Secretory Phospholipase A2: A New Risk Factor and Soon a New Target of Therapy Rabih R. Azar, MD, MSc, FACC Associate Professor of Medicine Division of Cardiology Hotel Dieu de France Saint Joseph University
Transcript
Secretory Phospholipase A2: A New Risk Factor and Soon a New Target of
Therapy
Rabih R. Azar, MD, MSc, FACCAssociate Professor of Medicine
Division of CardiologyHotel Dieu de France
Saint Joseph University
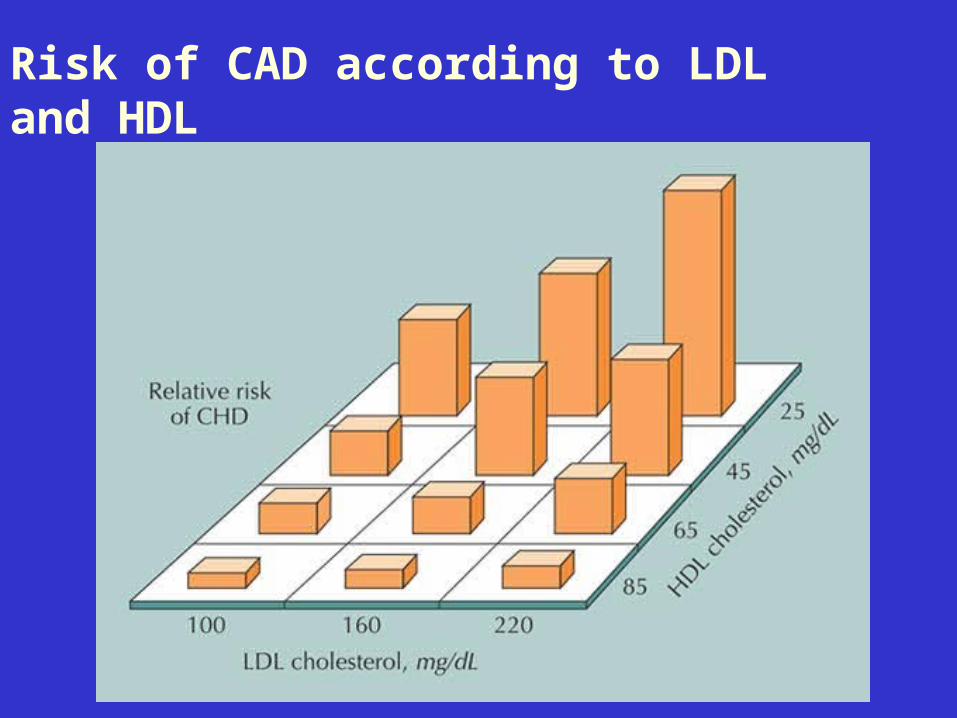
Risk of CAD according to LDL and HDL
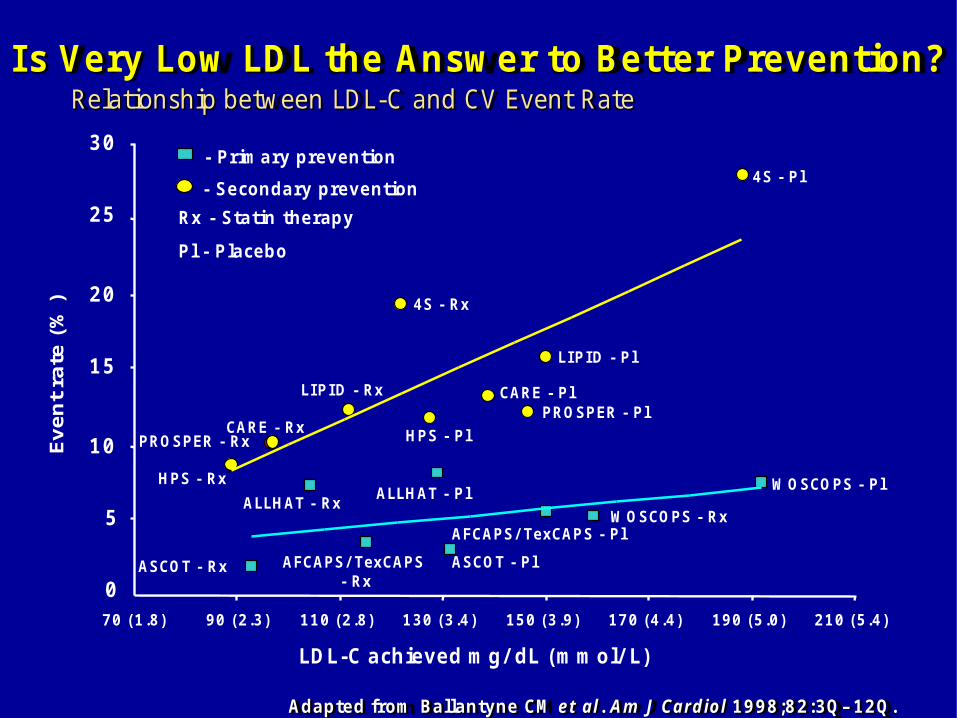
Relationship between LDL-C and CV Event Rate
Adapted from Ballantyne CM et al. Am J Cardiol 1998;82:3Q– 12Q.
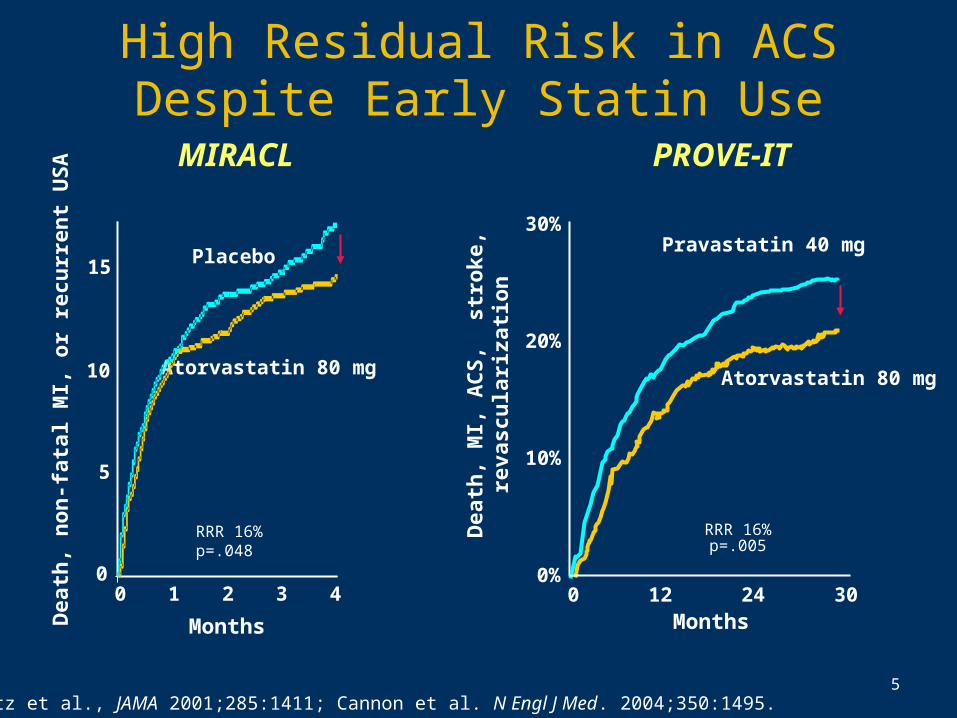
Schwartz et al., JAMA 2001;285:1411; Cannon et al. N Engl J Med. 2004;350:1495.
Atorvastatin 80 mg
Placebo
0
5
10
15
0 1 2 3 4
RRR 16%p=.048
Dea
th, n
on
-fat
al M
I, o
r re
curr
ent
US
A
Months
Atorvastatin 80 mg
Months
Dea
th, M
I, A
CS
, st
roke
,re
vasc
ula
riza
tio
n
Pravastatin 40 mg
RRR 16%p=.005
30%
20%
10%
0%0 12 24 30
High Residual Risk in ACS Despite Early Statin Use
IS LDL CHOLESTEROL THE “ONLY” PLAYER IN ATHEROSCLEROSIS?
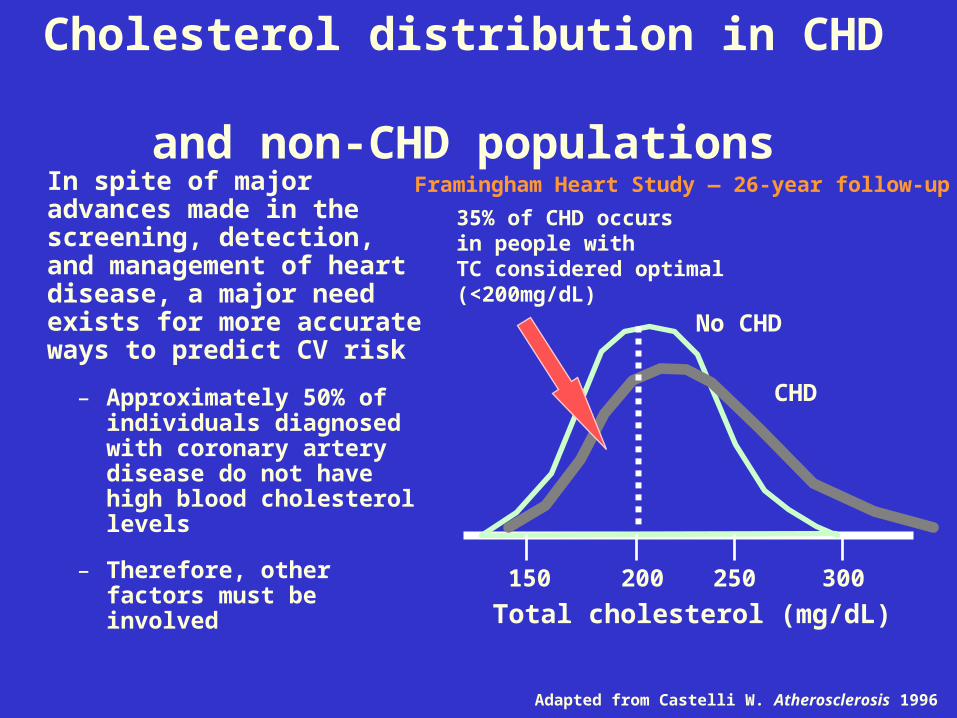
Cholesterol distribution in CHD and non-CHD populations
In spite of major advances made in the screening, detection, and management of heart disease, a major need exists for more accurate ways to predict CV risk
– Approximately 50% of individuals diagnosed with coronary artery disease do not have high blood cholesterol levels
– Therefore, other factors must be involved
35% of CHD occurs in people with TC considered optimal (<200mg/dL)
Adapted from Castelli W. Atherosclerosis 1996
Framingham Heart Study — 26-year follow-up
150 200
No CHD
Total cholesterol (mg/dL)250 300
CHD
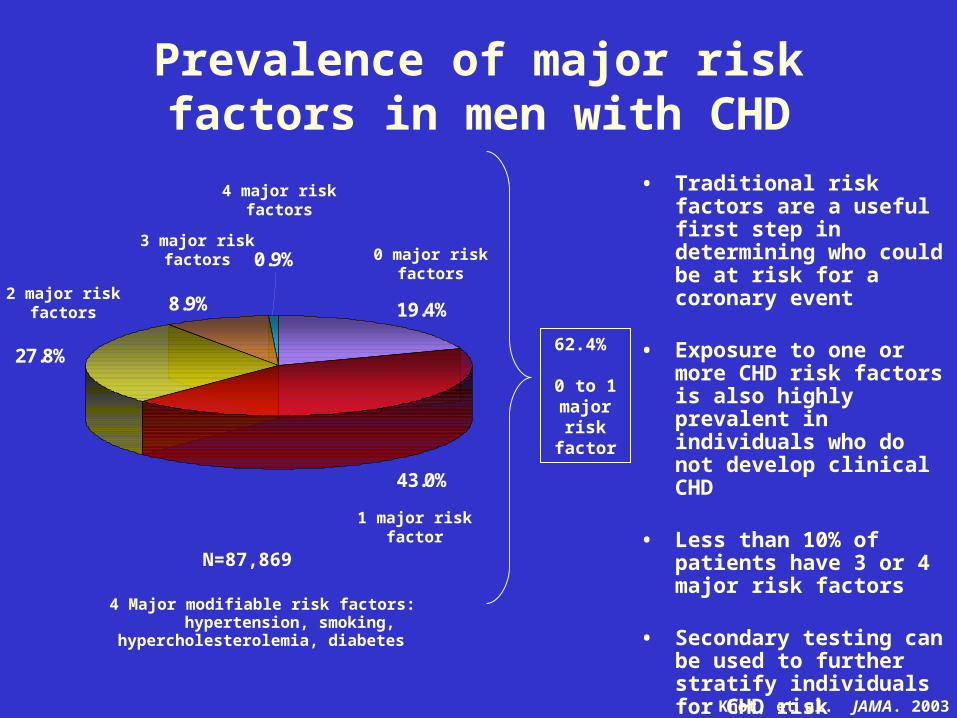
19.4%8.9%
43.0%
0.9%
27.8%
1 major risk factor
0 major risk factors
2 major risk factors
3 major risk factors
4 major risk factors
62.4% 0 to 1
major risk
factor
N=87,869
4 Major modifiable risk factors: hypertension, smoking,
hypercholesterolemia, diabetes
• Traditional risk factors are a useful first step in determining who could be at risk for a coronary event
• Exposure to one or more CHD risk factors is also highly prevalent in individuals who do not develop clinical CHD
• Less than 10% of patients have 3 or 4 major risk factors
• Secondary testing can be used to further stratify individuals for CHD risk
Prevalence of major risk factors in men with CHD
Khot, et al. JAMA. 2003
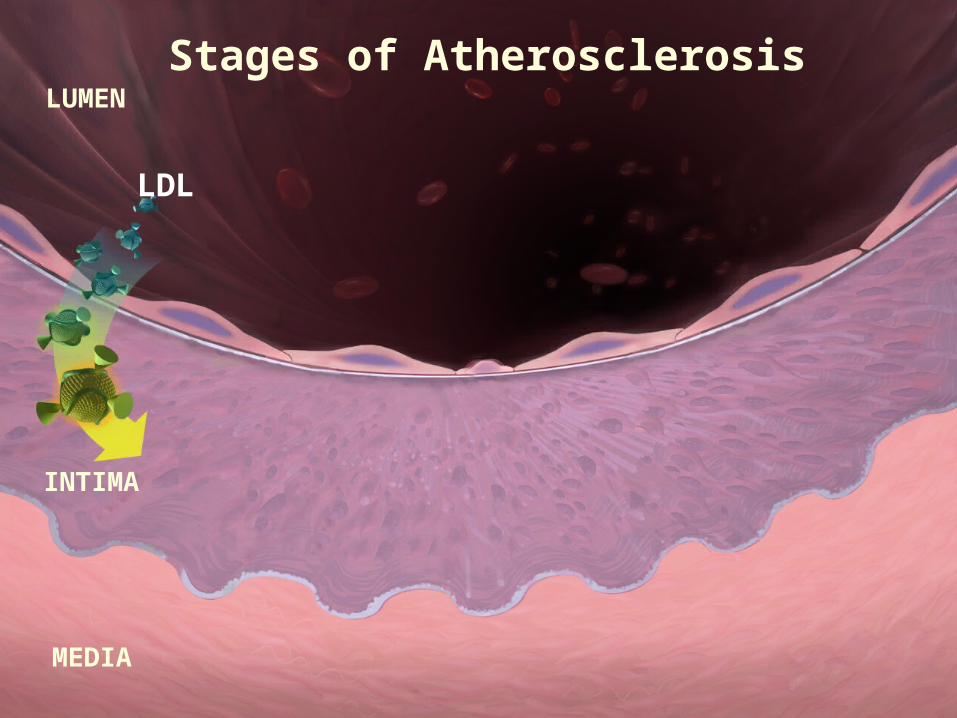
LUMEN
MEDIA
INTIMA
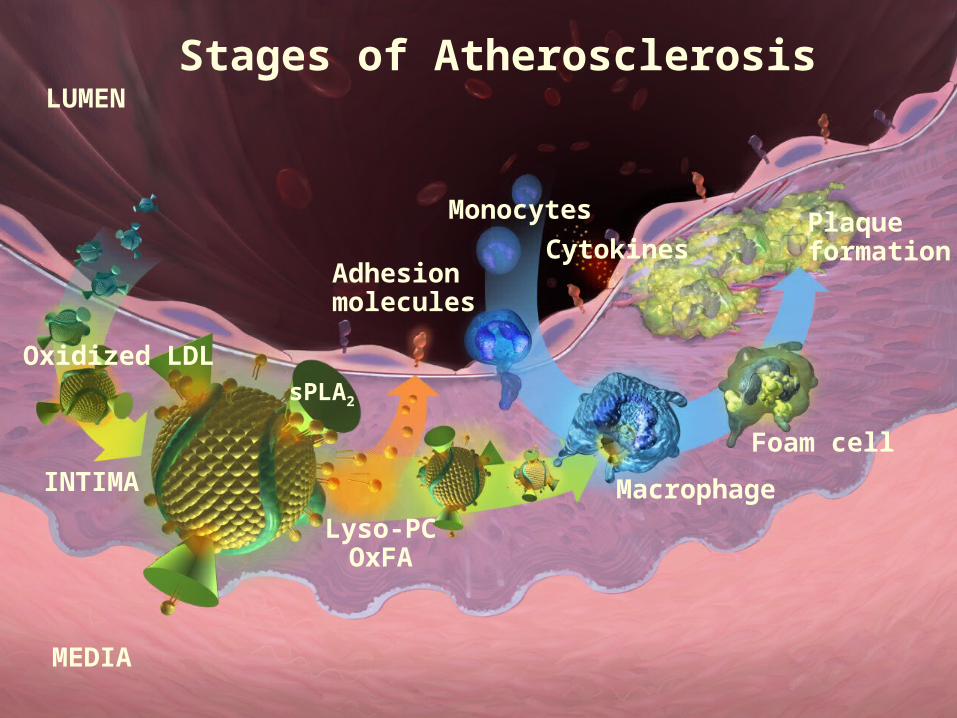
Stages of Atherosclerosis
LDL
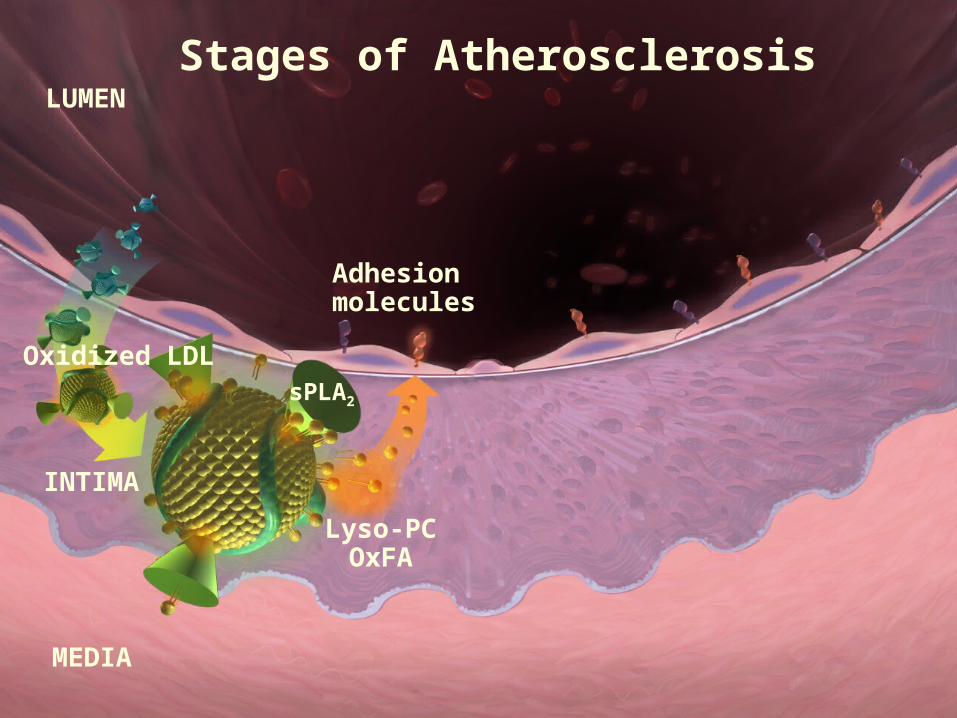
LUMEN
MEDIA
INTIMA
Oxidized LDL
Adhesion molecules
Lyso-PCOxFA
sPLA2
Stages of Atherosclerosis
LUMEN
MEDIA
INTIMA
Oxidized LDL
Adhesion molecules
Lyso-PCOxFA
sPLA2
Stages of Atherosclerosis
CytokinesPlaque formation
Foam cell
Monocytes
Macrophage
Stages of AtherosclerosisLUMEN
MEDIA
INTIMA
Oxidized LDL
Adhesion molecules
Lyso-PCOxFA
sPLA2
13
What is sPLA2?
• Family of Ca2+ dependent proteins
• Exact physiologic role in humans is not clearly known
• Type IIA is an acute phase protein secreted from liver in response to inflammatory cytokines
• Groups IIA, V, X have each been implicated in CVD
• All types cleave phospholipids at sn-2 position
• By generating intermediates acts as mediator between proximal and distal effectors of inflammation
sPLA2 levels increased with atherosclerotic development in human plaques
The extent of sPLA2s expression increased with atherosclerosis development.
Kimura-Matsumoto et al., Atherosclerosis, 196 (2008) 81–91
19
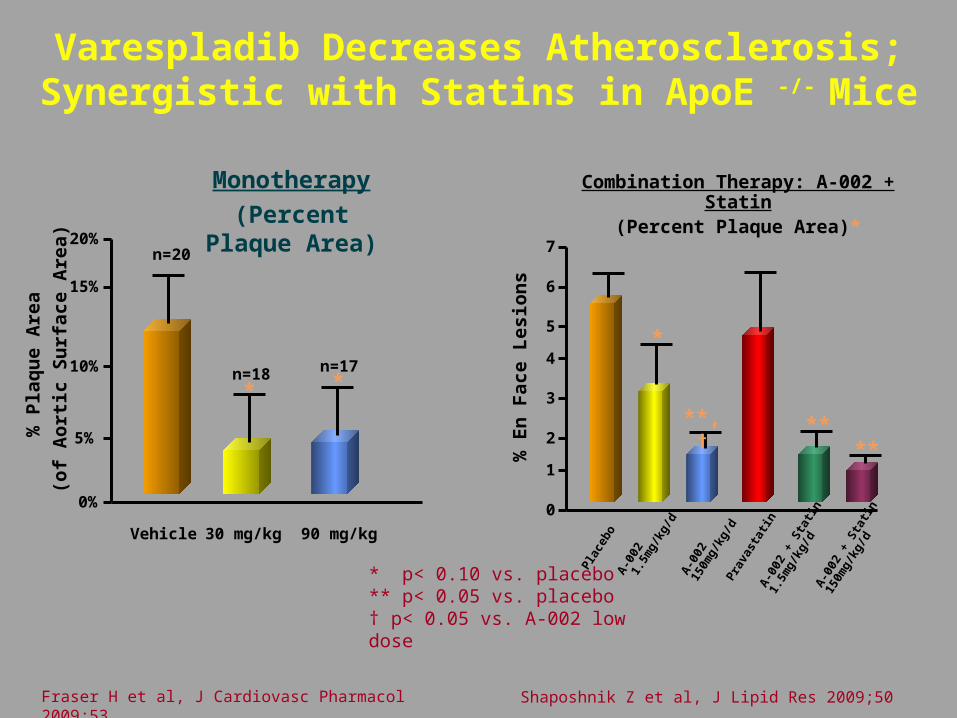
sPLA2 family plays a causal role in atherosclerosis
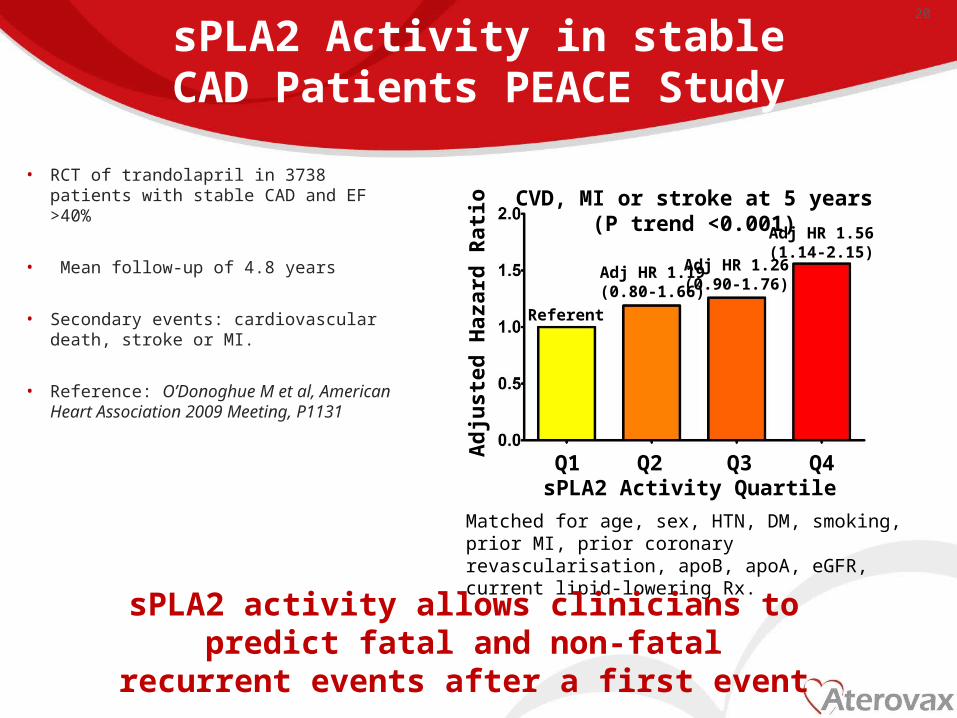
sPLA2 Activity in stable CAD Patients PEACE Study
• RCT of trandolapril in 3738 patients with stable CAD and EF >40%
• Mean follow-up of 4.8 years
• Secondary events: cardiovascular death, stroke or MI.
• Reference: O’Donoghue M et al, American Heart Association 2009 Meeting, P1131
20
Matched for age, sex, HTN, DM, smoking, prior MI, prior coronary revascularisation, apoB, apoA, eGFR, current lipid-lowering Rx.
sPLA2 activity allows clinicians to predict fatal and non-fatal recurrent events after a first event
Adj HR 1.19(0.80-1.66)
Adj HR 1.26(0.90-1.76)
Adj HR 1.56(1.14-2.15)
Referent
sPLA2 Activity QuartileA
djus
ted
Haz
ard
Rat
ioQ1 Q2 Q3 Q4
CVD, MI or stroke at 5 years(P trend <0.001)
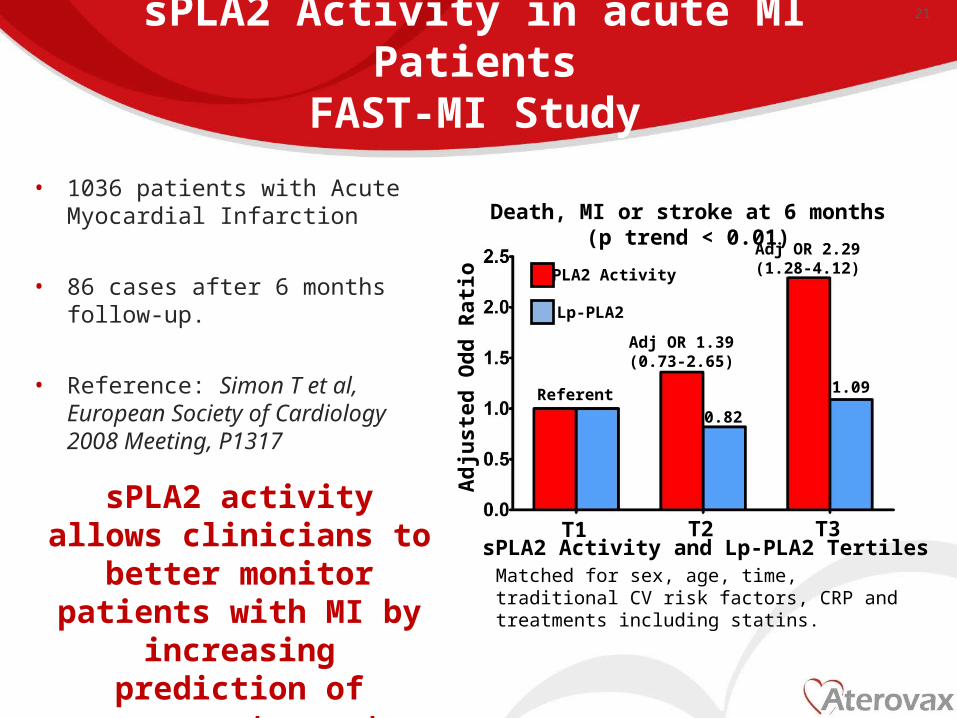
sPLA2 Activity in acute MI PatientsFAST-MI Study
• 1036 patients with Acute Myocardial Infarction
• 86 cases after 6 months follow-up.
• Reference: Simon T et al, European Society of Cardiology 2008 Meeting, P1317
21
Matched for sex, age, time, traditional CV risk factors, CRP and treatments including statins.
sPLA2 activity allows clinicians to better monitor patients with MI by increasing prediction of
recurrent event
Adj OR 1.39(0.73-2.65)
0.82
Adj OR 2.29(1.28-4.12)
Referent
sPLA2 Activity and Lp-PLA2 Tertiles
Adj
uste
d O
dd R
atio
T1 T2 T3
1.09
Lp-PLA2
sPLA2 Activity
Death, MI or stroke at 6 months(p trend < 0.01)
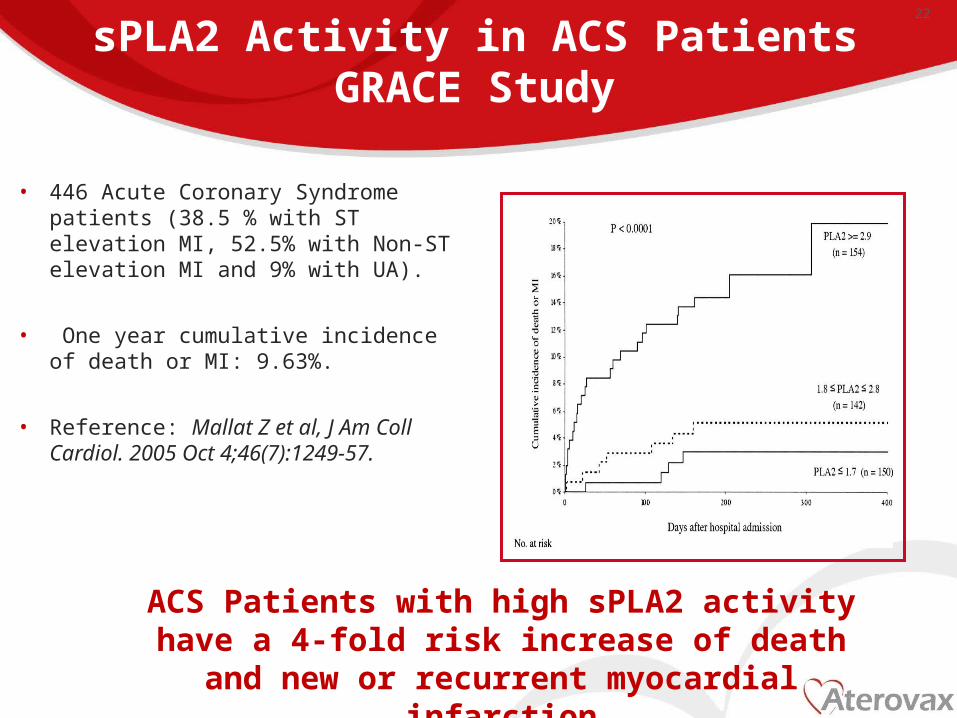
sPLA2 Activity in ACS PatientsGRACE Study
• 446 Acute Coronary Syndrome patients (38.5 % with ST elevation MI, 52.5% with Non-ST elevation MI and 9% with UA).
• One year cumulative incidence of death or MI: 9.63%.
• Reference: Mallat Z et al, J Am Coll Cardiol. 2005 Oct 4;46(7):1249-57.
22
ACS Patients with high sPLA2 activity have a 4-fold risk increase of death and new or recurrent myocardial infarction
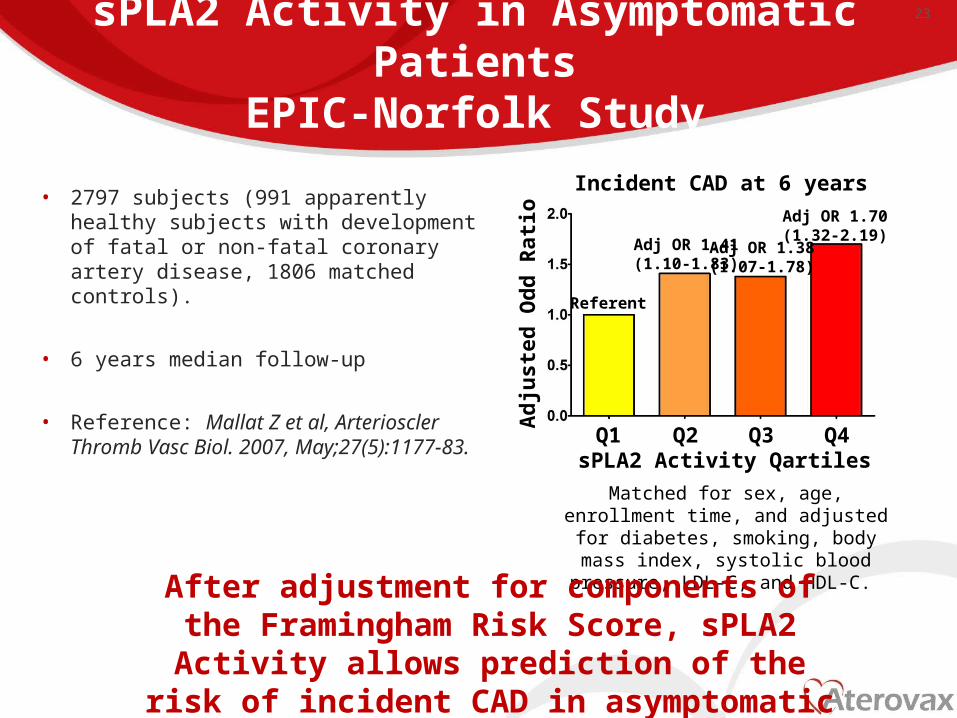
sPLA2 Activity in Asymptomatic PatientsEPIC-Norfolk Study
• 2797 subjects (991 apparently healthy subjects with development of fatal or non-fatal coronary artery disease, 1806 matched controls).
• 6 years median follow-up
• Reference: Mallat Z et al, Arterioscler Thromb Vasc Biol. 2007, May;27(5):1177-83.
23
Matched for sex, age, enrollment time, and adjusted for diabetes, smoking, body mass index, systolic
blood pressure, LDL-C, and HDL-C.
After adjustment for components of the Framingham Risk Score, sPLA2 Activity allows prediction of the risk of incident CAD in asymptomatic patients on top of FRS
Adj OR 1.41(1.10-1.83)
Adj OR 1.70(1.32-2.19)
Referent
sPLA2 Activity Qartiles
Adj
uste
d O
dd R
atio
Q1 Q2 Q3 Q4
Adj OR 1.38(1.07-1.78)
Incident CAD at 6 years
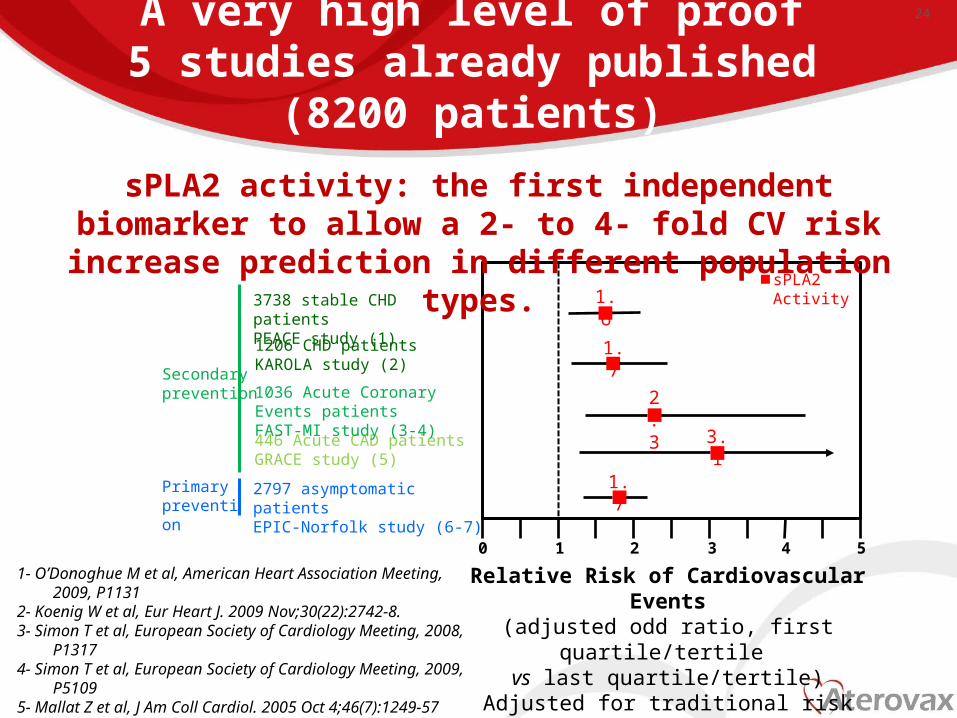
A very high level of proof5 studies already published (8200 patients)
Relative Risk of Cardiovascular Events(adjusted odd ratio, first quartile/tertile
vs last quartile/tertile)Adjusted for traditional risk factors, treatments and
biomarkers when available
0 1 2 3 4 5
sPLA2 Activity
3.1446 Acute CAD patientsGRACE study (5)
Primary prevention
Secondary prevention
2797 asymptomatic patientsEPIC-Norfolk study (6-7)
1.7
2.31036 Acute Coronary Events patientsFAST-MI study (3-4)
1.71206 CHD patientsKAROLA study (2)
1- O’Donoghue M et al, American Heart Association Meeting, 2009, P11312- Koenig W et al, Eur Heart J. 2009 Nov;30(22):2742-8.3- Simon T et al, European Society of Cardiology Meeting, 2008, P13174- Simon T et al, European Society of Cardiology Meeting, 2009, P51095- Mallat Z et al, J Am Coll Cardiol. 2005 Oct 4;46(7):1249-576- Mallat Z et al, Arterioscler Thromb Vasc Biol. 2007, May;27(5):1177-837- Tsimikas S et al, American Heart Association Meeting, 2008, P4998
sPLA2 activity: the first independent biomarker to allow a 2- to 4- fold CV risk increase prediction in different population types.
3738 stable CHD patientsPEACE study (1)
1.6
24
Multimarker Approach in Asymptomic Patients
EPIC-Norfolk Study
Mallat Z et al, Arterioscler Thromb Vasc Biol. 2007, May;27(5):1177-83.
Tsimikas S et al, American Heart Association 2008 Meeting, P4998.
25
OR=2.89(1.78-4.68)
Adj
uste
d O
dd R
atio
1
21 2 3
4
4
3
C-re
activ
e Pr
otei
n
In asymptomatic patients, sPLA2 activity allows a increased prediction of CV risk:• 3-fold higher risk combined with CRP• 4-fold higher risk combined with oxPL/apoB100
Both matched for sex, age, enrollment time, adjusted for diabetes, smoking, BMI, SBP, LDL-C
and HDL-C
1 23
sPLA2 ActivitysPLA2 Activity1
23
oxP
L/ap
oB
Ad
just
ed O
dd
Rat
io
OR=3.67 (2.38-5.65)
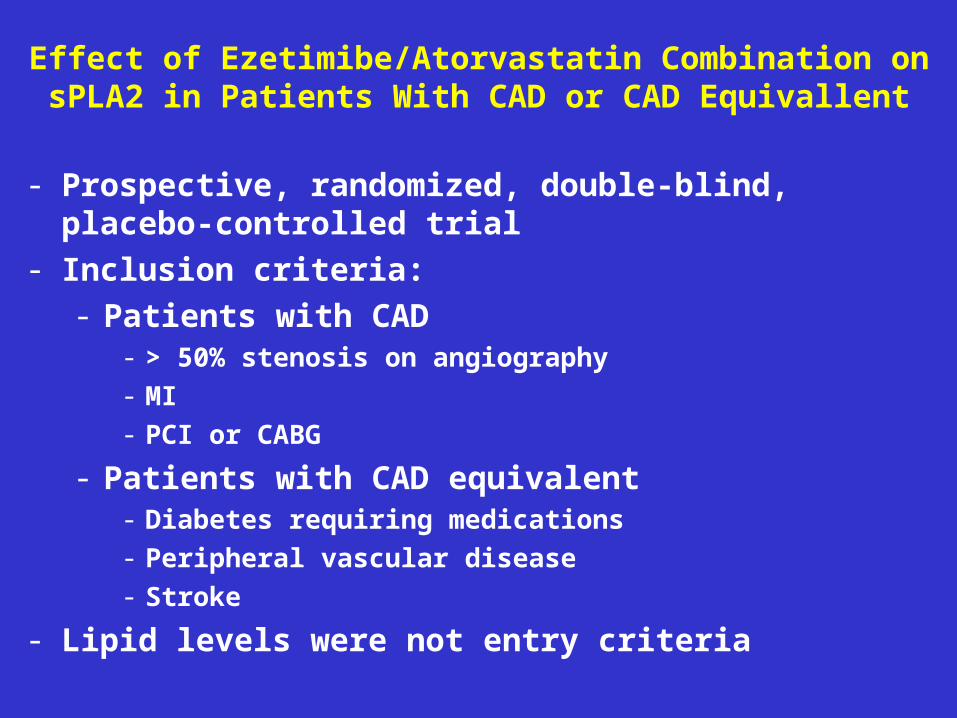
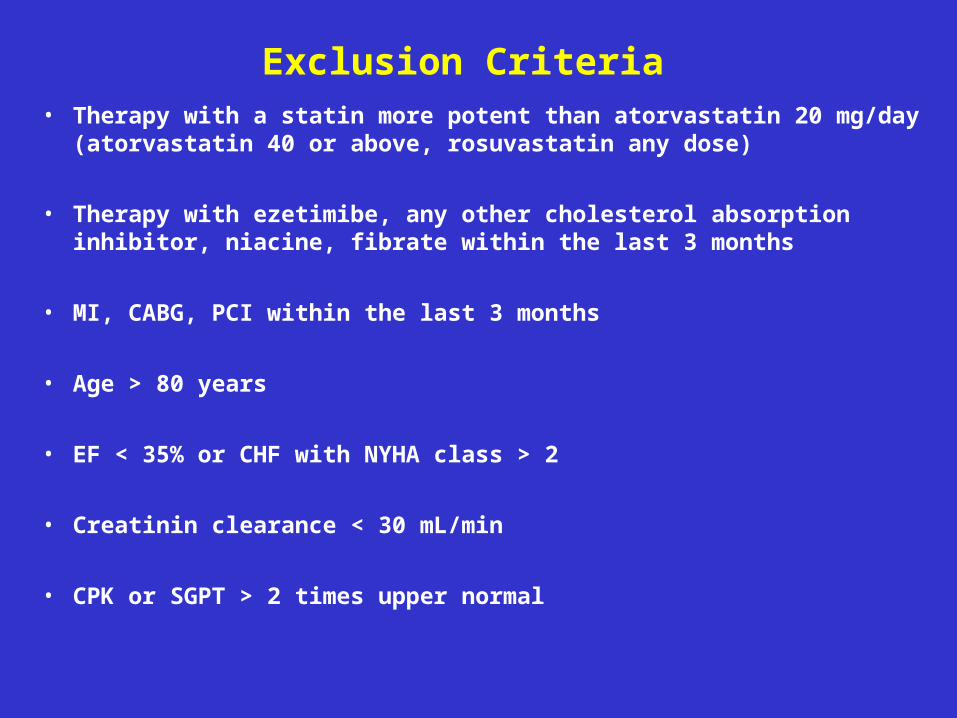
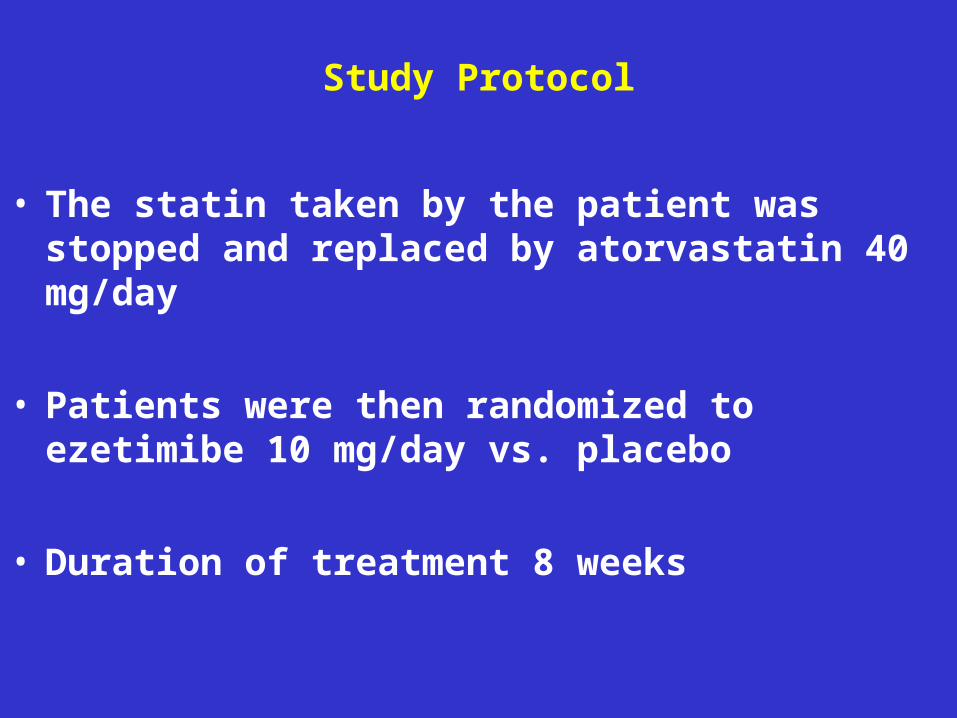
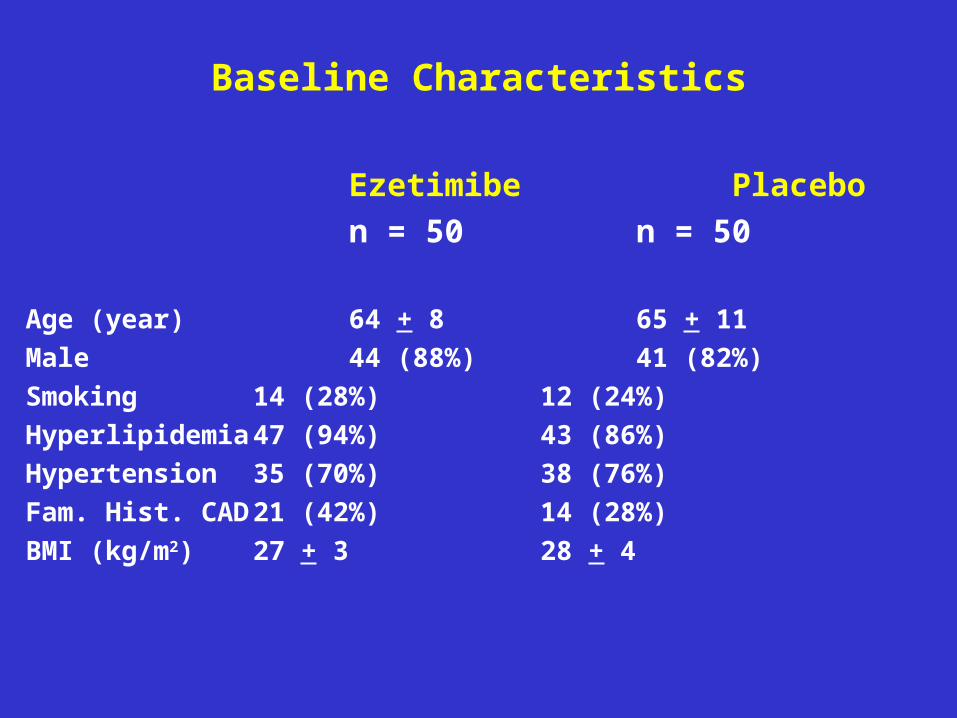
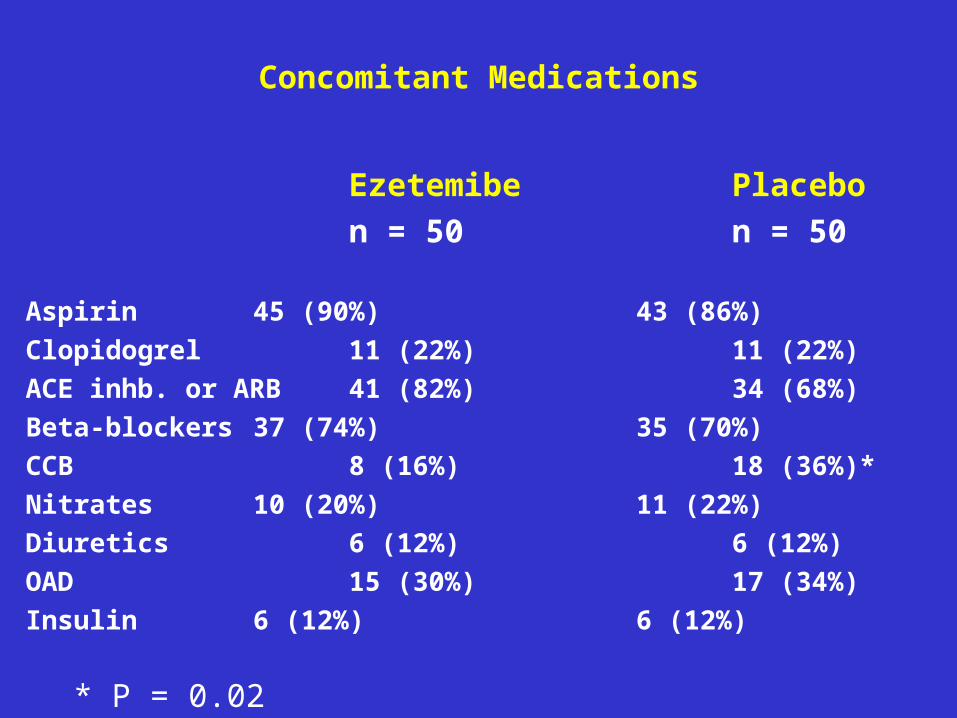
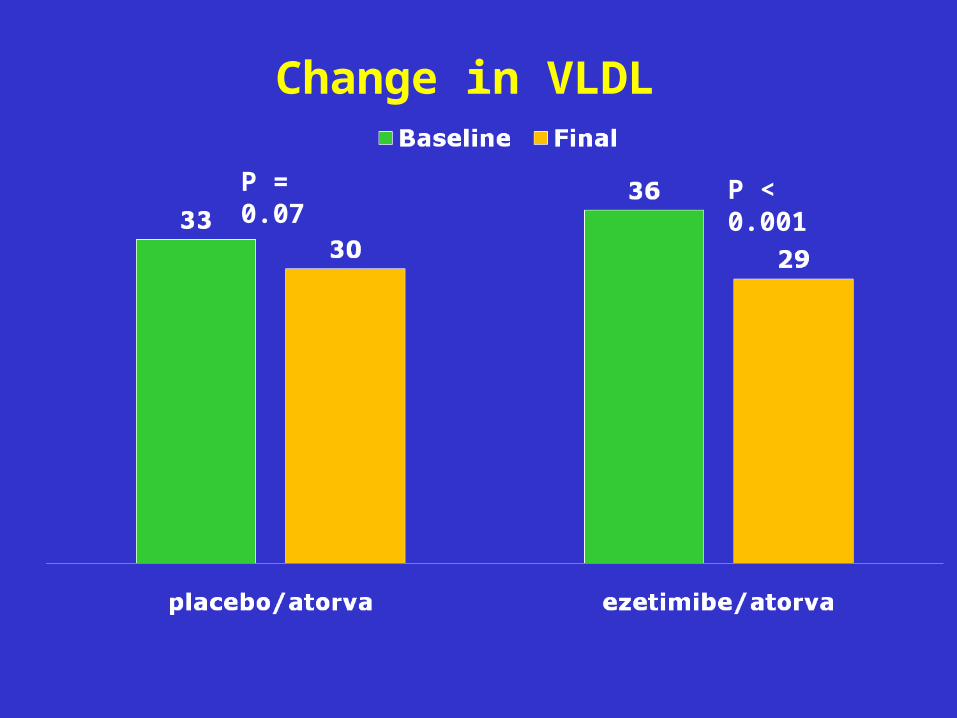
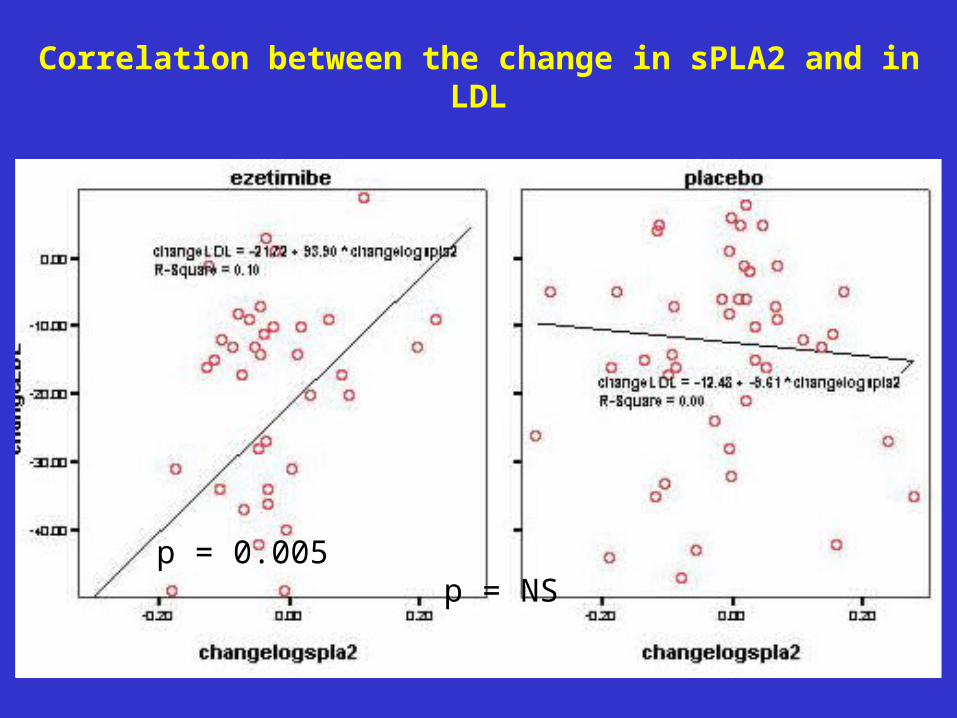
Effect of Ezetimibe/Atorvastatin Combination on sPLA2 in Patients With
CAD or CAD Equivallent
Mireille Azar, Emmanuel Valentin, Georges Badaoui, Roland Kassab, Antoine Sarkis, and
Rabih Azar
• Am J Cardiol May 2011 (manuscript)
• Sponsored by Pharmaline
OBJECTIVE
TO EVALUATE THE EFFECT OF ATORVASTATIN 40 mg and of
ATORVASTATIN 40 mg + EZETIMIBE ON sPLA2
Slide 28
DIETARY CHOLESTEROL
BILIARY SECRETION
INTESTINE
Excretion
VLDL LDL
Absorption
synthesis
IDL
Statins
CholesterolAbsorptionInhibition
Endogenous
Endogenous
Exogenous
Exogenous
Cholesterol Absorption Inhibition for Broader Lipid Cholesterol Absorption Inhibition for Broader Lipid ControlControl
Slide 29
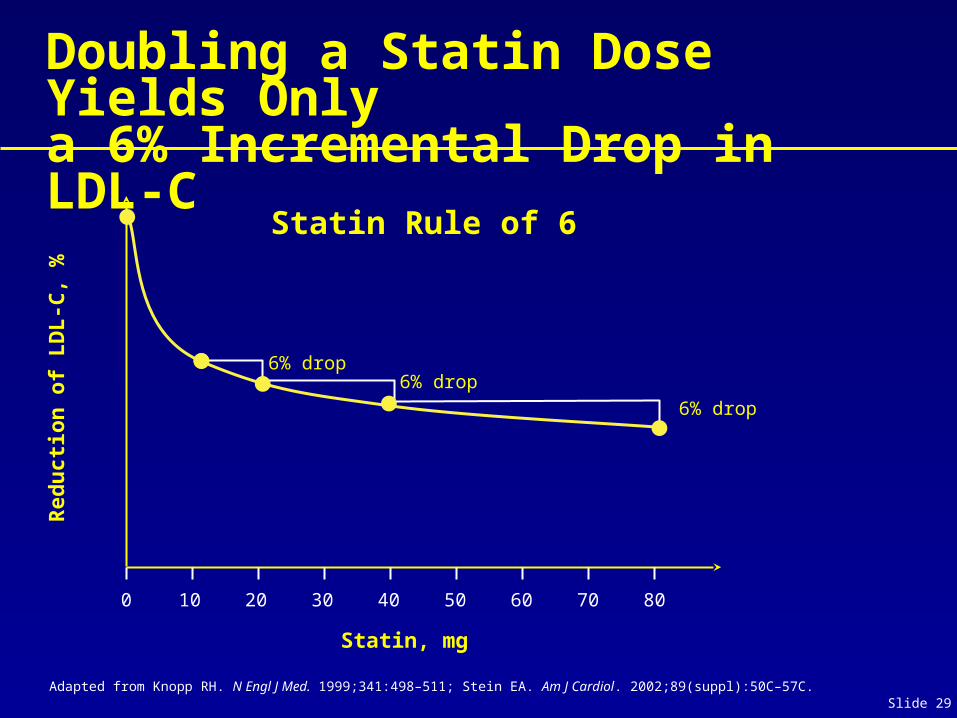
Doubling a Statin Dose Yields Only
a 6% Incremental Drop in LDL-C
Adapted from Knopp RH. N Engl J Med. 1999;341:498–511; Stein EA. Am J Cardiol. 2002;89(suppl):50C–57C.
0 10 30 50 80
Statin, mg
Red
uct
ion
of
LD
L-C
, %
Statin Rule of 6
20 40 7060
6% drop
6% drop6% drop
Slide 30
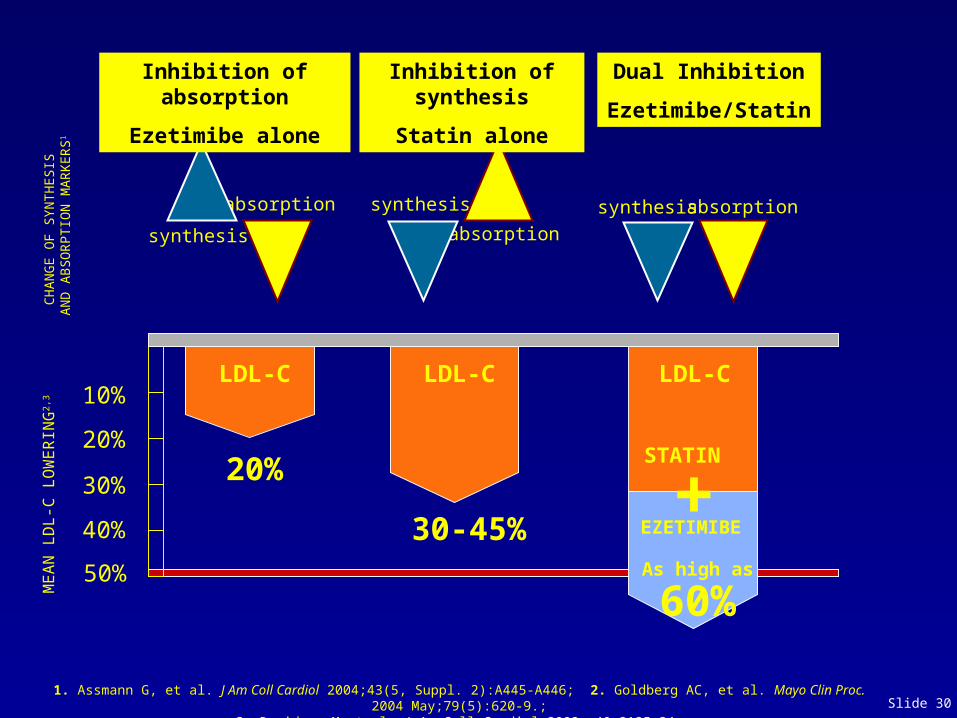
LDL-C LDL-C LDL-C
20%
30-45%
STATIN
+As high as
60%
10%
20%
30%
40%
50%
ME
AN
LD
L-C
LO
WE
RIN
G2,
3
synthesis absorptionsynthesis
absorptionsynthesis
absorption
1. Assmann G, et al. J Am Coll Cardiol 2004;43(5, Suppl. 2):A445-A446; 2. Goldberg AC, et al. Mayo Clin Proc. 2004 May;79(5):620-9.;3. Davidson M et al. J Am Coll Cardiol 2002; 40:2125-34.
CH
AN
GE
OF
SYN
TH
ESI
S A
ND
AB
SOR
PTIO
N M
AR
KE
RS1
Inhibition of absorption
Ezetimibe alone
Inhibition of synthesis
Statin alone
EZETIMIBE
Dual Inhibition
Ezetimibe/Statin
Effect of Ezetimibe/Atorvastatin Combination on sPLA2 in Patients With CAD or CAD Equivallent
There was no elevation of CPK or SGPT in any patient of the 2
groups
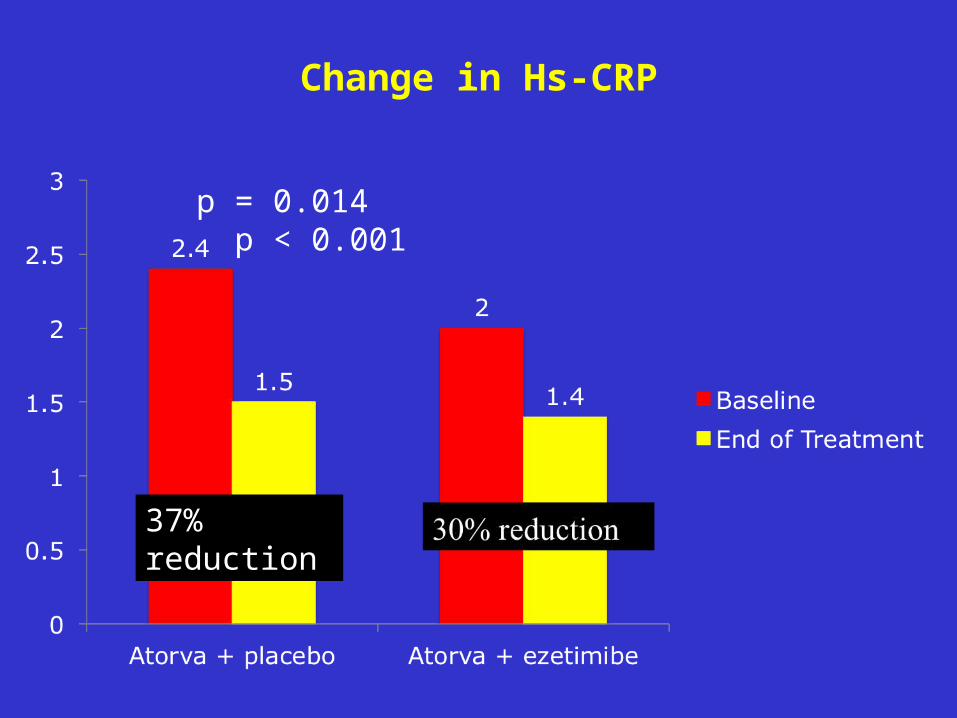
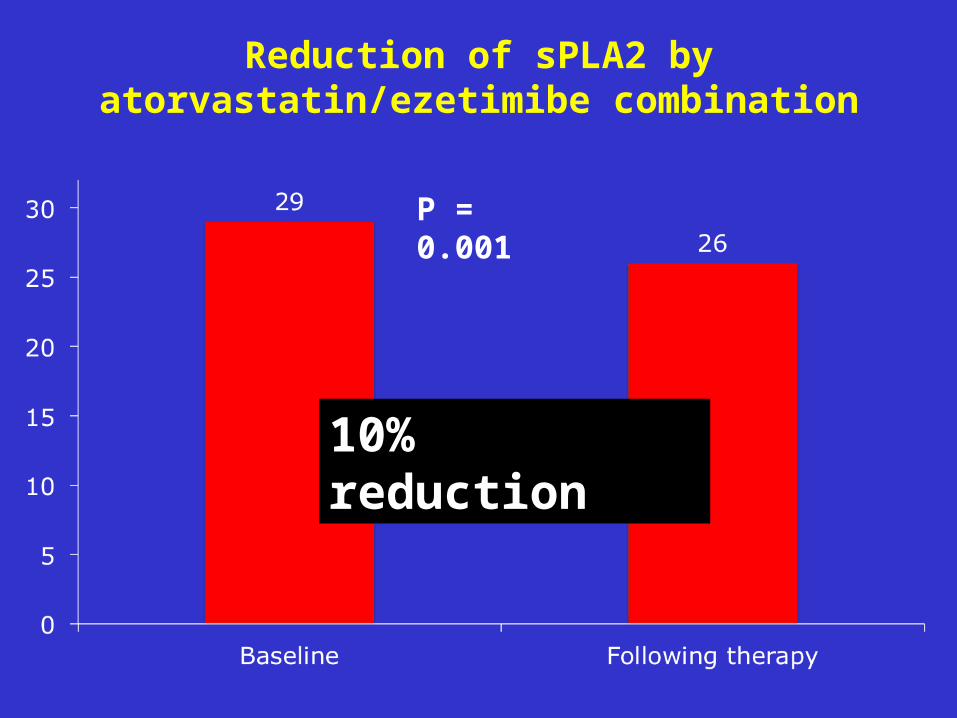
Major Findings of the Study
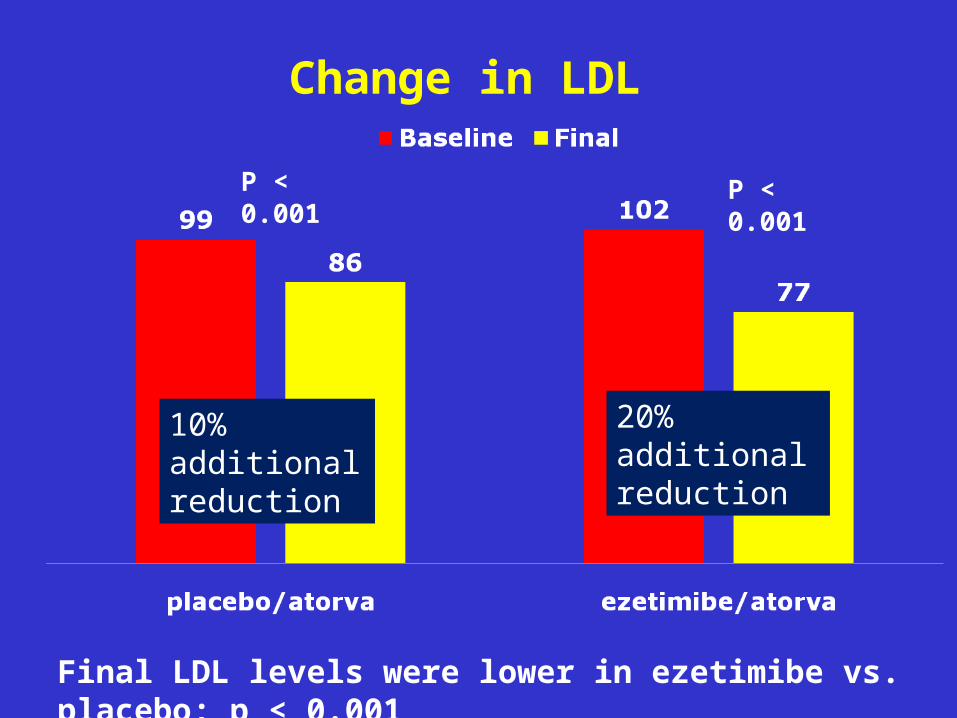
• First to demonstrate a reduction in sPLA2 with lipid lowering therapy
• Effect was weak: 10% reduction
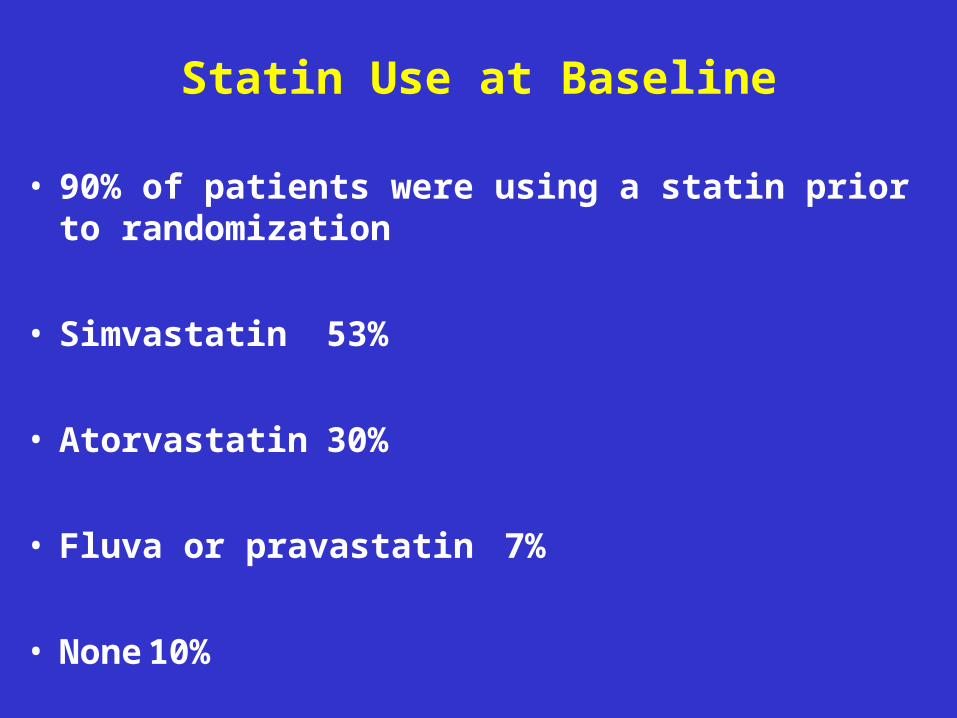
• Low LDL level at baseline. If LDL was higher, reduction might have been more potent
• Cannot exclude that statins do not decrease sPLA2, because 90% of our patients were on statin at baseline and because statins decrease both LDL and hs-CRP
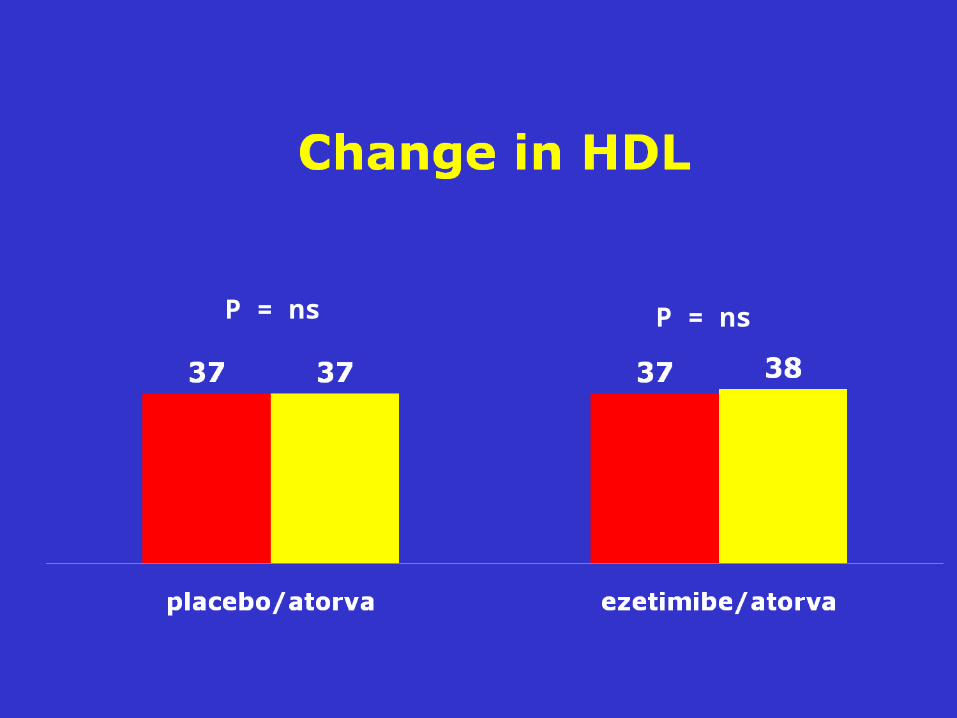
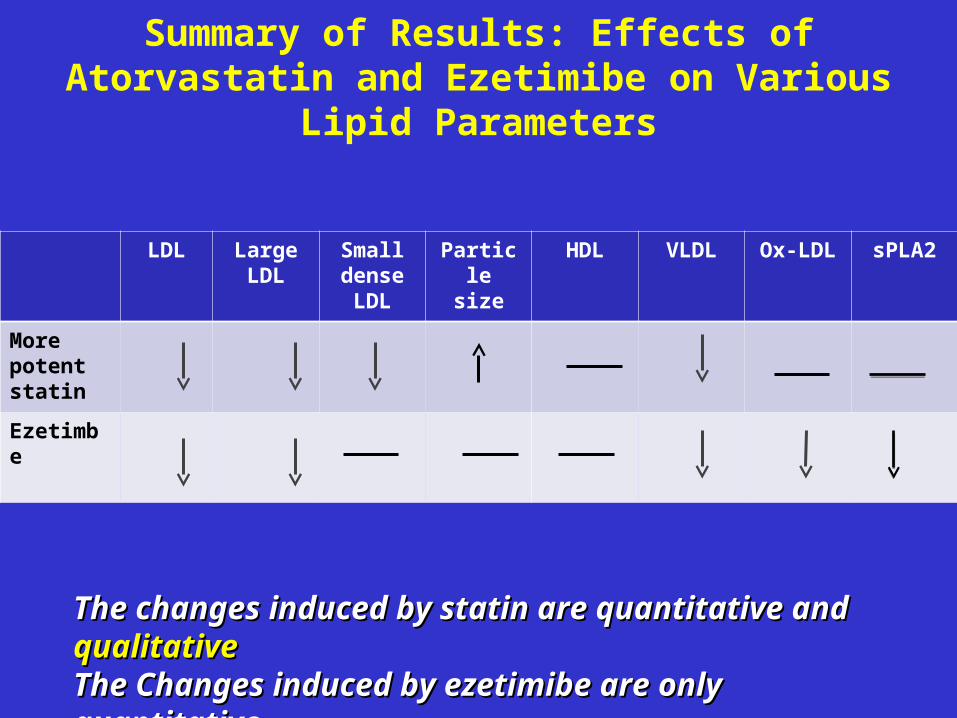
Summary of Results: Effects of Atorvastatin and Ezetimibe on Various
Lipid Parameters
LDL Large LDL
Small dense LDL
Particle size
HDL VLDL Ox-LDL sPLA2
More potent statin
Ezetimbe
The changes induced by statin are quantitative and The changes induced by statin are quantitative and qualitativequalitativeThe Changes induced by ezetimibe are only quantitativeThe Changes induced by ezetimibe are only quantitative
Enhance-Study
Kastelein et al., NEJM 2008, 358: 1431-43
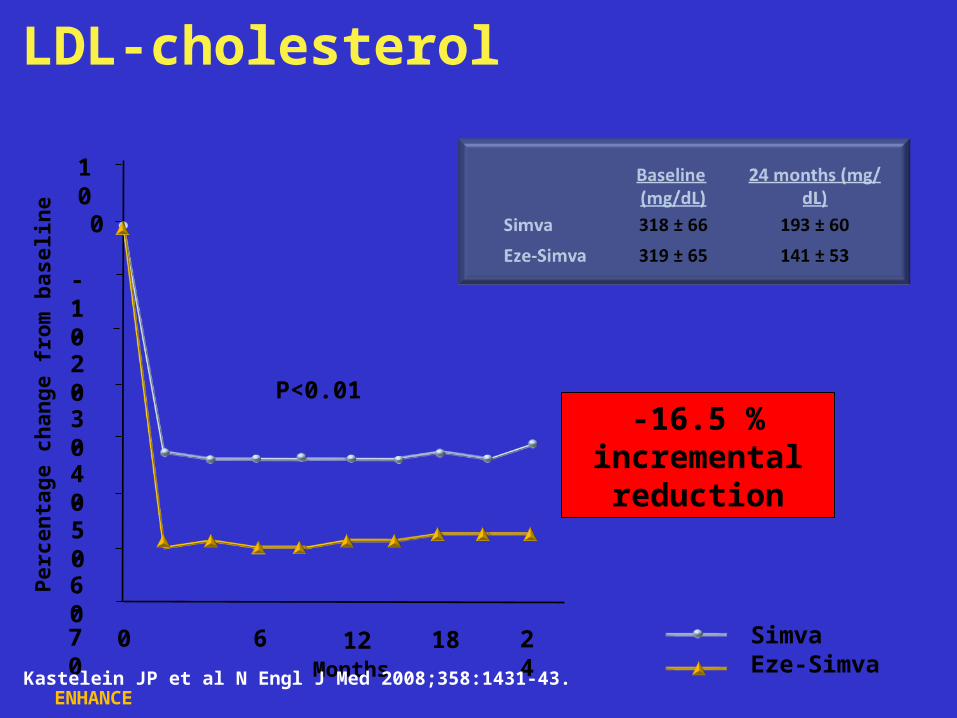
Months
LDL-cholesterol
ENHANCE
SimvaEze-Simva
-40
0 6 12 18 24
-50-60-70
0
-10-20-30
10
Perc
enta
ge c
hang
e fr
om b
asel
ine
P<0.01-16.5 %
incremental reduction
Kastelein JP et al N Engl J Med 2008;358:1431-43.
Slide 55
Mean cIMT during 24 months of therapyLongitudinal, repeated measures analysis
ENHANCE
Mea
n IM
T (m
m)
SimvaEze-Simva
6 12 18 240.60
0.70
0.75
0.80
0.65
Months
P=0.88
Kastelein JP et al N Engl J Med 2008;358:1431-43.
Slide 56
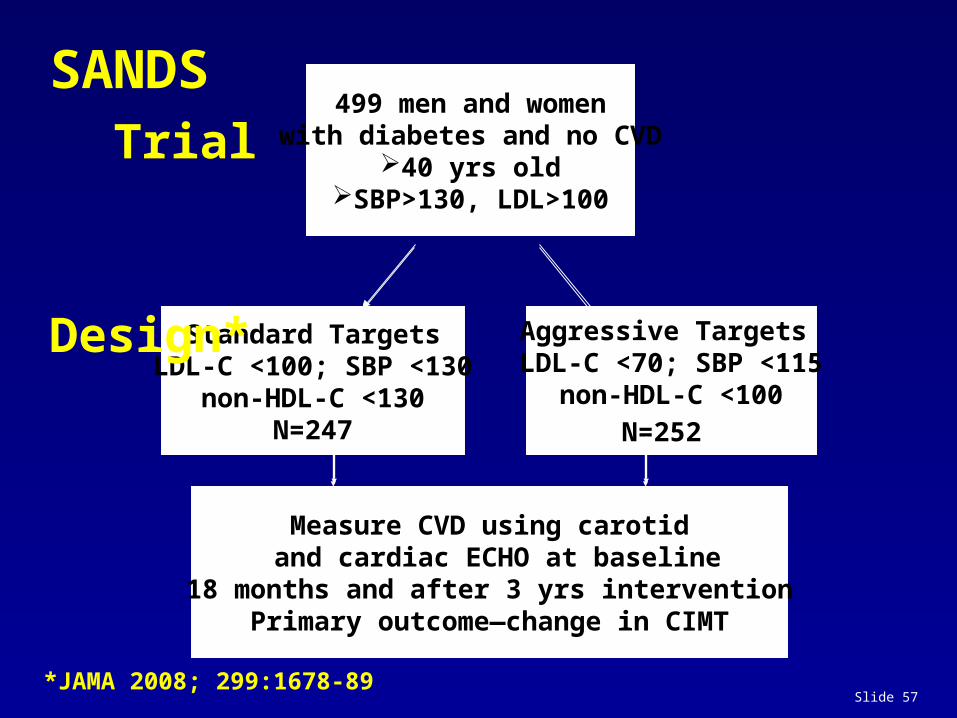
SANDS-Study
Fleg et al., JACC 2008; 52
Slide 57
499 men and womenwith diabetes and no CVD
40 yrs oldSBP>130, LDL>100
Standard TargetsLDL-C <100; SBP <130
non-HDL-C <130N=247
Aggressive Targets LDL-C <70; SBP <115
non-HDL-C <100
N=252
Measure CVD using carotid and cardiac ECHO at baseline
18 months and after 3 yrs interventionPrimary outcome—change in CIMT
SANDS Trial Design*
*JAMA 2008; 299:1678-89
Slide 58
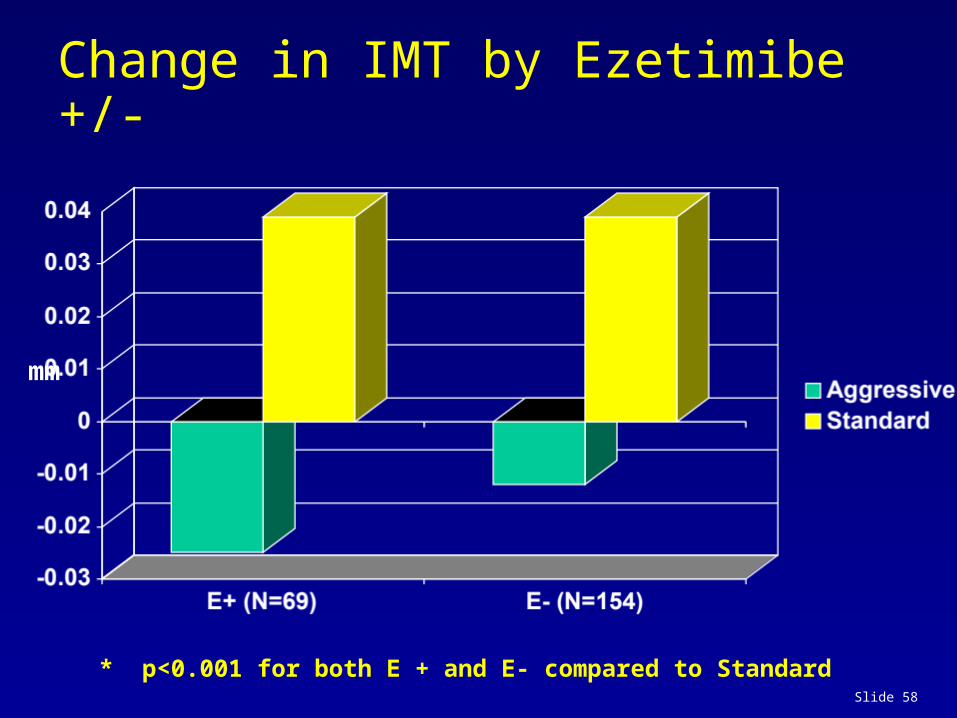
Change in IMT by Ezetimibe +/-
* p<0.001 for both E + and E- compared to Standard
mm
nhlbihelp
Need p values.
Slide 59
The results of the Study of Heart and Renal Protection (SHARP)
Colin Baigent, Martin Landray on behalf of the SHARP Investigators
Disclosure: SHARP was sponsored, designed, run, and analysed by the University of Oxford. Funding was received from Merck, the UK MRC, British Heart Foundation, and
Australian NHMRC.
Slide 60
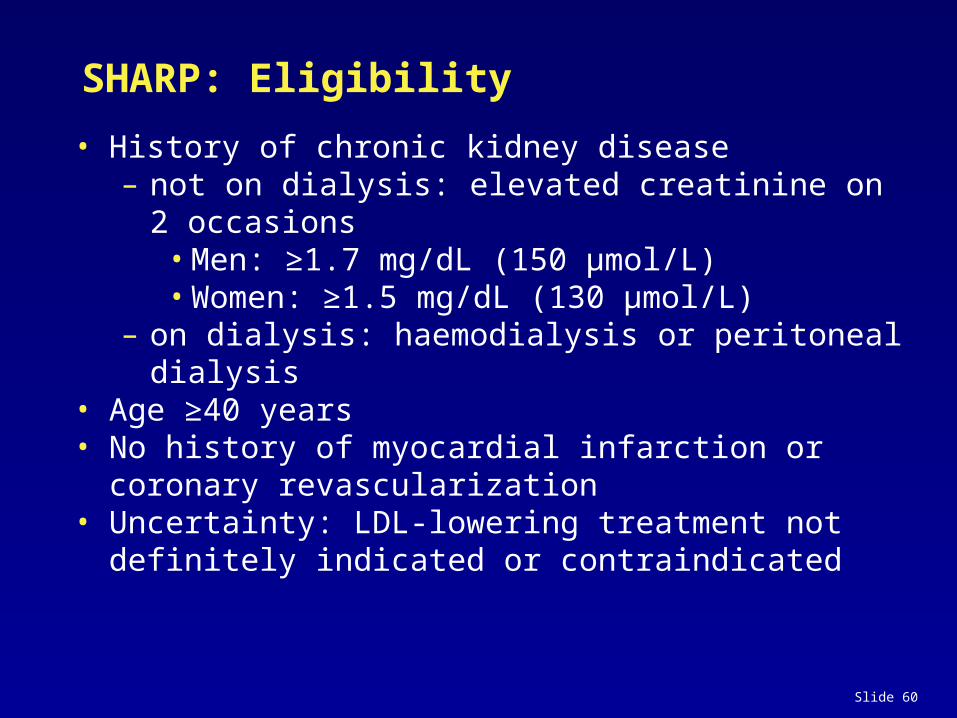
SHARP: Eligibility
• History of chronic kidney disease– not on dialysis: elevated creatinine on 2 occasions
– on dialysis: haemodialysis or peritoneal dialysis• Age ≥40 years• No history of myocardial infarction or coronary
revascularization• Uncertainty: LDL-lowering treatment not definitely
indicated or contraindicated
Slide 61
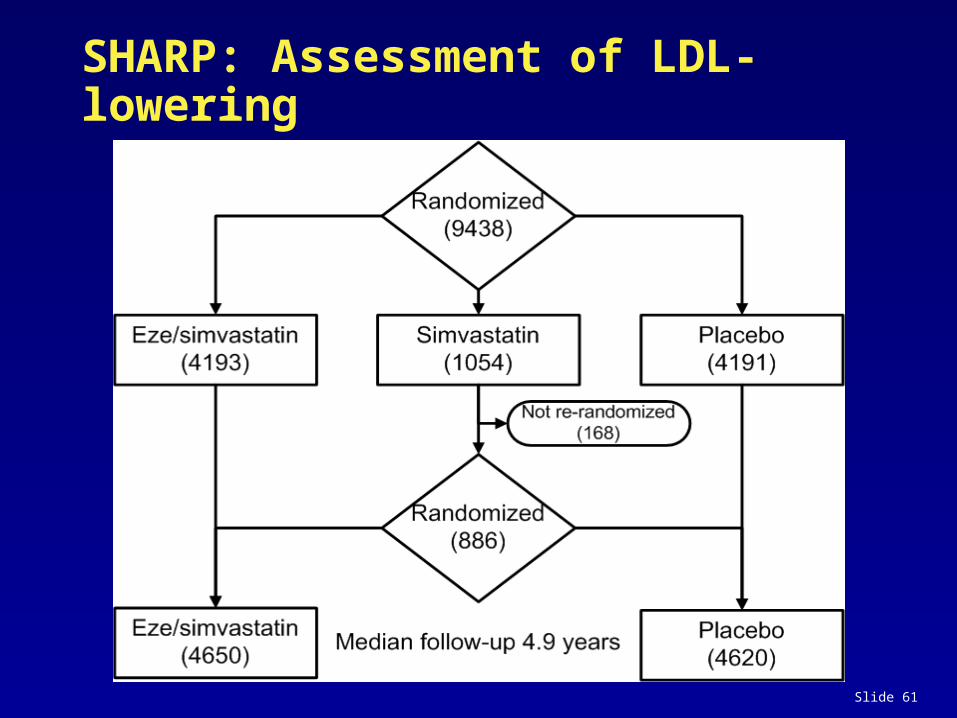
SHARP: Assessment of LDL-lowering
Slide 62
0 1 2 3 4 5
Years of follow-up
0
5
10
15
20
25
Prop
ortio
n su
fferin
g ev
ent (
%) Risk ratio 0.83 (0.74 – 0.94)
Logrank 2P=0.0022 Placebo
Eze/simv
SHARP: Major Atherosclerotic Events
Slide 63
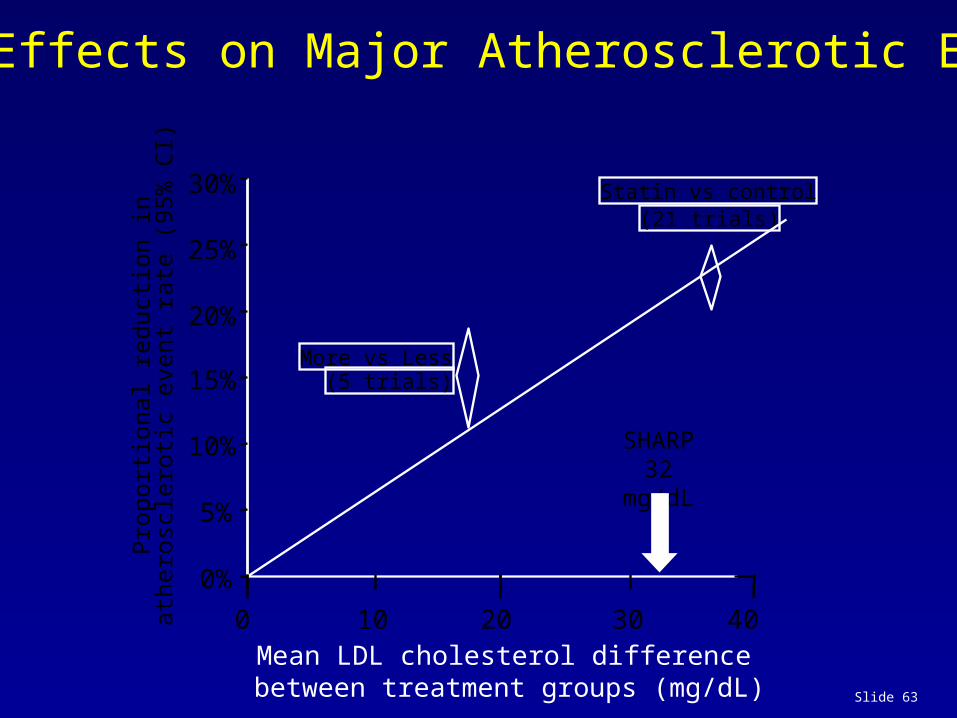
CTT: Effects on Major Atherosclerotic Events
Prop
ortio
nal r
educ
tion
inat
hero
scle
rotic
eve
nt ra
te (9
5% C
I)
0%
5%
10%
15%
20%
25%
30% Statin vs control(21 trials)
Mean LDL cholesterol differencebetween treatment groups (mg/dL)
More vs Less(5 trials)
SHARP32 mg/dL
0 20 4010 30
Slide 64
Prop
ortio
nal r
educ
tion
inat
hero
scle
rotic
eve
nt ra
te (9
5% C
I)
0%
5%
10%
15%
20%
25%
30% Statin vs control(21 trials)
Mean LDL cholesterol differencebetween treatment groups (mg/dL)
More vs Less(5 trials)
SHARP32 mg/dL
0 20 4010 30
SHARP17% risk reduction
CTT: Effects on Major Atherosclerotic Events
Varespladib: a New and Potent sPLA2 Inhibitor
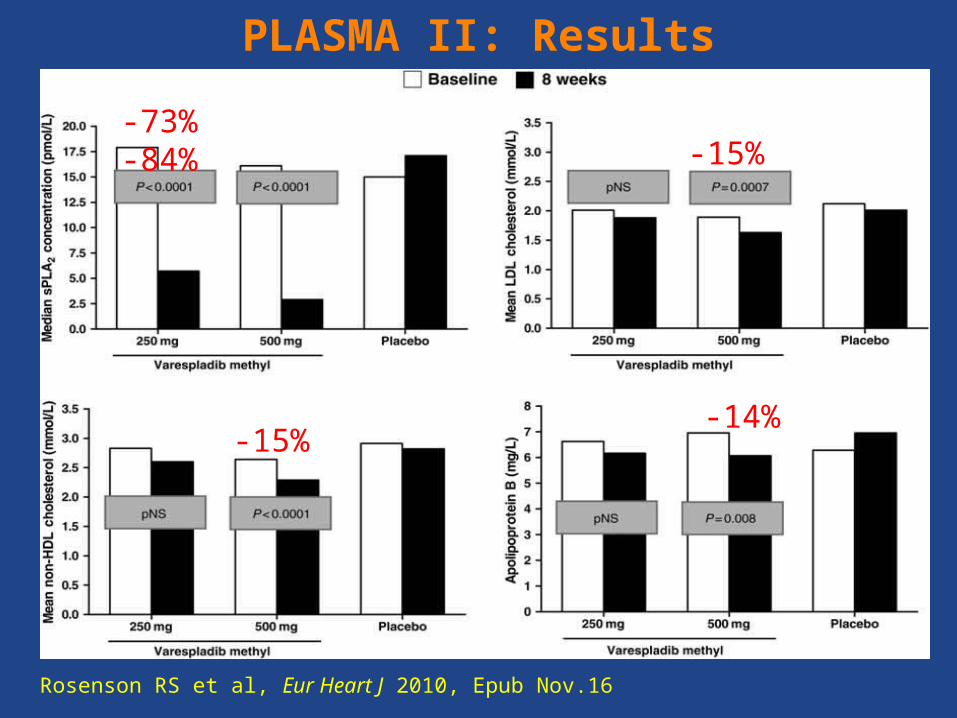
PLASMA II
• 135 patients with stable CHD randomized to 8 weeks of therapy
with placebo, varespladib 250 or 500 mg/day
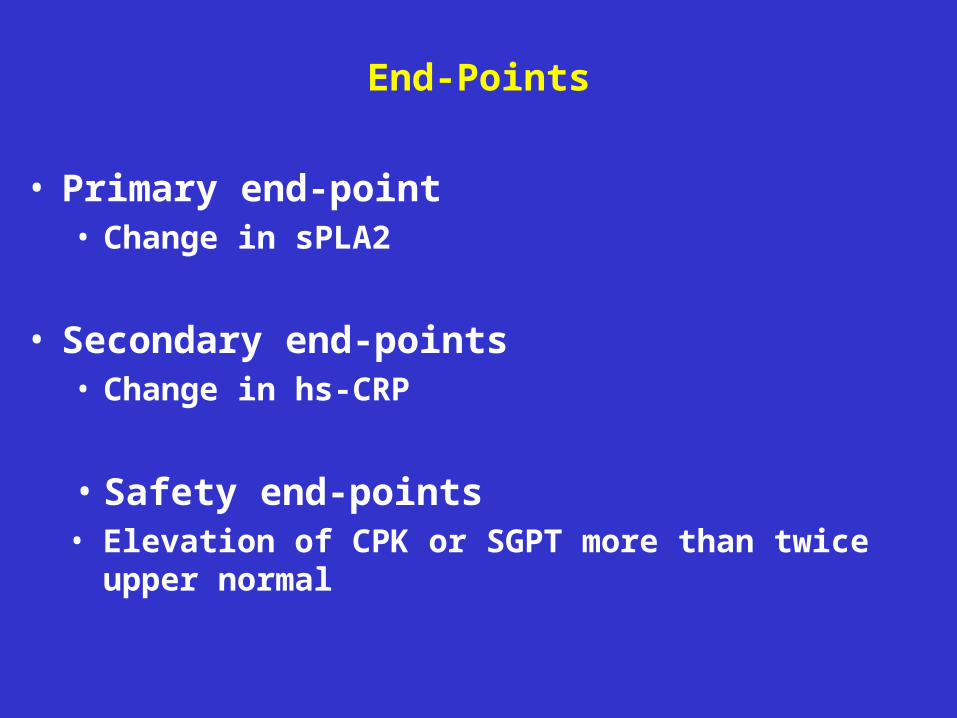
• primary endpoint was change in sPLA2-IIA concentration
between placebo and varespladib groups
• The 2 doses of varespladib lowered sPLA2 by 73% and 84%
respectively (p<0.0001)
• compared with placebo, varespladib 500 mg reduced LDL-C by
15% (p<0.001), non-HDL-C by 15% (p<0.001), total VLDL
particle concentration by 14% (p=0.022), and small VLDL
particle concentration by 24% (p=0.030)
Rosenson RS et al, Eur Heart J 2010, epub Nov.16
PLASMA II: Results
Rosenson RS et al, Eur Heart J 2010, Epub Nov.16
-73% -84%-15%
-15%-14%
69
FRANCIS-ACS Trial: Safety and Efficacy of Varespladib in Acute Coronary SyndromesFRANCIS-ACS Trial: Safety and Efficacy of Varespladib in Acute Coronary Syndromes
625 Patients• Men/Women
• Unstable Angina, NSTEMI or STEMI
• Any one of
• Diabetes
• CRP ≥2 mg/L
• Met. syndrome
• Randomized within 96 hours of event
Varespladib 500mg QD + Atorvastatin 80mg QD
Placebo + Atorvastatin 80mg QD
Rosenson RS et al, J Am Coll Cardiol 2010;56:1079-88
Primary End Point at 8 wks LDL-C hs-CRP sPLA2 concentration
Secondary End Points Occurrence of MACEs for treatment-
related trends at study completion.
6 Month Minimum Treatment Period
70
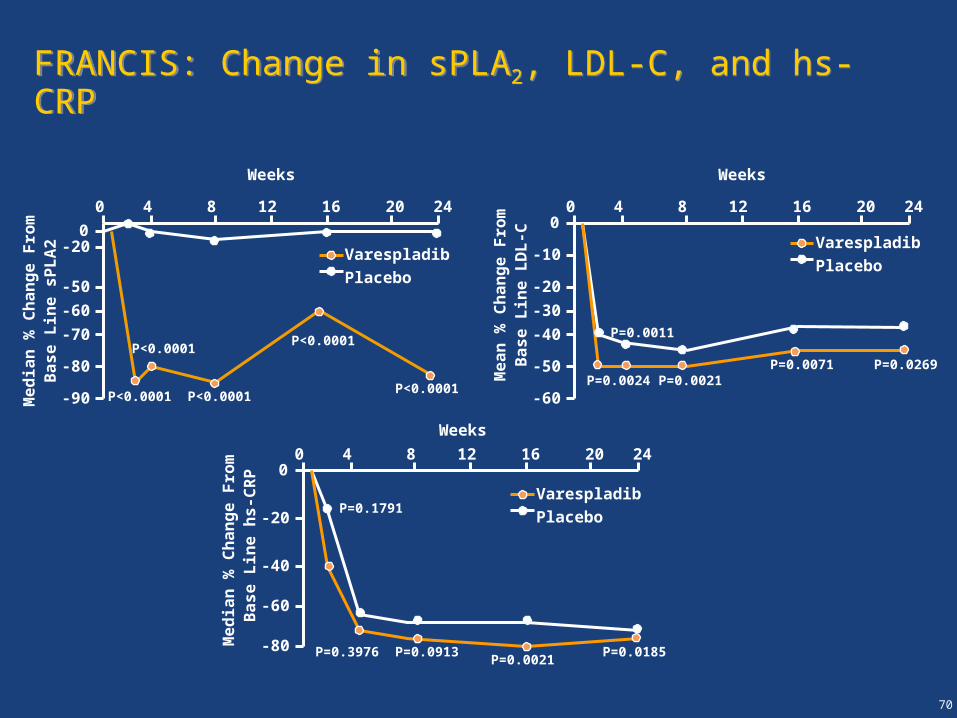
FRANCIS: Change in sPLA2, LDL-C, and hs-CRPFRANCIS: Change in sPLA2, LDL-C, and hs-CRP
0
0 4 8 12 16 20 24
-20
-50
-60
-70
-80
-90Me
dia
n %
Ch
an
ge
Fro
m B
as
e L
ine
sP
LA
2
00 4 8 12 16 20 24
-10
-20
-30
-40
-50
-60
Me
an
% C
ha
ng
e F
rom
Ba
se
Lin
e L
DL
-C
Weeks Weeks
Varespladib
Placebo
Varespladib
Placebo
P<0.0001
P<0.0001
P<0.0001
P<0.0001
P<0.0001P=0.0024
P=0.0011
P=0.0021P=0.0071 P=0.0269
00 4 8 12 16 20 24
-20
-40
-60
-80
Me
dia
n %
Ch
an
ge
Fro
m B
as
e L
ine
hs
-CR
P
Varespladib
Placebo
Weeks
P=0.1791
P=0.3976 P=0.0913P=0.0021
P=0.0185
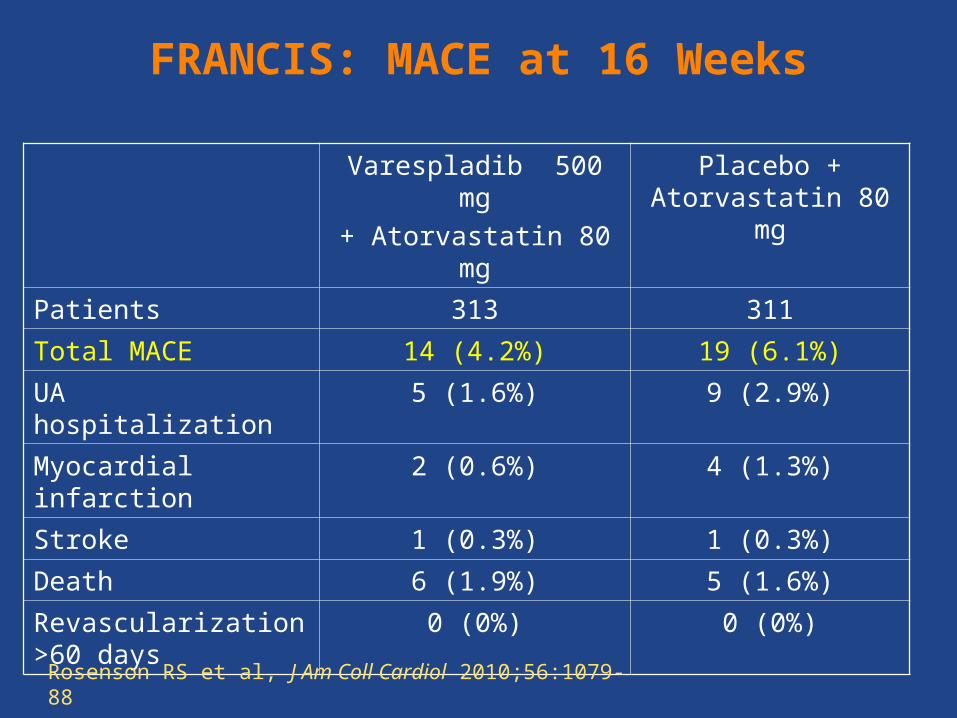
FRANCIS: MACE at 16 Weeks
Varespladib 500 mg
+ Atorvastatin 80 mg
Placebo + Atorvastatin 80 mg
Patients 313 311
Total MACE 14 (4.2%) 19 (6.1%)
UA hospitalization 5 (1.6%) 9 (2.9%)
Myocardial infarction 2 (0.6%) 4 (1.3%)
Stroke 1 (0.3%) 1 (0.3%)
Death 6 (1.9%) 5 (1.6%)
Revascularization >60 days
0 (0%) 0 (0%)
Rosenson RS et al, J Am Coll Cardiol 2010;56:1079-88
72
Acute Coronary Syndrome
Patient1
(STEMI, NSTEMI, UA)
Patient Screening
Interventional procedures if
necessary
Patient Randomization
< 96 hours< 96 hours
Varespladib + Atorvastatin
Placebo + Atorvastatin
16 week treatment 16 week
treatment 6 Months6 Months
Primary Endpoint
MACE
Survival Status
1As per FDA Guidance Major Adverse Coronary Events (MACE) are defined as Cardiovascular Death, Non-Fatal Myocardial Infarction, Non-Fatal Stroke, and Unstable Angina requiring urgent
hospitalization
VVascular ascular IInflammation nflammation SSuppression to uppression to TTreat reat AAcute Coronary Syndrome (VISTA-16)cute Coronary Syndrome (VISTA-16)
VVascular ascular IInflammation nflammation SSuppression to uppression to TTreat reat AAcute Coronary Syndrome (VISTA-16)cute Coronary Syndrome (VISTA-16)
Conclusions
• sPLA2 plays an important role in atherosclerosis and is an independent marker of future cardiovascular events
• We demonstrated for the first time that combination of statin/ezetimibe lowers sPLA2
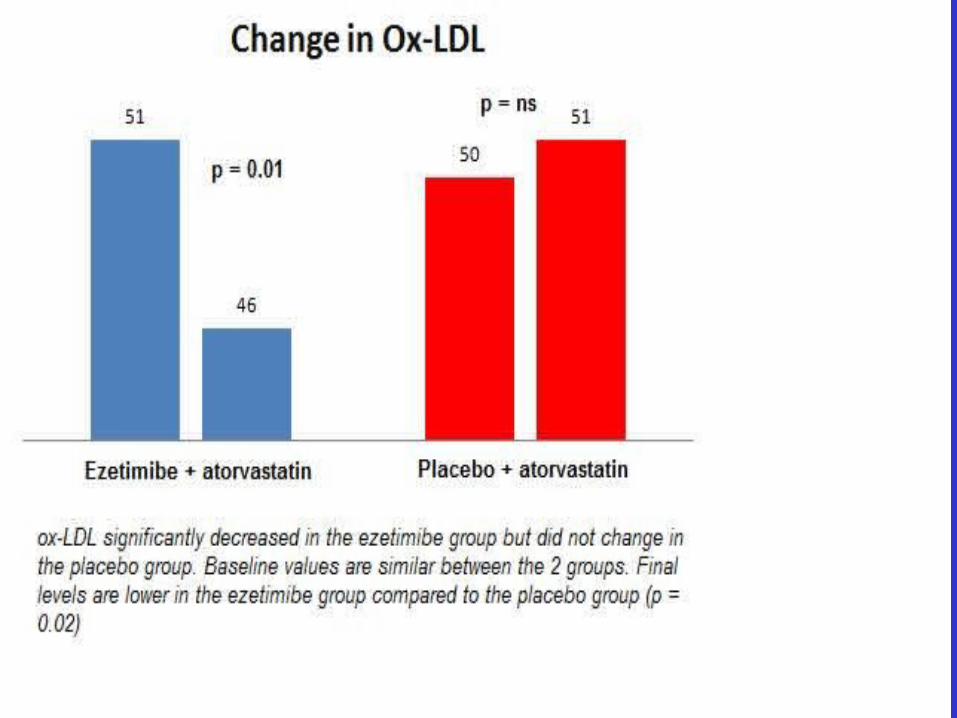
• In patients with stable CAD, increasing the potency of statin to atorvastatin 40 and adding ezetimibe is safe and results in effects that go beyond LDL lowering: decrease in small dense LDL, decrease in oxidized LDL, decrease in CRP and decrease in sPLA2
• Potent and specific inhibitors of sPLA2 are currently available
• Whether inhibiting sPLA2 is clinically beneficial is awaiting the result of the on-going VISTA-16 trial