SECLUSION AND RESTRAINTS IN EMERGENCY PSYCHIATRY Dr Tuti Iryani Mohd Daud Senior Lecturer & Psychiatrist, National University of Malaysia Medical Centre. Seclusion and restraints in emergency psychiatry by Tuti Mohd Daud is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
Transcript
SECLUSION AND RESTRAINTS IN
EMERGENCY PSYCHIATRYDr Tuti Iryani Mohd Daud
Senior Lecturer & Psychiatrist, National University of Malaysia Medical Centre.
Seclusion and restraints in emergency psychiatry by Tuti Mohd Daud is licensed under a Creative Commons Attribution-NonCommercial 4.0
Explain the principles of seclusion and restraints
Discuss the indications, advantages & disadvantages of various types of restraints
Explain ethical issues related to seclusion and restraints
Explain ways that seclusion and restraints can be reduced
Trigger
Escalation phase
Crisis phase
Recovery phase
Post-crisis depression
phase
CYCLE OF ASSAULT (Kaplan & Wheeler,1983)
Perceived as serious threat
body and mind prepare for a fight.
Violent act
body and mind relaxes
fatigue, depression, and
guilt.
Source: Wolf,K & Knight,M. The Assault Cycle and Verbal Diffusion Handout. Retrieved from http://www.ala.org/pla/sites/ala.org.pla/files/content/onlinelearning/webinars/Assault_Cycle_Rev.pdf
“A set of physical skills to help separate or break away from an aggressor in a safe manner. They
do not involve the use of restraint.”
(NICE, 2015)
Reference:
NICE (2015). NICE Guideline: Violence and aggression: short-term management in mental health, health and community settings. Retrieved from http://www.nice.org.uk/guidance/ng10
“Use of medication by the parenteral route (usually intramuscular or, exceptionally,
intravenous) if oral medication is not possible or appropriate and urgent sedation with
medication is needed.”
(NICE, 2015)Reference:
NICE (2015). NICE Guideline: Violence and aggression: short-term management in mental health, health and community settings. Retrieved from http://www.nice.org.uk/guidance/ng10
• availability of I.M., liquid, or rapidly dissolving formulation
• patient’s history of response to the medication
• limited liability for side effects
• patient preference
• ease of administration
(no need for laboratory tests and simple dosing requirements)
PROPERTIES
References:Allen, M. H., et al. (2005). "The expert consensus guideline series. Treatment of behavioral emergencies 2005." Journal of Psychiatric Practice 11 Suppl 1: 5-108; quiz 110-102.
From: Neurobiology of Aggression and Violence American Journal of Psychiatry
Figure 5. Posttreatment Abnormalities in the Pathophysiology of Aggression
“the supervised confinement of a patient in a room, which may be locked.
Its sole aim is to contain severely disturbed behaviour that is likely to cause harm to others”
(Department of Health, 2015)
Reference:
Department of Health (2015). Mental Health Act 1983 Code of Practice. Surrey: The Stationery Office: Surrey. Retrieved from https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/435512/MHA_Code_of_Practice.PDF
“A skilled, hands-on method of physical restraint used by trained healthcare professionals to
prevent service users from harming themselves, endangering others or compromising the
therapeutic environment. Its purpose is to safely immobilise the service user.”
Reference:
NICE (2015). NICE Guideline: Violence and aggression: short-term management in mental health, health and community settings. Retrieved from http://www.nice.org.uk/guidance/ng10
“A method of physical intervention involving the use of authorised equipment, for example
handcuffs or restraining belts, applied in a skilled manner by designated healthcare”
(NICE, 2015)
Reference:
NICE (2015). NICE Guideline: Violence and aggression: short-term management in mental health, health and community settings.
Physical restraints should be used as the last resort
(Allen et al. ,2003)
Reference: Allen, M. H. M., et al. (2003). "Treatment of Behavioral Emergencies: A Summary of the Expert Consensus Guidelines." Journal of Psychiatric Practice 9(1): 16-38.
RISKSPatients
dehydration
rhabdomyolysis
lactic acidosis
sudden death
Staff
Injury
psychological distress
References: Stewart D, Bowers L, Simpson A, Ryan C & Tziggili M (2009). Manual restraint of adult psychiatric inpatients: a literature review. Journal of Psychiatric and Mental Health Nursing 16 pp 749-757. Stubbs B, Leadbetter D, Paterson B, Yorston G, Knight C & Davis S (2009). Physical intervention: a review of the literature on its use, staff and patient views, and the impact of training. Journal of Psychiatric and Mental Health Nursing, 16, pp 99- 105.
• Safety of staff
• Minimum period of time
• Seclusion or restraint is justifiable proportional to patient’s behaviour
• Least restrictive
• Close monitoring
PRINCIPLES OF SECLUSION & RESTRAINT
• breathing • behaviour • skin colour • care for the patient’s head and airway • ensure no pressure is applied to the neck,
thorax, abdomen or pelvic area
MONITOR
ETHICAL ISSUES
Human rights (autonomy)
Abused:
used as punishment to patients
staff’s convenience
References: Hay D, Cromwell R. Reducing the use of full-leather restraints on an acute adult inpatient ward. Hospital and Community Psychiatry 1980; 31: 198-200.Moosa, M. and F. Jeenah (2009). "The use of restraints in psychiatric patients." South African Journal of Psychiatry 15(3): 72-75.
Photo: Minas, H. and H. Diatri (2008). "Pasung: Physical restraint and confinement of the mentally ill in the community.” International Journal of Mental Health Systems 2(1): 8.
Pasung: ”physical restraint or confinement of criminals, crazy and dangerously aggressive people." (Broch, 2001 cited in Minas &
Diatri, 2008)
• Minas & Diatri (2008) • location: Samosir Island, Sumatra • duration 6 months • 15 cases • Pasung was built by family
members • duration of pasung: 2-21 years • diagnosis: Schizophrenia, dementia,
epilepsy • Main reason for pasung: prevent
harm to others and ill person • Treatment was not affordable
Iron shackles are fixed to the wooden floor of a hut in which the person is confined.
This man has his ankles in wooden stocks
Photo: Minas, H. and H. Diatri (2008). "Pasung: Physical restraint and confinement of the mentally ill in the community.”International Journal of Mental Health Systems 2(1): 8.
HOW TO APPROACH THE AGITATED PATIENT
Medical assessment: • identifying any medical conditions (delirium: underlying etiology)
• vital signs and a medical history, perform a visual examination of the patient, a urine toxicology screen, a cognitive examination, and a pregnancy test if the patient is a woman of childbearing age.
• head trauma, respiration, heart rhythm, color, smell of alcohol, diameter/reactivity of pupils, lacerations, nuchal rigidity, and fractures
• glucometry and urine for toxicology.
Psychiatric assessment
• brief assessment leading to a general category of diagnosis
References:Allen, M. H., et al. (2005). "The expert consensus guideline series. Treatment of behavioral emergencies 2005." Journal of Psychiatric Practice 11 Suppl 1: 5-108; quiz 110-102.
INITIAL ASSESSMENT
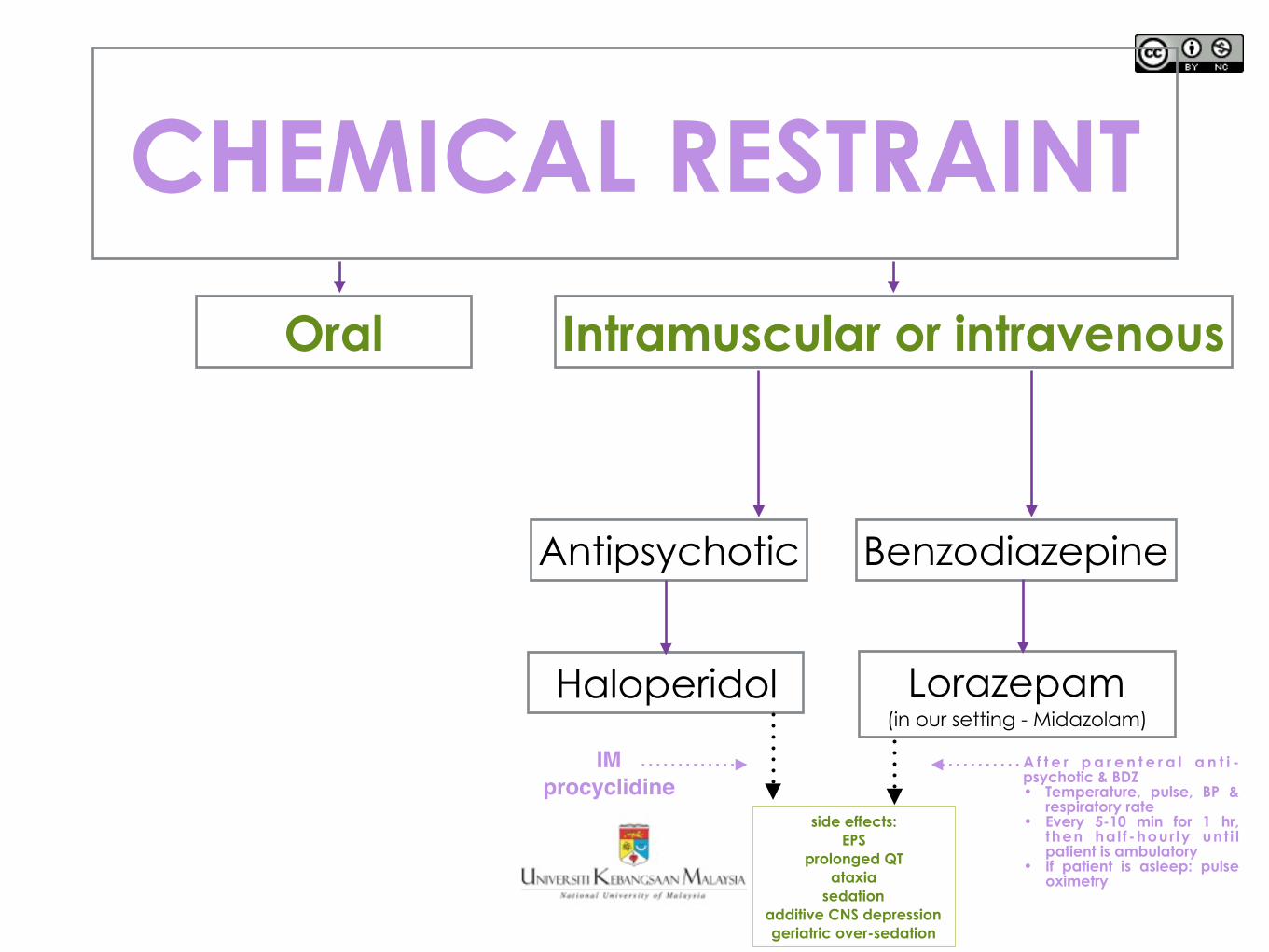
No additional information is available: Patient is willing to take oral medication: lorazepam, risperidone, olanzapine, haloperidol, quetiapine. (Allen, 2005) (our setting: lorazepam, risperidone, olanzapine)
If I.M. medication is needed before assessment can be done: I.M. lorazepam, with I.M. ziprasidone, olanzapine, and haloperidol. (our setting: IM Midazolam + IM Haloperidol)
Patient continues to be violent and extremely agitated while in restraints
•parenteral medication + restraints
•Not appropriate to leave such a patient unmedicated in restraints
•The goal in this situation is to use medication to reduce time in and complications of restraints.
References:Allen, M. H., et al. (2005). "The expert consensus guideline series. Treatment of behavioral emergencies 2005." Journal of Psychiatric Practice 11 Suppl 1: 5-108; quiz 110-102.
MANAGEMENT
Source:Knox, D. K. and G. H. Holloman (2012). "Use and Avoidance of Seclusion and Restraint: Consensus Statement of the American Association for Emergency Psychiatry Project BETA Seclusion and Restraint Workgroup." Western Journal of Emergency Medicine 13(1): 35-40.
Recommended algorithm for seclusion and restraint (Knox and Holloman, 2012)
REDUCING SECLUSION & RESTRAINTS
All level (policy, infrastructure, training, attitude)
• Timely and comprehensive assessments of patients. • earlier intervention with appropriate treatment can avoid behavioral
emergencies
• Decide whether restraint is contraindicated or must be used with caution.
• Training of staff (i.e. de-escalation and crisis management skills)
• Restraints as extraordinary event and use should be limited • Dignity of patients should be protected, e.g. regular personal
hygiene, bathroom, exercise, nutritional and fluid breaks.
References: Currier, G. W. M. M. (2003). "The Controversy over "Chemical Restraint" in Acute Care Psychiatry." Journal of Psychiatric Practice 9(1): 59-70. Moosa, M. and F. Jeenah (2009). "The use of restraints in psychiatric patients." South African Journal of Psychiatry 15(3): 72-75. SCANLAN, J. N. (2009). "Interventions to reduce the use of seclusion and restraint in inpatient psychiatric settings: what we know so far. A review of the literature." International
Journal of Social Psychiatry.
Before discharge: discuss experience with patients
encourage to ask questions give patients (and family) information about prescribed
medications
References:Allen, M. H., et al. (2005). "The expert consensus guideline series. Treatment of behavioral emergencies 2005." Journal of Psychiatric Practice 11 Suppl 1: 5-108; quiz 110-102.
minimize negative impact on: the therapeutic relationship
the person’s willingness to seek use mental health service
SUMMARY• The purpose of restraint is to ensure safety for the
patient, staff and others
• There are several type of restraints, each has its advantages and disadvantages
• Seclusion and restraint should be used judiciously
• Preventative measures for seclusion and restraint i.e. de-escalation technique
Seclusion and restraints in emergency psychiatry by Tuti Mohd Daud is licensed under a Creative Commons Attribution-NonCommercial 4.0