What are Leopold's maneuvers? Leopold's maneuvers are four specific steps in palpating the uterus through the abdomen in order to determine the lie and presentation of the fetus. In summary the steps are : Step 1. The top of the uterus (fundus) is felt (palpated) to establish which end of the fetus (fetal pole) is in the upper part of the uterus. If either the head or breech (buttocks) of the fetus are in the fundus then the fetus is in vertical lie. Otherwise the fetus is most likely in transverse lie. Step 2. Firm pressure is applied to the sides of the abdomen to establish the location of the spine and extremities (small parts). Step 3. Using the thumb and fingers of one hand the lower abdomen is grasped just above the pubic symphysis to establish if the presenting part is engaged. If not engaged a movable body part will be felt. The presenting part is the part of the fetus that is felt to be in closest proximity to the birth canal. Step 4. Facing the maternal feet the tips of the fingers of each hand are used to apply deep pressure in the direction of the axis of the pelvic outlet. If the head presents, one hand is
Transcript
What are Leopold's maneuvers?
Leopold's maneuvers are four specific steps in palpating the uterus through the abdomen in order to determine the lie and presentation of the fetus. In summary the steps are :
Step 1. The top of the uterus (fundus) is felt (palpated) to establish which end of the fetus (fetal pole) is in the upper part of the uterus. If either the head or breech (buttocks) of the fetus are in the fundus then the fetus is in vertical lie. Otherwise the fetus is most likely in transverse lie.
Step 2. Firm pressure is applied to the sides of the abdomen to establish the location of the spine and extremities (small parts).
Step 3. Using the thumb and fingers of one hand the lower abdomen is grasped just above the pubic symphysis to establish if the presenting part is engaged. If not engaged a movable body part will be felt. The presenting part is the part of the fetus that is felt to be in closest proximity to the birth canal.
Step 4. Facing the maternal feet the tips of the fingers of each hand are used to apply deep pressure in the direction of the axis of the pelvic outlet. If the head presents, one hand is arrested sooner than the other by a rounded body (the cephalic prominence) while the other hand descends deeply into the pelvis. If the cephalic prominence is on the same side as the small parts, then the fetus is in vertex presentation. If the cephalic prominence is on the same side as the back , then the head is extended and the fetus is in face presentation.
******Labels: Maternal and Child Leopold's maneuver- are a systematic method of observation and palpation to determine
fetal position, presentation, lie and attitude which helps in predicting course of labor. - woman who emptied her bladder should lie in supine position with her knees flexed slightly so abdomen is relaxed.- Warm hands to avoid contraction of abdominal muscles.- gentle but firm touch
Keen observation of abdomen should give data about
1. longest diameter in appearance2. location of apparent fetal movement
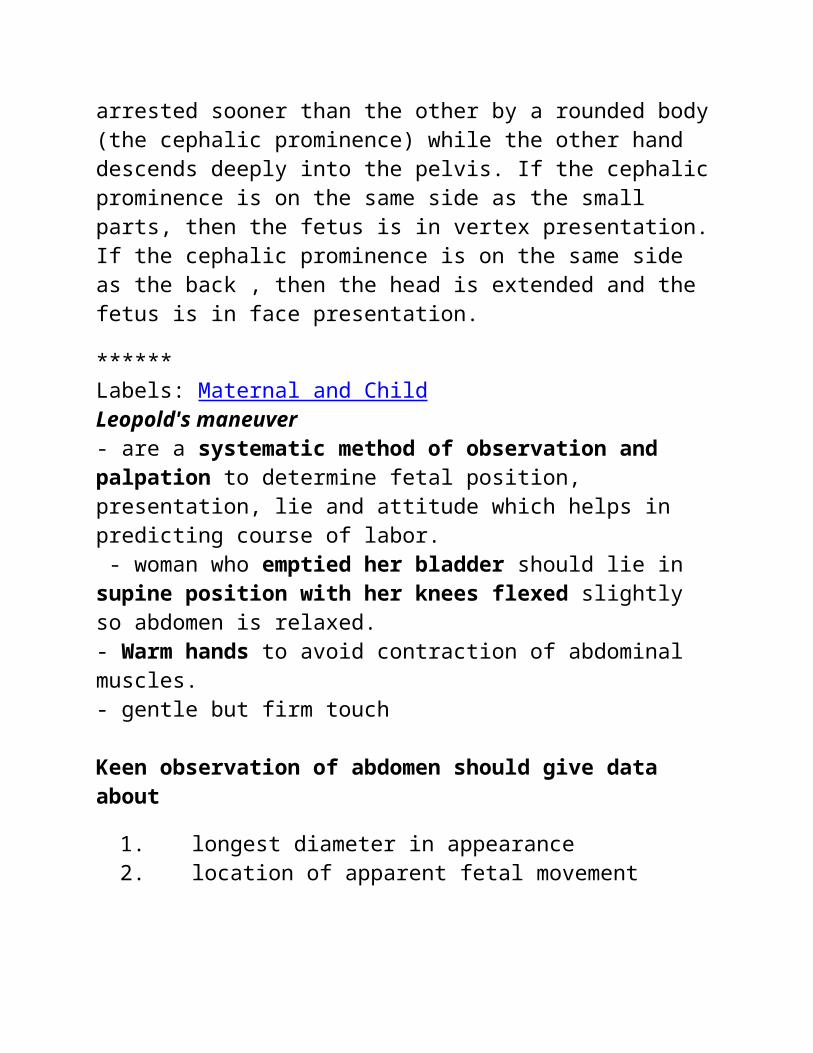
The four Leopold's maneuver are:
1. First Maneuver- to determine presenting part at the fundus- head is more firm, hard and round that moves independently of the body
- Breech is less well defined that moves only in conjunction with the body
2. Second Maneuver- to determine fetal back- one hand: will feel smooth, hard resistant surface (the back)- the opposite side, a number of angular nodulation (knees and elbows of fetus)
3. Third Maneuver- to determine position and mobility of presenting part by grasping the lower portion of the abdomen (just above the symphysis pubis).- if the presenting part moves upward so the examiner's hand can be pressed together, then presenting part is not engaged
4. Fourth Maneuver- to determine fetal descent- fingers are pressed in both side of the uterus approximately 2 inches above the inguinal ligaments, then press upward and inward.- the fingers of the hand that do not meet obstruction palpates the fetal neck, as the fingers of the other hand meet an obstruction above the ligaments palpates the fetal brow.- Good attitude if brow correspond to the side (2nd maneuver) that contained the elbows and knees.- Poor attitude if examining fingers will meet an obstruction on the same side as fetal back (hyperextended head).- also palpates infant's anteroposterior position. If brow is very easily palpated, fetus is at posterior position (occiput pointing towards
woman's back).
Leopold's maneuvers
From Wikipedia, the free encyclopediaJump to: navigation, search
Leopold's Maneuvers
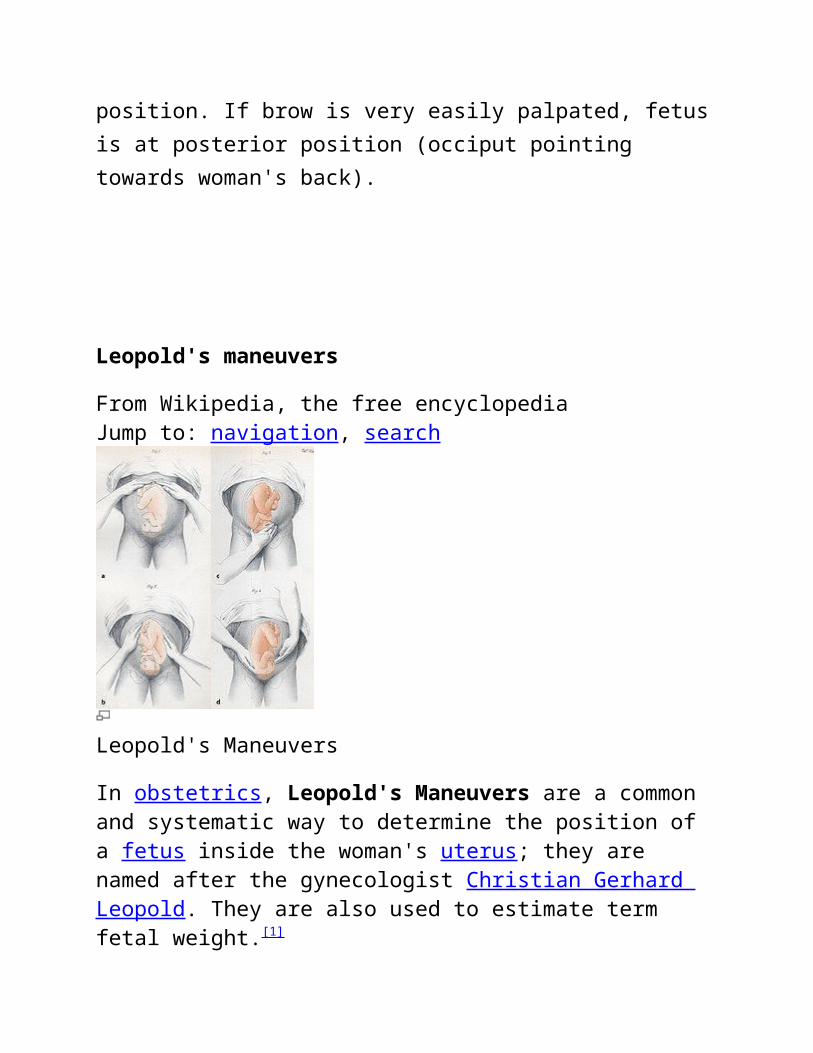
In obstetrics, Leopold's Maneuvers are a common and systematic way to determine the position of a fetus inside the woman's uterus; they are named after the gynecologist Christian Gerhard Leopold. They are also used to estimate term fetal weight.[1]
The maneuvers consist of four distinct actions, each helping to determine the position of the fetus. The maneuvers are important because they help determine the position and presentation of the fetus, which in conjunction with correct assessment of the shape of the
maternal pelvis can indicate whether the delivery is going to be complicated, or whether a Cesarean section is necessary.
The examiner's skill and practice in performing the maneuvers are the primary factor in whether the fetal lie is correctly ascertained, and so the maneuvers are not truly diagnostic. Actual position can only be determined by ultrasound performed by a competent technician or physician.
Performing the maneuvers
Leopold's Maneuvers are difficult to perform on obese women and women who have polyhydramnios. The palpation can sometimes be uncomfortable for the woman if care is not taken to ensure she is relaxed and adequately positioned. To aid in this, the health care provider should first ensure that the woman has recently emptied her bladder. If she has not, she may need to have a straight urinary catheter inserted to empty it if she is unable to micturate herself. The woman should lie on her back with her shoulders raised slightly on a pillow and her knees drawn up a little. Her abdomen should be uncovered, and most women appreciate it if the individual performing the maneuver warms their hands prior to palpation.
First maneuver: Fundal Grip
While facing the woman, palpate the woman's upper abdomen with both hands. A professional can often determine the size, consistency, shape, and mobility of the form that is felt. The fetal head is hard, firm, round, and moves independently of the trunk while the buttocks feel softer, are symmetric, and the shoulders and limbs have small bony processes; unlike the head, they move with the trunk.
After the upper abdomen has been palpated and the form that is found is identified, the individual performing the maneuver attempts to determine the location of the fetal back. Still facing the woman, the health care provider palpates the abdomen with gentle but also deep pressure using the palm of the hands. First the right hand remains steady on one side of the abdomen while the left hand explores the right side of the woman's uterus. This is then repeated using the opposite side and hands. The fetal back will feel firm and smooth while fetal extremities (arms, legs, etc.) should feel like small irregularities and protrusions. The fetal back, once determined, should connect with the form found in the upper abdomen and also a mass in the maternal inlet, lower abdomen.
Third maneuver: Pawlick's Grip
In the third maneuver the health care provider attempts to determine what fetal part is lying above the inlet, or lower abdomen.[2] The individual performing the maneuver first grasps the lower portion of the abdomen just above the pubic symphysis with the thumb and fingers of the right hand. This maneuver should yield the opposite information and validate the findings of the first maneuver. If the woman enters labor, this is the part which will most likely come first in a vaginal birth. If it is the head and is not actively engaged in the birthing process, it may be gently pushed back and forth. The Pawlick's Grip, although still used by some obstetricians, is not recommended as it is more uncomfortable for the woman. Instead, a two-handed approach is favored by placing the fingers of both hands laterally on either side of the presenting part.
The last maneuver requires that the health care provider face the woman's feet, as he or she will attempt to locate the fetus' brow. The fingers of both hands are moved gently down the sides of the uterus toward the pubis. The side where there is resistance to the descent of the fingers toward the pubis is greatest is where the brow is located. If the head of the fetus is well-flexed, it should be on the opposite side from the fetal back. If the fetal head is extended though, the occiput is instead felt and is located on the same side as the back.
Cautions
Leopold's maneuvers are intended to be performed by health care professionals, as they have received the training and instruction in how to perform them. That said, as long as care taken not to roughly or excessively disturb the fetus, there is no real reason it cannot be performed at home as an informational exercise. It is important to note that all findings are not truly diagnostic, and as such ultrasound is required to conclusively determine the fetal position.
When to do a bed bath
If the person you're caring for is sedentary or on bed rest, the best approach to bathing may be a bed bath. It sounds simple enough -- you
basically wipe her clean with a wet cloth. But in reality, giving a good bed bath is a bit tricky.
Giving a bed bath requires you to wash the person's front, sides, and back, not to mention crevasses and folds -- while she's lying down. Depending on her condition, merely touching or moving her body may cause discomfort. If she weighs a lot, it can be strenuous for you. Not to mention the challenge of keeping the mattress dry.
Don't worry! People have been giving bed baths for centuries: They're a standard of hospital and home healthcare. All this practice has produced practical techniques that make giving a bed bath much easier.
Beginning the bed bath
By Kate Rauch, Caring.com senior editor
Before you begin a bed bath, make sure you have a huge pile of clean, dry bath towels and clean, dry washcloths, at least a dozen of each. Also, there should be a table or shelf within easy reach to hold a water container and supplies. A wheeled cart -- such as a basic TV or kitchen cart -- is ideal. Finally, adjust the room temperature so it's toasty warm.
Lay thick bath towels under the person from head to toe. These are to absorb water, protecting the bedding and mattress. You might want to also use a waterproof sheet under the cloth sheet to ensure that the mattress stays dry.
Undress her but keep her under a blanket or large towel. This covering stays on during the whole bath for both warmth and privacy.
Fill two large bowls with warm water, one for washing and one for rinsing. Put the bowls within easy reach.
Stand at her shoulder. You'll be washing down one side of her body, section by section, lifting the cover away only as much as
necessary. It helps to tilt her up on the side a little, facing away from you, so you can reach underneath her body. Start with her shoulder, then her arm and hand, including the fingers. Move to the side of her torso and hips, then wash her thigh, lower leg, foot, and toes.
The washing itself is straightforward: Soap then rinse, using a different washcloth for each. Rinse sufficiently to get all the soap off. (Soap residue is drying to the skin, and elderly skin is prone to dryness.) Refill the water bowls as needed. Make sure the temperature of the water stays warm to the touch. When washing, stroke in the direction of the heart, toward the torso, to help blood circulation.
After a section is rinsed, pat it dry with a towel and lay the cover down as quickly as you can for warmth.
After you've finished one side of the body, start at the other shoulder and work down. Afterward, move to the head and neck. This is a great time to shampoo, which is easiest with a soft plastic bed bath shampoo bowl, sold at hospital or medical supply stores. The shampoo bowl can be placed right on the mattress, and all you need to do is lift or edge your family member's head into it. (Don't leave her unattended for even a few seconds when a bowl of water is near her head.) If you don't have a shampoo bowl, lay dry towels under her head and do the best you can with your bowls of water, soaping and rinsing. Consider using baby shampoo, which rinses out easily.
Save the privates for last. Do these quickly, lifting the cover only as much as necessary to soap and rinse. With a man, you'll need to wash under his testicles. With a woman, wash the labia; there's no need for a deep cleaning. To reach the rear, tilt the person's body to the side as much as you need to or can. Or you can bend her knees and reach under from the front.
When you're done, the person's entire body should remain covered with the blanket or towel. If it's damp, exchange it for a
dry one. You may need to add another layer. Slowly pull the wet towels from under her body.
Take a deep breath and relax before dressing her. Giving a bed bath is a bona fide workout, and you've earned a break.
Alternative bed bath techniques: through-the-towel, the chair bath, and more
By Kate Rauch, Caring.com senior editor In addition to the standard bed bath described above, there are
variations on the theme. You may very well discover your own useful adaptations as you gain experience.
One alternative method of giving a bed bath is to wash and rinse through a towel, never touching the person's skin. Using a washcloth, you soap and rinse through the layer of towel, which acts as a sort of second skin. This is one way around modesty concerns, which can be extremely uncomfortable for you and her.
This technique for giving a bed bath minimizes the need to rub or stroke. Instead, you pat or gently massage the wet towel that covers a section of her body. When you're done with that section, take off the wet towel and quickly replace it with a dry one or a blanket to avoid a post-bathing chill.
Another twist on giving a bed bath: Keep several washcloths in large plastic zip-close bags of warm water, one clean and the other soapy, and take them out as needed. This eliminates the need to rinse washcloths in bowls of water. As soon as a washcloth gets dirty, stop using it and get a clean one from the bag. Check the bags regularly to make sure the water remains warm.
Then there's the chair bath. If the person you're caring for feels comfortable sitting up in a chair, this may be the best position for bathing. The routine is pretty much the same as for a bed bath.
Of course, you'll need to protect the chair from water. Vinyl-covered chairs can work, or you can get creative with plastic garbage bags or a tarp.
Tips for giving a bed bath to overweight or sensitive people By Kate Rauch, Caring.com senior editor If the person you're bathing is resistant to a bath or particularly
sensitive to water, try using no-rinse soaps and shampoos. You rub them in and towel them off -- the dirt comes off in the toweling. No-rinse bathing products can be a huge help, but they do leave a residue, so you'll need to rinse with water every now and then.
Giving a good bed bath requires a lot of movement on your part -- lifting, holding, and tilting the person's body. If she's overweight or heavy, a bath may be a two-person job. The same is true if she's easily irritated or feels pain when touched.
"You may need other people to help, like a relative or home health aide," says Jennifer Serafin, a registered nurse and geriatric nurse practitioner at the Jewish Home for the Aged in San Francisco.
You can hire a home heath worker to assist you, enlist relatives or friends, or try a combination of the two. Hiring a professional for a one-time crash course on giving a bed bath could also be extremely helpful.
You won't need to give a full-body bed bath daily. Ask the medical team, but in most cases a full bath once or twice a week should be sufficient.
It's recommended that you clean the private areas and under any skin folds daily. You'll need to wash under the testicles, breasts, armpits, and tummy rolls, which are more of an issue with overweight people.
Once-a-day washing can be done efficiently with a wipe or damp washcloth. If the person in your care uses the toilet, take this opportunity for a quick cleaning.
Definition of Last menstrual period
Last menstrual period: By convention, pregnancies are dated in weeks starting from the first day of a woman's last menstrual period (LMP). If her menstrual periods are regular and ovulation occurs on day 14 of her cycle, conception takes place about 2 weeks after her LMP. A woman is therefore considered to be 6 weeks pregnant 2 weeks after her first missed period.
A woman's obstetric date is different from the embryologic date (the age of the embryo). The obstetric date is about 2 weeks longer than the embryologic date.
Pregnancy Due DateHow Pregnancy Due Date is Calculated
From conception vs last menstrual period
The average duration of pregnancy is 38 weeks (266 days) from conception. Predicting the pregnancy due date based on conception is the most accurate way to calculate one's due date, but usually the date of conception is not known. Therefore, the due date is generally calculated from the first day of the last menstrual period (LMP). In this case, 2 weeks are added to the calculation giving a total of 40 weeks (280 days). This is based on the assumption that ovulation/conception occurs on cycle day 14 in the "average" 28 day menstrual cycle.
From ovulation
Calculating the due date from LMP is subject to error since ovulation varies in its timing from the onset of menstruation among different women and from cycle to cycle. Many of Dr. Berger's tubal reversal
patients know their date of ovulation from using an ovulation predictor kit (OPK) or keeping a basal body temperature (BBT) chart. Calculating the pregnancy due date from ovulation is more accurate than from the last menstrual period.
Last Menstrual Period Dating
How to Calculate Pregnancy Due Date
The first day of the last menstrual period is used to initially determine the age of a pregnancy.
Pregnancy is a time of joyful waiting and excitement. Expectant parents want to know when to expect their new little bundle of joy so they can prepare mentally and physically for childbirth and prepare a safe home for the baby. Obstetricians want to know the due date so they can monitor fetal growth, which can be an indicator of problems with the pregnancy. The last menstrual period is used to determine the approximate age of the pregnancy. Ultrasound is often used to confirm the due date and to monitor growth.
Last Menstrual Period (LMP)
The age of a pregnancy is determined by the first day of the last menstrual period. Gestational age includes the weeks of menstruation, follicular development, and ovulation, which is when conception occurs. For this reason, gestational age can also be referred to as
menstrual age. It should be about two weeks longer than the fetal age, which is the actual age of the fetus.
The following is an example of last menstrual period dating and how it compares to fetal age:
Last menstrual period: January 1
On February 12 (six weeks after the last menstrual period), the following would be true:
Gestational age / Menstrual age: 6 weeks
Fetal age: 4 weeks
Gestational age is commonly used while fetal age is not.
Menstrual Cycle Variations and Pregnancy Due Date
The pregnancy due date can be easy to calculate because pregnancy calculators are widely available on the Internet. Many of these are combined with ovulation calculators. For many women, however, these calculators are not accurate.
Most women do not have a 28-day menstrual cycle. Some have periods every three weeks while others may have them as far apart as five weeks. Ovulation occurs at different times for these women. Generally, those with shorter menstrual cycles will be given a gestational age that is farther along than their LMP suggests, and those with longer menstrual cycles will be given a gestational age that is earlier than their LMP suggests. This is because ovulation occurs at different times for those with shorter and longer cycles. Some women have menstrual cycles that vary in length, so an ultrasound may be necessary for calculating the pregnancy due date.
Ultrasound
When the first day of the last menstrual period is unknown, or the lengths of the menstrual cycles are varied, ultrasound will most likely be used to determine the age of the pregnancy. First trimester ultrasound is done to acquire a crown-rump length. The ultrasound machine determines the due date and gestational age based upon the crown-rump length. Second trimester ultrasound is used to acquire measurements of the head, abdomen, and femur bone to determine an approximate due date, gestational age, and weight. This method becomes less accurate as the pregnancy progresses.
****
Naegele's rule
From Wikipedia, the free encyclopedia
Jump to: navigation, search
Naegele's Rule is a standard way of calculating the due date for a pregnancy. The rule estimates the expected date of delivery (EDD) by adding one year, subtracting three months, and adding seven days to the first day of a woman's last menstrual period (LMP). The result is approximately 280 days (40 weeks) from the LMP.
History
Naegele's Rule is named after Franz Karl Naegele (1778–1851), the German obstetrician who devised the rule. Naegele was born July 12, 1778, in Düsseldorf, Germany. In 1806 Naegele became ordinary professor and director of the lying-in hospital in Heidelberg. His
"Lehrbuch der Geburtshilfe," published in 1830 for midwives, enjoyed a successful 14 editions.
The rule estimates the expected date of delivery (EDD) (also called EDC, for estimated date of confinement) from the first day of the woman's LMP by adding 1 year, subtracting three months and adding seven days to that date. The result is approximately 280 days (40 weeks) from the LMP.
Example:LMP = 8 May 2009
+1 year = 8 May 2010
-3 months = 8 February 2010
+7 days = 15 February 2010
280 days past LMP is found by checking the day of the week of the LMP and adjusting the calculated date to land on the same day of the week. Using the example above, 8 May 2009 is a Tuesday. The calculated date (15 February) is a Friday; adjusting to the closest Tuesday produces 12 February, which is exactly 280 days past 8 May. The calculation method does not always result in a 280 days because not all calendar months are the same length, it does not account for leap years.
Parikh's Formula is a calculation method that considers considers cycle duration. Naegele's Rule assumes an average cycle length of 28 days, which is not true for everyone. EDD is calculated using Parikh's Formula by adding 9 months to LMP, subtracting 21 days, then adding duration of previous cycles.[1]
In modern practice, calculators, reference cards, or sliding wheel calculators are used to add 280 days to LMP.
LMP may not be the best date to use as the basis of a due date calculation, but it remains popular because few women know exactly what day they ovulate or conceive a pregnancy, and because no algorithm can predict the exact day that spontaneous labor will occur no matter what considerations are taken into account.
Average gestation of 40 weeks
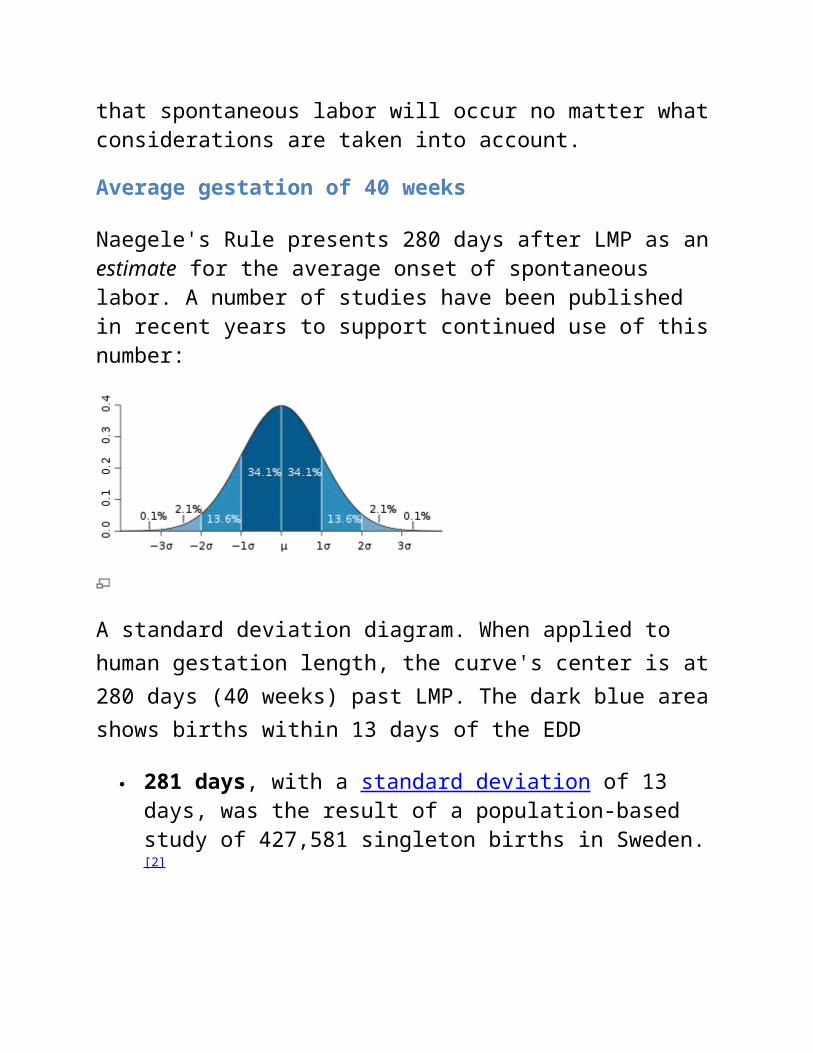
Naegele's Rule presents 280 days after LMP as an estimate for the average onset of spontaneous labor. A number of studies have been published in recent years to support continued use of this number:
A standard deviation diagram. When applied to human gestation length, the curve's center is at 280 days (40 weeks) past LMP. The dark blue area shows births within 13 days of the EDD
281 days, with a standard deviation of 13 days, was the result of a population-based study of 427,581 singleton births in Sweden.[2]
281 days for first-time mothers and 280 days for all others were the medians found by a 1995 American study of 1,970 spontaneous births. Standard deviation was between 7–9 days.[3][4]
282 days was recommended for cases where LMP is the only known factor in a study of 17,450 patients combining LMP and ultrasound measurement techniques.[5]
A median of 288 days (274 days from the date of ovulation) for first time mothers and 283 days (269 days from the date of ovulation) for mothers with at least one previous pregnancy was found by a 1990 study of white, private-care patients with uncomplicated pregnancies and spontaneous labor. The authors suggest that excluding pregnancies involving complications (that often lead to pre-term deliveries) accounts for the longer time periods.[6]
Given the fact that these gestation lengths are only estimates of an average, it is helpful to consider gestation time as a range of dates rather than a single "due date". The median found by Naegele's Rule is merely a guideline for the day at which half of all births occur earlier, and half of all births occur later. Births rarely occur on a due date, but they are clustered around due dates.[7]
For instance, a standard deviation of 13 days means that 90% of babies will be born within three weeks of their EDD, and 21% will be born within 3 days of it. Only 4% of births will occur on the EDD, but this is similar to most other days around the EDD, in fact each day within a week of the EDD has a 3-4% probability of being the day that birth will occur. However, any given day two weeks away from the EDD has a less than 2% chance of being the day that birth will occur.
Ultrasound confirmation of gestational age
Since the 1970s ultrasound scans have allowed measurement of the size of developing embryos directly and so allow for an estimation of gestation age. Ultrasound dating is most accurate if undertaken in the first trimester (first 12 weeks of pregnancy) with a 95% error margin of
6 days. Scans performed in the second trimester have an error margin of 8 days and those in the third trimester a margin of 2 weeks.
Most obstetric departments in Australia, Canada, United Kingdom, and United States use a combination of LMP and ultrasound based estimates for the EDD using either 10-day or 7-day rules, so that if LMP dates and ultrasonographic dates are in agreement within 7 (or 10) days, then the LMP dates are accepted.
The Estimated Date of Confinement (EDC) is a term describing the estimated delivery date for a pregnant woman.[1] Normal pregnancies last between 37 and 42 weeks.[2]
It is a calculated date (i.e., an estimation), determined by counting forward 280 days (40 weeks) from the first day of the woman's last menstrual period.[3]
Origins of the Term
The term confinement is a traditional term referring to the period of pregnancy whereby a woman would be confined to bed (in an effort to reduce risk of premature delivery). Except in threatened pregnancies (for example, in pre-eclampsia), this is no longer a part of antenatal care.
es·ti·mat·ed date of confinement ( s t -m t d)n. Abbr. EDCThe date at which an infant is expected to be born, calculated from the date of the last menstrual period. Also called due date.
es·ti·mat·ed date of confinement ( s t -m t d)n. Abbr. EDCThe date at which an infant is expected to be born, calculated from the date of the last menstrual period. Also called due date.
Patient discussion about estimated date of confinement.
Q. How many women actually give birth on their EDD (expected delivery date)? I am pregnant and my EDD is January 22nd. I was wondering what are the chances I will give birth on that day exactly?
A. If it's your first pregnancy, you probably will give birth after your EDD, as first pregnancies tend to be longer. Your EDD is after a full 40 weeks of pregnancy. It is most common to give birth between 38- 42 weeks of pregnancy.
????????
Q. How many women actually give birth on their EDD (expected delivery date)? I am pregnant and my EDD is January 22nd. I was wondering what are the chances I will give birth on that day exactly?A1 If it's your first pregnancy, you probably will give birth after your
EDD, as first pregnancies tend to be longer. Your EDD is after a full 40 weeks of pregnancy. It is most common to give birth between 38- 42 weeks of pregnancy.
A2 Most people are used to being assigned a EDD. Your expected delivery date (EDD) is 40 weeks from the first day of your last menstrual period (LMP). If you birth on your EDD, your baby is actually only 38 weeks old - that's because your menstrual period and ovulation are counted as the first 2 weeks of pregnancy. It's important to remember that your due date is only an estimate - most babies are born between 38 and 42 weeks and only a small percentage of women actually birth on their due date.
http://www.naturalattachment.com/BirthMonth.html Hope this helps.
A3 Your EDD is 40 weeks from the first day of your last menstrual period (LMP). If you deliver on your EDD, your baby is actually only about 38 weeks old — that's because your egg didn't become fertilized until about 2 weeks after the start of your last menstrual period. It's important to remember that your due date is only an estimate — most babies are born between 38 and 42 weeks from the first day of their mom’s LMP and only a small percentage of women actually deliver on their due date.
Diabetes mellitus type 2
Diabetes mellitus type 2 – formerly non-insulin-dependent diabetes mellitus (NIDDM) or adult-onset diabetes – is a metabolic disorder that is characterized by high blood glucose in the context of insulin resistance and relative insulin deficiency.[2] This is in contrast to diabetes mellitus type 1 in which there is an absolute insulin deficiency due to destruction of islet cells in the pancreas.[3] The classic symptoms are excess thirst, frequent urination, and constant hunger. Type 2 diabetes makes up about 90% of cases of diabetes with the other 10% due primarily to diabetes mellitus type 1 and gestational diabetes. Obesity is thought to be the primary cause of type 2 diabetes in people who are genetically predisposed to the disease.
Type 2 diabetes is initially managed by increasing exercise and dietary modification. If blood glucose levels are not adequately lowered by these measures, medications such as metformin or insulin may be needed. In those on insulin there is typically the requirement to routinely check blood sugar levels.
Rates of diabetes have increased markedly over the last 50 years in parallel with obesity. As of 2010 there are approximately 285 million people with the disease compared to around 30 million in 1985. Long-term complications from high blood sugar can include heart disease, strokes, diabetic retinopathy where eyesight is affected, kidney failure which may require dialysis, and poor circulation of limbs leading to amputations. The acute complication of ketoacidosis, a feature of type 1 diabetes, is uncommon.[4] However, nonketotic hyperosmolar coma may occur.
Signs and symptoms
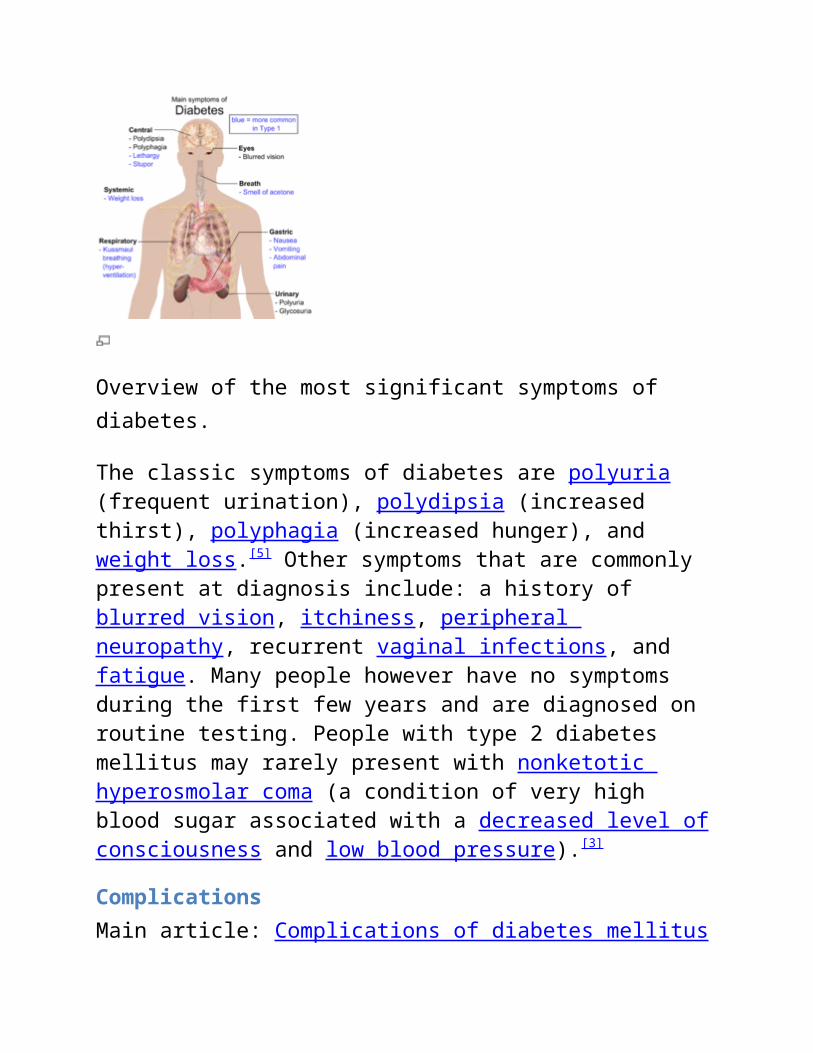
Overview of the most significant symptoms of diabetes.
The classic symptoms of diabetes are polyuria (frequent urination), polydipsia (increased thirst), polyphagia (increased hunger), and weight loss.[5] Other symptoms that are commonly present at diagnosis include: a history of blurred vision, itchiness, peripheral neuropathy, recurrent vaginal infections, and fatigue. Many people however have no symptoms during the first few years and are diagnosed on routine testing. People with type 2 diabetes mellitus may rarely present with nonketotic hyperosmolar coma (a condition of very high blood sugar
associated with a decreased level of consciousness and low blood pressure).[3]
ComplicationsMain article: Complications of diabetes mellitus
Type 2 diabetes is typically a chronic disease, associated with a ten year shorter life expectancy.[6] This is partly due to a number of complications with which it is associated including: two to four times the risk of cardiovascular disease, including ischemic heart disease and stroke, a 20 fold increase in lower limb amputations, and increased rates of hospitalizations.[6] In the developed world, and increasingly elsewhere, type 2 diabetes is the largest cause of non-traumatic blindness and kidney failure.[7] It has also been associated with an increased risk of cognitive dysfunction and dementia through disease processes such as Alzheimer's disease and vascular dementia.[8] Other complications include: acanthosis nigricans, sexual dysfunction, and frequent infections.[5]
Cause
The development of type 2 diabetes is caused by a combination of lifestyle and genetic factors.[7][9] While some are under personal control such as diet and obesity others such as increasing age, female gender, and genetics are not.[6] A lack of sleep has been linked to type 2 diabetes.[10] This is believed to act through its effect on metabolism.[10] The nutritional status of a mother during fetal development may also play a role with one proposed mechanism being that of altered DNA methylation.[11]
LifestyleMain article: Lifestyle causes of diabetes mellitus type 2
A number of lifestyle factors are known to be important to the development of type 2 diabetes including: obesity (defined by a body mass index of greater than thirty), lack of physical activity, poor diet, stress, and urbanization.[6] Excess body fat is associated with 30% of cases in those of Chinese and Japanese descent, 60-80% of cases in those of European and African descent, and 100% of Pima Indians and Pacific Islanders.[3] Those who are not obese often have a high waist–hip ratio.[3] Dietary factors also influence the risk of developing type 2 diabetes. Consumption of sugar sweetened drinks in excess is associated with an increased risk.[12][13] The type of fats in the diet are also important, with saturated fats and trans fatty acids increasing the risk and polyunsaturated and monounsaturated fat decreasing the risk.[9] Eating lots of white rice appears to also play a role in increasing risk.[14]
GeneticsMain article: Genetic causes of diabetes mellitus type 2
Most cases of diabetes involve many genes with each being a small contributor to an increased probability of becoming a type 2 diabetic.[6] If one identical twin has diabetes the chance of the other developing diabetes within their lifetime is greater than 90% while the rate for non-identical siblings is 25-50%.[3] As of 2011, more than 36 genes have been found that contribute to the risk of type 2 diabetes.[15] All of these genes together still only account for 10% of the total heritable component of the disease. The TCF7L2 allele for example increases the risk of developing diabetes by 1.5 times and is the greatest risk of the common genetic variants. Most of the genes link to diabetes are involved in beta cell functions.[3]
There are a number of rare cases of diabetes that arise due to an abnormality in a single gene (known as monogenic forms of diabetes or "other specific types of diabetes").[3][6] These include maturity onset
diabetes of the young (MODY), Donohue syndrome, and Rabson-Mendenhall syndrome, among others.[6] Maturity onset diabetes of the young constitute 1–5 % of all cases of diabetes in young people.[16]
Medical conditions
There are a number of medications and other health problems that can predispose to diabetes.[17] Some of the medications include: glucocorticoids, thiazides, beta blockers, atypical antipsychotics,[18] and statins.[19] Those who have previously had gestational diabetes are at a higher risk of developing type 2 diabetes.[5] Other health problems that are associated include: acromegaly, Cushing's syndrome, hyperthyroidism, pheochromocytoma, and certain cancers such as glucagonomas.[17] Testosterone deficiency is also associated with type 2 diabetes.[20][21]
Pathophysiology
Type 2 diabetes is due to insufficient insulin production from beta cells in the setting of insulin resistance.[3] Insulin resistance, which is the inability of cells to respond adequately to normal levels of insulin, occurs primarily within the muscles, liver and fat tissue.[22] In the liver, insulin normally suppresses glucose release. However in the setting of insulin resistance, the liver inappropriately releases glucose into the blood.[6] The proportion of insulin resistance verses beta cell dysfunction differs among individuals with some having primarily insulin resistance and only a minor defect in insulin secretion and others with slight insulin resistance and primarily a lack of insulin secretion.[3]
Other potentially important mechanisms associated with type 2 diabetes and insulin resistance include: increased breakdown of lipids within fat cells, resistance to and lack of incretin, high glucagon levels in the blood, increased retention of salt and water by the kidneys, and
inappropriate regulation of metabolism by the central nervous system.[6] However not all people with insulin resistance develop diabetes, since an impairment of insulin secretion by pancreatic beta cells is also required.[3]
Diagnosis
Diabetes diagnostic criteria[23][24] edit
Condition 2 hour glucose Fasting glucose HbA1c
mmol/l(mg/dl) mmol/l(mg/dl) %
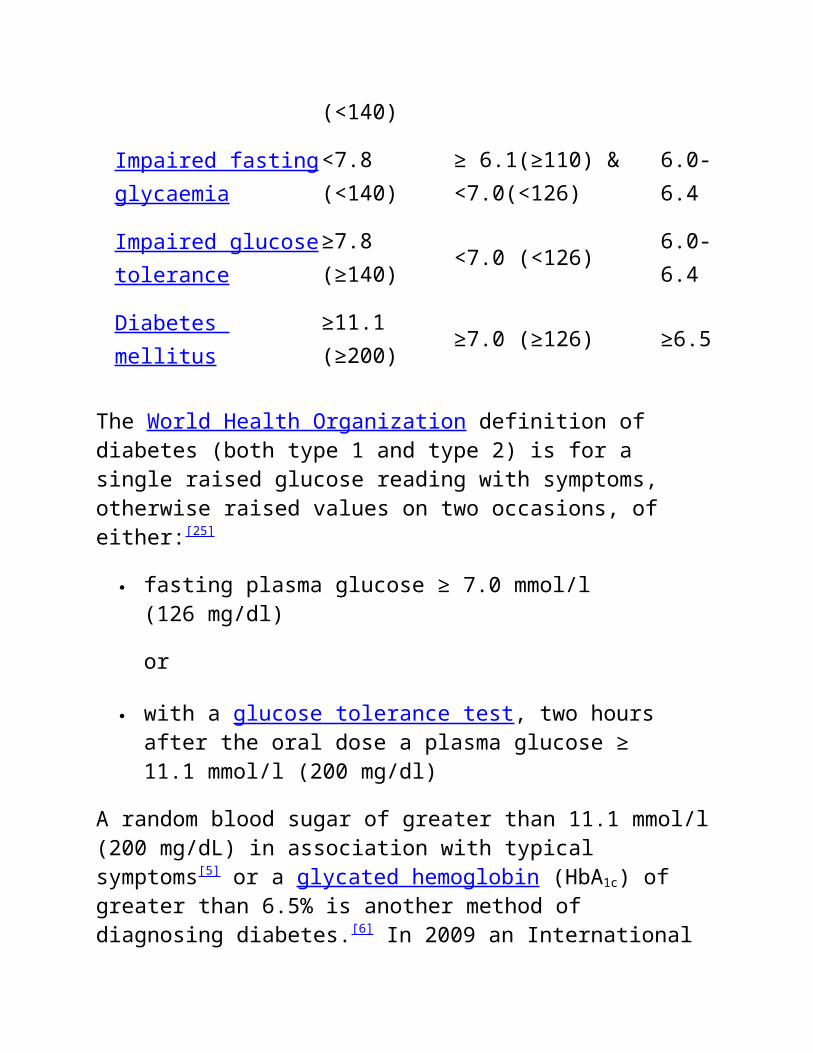
Normal <7.8 (<140) <6.1 (<110) <6.0
Impaired fasting glycaemia
<7.8 (<140)≥ 6.1(≥110) & <7.0(<126)
6.0-6.4
Impaired glucose tolerance
≥7.8 (≥140) <7.0 (<126) 6.0-6.4
Diabetes mellitus ≥11.1 (≥200) ≥7.0 (≥126) ≥6.5
The World Health Organization definition of diabetes (both type 1 and type 2) is for a single raised glucose reading with symptoms, otherwise raised values on two occasions, of either:[25]
fasting plasma glucose ≥ 7.0 mmol/l (126 mg/dl)
or
with a glucose tolerance test, two hours after the oral dose a plasma glucose ≥ 11.1 mmol/l (200 mg/dl)
A random blood sugar of greater than 11.1 mmol/l (200 mg/dL) in association with typical symptoms[5] or a glycated hemoglobin (HbA1c) of greater than 6.5% is another method of diagnosing diabetes.[6] In 2009 an International Expert Committee that included representatives of the American Diabetes Association (ADA), the International Diabetes Federation (IDF), and the European Association for the Study of Diabetes (EASD) recommended that a threshold of ≥6.5% HbA1c should be used to diagnose diabetes. This recommendation was adopted by the American Diabetes Association in 2010.[26] Positive tests should be repeated unless the person presents with typical symptoms and blood sugars >11.1 mmol/l (>200 mg/dl).[27]
Threshold for diagnosis of diabetes are based on the relationship between results of glucose tolerance tests, fasting glucose or HbA1c and complications such as retinal problems.[6] A fasting or random blood sugar is preferred over the glucose tolerance test as they are more convenient for people.[6] HbA1c has the advantages that fasting is not required and results are more stable, but has the disadvantage that the test is more costly than measurement of blood glucose.[28] It is estimated that 20% of people with diabetes in the United States do not realize that they have the disease.[6] Diabetes mellitus type 2 is characterized by high blood glucose in the context of insulin resistance and relative insulin deficiency.[2] This is in contrast to diabetes mellitus type 1 in which there is an absolute insulin deficiency due to destruction of islet cells in the pancreas and gestational diabetes mellitus that is a new onset of high blood sugars in associated with pregnancy.[3] Type 1 and type 2 diabetes can typically be distinguished based on the presenting circumstances.[27] If the diagnosis is in doubt antibody testing may be useful to confirm type 1 diabetes and C-peptide levels may be useful to confirm type 2 diabetes.[29]
No major organization recommends universal screening for diabetes as there is no evidence that such a program would improve outcomes.[30] Screening is recommended by the United States Preventive Services Task Force in adults without symptoms whose blood pressure is greater than 135/80 mmHg.[31] For those whose blood pressure is less, the evidence is insufficient to recommend for or against screening.[31] The World Health Organization recommends only testing those groups at high risk.[30] High risk groups in the United States include: those over 45 years old, those with a first degree relative with diabetes, some ethnic groups including Hispanics, African-Americans, and Native-Americans, a history of gestational diabetes, polycystic ovary syndrome, excess weight, and conditions associated with metabolic syndrome.[5]
Prevention
Main article: Prevention of diabetes mellitus type 2
Onset of type 2 diabetes can be delayed or prevented through proper nutrition and regular exercise.[32][33] Intensive lifestyle measures may reduce the risk by over half.[7] The benefit of exercise occurs regardless of the person's initial weight or subsequent weight loss.[34] Evidence for the benefit of dietary changes alone, however, is limited,[35] with some evidence for a diet high in green leafy vegetables[36] and some for limiting the intake of sugary drinks.[12] In those with impaired glucose tolerance, diet and exercise either alone or in combination with metformin or acarbose may decrease the risk of developing diabetes.[7]
[37] Lifestyle interventions are more effective than metformin.[7]
Management
Further information: Diabetes management
Management of type 2 diabetes focuses on lifestyle interventions, lowering other cardiovascular risk factors, and maintaining blood
glucose levels in the normal range.[7] Self-monitoring of blood glucose for people with newly diagnosed type 2 diabetes was recommended by the National Health Services in 2008,[38] however the benefit of self monitoring in those not using multi-dose insulin is questionable.[7][39] Managing other cardiovascular risk factors including:hypertension, high cholesterol, and microalbuminuria, improves a person's life expectancy.[7] Intensive blood sugar lowering (HbA1C<6%) as opposed to standard blood sugar lowering (HbA1C of 7-7.9%) does not appear to change mortality.[40][41] The goal of treatment is typically an HbA1C of less than 7% or a fasting glucose of less than 6.7 mmol/L (120 mg/dL) however these goals may be changed after professional clinical consultation, taking into account particular risks of hypoglycemia and life expectancy.[5] It is recommended that all people with type 2 diabetes get regular ophthalmology examination.[3]
Lifestyle
A proper diet and exercise are the foundations of diabetic care[5] with a greater amount of exercise yielding better results.[42] Aerobic exercise leads to a decrease in HbA1C and improved insulin sensitivity.[42] Resistance training is also useful and the combination of both types of exercise may be most effective.[42] A diabetic diet that promotes weight loss is important.[43] While the best diet type to achieve this is controversial[43] a low glycemic index diet has been found to improve blood sugar control.[44] Culturally appropriate education may help people with Type 2 diabetes control their blood sugar levels, for up to six months at least.[45] If changes in lifestyle, in those with mild diabetes, has not resulted in improved blood sugars within six weeks medications should then be considered.[5]
There are several classes of anti-diabetic medications available. Metformin is generally recommended as a first line treatment as there is some evidence that it decreases mortality.[7] A second oral agent of another class may be used if metformin is not sufficient.[46] Other classes of medications include: sulfonylureas, nonsulfonylurea secretagogues, alpha glucosidase inhibitors, thiazolidinediones, glucagon-like peptide-1 analog, and dipeptidyl peptidase-4 inhibitors.[7]
[47] Metformin should not be used in those with severe kidney or liver problems.[5] Injections of insulin may either be added to oral medication or used alone.[7]
Most people do not initially need insulin.[3] When it is used, a long-acting formulation is typically added at night, with oral medications being continued.[5][7] Doses are then increased to effect (blood sugar levels being well controlled).[7] When nightly insulin is insufficient twice daily insulin may achieve better control.[5] The long acting insulins, glargine and detemir, do not appear much better than neutral protamine Hagedorn (NPH) insulin but have a significantly greater cost making them, as of 2010, not cost effective.[48] In those who are pregnant insulin is generally the treatment of choice.[5]
Weight loss surgery in those who are obese appears to be an effective measure to treat diabetes.[49] Many are able to maintain normal blood sugar levels with little or no medications following surgery[50] and long term mortality is decreased.[51] There however is some short term mortality risk of less than 1% from the surgery.[52] The body mass index cutoffs for when surgery is appropriate are not yet clear.[51]
Epidemiology
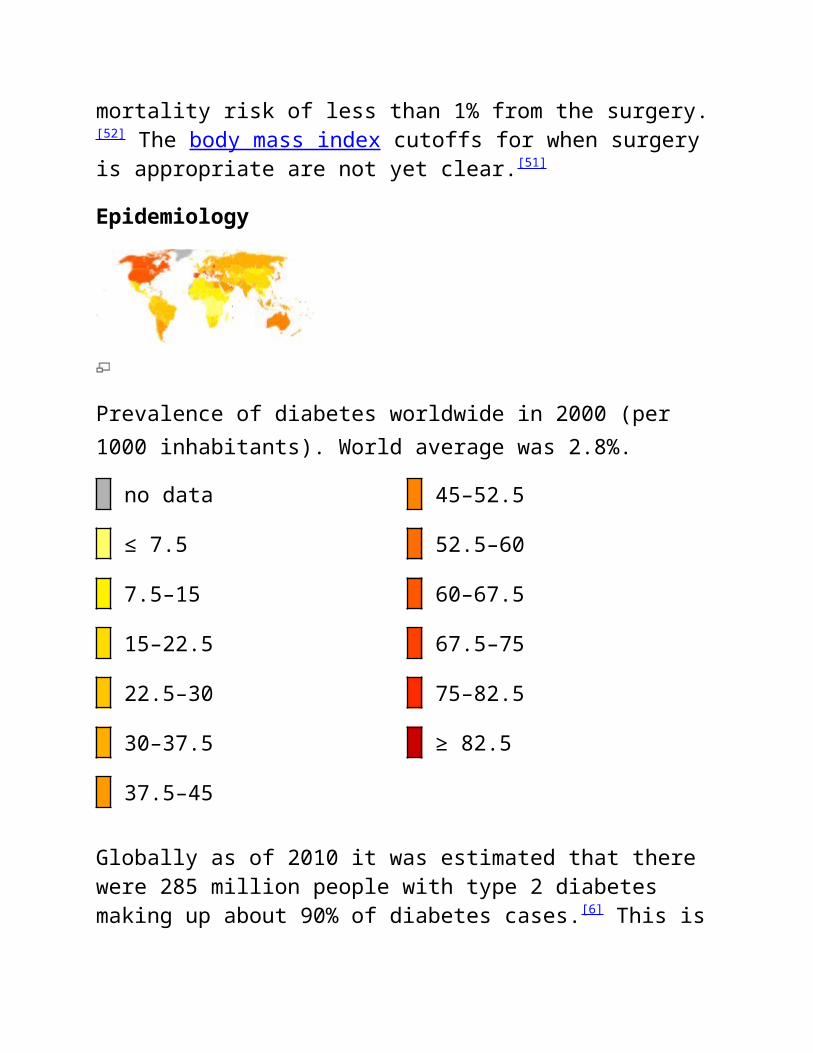
Prevalence of diabetes worldwide in 2000 (per 1000 inhabitants). World average was 2.8%.
Globally as of 2010 it was estimated that there were 285 million people with type 2 diabetes making up about 90% of diabetes cases.[6] This is equivalent to about 6% of the worlds adult population.[53] Diabetes is common both in the developed and the developing world.[6] However remains uncommon in the underdeveloped world.[3] Women seem to be at a greater risk as do certain ethnic groups,[6][54] such as South Asians, Pacific Islanders, Latinos, and Native Americans.[5] This may be due to enhanced sensitivity to a Western lifestyle in certain ethnic groups.[55] Traditionally considered a disease of adults, type 2 diabetes is increasingly diagnosed in children in parallel with rising obesity rates.[6] Type 2 diabetes is now diagnosed as frequently as type 1 diabetes in teenagers in the United States.[3]
Rates of diabetes in 1985 were estimated at 30 million, increasing to 135 million in 1995 and 217 million in 2005.[56] This increase is believed to be primarily due to the global population aging, a decrease in exercise, and increasing rates of obesity.[56] The five countries with the greatest number of people with diabetes as of 2000 are India having 31.7 million, China 20.8 million, the United States 17.7 million, Indonesia 8.4 million, and Japan 6.8 million.[57] It is recognized as a global epidemic by the World Health Organization.[58]
History
Main article: History of diabetes
Diabetes is one of the first diseases described[59] with an Egyptian manuscript from c. 1500 BCE mentioning "too great emptying of the urine."[60] The first described cases are believed to be of type 1 diabetes.[60] Indian physicians around the same time identified the disease and classified it as madhumeha or honey urine noting that the urine would attract ants.[60] The term "diabetes" or "to pass through" was first used in 230 BCE by the Greek Appollonius Of Memphis.[60] The disease was
rare during the time of the Roman empire with Galen commenting that he had only seen two cases during his career.[60] Type 1 and type 2 diabetes were identified as separate conditions for the first time by the Indian physicians Sushruta and Charaka in 400-500 AD with type 1 associated with youth and type 2 with being overweight.[60] The term "mellitus" or "from honey" was added by the Briton John Rolle in the late 1700s to separate the condition from diabetes insipidus which is also associated with frequent urination.[60] Effective treatment was not developed until the early part of the 20th century when the Canadians Frederick Banting and Charles Best developed insulin in 1921 and 1922.[60] This was followed by the development of the long acting NPH insulin in the 1940s.[60]
Background
Type 2 diabetes mellitus consists of an array of dysfunctions characterized by hyperglycemia and resulting from the combination of resistance to insulin action, inadequate insulin secretion, and excessive or inappropriate glucagon secretion. Poorly controlled type 2 diabetes is associated with an array of microvascular, macrovascular, and neuropathic complications.
Microvascular complications of diabetes include retinal, renal, and possibly neuropathic disease. Macrovascular complications include coronary artery and peripheral vascular disease. Diabetic neuropathy affects autonomic and peripheral nerves. (See Pathophysiology and Presentation.)
Unlike patients with type 1 diabetes mellitus, patients with type 2 are not absolutely dependent on insulin for life. This distinction was the basis for the older terms for types 1 and 2, insulin dependent and non–insulin dependent diabetes.
However, many patients with type 2 diabetes are ultimately treated with insulin. Because they retain the ability to secrete some endogenous insulin, they are considered to require insulin but not to depend on insulin. Nevertheless, given the potential for confusion due to classification based on treatment rather than etiology, the older terms have been abandoned.[1] Another older term for type 2 diabetes mellitus was adult-onset diabetes. Currently, because of the epidemic of obesity and inactivity in children, type 2 diabetes mellitus is occurring at younger and younger ages. Although type 2 diabetes mellitus typically affects individuals older than 40 years, it has been diagnosed in children as young as 2 years of age who have a family history of diabetes. In many communities, type 2 diabetes now outnumbers type 1 among children with newly diagnosed diabetes. (See Epidemiology.)
Diabetes mellitus is a chronic disease that requires long-term medical attention to limit the development of its devastating complications and to manage them when they do occur. It is a disproportionately expensive disease; in the United States in 2007, the direct medical costs of diabetes were $116 billion, and the total costs were $174 billion; people with diabetes had average medical expenditures 2.3 times those of people without diabetes. The emergency department utilization rate by people with diabetes is twice that of the unaffected population.[2, 3]
This article focuses on the diagnosis and treatment of type 2 diabetes and its acute and chronic complications, other than those directly associated with hypoglycemia and severe metabolic disturbances, such as hyperosmolar hyperglycemic state (HHS) and diabetic ketoacidosis (DKA). For more information on those topics, see Hyperosmolar Hyperglycemic State and Diabetic Ketoacidosis.
Type 2 diabetes is characterized by a combination of peripheral insulin resistance and inadequate insulin secretion by pancreatic beta cells. Insulin resistance, which has been attributed to elevated levels of free fatty acids and proinflammatory cytokines in plasma, leads to decreased glucose transport into muscle cells, elevated hepatic glucose production, and increased breakdown of fat.
A role for excess glucagon cannot be underestimated; indeed, type 2 diabetes is an islet paracrinopathy in which the reciprocal relationship between the glucagon-secreting alpha cell and the insulin-secreting beta cell is lost, leading to hyperglucagonemia and hence the consequent hyperglycemia.[2]
For type 2 diabetes mellitus to occur, both insulin resistance and inadequate insulin secretion must exist. For example, all overweight individuals have insulin resistance, but diabetes develops only in those who cannot increase insulin secretion sufficiently to compensate for their insulin resistance. Their insulin concentrations may be high, yet inappropriately low for the level of glycemia.
A simplified scheme for the pathophysiology of abnormal glucose metabolism in type 2 diabetes mellitus is depicted in the image below.
Simplified scheme for the pathophysiology of type 2 diabetes mellitus.
With prolonged diabetes, atrophy of the pancreas may occur. A study by Philippe et al used computed tomography (CT) scan findings, glucagon stimulation test results, and fecal elastase-1 measurements to
confirm reduced pancreatic volume in individuals with a median 15-year history of diabetes mellitus (range, 5-26 years).[4] This may also explain the associated exocrine deficiency seen in prolonged diabetes.
Beta-cell dysfunction
Beta-cell dysfunction is a major factor across the spectrum of prediabetes to diabetes. A study of obese adolescents by Bacha et al confirms what is increasingly being stressed in adults as well: Beta-cell dysfunction develops early in the pathologic process and does not necessarily follow the stage of insulin resistance.[5] Singular focus on insulin resistance as the "be all and end all" is gradually shifting, and hopefully better treatment options that address the beta-cell pathology will emerge for early therapy.
Insulin resistance
In the progression from normal to abnormal glucose tolerance, postprandial blood glucose levels increase first. Eventually, fasting hyperglycemia develops as suppression of hepatic gluconeogenesis fails.
During the induction of insulin resistance (such as occurs with a high-calorie diet, steroid administration, or physical inactivity), increased glucagon levels and increased glucose-dependent insulinotropic polypeptide (GIP) levels accompany glucose intolerance. However, the postprandial glucagonlike peptide-1 (GLP-1) response is unaltered.[6]
Genomic factors
Genome-wide association studies of single-nucleotide polymorphisms (SNPs) have identified a number of genetic variants that are associated with beta-cell function and insulin resistance. Some of these SNPs appear to increase the risk for type 2 diabetes. Over 40 independent
loci demonstrating an association with an increased risk for type 2 diabetes have been shown.[7] A subset of the most potent are shared below[8] :
Decreased beta-cell responsiveness, leading to impaired insulin processing and decreased insulin secretion (TCF7L2)
Lowered early glucose-stimulated insulin release (MTNR1B, FADS1, DGKB, GCK)
Altered metabolism of unsaturated fatty acids (FSADS1) Dysregulation of fat metabolism (PPARG) Inhibition of serum glucose release (KCNJ11)[9]
Increased adiposity and insulin resistance (FTO and IGF2BP2)[10, 11]
Control of the development of pancreatic structures, including beta-islet cells (HHEX)[12]
Transport of zinc into the beta-islet cells, which influences the production and secretion of insulin (SLC30A8)[12]
Survival and function of beta-islet cells (WFS1)[13]
Susceptibility to type 2 diabetes may also be affected by genetic variants involving incretin hormones, which are released from endocrine cells in the gut and stimulate insulin secretion in response to digestion of food. For example, reduced beta-cell function has been associated with a variant in the gene that codes for the receptor of gastric inhibitory polypeptide (GIPR).[14]
The high mobility group A1 (HMGA1) protein is a key regulator of the insulin receptor gene (INSR).[15] Functional variants of the HMGA1 gene are associated with an increased risk of diabetes.
Amino acid metabolism
Amino acid metabolism may play a key role early in the development of type 2 diabetes. Wang et al reported that the risk of future diabetes was at least 4-fold higher in normoglycemic individuals with high fasting
plasma concentrations of 3 amino acids (isoleucine, phenylalanine, and tyrosine). Concentrations of these amino acids were elevated up to 12 years prior to the onset of diabetes.[16] In this study, amino acids, amines, and other polar metabolites were profiled using liquid chromatography tandem mass spectrometry.
Diabetes complications
Although the pathophysiology of the disease differs between the types of diabetes, most of the complications, including microvascular, macrovascular, and neuropathic, are similar regardless of the type of diabetes. Hyperglycemia appears to be the determinant of microvascular and metabolic complications. Macrovascular disease may be less related to glycemia.
Telomere attrition may be a marker associated with presence and the number of diabetic complications. Whether it is a cause or a consequence of diabetes remains to be seen.[17]
Cardiovascular risk
Cardiovascular risk in people with diabetes is related in part to insulin resistance, with the following concomitant lipid abnormalities:
Elevated levels of small, dense low-density lipoprotein (LDL) cholesterol particles
Low levels of high-density lipoprotein (HDL) cholesterol Elevated levels of triglyceride-rich remnant lipoproteins
Thrombotic abnormalities (ie, elevated type-1 plasminogen activator inhibitor [PAI-1], elevated fibrinogen) and hypertension are also involved. Other conventional atherosclerotic risk factors (eg, family history, smoking, elevated LDL cholesterol) also affect cardiovascular risk.
Insulin resistance is associated with increased lipid accumulation in liver and smooth muscle, but not with increased myocardial lipid accumulation.[18] Persistent lipid abnormalities remain in patients with diabetes despite the use of lipid-modifying drugs, although evidence supports the benefits of these drugs. Statin dose up-titration and the addition of other lipid-modifying agents are needed.[19]
Increased cardiovascular risk appears to begin prior to the development of frank hyperglycemia, presumably because of the effects of insulin resistance. Stern in 1996[20] and Haffner and D'Agostino in 1999[21]
developed the "ticking clock" hypothesis of complications, asserting that the clock starts ticking for microvascular risk at the onset of hyperglycemia, while the clock starts ticking for macrovascular risk at some antecedent point, presumably with the onset of insulin resistance.
The question of when diabetes becomes a cardiovascular risk equivalent has not yet been settled. Debate has moved beyond automatically considering diabetes a cardiovascular risk equivalent. Perhaps it would be prudent to assume the equivalency with diabetes that is more than 5-10 years in duration.
Secondary diabetes
Various other types of diabetes, previously called secondary diabetes, are caused by other illnesses or medications. Depending on the primary process involved (eg, destruction of pancreatic beta cells or development of peripheral insulin resistance), these types of diabetes behave similarly to type 1 or type 2 diabetes.
The most common causes of secondary diabetes are as follows:
Diseases of the pancreas that destroy the pancreatic beta cells (eg, hemochromatosis, pancreatitis, cystic fibrosis, pancreatic cancer)
Hormonal syndromes that interfere with insulin secretion (eg, pheochromocytoma)
Hormonal syndromes that cause peripheral insulin resistance (eg, acromegaly, Cushing syndrome, pheochromocytoma)
Drugs (eg, phenytoin, glucocorticoids, estrogens)
Gestational diabetes
Gestational diabetes mellitus is defined as any degree of glucose intolerance with onset or first recognition during pregnancy. Gestational diabetes mellitus is a complication of approximately 4% of all pregnancies in the United States. A steady decline in insulin sensitivity as gestation progresses is a normal feature of pregnancy; gestational diabetes mellitus results when maternal insulin secretion cannot increase sufficiently to counteract the decrease in insulin sensitivity. (For more information, see Diabetes Mellitus and Pregnancy.)
tiology
The etiology of type 2 diabetes mellitus appears to involve complex interactions between environmental and genetic factors. Presumably, the disease develops when a diabetogenic lifestyle (ie, excessive caloric intake, inadequate caloric expenditure, obesity) is superimposed on a susceptible genotype.
The body mass index (BMI) at which excess weight increases risk for diabetes varies with different racial groups. For example, compared with persons of European ancestry, persons of Asian ancestry are at increased risk for diabetes at lower levels of overweight.[22]
Hypertension and prehypertension are associated with a greater risk of developing diabetes in whites than in African Americans.[23]
In addition, an in utero environment resulting in low birth weight may predispose some individuals to develop type 2 diabetes mellitus.[24, 25]
Infant weight velocity has a small, indirect effect on adult insulin resistance, and this is primarily mediated through its effect on BMI and waist circumference.[26]
About 90% of patients who develop type 2 diabetes mellitus are obese. However, a large, population-based, prospective study has shown that an energy-dense diet may be a risk factor for the development of diabetes that is independent of baseline obesity.[27]
Some studies suggest that environmental pollutants may play a role in the development and progression of type 2 diabetes mellitus.[28] A structured and planned platform is needed to fully explore the diabetes-inducing potential of environmental pollutants.
Secondary diabetes may occur in patients taking glucocorticoids or when patients have conditions that antagonize the actions of insulin (eg, Cushing syndrome, acromegaly, pheochromocytoma).
Major risk factors
The major risk factors for type 2 diabetes mellitus are the following:
Age greater than 45 years (though, as noted above, type 2 diabetes mellitus is occurring with increasing frequency in young individuals)
Weight greater than 120% of desirable body weight Family history of type 2 diabetes in a first-degree relative (eg,
parent or sibling)
Hispanic, Native American, African American, Asian American, or Pacific Islander descent
History of previous impaired glucose tolerance (IGT) or impaired fasting glucose (IFG)
Hypertension (>140/90 mm Hg) or dyslipidemia (HDL cholesterol level < 40 mg/dL or triglyceride level >150 mg/dL)
History of gestational diabetes mellitus or of delivering a baby with a birth weight of over 9 lb
Polycystic ovarian syndrome (which results in insulin resistance)
Genetic influences
The genetics of type 2 diabetes are complex and not completely understood. Evidence supports the involvement of multiple genes in pancreatic beta-cell failure and insulin resistance.
Genome-wide association studies have identified dozens of common genetic variants associated with increased risk for type 2 diabetes.[8] Of the variants thus far discovered, the one with the strongest effect on susceptibility is the transcription factor 7–like 2 (TCF7L2) gene. (For more information, see Type 2 Diabetes and TCF7L2.)
Identified genetic variants account for only about 10% of the heritable component of most type 2 diabetes.[8] An international research consortium found that use of a 40-SNP genetic risk score improves the ability to make an approximate 8-year risk prediction for diabetes beyond that which is achievable when only common clinical diabetes risk factors are used. Moreover, the predictive ability is better in younger persons (in whom early preventive strategies could delay diabetes onset) than in those older than 50 years.[29]
Some forms of diabetes have a clear association with genetic defects. The syndrome historically known as maturity onset diabetes of youth (MODY), which is now understood to be a variety of defects in beta-cell
function, accounts for 2-5% of individuals with type 2 diabetes who present at a young age and have mild disease. The trait is autosomal dominant and can be screened for through commercial laboratories.
To date, 11 MODY subtypes have been identified, involving mutations in the following genes[30, 31] :
Most of the MODY subtypes are associated with diabetes only; however, MODY type 5 is known to be associated with renal cysts,[36]
and MODY type 8 is associated with exocrine pancreatic dysfunction.[33]
A number of variants in mitochondrial deoxyribonucleic acid (DNA) have been proposed as an etiologic factor for a small percentage of patients with type 2 diabetes. Two specific point mutations and some deletions and duplications in the mitochondrial genome can cause type 2 diabetes and sensorineural hearing loss.[37]
Diabetes can also be a finding in more severe mitochondrial disorders such as Kearns-Sayre syndrome and mitochondrial encephalomyopathy, lactic acidosis, and strokelike episode (MELAS). Mitochondrial forms of diabetes mellitus should be considered when diabetes occurs in conjunction with hearing loss, myopathy, seizure
disorder, strokelike episodes, retinitis pigmentosa, external ophthalmoplegia, or cataracts. These findings are of particular significance if there is evidence of maternal inheritance.
Depression
Accumulating evidence suggests that depression is a significant risk factor for developing type 2 diabetes. Pan et al found that the relative risk was 1.17 in women with depressed mood and 1.25 in women using antidepressants.[38] Antidepressant use may be a marker of more severe, chronic, or recurrent depression, or antidepressant use itself may increase diabetes risk, possibly by altering glucose homeostasis or promoting weight gain.
In turn, type 2 diabetes has been identified as a risk factor for the development of depression. Depressive symptoms and major depressive disorder are twice as prevalent in patients with type 2 diabetes as in the general population.[39]
Schizophrenia
Schizophrenia has been linked to the risk for type 2 diabetes. Dysfunctional signaling involving protein kinase B (Akt) is a possible mechanism for schizophrenia; moreover, acquired Akt defects are associated with impaired regulation of blood glucose and diabetes, which is overrepresented in first-episode, medication-naive patients with schizophrenia.[40] In addition, second-generation antipsychotics are associated with greater risk for type-2 diabetes.
Epidemiology
Occurrence in the United States
A 2011 Centers for Disease Control and Prevention (CDC) report estimated that nearly 26 million Americans have diabetes.[3]
Additionally, an estimated 79 million Americans have prediabetes.
Diabetes affects 8.3% of Americans of all ages, 11.3% of adults aged 20 years and older, and 25% of persons age 65 and older, according to the National Diabetes Fact Sheet for 2011.[3] About 27% of those with diabetes—7 million Americans—do not know that they have the disease. About 215,000 people younger than 20 years had diabetes (type 1 or type 2) in the United States in 2010.[3]
Prediabetes affects 35% of adults aged 20 years and older. Prediabetes, as defined by the American Diabetes Association, is that state in which blood glucose levels are higher than normal but not high enough to be diagnosed as diabetes. It is presumed that most persons with prediabetes will subsequently progress to diabetes. The CDC estimated that in 2010, 79 million Americans aged 20 years or older had prediabetes—35% of US adults aged 20 years or older and 50% of those aged 65 years or older.
A study by Ludwig et al found that neighborhoods with high levels of poverty are associated with increases in the incidence of extreme obesity and diabetes. Although the mechanisms behind this association is unclear, further investigation is warranted.[41]
International occurrence
Type 2 diabetes mellitus is less common in non-Western countries where the diet contains fewer calories and daily caloric expenditure is higher. However, as people in these countries adopt Western lifestyles, weight gain and type 2 diabetes mellitus are becoming virtually epidemic.
Rates of diabetes are increasing worldwide. The International Diabetes Federation predicts that the number of people living with diabetes will to rise from 366 million in 2011 to 552 million by 2030.[42] In the United States, the prevalence of diagnosed diabetes has more than doubled in the last 3 decades, largely because of the increase in obesity.
The top 10 countries in number of people with diabetes are currently India, China, the United States, Indonesia, Japan, Pakistan, Russia, Brazil, Italy, and Bangladesh. The greatest percentage increase in rates of diabetes will occur in Africa over the next 20 years. Unfortunately, at least 80% of people in Africa with diabetes are undiagnosed, and many in their 30s to 60s will die from diabetes there.
Race-related demographics
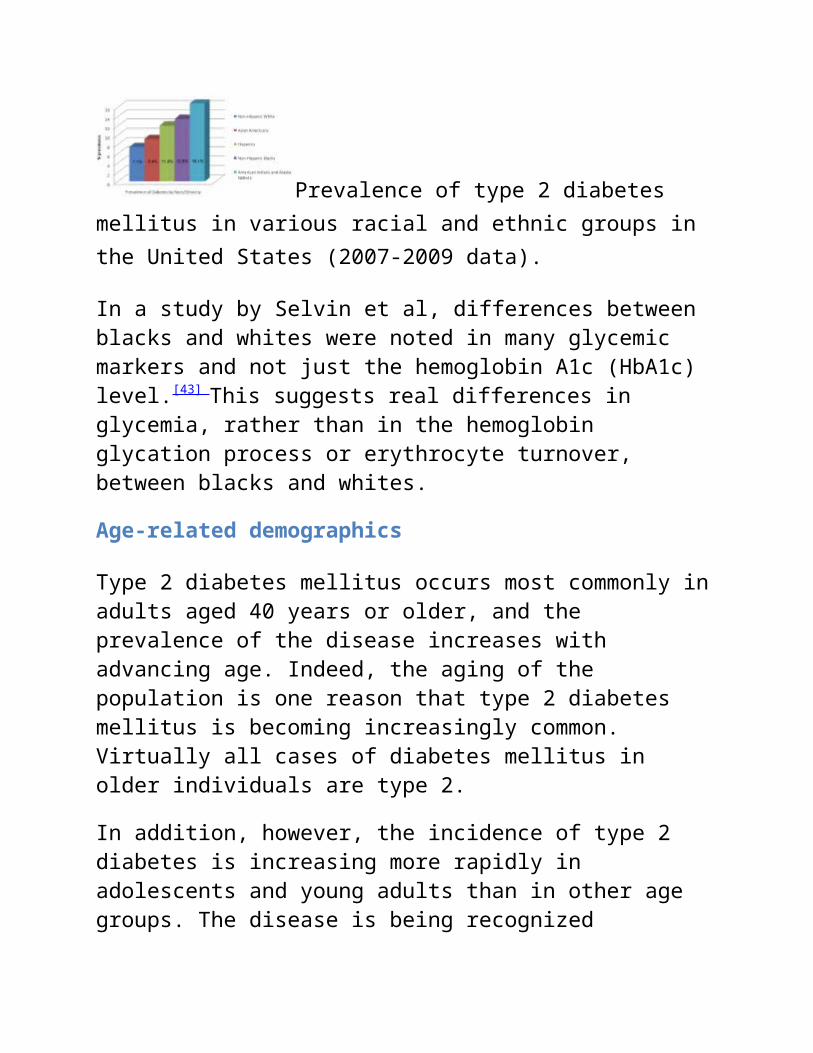
The prevalence of type 2 diabetes mellitus varies widely among various racial and ethnic groups. The image below shows data for various populations. Type 2 diabetes mellitus is more prevalent among Hispanics, Native Americans, African Americans, and Asians/Pacific Islanders than in non-Hispanic whites. Indeed, the disease is becoming virtually pandemic in some groups of Native Americans and Hispanic people. The risk of retinopathy and nephropathy appears to be greater in blacks, Native Americans, and Hispanics.
Prevalence of type 2 diabetes mellitus in various racial and ethnic groups in the United States (2007-2009 data).
In a study by Selvin et al, differences between blacks and whites were noted in many glycemic markers and not just the hemoglobin A1c (HbA1c) level.[43] This suggests real differences in glycemia, rather than
in the hemoglobin glycation process or erythrocyte turnover, between blacks and whites.
Age-related demographics
Type 2 diabetes mellitus occurs most commonly in adults aged 40 years or older, and the prevalence of the disease increases with advancing age. Indeed, the aging of the population is one reason that type 2 diabetes mellitus is becoming increasingly common. Virtually all cases of diabetes mellitus in older individuals are type 2.
In addition, however, the incidence of type 2 diabetes is increasing more rapidly in adolescents and young adults than in other age groups. The disease is being recognized increasingly in younger persons, particularly in highly susceptible racial and ethnic groups and the obese. In some areas, more type 2 than type 1 diabetes mellitus is being diagnosed in prepubertal children, teenagers, and young adults. The prevalence of diabetes mellitus by age is shown in the image below.
Prevalence of diabetes mellitus type 2 by age in the United States (2007 estimates).
Prognosis
The prognosis in patients with diabetes mellitus is strongly influenced by the degree of control of their disease. Chronic hyperglycemia is associated with an increased risk of microvascular complications, as shown in the Diabetes Control and Complications Trial (DCCT) in individuals with type 1 diabetes[44, 45] and the United Kingdom Prospective Diabetes Study (UKPDS) in people with type 2 diabetes.[46]
Prognosis in intensive therapy
In the UKPDS, more than 5000 patients with type 2 diabetes were followed up for up to 15 years. Those in the intensely treated group had a significantly lower rate of progression of microvascular complications than did patients receiving standard care. Rates of macrovascular disease were not altered except in the metformin-monotherapy arm in obese individuals, in which the risk of myocardial infarction was significantly decreased.
In the 10-year follow-up to the UKPDS, patients in the previously intensively treated group demonstrated a continued reduction in microvascular and all-cause mortality, as well as in cardiovascular events, despite early loss of differences in glycated hemoglobin levels between the intensive-therapy and conventional-therapy groups.[47] The total follow-up was 20 years, half while in the study and half after the study ended.
Other, shorter studies, such as Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation (ADVANCE) and the Veterans Affairs Diabetes Trial (VADT), showed no improvement in cardiovascular disease and death with tight control (lower targets than in the UKPDS).[48, 49, 50]
In the Action to Control Cardiovascular Risk in Diabetes (ACCORD) study, increased mortality was noted among the poorly-controlled patients in the intensive glycemic arm; indeed there was a 66% increase in mortality for each 1% increase in HbA1c; the best outcome occurred among patients who achieved the target of an HbA1c of less than 6%. The excess mortality between the intensive and conventional glycemic arms occurred for A1c above 7%.
Differences between the patient populations in these studies and the UKPDS may account for some of the differences in outcome. The
patients in these 3 studies had established diabetes and had a prior cardiovascular disease event or were at high risk for a cardiovascular disease event, whereas patients in the UKPDS study were younger, with new-onset diabetes and low rates of cardiovascular disease.
Early, intensive, multifactorial (blood pressure, cholesterol) management in patients with type 2 diabetes mellitus was associated with a small, nonsignificant reduction in the incidence of cardiovascular disease events and death in a multinational European study.[51] The 3057 patients in this study had diabetes detected by screening and were randomized to receive either standard diabetes care or intensive management of hyperglycemia (target HbA1c < 7.0%), blood pressure, and cholesterol levels.
The benefits of intensive intervention were demonstrated in the Steno-2 study in Denmark, which included 160 patients with type 2 diabetes and persistent microalbuminuria; the mean treatment period was 7.8 years, followed by an observational period for a mean of 5.5 years. Intensive therapy was associated with a lower risk of cardiovascular events, death from cardiovascular causes, progression to end-stage renal disease, and need for retinal photocoagulation.[52]
A British study indicated that the HbA1c level achieved 3 months after the initial diagnosis of type 2 diabetes mellitus predicts subsequent mortality. In other words, according to the report, aggressive lowering of glucose after diagnosis bodes well for long-term survival. (Intensified diabetes control must be introduced gradually in newly diagnosed patients.)[53]
Another study, a review of randomized clinical trials, showed that intensive glycemic control reduces the risk of microvascular complications, but at the expense of increased risk of hypoglycemia. All-cause mortality and cardiovascular mortality in the study did not differ significantly with intensive versus conventional glycemic control;
however, trials conducted in usual-care settings showed a reduction in the risk of nonfatal myocardial infarction.[54]
Overall, these studies suggest that tight glycemic control (HbA1c < 7% or lower) is valuable for microvascular and macrovascular disease risk reduction in patients with recent-onset disease, no known cardiovascular diseases, and a longer life expectancy. In patients with known cardiovascular disease, a longer duration of diabetes (15 or more years), and a shorter life expectancy, however, tighter glycemic control is not as beneficial, particularly with regard to cardiovascular disease risk. Episodes of severe hypoglycemia may be particularly harmful in older individuals with poorer glycemic control and existing cardiovascular disease.
Vascular disease considerations
One prospective study with a long follow-up challenges the concept of coronary disease risk equivalency between nondiabetic patients with a first myocardial infarction and patients with type 2 diabetes but without any cardiovascular disease. The study found that patients with type 2 diabetes had lower long-term cardiovascular risk compared with patients with first myocardial infarction. Other studies have similarly questioned this risk equivalency.[55]
Patients with diabetes have a lifelong challenge to achieve and maintain blood glucose levels as close to the reference range as possible. With appropriate glycemic control, the risk of microvascular and neuropathic complications is decreased markedly. In addition, if hypertension and hyperlipidemia are treated aggressively, the risk of macrovascular complications decreases as well.
These benefits are weighed against the risk of hypoglycemia and the short-term costs of providing high-quality preventive care. Studies have shown cost savings due to a reduction in acute diabetes-related
complications within 1-3 years after starting effective preventive care. Some studies suggest that broad-based focus on treatment (eg, glycemia, nutrition, exercise, lipids, hypertension, smoking cessation) is much more likely to reduce the burden of excess microvascular and macrovascular events.
Yamasaki et al found that abnormal results on single-photon CT myocardial perfusion imaging in asymptomatic patients with type 2 diabetes indicated a higher risk for cardiovascular events (13%), including cardiac death. Smoking and low glomerular filtration rate were significant contributing factors.[56] However, an earlier study questioned the merit of routine screening with adenosine-stress radionuclide myocardial perfusion imaging (MPI) in otherwise asymptomatic type 2 diabetic patients (the Detection of Ischemia in Asymptomatic Diabetics [DIAD] study).[57]
Diabetes-associated mortality and morbidity
In 2009, diabetes mellitus was the seventh leading cause of death in the United States.[58] In addition, diabetes is a contributing cause of death in many cases, and it is probably underreported as a cause of death. Overall, the death rate among people with diabetes is about twice that of people of similar age but without diabetes.[3]
Diabetes mellitus causes morbidity and mortality because of its role in the development of cardiovascular, renal, neuropathic, and retinal disease. These complications, particularly cardiovascular disease (approximately 50-75% of medical expenditures), are the major sources of expenses for patients with diabetes mellitus.
The American Diabetes Association estimated that in 2007, direct medical costs due to diabetes in the United States were $116 billion, with another $58 billion in indirect costs (eg, disability, work loss, premature mortality). Approximately 1 in 5 health care dollars in the
United States was spent caring for someone with diagnosed diabetes, while 1 in 10 health care dollars was attributed to diabetes.[59]
Diabetic retinopathy
Diabetes mellitus is the major cause of blindness in adults aged 20-74 years in the United States; diabetic retinopathy accounts for 12,000-24,000 newly blind persons every year.[60] The National Eye Institute estimates that laser surgery and appropriate follow-up care can reduce the risk of blindness from diabetic retinopathy by 90%.[60]
End-stage renal disease
Diabetes mellitus, and particularly type 2 diabetes mellitus, is the leading contributor to end-stage renal disease (ESRD) in the United States.[60] According to the Centers for Disease Control and Prevention, diabetes accounts for 44% of new cases of ESRD.[3] In 2008, 48,374 people with diabetes in the United States and Puerto Rico began renal replacement therapy, and 202,290 people with diabetes were on dialysis or had received a kidney transplant.[60]
Neuropathy and vasculopathy
Diabetes mellitus is the leading cause of nontraumatic lower limb amputations in the United States, with a 15- to 40-fold increase in risk over that of the nondiabetic population. In 2006, about 65,700 nontraumatic lower limb amputations were performed related to neuropathy and vasculopathy.[60]
Cardiovascular disease
The risk for coronary heart disease (CHD) is 2-4 times greater in patients with diabetes than in individuals without diabetes. Cardiovascular disease is the major source of mortality in patients with type 2 diabetes mellitus. Approximately two thirds of people with
diabetes die of heart disease or stroke. Men with diabetes face a 2-fold increased risk for CHD, and women have a 3- to 4-fold increased risk.
Although type 2 diabetes mellitus, both early onset (< 60 y) and late onset (>60 y), is associated with an increased risk of major CHD and mortality, only the early onset type (duration >10 y) appears to be a CHD risk equivalent.[61]
In patients with type 2 diabetes mellitus, a fasting glucose level of more than 100 mg/dL significantly contributes to the risk of cardiovascular disease and death, independent of other known risk factors.[62] This is based on a review of 97 prospective studies involving 820,900 patients.
Adolescents with obesity and obesity-related type 2 diabetes mellitus demonstrate a decrease in diastolic dysfunction.[63] This suggests that they may be at increased risk of progressing to early heart failure compared with adolescents who are either lean or obese but do not have type 2 diabetes mellitus.
Cancer
A 2010 Consensus Report from a panel of experts chosen jointly by the American Diabetes Association and the American Cancer Society suggested that people with type 2 diabetes are at an increased risk for many types of cancer.[64] Patients with diabetes have a higher risk for bladder cancer.[65] Age, male gender, neuropathy, and urinary tract infections were associated with this risk.
Pregnancy outcome
Untreated gestational diabetes mellitus can lead to fetal macrosomia, hypoglycemia, hypocalcemia, and hyperbilirubinemia. In addition, mothers with gestational diabetes mellitus have increased rates of cesarean delivery and chronic hypertension.
Despite advanced age, multiparity, obesity, and social disadvantage, patients with type 2 diabetes were found to have better glycemic control, fewer large-for-gestational-age infants, fewer preterm deliveries, and fewer neonatal care admissions compared with patients with type 1 diabetes. This suggests that better tools are needed to improve glycemic control in patients with type 1 diabetes.[66] (For more information, see Diabetes Mellitus and Pregnancy.)
Patient Education
No longer is it satisfactory to provide patients who have diabetes with brief instructions and a few pamphlets and expect them to manage their disease adequately. Instead, education of these patients should be an active and concerted effort involving the physician, nutritionist, diabetes educator, and other health professionals. Moreover, diabetes education needs to be a lifetime exercise; believing that it can be accomplished in 1 or 2 encounters is misguided.
A randomized, controlled trial found that for patients with poorly controlled diabetes, individual attention and education is superior to group education.[67] Nonphysician health professionals are usually much more proficient at diabetes education and have much more time for this very important activity.
A systematic review suggested that patients with type 2 diabetes who have a baseline HbA1c of greater than 8% may achieve better glycemic control when given individual education rather than usual care. Outside that subgroup, however, the report found no significant difference between usual care and individual education. In addition, comparison of individual education with group education showed equal impact on HbA1c at 12-18 months.[68]
Patient education is an immensely complex topic, however. The clinical impression of most experts in the field is that there is merit in the provision of careful diabetes education at all stages of the disease.
Parasitism
From Wikipedia, the free encyclopedia
Jump to: navigation, search
"Parasite" redirects here. For other uses, see Parasite (disambiguation).
Brood parasitism is a form of parasitism
Parasitism is a type of non mutual relationship between organisms of different species where one organism, the parasite, benefits at the expense of the other, the host. Traditionally parasite referred to organisms with lifestages that needed more than one host (e.g. Taenia solium). These are now called macroparasites (typically protozoa and helminths). The word parasite now also refers to microparasites, which are typically smaller, such as viruses and bacteria, and can be directly transmitted between hosts of the same species [1]. Examples of parasites include the plants mistletoe and cuscuta, and organisms such as leeches.
Unlike predators, parasites are generally much smaller than their host; both are special cases of consumer-resource interactions.[2] Parasites show a high degree of specialization, and reproduce at a faster rate than their hosts. Classic examples of parasitism include interactions between vertebrate hosts and diverse animals such as tapeworms, flukes, the Plasmodium species, and fleas.
Parasitism is differentiated from the parasitoid relationship, though not sharply, by the fact that parasitoids generally kill or sterilise their hosts. Parasitoidism occurs in much the same variety of organisms that parasitism does.
The harm and benefit in parasitic interactions concern the biological fitness of the organisms involved. Parasites reduce host fitness in many ways, ranging from general or specialized pathology, such as parasitic castration and impairment of secondary sex characteristics, to the modification of host behaviour. Parasites increase their fitness by exploiting hosts for resources necessary for the parasite's survival, e.g. food, water, heat, habitat, and genetic dispersion.
Although the concept of parasitism applies unambiguously to many cases in nature, it is best considered part of a continuum of types of interactions between species, rather than an exclusive category. Particular interactions between species may satisfy some but not all parts of the definition. In many cases, it is difficult to demonstrate that the host is harmed. In others, there may be no apparent specialization on the part of the parasite, or the interaction between the organisms may be short-lived.
5 Ecology o 5.1 Quantitative ecology o 5.2 Diversity ecology
6 Adaptation o 6.1 Transmission o 6.2 Roles in ecosystems
7 Effects on host behavior 8 Value 9 See also 10 References 11 Further reading 12 External links
Etymology
First used in English 1539, the word parasite comes from the Medieval French parasite, from the Latin parasitus, the latinisation of the Greek παράσιτος (parasitos), "one who eats at the table of another"[3] and that from παρά (para), "beside, by"[4] + σῖτος (sitos), "wheat".[5] Coined in English in 1611, the word parasitism comes from the Greek παρά (para) + σιτισμός (sitismos) "feeding, fattening".[6]
Types
Parasites are classified based on their interactions with their hosts and on their life cycles.
Parasites that live on the surface of the host are called ectoparasites (e.g. some mites). Those that live inside the host are called endoparasites (including all parasitic worms). Endoparasites can exist in one of two forms: intercellular parasites (inhabiting spaces in the
host’s body) or intracellular parasites (inhabiting cells in the host’s body). Intracellular parasites, such as protozoa, bacteria or viruses, tend to rely on a third organism, which is generally known as the carrier or vector.[citation needed] The vector does the job of transmitting them to the host. An example of this interaction is the transmission of malaria, caused by a protozoan of the genus Plasmodium, to humans by the bite of an anopheline mosquito. Those parasites living in an intermediate position, being half-ectoparasites and half-endoparasites, are sometimes called mesoparasite.
An epiparasite is one that feeds on another parasite. This relationship is also sometimes referred to as hyperparasitism, exemplified by a protozoan (the hyperparasite) living in the digestive tract of a flea living on a dog.
Social parasites take advantage of interactions between members of social organisms such as ants or termites. In kleptoparasitism, parasites appropriate food gathered by the host. An example is the brood parasitism practiced by many species of cuckoo and cowbird, which do not build nests of their own but rather deposit their eggs in nests of other species and abandon them there. The host behaves as a "babysitter" as they raise the young as their own. If the host removes the cuckoo's eggs, some cuckoos will return and attack the nest to compel host birds to remain subject to this parasitism.[7] The cowbird’s parasitism does not necessarily harm its host’s brood; however, the cuckoo may remove one or more host eggs to avoid detection, and furthermore the young cuckoo may heave the host’s eggs and nestlings out of the nest.
Parasitism can take the form of isolated cheating or exploitation among more generalized mutualistic interactions. For example, broad classes of plants and fungi exchange carbon and nutrients in common mutualistic mycorrhizal relationships; however, some plant species
known as myco-heterotrophs "cheat" by taking carbon from a fungus rather than donating it.
Parasitoids are organisms whose larval development occurs inside or on the surface of another organism, resulting in the death of the host.[8]
This means that the interaction between the parasitoid and the host is fundamentally different from that of a true parasite and shares some of the characteristics of predation.
An adelpho-parasite is a parasite in which the host species is closely related to the parasite, often being a member of the same family or genus. An example of this is the citrus blackfly parasitoid, Encarsia perplexa, unmated females of which may lay haploid eggs in the fully developed larvae of their own species. These result in the production of male offspring.[9] The marine worm Bonellia viridis has a similar reproductive strategy, although the larvae are planktonic.[10]
Host defenses
This section requires expansion.
Hosts respond to parasitisms in many ways ranging from the morphological to the behavioural. In some cases, plants produce toxins to deter parasitic fungi and bacteria.[citation needed] Vertebrate animals have developed complex immune systems, which can target parasites through contact with bodily fluids.[citation needed] Animals are also known to resort to behavioral defenses, examples of which are the avoidance by sheep of open pastures during spring, when roundworm eggs accumulated over the previous year hatch en masse;[citation needed] and the ingestion of alcohol by infected fruit flies as self medication against blood-borne parasites.[11] In humans, parasite immunity is developed prominently by Immunoglobulin E antibodies.
Biotrophic parasitism is a common mode of life that has arisen independently many times in the course of evolution. Depending on the definition used, as many as half of all animals have at least one parasitic phase in their life cycles,[12] and it is also frequent in plants and fungi. Moreover, almost all free-living animals are host to one or more parasites taxa.[12]
Restoration of a Tyrannosaurus with parasite infections. A 2009 study showed that holes in the skulls of several specimens might have been caused by Trichomonas-like parasites[13]
Parasites evolve in response to the defense mechanisms of their hosts. As a result of host defenses, some parasites evolve adaptations that are specific to a particular host taxon, specializing to the point where they infect only a single species. Such narrow host specificity can be costly over evolutionary time, however, if the host species becomes extinct. Therefore many parasites can infect a variety of more or less closely related host species, with different success rates.
Host defenses also evolve in response to attacks by parasites. Theoretically, parasites may have an advantage in this evolutionary arms race because of their more rapid generation time. Hosts reproduce less quickly than parasites, and therefore have fewer chances to adapt than their parasites do over a given span of time.
In some cases, a parasite species may coevolve with its host taxa. Long-term coevolution sometimes leads to a relatively stable relationship tending to commensalism or mutualism, as, all else being equal, it is in the evolutionary interest of the parasite that its host thrives. A parasite may evolve to become less harmful for its host or a host may evolve to cope with the unavoidable presence of a parasite-- to the point that the parasite's absence causes the host harm. For example, although animals infected with parasitic worms are often clearly harmed, and therefore parasitized, such infections may also reduce the prevalence and effects of autoimmune disorders in animal hosts, including humans.[14]
Competition between parasites tends to favor faster reproducing and therefor more virulent parasites. Parasites whose life cycle involves the death of the host, to exit the present host and sometimes to enter the next, evolve to be more virulent or even alter the behavior or other properties of the host to make it more vulnerable to predators. Parasites that reproduce largely to the offspring of the previous host tend to become less virulent or mutualist, so that its hosts reproduce more effectively.[1]
The presumption of a shared evolutionary history between parasites and hosts can sometimes elucidate how host taxa are related. For instance, there has been dispute about whether flamingos are more closely related to the storks and their allies, or to ducks, geese and their relatives. The fact that flamingos share parasites with ducks and geese is evidence these groups may be more closely related to each other than either is to storks.
Parasitism is part of one explanation for the evolution of secondary sex characteristics seen in breeding males throughout the animal world, such as the plumage of male peacocks and manes of male lions. According to this theory, female hosts select males for breeding based
on such characteristics because they indicate resistance to parasites and other disease.
Co-speciation
In rare cases, a parasite may even undergo co-speciation with its host. One particularly remarkable example of co-speciation exists between the simian foamy virus (SFV) and its primate hosts. In one study, the phylogenies of SFV polymerase and the mitochondrial cytochrome oxidase subunit II from African and Asian primates were compared.[15] Surprisingly, the phylogenetic trees were very congruent in branching order and divergence times. Thus, the simian foamy viruses may have co-speciated with Old World primates for at least 30 million years.
Ecology
Quantitative ecology
A single parasite species usually has an aggregated distribution across host individuals, which means that most hosts harbor few parasites, while a few hosts carry the vast majority of parasite individuals. This poses considerable problems for students of parasite ecology: the use of parametric statistics should be avoided.[citation needed] Log-transformation of data before the application of parametric test, or the use of non-parametric statistics is recommended by several authors. However, this can give rise to further problems.[16] Therefore, modern day quantitative parasitology is based on more advanced biostatistical methods.
Diversity ecology
Hosts represent discrete habitat patches that can be occupied by parasites. A hierarchical set of terminology has come into use to describe parasite assemblages at different host scales.
All the parasites of one species in a single individual host.
Metapopulation
All the parasites of one species in a host population.
Infracommunity
All the parasites of all species in a single individual host.
Component community
All the parasites of all species in a host population.
Compound community
All the parasites of all species in all host species in an ecosystem.
The diversity ecology of parasites differs markedly from that of free-living organisms. For free-living organisms, diversity ecology features many strong conceptual frameworks including Robert MacArthur and E. O. Wilson's theory of island biogeography, Jared Diamond's assembly rules and, more recently, null models such as Stephen Hubbell's unified neutral theory of biodiversity and biogeography. Frameworks are not so well-developed for parasites and in many ways they do not fit the free-living models. For example, island biogeography is predicated on fixed spatial relationships between habitat patches ("sinks"), usually with reference to a mainland ("source"). Parasites inhabit hosts, which represent mobile habitat patches with dynamic spatial relationships. There is no true "mainland" other than the sum of hosts (host population), so parasite component communities in host populations are metacommunities.
Nonetheless, different types of parasite assemblages have been recognized in host individuals and populations, and many of the patterns observed for free-living organisms are also pervasive among parasite assemblages. The most prominent of these is the interactive-isolationist continuum. This proposes that parasite assemblages occur along a cline from interactive communities, where niches are saturated and interspecific competition is high, to isolationist communities, where there are many vacant niches and interspecific interaction is not as important as stochastic factors in providing structure to the community. Whether this is so, or whether community patterns simply reflect the sum of underlying species distributions (no real "structure" to the community), has not yet been established.
Adaptation
Parasites infect hosts that exist within their same geographical area (sympatric) more effectively. This phenomenon supports the "Red Queen hypothesis—which states that interactions between species (such as host and parasites) lead to constant natural selection for adaptation and counter adaptation."[17] The parasites track the locally common host phenotypes, therefore the parasites are less infective to allopatric (from different geographical region) hosts.[citation needed]
Experiments published in 2000 discuss the analysis of two different snail populations from two different sources- Lake Ianthe and Lake Poerua in New Zealand. The populations were exposed to two pure parasites (digenetic trematode) taken from the same lakes. In the experiment, the snails were infected by their sympatric parasites, allopatric parasites and mixed sources of parasites. The results suggest that the parasites were more highly effective in infecting their sympatric snails than their allopatric snails. Though the allopatric snails were still infected by the parasites, the infectivity was much less when
compared to the sympatric snails. Hence, the parasites were found to have adapted to infecting local populations of snails.[17]
Transmission
Life cycle of Entamoeba histolytica, an anaerobic parasitic protozoan.
Parasites inhabit living organisms and therefore face problems that free-living organisms do not. Hosts, the only habitats in which parasites can survive, actively try to avoid, repel, and destroy parasites. Parasites employ numerous strategies for getting from one host to another, a process sometimes referred to as parasite transmission or colonization.
Some endoparasites infect their host by penetrating its external surface, while others must be ingested. Once inside the host, adult endoparasites need to shed offspring into the external environment to infect other hosts. Many adult endoparasites reside in the host’s gastrointestinal tract, where offspring can be shed along with host excreta. Adult stages of tapeworms, thorny-headed worms and most flukes use this method.
Among protozoan endoparasites, such as the malarial parasites and trypanosomes, infective stages in the host’s blood are transported to new hosts by biting-insects, or vectors.
Larval stages of endoparasites often infect sites in the host other than the blood or gastrointestinal tract. In many such cases, larval endoparasites require their host to be consumed by the next host in the parasite’s life cycle in order to survive and reproduce. Alternatively, larval endoparasites may shed free-living transmission stages that migrate through the host’s tissue into the external environment, where they actively search for or await ingestion by other hosts. The foregoing strategies are used, variously, by larval stages of tapeworms, thorny-headed worms, flukes and parasitic roundworms.
Some ectoparasites, such as monogenean worms, rely on direct contact between hosts. Ectoparasitic arthropods may rely on host-host contact (e.g. many lice), shed eggs that survive off the host (e.g. fleas), or wait in the external environment for an encounter with a host (e.g. ticks). Some aquatic leeches locate hosts by sensing movement and only attach when certain temperature and chemical cues are present.
Some parasites modify host behavior to make transmission to other hosts more likely. For example, in California salt marshes, the fluke Euhaplorchis californiensis reduces the ability of its killifish host to avoid predators.[18] This parasite matures in egrets, which are more likely to feed on infected killifish than on uninfected fish. Another example is the protozoan Toxoplasma gondii, a parasite that matures in cats but can be carried by many other mammals. Uninfected rats avoid cat odors, but rats infected with T. gondii are drawn to this scent, which may increase transmission to feline hosts.[19]
Roles in ecosystems
Modifying the behavior of infected hosts, to make transmission to other hosts more likely to occur, is one way parasites can affect the structure of ecosystems. For example, in the case of Euhaplorchis californiensis (discussed above) it is plausible that the local predator
and prey species might be different if this parasite were absent from the system.
Although parasites are often omitted in depictions of food webs, they usually occupy the top position. Parasites can function like keystone species, reducing the dominance of superior competitors and allowing competing species to co-exist.
Many parasites require multiple hosts of different species to complete their life cycles and rely on predator-prey or other stable ecological interactions to get from one host to another. In this sense, the parasites in an ecosystem reflect the "health" of that system.
Effects on host behavior
Animal behavior is typically motivated by proximate level mechanisms that promote particular actions. In most cases, proximate level mechanisms are a result of the individual’s interaction with the environment but some parasites have been shown to interact and manipulate these mechanisms to produce behaviors beneficial to the parasite alone. Parasites are known to drastically affect how animals behave. [20] Parasites most commonly target the central nervous system (CNS) in order to alter animal behavior. By affecting hormone secretions or by physical restructuring, parasites successfully change how an animal’s body functions and delivers, interprets and and reacts to messages. Some parasites, like toxoplasma, form vacuoles that travel through the nervous system interrupting key functions in intraneural communications. The emerald jewel wasp alters behavior through the injection of venom directly into the host’s brain, causing hypokinesia. [21] Parasitic life cycles can have the capacity to infect a singular host or a series of hosts. Direct life cycles are related to a single host while indirect life cycles, or complex life cycles, rely on a series of intermediate hosts in order to complete the life cycle. Indirect life cycles likely arose in order to increase the efficiency of spreading to
new hosts. By using intermediary’s the parasite DNA can spread to several hosts instead of remain concentrated within a single host, therefore promising a higher likelihood of DNA continuation. In some cases, intermediary hosts are accidental. [22]
Toxoplasma gondii is a noted case of unintended intermediary hosts. Typically, Toxoplasma infects animals from the Felidae family and oocysts are shed with the feces. When rodents consume the fecal matter, they become infected themselves and the parasite begins to alter their behavior. Rodents become more extroverted and less fearful of felines. Toxoplasma, however, has begun to infect humans. In doing so, human behavior has been altered in similar ways to rodents. Further, Toxoplasma has been linked to cases of schizophrenia. [23]
The emerald jewel wasp (Ampulex compressa) takes advantage of its host, the American cockroach (Periplaneta americana) specifically as a food source and home for its growing larvae. The wasp begins by injecting venom into the brain which paralyses the central nervous system system of the cockroach and puts it into a state of “hypokinesia”. “Hypokinesia...is a reversible long-term lethargy characterized by lack of spontaneous movement or response to external stimuli,” (Banks and Adams). After dragging the cockroach to a burrow, the wasp deposits an egg into its carcass, burying it for the growing larvae to feed off until it emerges in 6 weeks, leaving nothing but a hard outer cockroach shell. [24] Although the circuitry in control of movement is functional, the nervous system acts from a depressed state. They are not killed by this hypokinesia, but would recover if not for the larvae eating them from the inside out. The movement is controlled by dopamine and octopamine which affect transmission of interneurons involved in the natural response to escape. Reduced motor activity results from a reduction of these amines. [25]
Although parasites are generally considered to be harmful, the eradication of all parasites would not necessarily be a noble aim. Among other things, parasites may account for as much as or more than half of life's diversity; they perform an important ecological role (by weakening prey) that ecosystems would take some time to adapt to; and without parasites organisms may eventually tend to asexual reproduction, dinimishing the diversity of sexually dimorphic traits.[26] Parasites provide an opportunity for the transfer of genetic material between species. On rare but significant occasions this may provide a path for evolutionary changes that would not otherwise occur, or that would otherwise take even longer.[1]
*******
Parasitism
From Wikipedia, the free encyclopedia
Jump to: navigation, search
Parasitism is a form of symbiosis. It means that a parasite is any organism or living thing that benefits from another creature's harm. In other words, the parasites harm the host organism while the parasite benefits. A parasitic relationship is the opposite of a mutualistic relationship.[1] Examples of parasites in humans include tapeworms and leeches. World-wide, the most serious cause of human death by a parasite is malaria. A definition:
A parasite is an organism living in or on another living organism, obtaining from it part or all of its food. It usually shows some degree of adaptive modification, and causes some degree of damage to its host.[2]
1 Biological context 2 Terminology of parasitism 3 Ecology
o 3.1 Dispersal and reproduction o 3.2 Parasites are highly specialised o 3.3 Complex life cycles
4 Evolution o 4.1 Rapid speciation o 4.2 Adaptive radiation o 4.3 More time, more species o 4.4 Selection for co-evolution o 4.5 Sympatric speciation
5 References
Biological context
When the above definition is applied, many organisms which eat plants can be seen as parasites, because they feed largely or wholly on one individual plant. Examples would include many herbivorous insects: the Hemiptera or true bugs (leafhoppers, froghoppers, aphids, scale insects and whiteflies). The larvae of Lepidoptera usually feed and mature on a single individual of the host plant species, and what they eat accounts for most of the food for their complete life span. Moreover, caterpillars can and often do serious damage to the host's foliage. Other orders also have many parasitic herbivores: Thysanoptera (thrips), Coleoptera (beetles), Diptera (flies).
Parasites of larger animals account for much research done for veterinarian and medical purposes. These parasites include viruses, bacteria, protozoa, flatworms (flukes and tapeworms), nematodes (roundworms), arthropods (crustacea, insects, mites). Parasitic wasps and flies are of great interest to the entomologist, and may be used in biological control.
On the other hand, many blood-sucking insects (such as mosquitoes) have only brief contact with a host, and so perhaps should not be regarded as parasites.[3]p5
A huge number of species are parasitic. A survey of the feeding habits of British insects showed that about 35% were parasites on plants, and slightly more were parasites on animals.[4] That means that nearly 71% of insects in Britain are parasitic. Since British insects are better known than those elsewhere (because of the length of time they have been studied), this means that the majority of insect species throughout the world are parasitic. Also, there are several other invertebrate phyla which are wholly or largely parasitic. Flatworms and roundworms are found in virtually every wild species of vertebrate. Protozoan parasites
are also ubiquitous.[5] Hence parasitism is almost certainly the most common feeding method on Earth.
"It is clear that parasitism as a way of life is more common than all other feeding strategies combined".[3]p8
Terminology of parasitism
Ectoparasites live on the outside of a plant or animal. Endoparasites live inside a plant or animal. Intracellular parasites
live inside cells; Intercellular parasites live in the spaces between cells.
Parasitoids are organisms whose larval development takes place within another organism's body, resulting in the death of the host. There are twelve Superfamilies of wasps which are entirely or mainly parasitoid, such as the ichneumonoid wasps, whose species number over 80,000. The interaction between the parasitoid and the host is fundamentally different from true parasites and their host, and shares some characteristics with predation.
A vector is a third party that carries the parasite to the host. Thus, with malaria, the mosquito is the vector, the sporozoite protozoan is the parasite, and the mammal is the host.
An epiparasite is one that feeds on another parasite. Kleptoparasites steal food from other species. Brood parasites (such as the Cuckoo) induce other species to raise
their young. The Cowbird is another brood parasite. Social parasites take advantage of interactions between members
Parasites are adapted to small, separated habitats. For a parasite, each host is an island surrounded by a hostile environment.[6] For a small organism, the distances between hosts, or groups of hosts, is a hazard. Adaptations to bridge this hazard are:
Mass production of spores or eggs. Dispersal of fertile females. Dispersal by attaching to a larger organism (many ectoparasites). Extreme longevity of resting stages (spores or cysts). For example,
plant parasitic nematodes may remain quiescent for 23 years.[7]
Parthenogenesis , and inbreeding among offspring of a single female, are common in parasites.
So parasites exist in small, genetically similar groups with little flow of genes between them. In consequence, they have adaptations to solve their problems of dispersal and reproduction.[3]
Parasites are highly specialised
Parasites face an environment which varies in time and space. Consequently, both local (geographic) races and polymorphism occur. Both may occur in the same species. Parasites are very specialised feeders: many species have only one host at any stage of their life cycle. A few use more than two host species.[3]
Complex life cycles
Many parasites have complex life-cycles. Tremadodes, the flukes, are a parasitic class of flatworms (Platyhelminths), with over 20,000 species. Most of them infect molluscs in the first part of the life-cycle, and vertebrates in the second part. The biology of scrub typhus is even more complex. It involves these factors:[8]
5. Humans passing through patches where the above are present.
The occurrence of all these factors together would be limited in space, and brief in time. This is typical of the ecology of parasitic infections.
Evolution
Rapid speciation
Both evolutionary rates and speciation rates can be high. Sibling species are very common in the bug Erythroneura, in which about 150 transfers from one host to another has resulted in about 500 species in the genus.[9]
The clearest evidence comes from the large size of many parasitic families.
"Even though some parasitic taxa evolved much later than predatory taxa, families of parasites on plants are on average almost eight times larger than those of predators, and families of parasites on animals are over ten times larger".[3]p26
Sometimes there is good evidence of the speed of speciation. For example, five or more species of the moth Hedylepta must have evolved within 1000 years in Hawaii, because they are specific to banana, which was only introduced then.[10]
Adaptive radiation in parasites is extensive. Its development in each taxon (group) depends on:
The diversity of the hosts. How many species there are in the group being parastised, and how different they are from each other.
The size of the host target: body size, population, geographical distribution.
The evolutionary time available for colonisation of hosts.
The selective pressure for evolutionary modification.
Diversity of hosts is a big factor. If many related species of host are available, then many related species of parasite will evolve. Mites on Lepidoptera families or fleas on mammals and birds are good examples. Eichler's rule goes as follows:
"When a large group of hosts consisting of a wide variety of species is compared with an equivalent group consisting of few representatives, the larger group has the greater diversity of parasitic fauna".[11]
The two British oaks support some 439 species of parasite directly, and indirectly many hundred more which parasitise these parasites. "It would certainly be an underestimate to say that the two British species of oak are the primary products for a thousand species of parasite".[3]p28 Obviously, the large size of these trees is a factor in the number of parasite species. In general, this holds whether the host is a plant or an animal. A larger bird will harbour more species of ectoparasite than a small bird.
One of the reasons large trees have so many parasites is that they may have lived a long time in a particular area compared with other types of plant. They have had longer to accumulate parasites.
Parasites can be most useful in sorting out the phylogenetic relationships of their hosts. Sibling host species have been discovered when their parasites diverged. Common ancestors of present-day parasites were themselves parasites of the common ancestors of present-day hosts.
Selection for co-evolution
As the host evolves defences, so the parasite evolves to cope with this. Compare two families of host plants, the Umbellifers (fennel, cumin, parsley, hemlock) and the Graminae (grasses). The umbellifers have many aromatic species, and are chemically diverse and pharmaceutically interesting. Their resins and oils are defences against herbivory and parasitism. On the other hand, grasses have one big defence to herbivores: their stony inclusions in their cells wear down the teeth of herbivorous mammals, but they have few chemical defences. Both families are attacked by leaf-miner flies. There are four times as many grass species as there are umbellifers, but there are twice as many leaf-miner species on the umbellifers.
"This is apparently because the chemical diversity of potential hosts within the Umbelliferae has forced specialisation of the parasites. Eighty-two percent of the species of leaf-miner attack only one genus each".[3]
This is speciation which does not require geographical isolation. Ernst Mayr, the chief exponent of geographical speciation, admitted that host races of phytophagous animals "constitute the only known case indicating the possible occurrence of incipient sympatric speciation".[12]