect at the vertebrae (3,35). A spondy- lolysis occurs when there is a fracture, found in a region of the vertebrae called the pars interarticularis (Figure 2) (25). A spondylolysis disorder does not imply a forward slippage of the verte- bra (33). Spondylolysis defects may be unilateral or bilateral and may progress to a spondylolisthesis over time (13). Researchers have indicated that ath- letes with a unilateral spondylolysis may be at risk for developing a fracture of the contralateral pars interarticularis (27). For the purpose of clarity, we will refer to spondylolysis and spondylolis- thesis conditions collectively as spon- dylolitic disorders. Where necessary, a distinction will be made. EPIDEMIOLOGY AND PRECIPITATING FACTORS As stated previously, athletes are more prone to degenerative and spondylo- lytic-related injuries when compared with the general population (2,5,8,10, 13,16,26). Spondylolitic disorders are primary causes of back pain among gymnasts, divers, weightlifters, wres- tlers, and football players, with a re- ported prevalence of up to 40% (2,15). Within individual sports, the great- est incidence is found in gymnasts, weightlifters, rowing, and those who participate in throwing sports (14). KEY WORDS: low back pain; spondylosis; spondylol- ysis; spondylolisthesis; athletic injury Ó National Strength and Conditioning Association Strength and Conditioning Journal | www.nsca-lift.org 43
Transcript
Spinal Conditioningfor Athletes With LumbarSpondylolysisand SpondylolisthesisErin Nau, ATC,1 William J. Hanney, PT, DPT, ATC, CSCS,1 and Morey J. Kolber, PT, PhD, CSCS2
1University of Central Florida, Orlando, Florida; 2Nova Southeastern University,Fort Lauderdale, Florida
S U M M A R Y
LOW BACK PAIN IS A COMMON
CONDITION IN ATHLETIC
POPULATIONS. PARTICIPATION IN
ATHLETICS HAS BEEN LINKED TO
SPECIFIC ANATOMICAL CHANGES
TO THE LUMBER SPINE
(SPONDYLOLYSIS AND
SPONDYLOLISTHESIS). PRACTICAL
GUIDELINES FOR STRENGTH AND
CONDITIONING PROFESSIONALS
SHOULD RECOGNIZE THE
BIOMECHANICAL STRESSES
ASSOCIATED WITH ATHLETIC
PARTICIPATION IN THIS
POPULATION. PROGRAM
MODIFICATIONS CAN BE MADE IN
ATHLETES WITH SPONDYLOLITIC
DISORDERS. CONDITIONING
ROUTINES SHOULD EMPHASIZE
SPINAL STABILIZATION AND
SPORT-SPECIFIC FLEXIBILITY. THIS
ARTICLE MAKES RECOMMENDA-
TIONS FOR ATHLETES WITH
SPONDYLOLITIC DISORDERS THAT
SHOULD ALLOW PARTICIPATION IN
LUMBAR CONDITIONING WHILE
PROTECTING THE BACK FROM
UNDUE STRESS.
INTRODUCTION
Low back pain (LBP) is a preva-lent condition in the athleticpopulation (10,19). Among
athletes, LBP accounts for up to 40%of documented injuries (2,9,25). Al-though LBP is not the most frequentdisorder encountered among the ath-letic population, it is one of the mostchallenging to treat, perhaps as a resultof training demands. Although theetiology of LBP is multifactorial, epi-demiological data have suggested thatathletes are more prone to degenera-tive and spondylolytic related injurieswhen compared with the generalpopulation (2,5,8,10,13,16,26). Thepurpose of this article is to presenta brief overview of spondylolitic dis-orders and to provide a comprehensivespinal-conditioning program designedto achieve the dual benefit of improvedspinal conditioning while protectingthe spondylolitic region from unduestress.
Spondylolitic disorders among athletestypically comprise the diagnosis ofeither a spondylolysis or a spondylolis-thesis. The term spondylolisthesiscomes from the derivative of ‘‘spondy-lo,’’ which means vertebrae, and ‘‘lis-thesis’’ which means forward slippage(34). Therefore, a spondylolisthesis isessentially a forward slippage of onevertebra on another (Figure 1) (10,34).Spondylolisthesis often are attributedto degenerative changes and/or a de-fect at the vertebrae (3,35). A spondy-lolysis occurs when there is a fracture,found in a region of the vertebrae called
the pars interarticularis (Figure 2) (25).A spondylolysis disorder does notimply a forward slippage of the verte-bra (33). Spondylolysis defects may beunilateral or bilateral and may progressto a spondylolisthesis over time (13).Researchers have indicated that ath-letes with a unilateral spondylolysismay be at risk for developing a fractureof the contralateral pars interarticularis(27). For the purpose of clarity, we willrefer to spondylolysis and spondylolis-thesis conditions collectively as spon-dylolitic disorders. Where necessary,a distinction will be made.
EPIDEMIOLOGY ANDPRECIPITATING FACTORS
As stated previously, athletes are moreprone to degenerative and spondylo-lytic-related injuries when comparedwith the general population (2,5,8,10,13,16,26). Spondylolitic disorders areprimary causes of back pain amonggymnasts, divers, weightlifters, wres-tlers, and football players, with a re-ported prevalence of up to 40% (2,15).Within individual sports, the great-est incidence is found in gymnasts,weightlifters, rowing, and those whoparticipate in throwing sports (14).
KEY WORDS :
low back pain; spondylosis; spondylol-ysis; spondylolisthesis; athletic injury
� National Strength and Conditioning Association Strength and Conditioning Journal | www.nsca-lift.org 43
An explanation for gymnasts having ahigh incidence lies in the demandsplaced on his or her spine while inpositions that load the pars interarticu-laris. It has been estimated the spine of a
gymnast is loaded approximately 4times the amount in that of the generalfemale population (15,23). Conse-quently, the incidence of spondyloliticdisorders has been approximated at
11% among female competitive gym-nasts (15,23). Gender also plays a role,as spondylolitic disorders are 4 timesmore common in women than men(7). Age may also be a factor to con-sider as vertebral slippage is shown tooccur more drastically during an ado-lescent growth spurt, and if the athletewas asymptomatic to begin with, theproblem potential becomes all themore accentuated (29). It has beensuggested, although not universallyagreed upon, that in the skeletallyimmature athlete, spondylolitic disor-ders should be considered until diag-nostic testing suggests otherwise (33).
DIAGNOSIS
Athletes with spondylolitic disordersmay present with a wide range of signsand symptoms, making clinical diag-nosis elusive. Although a detailed dis-cussion of the diagnostic signs andsymptoms is beyond the scope of thisarticle, a brief overview is necessary.The athlete’s history leading to injuryis often inclusive of repetitive loadinginto extension, flexion, twisting, or acombination of movements (4). Plainfilm radiographs possess the diagnosticutility to identify spondylolytic disor-ders using standard views; however,more sensitive imaging modalities,such as a technetium bone scan, maybe required in certain cases (25). Incases of a spondylolisthesis, radio-graphs are able to provide informationon the severity of the ‘‘slip.’’ A slip ofless than 50% is considered mild andoften managed conservatively, whereasslips of greater than 50% are oftenreferred for a surgical consult (25).Ultimately, the diagnosis of a spondy-lolytic disorder will be made bya physician who has interpreted theradiological and clinical presentation.Moreover, individuals diagnosed withspondylolytic disorders must be clearedby their physician prior to the initiationof any exercise programs.
ANATOMY
Although our intent is not to providean exhaustive discussion of the lumbaranatomy, a brief review is necessary
Spinal Conditioning for Lumbar Spondylolysisand Spondylolisthesis
to establish a clear understanding ofthe information presented. The lum-bar spine consists of 5 vertebrae, andbetween each lies a disk providingcushion between the vertebrae whenloaded. The joints of the lumbar spineare referred to as facet joints (Figure 3).A facet is a small smooth area ona bone that creates an articulationbetween neighboring vertebrae (34).Each vertebra contains 2 superior and2 inferior articular facets providinga connection to the adjoining vertebraabove and below (25). Between thesuperior and inferior facet lies a small,very thin area of primarily corticalbone called the pars interarticulariswhich is illustrated in Figures 1 and 2(34). The pars interarticularis is theweakest area in this unit, and in youngpeople it is particularly thin and injurysusceptible (5). Because of its fragilenature, the pars interarticularis issometimes not capable of withstandingexcessive or repetitive forces; thus,it fractures (25). Defects or fracturesleading to spondylolitic disorders willinvariably originate at the pars inter-articularis. Although this disruptioncan occur at any vertebral level, it
most commonly occurs at the L5 seg-ment (30,33). A fracture of the parsinterarticularis (spondylolysis) may, inresponse to stress progress to a spon-dylolisthesis without causative modifi-cations and appropriate interventions.
PATHOGENESIS
Although the etiology of LBP ismultifactorial and the precise cause ofspondylolitic disorders is unknown, themechanisms precipitating these disor-ders among the athletic population aredescribed in literature (6,13). It hasbeen suggested that repetitive hyper-extension movements (extension of thelumbar spine beyond the anatomicallimits) place stress through the parsinterarticularis and over time may leadto a spondylolysis (9). This notion maylie in the association between thefrequently extended and loaded posi-tion for which gymnasts, dancers,divers, football lineman and weight-lifters assume and their increasedprevalence of spondylolitic conditions.It has been purported that accumula-tive extension at the end-range ofmobility, combined with the powerand force of jumps, landings, and
dismounts, can cause microtrauma tothe pars-interarticularis area, leading tospondylolitic disorders. Although theextended position has been establishedas both a precipitating and provocatingfactor for spondylolitic disorders (1,16,17,28), one must exercise caution whenasserting that extension should abso-lutely be avoided in the presence ofa forward slippage. Researchers havepresented conflicting findings regard-ing the effect of extension on someindividuals with spondylolitic disorders(12,17,31). In particular, extension hasshown to be efficacious in someindividuals with spondylolitic disorders(31). Nevertheless, one should exercisecaution with lumbar extension in theathletic population as it is a factorthat places stress on the pars inter-articularis and may lead to worseningof the condition.
Finally, spondylolitic disorders result-ing from a defect or fracture of the parsinterarticularis frequently present withspinal instability (24), thus interven-tions designed to increase spinal sta-bility may be efficacious (26). Studieshave reported that hypermobility (ex-cessive) and/or instability occurs at thespine levels afflicted with a spondylo-litic disorder (20,24). It is therefore thegoal of treatment to directly strengthenthe muscles that insert on the affectedvertebrae in order to increase stability.As a result spinal stabilization toachieve ‘‘core stability’’ is a key com-ponent in the training of these indi-viduals. Researchers have establishedthat exercise training of the stabilizingmuscles of the trunk reduces pain anddisability in those with spondyloliticdisorders (26). Despite compellingresearch spinal stabilization exercisesare often a neglected portion of strengthand conditioning regimens (26,32).
SPINAL CONDITIONING
In our experience, athletes often focuson the large muscles groups responsi-ble for performance and tend to neglectthe muscles responsible for spinalstabilization. It is essential that athleteswith spondylolitic disorders work bothto strengthen the stabilizing muscula-ture and spend necessary time onFigure 3. Facet joints of the lumbar spine. (� Primal Pictures Ltd.)
Strength and Conditioning Journal | www.nsca-lift.org 45
specific flexibility exercises in additionto performance training. After medicalclearance to begin activity, a compre-hensive spinal conditioning that con-siders evidence-based interventionswill serve a key role in both preventionand progression of the disorder. More-over, addressing more common im-pairments in flexibility and strength ofthe stabilizing musculature will posi-tively affect performance that may beotherwise affected as a result of suchimpairments. As with any exerciseprogram the strength and conditioningor rehabilitation professional mustmonitor the individuals exercise toler-ance to avoid an exacerbation ofsymptoms.
FLEXIBILITY
Flexibility is an important componentof spinal conditioning programs. Asecondary finding of hamstring andparaspinal muscle tightness may befound among the spondylolitic popu-lation perhaps in an effort to providestabilization (8). A direct association,however, between tightness of theparaspinals and hamstrings has notbeen established. It should also benoted that not all athletes will presentwith traditional hamstring and para-spinal tightness as the length of themuscle is relative to the athlete, and therequirements of the sport. Some sports,such as gymnastics and dance, willrequire a great deal of flexibilitytherefore the athletes sport and pre-vious flexibility level must be consid-ered, or the hamstring spasm may beoverlooked, and perceived as normal.
Flexibility of the hip flexor, hamstring,rectus femoris, and tensor fascia latamusculature has been recognized as anintegral component of the spinalconditioning program in those withspondylolitic disorders (7,9,22). It hasbeen postulated in the literature thattightness of the rectus femoris mayincrease the lumbar lordosis due todirect effects on pelvic alignment (21).Rectus femoris tightness may alterpelvic positioning thus increasingstrain on the already unstable verte-brae. With proper flexibility exercisesthese muscles can maintain their
necessary flexibility for athletic partic-ipation and minimize undue stress onthe spine from aberrant tightness. Thefollowing flexibility exercises are rec-ommended as part of a comprehensivefitness routine in the athlete with aspondylolitic disorder. Static stretchingis advocated for a duration of 30 sec-onds for 3 repetitions.
FLEXIBILITY EXERCISES
Hip flexor stretch.Hip flexor stretch-ing is illustrated in Figure 4. The hipflexor stretch requires the athlete toassume a kneeling lunge position withthe extremity to be stretched extendedback. Rotate the pelvis backward byisometrically contracting the glutealmuscles in order to maintain a neutralspinal position. It is very important tomaintain this neutral pelvic position inorder to eliminate hyperextension ofthe spine. Once in position, furtherbend the front leg until a stretch is feltin the hip flexors (front of thigh) of theback leg.
Supine hamstring stretch. The su-pine hamstring stretch (Figure 5) re-quires the athlete to begin in a supineposition with a towel wrapped aroundone foot and the ends in both hands.While keeping the leg straight, theathlete uses the towel to gently pull the
leg toward the upper body untila stretch is felt in the hamstrings. Ifthe athlete reports LBP, the non-stretched leg may be bent to reducepressure on the spine.
Rectus femoris stretch. The rectusfemoris stretch (Figure 6) requires theathlete to assume a prone position(lying flat on the stomach) with oneknee bent and a pillow under theirwaist to maintain a neutral spine.While maintaining a neutral spine,the athlete is instructed to grab theankle of the bent knee with one handand pull toward the gluteal area untila stretch is felt. As flexibility increasesa rolled towel can be placed under thedistal thigh to create an increasedstretch. Athletes reporting discomfortduring this procedure may simplytighten their gluteal muscles to reduceloading of the spine and increase theefficiency of the stretch by posteriorlyrotating the pelvis (21).
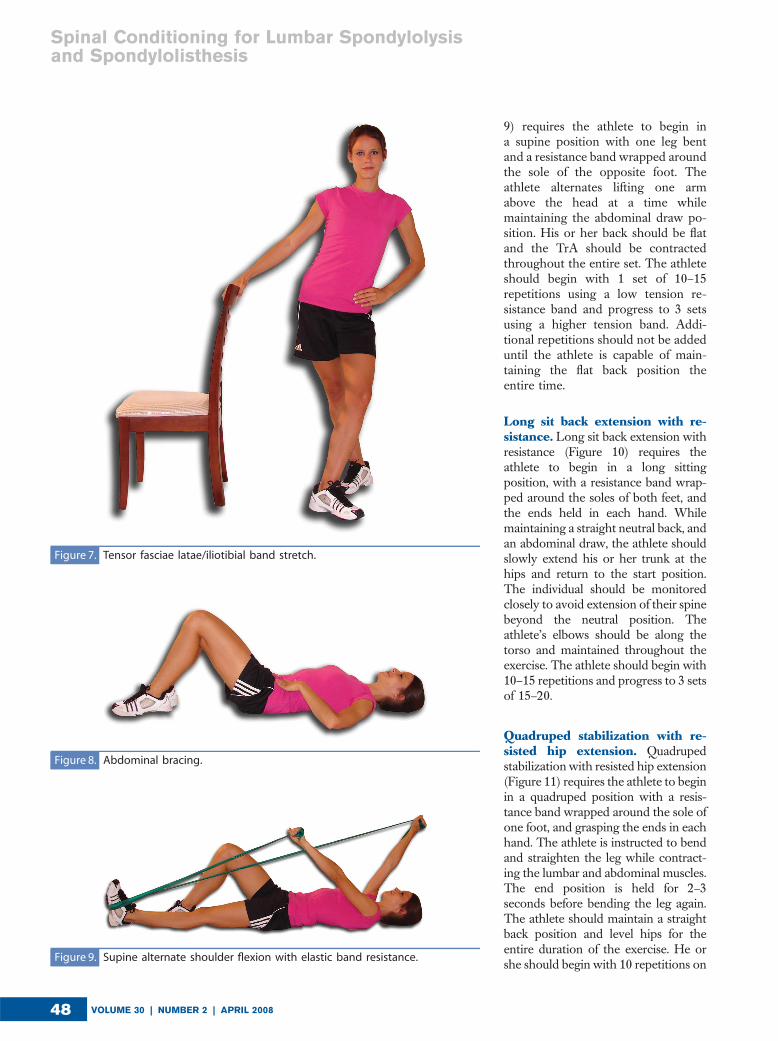
Iliotibial band stretch. The iliotibialband or tensor fasciae latae stretch(Figure 7) requires the athlete to standwith one hand placed along a wall/-chair for support and place the leg tobe stretched closest to the wall/chair.The athlete is then instructed toexternally rotate the stretching leg
Figure 4. Hip flexor stretch.
VOLUME 30 | NUMBER 2 | APRIL 200846
Spinal Conditioning for Lumbar Spondylolysisand Spondylolisthesis
and position it behind the opposite legand, once in position, bend the frontleg into a slight lunge position and shiftthe back hip toward the wall. Thismove will require a slight side bendaway from the wall.
DYNAMIC STABILIZATION
Several muscles play a roll in dynamicspinal movements and stabilization.Among these are the transversus ab-dominis (TrA), paraspinals, internal andexternal obliques, rectus abdominus,and the multifidus (32). Strengtheningof these muscles will provide support toa pre-existing spondylolitic disorder bylifting the spine and maintaining neutralpelvic alignment thus transferring theforce and thereby decreasing theamount of load to the area (32).Furthermore, the intrinsic muscles suchas the TrA and multifidus have localstabilization function necessary to pre-vent excessive movement at regions ofinstability or hypermobility.
The TrA and lumbar multifidus havea particular function in aiding withsegmental motion, and providing spi-nal stabilization (32). These 2 groups ofmuscles work together by co-contract-ing to provide a balancing effect to thespine (26). The TrA is the first muscleactivated in any trunk movement, so itbecomes an important stabilizationmechanism (11). Studies show thatactivation of both the TrA and multi-fidus is delayed in those with low backpain (11,26).
The multifidus is the deepest spinalmuscle, and because of its directinsertion to each vertebra, it is of theutmost importance to the spondyloliticpatient (6). Of the back extensor mus-cles, the lumbar multifidus can providethe greatest control to the vertebralsegment, and can potentially functionto stiffen, or bind the lumbar spine(18,26). This muscle may atrophy overtime without direct efforts to facilitateits function after an episode of low back
pain. Electromyography studies ofvertebral irregularities such as that ofa spondylolisthesis with spinal insta-bility indicated abnormal and de-creased activity of the multifidusdirectly at the unstable segment (18).When functioning properly, this mus-cle will pull the vertebra backwardsand has the ability to stabilize thespondylolisthesis directly (18). Further-more, research has shown that aftercompleting an exercise program whichspecifically strengthens the multifidusparticipants with spondylolytic disor-ders will demonstrate a significantdecrease in pain and disability (18).The following stabilization exercisesare recommended as part of a compre-hensive fitness routine in the athletewith a spondylolitic disorder. Theseexercises may be performed daily duringthe initial stages of the disorder toimprove neural activation such asrate coding and motor unit recruitment.Once in the advanced stage may beperformed 2–3 times a weeks as neces-sary to increase muscular performance.
DYNAMIC STABILIZATIONEXERCISES
Abdominal bracing. Abdominalbracing (Figure 8) requires the athleteto begin in a supine position, with legsbent. The athlete should attempt todraw the stomach up toward thesternum, and back toward the floor,holding the position for 3 seconds, andthen returning to start position. Thismotion is referred to as an abdominaldraw. This exercise comprises a verysmall movement that may requirea great deal of concentration toappropriately target that TrA muscu-lature. Beginning with 1 set of 10–15repetitions and progressing toward 3sets of 10–15 repetitions is recommen-ded. This abdominal bracing techniquewill be carried over to all advancingexercises, and the athlete should not beprogressed to further exercises until theform of this exercise is mastered.
Strength and Conditioning Journal | www.nsca-lift.org 47
9) requires the athlete to begin ina supine position with one leg bentand a resistance band wrapped aroundthe sole of the opposite foot. Theathlete alternates lifting one armabove the head at a time whilemaintaining the abdominal draw po-sition. His or her back should be flatand the TrA should be contractedthroughout the entire set. The athleteshould begin with 1 set of 10–15repetitions using a low tension re-sistance band and progress to 3 setsusing a higher tension band. Addi-tional repetitions should not be addeduntil the athlete is capable of main-taining the flat back position theentire time.
Long sit back extension with re-sistance. Long sit back extension withresistance (Figure 10) requires theathlete to begin in a long sittingposition, with a resistance band wrap-ped around the soles of both feet, andthe ends held in each hand. Whilemaintaining a straight neutral back, andan abdominal draw, the athlete shouldslowly extend his or her trunk at thehips and return to the start position.The individual should be monitoredclosely to avoid extension of their spinebeyond the neutral position. Theathlete’s elbows should be along thetorso and maintained throughout theexercise. The athlete should begin with10–15 repetitions and progress to 3 setsof 15–20.
Quadruped stabilization with re-sisted hip extension. Quadrupedstabilization with resisted hip extension(Figure 11) requires the athlete to beginin a quadruped position with a resis-tance band wrapped around the sole ofone foot, and grasping the ends in eachhand. The athlete is instructed to bendand straighten the leg while contract-ing the lumbar and abdominal muscles.The end position is held for 2–3seconds before bending the leg again.The athlete should maintain a straightback position and level hips for theentire duration of the exercise. He orshe should begin with 10 repetitions on
Figure 7. Tensor fasciae latae/iliotibial band stretch.
Figure 8. Abdominal bracing.
Figure 9. Supine alternate shoulder flexion with elastic band resistance.
VOLUME 30 | NUMBER 2 | APRIL 200848
Spinal Conditioning for Lumbar Spondylolysisand Spondylolisthesis
each leg using a low tension resistanceband and progress to 3 sets of 15repetitions on each leg is advised.
Standing lunge extension with re-sistance. Standing lunge extensionwith resistance (Figure 12) requires theathlete to begin in a deep standing lungeposition with a resistance band under thefront foot and the ends held in each handat the level of the chest. The athlete isfirst asked to simultaneously draw in andcontract the abdominals to stabilize thespine in a neutral position. The trunk isthen slowly extended backward to theneutral position and then returned to theoriginal start position. The extensionmotion is relative as it occurs froma flexed to neutral position. At no pointduring the exercise should the athlete’s
back hyperextend in the patient witha confirmed spondylolysis. He or sheshould begin with one set of 10– 15repetitions and progress to 3 sets of 15–20 repetitions.
Stability ball leg lifts. Stability ballleg lifts (Figure 13) require the athleteto begin in a bridge position with thestability ball centered on the upperback and head, and feet planted on theground. With an abdominal draw, anda straight-neutral back position main-tained, the athlete should extend theknee to the level of trunk whileremaining centered on the ball. He orshe should then hold the lifted legposition for 3 seconds and repeat withthe opposite leg. The focus should beupward in order to maintain a neutral
cervical spine. He or she should beginwith one set of 10–15 repetitions oneach leg and progress to 3 sets.
Stability ball pikes. Stability ballpikes (Figure 14) require the athleteto begin in a supine position, with theirarms extended over the head anda stability ball held tightly betweenthe lower legs. The stability ball is thenlifted to meet the arms (creating a Vposition), transferred to the arms, andthe body is returned to start position.The movement is then repeated trans-ferring the ball back to the feet andreturned to the original starting posi-tion. The exercise can be made easierby bending the legs and holding theball at knee level. The abdominal drawshould be maintained throughout theexercise, and a straight back main-tained. He or she should begin withone set of 10 repetitions and progressto 3 sets of 15–20 repetitions.
Stability ball back bridge. Thestability ball back bridge exercise(Figure 15) requires the athlete tobegin in a supine position, with theirarms flat on the floor and feet andlower legs positioned on top of thestability ball. While maintaining anabdominal draw, the athlete lifts thestomach to the level of the legs(creating a straight body position),holds for 3 seconds, and returns tothe start position. It is important tomake sure the start and end position ofeach lift is performed while maintain-ing the abdominal draw and a neutralspine. Beginning with one set of 10–15repetitions, and progressing to 3 sets of15–20 is advised. The difficulty levelmay be increased by crossing the armsover the chest or performing a singleleg version.
SPORT-SPECIFIC CONSIDERATIONS
Athletic demands on the spine varydepending upon the sport, position,and level of competition. Each sportmay have unique biomechanics thatcan affect the efficacy of a spinalconditioning program and future pre-vention efforts. Certain sports such as
Figure 10. Long sit back extension with resistance.
Figure 11. Quadruped stabilization with resisted hip extension.
Strength and Conditioning Journal | www.nsca-lift.org 49
gymnastics, dance, cheerleading andweight-lifting will require activity mod-ifications due to their particularly highdemands on the spine.
Athletic movements that require load-ing of the spine while in the hyper-extended position can be detrimentalto the spine, particularly in patientsdiagnosed with a spondylolysis. In gym-nastics, for example, this movementoccurs frequently during performance
of such skills as that of back walkovers,back handsprings, giants on unevenbars, or improper dismount landings.All of the skills, whether performedcorrectly or not, can place the athleteinto a forceful hyperextension. Thegymnast should therefore be educatedin proper, non extended dismountlanding in order to illuminate anyunnecessary vertebral strain. On cer-tain skills, such as giants on uneven
bars, a hyperextended position mayindicate improper technique. Essen-tially undue stress on the spine fromathletic positioning or movements canbe minimized by retraining the athleteto perform the skill with modifications.The spinal conditioning exercises pre-sented are designed to have broadapplicability and will serve useful for alllevels of athletic participation. Further-more, with appropriate stabilizationand flexibility the athlete may benefitfrom improved performance, particu-larly if impairments were present.
CONCLUSION
Recognizing the need for activity mod-ifications and implementation of effica-cious strength and conditioning routinesis essential for the athlete with a spon-dylolitic disorder. Studies show that thelonger symptoms are present beforeintervention takes place, the lesserchance there is for optimum recovery(1). Early intervention that respects theunderlying anatomical irregularities andpresenting impairments is therefore ofprimary importance in maintainingparticipation in athletics.
GENERAL GUIDELINES FORSPINAL CONDITIONING
� Athletes with a spondylolitic disor-der must receive appropriate medi-cal clearance before participation.
� Athletes should begin spinal condi-tioning slowly, focusing on flexibilityexercises, and basic static stabi-lization exercises. Incorporate moreadvanced stabilization exercises ina graduated manner avoiding painand/or compromised performance.
� Any exercise that increases painshould be avoided. If this situationoccurs, the exercises should bereverted back to the less advancedstage of the regimen.
� The performance of quality exercisesis far more important than quantity.Many exercises will require a greatdeal of focus while learning in orderto master correct form and thisshould not be mistaken for slowprogress.
� Athletes should be encouraged tohold their spines in a comfortableposition during the exercises.
Figure 12. Standing lunge extension with resistance.
Figure 13. Stability ball leg lifts.
VOLUME 30 | NUMBER 2 | APRIL 200850
Spinal Conditioning for Lumbar Spondylolysisand Spondylolisthesis
Aberrant postures that increase painor asymmetrically load the spinemay place additional stress to thearea, and is an indication that theathlete has been progressed torapidly.
� The flexibility and stabilization ex-ercises recommended in thisarticle should be continued through-out the year and not reduced to theathlete’s periodized model. Mainte-nance is the key to preventingworsening, progression of the slip-page, or any future spondyloliticoccurrences at neighboring vertebrallevels.j
Erin Nau is an athletictrainer and coach at HarborCity Gymnastics and a physi-cal therapy student at theUniversity of Central Florida.
William J. Hanney is aninstructor at the University ofCentral Florida in the Phys-ical Therapy Program.
Morey J. Kolber is anAssistant Professor in thePhysical Therapy Departmentat Nova SoutheasternUniversity.
REFERENCES1. Blanda, J, Bethem, D, Moats, W, and Lew,
M. Defects of pars interarticularis in
athletes: A protocol for nonoperative
treatment. J Spinal Disord 6: 406–411,
1993.
2. Calhoon, G and Fry, AC. Injury rates and
profiles of elite competitive weightlifters.
J Athl Train 34: 232–238, 1999.
3. Cinotti, G, Postacchini, F, Fassari, F, and
Urso, S. Predisposing factors in
degenerative spondylolisthesis. A
radiographic and CT study. Int Orthop 21:
337–342, 1997.
4. Commandre, FA, Taillan, B, Gagnerie, F,
Zakarian H, Lescourgues M, and Fourre JM.
Spondylolysis and spondylolisthesis in
young athletes. J Sports Med Phys Fitness
28: 104–107, 1988.
5. Congeni, J, Mcculloch, J, and Swanson, K.
Lumbar spondylolysis. A study of natural
progression in athletes. Am J Sports Med
25: 248–253, 1997.
6. Cyron, BM and Hutton, WC. The fatigue
strength of the lumbar neural arch in
spondylolysis. J Bone Joint Surg Br 60-B:
234–238, 1978.
7. Dutton, M. Orthopaedic Examination,
Evaluation, and Intervention. Pittsburgh,
Pa: McGraw-Hill, 2004. pp. 1217–1218.
8. Garry, JP and McShane, J. Lumbar
spondylolysis in adolescent athletes. J Fam
Pract 47: 145–149, 1998.
9. Harvey, J and Tanner, S. Low back pain in
young athletes. A practical approach.
Sports Med 12: 394–406, 1991.
10. Herman, J. Spondylolysis and
spondylolisthesis in the child and
adolescent athlete. Orthop Clin North Am
34: 461–467, 2003.
11. Hodges, PW and Richardson, CA.
Inefficient muscular stabilization of the
lumbar spine associated with low back
pain. A motor control evaluation of
transversus abdominis. Spine 21:
2640–2650, 1996.
12. Huang, RP, Bohlman, HH, Thompson, GH,
and Poe-Kochert, C. Predictive value of
pelvic incidence in progression of
spondylolisthesis. Spine 28: 2381–2385,
2003.
13. Ikata, T, Miyake, R, Katoh, S, Morita, T, and
Murase, M. Pathogenesis of sports-related
spondylolisthesis in adolescents.
Radiographic and magnetic resonance
imaging study. Am J Sports Med 24:
94–98 1996.
14. Iwamoto, J, Takeda, T, and Wakano, K.
Returning athletes with severe low back
pain and spondylolysis to original sporting
activities with conservative treatment.
Scand J Med Sci Sports 14: 346–351,
2004.
15. Jackson, DW. Low back pain in young
athletes: evaluation of stress reaction and
discogenic problems. Am J Sports Med
7: 364–366, 1979.
16. Jackson, DW, Wiltse, LL, Dingeman, RD,
and Hayes, M. Stress reactions involving
the pars interarticularis in young athletes.
Am J Sports Med 9: 304–312, 1981.
17. Jackson, RP, Phipps, T, Hales, C, and
Surber, J. Pelvic Lordosis and Alignment in
Spondylolisthesis. Spine 28: 151–160,
2003.
18. Johnson, J. The Multifidus Back Pain
Solution. Oakland: New Harbinger
Publications, Inc., 2002. pp. 19–27.
19. Keene, JS. Low back pain in the athlete.
From spondylogenic injury during
Figure 15. Stability ball back bridge.
Figure 14. Stability ball pikes.
Strength and Conditioning Journal | www.nsca-lift.org 51
recreation or competition. Postgrad Med
74: 209–12, 213–217, 1983.
20. Keessen, W, During, J, Beeker, TW,
Goudfrooij, H, and Crowe, A. Recordings
of the movement at the intervertebral
segment L5–S1: A technique for the
determination of the movement in the L5–
S1 spinal segment by using three specified
postural positions. Spine 9: 83–90, 1984.
21. Kolber, MJ and Fiebert, IM. Addressing
flexibility of the rectus femoris in the athlete
with low back pain. Strength Cond J 27:
66–77, 2005.
22. Lonstein, JE. Spondylolisthesis in children.
Cause, natural history, and management.
Spine 24: 2640–2648, 1999.
23. McCarroll, JR, Miller, JM, and Ritter, MA.
Lumbar spondylolysis and
spondylolisthesis in college football
players. A prospective study. Am J Sports
Med 14: 404–406, 1986.
24. McGregor, AH, Cattermole, HR, and
Hughes, SP. Global spinal motion in
subjects with lumbar spondylolysis and
spondylolisthesis: Does the grade or type
of slip affect spinal motion? Spine 26:
282–286, 2001.
25. Motley, G, Nyland, J, Jacobs, J, and
Caborn, DN. The pars interarticularis stress
reaction, spondylolysis, and
spondylolisthesis progression. J Athl Train
33: 351–358, 1998.
26. O’Sullivan, PB, Phyty, GD, Twomey, LT,
and Allison, GT. Evaluation of specific
stabilizing exercise in the treatment of
chronic low back pain with radiologic
diagnosis of spondylolysis or
spondylolisthesis. Spine 22: 2959–67,
1997.
27. Sairyo, K, Katoh, S, Sasa, T, Yasui, N,
Goel, VK, Vadapalli, S, Masuda, A, Biyani,
A, and Ebrahaim, N. Athletes with unilateral
spondylolysis are at risk of stress fracture at
the contralateral pedicle and pars
interarticularis: A clinical and
biomechanical study. Am J Sports Med 33:
583–590, 2005.
28. Saraste, H, Nilsson, B, Brostrom, LA, and
Aparisi, T. Relationship between
radiological and clinical variables in
spondylolysis. Int Orthop 8: 163–174,
1984.
29. Seitsalo, S, Osterman, K, Hyvarinen, H,
Tallroth, K, Schlenzka, D, and Poussa, M.
Progression of spondylolisthesis in
children and adolescents. A long-term
follow-up of 272 patients. Spine 16:
417–421, 1991.
30. Sonne-Holm, S, Jacobsen, S, Rovsing, HC,
Monrad, H, and Gebuhr, P. Lumbar
spondylolysis: A life long dynamic
condition? A cross sectional survey of
4,151 adults. Eur Spine J 16: 821–828,
2007.
31. Spratt, KF, Weinstein, JN, Lehmann, TR,
Woody, J, and Sayre, H. Efficacy of
flexion and extension treatments
incorporating braces for low-back pain
patients with retrodisplacement,
spondylolisthesis or normal sagittal
translation. Spine 18: 1839–1849,
1993.
32. Standaert, C. Rehabilitation of the athlete
with low back pain. Curr Sports Med Rep
3: 35–40, 2004.
33. Stinson, JT. Spondylolysis and
spondylolisthesis in the athlete. Clin Sports
Med 12: 517–528, 1993.
34. Venes, D, ed. Taber’s Cyclopedic Medical
Dictionary (20th ed). Philadelphia, Pa:
F.A Davis Company, 2005.
35. Wiltse, LL and Jackson, DW. Treatment of
spondylolisthesis and spondylolysis in
children. Clin Orthop Relat Res 92–100,
1976.
VOLUME 30 | NUMBER 2 | APRIL 200852
Spinal Conditioning for Lumbar Spondylolysisand Spondylolisthesis